REVIEW OF CAUSES, EVALUATION, AND TREATMENTS URINARY INCONTINENCE 101
|
|
|
- Madlyn Ford
- 5 years ago
- Views:
Transcription
1 REVIEW OF CAUSES, EVALUATION, AND TREATMENTS URINARY INCONTINENCE 101
2 March 5, 2014 Kevin E Miller, MD Department of Obstetrics and Gynecology University of Kansas School of Medicine- Wichita URINARY INCONTINENCE
3 PICK A NUMBER
4
5 Urinary incontinence 103 I
6 Female Urinary Incontinence Definition International Continence Society- defines urinary incontinence as the involuntary loss of urine which is severe enough to be a social or hygienic problem, and which is objectively demonstrable.
7 Urinary Incontinence Types Stress incontinence Urgency incontinence (overactive bladder) Mixed incontinence Overflow incontinence Bypass of anatomic continence mechanism Functional / Transient incontinence (DIAPPERS)
 Impaired detrusor contractility (bladder atony) Impaired sensation (neurologic-autonomic or peripheral neuropathy) Drugs-anticholinergics, Ca++ channel blockers, α, β")
8 Female Urinary Incontinence Overflow Incontinence (OI) Involuntary urine loss associated with an overdistended bladder caused by chronic urinary retention secondary to either: Bladder outlet obstruction (mechanical) Impaired detrusor contractility (bladder atony) Impaired sensation (neurologic-autonomic or peripheral neuropathy) Drugs-anticholinergics, Ca++ channel blockers, α, β agonists, radiation fibrosis
 (less common and characterized by continuous")
9 Female Urinary Incontinence Bypass of anatomic continence mechanism Fistula Vesicovaginal Urethrovaginal Vesicouterine Diverticulum- urethral Ectopic ureters Urethra Vagina Cervix/uterus Epispadias (incomplete midline fusion of genitals) (less common and characterized by continuous leakage )
10 Female Urinary Incontinence Transient/Reversible Causes Delirium/Dementia (prompted voiding) Infection (topical estrogen) Atrophy (topical estrogen) Pharmacology (psychotropics) Psychological (OCD, severe depression) Endocrine ( glucose control, polydipsia) Restricted mobility (bedside commode) Stool impaction (colon laxatives, enemas)
11 Stress Urinary Incontinence (SUI) Involuntary loss of urine with increases in intra-abdominal pressure (cough, sneeze, lifting, running) Dx made when urine loss from urethra seen with valsalva Two causes of SUI Hypermobility of urethrovesicle junction Intrinsic Sphincteric Deficiency (ISD)= impaired urethral function-intrinsically low pressure urethra
12 ISD Intrinsic Sphincteric Deficiency Inability of urethra to occlude Causes: trauma, aging, atrophy, neuromuscular changes May occur without increases in intraabdominal pressures MUCP < 20 cm H2O; VLPP <50 cm H2O
13
14 Urgency Urinary Incontinence (UUI) Overactive Bladder Function Disorder of urine storage phase characterized by involuntary detrusor contractions (detrusor overactivity, unstable bladder) Characterized by urgency / frequency, small volume voids Bladder contracts spontaneously or with provocation during filling Neurologic disorders commonly associated with Neurogenic DO, detrusor sphincter dyssynergiastroke, dementia, MS, brain tumor, Parkinson disease (neurogenic bladder)
15 OAB Terminology Urgency Frequency Nocturia Urgency Urinary Incontinence OAB Syndrome
16 OAB Detrusor Overactivity Neurogenic Detrusor Overactivity Associated with known neurologic disease Detrusor hyperreflexia- old terminology Idiopathic Detrusor Overactivity Most common type - 90% No specific cause found
17 Idiopathic Detrusor Overactivity No specific cause (90% of OAB / DO) Non neurologic Behavioral ( high volume intake, irritants, constipation) Obstruction of bladder outlet (severe POP) Aging
18 Mixed Incontinence (MUI) Stress and Urge together Larger volumes of urine loss and more episodes /week Incontinence continuum 100% SUI SUI/UUI % UUI
19 REVIEW- The 3 most common and 3 less common types of incontinence are?
20 Urinary Incontinence Major types in the neurologically intact female Stress incontinence (SUI) Urgency incontinence (UUI) Mixed incontinence (MUI) Overflow incontinence (OI) Bypass of anatomic continence mechanism Functional /Transient incontinence (DIAPPERS)
21 EVALUATION
22 INCONTINENCE EVALUATION MINIMUM 1. H+P 2. URINALYSIS (UA) 3. POST VOID RESIDUAL VOLUME (PVRV)
23 AUA /SUFU GUIDELINES If considering invasive surgical therapy Assess Post void residual volume (PVRV) Expert opinion May perform multi-channel UDS in patients with stress incontinence (Grade C)- to confirm or refute dx, not to predict outcome Should assess urethral function If prolapse- perform stress testing with prolapse reduction

24 Strain angle/q tip test for urethral hypermobility > 30
25 Urinary Incontinence- Evaluation UA Negative predictive value 97% ( neg dipstick reliably rules out infection) Culture if positive or suspicious
26 Urinary Incontinence- Evaluation Post-void residual volume Normal <50 ml Abnormal >200 ml Measured by straight cath or bladder scan U/S immediately after void
27 Urinary Incontinence Evaluation- Additional Tests Bladder diary Simple cystometrogram Multi-channel urodynamic studies
28 Voiding Diary (Bladder diary) GIVES INFORMATION CONCERNING PATIENT S VOIDING VOLUMES, HABITS, FLUID CONSUMPTION, FUNCTIONAL CAPACITY, LEAKAGE EPISODES, NOCTURIA, COGNITIVE STATUS.
29 Urinary Incontinence- Evaluation Voiding diary voided volumes (250 ml/ void) intake volume (1,500 ml/day) frequency (6 X / day) nocturia (1-3X) # incontinence episodes / day
30 Urinary Incontinence-Evaluation Urinary Diary TimeIncontinence 0710 arise urgent leaked urge urge leaked bed 0200 urge leaked voids/ 24 hr Voided volume (ml) ,470 ml / 24 hr
 Voiding")
31 Which patients should have complex urodynamic studies? Mixed incontinence Severe POP beyond hymen Elevated PVR volume Urge incontinence-refractory to conservation Rx Failed previous surgery for incontinence Suspicion of ISD (fixed urethra, +EBST) Voiding dysfunction Continuous incontinence/severe incontinence Neurologic disorders Decreased bladder capacity Bladder pain syndrome with urge frequency refractory to Rx History of pelvic radiation Nocturnal enuresis refractory to therapy
32
33 REVIEW Q. A 28 yo woman complains of having to void every 1-2 hours during the day (voiding diary confirms 75ml average voided volume) with leakage from sudden urge and with running and exercise. She has a positive supine stress test with 300ml in the bladder and a PVRV of 15 ml. Her diagnosis is: A. urgency incontinence B. stress incontinence C. overflow incontinence D. mixed incontinence E. athletes incontinence
34 REVIEW Q. A surgical procedure is being contemplated for a 55yo woman with multiple sclerosis who had previous bladder lift. Which of the following is the least important part of the evaluation. A. History- ascertain what her previous operation was B. Urinalysis or urine culture C. Post void residual volume ( rule out urinary retention) D. Physical exam- cough stress test and evaluate urethra E. Multichannel urodynamic evaluation F. Tampon test with methylene blue dye instillation into bladder (rule out VVF)
35 Non Surgical INCONTINENCE THERAPY
36 Non surgical therapy: Primary options STRESS INCONTINENCE PFM Exercises Vaginal devices Bladder training Weight loss URGENCY INCONTINENCE Anti-muscarinic therapy Behavioral therapy Timed voiding Urge suppression Physical therapy
37 Pessary for SUI Requires willing, motivated patient Is helpful therapy in 25% Requires ongoing maintenance


