CARDIOLOGY. Certification Updates with Clinical Aspects. Federal Aviation Administration
|
|
|
- Robyn Hensley
- 5 years ago
- Views:
Transcription


1 CARDIOLOGY Certification Updates with Clinical Aspects Presented to: 2017 By: John S. Raniolo, D.O. Date: September 14, 2017

2 2
3 2012 Roundtable discussion (OKC, AAM 100 & 200) reviewed the current FAA cardiology policies that were in use identified policies that were outdated identified policies that were inconsistent or in conflict made recommendations to bring the current FAA cardiology policies in line with current clinical practices as outlined in the ACC guidelines 3
4 Coronary artery disease that require: Coronary stents (bare metal or drug-eluting) Percutaneous transluminal coronary angioplasty (PTCA) Percutaneous transluminal coronary rotational athrectomy (PTCRA) Coronary artery disease requiring Coronary artery bypass surgery Myocardial infarctions (with or without PCI) 4
5 Valve replacements (aortic, mitral) Pacemakers single chamber dual chamber bi-ventricular (with and without ICD) Hypertrophic cardiomyopathy (HCM) Atrial fibrillation Under Construction 5
6 Coronary Artery Disease Initial certification Post PCI 6
7 Initial certification Applicants for 1st and 2nd class medical certification The recovery time was reduced from 6 months to 3 months No change in the documentation is required, i.e., Hospital records to include Admission H&P Discharge summary Consultation reports (All) Procedure reports CD of the diagnostic & interventional procedure 7
8 Initial certification Current cardiovascular status report (CVE) to include diagnosis, prognosis and treatment plan. should make mention that the airman demonstrates attempting to meet goal regarding the modifiable risk factors as recommended by the ACC or AHA guidelines (i.e., lipid control, weight reduction, smoking cessation, etc.) 8
9 Initial certification Current laboratory data to include a fasting serum glucose, HgbA1C (DM) and 12 hour fasting lipid panel will require a nuclear treadmill stress test A post-event cardiac catheterization FASCC Panel review 9
10 Initial certification (PCI) Applicants for 3rd class medical certification No change in the documentation required, i.e., Hospital records to include Admission H&P Discharge summary Consultation reports (All) Procedure reports CD of the diagnostic & interventional procedure 10
11 Initial certification Current laboratory data to include a fasting serum glucose, HgbA1C (DM) and 12 hour fasting lipid panel routine exercise treadmill stress test no cardiac catheterization required no FASCC Panel review WILL NO LONGER REQUIRE A 90 DAY RECOVERY PERIOD 11
12 Initial Certification Left main stents 12
13 Initial Certification Left main stents Applicants for 1st and 2nd class medical certification previously required a 6 month recovery period and will remain unchanged A current cardiac status report nuclear treadmill stress test laboratory data (to include a fasting serum glucose, 12 hour fasting lipid panel and HgbA1C if diabetic ) FASCC Panel review 13
14 Initial Certification Left main stents Applicants for 3rd class medical certification A current cardiac status report laboratory data (to include a fasting serum glucose, 12 hour fasting lipid panel and HgbA1C if diabetic ) routine exercise stress test WILL NO LONGER REQUIRE A 90 DAY RECOVERY PERIOD All classes will require a post-event cardiac catheterization 14
15 Recertification 15
16 Recertification Applicants for ALL CLASSES medical certification A current cardiovascular status report (CVE) Laboratory data to include a fasting serum glucose and 12 hour fasting lipid panel Routine exercise treadmill stress test using the Bruce protocol 16
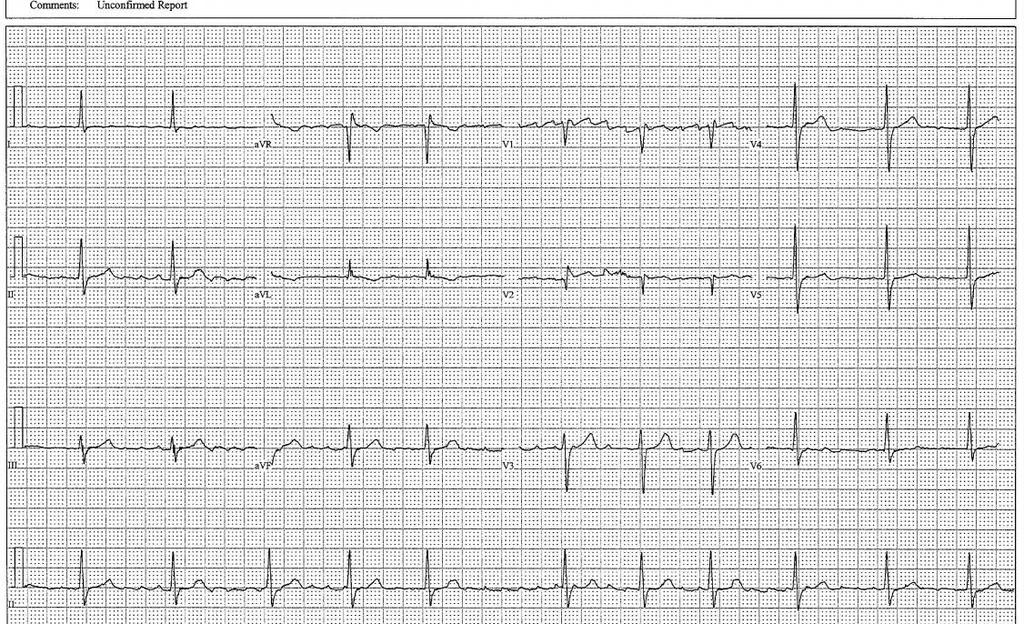
17 Bruce protocol: increasing speed & elevation 10% grade 12% grade 14% grade Heart rate achieved: must be no less than 85% of the calculated maximum predicted heart rate Airman must walk for: a minimum of 9 minutes under the age of 70 a minimum of 6 minutes 70 and older 17
18 Prior to these changes, airmen possessing a 1 st or 2nd class medical certificate were routinely placed on a 12/24 schedule. Now, all airmen requesting recertification will only require a routine exercise treadmill stress test, unless a caveat exists. 18
19 Caveats include: Complete left bundle branch block (CLBBB) uninterpretable electrocardiogram false-positive study 19
20 Caveats for treadmill stress testing Complete Left bundle branch block (CLBBB) Idiopathic Pacemaker induced the airman will be required to provide a pharmacologic stress test for initial certification. Recertification with require a pharmacologic stress test alternating with a routine exercise treadmill stress test on a 12 month basis 20
21 Caveats for treadmill stress testing uninterpretable electrocardiogram false-positive study Airmen will be asked to provide some combination of nuclear treadmill stress testing, routine exercise treadmill stress testing and stress echocardiogram, alternating on a 12 month basis 21
22 EXERCISE TREADMILL STRESS TEST It will no longer be required to include: METS Double product in the treadmill stress test reports. It is considered of minimal clinical value 22
23 Airman will not be asked to routinely discontinue Beta-blockers or calcium channel blockers prior to treadmill stress testing. However, it does not change the requirement to achieve both the required heart rate and time duration. 23
24 Medication Current ACC guidelines for stents recommend dual anti-platelet therapy with Aspirin and one of the approved anti-platelet medications (Plavix (Clopidogrel), Brilinta (Ticagrelor) or Effient (Prasugrel) a minimum of one year for Drug-eluting stents a minimum of thirty days for bare metal stents 24
25 *Remember: Any established history or clinical diagnosis of coronary artery disease, that is clinically significant or has required treatment, is one of the 16 specifically disqualifying conditions 25
26 Coronary artery bypass surgery 26
27 Initial Certification Coronary artery bypass surgery Applicants for 1st and 2nd class medical certification The recovery time remains 6 months The same documentation is required, i.e., Hospital records to include o Admission H&P o Discharge summary o Consultation reports (All) o Operative reports 27
28 Initial certification A current status report (CVE) Current laboratory data to include a fasting serum glucose, 12 hour fasting lipid panel and HgbA1C (DM) provide a nuclear treadmill stress test A post-event cardiac catheterization is required. FASCC Panel review is required 28
29 Initial certification Applicants for 3rd class medical certification The same documentation is required, i.e., Hospital records to include o Admission H&P o Discharge summary o Consultation reports (All) o Operative reports 29
30 Initial certification Applicants for 3rd class medical certification Current status report (CVE) Current laboratory data to include a fasting serum glucose, 12 hour fasting lipid panel and HgbA1C (DM) A routine exercise treadmill stress test is required 30
31 Initial certification There is no FASCC Panel review There is no post-event cardiac catheterization required. WILL NO LONGER REQUIRE A 6 MONTH RECOVERY PERIOD However, should the airman have an abnormal routine exercise stress test, he or she will be required to provide a nuclear study. Should the nuclear study be abnormal (ischemia), a cardiac catheterization will be required before a Special Issuance can be considered 31
32 Initial certification *An applicant presents to you with a history of coronary artery disease, with or with out a history of myocardial infarction, followed by bypass surgery. The AME s responsibility is to: explain the Special Issuance process outline and assist the applicant with the necessary workup defer the case to Aerospace Medical Certification Division (AMCD) 32

