Triple Therapy: A review of the evidence in acute coronary syndrome. Stephanie Kling, PharmD, BCPS Sanford Health
|
|
|
- Piers Hunter
- 5 years ago
- Views:
Transcription
1 Triple Therapy: A review of the evidence in acute coronary syndrome Stephanie Kling, PharmD, BCPS Sanford Health
2 Objectives 1. Describe how the presented topic impacts patient outcomes. 2. Review evidence based guidelines and best practices described. 3. Identify two clinical endpoints of the presented topic. 4. Recommend therapeutic means to achieve clinical endpoints.
3 Outline Background Current Literature Warfarin within TT NOAC within TT Ticagrelor/Prasugrel within TT Future studies
4 Aspirin Anticoagulant P2Y12 inhibitor
5 Abbreviations TT= triple therapy PCI= percutaneous coronary intervention MACCE= major adverse cardiovascular and cerebrovascular events MI= myocardial infarction CABG= coronary artery bypass graft NOAC= novel oral anticoagulant BARC = bleeding academic research consortium TIMI= thrombolysis in myocardial infarction GUSTO= global use of strategies to open occluded arteries DES= drug eluting stent BMS = bare metal stent CABG= coronary artery bypass graft Hgb= hemoglobin ISTH= international society on thrombosis and heamostasis
6 BARC Definitions Type Type 0 Type 1 Type 2 Type 3 Type 4 Type 5 Definition No bleeding Bleeding that is not actionable and does not cause the patient to seek treatment Any clinically overt sign of hemorrhage that is actionable and requires diagnostic studies, hospitalization, or treatment by a health care professional a. Overt bleeding plus hemoglobin drop of 3-5 g/dl (provided hemoglobin drop is related to bleed); transfusion with overt bleeding b. Overt bleeding plus hemoglobin drop of < 5 g/dl (provided hemoglobin drop is related to bleed); cardiac tamponade; bleeding requiring surgical intervention for control; bleeding requiring IV vasoactive agents c. Intracranial hemorrhage confirmed by autopsy, imaging, or lumbar puncture; intraocular bleed compromising vision CABG-related bleeding within 48 hours a. Probable fatal bleed b. Definite fatal bleeding (overt or autopsy or imaging confirmation)
7 TIMI Definitions Type Major Minor Minimal Definition Intracranial hemorrhage > 5 g/dl decrease in the hemoglobin concentration > 15% absolute decrease in hematocrit Observed blood loss: > 3g/dL decrease in the hemoglobin concentration >10% decrease in the hematocrit No observed blood loss: >4 g/dl decrease in the hemoglobin concentration >12% decrease in hemaotcrit Any clinically overt sign of hemorrhage associated with a < 3 g/dl decrease in the hemoglobin concentration or < 9% decrease in the hematocrit
8 GUSTO Definitions Type Definition Severe or lifethreatening Moderate Mild Intracranial hemorrhage Bleeding that causes hemodynamic compromise and intervention Bleeding that requires blood transfusion but does not lead to hemodynamic instability Bleeding that does not meet criteria for severe or moderate bleeding
9 ISTH Assessment Tool Symptoms Criteria Normal Range Major Epistaxis Cutaneous symptoms Bleeding from minor wounds Oral cavity symptoms GI Bleeding Hematuria Tooth extraction Surgery Menorrhagia Post-partum hemorrhage Muscle hematoma Hemarthrosis CNS bleeding Other bleeding Score 0-4 for each symptom based on specific criteria, such as not needing treatment, needing consultation from health care professional, requiring transfusions, surgery, etc. < 4 adult males < 6 adult females < 3 children Fatal bleed And/or Symptomatic bleeding in a critical area or organ And/or Bleeding causing fall in hemoglobin level of 2 g/dl or more, leading to transfusion of 2 or more units of blood
10 Background Approximately 10% of the nearly 1 million patients who undergo PCI in US each year have an indication for chronic oral anticoagulation therapy Dual antiplatelet therapy (DAPT) is mainstay treatment for secondary prevention of MACE in patients who have survived acute coronary syndrome and/or have received a stent Triple therapy results in at least a 2- to 3 fold increase in bleeding complications
11 Guidelines 2016 ACC/AHA Guideline Focused Update on Duration of Dual Antiplatelet Therapy in Patients with Coronary Artery Disease Assess ischemic and bleeding risks using validated risk predictors Keep triple therapy duration as short as possible Consider target INR Clopidogrel is P2Y12 inhibitor of choice Use low dose aspirin PPI should be used in patients with history of GI bleed and are reasonable in patients with increased risk of GI bleed Levine GN et al. Journal of the American College of Cardiology 2016; 68 (10):
12 European Consensus Document Newer generation DES preferable over BMS, particularly in patients at low risk of bleeding New generation p2y12 inhibitors should not be used in antithrombotic combination therapy with anticoagulants NOACs and VKAs are interchangeable and patients already receiving a NOAC should not be switched to VKA if a NOAC is used in combination. Use lower doses: dabigatran 110 mg BID, rivaroxaban 15 mg daily, apixaban 2.5 mg BID VKA: INR Rohla et al. European Heart Journal-Cardiovascular Pharmacotherapy 2015: 1:
13 Warfarin
14 Use of Clopidogrel with or without Aspirin in Patients Taking Oral Anticoagulant Therapy and Undergoing Percutaneous Coronary Intervention: an Open-Label, Randomized, Controlled Trial Dewilde WJM et al. Lancet 2013; 381: WOEST What is the Optimal antiplatelet and anticoagulant therapy in patients with oral anticoagulation and coronary StenTing
15 WOEST N= 573 Warfarin + clopidogrel N= 284 Warfarin + clopidogrel + aspirin N= 289
16 WOEST Age Inclusion Long term indication for oral anticoagulation treatment Severe coronary lesion with indication for PCI Exclusion History of intracranial bleeding Cardiogenic shock Peptic ulcer in previous 6 months Thrombocytopenia TIMI major bleed in past 12 months Contraindication to study medications
17 WOEST Primary Outcome Secondary Outcomes Occurrence of any bleeding episode during 1 year follow-up (TIMI, GUSTO, and BARC) Composite of death, MI, stroke, target-vessel revascularization, and stent thrombosis Separate assessment of each component of primary and secondary
18 WOEST Warfarin + clopidogrel Triple therapy Hazard Ratio and P-Value Any bleeding 54 (19.4%) 126 (44.4%) 0.36 (95% CI ) P < Composite of death, MI, stroke, target-vessel revascularization, and stent thrombosis 31 (11.1%) 50 (17.6%) 0.6 (95% CI ) P 0.025
19 WOEST Risk of bleeding is high using triple oral antithrombotic therapy At 1 year oral anticoagulation was being used by 92.5% of patients in the double-therapy group and 91.2% of the triple-therapy group Use of clopidogrel without aspirin was associated with a significant reduction in bleeding complications and no increase in the rate of thrombotic events
20 Duration of Triple Therapy in Patients Requiring Oral Anticoagulation After Drug-Eluting Stent Implantation Fiedler et al. Journal of the American College of Cardiology 2015; 65(16): ISAR-TRIPLE
21 ISAR-TRIPLE Aspirin + clopidogrel + VKA N= weeks N= months N= 307
22 ISAR-TRIPLE Inclusion Age 18 and above Long term indication for oral anticoagulation treatment (1 year or more) Receiving DES for stable angina or ACS Exclusion Previous stent thrombosis, DES left main stem Active bleeding History of intracranial bleeding
23 ISAR-TRPLE Primary Outcome Secondary Outcomes Composite of death, MI, definite stent thrombosis, stroke, or TIMI major bleeding at 9 months after randomization Incidence of ischemic complications (cumulative incidence of cardiac death, MI, definite stent thrombosis, or ischemic stroke or bleeding complications (TIMI major) Each individual component of primary and secondary endpoints
24 ISAR-TRIPLE 6 weeks 6 months Hazard Ratio and P-Value Primary Outcome 30 (9.8%) 27 (8.8%) 1.14 (95% CI ) P= 0.63 Secondary Outcome 12 (4%) 13 (4.3%) 0.93 (95% CI ) P=0.87
25 ISAR-TRIPLE Six weeks of triple therapy was not superior to 6 months with respect to net clinical outcomes Post-hoc landmark analysis from 6 weeks to 9 months: no differences for major bleeding Not designed to show non-inferiority
26 Prasugrel or Ticagrelor
27 Triple Antithrombotic Therapy with Aspirin, P2Y12 Inhibitor, and Warfarin After Percutaneous Coronary Intervention: An Evaluation of Prasugrel or Ticagrelor Versus Clopidogrel Verlinden NJ et al. Journal of Cardiovascular Pharmacology and Therapeutics 2017; [Epub ahead of print]
28 Verlinden et al. N= 168 Prasugrel N= 32 Ticagrelor N= 10 Clopidogrel N= 126
29 Verlinden et al. Primary Outcome Secondary Outcome Incidence of any bleeding during the 12 month period after index hospitalization MACCE: cumulative incidence of a composite of cardiac death, nonfatal MI, or nonfatal ischemic stroke within 12 months after index visit
30 Verlinden et al. Ticagrelor or prasugrel (n=42) Clopidogrel (n=126) P-value Any bleeding 12 (28.6%) 16 (12.7%) odds ratio: 3.3 (95% CI ). MACCE 8 (19%) 23 (18.3%) 0.91 Cardiac death 3 (7.1%) 4 (3.2%) 0.37 MI 7 (16.7%) 20 (15.9%) 0.9 Ischemic stroke 1 (2.4%) 4 (3.2%) 1.0