38 When Pessaries don t work out Possible alternative uses Stylish too!
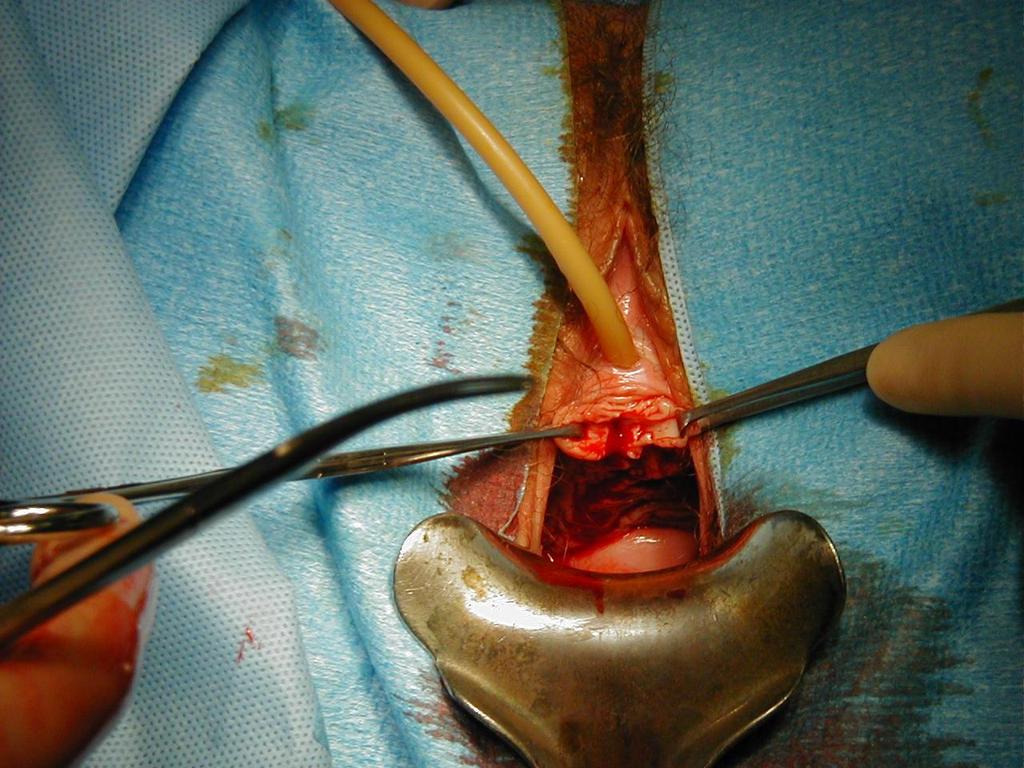
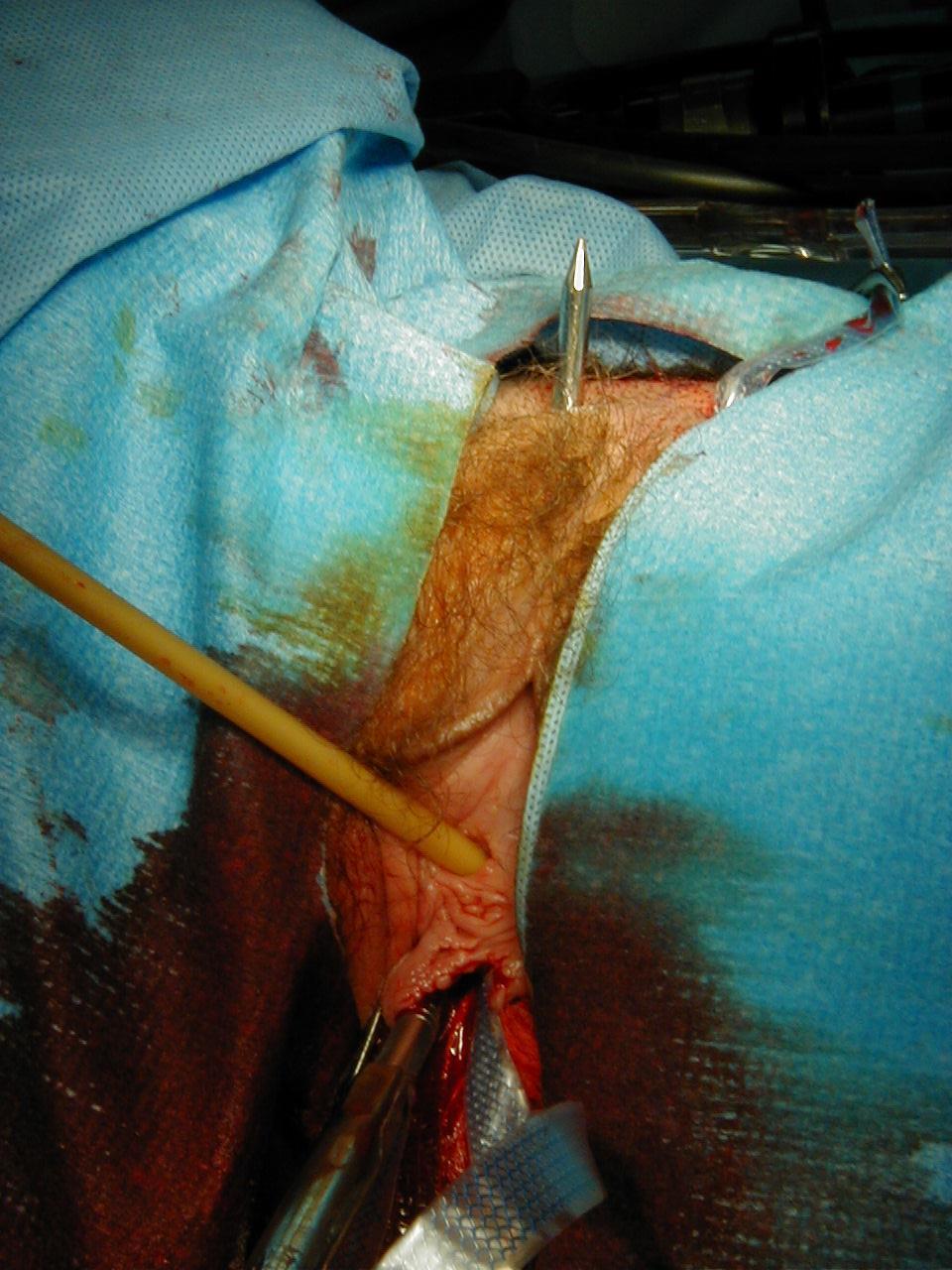
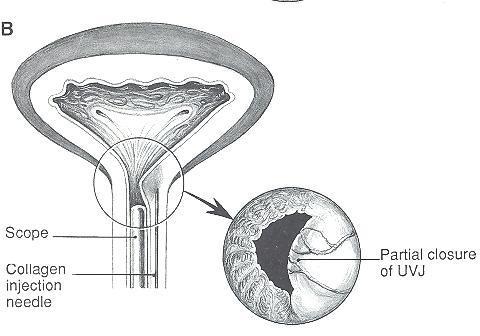
39 3 Surgical therapies for stress urinary incontinence 1. Slings ( synthetic MUS, auto, allo/xeno PVS) 2. retropubic urethropexy 3. urethral bulking injections
 MMK-attach to")

40 Retro-pubic Urethropexy / Colposuspension Marshall-Marchetti-Krantz 1949 Burch 1961 Permanent suture 2-3 per side Double purchase into full thickness of muscularis of anterior vaginal wall (pubocervical fascia) MMK-attach to cartilaginous periosteum of median raphe Burch- attach to Cooper s ligament Tanagho modification 1976 Routine obliteration of cul de sac recommended to reduce enterocele formation 7.6% (Burch 1967)- unconfirmed if this reduces recurrent prolapse
41 TVT(tension free vaginal tape) & TOT(transobturator TVT) What is the difference? Trocar passage through retro-pubic space Theoretically less risk of bladder, nerve, vascular, and intra-abdominal viscera injury with trocar passage
42
43
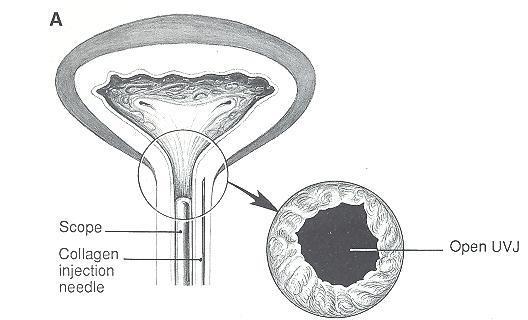
44 Periurethral Bulking
