Acute Coronary Syndromes: Challenges to Management. Claire Williams November 2017
|
|
|
- Clement Walters
- 5 years ago
- Views:
Transcription

1 Acute Coronary Syndromes: Challenges to Management Claire Williams November 2017




2 Challenge 1: Diagnosis Chest pain >20 minutes ECG
3 Challenge 1: Diagnosis Treat as STEMI Chest pain >20 minutes ECG
4 STEMI - management Direct paramedic transfer to PPCI centre DGH attenders transferred to PPCI centre Exclusions: Overriding comorbidity Terminal cancer Severe dementia Ventilated patients LBBB/paced rhythm NB: exclusion from PPCI protocol does not preclude discussion with PPCI centre
5

6

7 PPCI access challenges Geography Public education - dial 999 not attend A&E Ambulance availability for PPCI transfer from DGH
8 Challenge 1: Diagnosis Treat as STEMI Chest pain >20 minutes ECG History Examination Biomarkers Repeat ECG

9 Clinical presentation Typical: Prolonged chest pain (> 20 mins) New onset severe CCS III angina Destabilisation of stable angina to CCS III Atypical: Epigastric pain, recent onset indigestion Pleuritic chest pain Recent onset dyspnoea Pain reproduced on palpation More common in women, DM, elderly, CKD, dementia
 Spot potential")
10 Examination in ACS: what are you looking for? Often normal Aim to exclude non-cardiac / non-ischaemic causes of chest pain (remember acute aortic syndromes) Spot potential haemodynamic instability Assess for LV dysfunction Stratify risk for appropriate management
 Spot potential")
11 Examination in ACS: what are you looking for? Often normal Aim to exclude non-cardiac / non-ischaemic causes of chest pain (remember acute aortic syndromes) Spot potential haemodynamic instability Assess for LV dysfunction Stratify risk for appropriate management
12 Risk stratification high risk patients age Male Previous CAD DM BP LVF/CCF Recurrent symptoms despite treatment ST segment depression Dynamic ST changes Elevated troponin Haemodynamic instability Major arrhythmias

13 Biomarkers Highly Sensitive troponin T Early detection within 1 hour of myocyte necrosis Advantages: second assay at 6-9 hours not 12, high negative predictive value for ACS Values >5 x ULN have >90% positive predictive value for ACS Disadvantages: confusing normal range, concept of delta change Still requires presence of a fully functional brain in the requestor to interpret results
14 HS troponin T reference ranges HS trop T initial HS trop T 6 hours HS trop T Δ change Brain needed? Normal <14 ng/l <14 ng/l <20% Myocardial damage unlikely Further consideration required Myocardial damage <14 ng/l >14 ng/l <20% <14 ng/l >14 ng/l 20%- 100% >14 ng/l >14 ng/l >100%
15 HS troponin T reference ranges HS trop T initial HS trop T 6 hours HS trop T Δ change Brain needed? Normal <14 ng/l <14 ng/l <20% Myocardial damage unlikely Further consideration required Myocardial damage <14 ng/l >14 ng/l <20% <14 ng/l >14 ng/l 20%- 100% >14 ng/l >14 ng/l >100%
16 HS troponin T reference ranges HS trop T initial HS trop T 6 hours HS trop T Δ change Brain needed? Normal <14 ng/l <14 ng/l <20% Myocardial damage unlikely Further consideration required Myocardial damage <14 ng/l >14 ng/l <20% <14 ng/l >14 ng/l 20%- 100% >14 ng/l >14 ng/l >100%
17 HS troponin T reference ranges HS trop T initial HS trop T 6 hours HS trop T Δ change Brain needed? Normal <14 ng/l <14 ng/l <20% Myocardial damage unlikely Further consideration required Myocardial damage <14 ng/l >14 ng/l <20% <14 ng/l >14 ng/l 20%- 100% >14 ng/l >14 ng/l >100%


18 Mr L We think he s having a STEMI HS trop 3150 Fit and well 44 yr old NO chest pain history EF<15% on bedside echo Dx: viral myocarditis
19 Challenge 2: Troponinitis Myocarditis / myopericarditis / pericarditis Severe CCF Aortic dissection Exacerbation of COPD PE Cardiotoxic chemotherapy Severe sepsis Prolonged acidosis Ultra-endurance exertion HCM variants Hypertensive crisis Tachy/bradyarrhythmias Infiltrative e.g. Sarcoid Renal failure Non-coronary myocardial injury has prognostic implications
20 Mrs X 55 yr old female, smoker, positive family hx CAD, taxi driver 2/7 hx central chest pain at rest Initial dx ACS Given aspirin, clopidogrel, fondaparinux Initial hs trop 35 then 2 nd hs trop 21 troponin profile not suggestive of ACS Sent home (3am), Dx oesophageal spasm No follow up Meds unchanged No advice re: driving (taxi driver)
, Dx oesophageal spasm No follow up Meds unchanged No advice re: driving (taxi")
21 Mrs X 55 yr old female, smoker, positive family hx CAD, taxi driver 2/7 hx central chest pain at rest Initial dx ACS Given aspirin, clopidogrel, fondaparinux Initial hs trop 35 then 2 nd hs trop 21 troponin profile not suggestive of ACS Sent home (3am), Dx oesophageal spasm No follow up Meds unchanged No advice re: driving (taxi driver)

22 ECG: Suggests severe proximal LAD stenosis T inversion extends to I and avl indicating large ischaemic territory involved Ischaemic QTc prolongation (524ms) High probability of sudden death from future ischaemic events: - sudden severe pump failure - polymorphic VT Recalled and admitted Discharging Dr given opportunity to reflect
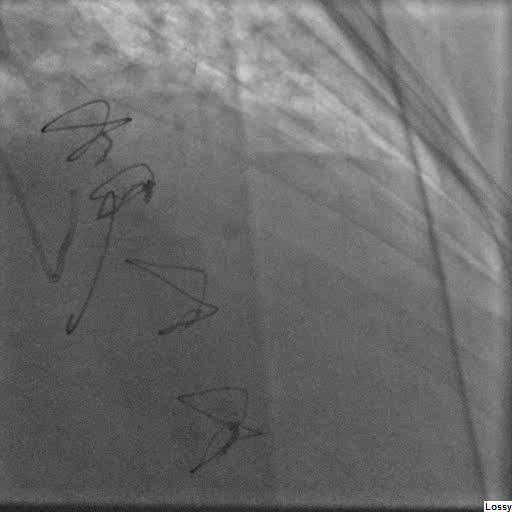
23 Pre-PCI Post-PCI

24 Pre-PCI Post-PCI


25 Pathophysiology a reminder CoffeyMJ@Cardiff.ac.uk

26

27 Challenge 3: Which Anti Platelet Agents?
28 Clopidogrel Prodrug requiring CYP3A4 mediated oxidation to active form (2-6 hours) Selectively and irreversibly inhibits platelet ADP P2Y 12 receptors 85% is hydrolysed to an inactive form High individual variability in response due to genetic polymorphisms Yusuf S et al. The Clopidogrel in Unstable angina to prevent Recurrent Events trial investigators. NEJM. 2001; 345:

 Therefore utilised in")
29 Prasugrel Also a prodrug irreversibly inhibiting platelet ADP P2Y 12 receptors Faster onset than clopidogrel (30 mins vs. 2-6 hours to clinical effect) Therefore utilised in PPCI for STEMI Increased bleeding risk
30 Ticagrelor Reversible inhibitor of platelet ADP P2Y 12 receptors Faster onset than clopidogrel (30 mins vs. 2-6 hours to clinical effect) Faster recovery of platelet function on cessation May cause dyspnoea and bradyarrhythmias Reduced mortality without increased bleeding (PLATO)
31 Which DAPT at the front door? ALWAYS ASPIRIN If STEMI for PPCI use prasugrel 60mg with aspirin 300mg If NSTE-ACS consider ticagrelor but clopidogrel more likely to be available Cardiologist may switch from clopidogrel to ticagrelor when patient reviewed For patients undergoing coronary intervention DAPT regime and duration should be determined by operator

