Disclosures. I have no financial disclosures relevant to the talk
|
|
|
- Stuart Washington
- 5 years ago
- Views:
Transcription
1 Syncope Sachin S. Sule, MD, FACP Associate Professor of Integrated Medical Science Division of Medicine Director,Internal Medicine Residency Program Charles E. Schmidt College of Medicine, Florida Atlantic University
2 Disclosures I have no financial disclosures relevant to the talk
3 Objectives Define Syncope and classify the types of syncope Discuss risk assessment and evaluation Discuss management of common causes of syncope

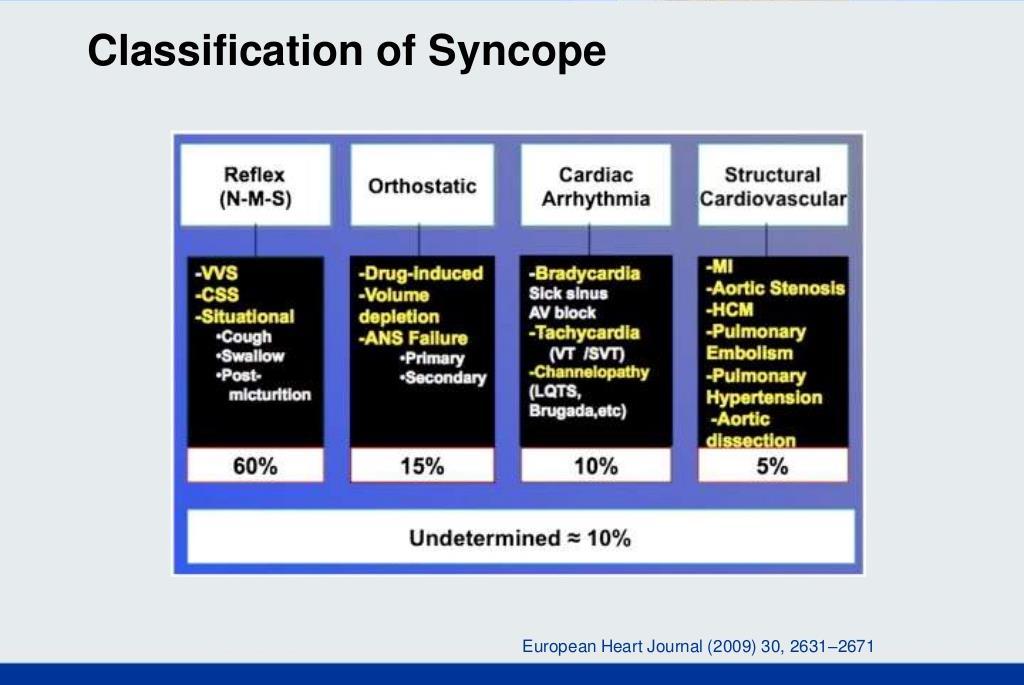
4 Definition Syncope is defined as a transient loss of consciousness (TLOC) attributable to global cerebral hypo-perfusion, further characterized by rapid onset, brevity, and spontaneous recovery.

5

6

7
8 Background Among patients >80 years of age, 58% were admitted to hospital. Older institutionalized patients: 23 % prevalence with 30% 2-year recurrence rate One year fall rate when syncope occurs in older adults: 38%
9
10

11
12 Salient features that differentiate syncope and non syncopal events Vasovagal syncope Provoked by prolonged standing classically in a hot, or crowded environment or associated with pain or medical procedure. Syncope at rest, after exercise. Prodrome of nausea, diaphoresis, dyspnea or warmth (often absent in older population) Brief LOC (<5min) Postdrome of somnolence or fatigue lasting minutes to hours Cardiac syncope Seizures Syncope at rest or exertion Brief or absent prodrome Rapid recovery Brief LOC (<5min) May be preceded by palpitations Prodromal aura (eg, odd smell), preoccupation, déjà vu or jamais vu Tongue bitten Head turning to one side during LOC Unusual posturing during LOC Postictal confusion Coarse, rhythmic and synchronous limb jerking of 1min beginning before or coinciding with LOC. Pseudo-syncope Prolonged LOC >15-20min Lack of injury in spite of the frequency of episodes Resists eye opening during LOC Known psychiatric disorder

13 Table 1. Applying Class of Recommendation and Level of Evidence to Clinical Strategies, Interventions, Treatments, or Diagnostic Testing in Patient Care* (Updated August 2015) Circulation. 2017;136:e25 e59. DOI: /CIR
14 History and Physical Examination COR LOE Recommendation I B-NR A detailed history and physical examination should be performed in patients with syncope. Electrocardiography COR LOE Recommendation I B-NR In the initial evaluation of patients with syncope, a resting 12-lead ECG is useful.

15
16 The physical examination should focus on the following: Heart rate Orthostatic hypotension Valvular heart disease. Focal neurological deficits.

17
18 Syncope Initial Evaluation General Principles Transient loss of consciousness* Suspected syncope No Evaluation as clinically indicated Yes Initial evaluation: history, physical examination, and ECG (Class I) Cause of syncope certain Risk assessment Cause of syncope uncertain Treatment Further evaluation
19 Risk Assessment COR LOE Recommendations I B-NR Evaluation of the cause and assessment for the short- and long-term morbidity and mortality risk of syncope are recommended. IIb B-NR Use of risk stratification scores may be reasonable in the management of patients with syncope.

20

21

22

23

24
25 Etiology of syncope in patients hospitalized with syncope and predictors of mortality and rehospitalization for syncope at 27-month follow-up. Sule S 1, Palaniswamy C, Aronow WS, Ahn C, Peterson SJ, Adapa S, Mudambi L. Clin Cardiol Jan;34(1):35-8. doi: /clc The authors investigated the etiologies of syncope and risk factors for mortality and rehospitalization for syncope at 27-month follow-up in 325 consecutive patients, mean age 66 years, hospitalized for syncope. The causes of syncope were diagnosed in 241 patients (74%). Of 325 patients, 13 (4%) were rehospitalized for syncope and 38 (12%) died. Stepwise logistic regression analysis showed that significant independent prognostic factors for rehospitalization for syncope were diabetes (odds ratio [OR], 5.7; 95% confidence interval [CI], ), atrial fibrillation (OR, 4.0; 95% CI, ), and smoking (OR, 4.6; 95% CI, ). Stepwise Cox regression analysis showed that significant independent prognostic factors for time to mortality were diabetes (hazard ratio [HR], 2.7; 95% CI, ), coronary artery bypass graft surgery (HR, 2.9; 95% CI, ), malignancy history (HR, 2.5; 95% CI, ), narcotics use (HR, 4.0; 95% CI, ), smoking (HR, 2.8; 95% CI, ), atrial fibrillation (HR, 2.4; 95% CI, ), and volume depletion (HR, 2.8; 95% CI, ).
26 Patient Disposition After Initial Evaluation for Syncope Syncope initial evaluation Serious medical conditions present? (Table 7) Yes No Inpatient evaluation (Class I) Manage presumptive reflex-mediated syncope in outpatient setting (Class IIa) Structured ED observation protocol for intermediaterisk pts (Class IIa) Manage selected pts with suspected cardiac syncope in outpatient setting (Class IIb) Colors correspond to Class of Recommendation in Table 1. ED indicates emergency department; pts, patients.
27 Disposition After Initial Evaluation COR LOE Recommendations I IIa IIa IIb B-NR C-LD B-R C-LD Hospital evaluation and treatment are recommended for patients presenting with syncope who have a serious medical condition potentially relevant to the cause of syncope identified during initial evaluation. It is reasonable to manage patients with presumptive reflexmediated syncope in the outpatient setting in the absence of serious medical conditions. In intermediate-risk patients with an unclear cause of syncope, use of a structured ED observation protocol can be effective in reducing hospital admission. It may be reasonable to manage selected patients with suspected cardiac syncope in the outpatient setting in the absence of serious medical condition.
28 Additional Evaluation and Diagnosis Syncope additional evaluation and diagnosis Initial evaluation: history, physical exam, ECG (Class I) Initial evaluation clear Initial evaluation unclear Stress testing (Class IIa) No additional evaluation needed* Targeted blood testing (Class IIa) Initial evaluation suggests neurogenic OH Initial evaluation suggests reflex syncope Initial evaluation suggests CV abnormalities Options TTE (Class IIa) EPS (Class IIa) Referral for autonomic evaluation (Class IIa) Tilt-table testing (Class IIa) Cardiac monitor selected based on frequency and nature (Class I) MRI or CT (Class Ilb) Options Implantable cardiac monitor (Class IIa) Ambulatory external cardiac monitor (Class IIa) *Applies to patients after a normal initial evaluation without significant injury or cardiovascular morbidities; patients followed up by primary care physician as needed. In selected patients (see Section 1.4). CT indicates computed tomography; CV, cardiovascular; ECG, electrocardiogram; EPS, electrophysiological study; MRI, magnetic resonance imaging; OH, orthostatic hypotension; and TTE, transthoracic echocardiography.
29 Blood Testing COR LOE Recommendations IIa B-NR Targeted blood tests are reasonable in the evaluation of selected patients with syncope identified on the basis of clinical assessment from history, physical examination, and ECG. IIb C-LD Usefulness of brain natriuretic peptide and high-sensitivity troponin measurement is uncertain in patients for whom a cardiac cause of syncope is suspected. III: No Benefit B-R Routine and comprehensive laboratory testing is not useful in the evaluation of patients with syncope.
30 Cardiovascular Testing Cardiac Imaging COR LOE Recommendations IIa IIb III: No Benefit B-NR B-NR B-R Transthoracic echocardiography can be useful in selected patients presenting with syncope if structural heart disease is suspected. CT or MRI may be useful in selected patients presenting with syncope of suspected cardiac etiology. Routine cardiac imaging is not useful in the evaluation of patients with syncope unless cardiac etiology is suspected on the basis of an initial evaluation, including history, physical examination, or ECG.
31 Stress Testing COR LOE Recommendation IIa C-LD Exercise stress testing can be useful to establish the cause of syncope in selected patients who experience syncope or presyncope during exertion.
32 Cardiac Monitoring COR LOE Recommendations I C-EO The choice of a specific cardiac monitor should be determined on the basis of the frequency and nature of syncope events. IIa IIa B-NR B-R To evaluate selected ambulatory patients with syncope of suspected arrhythmic etiology, the following external cardiac monitoring approaches can be useful: 1. Holter monitor 2. Transtelephonic monitor 3. External loop recorder 4. Patch recorder 5. Mobile cardiac outpatient telemetry. To evaluate selected ambulatory patients with syncope of suspected arrhythmic etiology, an ICM can be useful.

