Female Urology Update. Lynnetta Faith Payne, DO, FACOS Urological Surgeon
|
|
|
- Maximilian Cross
- 5 years ago
- Views:
Transcription

1
2 Female Urology Update Lynnetta Faith Payne, DO, FACOS Urological Surgeon
3 Objectives: -diagnosis -risk factors -treatment UTI Incontinence
4 64 year old woman presents with a 3 year history of recurrent urinary tract infections (UTIs) treated with multiple antibiotic courses by a walk-in clinic
5 What are the clinical symptoms associated with UTI? Irritative symptoms Urgency Frequency Dysuria Hematuria Foul odor Suprapubic pain Upper tract infections (pyelonephritis) fevers rigors flank pain nausea and emesis

6 Congested vasculatures and extensive lamina propria hemorrhage Can be accompanied by sloughing of surface urothelium, ulceration or cytologic atypia depending on the cause of hemorrhagic cystitis
7 Patient reports presumed bladder infections which occur every month or two associated with dysuria, urgency, and frequency. No gross hematuria, flank pain, or fevers.
8 What is the differential diagnosis? Many processes and conditions may mimic the symptoms of bacterial urinary tract infection, so it is critical to rule out other causes during the evaluation prior to initiating treatment. Urologic neoplasm Atrophic vaginitis Overactive bladder Trauma Congenital abnormalities Urethral diverticulum Sexually transmitted diseases Herpes, Chlamydia, Trichomonas, Gonorrhea Urinary lithiasis Interstitial cystitis/painful bladder syndrome Sepsis from non-urologic source


9 Interstitial cystitis



10 Urethral diverticulum


11 Renal atrophy
12 Diagnosis of UTI Presentation of clinical symptoms Physical exam for atrophic vaginitis, urethral diverticulum etc Clean-catch midstream urine sample Chemical dipstick urinalysis Quantitative urine culture; In general > 100,000 colonies/ml diagnostic
13 Dipstick urinalysis evaluation Leukocyte esterase 63-90% specific Nitrite very specific for gram negative but only 50% sensitive **Bottom Line Positive dipstick + symptoms: consider treatment (and culture) Negative dipstick + symptoms: consider culture
14 When do you need radiologic imagining or further evaluation for diagnosis of UTI? Generally, uncomplicated cystitis or pyelonephritis does not benefit from imaging Consider CT, ultrasound, voiding cystourethrogram (VCUG) and cystoscopic or ureteroscopic evaluation for patients with *known anatomic abnormality *those who do not respond to treatment
15 Pathogenesis of urinary tract infections Ascending infection from periurethral area critical Hematogenous spread is uncommon Risk factors Reduced urine flow Obstruction, stricture, neurogenic bladder Factors that promote colonization Sexual activity, spermacide, estrogen depletion Facilitation of ascent Catheterization, incontinence, residual urine
16 What bacteria are associated with urinary infections and what pathogenic factors from both bacteria and the host contribute to colonization?
17 Uropathogens Escherichia coli (80% of outpatient UTIs) Klebsiella Enterobacter Proteus Pseudomonas Staphylococcus saprophyticus (5-15%) Enterococcus Candida Adenovirus Normal perineal flora: Lactobacillus, Corynebacteria, Staphylococcus, Streptococcus, anaerobes

18 -The bladder mucosal surface has antibacterial properties that eliminate some organisms, presumably through mucus trapping and a polymorphonuclear leukocyte response. -In addition, urine that has a low ph, high or very low osmolarity, high urea concentration, or high organic acid content inhibits bacterial growth -Abnormal micturition, a significant residual urine volume, or both will promote true infection. -There are also acquired and intrinsic host factors, as well as bacterial virulence factors, which increase the likelihood of development of UTI.
19 What are some correctable Urologic abnormalities that may provoke bacterial persistence?
20 Bacterial persistence Infected stones Fistula disease (colovesical, vesicovaginal) Unilateral infected atrophic kidneys Ureteral duplication and ectopic ureters Foreign bodies (such as retained ureteral stent) Urethral diverticula Unilateral medullary sponge kidneys Infected ureteral stump after nephrectomy Infected urachal or renal cyst Papillary necrosis


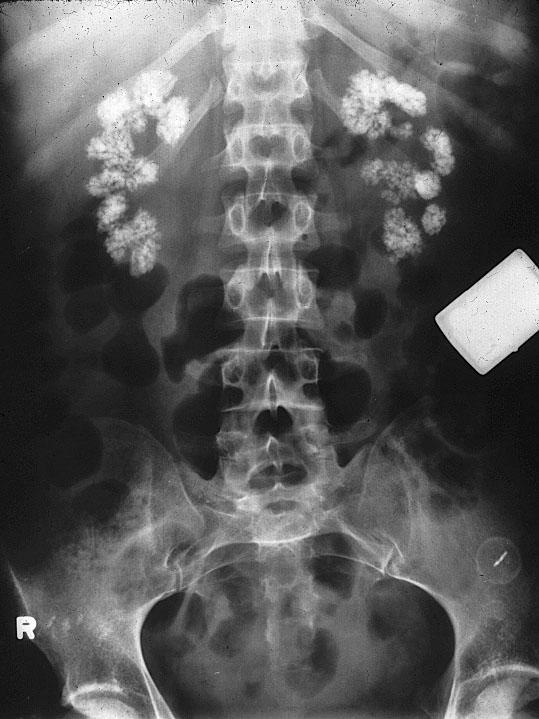
21 Medullary sponge kidneys



22 Kidney stones
23 Patient found on exam to have poor water intake, atrophic vaginitis, and urine dipstick consistent with acute bacterial infection. What are the treatment options?
24 Treatment Encourage hydration and behavioral measures to increase fluid intake Treat atrophic vaginitis with topical transvaginal estrogen if appropriate Determine if infection represents uncomplicated or complicated infection
25 Uncomplicated UTI treatment 3 day course of trimethoprim/sulfamethoxazole (TMP/SMX) For local TMP/SMX resistance pattern > 20%, consider fluoroquinolones Full 7 day course in patients with diabetes, long duration of symptoms, pregnancy, > 65 years old, past history of pyelonephritis
26 Complicated UTI treatment Culture essential Ampicillin + aminoglycoside Amp/Vancomycin + aminoglycoside or 3rd generation cephalosporin Adjust according to culture results If good clinical response, switch to oral agents in 48 hours Treat for 14 days
27 Follow-up and general rules of thumb Test for cure by repeat culture for pregnancy, pyelonephritis, and complicated or relapsing UTI Consider single dose post-coital self-treatment in select cases Do not treat asymptomatic bacteruria Treatment often not indicated for patients on self catheterization protocols

28
29 Urinary Incontinence Bladder dysfunction Urethral dysfunction
30 Bladder dysfunction Urge incontinence detrusor overactivity detrusor overactivity of nonneurogenic origin detrusor overactivity of neurogenic origin poor compliance Overflow incontinence
31 Urethral dysfunction Stress incontinence anatomic ( due to mobility of the bladder neck) Intrinsic sphincter deficiency (due to bladder neck dysfunction)
32 Transient Causes of Incontinence Cause Delirium Comment Incontinence may be secondary to delirium and will often stop when acute delirium resolves. Infection Symptomatic infection may increase urinary tract irritation and resulting incontinence Atrophic vaginitis Vaginitis may result in the same symptoms of an infection. Pharmacologic Sedatives Alcohol and long-acting benzodiazepines may cause confusion and secondary incontinence. Diuretics brisk diuresis may overwhelm the bladder's capacity and cause uninhibited detrusor contractions, resulting in urge incontinence. Anticholinergics Many nonprescription and prescription medications have anticholinergic properties. Side effects of anticholinergics include urinary retention with associated frequency and overflow incontinence. Alpha-adrenergics Tone in the bladder neck and proximal sphincter is increased by alpha adrenergic agonists and can manifest with urinary retention, particularly in men with prostatism. Alpha-antagonists Tone in the smooth muscles of the bladder neck and proximal sphincter is decreased with alpha adrenergic antagonists. Women treated with these drugs for hypertension may develop or have an exacerbation of stress incontinence. Psychological Depression may be occasionally associated with incontinence. Excessive urine production Excessive intake, diabetes, hypercalcemia, congestive heart failure and peripheral edema can all lead to polyuria, which can exacerbate incontinence. Restricted mobility Incontinence may be precipitated or aggravated if the patient is unable to toilet in a timely fashion. Stool impaction Patients with impacted stool can have urge or overflow urinary incontinence and may also have concomitant fecal incontinence.
33 Bladder dysfunction Storage Emptying Urge incontinence occurs when the bladder pressure is sufficient to overcome the sphincter mechanism. The sphincter is programmed to open during periods of elevated detrusor pressure and this occurs during normal voiding. Elevation in detrusor pressure may occur from abnormal bladder contractions also known as detrusor overactivity. Elevation in pressures also occur in a poorly compliant bladder.
34 Detrusor overactivity with UUI Idiopathic Neurologic disease (detrusor overactivity of neurogenic origin) Detrusor overactivity is exceedingly common in the elderly and may be associated with bladder outlet obstruction Poor bladder compliance results from loss of the visicoelastic features of the bladder or because of a change in neural-regulatory activity Patients with urgency incontinence may appreciate a sudden sensation to void which is difficult to defer.
35 Urge incontinence The patient may not be aware of the sensation of needing to void until they are actually leaking. The amount of leakage in patients with urgency incontinence is variable, depending on the patient's ability to suppress the contraction and the strength of their outlet. Patients with urgency incontinence will often manifest frequency, nocturia, and occasionally nocturnal enuresis. Overactive bladder has become the popularized term for describing patients with frequency and urgency with or without urgency incontinence.
36 Overflow incontinence Occurs at extreme bladder volumes or when the bladder volume reaches the limit of the urethral mechanism or the bladder's viscoelastic properties The loss of urine is driven by an elevation in detrusor pressure which overcomes the outlet resistance Overflow incontinence is seen with incomplete bladder emptying caused either by obstruction or poor bladder contractility Obstruction is rare in women but can result from severe pelvic prolapse or following surgery for stress incontinence Patients with overflow incontinence will complain of constant dribbling and often describe extreme frequency