32 DAPT and AF
33 Challenge 3: ACS in the elderly Proportion of those >80 yrs to triple by 2050 (CDC data) Underrepresentation in clinical trials those that do participate may not be representative of real elderly Multi-morbidity common Frequently present atypically (dyspnoea) and late Challenging for stress testing Higher risk of complications following any form of revascularisation: Bleeding Hypotension Bradycardia Renal failure


34 Challenge 3: ACS in the elderly Elderly less likely to undergo invasive risk stratification 1 Patients >75 years derive largest benefit in risk reduction from invasive strategy 2 Individualised approach needed: frailty patient choice renal function bleeding risk cognitive function Trial data pending: SENIOR trial 1: Baywani SB et al. ACS in Octogenarians. Clin. Interv. Aging. 2015; 10: : Bach RG et al. The effect of routine early invasive management on outcome for elderly patients with NSTEACS. Ann. Int Med. 2004; 141:
35 Challenge 4: ACS in CKD Many CKD patients have CAD risk factors Diagnosis more challenging ECG changes plus troponin elevation are common Worse prognosis from ACS Little safety data for P2Y 12 inhibitors in CKD 5 (use clopidogrel) Fondaparinux contraindicated if Cr clearance <20mls/min (use enoxaparin) Less likely to receive evidence-based Rx 1, 2 Concern re: contrast nephropathy 1: Esekowitz J et al. Association of renal insufficiency with outcome in HF and CAD JACC. 2004; 44: : Szummer K et al. SWEDEHEART registry. J. Intern. Med. 2010; 268: 40-49
36 Mr P Mr RP, 71 yr old male, new chest pain at rest CKD 4, asthma, endocarditis 2013 (MV repair) Initial trop 43, 6 hour trop 53 Cr 204 (stable) Troponin rise attributed to CKD Discharged home with ISMN and referral to RACPC Attended routine yearly review in my OPD 2/52 later


37
38 Challenge 4: ACS in CKD Serial and old ECGs useful to determine new changes Rise and fall pattern of HS trop suggests myocardial injury Requires individualised assessment of relative risk of invasive assessment Prehydration for all patients with egfr<60

