Perioperative Cardiovascular Evaluation and Care for Noncardiac. Dr Mahmoud Ebrahimi Interventional cardiologist 91/9/30
|
|
|
- Gabriel Shepherd
- 5 years ago
- Views:
Transcription


1
2 Perioperative Cardiovascular Evaluation and Care for Noncardiac Surgery Dr Mahmoud Ebrahimi Interventional cardiologist 91/9/30
3
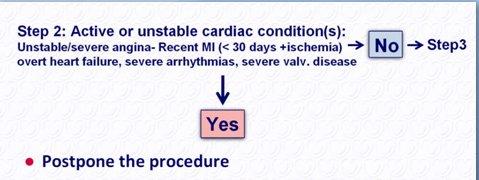
4 Active Cardiac Conditions for Which the Patient Should Undergo Evaluation and Treatment Before Noncardiac Surgery Condition Unstable coronary syndromes Decompensated HF Examples Unstable or severe angina* (CCS class III or IV) Recent MI NYHA functional class IV; Worsening or new-onset HF Significant arrhythmias High-grade atrioventricular block Mobitz II atrioventricular block Third-degree atrioventricular heart block Symptomatic ventricular arrhythmias Supraventricular arrhythmias (including atrial fibrillation) with uncontrolled ventricular rate (HR > 100 bpm at rest) Symptomatic bradycardia Newly recognized ventricular tachycardia Severe valvular disease Severe aortic stenosis (mean pressure gradient greater than 40 mm Hg, aortic valve area less than 1.0 cm2, or symptomatic) Symptomatic mitral stenosis (progressive dyspnea on exertion, exertional presyncope, or HF) May include stable angina in patients who are unusually sedentary. The ACC National Database Library defines recent MI as more than 7 days but within 30 days)
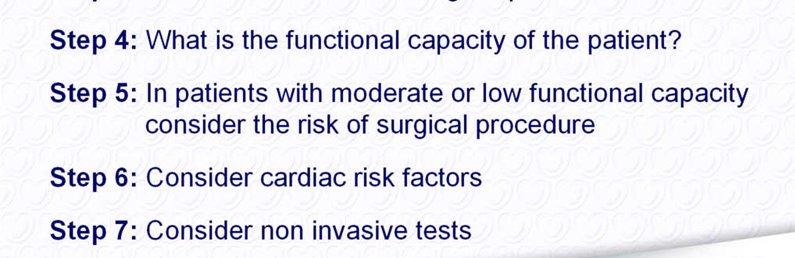
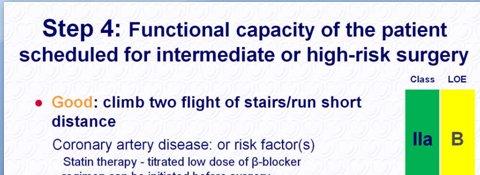
5 Estimated Energy Requirements for Various Activities Can You Can You 1 Met Take care of yourself? 4 Mets Climb a flight of stairs or walk up a hill? Eat, dress, or use the toilet? Walk on level ground at 4 mph (6.4 kph)? Walk indoors around the Do heavy work around the house? house like scrubbing floors or lifting or moving heavy furniture? Walk a block or 2 on level Participate in moderate ground at 2 to 3 mph (3.2 to recreational activities like golf, 4.8 kph)? bowling, dancing, doubles tennis, or throwing a baseball 4 Mets Do light work around the house like dusting or washing dishes? 10 Mets or football? Participate in strenuous sports like swimming, singles tennis, football, basketball, or skiing? MET indicates metabolic equivalent; mph, miles per hour; kph, kilometers per hour. *Modified from Hlatky et al,11 copyright 1989, with permission from Elsevier, and adapted from Fletcher et al.12
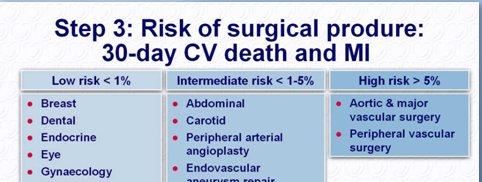
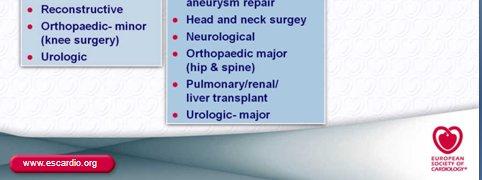
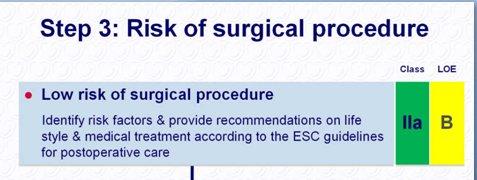
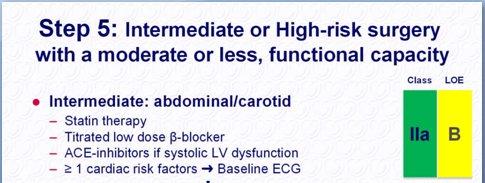
6 Cardiac Risk Stratification for Noncardiac Surgical Procedures Risk Stratification Vascular (reported cardiac risk often > 5%) Procedure Examples Aortic and other major vascular surgery Peripheral vascular surgery Intermediate (reported cardiac risk generally 1%-5%) Low (reported cardiac risk generally <1% Intraperitoneal and intrathoracic surgery Carotid endarterectomy Head and neck surgery Orthopedic surgery Prostate surgery Endoscopic procedures Superficial procedure Cataract surgery Breast surgery Ambulatory surgery
7 Recommendations for Preoperative Noninvasive Evaluation of LV Function Class I (none) Class IIa It is reasonable for patients with dyspnea of unknown origin to undergo preoperative evaluation of LV function. (C) It is reasonable for patients with current or prior HF with worsening dyspnea or other change in clinical status to undergo preoperative evaluation of LV function if not performed within 12 months. (C) Class IIb Reassessment of LV function in clinically stable patients with previously documented cardiomyopathy is not well established. (C) Class III Routine perioperative evaluation of LV function in patients is not recommended. (B)
8 Recommendations for Preoperative Resting 12-Lead ECG Class I: recommended for pts with: At least 1 clinical risk factor* who are undergoing vascular surgical procedures. (B) Known CHD, peripheral arterial disease, or cerebrovascular disease who are undergoing intermediate-risk surgical procedures. (C) Class IIa: reasonable in persons with no clinical risk factors who are undergoing vascular surgical procedures. (B) Class IIb: may be reasonable in patients with at least 1 clinical risk factor who are undergoing intermediate-risk operative procedures. (B) Class III: Preoperative and postoperative resting 12-lead ECGs are not indicated in asymptomatic persons undergoing low-risk surgical procedures. (B) *Clinical risk factors include history of ischemic heart disease, history of compensated or prior HF, history of cerebrovascular disease, DM, and renal insufficiency.