33 MYOCARDIAL INFARCTION 33
34 Initial certification Applicants for 1st and 2nd class medical certification The previously 6 month recovery period has been decreased to 3 months Hospital records to include Admission H&P Discharge summary Consultation reports (All) Procedure reports (if performed) CD of interventional procedure (if the procedure is performed) 34
35 A current status report (CVE) Current laboratory data to include a fasting serum glucose, 12 hour fasting lipid panel and HgbA1C (DM) Nuclear treadmill stress test A post-event cardiac catheterization FASCC Panel review 35
36 Applicants for 3rd class medical certification A current status report (CVE) provide a routine exercise treadmill stress test Current laboratory data to include a fasting serum glucose, 12 hour fasting lipid panel and HgbA1C (DM) FASCC Panel review is not required No post-event cardiac catheterization is required. NO SPECIFIED RECOVERY TIME IS REQUIRED 36
37 However, should the airman have an abnormal exercise treadmill stress test, he or she will be required to provide a nuclear study. Should the nuclear study be abnormal (ischemia), a cardiac catheterization will be required before a Special Issuance can be considered 37
38 MYOCARDIAL INFARCTION Not due to coronary artery disease 38
39 MYOCARDIAL INFARCTION Not due to coronary artery disease Examples: epinephrine injections cardiac trauma Hyper-coagulopathies, e.g., Factor V Leiden deficiency Complication of cardiac catheterization 39
40 Applicants for 1st and 2nd class medical certification A current status report (CVE) Current laboratory data to include a fasting serum glucose, 12 hour fasting lipid panel and HgbA1C (DM) Airmen will be required to provide a nuclear treadmill stress test FASCC Panel review is required This information will be forwarded to the FASCC Panel for review. A post-event cardiac catheterization will be required, only if recommended by the FASCC Panel review. 40
41 Applicants for 3rd class medical certification Current status report (CVE) Current laboratory data to include a fasting serum glucose, 12 hour fasting lipid panel and HgbA1C (DM) a routine exercise treadmill stress test There is no FASCC Panel review WILL NO LONGER REQUIRE A 90 DAY RECOVERY PERIOD 41
42 Applicants for 3rd class medical certification Should the airman have an abnormal exercise treadmill stress test, he or she will be required to provide a nuclear study. Should the study be abnormal (ischemia), a cardiac catheterization will be required before a Special Issuance can be considered 42
43 MYOCARDIAL INFARCTION Recertification for all classes Airmen will be required to provide information consistent with the FAA Coronary artery disease policy (Requirements are listed in the Authorization for Special Issuance) 43
44 *Remember, when the disqualifying condition is coronary artery disease, there is an AASI for 3rd class only. For recertification, only if an AASI has been granted and the airman has had no change in his or her condition, and all data supplied meet FAA standards, only then, can the AME issue the time-limited medical certificate (NVFAC after 12 months ) 44
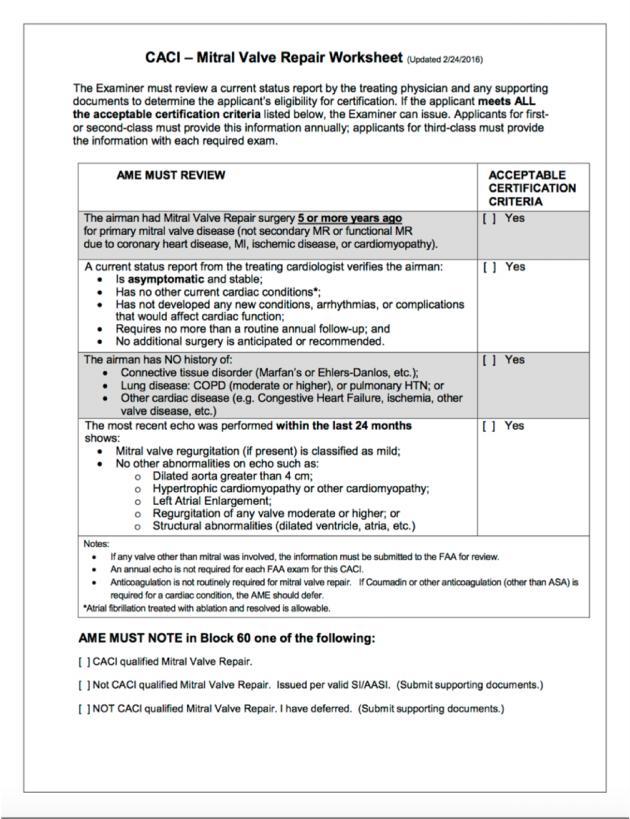
45 VALVE REPLACEMENTS 45
46 Previous policy had provisions for medical certification for: A single tissue valve replacement A single mechanical valve replacement New change: Double valve replacement can now be considered for medical certification on an individual basis. 46
47 Double valve replacement Applicants for 1st and 2nd class medical certification (INITIAL) 6 month recovery period Hospital records to include Admission H&P Discharge summary Consultation reports Operative reports 47
48 Double valve replacement Current cardiovascular status report (CVE) 2D/M-mode echocardiogram, cardiac doppler with color flow (No peri-valvular leaks) 24 hour Holter monitor 48
49 Double valve replacement Routine exercise treadmill stress test may be required Mechanical valves that require Coumadin. Airmen must provide INR s (80% within 2.5 to 3.5 unless St. Jude bi-leaflet valve or ON-X then allow 1.5 to 2.5) Manufacturer s recommendations. Remember: The new oral anticoagulant agents cannot be used for prosthetic valves. 49
50 Double valve replacement Path report, if available (Cystic medial necrosis remains disqualifying) FASCC Panel review The FASCC Panel s recommendation will be sent to AAM200 for final decision on a case by case basis 50
51 Double valve replacement Applicants for 3rd class medical certification The only change will be NO SPECIFIED RECOVERY TIME REQUIRED 51
52 Double valve replacement Recertification for all classes 52
53 Double valve replacement Current status report (CVE) 2D/M-mode echocardiogram, cardiac doppler with color flow 12 lead electrocardiogram Routine exercise treadmill stress test, unless otherwise specified, e.g., if coronary artery disease exists. 53
54 Double valve replacement INR requirements are the same for mechanical valves (80% of the values must be between for most valves. On-x valves should have 80% of the values between ) 54
55 Initial certification *The 1st step in discovering valvular heart disease is the physical examination. Heart murmurs: Timing (systolic v. diastolic) Character (harsh, soft, blowing) Intensity, grade 1 thru 6 Location Radiation Any change with respiration 55
56 Initial certification Functional v. pathologic 2D/M-mode echocardiogram, cardiac doppler with color flow *If you conclude that the murmur is functional, enter these remarks in Block 60 and issue the medical certificate. 56
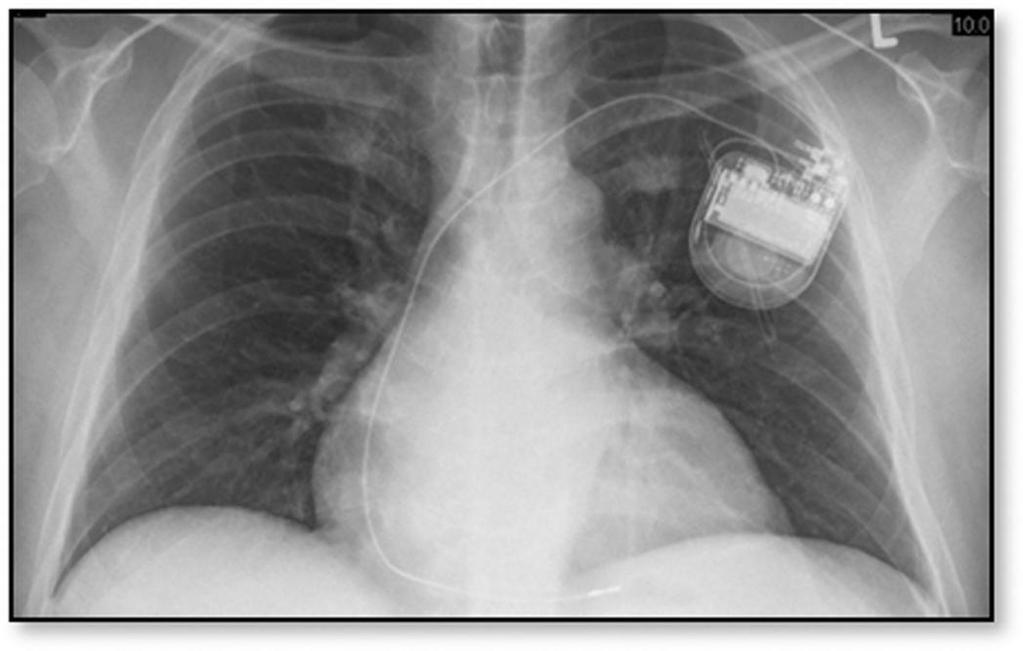
57 PACEMAKERS 57

