Syncope Guidelines Update. Bernard Harbieh, FHRS AUBMC-KMC Beirut-Lebanon
|
|
|
- Kelly Watts
- 5 years ago
- Views:
Transcription



1 Syncope Guidelines Update Bernard Harbieh, FHRS AUBMC-KMC Beirut-Lebanon
2 New Syncope Guidelines Increase the volume of information on diagnosis and management Incorporation of emergency specialists, neurologists, and geriatricians into the working group
3 69 pages and 440 references vs the 41 pages and 213 references of the previous guidelines Practical Instructions: 38 pages and 192 references The number of recommendations has increased by 7%; however, 40% are level I (49% in 2009) and only 3% are level III (14% in 2009). Neither has the level of evidence changed substantially: only 5% of recommendations are level A (3% in 2009) and most 50% are level C (52% in 2009).
4 The role of syncope units (SUs) is emphasized in a commitment to improved patient-focused safety and efficiency. This same commitment is reflected in the definition of the initial evaluation and risk stratification in the emergency department.

5 From: 2018 ESC Guidelines for the diagnosis and management of syncope Eur Heart J. 2018;39(21): doi: /eurheartj/ehy037 Eur Heart J The European Society of Cardiology All rights reserved. For permissions please journals.permissions@oxfordjournals.orgthis article is published and distributed under the terms of the Oxford University Press, Standard Journals Publication Model (
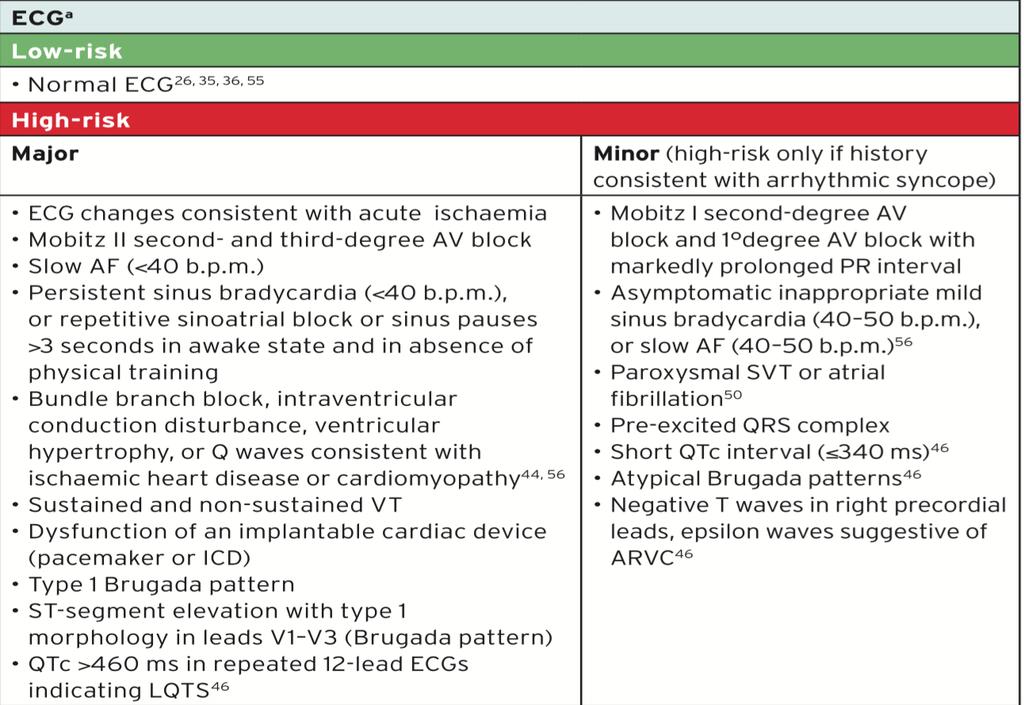
6 Management of syncope in the emergency department according to risk stratification One of the most novel aspects of the guidelines To reduce the hospital admission rate without compromising patient safety. Low and high-risk factors can be obtained from the clinical history, physical examination, and electrocardiogram.
7 High-risk patients are more likely to have cardiac syncope and, therefore, have a higher risk of sudden death than low-risk patients who, in contrast, are more likely to have reflex syncope and good prognosis
8 Class I B Low-risk patients without recurrence can be discharged from emergency departments High-risk patients: admitted or exhaustively evaluated in emergency departments or SUs Patients without high- or low-risk criteria: studied in emergency department observation units or referred to SUs instead of being admitted
9 A novelty is the equal consideration of presyncope and syncope, introduced because evidence indicates that they have the same prognosis
10 Carotid sinus massage Because it is one of the most cost-effective tests, CSM can be performed in the initial evaluation of patients older than 40 years. There are no changes in the level of indication or in the positive diagnostic criteria (presence of syncope together with ventricular pause > 3 seconds or a systolic blood pressure fall > 50 mmhg). The guidelines no longer deem the test contraindicated in patients with stroke in the previous 3 months or with carotid murmurs
11 Orthostatic challenge Its level of indication has fallen from I B to I C but the classic diagnostic criteria are maintained (I C if syncope occurs during the test and IIa C if there is a significant fall in blood pressure but no syncope). The initial orthostatic intolerance (that occurring < 30 seconds after the orthostatism) cannot be diagnosed with a sphygmomanometer and a beat-to-beat measurement is necessary (IIb C indication).
12 Tilt-table Recommendation drops from I B to IIa B The diagnostic criteria indication falls from I to IIa. In addition, its lack of ability to direct management is maintained. The TT is now considered useful for assessing hypotensive tendency. Its usefulness is clear in the context of orthostatic intolerance (either POTS or neurogenic hypotension) However, its applications are numerous: vasodepressor component assessment, differential diagnosis (epilepsy, psychiatric syncope), ventricular pause evaluation, prodrome recognition training, research, or videoelectroencephalography.
13 Electrocardiographic monitoring 1. In-hospital monitoring. Immediate monitoring is recommended in high-risk patients (I C), without changes. A clear recommendation for monitoring time is missing, and the lack of evidence is notable. A 6-hour emergency department time and a 24-hour hospitalization time are recommended in high-risk patients, without scientific support.
14 2. Holter monitoring, event recorders, smartphone applications, and external loop recorders. There are no major changes. Smartphone applications, although innovative, are undermined by their need to be activated by patients before the syncope. In the case of external loop recorders, the guidelines again apply a class IIa B recommendation for patients with an intersymptom interval less than 4 weeks
15 3. Implantable loop recording. The recommendations remain class I, but with a higher level of evidence, for patients not at high risk with recurrent syncope of uncertain origin and a high probability of recurrence during the battery life of the device and for high-risk patients after an exhaustive and unsuccessful investigation
16 Two new recommendations with clinical implications for ILRs Patients with unexplained falls (esp Elderly) and patients with suspected epilepsy whose treatment is ineffective A novelty is the mention of the possibility of remote monitoring, which improves the diagnostic performance by shortening the detection time
17 4. Diagnostic criteria of implantable loop recording findings. The number of recommendations decreases to 2: the findings are diagnostic when there is a correlation between syncope and arrhythmia and when, in the absence of syncope during the recording, prolonged pauses are observed, as well as third-degree or Mobitz II atrioventricular block or rapid tachycardia. It is presented as advice, and not as a recommendation, that the absence of arrhythmia during syncope rules out arrhythmic syncope and that the presence of significant arrhythmia during presyncope can be considered a diagnostic finding
18 5. Video recording This technique appears as a recommendation for the first time, in 2 situations. In the first case, for syncope occurring at home The second situation is the use of video recording during the TT test to improve the clinical observation of the events induced. Although class IIb, this recommendation is better documented and more feasible
19 6. Electrophysiological study. Its use would be restricted to 2% to 3% of syncopes of uncertain origin. Its limitations include the low negative predictive value and the nonspecificity of the induction of polymorphous ventricular tachycardia or ventricular fibrillation in most structural heart diseases. It continues to be useful in specific situations such as: Asymptomatic sinus bradycardia (CSNRT > 525 ms: PM IIa B) Bifascicular block (IIa B, unchanged) Suspected tachycardia In syncope preceded by palpitations: a IIb C indication
20 Endogenous adenosine and other biomarkers 1. Adenosine test. The guidelines newly introduce adenosine-sensitive syncope, a type of asystolic syncope seen in patients without prodromes and heart disease and with normal baseline ECG that could be due to endogenous adenosine release.