39 Summary History taking is still crucial to diagnosis in ACS Beware late presenters with a falling troponin Always aspirin; DAPT regime should be guided by cardiology One size does not fit all for high risk groups
Chest pain and troponins on the acute take. J N Townend Queen Elizabeth Hospital Birmingham
 Chest pain and troponins on the acute take J N Townend Queen Elizabeth Hospital Birmingham 3 rd Universal Definition of Myocardial Infarction Type 1: Spontaneous MI related to atherosclerotic plaque rupture
Chest pain and troponins on the acute take J N Townend Queen Elizabeth Hospital Birmingham 3 rd Universal Definition of Myocardial Infarction Type 1: Spontaneous MI related to atherosclerotic plaque rupture
Medical Management of Acute Coronary Syndrome: The roles of a noncardiologist. Norbert Lingling D. Uy, MD Professor of Medicine UERMMMCI
 Medical Management of Acute Coronary Syndrome: The roles of a noncardiologist physician Norbert Lingling D. Uy, MD Professor of Medicine UERMMMCI Outcome objectives of the discussion: At the end of the
Medical Management of Acute Coronary Syndrome: The roles of a noncardiologist physician Norbert Lingling D. Uy, MD Professor of Medicine UERMMMCI Outcome objectives of the discussion: At the end of the
What is a myocardial infarction and how do we treat it? Paul Das Consultant Cardiologist North Wales Cardiac Centre Glan Clwyd Hospital
 What is a myocardial infarction and how do we treat it? Paul Das Consultant Cardiologist North Wales Cardiac Centre Glan Clwyd Hospital What is a myocardial infarction? THEY AINT WHAT THEY USED TO BE Case
What is a myocardial infarction and how do we treat it? Paul Das Consultant Cardiologist North Wales Cardiac Centre Glan Clwyd Hospital What is a myocardial infarction? THEY AINT WHAT THEY USED TO BE Case
Non ST Elevation-ACS. Michael W. Cammarata, MD
 Non ST Elevation-ACS Michael W. Cammarata, MD Case Presentation 65 year old man PMH: CAD s/p stent in 2008 HTN HLD Presents with chest pressure, substernally and radiating to the left arm and jaw, similar
Non ST Elevation-ACS Michael W. Cammarata, MD Case Presentation 65 year old man PMH: CAD s/p stent in 2008 HTN HLD Presents with chest pressure, substernally and radiating to the left arm and jaw, similar
Ticagrelor compared with clopidogrel in patients with acute coronary syndromes the PLATO trial
 compared with clopidogrel in patients with acute coronary syndromes the PLATO trial August 30, 2009 at 08.00 CET PLATO background In NSTE-ACS and STEMI, current guidelines recommend 12 months aspirin and
compared with clopidogrel in patients with acute coronary syndromes the PLATO trial August 30, 2009 at 08.00 CET PLATO background In NSTE-ACS and STEMI, current guidelines recommend 12 months aspirin and
Richard Grocott Mason
 Richard Grocott Mason What to do with a 50 year old man with chest pain? Does the pain sound cardiac? Is this a possible acute coronary syndrome? Does patient have a previous cardiac history? Natural history
Richard Grocott Mason What to do with a 50 year old man with chest pain? Does the pain sound cardiac? Is this a possible acute coronary syndrome? Does patient have a previous cardiac history? Natural history
Acute Coronary Syndromes
 Overview Acute Coronary Syndromes Rabeea Aboufakher, MD, FACC, FSCAI Section Chief of Cardiology Altru Health System Grand Forks, ND Epidemiology Pathophysiology Clinical features and diagnosis STEMI management
Overview Acute Coronary Syndromes Rabeea Aboufakher, MD, FACC, FSCAI Section Chief of Cardiology Altru Health System Grand Forks, ND Epidemiology Pathophysiology Clinical features and diagnosis STEMI management
Preliminary Programme
 Preliminary Programme The scientific programme comprises various styles of presentations and sessions, each offering a unique opportunity to amass new and important scientific information. Optimal management
Preliminary Programme The scientific programme comprises various styles of presentations and sessions, each offering a unique opportunity to amass new and important scientific information. Optimal management
Belinda Green, Cardiologist, SDHB, 2016
 Acute Coronary syndromes All STEMI ALL Non STEMI Unstable angina Belinda Green, Cardiologist, SDHB, 2016 Thrombus in proximal LAD Underlying pathophysiology Be very afraid for your patient Wellens
Acute Coronary syndromes All STEMI ALL Non STEMI Unstable angina Belinda Green, Cardiologist, SDHB, 2016 Thrombus in proximal LAD Underlying pathophysiology Be very afraid for your patient Wellens
OVERVIEW ACUTE CORONARY SYNDROME SYMPTOMS 9/30/14 TYPICAL WHAT IS ACUTE CORONARY SYNDROME? SYMPTOMS, IDENTIFICATION, MANAGEMENT
 OVERVIEW ACUTE CORONARY SYNDROME SYMPTOMS, IDENTIFICATION, MANAGEMENT OCTOBER 7, 2014 PETE PERAUD, MD SYMPTOMS TYPICAL ATYPICAL IDENTIFICATION EKG CARDIAC BIOMARKERS STEMI VS NON-STEMI VS USA MANAGEMENT
OVERVIEW ACUTE CORONARY SYNDROME SYMPTOMS, IDENTIFICATION, MANAGEMENT OCTOBER 7, 2014 PETE PERAUD, MD SYMPTOMS TYPICAL ATYPICAL IDENTIFICATION EKG CARDIAC BIOMARKERS STEMI VS NON-STEMI VS USA MANAGEMENT
HeFSSA Practitioners Program 2014
 HeFSSA Practitioners Program 2014 08:00 08:30 Registration 08:30 09:15 Clinical Case Presentation 1 09:15 10:00 Clinical Case Presentation 2 10:00 10:30 Tea Break 10:30 11:15 Clinical Case Presentation
HeFSSA Practitioners Program 2014 08:00 08:30 Registration 08:30 09:15 Clinical Case Presentation 1 09:15 10:00 Clinical Case Presentation 2 10:00 10:30 Tea Break 10:30 11:15 Clinical Case Presentation
What oral antiplatelet therapy would you choose? a) ASA alone b) ASA + Clopidogrel c) ASA + Prasugrel d) ASA + Ticagrelor
 ASA alone b) ASA + Clopidogrel c) ASA + Prasugrel d) ASA + Ticagrelor") 76 year old female Prior Hypertension, Hyperlipidemia, Smoking On Hydrochlorothiazide, Atorvastatin New onset chest discomfort; 2 episodes in past 24 hours Heart rate 122/min; BP 170/92 mm Hg, Killip Class
76 year old female Prior Hypertension, Hyperlipidemia, Smoking On Hydrochlorothiazide, Atorvastatin New onset chest discomfort; 2 episodes in past 24 hours Heart rate 122/min; BP 170/92 mm Hg, Killip Class
DIFFERENTIATING THE PATIENT WITH UNDIFFERENTIATED CHEST PAIN
 DIFFERENTIATING THE PATIENT WITH UNDIFFERENTIATED CHEST PAIN Objectives Gain competence in evaluating chest pain Recognize features of moderate risk unstable angina Review initial management of UA and
DIFFERENTIATING THE PATIENT WITH UNDIFFERENTIATED CHEST PAIN Objectives Gain competence in evaluating chest pain Recognize features of moderate risk unstable angina Review initial management of UA and
Acute Coronary Syndrome. Cindy Baker, MD FACC Director Peripheral Vascular Interventions Division of Cardiovascular Medicine
 Acute Coronary Syndrome Cindy Baker, MD FACC Director Peripheral Vascular Interventions Division of Cardiovascular Medicine Topics Timing is everything So many drugs to choose from What s a MINOCA? 2 Acute
Acute Coronary Syndrome Cindy Baker, MD FACC Director Peripheral Vascular Interventions Division of Cardiovascular Medicine Topics Timing is everything So many drugs to choose from What s a MINOCA? 2 Acute
STEMI, Non-STEMI, Chest Pain?
 Minnesota Chest Pain / Acute Coronary Syndrome Tool-Kit Patient with Chest Pain Or Potential Acute Coronary Syndrome STEMI, n-stemi, Chest Pain? Follow MN STEMI Guideline Follow MN n-stemi Guideline Follow
Minnesota Chest Pain / Acute Coronary Syndrome Tool-Kit Patient with Chest Pain Or Potential Acute Coronary Syndrome STEMI, n-stemi, Chest Pain? Follow MN STEMI Guideline Follow MN n-stemi Guideline Follow
Chest Pain. Dr Robert Huggett Consultant Cardiologist
 Chest Pain Dr Robert Huggett Consultant Cardiologist Outline Diagnosis of cardiac chest pain 2016 NICE update on stable chest pain Assessment of unstable chest pain/acs and MI definition Scope of the
Chest Pain Dr Robert Huggett Consultant Cardiologist Outline Diagnosis of cardiac chest pain 2016 NICE update on stable chest pain Assessment of unstable chest pain/acs and MI definition Scope of the