33
34 In-Hospital Telemetry COR LOE Recommendation I B-NR Continuous ECG monitoring is useful for hospitalized patients admitted for syncope evaluation with suspected cardiac etiology.
35 Electrophysiological Study COR LOE Recommendations IIa III: No Benefit B-NR B-NR EPS can be useful for evaluation of selected patients with syncope of suspected arrhythmic etiology. EPS is not recommended for syncope evaluation in patients with a normal ECG and normal cardiac structure and function, unless an arrhythmic etiology is suspected.
36 Tilt-Table Testing COR LOE Recommendations IIa B-R If the diagnosis is unclear after initial evaluation, tilt-table testing can be useful for patients with suspected VVS. IIa B-NR Tilt-table testing can be useful for patients with syncope and suspected delayed OH when initial evaluation is not diagnostic. IIa IIa III: No Benefit B-NR B-NR B-R Tilt-table testing is reasonable to distinguish convulsive syncope from epilepsy in selected patients. Tilt-table testing is reasonable to establish a diagnosis of pseudosyncope. Tilt-table testing is not recommended to predict a response to medical treatments for VVS.
37
38 Neurological Testing Autonomic Evaluation COR LOE Recommendation IIa C-LD Referral for autonomic evaluation can be useful to improve diagnostic and prognostic accuracy in selected patients with syncope and known or suspected neurodegenerative disease.
39 Neurological and Imaging Diagnostics COR LOE Recommendations IIa C-LD Simultaneous monitoring of an EEG and hemodynamic parameters during tilt-table testing can be useful to distinguish among syncope, pseudosyncope, and epilepsy. III: No Benefit III: No Benefit III: No Benefit B-NR B-NR B-NR MRI and CT of the head are not recommended in the routine evaluation of patients with syncope in the absence of focal neurological findings or head injury that support further evaluation. Carotid artery imaging is not recommended in the routine evaluation of patients with syncope in the absence of focal neurological findings that support further evaluation. Routine recording of an EEG is not recommended in the evaluation of patients with syncope in the absence of specific neurological features suggestive of a seizure.
40 2017 ACC/AHA/HRS Guideline for the Evaluation and Management of Patients With Syncope Reflex Conditions
41 Reflex Conditions COR LOE Recommendations I C-EO Patient education on the diagnosis and prognosis of VVS is recommended. IIa B-R Vasovagal Syncope Physical counter-pressure maneuvers can be useful in patients with VVS who have a sufficiently long prodromal period. IIa IIb IIb B-R B-R B-R Midodrine is reasonable in patients with recurrent VVS with no history of hypertension, HF, or urinary retention. The usefulness of orthostatic training is uncertain in patients with frequent VVS. Fludrocortisone might be reasonable for patients with recurrent VVS and inadequate response to salt and fluid intake, unless contraindicated.


42

43
44 Vasovagal Syncope (cont.) IIb IIb IIb IIb B-NR C-LD C-LD C-LD Beta blockers might be reasonable in patients 42 years of age or older with recurrent VVS. Encouraging increased salt and fluid intake may be reasonable in selected patients with VVS, unless contraindicated. In selected patients with VVS, it may be reasonable to reduce or withdraw medications that cause hypotension when appropriate. In patients with recurrent VVS, a selective serotonin reuptake inhibitor might be considered.
45 Vasovagal Syncope VVS Education on diagnosis and prognosis (Class I) Options Counter pressure maneuvers (Class IIa) Salt and fluid intake (Class IIb) VVS recurs Options Midodrine (Class IIa) Fludrocortisone (Class IIb) Beta blocker (in patients >42 y) (Class IIb) Orthostatic training (Class IIb) Selected serotonin reuptake inhibitors (Class IIb) Dual-chamber pacemaker therapy (Class IIb) Colors correspond to Class of Recommendation in Table 1. VVS indicates vasovagal syncope.
46 Pacemakers in Vasovagal Syncope COR LOE Recommendation IIb B-R SR population of patients 40 years of age or older with recurrent VVS and prolonged spontaneous pauses. Dual-chamber pacing might be reasonable in a select SR indicated systematic review.
47 Carotid Sinus Syndrome COR LOE Recommendations Permanent cardiac pacing is reasonable in patients with IIa B-R carotid sinus syndrome that is cardioinhibitory or mixed. IIb B-R It may be reasonable to implant a dual-chamber pacemaker in patients with carotid sinus syndrome who require permanent pacing.

48
49 2017 ACC/AHA/HRS Guideline for the Evaluation and Management of Patients With Syncope Orthostatic Hypotension
50 Orthostatic Hypotension Neurogenic Orthostatic Hypotension COR LOE Recommendations Acute water ingestion is recommended in patients with I B-R syncope caused by neurogenic OH for occasional, temporary relief. IIa IIa IIa IIa C-LD C-LD B-R B-R Physical counter-pressure maneuvers can be beneficial in patients with neurogenic OH with syncope. Compression garments can be beneficial in patients with syncope and OH. Midodrine can be beneficial in patients with syncope due to neurogenic OH. Droxidopa can be beneficial in patients with syncope due to neurogenic OH.
51 Neurogenic Orthostatic Hypotension (cont.) IIa IIb IIb IIb C-LD C-LD C-LD C-LD Fludrocortisone can be beneficial in patients with syncope due to neurogenic OH. Encouraging increased salt and fluid intake may be reasonable in selected patients with neurogenic OH. Pyridostigmine may be beneficial in patients with syncope due to neurogenic OH who are refractory to other treatments. Octreotide may be beneficial in patients with syncope and refractory recurrent postprandial or neurogenic OH.
52 Dehydration and Drugs COR LOE Recommendations I C-LD Fluid resuscitation via oral or intravenous bolus is recommended in patients with syncope due to acute dehydration. IIa IIa B-NR C-LD Reducing or withdrawing medications that may cause hypotension can be beneficial in selected patients with syncope. In selected patients with syncope due to dehydration, it is reasonable to encourage increased salt and fluid intake.

