Steven Frachtman, M.D. Division of Gastroenterology/Hepatology August 18, 2011
|
|
|
- Grant Joseph
- 5 years ago
- Views:
Transcription




1 Steven Frachtman, M.D. Division of Gastroenterology/Hepatology August 18, 2011
2 Review normal esophageal anatomy and physiology Classifications of esophageal motility disorders Clinical features/diagnosis/management of specific disorders
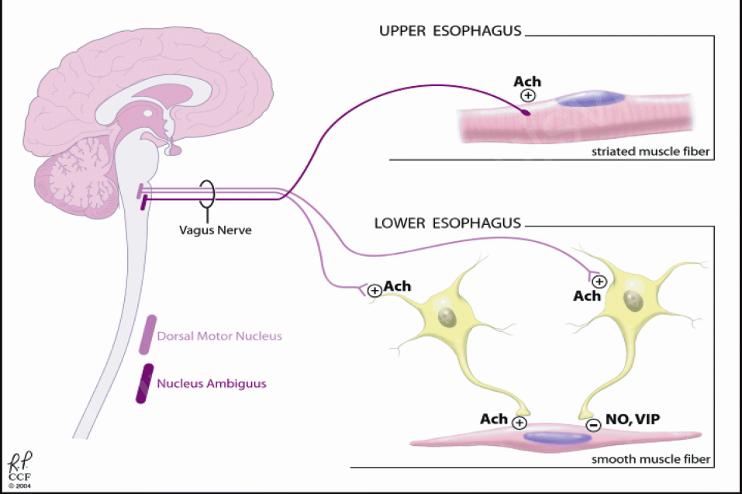
3 20-22 cm muscular tube (skeletal + smooth) Proximal 5% striated including the UES, middle 35-40% smooth, distal 50-60% entirely smooth Peristalsis controlled by: 1. Extrinsic innervation via the vagus nerve 2. Autonomous control in the myenteric plexus
4 Proximal striated muscle receives excitatory vagal innervation only Distal smooth muscle/les receives vagal innervation via synapses within the myenteric plexus (autonomic nerve network between the longitudinal and circular muscle layers) Excitatory neurons mediate contraction via nicotnic cholinergic receptors Inhibitory neurons mediate relaxation via nitric oxide inhibition of muscarinic cholinergic neurons
5 Primary peristalsis initiated by a swallow, secondary peristalsis by esophageal distention Deglutitive inhibition: second swallow (initiated while an earlier peristaltic contraction is still progressing) causes inhibition of the contraction induced by first swallow 1. Vagal mediated contraction in the proximal esophagus 2. Vagal mediated contraction/inhibition in the distal esophagus via the myenteric plexus 3. Autonomous myenteric plexus control of peristaltic progression/secondary peristalsis
6
7
8 Dysphagia to both solids and liquids Associated GERD, regurgitation, chest pain, odynophagia Absence of immediate symptoms, associated aspiration, or cough (suggestive of oropharyngeal dysphagia) Patient localization of obstruction in esophageal dysphagia is inaccurate
9 Barium swallow with tablet EGD MBS (1. delay in initiation of pharyngeal swallowing 2. aspiration 3. nasopharyngeal regurgitation 4. residue of the ingestate within the pharyngeal cavity after swallowing) Esophageal manometry: most useful when esophageal motility disorder suspected (obstruction or oropharyngeal cause ruled out), in confirming a diagnosis of Achalasia, pre-op assessment prior to anti-reflux surgery
10 Primary vs. Secondary disorders (associated with generalized disease) Chicago Classification (Normal vs. Impaired GEJ relaxation Hypercontracting vs. Hypocontracting esophagus
11 Hypercontracting Esophagus: DES Nutcracker Hypertensive LES Hypocontracting Esophagus: Primary Achalasia Secondary Achalasia/Impaired Esohageal Motility: Connective tissue diseases, Endocrine diseases, Neuromuscular diseases, Paraneoplastic syndromes
12 Epidemiology Most easily recognized and best defined motor disorder of the esophagus Annual incidence 1/100,000 Affects both genders equally Presents between ages yrs old Reports of familial clustering but a genetic determinant is not strong
13 Pathogenesis Characterized by impaired LES relaxation with swallowing and aperistalsis in the smooth muscle esophagus Resting LES pressure elevated in about 60% of cases (normal mmhg) Loss of inhibitory neurons in the Myenteric Plexus which mediate deglutitive inhibition (including LES relaxation) and sequenced propagation of esophageal peristalsis Autoimmune response to viral infection (HSV-1 possible culprit)
14 Clinical features: Solid food dysphagia with variable degrees of liquid dysphagia Nocturnal regurgitation Chest pain (spasm, progressive esophageal dilation) Paradoxical complaint of heartburn (periods of esophageal acidification due to bacterial fermentation of retained food as opposed to frank GERD) Weight loss Aspiration/Choking
15 Risk of Squamous Cell Cancer Relative risk estimated at 33-fold Exact pathogenesis unclear but stasis esophagitis a likely precipitating factor Often advanced at time of detection Given 0.15% incidence, surveillance program currently not the standard practice

16

17
18
19 Chagas disease Endemic to Brazil, Venezuela, Argentina Spread by bite of reduvid bug that transmits T. cruzi Destruction of autonomic ganglion cells (can be indistinguishable from Achalasia) Most obvious clinical distinction is evidence of additional organ involvement Treatment for esophageal involvement similar to Achalasia
20 Pseudoachalasia: Tumor related pseudoachalasia accounts for up to 5% of cases with manometrically defined achalasia More likely in older age groups, recent onset of symptoms, early weight loss Tumor infiltration (carcinoma in gastric fundus) can completely mimic functional impairment in achalasia (thorough examination during EGD) Higher resistance to scope passage across GE junction
21 Pseudoachalasia: Adenocarcinoma of GE junction accounts for more than ½ of pseudoachalasia cases Pancreatic, hepatoma, lung, SCC esophagus, prostate, lymphoma reported (infiltrating wall of esophagus at GE junction) Esophageal infiltration by Amyloid Paraneoplastic syndrome?