21 2. Cardiovascular and immunological biomarkers. The possible future usefulness of biomarkers and autoantibodies for autonomic dysfunction is mentioned, although the authors stress the need for more evidence
22 Treatment of Reflex Syncope The recommendation level of the indication for isometric physical counterpressure maneuvers is reduced (from I B to IIa B). This reduction is due to its low usefulness in the ISSUE-3 trial in elderly patients without prolonged and recognizable prodromes
23 Treatment of Orthostatic Hypotension and Orthostatic Intolerance Syndromes Years have passed but the treatment remains the same and as weakly effective as ever. Only water and salt intake has a class I C indication. There is little evidence of its effectiveness: in the American guidelines, the recommendation is IIb only midodrine and fludrocortisone have a IIa indication
24 Treatment of Syncope Due to Arrhythmias 1. Syncope due to intrinsic sinoatrial or atrioventricular conduction system disease The indications for PM implantation have not been substantially modified. Two aspects are detailed: a) in patients with sinus node disease without documentation of symptomatic pauses, the recommendation is to rule out other diagnostic alternatives (particularly reflex syncope) before PM implantation in order to reduce the high rate of syncopal recurrences, which is as high as 28% in some series; and b) in patients with syncopes and bifascicular block on ECG, in order to establish the PM indication, the recommendation is to document the pathological findings in an electrophysiological study or via a significant pause on an implantable loop recorder
25 2. Syncope due to tachyarrhythmias. Catheter ablation is the treatment of choice Two notes are made: a) to individualize the therapeutic option (ablation or drugs) for atrial fibrillation and left atrial flutter (medical therapy was prioritized in previous guidelines); b) to consider implantable cardioverter-defibrillator (ICD) placement after documentation of ventricular arrhythmias in order to reduce mortality in individuals with a left ventricular ejection fraction (LVEF) 35% (I A) or with previous infarction and induction of tachycardia ventricular (I C).
26 3. Treatment of unexplained syncope in patients at high risk of sudden cardiac death. There are 2 options: a) ICD therapy, given that, in this environment, syncope significantly increases the risk of sudden cardiac death; b) completion of the etiological study (with the intention of documenting the clinical arrhythmia) via placement of an implantable loop recorder in low-risk individuals without an indication for ICD
27 NEUROLOGICAL CAUSES AND PSEUDOSYNCOPES Electroencephalography, Doppler imaging of the supraaortic trunks, and brain computed tomography or magnetic resonance imaging (MRI) are not indicated for syncope (class III B recommendation). However, importantly, in contrast to the previous guidelines, brain MRI (I C) is recommended in patients with signs of parkinsonism, ataxia, or cognitive impairment. Electroencephalography is only useful in doubtful cases or to establish the diagnosis of psychogenic syncope if an induced episode is recorded. A novelty is the recommendation (I B) for paraneoplastic antibody screening (and active searching for occult neoplasia if positive) and antiganglionic acetylcholine receptor antibodies in patients with acute or subacute onset of autonomic dysfunction

28 From: 2018 ESC Guidelines for the diagnosis and management of syncope Eur Heart J. 2018;39(21): doi: /eurheartj/ehy037 Eur Heart J The European Society of Cardiology All rights reserved. For permissions please journals.permissions@oxfordjournals.orgthis article is published and distributed under the terms of the Oxford University Press, Standard Journals Publication Model (
29 Thank You

30

31

32

33
34

35

36
37 The following are key points to remember from the 2018 European Society of Cardiology (ESC) Guidelines for the Diagnosis and Management of Syncope
38 1 Syncope is defined as transient loss of consciousness (TLOC) due to cerebral hypoperfusion, characterized by a rapid onset, short duration, and spontaneous complete recovery
39 2 At the time of initial evaluation, clinicians should answer the following key questions: Was the event TLOC? In cases of TLOC, are they of syncopal or nonsyncopal origin? In cases of suspected syncope, is there a clear etiological diagnosis? Is there evidence to suggest a high risk of cardiovascular events or death? Is there a serious underlying cause that can be identified? If the cause is uncertain, what is the risk of a serious outcome? Should the patient be admitted to the hospital?
40 3 All patients should undergo a complete history, physical examination (including standing blood pressure measurement), and standard electrocardiogram (ECG). ECG monitoring (in bed or telemetry) should be performed in high-risk patients when there is a suspicion of arrhythmic syncope
41 4 An echocardiogram should be performed when there is previous known heart disease, or data suggestive of structural heart disease or syncope secondary to cardiovascular cause. Carotid sinus massage should be performed in patients >40 years of age with syncope of unknown origin compatible with a reflex mechanism. In addition, tilt testing should be performed in cases where there is suspicion of syncope due to reflex or an orthostatic cause
42 5 Prolonged ECG monitoring (external or implantable) should be performed in patients with recurrent severe unexplained syncope who have all of the following three features: Clinical or ECG features suggesting arrhythmic syncope. A high probability of recurrence of syncope in a reasonable time. Who may benefit from a specific therapy if a cause for syncope is found
43 6 Electrophysiological study should be performed in patients with unexplained syncope and bifascicular bundle branch block (impending high-degree atrioventricular [AV] block) or suspected tachycardia An exercise stress test performed in patients who experience syncope during or shortly after exertion
44 7 All patients with reflex syncope and orthostatic hypotension should have the diagnosis explained, reassured, explained the risk of recurrence, and given advice on how to avoid triggers and situations. These measures are the cornerstone of treatment and have a high impact in reducing the recurrence of syncope
45 8 In patients with severe forms of reflex syncope, one or more of the following additional specific treatments according to the clinical features may be selected: Midodrine or fludrocortisone in young patients with low blood pressure phenotype. Counter-pressure maneuvers (including tilt training if needed) in young patients with prodromes. Implantable loop recorder guided management strategy in selected patients without or with short prodromes. Discontinuation/reduction of hypotensive therapy targeting a systolic blood pressure of 140 mm Hg in older hypertensive patients. Pacemaker implantation in older patients with dominant cardioinhibitory forms.
46 9 In patients with orthostatic hypotension, one or more of the following additional specific treatments may be selected according to clinical severity: Education regarding lifestyle maneuvers. Adequate hydration and salt intake. Discontinuation/reduction of hypotensive therapy. Counter-pressure maneuvers. Abdominal binders and/or support stockings. Head-up tilt sleeping. Midodrine or fludrocortisone
47 10 The diagnostic process should be reevaluated and alternative therapies considered if the above rules fail or are not applicable to an individual patient. Even though guidelines are based on the best available scientific evidence, treatment should always be tailored to an individual patient s need and be patient centered
48 The following are key points to remember from the Practical Instructions for the 2018 European Society of Cardiology (ESC) Guidelines for the Diagnosis and Management of Syncope
49 1 Reflex syncope is the most frequent cause of syncope in any setting and at all ages, with cardiac syncope as the second most common cause
50 2 Transient loss of consciousness is characterized by four specific characteristics: short duration, abnormal motor control, loss of responsiveness, and amnesia for the period of loss of consciousness
51 3 Carotid sinus massage (CSM) preferably is performed during continuous electrocardiogram (ECG) and noninvasive beat-to-beat blood pressure (BP) monitoring. Carotid sinus hypersensitivity is diagnosed when CSM elicits abnormal cardioinhibition (i.e., asystole 3 seconds) and/or vasodepression (i.e., a fall in systolic BP >50 mm Hg)
52 4 It is recommended that the following method be adopted for tilt testing: Patients should be fasted for 2 4 hours before the test. Ensure a supine pre-tilt phase of 5 minutes when there is no venous cannulation, and of 20 minutes when there is venous cannulation. Tilt angle between 60 and 70 degrees. Passive phase of tilt of 20 minutes in duration and a maximum of 45 minutes. Use either sublingual nitroglycerin or intravenous isoproterenol for drug provocation if the passive phase is negative. The duration of the drug-challenge phase is minutes. For nitroglycerin challenge, a fixed dose of μg sublingually administered with the patient in the upright position. For isoproterenol challenge, an incremental infusion rate from 1 μg/min rising to 3 μg/min to increase average heart rate by about 20 25% over baseline. The test should be continued until complete loss of consciousness occurs or completion of the protocol. Tilt tables have only one specific requirement: the tilt-down time should be short (<15 seconds), as longer times increase the duration of precipitated asystole
53 5 Autonomic function testing should be performed by a specialist trained in autonomic function testing and interpretation. The required equipment includes beatto-beat BP and ECG monitoring, a motorized tilt table, 24-hour ambulatory BP monitoring devices, and other specialized equipment depending on the range of testing
54 6 During the Valsalva maneuver, the patient is asked to conduct a maximally forced expiration for 15 seconds against a closed glottis, i.e., with closed nose and mouth, or into a closed loop system with a resistance of 40 mm Hg. The hemodynamic changes during the test should be monitored using beat-to-beat continuous noninvasive BP measurement and ECG
55 7 During the deep-breathing test, the patient is asked to breathe deeply at 6 breaths per minute for 1 minute under continuous heart rate and BP monitoring. In healthy individuals, heart rate rises during inspiration and falls during expiration
56 8 Classical orthostatic hypotension is defined as a sustained decrease in systolic BP 20 mm Hg, diastolic BP 10 mm Hg, or a sustained decrease in systolic BP to an absolute value <90 mm Hg within 3 minutes of active standing or head-up tilt of at least 60 degrees
57 9 Postural orthostatic tachycardia syndrome patients, mostly young women, present with severe orthostatic intolerance (light-headedness, palpitations, tremor, generalized weakness, blurred vision, and fatigue) and a marked orthostatic heart rate increase (>30 bpm, or >120 bpm) within 10 minutes of standing or head-up tilt in the absence of orthostatic hypotension
58 10 The BP fall of orthostatic vasovagal syncope differs from that in classical orthostatic hypotension. In vasovagal syncope, the BP drop starts several minutes after standing up and the rates of BP drop accelerate until people faint, lie down, or do both. Hence, low BP in orthostatic vasovagal syncope is short-lived. In classical orthostatic hypotension, the BP drop starts immediately on standing and the rate of drop decreases, so low BP may be sustained for many minutes
59 Thank You
60 Diagnostic Tests There are no changes to diagnostic tests, but a change in philosophy is seen with the promotion of the study of dysautonomia as a possible cause of neuromediated syncope. A reasoned step is the incorporation of the neurologist's viewpoint and of neurological tests into the diagnosis and, although to a lesser extent, into the treatment
61 POTS Postural orthostatic tachycardia syndrome (POTS) is precisely defined as an increase in heart rate of more than 30 beats or a rate exceeding 120 bpm with associated symptoms and without hypotension. The definition does not note that the increase should exceed 40 bpm in adolescents, as recommended by the consensus statement on orthostatic hypotension and POTS
62 3. Echocardiography. Echocardiography is still indicated (I B) when there is a suspicion of structural heart disease. The indication for exercise stress echocardiography (I C) is introduced to detect an inducible obstruction in the left ventricular outflow tract in patients with hypertrophic cardiomyopathy and postural or exertional syncope with a gradient less than 50 mmhg at rest or after induction
63 Cardiac pacing Four possible indications are defined, the first 3 for patients older than 40 years: a) documentation of spontaneous bradyarrhythmia (IIa B); b) carotid sinus syndrome with cardioinhibitory mechanism (IIa B); c) asystole induced in the TT test (IIb B); and d) adenosine-sensitive syncope (IIb B).