9 Preoperative Coronary Revascularization With CABG or Percutaneous Coronary Intervention in stable cardiac patients
10 Cardiac evaluation and care algorithm for noncardiac surgery
11
12

13
14
15

16
17
18
19

20


21

22
23
24 Proposed approach to the management of patients with previous PCI who require noncardiac surgery
25 Treatment for patients requiring PCI who need subsequent surgery
26 Drug Eluting Stents (DES) and Stent Thrombosis premature discontinuation of dual antiplatelet therapy markedly increases the risk of catastrophic stent thrombosis and death or MI. To eliminate the premature discontinuation of thienopyridine: 1. Before implantation of a stent, In patients not expected to comply with 12 months of thienopyridine therapy, whether for economic or other reasons, or are likely to require invasive or surgical procedures within the next 12 months, consideration should be given to implantation of a baremetal stent or performance of balloon angioplasty with provisional stent implantation instead of the routine use of a DES. Grines CL, et al. Circulation. 2007;115:
27 Drug Eluting Stents (DES) and Stent Thrombosis 3. properly and thoroughly patient education about the reasons they are prescribed thienopyridines and the significant risks associated with prematurely discontinuing such therapy. 4. Patients should be specifically instructed before hospital discharge to contact their treating cardiologist before stopping any antiplatelet therapy, even if instructed to stop such therapy by another healthcare provider. 5. Healthcare providers who perform invasive or surgical procedures and who are concerned about periprocedural and postprocedural bleeding must be made aware of the potentially catastrophic risks of premature discontinuation of thienopyridine therapy. Such professionals who perform these procedures should contact the patient s cardiologist if issues regarding the patient s antiplatelet therapy are unclear, to discuss optimal patient management strategy. Grines CL, et al. Circulation. 2007;115:
28 Drug Eluting Stents (DES) and Stent Thrombosis 6. Elective procedures for which there is significant risk of perioperative or postoperative bleeding should be deferred until patients have completed an appropriate course of thienopyridine therapy (12 months after DES implantation if they are not at high risk of bleeding and a minimum of 1 month for bare-metal stent implantation). 7. For patients treated with DES who are to undergo subsequent procedures that mandate discontinuation of thienopyridine therapy, aspirin should be continued if at all possible and the thienopyridine restarted as soon as possible after the procedure because of concerns about late stent thrombosis. Grines CL, et al. Circulation. 2007;115:
29 Recommendations for Beta-Blocker Medical Therapy CLASS I: Beta blockers should be continued 1. in patients undergoing surgery who are receiving beta blockers to treat angina, symptomatic arrhythmias, hypertension, or other ACC/AHA class I guideline indications. (C) 2. patients undergoing vascular surgery who are at high cardiac risk owing to the finding of ischemia on preoperative testing. (B) CLASS Iia: Beta blockers are probably recommended 1. for patients undergoing vascular surgery in whom preoperative assessment identifies CHD. (B) 2. for patients in whom preoperative assessment for vascular surgery identifies high cardiac risk, as defined by the presence of more than 1 clinical risk factor.* (B) 3. for patients in whom preoperative assessment identifies CHD or high cardiac risk, as defined by the presence of more than 1 clinical risk factor,* who are undergoing intermediate-risk or vascular surgery. (B)
30 Recommendations for Beta-Blocker Medical Therapy CLASS IIb: The usefulness of BB is uncertain 1. In intermediate-risk procedures or vascular surgery, in whom preoperative assessment identifies a single clinical risk factor.* (C) 2. In vascular surgery with no clinical risk factors who are not currently taking beta blockers. (B) CLASS III 1. Beta blockers should not be given to patients undergoing surgery who have absolute contraindications to beta blockade. (C)
31 Recommendations for Perioperative Beta-Blocker Therapy
32 Recommendations for Statin Therapy CLASS I 1. For patients currently taking statins and scheduled for noncardiac surgery, statins should be continued. (B) CLASS IIa 1. For patients undergoing vascular surgery with or without clinical risk factors, statin use is reasonable. (B) CLASS IIb 1. For patients with at least 1 clinical risk factor who are undergoing intermediate-risk procedures, statins may be considered. (C)
33 Intraoperative and Postoperative Use CLASS IIa of ST-Segment Monitoring can be useful to monitor patients with known CAD or those undergoing vascular surgery, to detect myocardial ischemia during the perioperative period. (B) CLASS IIb may be considered in patients with single or multiple risk factors for CAD who are undergoing noncardiac surgery.(b)
34 CLASS I: troponin measurement for Perioperative MI in patients with ECG changes or chest pain typical of acute coronary syndrome.(c) CLASS IIb:is not well established in patients who are clinically stable and have undergone vascular and intermediate-risk surgery. (C) CLASS III: in asymptomatic stable patients who have undergone low-risk surgery.(c)
35 1. You are asked to evaluate a 55-year-old man with a history of prior myocardial infarction in preparation for an abdominal aortic aneurysm repair. A dobutamine stress echocardiogram has been ordered and shows the following.
36 A 70-year-old man with hypertension and a recently diagnosed solitary pulmonary nodule is scheduled for wedge resection. He is otherwise healthy, active, and regularly plays golf. His ECG reveals left ventricular hypertrophy with secondary repolarization changes consistent with a strain pattern. Your recommendation is a. Stress echocardiography for risk stratification. b. Clear the patient for surgery. c. Coronary angiography. d. Echocardiogram. e. Stress SPECT thallium imaging.
37 An 80-year-old woman with hypertension and a history of congestive heart failure recently suffered a hip fracture and is in need of stabilization. She lives with family but is known to be inactive, primarily because of arthritis. Your recommendation is to do the following: a. Clear the patient for the orthopedic procedure with beta-blocker prophylaxis and careful hemodynamic monitoring. b. Coronary angiography. c. Dobutamine stress echocardiography for risk stratification. d. Echocardiogram, and if left ventricular function is normal, clear the patient for surgery. e. Exercise stress SPECT thallium.
38 A 78-year-old woman with a history of chronic stable angina is scheduled for cataract surgery. Your recommendation is a. Dipyridamole stress SPECT thallium imaging. b. Coronary angiography. c. Clear the patient for cataract surgery. d. Echocardiogram, and if left ventricular function is normal, clear the patient for surgery. e. Exercise stress echocardiography
39 Your patient is a 55-year-old man who is in need of a fem-pop bypass for claudication. What do you recommend for risk stratification? a. Exercise ECG b. Angiography c. Dobutamine stress echocardiography d. Dipyridamole thallium e. Clinical evaluation



40 With best wishes
Perioperative Cardiology Consultations for Noncardiac Surgery Ischemic Heart Disease
 2012 대한춘계심장학회 Perioperative Cardiology Consultations for Noncardiac Surgery Ischemic Heart Disease 울산의대울산대학병원심장내과이상곤 ECG CLASS IIb 1. Preoperative resting 12-lead ECG may be reasonable in patients with
2012 대한춘계심장학회 Perioperative Cardiology Consultations for Noncardiac Surgery Ischemic Heart Disease 울산의대울산대학병원심장내과이상곤 ECG CLASS IIb 1. Preoperative resting 12-lead ECG may be reasonable in patients with
Perioperative Cardiac Management. Emma Sargsyan, MD, FACP
 Perioperative Cardiac Management Emma Sargsyan, MD, FACP March 22-24, 2018 Outline Evaluation of cardiac risk prior to non-cardiac surgery Management of cardiac risk for non-cardiac surgery 2 Preop medical
Perioperative Cardiac Management Emma Sargsyan, MD, FACP March 22-24, 2018 Outline Evaluation of cardiac risk prior to non-cardiac surgery Management of cardiac risk for non-cardiac surgery 2 Preop medical
Cardiac evaluation for the noncardiac. Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology
 Cardiac evaluation for the noncardiac patient Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology Objectives! Review ACC / AHA guidelines as updated for 2009! Discuss new recommendations
Cardiac evaluation for the noncardiac patient Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology Objectives! Review ACC / AHA guidelines as updated for 2009! Discuss new recommendations
Evaluation and Management of the Patient with Cardiac Disease for Non-Cardiac Surgery WINTER CONFRENCE 2016 RONY GORGES, MD