53 Orthostatic Hypotension Syncope of suspected OH origin Postural decrease in BP 20/10 mm Hg No Continue to evaluate Options Neurogenic OH Drugs Dehydration Colors correspond to Class of Recommendation in Table 1. BP indicates blood pressure; OH, orthostatic hypotension. Compression garments (Class IIa) Counter-pressure maneuvers (Class IIa) Midodrine (Class IIa) Droxidopa (Class IIa) Acute water ingestion (Class I) Therapy options in selected patients Increase salt and fluid intake (Class IIb) Octreotide (Class IIb) Pydridostigmine (Class IIb) Reduce or withdraw medications (Class IIa) Reduce or withdraw medications (Class IIa) Acute water ingestion (Class I) Increase salt and fluid intake (Class IIa) Fludrocortisone (Class IIa)
54 2017 ACC/AHA/HRS Guideline for the Evaluation and Management of Patients With Syncope Management of Cardiovascular Conditions
55 Arrhythmic Conditions COR LOE Recommendations Bradycardia I C-EO Supraventricular Tachycardia I C-EO In patients with syncope associated with bradycardia, GDMT is recommended. In patients with syncope and SVT, GDMT is recommended. I C-EO In patients with AF, GDMT is recommended. Ventricular Arrhythmia I C-EO In patients with syncope and VA, GDMT is recommended.
56 Structural Conditions COR LOE Recommendations Ischemic and Nonischemic Cardiomyopathy In patients with syncope associated with ischemic and I C-EO nonischemic cardiomyopathy, GDMT is recommended. Valvular Heart Disease I C-EO In patients with syncope associated with valvular heart disease, GDMT is recommended. Hypertrophic Cardiomyopathy I C-EO In patients with syncope associated with HCM, GDMT is recommended.
57 Arrhythmogenic Right Ventricular Cardiomyopathy COR LOE Recommendations ICD implantation is recommended in patients with ARVC who I B-NR present with syncope and have a documented sustained VA. IIa B-NR ICD implantation is reasonable in patients with ARVC who present with syncope of suspected arrhythmic etiology.
58 Cardiac Sarcoidosis COR LOE Recommendations I B-NR ICD implantation is recommended in patients with cardiac sarcoidosis presenting with syncope and documented spontaneous sustained VA. I IIa IIa C-EO B-NR B-NR In patients with cardiac sarcoidosis presenting with syncope and conduction abnormalities, GDMT is recommended. ICD implantation is reasonable in patients with cardiac sarcoidosis and syncope of suspected arrhythmic origin, particularly with LV dysfunction or pacing indication. EPS is reasonable in patients with cardiac sarcoidosis and syncope of suspected arrhythmic etiology.
59 Inheritable Arrhythmic Conditions Brugada Syndrome COR LOE Recommendations IIa IIb III: No Benefit B-NR B-NR B-NR ICD implantation is reasonable in patients with Brugada ECG pattern and syncope of suspected arrhythmic etiology. Invasive EPS may be considered in patients with Brugada ECG pattern and syncope of suspected arrhythmic etiology. ICD implantation is not recommended in patients with Brugada ECG pattern and reflex-mediated syncope in the absence of other risk factors.
60 Short-QT Syndrome COR LOE Recommendation IIb C-EO ICD implantation may be considered in patients with short-qt pattern and syncope of suspected arrhythmic etiology.
61 Long-QT Syndrome COR LOE Recommendations I IIa IIa B-NR B-NR C-LD Beta-blocker therapy, in the absence of contraindications, is indicated as a first-line therapy in patients with LQTS and suspected arrhythmic syncope. ICD implantation is reasonable in patients with LQTS and suspected arrhythmic syncope who are on beta-blocker therapy or are intolerant to beta-blocker therapy. Left cardiac sympathetic denervation (LCSD) is reasonable in patients with LQTS and recurrent syncope of suspected arrhythmic mechanism who are intolerant to beta-blocker therapy or for whom beta-blocker therapy has failed.
62 Catecholaminergic Polymorphic Ventricular Tachycardia COR LOE Recommendations Exercise restriction is recommended in patients with CPVT I C-LD presenting with syncope of suspected arrhythmic etiology. I IIa IIa IIb IIb C-LD C-LD B-NR C-LD C-LD Beta blockers lacking intrinsic sympathomimetic activity are recommended in patients with CPVT and stress-induced syncope. Flecainide is reasonable in patients with CPVT who continue to have syncope of suspected VA despite beta-blocker therapy. ICD therapy is reasonable in patients with CPVT and a history of exercise- or stress-induced syncope despite use of optimal medical therapy or LCSD. In patients with CPVT who continue to experience syncope or VA, verapamil with or without beta-blocker therapy may be considered. LCSD may be reasonable in patients with CPVT, syncope, and symptomatic VA despite optimal medical therapy.
63 Early Repolarization Pattern COR LOE Recommendations IIb III: Harm C-EO B-NR ICD implantation may be considered in patients with early repolarization pattern and suspected arrhythmic syncope in the presence of a family history of early repolarization pattern with cardiac arrest. EPS should not be performed in patients with early repolarization pattern and history of syncope in the absence of other indications.
64 Adult Congenital Heart Disease COR LOE Recommendations For evaluation of patients with ACHD and syncope, referral to a IIa C-EO specialist with expertise in ACHD can be beneficial. IIa B-NR EPS is reasonable in patients with moderate or severe ACHD and unexplained syncope.
65 2017 ACC/AHA/HRS Guideline for the Evaluation and Management of Patients With Syncope Pseudosyncope
66 Treatment of Pseudosyncope COR LOE Recommendations In patients with suspected pseudosyncope, a candid discussion IIb C-LD with the patient about the diagnosis may be reasonable. IIb C-LD Cognitive behavioral therapy may be beneficial in patients with pseudosyncope.
67 2017 ACC/AHA/HRS Guideline for the Evaluation and Management of Patients With Syncope Age, Lifestyle, and Special Populations
68 Geriatric Patients COR LOE Recommendations For the assessment and management of older adults with IIa C-EO syncope, a comprehensive approach in collaboration with an expert in geriatric care can be beneficial. IIa B-NR It is reasonable to consider syncope as a cause of nonaccidental falls in older adults.
69 Predictors of mortality, rehospitalization for syncope, and cardiac syncope in 352 consecutive elderly patients with syncope. Khera S 1, Palaniswamy C, Aronow WS, Sule S, Doshi JV, Adapa S, Balasubramaniyam N, Ahn C, Peterson SJ, Nabors C. J Am Med Dir Assoc May;14(5): Participants were 352 consecutive patients aged 65 years or older with syncope admitted to hospital from the emergency department. Significant independent prognostic factors for mortality were diabetes mellitus (OR 2.08; 95% CI , P =.0263), history of smoking (OR 2.23; 95% CI , P =.0255), and use of statins (OR 0.37; 95% CI , P =.0036). Independent risk factors for predicting a cardiac cause of syncope were an abnormal electrocardiogram (OR 2.58; 95% CI , P =.0012) and reduced ejection fraction (OR 2.92; 95% CI , P <.001). The San Francisco Syncope Rule and Osservatorio Epidemiologico sulla Sincope nel Lazio scores did not predict mortality or rehospitalization in our study population.
70 Athletes COR LOE Recommendations I IIa C-EO C-LD Cardiovascular assessment by a care provider experienced in treating athletes with syncope is recommended prior to resuming competitive sports. Assessment by a specialist with disease-specific expertise is reasonable for athletes with syncope and high-risk markers. IIa III: Harm C-LD B-NR Extended monitoring can be beneficial for athletes with unexplained exertional syncope after an initial cardiovascular evaluation. Participation in competitive sports is not recommended for athletes with syncope and phenotype-positive HCM, CPVT, LQTS1, or ARVC before evaluation by a specialist.
71 Driving and Syncope COR LOE Recommendation IIa C-EO It can be beneficial for healthcare providers managing patients with syncope to know the driving laws and restrictions in their regions and discuss implications with the patient.
72 Syncope and Driving recommendations Condition OH VVS, no syncope in prior year (698) VVS, 1 6 syncope per year (694) VVS, >6 syncope per year (694,698) Situational syncope other than cough syncope Cough syncope, untreated Cough syncope, treated with cough suppression Carotid sinus syncope, untreated (698) Carotid sinus syncope, treated with permanent pacemaker (698) Syncope due to nonreflex bradycardia, untreated (698) Syncope due to nonreflex bradycardia, treated with permanent pacemaker (12,698) Syncope due to SVT, untreated (698) Syncope due to SVT, pharmacologically suppressed (698) Syncope due to SVT, treated with ablation (698) Syncope with LVEF <35% and a presumed arrhythmic etiology without an ICD (699,700) Syncope with LVEF <35% and presumed arrhythmic etiology with an ICD (701,702) Syncope presumed due to VT/VF, structural heart disease, and LVEF 35%, untreated Syncope presumed due to VT/VF, structural heart disease, and LVEF 35%, treated with an ICD and guideline-directed drug therapy (701,702) Syncope presumed due to VT with a genetic cause, untreated Syncope presumed due to VT with a genetic cause, treated with an ICD or guideline-directed drug therapy Syncope presumed due to a nonstructural heart disease VT, such as RVOT or LVOT, untreated Syncope presumed due to a nonstructural heart disease VT, such as RVOT or LVOT, treated successfully with ablation or suppressed pharmacologically (698) Syncope of undetermined etiology Symptom-Free Waiting Time 1 month No restriction 1 month Not fit to drive until symptoms resolved 1 month Not fit to drive 1 month Not fit to drive 1 week Not fit to drive 1 week Not fit to drive 1 month 1 week Not fit to drive 3 months Not fit to drive 3 months Not fit to drive 3 months Not fit to drive 3 months 1 month