37 Overflow incontinence continued Cystocele


38
39 Urethral dysfunction Stress incontinence anatomic ( due to mobility of the bladder neck) Intrinsic sphincter deficiency (due to bladder neck dysfunction)
40 Stress incontinence Leakage of urine with any sudden increase in abdominal pressure Incontinence associated with urethral hypermobility has been called anatomic incontinence, since the incontinence is due to malposition of the sphincter unit Displacement of the proximal urethra below the level of the pelvic floor does not allow for the appropriate transmission of abdominal pressure that normally aids in closing the urethra. ISD (Intrinsic sphincter deficiency) dysfunction of the proximal smooth muscle sphincter at the bladder neck and is often correlated with more severe stress incontinence.


41
42 History Diagnosis onset, frequency, and severity of incontinence pad usage obstructive symptoms previous treatments comorbidities including diabetes, hypertension, and medications Exam pelvic organ prolapse hypermobile urethra; what is the Q angle urethral diverticulum atrophic vaginitis rectal sphincter tone perineal sensation

43 Diagnosis voiding diary Mixed incontinence is very common, with at least 65% of patients with stress incontinence reporting associated urgency or urgency incontinence.
44 Diagnosis Urinalysis and culture hematuria, pyuria, glucosuria, or proteinuria Post void residual A normal PVR is less than 50 ml A PVR in excess of 200 ml when associated with urinary symptoms should raise concern A significant PVR may reflect either bladder outlet obstruction or poor bladder contractility The only way to distinguish outlet obstruction from poor contractility is with functional urodynamic testing
45 Diagnosis Urodynamics to accurately diagnose the etiology of patient's incontinence examine bladder compliance, detrusor overactivity, urethral function, and to rule out obstruction as a cause of either overflow or urgency incontinence.
46 Treatment Urge incontinence Stress incontinence Overflow incontinence
47 Urge incontinence First line treatment will involve behavioral measures such as timed voiding modification of fluid intake avoidance of bladder irritants bladder retraining, where the patient attempts to consciously delay voiding and to increase the interval between voids
48 Urge incontinence Medications Anticholinergic-antimuscarinics also used to decrease bladder pressure in patients with poor compliance combined with clean intermittent catheterization in patients who have a significant PVR prior to treatment, or in patients who develop retention while on anticholinergics Side effects: urinary retention, dry mouth, constipation, nausea, blurred vision, tachycardia, drowsiness and confusion contraindicated in patients with narrow-angle glaucoma caution should be employed utilizing anticholinergic medications in the elderly Beta 3 adrenergic receptor agonists promote detrusor relaxation during bladder filling and may reduce urgency incontinence without many of the adverse side effects of antimuscarinic agents
49 Urge incontinence Surgical intervention Indicated when medications failed Botox Lasts average of 10 months Sacral nerve stimulation



50 Sacral nerve stimulation -Urge incontinence refractory to medications -Urinary urgency and frequency refractory to medications -Idiopathic nonobstructive urinary retention -Fecal incontinence
51 Stress incontinence Pelvic floor exercises Kegels Weighted vaginal cones Pessaries that support the bladder neck Alpha agonists ; Sudafed The bladder neck and proximal urethra have abundant alpha receptors. Activation of these receptors by alpha-agonists leads to an increase in smooth muscle tone


52 Stress incontinence Urethral bulking agents Urethral sling


53 Sling Studies have shown an 88 to 95 percent success rate in correcting urinary incontinence with the sling procedure.
54 Overflow incontinence Overflow incontinence is treated by emptying the bladder Poor detrusor contractility CIC Urinary diversion Suprapubic cystotomy, Ileal conduit etc If the cause of overflow is obstruction, then relieving the obstruction should lead to improved emptying Cystocele repair or pessary Urethrolysis
55 References Pontari, M. AUA Core Curriculum for Residents: Urinary Tract Infections Shoskes, D. (2011): Urinary Tract Infections Retrieved From: The American Urological Association Educational Review Manual in Urology: 3rd Edition Chapter: 23 Page: Smith's General Urology 16th edition Tanagho and McAninch, eds. Chapter 13. "Bacterial Infections of the Urinary Tract" Nguyen, Hiep. pp Stamm, WE, Norrby, SR. Urinary Tract Infections: Disease Panorama and Challenges. J Infect Dis Mar 1; 183 Suppl 1:S1-4. Hooten, TM, Scholes, D, Hughes, JP, et al. A Prospective Study of Risk Factors for Symptomatic Urinary Tract Infection in Young Women. NEJM 1996; 335: Nitti VW, Blaivas JG: Urinary incontinence: Epidemiology, pathophysiology, evaluation, and management overview, in Wein AJ, Kavoussi LR, Novick AC, Partin AW, Peters CA (eds): CAMPBELL'S UROLOGY, ed 9. Philadelphia, WB Saunders Co, 2007, vol 3, chap 60, p Burgio K. L et al. Behavioural vs drug treatment for urge urinary incontinence in older women. JAMA 280, 1995, Dmchowski, Blaivas, Gormley et al. Female Stress Urinary Incontinence Clinical Guidelines Panel summary report on surgical management of female stress urinary incontinence. The American Urological Association. J Urol Ward KL, Hilton P: A randomized trial of colpsuspension and tension-free vaginal tape (TVT) for primary genuine stress incontinence: 2 year follow-up. Int Urogynecol J Pelvic Floor Dysfunct 12 (supple 2): S7-8, Gormley E.A. Urinary Incontinence. In Rakel, Robert E. (ed.) Conn's Current Therapy. W. B. Saunders Co, Caruso L.B., Silliman R.A. Geriatric Medicine. In Fauci, et. Al (eds) Harrison's Principles of Internal Medicine, 17th Edition. 2008, pages Richter HE, Albo ME, Zyczynski HM, et al. Retropubic versus transobturator midurethral slings for stress incontinence. N Engl J Med 2010, 362:





56 Thank You
MODULE 9: URINARY INCONTINENCE
 MODULE 9: URINARY INCONTINENCE KEYWORDS: PROSTATIC HYPERTROPHY, PROSTATIC HYPERPLASIA, PSA, VOIDING DYSFUNCTION, LOWER URINARY TRACT SYMPTOMS (LUTS). Learning Objectives At the end of this clerkship, the
MODULE 9: URINARY INCONTINENCE KEYWORDS: PROSTATIC HYPERTROPHY, PROSTATIC HYPERPLASIA, PSA, VOIDING DYSFUNCTION, LOWER URINARY TRACT SYMPTOMS (LUTS). Learning Objectives At the end of this clerkship, the
Overactive Bladder: Diagnosis and Approaches to Treatment
 Overactive Bladder: Diagnosis and Approaches to Treatment A Hidden Condition* Many Many patients self-manage by voiding frequently, reducing fluid intake, and wearing pads Nearly Nearly two-thirds thirds
Overactive Bladder: Diagnosis and Approaches to Treatment A Hidden Condition* Many Many patients self-manage by voiding frequently, reducing fluid intake, and wearing pads Nearly Nearly two-thirds thirds
Objectives. Prevalence of Urinary Incontinence URINARY INCONTINENCE: EVALUATION AND CURRENT TREATMENT OPTIONS
 URINARY INCONTINENCE: EVALUATION AND CURRENT TREATMENT OPTIONS Lisa S Pair, MSN, CRNP Division of Urogynecology and Pelvic Reconstructive Surgery Department of Obstetrics and Gynecology University of Alabama
URINARY INCONTINENCE: EVALUATION AND CURRENT TREATMENT OPTIONS Lisa S Pair, MSN, CRNP Division of Urogynecology and Pelvic Reconstructive Surgery Department of Obstetrics and Gynecology University of Alabama
URINARY TRACT INFECTIONS
 URINARY TRACT INFECTIONS Learning Objectives Identify signs and symptoms that may indicate presence of UTI (both complicated and uncomplicated) List common causative organisms and risk factors for UTIs
URINARY TRACT INFECTIONS Learning Objectives Identify signs and symptoms that may indicate presence of UTI (both complicated and uncomplicated) List common causative organisms and risk factors for UTIs
UTI are the most common genitourinary disease of childhood. The prevalence of UTI at all ages is girls and 1% of boys.
 UTI are the most common genitourinary disease of childhood. The prevalence of UTI at all ages is girls and 1% of boys. 1-3% of Below 1 yr. male: female ratio is 4:1 especially among uncircumcised males,
UTI are the most common genitourinary disease of childhood. The prevalence of UTI at all ages is girls and 1% of boys. 1-3% of Below 1 yr. male: female ratio is 4:1 especially among uncircumcised males,
The Management of Female Urinary Incontinence. Part 1: Aetiology and Investigations
 The Management of Female Urinary Incontinence Part 1: Aetiology and Investigations Dr Oseka Onuma Gynaecologist and Pelvic Reconstructive Surgeon 4 Robe Terrace Medindie SA 5081 Urinary incontinence has
The Management of Female Urinary Incontinence Part 1: Aetiology and Investigations Dr Oseka Onuma Gynaecologist and Pelvic Reconstructive Surgeon 4 Robe Terrace Medindie SA 5081 Urinary incontinence has
Lower Urinary Tract Symptoms (LUTS) and Nurse-Led Clinics. Sean Diver Urology Advanced Nurse Practitioner candidate Letterkenny University Hospital
 and Nurse-Led Clinics. Sean Diver Urology Advanced Nurse Practitioner candidate Letterkenny University Hospital") Lower Urinary Tract Symptoms (LUTS) and Nurse-Led Clinics Sean Diver Urology Advanced Nurse Practitioner candidate Letterkenny University Hospital 01/02/2018 Lower Urinary Tract Symptoms LUTS - one of
Lower Urinary Tract Symptoms (LUTS) and Nurse-Led Clinics Sean Diver Urology Advanced Nurse Practitioner candidate Letterkenny University Hospital 01/02/2018 Lower Urinary Tract Symptoms LUTS - one of
Urogynaecology. Colm McAlinden
 Urogynaecology Colm McAlinden Definitions Urinary incontinence compliant of any involuntary leakage of urine with many different causes Two main types: Stress Urge Definitions Nocturia: More than a single
Urogynaecology Colm McAlinden Definitions Urinary incontinence compliant of any involuntary leakage of urine with many different causes Two main types: Stress Urge Definitions Nocturia: More than a single
Lower Urinary Tract Symptoms K Kuruvilla Zachariah Associate Specialist
 Lower Urinary Tract Symptoms K Kuruvilla Zachariah Associate Specialist Lower Urinary Tract Symptoms Storage Symptoms Frequency, urgency, incontinence, Nocturia Voiding Symptoms Hesitancy, poor flow, intermittency,
Lower Urinary Tract Symptoms K Kuruvilla Zachariah Associate Specialist Lower Urinary Tract Symptoms Storage Symptoms Frequency, urgency, incontinence, Nocturia Voiding Symptoms Hesitancy, poor flow, intermittency,
Urogynecology in EDS. Joan L. Blomquist, MD Greater Baltimore Medical Center August 2018
 Urogynecology in EDS Joan L. Blomquist, MD Greater Baltimore Medical Center August 2018 One in three like me Voiding Issues Frequency/Urgency Urinary Incontinence neurogenic bladder Neurologic supply
Urogynecology in EDS Joan L. Blomquist, MD Greater Baltimore Medical Center August 2018 One in three like me Voiding Issues Frequency/Urgency Urinary Incontinence neurogenic bladder Neurologic supply
Urinary Incontinence for the Primary Care Provider
 Urinary Incontinence for the Primary Care Provider Diana J Scott FNP-BC https://youtu.be/gmzaue1ojn4 1 Assessment of Urinary Incontinence Urge Stress Mixed Other overflow, postural, continuous, insensible,
Urinary Incontinence for the Primary Care Provider Diana J Scott FNP-BC https://youtu.be/gmzaue1ojn4 1 Assessment of Urinary Incontinence Urge Stress Mixed Other overflow, postural, continuous, insensible,
Urogynecology ICD-9 to ICD-10 Crosswalks
 1100 Wayne Ave, Suite 825 Silver Spring, MD 20910 301.273.0570 Fax 301.273.0778 info@augs.org www.augs.org Urogynecology ICD-9 to ICD-10 Crosswalks ICD 9 ICD 9 Description ICD 10 Code ICD 10 Description
1100 Wayne Ave, Suite 825 Silver Spring, MD 20910 301.273.0570 Fax 301.273.0778 info@augs.org www.augs.org Urogynecology ICD-9 to ICD-10 Crosswalks ICD 9 ICD 9 Description ICD 10 Code ICD 10 Description
Dr. Aso Urinary Symptoms
 Haematuria The presence of blood in the urine (haematuria) is always abnormal and may be the only indication of pathology in the urinary tract. False positive stick tests and the discolored urine caused
Haematuria The presence of blood in the urine (haematuria) is always abnormal and may be the only indication of pathology in the urinary tract. False positive stick tests and the discolored urine caused
Urinary tract infection. Mohamed Ahmed Fouad Lecturer of pediatrics Jazan faculty of medicine
 Urinary tract infection Mohamed Ahmed Fouad Lecturer of pediatrics Jazan faculty of medicine Objectives To differentiate between types of urinary tract infections To recognize the epidemiology of UTI in
Urinary tract infection Mohamed Ahmed Fouad Lecturer of pediatrics Jazan faculty of medicine Objectives To differentiate between types of urinary tract infections To recognize the epidemiology of UTI in
Various Types. Ralph Boling, DO, FACOG
 Various Types Ralph Boling, DO, FACOG The goal of this lecture is to increase assessment and treatment abilities for physicians managing urinary incontinence (UI) patients. 1. Effectively communicate with
Various Types Ralph Boling, DO, FACOG The goal of this lecture is to increase assessment and treatment abilities for physicians managing urinary incontinence (UI) patients. 1. Effectively communicate with
MODULE 2: ADULT URINARY TRACT INFECTIONS
 MODULE 2: ADULT URINARY TRACT INFECTIONS KEYWORDS: Urinary tract infection (UTI); cystitis; pyelonephritis; uropathogens; antibiotics LEARNING OBJECTIVES At the end of this clerkship, the learner will
MODULE 2: ADULT URINARY TRACT INFECTIONS KEYWORDS: Urinary tract infection (UTI); cystitis; pyelonephritis; uropathogens; antibiotics LEARNING OBJECTIVES At the end of this clerkship, the learner will
UTI IN ELDERLY. Zeinab Naderpour
 UTI IN ELDERLY Zeinab Naderpour Urinary tract infection (UTI) is the most frequent bacterial infection in elderly populations. While urinary infection in the elderly person is usually asymptomatic, symptomatic
UTI IN ELDERLY Zeinab Naderpour Urinary tract infection (UTI) is the most frequent bacterial infection in elderly populations. While urinary infection in the elderly person is usually asymptomatic, symptomatic