 Evaluation and Management of the Patient with Cardiac Disease for Non-Cardiac Surgery WINTER CONFRENCE 2016 RONY GORGES, MD 67 yo man Asymptomatic carotid stenosis, CEA planned Golfs regularly, walks and
Evaluation and Management of the Patient with Cardiac Disease for Non-Cardiac Surgery WINTER CONFRENCE 2016 RONY GORGES, MD 67 yo man Asymptomatic carotid stenosis, CEA planned Golfs regularly, walks and
Pre-Operative Services Teaching Rounds 3 Jan 2011
 Pre-Operative Services Teaching Rounds 3 Jan 2011 Deborah Richman MBChB FFA(SA) Director Pre-Operative Services Department of Anesthesia Stony Brook University Medical Center, NY drichman@notes.cc.sunysb.edu
Pre-Operative Services Teaching Rounds 3 Jan 2011 Deborah Richman MBChB FFA(SA) Director Pre-Operative Services Department of Anesthesia Stony Brook University Medical Center, NY drichman@notes.cc.sunysb.edu
Perioperative myocardial infarction is a major cause of morbidity and mortality in patients who
 Focused Issue of This Month Anesthesia for Noncardiac Surgery in the Patients with Cardiac Disease Kyung Yeon Yoo, MD Department of Anesthesiology and Pain Medicine, Chonnam National University College
Focused Issue of This Month Anesthesia for Noncardiac Surgery in the Patients with Cardiac Disease Kyung Yeon Yoo, MD Department of Anesthesiology and Pain Medicine, Chonnam National University College
Assessing Cardiac Risk in Noncardiac Surgery. Murali Sivarajan, M.D. Professor University of Washington Seattle, Washington
 Assessing Cardiac Risk in Noncardiac Surgery Murali Sivarajan, M.D. Professor University of Washington Seattle, Washington Disclosure None. I have no conflicts of interest, financial or otherwise. CME
Assessing Cardiac Risk in Noncardiac Surgery Murali Sivarajan, M.D. Professor University of Washington Seattle, Washington Disclosure None. I have no conflicts of interest, financial or otherwise. CME
Preoperative Evaluation Guidelines and Work up
 Preoperative Evaluation Guidelines and Work up Wesley Fiser, MD Disclosures: None 1 Case An 80 year old woman with osteoarthritis of the hip, DM, CKD (Cr 2.1), and HTN is diagnosed with an obstructing
Preoperative Evaluation Guidelines and Work up Wesley Fiser, MD Disclosures: None 1 Case An 80 year old woman with osteoarthritis of the hip, DM, CKD (Cr 2.1), and HTN is diagnosed with an obstructing
Preoperative Risk. Geoffrey C Zarrella DO FACC. Assessment
 Preoperative Risk Geoffrey C Zarrella DO FACC Assessment your late add ons keep calm use your tools stick to your guns PURPOSE OF THE PREOP EVAL ASSESS PERIOP RISK CAN INFORM DECISION TO PROCEED OR
Preoperative Risk Geoffrey C Zarrella DO FACC Assessment your late add ons keep calm use your tools stick to your guns PURPOSE OF THE PREOP EVAL ASSESS PERIOP RISK CAN INFORM DECISION TO PROCEED OR
Preoperative Cardiac Risk Assessment: Approach & Guidelines
 Preoperative Cardiac Risk Assessment: Approach & Guidelines By, Liam Morris, MD., FACC (02/03/18) CPG : Clinical Practice Guidelines GDMT : Guidelines Directed Medical Therapy GWC : Guideline Writing Committee
Preoperative Cardiac Risk Assessment: Approach & Guidelines By, Liam Morris, MD., FACC (02/03/18) CPG : Clinical Practice Guidelines GDMT : Guidelines Directed Medical Therapy GWC : Guideline Writing Committee
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014
 Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
ACC/AHA Guideline. Downloaded from by on September 30, 2018
 ACC/AHA Guideline ACC/AHA 2007 Guidelines on Perioperative Cardiovascular Evaluation and Care for Noncardiac Surgery: Executive Summary A Report of the American College of Cardiology/American Heart Association
ACC/AHA Guideline ACC/AHA 2007 Guidelines on Perioperative Cardiovascular Evaluation and Care for Noncardiac Surgery: Executive Summary A Report of the American College of Cardiology/American Heart Association
8/28/2018. Pre-op Evaluation for non cardiac surgery. A quick review from 2007!! Disclosures. John Steuter, MD. None
 Pre-op Evaluation for non cardiac surgery John Steuter, MD Disclosures None A quick review from 2007!! Fliesheret al, ACC/AHA 2007 Guidelines on Perioperative Cardiovascular Evaluation and are for Noncardiac
Pre-op Evaluation for non cardiac surgery John Steuter, MD Disclosures None A quick review from 2007!! Fliesheret al, ACC/AHA 2007 Guidelines on Perioperative Cardiovascular Evaluation and are for Noncardiac
Timing of Surgery After Percutaneous Coronary Intervention
 Timing of Surgery After Percutaneous Coronary Intervention Deepak Talreja, MD, FACC Bayview/EVMS/Sentara Outline/Highlights Timing of elective surgery What to do with medications Stopping anti-platelet
Timing of Surgery After Percutaneous Coronary Intervention Deepak Talreja, MD, FACC Bayview/EVMS/Sentara Outline/Highlights Timing of elective surgery What to do with medications Stopping anti-platelet
Agenda. Disclosures. Surgical Mortality: What is High Risk?
 Pre-Operative Cardiac Evaluation of the Vascular Patient: Updated AHA/ACC Guidelines Choosing Wisely UCSF Vascular Symposium 2015 Joshua A. Beckman, M.D., M.S. Brigham and Women s Hospital Consulting Merck
Pre-Operative Cardiac Evaluation of the Vascular Patient: Updated AHA/ACC Guidelines Choosing Wisely UCSF Vascular Symposium 2015 Joshua A. Beckman, M.D., M.S. Brigham and Women s Hospital Consulting Merck
Agenda. Perioperative Cardiac Risk Stratification circa Surgical Mortality: What is High Risk? Presenter Disclosure Information
 9:45 1:45 am Perioperative Evaluation and Management of the Cardiac Patient in Noncardiac Surgery SPEAKER Joshua A. Beckman, MD, MS Presenter Disclosure Information The following relationships exist related
9:45 1:45 am Perioperative Evaluation and Management of the Cardiac Patient in Noncardiac Surgery SPEAKER Joshua A. Beckman, MD, MS Presenter Disclosure Information The following relationships exist related
Pre-op Risk Assessment. Hal Blanks MD FACC
 Pre-op Risk Assessment Hal Blanks MD FACC Objectives: Identify and manage patients with known or suspected CAD and other cardiac diseases who are at risk of cardiac complications during noncardiac surgery.
Pre-op Risk Assessment Hal Blanks MD FACC Objectives: Identify and manage patients with known or suspected CAD and other cardiac diseases who are at risk of cardiac complications during noncardiac surgery.
PERIOPERATIVE CARDIAC RISK ASSESSMENT. Divya Gollapudi, MD
 PERIOPERATIVE CARDIAC RISK ASSESSMENT Divya Gollapudi, MD Clinical Assistant Professor Hospital Medicine Program Division of General Internal Medicine Harborview Medical Center None Disclosures Objectives
PERIOPERATIVE CARDIAC RISK ASSESSMENT Divya Gollapudi, MD Clinical Assistant Professor Hospital Medicine Program Division of General Internal Medicine Harborview Medical Center None Disclosures Objectives
John B. Hill D.O. Department of Anesthesiology NORMAN ANESTHESIA PROVIDERS 03/05/2013
 Pre-op Assessment by Primary Providers What we really want to know John B. Hill D.O. Department of Anesthesiology NORMAN ANESTHESIA PROVIDERS 03/05/2013 Outline Discuss anesthesia specific risk Discuss
Pre-op Assessment by Primary Providers What we really want to know John B. Hill D.O. Department of Anesthesiology NORMAN ANESTHESIA PROVIDERS 03/05/2013 Outline Discuss anesthesia specific risk Discuss
Guidelines PATHOLOGY: FATAL PERIOPERATIVE MI NON-PMI N = 25 PMI N = 42. Prominent Dutch Cardiovascular Researcher Fired for Scientific Misconduct
 PATHOLOGY: FATAL PERIOPERATIVE MI NON-PMI N = 25 PMI N = 42 Preoperative, Intraoperative, and Postoperative Factors Associated with Perioperative Cardiac Complications in Patients Undergoing Major Noncardiac
PATHOLOGY: FATAL PERIOPERATIVE MI NON-PMI N = 25 PMI N = 42 Preoperative, Intraoperative, and Postoperative Factors Associated with Perioperative Cardiac Complications in Patients Undergoing Major Noncardiac
Perioperative Decision Making The decision has been made to proceed with operative management timing and site of surgery the type of anesthesia preope
 Preoperative Evaluation In Endocrine Disorders Dr Nahid Zirak 2012 Perioperative Decision Making The decision has been made to proceed with operative management timing and site of surgery the type of anesthesia
Preoperative Evaluation In Endocrine Disorders Dr Nahid Zirak 2012 Perioperative Decision Making The decision has been made to proceed with operative management timing and site of surgery the type of anesthesia
My Patient Needs a Stress Test
 My Patient Needs a Stress Test Amy S. Burhanna,, MD, FACC Coastal Cardiology Cape May Court House, New Jersey Absolute and relative contraindications to exercise testing Absolute Acute myocardial infarction
My Patient Needs a Stress Test Amy S. Burhanna,, MD, FACC Coastal Cardiology Cape May Court House, New Jersey Absolute and relative contraindications to exercise testing Absolute Acute myocardial infarction
AAA CAG CAG. ACC / AHA Guidelines for Perioperative Cardiovascular Evaluation for Noncardiac. Group Group AAA AAA.