73 Summary Syncope is not an uncommon event. It is important to classify syncope and recognize high risk features Appropriate diagnostic and therapeutic tools can prevent recurrence.
Syncope Guidelines: What s New?
 Syncope Guidelines: What s New? Dr. Samuel Asirvatham Professor of Medicine and Pediatrics Mayo Clinic College of Medicine Medical Director, Electrophysiology Laboratory Program Director, EP Fellowship
Syncope Guidelines: What s New? Dr. Samuel Asirvatham Professor of Medicine and Pediatrics Mayo Clinic College of Medicine Medical Director, Electrophysiology Laboratory Program Director, EP Fellowship
Syncope Guidelines What s new? October 19 th 2017 Mohamed Aljaabari MBBCh, FACC, FHRS Consultant Electrophysiologist - Mafraq Hospital
 Syncope Guidelines What s new? October 19 th 2017 Mohamed Aljaabari MBBCh, FACC, FHRS Consultant Electrophysiologist - Mafraq Hospital Case Presentation 35 Male presented with sudden loss of consciousness
Syncope Guidelines What s new? October 19 th 2017 Mohamed Aljaabari MBBCh, FACC, FHRS Consultant Electrophysiologist - Mafraq Hospital Case Presentation 35 Male presented with sudden loss of consciousness
Clinical Evaluation & Management of Syncope:UPDATE
 Clinical Evaluation & Management of Syncope:UPDATE 2017 ACC/AHA/HRS Guideline for the Evaluation and Management of Patients With Syncope Developed in Collaboration with the American College of Emergency
Clinical Evaluation & Management of Syncope:UPDATE 2017 ACC/AHA/HRS Guideline for the Evaluation and Management of Patients With Syncope Developed in Collaboration with the American College of Emergency
Index. cardiology.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Adenosine in idiopathic AV block, 445 446 Adolescent(s) syncope in, 397 409. See also Syncope, in children and adolescents AECG monitoring.
Index Note: Page numbers of article titles are in boldface type. A Adenosine in idiopathic AV block, 445 446 Adolescent(s) syncope in, 397 409. See also Syncope, in children and adolescents AECG monitoring.
Syncope (From a Cardiologist s Perspective) Patrick Henderson, DO 118 th OOA Annual Convention Internal Medicine Specialty Track April 28 th, 2018
 Patrick Henderson, DO 118 th OOA Annual Convention Internal Medicine Specialty Track April 28 th, 2018") Syncope (From a Cardiologist s Perspective) Patrick Henderson, DO 118 th OOA Annual Convention Internal Medicine Specialty Track April 28 th, 2018 No financial disclosures to report Goals Formally define
Syncope (From a Cardiologist s Perspective) Patrick Henderson, DO 118 th OOA Annual Convention Internal Medicine Specialty Track April 28 th, 2018 No financial disclosures to report Goals Formally define
Cardiology Updates: Syncope and Stress Testing. Kathleen Morris, DO Cardiology Fellow St. Vincent Hospital
 Cardiology Updates: Syncope and Stress Testing Kathleen Morris, DO Cardiology Fellow St. Vincent Hospital Disclosures NONE PART ONE: Let s start with SYNCOPE Objectives: Definition of Syncope Brief review
Cardiology Updates: Syncope and Stress Testing Kathleen Morris, DO Cardiology Fellow St. Vincent Hospital Disclosures NONE PART ONE: Let s start with SYNCOPE Objectives: Definition of Syncope Brief review
Syncope: Evaluation of the Weak and Dizzy
 Syncope: Evaluation of the Weak and Dizzy William M. Miles, MD, FACC, FHRS Professor of Medicine Silverstein Chair for Cardiovascular Education University of Florida College of Medicine Disclosures Medtronic,
Syncope: Evaluation of the Weak and Dizzy William M. Miles, MD, FACC, FHRS Professor of Medicine Silverstein Chair for Cardiovascular Education University of Florida College of Medicine Disclosures Medtronic,
Syncope: Evaluation of the Weak and Dizzy
 Syncope: Evaluation of the Weak and Dizzy William M. Miles, MD, FACC, FHRS Professor of Medicine Silverstein Chair for Cardiovascular Education University of Florida College of Medicine Disclosures Medtronic,
Syncope: Evaluation of the Weak and Dizzy William M. Miles, MD, FACC, FHRS Professor of Medicine Silverstein Chair for Cardiovascular Education University of Florida College of Medicine Disclosures Medtronic,
Pattarapong Makarawate MD, FHRS Assistant Professor. Division Of Cardiology Faculty of Medicine, Khon Kaen University
 Pattarapong Makarawate MD, FHRS Assistant Professor. Division Of Cardiology Faculty of Medicine, Khon Kaen University 1. Important and impact of ICD in primary prevention 2. Risk stratification for ICD
Pattarapong Makarawate MD, FHRS Assistant Professor. Division Of Cardiology Faculty of Medicine, Khon Kaen University 1. Important and impact of ICD in primary prevention 2. Risk stratification for ICD
Syncope Update Dr Matthew Lovell, Consultant in Cardiology
 Syncope Update Dr Matthew Lovell, Consultant in Cardiology Definition of Syncope Syncope is defined as TLOC due to cerebral hypoperfusion Characterized by a rapid onset, short duration, and spontaneous
Syncope Update Dr Matthew Lovell, Consultant in Cardiology Definition of Syncope Syncope is defined as TLOC due to cerebral hypoperfusion Characterized by a rapid onset, short duration, and spontaneous
Applying Syncope Guidelines to Clinical Practice
 Applying Syncope Guidelines to Clinical Practice ACC Rockies February 27, 2018 Roopinder K Sandhu Associate Professor of Medicine U of A Director of Edmonton Cardiac Arrhythmia Trials Research Group Visiting
Applying Syncope Guidelines to Clinical Practice ACC Rockies February 27, 2018 Roopinder K Sandhu Associate Professor of Medicine U of A Director of Edmonton Cardiac Arrhythmia Trials Research Group Visiting
Improving Patient Outcomes with a Syncope Center. Suneet Mittal, MD
 Improving Patient Outcomes with a Syncope Center Suneet Mittal, MD Improving Patient Outcomes with a Syncope Center: Early Risk Stratification of Patients who Require Device Therapy Suneet Mittal, MD Director,
Improving Patient Outcomes with a Syncope Center Suneet Mittal, MD Improving Patient Outcomes with a Syncope Center: Early Risk Stratification of Patients who Require Device Therapy Suneet Mittal, MD Director,
Syncope Guidelines Update. Bernard Harbieh, FHRS AUBMC-KMC Beirut-Lebanon
 Syncope Guidelines Update Bernard Harbieh, FHRS AUBMC-KMC Beirut-Lebanon New Syncope Guidelines Increase the volume of information on diagnosis and management Incorporation of emergency specialists, neurologists,
Syncope Guidelines Update Bernard Harbieh, FHRS AUBMC-KMC Beirut-Lebanon New Syncope Guidelines Increase the volume of information on diagnosis and management Incorporation of emergency specialists, neurologists,
2018 ESC Guidelines for the diagnosis and management of syncope
 2018 ESC Guidelines for the diagnosis and management of syncope Michele Brignole (Chairperson) (Italy); Angel Moya (Co-chairperson) (Spain); Jean-Claude Deharo (France); Frederik de Lange (The Netherlands);
2018 ESC Guidelines for the diagnosis and management of syncope Michele Brignole (Chairperson) (Italy); Angel Moya (Co-chairperson) (Spain); Jean-Claude Deharo (France); Frederik de Lange (The Netherlands);
Syncope By Remus Popa
 Syncope By Remus Popa A 66 years old male is brought to the ED from a restaurant where he fainted while dining out with his family. He complained of nausea and stood up to go to the restroom but immediately
Syncope By Remus Popa A 66 years old male is brought to the ED from a restaurant where he fainted while dining out with his family. He complained of nausea and stood up to go to the restroom but immediately
Syncope. A Symptom not a Diagnosis
 A Symptom not a Diagnosis Vijay Duggirala, MD Assistant Professor-Clinical Department of Internal Medicine Division of Hospital Medicine The Ohio State University Wexner Medical Center Objectives Define
A Symptom not a Diagnosis Vijay Duggirala, MD Assistant Professor-Clinical Department of Internal Medicine Division of Hospital Medicine The Ohio State University Wexner Medical Center Objectives Define
Syncope. A Symptom not a Diagnosis. Vijay Duggirala, MD
 Syncope A Symptom not a Diagnosis Vijay Duggirala, MD Assistant Professor-Clinical Department of Internal Medicine Division of Hospital Medicine The Ohio State University Wexner Medical Center Objectives
Syncope A Symptom not a Diagnosis Vijay Duggirala, MD Assistant Professor-Clinical Department of Internal Medicine Division of Hospital Medicine The Ohio State University Wexner Medical Center Objectives
Death after Syncope: Can we predict it? Daniel Zamarripa, MD Senior Medical Director December 2013
 Death after Syncope: Can we predict it? Daniel Zamarripa, MD Senior Medical Director December 2013 Death after Syncope: Can we predict it? Those who suffer from frequent and severe fainting often die suddenly
Death after Syncope: Can we predict it? Daniel Zamarripa, MD Senior Medical Director December 2013 Death after Syncope: Can we predict it? Those who suffer from frequent and severe fainting often die suddenly
Valutazione iniziale e stratificazione del rischio
 Valutazione iniziale e stratificazione del rischio Paolo Alboni Sezione di Cardiologia Ospedale Privato Quisisana Ferrara DEFINITION OF SYNCOPE Syncope is a transient loss of consciousness due to global
Valutazione iniziale e stratificazione del rischio Paolo Alboni Sezione di Cardiologia Ospedale Privato Quisisana Ferrara DEFINITION OF SYNCOPE Syncope is a transient loss of consciousness due to global
Lee Chee Wan. Senior Consultant Pacing and Cardiac Electrophysiology. GP Symposium 2 nd April 2016