31 Verlinden et al. The use of prasugrel or ticagrelor as part of triple antithrombotic therapy among patients who underwent PCI and received warfarin was associated with significantly more bleeding compared to patients who received clopidogrel Higher potency P2Y12 Inhibitors should be used cautiously in these patients
32 Verlinden et al. Small study population Major/minor bleeding not specified Adherence and duration of DAPT unknown INR values and time in therapeutic range during follow up unknown
33 Triple Therapy with Aspirin, Prasugrel, and Vitamin K Antagonists in Patients with Drug- Eluting Stent Implantation and an Indication for Oral Anticoagulation Sarafoff et al. JACC 2013; 61(20):
34 Sarafoff et al. DES placement and 6 months TT N= 377 Triple Therapy with clopidogrel N= 256 Triple Therapy with prasugrel N= 21
35 Sarafoff et al. Prasugrel used if: Patients had high platelet reactivity and deemed at increased risk of stent thrombosis (comorbidities, complexity of intervention) ACS and already gotten 60 mg prasugrel load Patients with clopidogrel allergy Patients with previous stent thrombosis while receiving treatment with clopidogrel
36 Sarafoff et al. Assessment of platelet function High platelet reactivity to clopidogrel treatment set at 468 arbitrary aggregation units (AU) x min Majority patients given 600 mg clopidogrel load, then platelet reactivity tested If levels tested and > 468 AU x min, then re-loaded with clopidogrel If levels still > 468 after the 2 nd clopidogrel load, then patient got 60 mg prasugrel load
37 Sarafoff et al. Primary Outcome Secondary Outcome Composite of TIMI major and minor bleeding at 6 months Composite of death, MI, ischemic stroke, or definite stent thrombosis
38 Sarafoff et al. Prasugrel Clopidogrel Hazard Ratio and P-Value TIMI Bleeding 6 (28.6%) 24 (6.7%) 4.6 (95% CI ) P < MACCE 2 (9.5%) 25 (7.0%) 1.4 (95% CI ) P 0.61
39 Sarafoff et al. Prasugrel is able to overcome high platelet reactivity to clopidogrel in patients treated with OAC after DES implantation Substitution of prasugrel for clopidogrel in patients needing TT increases risk of bleeding Lower INR goals used in this trial in patients with mechanical valves for other indications
40 TRANSLATE-ACS Comparison of clopidogrel versus prasugrel in nearly 12,000 ACS patients undergoing PCI Observational study enrolled STEMI and NSTEMI patients from Evaluate real world effectiveness and use of prasugrel among MI patients
41 TRANSLATE-ACS Subanalysis Describes prevalence of triple therapy use Compares clinical characteristics and outcomes between patients receiving TT and DAPT Compares clinical characteristics and outcomes between patients receiving TT with clopidogrel versus prasugrel Jackson et al. JACC: Cardiovascular Interventions 2015; 8(14):
42 TRANSLATE-ACS Subanalysis N= 11,756 Triple Therapy with clopidogrel Triple Therapy with prasugrel DAPT with clopidogrel DAPT with prasugrel N= 526 N= 91 N= 7715 N= 3424
43 TRANSLATE-ACS Subanalysis TT associated with greater risk of bleeding than DAPT, regardless of which P2Y12 inhibitor used No significant difference in composite risk of MACE between groups Among those patients discharged on TT, prasugrel associated with higher risk of bleeding than clopidogrel Driven by patient reported events No significant difference in risk of bleeding requiring rehospitalization between the two groups
44 Novel Anticoagulants
45 Rivaroxaban 2009: ATLAS ACS-TIMI 46 Rivaroxaban in Combination with Aspirin Alone or with Aspirin and a Thienopyridine in Patients with Acute Coronary Syndrome Dose escalation study: placebo, rivaroxaban 5-20 mg total given once daily, and rivaroxaban 5-20 mg total given twice daily Bleed risk increased in a dose-dependent manner Reduction in risk of death, MI, stroke, or severe recurrent ischemia 2012: ATLAS ACS 2-TIMI 51 Rivaroxaban in Patients with Recent Acute Coronary Syndrome Phase 3 Trial: Placebo vs 2.5 mg twice daily vs 5 mg twice daily Increased risk of bleeding (fewer fatal bleeds with 2.5 mg twice daily dose) Significant reduction in composite of death from CV causes, MI, or stroke Mega JL et al. Lancet 2009; 374: Mega JL et al. N Engl J Med 2012; 366: 9-1
46 Rivaroxaban 2013: European Medicines Agency (EMA) approved rivaroxaban 2.5 mg twice daily for secondary prevention after ACS in combination with DAPT 2014: Food and Drug Administration (FDA) rejects approval for expanded indication 2015: National Institute for Health and Care Excellence (NICE) in United Kingdom approves use
47 Prevention of Bleeding in Patients with Atrial Fibrillation Undergoing PCI Gibson CM et al. N Engl J Med 2016; 375: PIONEER AF-PCI
48 PIONEER AF-PCI Randomized N= 2124 Vitamin K Antagonist plus DAPT N= 706 Rivaroxaban 15 mg once daily plus P2Y12 inhibitor for 12 months N= 709 Rivaroxaban 2.5 mg twice daily plus DAPT N= month N= months N= months N= month N= months N= months N= 352
49 PIONEER AF-PCI Inclusion 18 years of age or older Paroxysmal, persistent, or permanent nonvalvular atrial fibrillation Undergone PCI with stent placement Exclusion Any condition that contraindicates anticoagulant therapy: Active bleeding, Hgb < 10 g/dl or platelet count < 90,000 mm 3 History of ICH Clinically significant GI bleed within 12 months before randomization Any other condition known to increase risk of bleeding History of stroke or TIA Cardiogenic shock at time of randomization CrCL < 30 ml/min Significant liver disease
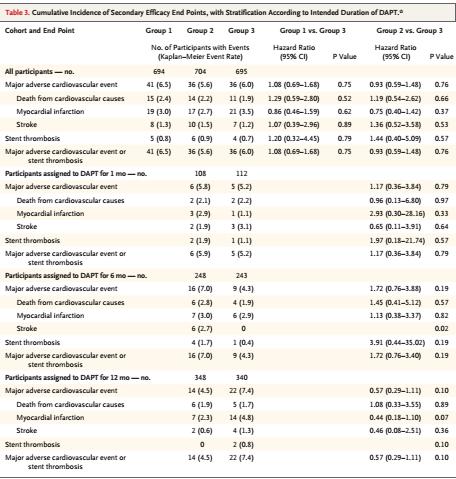
50 PIONEER AF-PCI Clinically significant bleeding= composite of major bleeding or minor bleeding (TIMI) at 12 months Major adverse CV event composite of death from CV causes, MI, or stroke) Rivaroxaban 15 mg once daily plus P2Y12 inhibitor (Group 1) Rivaroxaban 2.5 mg twice daily plus DAPT (Group 2) Vitamin K Antagonist plus DAPT (Group 3) Hazard Ratio and P-Value 16.8% 18% 26.7% Group 1 vs Group 3: 0.59 (95% CI ) P < Group 2 vs Group 3: 0.63 (95% CI ) P < % 5.6% 6.0% P > 0.05 for both comparisons
51 PIONEER AF-PCI Treatment that included either low dose or verylow-dose rivaroxaban was associated with a lower risk of clinically significant bleeding than was standard triple therapy that included a VKA Rates of major adverse CV events were similar Broad confidence intervals diminish surety of any conclusions regarding efficacy
52
53 PIONEER AF-PCI Trial not powered to establish superiority or noninferiority Individual efficacy endpoints within subgroups are underpowered
54 Apixaban with Antiplatelet Therapy after Acute Coronary Syndrome Alexander JH et al. N Engl J Med 2011; 365: APPRAISE-2
55 APPRAISE-2 Randomized N= 7392 Placebo N= 3687 Apixaban 5 mg twice daily N= 3705
56 APPRAISE-2 Inclusion ACS within last 7 days at least two or more high-risk characteristics: age 65 years or above diabetes mellitus MI within the previous 5 years Cerebrovascular disease Clinical heart failure requiring or left ventricular ejection fraction < 40% associated with index event peripheral vascular disease, Impaired renal function CrCl < 60 ml/min] no revascularization after the index event Exclusion Persistent severe hypertension Severe renal dysfunction with CrCl < 20 ml/min Active bleeding or high risk for bleeding Known coagulopathy Ischemic stroke within 7 days NYHA class IV heart failure Any history of intracranial bleeding Hgb < 9 g/dl or platelet count < 100,000 mm 3 Required ongoing treatment with a parenteral or oral anticoagulant Required treatment with high dose aspirin >325 mg daily or strong inhibitor of CYP 3A4 Severe comorbid condition with life expectancy < 6 months Acute pericarditis
57 APPRAISE-2 Efficacy Outcome Primary Composite of CV death, MI, or ischemic stroke Secondary Composite of CV death, MI, ischemic stroke, or unstable angina Individual components of primary efficacy outcome, unstable angina, and stent thrombosis Safety Outcome Primary Major bleeding (TIMI) Secondary TIMI major and minor bleeding, major or clinically relevant nonmajor bleeding (ISTH) Severe or moderate bleeding (GUSTO)
58 APPRAISE-2 After ~7000 patients had been recruited, the independent data monitoring committee recommended that the trial be stopped Excess of clinically important bleeding events with apixaban in the absence of a counterbalancing reduction of ischemic events
59 APPRAISE-2 Placebo Apixaban 5 mg twice daily Hazard Ratio with Apixaban (95% CI) and P value TIMI Major Bleeding 18 (0.5%) 46 (1.3%) 2.59 ( ) P value TIMI Major or Minor Bleeding 29 (0.8%) 80 (2.2%) 2.79 ( ) P value < Efficacy: Composite of CV death, MI, or ischemic stroke 293 (7.9%) 279 (7.5%) 0.95 ( ) P value 0.51
60 APPRAISE-2 Treatment with apixaban (as compared with placebo), was associated with a significant increase in risk of bleeding without a significant effect on the incidence of recurrent ischemic events Majority of patients (81%) were receiving DAPT at the time of randomization* Trial population had high-risk characteristics More than half-the patients had 3 or more high-risk characteristics defined at time of enrollment