 13 591 596 2004 AAA CAG CAG 5527 15 CAG ACC / AHA Guidelines for Perioperative Cardiovascular Evaluation for Noncardiac Surgery CAG 55 34 62CAG 75 CAG 73 63 66 ACC / AHA CAGGroup 1 9 8 Group 225 22 Group
13 591 596 2004 AAA CAG CAG 5527 15 CAG ACC / AHA Guidelines for Perioperative Cardiovascular Evaluation for Noncardiac Surgery CAG 55 34 62CAG 75 CAG 73 63 66 ACC / AHA CAGGroup 1 9 8 Group 225 22 Group
2010, Metzler Helfried
 Perioperative Strategies in Patients on Dual Antiplatelet Drug Therapy: Noncardiac Surgery H. Metzler Department of Anaesthesiology and Intensive Care Medicine Medical University of Graz, Austria What
Perioperative Strategies in Patients on Dual Antiplatelet Drug Therapy: Noncardiac Surgery H. Metzler Department of Anaesthesiology and Intensive Care Medicine Medical University of Graz, Austria What
COMPARISON OF 2014 ACCAHA VS. ESC GUIDELINES EDITORIAL
 COMPARISON OF 2014 ACCAHA VS. ESC GUIDELINES EDITORIAL Guidelines in review: Comparison of the 2014 ACC/AHA guidelines on perioperative cardiovascular evaluation and management of patients undergoing noncardiac
COMPARISON OF 2014 ACCAHA VS. ESC GUIDELINES EDITORIAL Guidelines in review: Comparison of the 2014 ACC/AHA guidelines on perioperative cardiovascular evaluation and management of patients undergoing noncardiac
SESSION 5 2:20 3:35 pm
 SESSION 2:2 3:3 pm Strategies to Reduce Cardiac Risk for Noncardiac Surgery SPEAKER Lee A. Fleisher, MD Presenter Disclosure Information The following relationships exist related to this presentation:
SESSION 2:2 3:3 pm Strategies to Reduce Cardiac Risk for Noncardiac Surgery SPEAKER Lee A. Fleisher, MD Presenter Disclosure Information The following relationships exist related to this presentation:
Beta Blockade: Protection or Panacea
 Beta Blockade: Protection or Panacea Jason Axt Jason s Recommendations Perioperative β Blockade (BB) If on BB stay on If Vascular Sx + documented ischemia - start. 2+ risk factors - start Use in isolated
Beta Blockade: Protection or Panacea Jason Axt Jason s Recommendations Perioperative β Blockade (BB) If on BB stay on If Vascular Sx + documented ischemia - start. 2+ risk factors - start Use in isolated
Anesthesia for Cardiac Patients for Non Cardiac Surgery. Kimberly Westra DNP, MSN, CRNA
 Anesthesia for Cardiac Patients for Non Cardiac Surgery Kimberly Westra DNP, MSN, CRNA Anesthesia for Cardiac Patients for Non Cardiac Surgery Heart Disease is a significant problem in the United States:
Anesthesia for Cardiac Patients for Non Cardiac Surgery Kimberly Westra DNP, MSN, CRNA Anesthesia for Cardiac Patients for Non Cardiac Surgery Heart Disease is a significant problem in the United States:
Controversies in Perioperative Medicine
 Controversies in Perioperative Medicine Staying Abreast & Ahead of the Guidelines Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Controversies in Perioperative
Controversies in Perioperative Medicine Staying Abreast & Ahead of the Guidelines Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Controversies in Perioperative
I have no disclosures
 Preparing patients for out of hospital anesthesia BobbieJean Sweitzer, M.D. Director, Anesthesia Perioperative Medicine Clinic Professor of Anesthesia and Critical Care Professor of Medicine University
Preparing patients for out of hospital anesthesia BobbieJean Sweitzer, M.D. Director, Anesthesia Perioperative Medicine Clinic Professor of Anesthesia and Critical Care Professor of Medicine University
Quality Measures MIPS CV Specific
 Quality Measures MIPS CV Specific MEASURE NAME Atrial Fibrillation and Atrial Flutter: Chronic Anticoagulation Therapy CAHPS for MIPS Clinician/Group Survey Cardiac Rehabilitation Patient Referral from
Quality Measures MIPS CV Specific MEASURE NAME Atrial Fibrillation and Atrial Flutter: Chronic Anticoagulation Therapy CAHPS for MIPS Clinician/Group Survey Cardiac Rehabilitation Patient Referral from
Perioperative Medical Therapy: Beta Blockers, Statins, ACE-Inhibitors, ARB Effects on Mortality
 Perioperative Medical Therapy: Beta Blockers, Statins, ACE-Inhibitors, ARB Effects on Mortality Art Wallace, MD, PhD SF VAMC Chief of Anethesia and Vice Chair of Anesthesia and Perioperative Care UCSF
Perioperative Medical Therapy: Beta Blockers, Statins, ACE-Inhibitors, ARB Effects on Mortality Art Wallace, MD, PhD SF VAMC Chief of Anethesia and Vice Chair of Anesthesia and Perioperative Care UCSF
Update on Perioperative Medicine. Update on Perioperative Medicine. Question 1: Clinical Risk Prediction. for the Office-based Practitioner
 Update on Perioperative Medicine Update on Perioperative Medicine for the Office-based Practitioner Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Predicting
Update on Perioperative Medicine Update on Perioperative Medicine for the Office-based Practitioner Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Predicting
7. Echocardiography Appropriate Use Criteria (by Indication)
") Criteria for Echocardiography 1133 7. Echocardiography Criteria (by ) Table 1. TTE for General Evaluation of Cardiac Structure and Function Suspected Cardiac Etiology General With TTE 1. Symptoms or conditions
Criteria for Echocardiography 1133 7. Echocardiography Criteria (by ) Table 1. TTE for General Evaluation of Cardiac Structure and Function Suspected Cardiac Etiology General With TTE 1. Symptoms or conditions
Objectives. Old School. Preoperative Evaluation and Postoperative Complications: Where are the opportunities for risk reduction?