 Lee Chee Wan Senior Consultant Pacing and Cardiac Electrophysiology GP Symposium 2 nd April 2016 Objectives Definition of syncope Common causes of syncope & impacts How to clinically assess patient with
Lee Chee Wan Senior Consultant Pacing and Cardiac Electrophysiology GP Symposium 2 nd April 2016 Objectives Definition of syncope Common causes of syncope & impacts How to clinically assess patient with
Rapid Access Clinics for Transient Loss of Consciousness
 Rapid Access Clinics for Transient Loss of Consciousness Michael Gammage Department of Cardiovascular Medicine University of Birmingham and University Hospital Birmingham NHS Foundation Trust Those who
Rapid Access Clinics for Transient Loss of Consciousness Michael Gammage Department of Cardiovascular Medicine University of Birmingham and University Hospital Birmingham NHS Foundation Trust Those who
Department of Paediatrics Clinical Guideline. Syncope Guideline
 Department of Paediatrics Clinical Guideline Syncope Guideline Definition Transient, self-limited loss of consciousness (TLOC), usually leading to falling. Onset is relatively rapid. Recovery is spontaneous,
Department of Paediatrics Clinical Guideline Syncope Guideline Definition Transient, self-limited loss of consciousness (TLOC), usually leading to falling. Onset is relatively rapid. Recovery is spontaneous,
Management of Syncope in Heart Failure. University of Iowa
 Management of Syncope in Heart Failure Brian Olshansky University of Iowa 1 Syncope Transient loss of consciousness, with rapid, usually complete, recovery, with or without prodrome A common, non-specific,
Management of Syncope in Heart Failure Brian Olshansky University of Iowa 1 Syncope Transient loss of consciousness, with rapid, usually complete, recovery, with or without prodrome A common, non-specific,
IHCP bulletin INDIANA HEALTH COVERAGE PROGRAMS BT JANUARY 24, 2012
 IHCP bulletin INDIANA HEALTH COVERAGE PROGRAMS BT201203 JANUARY 24, 2012 The IHCP to reimburse implantable cardioverter defibrillators separately from outpatient implantation Effective March 1, 2012, the
IHCP bulletin INDIANA HEALTH COVERAGE PROGRAMS BT201203 JANUARY 24, 2012 The IHCP to reimburse implantable cardioverter defibrillators separately from outpatient implantation Effective March 1, 2012, the
2018 ESC SYNCOPE GUIDELINES SUMMARY
 208 ESC SYNCOPE GUIDELINES SUMMARY NEW GUIDELINES OVERVIEW OF UPDATED RECOMMENDATIONS SINCE 2009 208 EUROPEAN SOCIETY OF CARDIOLOGY SYNCOPE GUIDELINES Goals of 208 Task Force Reducing Cost & Admissions:
208 ESC SYNCOPE GUIDELINES SUMMARY NEW GUIDELINES OVERVIEW OF UPDATED RECOMMENDATIONS SINCE 2009 208 EUROPEAN SOCIETY OF CARDIOLOGY SYNCOPE GUIDELINES Goals of 208 Task Force Reducing Cost & Admissions:
Le linee guida Sincope 2018 della Società Europea di Cardiologia La Syncope Unit Multidisciplinare. Andrea Ungar, MD, PhD, FESC
 Le linee guida Sincope 2018 della Società Europea di Cardiologia La Syncope Unit Multidisciplinare Andrea Ungar, MD, PhD, FESC Syncope Unit, Hypertension Centre Geriatric and Intensive care Medicine University
Le linee guida Sincope 2018 della Società Europea di Cardiologia La Syncope Unit Multidisciplinare Andrea Ungar, MD, PhD, FESC Syncope Unit, Hypertension Centre Geriatric and Intensive care Medicine University
DECLARATION OF CONFLICT OF INTEREST
 DECLARATION OF CONFLICT OF INTEREST The Management of Syncope remains a challenge: Clues from the History Richard Sutton, DSc Emeritus Professor of Cardiology Imperial College, St Mary s Hospital, London,
DECLARATION OF CONFLICT OF INTEREST The Management of Syncope remains a challenge: Clues from the History Richard Sutton, DSc Emeritus Professor of Cardiology Imperial College, St Mary s Hospital, London,
La strategia diagnostica: il monitoraggio ecg prolungato. Michele Brignole
 La strategia diagnostica: il monitoraggio ecg prolungato Michele Brignole ECG monitoring and syncope In-hospital monitoring Holter Monitoring External loop recorder Remote (at home) telemetry Implantable
La strategia diagnostica: il monitoraggio ecg prolungato Michele Brignole ECG monitoring and syncope In-hospital monitoring Holter Monitoring External loop recorder Remote (at home) telemetry Implantable
FANS Paediatric Pathway for Inherited Arrhythmias*
 FANS Paediatric Pathway for Inherited Arrhythmias* The pathway is based on the HRS/EHRA/APHRS Expert Consensus Statement on the Diagnosis and Management of Patients with Inherited Primary Arrhythmia Syndromes
FANS Paediatric Pathway for Inherited Arrhythmias* The pathway is based on the HRS/EHRA/APHRS Expert Consensus Statement on the Diagnosis and Management of Patients with Inherited Primary Arrhythmia Syndromes
NICE Action Plan 6/13 Transient loss of consciousness ('blackouts') management in adults and young people NICE CG 109 December 2013
 management in adults and young people NICE CG 109 December 2013") NICE Action Plan 6/13 Transient loss of consciousness ('blackouts') management in adults and young people NICE CG 109 December 2013 Title: Prepared by: Presented by: Main aim: Recommendations: Previous
NICE Action Plan 6/13 Transient loss of consciousness ('blackouts') management in adults and young people NICE CG 109 December 2013 Title: Prepared by: Presented by: Main aim: Recommendations: Previous
TLOC - What are the red flags? John Dean March 2018
 TLOC - What are the red flags? John Dean March 2018 What is TLOC? Transient loss of consciousness It is very common It accounts for 5% of ED attendances It accounts for 6% of hospital admissions It consumes
TLOC - What are the red flags? John Dean March 2018 What is TLOC? Transient loss of consciousness It is very common It accounts for 5% of ED attendances It accounts for 6% of hospital admissions It consumes
Clinical Case 1 A patient with a syncope Panos E. Vardas President Elect of the ESC, Prof of Cardiology, University Hospital of Crete
 Clinical Case 1 A patient with a syncope Panos E. Vardas President Elect of the ESC, Prof. of Cardiology, University Hospital of Crete Case presentation A 64-year-old male smoker, with arterial hypertension
Clinical Case 1 A patient with a syncope Panos E. Vardas President Elect of the ESC, Prof. of Cardiology, University Hospital of Crete Case presentation A 64-year-old male smoker, with arterial hypertension
Diagnostic and therapeutic management of the patient with syncope M. Brignole Arrhythmologic Centre and Syncope Unit Lavagna, Italy
 Diagnostic and therapeutic management of the patient with syncope M. Brignole Arrhythmologic Centre and Syncope Unit Lavagna, Italy Eur Heart J. 2009 Nov;30(21):2631-71 Available on www.escardio.org/guidelines
Diagnostic and therapeutic management of the patient with syncope M. Brignole Arrhythmologic Centre and Syncope Unit Lavagna, Italy Eur Heart J. 2009 Nov;30(21):2631-71 Available on www.escardio.org/guidelines
An Approach to the Patient with Syncope. Guy Amit MD, MPH Soroka University Medical Center Beer-Sheva
 An Approach to the Patient with Syncope Guy Amit MD, MPH Soroka University Medical Center Beer-Sheva Case presentation A 23 y.o. man presented with 2 episodes of syncope One during exercise,one at rest
An Approach to the Patient with Syncope Guy Amit MD, MPH Soroka University Medical Center Beer-Sheva Case presentation A 23 y.o. man presented with 2 episodes of syncope One during exercise,one at rest
Index. cardiacep.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A AEDs. See Automated external defibrillators (AEDs) AF. See Atrial fibrillation (AF) Age as factor in SD in marathon runners, 45 Antiarrhythmic
Note: Page numbers of article titles are in boldface type. A AEDs. See Automated external defibrillators (AEDs) AF. See Atrial fibrillation (AF) Age as factor in SD in marathon runners, 45 Antiarrhythmic
Silvia G Priori MD PhD
 The approach to the cardiac arrest survivor Silvia G Priori MD PhD Molecular Cardiology, IRCCS Fondazione Salvatore Maugeri Pavia, Italy AND Leon Charney Division of Cardiology, Cardiovascular Genetics
The approach to the cardiac arrest survivor Silvia G Priori MD PhD Molecular Cardiology, IRCCS Fondazione Salvatore Maugeri Pavia, Italy AND Leon Charney Division of Cardiology, Cardiovascular Genetics
Transient loss of consciousness
 Issue date: August 2010 Transient loss of consciousness Transient loss of consciousness ( blackouts ) management in adults and young people Developed by the National Clinical Guideline Centre Transient
Issue date: August 2010 Transient loss of consciousness Transient loss of consciousness ( blackouts ) management in adults and young people Developed by the National Clinical Guideline Centre Transient
Clinical Cardiac Electrophysiology
 Clinical Cardiac Electrophysiology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of
Clinical Cardiac Electrophysiology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of
2017 AHA/ACC/HRS Ventricular Arrhythmias and Sudden Cardiac Death Guideline. Top Ten Messages. Eleftherios M Kallergis, MD, PhD, FESC
 2017 AHA/ACC/HRS Ventricular Arrhythmias and Sudden Cardiac Death Guideline Top Ten Messages Eleftherios M Kallergis, MD, PhD, FESC Cadiology Department - Heraklion University Hospital No actual or potential
2017 AHA/ACC/HRS Ventricular Arrhythmias and Sudden Cardiac Death Guideline Top Ten Messages Eleftherios M Kallergis, MD, PhD, FESC Cadiology Department - Heraklion University Hospital No actual or potential
Adult with transient loss of consciousness faints, fits and funny turns
 Adult with transient loss of consciousness faints, fits and funny turns Introduction Problem-specific video guides to diagnosing patients and helping them with management and prevention to transient loss