58 58
59 59
60 PACEMAKERS Initial certification for all classes Single chamber pacemaker Dual chamber pacemaker Bi-ventricular pacemaker Biventricular pacemaker with ICD *ICDs are disqualifying for all classes 60
61 PACEMAKERS Initial pacemaker implantation recovery time is 2 months Lead replacement and generator replacement recovery time is 2 months Acute thresholds, post-implant Chronic thresholds, 8-12 weeks post implant Generator replacement can be certified as soon as the airman has fully recovered (as little as 10 days) 61
62 Initial Certification For all classes All hospital records to include: Operative report Consultation report Discharge Summary A current status report by the treating cardiologist 24 hour Holter monitor 62
63 Initial Certification For all classes 2D/M-mode echocardiogram, cardiac doppler with color flow Lipid profile and fasting serum glucose Exercise treadmill stress test FAA Pacemaker protocol worksheet 63
64 64
65 PACEMAKER DEPENDENCY 13. Is the airman pacer dependent (Class 1 and 2)? Yes No ANNUAL: Obtain a 3 minute rhythm strip, sitting, pacer reset to 30. Dependent: If remains paced, symptomatic or blood pressure drops 65
66 PACEMAKER DEPENDENCY The pacemaker is to be set at its lowest rate (30) PPM for 3 minutes. A rhythm strip is to be obtained to document the underlying rhythm. If the underlying rhythm remains paced rhythm, or if the airman develops symptoms or if the blood pressure falls, the airman will be considered pacemaker dependent. 3rd class only can be issued a medical certificate if pacemaker dependent. 66
67 All the information should be forwarded to OKC or to the RFS for review. 67
68 Recertification 68
69 Recertification Pacemaker analysis will be required every 6 months with completion of pacemaker worksheet 6 and 12 month worksheets will be submitted with a current status report from the airman s treating cardiologist (as long as the Estimated Battery Longevity is more than 18 months) 69
70 Recertification If the estimated battery life is less than 18 months: A current status report will be required at each six (6) month interval. The pacemaker analysis and pacemaker worksheets will be required every six (6) months. The information will be forwarded to OKC or your RFS every six (6) months 70
71 Recertification When the EBL reaches 6 months, the airman will be DENIED. Once the generator has been replaced, the airman can apply for recertification. The airman can potentially be in Limbo for up to six months. 71
72 HYPERTROPHIC CARDIOMYOPATHY (HCM) 72
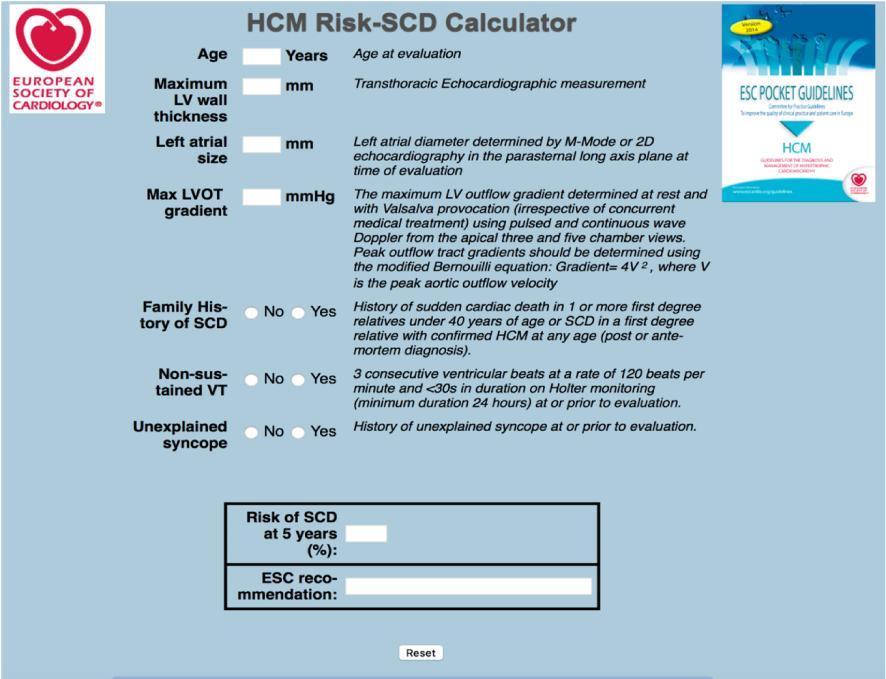
73 Initial Certification (for all classes) MAJOR risk factors used to determine whether or not the airman is considered high risk: Family history of sudden death Unexplained syncope Documented ventricular tachycardia Symptoms of angina 73
74 Initial Certification (for all classes) Risk factors used to determine whether or not the airman is considered high risk: Congestive heart failure Lack of blood pressure augmentation during exercise treadmill stress testing Left ventricular wall thickness 30mm 74
75 Initial Certification (for all classes) If the applicant has any of these risk factors, the applicant will be considered high risk and denied consideration for medical certification. 75
76 Initial Certification (for all classes) If the airman has none of the high risk factors, the airman s medical information will be reviewed by the FASCC Panel, and their recommendations will be forwarded to AAM200 for further reconsideration 76

77 APICAL HYPERTROPHIC CARDIOMYOPATHY 77
78 78
79 Initial Certification (for all classes) Hypertrophic cardiomyopathies that have undergone alcohol septal ablation or surgical myomectomy will be evaluated in the same manner following an appropriate recovery time from the procedure. 79
80 80

81 HYPERTROPHIC CARDIOMYOPATHY 81

82 HYPERTROPHIC CARDIOMYOPATHY 82

83 HYPERTROPHIC CARDIOMYOPATHY 83

84 HYPERTROPHIC CARDIOMYOPATHY 84

85 HYPERTROPHIC CARDIOMYOPATHY 85

86 HYPERTROPHIC CARDIOMYOPATHY 86
87 Recertification 87
88 Recertification For all classes All information as required by the Authorization for Special Issuance will be sent to OKC for review and disposition. 88
89 ATRIAL FIBRILLATION 89
90 90
91 ANTICOAGULATION 91
92 CHADS2 score Congestive heart failure (1) Hypertension (1) Age (75) (1) Diabetes mellitus (1) Stroke (2) 92
93 A score of 0 requires no anticoagulation A score of 1, requires Aspirin (can opt to use Coumadin) A score of 2 or higher, requires anticoagulation with Coumadin or one of the new oral anticoagulants (Xarelto, Eliquis or Pradaxa) 93
94 CHA2DS2VASc This was based on two groups of risk factors DEFINITIVE risk factors Prior history of stroke or TIA Age 75 or older COMBINATION risk factors Hypertension Heart failure Diabetes mellitus Age Female gender Vascular disease 94
95 CHA2DS2VASc C H A2 D S2 V A Sc Congestive heart failure or LV dysfunction Hypertension Age (75 or older) Diabetes mellitus Stroke/TIA/TE (thromboembolism) Vascular disease (CAD, MI, PAD or Aortic plaque) Age Sex category High risk equals a score of two or greater
96 96
97 24 HOUR HOLTER MONITOR The maximum average heart rate was changed from 100 to 110 beats per minute. 3 second or greater pauses remain disqualifying if the airman is symptomatic or if occurring during waking hours with activity. Increased vagal tone during sleep is not disqualifying. 97
98 AMBULATORY ECG MONITORING Holter monitors These recorders are typically used for 24 or 48 hours to record events which might reasonably be expected to occur within that time-frame, i.e., frequent, or at least once a day symptoms. 98
99 AMBULATORY ECG MONITORING Intermittent recorders: These are generally for recording infrequent symptoms, and are one of two types: Event recorders, which store only a brief recording of ECG activity when activated by the patient in response to symptoms. Loop recorders, which record the ECG in a continuous fashion, but store only a brief record when activated by the patient or triggered by the preprogrammed parameters. Both types of intermittent recorder may be worn by patients for periods of many weeks in order to capture infrequently occurring events. 99
100 AMBULATORY ECG MONITORING Implantable loop recorders (ILR) It is used to record the heart rate and rhythm and help diagnose whether symptoms like fainting, dizziness, palpitations and unexplained seizure-like episodes have a cardiovascular cause. 100
101 Indications for ambulatory monitoring Patients with syncope, near syncope or dizziness Patients with palpitations Continuous ECG monitoring for AF is useful to detect silent paroxysmal AF in patients without previously documented arrhythmic episodes, such as those with cryptogenic stroke. Early diagnosis enables earlier treatment for both primary and secondary stroke prevention 101
102 AMBULATORY ECG MONITORING may be used to assess a patient's response to antiarrhythmic treatment, e.g., the rate of atrial fibrillation, or pro-arrhythmic responses to drugs. may be used to assess the function of a pacemaker device or ICD. 102
103 CACI 103
104 104

105 105
106 UNDER CONSTRUCTION Aortic root dilatation and ascending aortic aneurysm Top normal dimension is 37mm (3.7cm) >37mm and <40mm (4.cm) do not get a Special Issuance but fall under General review 40mm (4.0cm) to <50mm (5.0cm) will be placed on a Special Issuance Currently 50mm (5.0cm) is disqualifying 106
107 UNDER CONSTRUCTION Aortic root dilatation and abdominal aortic aneurysm 50mm-55mm ( cm): LIMBO 55mm or greater consider surgical repair Pertinent values on echocardiogram will need to be reviewed by the AME in order to issue a medical certificate. This disqualifying condition will likely remain as an Special Issuance and not become a CACI. New policy to address airmen in LIMBO is in progress 107
108 UNDER CONSTRUCTION The New oral anticoagulants (NOAC) (Pradaxa, Eliquis, Xarelto) Current policy requires a status report from the treating physician every six (6) months. It is being considered to extend to every twelve (12) months. 108
109 UNDER CONSTRUCTION 12 Lead Electrocardiogram Normal, Normal variants and Abnormal The criteria have been placed in the AME guide, along with the required testing for the abnormal ECGs 109
110 UNDER CONSTRUCTION Pacemaker worksheet Currently, the only way to get a worksheet is when it is included in the authorization (AASI or SI) to the airman It will be going into the AME guide 110
111 UNDER CONSTRUCTION Hypertrophic Cardiomyopathy It is not currently in the AME Guide but plans are being made for it to be placed under the protocol section 111