 Preoperative Evaluation and Postoperative Complications: Where are the opportunities for risk reduction? Jeffrey Carter, MD RMHMS October 5, 2010 Objectives Understand the preoperative cardiac evaluation
Preoperative Evaluation and Postoperative Complications: Where are the opportunities for risk reduction? Jeffrey Carter, MD RMHMS October 5, 2010 Objectives Understand the preoperative cardiac evaluation
Conflicts of Interest. Evaluation of Cardiac and Pulmonary Risk in the Preop Patient. Introduction. Risk Assessment. Risk Assessment: RCRI
 Evaluation of Cardiac and Pulmonary Risk in the Preop Patient Conflicts of Interest I have no conflicts of interest to declare Adam Schaffer, MD Brigham and Women s Hospital July 20, 2012 Introduction
Evaluation of Cardiac and Pulmonary Risk in the Preop Patient Conflicts of Interest I have no conflicts of interest to declare Adam Schaffer, MD Brigham and Women s Hospital July 20, 2012 Introduction
Preoperative Evaluation of Patients Undergoing Noncardiac Surgery
 Preoperative Evaluation of Patients Undergoing Noncardiac Surgery Shazia Khan, MD Assistant Professor of Clinical Medicine Keck School of Medicine LAC+USC Medical Center Learning Objectives Use a risk
Preoperative Evaluation of Patients Undergoing Noncardiac Surgery Shazia Khan, MD Assistant Professor of Clinical Medicine Keck School of Medicine LAC+USC Medical Center Learning Objectives Use a risk
ASE 2011 Appropriate Use Criteria for Echocardiography
 ASE 2011 Appropriate Use Criteria for Echocardiography Table 1. TTE for General Evaluation of Cardiac Structure and Function 1 2 Suspected Cardiac Etiology General With TTE Symptoms or conditions potentially
ASE 2011 Appropriate Use Criteria for Echocardiography Table 1. TTE for General Evaluation of Cardiac Structure and Function 1 2 Suspected Cardiac Etiology General With TTE Symptoms or conditions potentially
2018 David Stultz. The Consultant s Job
 The Consultant s Job Cardiac Pre-Operative Evaluation ACC 2014 Guidelines David Stultz, MD September 8, 2017 www.drstultz.com KPN Heart & Vascular Objectives of Conference Understand Cardiac Clearance
The Consultant s Job Cardiac Pre-Operative Evaluation ACC 2014 Guidelines David Stultz, MD September 8, 2017 www.drstultz.com KPN Heart & Vascular Objectives of Conference Understand Cardiac Clearance
Preoperative Evaluation: Patients with Cardiac Disease
 Advances in Internal Medicine 2012 Preoperative Evaluation: Patients with Cardiac Disease Mary O. Gray, MD Professor of Medicine UC San Francisco Circulation 2007:100:e418-e500 (1) Cardiac Risk Assessment
Advances in Internal Medicine 2012 Preoperative Evaluation: Patients with Cardiac Disease Mary O. Gray, MD Professor of Medicine UC San Francisco Circulation 2007:100:e418-e500 (1) Cardiac Risk Assessment
Cardiovascular Disorders Lecture 3 Coronar Artery Diseases
 Cardiovascular Disorders Lecture 3 Coronar Artery Diseases By Prof. El Sayed Abdel Fattah Eid Lecturer of Internal Medicine Delta University Coronary Heart Diseases It is the leading cause of death in
Cardiovascular Disorders Lecture 3 Coronar Artery Diseases By Prof. El Sayed Abdel Fattah Eid Lecturer of Internal Medicine Delta University Coronary Heart Diseases It is the leading cause of death in
Exercise Test: Practice and Interpretation. Jidong Sung Division of Cardiology Samsung Medical Center Sungkyunkwan University School of Medicine
 Exercise Test: Practice and Interpretation Jidong Sung Division of Cardiology Samsung Medical Center Sungkyunkwan University School of Medicine 2 Aerobic capacity and survival Circulation 117:614, 2008
Exercise Test: Practice and Interpretation Jidong Sung Division of Cardiology Samsung Medical Center Sungkyunkwan University School of Medicine 2 Aerobic capacity and survival Circulation 117:614, 2008
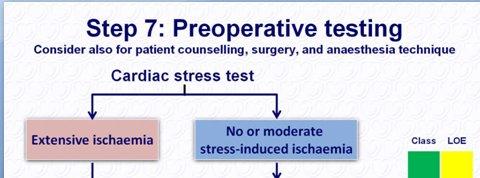
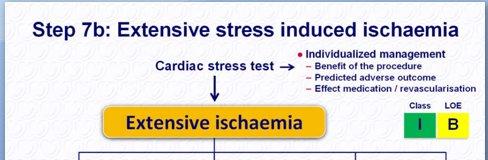
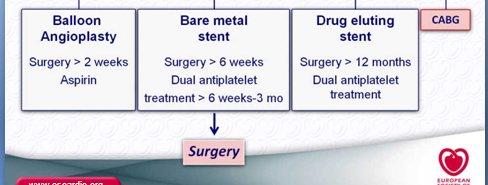
Preoperative cardiac management of the patient for non-cardiac surgery: an individualized and evidence-based approach
 British Journal of Anaesthesia 107 (1): 83 96 (2011) Advance Access publication 24 May 2011. doi:10.1093/bja/aer121 Preoperative cardiac management of the patient for non-cardiac surgery: an individualized
British Journal of Anaesthesia 107 (1): 83 96 (2011) Advance Access publication 24 May 2011. doi:10.1093/bja/aer121 Preoperative cardiac management of the patient for non-cardiac surgery: an individualized
Choosing the Appropriate Stress Test: Brett C. Stoll, MD, FACC February 24, 2018
 Choosing the Appropriate Stress Test: Brett C. Stoll, MD, FACC February 24, 2018 Choosing the Appropriate Stress Test: Does it Really Matter? Brett C. Stoll, MD, FACC February 24, 2018 Conflicts of Interest
Choosing the Appropriate Stress Test: Brett C. Stoll, MD, FACC February 24, 2018 Choosing the Appropriate Stress Test: Does it Really Matter? Brett C. Stoll, MD, FACC February 24, 2018 Conflicts of Interest
Perioperative Medicine 2016 Some Answers, Even More Questions
 Learning Objectives Perioperative Medicine 2016 Some Answers, Even More Questions Kurt Pfeifer, MD, FACP, FHM Professor of Medicine Medical College of Wisconsin Outline changes to the ACC/AHA perioperative
Learning Objectives Perioperative Medicine 2016 Some Answers, Even More Questions Kurt Pfeifer, MD, FACP, FHM Professor of Medicine Medical College of Wisconsin Outline changes to the ACC/AHA perioperative
Preoperative Management. Presley Regional Trauma Center Department of Surgery University of Tennessee Health Science Center Memphis, Tennessee
 Preoperative Management Presley Regional Trauma Center Department of Surgery University of Tennessee Health Science Center Memphis, Tennessee Perioperative Care Consideration Medical care provided to prepare
Preoperative Management Presley Regional Trauma Center Department of Surgery University of Tennessee Health Science Center Memphis, Tennessee Perioperative Care Consideration Medical care provided to prepare
Coronary Artery Disease: Revascularization (Teacher s Guide)
") Stephanie Chan, M.D. Updated 3/15/13 2008-2013, SCVMC (40 minutes) I. Objectives Coronary Artery Disease: Revascularization (Teacher s Guide) To review the evidence on whether percutaneous coronary intervention
Stephanie Chan, M.D. Updated 3/15/13 2008-2013, SCVMC (40 minutes) I. Objectives Coronary Artery Disease: Revascularization (Teacher s Guide) To review the evidence on whether percutaneous coronary intervention
Clinical Controversies in Perioperative Medicine
 Clinical Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Predicting & Managing Cardiac Risk A 70-y.o. man with progressive
Clinical Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Predicting & Managing Cardiac Risk A 70-y.o. man with progressive
4/27/2015. Cardiac Events #1 cause of postoperative complications/ mortality- CHF, complete heart block, MI,
 Not intended for medical clearance Identify, document, and evaluate health conditions Medication Management Stratify Risks Optimize conditions within context of surgical illness Recommend measures that
Not intended for medical clearance Identify, document, and evaluate health conditions Medication Management Stratify Risks Optimize conditions within context of surgical illness Recommend measures that
Severe Hypertension. Pre-referral considerations: 1. BP of arm and Leg 2. Ambulatory BP 3. Renal causes
 Severe Hypertension *Prior to making a referral, call office or Doc Halo, to speak with a Cardiologist or APP to discuss patient and possible treatment options. Please only contact the patient's cardiologist.
Severe Hypertension *Prior to making a referral, call office or Doc Halo, to speak with a Cardiologist or APP to discuss patient and possible treatment options. Please only contact the patient's cardiologist.
Perioperative Medicine 2017 November 3, Disclosures
 Perioperative Medicine 2017 November 3, 2017 Scott Marsal, MD MSc FACP Chief, Medicine Division Medical Director, Quality & Patient Safety Providence St. Vincent Medical Center Disclosures No conflicts
Perioperative Medicine 2017 November 3, 2017 Scott Marsal, MD MSc FACP Chief, Medicine Division Medical Director, Quality & Patient Safety Providence St. Vincent Medical Center Disclosures No conflicts
Imaging ischemic heart disease: role of SPECT and PET. Focus on Patients with Known CAD
 Imaging ischemic heart disease: role of SPECT and PET. Focus on Patients with Known CAD Hein J. Verberne Academic Medical Center, University of Amsterdam, Amsterdam, Netherlands International Conference
Imaging ischemic heart disease: role of SPECT and PET. Focus on Patients with Known CAD Hein J. Verberne Academic Medical Center, University of Amsterdam, Amsterdam, Netherlands International Conference
Update in Perioperative Medicine
 Update in Perioperative Medicine Linda Venner MD FACP March 2018 Agenda 1 2 3 4 5 Optimized not Cleared Identify red flags for cardiac and pulmonary complications Optimize management Prevent delirium Don
Update in Perioperative Medicine Linda Venner MD FACP March 2018 Agenda 1 2 3 4 5 Optimized not Cleared Identify red flags for cardiac and pulmonary complications Optimize management Prevent delirium Don
Clinical Controversies in Perioperative Medicine
 Clinical Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Cardiac Evaluation: New Guidelines A 70-y.o. man with progressive
Clinical Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Cardiac Evaluation: New Guidelines A 70-y.o. man with progressive
Cardiovascular nuclear imaging employs non-invasive techniques to assess alterations in coronary artery flow, and ventricular function.