URINARY INCONTINENCE. Urology Division, Surgery Department Medical Faculty, University of Sumatera Utara
 URINARY INCONTINENCE Urology Division, Surgery Department Medical Faculty, University of Sumatera Utara Definition The involuntary loss of urine May denote a symptom, a sign or a condition Symptom the
URINARY INCONTINENCE Urology Division, Surgery Department Medical Faculty, University of Sumatera Utara Definition The involuntary loss of urine May denote a symptom, a sign or a condition Symptom the
The Neurogenic Bladder
 The Neurogenic Bladder Outline Brandon Haynes, MD Resident Physician Department of Urology Jelena Svircev, MD Assistant Professor Department of Rehabilitation Medicine Anatomy and Bladder Physiology Bladder
The Neurogenic Bladder Outline Brandon Haynes, MD Resident Physician Department of Urology Jelena Svircev, MD Assistant Professor Department of Rehabilitation Medicine Anatomy and Bladder Physiology Bladder
Disclosures. Geriatric Incontinence and Voiding Dysfunction. Agenda. Agenda. UI: a Geriatric Syndrome. Geriatric Syndromes 9/7/2018.
 Disclosures Geriatric Incontinence and Voiding Dysfunction None Shachi Tyagi MD, MS Assistant Professor Division of Geriatric Medicine University of Pittsburgh Medical Center UI: a Geriatric Syndrome Geriatric
Disclosures Geriatric Incontinence and Voiding Dysfunction None Shachi Tyagi MD, MS Assistant Professor Division of Geriatric Medicine University of Pittsburgh Medical Center UI: a Geriatric Syndrome Geriatric
SHABNAM TEHRANI M.D., MPH ASSISTANT PROFESSOR OF INFECTIOUS DISEASESE &TROPICAL MEDICINE RESEARCH CENTER, SHAHID BEHESHTI UNIVERSITY OF MEDICAL
 URINARY TRACT INFECTION SHABNAM TEHRANI M.D., MPH ASSISTANT PROFESSOR OF INFECTIOUS DISEASESE &TROPICAL MEDICINE RESEARCH CENTER, SHAHID BEHESHTI UNIVERSITY OF MEDICAL SCIENCES Definition inflammatory
URINARY TRACT INFECTION SHABNAM TEHRANI M.D., MPH ASSISTANT PROFESSOR OF INFECTIOUS DISEASESE &TROPICAL MEDICINE RESEARCH CENTER, SHAHID BEHESHTI UNIVERSITY OF MEDICAL SCIENCES Definition inflammatory
Urodynamic findings in women with insensible incontinence
 bs_bs_banner International Journal of Urology (2013) 20, 429 433 doi: 10.1111/j.1442-2042.2012.03146.x Original Article: Clinical Investigation Urodynamic findings in women with insensible Benjamin M Brucker,
bs_bs_banner International Journal of Urology (2013) 20, 429 433 doi: 10.1111/j.1442-2042.2012.03146.x Original Article: Clinical Investigation Urodynamic findings in women with insensible Benjamin M Brucker,
Incontinence: Risks, Causes and Care
 Welcome To Incontinence: Risks, Causes and Care Presented by Kamal Masaki, MD Professor and Chair Department of Geriatric Medicine John A. Burns School of Medicine, UH Manoa September 5, 2018 10:00 11:00
Welcome To Incontinence: Risks, Causes and Care Presented by Kamal Masaki, MD Professor and Chair Department of Geriatric Medicine John A. Burns School of Medicine, UH Manoa September 5, 2018 10:00 11:00
Tools for Evaluation. Urodynamics Case Studies. Case 1. Evaluation. Case 1. Bladder Diary SUI 19/01/2018
 Urodynamics Case Studies Christopher K. Payne, MD Vista Urology & Pelvic Pain Partners Emeritus Professor of Urology, Stanford University Tools for Evaluation Ears, Eyes, and Brain Bladder diary Stress
Urodynamics Case Studies Christopher K. Payne, MD Vista Urology & Pelvic Pain Partners Emeritus Professor of Urology, Stanford University Tools for Evaluation Ears, Eyes, and Brain Bladder diary Stress
Bacterial Infections of the Urinary System *
 OpenStax-CNX module: m64804 1 Bacterial Infections of the Urinary System * Douglas Risser This work is produced by OpenStax-CNX and licensed under the Creative Commons Attribution License 4.0 1 Learning
OpenStax-CNX module: m64804 1 Bacterial Infections of the Urinary System * Douglas Risser This work is produced by OpenStax-CNX and licensed under the Creative Commons Attribution License 4.0 1 Learning
Management of Urinary Incontinence in Older Women. Dr. Cecilia Cheon Department of Obs. & Gyn. Queen Elizabeth Hospital
 Management of Urinary Incontinence in Older Women Dr. Cecilia Cheon Department of Obs. & Gyn. Queen Elizabeth Hospital Epidemiology Causes Investigation Treatment Conclusion Elderly Women High prevalence
Management of Urinary Incontinence in Older Women Dr. Cecilia Cheon Department of Obs. & Gyn. Queen Elizabeth Hospital Epidemiology Causes Investigation Treatment Conclusion Elderly Women High prevalence
Incontinence; Lets talk about it. Karanvir Virk M.D. Minimally Invasive and Pelvic Reconstructive Surgery
 Incontinence; Lets talk about it Karanvir Virk M.D. Minimally Invasive and Pelvic Reconstructive Surgery Select the most appropriate subtitle for this talk A: Bladders gone wild! B: There s no such thing
Incontinence; Lets talk about it Karanvir Virk M.D. Minimally Invasive and Pelvic Reconstructive Surgery Select the most appropriate subtitle for this talk A: Bladders gone wild! B: There s no such thing
Overactive Bladder Syndrome
 Overactive Bladder Syndrome behavioural modifications to pharmacological and surgical treatments Dr Jos Jayarajan Urologist Austin Health, Eastern Health Warringal Private, Northpark Private, Epworth Overactive
Overactive Bladder Syndrome behavioural modifications to pharmacological and surgical treatments Dr Jos Jayarajan Urologist Austin Health, Eastern Health Warringal Private, Northpark Private, Epworth Overactive
NON-Neurogenic Chronic Urinary Retention AUA White Paper
 NON-Neurogenic Chronic Urinary Retention AUA White Paper Great Lakes SUNA Inside Urology March 16, 2018 Michelle J. Lajiness FNP-BC Nurse Practitioner DMC Urology Incidence Really unknown Lack consensus
NON-Neurogenic Chronic Urinary Retention AUA White Paper Great Lakes SUNA Inside Urology March 16, 2018 Michelle J. Lajiness FNP-BC Nurse Practitioner DMC Urology Incidence Really unknown Lack consensus
EMPIRICAL TREATMENT OF SELECT INFECTIONS ADULT GUIDELINES. Refer to VIHA Algorithm for the empiric treatment of Urinary Tract Infection
 URINARY TRACT Refer to VIHA Algorithm for the empiric treatment of Urinary Tract Infection and Asymptomatic Bacteriuria on the VIHA Intranet: https://intranet.viha.ca/departments/pharmacy/clinical_pharmacy/pages/infec
URINARY TRACT Refer to VIHA Algorithm for the empiric treatment of Urinary Tract Infection and Asymptomatic Bacteriuria on the VIHA Intranet: https://intranet.viha.ca/departments/pharmacy/clinical_pharmacy/pages/infec
REVIEW OF CAUSES, EVALUATION, AND TREATMENTS URINARY INCONTINENCE 101
 REVIEW OF CAUSES, EVALUATION, AND TREATMENTS URINARY INCONTINENCE 101 March 5, 2014 Kevin E Miller, MD Department of Obstetrics and Gynecology University of Kansas School of Medicine- Wichita URINARY INCONTINENCE
REVIEW OF CAUSES, EVALUATION, AND TREATMENTS URINARY INCONTINENCE 101 March 5, 2014 Kevin E Miller, MD Department of Obstetrics and Gynecology University of Kansas School of Medicine- Wichita URINARY INCONTINENCE
Urinary tract infections Dr. Hala Al Daghistani
 Urinary tract infections Dr. Hala Al Daghistani UTIs are considered to be one of the most common bacterial infections. Diagnosis depends on the symptoms, urinalysis, and urine culture. UTIs occur more
Urinary tract infections Dr. Hala Al Daghistani UTIs are considered to be one of the most common bacterial infections. Diagnosis depends on the symptoms, urinalysis, and urine culture. UTIs occur more
Management, Evaluation, and Treatment of Overactive Bladder and Urinary Incontinence
 Management, Evaluation, and Treatment of Overactive Bladder and Urinary Incontinence Arthur Mourtzinos, MD, MBA Co-Vice Chair, Institute of Urology Director, Continence Center Assistant Professor of Urology,
Management, Evaluation, and Treatment of Overactive Bladder and Urinary Incontinence Arthur Mourtzinos, MD, MBA Co-Vice Chair, Institute of Urology Director, Continence Center Assistant Professor of Urology,
Voiding Dysfunction Block lecture, 5 th year student. Choosak Pripatnanont, Department of Surgery, PSU.
 Voiding Dysfunction 2009 Block lecture, 5 th year student. Choosak Pripatnanont, Department of Surgery, PSU. Objectives Understand and explain physiologic function and dysfunction of lower urinary tract.