22 Postsurgical: Aperistalsis and impaired LES relaxation can be seen following fundoplication Administer amyl nitrite during manometry Mechanical effect of a fundoplication is less affected by the smooth muscle relaxing effects compared to the hypertensive sphincter of a person with achalasia
23 Pharmacologic Therapy Largest reported experience with Isordil and Nifedepine Isordil 5 to 10 mg sl qac reducing LES pressure by 66% for about 90 mins (no placebo controlled trials) Nifedepine 10 mg sl qac reduced LES pressure by 30-40% for more than one hour (subsequent placebo controlled trials showed minimal benefit)
24 Botox injections Initial landmark study reported injection of 80 units (divided doses into 4 quadrants of the LES) decreased LES pressure by 33% and improved dysphagia in 66% of patients for 6 month period Irreversibly inhibits release of acetylcholine from presynaptic cholingergic terminals Inhibitory effect eventually reversed by growth of new axons Not a long lasting therapy; minimal continued efficacy at one year Reserved for older patients who are not candidates for more definitive therapy
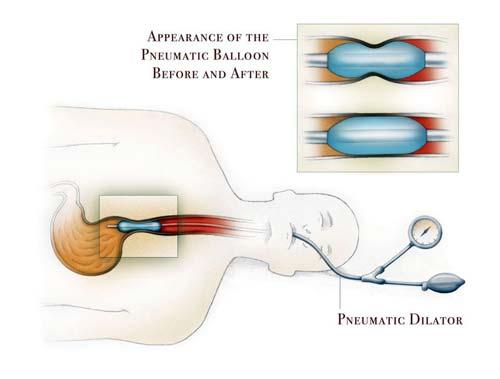
25 Pneumatic Dilation Therapeutic dilation requires distention of LES to diameter of at least 3 cm for lasting reduction of LES pressure (partially disrupting circular muscle of the sphincter) Dilation with endoscope, standard bougies, balloon dilators provides temporary benefit at best Achalasia dilator: long noncompliant cylindrical balloon that can be positioned across LES fluoroscopically or endoscopically and inflated in a controlled fashion with a handheld manometer
26 Pneumatic Dilation Technique variable in terms of patient preparation, parameters of balloon inflation, and post-dilation monitoring Cautious approach of starting with small diameter dilator (3 cm) and progressing only when smaller dilator ineffective is fairly universal Proper position at LES (observe waist of the hourglass shaped balloon silhouette and that the waist fully effaces as inflation proceeds)
27
28 Pneumatic Dilation Major complication is esophageal perforation (1% to 5%) Fluoroscopic examination after dilation (water soluble contrast followed by barium) Suspect when there is post-procedure pain or subcutaneous emphysema If perforation appears small, contained, intramural then conservative management in hospital Substantial perforation surgical repair Best predictor of efficacy is post-dilation LES pressure less than 10 mmhg
29 Pneumatic Dilation In cases of unsatisfactory result, reasonable to perform subsequent dilation within matter of weeks If benefit lasted > 1 yr, neither unusual or dangerous to repeat dilation as necessary Clinical efficacy 32% to 98% Patient with poor initial result or rapid recurrence of symptoms are less likely to respond to additional dilations Subsequent response to surgical myotomy not influenced by history of previous dilations
30 Heller Myotomy Offers more predictable method of reducing LES pressure Considerable morbidity related to thoracotomy Laparoscopic approach with similar efficacy, reduced morbidity Overall mortality less than 2% Published series report good to excellent results in 62 to 100% of pts with persistent dysphagia present in less than 10% Postmyotomy reflux Laparoscopic Heller myotomy combined with partial fundoplication become preferred surgical procedure Unsatisfactory results: incomplete myotomy, scarring of myotomy, functional esophageal obstruction
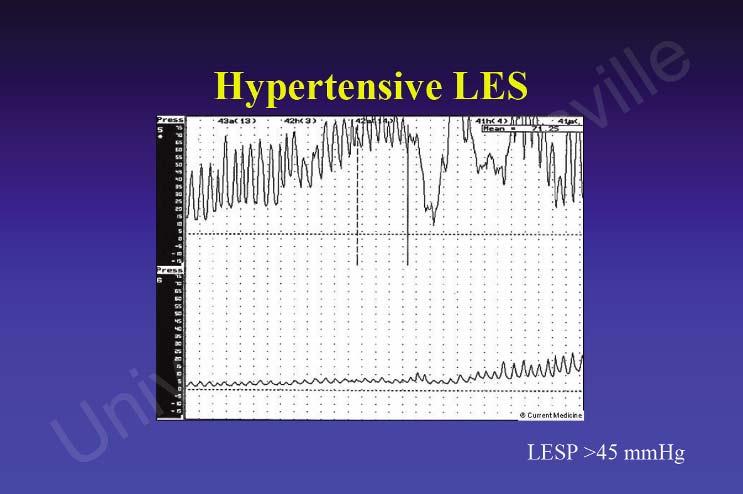
31 DES Nutcracker Esophagus Hypertensive LES
32 Epidemiology Also known as distal esophageal spasm (only smooth muscle affected) A disorder or peristalsis but in most pts, esophagus retains ability propagate normally majority of the time No known risk factors or other associated conditions Neuromuscular pathology more subtle than in Achalasia and is unknown Most striking reported pathologic change is diffuse muscular hypertrophy/hyperplasia in distal esophagus Despite absence of defined histopathology, physiologic evidence suggests myenteric plexus neuronal dysfunction
33 Epidemiology: Vagal impulses reach entire smooth muscle segment of esophagus simultaneously and activate myenteric plexus neurons Ganglionic neurons intervening between vagal fibers and smooth muscle belong to either inhibitory population (inhibit contraction) or excitatory population (promoting contraction) Experimental evidence suggest heterogeneity among patients, some with primarily a defect in inhibitory function vs. others with primarily excess excitation Imbalance between excitatory and inhibitory influences on the esophageal smooth muscle
34 Clinical Features: Main symptoms are dysphagia and chest pain Dysphagia usually intermittent and sometimes related to swallowing specific substances (liquids at extreme temps) Chest pain description often sounds like angina Pain lasts mins to hours; continued swallowing not always impaired Mechanism of pain unclear sustained contraction? Symptoms non-specific Rule out more common esophageal disorders (peptic or infectious esophagitis)

35 Diagnosis Barium Swallow: Radiographic findings variable from normal to severe non-peristaltic contractions that can produce striking abnormalities in barium column ( corkscrew esophagus )
36 Diagnosis Manometry: Variety of motility patterns high amplitude (>180 mmhg), repetitive simultaneous, and prolonged duration contractions (>6sec) 20% or more simultaneous contractions in distal esophagus is hallmark to suggest the diagnosis 1/3 of pts with DES will have associated abnormalities of the LES including high resting pressure (> 40 mmhg) or incomplete relaxation
37

38
39 Manometric finding of high amplitude peristaltic contractions in the distal 10 cm of the esophagus with average pressures exceeding 220 mmhg Normal deglutitive LES relaxation The following may or may not be present: repetitive contractions (> 2 peaks), prolonged contractions (>6sec), increased resting LES pressure (>40 mmhg) Studies using high frequency intraluminal US have demonstrated asynchronous contractions of the circular and longitudinal muscle layers Asynchrony reversed after administration of atropine (suggesting pathogenesis in part related to hypercholinergic state)
40
41 Manometric finding of increased resting LES pressure (> 40 mmhg) Incomplete relaxation may be present Two studies demonstrated that 50% of patients with hypertensive LES also had the high amplitude distal peristaltic waves of nutcracker esophagus
42
43 Specific therapies difficult to define since both the pathophysiology and relation of motility findings to symptoms remain obscure Minimal data from prospective controlled observations; those that are positive with small number patients Therapies initially centered on improving esophageal contractility and emptying (limited efficacy other than in achalasia)
44 Treatment with smooth muscle relaxants supported by clinical trials but response is variable at best Positive anecdotal results with nitrates, anticholinergic drugs, bougie dilation, botox, sidenafil 29 symptomatic pts with spastic motility disorder treated with total of 100 units z-line. Response(50% reduction in sx s) seen in 70% of patients with average duration of relief 7 months. (Miller et al, Am J Gastro 2002) Sildenafil (50 mg po qd) associated with symptom relief in group of 11 pts with spastic motility disorders (Eherer et al Gut 2002) Minimal clinical support/greater potential adverse effects Pneumatic dilation Esophagomyotomy
45 Paradigm shift: abnormal manometric findings indicative of symptomatic hypercontractility states may actually be related to hypersensitivity syndromes or external stimuli (GERD) Many pts with hypercontracting esophagus have GERD and have improvement in symptoms with PPI (Achem et al Am J Gastroenterology 1993). Trazadone shown to be effective in controlled trials in relieving chest pain (Clouse et al, Gastro 1987)
A CURIOUS CASE OF HYPERTENSIVE LES. Erez Hasnis Department of Gastroenterology Rambam Health Care Campus
 A CURIOUS CASE OF HYPERTENSIVE LES Erez Hasnis Department of Gastroenterology Rambam Health Care Campus CASE DESCRIPTION 63yo, F, single, attending nurse. PMH includes T2DM (Sitagliptin/Metformin), Hyperlipidemia
A CURIOUS CASE OF HYPERTENSIVE LES Erez Hasnis Department of Gastroenterology Rambam Health Care Campus CASE DESCRIPTION 63yo, F, single, attending nurse. PMH includes T2DM (Sitagliptin/Metformin), Hyperlipidemia
Esophageal Manometry. John M. Wo, M.D. October 1, 2009