Adult with transient loss of consciousness faints, fits and funny turns Introduction Problem-specific video guides to diagnosing patients and helping them with management and prevention to transient loss
Syncope Cardiac or not? Dr Jaycen Cruickshank Emergency Physician Director of Clinical Training BHS
 Syncope Cardiac or not? Dr Jaycen Cruickshank Emergency Physician Director of Clinical Training BHS Syncope( (cardiac(or(not?( What(is(syncope?( Syncope( is( a( brief( loss( of( consciousness( that( resolves(
Syncope Cardiac or not? Dr Jaycen Cruickshank Emergency Physician Director of Clinical Training BHS Syncope( (cardiac(or(not?( What(is(syncope?( Syncope( is( a( brief( loss( of( consciousness( that( resolves(
CLINICAL CARDIAC ELECTROPHYSIOLOGY Maintenance of Certification (MOC) Examination Blueprint
 Examination Blueprint") CLINICAL CARDIAC ELECTROPHYSIOLOGY Maintenance of Certification (MOC) Examination Blueprint ABIM invites diplomates to help develop the Clinical Cardiac Electrophysiology MOC exam blueprint Based on feedback
CLINICAL CARDIAC ELECTROPHYSIOLOGY Maintenance of Certification (MOC) Examination Blueprint ABIM invites diplomates to help develop the Clinical Cardiac Electrophysiology MOC exam blueprint Based on feedback
C1: Medical Standards for Safety Critical Workers with Cardiovascular Disorders
 C1: Medical Standards for Safety Critical Workers with Cardiovascular Disorders GENERAL ISSUES REGARDING MEDICAL FITNESS-FOR-DUTY 1. These medical standards apply to Union Pacific Railroad (UPRR) employees
C1: Medical Standards for Safety Critical Workers with Cardiovascular Disorders GENERAL ISSUES REGARDING MEDICAL FITNESS-FOR-DUTY 1. These medical standards apply to Union Pacific Railroad (UPRR) employees
SYNCOPE. Sanjay P. Singh, MD Chairman & Professor, Department of Neurology. Syncope
 SYNCOPE Sanjay P. Singh, MD Chairman & Professor, Department of Neurology. Syncope Syncope is a clinical syndrome characterized by transient loss of consciousness (TLOC) and postural tone that is most
SYNCOPE Sanjay P. Singh, MD Chairman & Professor, Department of Neurology. Syncope Syncope is a clinical syndrome characterized by transient loss of consciousness (TLOC) and postural tone that is most
Tachycardia Devices Indications and Basic Trouble Shooting
 Tachycardia Devices Indications and Basic Trouble Shooting Peter A. Brady, MD., FRCP Cardiology Review Course London, March 6 th, 2014 2011 MFMER 3134946-1 Tachycardia Devices ICD Indications Primary and
Tachycardia Devices Indications and Basic Trouble Shooting Peter A. Brady, MD., FRCP Cardiology Review Course London, March 6 th, 2014 2011 MFMER 3134946-1 Tachycardia Devices ICD Indications Primary and
Invasive Risk Stratification: When is it needed?
 Inherited Cardiomyopathies and Channelopathies: Who is at risk for Sudden Cardiac Death? Invasive Risk Stratification: When is it needed? Hung-Fat Tse, MD, PhD Department of Medicine The University of
Inherited Cardiomyopathies and Channelopathies: Who is at risk for Sudden Cardiac Death? Invasive Risk Stratification: When is it needed? Hung-Fat Tse, MD, PhD Department of Medicine The University of
Syncope : What tests should I do? Boon Lim Consultant Cardiologist Clinical Lead for Imperial Syncope Unit Hammersmith Hospital
 Syncope : What tests should I do? Boon Lim Consultant Cardiologist Clinical Lead for Imperial Syncope Unit Hammersmith Hospital The most important diagnostic test is History taking Why is history taking
Syncope : What tests should I do? Boon Lim Consultant Cardiologist Clinical Lead for Imperial Syncope Unit Hammersmith Hospital The most important diagnostic test is History taking Why is history taking
Antony French Consultant Cardiologist & Electrophysiologist
 Antony French Consultant Cardiologist & Electrophysiologist Palpitations Unpleasant awareness of rapid or forceful heart beat Not all tachycardias cause palpitations, and not all palpitations are due to
Antony French Consultant Cardiologist & Electrophysiologist Palpitations Unpleasant awareness of rapid or forceful heart beat Not all tachycardias cause palpitations, and not all palpitations are due to
June 8, 2018, London UK TREATMENT OF VASOVAGAL SYNCOPE
 June 8, 2018, London UK TREATMENT OF VASOVAGAL SYNCOPE Where to go for help Syncope: HRS Definition Syncope is defined as: a transient loss of consciousness, associated with an inability to maintain postural
June 8, 2018, London UK TREATMENT OF VASOVAGAL SYNCOPE Where to go for help Syncope: HRS Definition Syncope is defined as: a transient loss of consciousness, associated with an inability to maintain postural
Faculty Disclosure. Sanjay P. Singh, MD, FAAN. Dr. Singh has listed an affiliation with: Consultant Sun Pharma Speaker s Bureau Lundbeck, Sunovion
 Faculty Disclosure Sanjay P. Singh, MD, FAAN Dr. Singh has listed an affiliation with: Consultant Sun Pharma Speaker s Bureau Lundbeck, Sunovion however, no conflict of interest exists for this conference.
Faculty Disclosure Sanjay P. Singh, MD, FAAN Dr. Singh has listed an affiliation with: Consultant Sun Pharma Speaker s Bureau Lundbeck, Sunovion however, no conflict of interest exists for this conference.
Guidelines Pediatric Congenital Heart Disease SYNCOPE
 Guidelines Pediatric Congenital Heart Disease SYNCOPE www.kinderkardiologie.org/dgpkleitlinien.shtm Definition and Characteristics of Syncope temporary loss of consciousness and tonicity due to inadequate
Guidelines Pediatric Congenital Heart Disease SYNCOPE www.kinderkardiologie.org/dgpkleitlinien.shtm Definition and Characteristics of Syncope temporary loss of consciousness and tonicity due to inadequate
Rhythm Control: Is There a Role for the PCP? Blake Norris, MD, FACC BHHI Primary Care Symposium February 28, 2014
 Rhythm Control: Is There a Role for the PCP? Blake Norris, MD, FACC BHHI Primary Care Symposium February 28, 2014 Financial disclosures Consultant Medtronic 3 reasons to evaluate and treat arrhythmias
Rhythm Control: Is There a Role for the PCP? Blake Norris, MD, FACC BHHI Primary Care Symposium February 28, 2014 Financial disclosures Consultant Medtronic 3 reasons to evaluate and treat arrhythmias
2017 ACC/AHA/HRS SYNCOPE GUIDELINES
 2017 ACC/AHA/HRS SYNCOPE GUIDELINES 2017 ACC/AHA/HRS Guideline for the Evaluation and Management of Patients With Syncope A Report of the American College of Cardiology/American Heart Association Task
2017 ACC/AHA/HRS SYNCOPE GUIDELINES 2017 ACC/AHA/HRS Guideline for the Evaluation and Management of Patients With Syncope A Report of the American College of Cardiology/American Heart Association Task
Syncope in patients with inherited arrhythmogenic syndromes. Is it enough to justify ICD implantation?
 Innovations in Interventional Cardiology and Electrophysiology Thessaloniki 2014 Syncope in patients with inherited arrhythmogenic syndromes. Is it enough to justify ICD implantation? K. Letsas, MD, FESC
Innovations in Interventional Cardiology and Electrophysiology Thessaloniki 2014 Syncope in patients with inherited arrhythmogenic syndromes. Is it enough to justify ICD implantation? K. Letsas, MD, FESC
Remote Monitoring & the Smart Home of the 21 Century
 Cardiostim EHRA Europace 2016, Nice - June 8-11, 2016 Remote Monitoring & the Smart Home of the 21 Century Antonio Raviele, MD, FESC, FHRS President ALFA -Alliance to Fight Atrial fibrillation- Venezia
Cardiostim EHRA Europace 2016, Nice - June 8-11, 2016 Remote Monitoring & the Smart Home of the 21 Century Antonio Raviele, MD, FESC, FHRS President ALFA -Alliance to Fight Atrial fibrillation- Venezia
Syncope evaluation: the role of syncope clinics Michele Brignole Arrhythmologic Centre, Lavagna, Italy
 Syncope evaluation: the role of syncope clinics Michele Brignole Arrhythmologic Centre, Lavagna, Italy Why should we need a Syncope Management Unit? We are not happy with current strategies: - not standardized
Syncope evaluation: the role of syncope clinics Michele Brignole Arrhythmologic Centre, Lavagna, Italy Why should we need a Syncope Management Unit? We are not happy with current strategies: - not standardized
APPENDIX D1 - CHARACTERISTICS OF INCLUDED STUDIES
 APPENDIX D1 - CHARACTERISTICS OF INCLUDED STUDIES 1 Initial Assessment included studies table... 3 1.1 Initial symptoms for diagnosis review... 3 1.2 Decision rules for diagnosis review... 8 1.3 Initial
APPENDIX D1 - CHARACTERISTICS OF INCLUDED STUDIES 1 Initial Assessment included studies table... 3 1.1 Initial symptoms for diagnosis review... 3 1.2 Decision rules for diagnosis review... 8 1.3 Initial
Vasovagal Syncope and Bradyarrhythmias Mechanisms, distinguishing cause and effect
 Vasovagal Syncope and Bradyarrhythmias Mechanisms, distinguishing cause and effect Walid Saliba, MD, FHRS, FACC Director EP lab Director Atrial Fibrillation Center Department of Cardiovascular Medicine
Vasovagal Syncope and Bradyarrhythmias Mechanisms, distinguishing cause and effect Walid Saliba, MD, FHRS, FACC Director EP lab Director Atrial Fibrillation Center Department of Cardiovascular Medicine
Clinical guideline Published: 25 August 2010 nice.org.uk/guidance/cg109
 Transient loss of consciousness ('blackouts') in over 16s Clinical guideline Published: 25 August 2010 nice.org.uk/guidance/cg109 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Transient loss of consciousness ('blackouts') in over 16s Clinical guideline Published: 25 August 2010 nice.org.uk/guidance/cg109 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Syncope: The Pediatric Patient