61 Dabigatran vs placebo in patients with acute coronary syndromes on dual antiplatelet therapy: a randomized, double-blind, phase II trial Oldgren J et al. European Heart Journal 2011;32: RE-DEEM
62 RE-DEEM Randomized N= 1878 Placebo Dabigatran 50 mg twice daily Dabigatran 75 mg twice daily Dabigatran 110 mg twice daily Dabigatran 150 mg twice daily Initially randomized 1:1:1 Patients randomized to this dose in 2 nd stage Patients randomized to this dose in 3 rd stage
63 RE-DEEM 4 th stage Placebo 50 mg twice daily 75 mg twice daily 110 mg twice daily 150 mg twice daily N
64 RE-DEEM 18 years or older Inclusion Hospitalized with MI within last 14 days Receiving DAPT* at least one risk factor for subsequent cardiovascular complications: age 65 years or above diabetes mellitus on treatment, previous MI left bundle branch block, congestive heart failure requiring treatment or left ventricular ejection fraction,40%, peripheral arterial disease, moderate renal insufficiency [creatinine clearance (CrCl) ml/min] no revascularization for the index event Exclusion Ongoing or planned treatment with VKA Severe disabling stroke within the previous 6 months or any stroke within the previous 14 days Conditions associated with an increased risk of bleeding: major surgery (including bypass surgery) in the previous month, history of severe bleeding gastrointestinal hemorrhage within the past year gastroduodenal ulcer in the previous 30 days fibrinolytic agents within 48 h of study entry uncontrolled hypertension Hgb < 10 g/dl or platelet count < 100 x 10 9 L Normal coronary arteries at angiogram for index event Congestive heart failure NYHA Class IV Severe renal impairment (CrCl <30 ml/min)
65 RE-DEEM Primary outcome Secondary outcome Incidence of major or clinically relevant minor bleeding Major bleeding events were assessed by: ISTH definition fall in Hgb of 2 g/dl or more transfusion of two units or more of whole blood or packed red blood cells Clinically relevant minor bleeding was defined as a clinically overt bleed that did not meet criteria for major bleed Indicators of efficacy Reduction in incidences of CV ischemic events: Composite of CV death, non-fatal MI, and non-hemorrhagic stroke Individual occurrence of death (CV and all-cause), non-fatal MI, severe recurrent ischemia, and nonhemorrhagic stroke Reduction in D-dimer levels
66 RE-DEEM Primary Outcome (%) Placebo Dabigatran 50 mg twice daily Dabigatran 75 mg twice daily Dabigatran 110 mg twice daily Dabigatran 150 mg twice daily Hazard Ratio % CI ( ) % CI ( ) % CI ( ) % CI ( )
67 RE-DEEM Secondary Outcome (%) Placebo Dabigatran 50 mg twice daily Dabigatran 75 mg twice daily Dabigatran 110 mg twice daily Dabigatran 150 mg twice daily
68 RE-DEEM The addition of dabigatran to DAPT for 6 months in post- MI patients was associated with increased risk of bleeding The total number of patients experiencing ischemic CV events during the study was low, with minor differences between the treatment groups
69 Upcoming Studies
70 AUGUSTUS Apixaban 5 mg twice daily + P2Y12 inhibitor + aspirin or placebo Vs Warfarin + P2Y12 inhibitor + aspirin or placebo N= 4600 Primary outcome: major/clinically relevant bleeding (6 months) Secondary objective: death, MI, stroke, stent thrombosis Estimated study completion date: December 2018
71 REDUAL-PCI 110 mg dabigatran twice daily + clopidogrel or ticagrelor vs 150 mg dabigatran BID + clodpidogrel or ticagrelor vs Triple therapy: warfarin + clopidogrel or ticagrelor + aspirin Study aims to show non-inferiority of each dose of dual antithrombotic therapy when compared to triple antithrombotic therapy Safety endpoint= time to first major bleeding event (30 month) Efficacy endpoint= composite of time to death or first thrombotic event (all death, MI, stroke, or systemic embolism) and unplanned revascularization N= 2727 Estimated completion date: final data collection June 2017 (results end of year)
72 WOEST ISAR-TRIPLE Verlinden et al. Sarafoff et al. Translate-ACS PIONEER AF-PCI APPRAISE-2 RE-DEEM Summary Triple therapy for 1 year increased risk of bleeding Six weeks of triple therapy was not superior to 6 months with respect to net clinical outcomes Prasugrel or ticagrelor as part of TT was associated with significantly more bleeding compared to patients who received clopidogrel Substitution of prasugrel for clopidogrel in patients needing TT increases risk of bleeding Prasugrel has higher risk of bleeding in TT than clopidogrel Low dose or very-low-dose rivaroxaban was associated with a lower risk of clinically significant bleeding than was standard triple therapy that included a VKA Apixaban (as compared with placebo), was associated with a significant increase in risk of bleeding without a significant effect on the incidence of recurrent ischemic events The addition of dabigatran to DAPT for 6 months in post-mi patients was associated with increased risk of bleeding
73 Conclusions Assess each patient for risk of bleeding and risk of ischemic events TT for as short of duration as possible Clopidogrel preferred P2Y12 inhibitor Newer oral anticoagulants have higher risk of bleeding Low dose rivaroxaban and DAPT had lower risk of bleeding than warfarin and DAPT
PCI in Patients with AF Optimizing Oral Anticoagulation Regimen
 PCI in Patients with AF Optimizing Oral Anticoagulation Regimen Walid I. Saliba, MD Director, Atrial Fibrillation Center Heart and Vascular Institute Cleveland Clinic 1 Epidemiology and AF and PCI AF and
PCI in Patients with AF Optimizing Oral Anticoagulation Regimen Walid I. Saliba, MD Director, Atrial Fibrillation Center Heart and Vascular Institute Cleveland Clinic 1 Epidemiology and AF and PCI AF and
NAVIGATING THROMBOSIS AND BLEEDING AT THE INTERSECTION OF ATRIAL FIBRILLATION AND CORONARY STENTING
 NAVIGATING THROMBOSIS AND BLEEDING AT THE INTERSECTION OF ATRIAL FIBRILLATION AND CORONARY STENTING Snehal H. Bhatt, Pharm.D., BCPS-AQ Cardiology, FASHP, AACC Associate Professor of Pharmacy Practice MCPHS
NAVIGATING THROMBOSIS AND BLEEDING AT THE INTERSECTION OF ATRIAL FIBRILLATION AND CORONARY STENTING Snehal H. Bhatt, Pharm.D., BCPS-AQ Cardiology, FASHP, AACC Associate Professor of Pharmacy Practice MCPHS
When and how to combine antiplatelet agents and anticoagulant?
 When and how to combine antiplatelet agents and anticoagulant? Christophe Beauloye, MD, PhD Head, Division of Cardiology Cliniques Universitaires Saint-Luc Brussels, Belgium Introduction Anticoagulation
When and how to combine antiplatelet agents and anticoagulant? Christophe Beauloye, MD, PhD Head, Division of Cardiology Cliniques Universitaires Saint-Luc Brussels, Belgium Introduction Anticoagulation
Which drug do you prefer for stable CAD? - P2Y12 inhibitor
 Which drug do you prefer for stable CAD? - P2Y12 inhibitor Jung Rae Cho, MD, PhD Cardiovascular Division, Department of Internal Medicine Kangnam Sacred Heart Hospital, Hallym University Medical Center,
Which drug do you prefer for stable CAD? - P2Y12 inhibitor Jung Rae Cho, MD, PhD Cardiovascular Division, Department of Internal Medicine Kangnam Sacred Heart Hospital, Hallym University Medical Center,
Asif Serajian DO FACC FSCAI
 Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
3/23/2017. Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate Europace Oct;14(10): Epub 2012 Aug 24.
: Epub 2012 Aug 24.") Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017
 Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Low Dose Rivaroxaban Versus Aspirin, in Addition to P2Y12 Inhibition, in Acute Coronary Syndromes (GEMINI-ACS-1)
") Low Dose Rivaroxaban Versus Aspirin, in Addition to P2Y12 Inhibition, in Acute Coronary Syndromes (GEMINI-ACS-1) Caitlin C. Akerman, PharmD PGY2 Cardiology Resident WakeMed Health & Hospitals Raleigh,
Low Dose Rivaroxaban Versus Aspirin, in Addition to P2Y12 Inhibition, in Acute Coronary Syndromes (GEMINI-ACS-1) Caitlin C. Akerman, PharmD PGY2 Cardiology Resident WakeMed Health & Hospitals Raleigh,
Management of Patients with Atrial Fibrillation and Stents: Is Three Drugs Too Many?
 Management of Patients with Atrial Fibrillation and Stents: Is Three Drugs Too Many? Neal S. Kleiman, MD Houston Methodist DeBakey Heart and Vascular Center, Houston, TX Some Things Are Really Clear 2013
Management of Patients with Atrial Fibrillation and Stents: Is Three Drugs Too Many? Neal S. Kleiman, MD Houston Methodist DeBakey Heart and Vascular Center, Houston, TX Some Things Are Really Clear 2013
The Challenge. Warfarin or Novel Oral Anti-Coagulants in the PCI patient? Anticoagulation/Stroke
 Anticoagulation/Stroke Warfarin v new oral anticoagulants post PCI Warfarin or Novel Oral Anti-Coagulants in the PCI patient? Gerry Devlin Chairs: Phillip Matsis & Tony Scott Gerry Devlin Honorary Associate
Anticoagulation/Stroke Warfarin v new oral anticoagulants post PCI Warfarin or Novel Oral Anti-Coagulants in the PCI patient? Gerry Devlin Chairs: Phillip Matsis & Tony Scott Gerry Devlin Honorary Associate
The Poor Long-Term Candidate for Warfarin: NOAC or Left Atrial Appendage Closure?