 National Imaging Associates, Inc. Clinical guidelines CARDIOVASCULAR NUCLEAR MEDICINE -MYOCARDIAL PERFUSION IMAGING -MUGA CPT4 Codes: Refer to pages 6-9 LCD ID Number: L33960 J 15 = KY, OH Responsible
National Imaging Associates, Inc. Clinical guidelines CARDIOVASCULAR NUCLEAR MEDICINE -MYOCARDIAL PERFUSION IMAGING -MUGA CPT4 Codes: Refer to pages 6-9 LCD ID Number: L33960 J 15 = KY, OH Responsible
Quality Payment Program: Cardiology Specialty Measure Set
 Quality Payment Program: Cardiology Specialty Set Title Number CMS Reporting Method(s) Heart Failure (HF): Angiotensin- Converting Enzyme (ACE) Inhibitor or Angiotensin Receptor Blocker (ARB) Therapy for
Quality Payment Program: Cardiology Specialty Set Title Number CMS Reporting Method(s) Heart Failure (HF): Angiotensin- Converting Enzyme (ACE) Inhibitor or Angiotensin Receptor Blocker (ARB) Therapy for
Acute Coronary Syndrome. Sonny Achtchi, DO
 Acute Coronary Syndrome Sonny Achtchi, DO Objectives Understand evidence based and practice based treatments for stabilization and initial management of ACS Become familiar with ACS risk stratification
Acute Coronary Syndrome Sonny Achtchi, DO Objectives Understand evidence based and practice based treatments for stabilization and initial management of ACS Become familiar with ACS risk stratification
CHAPTER 70 PREOPERATIVE EVALUATION OF THE HIGH-RISK SURGICAL PATIENT
 CHAPTER 70 PREOPERATIVE EVALUATION OF THE HIGH-RISK SURGICAL PATIENT BHIKEN I. NAIK DEANE MURFIN LISA THANNIKARY OVERVIEW The perioperative mortality rate for elective surgical procedures is low, ranging
CHAPTER 70 PREOPERATIVE EVALUATION OF THE HIGH-RISK SURGICAL PATIENT BHIKEN I. NAIK DEANE MURFIN LISA THANNIKARY OVERVIEW The perioperative mortality rate for elective surgical procedures is low, ranging
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know
 Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
Acute Coronary syndrome
 Acute Coronary syndrome 7th Annual Pharmacotherapy Conference ACS Pathophysiology rupture or erosion of a vulnerable, lipidladen, atherosclerotic coronary plaque, resulting in exposure of circulating blood
Acute Coronary syndrome 7th Annual Pharmacotherapy Conference ACS Pathophysiology rupture or erosion of a vulnerable, lipidladen, atherosclerotic coronary plaque, resulting in exposure of circulating blood
Perioperative Cardiovascular Evaluation and Care for Noncardiac Surgery
 Perioperative Cardiovascular Evaluation and Care for Noncardiac Surgery 2008 Update Plus Overview of the Guidelines Concept John Coyle, M.D. October 16, 2008 The History of Medicine As Mountaineering Feat
Perioperative Cardiovascular Evaluation and Care for Noncardiac Surgery 2008 Update Plus Overview of the Guidelines Concept John Coyle, M.D. October 16, 2008 The History of Medicine As Mountaineering Feat
Stable Angina: Indication for revascularization and best medical therapy
 Stable Angina: Indication for revascularization and best medical therapy Cardiology Basics and Updated Guideline 2018 Chang-Hwan Yoon, MD/PhD Cardiovascular Center, Department of Internal Medicine Bundang
Stable Angina: Indication for revascularization and best medical therapy Cardiology Basics and Updated Guideline 2018 Chang-Hwan Yoon, MD/PhD Cardiovascular Center, Department of Internal Medicine Bundang
D M Y Y Y Y D D M M Y Y Y Y. Previous MI (apart from acute PCI) 0=no 1=yes 9=unknown
 0=no 1=yes 9=unknown") I Patient details and Preoperative Data Date of Informed Consent dd-mm-yyyy (Please leave blank if waived by Ethics Committee) Please enter Patient ID in this format xxx-xx-xxx 3 digit code for the country,
I Patient details and Preoperative Data Date of Informed Consent dd-mm-yyyy (Please leave blank if waived by Ethics Committee) Please enter Patient ID in this format xxx-xx-xxx 3 digit code for the country,
IHCP bulletin INDIANA HEALTH COVERAGE PROGRAMS BT JANUARY 24, 2012
 IHCP bulletin INDIANA HEALTH COVERAGE PROGRAMS BT201203 JANUARY 24, 2012 The IHCP to reimburse implantable cardioverter defibrillators separately from outpatient implantation Effective March 1, 2012, the
IHCP bulletin INDIANA HEALTH COVERAGE PROGRAMS BT201203 JANUARY 24, 2012 The IHCP to reimburse implantable cardioverter defibrillators separately from outpatient implantation Effective March 1, 2012, the
03/07/ Background. + High Risk Features Are Prevalent in Dialysis Patients
 + When Does Cardiovascular Disease Preclude Consideration of Renal Transplantation? Kul Aggarwal, MD, MRCP (UK), FACC Professor of Clinical Medicine Division of Cardiology University of Missouri & Chief,
+ When Does Cardiovascular Disease Preclude Consideration of Renal Transplantation? Kul Aggarwal, MD, MRCP (UK), FACC Professor of Clinical Medicine Division of Cardiology University of Missouri & Chief,
6/1/18 LEARNING OBJECTIVES PATIENT POPULATION PRESENTATIONS
 PREVENTING HOSPITAL READMISSIONS IN CARDIOVASCULAR PATIENTS Christina Cortez Perry, MSN, FNP-C, CCCC Cardiology Coordinator- Corpus Christi Medical Center 1 2 LEARNING OBJECTIVES Identify the target patient
PREVENTING HOSPITAL READMISSIONS IN CARDIOVASCULAR PATIENTS Christina Cortez Perry, MSN, FNP-C, CCCC Cardiology Coordinator- Corpus Christi Medical Center 1 2 LEARNING OBJECTIVES Identify the target patient
Measurement Name Beta-Blocker Therapy Prior Myocardial Infarction (MI)
") Program Metrics The list below includes the metrics that will be calculated by the PINNACLE Registry for the outpatient office setting. These include metrics for Artery, Atrial Fibrillation, Hypertension
Program Metrics The list below includes the metrics that will be calculated by the PINNACLE Registry for the outpatient office setting. These include metrics for Artery, Atrial Fibrillation, Hypertension
Non ST Elevation-ACS. Michael W. Cammarata, MD
 Non ST Elevation-ACS Michael W. Cammarata, MD Case Presentation 65 year old man PMH: CAD s/p stent in 2008 HTN HLD Presents with chest pressure, substernally and radiating to the left arm and jaw, similar
Non ST Elevation-ACS Michael W. Cammarata, MD Case Presentation 65 year old man PMH: CAD s/p stent in 2008 HTN HLD Presents with chest pressure, substernally and radiating to the left arm and jaw, similar
Guideline Number: NIA_CG_024 Last Review Date: January 2011 Responsible Department: Last Revised Date: May 2, 2011 Clinical Operations
 National Imaging Associates, Inc. Clinical guidelines NUCLEAR CARDIAC IMAGING (MYOCARDIAL PERFUSION STUDY) CPT Codes: 78451, 78452, 78453, 78454, 78466, 78468, 78469, 78481, 78483, 78494, 78499 Original
National Imaging Associates, Inc. Clinical guidelines NUCLEAR CARDIAC IMAGING (MYOCARDIAL PERFUSION STUDY) CPT Codes: 78451, 78452, 78453, 78454, 78466, 78468, 78469, 78481, 78483, 78494, 78499 Original
An algorithmic approach to the very high risk surgical patient
 An algorithmic approach to the very high risk surgical patient Daniel A. Reuter Center of Anesthesiology and Intensive Care Medicine Hamburg-Eppendorf Universiy Medical Center Disclosures: Member of the
An algorithmic approach to the very high risk surgical patient Daniel A. Reuter Center of Anesthesiology and Intensive Care Medicine Hamburg-Eppendorf Universiy Medical Center Disclosures: Member of the
PREOPERATIVE ASSESSMENT OF THE PATIENT WITH CARDIAC DISEASE
 CHAPTER 7 V O L U M E T H I R T Y - T H R E E PREOPERATIVE ASSESSMENT OF THE PATIENT WITH CARDIAC DISEASE LEE A. FLEISHER, M.D. ROBERT D. DRIPPS PROFESSOR AND CHAIR DEPARTMENT OF ANESTHESIOLOGY AND CRTICAL
CHAPTER 7 V O L U M E T H I R T Y - T H R E E PREOPERATIVE ASSESSMENT OF THE PATIENT WITH CARDIAC DISEASE LEE A. FLEISHER, M.D. ROBERT D. DRIPPS PROFESSOR AND CHAIR DEPARTMENT OF ANESTHESIOLOGY AND CRTICAL
Preoperative Cardiac Evaluation:
 Preoperative Cardiac Evaluation: The New Guidelines Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Disclosures No financial relationships with pharmaceutical