64 Thank You
Index. cardiology.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Adenosine in idiopathic AV block, 445 446 Adolescent(s) syncope in, 397 409. See also Syncope, in children and adolescents AECG monitoring.
Index Note: Page numbers of article titles are in boldface type. A Adenosine in idiopathic AV block, 445 446 Adolescent(s) syncope in, 397 409. See also Syncope, in children and adolescents AECG monitoring.
Syncope By Remus Popa
 Syncope By Remus Popa A 66 years old male is brought to the ED from a restaurant where he fainted while dining out with his family. He complained of nausea and stood up to go to the restroom but immediately
Syncope By Remus Popa A 66 years old male is brought to the ED from a restaurant where he fainted while dining out with his family. He complained of nausea and stood up to go to the restroom but immediately
Syncope Update Dr Matthew Lovell, Consultant in Cardiology
 Syncope Update Dr Matthew Lovell, Consultant in Cardiology Definition of Syncope Syncope is defined as TLOC due to cerebral hypoperfusion Characterized by a rapid onset, short duration, and spontaneous
Syncope Update Dr Matthew Lovell, Consultant in Cardiology Definition of Syncope Syncope is defined as TLOC due to cerebral hypoperfusion Characterized by a rapid onset, short duration, and spontaneous
2018 ESC Guidelines for the diagnosis and management of syncope
 2018 ESC Guidelines for the diagnosis and management of syncope Michele Brignole (Chairperson) (Italy); Angel Moya (Co-chairperson) (Spain); Jean-Claude Deharo (France); Frederik de Lange (The Netherlands);
2018 ESC Guidelines for the diagnosis and management of syncope Michele Brignole (Chairperson) (Italy); Angel Moya (Co-chairperson) (Spain); Jean-Claude Deharo (France); Frederik de Lange (The Netherlands);
Syncope: Evaluation of the Weak and Dizzy
 Syncope: Evaluation of the Weak and Dizzy William M. Miles, MD, FACC, FHRS Professor of Medicine Silverstein Chair for Cardiovascular Education University of Florida College of Medicine Disclosures Medtronic,
Syncope: Evaluation of the Weak and Dizzy William M. Miles, MD, FACC, FHRS Professor of Medicine Silverstein Chair for Cardiovascular Education University of Florida College of Medicine Disclosures Medtronic,
Syncope: Evaluation of the Weak and Dizzy
 Syncope: Evaluation of the Weak and Dizzy William M. Miles, MD, FACC, FHRS Professor of Medicine Silverstein Chair for Cardiovascular Education University of Florida College of Medicine Disclosures Medtronic,
Syncope: Evaluation of the Weak and Dizzy William M. Miles, MD, FACC, FHRS Professor of Medicine Silverstein Chair for Cardiovascular Education University of Florida College of Medicine Disclosures Medtronic,
Syncope Guidelines: What s New?
 Syncope Guidelines: What s New? Dr. Samuel Asirvatham Professor of Medicine and Pediatrics Mayo Clinic College of Medicine Medical Director, Electrophysiology Laboratory Program Director, EP Fellowship
Syncope Guidelines: What s New? Dr. Samuel Asirvatham Professor of Medicine and Pediatrics Mayo Clinic College of Medicine Medical Director, Electrophysiology Laboratory Program Director, EP Fellowship
Le linee guida Sincope 2018 della Società Europea di Cardiologia La Syncope Unit Multidisciplinare. Andrea Ungar, MD, PhD, FESC
 Le linee guida Sincope 2018 della Società Europea di Cardiologia La Syncope Unit Multidisciplinare Andrea Ungar, MD, PhD, FESC Syncope Unit, Hypertension Centre Geriatric and Intensive care Medicine University
Le linee guida Sincope 2018 della Società Europea di Cardiologia La Syncope Unit Multidisciplinare Andrea Ungar, MD, PhD, FESC Syncope Unit, Hypertension Centre Geriatric and Intensive care Medicine University
Death after Syncope: Can we predict it? Daniel Zamarripa, MD Senior Medical Director December 2013
 Death after Syncope: Can we predict it? Daniel Zamarripa, MD Senior Medical Director December 2013 Death after Syncope: Can we predict it? Those who suffer from frequent and severe fainting often die suddenly
Death after Syncope: Can we predict it? Daniel Zamarripa, MD Senior Medical Director December 2013 Death after Syncope: Can we predict it? Those who suffer from frequent and severe fainting often die suddenly
Clinical Case 1 A patient with a syncope Panos E. Vardas President Elect of the ESC, Prof of Cardiology, University Hospital of Crete
 Clinical Case 1 A patient with a syncope Panos E. Vardas President Elect of the ESC, Prof. of Cardiology, University Hospital of Crete Case presentation A 64-year-old male smoker, with arterial hypertension
Clinical Case 1 A patient with a syncope Panos E. Vardas President Elect of the ESC, Prof. of Cardiology, University Hospital of Crete Case presentation A 64-year-old male smoker, with arterial hypertension
Improving Patient Outcomes with a Syncope Center. Suneet Mittal, MD
 Improving Patient Outcomes with a Syncope Center Suneet Mittal, MD Improving Patient Outcomes with a Syncope Center: Early Risk Stratification of Patients who Require Device Therapy Suneet Mittal, MD Director,
Improving Patient Outcomes with a Syncope Center Suneet Mittal, MD Improving Patient Outcomes with a Syncope Center: Early Risk Stratification of Patients who Require Device Therapy Suneet Mittal, MD Director,
An Approach to the Patient with Syncope. Guy Amit MD, MPH Soroka University Medical Center Beer-Sheva
 An Approach to the Patient with Syncope Guy Amit MD, MPH Soroka University Medical Center Beer-Sheva Case presentation A 23 y.o. man presented with 2 episodes of syncope One during exercise,one at rest
An Approach to the Patient with Syncope Guy Amit MD, MPH Soroka University Medical Center Beer-Sheva Case presentation A 23 y.o. man presented with 2 episodes of syncope One during exercise,one at rest
Valutazione iniziale e stratificazione del rischio
 Valutazione iniziale e stratificazione del rischio Paolo Alboni Sezione di Cardiologia Ospedale Privato Quisisana Ferrara DEFINITION OF SYNCOPE Syncope is a transient loss of consciousness due to global
Valutazione iniziale e stratificazione del rischio Paolo Alboni Sezione di Cardiologia Ospedale Privato Quisisana Ferrara DEFINITION OF SYNCOPE Syncope is a transient loss of consciousness due to global
La strategia diagnostica: il monitoraggio ecg prolungato. Michele Brignole
 La strategia diagnostica: il monitoraggio ecg prolungato Michele Brignole ECG monitoring and syncope In-hospital monitoring Holter Monitoring External loop recorder Remote (at home) telemetry Implantable
La strategia diagnostica: il monitoraggio ecg prolungato Michele Brignole ECG monitoring and syncope In-hospital monitoring Holter Monitoring External loop recorder Remote (at home) telemetry Implantable
Syncope Guidelines What s new? October 19 th 2017 Mohamed Aljaabari MBBCh, FACC, FHRS Consultant Electrophysiologist - Mafraq Hospital
 Syncope Guidelines What s new? October 19 th 2017 Mohamed Aljaabari MBBCh, FACC, FHRS Consultant Electrophysiologist - Mafraq Hospital Case Presentation 35 Male presented with sudden loss of consciousness
Syncope Guidelines What s new? October 19 th 2017 Mohamed Aljaabari MBBCh, FACC, FHRS Consultant Electrophysiologist - Mafraq Hospital Case Presentation 35 Male presented with sudden loss of consciousness
Lee Chee Wan. Senior Consultant Pacing and Cardiac Electrophysiology. GP Symposium 2 nd April 2016
 Lee Chee Wan Senior Consultant Pacing and Cardiac Electrophysiology GP Symposium 2 nd April 2016 Objectives Definition of syncope Common causes of syncope & impacts How to clinically assess patient with
Lee Chee Wan Senior Consultant Pacing and Cardiac Electrophysiology GP Symposium 2 nd April 2016 Objectives Definition of syncope Common causes of syncope & impacts How to clinically assess patient with
Syncope: diagnosis and management according to the 2009 guidelines of the European Society of Cardiology
 REVIEW ARTICLE Syncope: diagnosis and management according to the 2009 guidelines of the European Society of Cardiology Richard Sutton 1, David Benditt 2, Michele Brignole 3, Angel Moya 4 1 Imperial College,
REVIEW ARTICLE Syncope: diagnosis and management according to the 2009 guidelines of the European Society of Cardiology Richard Sutton 1, David Benditt 2, Michele Brignole 3, Angel Moya 4 1 Imperial College,
SYNCOPE. Sanjay P. Singh, MD Chairman & Professor, Department of Neurology. Syncope