45 Therapies for stress incontinence SUMMARY MUS is most effective treatment (80-85%) Pessary helpful in 25%- ½ will go to surg Pelvic floor muscle training is effective- if sustained Medications are NOT effective Urethral bulking injections- for severe refractory ISD
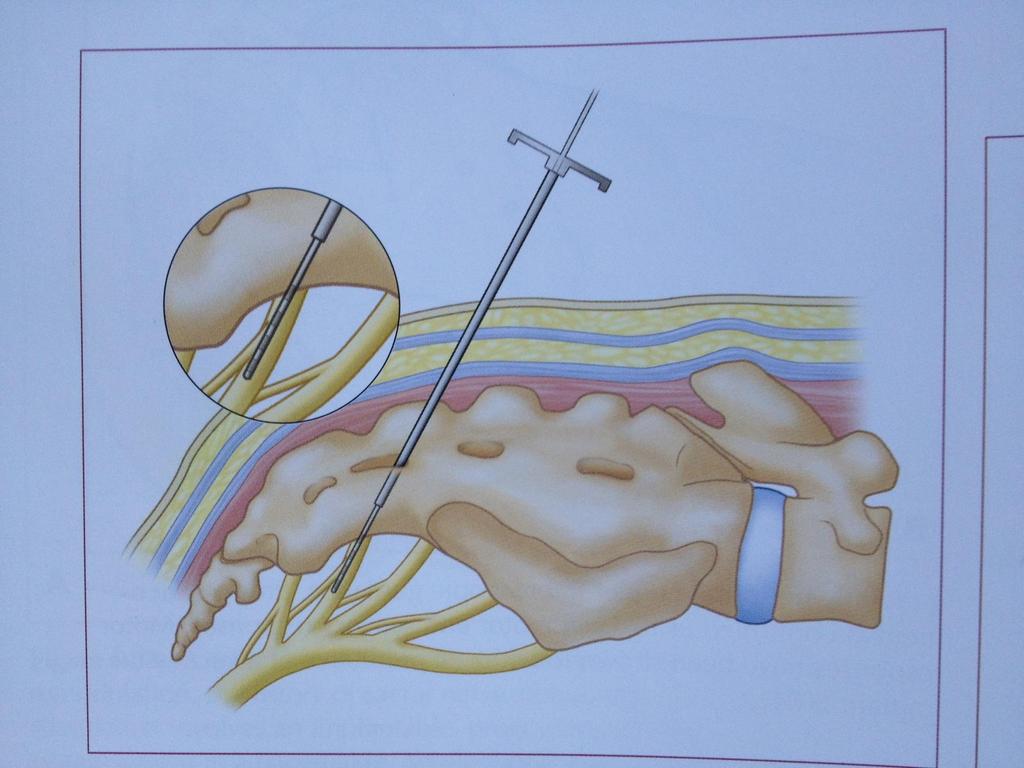
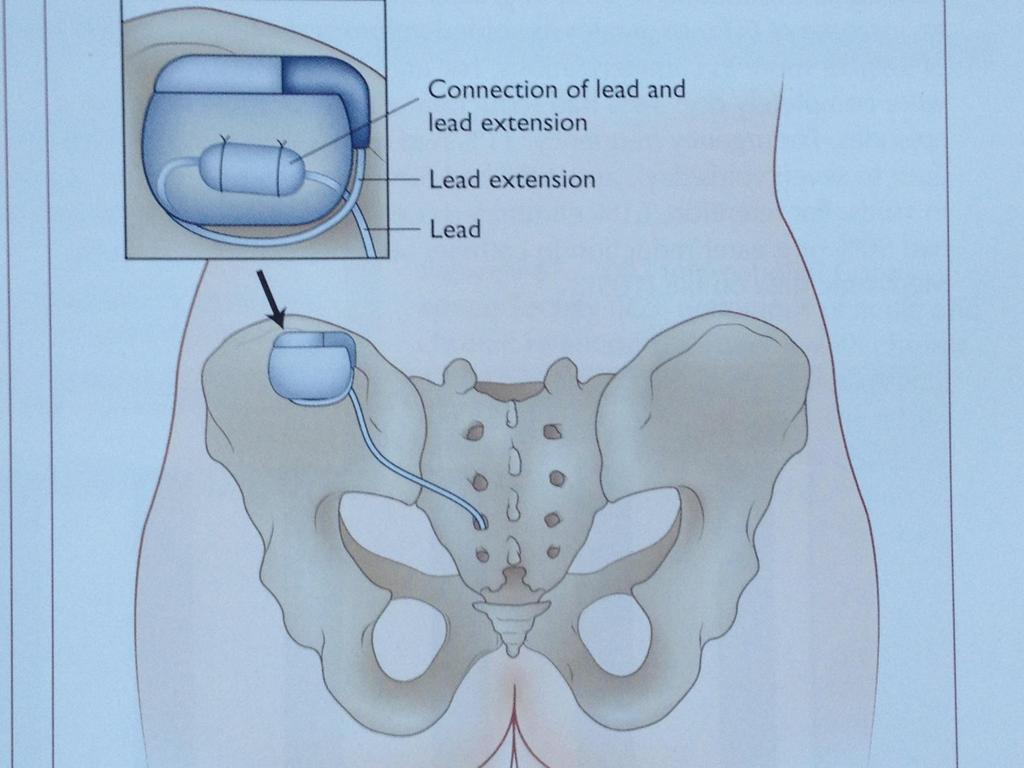
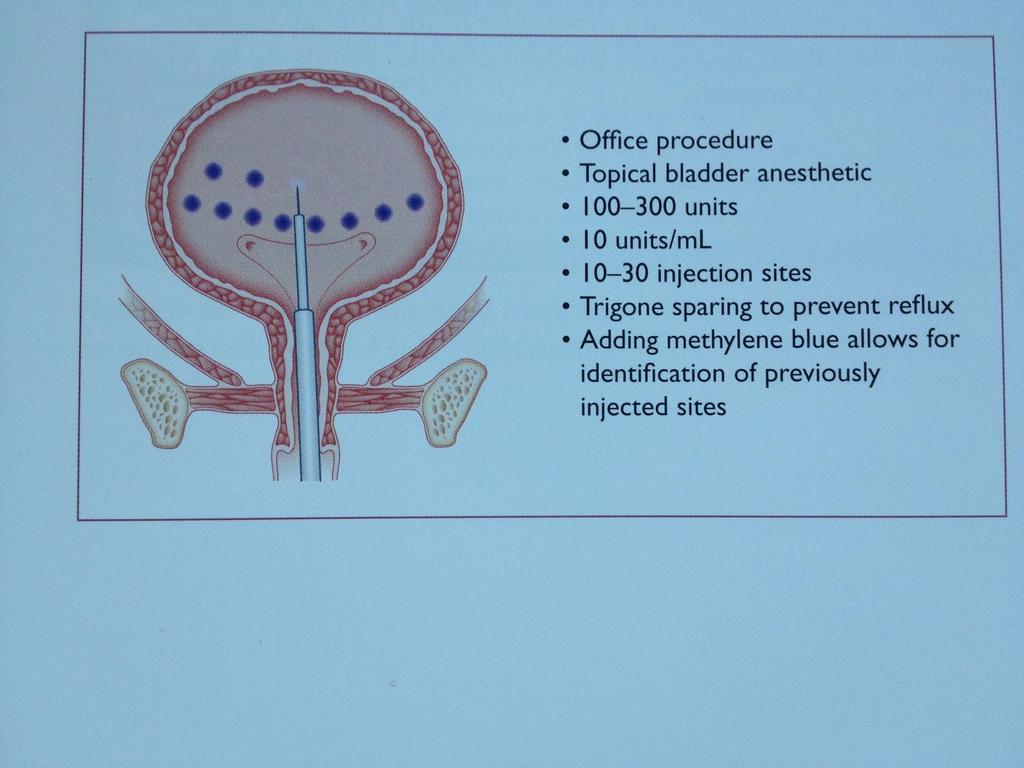
46 Overactive Bladder Therapy First 1. Lifestyle modification / Behavioral 2. Pelvic floor muscle exercises/biofeedback/ FES 3. Medications More invasive 1. Sacral nerve stimulation (InterStim) 2. Intravesical injections (Botox) 3. Radical surgery (bladder augmentation)-rare
47 Lifestyle / Behavioral Modifications Urge suppression techniques Timed voiding Fluid management Diuretic management Weight loss
48 Non surgical therapy for incontinence Pelvic floor muscle training (PFMT) - For Urgency Urinary Incontinence (UUI) PFM contractions inhibit detrusor contractions Improves UUI in combination with behavioral therapies
49 1/5 patients will fail conservative therapy for OAB Sacral nerve stimulation = sacral neuromodulation = InterStim Is an electrode placed through the 3 rd sacral foramen (with or without fluoroscopy) With a test phase of 3-14 days before longterm implant Success defined as > 50% improvement in urgency / urge incontinence episodes or <8 voids per day.