Preoperative Cardiac Evaluation: The New Guidelines Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Disclosures No financial relationships with pharmaceutical
Ischemic Heart Disease Interventional Treatment
 Ischemic Heart Disease Interventional Treatment Cardiac Catheterization Laboratory Procedures (N = 11,61) is a regional and national referral center for percutaneous coronary intervention (PCI). A total
Ischemic Heart Disease Interventional Treatment Cardiac Catheterization Laboratory Procedures (N = 11,61) is a regional and national referral center for percutaneous coronary intervention (PCI). A total
DIFFERENTIATING THE PATIENT WITH UNDIFFERENTIATED CHEST PAIN
 DIFFERENTIATING THE PATIENT WITH UNDIFFERENTIATED CHEST PAIN Objectives Gain competence in evaluating chest pain Recognize features of moderate risk unstable angina Review initial management of UA and
DIFFERENTIATING THE PATIENT WITH UNDIFFERENTIATED CHEST PAIN Objectives Gain competence in evaluating chest pain Recognize features of moderate risk unstable angina Review initial management of UA and
Chest Pain: To Cath or Not? Part I
 Chest Pain: To Cath or Not? Part I Georgios Papaioannou, MD Ioannis Karavas, MD Newton-Wellesley Hospital 5/3/2000 1 A Typical Scenario... 57 year old female, Mrs. X., presents to your office with a 2
Chest Pain: To Cath or Not? Part I Georgios Papaioannou, MD Ioannis Karavas, MD Newton-Wellesley Hospital 5/3/2000 1 A Typical Scenario... 57 year old female, Mrs. X., presents to your office with a 2
Acute Coronary Syndromes
 Overview Acute Coronary Syndromes Rabeea Aboufakher, MD, FACC, FSCAI Section Chief of Cardiology Altru Health System Grand Forks, ND Epidemiology Pathophysiology Clinical features and diagnosis STEMI management
Overview Acute Coronary Syndromes Rabeea Aboufakher, MD, FACC, FSCAI Section Chief of Cardiology Altru Health System Grand Forks, ND Epidemiology Pathophysiology Clinical features and diagnosis STEMI management
Cardiovascular nuclear imaging employs non-invasive techniques to assess alterations in coronary artery flow, and ventricular function.
 National Imaging Associates, Inc. Clinical guidelines CARDIOVASCULAR NUCLEAR MEDICINE -MYOCARDIAL PERFUSION IMAGING -MUGA Original Date: October 2015 Page 1 of 9 FOR CMS (MEDICARE) MEMBERS ONLY CPT4 Codes:
National Imaging Associates, Inc. Clinical guidelines CARDIOVASCULAR NUCLEAR MEDICINE -MYOCARDIAL PERFUSION IMAGING -MUGA Original Date: October 2015 Page 1 of 9 FOR CMS (MEDICARE) MEMBERS ONLY CPT4 Codes:
When Should I Order a Stress Test or an Echocardiogram
 When Should I Order a Stress Test or an Echocardiogram Updates in Cardiology 2015 March 7, 2015 Donald L. Lappé, MD, FAHA, FACC Chairman, Cardiovascular Department Medical Director, Intermountain Cardiovascular
When Should I Order a Stress Test or an Echocardiogram Updates in Cardiology 2015 March 7, 2015 Donald L. Lappé, MD, FAHA, FACC Chairman, Cardiovascular Department Medical Director, Intermountain Cardiovascular
ARIC HEART FAILURE HOSPITAL RECORD ABSTRACTION FORM. General Instructions: ID NUMBER: FORM NAME: H F A DATE: 10/13/2017 VERSION: CONTACT YEAR NUMBER:
 ARIC HEART FAILURE HOSPITAL RECORD ABSTRACTION FORM General Instructions: The Heart Failure Hospital Record Abstraction Form is completed for all heart failure-eligible cohort hospitalizations. Refer to
ARIC HEART FAILURE HOSPITAL RECORD ABSTRACTION FORM General Instructions: The Heart Failure Hospital Record Abstraction Form is completed for all heart failure-eligible cohort hospitalizations. Refer to
Optimal testing for coronary artery disease in symptomatic and asymptomatic patients
 Optimal testing for coronary artery disease in symptomatic and asymptomatic patients Alexandre C Ferreira, MD Clinical Chief of Cardiology Jackson Health System Director, Interventional Cardiology Training
Optimal testing for coronary artery disease in symptomatic and asymptomatic patients Alexandre C Ferreira, MD Clinical Chief of Cardiology Jackson Health System Director, Interventional Cardiology Training
AMERICAN SOCIETY OF ANESTHESIOLOGISTS ANESTHESIA PRE OPERATIVE SCREENING ASA PHYSICAL STATUS CLASSIFICATION ANESTHESIOLOGISTS
 ANESTHESIA PRE OPERATIVE SCREENING CAPA S 37 TH ANNUAL CONFERENCE PALM SPRINGS OCTOBER 5, 2013 ROBERT F. KOPEL, MD, FACP, FCCP HOAG HOSPITAL ASSISTANT CLINICAL PROFESSOR UCLA SCHOOL OF MEDICINE AMERICAN
ANESTHESIA PRE OPERATIVE SCREENING CAPA S 37 TH ANNUAL CONFERENCE PALM SPRINGS OCTOBER 5, 2013 ROBERT F. KOPEL, MD, FACP, FCCP HOAG HOSPITAL ASSISTANT CLINICAL PROFESSOR UCLA SCHOOL OF MEDICINE AMERICAN
Management of Patients with Atrial Fibrillation Undergoing Coronary Artery Stenting 경북대의전원내과조용근
 Management of Patients with Atrial Fibrillation Undergoing Coronary Artery Stenting 경북대의전원내과조용근 Case (2011, 5) 74-years old gentleman Exertional chest pain Warfarin with good INR control Ex-smoker, social(?)
Management of Patients with Atrial Fibrillation Undergoing Coronary Artery Stenting 경북대의전원내과조용근 Case (2011, 5) 74-years old gentleman Exertional chest pain Warfarin with good INR control Ex-smoker, social(?)
Detailed Order Request Checklists for Cardiology
 Next Generation Solutions Detailed Order Request Checklists for Cardiology 8600 West Bryn Mawr Avenue South Tower Suite 800 Chicago, IL 60631 www.aimspecialtyhealth.com Appropriate.Safe.Affordable 2018
Next Generation Solutions Detailed Order Request Checklists for Cardiology 8600 West Bryn Mawr Avenue South Tower Suite 800 Chicago, IL 60631 www.aimspecialtyhealth.com Appropriate.Safe.Affordable 2018
Aerobic Exercise Screening Stratification Tool
 Aerobic Screening Stratification Tool Disclaimer: The Aerobics Screening Stratification Tool is a working document currently used within the Stroke Rehabilitation Service of St. Joseph s Care Group- Thunder
Aerobic Screening Stratification Tool Disclaimer: The Aerobics Screening Stratification Tool is a working document currently used within the Stroke Rehabilitation Service of St. Joseph s Care Group- Thunder
2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY. MEASURE TYPE: Process
 Quality ID #44 (NQF 0236): Coronary Artery Bypass Graft (CABG): Preoperative Beta-Blocker in Patients with Isolated CABG Surgery National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR
Quality ID #44 (NQF 0236): Coronary Artery Bypass Graft (CABG): Preoperative Beta-Blocker in Patients with Isolated CABG Surgery National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR
Ischemic Heart Disease Interventional Treatment
 Ischemic Heart Disease Interventional Treatment Cardiac Catheterization Laboratory Procedures (N = 89) is a regional and national referral center for percutaneous coronary intervention (PCI). A total of
Ischemic Heart Disease Interventional Treatment Cardiac Catheterization Laboratory Procedures (N = 89) is a regional and national referral center for percutaneous coronary intervention (PCI). A total of
PERIOPERATIVE EVALUATION AND ANESTHETIC MANAGEMENT OF PATIENTS WITH CARDIAC DISEASE FOR NON CARDIAC SURGERY
 PERIOPERATIVE EVALUATION AND ANESTHETIC MANAGEMENT OF PATIENTS WITH CARDIAC DISEASE FOR NON CARDIAC SURGERY WHICH PATIENT IS AT HIGHEST RISK? 1. 70 yo asymptomatic patient with history of heart failure
PERIOPERATIVE EVALUATION AND ANESTHETIC MANAGEMENT OF PATIENTS WITH CARDIAC DISEASE FOR NON CARDIAC SURGERY WHICH PATIENT IS AT HIGHEST RISK? 1. 70 yo asymptomatic patient with history of heart failure
Stress ECG is still Viable in Suleiman M Kharabsheh, MD, FACC Consultant Invasive Cardiologist KFHI KFSHRC-Riyadh
 Stress ECG is still Viable in 2016 Suleiman M Kharabsheh, MD, FACC Consultant Invasive Cardiologist KFHI KFSHRC-Riyadh Stress ECG Do we still need stress ECG with all the advances we have in the CV field?