 Esophageal Manometry John M. Wo, M.D. October 1, 2009 Esophageal Manometry Anatomy and physiology of the esophagus Conventional esophageal manometry High resolution esophageal manometry (Pressure Topography)
Esophageal Manometry John M. Wo, M.D. October 1, 2009 Esophageal Manometry Anatomy and physiology of the esophagus Conventional esophageal manometry High resolution esophageal manometry (Pressure Topography)
Oesophageal Disorders
 Oesophageal Disorders Anatomy Upper sphincter Oesophageal body Diaphragm Lower sphincter Gastric Cardia Symptoms Of Oesophageal Disorders Dysphagia Odynophagia Heartburn Atypical Chest Pain Regurgitation
Oesophageal Disorders Anatomy Upper sphincter Oesophageal body Diaphragm Lower sphincter Gastric Cardia Symptoms Of Oesophageal Disorders Dysphagia Odynophagia Heartburn Atypical Chest Pain Regurgitation
Treating Achalasia. When to consider surgery and New options for therapy
 Treating Achalasia When to consider surgery and New options for therapy James B. Wooldridge,Jr., MD Ochsner Medical Center Senior Staff Surgeon General, Laparoscopic, and Bariatric Surgery Disclosures
Treating Achalasia When to consider surgery and New options for therapy James B. Wooldridge,Jr., MD Ochsner Medical Center Senior Staff Surgeon General, Laparoscopic, and Bariatric Surgery Disclosures
9/18/2015. Disclosures. Objectives. Dysphagia Sherri Ekobena PA-C. I have no relevant financial interests to disclose I have no conflicts of interest
 Dysphagia Sherri Ekobena PA-C Disclosures I have no relevant financial interests to disclose I have no conflicts of interest Objectives Define what dysphagia is Define types of dysphagia Define studies
Dysphagia Sherri Ekobena PA-C Disclosures I have no relevant financial interests to disclose I have no conflicts of interest Objectives Define what dysphagia is Define types of dysphagia Define studies
Esophageal Motor Abnormalities
 Esophageal Motor Abnormalities Brooks D. Cash, MD, FACP, AGAF, FACG, FASGE Professor of Medicine Gastroenterology Division University of South Alabama Mobile, AL High Resolution Manometry Late Ray Clouse,
Esophageal Motor Abnormalities Brooks D. Cash, MD, FACP, AGAF, FACG, FASGE Professor of Medicine Gastroenterology Division University of South Alabama Mobile, AL High Resolution Manometry Late Ray Clouse,
Gastroesophageal Reflux Disease, Paraesophageal Hernias &
 530.81 553.3 & 530.00 43289, 43659 1043432842, MD Assistant Clinical Professor of Surgery, UH JABSOM Associate General Surgery Program Director Director of Minimally Invasive & Bariatric Surgery Programs
530.81 553.3 & 530.00 43289, 43659 1043432842, MD Assistant Clinical Professor of Surgery, UH JABSOM Associate General Surgery Program Director Director of Minimally Invasive & Bariatric Surgery Programs
THORACIC SURGERY: Dysphagia. Dr. Robert Zeldin Dr. John Dickie Dr. Carmine Simone. Thoracic Surgery Toronto East General Hospital
 THORACIC SURGERY: Dysphagia Dr. Robert Zeldin Dr. John Dickie Dr. Carmine Simone Thoracic Surgery Toronto East General Hospital Objectives Definitions Common causes Investigations Treatment options Anatomy
THORACIC SURGERY: Dysphagia Dr. Robert Zeldin Dr. John Dickie Dr. Carmine Simone Thoracic Surgery Toronto East General Hospital Objectives Definitions Common causes Investigations Treatment options Anatomy
Surgical aspects of dysphagia
 Dysphagia Why is dysphagia important? Surgery Surgical aspects of dysphagia Adrian P. Ireland aireland@eircom.net Academic RCSI Department of Surgery, Beaumont Hospital Why important Definitons Swallowing
Dysphagia Why is dysphagia important? Surgery Surgical aspects of dysphagia Adrian P. Ireland aireland@eircom.net Academic RCSI Department of Surgery, Beaumont Hospital Why important Definitons Swallowing
Per-oral Endoscopic Myotomy
 POEM With the Flexible Scope as a Treatment for Achalasia and Zenker's Diverticulum Abraham Mathew, MD, MSc Professor of Medicine Penn State College of Medicine Penn State Hershey Medical Center Per-oral
POEM With the Flexible Scope as a Treatment for Achalasia and Zenker's Diverticulum Abraham Mathew, MD, MSc Professor of Medicine Penn State College of Medicine Penn State Hershey Medical Center Per-oral
ESOPHAGEAL MOTOR DISORDERS
 Medicine Dr. Taha Alkarbuli Lecture 1 (Esophageal & GIT Disorders) ESOPHAGEAL DISORDERS: - ESOPHAGEAL MOTOR DISORDERS. - GERD - ESOPHAGEAL TUMORS. ESOPHAGEAL MOTOR DISORDERS Present with chest pain, dysphagia,
Medicine Dr. Taha Alkarbuli Lecture 1 (Esophageal & GIT Disorders) ESOPHAGEAL DISORDERS: - ESOPHAGEAL MOTOR DISORDERS. - GERD - ESOPHAGEAL TUMORS. ESOPHAGEAL MOTOR DISORDERS Present with chest pain, dysphagia,
Oro-pharyngeal and Esophageal Motility and Dysmotility John E. Pandolfino, MD, MSci
 Oro-pharyngeal and Esophageal Department of Medicine Feinberg School of Medicine Northwestern University 1 Oro-pharyngeal and Esophageal Motility Function: Oropharynx Transfer food Prevent aspiration Breathing
Oro-pharyngeal and Esophageal Department of Medicine Feinberg School of Medicine Northwestern University 1 Oro-pharyngeal and Esophageal Motility Function: Oropharynx Transfer food Prevent aspiration Breathing
Esophageal Motility Disorders
 GASTROENTEROLOGY BOARD REVIEW MANUAL PUBLISHING STAFF PRESIDENT, GROUP PUBLISHER Bruce M. White EXECUTIVE EDITOR Debra Dreger SENIOR EDITOR Becky Krumm, ELS ASSOCIATE EDITOR Lamont Williams ASSISTANT EDITOR
GASTROENTEROLOGY BOARD REVIEW MANUAL PUBLISHING STAFF PRESIDENT, GROUP PUBLISHER Bruce M. White EXECUTIVE EDITOR Debra Dreger SENIOR EDITOR Becky Krumm, ELS ASSOCIATE EDITOR Lamont Williams ASSISTANT EDITOR
ACHALASIA ACHALASIA. Current Management of Achalasia
 Current Management of Achalasia Guilherme M Campos, MD, FACS Assistant Professor of Surgery Director G.I. Motility Center Director Bariatric Surgery Program University of California San Francisco ACHALASIA
Current Management of Achalasia Guilherme M Campos, MD, FACS Assistant Professor of Surgery Director G.I. Motility Center Director Bariatric Surgery Program University of California San Francisco ACHALASIA
Joel A. Ricci MD SUNY Downstate Medical Center Lutheran Medical Center Department of Surgery June 26, 2009
 Joel A. Ricci MD SUNY Downstate Medical Center Lutheran Medical Center Department of Surgery June 26, 2009 History Xx year old female with worsening dysphagia and solid food regurgitation for 2 days Other
Joel A. Ricci MD SUNY Downstate Medical Center Lutheran Medical Center Department of Surgery June 26, 2009 History Xx year old female with worsening dysphagia and solid food regurgitation for 2 days Other
34th Annual Toronto Thoracic Surgery Refresher Course
 34th Annual Toronto Thoracic Surgery Refresher Course TREATMENT OPTIONS FOR ACHALASIA Dr. Carmine Simone Director, Intensive Care Unit Head, Division of Critical Care Departments of Medicine and Surgery
34th Annual Toronto Thoracic Surgery Refresher Course TREATMENT OPTIONS FOR ACHALASIA Dr. Carmine Simone Director, Intensive Care Unit Head, Division of Critical Care Departments of Medicine and Surgery
Duke Masters of Minimally Invasive Thoracic Surgery Orlando, FL. September 17, Session VI: Minimally Invasive Thoracic Surgery: Miscellaneous
 Duke Masters of Minimally Invasive Thoracic Surgery Orlando, FL September 17, 2016 Session VI: Minimally Invasive Thoracic Surgery: Miscellaneous NOTES and POEM James D. Luketich MD, FACS Henry T. Bahnson
Duke Masters of Minimally Invasive Thoracic Surgery Orlando, FL September 17, 2016 Session VI: Minimally Invasive Thoracic Surgery: Miscellaneous NOTES and POEM James D. Luketich MD, FACS Henry T. Bahnson
Achalasia: Classic View
 Achalasia: Dilate, Botox, Knife or POEM Prateek Sharma, MD Kansas University School of Medicine Achalasia: Classic View 1 Diagnosis of Achalasia Endoscopy may be normal in as many as 44% Upper GI series
Achalasia: Dilate, Botox, Knife or POEM Prateek Sharma, MD Kansas University School of Medicine Achalasia: Classic View 1 Diagnosis of Achalasia Endoscopy may be normal in as many as 44% Upper GI series
David Markowitz, MD. Physicians and Surgeons
 Esophageal Motility David Markowitz, MD Columbia University, College of Columbia University, College of Physicians and Surgeons Alimentary Tract Motility Propulsion Movement of food and endogenous secretions
Esophageal Motility David Markowitz, MD Columbia University, College of Columbia University, College of Physicians and Surgeons Alimentary Tract Motility Propulsion Movement of food and endogenous secretions
A Multidisciplinary Approach to Esophageal Dysphagia: Role of the SLP. Darlene Graner, M.A., CCC-SLP, BRS-S Sharon Burton, M.D.