Voiding Dysfunction 2009 Block lecture, 5 th year student. Choosak Pripatnanont, Department of Surgery, PSU. Objectives Understand and explain physiologic function and dysfunction of lower urinary tract.
Management of Female Stress Incontinence
 Management of Female Stress Incontinence Dr. Arvind Goyal Associate Professor (Urology& Renal Transplant) Dayanand Medical College & Hospital, Ludhiana, Punjab, India Stress Incontinence Involuntary loss
Management of Female Stress Incontinence Dr. Arvind Goyal Associate Professor (Urology& Renal Transplant) Dayanand Medical College & Hospital, Ludhiana, Punjab, India Stress Incontinence Involuntary loss
It is an infection affecting any of the following parts like kidney,ureter,bladder or urethra
 UTI Dr jayaprakash.k.p,asst prof,ich,govt.medical college,kottayam What is UTI? It is an infection affecting any of the following parts like kidney,ureter,bladder or urethra What is prevalence of UTI?
UTI Dr jayaprakash.k.p,asst prof,ich,govt.medical college,kottayam What is UTI? It is an infection affecting any of the following parts like kidney,ureter,bladder or urethra What is prevalence of UTI?
Urinary Tract Infections
 Urinary Tract Infections Michelle Eslami, M.D., FACP Professor of Medicine Division of Geriatrics David Geffen SOM at UCLA Urinary Tract Infection (UTI) One of most common infections in outpatient and
Urinary Tract Infections Michelle Eslami, M.D., FACP Professor of Medicine Division of Geriatrics David Geffen SOM at UCLA Urinary Tract Infection (UTI) One of most common infections in outpatient and
Advanced Care for Female Overactive Bladder & Urinary Incontinence. Department of Urology Kaiser Permanente Santa Rosa
 Advanced Care for Female Overactive Bladder & Urinary Incontinence Department of Urology Kaiser Permanente Santa Rosa Goals Participants will: Review normal urinary tract anatomy and function Understand
Advanced Care for Female Overactive Bladder & Urinary Incontinence Department of Urology Kaiser Permanente Santa Rosa Goals Participants will: Review normal urinary tract anatomy and function Understand
Urinary Incontinence. Lee A. Jennings, MD, MSHS. Assistant Professor Reynolds Department of Geriatrics University of Oklahoma Health Sciences Center
 Urinary Incontinence Lee A. Jennings, MD, MSHS Assistant Professor Reynolds Department of Geriatrics University of Oklahoma Health Sciences Center Slides adapted from Alison Moore, MD, MPH University of
Urinary Incontinence Lee A. Jennings, MD, MSHS Assistant Professor Reynolds Department of Geriatrics University of Oklahoma Health Sciences Center Slides adapted from Alison Moore, MD, MPH University of
MANAGING BENIGN PROSTATIC HYPERTROPHY IN PRIMARY CARE DR GEORGE G MATHEW CONSULTANT FAMILY PHYSICIAN FELLOW IN SEXUAL & REPRODUCTIVE HEALTH
 MANAGING BENIGN PROSTATIC HYPERTROPHY IN PRIMARY CARE DR GEORGE G MATHEW CONSULTANT FAMILY PHYSICIAN FELLOW IN SEXUAL & REPRODUCTIVE HEALTH INTRODUCTION (1) Part of male sexual reproductive organ Size
MANAGING BENIGN PROSTATIC HYPERTROPHY IN PRIMARY CARE DR GEORGE G MATHEW CONSULTANT FAMILY PHYSICIAN FELLOW IN SEXUAL & REPRODUCTIVE HEALTH INTRODUCTION (1) Part of male sexual reproductive organ Size
Urinary tract infections, renal malformations and scarring
 Urinary tract infections, renal malformations and scarring Yaacov Frishberg, MD Division of Pediatric Nephrology Shaare Zedek Medical Center Jerusalem, ISRAEL UTI - definitions UTI = growth of bacteria
Urinary tract infections, renal malformations and scarring Yaacov Frishberg, MD Division of Pediatric Nephrology Shaare Zedek Medical Center Jerusalem, ISRAEL UTI - definitions UTI = growth of bacteria
Management of OAB. Lynsey McHugh. Consultant Urological Surgeon. Lancashire Teaching Hospitals
 Management of OAB Lynsey McHugh Consultant Urological Surgeon Lancashire Teaching Hospitals Summary Physiology Epidemiology Definitions NICE guidelines Evaluation Conservative management Medical management
Management of OAB Lynsey McHugh Consultant Urological Surgeon Lancashire Teaching Hospitals Summary Physiology Epidemiology Definitions NICE guidelines Evaluation Conservative management Medical management
Lecture 1: Genito-urinary system. ISK
 Urinary Tract Infections Lecture 1: Genito-urinary system. ISK 07 08 2009. Getting Clear on the Terminology UTI Cystitis Urosepsis Asymptomatic Bacteriuria Asymptomatic UTI Pyuria Symptomatic UTI Pylonephritis
Urinary Tract Infections Lecture 1: Genito-urinary system. ISK 07 08 2009. Getting Clear on the Terminology UTI Cystitis Urosepsis Asymptomatic Bacteriuria Asymptomatic UTI Pyuria Symptomatic UTI Pylonephritis
Physiology & Neurophysiology of lower U.T.
 Physiology & Neurophysiology of lower U.T. Classification of voiding dysfunction Evaluation of a child with voiding dysfunction Management Storage Ø Adequate volume of urine Ø At LOW pressure Ø With NO
Physiology & Neurophysiology of lower U.T. Classification of voiding dysfunction Evaluation of a child with voiding dysfunction Management Storage Ø Adequate volume of urine Ø At LOW pressure Ø With NO
The McMaster at night Pediatric Curriculum
 The McMaster at night Pediatric Curriculum Robinson, J, et al. and the Canadian Pediatric Society. Urinary tract infection in infants and children: Diagnosis and management. Pediatr Child Health 2014;
The McMaster at night Pediatric Curriculum Robinson, J, et al. and the Canadian Pediatric Society. Urinary tract infection in infants and children: Diagnosis and management. Pediatr Child Health 2014;
Prolapse and Urogynae Incontinence. Lucy Tiffin and Hannah Wheldon-Holmes
 Prolapse and Urogynae Incontinence Lucy Tiffin and Hannah Wheldon-Holmes 66 year old woman with incontinence PC: 7 year Hx of urgency, frequency, nocturia (incl. incontinence at night), and stress incontinence
Prolapse and Urogynae Incontinence Lucy Tiffin and Hannah Wheldon-Holmes 66 year old woman with incontinence PC: 7 year Hx of urgency, frequency, nocturia (incl. incontinence at night), and stress incontinence
Module 3 Causes Of Urinary Incontinence
 Causes Of Urinary Incontinence V4: Last Reviewed September 2017 Learning Outcomes Appreciate the numerous requirements and skills necessary for the person to achieve and maintain urinary continence Discuss
Causes Of Urinary Incontinence V4: Last Reviewed September 2017 Learning Outcomes Appreciate the numerous requirements and skills necessary for the person to achieve and maintain urinary continence Discuss
URINARY TRACT INFECTIONS 3 rd Y Med Students. Prof. Dr. Asem Shehabi Faculty of Medicine, University of Jordan
 URINARY TRACT INFECTIONS 3 rd Y Med Students Prof. Dr. Asem Shehabi Faculty of Medicine, University of Jordan Urinary Tract Infections-1 Normal urine is sterile.. It contains fluids, salts, and waste products,
URINARY TRACT INFECTIONS 3 rd Y Med Students Prof. Dr. Asem Shehabi Faculty of Medicine, University of Jordan Urinary Tract Infections-1 Normal urine is sterile.. It contains fluids, salts, and waste products,
Urinary Incontinence. Alison A Moore, MD, FACP
 Urinary Incontinence Alison A Moore, MD, FACP Professor of Medicine/Geriatric Medicine David Geffen School of Medicine at UCLA Department of Medicine, Division of Geriatrics Urinary Incontinence (UI) Involuntary
Urinary Incontinence Alison A Moore, MD, FACP Professor of Medicine/Geriatric Medicine David Geffen School of Medicine at UCLA Department of Medicine, Division of Geriatrics Urinary Incontinence (UI) Involuntary
NEUROGENIC BLADDER. Dr Harriet Grubb Dr Alison Seymour Dr Alexander Joseph
 NEUROGENIC BLADDER Dr Harriet Grubb Dr Alison Seymour Dr Alexander Joseph OUTLINE Definition Anatomy and physiology of bladder function Types of neurogenic bladder Assessment and management Complications
NEUROGENIC BLADDER Dr Harriet Grubb Dr Alison Seymour Dr Alexander Joseph OUTLINE Definition Anatomy and physiology of bladder function Types of neurogenic bladder Assessment and management Complications
Urinary Incontinence. Vibhash Mishra Consultant Urological Surgeon Royal Free Hospital
 Urinary Incontinence Vibhash Mishra Consultant Urological Surgeon Royal Free Hospital Affects women of all ages Impacts physical, psychological & social wellbeing Impact on families & carers Costs the