112 112
113 113

114 114

115 THE END 115
116 QUESTIONS 116
117 QUESTIONS 117
118 CHA2DS2VASc v. CHADS2 CHADS2 left too many gray areas and sometimes used as an excuse not to prescribe Warfarin CHADS2 failed to consider women s greater stroke risk with atrial fibrillation where CHA2DS2VASc does. When women do take Coumadin and have comparable INR control, the risk of stroke is reduced and they are not more likely to suffer a major bleed. 118
119 CHA2DS2VASc An additional way of identifying who should be on anticoagulants Question 1. Age 75 or older?...if yes, oral anticoagualtion. If no, then: Question 2. History of Sroke, TIA or thromboembolic event? If yes, then oral anticoagulation. If no, then: Question 3. Gender? If male, go to risk factors. Male + 2 risk factors = oral anticoagulation. If female, go to risk factors. If female + one risk factor, then oral anticoagulation. 119
Recommended Evaluation Data Excerpt from NVIC 04-08
 Recommended Evaluation Data Excerpt from NVIC 04-08 Purpose: This document is an excerpt from the Medical and Physical Evaluations Guidelines for Merchant Mariner Credentials, contained in enclosure 3
Recommended Evaluation Data Excerpt from NVIC 04-08 Purpose: This document is an excerpt from the Medical and Physical Evaluations Guidelines for Merchant Mariner Credentials, contained in enclosure 3
Holy Crap! Why is a Cardiologist Speaking at a GI Meeting? Jonathan A. Rapp, MD, FACC, FSCAI Cardiologist, Mercy Heart Institute Cincinnati, OH
 Holy Crap! Why is a Cardiologist Speaking at a GI Meeting? Jonathan A. Rapp, MD, FACC, FSCAI Cardiologist, Mercy Heart Institute Cincinnati, OH Goals and Objectives Discuss cardiac considerations for patients
Holy Crap! Why is a Cardiologist Speaking at a GI Meeting? Jonathan A. Rapp, MD, FACC, FSCAI Cardiologist, Mercy Heart Institute Cincinnati, OH Goals and Objectives Discuss cardiac considerations for patients
Bleeding Management Strategies. Aiming for the best Outcomes August 27, Amit Gupta, MD FACC FSCAI Interventional Cardiologist CANM
 Bleeding Management Strategies Aiming for the best Outcomes August 27, 2016 Amit Gupta, MD FACC FSCAI Interventional Cardiologist CANM Learning Objectives Review the use of anti-coagulants in patients
Bleeding Management Strategies Aiming for the best Outcomes August 27, 2016 Amit Gupta, MD FACC FSCAI Interventional Cardiologist CANM Learning Objectives Review the use of anti-coagulants in patients
(For items 1-12, each question specifies mark one or mark all that apply.)
") Form 121 - Report of Cardiovascular Outcome Ver. 9.2 COMMENTS -Affix label here- Member ID: - - To be completed by Physician Adjudicator Date Completed: - - (M/D/Y) Adjudicator Code: - Central Case No.:
Form 121 - Report of Cardiovascular Outcome Ver. 9.2 COMMENTS -Affix label here- Member ID: - - To be completed by Physician Adjudicator Date Completed: - - (M/D/Y) Adjudicator Code: - Central Case No.:
C1: Medical Standards for Safety Critical Workers with Cardiovascular Disorders
 C1: Medical Standards for Safety Critical Workers with Cardiovascular Disorders GENERAL ISSUES REGARDING MEDICAL FITNESS-FOR-DUTY 1. These medical standards apply to Union Pacific Railroad (UPRR) employees
C1: Medical Standards for Safety Critical Workers with Cardiovascular Disorders GENERAL ISSUES REGARDING MEDICAL FITNESS-FOR-DUTY 1. These medical standards apply to Union Pacific Railroad (UPRR) employees
Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition
 Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition Table of Contents Volume 1 Chapter 1: Cardiovascular Anatomy and Physiology Basic Cardiac
Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition Table of Contents Volume 1 Chapter 1: Cardiovascular Anatomy and Physiology Basic Cardiac
Ambulatory Cardiac Monitors and Outpatient Telemetry Corporate Medical Policy
 Ambulatory Cardiac Monitors and Outpatient Telemetry Corporate Medical Policy File Name: Ambulatory Event Monitors and Mobile Cardiac Outpatient Telemetry File Code: UM.SPSVC.13 Origination: 10/2015 Last
Ambulatory Cardiac Monitors and Outpatient Telemetry Corporate Medical Policy File Name: Ambulatory Event Monitors and Mobile Cardiac Outpatient Telemetry File Code: UM.SPSVC.13 Origination: 10/2015 Last
Dysrhythmias 11/7/2017. Disclosures. 3 reasons to evaluate and treat dysrhythmias. None. Eliminate symptoms and improve hemodynamics
 Dysrhythmias CYDNEY STEWART MD, FACC NOVEMBER 3, 2017 Disclosures None 3 reasons to evaluate and treat dysrhythmias Eliminate symptoms and improve hemodynamics Prevent imminent death/hemodynamic compromise
Dysrhythmias CYDNEY STEWART MD, FACC NOVEMBER 3, 2017 Disclosures None 3 reasons to evaluate and treat dysrhythmias Eliminate symptoms and improve hemodynamics Prevent imminent death/hemodynamic compromise
Management of ATRIAL FIBRILLATION. in general practice. 22 BPJ Issue 39
 Management of ATRIAL FIBRILLATION in general practice 22 BPJ Issue 39 What is atrial fibrillation? Atrial fibrillation (AF) is the most common cardiac arrhythmia encountered in primary care. It is often
Management of ATRIAL FIBRILLATION in general practice 22 BPJ Issue 39 What is atrial fibrillation? Atrial fibrillation (AF) is the most common cardiac arrhythmia encountered in primary care. It is often
Seek and Ye Shall Find: Surprising Findings When Using the ILR-LINQ
 Seek and Ye Shall Find: Surprising Findings When Using the ILR-LINQ Suneet Mittal, MD, FACC, FHRS Director, Electrophysiology Laboratory Valley Health System www.arrhythmia.org; @drsuneet October 31, 2015
Seek and Ye Shall Find: Surprising Findings When Using the ILR-LINQ Suneet Mittal, MD, FACC, FHRS Director, Electrophysiology Laboratory Valley Health System www.arrhythmia.org; @drsuneet October 31, 2015
7. Echocardiography Appropriate Use Criteria (by Indication)
") Criteria for Echocardiography 1133 7. Echocardiography Criteria (by ) Table 1. TTE for General Evaluation of Cardiac Structure and Function Suspected Cardiac Etiology General With TTE 1. Symptoms or conditions
Criteria for Echocardiography 1133 7. Echocardiography Criteria (by ) Table 1. TTE for General Evaluation of Cardiac Structure and Function Suspected Cardiac Etiology General With TTE 1. Symptoms or conditions
Common Codes for ICD-10
 Common Codes for ICD-10 Specialty: Cardiology *Always utilize more specific codes first. ABNORMALITIES OF HEART RHYTHM ICD-9-CM Codes: 427.81, 427.89, 785.0, 785.1, 785.3 R00.0 Tachycardia, unspecified
Common Codes for ICD-10 Specialty: Cardiology *Always utilize more specific codes first. ABNORMALITIES OF HEART RHYTHM ICD-9-CM Codes: 427.81, 427.89, 785.0, 785.1, 785.3 R00.0 Tachycardia, unspecified
Antiplatelet and Anti-Thrombotic Therapy. Ivan Anderson, MD RIHVH Cardiology
 Antiplatelet and Anti-Thrombotic Therapy Ivan Anderson, MD RIHVH Cardiology Outline Anti-thrombotic therapy Risk stratification of stroke with atrial fibrillation DVT and PE treatment Pharmacology Anti-platelet
Antiplatelet and Anti-Thrombotic Therapy Ivan Anderson, MD RIHVH Cardiology Outline Anti-thrombotic therapy Risk stratification of stroke with atrial fibrillation DVT and PE treatment Pharmacology Anti-platelet
Invasive and Medical Treatments for Atrial Fibrillation. Thomas J Dresing, MD Section of Electrophysiology and Pacing Cleveland Clinic
 Invasive and Medical Treatments for Thomas J Dresing, MD Section of Electrophysiology and Pacing Cleveland Clinic Disclosures Fellow s advisory panel for St Jude Medical Speaking honoraria from: Boston
Invasive and Medical Treatments for Thomas J Dresing, MD Section of Electrophysiology and Pacing Cleveland Clinic Disclosures Fellow s advisory panel for St Jude Medical Speaking honoraria from: Boston
Measurement Name Beta-Blocker Therapy Prior Myocardial Infarction (MI)
") Program Metrics The list below includes the metrics that will be calculated by the PINNACLE Registry for the outpatient office setting. These include metrics for Artery, Atrial Fibrillation, Hypertension
Program Metrics The list below includes the metrics that will be calculated by the PINNACLE Registry for the outpatient office setting. These include metrics for Artery, Atrial Fibrillation, Hypertension
Asif Serajian DO FACC FSCAI
 Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Managing Hypertrophic Cardiomyopathy with Imaging. Gisela C. Mueller University of Michigan Department of Radiology
 Managing Hypertrophic Cardiomyopathy with Imaging Gisela C. Mueller University of Michigan Department of Radiology Disclosures Gadolinium contrast material for cardiac MRI Acronyms Afib CAD Atrial fibrillation
Managing Hypertrophic Cardiomyopathy with Imaging Gisela C. Mueller University of Michigan Department of Radiology Disclosures Gadolinium contrast material for cardiac MRI Acronyms Afib CAD Atrial fibrillation
HEART OF THE MATTER: cardiac issues in safe endoscopy & sedation
 HEART OF THE MATTER: cardiac issues in safe endoscopy & sedation YUVAL KONSTANTINO M.D. CARDIOLOGY DEPARTMENT, ELECTROPHYSIOLOGY UNIT, SOROKA MEDICAL CENTER, BEN-GURION UNIVERSITY OUTLINE 1 2 3 Anticoagulation
HEART OF THE MATTER: cardiac issues in safe endoscopy & sedation YUVAL KONSTANTINO M.D. CARDIOLOGY DEPARTMENT, ELECTROPHYSIOLOGY UNIT, SOROKA MEDICAL CENTER, BEN-GURION UNIVERSITY OUTLINE 1 2 3 Anticoagulation
Perioperative Cardiovascular Evaluation and Care for Noncardiac. Dr Mahmoud Ebrahimi Interventional cardiologist 91/9/30
 Perioperative Cardiovascular Evaluation and Care for Noncardiac Surgery Dr Mahmoud Ebrahimi Interventional cardiologist 91/9/30 Active Cardiac Conditions for Which the Patient Should Undergo Evaluation