TROPONIN POSITIVE 2/20/2015 WHAT DOES IT MEAN? When should a troponin level be obtained?
 TROPONIN POSITIVE WHAT DOES IT MEAN? Frequently Asked Questions Regarding the Use of Troponin in the Clinical Setting What does an elevated troponin level mean? Elevated troponin is a sensitive and specific
TROPONIN POSITIVE WHAT DOES IT MEAN? Frequently Asked Questions Regarding the Use of Troponin in the Clinical Setting What does an elevated troponin level mean? Elevated troponin is a sensitive and specific
Acute Coronary Syndromes. January 9, 2013 Chris Chiles M.D. FACC
 Acute Coronary Syndromes January 9, 2013 Chris Chiles M.D. FACC Disclosures None- not even a breakfast burrito from a drug company Hospitalizations in the U.S. Due to ACS Acute Coronary Syndromes* 1.57
Acute Coronary Syndromes January 9, 2013 Chris Chiles M.D. FACC Disclosures None- not even a breakfast burrito from a drug company Hospitalizations in the U.S. Due to ACS Acute Coronary Syndromes* 1.57
Cindy Stephens, MSN, ANP Kelly Walker, MS, ACNP Peter Cohn, MD, FACC
 Cindy Stephens, MSN, ANP Kelly Walker, MS, ACNP Peter Cohn, MD, FACC Define Acute Coronary syndromes Explain the Cause Assessment, diagnosis and therapy Reperfusion for STEMI Complications to look for
Cindy Stephens, MSN, ANP Kelly Walker, MS, ACNP Peter Cohn, MD, FACC Define Acute Coronary syndromes Explain the Cause Assessment, diagnosis and therapy Reperfusion for STEMI Complications to look for
Disclosures. Inpatient Management of Non-ST Elevation Acute Coronary Syndromes. Edward McNulty MD, FACC. None
 Inpatient Management of Non-ST Elevation Acute Coronary Syndromes Edward McNulty MD, FACC Assistant Clinical Professor UCSF Director, SF VAMC Cardiac Catheterization Laboratory Disclosures None New Guidelines
Inpatient Management of Non-ST Elevation Acute Coronary Syndromes Edward McNulty MD, FACC Assistant Clinical Professor UCSF Director, SF VAMC Cardiac Catheterization Laboratory Disclosures None New Guidelines
Recognizing the High Risk NSTEMI Patient for Early Appropriate Therapy
 Recognizing the High Risk NSTEMI Patient for Early Appropriate Therapy Learning Objectives Learn to recognize the high risk patient Discuss effective management of a high risk NSTEMI patient Review CCS
Recognizing the High Risk NSTEMI Patient for Early Appropriate Therapy Learning Objectives Learn to recognize the high risk patient Discuss effective management of a high risk NSTEMI patient Review CCS
Antithrombotic therapy in CAD patients with concomitant NAFV: why and for whom?
 Antithrombotic therapy in CAD patients with concomitant NAFV: why and for whom? Institut de Cardiologie de la Pitié-Salpêtrière jean-philippe.collet@psl.aphp.fr www.action-coeur.org Patients (%) Patients
Antithrombotic therapy in CAD patients with concomitant NAFV: why and for whom? Institut de Cardiologie de la Pitié-Salpêtrière jean-philippe.collet@psl.aphp.fr www.action-coeur.org Patients (%) Patients
On admission Acute extensive anterior STEMI
 Mr B 52 years old male Smoker No prior known CAD Presents with 1 hour intermittent crushing retrosternal chest pain Transferred by MICU directly to CCU (ASA, Heparin) On admission Intense pain, diaphoretic
Mr B 52 years old male Smoker No prior known CAD Presents with 1 hour intermittent crushing retrosternal chest pain Transferred by MICU directly to CCU (ASA, Heparin) On admission Intense pain, diaphoretic
Cardiology. Self Learning Package. Module 5: Pharmacology: Treatment of Acute Coronary. Prevention
 Cardiology Self Learning Package Module 5: Pharmacology: Treatment of Acute Coronary Syndromes, Module 5: Pharmacology: Hyperlipidaemia, Treatment of Acute Coronary Hypertension, Symdrome, Hyperlipidaemia,
Cardiology Self Learning Package Module 5: Pharmacology: Treatment of Acute Coronary Syndromes, Module 5: Pharmacology: Hyperlipidaemia, Treatment of Acute Coronary Hypertension, Symdrome, Hyperlipidaemia,
An Approach to Chest Pain
 Oesophageal Spasm Acute Coronary Syndrome Pneumothorax An Approach to Chest Pain Musculoskeletal Pulmonary Embolism Aortic Dissection Ema Pitts Cardiology Registrar Basic Trainee Pain S Site O Onset C
Oesophageal Spasm Acute Coronary Syndrome Pneumothorax An Approach to Chest Pain Musculoskeletal Pulmonary Embolism Aortic Dissection Ema Pitts Cardiology Registrar Basic Trainee Pain S Site O Onset C
Antiplatelet and Anti-Thrombotic Therapy. Ivan Anderson, MD RIHVH Cardiology
 Antiplatelet and Anti-Thrombotic Therapy Ivan Anderson, MD RIHVH Cardiology Outline Anti-thrombotic therapy Risk stratification of stroke with atrial fibrillation DVT and PE treatment Pharmacology Anti-platelet
Antiplatelet and Anti-Thrombotic Therapy Ivan Anderson, MD RIHVH Cardiology Outline Anti-thrombotic therapy Risk stratification of stroke with atrial fibrillation DVT and PE treatment Pharmacology Anti-platelet
European Heart Journal 2015 doi: /eurheartj/ehv320
 European Heart Journal 2015 doi: 10.1093/eurheartj/ehv320 1 2 Clinical implications of high-sensivity troponin assays European Heart Journal 2015 doi: 10.1093/eurheartj/ehv320 Conditions other than Type
European Heart Journal 2015 doi: 10.1093/eurheartj/ehv320 1 2 Clinical implications of high-sensivity troponin assays European Heart Journal 2015 doi: 10.1093/eurheartj/ehv320 Conditions other than Type
2015 ESC Guidelines for the Management of Acute Coronary Syndromes in Patients Presenting Without Persistent ST-Segment Elevation
 2015 ESC Guidelines for the Management of Acute Coronary Syndromes in Patients Presenting Without Persistent ST-Segment Elevation Thierry Gillebert European Society of Cardiology, Slides kindly provided
2015 ESC Guidelines for the Management of Acute Coronary Syndromes in Patients Presenting Without Persistent ST-Segment Elevation Thierry Gillebert European Society of Cardiology, Slides kindly provided
Medicine Dr. Omed Lecture 2 Stable and Unstable Angina
 Medicine Dr. Omed Lecture 2 Stable and Unstable Angina Risk stratification in stable angina. High Risk; *post infarct angina, *poor effort tolerance, *ischemia at low workload, *left main or three vessel
Medicine Dr. Omed Lecture 2 Stable and Unstable Angina Risk stratification in stable angina. High Risk; *post infarct angina, *poor effort tolerance, *ischemia at low workload, *left main or three vessel
CHRONIC CAD DIAGNOSIS
 CHRONIC CAD DIAGNOSIS Chest Pain Evaluation 1. Approach to diagnosis of CAD 2. Classification of chest pain 3. Pre-test likelihood CAD 4. Algorithm for chest pain evaluation in women 5. Indications for
CHRONIC CAD DIAGNOSIS Chest Pain Evaluation 1. Approach to diagnosis of CAD 2. Classification of chest pain 3. Pre-test likelihood CAD 4. Algorithm for chest pain evaluation in women 5. Indications for
Non-Ischemic Causes of Troponin Elevation: Getting It Right. March 28, 2015
 Non-Ischemic Causes of Troponin Elevation: Getting It Right March 28, 2015 WHY discuss this...? Misconceptions about meaning of elevated troponin Validation of troponin when utilized properly Prognostic
Non-Ischemic Causes of Troponin Elevation: Getting It Right March 28, 2015 WHY discuss this...? Misconceptions about meaning of elevated troponin Validation of troponin when utilized properly Prognostic
Management of Stable Ischemic Heart Disease. Vinay Madan MD February 10, 2018
 Management of Stable Ischemic Heart Disease Vinay Madan MD February 10, 2018 1 Disclosure No financial disclosure. 2 Overview of SIHD Diagnosis Outline of talk Functional vs. Anatomic assessment Management
Management of Stable Ischemic Heart Disease Vinay Madan MD February 10, 2018 1 Disclosure No financial disclosure. 2 Overview of SIHD Diagnosis Outline of talk Functional vs. Anatomic assessment Management
Αντιαιμοπεταλιακη αγωγη (ποια, πο τε και για πο σο)
") Αντιαιμοπεταλιακη αγωγη (ποια, πο τε και για πο σο) Dimitrios Alexopoulos, MD, FESC, FACC Cardiology Department, Patras University Hospital, Patras, Rio, Greece. Patras University Hospital I, Dimitrios