 SYNCOPE Sanjay P. Singh, MD Chairman & Professor, Department of Neurology. Syncope Syncope is a clinical syndrome characterized by transient loss of consciousness (TLOC) and postural tone that is most
SYNCOPE Sanjay P. Singh, MD Chairman & Professor, Department of Neurology. Syncope Syncope is a clinical syndrome characterized by transient loss of consciousness (TLOC) and postural tone that is most
Remote Monitoring & the Smart Home of the 21 Century
 Cardiostim EHRA Europace 2016, Nice - June 8-11, 2016 Remote Monitoring & the Smart Home of the 21 Century Antonio Raviele, MD, FESC, FHRS President ALFA -Alliance to Fight Atrial fibrillation- Venezia
Cardiostim EHRA Europace 2016, Nice - June 8-11, 2016 Remote Monitoring & the Smart Home of the 21 Century Antonio Raviele, MD, FESC, FHRS President ALFA -Alliance to Fight Atrial fibrillation- Venezia
13/09/2018. The ISSUE Studies. International (Italy & Spain) Study of Syncope of Uncertain Etiology. ISSUE study Pre-defined inclusion cathegories
 Study of Syncope of Uncertain Etiology. ISSUE study Pre-defined inclusion cathegories") The Studies Jean-Claude Deharo Aix-Marseille Université, France In Cardiac Electrophysiology Methods and Models Editors: Daniel C. Sigg, Paul A. Iaizzo, Yong-Fu Xiao, Bin He Springer 2010 study Pre-defined
The Studies Jean-Claude Deharo Aix-Marseille Université, France In Cardiac Electrophysiology Methods and Models Editors: Daniel C. Sigg, Paul A. Iaizzo, Yong-Fu Xiao, Bin He Springer 2010 study Pre-defined
Diagnostic and therapeutic management of the patient with syncope M. Brignole Arrhythmologic Centre and Syncope Unit Lavagna, Italy
 Diagnostic and therapeutic management of the patient with syncope M. Brignole Arrhythmologic Centre and Syncope Unit Lavagna, Italy Eur Heart J. 2009 Nov;30(21):2631-71 Available on www.escardio.org/guidelines
Diagnostic and therapeutic management of the patient with syncope M. Brignole Arrhythmologic Centre and Syncope Unit Lavagna, Italy Eur Heart J. 2009 Nov;30(21):2631-71 Available on www.escardio.org/guidelines
Orthostatic instability is an important co-factor and trigger of reflex syncope
 Orthostatic instability is an important co-factor and trigger of reflex syncope Artur Fedorowski 1,2, Philippe Burri 2, Steen Juul-Möller 2, and Olle Melander 1,2 1 Lund University, Sweden 2 Skåne University
Orthostatic instability is an important co-factor and trigger of reflex syncope Artur Fedorowski 1,2, Philippe Burri 2, Steen Juul-Möller 2, and Olle Melander 1,2 1 Lund University, Sweden 2 Skåne University
2018 ESC SYNCOPE GUIDELINES SUMMARY
 208 ESC SYNCOPE GUIDELINES SUMMARY NEW GUIDELINES OVERVIEW OF UPDATED RECOMMENDATIONS SINCE 2009 208 EUROPEAN SOCIETY OF CARDIOLOGY SYNCOPE GUIDELINES Goals of 208 Task Force Reducing Cost & Admissions:
208 ESC SYNCOPE GUIDELINES SUMMARY NEW GUIDELINES OVERVIEW OF UPDATED RECOMMENDATIONS SINCE 2009 208 EUROPEAN SOCIETY OF CARDIOLOGY SYNCOPE GUIDELINES Goals of 208 Task Force Reducing Cost & Admissions:
Syncope evaluation: the role of syncope clinics Michele Brignole Arrhythmologic Centre, Lavagna, Italy
 Syncope evaluation: the role of syncope clinics Michele Brignole Arrhythmologic Centre, Lavagna, Italy Why should we need a Syncope Management Unit? We are not happy with current strategies: - not standardized
Syncope evaluation: the role of syncope clinics Michele Brignole Arrhythmologic Centre, Lavagna, Italy Why should we need a Syncope Management Unit? We are not happy with current strategies: - not standardized
Syncope : What tests should I do? Boon Lim Consultant Cardiologist Clinical Lead for Imperial Syncope Unit Hammersmith Hospital
 Syncope : What tests should I do? Boon Lim Consultant Cardiologist Clinical Lead for Imperial Syncope Unit Hammersmith Hospital The most important diagnostic test is History taking Why is history taking
Syncope : What tests should I do? Boon Lim Consultant Cardiologist Clinical Lead for Imperial Syncope Unit Hammersmith Hospital The most important diagnostic test is History taking Why is history taking
C1: Medical Standards for Safety Critical Workers with Cardiovascular Disorders
 C1: Medical Standards for Safety Critical Workers with Cardiovascular Disorders GENERAL ISSUES REGARDING MEDICAL FITNESS-FOR-DUTY 1. These medical standards apply to Union Pacific Railroad (UPRR) employees
C1: Medical Standards for Safety Critical Workers with Cardiovascular Disorders GENERAL ISSUES REGARDING MEDICAL FITNESS-FOR-DUTY 1. These medical standards apply to Union Pacific Railroad (UPRR) employees
DECLARATION OF CONFLICT OF INTEREST
 DECLARATION OF CONFLICT OF INTEREST The Management of Syncope remains a challenge: Clues from the History Richard Sutton, DSc Emeritus Professor of Cardiology Imperial College, St Mary s Hospital, London,
DECLARATION OF CONFLICT OF INTEREST The Management of Syncope remains a challenge: Clues from the History Richard Sutton, DSc Emeritus Professor of Cardiology Imperial College, St Mary s Hospital, London,
Vasovagal Syncope and Bradyarrhythmias Mechanisms, distinguishing cause and effect
 Vasovagal Syncope and Bradyarrhythmias Mechanisms, distinguishing cause and effect Walid Saliba, MD, FHRS, FACC Director EP lab Director Atrial Fibrillation Center Department of Cardiovascular Medicine
Vasovagal Syncope and Bradyarrhythmias Mechanisms, distinguishing cause and effect Walid Saliba, MD, FHRS, FACC Director EP lab Director Atrial Fibrillation Center Department of Cardiovascular Medicine
Disclosures. I have no financial disclosures relevant to the talk
 Syncope Sachin S. Sule, MD, FACP Associate Professor of Integrated Medical Science Division of Medicine Director,Internal Medicine Residency Program Charles E. Schmidt College of Medicine, Florida Atlantic
Syncope Sachin S. Sule, MD, FACP Associate Professor of Integrated Medical Science Division of Medicine Director,Internal Medicine Residency Program Charles E. Schmidt College of Medicine, Florida Atlantic
Transient loss of consciousness
 Issue date: August 2010 Transient loss of consciousness Transient loss of consciousness ( blackouts ) management in adults and young people Developed by the National Clinical Guideline Centre Transient
Issue date: August 2010 Transient loss of consciousness Transient loss of consciousness ( blackouts ) management in adults and young people Developed by the National Clinical Guideline Centre Transient
Neurocardiogenic syncope
 Neurocardiogenic syncope Syncope Definition Collapse,Blackout A sudden, transient loss of consciousness and postural tone, with spontaneous recovery Very common Syncope Prevalence All age groups (particularly
Neurocardiogenic syncope Syncope Definition Collapse,Blackout A sudden, transient loss of consciousness and postural tone, with spontaneous recovery Very common Syncope Prevalence All age groups (particularly
Clinical Evaluation & Management of Syncope:UPDATE
 Clinical Evaluation & Management of Syncope:UPDATE 2017 ACC/AHA/HRS Guideline for the Evaluation and Management of Patients With Syncope Developed in Collaboration with the American College of Emergency
Clinical Evaluation & Management of Syncope:UPDATE 2017 ACC/AHA/HRS Guideline for the Evaluation and Management of Patients With Syncope Developed in Collaboration with the American College of Emergency
Il massaggio del seno carotideo Roberto Maggi Centro Aritmologico e Syncope Unit Lavagna, Italia
 Il massaggio del seno carotideo Roberto Maggi Centro Aritmologico e Syncope Unit Lavagna, Italia Tigullio Cardiologia, 7 aprile 2016 Carotid sinus hypersensitivity Vagus nerve Glossopharyngeal nerve Carotid
Il massaggio del seno carotideo Roberto Maggi Centro Aritmologico e Syncope Unit Lavagna, Italia Tigullio Cardiologia, 7 aprile 2016 Carotid sinus hypersensitivity Vagus nerve Glossopharyngeal nerve Carotid
13/09/2018. Reflex syncope Diagnosis and treatment. Classification. ficat Reflex (neurally
 Classification TLOC Diagnosis and treatment Jean-Claude Deharo Aix-Marseille Université, France Nontraumatic TLOC Syncope Epileptic seizures TLOC due to head trauma Psychogenic Tonic-clonic seizures Psychogenic
Classification TLOC Diagnosis and treatment Jean-Claude Deharo Aix-Marseille Université, France Nontraumatic TLOC Syncope Epileptic seizures TLOC due to head trauma Psychogenic Tonic-clonic seizures Psychogenic
Tilt Table Testing MM /01/2015. HMO; PPO; QUEST Integration 09/22/2017 Section: Medicine Place(s) of Service: Office, Outpatient