50
51
52 Risks: urinary tract infection 20-40% urinary retention 5-30% (clean self cath) Repeat injections (9 mo) INTRADETRUSOR ONABOTULINUMTOXIN A (BOTOX)
53
54 REVIEW TREATMENTS FOR INCONTINENCE A 85 yo woman who complains of always leaking urine with minimal exertion after a synthetic mini sling, has an immobile urethra had UDS with stable detrusor to fill and VLPPs of < 60 cm H20 and UPPs <20 cm H2o. Her diagnosis and best treatment is: A. Mixed incontinence: retropubic MUS B. Neurogenic bladder: Sacral neuromodulation (InterStim) C. Stress incontinence : retropubic urethropexy D. Urgency incontinence: intravesicle Botox injection E. Intrinsic Sphincteric Deficiency(ISD): Urethral bulking F. Vesico-vaginal fistula secondary to sling: pessary
55 REVIEW- Treatments Effective treatments for Stress Urinary Incontinence (SUI) include. A. Vaginal pessary B. Retropubic urethropexy (MMK, Burch) C. Synthetic mid-urethral sling D. Anterior colporrhaphy (cystocele repair) E. A,B,and C F. All of the above
56 THE END

57 The end
58
59
60 Non surgical therapy for incontinence Pelvic floor muscle training (PFMT) For STRESS INCONTINENCE Increased continence rates and improved UI PFMT combined with bladder training Increased continence rates and improved MUI PFMT with biofeedback improved UI
61 Non surgical therapy PFMT +/- Biofeedback No differences in clinical outcomes No consistent differences in continence No difference in QOL
Objectives. Prevalence of Urinary Incontinence URINARY INCONTINENCE: EVALUATION AND CURRENT TREATMENT OPTIONS
 URINARY INCONTINENCE: EVALUATION AND CURRENT TREATMENT OPTIONS Lisa S Pair, MSN, CRNP Division of Urogynecology and Pelvic Reconstructive Surgery Department of Obstetrics and Gynecology University of Alabama
URINARY INCONTINENCE: EVALUATION AND CURRENT TREATMENT OPTIONS Lisa S Pair, MSN, CRNP Division of Urogynecology and Pelvic Reconstructive Surgery Department of Obstetrics and Gynecology University of Alabama
Management of Female Stress Incontinence
 Management of Female Stress Incontinence Dr. Arvind Goyal Associate Professor (Urology& Renal Transplant) Dayanand Medical College & Hospital, Ludhiana, Punjab, India Stress Incontinence Involuntary loss
Management of Female Stress Incontinence Dr. Arvind Goyal Associate Professor (Urology& Renal Transplant) Dayanand Medical College & Hospital, Ludhiana, Punjab, India Stress Incontinence Involuntary loss
URINARY INCONTINENCE. Urology Division, Surgery Department Medical Faculty, University of Sumatera Utara
 URINARY INCONTINENCE Urology Division, Surgery Department Medical Faculty, University of Sumatera Utara Definition The involuntary loss of urine May denote a symptom, a sign or a condition Symptom the
URINARY INCONTINENCE Urology Division, Surgery Department Medical Faculty, University of Sumatera Utara Definition The involuntary loss of urine May denote a symptom, a sign or a condition Symptom the
Incontinence; Lets talk about it. Karanvir Virk M.D. Minimally Invasive and Pelvic Reconstructive Surgery
 Incontinence; Lets talk about it Karanvir Virk M.D. Minimally Invasive and Pelvic Reconstructive Surgery Select the most appropriate subtitle for this talk A: Bladders gone wild! B: There s no such thing
Incontinence; Lets talk about it Karanvir Virk M.D. Minimally Invasive and Pelvic Reconstructive Surgery Select the most appropriate subtitle for this talk A: Bladders gone wild! B: There s no such thing
Tools for Evaluation. Urodynamics Case Studies. Case 1. Evaluation. Case 1. Bladder Diary SUI 19/01/2018
 Urodynamics Case Studies Christopher K. Payne, MD Vista Urology & Pelvic Pain Partners Emeritus Professor of Urology, Stanford University Tools for Evaluation Ears, Eyes, and Brain Bladder diary Stress
Urodynamics Case Studies Christopher K. Payne, MD Vista Urology & Pelvic Pain Partners Emeritus Professor of Urology, Stanford University Tools for Evaluation Ears, Eyes, and Brain Bladder diary Stress
Various Types. Ralph Boling, DO, FACOG
 Various Types Ralph Boling, DO, FACOG The goal of this lecture is to increase assessment and treatment abilities for physicians managing urinary incontinence (UI) patients. 1. Effectively communicate with
Various Types Ralph Boling, DO, FACOG The goal of this lecture is to increase assessment and treatment abilities for physicians managing urinary incontinence (UI) patients. 1. Effectively communicate with
Urogynaecology. Colm McAlinden
 Urogynaecology Colm McAlinden Definitions Urinary incontinence compliant of any involuntary leakage of urine with many different causes Two main types: Stress Urge Definitions Nocturia: More than a single
Urogynaecology Colm McAlinden Definitions Urinary incontinence compliant of any involuntary leakage of urine with many different causes Two main types: Stress Urge Definitions Nocturia: More than a single
Urinary Incontinence. Lora Keeling and Byron Neale
 Urinary Incontinence Lora Keeling and Byron Neale Not life threatening. Introduction But can have a huge impact on quality of life. Two main types of urinary incontinence (UI). Stress UI leakage on effort,
Urinary Incontinence Lora Keeling and Byron Neale Not life threatening. Introduction But can have a huge impact on quality of life. Two main types of urinary incontinence (UI). Stress UI leakage on effort,
Practical urodynamics What PA s need to know. Gary E. Lemack, MD Professor of Urology and Neurology
 Practical urodynamics What PA s need to know Gary E. Lemack, MD Professor of Urology and Neurology Urodynamics essential elements Urethral catheter Fill rate Catheter size Intravesical pressure measurements
Practical urodynamics What PA s need to know Gary E. Lemack, MD Professor of Urology and Neurology Urodynamics essential elements Urethral catheter Fill rate Catheter size Intravesical pressure measurements
Content. Terminology Anatomy Aetiology Presentation Classification Management
 Prolapse Content Terminology Anatomy Aetiology Presentation Classification Management Terminology Prolapse Descent of pelvic organs into the vagina Cystocele ant. vaginal wall involving bladder Uterine
Prolapse Content Terminology Anatomy Aetiology Presentation Classification Management Terminology Prolapse Descent of pelvic organs into the vagina Cystocele ant. vaginal wall involving bladder Uterine
Overactive Bladder: Diagnosis and Approaches to Treatment
 Overactive Bladder: Diagnosis and Approaches to Treatment A Hidden Condition* Many Many patients self-manage by voiding frequently, reducing fluid intake, and wearing pads Nearly Nearly two-thirds thirds
Overactive Bladder: Diagnosis and Approaches to Treatment A Hidden Condition* Many Many patients self-manage by voiding frequently, reducing fluid intake, and wearing pads Nearly Nearly two-thirds thirds
Prolapse and Urogynae Incontinence. Lucy Tiffin and Hannah Wheldon-Holmes
 Prolapse and Urogynae Incontinence Lucy Tiffin and Hannah Wheldon-Holmes 66 year old woman with incontinence PC: 7 year Hx of urgency, frequency, nocturia (incl. incontinence at night), and stress incontinence
Prolapse and Urogynae Incontinence Lucy Tiffin and Hannah Wheldon-Holmes 66 year old woman with incontinence PC: 7 year Hx of urgency, frequency, nocturia (incl. incontinence at night), and stress incontinence
Medical Review Criteria Invasive Treatment for Urinary Incontinence
 Medical Review Criteria Invasive Treatment for Urinary Incontinence Effective Date: December 21, 2016 Subject: Invasive Treatment for Urinary Incontinence Background: Urinary incontinence (the involuntary
Medical Review Criteria Invasive Treatment for Urinary Incontinence Effective Date: December 21, 2016 Subject: Invasive Treatment for Urinary Incontinence Background: Urinary incontinence (the involuntary
Urodynamics in women. Aims of Urodynamics in women. Why do Urodynamics?