 A Multidisciplinary Approach to Esophageal Dysphagia: Role of the SLP Darlene Graner, M.A., CCC-SLP, BRS-S Sharon Burton, M.D. What is the role of the SLP? Historically SLPs the preferred providers for
A Multidisciplinary Approach to Esophageal Dysphagia: Role of the SLP Darlene Graner, M.A., CCC-SLP, BRS-S Sharon Burton, M.D. What is the role of the SLP? Historically SLPs the preferred providers for
Myogenic Control. Esophageal Motility. Enteric Nervous System. Alimentary Tract Motility. Determinants of GI Tract Motility.
 Myogenic Control Esophageal Motility David Markowitz, MD Columbia University, College of Physicians and Surgeons Basic Electrical Rythym: intrinsic rhythmic fluctuation of smooth muscle membrane potential
Myogenic Control Esophageal Motility David Markowitz, MD Columbia University, College of Physicians and Surgeons Basic Electrical Rythym: intrinsic rhythmic fluctuation of smooth muscle membrane potential
Esophageal Motility. Alimentary Tract Motility
 Esophageal Motility David Markowitz, MD Columbia University, College of Physicians and Surgeons Alimentary Tract Motility Propulsion Movement of food and endogenous secretions Mixing Allows for greater
Esophageal Motility David Markowitz, MD Columbia University, College of Physicians and Surgeons Alimentary Tract Motility Propulsion Movement of food and endogenous secretions Mixing Allows for greater
Dysphagia. Conflicts of Interest
 Dysphagia Bob Kizer MD Assistant Professor of Medicine Creighton University School of Medicine August 25, 2018 Conflicts of Interest None 1 Which patient does not need an EGD as the first test? 1. 50 year
Dysphagia Bob Kizer MD Assistant Professor of Medicine Creighton University School of Medicine August 25, 2018 Conflicts of Interest None 1 Which patient does not need an EGD as the first test? 1. 50 year
Achalasia: Inject, Dilate, or Surgery?
 Achalasia: Inject, Dilate, or Surgery? John E. Pandolfino, MD, MSCI, FACG Professor of Medicine Feinberg School of Medicine Northwestern University Chief, Division of Gastroenterology and Hepatology Northwestern
Achalasia: Inject, Dilate, or Surgery? John E. Pandolfino, MD, MSCI, FACG Professor of Medicine Feinberg School of Medicine Northwestern University Chief, Division of Gastroenterology and Hepatology Northwestern
Gastroesophageal reflux disease Principles of GERD treatment Treatment of reflux diseases GERD
 Esophagus Anatomy/Physiology Gastroesophageal reflux disease Principles of GERD treatment Treatment of reflux diseases GERD Manometry Question 50 years old female with chest pain and dysphagia. Manometry
Esophagus Anatomy/Physiology Gastroesophageal reflux disease Principles of GERD treatment Treatment of reflux diseases GERD Manometry Question 50 years old female with chest pain and dysphagia. Manometry
High Resolution Manometry: A new perspective on esophageal motility disorders. Chris Andrews & Bill Paterson
 High Resolution Manometry: A new perspective on esophageal motility disorders Chris Andrews & Bill Paterson CDDW/CASL Meeting Session: CanMEDS Roles Covered in this Session: Medical Expert (as Medical
High Resolution Manometry: A new perspective on esophageal motility disorders Chris Andrews & Bill Paterson CDDW/CASL Meeting Session: CanMEDS Roles Covered in this Session: Medical Expert (as Medical
Diagnosis and Management of Achalasia: Past, Present, & Future
 Diagnosis and Management of Achalasia: Past, Present, & Future Kyle A. Perry, MD, FACS Assistant Professor of Surgery Division of General & Gastrointestinal Surgery The Ohio State University Wexner Medical
Diagnosis and Management of Achalasia: Past, Present, & Future Kyle A. Perry, MD, FACS Assistant Professor of Surgery Division of General & Gastrointestinal Surgery The Ohio State University Wexner Medical
Surgical Evaluation for Benign Esophageal Disease. Kimberly Howard, PA-C, MHS Duke University Medical Center April 7, 2018
 Surgical Evaluation for Benign Esophageal Disease Kimberly Howard, PA-C, MHS Duke University Medical Center April 7, 2018 Disclosures No disclosures relevant to this presentation. Objectives (for CME purposes)
Surgical Evaluation for Benign Esophageal Disease Kimberly Howard, PA-C, MHS Duke University Medical Center April 7, 2018 Disclosures No disclosures relevant to this presentation. Objectives (for CME purposes)
Two Distinct Types of Hypercontractile Esophagus: Classic and Spastic Jackhammer
 Brief communication Gut and Liver, Vol. 10, No. 5, September 2016, pp. 859-863 Two Distinct Types of Hypercontractile Esophagus: Classic and Spastic Jackhammer Yun Soo Hong, Yang Won Min, and Poong-Lyul
Brief communication Gut and Liver, Vol. 10, No. 5, September 2016, pp. 859-863 Two Distinct Types of Hypercontractile Esophagus: Classic and Spastic Jackhammer Yun Soo Hong, Yang Won Min, and Poong-Lyul
A collection of High Resolution Esophageal Manometry Patterns
 A collection of High Resolution Esophageal Manometry Patterns Distinctive color maps of motility disorders Table of contents Introduction... 3 Normal HRM [B.1]... 4 Achalasia... 5 Classic Achalasia with
A collection of High Resolution Esophageal Manometry Patterns Distinctive color maps of motility disorders Table of contents Introduction... 3 Normal HRM [B.1]... 4 Achalasia... 5 Classic Achalasia with
Departement of Surgery Faculty of Medicine University Sumatera Utara
 SSS EESOPHAGEAL HPOSAGEAL DISORDERS IN SURGICAL PERSPECTIVE Departement of Surgery Faculty of Medicine University Sumatera Utara CONTENT 1. Esophageal Atresia 2. Achalasia 3. Esophageal Rupture 4. Tumor
SSS EESOPHAGEAL HPOSAGEAL DISORDERS IN SURGICAL PERSPECTIVE Departement of Surgery Faculty of Medicine University Sumatera Utara CONTENT 1. Esophageal Atresia 2. Achalasia 3. Esophageal Rupture 4. Tumor
Combined Experience of Two European Centers
 Minimally Invasive Surgery for Achalasia: Combined Experience of Two European Centers Garzi A, Valla JS*, Molinaro F, Amato G, Messina M. Unit of Pediatric Surgery, University of Siena (Italy) *Lenval
Minimally Invasive Surgery for Achalasia: Combined Experience of Two European Centers Garzi A, Valla JS*, Molinaro F, Amato G, Messina M. Unit of Pediatric Surgery, University of Siena (Italy) *Lenval
High Resolution Impedance Manometry (HRiM ) Swallow Atlas
 Swallow Atlas") High Resolution Impedance Manometry (HRiM ) Swallow Atlas Normal Esophageal Function Bolus Transit UES Esophageal Body LES Complete bolus transit Peristaltic contractions with pressure amplitude of at
High Resolution Impedance Manometry (HRiM ) Swallow Atlas Normal Esophageal Function Bolus Transit UES Esophageal Body LES Complete bolus transit Peristaltic contractions with pressure amplitude of at
What part of the gastrointestinal (GI) tract is composed of striated muscle and smooth muscle?
 tract is composed of striated muscle and smooth muscle?") CASE 29 A 34-year-old man presents to his primary care physician with the complaint of increased difficulty swallowing both solid and liquid foods. He notices that he sometimes has more difficulty when
CASE 29 A 34-year-old man presents to his primary care physician with the complaint of increased difficulty swallowing both solid and liquid foods. He notices that he sometimes has more difficulty when
The Frequency of Gastroesophageal Reflux Disease in Nutcracker Esophagus and the Effect of Acid-Reduction Therapy on the Motor Abnormality
 Bahrain Medical Bulletin, Vol.22, No.4, December 2000 The Frequency of Gastroesophageal Reflux Disease in Nutcracker Esophagus and the Effect of Acid-Reduction Therapy on the Motor Abnormality Saleh Mohsen
Bahrain Medical Bulletin, Vol.22, No.4, December 2000 The Frequency of Gastroesophageal Reflux Disease in Nutcracker Esophagus and the Effect of Acid-Reduction Therapy on the Motor Abnormality Saleh Mohsen
Achalasia is a rare disease with an annual incidence estimated REVIEWS. Erroneous Diagnosis of Gastroesophageal Reflux Disease in Achalasia
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2011;9:1020 1024 REVIEWS Erroneous Diagnosis of Gastroesophageal Reflux Disease in Achalasia BOUDEWIJN F. KESSING, ALBERT J. BREDENOORD, and ANDRÉ J. P. M. SMOUT
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2011;9:1020 1024 REVIEWS Erroneous Diagnosis of Gastroesophageal Reflux Disease in Achalasia BOUDEWIJN F. KESSING, ALBERT J. BREDENOORD, and ANDRÉ J. P. M. SMOUT
Clearance mechanisms of the aperistaltic esophagus. The pump-gun hypothesis.