Perioperative Cardiovascular Evaluation and Care for Noncardiac Surgery Dr Mahmoud Ebrahimi Interventional cardiologist 91/9/30 Active Cardiac Conditions for Which the Patient Should Undergo Evaluation
HEART CONDITIONS IN SPORT
 HEART CONDITIONS IN SPORT Dr. Anita Green CHD Risk Factors Smoking Hyperlipidaemia Hypertension Obesity Physical Inactivity Diabetes Risks are cumulative (multiplicative) Lifestyles predispose to RF One
HEART CONDITIONS IN SPORT Dr. Anita Green CHD Risk Factors Smoking Hyperlipidaemia Hypertension Obesity Physical Inactivity Diabetes Risks are cumulative (multiplicative) Lifestyles predispose to RF One
LVHN Cardiac Diagnostic Testing PCP/PCP Office Testing Cheat Sheet. September 2017
 LVHN Cardiac Diagnostic Testing PCP/PCP Office Testing Cheat Sheet September 2017 1. ECHOCARDIOGRAM A (transthoracic) echocardiogram (2D Echo) is a 2-dimensional graphic of the heart s movement, valves
LVHN Cardiac Diagnostic Testing PCP/PCP Office Testing Cheat Sheet September 2017 1. ECHOCARDIOGRAM A (transthoracic) echocardiogram (2D Echo) is a 2-dimensional graphic of the heart s movement, valves
Clinical Policy: Holter Monitors Reference Number: CP.MP.113
 Clinical Policy: Reference Number: CP.MP.113 Effective Date: 05/18 Last Review Date: 04/18 Coding Implications Revision Log Description Ambulatory electrocardiogram (ECG) monitoring provides a view of
Clinical Policy: Reference Number: CP.MP.113 Effective Date: 05/18 Last Review Date: 04/18 Coding Implications Revision Log Description Ambulatory electrocardiogram (ECG) monitoring provides a view of
Patient Resources: Arrhythmias and Congenital Heart Disease
 Patient Resources: Arrhythmias and Congenital Heart Disease Overview Arrhythmias (abnormal heart rhythms) can develop in patients with congenital heart disease (CHD) due to thickening/weakening of their
Patient Resources: Arrhythmias and Congenital Heart Disease Overview Arrhythmias (abnormal heart rhythms) can develop in patients with congenital heart disease (CHD) due to thickening/weakening of their
ASE 2011 Appropriate Use Criteria for Echocardiography
 ASE 2011 Appropriate Use Criteria for Echocardiography Table 1. TTE for General Evaluation of Cardiac Structure and Function 1 2 Suspected Cardiac Etiology General With TTE Symptoms or conditions potentially
ASE 2011 Appropriate Use Criteria for Echocardiography Table 1. TTE for General Evaluation of Cardiac Structure and Function 1 2 Suspected Cardiac Etiology General With TTE Symptoms or conditions potentially
Cardiac Diagnostic Testing Reference Guide January 2018
 STAT Cardiac Testing is available for inpatients only. ECHOCARDIOGRAM Cardiac Diagnostic Testing A (transthoracic) echocardiogram (2D Echo) is a 2-dimensional graphic of the heart's movement, valves and
STAT Cardiac Testing is available for inpatients only. ECHOCARDIOGRAM Cardiac Diagnostic Testing A (transthoracic) echocardiogram (2D Echo) is a 2-dimensional graphic of the heart's movement, valves and
Anticoagulation Management Around Endoscopy: GI Perspective. Nathan Landesman, DO FACOI Flint Gastroenterology Associates October 11, 2017
 Anticoagulation Management Around Endoscopy: GI Perspective Nathan Landesman, DO FACOI Flint Gastroenterology Associates October 11, 2017 EDUCATIONAL OBJECTIVES Understand risks of holding anticoagulation
Anticoagulation Management Around Endoscopy: GI Perspective Nathan Landesman, DO FACOI Flint Gastroenterology Associates October 11, 2017 EDUCATIONAL OBJECTIVES Understand risks of holding anticoagulation
Basics of Atrial Fibrillation. By Mini Thannikal NP-BC Mount Sinai St Luke s Hospital New York, NY
 Basics of Atrial Fibrillation By Mini Thannikal NP-BC Mount Sinai St Luke s Hospital New York, NY Atrial Fibrillation(AF) is a supraventricular tachyarrhythmia characterized by uncoordinated atrial activation
Basics of Atrial Fibrillation By Mini Thannikal NP-BC Mount Sinai St Luke s Hospital New York, NY Atrial Fibrillation(AF) is a supraventricular tachyarrhythmia characterized by uncoordinated atrial activation
Cryptogenic Stroke: A logical approach to a common clinical problem
 Cryptogenic Stroke: A logical approach to a common clinical problem Alphonse M. Ambrosia, DO, FACC Interventional Cardiologist CardioVascular Associates of Mesa Mesa, Arizona Speakers Bureau Boston Scientific
Cryptogenic Stroke: A logical approach to a common clinical problem Alphonse M. Ambrosia, DO, FACC Interventional Cardiologist CardioVascular Associates of Mesa Mesa, Arizona Speakers Bureau Boston Scientific
ESC Stockholm Arrhythmias & pacing
 ESC Stockholm 2010 Take Home Messages for Practitioners Arrhythmias & pacing Prof. Panos E. Vardas Professor of Cardiology Heraklion University Hospital Crete, Greece Disclosures Small teaching fees from
ESC Stockholm 2010 Take Home Messages for Practitioners Arrhythmias & pacing Prof. Panos E. Vardas Professor of Cardiology Heraklion University Hospital Crete, Greece Disclosures Small teaching fees from
Rhythm Control: Is There a Role for the PCP? Blake Norris, MD, FACC BHHI Primary Care Symposium February 28, 2014
 Rhythm Control: Is There a Role for the PCP? Blake Norris, MD, FACC BHHI Primary Care Symposium February 28, 2014 Financial disclosures Consultant Medtronic 3 reasons to evaluate and treat arrhythmias
Rhythm Control: Is There a Role for the PCP? Blake Norris, MD, FACC BHHI Primary Care Symposium February 28, 2014 Financial disclosures Consultant Medtronic 3 reasons to evaluate and treat arrhythmias
OUTPATIENT ANTITHROMBOTIC MANAGEMENT POST NON-ST ELEVATION ACUTE CORONARY SYNDROME. TARGET AUDIENCE: All Canadian health care professionals.
 OUTPATIENT ANTITHROMBOTIC MANAGEMENT POST NON-ST ELEVATION ACUTE CORONARY SYNDROME TARGET AUDIENCE: All Canadian health care professionals. OBJECTIVE: To review the use of antiplatelet agents and oral
OUTPATIENT ANTITHROMBOTIC MANAGEMENT POST NON-ST ELEVATION ACUTE CORONARY SYNDROME TARGET AUDIENCE: All Canadian health care professionals. OBJECTIVE: To review the use of antiplatelet agents and oral
IHCP bulletin INDIANA HEALTH COVERAGE PROGRAMS BT JANUARY 24, 2012
 IHCP bulletin INDIANA HEALTH COVERAGE PROGRAMS BT201203 JANUARY 24, 2012 The IHCP to reimburse implantable cardioverter defibrillators separately from outpatient implantation Effective March 1, 2012, the
IHCP bulletin INDIANA HEALTH COVERAGE PROGRAMS BT201203 JANUARY 24, 2012 The IHCP to reimburse implantable cardioverter defibrillators separately from outpatient implantation Effective March 1, 2012, the
Program Metrics. New Unique ID. Old Unique ID. Metric Set Metric Name Description. Old Metric Name
 Program Metrics The list below includes the metrics that will be calculated by the PINNACLE Registry for the outpatient office setting. These include metrics for, Atrial Fibrillation, Hypertension and.
Program Metrics The list below includes the metrics that will be calculated by the PINNACLE Registry for the outpatient office setting. These include metrics for, Atrial Fibrillation, Hypertension and.
Cardiovascular Disorders Lecture 3 Coronar Artery Diseases
 Cardiovascular Disorders Lecture 3 Coronar Artery Diseases By Prof. El Sayed Abdel Fattah Eid Lecturer of Internal Medicine Delta University Coronary Heart Diseases It is the leading cause of death in
Cardiovascular Disorders Lecture 3 Coronar Artery Diseases By Prof. El Sayed Abdel Fattah Eid Lecturer of Internal Medicine Delta University Coronary Heart Diseases It is the leading cause of death in
Cardiology/Cardiothoracic
 Cardiology/Cardiothoracic ICD-9-CM to ICD-10-CM Code Mapper 800-334-5724 www.contexomedia.com 2013 ICD-9-CM 272.0 Pure hypercholesterolemia 272.2 Mixed hyperlipidemia 272.4 Other and hyperlipidemia 278.00
Cardiology/Cardiothoracic ICD-9-CM to ICD-10-CM Code Mapper 800-334-5724 www.contexomedia.com 2013 ICD-9-CM 272.0 Pure hypercholesterolemia 272.2 Mixed hyperlipidemia 272.4 Other and hyperlipidemia 278.00
2018 HPN Provider Summary Guide. Adult Cardiology Patients (18 Years and Older) Referral Guidelines
 Referral Guidelines") 12.2 CARDIOLOGY REFERRAL GUIDELINES Contracted Group: Southwest Medical Associates For Appointments: 888 S. Rancho Las Vegas, NV 89109 Phone: (702) 877-8654 Fax: (702) 242-7998 Adult Cardiology Patients
12.2 CARDIOLOGY REFERRAL GUIDELINES Contracted Group: Southwest Medical Associates For Appointments: 888 S. Rancho Las Vegas, NV 89109 Phone: (702) 877-8654 Fax: (702) 242-7998 Adult Cardiology Patients
Mission Statement for our Arrhythmia Care
 Mission Statement for our Arrhythmia Care We are dedicated to provide a compassionate and an outstanding care for patients with cardiac arrhythmias. We will be utilizing the cutting edge and the most advanced
Mission Statement for our Arrhythmia Care We are dedicated to provide a compassionate and an outstanding care for patients with cardiac arrhythmias. We will be utilizing the cutting edge and the most advanced
Detection Of Heart. By Dr Gary Mo
 Detection Of Heart Disease By Dr Gary Mo Types Of Heart Disease A. Coronary Heart Disease B. Valvular Heart Disease C. Cardiac Arrhythmia ( Rhythm disturbance ) D. Heart Blocks ( Conduction Abnormalities
Detection Of Heart Disease By Dr Gary Mo Types Of Heart Disease A. Coronary Heart Disease B. Valvular Heart Disease C. Cardiac Arrhythmia ( Rhythm disturbance ) D. Heart Blocks ( Conduction Abnormalities
Cardiac Conditions in Sport & Exercise. Cardiac Conditions in Sport. USA - Sudden Cardiac Death (SCD) Dr Anita Green. Sudden Cardiac Death
 Dr Anita Green. Sudden Cardiac Death") Cardiac Conditions in Sport & Exercise Dr Anita Green Cardiac Conditions in Sport Sudden Cardiac Death USA - Sudden Cardiac Death (SCD)