 Urodynamics in women Chendrimada Madhu MD, MA, MRCOG Subspecialty Trainee in Urogynaecology Southmead Hospital 2013 Aims of Urodynamics in women n Confirmation of incontinence and its cause n Definition
Urodynamics in women Chendrimada Madhu MD, MA, MRCOG Subspecialty Trainee in Urogynaecology Southmead Hospital 2013 Aims of Urodynamics in women n Confirmation of incontinence and its cause n Definition
John Laughlin 4 th year Cardiff University Medical Student
 John Laughlin 4 th year Cardiff University Medical Student Prolapse/incontinence You need to know: Pelvic floor anatomy in relation to uterovaginal support and continence The classification of uterovaginal
John Laughlin 4 th year Cardiff University Medical Student Prolapse/incontinence You need to know: Pelvic floor anatomy in relation to uterovaginal support and continence The classification of uterovaginal
Lower Urinary Tract Symptoms K Kuruvilla Zachariah Associate Specialist
 Lower Urinary Tract Symptoms K Kuruvilla Zachariah Associate Specialist Lower Urinary Tract Symptoms Storage Symptoms Frequency, urgency, incontinence, Nocturia Voiding Symptoms Hesitancy, poor flow, intermittency,
Lower Urinary Tract Symptoms K Kuruvilla Zachariah Associate Specialist Lower Urinary Tract Symptoms Storage Symptoms Frequency, urgency, incontinence, Nocturia Voiding Symptoms Hesitancy, poor flow, intermittency,
PREVENTING URINARY INCONTINENCE through PELVIC FLOOR REHABILITATION in DISABLED ELDERLY
 PREVENTING URINARY INCONTINENCE through PELVIC FLOOR REHABILITATION in DISABLED ELDERLY Paolo DI BENEDETTO Lecturer, Tor Vergata University, Rome, Italy Former Director of Rehabilitation Department Institute
PREVENTING URINARY INCONTINENCE through PELVIC FLOOR REHABILITATION in DISABLED ELDERLY Paolo DI BENEDETTO Lecturer, Tor Vergata University, Rome, Italy Former Director of Rehabilitation Department Institute
Urinary Incontinence. Vibhash Mishra Consultant Urological Surgeon Royal Free Hospital
 Urinary Incontinence Vibhash Mishra Consultant Urological Surgeon Royal Free Hospital Affects women of all ages Impacts physical, psychological & social wellbeing Impact on families & carers Costs the
Urinary Incontinence Vibhash Mishra Consultant Urological Surgeon Royal Free Hospital Affects women of all ages Impacts physical, psychological & social wellbeing Impact on families & carers Costs the
Operative Approach to Stress Incontinence. Goals of presentation. Preoperative evaluation: Urodynamic Testing? Michelle Y. Morrill, M.D.
 Operative Approach to Stress Incontinence Goals of presentation Michelle Y. Morrill, M.D. Director of Urogynecology The Permanente Medical Group Kaiser, San Francisco Review preoperative care & evaluation
Operative Approach to Stress Incontinence Goals of presentation Michelle Y. Morrill, M.D. Director of Urogynecology The Permanente Medical Group Kaiser, San Francisco Review preoperative care & evaluation
UP DATE MANAGEMENT OF URINARY INCONTINENCE IN ADULT
 UP DATE MANAGEMENT OF URINARY INCONTINENCE IN ADULT Yunizaf, MD Division of Urogynecology Department of Obstetrics and Gynecology School of Medicine, University of Indonesia/ Dr. Cipto Mangunkusumo Hospital
UP DATE MANAGEMENT OF URINARY INCONTINENCE IN ADULT Yunizaf, MD Division of Urogynecology Department of Obstetrics and Gynecology School of Medicine, University of Indonesia/ Dr. Cipto Mangunkusumo Hospital
NATIONAL INSTITUTE FOR CLINICAL EXCELLENCE SCOPE. Urinary incontinence: the management of urinary incontinence in women
 NATIONAL INSTITUTE FOR CLINICAL EXCELLENCE 1 Guideline title SCOPE Urinary incontinence: the management of urinary incontinence in women 1.1 Short title Urinary incontinence 2 Background a) The National
NATIONAL INSTITUTE FOR CLINICAL EXCELLENCE 1 Guideline title SCOPE Urinary incontinence: the management of urinary incontinence in women 1.1 Short title Urinary incontinence 2 Background a) The National
Loss of Bladder Control
 BLADDER HEALTH: Surgery for Urinary Incontinence Loss of Bladder Control Surgery for Urinary Incontinence Don t Let Urinary Incontinence Keep You from Enjoying Life. What is Urinary Incontinence? What
BLADDER HEALTH: Surgery for Urinary Incontinence Loss of Bladder Control Surgery for Urinary Incontinence Don t Let Urinary Incontinence Keep You from Enjoying Life. What is Urinary Incontinence? What
Advanced Care for Female Overactive Bladder & Urinary Incontinence. Department of Urology Kaiser Permanente Santa Rosa
 Advanced Care for Female Overactive Bladder & Urinary Incontinence Department of Urology Kaiser Permanente Santa Rosa Goals Participants will: Review normal urinary tract anatomy and function Understand
Advanced Care for Female Overactive Bladder & Urinary Incontinence Department of Urology Kaiser Permanente Santa Rosa Goals Participants will: Review normal urinary tract anatomy and function Understand
Pathophysiological Rationale for Surgical Treatments of Stress Urinary Incontinence
 Pathophysiological Rationale for Surgical Treatments of Stress Urinary Incontinence Urology Grand Rounds April 6, 2005 Herman Christopher Kwan R4 A familiar case? 62 year old female initial presentation
Pathophysiological Rationale for Surgical Treatments of Stress Urinary Incontinence Urology Grand Rounds April 6, 2005 Herman Christopher Kwan R4 A familiar case? 62 year old female initial presentation
A PATIENT GUIDE TO Understanding Stress Urinary Incontinence
 A PATIENT GUIDE TO Understanding Stress Urinary Incontinence Q: What is SUI? A: Stress urinary incontinence is defined as the involuntary leakage of urine. The problem afflicts approximately 18 million
A PATIENT GUIDE TO Understanding Stress Urinary Incontinence Q: What is SUI? A: Stress urinary incontinence is defined as the involuntary leakage of urine. The problem afflicts approximately 18 million
Urogynecology in EDS. Joan L. Blomquist, MD Greater Baltimore Medical Center August 2018
 Urogynecology in EDS Joan L. Blomquist, MD Greater Baltimore Medical Center August 2018 One in three like me Voiding Issues Frequency/Urgency Urinary Incontinence neurogenic bladder Neurologic supply
Urogynecology in EDS Joan L. Blomquist, MD Greater Baltimore Medical Center August 2018 One in three like me Voiding Issues Frequency/Urgency Urinary Incontinence neurogenic bladder Neurologic supply
4. Know how to examine and name relevant test performed on patients
 Chapter 18 Female Urinary lncontinence Dr Zeelha Abdool Ed ucational Objectives : After completion of this chapter you should be able to: 1. Understand the pathophysiology of incontinence 2. Define and
Chapter 18 Female Urinary lncontinence Dr Zeelha Abdool Ed ucational Objectives : After completion of this chapter you should be able to: 1. Understand the pathophysiology of incontinence 2. Define and
Incontinence: Risks, Causes and Care
 Welcome To Incontinence: Risks, Causes and Care Presented by Kamal Masaki, MD Professor and Chair Department of Geriatric Medicine John A. Burns School of Medicine, UH Manoa September 5, 2018 10:00 11:00
Welcome To Incontinence: Risks, Causes and Care Presented by Kamal Masaki, MD Professor and Chair Department of Geriatric Medicine John A. Burns School of Medicine, UH Manoa September 5, 2018 10:00 11:00
Disclosures. Geriatric Incontinence and Voiding Dysfunction. Agenda. Agenda. UI: a Geriatric Syndrome. Geriatric Syndromes 9/7/2018.