 Gut Online First, published on December 14, 2005 as 10.1136/gut.2005.085423 Clearance mechanisms of the aperistaltic esophagus. The pump-gun hypothesis. Radu Tutuian 1, Daniel Pohl 1, Donald O Castell
Gut Online First, published on December 14, 2005 as 10.1136/gut.2005.085423 Clearance mechanisms of the aperistaltic esophagus. The pump-gun hypothesis. Radu Tutuian 1, Daniel Pohl 1, Donald O Castell
Esophageal Motility Disorders. Disclosures
 Esophageal Motility Disorders V. Raman Muthusamy, MD FACG Director of Endoscopy Clinical i l Professor of Medicine i David Geffen School of Medicine at UCLA UCLA Health System Disclosures I am an interventional
Esophageal Motility Disorders V. Raman Muthusamy, MD FACG Director of Endoscopy Clinical i l Professor of Medicine i David Geffen School of Medicine at UCLA UCLA Health System Disclosures I am an interventional
Manometry Conundrums
 Manometry Conundrums Gastroenterology and Hepatology Symposium February 10, 2018 Reena V. Chokshi, MD Assistant Professor of Medicine Division of Gastroenterology, Hepatology, & Nutrition Department of
Manometry Conundrums Gastroenterology and Hepatology Symposium February 10, 2018 Reena V. Chokshi, MD Assistant Professor of Medicine Division of Gastroenterology, Hepatology, & Nutrition Department of
Oesophageal motor changes in diabetes mellitus
 Thorax (1976), 31, 278. Oesophageal motor changes in diabetes mellitus I. M. STEWART, D. J. HOSKING, B. J. PRESTON, and M. ATKINSON General Hospital, Nottingham Stewart, I. M., Hosking, D. J., Preston,
Thorax (1976), 31, 278. Oesophageal motor changes in diabetes mellitus I. M. STEWART, D. J. HOSKING, B. J. PRESTON, and M. ATKINSON General Hospital, Nottingham Stewart, I. M., Hosking, D. J., Preston,
What can you expect from the lab?
 Role of the GI Motility Lab in the Diagnosis and Treatment of Esophageal Disorders Kenneth R. DeVault MD, FACG, FACP Professor and Chair Department of Medicine Mayo Clinic Florida What can you expect from
Role of the GI Motility Lab in the Diagnosis and Treatment of Esophageal Disorders Kenneth R. DeVault MD, FACG, FACP Professor and Chair Department of Medicine Mayo Clinic Florida What can you expect from
127 Chapter 1 Chapter 2 Chapter 3
 CHAPTER 8 Summary Summary 127 In Chapter 1, a general introduction on the principles and applications of intraluminal impedance monitoring in esophageal disorders is provided. Intra-esophageal impedance
CHAPTER 8 Summary Summary 127 In Chapter 1, a general introduction on the principles and applications of intraluminal impedance monitoring in esophageal disorders is provided. Intra-esophageal impedance
Pseudoachalasia: Still a Tough Clinical Challenge
 ISSN 1941-5923 DOI: 10.12659/AJCR.894444 Received: 2015.04.23 Accepted: 2015.06.24 Published: 2015.10.29 : Still a Tough Clinical Challenge Authors Contribution: Study Design A Data Collection B Statistical
ISSN 1941-5923 DOI: 10.12659/AJCR.894444 Received: 2015.04.23 Accepted: 2015.06.24 Published: 2015.10.29 : Still a Tough Clinical Challenge Authors Contribution: Study Design A Data Collection B Statistical
Catherine Kerschen DO, FACOI Michigan State University College of Osteopathic Medicine
 Catherine Kerschen DO, FACOI Michigan State University College of Osteopathic Medicine none 32 yo male presents with a burning sensation in chest following most large meals for 2-3 months. He denies dysphagia,
Catherine Kerschen DO, FACOI Michigan State University College of Osteopathic Medicine none 32 yo male presents with a burning sensation in chest following most large meals for 2-3 months. He denies dysphagia,
An Overview on Pediatric Esophageal Disorders. Annamaria Staiano Department of Translational Medical Sciences University of Naples Federico II
 An Overview on Pediatric Esophageal Disorders Annamaria Staiano Department of Translational Medical Sciences University of Naples Federico II Case report F.C. 3 year old boy Preterm born from emergency
An Overview on Pediatric Esophageal Disorders Annamaria Staiano Department of Translational Medical Sciences University of Naples Federico II Case report F.C. 3 year old boy Preterm born from emergency
A Novel Endoscopic Treatment for Achalasia Is the POEM mightier than the sword?
 A Novel Endoscopic Treatment for Achalasia Is the POEM mightier than the sword? Pavlos Kaimakliotis, MD Department of Gastroenterology Lahey Hospital and Medical Center Assistant Professor of Medicine
A Novel Endoscopic Treatment for Achalasia Is the POEM mightier than the sword? Pavlos Kaimakliotis, MD Department of Gastroenterology Lahey Hospital and Medical Center Assistant Professor of Medicine
01/26/2010 GENERAL SURGERY ABSITE ANATOMY ANATOMY. Yvonne M. Carter, MD Georgetown University Medical Center. Layers. mucosa. squamous epithelium
 GENERAL SURGERY ABSITE REVIEW: ESOPHAGUS Yvonne M. Carter, MD Georgetown University Medical Center ANATOMY Layers mucosa muscle squamous epithelium columnar epithelium (distal 2cm) inner = circular outer
GENERAL SURGERY ABSITE REVIEW: ESOPHAGUS Yvonne M. Carter, MD Georgetown University Medical Center ANATOMY Layers mucosa muscle squamous epithelium columnar epithelium (distal 2cm) inner = circular outer
High Resolution Esophageal Manometry
 High Resolution Esophageal Manometry Dr. Geoffrey Turnbull MD, FRCPC Dalhousie University Dr. Yvonne Tse MD, FRCPC University of Toronto Name: Dr. Geoffrey Turnbull Conflict of Interest Disclosure (over
High Resolution Esophageal Manometry Dr. Geoffrey Turnbull MD, FRCPC Dalhousie University Dr. Yvonne Tse MD, FRCPC University of Toronto Name: Dr. Geoffrey Turnbull Conflict of Interest Disclosure (over
Pressure topography metrics
 Aim: The Chicago Classification (CC) categorizes esophageal motility disorders in high-resolution manometry (HRM) depicted with color pressure topography plots, also known as Clouse plots in honor of Ray
Aim: The Chicago Classification (CC) categorizes esophageal motility disorders in high-resolution manometry (HRM) depicted with color pressure topography plots, also known as Clouse plots in honor of Ray
An Atlas of Investigation and Management ESOPHAGEAL DISEASES
 An Atlas of Investigation and Management ESOPHAGEAL DISEASES Michael F Vaezi, MD, PhD, MS(epi) Clinical Director Division of Gastroenerology and Hepatology Director Clinical Research Director Swallowing
An Atlas of Investigation and Management ESOPHAGEAL DISEASES Michael F Vaezi, MD, PhD, MS(epi) Clinical Director Division of Gastroenerology and Hepatology Director Clinical Research Director Swallowing
Slide 4. Slide 5. Slide 6
 Slide 1 Slide 4 Measure Pressures within the Esophagus Evaluate Coordination of Muscles Presented by: Donna Dickinson, RN, Clin II, Manometry Specialist Bon Secours Richmond Health System Slide 2 Slide
Slide 1 Slide 4 Measure Pressures within the Esophagus Evaluate Coordination of Muscles Presented by: Donna Dickinson, RN, Clin II, Manometry Specialist Bon Secours Richmond Health System Slide 2 Slide
Esophageal Disease. Objectives:
 Esophageal Disease Objectives: Basic function of esophagus Definition of dysphagia Mechanism of dysphagia Types of dysphagia Common causes Algorithm to approach dysphagia Doctor: prof. Saleh Alamri Team
Esophageal Disease Objectives: Basic function of esophagus Definition of dysphagia Mechanism of dysphagia Types of dysphagia Common causes Algorithm to approach dysphagia Doctor: prof. Saleh Alamri Team
Supplementary appendix
 Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Ang D, Misselwitz B, Hollenstein M, et al.
Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Ang D, Misselwitz B, Hollenstein M, et al.
Radiological evaluation of esophageal. function in dysphagia with special. emphasis on achalasia
 Radiological evaluation of esophageal function in dysphagia with special emphasis on achalasia Mats Andersson Department of Radiology, Institute of Clinical Sciences, The Sahlgrenska Academy, University
Radiological evaluation of esophageal function in dysphagia with special emphasis on achalasia Mats Andersson Department of Radiology, Institute of Clinical Sciences, The Sahlgrenska Academy, University
Manometric and symptomatic spectrum of motor dysphagia in a tertiary referral center in northern India
 Indian J Gastroenterol 2010(January February):29(1):18 22 ORIGINAL ARTICLE Manometric and symptomatic spectrum of motor dysphagia in a tertiary referral center in northern India Asha Misra Dipti Chourasia
Indian J Gastroenterol 2010(January February):29(1):18 22 ORIGINAL ARTICLE Manometric and symptomatic spectrum of motor dysphagia in a tertiary referral center in northern India Asha Misra Dipti Chourasia
Achalasia Current Diagnosis and Management
 時間 :2017 年 9 月 16 日 14:45PM-17:50PM 地點 : 臺中榮民總醫院研究大樓一樓第二會場 Achalasia Current Diagnosis and Management 蔡成枝醫師 Seng-Kee Chuah, M.D. Professor of Medicine Division of Hepato-gastroenterology Department of
時間 :2017 年 9 月 16 日 14:45PM-17:50PM 地點 : 臺中榮民總醫院研究大樓一樓第二會場 Achalasia Current Diagnosis and Management 蔡成枝醫師 Seng-Kee Chuah, M.D. Professor of Medicine Division of Hepato-gastroenterology Department of
ESOPHAGEAL CANCER AND GERD. Prof Salman Guraya FRCS, Masters MedEd
 ESOPHAGEAL CANCER AND GERD Prof Salman Guraya FRCS, Masters MedEd Learning objectives Esophagus anatomy and physiology Esophageal cancer Causes, presentations of esophageal cancer Diagnosis and management
ESOPHAGEAL CANCER AND GERD Prof Salman Guraya FRCS, Masters MedEd Learning objectives Esophagus anatomy and physiology Esophageal cancer Causes, presentations of esophageal cancer Diagnosis and management
and not explained by an obstruction or inflammatory process. Responses to treatment vary based on which achalasia subtype is present.
 Clinical Review & Education Review A Systematic Review John E. Pandolfino, MD, MSCI; Andrew J. Gawron, MD, PhD, MS IMPORTANCE significantly affects patients quality of life and can be difficult to diagnose
Clinical Review & Education Review A Systematic Review John E. Pandolfino, MD, MSCI; Andrew J. Gawron, MD, PhD, MS IMPORTANCE significantly affects patients quality of life and can be difficult to diagnose
Abstract. Abnormal peristaltic waves like aperistalsis of the esophageal body, high amplitude and broader waves,
 Original Article Esophageal Motility Disorders in Diabetics Waquaruddin Ahmed, Ejaz Ahmed Vohra Department of Medicine, Dr. Ziauddin Medical University, Karachi. Abstract Objective: To see the presence
Original Article Esophageal Motility Disorders in Diabetics Waquaruddin Ahmed, Ejaz Ahmed Vohra Department of Medicine, Dr. Ziauddin Medical University, Karachi. Abstract Objective: To see the presence
Health-related quality of life and physiological measurements in achalasia
 Diseases of the Esophagus (2017) 30, 1 5 DOI: 10.1111/dote.12494 Original Article Health-related quality of life and physiological measurements in achalasia Daniel Ross, 1 Joel Richter, 2 Vic Velanovich
Diseases of the Esophagus (2017) 30, 1 5 DOI: 10.1111/dote.12494 Original Article Health-related quality of life and physiological measurements in achalasia Daniel Ross, 1 Joel Richter, 2 Vic Velanovich
Management of the Difficult Patient with Type 3 Achalasia. Steven R. DeMeester Professor and Clinical Scholar Department of Surgery
 Management of the Difficult Patient with Type 3 Achalasia Steven R. DeMeester Professor and Clinical Scholar Department of Surgery Achalasia Treatment Concepts Disease leads to non-relaxing LES and loss
Management of the Difficult Patient with Type 3 Achalasia Steven R. DeMeester Professor and Clinical Scholar Department of Surgery Achalasia Treatment Concepts Disease leads to non-relaxing LES and loss
EGD. John M. Wo, M.D. University of Louisville July 3, 2008
 EGD John M. Wo, M.D. University of Louisville July 3, 2008 Different Ways to do an EGD Which scope? Pediatric, regular, jumbo EGD endoscope or pediatric colonoscope Transnasal vs. transoral insertion Sedation
EGD John M. Wo, M.D. University of Louisville July 3, 2008 Different Ways to do an EGD Which scope? Pediatric, regular, jumbo EGD endoscope or pediatric colonoscope Transnasal vs. transoral insertion Sedation
Peptic ulcer disease Disorders of the esophagus
 Peptic ulcer disease Disorders of the esophagus Peptic ulcer disease Burning epigastric pain Exacerbated by fasting Improved with meals Ulcer: disruption of mucosal integrity >5 mm in size, with depth
Peptic ulcer disease Disorders of the esophagus Peptic ulcer disease Burning epigastric pain Exacerbated by fasting Improved with meals Ulcer: disruption of mucosal integrity >5 mm in size, with depth
PAPER. Spectrum of Esophageal Motility Disorders
 PAPER Spectrum of Esophageal Motility Disorders Implications for Diagnosis and Treatment Marco G. Patti, MD; Maria V. Gorodner, MD; Carlos Galvani, MD; Pietro Tedesco, MD; Piero M. Fisichella, MD; James
PAPER Spectrum of Esophageal Motility Disorders Implications for Diagnosis and Treatment Marco G. Patti, MD; Maria V. Gorodner, MD; Carlos Galvani, MD; Pietro Tedesco, MD; Piero M. Fisichella, MD; James
Propulsion and mixing of food in the alimentary tract Chapter 63
 Propulsion and mixing of food in the alimentary tract Chapter 63 Types of GI movements: Propulsive movement-peristalsis Propulsion: controlled movement of ingested foods, liquids, GI secretions, and sloughed
Propulsion and mixing of food in the alimentary tract Chapter 63 Types of GI movements: Propulsive movement-peristalsis Propulsion: controlled movement of ingested foods, liquids, GI secretions, and sloughed
Post-Prandial Trouble! KPA 2017 Nutrition pre-congress case Presentation Dr. Esther Kimani. Facilitator- Dr. A. Laving. 25/04/2017
 Post-Prandial Trouble! KPA 2017 Nutrition pre-congress case Presentation Dr. Esther Kimani. Facilitator- Dr. A. Laving. 25/04/2017 Biodata. Name- I.M.M. Age-6 years Gender- female Referred to the Paediatric
Post-Prandial Trouble! KPA 2017 Nutrition pre-congress case Presentation Dr. Esther Kimani. Facilitator- Dr. A. Laving. 25/04/2017 Biodata. Name- I.M.M. Age-6 years Gender- female Referred to the Paediatric
Hiatal Hernias and Barrett s esophagus. Dr Sajida Ahad Mercy General Surgery
 Hiatal Hernias and Barrett s esophagus Dr Sajida Ahad Mercy General Surgery Objectives Identify the use of different diagnostic modalities for hiatal hernias List the different types of hiatal hernias
Hiatal Hernias and Barrett s esophagus Dr Sajida Ahad Mercy General Surgery Objectives Identify the use of different diagnostic modalities for hiatal hernias List the different types of hiatal hernias
Gastrointestinal Imaging Clinical Observations
 Esophageal Motility Disorders After Laparoscopic Nissen Fundoplication Gastrointestinal Imaging Clinical Observations Natasha E. Wehrli 1 Marc S. Levine 1 Stephen E. Rubesin 1 David A. Katzka 2 Igor Laufer
Esophageal Motility Disorders After Laparoscopic Nissen Fundoplication Gastrointestinal Imaging Clinical Observations Natasha E. Wehrli 1 Marc S. Levine 1 Stephen E. Rubesin 1 David A. Katzka 2 Igor Laufer
Esophageal Impedance: Role in the Evaluation of Esophageal Motility