Cardiac Conditions in Sport & Exercise Dr Anita Green Cardiac Conditions in Sport Sudden Cardiac Death USA - Sudden Cardiac Death (SCD)
Performance and Quality Measures 1. NQF Measure Number. Coronary Artery Disease Measure Set
 Unless indicated, the PINNACLE Registry measures are endorsed by the American College of Cardiology Foundation and the American Heart Association and may be used for purposes of health care insurance payer
Unless indicated, the PINNACLE Registry measures are endorsed by the American College of Cardiology Foundation and the American Heart Association and may be used for purposes of health care insurance payer
Rebuttal. Jerónimo Farré MD 2010
 Rebuttal 1.We do not know what are the types of AF in which ablation is worthless or most effective 2.Waiting implies to consider the ablation at an older age and when the duration of the history of AF
Rebuttal 1.We do not know what are the types of AF in which ablation is worthless or most effective 2.Waiting implies to consider the ablation at an older age and when the duration of the history of AF
Quality Measures MIPS CV Specific
 Quality Measures MIPS CV Specific MEASURE NAME Atrial Fibrillation and Atrial Flutter: Chronic Anticoagulation Therapy CAHPS for MIPS Clinician/Group Survey Cardiac Rehabilitation Patient Referral from
Quality Measures MIPS CV Specific MEASURE NAME Atrial Fibrillation and Atrial Flutter: Chronic Anticoagulation Therapy CAHPS for MIPS Clinician/Group Survey Cardiac Rehabilitation Patient Referral from
AF in the ER: Common Scenarios CASE 1. Fast facts. Diagnosis. Management
 AF in the ER: Common Scenarios Atrial fibrillation is a common problem with a wide spectrum of presentations. Below are five common emergency room scenarios and the management strategies for each. Evan
AF in the ER: Common Scenarios Atrial fibrillation is a common problem with a wide spectrum of presentations. Below are five common emergency room scenarios and the management strategies for each. Evan
Index of subjects. effect on ventricular tachycardia 30 treatment with 101, 116 boosterpump 80 Brockenbrough phenomenon 55, 125
 145 Index of subjects A accessory pathways 3 amiodarone 4, 5, 6, 23, 30, 97, 102 angina pectoris 4, 24, 1l0, 137, 139, 140 angulation, of cavity 73, 74 aorta aortic flow velocity 2 aortic insufficiency
145 Index of subjects A accessory pathways 3 amiodarone 4, 5, 6, 23, 30, 97, 102 angina pectoris 4, 24, 1l0, 137, 139, 140 angulation, of cavity 73, 74 aorta aortic flow velocity 2 aortic insufficiency
Arrhythmia 341. Ahmad Hersi Professor of Cardiology KSU
 Arrhythmia 341 Ahmad Hersi Professor of Cardiology KSU Objectives Epidemiology and Mechanisms of AF Evaluation of AF patients Classification of AF Treatment and Risk stratification of AF Identify other
Arrhythmia 341 Ahmad Hersi Professor of Cardiology KSU Objectives Epidemiology and Mechanisms of AF Evaluation of AF patients Classification of AF Treatment and Risk stratification of AF Identify other
GRAND ROUNDS - DILEMMAS IN ANTICOAGULATION AND ANTIPLATELET THERAPY. Nick Collins February 2017
 GRAND ROUNDS - DILEMMAS IN ANTICOAGULATION AND ANTIPLATELET THERAPY Nick Collins February 2017 DISCLOSURES Before I commence Acknowledge.. Interventional Cardiologist Perception evolved. Interventional
GRAND ROUNDS - DILEMMAS IN ANTICOAGULATION AND ANTIPLATELET THERAPY Nick Collins February 2017 DISCLOSURES Before I commence Acknowledge.. Interventional Cardiologist Perception evolved. Interventional
A. AOPA Pilot magazine B. epilot newsletter C. invitation D. Previous medical webinar
 A. AOPA Pilot magazine B. epilot newsletter C. Email invitation D. Previous medical webinar Perhaps one of the most important regulations It is the self-certification mechanism that places the burden on
A. AOPA Pilot magazine B. epilot newsletter C. Email invitation D. Previous medical webinar Perhaps one of the most important regulations It is the self-certification mechanism that places the burden on
6/1/18 LEARNING OBJECTIVES PATIENT POPULATION PRESENTATIONS
 PREVENTING HOSPITAL READMISSIONS IN CARDIOVASCULAR PATIENTS Christina Cortez Perry, MSN, FNP-C, CCCC Cardiology Coordinator- Corpus Christi Medical Center 1 2 LEARNING OBJECTIVES Identify the target patient
PREVENTING HOSPITAL READMISSIONS IN CARDIOVASCULAR PATIENTS Christina Cortez Perry, MSN, FNP-C, CCCC Cardiology Coordinator- Corpus Christi Medical Center 1 2 LEARNING OBJECTIVES Identify the target patient
When Should I Order a Stress Test or an Echocardiogram
 When Should I Order a Stress Test or an Echocardiogram Updates in Cardiology 2015 March 7, 2015 Donald L. Lappé, MD, FAHA, FACC Chairman, Cardiovascular Department Medical Director, Intermountain Cardiovascular
When Should I Order a Stress Test or an Echocardiogram Updates in Cardiology 2015 March 7, 2015 Donald L. Lappé, MD, FAHA, FACC Chairman, Cardiovascular Department Medical Director, Intermountain Cardiovascular
Atrial Fibrillation. Ivan Anderson, MD RIHVH Cardiology
 Atrial Fibrillation Ivan Anderson, MD RIHVH Cardiology Outline Definition and Pathophysiology Rate versus rhythm control Rate control thresholds (how much is enough) Anti-coagulation CHADS2VASc score HASBLED
Atrial Fibrillation Ivan Anderson, MD RIHVH Cardiology Outline Definition and Pathophysiology Rate versus rhythm control Rate control thresholds (how much is enough) Anti-coagulation CHADS2VASc score HASBLED
Quality Payment Program: Cardiology Specialty Measure Set
 Quality Payment Program: Cardiology Specialty Set Title Number CMS Reporting Method(s) Heart Failure (HF): Angiotensin- Converting Enzyme (ACE) Inhibitor or Angiotensin Receptor Blocker (ARB) Therapy for
Quality Payment Program: Cardiology Specialty Set Title Number CMS Reporting Method(s) Heart Failure (HF): Angiotensin- Converting Enzyme (ACE) Inhibitor or Angiotensin Receptor Blocker (ARB) Therapy for
Atrial Fibrillation. A guide for Southwark General Practice. Key Messages. Always work within your knowledge and competency
 Atrial Fibrillation A guide for Southwark General Practice Key Messages 1. Routinely offer pulse checks to patients at high risk of AF 2. Use the CHA 2 DS 2 VASc score to identify patients for anticoagulation
Atrial Fibrillation A guide for Southwark General Practice Key Messages 1. Routinely offer pulse checks to patients at high risk of AF 2. Use the CHA 2 DS 2 VASc score to identify patients for anticoagulation
AWO has worked with the U.S. Coast Guard s National Maritime Center (NMC) to develop at-a-glance guides to the information that must be submitted
 to develop at-a-glance guides to the information that must be submitted") AWO has worked with the U.S. Coast Guard s National Maritime Center (NMC) to develop at-a-glance guides to the information that must be submitted when a mariner has one of several common medical conditions
AWO has worked with the U.S. Coast Guard s National Maritime Center (NMC) to develop at-a-glance guides to the information that must be submitted when a mariner has one of several common medical conditions
Assessing Cardiac Risk in Noncardiac Surgery. Murali Sivarajan, M.D. Professor University of Washington Seattle, Washington
 Assessing Cardiac Risk in Noncardiac Surgery Murali Sivarajan, M.D. Professor University of Washington Seattle, Washington Disclosure None. I have no conflicts of interest, financial or otherwise. CME
Assessing Cardiac Risk in Noncardiac Surgery Murali Sivarajan, M.D. Professor University of Washington Seattle, Washington Disclosure None. I have no conflicts of interest, financial or otherwise. CME
ARIC HEART FAILURE HOSPITAL RECORD ABSTRACTION FORM. General Instructions: ID NUMBER: FORM NAME: H F A DATE: 10/13/2017 VERSION: CONTACT YEAR NUMBER:
 ARIC HEART FAILURE HOSPITAL RECORD ABSTRACTION FORM General Instructions: The Heart Failure Hospital Record Abstraction Form is completed for all heart failure-eligible cohort hospitalizations. Refer to
ARIC HEART FAILURE HOSPITAL RECORD ABSTRACTION FORM General Instructions: The Heart Failure Hospital Record Abstraction Form is completed for all heart failure-eligible cohort hospitalizations. Refer to
Atrial Fibrillation and the NOAC s. John Raymond MS, PA-C, MHP February 10, 2018
 Atrial Fibrillation and the NOAC s John Raymond MS, PA-C, MHP February 10, 2018 Pathogenesis EPIDEMIOLOGY Arrhythmia-related hospitalisations in the US Ventricular fibrillation 2% Atrial fibrillation 34%
Atrial Fibrillation and the NOAC s John Raymond MS, PA-C, MHP February 10, 2018 Pathogenesis EPIDEMIOLOGY Arrhythmia-related hospitalisations in the US Ventricular fibrillation 2% Atrial fibrillation 34%
3/23/2017. Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate Europace Oct;14(10): Epub 2012 Aug 24.
: Epub 2012 Aug 24.") Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Congestive Heart Failure or Heart Failure
 Congestive Heart Failure or Heart Failure Dr Hitesh Patel Ascot Cardiology Group Heart Failure Workshop April, 2014 Question One What is the difference between congestive heart failure and heart failure?
Congestive Heart Failure or Heart Failure Dr Hitesh Patel Ascot Cardiology Group Heart Failure Workshop April, 2014 Question One What is the difference between congestive heart failure and heart failure?
Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017
 Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Specific Basic Standards for Osteopathic Fellowship Training in Cardiology
 Specific Basic Standards for Osteopathic Fellowship Training in Cardiology American Osteopathic Association and American College of Osteopathic Internists BOT 07/2006 Rev. BOT 03/2009 Rev. BOT 07/2011