Αντιαιμοπεταλιακη αγωγη (ποια, πο τε και για πο σο) Dimitrios Alexopoulos, MD, FESC, FACC Cardiology Department, Patras University Hospital, Patras, Rio, Greece. Patras University Hospital I, Dimitrios
EDUCATIONAL COMMENTARY CARDIAC FUNCTION: BIOCHEMICAL MARKERS UPDATE
 EDUCATIONAL COMMENTARY CARDIAC FUNCTION: BIOCHEMICAL MARKERS UPDATE Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE
EDUCATIONAL COMMENTARY CARDIAC FUNCTION: BIOCHEMICAL MARKERS UPDATE Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE
10 Steps to Managing Non-ST Elevation ACS
 Pathophysiology of Acute Coronary Syndromes and Potential Pharmacologic Interventions Acute Coronary Syndrome 4. Downstream from thrombus myocardial ischemia/necrosis (Beta-blockers, Nitrates etc) 3. Activation
Pathophysiology of Acute Coronary Syndromes and Potential Pharmacologic Interventions Acute Coronary Syndrome 4. Downstream from thrombus myocardial ischemia/necrosis (Beta-blockers, Nitrates etc) 3. Activation
CCS/CAIC/CSCS Position Statement on Revascularization Multi-vessel CAD. Teo et al, Canadian Journal of Cardiology 2014;30:
 CCS/CAIC/CSCS Position Statement on Revascularization Multi-vessel CAD Teo et al, Canadian Journal of Cardiology 2014;30: 1482-1491 Parallel Paper: Canadian Cardiovascular Society Guidelines for the Diagnosis
CCS/CAIC/CSCS Position Statement on Revascularization Multi-vessel CAD Teo et al, Canadian Journal of Cardiology 2014;30: 1482-1491 Parallel Paper: Canadian Cardiovascular Society Guidelines for the Diagnosis
Clinical Case. Management of ACS Based on ACC/AHA & ESC Guidelines. Clinical Case 4/22/12. UA/NSTEMI: Definition
 Clinical Case Management of ACS Based on ACC/AHA & ESC Guidelines Dr Badri Paudel Mr M 75M Poorly controlled diabetic Smoker Presented on Sat 7pm Intense burning in the retrosternal area Clinical Case
Clinical Case Management of ACS Based on ACC/AHA & ESC Guidelines Dr Badri Paudel Mr M 75M Poorly controlled diabetic Smoker Presented on Sat 7pm Intense burning in the retrosternal area Clinical Case
Coronary Heart Disease. Iqbal Malik
 Coronary Heart Disease Iqbal Malik Pathophysiology IHD Case chest pain Question -interactive What is the result of the exercise test? 1. negative 2. positive 3. equivocal 4. other Q2 answer STEMI! What
Coronary Heart Disease Iqbal Malik Pathophysiology IHD Case chest pain Question -interactive What is the result of the exercise test? 1. negative 2. positive 3. equivocal 4. other Q2 answer STEMI! What
2017 AHA/ACC Clinical Performance and Quality Measures for Adults With ST-Elevation and Non ST-Elevation Myocardial Infarction
 2017 AHA/ACC Clinical Performance and Quality Measures for Adults With ST-Elevation and Non ST-Elevation Myocardial Infarction Ramzi Khalil MD FACC Assistant Professor Allegheny Gen.Hospital AHN Speakers
2017 AHA/ACC Clinical Performance and Quality Measures for Adults With ST-Elevation and Non ST-Elevation Myocardial Infarction Ramzi Khalil MD FACC Assistant Professor Allegheny Gen.Hospital AHN Speakers
DECLARATION OF CONFLICT OF INTEREST. Lecture fees: AstraZeneca, Ely Lilly, Merck.
 DECLARATION OF CONFLICT OF INTEREST Lecture fees: AstraZeneca, Ely Lilly, Merck. Risk of stopping dual therapy. S D Kristensen, FESC Aarhus Denmark Acute coronary syndrome: coronary thrombus Platelets
DECLARATION OF CONFLICT OF INTEREST Lecture fees: AstraZeneca, Ely Lilly, Merck. Risk of stopping dual therapy. S D Kristensen, FESC Aarhus Denmark Acute coronary syndrome: coronary thrombus Platelets
Ischaemic Heart Disease
 Ischaemic Heart Disease Katherine Rothwell Case 1 65 yr old female PMHx : Eczema, is a smoker 20/day Comes to see you complaining of central chest pain Present past few months. Comes on when gardening
Ischaemic Heart Disease Katherine Rothwell Case 1 65 yr old female PMHx : Eczema, is a smoker 20/day Comes to see you complaining of central chest pain Present past few months. Comes on when gardening
Continuing Medical Education Post-Test
 Continuing Medical Education Post-Test Based on the information presented in this monograph, please choose one correct response for each of the following questions or statements. Record your answers on
Continuing Medical Education Post-Test Based on the information presented in this monograph, please choose one correct response for each of the following questions or statements. Record your answers on
GUIDELINES FOR THE MANAGEMENT OF PATIENTS WITH NON-ST SEGMENT ELEVATION ACUTE CORONARY SYNDROME (NSTEACS)
") GUIDELINES FOR THE MANAGEMENT OF PATIENTS WITH NON-ST SEGMENT ELEVATION ACUTE CORONARY SYNDROME (NSTEACS) INCLUDING UNSTABLE ANGINA AND NON-Q WAVE MYOCARDIAL INFARCTION Revised August 2011 First Edition
GUIDELINES FOR THE MANAGEMENT OF PATIENTS WITH NON-ST SEGMENT ELEVATION ACUTE CORONARY SYNDROME (NSTEACS) INCLUDING UNSTABLE ANGINA AND NON-Q WAVE MYOCARDIAL INFARCTION Revised August 2011 First Edition
Unstable angina and NSTEMI
 Issue date: March 2010 Unstable angina and NSTEMI The early management of unstable angina and non-st-segment-elevation myocardial infarction This guideline updates and replaces recommendations for the
Issue date: March 2010 Unstable angina and NSTEMI The early management of unstable angina and non-st-segment-elevation myocardial infarction This guideline updates and replaces recommendations for the
High-sensitive troponin. Introduction. Platelet aggregation inhibition at admission
 Neth Heart J (2017) 25:181 185 DOI 10.1007/s12471-016-0939-y GUIDELINES 2015 ESC guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation:
Neth Heart J (2017) 25:181 185 DOI 10.1007/s12471-016-0939-y GUIDELINES 2015 ESC guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation:
ACCP Cardiology PRN Journal Club
 ACCP Cardiology PRN Journal Club 1 Optimising Crossover from Ticagrelor to Clopidogrel in Patients with Acute Coronary Syndrome [CAPITAL OPTI-CROSS] Monique Conway, PharmD, BCPS PGY-2 Cardiology Pharmacy
ACCP Cardiology PRN Journal Club 1 Optimising Crossover from Ticagrelor to Clopidogrel in Patients with Acute Coronary Syndrome [CAPITAL OPTI-CROSS] Monique Conway, PharmD, BCPS PGY-2 Cardiology Pharmacy
Case Study 50 YEAR OLD MALE WITH UNSTABLE ANGINA
 Case Study 50 YEAR OLD MALE WITH UNSTABLE ANGINA Case History A 50-year-old man with type 1 diabetes mellitus and hypertension presents after experiencing 1 hour of midsternal chest pain that began after
Case Study 50 YEAR OLD MALE WITH UNSTABLE ANGINA Case History A 50-year-old man with type 1 diabetes mellitus and hypertension presents after experiencing 1 hour of midsternal chest pain that began after
TOPICS IN EMERGENCY MEDICINE SEMI-FINAL
 RISK ASSESSMENT IN PATIENTS WITH CHEST PAIN Nora Goldschlager, M.D. FACP, FACC, FAHA, FHRS Cardiology - San Francisco General Hospital UCSF Disclosures: None 1 CHEST PAIN NOT DUE TO MYOCARDIAL ISCHEMIA
RISK ASSESSMENT IN PATIENTS WITH CHEST PAIN Nora Goldschlager, M.D. FACP, FACC, FAHA, FHRS Cardiology - San Francisco General Hospital UCSF Disclosures: None 1 CHEST PAIN NOT DUE TO MYOCARDIAL ISCHEMIA
QUT Digital Repository:
 QUT Digital Repository: http://eprints.qut.edu.au/ This is the author s version of this journal article. Published as: Doggrell, Sheila (2010) New drugs for the treatment of coronary artery syndromes.
QUT Digital Repository: http://eprints.qut.edu.au/ This is the author s version of this journal article. Published as: Doggrell, Sheila (2010) New drugs for the treatment of coronary artery syndromes.
Essam Mahfouz, MD. Professor of Cardiology, Mansoura University
 By Essam Mahfouz, MD. Professor of Cardiology, Mansoura University Agenda Definitions Classifications Epidemiology Risk stratification What is new? What is MI? Myocardial infarction is the death of part
By Essam Mahfouz, MD. Professor of Cardiology, Mansoura University Agenda Definitions Classifications Epidemiology Risk stratification What is new? What is MI? Myocardial infarction is the death of part
Why and How Should We Switch Clopidogrel to Prasugrel?