Urinary Incontinence Vibhash Mishra Consultant Urological Surgeon Royal Free Hospital Affects women of all ages Impacts physical, psychological & social wellbeing Impact on families & carers Costs the
Geriatric Urinary Incontinence
 Geriatric Urinary Incontinence Neil M. Resnick, MD Thomas Detre Professor of Medicine Chief, Division of Geriatric Medicine University of Pittsburgh/UPMC UI: The Problem Prevalence in elderly 33% Morbidity
Geriatric Urinary Incontinence Neil M. Resnick, MD Thomas Detre Professor of Medicine Chief, Division of Geriatric Medicine University of Pittsburgh/UPMC UI: The Problem Prevalence in elderly 33% Morbidity
11/15/2010. Asymptomatic Bacteriuria UTI. Symptomatic UTI. Asymptomatic UTI. Cystitis. Pylonephritis. Pyuria. Urosepsis
 Urinary Tract Infections Renal vein Inferior vena cava Urinary bladder Urethra Renal artery Kidney Aorta Ureter Lecture 1: Genito-urinary system. 06 08 2010. (a) Sherwood Fig. 12-6a, p.530 An introduction
Urinary Tract Infections Renal vein Inferior vena cava Urinary bladder Urethra Renal artery Kidney Aorta Ureter Lecture 1: Genito-urinary system. 06 08 2010. (a) Sherwood Fig. 12-6a, p.530 An introduction
Nursing Care for Children with Genitourinary Dysfunction I
 Nursing Care for Children with Genitourinary Dysfunction I 1 Assessment of renal function Clinical manifestations Laboratory tests Urinalysis Urine culture and sensitivity Renal/bladder ultrasound Testicular
Nursing Care for Children with Genitourinary Dysfunction I 1 Assessment of renal function Clinical manifestations Laboratory tests Urinalysis Urine culture and sensitivity Renal/bladder ultrasound Testicular
December Objectives. Housekeeping Announcements
 Comprehensive Review of Regulations & Interpretive Guidance for Top F-Tags Bowel/Bladder Incontinence, Catheter, & UTI Requirements F690 Objectives 1. Identify the regulatory requirements related to Bowel/Bladder
Comprehensive Review of Regulations & Interpretive Guidance for Top F-Tags Bowel/Bladder Incontinence, Catheter, & UTI Requirements F690 Objectives 1. Identify the regulatory requirements related to Bowel/Bladder
URINARY TRACT INFECTIONS 3 rd Y Med Students. Prof. Dr. Asem Shehabi Faculty of Medicine, University of Jordan
 URINARY TRACT INFECTIONS 3 rd Y Med Students Prof. Dr. Asem Shehabi Faculty of Medicine, University of Jordan Urinary Tract Infections-1 Normal urine is sterile in urinary bladder.. It contains fluids,
URINARY TRACT INFECTIONS 3 rd Y Med Students Prof. Dr. Asem Shehabi Faculty of Medicine, University of Jordan Urinary Tract Infections-1 Normal urine is sterile in urinary bladder.. It contains fluids,
Anatomy kidney ureters bladder urethra upper lower
 Urinary tract Anatomy The urinary tract consists of the kidney, ureters, bladder, and urethra. Urinary tract infections can be either: upper or lower based primarily on the anatomic location of the infection.
Urinary tract Anatomy The urinary tract consists of the kidney, ureters, bladder, and urethra. Urinary tract infections can be either: upper or lower based primarily on the anatomic location of the infection.
Diagnostic approach and microorganism resistance pattern in UTI Yeva Rosana, Anis Karuniawati, Yulia Rosa, Budiman Bela
 Diagnostic approach and microorganism resistance pattern in UTI Yeva Rosana, Anis Karuniawati, Yulia Rosa, Budiman Bela Microbiology Department Medical Faculty, University of Indonesia Urinary Tract Infection
Diagnostic approach and microorganism resistance pattern in UTI Yeva Rosana, Anis Karuniawati, Yulia Rosa, Budiman Bela Microbiology Department Medical Faculty, University of Indonesia Urinary Tract Infection
INCONTINENCE AND OTHER UROLOGICAL DILEMMAS DR. ANNA LAWRENCE UROLOGIST AUCKLAND HOSPITAL 161 UROLOGY
 INCONTINENCE AND OTHER UROLOGICAL DILEMMAS DR. ANNA LAWRENCE UROLOGIST AUCKLAND HOSPITAL 161 UROLOGY COVERING INCONTINENCE BE ON JUST NAPPIES CATHETERS TYPES AVAILABLE AND WHEN TO USE THEM JJ STENTS???
INCONTINENCE AND OTHER UROLOGICAL DILEMMAS DR. ANNA LAWRENCE UROLOGIST AUCKLAND HOSPITAL 161 UROLOGY COVERING INCONTINENCE BE ON JUST NAPPIES CATHETERS TYPES AVAILABLE AND WHEN TO USE THEM JJ STENTS???
Mr. GIT KAH ANN. Pakar Klinikal Urologi Hospital Kuala Lumpur.
 Mr. GIT KAH ANN Pakar Klinikal Urologi Hospital Kuala Lumpur drgitka@yahoo.com 25 Jan 2007 HIGHLIGHTS Introduction ICS Definition Making a Diagnosis Voiding Chart Investigation Urodynamics Ancillary Investigations
Mr. GIT KAH ANN Pakar Klinikal Urologi Hospital Kuala Lumpur drgitka@yahoo.com 25 Jan 2007 HIGHLIGHTS Introduction ICS Definition Making a Diagnosis Voiding Chart Investigation Urodynamics Ancillary Investigations
John Laughlin 4 th year Cardiff University Medical Student
 John Laughlin 4 th year Cardiff University Medical Student Prolapse/incontinence You need to know: Pelvic floor anatomy in relation to uterovaginal support and continence The classification of uterovaginal
John Laughlin 4 th year Cardiff University Medical Student Prolapse/incontinence You need to know: Pelvic floor anatomy in relation to uterovaginal support and continence The classification of uterovaginal
Diagnosis and treatment of overactive bladder (non-neurogenic) in adults: AUA/SUFU guideline.
 in adults: AUA/SUFU guideline.") Diagnosis and treatment of overactive bladder (non-neurogenic) in adults: AUA/SUFU guideline. TARGET POPULATION Eligibility Decidable (Y or N) Inclusion Criterion non-neurogenic OAB Exclusion Criterion
Diagnosis and treatment of overactive bladder (non-neurogenic) in adults: AUA/SUFU guideline. TARGET POPULATION Eligibility Decidable (Y or N) Inclusion Criterion non-neurogenic OAB Exclusion Criterion
Table 1. International Consultation on Incontinence recommendations for frail older adults
 Table 1. International Consultation on Incontinence recommendations for frail older adults Clinicians need to assess and manage co-existing co morbid conditions which are known to have an impact on continence
Table 1. International Consultation on Incontinence recommendations for frail older adults Clinicians need to assess and manage co-existing co morbid conditions which are known to have an impact on continence
Evaluation and Treatment of Incontinence
 Evaluation and Treatment of Incontinence Classification of Incontinence Failure to empty: Overflow incontinence Failure to store Stress Incontinence Urge Incontinence Physiology of voiding CNS Brain sends
Evaluation and Treatment of Incontinence Classification of Incontinence Failure to empty: Overflow incontinence Failure to store Stress Incontinence Urge Incontinence Physiology of voiding CNS Brain sends
Diagnosis and Treatment of Urinary Incontinence. Urinary Incontinence
 Diagnosis and Treatment of Urinary Incontinence Leslee L. Subak, MD Professor Obstetrics, Gynecology & RS Epidemiology, Urology University of California, San Francisco Urinary Incontinence Common - 25%
Diagnosis and Treatment of Urinary Incontinence Leslee L. Subak, MD Professor Obstetrics, Gynecology & RS Epidemiology, Urology University of California, San Francisco Urinary Incontinence Common - 25%
Urinary Continence & Management Post Stroke
 Urinary Continence & Management Post Stroke Incontinence and Stroke occurs in greater than 50% of acute stroke patients despite the personal, economic and psychosocial impact treatment evidence specific
Urinary Continence & Management Post Stroke Incontinence and Stroke occurs in greater than 50% of acute stroke patients despite the personal, economic and psychosocial impact treatment evidence specific
Microbiology. Hani Masaadeh. Hadeel Al-Momani
 Microbiology UTI 1 Hani Masaadeh Hadeel Al-Momani 1 Page #1 Date :27/4/2016 Lecture#1 Micro Lecture#21 UGS Subject : UTI *Urinary tract is normally sterile due to the fact that bacteria moving upwards
Microbiology UTI 1 Hani Masaadeh Hadeel Al-Momani 1 Page #1 Date :27/4/2016 Lecture#1 Micro Lecture#21 UGS Subject : UTI *Urinary tract is normally sterile due to the fact that bacteria moving upwards
Ben Herbert Alex Wojtowicz