Specific Basic Standards for Osteopathic Fellowship Training in Cardiology American Osteopathic Association and American College of Osteopathic Internists BOT 07/2006 Rev. BOT 03/2009 Rev. BOT 07/2011
Atrial Fibrillation and Heart Failure: A Cause or a Consequence
 Atrial Fibrillation and Heart Failure: A Cause or a Consequence Rajat Deo, MD, MTR Assistant Professor of Medicine Division of Cardiology, Electrophysiology Section University of Pennsylvania November
Atrial Fibrillation and Heart Failure: A Cause or a Consequence Rajat Deo, MD, MTR Assistant Professor of Medicine Division of Cardiology, Electrophysiology Section University of Pennsylvania November
Cardiac Perioperative Risk Assessment American Heart Association Guidelines
 Cardiac Perioperative Risk Assessment American Heart Association Guidelines Dr Gary Liew, MBBS, PhD, FRACP US Board Certified in Cardiovascular CT Executive Committee, Cardiac Institute, Epworth Healthcare
Cardiac Perioperative Risk Assessment American Heart Association Guidelines Dr Gary Liew, MBBS, PhD, FRACP US Board Certified in Cardiovascular CT Executive Committee, Cardiac Institute, Epworth Healthcare
Course: Exercise and Aging for Special Populations
 Copyright EFS Inc. All Rights Reserved. Course: Exercise and Aging for Special Populations Session 2: Cardiovascular and Metabolic Disease Considerations for Exercise Program Design Presentation Created
Copyright EFS Inc. All Rights Reserved. Course: Exercise and Aging for Special Populations Session 2: Cardiovascular and Metabolic Disease Considerations for Exercise Program Design Presentation Created
THE CARDIOVASCULAR SYSTEM-PART 2
 Hello and welcome back to InterpreterPrep.com THE CARDIOVASCULAR SYSTEM-PART 2 In this second presentation on the CARDIOVASCULAR SYSTEM we're going to be covering diagnostic procedures and treatments used
Hello and welcome back to InterpreterPrep.com THE CARDIOVASCULAR SYSTEM-PART 2 In this second presentation on the CARDIOVASCULAR SYSTEM we're going to be covering diagnostic procedures and treatments used
National Imaging Associates, Inc. Clinical guidelines CARDIAC CATHETERIZATION -LEFT HEART CATHETERIZATION. Original Date: October 2015 Page 1 of 5
 National Imaging Associates, Inc. Clinical guidelines CARDIAC CATHETERIZATION -LEFT HEART CATHETERIZATION CPT Codes: 93451, 93452, 93453, 93454, 93455, 93456, 93457, 93458, 93459, 93460, 93461 LCD ID Number:
National Imaging Associates, Inc. Clinical guidelines CARDIAC CATHETERIZATION -LEFT HEART CATHETERIZATION CPT Codes: 93451, 93452, 93453, 93454, 93455, 93456, 93457, 93458, 93459, 93460, 93461 LCD ID Number:
was admitted to the Cardiology Service at the from Y /M /D to Y / M / D under the care of Dr..
 Patient: was admitted to the Cardiology Service at the from Y /M /D to Y / M / D under the care of Dr.. Discharge Diagnoses include: q CAD-CCS Class: m 0 m 1 m 2 m 3 m 4 q Unstable angina q Non STEMI (non-st
Patient: was admitted to the Cardiology Service at the from Y /M /D to Y / M / D under the care of Dr.. Discharge Diagnoses include: q CAD-CCS Class: m 0 m 1 m 2 m 3 m 4 q Unstable angina q Non STEMI (non-st
National Intervention Council
 National Intervention Council Cardiological Society of India Registry Performa for Coronary, Non- Coronary & Peripheral Interventions Period January 1st 2016 to December 31 st 2016 Dr. (Prof.) N.N. Khanna
National Intervention Council Cardiological Society of India Registry Performa for Coronary, Non- Coronary & Peripheral Interventions Period January 1st 2016 to December 31 st 2016 Dr. (Prof.) N.N. Khanna
New Therapies for the Heart Patient. Wilson They said "There's nothing more that can be done." Robert Federici MD, Presbyterian Heart
 New Therapies for the Heart Patient Wilson 2016 They said "There's nothing more that can be done." Robert Federici MD, Presbyterian Heart Disclosure Boston Scientific Physician Proctor for CTO's, Clinical
New Therapies for the Heart Patient Wilson 2016 They said "There's nothing more that can be done." Robert Federici MD, Presbyterian Heart Disclosure Boston Scientific Physician Proctor for CTO's, Clinical
New PINNACLE Measures The below measures for PINNACLE will be added as new measures to the outcomes reporting starting with Version 2.0.
 New PINNACLE Measures The below measures for PINNACLE will be added as new measures to the outcomes reporting starting with Version 2.0. Measure Steward Measure Name Measure Description Rationale for Adding
New PINNACLE Measures The below measures for PINNACLE will be added as new measures to the outcomes reporting starting with Version 2.0. Measure Steward Measure Name Measure Description Rationale for Adding
Treatment of Hypertrophic Cardiomyopathy in Bruce B. Reid, MD
 Treatment of Hypertrophic Cardiomyopathy in 2017 Bruce B. Reid, MD Disclosures I have no conflicts of interest to disclose I will not be discussing any off label medications and/or devices Objectives 1)
Treatment of Hypertrophic Cardiomyopathy in 2017 Bruce B. Reid, MD Disclosures I have no conflicts of interest to disclose I will not be discussing any off label medications and/or devices Objectives 1)
Individual Therapeutic Selection Of Anti-coagulants And Periprocedural. Miguel Valderrábano, MD
 Individual Therapeutic Selection Of Anti-coagulants And Periprocedural Management Miguel Valderrábano, MD Outline Does the patient need anticoagulation? Review of clinical evidence for each anticoagulant
Individual Therapeutic Selection Of Anti-coagulants And Periprocedural Management Miguel Valderrábano, MD Outline Does the patient need anticoagulation? Review of clinical evidence for each anticoagulant
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Myocardial infarction: secondary prevention in primary and secondary care for patients following a myocardial infarction 1.1
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Myocardial infarction: secondary prevention in primary and secondary care for patients following a myocardial infarction 1.1
Transient Atrial Fibrillation and Risk of Stroke after Acute Myocardial Infarction
 Transient Atrial Fibrillation and Risk of Stroke after Acute Myocardial Infarction Doron Aronson MD, Gregory Telman MD, Fadel BahouthMD, Jonathan Lessick MD, DSc and Rema Bishara MD Department of Cardiology
Transient Atrial Fibrillation and Risk of Stroke after Acute Myocardial Infarction Doron Aronson MD, Gregory Telman MD, Fadel BahouthMD, Jonathan Lessick MD, DSc and Rema Bishara MD Department of Cardiology
What the general cardiologist should know about arrhythmia Stroke prevention in AF" Peter Ammann Kantonsspital St. Gallen
 What the general cardiologist should know about arrhythmia Stroke prevention in AF" Peter Ammann Kantonsspital St. Gallen What the cardiologist should know about arrhythmia and stroke are there real low
What the general cardiologist should know about arrhythmia Stroke prevention in AF" Peter Ammann Kantonsspital St. Gallen What the cardiologist should know about arrhythmia and stroke are there real low
Atrial fibrillation: current approaches to management
 DRUG REVIEW n Atrial fibrillation: current approaches to management Upasana Tayal MA, MRCP and Robert Greenbaum BSc, MD, FRCP, FESC, FACC Atrial fibrillation is the commonest arrhythmia and GPs have an
DRUG REVIEW n Atrial fibrillation: current approaches to management Upasana Tayal MA, MRCP and Robert Greenbaum BSc, MD, FRCP, FESC, FACC Atrial fibrillation is the commonest arrhythmia and GPs have an
HYPERTROPHIC CARDIOMYOPATHY
 HYPERTROPHIC CARDIOMYOPATHY Most often diagnosed during infancy or adolescence, hypertrophic cardiomyopathy (HCM) is the second most common form of heart muscle disease, is usually genetically transmitted,
HYPERTROPHIC CARDIOMYOPATHY Most often diagnosed during infancy or adolescence, hypertrophic cardiomyopathy (HCM) is the second most common form of heart muscle disease, is usually genetically transmitted,
ATRIAL FIBRILLATION: REVISITING CONTROVERSIES IN AN ERA OF INNOVATION
 ATRIAL FIBRILLATION: REVISITING CONTROVERSIES IN AN ERA OF INNOVATION Frederick Schaller, DO, MACOI,FACP Adjunct Clinical Professor Touro University Nevada DISCLOSURES I have no financial relationships
ATRIAL FIBRILLATION: REVISITING CONTROVERSIES IN AN ERA OF INNOVATION Frederick Schaller, DO, MACOI,FACP Adjunct Clinical Professor Touro University Nevada DISCLOSURES I have no financial relationships
Antony French Consultant Cardiologist & Electrophysiologist
 Antony French Consultant Cardiologist & Electrophysiologist Palpitations Unpleasant awareness of rapid or forceful heart beat Not all tachycardias cause palpitations, and not all palpitations are due to
Antony French Consultant Cardiologist & Electrophysiologist Palpitations Unpleasant awareness of rapid or forceful heart beat Not all tachycardias cause palpitations, and not all palpitations are due to
The Management of HOCM: What are the Surgical Options
 The Management of HOCM: What are the Surgical Options Konstadinos A Plestis, MD System Chief of Cardiac Thoracic and Vascular Surgery Main Line Health Care System Professor Sidney Kimmel Medical College
The Management of HOCM: What are the Surgical Options Konstadinos A Plestis, MD System Chief of Cardiac Thoracic and Vascular Surgery Main Line Health Care System Professor Sidney Kimmel Medical College
Cardiology Services Bon Secours Hospital. Mary Buckley Staff Nurse Cardiology
 Cardiology Services Bon Secours Hospital Mary Buckley Staff Nurse Cardiology Overview Philosophy Cardiology Team Referral Criteria Electrocardiograph (ECG) 24/48 Hour Holter Monitor Event Monitors 24 Hour