 The Poor Long-Term Candidate for Warfarin: NOAC or Left Atrial Appendage Closure? Suneet Mittal, MD, FACC, FHRS Director, Electrophysiology Laboratory Valley Health System Ridgewood, NJ and New York, NY
The Poor Long-Term Candidate for Warfarin: NOAC or Left Atrial Appendage Closure? Suneet Mittal, MD, FACC, FHRS Director, Electrophysiology Laboratory Valley Health System Ridgewood, NJ and New York, NY
FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS
 New Horizons In Atherothrombosis Treatment 2012 순환기춘계학술대회 FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS Division of Cardiology, Jeonbuk National University Medical School Jei Keon Chae,
New Horizons In Atherothrombosis Treatment 2012 순환기춘계학술대회 FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS Division of Cardiology, Jeonbuk National University Medical School Jei Keon Chae,
GRAND ROUNDS - DILEMMAS IN ANTICOAGULATION AND ANTIPLATELET THERAPY. Nick Collins February 2017
 GRAND ROUNDS - DILEMMAS IN ANTICOAGULATION AND ANTIPLATELET THERAPY Nick Collins February 2017 DISCLOSURES Before I commence Acknowledge.. Interventional Cardiologist Perception evolved. Interventional
GRAND ROUNDS - DILEMMAS IN ANTICOAGULATION AND ANTIPLATELET THERAPY Nick Collins February 2017 DISCLOSURES Before I commence Acknowledge.. Interventional Cardiologist Perception evolved. Interventional
Clinical and Economic Value of Rivaroxaban in Coronary Artery Disease
 CHRISTOPHER B. GRANGER, MD Professor of Medicine Division of Cardiology, Department of Medicine; Director, Cardiac Care Unit Duke University Medical Center, Durham, NC Clinical and Economic Value of Rivaroxaban
CHRISTOPHER B. GRANGER, MD Professor of Medicine Division of Cardiology, Department of Medicine; Director, Cardiac Care Unit Duke University Medical Center, Durham, NC Clinical and Economic Value of Rivaroxaban
TRIPLE THERAPY, NOACs with concurrent indication for DAPT. Paul Wright Lead Cardiac Pharmacist The Heart, UCLH NHS Foundation Trust
 TRIPLE THERAPY, NOACs with concurrent indication for DAPT Paul Wright Lead Cardiac Pharmacist The Heart, UCLH NHS Foundation Trust Content Why consider triple therapy What we know of triple therapy Current
TRIPLE THERAPY, NOACs with concurrent indication for DAPT Paul Wright Lead Cardiac Pharmacist The Heart, UCLH NHS Foundation Trust Content Why consider triple therapy What we know of triple therapy Current
Dual Antiplatelet Therapy Made Practical
 Dual Antiplatelet Therapy Made Practical David Parra, Pharm.D., FCCP, BCPS Clinical Pharmacy Program Manager in Cardiology/Anticoagulation VISN 8 Pharmacy Benefits Management Clinical Associate Professor
Dual Antiplatelet Therapy Made Practical David Parra, Pharm.D., FCCP, BCPS Clinical Pharmacy Program Manager in Cardiology/Anticoagulation VISN 8 Pharmacy Benefits Management Clinical Associate Professor
Special Conditions of NOAC PCI 가톨릭의대 순환기내과 장성원
 Special Conditions of NOAC PCI 가톨릭의대 순환기내과 장성원 Issues on Patients with NOAC PCI Peri-procedural management CKD or dialysis Cardioversion Neurological situations Dual Antiplatelet Therapy with Oral Anticoagulants
Special Conditions of NOAC PCI 가톨릭의대 순환기내과 장성원 Issues on Patients with NOAC PCI Peri-procedural management CKD or dialysis Cardioversion Neurological situations Dual Antiplatelet Therapy with Oral Anticoagulants
Στεφανιαίος ασθενής με μη βαλβιδική Κολπική Μαρμαρυγή - Νέες στρατηγικές
 4 ο ΠΑΝΕΛΛΗΝΙΟ ΑΡΡΥΘΜΙΟΛΟΓΙΚΟ ΣΥΝΕΔΡΙΟ 21-22 ΣΕΠΤΕΜΒΡΙΟΥ 2018 HILTON, ΑΘΗΝΑ Στεφανιαίος ασθενής με μη βαλβιδική Κολπική Μαρμαρυγή - Νέες στρατηγικές Ι. Κανακάκης MD, PhD Διευθυντής Αιμοδυναμικού Τμήματος
4 ο ΠΑΝΕΛΛΗΝΙΟ ΑΡΡΥΘΜΙΟΛΟΓΙΚΟ ΣΥΝΕΔΡΙΟ 21-22 ΣΕΠΤΕΜΒΡΙΟΥ 2018 HILTON, ΑΘΗΝΑ Στεφανιαίος ασθενής με μη βαλβιδική Κολπική Μαρμαρυγή - Νέες στρατηγικές Ι. Κανακάκης MD, PhD Διευθυντής Αιμοδυναμικού Τμήματος
Dr Αντώνιος Στ. Ντάτσιος MSc, MRCP(UK), FESC. Επεμβατικός Καρδιολόγος Επιμελητής Β Γ. Ν. Θ. Παπαγεωργίου
, FESC. Επεμβατικός Καρδιολόγος Επιμελητής Β Γ. Ν. Θ. Παπαγεωργίου") Dr Αντώνιος Στ. Ντάτσιος MSc, MRCP(UK), FESC. Επεμβατικός Καρδιολόγος Επιμελητής Β Γ. Ν. Θ. Παπαγεωργίου Θεσσαλονίκη, 9/2/2018 Disclosures: None Primary efficacy outcome* (%/year) Antiplatelet Therapy
Dr Αντώνιος Στ. Ντάτσιος MSc, MRCP(UK), FESC. Επεμβατικός Καρδιολόγος Επιμελητής Β Γ. Ν. Θ. Παπαγεωργίου Θεσσαλονίκη, 9/2/2018 Disclosures: None Primary efficacy outcome* (%/year) Antiplatelet Therapy
Stable CAD, Elective Stenting and AFib
 Stable CAD, Elective Stenting and AFib Kurt Huber, MD, FESC, FACC, FAHA 3 rd Medical Department Cardiology & Intensive Care Medicine Wilhelminenhospital & Sigmund Freud Private University, Medical School
Stable CAD, Elective Stenting and AFib Kurt Huber, MD, FESC, FACC, FAHA 3 rd Medical Department Cardiology & Intensive Care Medicine Wilhelminenhospital & Sigmund Freud Private University, Medical School
A Randomized Trial Evaluating Clinically Significant Bleeding with Low-Dose Rivaroxaban vs Aspirin, in Addition to P2Y12 inhibition, in ACS
 A Randomized Trial Evaluating Clinically Significant Bleeding with Low-Dose Rivaroxaban vs Aspirin, in Addition to P2Y12 inhibition, in ACS Magnus Ohman MB, on behalf of the GEMINI-ACS-1 Investigators
A Randomized Trial Evaluating Clinically Significant Bleeding with Low-Dose Rivaroxaban vs Aspirin, in Addition to P2Y12 inhibition, in ACS Magnus Ohman MB, on behalf of the GEMINI-ACS-1 Investigators
UPDATES FROM THE 2018 ANTIPLATELET GUIDELINES
 UPDATES FROM THE 2018 ANTIPLATELET GUIDELINES Claudia Bucci BScPhm, PharmD Clinical Coordinator, Cardiovascular Diseases Sunnybrook Health Sciences Centre 21st Annual Contemporary Therapeutic Issues in
UPDATES FROM THE 2018 ANTIPLATELET GUIDELINES Claudia Bucci BScPhm, PharmD Clinical Coordinator, Cardiovascular Diseases Sunnybrook Health Sciences Centre 21st Annual Contemporary Therapeutic Issues in
8th Emirates Cardiac Society Congress in collaboration with ACC Middle East Conference Dubai: October Acute Coronary Syndromes
 8th Emirates Cardiac Society Congress in collaboration with ACC Middle East Conference 2017 Dubai: 19-21 October 2017 Acute Coronary Syndromes Antonio Colombo Centro Cuore Columbus and S. Raffaele Scientific
8th Emirates Cardiac Society Congress in collaboration with ACC Middle East Conference 2017 Dubai: 19-21 October 2017 Acute Coronary Syndromes Antonio Colombo Centro Cuore Columbus and S. Raffaele Scientific
Antiplatelet and Anti-Thrombotic Therapy. Ivan Anderson, MD RIHVH Cardiology
 Antiplatelet and Anti-Thrombotic Therapy Ivan Anderson, MD RIHVH Cardiology Outline Anti-thrombotic therapy Risk stratification of stroke with atrial fibrillation DVT and PE treatment Pharmacology Anti-platelet
Antiplatelet and Anti-Thrombotic Therapy Ivan Anderson, MD RIHVH Cardiology Outline Anti-thrombotic therapy Risk stratification of stroke with atrial fibrillation DVT and PE treatment Pharmacology Anti-platelet
Optimal lenght of DAPT in different clinical scenarios
 Optimal lenght of DAPT in different clinical scenarios After PCI with DES in the light of recent and ongoing studies Dr Grégoire Rangé / CH Chartres / France DAPT duration depend on the evolution of risk
Optimal lenght of DAPT in different clinical scenarios After PCI with DES in the light of recent and ongoing studies Dr Grégoire Rangé / CH Chartres / France DAPT duration depend on the evolution of risk
Anticoagulants and antiplatelet therapy in the older patient: Choosing wisely
 Anticoagulants and antiplatelet therapy in the older patient: Choosing wisely Rajiv Gulati, MD PhD Advances in Cardiac Arrhythmias & Great Innovations in Cardiology Torino, October 2015 2015 MFMER 3477310-1
Anticoagulants and antiplatelet therapy in the older patient: Choosing wisely Rajiv Gulati, MD PhD Advances in Cardiac Arrhythmias & Great Innovations in Cardiology Torino, October 2015 2015 MFMER 3477310-1
Let s Gi e The So ethi g To Clot About: Controversies in Anticoagulation
 Let s Gi e The So ethi g To Clot About: Controversies in Anticoagulation Janna Beavers, MS, PharmD, BCPS Cardiology Clinical Pharmacy Specialist WakeMed Health & Hospitals Raleigh, NC March 13, 2018 Pharmacist
Let s Gi e The So ethi g To Clot About: Controversies in Anticoagulation Janna Beavers, MS, PharmD, BCPS Cardiology Clinical Pharmacy Specialist WakeMed Health & Hospitals Raleigh, NC March 13, 2018 Pharmacist
Changing Course: Anticoagulation in Secondary Prevention of Cardiovascular Disease Events
 Changing Course: Anticoagulation in Secondary Prevention of Cardiovascular Disease Events Deepak L. Bhatt, MD, MPH Executive Director Interventional Cardiovascular Programs Brigham and Women s Hospital
Changing Course: Anticoagulation in Secondary Prevention of Cardiovascular Disease Events Deepak L. Bhatt, MD, MPH Executive Director Interventional Cardiovascular Programs Brigham and Women s Hospital
Individual Therapeutic Selection Of Anti-coagulants And Periprocedural. Miguel Valderrábano, MD
 Individual Therapeutic Selection Of Anti-coagulants And Periprocedural Management Miguel Valderrábano, MD Outline Does the patient need anticoagulation? Review of clinical evidence for each anticoagulant
Individual Therapeutic Selection Of Anti-coagulants And Periprocedural Management Miguel Valderrábano, MD Outline Does the patient need anticoagulation? Review of clinical evidence for each anticoagulant
Study design: multicenter, randomized, open-label trial following a PROBE design
 Subgroup Analysis from the RE-DUAL PCI Trial Dual Antithrombotic Therapy with in Patients with Atrial Fibrillation Undergoing Percutaneous Coronary Intervention Jonas Oldgren, Philippe Gabriel Steg, Stefan
Subgroup Analysis from the RE-DUAL PCI Trial Dual Antithrombotic Therapy with in Patients with Atrial Fibrillation Undergoing Percutaneous Coronary Intervention Jonas Oldgren, Philippe Gabriel Steg, Stefan
Triple Therapy After PCI in AF: A Quagmire Soon to be Drained
 Triple Therapy After PCI in AF: A Quagmire Soon to be Drained Freek W.A. Verheugt Department of Cardiology, Onze Lieve Vrouwe Gasthuis (OLVG) Amsterdam, Netherlands DISCLOSURES FOR FREEK W. A. VERHEUGT
Triple Therapy After PCI in AF: A Quagmire Soon to be Drained Freek W.A. Verheugt Department of Cardiology, Onze Lieve Vrouwe Gasthuis (OLVG) Amsterdam, Netherlands DISCLOSURES FOR FREEK W. A. VERHEUGT
DIRECT ORAL ANTICOAGULANTS
 2017 Cardiovascular Symposium DIRECT ORAL ANTICOAGULANTS ERNESTO UMAÑA, MD, FACC ORAL ANTICOAGULANTS Vitamin K Antagonists (VKAs): Warfarin Non Vitamin K Antagonists Direct oral anticoagulants Novel Oral
2017 Cardiovascular Symposium DIRECT ORAL ANTICOAGULANTS ERNESTO UMAÑA, MD, FACC ORAL ANTICOAGULANTS Vitamin K Antagonists (VKAs): Warfarin Non Vitamin K Antagonists Direct oral anticoagulants Novel Oral
TRIAL UPDATE 1. ISAR TRIPLE SECURITY Trial. Dr Deven Patel Royal Free Hospital
 TRIAL UPDATE 1 ISAR TRIPLE SECURITY Trial Dr Deven Patel Royal Free Hospital NO CONFLICT OF INTEREST TO DECLARE ISAR TRIPLE Comparison of 6 weeks vs 6 months Triple Therapy in patients on oral anticoagulation
TRIAL UPDATE 1 ISAR TRIPLE SECURITY Trial Dr Deven Patel Royal Free Hospital NO CONFLICT OF INTEREST TO DECLARE ISAR TRIPLE Comparison of 6 weeks vs 6 months Triple Therapy in patients on oral anticoagulation
Joshua D. Lenchus, DO, RPh, FACP, SFHM Associate Professor of Medicine and Anesthesiology University of Miami Miller School of Medicine
 Joshua D. Lenchus, DO, RPh, FACP, SFHM Associate Professor of Medicine and Anesthesiology University of Miami Miller School of Medicine Antithrombotics Antiplatelets Aspirin Ticlopidine Prasugrel Dipyridamole
Joshua D. Lenchus, DO, RPh, FACP, SFHM Associate Professor of Medicine and Anesthesiology University of Miami Miller School of Medicine Antithrombotics Antiplatelets Aspirin Ticlopidine Prasugrel Dipyridamole
OUTPATIENT ANTITHROMBOTIC MANAGEMENT POST NON-ST ELEVATION ACUTE CORONARY SYNDROME. TARGET AUDIENCE: All Canadian health care professionals.