 Ben Herbert Alex Wojtowicz 54 year old female presenting with: Dragging sensation Urinary incontinence Some faecal incontinence HPC Since May 14 had noticed a mass protruding from the vagina when going
Ben Herbert Alex Wojtowicz 54 year old female presenting with: Dragging sensation Urinary incontinence Some faecal incontinence HPC Since May 14 had noticed a mass protruding from the vagina when going
4) Urinary Incontinence - Dr. Abeer
 Urinary Incontinence - Dr. Abeer") 4) Urinary Incontinence - Dr. Abeer INTRODUCTION Involuntary loss of urine Social and hygienic problem It affects individuals physical, psychological and social which is associated with a significant reduction
4) Urinary Incontinence - Dr. Abeer INTRODUCTION Involuntary loss of urine Social and hygienic problem It affects individuals physical, psychological and social which is associated with a significant reduction
Incontinence. When I was given this topic in urology to discuss with you today I
 Incontinence When I was given this topic in urology to discuss with you today I was slightly disappointed. I personally see mostly men for problems such as stones, benign prostatic hyperplasia, prostate
Incontinence When I was given this topic in urology to discuss with you today I was slightly disappointed. I personally see mostly men for problems such as stones, benign prostatic hyperplasia, prostate
Pediatric urinary tract infection. Dr. Nariman Fahmi Pediatrics/2013
 Pediatric urinary tract infection Dr. Nariman Fahmi Pediatrics/2013 objectives EPIDEMIOLOGY CAUSATIVE PATHOGENS PATHOGENESIS CATEGORIES OF URINARY TRACT INFECTIONS AND CLINICAL MANIFESTATIONS IN pediatrics
Pediatric urinary tract infection Dr. Nariman Fahmi Pediatrics/2013 objectives EPIDEMIOLOGY CAUSATIVE PATHOGENS PATHOGENESIS CATEGORIES OF URINARY TRACT INFECTIONS AND CLINICAL MANIFESTATIONS IN pediatrics
PREVENTING URINARY INCONTINENCE through PELVIC FLOOR REHABILITATION in DISABLED ELDERLY
 PREVENTING URINARY INCONTINENCE through PELVIC FLOOR REHABILITATION in DISABLED ELDERLY Paolo DI BENEDETTO Lecturer, Tor Vergata University, Rome, Italy Former Director of Rehabilitation Department Institute
PREVENTING URINARY INCONTINENCE through PELVIC FLOOR REHABILITATION in DISABLED ELDERLY Paolo DI BENEDETTO Lecturer, Tor Vergata University, Rome, Italy Former Director of Rehabilitation Department Institute
SUMMARY OF THE GUIDELINE
 NEW PROPOSED GUIDELINE URINARY INCONTINENCE The CUA Guidelines Committee has been busy developing new guidelines and updating existing ones. A subcommittee chaired by Dr. Jacques Corcos has produced this
NEW PROPOSED GUIDELINE URINARY INCONTINENCE The CUA Guidelines Committee has been busy developing new guidelines and updating existing ones. A subcommittee chaired by Dr. Jacques Corcos has produced this
Bladder Dysfunction in Multiple Sclerosis. by Nancy J. Holland, EdD, RN and Nancy C. Reitman, MA, RN
 Clinical Bulletin Information for Health Professionals Bladder Dysfunction in Multiple Sclerosis by Nancy J. Holland, EdD, RN and Nancy C. Reitman, MA, RN Effective bladder management strategies make it
Clinical Bulletin Information for Health Professionals Bladder Dysfunction in Multiple Sclerosis by Nancy J. Holland, EdD, RN and Nancy C. Reitman, MA, RN Effective bladder management strategies make it
Appendix F: Continence Care and Bowel Management Program Training Presentation. Audience: For Front-line Staff Release Date: December 22, 2010
 Appendix F: Continence Care and Bowel Management Program Training Presentation Audience: For Front-line Staff Release Date: December 22, 2010 Objectives Address individual needs and preferences with respect
Appendix F: Continence Care and Bowel Management Program Training Presentation Audience: For Front-line Staff Release Date: December 22, 2010 Objectives Address individual needs and preferences with respect
Kathleen C. Kobashi, MD, FACS Head, Section of Urology and Renal Transplantation Virginia Mason Medical Center, Seattle, WA
 Kathleen C. Kobashi, MD, FACS Head, Section of Urology and Renal Transplantation Virginia Mason Medical Center, Seattle, WA Disclosures Advisory Board and/or Speaker Allergan Medtronic Astellas AUA Guidelines
Kathleen C. Kobashi, MD, FACS Head, Section of Urology and Renal Transplantation Virginia Mason Medical Center, Seattle, WA Disclosures Advisory Board and/or Speaker Allergan Medtronic Astellas AUA Guidelines
Definitions of IC: U.S. perspective. Edward Stanford MD MS FACOG FACS Western Colorado
 Definitions of IC: U.S. perspective Edward Stanford MD MS FACOG FACS Western Colorado PURPOSE OF A DEFINITION? Identifies with specificity those patients who are most likely to have the disease. Identifies
Definitions of IC: U.S. perspective Edward Stanford MD MS FACOG FACS Western Colorado PURPOSE OF A DEFINITION? Identifies with specificity those patients who are most likely to have the disease. Identifies
Appendix E: Continence Care and Bowel Management Program Training Presentation. Audience: For Registered Staff Release Date: December 22, 2010
 Appendix E: Continence Care and Bowel Management Program Training Presentation Audience: For Registered Staff Release Date: December 22, 2010 Objectives Address individual needs and preferences with respect
Appendix E: Continence Care and Bowel Management Program Training Presentation Audience: For Registered Staff Release Date: December 22, 2010 Objectives Address individual needs and preferences with respect
Treatment Regimens for Bacterial Urinary Tract Infections. Characteristic Pathogen. E. coli, S.saprophyticus P.mirabilis, K.
 HEALTHSPAN URINARY TRACT INFECTIONS (ADULT FEMALE) Methodology: Evidence-Based Issue Date: 1-98 Champion: Internal Medicine Most Recent Review: 4-10, 4-12, 4-14 Key Stakeholders: IM, Urology, Next Review:
HEALTHSPAN URINARY TRACT INFECTIONS (ADULT FEMALE) Methodology: Evidence-Based Issue Date: 1-98 Champion: Internal Medicine Most Recent Review: 4-10, 4-12, 4-14 Key Stakeholders: IM, Urology, Next Review:
Urinary Incontinence. Lora Keeling and Byron Neale
 Urinary Incontinence Lora Keeling and Byron Neale Not life threatening. Introduction But can have a huge impact on quality of life. Two main types of urinary incontinence (UI). Stress UI leakage on effort,
Urinary Incontinence Lora Keeling and Byron Neale Not life threatening. Introduction But can have a huge impact on quality of life. Two main types of urinary incontinence (UI). Stress UI leakage on effort,
Operative Approach to Stress Incontinence. Goals of presentation. Preoperative evaluation: Urodynamic Testing? Michelle Y. Morrill, M.D.
 Operative Approach to Stress Incontinence Goals of presentation Michelle Y. Morrill, M.D. Director of Urogynecology The Permanente Medical Group Kaiser, San Francisco Review preoperative care & evaluation
Operative Approach to Stress Incontinence Goals of presentation Michelle Y. Morrill, M.D. Director of Urogynecology The Permanente Medical Group Kaiser, San Francisco Review preoperative care & evaluation
Neurogenic bladder. Neurogenic bladder is a type of dysfunction of the bladder due to neurological disorder.
 Definition: Neurogenic bladder Neurogenic bladder is a type of dysfunction of the bladder due to neurological disorder. Types: Nervous system diseases: Congenital: like myelodysplasia like meningocele.
Definition: Neurogenic bladder Neurogenic bladder is a type of dysfunction of the bladder due to neurological disorder. Types: Nervous system diseases: Congenital: like myelodysplasia like meningocele.
Lower Urinary Tract Infection (UTI) in Males
 in Males") Lower Urinary Tract Infection (UTI) in Males Clinical presentation For patients in care homes see UTI in adults where IV Antibiotics in the community may be appropriate (under development) History and
Lower Urinary Tract Infection (UTI) in Males Clinical presentation For patients in care homes see UTI in adults where IV Antibiotics in the community may be appropriate (under development) History and
Diagnostic approach to LUTS in men. Prof Dato Dr. Zulkifli Md Zainuddin Consultant Urologist / Head Of Urology Unit UKM Medical Center
 Diagnostic approach to LUTS in men Prof Dato Dr. Zulkifli Md Zainuddin Consultant Urologist / Head Of Urology Unit UKM Medical Center Classification of LUTS Storage symptoms Voiding symptoms Post micturition