 Syncope: The Pediatric Patient Lindsey Malloy-Walton, DO, MPH, FAAP Division of Pediatric Cardiology Children s Mercy Hospital 2401 Gillham Road Kansas City, MO 64108 Phone (office): 816-234-3255 Email:
Syncope: The Pediatric Patient Lindsey Malloy-Walton, DO, MPH, FAAP Division of Pediatric Cardiology Children s Mercy Hospital 2401 Gillham Road Kansas City, MO 64108 Phone (office): 816-234-3255 Email:
What Every Physician Should Know:
 What Every Physician Should Know: The Canadian Heart Rhythm Society estimates that, in Canada, sudden cardiac death (SCD) is responsible for about 40,000 deaths annually; more than AIDS, breast cancer
What Every Physician Should Know: The Canadian Heart Rhythm Society estimates that, in Canada, sudden cardiac death (SCD) is responsible for about 40,000 deaths annually; more than AIDS, breast cancer
The ACC Heart Failure Guidelines
 The ACC Heart Failure Guidelines Fakhr Alayoubi, Msc,R Ph President of SCCP Cardiology Clinical Pharmacist Assistant Professor At King Saud University King Khalid University Hospital Riyadh-KSA 2017 ACC/AHA/HFSA
The ACC Heart Failure Guidelines Fakhr Alayoubi, Msc,R Ph President of SCCP Cardiology Clinical Pharmacist Assistant Professor At King Saud University King Khalid University Hospital Riyadh-KSA 2017 ACC/AHA/HFSA
Arrhythmias Focused Review. Who Needs An ICD?
 Who Needs An ICD? Cesar Alberte, MD, Douglas P. Zipes, MD, Krannert Institute of Cardiology, Indiana University School of Medicine, Indianapolis, IN Sudden cardiac arrest is one of the most common causes
Who Needs An ICD? Cesar Alberte, MD, Douglas P. Zipes, MD, Krannert Institute of Cardiology, Indiana University School of Medicine, Indianapolis, IN Sudden cardiac arrest is one of the most common causes
Ambulatory Cardiac Monitors and Outpatient Telemetry Corporate Medical Policy
 Ambulatory Cardiac Monitors and Outpatient Telemetry Corporate Medical Policy File Name: Ambulatory Event Monitors and Mobile Cardiac Outpatient Telemetry File Code: UM.SPSVC.13 Origination: 10/2015 Last
Ambulatory Cardiac Monitors and Outpatient Telemetry Corporate Medical Policy File Name: Ambulatory Event Monitors and Mobile Cardiac Outpatient Telemetry File Code: UM.SPSVC.13 Origination: 10/2015 Last
Role of Implantable Loop Recorder in the Evaluation of Syncope
 Role of Implantable Loop Recorder in the Evaluation of Syncope June Soo Kim, M.D., Ph.D. Department of Medicine Cardiac & Vascular Center Sungkyunkwan University School of Medicine Definition & Mechanism
Role of Implantable Loop Recorder in the Evaluation of Syncope June Soo Kim, M.D., Ph.D. Department of Medicine Cardiac & Vascular Center Sungkyunkwan University School of Medicine Definition & Mechanism
Arrhythmias (II) Ventricular Arrhythmias. Disclosures
 Ventricular Arrhythmias. Disclosures") Arrhythmias (II) Ventricular Arrhythmias Amy Leigh Miller, MD, PhD Cardiovascular Electrophysiology, Brigham & Women s Hospital Disclosures None Rhythms and Mortality Implantable loop recorder post-mi
Arrhythmias (II) Ventricular Arrhythmias Amy Leigh Miller, MD, PhD Cardiovascular Electrophysiology, Brigham & Women s Hospital Disclosures None Rhythms and Mortality Implantable loop recorder post-mi
Sudden Cardiac Death and Asians Disclosures
 Sudden Cardiac Death and Asians Disclosures 7 February 2009 Asian Heart and Vascular Symposium None Zian H. Tseng, M.D., M.A.S. Assistant Professor of Medicine Cardiac Electrophysiology Section University
Sudden Cardiac Death and Asians Disclosures 7 February 2009 Asian Heart and Vascular Symposium None Zian H. Tseng, M.D., M.A.S. Assistant Professor of Medicine Cardiac Electrophysiology Section University
Περίπτωση συγκοπής κατά τη διάρκεια άσκησης. Ποια είναι η ενδεδειγμένη προσέγγιση;
 Περίπτωση συγκοπής κατά τη διάρκεια άσκησης. Ποια είναι η ενδεδειγμένη προσέγγιση; Dr H. Θ. Ζάρβαλης Καρδιολόγος Διευθυντής ΕΣΥ Καρδιολογική Κλινική Γ. Ν. Παπαγεωργίου Θεσσαλονίκη ELPIDOFOROS S. SOTERIADES
Περίπτωση συγκοπής κατά τη διάρκεια άσκησης. Ποια είναι η ενδεδειγμένη προσέγγιση; Dr H. Θ. Ζάρβαλης Καρδιολόγος Διευθυντής ΕΣΥ Καρδιολογική Κλινική Γ. Ν. Παπαγεωργίου Θεσσαλονίκη ELPIDOFOROS S. SOTERIADES
ACC/AHA Guidelines for Ambulatory Electrocardiography: Executive Summary and Recommendations
 (Circulation. 1999;100:886-893.) 1999 American Heart Association, Inc. ACC/AHA Practice Guidelines ACC/AHA Guidelines for Ambulatory Electrocardiography: Executive Summary and Recommendations A Report
(Circulation. 1999;100:886-893.) 1999 American Heart Association, Inc. ACC/AHA Practice Guidelines ACC/AHA Guidelines for Ambulatory Electrocardiography: Executive Summary and Recommendations A Report
2016 Update to Heart Failure Clinical Practice Guidelines
 2016 Update to Heart Failure Clinical Practice Guidelines Mitchell T. Saltzberg, MD, FACC, FAHA, FHFSA Medical Director of Advanced Heart Failure Froedtert & Medical College of Wisconsin Stages, Phenotypes
2016 Update to Heart Failure Clinical Practice Guidelines Mitchell T. Saltzberg, MD, FACC, FAHA, FHFSA Medical Director of Advanced Heart Failure Froedtert & Medical College of Wisconsin Stages, Phenotypes
UNIVERSITY HOSPITALS OF LEICESTER NHS TRUST CARDIAC INVESTIGATIONS PAEDIATRIC & CONGENITAL SYNCOPE INVESTIGATIONS/QUESTIONNAIRE PROTOCOL
 UNIVERSITY HOSPITALS OF LEICESTER NHS TRUST CARDIAC INVESTIGATIONS PAEDIATRIC & CONGENITAL SYNCOPE INVESTIGATIONS/QUESTIONNAIRE PROTOCOL Written Date: 2009 by Dr Duke, then updated by Dr Sarita Makam 12/4/2016
UNIVERSITY HOSPITALS OF LEICESTER NHS TRUST CARDIAC INVESTIGATIONS PAEDIATRIC & CONGENITAL SYNCOPE INVESTIGATIONS/QUESTIONNAIRE PROTOCOL Written Date: 2009 by Dr Duke, then updated by Dr Sarita Makam 12/4/2016
WINDLAND SMITH RICE SUDDEN DEATH GENOMICS LABORATORY
 Learning Objectives to Disclose: To CRITIQUE the ICD and its role in the treatment of BrS, CPVT, and LQTS WINDLAND SMITH RICE SUDDEN DEATH GENOMICS LABORATORY Conflicts of Interest to Disclose: Consultant
Learning Objectives to Disclose: To CRITIQUE the ICD and its role in the treatment of BrS, CPVT, and LQTS WINDLAND SMITH RICE SUDDEN DEATH GENOMICS LABORATORY Conflicts of Interest to Disclose: Consultant
134 Adrian Baranchuk, MD FACC 1, William McIntyre BSc MD 1, William Harper, MD 2, Carlos A. Morillo, MD, FRCPC, FACC, FHRS, FESC 2.
 www.ipej.org 134 Original Article Application Of The American College Of Emergency Physicians (ACEP) Recommendations And a Risk Stratification Score (OESIL) For Patients With Syncope Admitted From The
www.ipej.org 134 Original Article Application Of The American College Of Emergency Physicians (ACEP) Recommendations And a Risk Stratification Score (OESIL) For Patients With Syncope Admitted From The
Arrhythmias and Heart Failure Dr Chris Lang Consultant Cardiologist and Electrophysiologist Royal Infirmary of Edinburgh
 Arrhythmias and Heart Failure Dr Chris Lang Consultant Cardiologist and Electrophysiologist Royal Infirmary of Edinburgh Arrhythmias and Heart Failure Ventricular Supraventricular VT/VF Primary prevention
Arrhythmias and Heart Failure Dr Chris Lang Consultant Cardiologist and Electrophysiologist Royal Infirmary of Edinburgh Arrhythmias and Heart Failure Ventricular Supraventricular VT/VF Primary prevention
Seek and Ye Shall Find: Surprising Findings When Using the ILR-LINQ
 Seek and Ye Shall Find: Surprising Findings When Using the ILR-LINQ Suneet Mittal, MD, FACC, FHRS Director, Electrophysiology Laboratory Valley Health System www.arrhythmia.org; @drsuneet October 31, 2015
Seek and Ye Shall Find: Surprising Findings When Using the ILR-LINQ Suneet Mittal, MD, FACC, FHRS Director, Electrophysiology Laboratory Valley Health System www.arrhythmia.org; @drsuneet October 31, 2015
What s new in my specialty?
 What s new in my specialty? Jon Melman, MD Heart Rhythm Specialists McKay-Dee Hospital some would say some would say my specialty 1 some would say my specialty First pacemaker 1958 some would say my specialty
What s new in my specialty? Jon Melman, MD Heart Rhythm Specialists McKay-Dee Hospital some would say some would say my specialty 1 some would say my specialty First pacemaker 1958 some would say my specialty
The Failing Heart in Primary Care
 The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
Contempo GIMSI Cosa cambia alla luce della letteratura in tema di terapia farmacologica
 Contempo GIMSI 2015-2017 Cosa cambia alla luce della letteratura in tema di terapia farmacologica Dott.ssa Diana Solari Centro Aritmologico e Sincope Unit, Lavagna www.gimsi.it POST 2 (Prevention of Syncope
Contempo GIMSI 2015-2017 Cosa cambia alla luce della letteratura in tema di terapia farmacologica Dott.ssa Diana Solari Centro Aritmologico e Sincope Unit, Lavagna www.gimsi.it POST 2 (Prevention of Syncope
Approach to Syncope in the ED
 Approach to Syncope in the ED Vukiet Tran, CCFP(EM), FCFP, MHSc, MBA Staff, Emergency Physician University Health Network Case 1 v 75 yo female presents with syncope Multiple previous episodes PMH: CAD,
Approach to Syncope in the ED Vukiet Tran, CCFP(EM), FCFP, MHSc, MBA Staff, Emergency Physician University Health Network Case 1 v 75 yo female presents with syncope Multiple previous episodes PMH: CAD,
13/09/2018. The ISSUE Studies. International (Italy & Spain) Study of Syncope of Uncertain Etiology. ISSUE study Pre-defined inclusion cathegories
 Study of Syncope of Uncertain Etiology. ISSUE study Pre-defined inclusion cathegories") The Studies Jean-Claude Deharo Aix-Marseille Université, France In Cardiac Electrophysiology Methods and Models Editors: Daniel C. Sigg, Paul A. Iaizzo, Yong-Fu Xiao, Bin He Springer 2010 study Pre-defined