 OUTPATIENT ANTITHROMBOTIC MANAGEMENT POST NON-ST ELEVATION ACUTE CORONARY SYNDROME TARGET AUDIENCE: All Canadian health care professionals. OBJECTIVE: To review the use of antiplatelet agents and oral
OUTPATIENT ANTITHROMBOTIC MANAGEMENT POST NON-ST ELEVATION ACUTE CORONARY SYNDROME TARGET AUDIENCE: All Canadian health care professionals. OBJECTIVE: To review the use of antiplatelet agents and oral
Learning Objectives. Epidemiology of Acute Coronary Syndrome
 Cardiovascular Update: Antiplatelet therapy in acute coronary syndromes PHILLIP WEEKS, PHARM.D., BCPS-AQ CARDIOLOGY Learning Objectives Interpret guidelines as they relate to constructing an antiplatelet
Cardiovascular Update: Antiplatelet therapy in acute coronary syndromes PHILLIP WEEKS, PHARM.D., BCPS-AQ CARDIOLOGY Learning Objectives Interpret guidelines as they relate to constructing an antiplatelet
After acute coronary syndromes patients continue to have recurrent ischemic events despite revascularization and dual antiplatelet therapy
 Randomised Dabigatran Etexilate Dose Finding Study In Patients With Acute Coronary Syndromes Post Index Event With Additional Risk Factors For Cardiovascular Complications Also Receiving Aspirin and Clopidogrel
Randomised Dabigatran Etexilate Dose Finding Study In Patients With Acute Coronary Syndromes Post Index Event With Additional Risk Factors For Cardiovascular Complications Also Receiving Aspirin and Clopidogrel
Controversies in Cardiac Pharmacology
 Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
Antiplatelet Therapy in Patients on Anticoagulation
 Antiplatelet Therapy in Patients on Anticoagulation Ziad A Ali MD DPhil Cardiovascular Research Foundation Columbia University New York, Medical NY Center Cardiovascular Research Foundation Disclosure
Antiplatelet Therapy in Patients on Anticoagulation Ziad A Ali MD DPhil Cardiovascular Research Foundation Columbia University New York, Medical NY Center Cardiovascular Research Foundation Disclosure
1. Whether the risks of stent thrombosis (ST) and major adverse cardiovascular and cerebrovascular events (MACCE) differ from BMS and DES
 and major adverse cardiovascular and cerebrovascular events (MACCE) differ from BMS and DES") 1 Comparison of Ischemic and Bleeding Events After Drug- Eluting Stents or Bare Metal Stents in Subjects Receiving Dual Antiplatelet Therapy: Results from the Randomized Dual Antiplatelet Therapy (DAPT)
1 Comparison of Ischemic and Bleeding Events After Drug- Eluting Stents or Bare Metal Stents in Subjects Receiving Dual Antiplatelet Therapy: Results from the Randomized Dual Antiplatelet Therapy (DAPT)
Paolo Gresele Dipartimento di Medicina Sezione di Medicina Interna e Cardiovascolare Università di Perugia
 Anticoagulanti e mono-antiaggregazione: a chi, quali e per quanto tempo Paolo Gresele Dipartimento di Medicina Sezione di Medicina Interna e Cardiovascolare Università di Perugia Anticoagulazione: Bologna,
Anticoagulanti e mono-antiaggregazione: a chi, quali e per quanto tempo Paolo Gresele Dipartimento di Medicina Sezione di Medicina Interna e Cardiovascolare Università di Perugia Anticoagulazione: Bologna,
Disclosures. Theodore A. Bass MD, FSCAI. The following relationships exist related to this presentation. None
 SCAI Fellows Course December 10, 2013 Disclosures Theodore A. Bass MD, FSCAI The following relationships exist related to this presentation None Current Controversies on DAPT in PCI Which drug? When to
SCAI Fellows Course December 10, 2013 Disclosures Theodore A. Bass MD, FSCAI The following relationships exist related to this presentation None Current Controversies on DAPT in PCI Which drug? When to
Balancing Efficacy and Safety of P2Y12 Inhibitors for ACS Patients
 SYP.CLO-A.16.07.01 Balancing Efficacy and Safety of P2Y12 Inhibitors for ACS Patients dr. Hariadi Hariawan, Sp.PD, Sp.JP (K) TOPICS Efficacy Safety Consideration from Currently Available Antiplatelet Agents
SYP.CLO-A.16.07.01 Balancing Efficacy and Safety of P2Y12 Inhibitors for ACS Patients dr. Hariadi Hariawan, Sp.PD, Sp.JP (K) TOPICS Efficacy Safety Consideration from Currently Available Antiplatelet Agents
Ticagrelor compared with clopidogrel in patients with acute coronary syndromes the PLATO trial
 compared with clopidogrel in patients with acute coronary syndromes the PLATO trial August 30, 2009 at 08.00 CET PLATO background In NSTE-ACS and STEMI, current guidelines recommend 12 months aspirin and
compared with clopidogrel in patients with acute coronary syndromes the PLATO trial August 30, 2009 at 08.00 CET PLATO background In NSTE-ACS and STEMI, current guidelines recommend 12 months aspirin and
What oral antiplatelet therapy would you choose? a) ASA alone b) ASA + Clopidogrel c) ASA + Prasugrel d) ASA + Ticagrelor
 ASA alone b) ASA + Clopidogrel c) ASA + Prasugrel d) ASA + Ticagrelor") 76 year old female Prior Hypertension, Hyperlipidemia, Smoking On Hydrochlorothiazide, Atorvastatin New onset chest discomfort; 2 episodes in past 24 hours Heart rate 122/min; BP 170/92 mm Hg, Killip Class
76 year old female Prior Hypertension, Hyperlipidemia, Smoking On Hydrochlorothiazide, Atorvastatin New onset chest discomfort; 2 episodes in past 24 hours Heart rate 122/min; BP 170/92 mm Hg, Killip Class
Oral anticoagulation/antiplatelet therapy in the secondary prevention of ACS patients the cost of reducing death!