 Disclosures Geriatric Incontinence and Voiding Dysfunction None Shachi Tyagi MD, MS Assistant Professor Division of Geriatric Medicine University of Pittsburgh Medical Center UI: a Geriatric Syndrome Geriatric
Disclosures Geriatric Incontinence and Voiding Dysfunction None Shachi Tyagi MD, MS Assistant Professor Division of Geriatric Medicine University of Pittsburgh Medical Center UI: a Geriatric Syndrome Geriatric
Prolapse and Urogynae. By Sarah Rangan & Daniel Warrell
 Prolapse and Urogynae By Sarah Rangan & Daniel Warrell Anatomy and physiology of the pelvic supports The pelvic floor supports the pelvic viscera and vaginal, urethral and rectal openings Endopelvic fascial
Prolapse and Urogynae By Sarah Rangan & Daniel Warrell Anatomy and physiology of the pelvic supports The pelvic floor supports the pelvic viscera and vaginal, urethral and rectal openings Endopelvic fascial
Appendix F: Continence Care and Bowel Management Program Training Presentation. Audience: For Front-line Staff Release Date: December 22, 2010
 Appendix F: Continence Care and Bowel Management Program Training Presentation Audience: For Front-line Staff Release Date: December 22, 2010 Objectives Address individual needs and preferences with respect
Appendix F: Continence Care and Bowel Management Program Training Presentation Audience: For Front-line Staff Release Date: December 22, 2010 Objectives Address individual needs and preferences with respect
Female Pelvic Medicine & Reconstructive Surgery
 Female Pelvic Medicine & Reconstructive Surgery APPLICATION FOR NEW FELLOWSHIP Name of Institution: McGill University Location: Royal Victoria Hospital (Glen Site), St Mary s Hospital Centre Type of Fellowship:
Female Pelvic Medicine & Reconstructive Surgery APPLICATION FOR NEW FELLOWSHIP Name of Institution: McGill University Location: Royal Victoria Hospital (Glen Site), St Mary s Hospital Centre Type of Fellowship:
Overactive Bladder Syndrome
 Overactive Bladder Syndrome behavioural modifications to pharmacological and surgical treatments Dr Jos Jayarajan Urologist Austin Health, Eastern Health Warringal Private, Northpark Private, Epworth Overactive
Overactive Bladder Syndrome behavioural modifications to pharmacological and surgical treatments Dr Jos Jayarajan Urologist Austin Health, Eastern Health Warringal Private, Northpark Private, Epworth Overactive
Urogynecology ICD-9 to ICD-10 Crosswalks
 1100 Wayne Ave, Suite 825 Silver Spring, MD 20910 301.273.0570 Fax 301.273.0778 info@augs.org www.augs.org Urogynecology ICD-9 to ICD-10 Crosswalks ICD 9 ICD 9 Description ICD 10 Code ICD 10 Description
1100 Wayne Ave, Suite 825 Silver Spring, MD 20910 301.273.0570 Fax 301.273.0778 info@augs.org www.augs.org Urogynecology ICD-9 to ICD-10 Crosswalks ICD 9 ICD 9 Description ICD 10 Code ICD 10 Description
Prediction and prevention of stress urinary incontinence after prolapse surgery van der Ploeg, J.M.
 UvA-DARE (Digital Academic Repository) Prediction and prevention of stress urinary incontinence after prolapse surgery van der Ploeg, J.M. Link to publication Citation for published version (APA): van
UvA-DARE (Digital Academic Repository) Prediction and prevention of stress urinary incontinence after prolapse surgery van der Ploeg, J.M. Link to publication Citation for published version (APA): van
Urodynamic findings in women with insensible incontinence
 bs_bs_banner International Journal of Urology (2013) 20, 429 433 doi: 10.1111/j.1442-2042.2012.03146.x Original Article: Clinical Investigation Urodynamic findings in women with insensible Benjamin M Brucker,
bs_bs_banner International Journal of Urology (2013) 20, 429 433 doi: 10.1111/j.1442-2042.2012.03146.x Original Article: Clinical Investigation Urodynamic findings in women with insensible Benjamin M Brucker,
Prolapse & Stress Incontinence
 Advanced Pelvic Floor Course Prolapse & Stress Incontinence OVERVIEW Day One and morning of Day Two- Pelvic Organ Prolapse The Prolapse component covers the detailed anatomy of POP including the DeLancey
Advanced Pelvic Floor Course Prolapse & Stress Incontinence OVERVIEW Day One and morning of Day Two- Pelvic Organ Prolapse The Prolapse component covers the detailed anatomy of POP including the DeLancey
Urinary Incontinence for the Primary Care Provider
 Urinary Incontinence for the Primary Care Provider Diana J Scott FNP-BC https://youtu.be/gmzaue1ojn4 1 Assessment of Urinary Incontinence Urge Stress Mixed Other overflow, postural, continuous, insensible,
Urinary Incontinence for the Primary Care Provider Diana J Scott FNP-BC https://youtu.be/gmzaue1ojn4 1 Assessment of Urinary Incontinence Urge Stress Mixed Other overflow, postural, continuous, insensible,
Urinary incontinence (UI) affects as many
 affects as many") EXPLORING NEW HORIZONS IN STRESS INCONTINENCE: THE NEUROUROLOGY CONNECTION W. Glenn Hurt, MD* ABSTRACT As many as one-third of women are affected by urinary incontinence, the most common of which being
EXPLORING NEW HORIZONS IN STRESS INCONTINENCE: THE NEUROUROLOGY CONNECTION W. Glenn Hurt, MD* ABSTRACT As many as one-third of women are affected by urinary incontinence, the most common of which being
Video-urodynamics. P J R Shah Institute of Urology and UCH
 Video-urodynamics P J R Shah Institute of Urology and UCH Bladder Function Storage Capacity and Pressure Emptying Pressure/flow/emptying URODYNAMIC INVESTIGATIONS Free urine flow rate Urethral pressure
Video-urodynamics P J R Shah Institute of Urology and UCH Bladder Function Storage Capacity and Pressure Emptying Pressure/flow/emptying URODYNAMIC INVESTIGATIONS Free urine flow rate Urethral pressure
BSUG Annual scientific update 5/6 th Nov 2012
 BSUG Annual scientific update 5/6 th Nov 2012 Zainab Khan SWIG 4/12/2012 New developments in drug therapy B3 Agonists: Mirabegron - FDA approval - Mirabegron (50 &100mg) vs tolterodine 4mg- similar efficacy,
BSUG Annual scientific update 5/6 th Nov 2012 Zainab Khan SWIG 4/12/2012 New developments in drug therapy B3 Agonists: Mirabegron - FDA approval - Mirabegron (50 &100mg) vs tolterodine 4mg- similar efficacy,
4) Urinary Incontinence - Dr. Abeer
 Urinary Incontinence - Dr. Abeer") 4) Urinary Incontinence - Dr. Abeer INTRODUCTION Involuntary loss of urine Social and hygienic problem It affects individuals physical, psychological and social which is associated with a significant reduction
4) Urinary Incontinence - Dr. Abeer INTRODUCTION Involuntary loss of urine Social and hygienic problem It affects individuals physical, psychological and social which is associated with a significant reduction
Management of Urinary Incontinence in Older Women. Dr. Cecilia Cheon Department of Obs. & Gyn. Queen Elizabeth Hospital