 Case Presentation Why and How Should We Switch Clopidogrel to Prasugrel? Shaul Atar Western Galilee Medical Center Nahariya, ISRAEL Case Description A 67 Y. Old Pt. admitted to IM with anginal CP. DM,
Case Presentation Why and How Should We Switch Clopidogrel to Prasugrel? Shaul Atar Western Galilee Medical Center Nahariya, ISRAEL Case Description A 67 Y. Old Pt. admitted to IM with anginal CP. DM,
UPDATES FROM THE 2018 ANTIPLATELET GUIDELINES
 UPDATES FROM THE 2018 ANTIPLATELET GUIDELINES Claudia Bucci BScPhm, PharmD Clinical Coordinator, Cardiovascular Diseases Sunnybrook Health Sciences Centre 21st Annual Contemporary Therapeutic Issues in
UPDATES FROM THE 2018 ANTIPLATELET GUIDELINES Claudia Bucci BScPhm, PharmD Clinical Coordinator, Cardiovascular Diseases Sunnybrook Health Sciences Centre 21st Annual Contemporary Therapeutic Issues in
Acute Coronary Syndrome. Sonny Achtchi, DO
 Acute Coronary Syndrome Sonny Achtchi, DO Objectives Understand evidence based and practice based treatments for stabilization and initial management of ACS Become familiar with ACS risk stratification
Acute Coronary Syndrome Sonny Achtchi, DO Objectives Understand evidence based and practice based treatments for stabilization and initial management of ACS Become familiar with ACS risk stratification
AIMS: CHEST PAIN. Causes of chest pain. Causes of chest pain: Cardiac causes: Acute coronary syndromes pericarditis thoracic aortic dissection
 CHEST PAIN Dr Susan Hertzberg Emergency Department Prince of Wales Hospital AIMS: To identify causes of chest pain in patients presenting to the ED. To identify and risk stratify patients presenting with
CHEST PAIN Dr Susan Hertzberg Emergency Department Prince of Wales Hospital AIMS: To identify causes of chest pain in patients presenting to the ED. To identify and risk stratify patients presenting with
Acute Coronary Syndrome (ACS) Initial Evaluation and Management
 Initial Evaluation and Management") Acute Coronary Syndrome (ACS) Initial Evaluation and Management Symptoms of Possible ACS Chest discomfort with or without radiation to the arm(s), jaw, or epigastrium Short of breath Weakness Diaphoresis
Acute Coronary Syndrome (ACS) Initial Evaluation and Management Symptoms of Possible ACS Chest discomfort with or without radiation to the arm(s), jaw, or epigastrium Short of breath Weakness Diaphoresis
M/39 CC D. => peak CKMB (12 hr later) ng/ml T.chol/TG/HDL/LDL 180/150/48/102 mg/dl #
 ng/ml T.chol/TG/HDL/LDL 180/150/48/102 mg/dl #") Acute Coronary Syndrome - Case Review - Young-Guk Ko, MD Yonsei Cardiovascular Center Yonsei University College of Medicine Case 1 M/39 #4306212 CC D : Severe squeezing chest pain : 4 hours, aggravated
Acute Coronary Syndrome - Case Review - Young-Guk Ko, MD Yonsei Cardiovascular Center Yonsei University College of Medicine Case 1 M/39 #4306212 CC D : Severe squeezing chest pain : 4 hours, aggravated
FastTest. You ve read the book now test yourself
 FastTest You ve read the book...... now test yourself To ensure you have learned the key points that will improve your patient care, read the authors questions below. The answers will refer you back to
FastTest You ve read the book...... now test yourself To ensure you have learned the key points that will improve your patient care, read the authors questions below. The answers will refer you back to
ST Elevation Myocardial Infarction
 ST Elevation Myocardial Infarction Scott M. Lilly, MD, PhD Assistant Professor Clinical Department of Cardiovascular Medicine The Ohio State University Wexner Medical Center Case Presentation 46 year old
ST Elevation Myocardial Infarction Scott M. Lilly, MD, PhD Assistant Professor Clinical Department of Cardiovascular Medicine The Ohio State University Wexner Medical Center Case Presentation 46 year old
Chest pain management. Ruvin Gabriel and Niels van Pelt August 2011
 Chest pain management Ruvin Gabriel and Niels van Pelt August 2011 Introduction Initial assessment Case 1 Case 2 and 3 Comparison of various diagnostic techniques Summary 1-2 % of GP consultations are
Chest pain management Ruvin Gabriel and Niels van Pelt August 2011 Introduction Initial assessment Case 1 Case 2 and 3 Comparison of various diagnostic techniques Summary 1-2 % of GP consultations are
Management of Coronary Artery Disease including Stable and Acute Coronary Syndromes
 Management of Coronary Artery Disease including Stable and Acute Coronary Syndromes Dr Sukhjinder Nijjer Consultant Cardiologist Chelsea & Westminster NHS Foundation Trust Imperial College Healthcare NHS
Management of Coronary Artery Disease including Stable and Acute Coronary Syndromes Dr Sukhjinder Nijjer Consultant Cardiologist Chelsea & Westminster NHS Foundation Trust Imperial College Healthcare NHS
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Centre for Clinical Practice
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Centre for Clinical Practice Review consultation document Review of Clinical Guideline (CG95) Chest pain of recent onset: Assessment and diagnosis
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Centre for Clinical Practice Review consultation document Review of Clinical Guideline (CG95) Chest pain of recent onset: Assessment and diagnosis
Acute Coronary syndrome
 Acute Coronary syndrome 7th Annual Pharmacotherapy Conference ACS Pathophysiology rupture or erosion of a vulnerable, lipidladen, atherosclerotic coronary plaque, resulting in exposure of circulating blood
Acute Coronary syndrome 7th Annual Pharmacotherapy Conference ACS Pathophysiology rupture or erosion of a vulnerable, lipidladen, atherosclerotic coronary plaque, resulting in exposure of circulating blood
Management of Patients with Atrial Fibrillation Undergoing Coronary Artery Stenting 경북대의전원내과조용근
 Management of Patients with Atrial Fibrillation Undergoing Coronary Artery Stenting 경북대의전원내과조용근 Case (2011, 5) 74-years old gentleman Exertional chest pain Warfarin with good INR control Ex-smoker, social(?)
Management of Patients with Atrial Fibrillation Undergoing Coronary Artery Stenting 경북대의전원내과조용근 Case (2011, 5) 74-years old gentleman Exertional chest pain Warfarin with good INR control Ex-smoker, social(?)
Case Presentation. ESIM 8 th 12 th June Doriella Galea Malta
 Case Presentation ESIM 8 th 12 th June 2015 Doriella Galea Malta 3am: Ward Call Asked to review Ms J.D. a 45 year old lady previously healthy in view of chest pain She described central chest pain radiating
Case Presentation ESIM 8 th 12 th June 2015 Doriella Galea Malta 3am: Ward Call Asked to review Ms J.D. a 45 year old lady previously healthy in view of chest pain She described central chest pain radiating
Acute Coronary Syndrome. Emergency Department Updated Jan. 2017
 Acute Coronary Syndrome Emergency Department Updated Jan. 2017 Goals and Objectives To reduce mortality and morbidity for people who have cardiovascular disease, with a focus on those who experience an
Acute Coronary Syndrome Emergency Department Updated Jan. 2017 Goals and Objectives To reduce mortality and morbidity for people who have cardiovascular disease, with a focus on those who experience an
(ClinicalTrials.gov ID: NCT ) Title: The Italian Elderly ACS Study Author: Stefano Savonitto. Date: 29 August 2011 Meeting: ESC congress, Paris
 Title: The Italian Elderly ACS Study Author: Stefano Savonitto. Date: 29 August 2011 Meeting: ESC congress, Paris") Early aggressive versus initially conservative strategy in elderly patients with non-st- elevation acute coronary syndrome: the Italian randomised trial (ClinicalTrials.gov ID: NCT00510185) Stefano Savonitto,
Early aggressive versus initially conservative strategy in elderly patients with non-st- elevation acute coronary syndrome: the Italian randomised trial (ClinicalTrials.gov ID: NCT00510185) Stefano Savonitto,
Date of Meeting: Ratified Date: 03/06/2009
 Document Type: PROTOCOL Title: Management And Transfer Of Patients With Acute Scope: Cardiac Network-wide Author/Originator and Title: Dr Ranjit More & members of the Cardiac Network Clinical Advisory