 Oral anticoagulation/antiplatelet therapy in the secondary prevention of ACS patients the cost of reducing death! Robert C. Welsh, MD, FRCPC Associate Professor of Medicine Director, Adult Cardiac Catheterization
Oral anticoagulation/antiplatelet therapy in the secondary prevention of ACS patients the cost of reducing death! Robert C. Welsh, MD, FRCPC Associate Professor of Medicine Director, Adult Cardiac Catheterization
Byeong-Keuk Kim, M.D. Ph D. Division of Cardiology, Severance Cardiovascular Hospital Yonsei University College of Medicine, Seoul, Korea
 Byeong-Keuk Kim, M.D. Ph D Division of Cardiology, Severance Cardiovascular Hospital Yonsei University College of Medicine, Seoul, Korea CASE, M/64 C.C; Recently aggravated chest discomfort for 3 days
Byeong-Keuk Kim, M.D. Ph D Division of Cardiology, Severance Cardiovascular Hospital Yonsei University College of Medicine, Seoul, Korea CASE, M/64 C.C; Recently aggravated chest discomfort for 3 days
Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical Trials Unit Bern Bern University Hospital, Switzerland
 Advances in Antiplatelet Therapy in PCI and ACS Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical Trials Unit Bern Bern University Hospital, Switzerland Targets for Platelet
Advances in Antiplatelet Therapy in PCI and ACS Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical Trials Unit Bern Bern University Hospital, Switzerland Targets for Platelet
Dual antiplatelet therapy (DAPT) in the era of Novel Oral Anticoagulants (NOACs) SACIS 2015
 in the era of Novel Oral Anticoagulants (NOACs) SACIS 2015") Dual antiplatelet therapy (DAPT) in the era of Novel Oral Anticoagulants (NOACs) SACIS 2015 Wesam A Alhejily MD FRCPC FACP FACC FSCAI Assistant Professor of Medicine Chief Of Adult Cardiology Consultant
Dual antiplatelet therapy (DAPT) in the era of Novel Oral Anticoagulants (NOACs) SACIS 2015 Wesam A Alhejily MD FRCPC FACP FACC FSCAI Assistant Professor of Medicine Chief Of Adult Cardiology Consultant
Prasugrel vs. Ticagrelor in ACS/PCI Which one to choose? V. Voudris MD FESC FACC 2 nd Cardiology Division Onassis Cardiac Surgery Center
 Prasugrel vs. Ticagrelor in ACS/PCI Which one to choose? V. Voudris MD FESC FACC 2 nd Cardiology Division Onassis Cardiac Surgery Center Hospitalizations in the U.S. Due to ACS Acute Coronary Syndromes
Prasugrel vs. Ticagrelor in ACS/PCI Which one to choose? V. Voudris MD FESC FACC 2 nd Cardiology Division Onassis Cardiac Surgery Center Hospitalizations in the U.S. Due to ACS Acute Coronary Syndromes
Disclosure. Financial disclosure: National Advisory Board & Research Grant from Boehringer-Ingelheim
 Randomised Dabigatran Etexilate Dose Finding Study In Patients With Acute Coronary Syndromes Post Index Event With Additional Risk Factors For Cardiovascular Complications Also Receiving Aspirin and Clopidogrel
Randomised Dabigatran Etexilate Dose Finding Study In Patients With Acute Coronary Syndromes Post Index Event With Additional Risk Factors For Cardiovascular Complications Also Receiving Aspirin and Clopidogrel
North Wales Cardiac Network Guidelines on oral antiplatelet therapy in cardiovascular disease
 Guidelines on oral antiplatelet therapy in cardiovascular disease This guidance should be considered as one part of the wider therapeutic management of patients. The indication for antiplatelet therapy
Guidelines on oral antiplatelet therapy in cardiovascular disease This guidance should be considered as one part of the wider therapeutic management of patients. The indication for antiplatelet therapy
Pros and Cons of Individual Agents Based on Large Trial Results: RELY, ROCKET, ARISTOTLE, AVERROES
 Pros and Cons of Individual Agents Based on Large Trial Results: RELY, ROCKET, ARISTOTLE, AVERROES Ralph L. Sacco, MS MD FAAN FAHA Olemberg Family Chair in Neurological Disorders Miller Professor of Neurology,
Pros and Cons of Individual Agents Based on Large Trial Results: RELY, ROCKET, ARISTOTLE, AVERROES Ralph L. Sacco, MS MD FAAN FAHA Olemberg Family Chair in Neurological Disorders Miller Professor of Neurology,
DOUBLE or TRIPLE ANTI-TROMBOTIC THERAPY in ACS. Maarten L Simoons Thoraxcenter - Erasmus MC Rotterdam - The Netherlands
 DOUBLE or TRIPLE ANTI-TROMBOTIC THERAPY in ACS Maarten L Simoons Thoraxcenter - Erasmus MC Rotterdam - The Netherlands RECENT DEVELOPMENTS Better anti-platelet agents: Prasugrel and Ticagrelor to replace
DOUBLE or TRIPLE ANTI-TROMBOTIC THERAPY in ACS Maarten L Simoons Thoraxcenter - Erasmus MC Rotterdam - The Netherlands RECENT DEVELOPMENTS Better anti-platelet agents: Prasugrel and Ticagrelor to replace
Xarelto (rivaroxaban)
") Xarelto (rivaroxaban) Policy Number: 5.01.575 Last Review: 7/2018 Origination: 6/2014 Next Review: 7/2019 LoB: ACA Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for Xarelto
Xarelto (rivaroxaban) Policy Number: 5.01.575 Last Review: 7/2018 Origination: 6/2014 Next Review: 7/2019 LoB: ACA Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for Xarelto
Using DOACs in CAD Patients in Sinus Ryhthm Results of the ATLAS ACS 2, COMPASS and COMMANDER-HF Trials
 Using DOACs in CAD Patients in Sinus Ryhthm Results of the ATLAS ACS 2, COMPASS and COMMANDER-HF Trials 19 th Annual San Diego Heart Failure Symposium for Primary Care Physicians January 11-12, 2019 La
Using DOACs in CAD Patients in Sinus Ryhthm Results of the ATLAS ACS 2, COMPASS and COMMANDER-HF Trials 19 th Annual San Diego Heart Failure Symposium for Primary Care Physicians January 11-12, 2019 La
State of the Art in the ACS Atrial Fibrillation Overlap Syndrome
 State of the Art in the ACS Atrial Fibrillation Overlap Syndrome C. Michael Gibson, M.S., M.D. Professor of Medicine, Harvard Medical School Chief, Clinical Research, Beth Israel Deaconess CV Division
State of the Art in the ACS Atrial Fibrillation Overlap Syndrome C. Michael Gibson, M.S., M.D. Professor of Medicine, Harvard Medical School Chief, Clinical Research, Beth Israel Deaconess CV Division
ANTIPLATELET REGIMENS:
 ANTIPLATELET REGIMENS: How Long, How Many? John Carter Hemphill, M.D., F.A.C.C. Chattanooga Heart Institute February 10, 2018 I have no financial disclosures. DISCLOSURES: OBJECTIVES Understand current
ANTIPLATELET REGIMENS: How Long, How Many? John Carter Hemphill, M.D., F.A.C.C. Chattanooga Heart Institute February 10, 2018 I have no financial disclosures. DISCLOSURES: OBJECTIVES Understand current
Surveying the Landscape of Oral Antiplatelet Therapy in Acute Coronary Syndrome Management
 Surveying the Landscape of Oral Antiplatelet Therapy in Acute Coronary Syndrome Management Jeffrey S Berger, MD, MS Assistant Professor of Medicine and Surgery Director of Cardiovascular Thrombosis Disclosures
Surveying the Landscape of Oral Antiplatelet Therapy in Acute Coronary Syndrome Management Jeffrey S Berger, MD, MS Assistant Professor of Medicine and Surgery Director of Cardiovascular Thrombosis Disclosures
A New Era for NOACs: What Does the Future Hold? CME
 This article is a CME certified activity. To earn credit for this activity visit: http://www.medscape.org/viewarticle/884772 www.medscape.org A New Era for NOACs: What Does the Future Hold? CME Manesh
This article is a CME certified activity. To earn credit for this activity visit: http://www.medscape.org/viewarticle/884772 www.medscape.org A New Era for NOACs: What Does the Future Hold? CME Manesh
INR as a Biomarker: Anticoagulation in Atrial Fib, Heart Failure, and Cardiovascular Disease Daniel Blanchard, MD, FACC, FAHA
 INR as a Biomarker: Anticoagulation in Atrial Fib, Heart Failure, and Cardiovascular Disease Daniel Blanchard, MD, FACC, FAHA Professor of Medicine Director, Cardiology Fellowship Program Sulpizio Cardiovascular
INR as a Biomarker: Anticoagulation in Atrial Fib, Heart Failure, and Cardiovascular Disease Daniel Blanchard, MD, FACC, FAHA Professor of Medicine Director, Cardiology Fellowship Program Sulpizio Cardiovascular
DECLARATION OF CONFLICT OF INTEREST. Lecture fees: AstraZeneca, Ely Lilly, Merck.
 DECLARATION OF CONFLICT OF INTEREST Lecture fees: AstraZeneca, Ely Lilly, Merck. Risk of stopping dual therapy. S D Kristensen, FESC Aarhus Denmark Acute coronary syndrome: coronary thrombus Platelets
DECLARATION OF CONFLICT OF INTEREST Lecture fees: AstraZeneca, Ely Lilly, Merck. Risk of stopping dual therapy. S D Kristensen, FESC Aarhus Denmark Acute coronary syndrome: coronary thrombus Platelets
Secondary Stroke Prevention: A Precautionary Tale
 Secondary Stroke Prevention: A Precautionary Tale Kirsten George-Phillips, BSP Clinical Practice Leader, AHS Clinical Pharmacist, AHS Owen Stroke Prevention Clinic Learning Objectives! Examine literature
Secondary Stroke Prevention: A Precautionary Tale Kirsten George-Phillips, BSP Clinical Practice Leader, AHS Clinical Pharmacist, AHS Owen Stroke Prevention Clinic Learning Objectives! Examine literature
DAPT in CAD, Acute & Chronic CAD, antiplatelet therapy non-responders
 DAPT in CAD, Acute & Chronic CAD, antiplatelet therapy non-responders Annual Ohio ACC Conference October 14, 2017 Ernest L. Mazzaferri Jr, MD, FACC, FSCAI Disclosures No financial disclosures related to
DAPT in CAD, Acute & Chronic CAD, antiplatelet therapy non-responders Annual Ohio ACC Conference October 14, 2017 Ernest L. Mazzaferri Jr, MD, FACC, FSCAI Disclosures No financial disclosures related to
Robert C. Welsh, MD, FRCPC Professor of Medicine, University of Alberta Zone Clinical Department Head, Cardiac Sciences
 Managing Atrial Fibrillation and ACS/PCI Applying New Evidence to Clinical Practice Dual Anti-Thrombotic Therapy in Acute Coronary Syndromes (ACS) and Afib + PCI/ACS Patients Robert C. Welsh, MD, FRCPC
Managing Atrial Fibrillation and ACS/PCI Applying New Evidence to Clinical Practice Dual Anti-Thrombotic Therapy in Acute Coronary Syndromes (ACS) and Afib + PCI/ACS Patients Robert C. Welsh, MD, FRCPC
Anti-platelet Therapies in Cardiovascular Disease: From Stable CAD to ACS and Afib!