 Management of Urinary Incontinence in Older Women Dr. Cecilia Cheon Department of Obs. & Gyn. Queen Elizabeth Hospital Epidemiology Causes Investigation Treatment Conclusion Elderly Women High prevalence
Management of Urinary Incontinence in Older Women Dr. Cecilia Cheon Department of Obs. & Gyn. Queen Elizabeth Hospital Epidemiology Causes Investigation Treatment Conclusion Elderly Women High prevalence
Adult Urodynamics: American Urological Association (AUA)/Society of Urodynamics, Female Pelvic Medicine & Urogenital Reconstruction (SUFU) Guideline
/Society of Urodynamics, Female Pelvic Medicine & Urogenital Reconstruction (SUFU) Guideline") Adult Urodynamics: American Urological Association (AUA)/Society of Urodynamics, Female Pelvic Medicine & Urogenital Reconstruction (SUFU) Guideline TARGET POPULATION Eligibility Decidable (Y or N) Inclusion
Adult Urodynamics: American Urological Association (AUA)/Society of Urodynamics, Female Pelvic Medicine & Urogenital Reconstruction (SUFU) Guideline TARGET POPULATION Eligibility Decidable (Y or N) Inclusion
Diagnosis and Treatment of Urinary Incontinence. Urinary Incontinence
 Diagnosis and Treatment of Urinary Incontinence Leslee L. Subak, MD Professor Obstetrics, Gynecology & RS Epidemiology, Urology University of California, San Francisco Urinary Incontinence Common - 25%
Diagnosis and Treatment of Urinary Incontinence Leslee L. Subak, MD Professor Obstetrics, Gynecology & RS Epidemiology, Urology University of California, San Francisco Urinary Incontinence Common - 25%
LONG TERM FOLLOW UP OF THE TRANSOBTURATOR TAPE PROCEDURE FOR THE TREATMENT OF STRESS URINARY INCONTINENCE IN A TERTIARY HOSPITAL IN SOUTH AFRICA
 LONG TERM FOLLOW UP OF THE TRANSOBTURATOR TAPE PROCEDURE FOR THE TREATMENT OF STRESS URINARY INCONTINENCE IN A TERTIARY HOSPITAL IN SOUTH AFRICA Dr. A. Chrysostomou MD, FCOG (SA), Mmed (WITS) Senior Specialist,
LONG TERM FOLLOW UP OF THE TRANSOBTURATOR TAPE PROCEDURE FOR THE TREATMENT OF STRESS URINARY INCONTINENCE IN A TERTIARY HOSPITAL IN SOUTH AFRICA Dr. A. Chrysostomou MD, FCOG (SA), Mmed (WITS) Senior Specialist,
Loss of Bladder Control
 BLADDER HEALTH Loss of Bladder Control SURGERY TO TREAT URINARY INCONTINENCE AUA FOUNDATION OFFICIAL FOUNDATION OF THE AMERICAN UROLOGICAL ASSOCIATION What Is Urinary Incontinence? Urinary incontinence
BLADDER HEALTH Loss of Bladder Control SURGERY TO TREAT URINARY INCONTINENCE AUA FOUNDATION OFFICIAL FOUNDATION OF THE AMERICAN UROLOGICAL ASSOCIATION What Is Urinary Incontinence? Urinary incontinence
The Management of Female Urinary Incontinence. Part 1: Aetiology and Investigations
 The Management of Female Urinary Incontinence Part 1: Aetiology and Investigations Dr Oseka Onuma Gynaecologist and Pelvic Reconstructive Surgeon 4 Robe Terrace Medindie SA 5081 Urinary incontinence has
The Management of Female Urinary Incontinence Part 1: Aetiology and Investigations Dr Oseka Onuma Gynaecologist and Pelvic Reconstructive Surgeon 4 Robe Terrace Medindie SA 5081 Urinary incontinence has
PRE-OPERATIVE URODYNAMIC
 PRE-OPERATIVE URODYNAMIC STUDIES: IS THERE VALUE IN PREDICTING POST-OPERATIVE STRESS URINARY INCONTINENCE IN WOMEN UNDERGOING PROLAPSE SURGERY? Dr K Janse van Rensburg Dr JA van Rensburg INTRODUCTION POP
PRE-OPERATIVE URODYNAMIC STUDIES: IS THERE VALUE IN PREDICTING POST-OPERATIVE STRESS URINARY INCONTINENCE IN WOMEN UNDERGOING PROLAPSE SURGERY? Dr K Janse van Rensburg Dr JA van Rensburg INTRODUCTION POP
URINARY INCONTINENCE
 Center for Continence Care and Pelvic Medicine What is urinary incontinence? URINARY INCONTINENCE Urinary incontinence is the uncontrollable loss of urine. The amount of urine leaked can vary from only
Center for Continence Care and Pelvic Medicine What is urinary incontinence? URINARY INCONTINENCE Urinary incontinence is the uncontrollable loss of urine. The amount of urine leaked can vary from only
25-Feb-16 MANAGEMENT OF URINARY INCONTINENCE IN WOMEN.
 Female Urinary Incontinence: GP resources MANAGEMENT OF URINARY INCONTINENCE IN WOMEN Dr Marcus Carey 20 February 2016 www.thewomens.org.au Clinical Practice Guidelines GP management of female urinary
Female Urinary Incontinence: GP resources MANAGEMENT OF URINARY INCONTINENCE IN WOMEN Dr Marcus Carey 20 February 2016 www.thewomens.org.au Clinical Practice Guidelines GP management of female urinary
Overactive bladder can result from one or more of the following causes:
 Overactive bladder can affect people of any age; however, it is more common in older people. Effective treatments are available and seeing your doctor for symptoms of overactive bladder often results in
Overactive bladder can affect people of any age; however, it is more common in older people. Effective treatments are available and seeing your doctor for symptoms of overactive bladder often results in
Table 1. International Consultation on Incontinence recommendations for frail older adults
 Table 1. International Consultation on Incontinence recommendations for frail older adults Clinicians need to assess and manage co-existing co morbid conditions which are known to have an impact on continence
Table 1. International Consultation on Incontinence recommendations for frail older adults Clinicians need to assess and manage co-existing co morbid conditions which are known to have an impact on continence
Physiology & Neurophysiology of lower U.T.
 Physiology & Neurophysiology of lower U.T. Classification of voiding dysfunction Evaluation of a child with voiding dysfunction Management Storage Ø Adequate volume of urine Ø At LOW pressure Ø With NO
Physiology & Neurophysiology of lower U.T. Classification of voiding dysfunction Evaluation of a child with voiding dysfunction Management Storage Ø Adequate volume of urine Ø At LOW pressure Ø With NO
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Urinary incontinence in women: the management of urinary incontinence in women 1.1 Short title Urinary incontinence in women
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Urinary incontinence in women: the management of urinary incontinence in women 1.1 Short title Urinary incontinence in women
Dr. Aso Urinary Symptoms
 Haematuria The presence of blood in the urine (haematuria) is always abnormal and may be the only indication of pathology in the urinary tract. False positive stick tests and the discolored urine caused
Haematuria The presence of blood in the urine (haematuria) is always abnormal and may be the only indication of pathology in the urinary tract. False positive stick tests and the discolored urine caused
Mr. GIT KAH ANN. Pakar Klinikal Urologi Hospital Kuala Lumpur.