Document Type: PROTOCOL Title: Management And Transfer Of Patients With Acute Scope: Cardiac Network-wide Author/Originator and Title: Dr Ranjit More & members of the Cardiac Network Clinical Advisory
2010 ACLS Guidelines. Primary goals of therapy for patients
 2010 ACLS Guidelines Part 10: Acute Coronary Syndrome Present : 內科 R1 鍾伯欣 Supervisor: F1 吳亮廷 991110 Primary goals of therapy for patients of ACS Reduce the amount of myocardial necrosis that occurs in
2010 ACLS Guidelines Part 10: Acute Coronary Syndrome Present : 內科 R1 鍾伯欣 Supervisor: F1 吳亮廷 991110 Primary goals of therapy for patients of ACS Reduce the amount of myocardial necrosis that occurs in
21/06/2018. MEASURING PERFORMANCE (AUDIT AND QUALITY IMPROVEMENT) Towards Reducing Inequity. What should we be measuring?
 Towards Reducing Inequity. What should we be measuring?") MEASURING PERFORMANCE (AUDIT AND QUALITY IMPROVEMENT) Towards Reducing Inequity Dr Raewyn Fisher Cardiologist Director of Waikato Integrated Heart Failure Service What should we be measuring? At risk,
MEASURING PERFORMANCE (AUDIT AND QUALITY IMPROVEMENT) Towards Reducing Inequity Dr Raewyn Fisher Cardiologist Director of Waikato Integrated Heart Failure Service What should we be measuring? At risk,
DR ALEXIA STAVRATI CARDIOLOGIST, DIRECTOR OF CARDIOLOGY DEPT, "G. PAPANIKOLAOU" GH, THESSALONIKI
 The Impact of AF on Natural History of CAD DR ALEXIA STAVRATI CARDIOLOGIST, DIRECTOR OF CARDIOLOGY DEPT, "G. PAPANIKOLAOU" GH, THESSALONIKI CAD MOST COMMON CARDIOVASCULAR DISEASE MOST COMMON CAUSE OF DEATH
The Impact of AF on Natural History of CAD DR ALEXIA STAVRATI CARDIOLOGIST, DIRECTOR OF CARDIOLOGY DEPT, "G. PAPANIKOLAOU" GH, THESSALONIKI CAD MOST COMMON CARDIOVASCULAR DISEASE MOST COMMON CAUSE OF DEATH
CHEST PAIN AND SUSPECTED ACUTE CORONARY SYNDROME GUIDELINES
 CHEST PAIN AND SUSPECTED ACUTE CORONARY SYNDROME GUIDELINES Policy authors Accountable Executive Lead Approving body Policy reference Dr. Vinoda Sharma; Dr. Chetan Varma Consultant Cardiologists Medical
CHEST PAIN AND SUSPECTED ACUTE CORONARY SYNDROME GUIDELINES Policy authors Accountable Executive Lead Approving body Policy reference Dr. Vinoda Sharma; Dr. Chetan Varma Consultant Cardiologists Medical
Post Operative Troponin Leak: David Smyth Christchurch New Zealand
 Post Operative Troponin Leak: Does It Really Matter? David Smyth Christchurch New Zealand Life Was Simple Once Transmural Infarction Subendocardial Infarction But the Blood Tests Were n t Perfect Creatine
Post Operative Troponin Leak: Does It Really Matter? David Smyth Christchurch New Zealand Life Was Simple Once Transmural Infarction Subendocardial Infarction But the Blood Tests Were n t Perfect Creatine
ECG Workshop. Nezar Amir
 ECG Workshop Nezar Amir Myocardial Ischemia ECG Infarct ECG in STEMI is dynamic & evolving Common causes of ST shift Infarct Localisation Left main artery occlusion: o diffuse ST-depression with ST elevation
ECG Workshop Nezar Amir Myocardial Ischemia ECG Infarct ECG in STEMI is dynamic & evolving Common causes of ST shift Infarct Localisation Left main artery occlusion: o diffuse ST-depression with ST elevation
10/22/16. Lay of the land. Definition of ACS. Why do we worry about ST elevations?
 Lay of the land Update on Acute Coronary Syndrome: Five Things Hospitalists Must Know Dhruv S. Kazi, MD, MSc, MS Assistant Professor Department of Medicine (Cardiology), Department of Epidemiology and
Lay of the land Update on Acute Coronary Syndrome: Five Things Hospitalists Must Know Dhruv S. Kazi, MD, MSc, MS Assistant Professor Department of Medicine (Cardiology), Department of Epidemiology and
Platelet function testing to guide P2Y 12 -inhibitor treatment in ACS patients after PCI: insights from a national program in Hungary
 Platelet function testing to guide P2Y 12 -inhibitor treatment in ACS patients after PCI: insights from a national program in Hungary Dániel Aradi MD PhD Interventional Cardiologist Assistant professor
Platelet function testing to guide P2Y 12 -inhibitor treatment in ACS patients after PCI: insights from a national program in Hungary Dániel Aradi MD PhD Interventional Cardiologist Assistant professor
Asif Serajian DO FACC FSCAI
 Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Women and Vascular Disease
 Women and Vascular Disease KEVIN F. REBECK PA-C VASCULAR TRANSPLANT SURGERY 1 The Scope of the Problem One woman dies every minute from cardiovascular disease in the U.S.! The Scope of the Problem CVD
Women and Vascular Disease KEVIN F. REBECK PA-C VASCULAR TRANSPLANT SURGERY 1 The Scope of the Problem One woman dies every minute from cardiovascular disease in the U.S.! The Scope of the Problem CVD
Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes
 Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes Seung-Jae Joo and other KAMIR-NIH investigators Department of Cardiology, Jeju National
Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes Seung-Jae Joo and other KAMIR-NIH investigators Department of Cardiology, Jeju National
A case of post myocardial infarction ventricular septal rupture CHRISTOFOROS KOBOROZOS, MD
 A case of post myocardial infarction ventricular septal rupture CHRISTOFOROS KOBOROZOS, MD NAVAL HOSPITAL OF ATHENS case presentation Female, 81yo Hx: diabetes mellitus, hypertension, chronic anaemia presented
A case of post myocardial infarction ventricular septal rupture CHRISTOFOROS KOBOROZOS, MD NAVAL HOSPITAL OF ATHENS case presentation Female, 81yo Hx: diabetes mellitus, hypertension, chronic anaemia presented
Troponin = 35. Objectives. Low Risk Chest Pain. Does this patient have ACS? Does this patient have ACS? Objectives
 Objectives Low Risk Chest Pain Jeffrey Tabas, MD Professor of Emergency Medicine Office of CME UCSF School of Medicine Improve speed and accuracy in assessing patients with possible ACS! Avoid pitfalls
Objectives Low Risk Chest Pain Jeffrey Tabas, MD Professor of Emergency Medicine Office of CME UCSF School of Medicine Improve speed and accuracy in assessing patients with possible ACS! Avoid pitfalls
How to manage ACS patients with Comorbidities? Patients with Renal Failure
 How to manage ACS patients with Comorbidities? Patients with Renal Failure François Schiele, MD, PhD Department of Cardiology, University Hospital Jean Minjoz, Besançon, France. Potential conflicts of
How to manage ACS patients with Comorbidities? Patients with Renal Failure François Schiele, MD, PhD Department of Cardiology, University Hospital Jean Minjoz, Besançon, France. Potential conflicts of
UPDATE ON THE MANAGEMENTACUTE CORONARY SYNDROME. DR JULES KABAHIZI, Psc (Rwa) Lt Col CHIEF CONSULTANT RMH/KFH 28 JUNE18
 Lt Col CHIEF CONSULTANT RMH/KFH 28 JUNE18") UPDATE ON THE MANAGEMENTACUTE CORONARY SYNDROME DR JULES KABAHIZI, Psc (Rwa) Lt Col CHIEF CONSULTANT RMH/KFH 28 JUNE18 INTRODUCTION The clinical entities that comprise acute coronary syndromes (ACS)-ST-segment
UPDATE ON THE MANAGEMENTACUTE CORONARY SYNDROME DR JULES KABAHIZI, Psc (Rwa) Lt Col CHIEF CONSULTANT RMH/KFH 28 JUNE18 INTRODUCTION The clinical entities that comprise acute coronary syndromes (ACS)-ST-segment
Ischemic and bleeding risk stratification in NSTE ACS. Andrzej Budaj Postgraduate Medical School Grochowski Hospital, Warsaw, Poland
 Ischemic and bleeding risk stratification in NSTE ACS Andrzej Budaj Postgraduate Medical School Grochowski Hospital, Warsaw, Poland Disclosure Andrzej Budaj, MD, PhD, reports the following potential conflicts
Ischemic and bleeding risk stratification in NSTE ACS Andrzej Budaj Postgraduate Medical School Grochowski Hospital, Warsaw, Poland Disclosure Andrzej Budaj, MD, PhD, reports the following potential conflicts
Oral anticoagulation/antiplatelet therapy in the secondary prevention of ACS patients the cost of reducing death!
 Oral anticoagulation/antiplatelet therapy in the secondary prevention of ACS patients the cost of reducing death! Robert C. Welsh, MD, FRCPC Associate Professor of Medicine Director, Adult Cardiac Catheterization