 of Service: Office, Outpatient") Tilt Table Testing Policy Number: Original Effective Date: MM.02.024 01/01/2015 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 09/22/2017 Section: Medicine Place(s) of Service:
Tilt Table Testing Policy Number: Original Effective Date: MM.02.024 01/01/2015 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 09/22/2017 Section: Medicine Place(s) of Service:
Sequoia Heart Symposium 2018: Syncope. Gregory Engel, MD
 Sequoia Heart Symposium 2018: Syncope Gregory Engel, MD Silicon Valley Cardiology Palo Alto Medical Foundation Sutter Health Palo Alto, Redwood City, and San Carlos, CA Chief, Cardiovascular Division Sequoia
Sequoia Heart Symposium 2018: Syncope Gregory Engel, MD Silicon Valley Cardiology Palo Alto Medical Foundation Sutter Health Palo Alto, Redwood City, and San Carlos, CA Chief, Cardiovascular Division Sequoia
Rhythm Control: Is There a Role for the PCP? Blake Norris, MD, FACC BHHI Primary Care Symposium February 28, 2014
 Rhythm Control: Is There a Role for the PCP? Blake Norris, MD, FACC BHHI Primary Care Symposium February 28, 2014 Financial disclosures Consultant Medtronic 3 reasons to evaluate and treat arrhythmias
Rhythm Control: Is There a Role for the PCP? Blake Norris, MD, FACC BHHI Primary Care Symposium February 28, 2014 Financial disclosures Consultant Medtronic 3 reasons to evaluate and treat arrhythmias
Faculty Disclosure. Sanjay P. Singh, MD, FAAN. Dr. Singh has listed an affiliation with: Consultant Sun Pharma Speaker s Bureau Lundbeck, Sunovion
 Faculty Disclosure Sanjay P. Singh, MD, FAAN Dr. Singh has listed an affiliation with: Consultant Sun Pharma Speaker s Bureau Lundbeck, Sunovion however, no conflict of interest exists for this conference.
Faculty Disclosure Sanjay P. Singh, MD, FAAN Dr. Singh has listed an affiliation with: Consultant Sun Pharma Speaker s Bureau Lundbeck, Sunovion however, no conflict of interest exists for this conference.
APPENDIX D1 - CHARACTERISTICS OF INCLUDED STUDIES
 APPENDIX D1 - CHARACTERISTICS OF INCLUDED STUDIES 1 Initial Assessment included studies table... 3 1.1 Initial symptoms for diagnosis review... 3 1.2 Decision rules for diagnosis review... 8 1.3 Initial
APPENDIX D1 - CHARACTERISTICS OF INCLUDED STUDIES 1 Initial Assessment included studies table... 3 1.1 Initial symptoms for diagnosis review... 3 1.2 Decision rules for diagnosis review... 8 1.3 Initial
Syncope is a clinical syndrome characterized by transient. Management of Syncope in Adults: An Update
 SYMPOSIUM MANAGEMENT OF SYNCOPE ON CARDIOVASCULAR DISEASES Management of Syncope in Adults: An Update LIN Y. CHEN, MD; DAVID G. BENDITT, MD; AND WIN-KUANG SHEN, MD Syncope is a clinical syndrome characterized
SYMPOSIUM MANAGEMENT OF SYNCOPE ON CARDIOVASCULAR DISEASES Management of Syncope in Adults: An Update LIN Y. CHEN, MD; DAVID G. BENDITT, MD; AND WIN-KUANG SHEN, MD Syncope is a clinical syndrome characterized
Rapid Access Clinics for Transient Loss of Consciousness
 Rapid Access Clinics for Transient Loss of Consciousness Michael Gammage Department of Cardiovascular Medicine University of Birmingham and University Hospital Birmingham NHS Foundation Trust Those who
Rapid Access Clinics for Transient Loss of Consciousness Michael Gammage Department of Cardiovascular Medicine University of Birmingham and University Hospital Birmingham NHS Foundation Trust Those who
Guidelines Pediatric Congenital Heart Disease SYNCOPE
 Guidelines Pediatric Congenital Heart Disease SYNCOPE www.kinderkardiologie.org/dgpkleitlinien.shtm Definition and Characteristics of Syncope temporary loss of consciousness and tonicity due to inadequate
Guidelines Pediatric Congenital Heart Disease SYNCOPE www.kinderkardiologie.org/dgpkleitlinien.shtm Definition and Characteristics of Syncope temporary loss of consciousness and tonicity due to inadequate
Applying Syncope Guidelines to Clinical Practice
 Applying Syncope Guidelines to Clinical Practice ACC Rockies February 27, 2018 Roopinder K Sandhu Associate Professor of Medicine U of A Director of Edmonton Cardiac Arrhythmia Trials Research Group Visiting
Applying Syncope Guidelines to Clinical Practice ACC Rockies February 27, 2018 Roopinder K Sandhu Associate Professor of Medicine U of A Director of Edmonton Cardiac Arrhythmia Trials Research Group Visiting
Indications for Permanent Pacing Joe Gallinghouse, M.D. Texas Cardiac Arrhythmia Austin, Texas
 Indications for Permanent Pacing Joe Gallinghouse, M.D. Texas Cardiac Arrhythmia Austin, Texas Remember the Suture! Impulse Formation and Conduction Disturbances Cardiac Electrical Anatomy Sinoatrial Node
Indications for Permanent Pacing Joe Gallinghouse, M.D. Texas Cardiac Arrhythmia Austin, Texas Remember the Suture! Impulse Formation and Conduction Disturbances Cardiac Electrical Anatomy Sinoatrial Node
Value of the implantable loop recorder for the management of patients with unexplained syncope
 Europace (2004) 6, 70e76 Value of the implantable loop recorder for the management of patients with unexplained syncope Lucas Boersma a, ), Lluís Mont b, Alessandro Sionis b, Emilio García b, Josep Brugada
Europace (2004) 6, 70e76 Value of the implantable loop recorder for the management of patients with unexplained syncope Lucas Boersma a, ), Lluís Mont b, Alessandro Sionis b, Emilio García b, Josep Brugada
Seek and Ye Shall Find: Surprising Findings When Using the ILR-LINQ
 Seek and Ye Shall Find: Surprising Findings When Using the ILR-LINQ Suneet Mittal, MD, FACC, FHRS Director, Electrophysiology Laboratory Valley Health System www.arrhythmia.org; @drsuneet October 31, 2015
Seek and Ye Shall Find: Surprising Findings When Using the ILR-LINQ Suneet Mittal, MD, FACC, FHRS Director, Electrophysiology Laboratory Valley Health System www.arrhythmia.org; @drsuneet October 31, 2015
Department of Paediatrics Clinical Guideline. Syncope Guideline
 Department of Paediatrics Clinical Guideline Syncope Guideline Definition Transient, self-limited loss of consciousness (TLOC), usually leading to falling. Onset is relatively rapid. Recovery is spontaneous,
Department of Paediatrics Clinical Guideline Syncope Guideline Definition Transient, self-limited loss of consciousness (TLOC), usually leading to falling. Onset is relatively rapid. Recovery is spontaneous,
I. Choudhuri, D. Krum, A. Agarwal, J. Hare, M. Belohlavek, A. Ahmad, M. Pinninti, B. Khandheria
 Vasovagal Syncope: Diagnostic Issues Familial Neurally Mediated Syncope I. Choudhuri, D. Krum, A. Agarwal, J. Hare, M. Belohlavek, A. Ahmad, M. Pinninti, B. Khandheria Aurora St. Luke s Medical Center
Vasovagal Syncope: Diagnostic Issues Familial Neurally Mediated Syncope I. Choudhuri, D. Krum, A. Agarwal, J. Hare, M. Belohlavek, A. Ahmad, M. Pinninti, B. Khandheria Aurora St. Luke s Medical Center
Presentation of transient loss of consciousness
 Presentation of transient loss of consciousness Definition of transient loss of consciousness Transient loss of consciousness: sudden onset, complete loss of consciousness of brief duration with relatively
Presentation of transient loss of consciousness Definition of transient loss of consciousness Transient loss of consciousness: sudden onset, complete loss of consciousness of brief duration with relatively
Section Editor Leonard I Ganz, MD, FHRS, FACC
 1 of 12 9/29/2013 6:53 PM Official reprint from UpToDate www.uptodate.com 2013 UpToDate The content on the UpToDate website is not intended nor recommended as a substitute for medical advice, diagnosis,
1 of 12 9/29/2013 6:53 PM Official reprint from UpToDate www.uptodate.com 2013 UpToDate The content on the UpToDate website is not intended nor recommended as a substitute for medical advice, diagnosis,
Cardiology Updates: Syncope and Stress Testing. Kathleen Morris, DO Cardiology Fellow St. Vincent Hospital
 Cardiology Updates: Syncope and Stress Testing Kathleen Morris, DO Cardiology Fellow St. Vincent Hospital Disclosures NONE PART ONE: Let s start with SYNCOPE Objectives: Definition of Syncope Brief review
Cardiology Updates: Syncope and Stress Testing Kathleen Morris, DO Cardiology Fellow St. Vincent Hospital Disclosures NONE PART ONE: Let s start with SYNCOPE Objectives: Definition of Syncope Brief review
National Coverage Determination (NCD) for Cardiac Pacemakers (20.8)
 for Cardiac Pacemakers (20.8)") Page 1 of 12 Centers for Medicare & Medicaid Services National Coverage Determination (NCD) for Cardiac Pacemakers (20.8) Tracking Information Publication Number 100-3 Manual Section Number 20.8 Manual