The Studies Jean-Claude Deharo Aix-Marseille Université, France In Cardiac Electrophysiology Methods and Models Editors: Daniel C. Sigg, Paul A. Iaizzo, Yong-Fu Xiao, Bin He Springer 2010 study Pre-defined
Management of Arrhythmias The General Practitioners role
 Management of Arrhythmias The General Practitioners role Rohan Gunawardena MD, FRCP, FCCP, FACC Consultant Cardiac Electrophysiologist National Hospital of Sri Lanka Arrhythmias not common Palpitations
Management of Arrhythmias The General Practitioners role Rohan Gunawardena MD, FRCP, FCCP, FACC Consultant Cardiac Electrophysiologist National Hospital of Sri Lanka Arrhythmias not common Palpitations
Syncope: Causes and Treatment
 March 01, 2006 By Avery Hayes, MD [1] and Mahendr S. Kochar, MD, MS [2] Because the causes of syncope are numerous and the diagnostic tests have low yield, this disorder is often difficult to evaluate.
March 01, 2006 By Avery Hayes, MD [1] and Mahendr S. Kochar, MD, MS [2] Because the causes of syncope are numerous and the diagnostic tests have low yield, this disorder is often difficult to evaluate.
Tachycardias II. Štěpán Havránek
 Tachycardias II Štěpán Havránek Summary 1) Supraventricular (supraventricular rhythms) Atrial fibrillation and flutter Atrial ectopic tachycardia / extrabeats AV nodal reentrant a AV reentrant tachycardia
Tachycardias II Štěpán Havránek Summary 1) Supraventricular (supraventricular rhythms) Atrial fibrillation and flutter Atrial ectopic tachycardia / extrabeats AV nodal reentrant a AV reentrant tachycardia
ECG Workshop. Carolyn Shepherd And Anya Horne UWE Principles of Cardiac Care
 ECG Workshop Carolyn Shepherd And Anya Horne UWE Principles of Cardiac Care ECG workshop case study1 44 Year old male. Reports SOB, Lethargy, tiredness. PMH: Hypertension, nil else. What tests? What treatment?
ECG Workshop Carolyn Shepherd And Anya Horne UWE Principles of Cardiac Care ECG workshop case study1 44 Year old male. Reports SOB, Lethargy, tiredness. PMH: Hypertension, nil else. What tests? What treatment?
SPORTS AND EXERCISE ADVICE IN PATIENTS WITH ICD AND PPM
 SPORTS AND EXERCISE ADVICE IN PATIENTS WITH ICD AND PPM Rio De Janeiro 2016 Sport and Exercise Cardiology Symposium SBC/SOCERJ ACC Sharlene M. Day, MD Associate Professor, Cardiovascular Medicine Director,
SPORTS AND EXERCISE ADVICE IN PATIENTS WITH ICD AND PPM Rio De Janeiro 2016 Sport and Exercise Cardiology Symposium SBC/SOCERJ ACC Sharlene M. Day, MD Associate Professor, Cardiovascular Medicine Director,
Tilt Table Testing MM /01/2015. HMO; PPO; QUEST Integration 09/22/2017 Section: Medicine Place(s) of Service: Office, Outpatient
 of Service: Office, Outpatient") Tilt Table Testing Policy Number: Original Effective Date: MM.02.024 01/01/2015 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 09/22/2017 Section: Medicine Place(s) of Service:
Tilt Table Testing Policy Number: Original Effective Date: MM.02.024 01/01/2015 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 09/22/2017 Section: Medicine Place(s) of Service:
Syncope in ED-Risk Stratification Ger McMahon
 Syncope in ED-Risk Stratification Ger McMahon 3-8% of ED presentations increasing with advancing age ED physicians ranked syncope as the 2 nd most common decision making dilemma >50% are admitted @ 75%
Syncope in ED-Risk Stratification Ger McMahon 3-8% of ED presentations increasing with advancing age ED physicians ranked syncope as the 2 nd most common decision making dilemma >50% are admitted @ 75%
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Implantable cardioverter defibrillators for the treatment of arrhythmias and cardiac resynchronisation therapy for the treatment of heart failure (review
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Implantable cardioverter defibrillators for the treatment of arrhythmias and cardiac resynchronisation therapy for the treatment of heart failure (review
Vasovagal syncope in 2016: the current state of the faint
 Interventional Cardiology Vasovagal syncope in 2016: the current state of the faint In this article, we will review the challenges in defining syncope and the evolution of its definition over the past
Interventional Cardiology Vasovagal syncope in 2016: the current state of the faint In this article, we will review the challenges in defining syncope and the evolution of its definition over the past
HEART CONDITIONS IN SPORT
 HEART CONDITIONS IN SPORT Dr. Anita Green CHD Risk Factors Smoking Hyperlipidaemia Hypertension Obesity Physical Inactivity Diabetes Risks are cumulative (multiplicative) Lifestyles predispose to RF One
HEART CONDITIONS IN SPORT Dr. Anita Green CHD Risk Factors Smoking Hyperlipidaemia Hypertension Obesity Physical Inactivity Diabetes Risks are cumulative (multiplicative) Lifestyles predispose to RF One
Beware the Red Flags in the Management of Syncope
 Beware the Red Flags in the Management of Syncope Mitchell Cohen MD FACC FHRS Co-Director of the Pediatric Heart Program Director of Pediatric Arrhythmia Services Inova Fairfax Children s Hospital President,
Beware the Red Flags in the Management of Syncope Mitchell Cohen MD FACC FHRS Co-Director of the Pediatric Heart Program Director of Pediatric Arrhythmia Services Inova Fairfax Children s Hospital President,
Clinical Policy: Holter Monitors Reference Number: CP.MP.113
 Clinical Policy: Reference Number: CP.MP.113 Effective Date: 05/18 Last Review Date: 04/18 Coding Implications Revision Log Description Ambulatory electrocardiogram (ECG) monitoring provides a view of
Clinical Policy: Reference Number: CP.MP.113 Effective Date: 05/18 Last Review Date: 04/18 Coding Implications Revision Log Description Ambulatory electrocardiogram (ECG) monitoring provides a view of
Sequoia Heart Symposium 2018: Syncope. Gregory Engel, MD
 Sequoia Heart Symposium 2018: Syncope Gregory Engel, MD Silicon Valley Cardiology Palo Alto Medical Foundation Sutter Health Palo Alto, Redwood City, and San Carlos, CA Chief, Cardiovascular Division Sequoia
Sequoia Heart Symposium 2018: Syncope Gregory Engel, MD Silicon Valley Cardiology Palo Alto Medical Foundation Sutter Health Palo Alto, Redwood City, and San Carlos, CA Chief, Cardiovascular Division Sequoia
The Therapeutic Role of the Implantable Cardioverter Defibrillator in Arrhythmogenic Right Ventricular Dysplasia
 The Therapeutic Role of the Implantable Cardioverter Defibrillator in Arrhythmogenic Right Ventricular Dysplasia By Sandeep Joshi, MD and Jonathan S. Steinberg, MD Arrhythmia Service, Division of Cardiology
The Therapeutic Role of the Implantable Cardioverter Defibrillator in Arrhythmogenic Right Ventricular Dysplasia By Sandeep Joshi, MD and Jonathan S. Steinberg, MD Arrhythmia Service, Division of Cardiology
Summary, conclusions and future perspectives
 Summary, conclusions and future perspectives Summary The general introduction (Chapter 1) of this thesis describes aspects of sudden cardiac death (SCD), ventricular arrhythmias, substrates for ventricular
Summary, conclusions and future perspectives Summary The general introduction (Chapter 1) of this thesis describes aspects of sudden cardiac death (SCD), ventricular arrhythmias, substrates for ventricular
APPENDIX D1 - CHARACTERISTICS OF INCLUDED STUDIES APPENDIX D1 - CHARACTERISTICS OF INCLUDED STUDIES... 1
 APPENDIX D1 - CHARACTERISTICS OF INCLUDED STUDIES APPENDIX D1 - CHARACTERISTICS OF INCLUDED STUDIES... 1 1 Initial Assessment included studies table... 3 1.1 Initial symptoms for diagnosis review... 3
APPENDIX D1 - CHARACTERISTICS OF INCLUDED STUDIES APPENDIX D1 - CHARACTERISTICS OF INCLUDED STUDIES... 1 1 Initial Assessment included studies table... 3 1.1 Initial symptoms for diagnosis review... 3
CURRICULUM GOALS AND OBJECTIVES CLINICAL CARDIOVASCULAR ELECTROPHYSIOLOGY TRAINING PROGRAM. University of Florida Gainesville, Florida
 CURRICULUM GOALS AND OBJECTIVES CLINICAL CARDIOVASCULAR ELECTROPHYSIOLOGY TRAINING PROGRAM University of Florida Gainesville, Florida 1. Mission Statement To achieve excellence in the training of fourth
CURRICULUM GOALS AND OBJECTIVES CLINICAL CARDIOVASCULAR ELECTROPHYSIOLOGY TRAINING PROGRAM University of Florida Gainesville, Florida 1. Mission Statement To achieve excellence in the training of fourth
How Do I Balance Bradycardia with Rate Control in Atrial Fibrillation?
 How Do I Balance Bradycardia with Rate Control in Atrial Fibrillation? Thang Nguyen MD FRCPC Assistant Professor Section of Cardiology Department of Internal Medicine University of Manitoba Objectives
How Do I Balance Bradycardia with Rate Control in Atrial Fibrillation? Thang Nguyen MD FRCPC Assistant Professor Section of Cardiology Department of Internal Medicine University of Manitoba Objectives
National Coverage Determination (NCD) for Cardiac Pacemakers (20.8)
 for Cardiac Pacemakers (20.8)") Page 1 of 12 Centers for Medicare & Medicaid Services National Coverage Determination (NCD) for Cardiac Pacemakers (20.8) Tracking Information Publication Number 100-3 Manual Section Number 20.8 Manual
Page 1 of 12 Centers for Medicare & Medicaid Services National Coverage Determination (NCD) for Cardiac Pacemakers (20.8) Tracking Information Publication Number 100-3 Manual Section Number 20.8 Manual
Cardiac Conditions in Sport & Exercise. Cardiac Conditions in Sport. USA - Sudden Cardiac Death (SCD) Dr Anita Green. Sudden Cardiac Death
 Dr Anita Green. Sudden Cardiac Death") Cardiac Conditions in Sport & Exercise Dr Anita Green Cardiac Conditions in Sport Sudden Cardiac Death USA - Sudden Cardiac Death (SCD)
Cardiac Conditions in Sport & Exercise Dr Anita Green Cardiac Conditions in Sport Sudden Cardiac Death USA - Sudden Cardiac Death (SCD)