 TZ CHI MED J June 2009 Vol 21 No 2 available at http://ajws.elsevier.com/tcmj Tzu Chi Medical Journal Review Article Esophageal Impedance: Role in the Evaluation of Esophageal Motility Chien-Lin Chen*
TZ CHI MED J June 2009 Vol 21 No 2 available at http://ajws.elsevier.com/tcmj Tzu Chi Medical Journal Review Article Esophageal Impedance: Role in the Evaluation of Esophageal Motility Chien-Lin Chen*
Achalasia is a primary esophageal motility disorder of unknown
 Laparoscopic Heller Myotomy for Achalasia Andrew Pierre, MD, MSc Achalasia is a primary esophageal motility disorder of unknown etiology. Pathologically, it is characterized by loss of ganglion cells in
Laparoscopic Heller Myotomy for Achalasia Andrew Pierre, MD, MSc Achalasia is a primary esophageal motility disorder of unknown etiology. Pathologically, it is characterized by loss of ganglion cells in
The Lower Esophageal Sphincter in Health and Disease. Steven R. DeMeester Professor and Clinical Scholar Department of Surgery
 The Lower Esophageal Sphincter in Health and Disease Steven R. DeMeester Professor and Clinical Scholar Department of Surgery The Lower Esophageal Sphincter Dual function: allow bolus from esophagus into
The Lower Esophageal Sphincter in Health and Disease Steven R. DeMeester Professor and Clinical Scholar Department of Surgery The Lower Esophageal Sphincter Dual function: allow bolus from esophagus into
CONCETTI GENERALI SULLE DISFAGIE DI ORIGINE ESOFAGEA
 MECCANISMI FISIOLOGICI AUTOMATICO-RIFLESSI DELL ESOFAGO CONCETTI GENERALI SULLE DISFAGIE DI ORIGINE ESOFAGEA Michele Di Stefano Clinica Medica 1 Fondazione IRCCS Policlinico S.Matteo Università di Pavia
MECCANISMI FISIOLOGICI AUTOMATICO-RIFLESSI DELL ESOFAGO CONCETTI GENERALI SULLE DISFAGIE DI ORIGINE ESOFAGEA Michele Di Stefano Clinica Medica 1 Fondazione IRCCS Policlinico S.Matteo Università di Pavia
The literal definition of achalasia is failure of a ring muscle
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2013;11:887 897 PERSPECTIVES IN CLINICAL GASTROENTEROLOGY AND HEPATOLOGY Presentation, Diagnosis, and Management of Achalasia JOHN E. PANDOLFINO and PETER J. KAHRILAS
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2013;11:887 897 PERSPECTIVES IN CLINICAL GASTROENTEROLOGY AND HEPATOLOGY Presentation, Diagnosis, and Management of Achalasia JOHN E. PANDOLFINO and PETER J. KAHRILAS
Surgery for achalasia is an anachronism. John C. Dugal Jr. MD
 Surgery for achalasia is an anachronism. John C. Dugal Jr. MD Outline: Overview of achalasia Traditional surgical treatments Heller ±fundoplication Less invasive treatments Nitrates/Ca channel blockers
Surgery for achalasia is an anachronism. John C. Dugal Jr. MD Outline: Overview of achalasia Traditional surgical treatments Heller ±fundoplication Less invasive treatments Nitrates/Ca channel blockers
University College Hospital. Achalasia. Gastrointestinal Services Division Physiology Unit
 University College Hospital Achalasia Gastrointestinal Services Division Physiology Unit Author: Dr Anton Emmanuel, Consultant Gastroenterologist First published: September 2012 Last review date: February
University College Hospital Achalasia Gastrointestinal Services Division Physiology Unit Author: Dr Anton Emmanuel, Consultant Gastroenterologist First published: September 2012 Last review date: February
Surgery for Esophageal Motor Disorders
 EDITORIAL Surgery for Esophageal Motor Disorders Tom R. DeMeester, M.D. Diffuse esophageal spasm is an esophageal motor disorder characterized clinically by substernal chest pain, dysphagia, or both. It
EDITORIAL Surgery for Esophageal Motor Disorders Tom R. DeMeester, M.D. Diffuse esophageal spasm is an esophageal motor disorder characterized clinically by substernal chest pain, dysphagia, or both. It
CONCETTI GENERALI SULLE DISFAGIE DI ORIGINE ESOFAGEA
 LA DISFAGIA ESOFAGEA Pavia, 12.1.217 CONCETTI GENERALI SULLE DISFAGIE DI ORIGINE ESOFAGEA Michele Di Stefano Clinica Medica 1 Fondazione IRCCS Policlinico S.Matteo Università di Pavia Pavia PHARYNGOESOPHAGEAL
LA DISFAGIA ESOFAGEA Pavia, 12.1.217 CONCETTI GENERALI SULLE DISFAGIE DI ORIGINE ESOFAGEA Michele Di Stefano Clinica Medica 1 Fondazione IRCCS Policlinico S.Matteo Università di Pavia Pavia PHARYNGOESOPHAGEAL
Radiology. Gastrointestinal. Transient Intraluminal Diverticulum of the Esophagus: A Significant Flow Artifact. Farooq P. Agha
 Gastrointest Radiol 9:9%103 (1984) Gastrointestinal Radiology 9 Springer-Verlag 1984 Transient Intraluminal Diverticulum of the Esophagus: A Significant Flow Artifact Farooq P. Agha Department of Radiology,
Gastrointest Radiol 9:9%103 (1984) Gastrointestinal Radiology 9 Springer-Verlag 1984 Transient Intraluminal Diverticulum of the Esophagus: A Significant Flow Artifact Farooq P. Agha Department of Radiology,
NIH Public Access Author Manuscript Am J Gastroenterol. Author manuscript; available in PMC 2010 June 21.
 NIH Public Access Author Manuscript Published in final edited form as: Am J Gastroenterol. 2010 May ; 105(5): 981 987. doi:10.1038/ajg.2010.43. Esophageal Motor Disorders in Terms of High-Resolution Esophageal
NIH Public Access Author Manuscript Published in final edited form as: Am J Gastroenterol. 2010 May ; 105(5): 981 987. doi:10.1038/ajg.2010.43. Esophageal Motor Disorders in Terms of High-Resolution Esophageal
pissn: eissn: Journal of Neurogastroenterology and Motility
 JNM J Neurogastroenterol Motil, Vol. 24 No. 3 July, 2018 pissn: 2093-0879 eissn: 2093-0887 https://doi.org/10.5056/jnm18038 Original Article 200 ml Rapid Drink Challenge During Highresolution Manometry
JNM J Neurogastroenterol Motil, Vol. 24 No. 3 July, 2018 pissn: 2093-0879 eissn: 2093-0887 https://doi.org/10.5056/jnm18038 Original Article 200 ml Rapid Drink Challenge During Highresolution Manometry
Falk Symposium, , , Portorož. Physiology of Swallowing and Anti-Gastroesophageal. Reflux-Mechanisms. Mechanisms: C.
 Falk Symposium, 15.-16.6.07, 16.6.07, Portorož Physiology of Swallowing and Anti-Gastroesophageal Reflux-Mechanisms Mechanisms: Anything new from a radiologist s view? C.Kulinna-Cosentini Cosentini Medical
Falk Symposium, 15.-16.6.07, 16.6.07, Portorož Physiology of Swallowing and Anti-Gastroesophageal Reflux-Mechanisms Mechanisms: Anything new from a radiologist s view? C.Kulinna-Cosentini Cosentini Medical
SAGES Guidelines for the Surgical Treatment of Esophageal Achalasia
 Practice/Clinical Guidelines published on: 05/2011 by the Society of American Gastrointestinal and Endoscopic Surgeons (SAGES) SAGES Guidelines for the Surgical Treatment of Esophageal Achalasia Dimitrios
Practice/Clinical Guidelines published on: 05/2011 by the Society of American Gastrointestinal and Endoscopic Surgeons (SAGES) SAGES Guidelines for the Surgical Treatment of Esophageal Achalasia Dimitrios
Anatomy: From cricoid cartilage to diaphragm 25 Cms. 4 portions: Cervical 5 cms. Thoracic 25 cms. Abdominal 2 cms. Blood supply Lymphatic spread
 Esophagus Anatomy: From cricoid cartilage to diaphragm 25 Cms. 4 portions: Cervical 5 cms. Thoracic 25 cms. Abdominal 2 cms. Blood supply Lymphatic spread Upper 2/3 Cephalad Lower 1/3 Caudad Physiology:
Esophagus Anatomy: From cricoid cartilage to diaphragm 25 Cms. 4 portions: Cervical 5 cms. Thoracic 25 cms. Abdominal 2 cms. Blood supply Lymphatic spread Upper 2/3 Cephalad Lower 1/3 Caudad Physiology:
Case 1- B.N. 66 yr old F with PMHx of breast cancer s/ p mastectomy, HTN, DM presented with dysphagia to solids and liquids.