Page 1 of 12 Centers for Medicare & Medicaid Services National Coverage Determination (NCD) for Cardiac Pacemakers (20.8) Tracking Information Publication Number 100-3 Manual Section Number 20.8 Manual
Tilt training EM R1 송진우
 Tilt training 2006.7.15. EM R1 송진우 Introduction North American Vasovagal Pacemaker Study Randomized, controlled trial Reduction in the likelihood of syncope by dual chamber pacing with rate drop response
Tilt training 2006.7.15. EM R1 송진우 Introduction North American Vasovagal Pacemaker Study Randomized, controlled trial Reduction in the likelihood of syncope by dual chamber pacing with rate drop response
Stepwise Evaluation of Unexplained Syncope in a Large Ambulatory Population
 Stepwise Evaluation of Unexplained Syncope in a Large Ambulatory Population JUAN F. IGLESIAS, M.D., DENIS GRAF, M.D., ANDREI FORCLAZ, M.D., JUERG SCHLAEPFER, M.D., MARTIN FROMER, M.D., and ETIENNE PRUVOT,
Stepwise Evaluation of Unexplained Syncope in a Large Ambulatory Population JUAN F. IGLESIAS, M.D., DENIS GRAF, M.D., ANDREI FORCLAZ, M.D., JUERG SCHLAEPFER, M.D., MARTIN FROMER, M.D., and ETIENNE PRUVOT,
Cardiac Implanted Electronic Devices Pacemakers, Defibrillators, Cardiac Resynchronization Devices, Loop Recorders, etc.
 Cardiac Implanted Electronic Devices Pacemakers, Defibrillators, Cardiac Resynchronization Devices, Loop Recorders, etc. The Miracle of Living February 21, 2018 Matthew Ostrom MD,FACC,FHRS Division of
Cardiac Implanted Electronic Devices Pacemakers, Defibrillators, Cardiac Resynchronization Devices, Loop Recorders, etc. The Miracle of Living February 21, 2018 Matthew Ostrom MD,FACC,FHRS Division of
Part 1. The initial evaluation of patients with syncope
 Europace (2001) 3, 253 260 doi:10.1053/eupc.2001.0190, available online at http://www.idealibrary.com on TASK FORCE ON SYNCOPE, EUROPEAN SOCIETY OF CARDIOLOGY Part 1. The initial evaluation of patients
Europace (2001) 3, 253 260 doi:10.1053/eupc.2001.0190, available online at http://www.idealibrary.com on TASK FORCE ON SYNCOPE, EUROPEAN SOCIETY OF CARDIOLOGY Part 1. The initial evaluation of patients
CLINICAL CARDIAC ELECTROPHYSIOLOGY Maintenance of Certification (MOC) Examination Blueprint
 Examination Blueprint") CLINICAL CARDIAC ELECTROPHYSIOLOGY Maintenance of Certification (MOC) Examination Blueprint ABIM invites diplomates to help develop the Clinical Cardiac Electrophysiology MOC exam blueprint Based on feedback
CLINICAL CARDIAC ELECTROPHYSIOLOGY Maintenance of Certification (MOC) Examination Blueprint ABIM invites diplomates to help develop the Clinical Cardiac Electrophysiology MOC exam blueprint Based on feedback
Clinical Policy: Holter Monitors Reference Number: CP.MP.113
 Clinical Policy: Reference Number: CP.MP.113 Effective Date: 05/18 Last Review Date: 04/18 Coding Implications Revision Log Description Ambulatory electrocardiogram (ECG) monitoring provides a view of
Clinical Policy: Reference Number: CP.MP.113 Effective Date: 05/18 Last Review Date: 04/18 Coding Implications Revision Log Description Ambulatory electrocardiogram (ECG) monitoring provides a view of
Clinical Cardiac Electrophysiology
 Clinical Cardiac Electrophysiology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of
Clinical Cardiac Electrophysiology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of
Ambulatory Cardiac Monitors and Outpatient Telemetry Corporate Medical Policy
 Ambulatory Cardiac Monitors and Outpatient Telemetry Corporate Medical Policy File Name: Ambulatory Event Monitors and Mobile Cardiac Outpatient Telemetry File Code: UM.SPSVC.13 Origination: 10/2015 Last
Ambulatory Cardiac Monitors and Outpatient Telemetry Corporate Medical Policy File Name: Ambulatory Event Monitors and Mobile Cardiac Outpatient Telemetry File Code: UM.SPSVC.13 Origination: 10/2015 Last
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Implantable cardioverter defibrillators for the treatment of arrhythmias and cardiac resynchronisation therapy for the treatment of heart failure (review
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Implantable cardioverter defibrillators for the treatment of arrhythmias and cardiac resynchronisation therapy for the treatment of heart failure (review
June 8, 2018, London UK TREATMENT OF VASOVAGAL SYNCOPE
 June 8, 2018, London UK TREATMENT OF VASOVAGAL SYNCOPE Where to go for help Syncope: HRS Definition Syncope is defined as: a transient loss of consciousness, associated with an inability to maintain postural
June 8, 2018, London UK TREATMENT OF VASOVAGAL SYNCOPE Where to go for help Syncope: HRS Definition Syncope is defined as: a transient loss of consciousness, associated with an inability to maintain postural
Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: WPW Revised: 11/2013
 Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: WPW Revised: 11/2013 Wolff-Parkinson-White syndrome (WPW) is a syndrome of pre-excitation of the
Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: WPW Revised: 11/2013 Wolff-Parkinson-White syndrome (WPW) is a syndrome of pre-excitation of the
Evaluation of Dizziness and Fainting in Children and Adolescents
 Evaluation of Dizziness and Fainting in Children and Adolescents Collin Cowley, MD - Pediatric Cardiology Lynne Kerr, MD, PhD Pediatric Neurology Chuck Norlin, MD General Pediatrics Bettina Smith Edmondson,
Evaluation of Dizziness and Fainting in Children and Adolescents Collin Cowley, MD - Pediatric Cardiology Lynne Kerr, MD, PhD Pediatric Neurology Chuck Norlin, MD General Pediatrics Bettina Smith Edmondson,
Syncope: The Pediatric Patient
 Syncope: The Pediatric Patient Lindsey Malloy-Walton, DO, MPH, FAAP Division of Pediatric Cardiology Children s Mercy Hospital 2401 Gillham Road Kansas City, MO 64108 Phone (office): 816-234-3255 Email:
Syncope: The Pediatric Patient Lindsey Malloy-Walton, DO, MPH, FAAP Division of Pediatric Cardiology Children s Mercy Hospital 2401 Gillham Road Kansas City, MO 64108 Phone (office): 816-234-3255 Email:
Research Article Recurrent Syncope in Patients with Carotid Sinus Hypersensitivity
 International Scholarly Research Network ISRN Cardiology Volume 2012, Article ID 216206, 5 pages doi:10.5402/2012/216206 Research Article Recurrent Syncope in Patients with Carotid Sinus Hypersensitivity
International Scholarly Research Network ISRN Cardiology Volume 2012, Article ID 216206, 5 pages doi:10.5402/2012/216206 Research Article Recurrent Syncope in Patients with Carotid Sinus Hypersensitivity
Guidelines on Management (Diagnosis and Treatment) of Syncope Update 2004 q Executive Summary
 of Syncope Update 2004 q Executive Summary") European Heart Journal (2004) 25, 2054 2072 ESC Guidelines Guidelines on Management ( and Treatment) of Syncope Update 2004 q Executive Summary The Task Force on Syncope, European Society of Cardiology
European Heart Journal (2004) 25, 2054 2072 ESC Guidelines Guidelines on Management ( and Treatment) of Syncope Update 2004 q Executive Summary The Task Force on Syncope, European Society of Cardiology
InterQual Care Planning SIM plus Criteria 2014 Clinical Revisions
 InterQual Care Planning SIM plus Criteria 2014 Clinical Revisions The Clinical Revisions provide details of changes to InterQual Clinical Criteria. They do not provide information on changes made to CareEnhance
InterQual Care Planning SIM plus Criteria 2014 Clinical Revisions The Clinical Revisions provide details of changes to InterQual Clinical Criteria. They do not provide information on changes made to CareEnhance
UNIVERSITY HOSPITALS OF LEICESTER NHS TRUST CARDIAC INVESTIGATIONS PAEDIATRIC & CONGENITAL SYNCOPE INVESTIGATIONS/QUESTIONNAIRE PROTOCOL
 UNIVERSITY HOSPITALS OF LEICESTER NHS TRUST CARDIAC INVESTIGATIONS PAEDIATRIC & CONGENITAL SYNCOPE INVESTIGATIONS/QUESTIONNAIRE PROTOCOL Written Date: 2009 by Dr Duke, then updated by Dr Sarita Makam 12/4/2016
UNIVERSITY HOSPITALS OF LEICESTER NHS TRUST CARDIAC INVESTIGATIONS PAEDIATRIC & CONGENITAL SYNCOPE INVESTIGATIONS/QUESTIONNAIRE PROTOCOL Written Date: 2009 by Dr Duke, then updated by Dr Sarita Makam 12/4/2016
Syncope: Causes and Treatment
 March 01, 2006 By Avery Hayes, MD [1] and Mahendr S. Kochar, MD, MS [2] Because the causes of syncope are numerous and the diagnostic tests have low yield, this disorder is often difficult to evaluate.