Stress ECG is still Viable in 2016 Suleiman M Kharabsheh, MD, FACC Consultant Invasive Cardiologist KFHI KFSHRC-Riyadh Stress ECG Do we still need stress ECG with all the advances we have in the CV field?
The importance of follow-up after a cardiac event: CARDIAC REHABILITATION. Dr. Guy Letcher
 The importance of follow-up after a cardiac event: CARDIAC REHABILITATION Dr. Guy Letcher The National Medicare Experience Mortality After Angioplasty 225,915 patients Mortality After Bypass Surgery 357,885
The importance of follow-up after a cardiac event: CARDIAC REHABILITATION Dr. Guy Letcher The National Medicare Experience Mortality After Angioplasty 225,915 patients Mortality After Bypass Surgery 357,885
CORONARY ARTERY BYPASS GRAFT (CABG) MEASURES GROUP OVERVIEW
 MEASURES GROUP OVERVIEW") CONARY ARTERY BYPASS GRAFT (CABG) MEASURES GROUP OVERVIEW 2015 PQRS OPTIONS F MEASURES GROUPS: 2015 PQRS MEASURES IN CONARY ARTERY BYPASS GRAFT (CABG) MEASURES GROUP: #43 Coronary Artery Bypass Graft (CABG):
CONARY ARTERY BYPASS GRAFT (CABG) MEASURES GROUP OVERVIEW 2015 PQRS OPTIONS F MEASURES GROUPS: 2015 PQRS MEASURES IN CONARY ARTERY BYPASS GRAFT (CABG) MEASURES GROUP: #43 Coronary Artery Bypass Graft (CABG):
ASA PLAVIX AND PREOPERATIVE OPTIMIZATION. John Hann, MD
 ASA PLAVIX AND PREOPERATIVE OPTIMIZATION John Hann, MD QUESTIONS: WHICH ANTI-PLATELETS DO YOU STOP AND WHEN? 1. 65 yo M with history of stroke on ASA PreOp eval for cataracts surgery 2. 65 yo M with RCRI
ASA PLAVIX AND PREOPERATIVE OPTIMIZATION John Hann, MD QUESTIONS: WHICH ANTI-PLATELETS DO YOU STOP AND WHEN? 1. 65 yo M with history of stroke on ASA PreOp eval for cataracts surgery 2. 65 yo M with RCRI
Stress Testing in Valvular Disease
 2017 ASE Florida Orlando, FL October 10, 2017 2:40 2:50 PM 10 min Grand Harbor Ballroom South Stress Testing in Valvular Disease Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
2017 ASE Florida Orlando, FL October 10, 2017 2:40 2:50 PM 10 min Grand Harbor Ballroom South Stress Testing in Valvular Disease Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
Choosing the Right Cardiac Test. Outline
 Choosing the Right Cardiac Test Atif Qasim, M.D., M.S.C.E. University of California, San Francisco Disclosures: None 2013 Outline Focus on choosing the optimal tests for coronary disease evaluation Overview
Choosing the Right Cardiac Test Atif Qasim, M.D., M.S.C.E. University of California, San Francisco Disclosures: None 2013 Outline Focus on choosing the optimal tests for coronary disease evaluation Overview
To provide information on the use of acetyl salicylic acid in the treatment and prevention of vascular events.
 ACETYL SALICYLIC ACID TARGET AUDIENCE: All Canadian health care professionals. OBJECTIVE: To provide information on the use of acetyl salicylic acid in the treatment and prevention of vascular events.
ACETYL SALICYLIC ACID TARGET AUDIENCE: All Canadian health care professionals. OBJECTIVE: To provide information on the use of acetyl salicylic acid in the treatment and prevention of vascular events.
Acute Coronary Syndrome
 ACUTE CORONOARY SYNDROME, ANGINA & ACUTE MYOCARDIAL INFARCTION Administrative Consultant Service 3/17 Acute Coronary Syndrome Acute Coronary Syndrome has evolved as a useful operational term to refer to
ACUTE CORONOARY SYNDROME, ANGINA & ACUTE MYOCARDIAL INFARCTION Administrative Consultant Service 3/17 Acute Coronary Syndrome Acute Coronary Syndrome has evolved as a useful operational term to refer to
2016 ACC/AHA Guideline Focused Update on Duration of Dual Antiplatelet Therapy in Patients With Coronary Artery Disease
 2016 ACC/AHA Guideline Focused Update on Duration of Dual Antiplatelet Therapy in Patients With Coronary Artery Disease Developed in Collaboration with American Association for Thoracic Surgery, American
2016 ACC/AHA Guideline Focused Update on Duration of Dual Antiplatelet Therapy in Patients With Coronary Artery Disease Developed in Collaboration with American Association for Thoracic Surgery, American
OUTPATIENT ANTITHROMBOTIC MANAGEMENT POST NON-ST ELEVATION ACUTE CORONARY SYNDROME. TARGET AUDIENCE: All Canadian health care professionals.
 OUTPATIENT ANTITHROMBOTIC MANAGEMENT POST NON-ST ELEVATION ACUTE CORONARY SYNDROME TARGET AUDIENCE: All Canadian health care professionals. OBJECTIVE: To review the use of antiplatelet agents and oral
OUTPATIENT ANTITHROMBOTIC MANAGEMENT POST NON-ST ELEVATION ACUTE CORONARY SYNDROME TARGET AUDIENCE: All Canadian health care professionals. OBJECTIVE: To review the use of antiplatelet agents and oral
HEART CONDITIONS IN SPORT
 HEART CONDITIONS IN SPORT Dr. Anita Green CHD Risk Factors Smoking Hyperlipidaemia Hypertension Obesity Physical Inactivity Diabetes Risks are cumulative (multiplicative) Lifestyles predispose to RF One
HEART CONDITIONS IN SPORT Dr. Anita Green CHD Risk Factors Smoking Hyperlipidaemia Hypertension Obesity Physical Inactivity Diabetes Risks are cumulative (multiplicative) Lifestyles predispose to RF One
Cardiac Conditions in Sport & Exercise. Cardiac Conditions in Sport. USA - Sudden Cardiac Death (SCD) Dr Anita Green. Sudden Cardiac Death
 Dr Anita Green. Sudden Cardiac Death") Cardiac Conditions in Sport & Exercise Dr Anita Green Cardiac Conditions in Sport Sudden Cardiac Death USA - Sudden Cardiac Death (SCD)
Cardiac Conditions in Sport & Exercise Dr Anita Green Cardiac Conditions in Sport Sudden Cardiac Death USA - Sudden Cardiac Death (SCD)
Aerobic Exercise Screening Stratification Tool
 Aerobic Screening Stratification Tool Disclaimer: The Aerobics Screening Stratification Tool is a working document currently used within the Stroke Rehabilitation Service of Toronto Rehabilitation Institute
Aerobic Screening Stratification Tool Disclaimer: The Aerobics Screening Stratification Tool is a working document currently used within the Stroke Rehabilitation Service of Toronto Rehabilitation Institute