Oral anticoagulation/antiplatelet therapy in the secondary prevention of ACS patients the cost of reducing death! Robert C. Welsh, MD, FRCPC Associate Professor of Medicine Director, Adult Cardiac Catheterization
Angina Luis Tulloch, MD 03/27/2012
 Angina Luis Tulloch, MD 03/27/2012 Acute coronary syndromes ACS STE > 1 mm, new LBBB* Increased cardiac enzymes STEMI Yes Yes NSTEMI No Yes UA No No *Recognize Wellen s sign/syndrome, posterior wall MI,
Angina Luis Tulloch, MD 03/27/2012 Acute coronary syndromes ACS STE > 1 mm, new LBBB* Increased cardiac enzymes STEMI Yes Yes NSTEMI No Yes UA No No *Recognize Wellen s sign/syndrome, posterior wall MI,
Imaging ischemic heart disease: role of SPECT and PET. Focus on Patients with Known CAD
 Imaging ischemic heart disease: role of SPECT and PET. Focus on Patients with Known CAD Hein J. Verberne Academic Medical Center, University of Amsterdam, Amsterdam, Netherlands International Conference
Imaging ischemic heart disease: role of SPECT and PET. Focus on Patients with Known CAD Hein J. Verberne Academic Medical Center, University of Amsterdam, Amsterdam, Netherlands International Conference
Practitioner Education Course
 2015 Practitioner Education Course ST Elevation Myocardial Infarction 2 Pathology Concept of vulnerable plaque Mild Atheroma Diagnosis IVUS OCT 3 Diagnosis This is based on : Clinical History ECG Changes.
2015 Practitioner Education Course ST Elevation Myocardial Infarction 2 Pathology Concept of vulnerable plaque Mild Atheroma Diagnosis IVUS OCT 3 Diagnosis This is based on : Clinical History ECG Changes.
Antithrombotic treatment in ACS: what do the guidelines say? Nicolas Danchin, HEGP, Paris France
 Antithrombotic treatment in ACS: what do the guidelines say? Nicolas Danchin, HEGP, Paris France Disclosures Research grants: Astra-Zeneca, Merck, Novartis, Pfizer, sanofi-aventis, Servier, The MedCo Fees
Antithrombotic treatment in ACS: what do the guidelines say? Nicolas Danchin, HEGP, Paris France Disclosures Research grants: Astra-Zeneca, Merck, Novartis, Pfizer, sanofi-aventis, Servier, The MedCo Fees
Know the Quality of our Care at Every Step. Kansas City ACS Summit BI-State Cardiovascular Education Consortium
 Know the Quality of our Care at Every Step Kansas City ACS Summit BI-State Cardiovascular Education Consortium Welcome to the Kansas City ACS Summit Objectives: Follow the flow and care of an ACS patient
Know the Quality of our Care at Every Step Kansas City ACS Summit BI-State Cardiovascular Education Consortium Welcome to the Kansas City ACS Summit Objectives: Follow the flow and care of an ACS patient
Acute coronary syndromes A European viewpoint. Felicita Andreotti, MD PhD FESC Catholic University Hospital Cardiovascular Diseases - Rome, IT
 Acute coronary syndromes A European viewpoint Felicita Andreotti, MD PhD FESC Catholic University Hospital Cardiovascular Diseases - Rome, IT Potential conflicts of interest In the past 2 years Felicita
Acute coronary syndromes A European viewpoint Felicita Andreotti, MD PhD FESC Catholic University Hospital Cardiovascular Diseases - Rome, IT Potential conflicts of interest In the past 2 years Felicita
David A. Orsinelli, MD, FACC, FASE Professor, Internal Medicine The Ohio State University Division of Cardiovascular Medicine Columbus, Ohio
 1 STABLE ISCHEMIC HEART DISEASE: A NON-INVASIVE CARDIOLOGIST S PERSECTIVE 2018 Cardiovascular Course for Trainees and Early Career Physicians APRIL 20, 2018 David A. Orsinelli, MD, FACC, FASE Professor,
1 STABLE ISCHEMIC HEART DISEASE: A NON-INVASIVE CARDIOLOGIST S PERSECTIVE 2018 Cardiovascular Course for Trainees and Early Career Physicians APRIL 20, 2018 David A. Orsinelli, MD, FACC, FASE Professor,
Doncaster & Bassetlaw Medicines Formulary
 Doncaster & Bassetlaw Medicines Formulary Section 2.9: Antiplatelet Drugs Aspirin 75mg Dispersible Tablets Aspirin 300mg Dispersible Tablets Aspirin 300mg Suppositories Clopidogrel 75mg Tablets Dipyridamole
Doncaster & Bassetlaw Medicines Formulary Section 2.9: Antiplatelet Drugs Aspirin 75mg Dispersible Tablets Aspirin 300mg Dispersible Tablets Aspirin 300mg Suppositories Clopidogrel 75mg Tablets Dipyridamole
OUTPATIENT ANTITHROMBOTIC MANAGEMENT POST NON-ST ELEVATION ACUTE CORONARY SYNDROME. TARGET AUDIENCE: All Canadian health care professionals.
 OUTPATIENT ANTITHROMBOTIC MANAGEMENT POST NON-ST ELEVATION ACUTE CORONARY SYNDROME TARGET AUDIENCE: All Canadian health care professionals. OBJECTIVE: To review the use of antiplatelet agents and oral
OUTPATIENT ANTITHROMBOTIC MANAGEMENT POST NON-ST ELEVATION ACUTE CORONARY SYNDROME TARGET AUDIENCE: All Canadian health care professionals. OBJECTIVE: To review the use of antiplatelet agents and oral
Cardiovascular emergencies. 05/March/2014 László Rudas Szeged
 Cardiovascular emergencies 05/March/2014 László Rudas Szeged Acute chest pain Acute heart failure Sudden cardiac death Acute chest pain What is the etiology? Chest pain signals emergency: - ACS - Pulmonary
Cardiovascular emergencies 05/March/2014 László Rudas Szeged Acute chest pain Acute heart failure Sudden cardiac death Acute chest pain What is the etiology? Chest pain signals emergency: - ACS - Pulmonary
More acute cardiology
 Case 1 RC 86, Male More acute cardiology Dr John Chambers Consultant Cardiologist A&E: SOB at rest. No chest pain. Exertional SOB for 6/12. PMHx: HT Rx: Ramipril 5mg od Examination: Afebrile, HR = 105,
Case 1 RC 86, Male More acute cardiology Dr John Chambers Consultant Cardiologist A&E: SOB at rest. No chest pain. Exertional SOB for 6/12. PMHx: HT Rx: Ramipril 5mg od Examination: Afebrile, HR = 105,
Case Challenges in ACS The Very Elderly in the Cath Lab
 Case Challenges in ACS The Very Elderly in the Cath Lab Sameh Salama, MD, FSCAI Professor of Cardiology, Cairo University 86 yrs old male IDDM (controlled on insulin and oral hypoglycemics) Hypertensive
Case Challenges in ACS The Very Elderly in the Cath Lab Sameh Salama, MD, FSCAI Professor of Cardiology, Cairo University 86 yrs old male IDDM (controlled on insulin and oral hypoglycemics) Hypertensive
STEMI and Cardiogenic Shock. The rules and solution. Dave Kettles St Dominics and Frere Hospitals East London ZA
 STEMI and Cardiogenic Shock. The rules and solution Dave Kettles St Dominics and Frere Hospitals East London ZA Definitions: Shock is a life threatening, but initially reversible state of cellular and
STEMI and Cardiogenic Shock. The rules and solution Dave Kettles St Dominics and Frere Hospitals East London ZA Definitions: Shock is a life threatening, but initially reversible state of cellular and
Aortic stenosis in octogenarians and comorbidities. Constantinos Evdoridis, MD Elpis General Hospital, Athens
 Aortic stenosis in octogenarians and comorbidities Constantinos Evdoridis, MD Elpis General Hospital, Athens Decision to operate according to age range European Heart Journal (2005) 26, 2714 2720 Fitness
Aortic stenosis in octogenarians and comorbidities Constantinos Evdoridis, MD Elpis General Hospital, Athens Decision to operate according to age range European Heart Journal (2005) 26, 2714 2720 Fitness
Path of care of patients with Acute Coronary Syndrome
 Path of care of patients with Acute Coronary Syndrome Inequalities by Aboriginality Dr Ben Scalley A/Professor Marisa Gilles A/Professor Judith Katzenellenbogen Professor Sandra Thompson Combined Universities
Path of care of patients with Acute Coronary Syndrome Inequalities by Aboriginality Dr Ben Scalley A/Professor Marisa Gilles A/Professor Judith Katzenellenbogen Professor Sandra Thompson Combined Universities
Acute coronary syndromes
 Clinical Medicine 2016 Vol 16, No 6: s43 s48 CARDIOVASCULAR Acute coronary syndromes Authors: Tush a r Kote c h a A a nd Ro by D Ra k hit B ABSTRACT In the UK, there are over 80,000 admissions annually
Clinical Medicine 2016 Vol 16, No 6: s43 s48 CARDIOVASCULAR Acute coronary syndromes Authors: Tush a r Kote c h a A a nd Ro by D Ra k hit B ABSTRACT In the UK, there are over 80,000 admissions annually