Cardiology Services Bon Secours Hospital Mary Buckley Staff Nurse Cardiology Overview Philosophy Cardiology Team Referral Criteria Electrocardiograph (ECG) 24/48 Hour Holter Monitor Event Monitors 24 Hour
Preoperative Evaluation: Patients with Cardiac Disease
 Advances in Internal Medicine 2012 Preoperative Evaluation: Patients with Cardiac Disease Mary O. Gray, MD Professor of Medicine UC San Francisco Circulation 2007:100:e418-e500 (1) Cardiac Risk Assessment
Advances in Internal Medicine 2012 Preoperative Evaluation: Patients with Cardiac Disease Mary O. Gray, MD Professor of Medicine UC San Francisco Circulation 2007:100:e418-e500 (1) Cardiac Risk Assessment
HEART AND SOUL STUDY OUTCOME EVENT - MORBIDITY REVIEW FORM
 REVIEW DATE REVIEWER'S ID HEART AND SOUL STUDY OUTCOME EVENT - MORBIDITY REVIEW FORM : DISCHARGE DATE: RECORDS FROM: Hospitalization ER Please check all that may apply: Myocardial Infarction Pages 2, 3,
REVIEW DATE REVIEWER'S ID HEART AND SOUL STUDY OUTCOME EVENT - MORBIDITY REVIEW FORM : DISCHARGE DATE: RECORDS FROM: Hospitalization ER Please check all that may apply: Myocardial Infarction Pages 2, 3,
Ischaemic heart disease. IInd Chair and Clinic of Cardiology
 Ischaemic heart disease IInd Chair and Clinic of Cardiology Definition Syndrome due to chronic insufficient oxygen supply to myocardial cells Nomenclature: ischaemic heart disease (IHD), coronary artery
Ischaemic heart disease IInd Chair and Clinic of Cardiology Definition Syndrome due to chronic insufficient oxygen supply to myocardial cells Nomenclature: ischaemic heart disease (IHD), coronary artery
Severe Hypertension. Pre-referral considerations: 1. BP of arm and Leg 2. Ambulatory BP 3. Renal causes
 Severe Hypertension *Prior to making a referral, call office or Doc Halo, to speak with a Cardiologist or APP to discuss patient and possible treatment options. Please only contact the patient's cardiologist.
Severe Hypertension *Prior to making a referral, call office or Doc Halo, to speak with a Cardiologist or APP to discuss patient and possible treatment options. Please only contact the patient's cardiologist.
Quality Payment Program: Cardiology Specialty Measure Set
 Measure Title * Reportable via PINNACLE α Reportable via Diabetes Collaborative CQMC v1.0 Measure High Priority Measure Cross Cutting Measure Heart Failure (HF): Angiotensin- Converting Enzyme (ACE) Inhibitor
Measure Title * Reportable via PINNACLE α Reportable via Diabetes Collaborative CQMC v1.0 Measure High Priority Measure Cross Cutting Measure Heart Failure (HF): Angiotensin- Converting Enzyme (ACE) Inhibitor
Make you feel better Make you live longer
 Drugs and Devices for Women with Heart Disease Sharonne N. Hayes MD, FACC Director, Women s Heart Clinic Mayo Clinic Rochester, MN CP986192-1 CP1045209-2 Goals of Medical Treatments for Heart Disease Make
Drugs and Devices for Women with Heart Disease Sharonne N. Hayes MD, FACC Director, Women s Heart Clinic Mayo Clinic Rochester, MN CP986192-1 CP1045209-2 Goals of Medical Treatments for Heart Disease Make
MEDICAL POLICY Cardiac Event Monitors/ Cardiac Event Detection
 POLICY: PG0039 ORIGINAL EFFECTIVE: 10/01/11 LAST REVIEW: 12/12/17 MEDICAL POLICY Cardiac Event Monitors/ Cardiac Event Detection GUIDELINES This policy does not certify benefits or authorization of benefits,
POLICY: PG0039 ORIGINAL EFFECTIVE: 10/01/11 LAST REVIEW: 12/12/17 MEDICAL POLICY Cardiac Event Monitors/ Cardiac Event Detection GUIDELINES This policy does not certify benefits or authorization of benefits,
National Coverage Determination (NCD) for Cardiac Pacemakers (20.8)
 for Cardiac Pacemakers (20.8)") Page 1 of 12 Centers for Medicare & Medicaid Services National Coverage Determination (NCD) for Cardiac Pacemakers (20.8) Tracking Information Publication Number 100-3 Manual Section Number 20.8 Manual
Page 1 of 12 Centers for Medicare & Medicaid Services National Coverage Determination (NCD) for Cardiac Pacemakers (20.8) Tracking Information Publication Number 100-3 Manual Section Number 20.8 Manual
Practice-Level Executive Summary Report
 PINNACLE Registry Metrics 0003, Test Practice_NextGen [Rolling: 1st April 2015 to 31st March 2016 ] Generated on 5/11/2016 11:37:35 AM American College of Cardiology Foundation National Cardiovascular
PINNACLE Registry Metrics 0003, Test Practice_NextGen [Rolling: 1st April 2015 to 31st March 2016 ] Generated on 5/11/2016 11:37:35 AM American College of Cardiology Foundation National Cardiovascular
Improving Patient Outcomes with a Syncope Center. Suneet Mittal, MD
 Improving Patient Outcomes with a Syncope Center Suneet Mittal, MD Improving Patient Outcomes with a Syncope Center: Early Risk Stratification of Patients who Require Device Therapy Suneet Mittal, MD Director,
Improving Patient Outcomes with a Syncope Center Suneet Mittal, MD Improving Patient Outcomes with a Syncope Center: Early Risk Stratification of Patients who Require Device Therapy Suneet Mittal, MD Director,
Exercise Test: Practice and Interpretation. Jidong Sung Division of Cardiology Samsung Medical Center Sungkyunkwan University School of Medicine
 Exercise Test: Practice and Interpretation Jidong Sung Division of Cardiology Samsung Medical Center Sungkyunkwan University School of Medicine 2 Aerobic capacity and survival Circulation 117:614, 2008
Exercise Test: Practice and Interpretation Jidong Sung Division of Cardiology Samsung Medical Center Sungkyunkwan University School of Medicine 2 Aerobic capacity and survival Circulation 117:614, 2008
Options for my no option Patients Treating Heart Conditions Via a Tiny Catheter
 Options for my no option Patients Treating Heart Conditions Via a Tiny Catheter Nirat Beohar, MD Associate Professor of Medicine Director Cardiac Catheterization Laboratory, Medical Director Structural
Options for my no option Patients Treating Heart Conditions Via a Tiny Catheter Nirat Beohar, MD Associate Professor of Medicine Director Cardiac Catheterization Laboratory, Medical Director Structural
Don t Forget the Basics
 Scary Arrhythmias in the Hospital Gregory M Marcus, MD, MAS Assistant Professor of Medicine Division of Cardiology University of California, San Francisc Don t Forget the Basics 79 yo man with a history
Scary Arrhythmias in the Hospital Gregory M Marcus, MD, MAS Assistant Professor of Medicine Division of Cardiology University of California, San Francisc Don t Forget the Basics 79 yo man with a history
Apical Hypertrophic Cardiomyopathy With Hemodynamically Unstable Ventricular Arrhythmia Atypical Presentation
 Cronicon OPEN ACCESS Hemant Chaturvedi* Department of Cardiology, Non-Invasive Cardiology, Eternal Heart Care Center & research Institute, Rajasthan, India Received: September 15, 2015; Published: October
Cronicon OPEN ACCESS Hemant Chaturvedi* Department of Cardiology, Non-Invasive Cardiology, Eternal Heart Care Center & research Institute, Rajasthan, India Received: September 15, 2015; Published: October
Dual antiplatelet therapy (DAPT) in the era of Novel Oral Anticoagulants (NOACs) SACIS 2015
 in the era of Novel Oral Anticoagulants (NOACs) SACIS 2015") Dual antiplatelet therapy (DAPT) in the era of Novel Oral Anticoagulants (NOACs) SACIS 2015 Wesam A Alhejily MD FRCPC FACP FACC FSCAI Assistant Professor of Medicine Chief Of Adult Cardiology Consultant
Dual antiplatelet therapy (DAPT) in the era of Novel Oral Anticoagulants (NOACs) SACIS 2015 Wesam A Alhejily MD FRCPC FACP FACC FSCAI Assistant Professor of Medicine Chief Of Adult Cardiology Consultant
Cardiovascular Recommendation Tables
 Cardiovascular Recommendation Tables Current as of: February, 2009 The first publication of the Cardiovascular Recommendation Tables occurred in the October 2002, Cardiovascular Advisory Panel Guidelines
Cardiovascular Recommendation Tables Current as of: February, 2009 The first publication of the Cardiovascular Recommendation Tables occurred in the October 2002, Cardiovascular Advisory Panel Guidelines
4/27/2015. Cardiac Events #1 cause of postoperative complications/ mortality- CHF, complete heart block, MI,
 Not intended for medical clearance Identify, document, and evaluate health conditions Medication Management Stratify Risks Optimize conditions within context of surgical illness Recommend measures that
Not intended for medical clearance Identify, document, and evaluate health conditions Medication Management Stratify Risks Optimize conditions within context of surgical illness Recommend measures that
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acute coronary syndrome(s), anticoagulant therapy in, 706, 707 antiplatelet therapy in, 702 ß-blockers in, 703 cardiac biomarkers in,
Index Note: Page numbers of article titles are in boldface type. A Acute coronary syndrome(s), anticoagulant therapy in, 706, 707 antiplatelet therapy in, 702 ß-blockers in, 703 cardiac biomarkers in,
Cardiac Pathology & Rehabilitation
 Cardiac Pathology & Rehabilitation Which of the following best describes the physical activity performed in my leisure time? A. I perform vigorous physical activity 3X/week for 20 minutes each time B.
Cardiac Pathology & Rehabilitation Which of the following best describes the physical activity performed in my leisure time? A. I perform vigorous physical activity 3X/week for 20 minutes each time B.
Aerobic Exercise Screening Stratification Tool
 Aerobic Screening Stratification Tool Disclaimer: The Aerobics Screening Stratification Tool is a working document currently used within the Stroke Rehabilitation Service of St. Joseph s Care Group- Thunder
Aerobic Screening Stratification Tool Disclaimer: The Aerobics Screening Stratification Tool is a working document currently used within the Stroke Rehabilitation Service of St. Joseph s Care Group- Thunder