March 01, 2006 By Avery Hayes, MD [1] and Mahendr S. Kochar, MD, MS [2] Because the causes of syncope are numerous and the diagnostic tests have low yield, this disorder is often difficult to evaluate.
Emergency Department Guidelines COLLAPSE? CAUSE / SYNCOPE. Version x (x 201x) Review date: x 2014 Page 1 of 5
 Review date: x 2014 Page 1 of 5") COLLAPSE? CAUSE / SYNCOPE Review date: x 2014 Page 1 of 5 KEY POINTS: Do not use this guideline for mechanical falls Definition: Syncope is a transient loss of consciousness with an inability to maintain
COLLAPSE? CAUSE / SYNCOPE Review date: x 2014 Page 1 of 5 KEY POINTS: Do not use this guideline for mechanical falls Definition: Syncope is a transient loss of consciousness with an inability to maintain
Medicine Dr. Aso Lecture 9 Syncope and Pre-syncope
 Medicine Dr. Aso Lecture 9 Syncope and Pre-syncope SYNCOPE AND PRE-SYNCOPE Syncope:- sudden, transient loss of consciousness, due to reduced cerebral perfusion. The patient is unresponsive with loss of
Medicine Dr. Aso Lecture 9 Syncope and Pre-syncope SYNCOPE AND PRE-SYNCOPE Syncope:- sudden, transient loss of consciousness, due to reduced cerebral perfusion. The patient is unresponsive with loss of
Pediatrics. Arrhythmias in Children: Bradycardia and Tachycardia Diagnosis and Treatment. Overview
 Pediatrics Arrhythmias in Children: Bradycardia and Tachycardia Diagnosis and Treatment See online here The most common form of cardiac arrhythmia in children is sinus tachycardia which can be caused by
Pediatrics Arrhythmias in Children: Bradycardia and Tachycardia Diagnosis and Treatment See online here The most common form of cardiac arrhythmia in children is sinus tachycardia which can be caused by
Medical Conditions, Sudden Incapacitation and Assessing Syncope & Unexplained Loss of Consciousness
 Medical Conditions, Sudden Incapacitation and Assessing Syncope & Unexplained Loss of Consciousness Kurt T. Hegmann, MD, MPH Professor and Center Director Dr. Paul S. Richards Endowed Chair in Occupational
Medical Conditions, Sudden Incapacitation and Assessing Syncope & Unexplained Loss of Consciousness Kurt T. Hegmann, MD, MPH Professor and Center Director Dr. Paul S. Richards Endowed Chair in Occupational
IHCP bulletin INDIANA HEALTH COVERAGE PROGRAMS BT JANUARY 24, 2012
 IHCP bulletin INDIANA HEALTH COVERAGE PROGRAMS BT201203 JANUARY 24, 2012 The IHCP to reimburse implantable cardioverter defibrillators separately from outpatient implantation Effective March 1, 2012, the
IHCP bulletin INDIANA HEALTH COVERAGE PROGRAMS BT201203 JANUARY 24, 2012 The IHCP to reimburse implantable cardioverter defibrillators separately from outpatient implantation Effective March 1, 2012, the
Vasovagal syncope in 2016: the current state of the faint
 Interventional Cardiology Vasovagal syncope in 2016: the current state of the faint In this article, we will review the challenges in defining syncope and the evolution of its definition over the past
Interventional Cardiology Vasovagal syncope in 2016: the current state of the faint In this article, we will review the challenges in defining syncope and the evolution of its definition over the past
TLOC - What are the red flags? John Dean March 2018
 TLOC - What are the red flags? John Dean March 2018 What is TLOC? Transient loss of consciousness It is very common It accounts for 5% of ED attendances It accounts for 6% of hospital admissions It consumes
TLOC - What are the red flags? John Dean March 2018 What is TLOC? Transient loss of consciousness It is very common It accounts for 5% of ED attendances It accounts for 6% of hospital admissions It consumes
Adult with transient loss of consciousness faints, fits and funny turns
 Adult with transient loss of consciousness faints, fits and funny turns Introduction Problem-specific video guides to diagnosing patients and helping them with management and prevention to transient loss
Adult with transient loss of consciousness faints, fits and funny turns Introduction Problem-specific video guides to diagnosing patients and helping them with management and prevention to transient loss
APPENDIX D1 - CHARACTERISTICS OF INCLUDED STUDIES APPENDIX D1 - CHARACTERISTICS OF INCLUDED STUDIES... 1
 APPENDIX D1 - CHARACTERISTICS OF INCLUDED STUDIES APPENDIX D1 - CHARACTERISTICS OF INCLUDED STUDIES... 1 1 Initial Assessment included studies table... 3 1.1 Initial symptoms for diagnosis review... 3
APPENDIX D1 - CHARACTERISTICS OF INCLUDED STUDIES APPENDIX D1 - CHARACTERISTICS OF INCLUDED STUDIES... 1 1 Initial Assessment included studies table... 3 1.1 Initial symptoms for diagnosis review... 3
Bradycardia and Syncope. P Boon Lim, MB BChir PhD Imperial College Healthcare London, UK
 Bradycardia and Syncope P Boon Lim, MB BChir PhD Imperial College Healthcare London, UK Disclosures Medtronic: Research Grant Boston Scientific: Consulting Fee, Research Grant Biosense Webster: Consulting
Bradycardia and Syncope P Boon Lim, MB BChir PhD Imperial College Healthcare London, UK Disclosures Medtronic: Research Grant Boston Scientific: Consulting Fee, Research Grant Biosense Webster: Consulting
Role of Implantable Loop Recorder in the Evaluation of Syncope
 Role of Implantable Loop Recorder in the Evaluation of Syncope June Soo Kim, M.D., Ph.D. Department of Medicine Cardiac & Vascular Center Sungkyunkwan University School of Medicine Definition & Mechanism
Role of Implantable Loop Recorder in the Evaluation of Syncope June Soo Kim, M.D., Ph.D. Department of Medicine Cardiac & Vascular Center Sungkyunkwan University School of Medicine Definition & Mechanism
S yncope is a common and difficult clinical problem with
 363 CARDIOVASCULAR MEDICINE Role of echocardiography in the evaluation of syncope: a prospective study F P Sarasin, A-F Junod, D Carballo, S Slama, P-F Unger, M Louis-Simonet... See end of article for
363 CARDIOVASCULAR MEDICINE Role of echocardiography in the evaluation of syncope: a prospective study F P Sarasin, A-F Junod, D Carballo, S Slama, P-F Unger, M Louis-Simonet... See end of article for
Syncope. Erica Flores, PGY-5
 Syncope Erica Flores, PGY-5 Learning Objectives Recognize the different etiologies of patients presenting with syncope Describe appropriate testing and management of patients presenting with syncope Syncope
Syncope Erica Flores, PGY-5 Learning Objectives Recognize the different etiologies of patients presenting with syncope Describe appropriate testing and management of patients presenting with syncope Syncope
POSTURAL ORTHOSTATIC TACHYCARDIA SYNDROME (POTS) IT S NOT THAT SIMPLE
 IT S NOT THAT SIMPLE") POSTURAL ORTHOSTATIC TACHYCARDIA SYNDROME (POTS) IT S NOT THAT SIMPLE POTS Irritable heart syndrome. Soldier s heart. Effort syndrome. Vasoregulatory asthenia. Neurocirculatory asthenia. Anxiety neurosis.