 Anti-platelet Therapies in Cardiovascular Disease: From Stable CAD to ACS and Afib! Roxana Mehran, MD Columbia University Medical Center Cardiovascular Research Foundation Disclosures Research support
Anti-platelet Therapies in Cardiovascular Disease: From Stable CAD to ACS and Afib! Roxana Mehran, MD Columbia University Medical Center Cardiovascular Research Foundation Disclosures Research support
Results from RE-LY and RELY-ABLE
 Results from RE-LY and RELY-ABLE Assessment of the safety and efficacy of dabigatran etexilate (Pradaxa ) in longterm stroke prevention EXECUTIVE SUMMARY Dabigatran etexilate (Pradaxa ) has shown a consistent
Results from RE-LY and RELY-ABLE Assessment of the safety and efficacy of dabigatran etexilate (Pradaxa ) in longterm stroke prevention EXECUTIVE SUMMARY Dabigatran etexilate (Pradaxa ) has shown a consistent
News Release. For UK Media
 News Release For UK Media Bayer plc 400 South Oak Way Reading RG2 6AD www.bayer.co.uk Bayer s Xarelto (rivaroxaban) in combination with single antiplatelet therapy receives positive CHMP opinion for treatment
News Release For UK Media Bayer plc 400 South Oak Way Reading RG2 6AD www.bayer.co.uk Bayer s Xarelto (rivaroxaban) in combination with single antiplatelet therapy receives positive CHMP opinion for treatment
New Antithrombotic and Antiplatelet Drugs in CAD : (Factor Xa inhibitors, Direct Thrombin inhibitors and Prasugrel)
") New Antithrombotic and Antiplatelet Drugs in CAD : (Factor Xa inhibitors, Direct Thrombin inhibitors and Prasugrel) Limitations and Advantages of UFH and LMWH Biological limitations of UFH : 1. immune-mediated
New Antithrombotic and Antiplatelet Drugs in CAD : (Factor Xa inhibitors, Direct Thrombin inhibitors and Prasugrel) Limitations and Advantages of UFH and LMWH Biological limitations of UFH : 1. immune-mediated
Disclosure Slide. Controversies in Anticoagulation. Presenter Disclosure Information. Challenges in Anticoagulation
 1:15 2:15 PM Challenges in Anticoagulation SPEAKER Nasser Lakkis, MD, FACC, FSCAI Presenter Disclosure Information The following relationships exist related to this presentation: Nasser Lakkis, MD, FACC,
1:15 2:15 PM Challenges in Anticoagulation SPEAKER Nasser Lakkis, MD, FACC, FSCAI Presenter Disclosure Information The following relationships exist related to this presentation: Nasser Lakkis, MD, FACC,
SCA ST- : recommandations européennes 2015 La durée de la bithérapie : à géométrie variable?
 SCA ST- : recommandations européennes 2015 La durée de la bithérapie : à géométrie variable? tielle est 2 ré Totielle est interdite. Prof. Marco Roffi Hôpitaux Universitaires de Genève Research funding
SCA ST- : recommandations européennes 2015 La durée de la bithérapie : à géométrie variable? tielle est 2 ré Totielle est interdite. Prof. Marco Roffi Hôpitaux Universitaires de Genève Research funding
What s new with DOACs? Defining place in therapy for edoxaban &
 What s new with DOACs? Defining place in therapy for edoxaban & Use of DOACs in cardioversion Caitlin M. Gibson, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy University of North Texas
What s new with DOACs? Defining place in therapy for edoxaban & Use of DOACs in cardioversion Caitlin M. Gibson, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy University of North Texas
A Patient with Chest Pain and Atrial Fibrillation
 A Patient with Chest Pain and Atrial Fibrillation Kurt Huber, Vienna, Austria Declaration of Interest Lecturing & Consulting Activities: AstraZeneca, Boehringer-Ingelheim, Bristol-Myers Squibb, Daiichi
A Patient with Chest Pain and Atrial Fibrillation Kurt Huber, Vienna, Austria Declaration of Interest Lecturing & Consulting Activities: AstraZeneca, Boehringer-Ingelheim, Bristol-Myers Squibb, Daiichi
Edoxaban in Atrial Fibrillation
 Edoxaban in Atrial Fibrillation Glenn Gormley, MD, PhD Senior Executive Officer and Global Head of R&D, Daiichi Sankyo Co., Ltd Nov. 4, 2014 Tuesday Background Based on the results of ENGAGE AF-TIMI 48,
Edoxaban in Atrial Fibrillation Glenn Gormley, MD, PhD Senior Executive Officer and Global Head of R&D, Daiichi Sankyo Co., Ltd Nov. 4, 2014 Tuesday Background Based on the results of ENGAGE AF-TIMI 48,
Acute Coronary syndrome
 Acute Coronary syndrome 7th Annual Pharmacotherapy Conference ACS Pathophysiology rupture or erosion of a vulnerable, lipidladen, atherosclerotic coronary plaque, resulting in exposure of circulating blood
Acute Coronary syndrome 7th Annual Pharmacotherapy Conference ACS Pathophysiology rupture or erosion of a vulnerable, lipidladen, atherosclerotic coronary plaque, resulting in exposure of circulating blood
The Great debate: thrombocardiology post-compass
 The Great debate: thrombocardiology post-compass Anticoagulation should replace antiplatelets in CAD prevention - CON Jean-Philippe COLLET Jean-philippe.collet@psl.aphp.fr Sorbonne Université_Action Study
The Great debate: thrombocardiology post-compass Anticoagulation should replace antiplatelets in CAD prevention - CON Jean-Philippe COLLET Jean-philippe.collet@psl.aphp.fr Sorbonne Université_Action Study
Novel Anticoagulants PHYSICIANS UPDATE 2014
 Novel Anticoagulants PHYSICIANS UPDATE 2014 Farouk Mookadam MD FRCPC FACC MSc Professor College of Medicine Mayo Consultant Cardiovascular Diseases Medical Director Anticoagulation Clinic Assoc Programme
Novel Anticoagulants PHYSICIANS UPDATE 2014 Farouk Mookadam MD FRCPC FACC MSc Professor College of Medicine Mayo Consultant Cardiovascular Diseases Medical Director Anticoagulation Clinic Assoc Programme
The Korean Society of Cardiology COI Disclosure
 The Korean Society of Cardiology COI Disclosure Name of First Author: Yongwhi Park The authors have no financial conflicts of interest to disclose concerning the presentation 2017 Annual Spring Scientific
The Korean Society of Cardiology COI Disclosure Name of First Author: Yongwhi Park The authors have no financial conflicts of interest to disclose concerning the presentation 2017 Annual Spring Scientific
Optimal antiplatelet and anticoagulant therapy for patients treated in STEMI network
 Torino 6 Joint meeting with Mayo Clinic Great Innovation in Cardiology 14-15 Ottobre 2010 Optimal antiplatelet and anticoagulant therapy for patients treated in STEMI network Diego Ardissino Ischemic vs
Torino 6 Joint meeting with Mayo Clinic Great Innovation in Cardiology 14-15 Ottobre 2010 Optimal antiplatelet and anticoagulant therapy for patients treated in STEMI network Diego Ardissino Ischemic vs
Direct Oral Anticoagulants An Update
 Oct. 26, 2017 Direct Oral Anticoagulants An Update Kathleen Heintz, DO, FACC Assistant Professor of Medicine Cooper Heart Institute Direct Oral Anticoagulants: DISCLAIMERS No Conflicts of Interest So what
Oct. 26, 2017 Direct Oral Anticoagulants An Update Kathleen Heintz, DO, FACC Assistant Professor of Medicine Cooper Heart Institute Direct Oral Anticoagulants: DISCLAIMERS No Conflicts of Interest So what
STEMI 2014 YAHYA KIWAN. Consultant Cardiologist Head Of Cardiology Belhoul Specialty Hospital
 STEMI 2014 YAHYA KIWAN Consultant Cardiologist Head Of Cardiology Belhoul Specialty Hospital Aspiration Thrombectomy Manual aspiration thrombectomy is reasonable for patients undergoing primary PCI. I
STEMI 2014 YAHYA KIWAN Consultant Cardiologist Head Of Cardiology Belhoul Specialty Hospital Aspiration Thrombectomy Manual aspiration thrombectomy is reasonable for patients undergoing primary PCI. I
Triple Antithrombotic Therapy: Is it Time to Drop the Aspirin?