Diagnostic approach to LUTS in men Prof Dato Dr. Zulkifli Md Zainuddin Consultant Urologist / Head Of Urology Unit UKM Medical Center Classification of LUTS Storage symptoms Voiding symptoms Post micturition
A PATIENT GUIDE TO Understanding Stress Urinary Incontinence
 A PATIENT GUIDE TO Understanding Stress Urinary Incontinence Q: What is SUI? A: Stress urinary incontinence is defined as the involuntary leakage of urine. The problem afflicts approximately 18 million
A PATIENT GUIDE TO Understanding Stress Urinary Incontinence Q: What is SUI? A: Stress urinary incontinence is defined as the involuntary leakage of urine. The problem afflicts approximately 18 million
q7:480499_P0 6/5/09 10:23 AM Page 1 WHAT YOU SHOULD KNOW ABOUT YOUR DIAGNOSIS OF STRESS URINARY INCONTINENCE
 493495.q7:480499_P0 6/5/09 10:23 AM Page 1 WHAT YOU SHOULD KNOW ABOUT YOUR DIAGNOSIS OF STRESS URINARY INCONTINENCE 493495.q7:480499_P0 6/5/09 10:23 AM Page 2 What is Stress Urinary Incontinence? Urinary
493495.q7:480499_P0 6/5/09 10:23 AM Page 1 WHAT YOU SHOULD KNOW ABOUT YOUR DIAGNOSIS OF STRESS URINARY INCONTINENCE 493495.q7:480499_P0 6/5/09 10:23 AM Page 2 What is Stress Urinary Incontinence? Urinary
Voiding Diary. Begin recording upon rising in the morning and continue for a full 24 hours.
 Urodvnamics Your physician has scheduled you for a test called URODYNAMICS. This test is a series of different measurements of bladder function and can be used to determine the cause of a variety of bladder
Urodvnamics Your physician has scheduled you for a test called URODYNAMICS. This test is a series of different measurements of bladder function and can be used to determine the cause of a variety of bladder
UP DATE MANAGEMENT OF URINARY INCONTINENCE IN ADULT
 UP DATE MANAGEMENT OF URINARY INCONTINENCE IN ADULT Yunizaf, MD Division of Urogynecology Department of Obstetrics and Gynecology School of Medicine, University of Indonesia/ Dr. Cipto Mangunkusumo Hospital
UP DATE MANAGEMENT OF URINARY INCONTINENCE IN ADULT Yunizaf, MD Division of Urogynecology Department of Obstetrics and Gynecology School of Medicine, University of Indonesia/ Dr. Cipto Mangunkusumo Hospital
Female Pelvic Medicine & Reconstructive Surgery
 Female Pelvic Medicine & Reconstructive Surgery APPLICATION FOR NEW FELLOWSHIP Name of Institution: McGill University Location: Royal Victoria Hospital (Glen Site), St Mary s Hospital Centre Type of Fellowship:
Female Pelvic Medicine & Reconstructive Surgery APPLICATION FOR NEW FELLOWSHIP Name of Institution: McGill University Location: Royal Victoria Hospital (Glen Site), St Mary s Hospital Centre Type of Fellowship:
MODULE 5: HEMATURIA LEARNING OBJECTIVES DEFINITION. KEY WORDS: Hematuria, Cystoscopy, Urine Cytology, UTI, bladder cancer
 MODULE 5: HEMATURIA KEY WORDS: Hematuria, Cystoscopy, Urine Cytology, UTI, bladder cancer LEARNING OBJECTIVES At the end of this clerkship, the learner will be able to: 1. Define microscopic hematuria.
MODULE 5: HEMATURIA KEY WORDS: Hematuria, Cystoscopy, Urine Cytology, UTI, bladder cancer LEARNING OBJECTIVES At the end of this clerkship, the learner will be able to: 1. Define microscopic hematuria.
Diane K. Newman DNP, ANP-BC, PCB-PMD, FAAN
 Diane K. Newman DNP, ANP-BC, PCB-PMD, FAAN Diane K. Newman, DNP is a Biofeedback Certified Continence Specialist. With over 35-years experience, she is an expert in the assessment and management of pelvic-floor
Diane K. Newman DNP, ANP-BC, PCB-PMD, FAAN Diane K. Newman, DNP is a Biofeedback Certified Continence Specialist. With over 35-years experience, she is an expert in the assessment and management of pelvic-floor
When should UTIs be treated in the Elderly? Shelby L. Wentworth, MS4 University of Florida College of Medicine 29 AUG 2018
 When should UTIs be treated in the Elderly? Shelby L. Wentworth, MS4 University of Florida College of Medicine 29 AUG 2018 UTIs in Patients >/ 65 yo - Most common infectious illness [1]. - Urinary tract
When should UTIs be treated in the Elderly? Shelby L. Wentworth, MS4 University of Florida College of Medicine 29 AUG 2018 UTIs in Patients >/ 65 yo - Most common infectious illness [1]. - Urinary tract
6/4/2018. Conflicts Disclosure. Objectives. Introduction. Classifications of UTI. Host Defenses. Management of Recurrent Urinary Tract Infections
 Conflicts Disclosure Presenter has no conflicts of interest to disclose Management of Recurrent Urinary Tract Infections COLIN M. GOUDELOCKE, M.D. JUNE 14, 2018 Objectives Attendees will review the identification
Conflicts Disclosure Presenter has no conflicts of interest to disclose Management of Recurrent Urinary Tract Infections COLIN M. GOUDELOCKE, M.D. JUNE 14, 2018 Objectives Attendees will review the identification
RECURRENT URINARY TRACT INFECTIONS: WHAT AN INTERNIST
 RECURRENT URINARY TRACT INFECTIONS: WHAT AN INTERNIST MUST KNOW PROF. MD. ENAMUL KARIM Professor of Medicine Green Life Medical College INTRODUCTION Urinary tract infection (UTI) is one of the commonest
RECURRENT URINARY TRACT INFECTIONS: WHAT AN INTERNIST MUST KNOW PROF. MD. ENAMUL KARIM Professor of Medicine Green Life Medical College INTRODUCTION Urinary tract infection (UTI) is one of the commonest
Disease Management. Incontinence Care. Chan Sau Kuen Continence Nurse Consultant United Christian Hospital 14/11/09
 Disease Management in Incontinence Care Chan Sau Kuen Continence Nurse Consultant United Christian Hospital 14/11/09 What is incontinence? Definition of Incontinence - Is the compliant of any involuntary
Disease Management in Incontinence Care Chan Sau Kuen Continence Nurse Consultant United Christian Hospital 14/11/09 What is incontinence? Definition of Incontinence - Is the compliant of any involuntary
URINARY INCONTINENCE
 Center for Continence Care and Pelvic Medicine What is urinary incontinence? URINARY INCONTINENCE Urinary incontinence is the uncontrollable loss of urine. The amount of urine leaked can vary from only
Center for Continence Care and Pelvic Medicine What is urinary incontinence? URINARY INCONTINENCE Urinary incontinence is the uncontrollable loss of urine. The amount of urine leaked can vary from only
Practical urodynamics What PA s need to know. Gary E. Lemack, MD Professor of Urology and Neurology
 Practical urodynamics What PA s need to know Gary E. Lemack, MD Professor of Urology and Neurology Urodynamics essential elements Urethral catheter Fill rate Catheter size Intravesical pressure measurements
Practical urodynamics What PA s need to know Gary E. Lemack, MD Professor of Urology and Neurology Urodynamics essential elements Urethral catheter Fill rate Catheter size Intravesical pressure measurements
INCONTINENCE What can Wee do about it?
 Prevalence INCONTINENCE What can Wee do about it? High risk groups Myths Aetiology Assessment-History Assessment-Drugs Assessment- Examination & Tests INCONTINENCE What can wee do about it? Treatment-First
Prevalence INCONTINENCE What can Wee do about it? High risk groups Myths Aetiology Assessment-History Assessment-Drugs Assessment- Examination & Tests INCONTINENCE What can wee do about it? Treatment-First
INCONTINENCE. Continence and Pelvic Floor Rehabilitation TYPES OF INCONTINENCE STRESS INCONTINENCE STRESS INCONTINENCE STRESS INCONTINENCE 11/08/2015
 INCONTINENCE Continence and Pelvic Floor Rehabilitation Dr Irmina Nahon PhD Pelvic Floor Physiotherapist www.nahonpfed.com.au Defined as the accidental and inappropriate passage of urine or faeces (ICI
INCONTINENCE Continence and Pelvic Floor Rehabilitation Dr Irmina Nahon PhD Pelvic Floor Physiotherapist www.nahonpfed.com.au Defined as the accidental and inappropriate passage of urine or faeces (ICI
Dysfunctional voiding
 Dysfunctional voiding The importance of assessment, diagnosis and treatment of dysfunctional voiding and its role in recurrent UTI Dr Dean Wallace Consultant Paediatric Nephrologist RMCH Objectives Development
Dysfunctional voiding The importance of assessment, diagnosis and treatment of dysfunctional voiding and its role in recurrent UTI Dr Dean Wallace Consultant Paediatric Nephrologist RMCH Objectives Development