 Case 1- B.N 66 yr old F with PMHx of breast cancer s/ p mastectomy, HTN, DM presented with dysphagia to solids and liquids. Reports retching to clear esophagus. Case 1- B.N EGD: Stricture in the distal
Case 1- B.N 66 yr old F with PMHx of breast cancer s/ p mastectomy, HTN, DM presented with dysphagia to solids and liquids. Reports retching to clear esophagus. Case 1- B.N EGD: Stricture in the distal
Endoscopic carbon dioxide laser cricopharyngeal myotomy for relief of oropharyngeal dysphagia
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Endoscopic carbon dioxide laser cricopharyngeal myotomy for relief of oropharyngeal dysphagia Difficulty
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Endoscopic carbon dioxide laser cricopharyngeal myotomy for relief of oropharyngeal dysphagia Difficulty
Classification of oesophageal motility abnormalities
 Gut 2001;49:145 151 145 Review Classification of oesophageal motility abnormalities Summary Manometric examination of the oesophagus frequently reveals abnormalities whose cause is unknown and whose physiological
Gut 2001;49:145 151 145 Review Classification of oesophageal motility abnormalities Summary Manometric examination of the oesophagus frequently reveals abnormalities whose cause is unknown and whose physiological
Chapter 14: Training in Radiology. DDSEP Chapter 1: Question 12
 DDSEP Chapter 1: Question 12 A 52-year-old white male presents for evaluation of sudden onset of abdominal pain and shoulder pain. His past medical history is notable for a history of coronary artery disease,
DDSEP Chapter 1: Question 12 A 52-year-old white male presents for evaluation of sudden onset of abdominal pain and shoulder pain. His past medical history is notable for a history of coronary artery disease,
Classifying Esophageal Motility by Pressure Topography Characteristics: A Study of 400 Patients and 75 Controls
 American Journal of Gastroenterology ISSN 0002-9270 C 2007 by Am. Coll. of Gastroenterology doi: 10.1111/j.1572-0241.2007.01532.x Published by Blackwell Publishing ORIGINAL CONTRIBUTIONS Classifying Esophageal
American Journal of Gastroenterology ISSN 0002-9270 C 2007 by Am. Coll. of Gastroenterology doi: 10.1111/j.1572-0241.2007.01532.x Published by Blackwell Publishing ORIGINAL CONTRIBUTIONS Classifying Esophageal
SAGES guidelines for the surgical treatment of esophageal achalasia
 Surg Endosc (2012) 26:296 311 DOI 10.1007/s00464-011-2017-2 and Other Interventional Techniques GUIDELINES SAGES guidelines for the surgical treatment of esophageal achalasia Dimitrios Stefanidis William
Surg Endosc (2012) 26:296 311 DOI 10.1007/s00464-011-2017-2 and Other Interventional Techniques GUIDELINES SAGES guidelines for the surgical treatment of esophageal achalasia Dimitrios Stefanidis William
Canadian Association of Gastroenterology Practice Guidelines: Evaluation of dysphagia
 CAG PRACTICE GUIDELINES Canadian Association of Gastroenterology Practice Guidelines: Evaluation of dysphagia Alan W Cockeram MD FRCPC DEFINITION Dysphagia may be defined as difficulty in swallowing. Dysphagia
CAG PRACTICE GUIDELINES Canadian Association of Gastroenterology Practice Guidelines: Evaluation of dysphagia Alan W Cockeram MD FRCPC DEFINITION Dysphagia may be defined as difficulty in swallowing. Dysphagia
Achalasia esophagus, a major motility disorder, results
 GASTROENTEROLOGY 2010;139:102 111 A Unique Esophageal Motor Pattern That Involves Longitudinal Muscles Is Responsible for Emptying in Achalasia Esophagus SU JIN HONG,* VALMIK BHARGAVA, YANFEN JIANG, DEBBIE
GASTROENTEROLOGY 2010;139:102 111 A Unique Esophageal Motor Pattern That Involves Longitudinal Muscles Is Responsible for Emptying in Achalasia Esophagus SU JIN HONG,* VALMIK BHARGAVA, YANFEN JIANG, DEBBIE
Gastrointestinal Motility 2: Intestinal and Colonic Motility Jack Grider, Ph.D.
 Gastrointestinal Motility 2: Intestinal and Colonic Motility Jack Grider, Ph.D. OBJECTIVES: 1. Contrast the types of motility in the small intestine. 2. Describe the neural circuits that mediate peristalsis.
Gastrointestinal Motility 2: Intestinal and Colonic Motility Jack Grider, Ph.D. OBJECTIVES: 1. Contrast the types of motility in the small intestine. 2. Describe the neural circuits that mediate peristalsis.
Gastroesophageal Reflux Disease:
 Gastroesophageal Reflux Disease: Introduction Gastroesophageal reflux is the involuntary movement of gastric contents to the esophagus. It is a common disease, occurring in one third of the population
Gastroesophageal Reflux Disease: Introduction Gastroesophageal reflux is the involuntary movement of gastric contents to the esophagus. It is a common disease, occurring in one third of the population
Motility - Difficult Issues in Practice and How to Investigate
 Motility - Difficult Issues in Practice and How to Investigate Geoff Hebbard The Issues (Upper GI) Difficult Dysphagia Non-Cardiac Chest pain Reflux Symptoms Regurgitation Belching 1 The Tools Oesophageal
Motility - Difficult Issues in Practice and How to Investigate Geoff Hebbard The Issues (Upper GI) Difficult Dysphagia Non-Cardiac Chest pain Reflux Symptoms Regurgitation Belching 1 The Tools Oesophageal
Marc F. Catalano, MD, FACG, FACP, AGAF, FASGE Professor of Medicine Department of Internal Medicine Division of Gastroenterology and Hepatology The
 Marc F. Catalano, MD, FACG, FACP, AGAF, FASGE Professor of Medicine Department of Internal Medicine Division of Gastroenterology and Hepatology The University of Texas, McGovern Medical School Review the
Marc F. Catalano, MD, FACG, FACP, AGAF, FASGE Professor of Medicine Department of Internal Medicine Division of Gastroenterology and Hepatology The University of Texas, McGovern Medical School Review the
PeriOperative Concerns for Anti Reflux Procedure Patients
 PeriOperative Concerns for Anti Reflux Procedure Patients Kevin Gillian, M.D., F.A.C.S. VHC Heartburn Center Director GERD word association Heartburn Chest pain Spicy food Tums Purple pills How big a problem
PeriOperative Concerns for Anti Reflux Procedure Patients Kevin Gillian, M.D., F.A.C.S. VHC Heartburn Center Director GERD word association Heartburn Chest pain Spicy food Tums Purple pills How big a problem
Diffuse oesophageal spasm
 Diffuse oesophageal spasm Thorax (1966), 21, 511. D. R. CRADDOCK, A. LOGAN, AND P. R. WALBAUM From the Incoordination of muscular contraction is sometimes seen in the apparently healthy oesophagus, but
Diffuse oesophageal spasm Thorax (1966), 21, 511. D. R. CRADDOCK, A. LOGAN, AND P. R. WALBAUM From the Incoordination of muscular contraction is sometimes seen in the apparently healthy oesophagus, but
NIH Public Access Author Manuscript J Clin Gastroenterol. Author manuscript; available in PMC 2010 June 30.
 NIH Public Access Author Manuscript Published in final edited form as: J Clin Gastroenterol. 2008 ; 42(5): 627 635. doi:10.1097/mcg.0b013e31815ea291. Esophageal Motility Disorders in Terms of Pressure
NIH Public Access Author Manuscript Published in final edited form as: J Clin Gastroenterol. 2008 ; 42(5): 627 635. doi:10.1097/mcg.0b013e31815ea291. Esophageal Motility Disorders in Terms of Pressure
Esophagus: Spectrum of pathologies on Barium Swallow
 Esophagus: Spectrum of pathologies on Barium Swallow Poster No.: C-1426 Congress: ECR 2013 Type: Authors: Keywords: DOI: Educational Exhibit E. Dhamija 1, D. Chandan 1, D. Srivastava 2 ; 1 New Delhi/IN,
Esophagus: Spectrum of pathologies on Barium Swallow Poster No.: C-1426 Congress: ECR 2013 Type: Authors: Keywords: DOI: Educational Exhibit E. Dhamija 1, D. Chandan 1, D. Srivastava 2 ; 1 New Delhi/IN,