POSTURAL ORTHOSTATIC TACHYCARDIA SYNDROME (POTS) IT S NOT THAT SIMPLE POTS Irritable heart syndrome. Soldier s heart. Effort syndrome. Vasoregulatory asthenia. Neurocirculatory asthenia. Anxiety neurosis.
Research Article Cerebral Blood Flow, Heart Rate, and Blood Pressure Patterns during the Tilt Test in Common Orthostatic Syndromes
 Neuroscience Journal Volume 216, Article ID 612734, 2 pages http://dx.doi.org/1.1155/216/612734 Research Article Cerebral Blood Flow, Heart Rate, and Blood Pressure Patterns during the Test in Common Orthostatic
Neuroscience Journal Volume 216, Article ID 612734, 2 pages http://dx.doi.org/1.1155/216/612734 Research Article Cerebral Blood Flow, Heart Rate, and Blood Pressure Patterns during the Test in Common Orthostatic
Syncope in ED-Risk Stratification Ger McMahon
 Syncope in ED-Risk Stratification Ger McMahon 3-8% of ED presentations increasing with advancing age ED physicians ranked syncope as the 2 nd most common decision making dilemma >50% are admitted @ 75%
Syncope in ED-Risk Stratification Ger McMahon 3-8% of ED presentations increasing with advancing age ED physicians ranked syncope as the 2 nd most common decision making dilemma >50% are admitted @ 75%
CURRICULUM GOALS AND OBJECTIVES CLINICAL CARDIOVASCULAR ELECTROPHYSIOLOGY TRAINING PROGRAM. University of Florida Gainesville, Florida
 CURRICULUM GOALS AND OBJECTIVES CLINICAL CARDIOVASCULAR ELECTROPHYSIOLOGY TRAINING PROGRAM University of Florida Gainesville, Florida 1. Mission Statement To achieve excellence in the training of fourth
CURRICULUM GOALS AND OBJECTIVES CLINICAL CARDIOVASCULAR ELECTROPHYSIOLOGY TRAINING PROGRAM University of Florida Gainesville, Florida 1. Mission Statement To achieve excellence in the training of fourth
Clinical guideline Published: 25 August 2010 nice.org.uk/guidance/cg109
 Transient loss of consciousness ('blackouts') in over 16s Clinical guideline Published: 25 August 2010 nice.org.uk/guidance/cg109 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Transient loss of consciousness ('blackouts') in over 16s Clinical guideline Published: 25 August 2010 nice.org.uk/guidance/cg109 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
PERMANENT PACEMAKERS AND IMPLANTABLE DEFIBRILLATORS Considerations for intensivists
 PERMANENT PACEMAKERS AND IMPLANTABLE DEFIBRILLATORS Considerations for intensivists Craig A. McPherson, MD, FACC Associate Professor of Medicine Constantine Manthous, MD, FACP, FCCP Associate Clinical
PERMANENT PACEMAKERS AND IMPLANTABLE DEFIBRILLATORS Considerations for intensivists Craig A. McPherson, MD, FACC Associate Professor of Medicine Constantine Manthous, MD, FACP, FCCP Associate Clinical
NICE Action Plan 6/13 Transient loss of consciousness ('blackouts') management in adults and young people NICE CG 109 December 2013
 management in adults and young people NICE CG 109 December 2013") NICE Action Plan 6/13 Transient loss of consciousness ('blackouts') management in adults and young people NICE CG 109 December 2013 Title: Prepared by: Presented by: Main aim: Recommendations: Previous
NICE Action Plan 6/13 Transient loss of consciousness ('blackouts') management in adults and young people NICE CG 109 December 2013 Title: Prepared by: Presented by: Main aim: Recommendations: Previous
Incidence, Clinical Presentation. and Outcome in Patients with Long. Asystole Induced by Head-up Tilt Test
 2005 16 134-138 Incidence, Clinical Presentation and Outcome in Patients with Long Asystole Induced by Head-up Tilt Test Ming-Ting Chou, Chen-Chuan Cheng, Wen-Shiann Wu, and Tseui-Yuen Huang Division of
2005 16 134-138 Incidence, Clinical Presentation and Outcome in Patients with Long Asystole Induced by Head-up Tilt Test Ming-Ting Chou, Chen-Chuan Cheng, Wen-Shiann Wu, and Tseui-Yuen Huang Division of
Syncope (From a Cardiologist s Perspective) Patrick Henderson, DO 118 th OOA Annual Convention Internal Medicine Specialty Track April 28 th, 2018
 Patrick Henderson, DO 118 th OOA Annual Convention Internal Medicine Specialty Track April 28 th, 2018") Syncope (From a Cardiologist s Perspective) Patrick Henderson, DO 118 th OOA Annual Convention Internal Medicine Specialty Track April 28 th, 2018 No financial disclosures to report Goals Formally define
Syncope (From a Cardiologist s Perspective) Patrick Henderson, DO 118 th OOA Annual Convention Internal Medicine Specialty Track April 28 th, 2018 No financial disclosures to report Goals Formally define
Sincope e bradicardia sinusale: quale è la terapia appropriata?
 Sincope e bradicardia sinusale: quale è la terapia appropriata? Paolo Alboni, Key points: 1 Fisiopatologia della sincope nei pz con BS 2 Diagnosi del tipo of sincope nei pz con BS 3 Trattamento della syncope
Sincope e bradicardia sinusale: quale è la terapia appropriata? Paolo Alboni, Key points: 1 Fisiopatologia della sincope nei pz con BS 2 Diagnosi del tipo of sincope nei pz con BS 3 Trattamento della syncope
2017 ACC/AHA/HRS SYNCOPE GUIDELINES
 2017 ACC/AHA/HRS SYNCOPE GUIDELINES 2017 ACC/AHA/HRS Guideline for the Evaluation and Management of Patients With Syncope A Report of the American College of Cardiology/American Heart Association Task
2017 ACC/AHA/HRS SYNCOPE GUIDELINES 2017 ACC/AHA/HRS Guideline for the Evaluation and Management of Patients With Syncope A Report of the American College of Cardiology/American Heart Association Task
Value Of Prodromal Signs And Symptoms In The Differential Diagnosis Of Cardiogenic And Neurogenic Syncope
 Value Of Prodromal Signs And Symptoms In The Differential Diagnosis Of Cardiogenic And Neurogenic Syncope P.J. Stryjewski, B. Nessler, A. Kuczaj, E. Nowalany-Kozielska, J. Nessler 1 Cardiology Department,
Value Of Prodromal Signs And Symptoms In The Differential Diagnosis Of Cardiogenic And Neurogenic Syncope P.J. Stryjewski, B. Nessler, A. Kuczaj, E. Nowalany-Kozielska, J. Nessler 1 Cardiology Department,
Arrhythmia Management Joshua M. Cooper, MD, FHRS, FACC
 Arrhythmia Management Joshua M. Cooper, MD, FHRS, FACC Professor of Medicine Director of Cardiac Electrophysiology Temple University Health System Plumbing Electrical System Bradyarrhythmias Sinus Node
Arrhythmia Management Joshua M. Cooper, MD, FHRS, FACC Professor of Medicine Director of Cardiac Electrophysiology Temple University Health System Plumbing Electrical System Bradyarrhythmias Sinus Node
as the cause of recurrent syncope 3 allows appropriate management aimed
 Case Report Hellenic J Cardiol 2009; 50: 155-159 The Role of the Implantable Loop Recorder in the Investigation of Recurrent Syncope SKEVOS K. SIDERIS 1, TERESA A. MOUSIAMA 1, PAVLOS N. STOUGIANNOS 1,
Case Report Hellenic J Cardiol 2009; 50: 155-159 The Role of the Implantable Loop Recorder in the Investigation of Recurrent Syncope SKEVOS K. SIDERIS 1, TERESA A. MOUSIAMA 1, PAVLOS N. STOUGIANNOS 1,
Patient Resources: Arrhythmias and Congenital Heart Disease
 Patient Resources: Arrhythmias and Congenital Heart Disease Overview Arrhythmias (abnormal heart rhythms) can develop in patients with congenital heart disease (CHD) due to thickening/weakening of their
Patient Resources: Arrhythmias and Congenital Heart Disease Overview Arrhythmias (abnormal heart rhythms) can develop in patients with congenital heart disease (CHD) due to thickening/weakening of their
CLINICAL MEDICAL POLICY
 Policy Name: Policy Number: Responsible Department(s): CLINICAL MEDICAL POLICY Single-use Ambulatory Electrocardiographic Monitors (e.g., Zio Patch) MP-076-MD-DE Medical Management Provider Notice Date:
Policy Name: Policy Number: Responsible Department(s): CLINICAL MEDICAL POLICY Single-use Ambulatory Electrocardiographic Monitors (e.g., Zio Patch) MP-076-MD-DE Medical Management Provider Notice Date:
Cardiac Event Monitors
 Last Review Date: July 14, 2017 Number: MG.MM.DM.18aCv2 Medical Guideline Disclaimer Property of EmblemHealth. All rights reserved. The treating physician or primary care provider must submit to EmblemHealth
Last Review Date: July 14, 2017 Number: MG.MM.DM.18aCv2 Medical Guideline Disclaimer Property of EmblemHealth. All rights reserved. The treating physician or primary care provider must submit to EmblemHealth