 HOSPITAL CHRONICLES 2015, 10(1): 7 18 Review Triple Antithrombotic Therapy: Is it Time to Drop the Aspirin? Prokopis Papadimitriou, MD, MSc Abstract Department of Cardiology, Evagelismos General Hospital
HOSPITAL CHRONICLES 2015, 10(1): 7 18 Review Triple Antithrombotic Therapy: Is it Time to Drop the Aspirin? Prokopis Papadimitriou, MD, MSc Abstract Department of Cardiology, Evagelismos General Hospital
Eliquis and plavix combination therapy
 Eliquis and plavix combination therapy ELIQUIS Dosing for Patients With NVAF. patients treated with aspirin or the combination of bleeding or completion of a course of therapy,. 9-11-2011 Thrombosis is
Eliquis and plavix combination therapy ELIQUIS Dosing for Patients With NVAF. patients treated with aspirin or the combination of bleeding or completion of a course of therapy,. 9-11-2011 Thrombosis is
Supplementary Table S1: Proportion of missing values presents in the original dataset
 Supplementary Table S1: Proportion of missing values presents in the original dataset Variable Included (%) Missing (%) Age 89067 (100.0) 0 (0.0) Gender 89067 (100.0) 0 (0.0) Smoking status 80706 (90.6)
Supplementary Table S1: Proportion of missing values presents in the original dataset Variable Included (%) Missing (%) Age 89067 (100.0) 0 (0.0) Gender 89067 (100.0) 0 (0.0) Smoking status 80706 (90.6)
ANTIPLATELET THERAPY ANTIPLATELET THERAPY ANTIPLATELET THERAPY
 ANTIPLATELET THERAPY 2018 UPDATE ANTIPLATELET THERAPY ANTIPLATELET THERAPY About this Pocket Guide This pocket guide is a quick-reference tool that features diagnostic and management recommendations based
ANTIPLATELET THERAPY 2018 UPDATE ANTIPLATELET THERAPY ANTIPLATELET THERAPY About this Pocket Guide This pocket guide is a quick-reference tool that features diagnostic and management recommendations based
תרופות מעכבות טסיות חדשות ד"ר אלי לב מנהל שרות הצנתורים ח השרון מרכז רפואי רבין
 תרופות מעכבות טסיות חדשות ד"ר אלי לב מנהל שרות הצנתורים ח השרון בי""י מרכז רפואי רבין 1. Why should clopidogrel be replaced? 2. Prasugrel 3. Ticagrelor 4. Conclusions CURE TRIAL ACS pts 20 % reduction
תרופות מעכבות טסיות חדשות ד"ר אלי לב מנהל שרות הצנתורים ח השרון בי""י מרכז רפואי רבין 1. Why should clopidogrel be replaced? 2. Prasugrel 3. Ticagrelor 4. Conclusions CURE TRIAL ACS pts 20 % reduction
Updates in Stroke Management. Jessica A Starr, PharmD, FCCP, BCPS Associate Clinical Professor Auburn University Harrison School of Pharmacy
 Updates in Stroke Management Jessica A Starr, PharmD, FCCP, BCPS Associate Clinical Professor Auburn University Harrison School of Pharmacy Disclosure I have no actual or potential conflict of interest
Updates in Stroke Management Jessica A Starr, PharmD, FCCP, BCPS Associate Clinical Professor Auburn University Harrison School of Pharmacy Disclosure I have no actual or potential conflict of interest
HERTFORDSHIRE MEDICINES MANAGEMENT COMMITTEE (HMMC) DABIGATRAN RECOMMENDED What it is Indications Date decision last revised
 DABIGATRAN RECOMMENDED What it is Indications Date decision last revised") Name: generic (trade) Dabigatran etexilate (Pradaxa ) HERTFORDSHIRE MEDICINES MANAGEMENT COMMITTEE (HMMC) DABIGATRAN RECOMMENDED What it is Indications Date decision last revised Direct thrombin inhibitor
Name: generic (trade) Dabigatran etexilate (Pradaxa ) HERTFORDSHIRE MEDICINES MANAGEMENT COMMITTEE (HMMC) DABIGATRAN RECOMMENDED What it is Indications Date decision last revised Direct thrombin inhibitor
Randomized Comparison of Prasugrel and Bivalirudin versus Clopidogrel and Heparin in Patients with ST-Segment Elevation Myocardial Infarction
 Randomized Comparison of Prasugrel and Bivalirudin versus Clopidogrel and Heparin in Patients with ST-Segment Elevation Myocardial Infarction The Bavarian Reperfusion Alternatives Evaluation (BRAVE) 4
Randomized Comparison of Prasugrel and Bivalirudin versus Clopidogrel and Heparin in Patients with ST-Segment Elevation Myocardial Infarction The Bavarian Reperfusion Alternatives Evaluation (BRAVE) 4
Διάρκεια διπλής αντιαιμοπεταλιακής αγωγής. Νικόλαος Γ.Πατσουράκος Καρδιολόγος, Επιμελητής Α ΕΣΥ Τζάνειο Γενικό Νοσοκομείο Πειραιά
 Διάρκεια διπλής αντιαιμοπεταλιακής αγωγής Νικόλαος Γ.Πατσουράκος Καρδιολόγος, Επιμελητής Α ΕΣΥ Τζάνειο Γενικό Νοσοκομείο Πειραιά International ACS guidelines: Recommendations on duration of dual
Διάρκεια διπλής αντιαιμοπεταλιακής αγωγής Νικόλαος Γ.Πατσουράκος Καρδιολόγος, Επιμελητής Α ΕΣΥ Τζάνειο Γενικό Νοσοκομείο Πειραιά International ACS guidelines: Recommendations on duration of dual
Update on Antiplatelet Therapy
 Update on Antiplatelet Therapy Christine Ibarra Pharm.D. PGY-1 Baptist Hospital of Miami Objectives Explain the role of antiplatelettherapy in prevention of cardiovascular events Appreciate differences
Update on Antiplatelet Therapy Christine Ibarra Pharm.D. PGY-1 Baptist Hospital of Miami Objectives Explain the role of antiplatelettherapy in prevention of cardiovascular events Appreciate differences
7 th Munich Vascular Conference
 7 th Munich Vascular Conference Secondary prevention of major cardiovascular events in patients with CHD or PAD - What can we learn from EUCLID and COMPASS, evaluating Clopidogrel, Ticagrelor and Univ.-Prof.
7 th Munich Vascular Conference Secondary prevention of major cardiovascular events in patients with CHD or PAD - What can we learn from EUCLID and COMPASS, evaluating Clopidogrel, Ticagrelor and Univ.-Prof.
The Future of Oral Antiplatelets in PAD and CAD Christopher Paris, MD, FACC, FSCAI
 The Future of Oral Antiplatelets in PAD and CAD Christopher Paris, MD, FACC, FSCAI Interventional Cardiologist Cardiovascular Institute of the South Director of Cardiovascular Services St. Charles Parish
The Future of Oral Antiplatelets in PAD and CAD Christopher Paris, MD, FACC, FSCAI Interventional Cardiologist Cardiovascular Institute of the South Director of Cardiovascular Services St. Charles Parish
Belinda Green, Cardiologist, SDHB, 2016
 Acute Coronary syndromes All STEMI ALL Non STEMI Unstable angina Belinda Green, Cardiologist, SDHB, 2016 Thrombus in proximal LAD Underlying pathophysiology Be very afraid for your patient Wellens
Acute Coronary syndromes All STEMI ALL Non STEMI Unstable angina Belinda Green, Cardiologist, SDHB, 2016 Thrombus in proximal LAD Underlying pathophysiology Be very afraid for your patient Wellens
Investor Conference Call
 Investor Conference Call Data from the Phase III COMPASS trial, A Randomized Controlled Trial of Rivaroxaban for the Prevention of Major Cardiovascular Events in Patients With Coronary or Peripheral Artery
Investor Conference Call Data from the Phase III COMPASS trial, A Randomized Controlled Trial of Rivaroxaban for the Prevention of Major Cardiovascular Events in Patients With Coronary or Peripheral Artery
Προβληματισμοι στην χρηση αντιαιμοπεταλιακων στα οξέα ισχαιμικά σύνδρομα
 Α ΚΑΡΔΙΟΛΟΓΙΚΗ ΚΛΙΝΙΚΗ ΚΑΙ ΟΜΩΝΥΜΟ ΕΡΓΑΣΤΗΡΙΟ ΙΑΤΡΙΚΗ ΣΧΟΛΗ ΠΑΝΕΠΙΣΤΗΜΙΟΥ ΑΘΗΝΩΝ ΙΠΠΟΚΡΑΤΕΙΟ ΓΕΝΙΚΟ ΝΟΣΟΚΟΜΕΙΟ ΑΘΗΝΩΝ Διευθυντής: Καθηγητής ΔΗΜΗΤΡΙΟΣ ΤΟΥΣΟΥΛΗΣ Προβληματισμοι στην χρηση αντιαιμοπεταλιακων
Α ΚΑΡΔΙΟΛΟΓΙΚΗ ΚΛΙΝΙΚΗ ΚΑΙ ΟΜΩΝΥΜΟ ΕΡΓΑΣΤΗΡΙΟ ΙΑΤΡΙΚΗ ΣΧΟΛΗ ΠΑΝΕΠΙΣΤΗΜΙΟΥ ΑΘΗΝΩΝ ΙΠΠΟΚΡΑΤΕΙΟ ΓΕΝΙΚΟ ΝΟΣΟΚΟΜΕΙΟ ΑΘΗΝΩΝ Διευθυντής: Καθηγητής ΔΗΜΗΤΡΙΟΣ ΤΟΥΣΟΥΛΗΣ Προβληματισμοι στην χρηση αντιαιμοπεταλιακων
FastTest. You ve read the book now test yourself
 FastTest You ve read the book...... now test yourself To ensure you have learned the key points that will improve your patient care, read the authors questions below. The answers will refer you back to
FastTest You ve read the book...... now test yourself To ensure you have learned the key points that will improve your patient care, read the authors questions below. The answers will refer you back to
Optimal Duration and Dose of Antiplatelet Therapy after PCI
 Optimal Duration and Dose of Antiplatelet Therapy after PCI Donghoon Choi, MD, PhD Severance Cardiovascular Center Yonsei University College of Medicine Optimal Duration of Antiplatelet Therapy after PCI
Optimal Duration and Dose of Antiplatelet Therapy after PCI Donghoon Choi, MD, PhD Severance Cardiovascular Center Yonsei University College of Medicine Optimal Duration of Antiplatelet Therapy after PCI
Dual Antiplatelet Therapy: Time for a Paradigm Shift?
 Dual Antiplatelet Therapy: Time for a Paradigm Shift? 5 years after PLATO Experience from the Daily Clinical Practice Hans Rickli Goals with antithrombotic treatment Acute coronary syndrome Risk reduction
Dual Antiplatelet Therapy: Time for a Paradigm Shift? 5 years after PLATO Experience from the Daily Clinical Practice Hans Rickli Goals with antithrombotic treatment Acute coronary syndrome Risk reduction
ΔΙΑΧΕΙΡΙΣΗ ΑΣΘΕΝΩΝ ΜΕ ΣΤΕΦΑΝΙΑΙΑ ΚΑΡΔΙΟΠΑΘΕΙΑ ΚΑΙ ΚΟΛΠΙΚΗ ΜΑΡΜΑΡΥΓΗ:ΚΙΝΔΥΝΟΙ ΚΑΙ ΟΦΕΛΗ ΔΙΠΛΗΣ ΚΑΙ ΤΡΙΠΛΗΣ ΘΕΡΑΠΕΙΑΣ
 ΔΙΑΧΕΙΡΙΣΗ ΑΣΘΕΝΩΝ ΜΕ ΣΤΕΦΑΝΙΑΙΑ ΚΑΡΔΙΟΠΑΘΕΙΑ ΚΑΙ ΚΟΛΠΙΚΗ ΜΑΡΜΑΡΥΓΗ:ΚΙΝΔΥΝΟΙ ΚΑΙ ΟΦΕΛΗ ΔΙΠΛΗΣ ΚΑΙ ΤΡΙΠΛΗΣ ΘΕΡΑΠΕΙΑΣ Χρήστος Δ.Καλλιάνος Α Καρδιολογικό τμήμα και Ηλεκτροφυσιολογικό Εργαστήριο ΓΝΑ «Ο Ευαγγελισμός»
ΔΙΑΧΕΙΡΙΣΗ ΑΣΘΕΝΩΝ ΜΕ ΣΤΕΦΑΝΙΑΙΑ ΚΑΡΔΙΟΠΑΘΕΙΑ ΚΑΙ ΚΟΛΠΙΚΗ ΜΑΡΜΑΡΥΓΗ:ΚΙΝΔΥΝΟΙ ΚΑΙ ΟΦΕΛΗ ΔΙΠΛΗΣ ΚΑΙ ΤΡΙΠΛΗΣ ΘΕΡΑΠΕΙΑΣ Χρήστος Δ.Καλλιάνος Α Καρδιολογικό τμήμα και Ηλεκτροφυσιολογικό Εργαστήριο ΓΝΑ «Ο Ευαγγελισμός»