 Mr. GIT KAH ANN Pakar Klinikal Urologi Hospital Kuala Lumpur drgitka@yahoo.com 25 Jan 2007 HIGHLIGHTS Introduction ICS Definition Making a Diagnosis Voiding Chart Investigation Urodynamics Ancillary Investigations
Mr. GIT KAH ANN Pakar Klinikal Urologi Hospital Kuala Lumpur drgitka@yahoo.com 25 Jan 2007 HIGHLIGHTS Introduction ICS Definition Making a Diagnosis Voiding Chart Investigation Urodynamics Ancillary Investigations
q7:480499_P0 6/5/09 10:23 AM Page 1 WHAT YOU SHOULD KNOW ABOUT YOUR DIAGNOSIS OF STRESS URINARY INCONTINENCE
 493495.q7:480499_P0 6/5/09 10:23 AM Page 1 WHAT YOU SHOULD KNOW ABOUT YOUR DIAGNOSIS OF STRESS URINARY INCONTINENCE 493495.q7:480499_P0 6/5/09 10:23 AM Page 2 What is Stress Urinary Incontinence? Urinary
493495.q7:480499_P0 6/5/09 10:23 AM Page 1 WHAT YOU SHOULD KNOW ABOUT YOUR DIAGNOSIS OF STRESS URINARY INCONTINENCE 493495.q7:480499_P0 6/5/09 10:23 AM Page 2 What is Stress Urinary Incontinence? Urinary
Ben Herbert Alex Wojtowicz
 Ben Herbert Alex Wojtowicz 54 year old female presenting with: Dragging sensation Urinary incontinence Some faecal incontinence HPC Since May 14 had noticed a mass protruding from the vagina when going
Ben Herbert Alex Wojtowicz 54 year old female presenting with: Dragging sensation Urinary incontinence Some faecal incontinence HPC Since May 14 had noticed a mass protruding from the vagina when going
LAPAROSCOPIC REPAIR OF PELVIC FLOOR
 LAPAROSCOPIC REPAIR OF PELVIC FLOOR Dr. R. K. Mishra Elements comprising the Pelvis Bones Ilium, ischium and pubis fusion Ligaments Muscles Obturator internis muscle Arcus tendineus levator ani or white
LAPAROSCOPIC REPAIR OF PELVIC FLOOR Dr. R. K. Mishra Elements comprising the Pelvis Bones Ilium, ischium and pubis fusion Ligaments Muscles Obturator internis muscle Arcus tendineus levator ani or white
INCONTINENCE. Continence and Pelvic Floor Rehabilitation TYPES OF INCONTINENCE STRESS INCONTINENCE STRESS INCONTINENCE STRESS INCONTINENCE 11/08/2015
 INCONTINENCE Continence and Pelvic Floor Rehabilitation Dr Irmina Nahon PhD Pelvic Floor Physiotherapist www.nahonpfed.com.au Defined as the accidental and inappropriate passage of urine or faeces (ICI
INCONTINENCE Continence and Pelvic Floor Rehabilitation Dr Irmina Nahon PhD Pelvic Floor Physiotherapist www.nahonpfed.com.au Defined as the accidental and inappropriate passage of urine or faeces (ICI
Pelvic Floor Therapy for the Neurologic Client Carina Siracusa, PT, DPT, WCS
 Pelvic Floor Therapy for the Neurologic Client Carina Siracusa, PT, DPT, WCS OhioHealth, Columbus Ohio Disclosures I have nothing to disclose Objectives Describe the role of a pelvic floor therapist in
Pelvic Floor Therapy for the Neurologic Client Carina Siracusa, PT, DPT, WCS OhioHealth, Columbus Ohio Disclosures I have nothing to disclose Objectives Describe the role of a pelvic floor therapist in
Taking Control of your Bladder, or. Don't make me laugh when laughter isn't the best medicine: a discussion on urinary incontinence
 Taking Control of your Bladder, or Don't make me laugh when laughter isn't the best medicine: a discussion on urinary incontinence Brett Vassallo, MD, FACOG, FAC Female Pelvic Medicine and Reconstructive
Taking Control of your Bladder, or Don't make me laugh when laughter isn't the best medicine: a discussion on urinary incontinence Brett Vassallo, MD, FACOG, FAC Female Pelvic Medicine and Reconstructive
SUMMARY OF THE GUIDELINE
 NEW PROPOSED GUIDELINE URINARY INCONTINENCE The CUA Guidelines Committee has been busy developing new guidelines and updating existing ones. A subcommittee chaired by Dr. Jacques Corcos has produced this
NEW PROPOSED GUIDELINE URINARY INCONTINENCE The CUA Guidelines Committee has been busy developing new guidelines and updating existing ones. A subcommittee chaired by Dr. Jacques Corcos has produced this
Female Urinary Incontinence
 Primary Care Internal Medicine Female Urinary Incontinence May Wakamatsu, MD MGH Vincent Obstetrics & Gynecology Dept Division of Female Pelvic Medicine & Reconstructive Surgery 2015 Female Urinary Incontinence
Primary Care Internal Medicine Female Urinary Incontinence May Wakamatsu, MD MGH Vincent Obstetrics & Gynecology Dept Division of Female Pelvic Medicine & Reconstructive Surgery 2015 Female Urinary Incontinence
Appendix E: Continence Care and Bowel Management Program Training Presentation. Audience: For Registered Staff Release Date: December 22, 2010
 Appendix E: Continence Care and Bowel Management Program Training Presentation Audience: For Registered Staff Release Date: December 22, 2010 Objectives Address individual needs and preferences with respect
Appendix E: Continence Care and Bowel Management Program Training Presentation Audience: For Registered Staff Release Date: December 22, 2010 Objectives Address individual needs and preferences with respect
Module 3 Causes Of Urinary Incontinence
 Causes Of Urinary Incontinence V4: Last Reviewed September 2017 Learning Outcomes Appreciate the numerous requirements and skills necessary for the person to achieve and maintain urinary continence Discuss
Causes Of Urinary Incontinence V4: Last Reviewed September 2017 Learning Outcomes Appreciate the numerous requirements and skills necessary for the person to achieve and maintain urinary continence Discuss
Stress Incontinence. Susannah Elvy Urogynaecology CNS
 Stress Incontinence Susannah Elvy Urogynaecology CNS Definitions Prevalence Assessment Investigation Treatment Surgery Men International Continence Society define as the complaint of any involuntary leakage
Stress Incontinence Susannah Elvy Urogynaecology CNS Definitions Prevalence Assessment Investigation Treatment Surgery Men International Continence Society define as the complaint of any involuntary leakage
International Federation of Gynecology and Obstetrics
 International Federation of Gynecology and Obstetrics COMMITTEE FOR UROGYNAECOLOGY AND PELVIC FLOOR MEMBER: TSUNG-HSIEN (CHARLES) SU, CHAIR (TAIWAN) DAVID RICHMOND, CO-CHAIR (UK) CHITTARANJAN PURANDARE,
International Federation of Gynecology and Obstetrics COMMITTEE FOR UROGYNAECOLOGY AND PELVIC FLOOR MEMBER: TSUNG-HSIEN (CHARLES) SU, CHAIR (TAIWAN) DAVID RICHMOND, CO-CHAIR (UK) CHITTARANJAN PURANDARE,
Diane K. Newman DNP, ANP-BC, PCB-PMD, FAAN
 Diane K. Newman DNP, ANP-BC, PCB-PMD, FAAN Diane K. Newman, DNP is a Biofeedback Certified Continence Specialist. With over 35-years experience, she is an expert in the assessment and management of pelvic-floor
Diane K. Newman DNP, ANP-BC, PCB-PMD, FAAN Diane K. Newman, DNP is a Biofeedback Certified Continence Specialist. With over 35-years experience, she is an expert in the assessment and management of pelvic-floor
Neurogenic bladder. Neurogenic bladder is a type of dysfunction of the bladder due to neurological disorder.
 Definition: Neurogenic bladder Neurogenic bladder is a type of dysfunction of the bladder due to neurological disorder. Types: Nervous system diseases: Congenital: like myelodysplasia like meningocele.
Definition: Neurogenic bladder Neurogenic bladder is a type of dysfunction of the bladder due to neurological disorder. Types: Nervous system diseases: Congenital: like myelodysplasia like meningocele.
Guidelines on Urinary Incontinence
 Guidelines on Urinary Incontinence J. Thüroff (chairman), P. Abrams, K.E. Andersson, W. Artibani, E. Chartier-Kastler, C. Hampel, Ph. van Kerrebroeck European Association of Urology 2006 TABLE OF CONTENTS
Guidelines on Urinary Incontinence J. Thüroff (chairman), P. Abrams, K.E. Andersson, W. Artibani, E. Chartier-Kastler, C. Hampel, Ph. van Kerrebroeck European Association of Urology 2006 TABLE OF CONTENTS
Urogynaecology & Prolapse. Alexander Denning and Leifa Jennings
 + Urogynaecology & Prolapse Alexander Denning and Leifa Jennings + Contents What even is prolapse / urogynaecology? Pelvic floor anatomy Prolapse Urinary incontinence Prevention The end (woot) + Urogynaecology
+ Urogynaecology & Prolapse Alexander Denning and Leifa Jennings + Contents What even is prolapse / urogynaecology? Pelvic floor anatomy Prolapse Urinary incontinence Prevention The end (woot) + Urogynaecology
Urinary Incontinence
 Urinary Incontinence Millions of women experience involuntary loss of urine called urinary incontinence (UI). Some women may lose a few drops of urine while running or coughing. Others may feel a strong,
Urinary Incontinence Millions of women experience involuntary loss of urine called urinary incontinence (UI). Some women may lose a few drops of urine while running or coughing. Others may feel a strong,
Urinary Incontinence. Lee A. Jennings, MD, MSHS. Assistant Professor Reynolds Department of Geriatrics University of Oklahoma Health Sciences Center
 Urinary Incontinence Lee A. Jennings, MD, MSHS Assistant Professor Reynolds Department of Geriatrics University of Oklahoma Health Sciences Center Slides adapted from Alison Moore, MD, MPH University of
Urinary Incontinence Lee A. Jennings, MD, MSHS Assistant Professor Reynolds Department of Geriatrics University of Oklahoma Health Sciences Center Slides adapted from Alison Moore, MD, MPH University of
This information is intended as an overview only
 This information is intended as an overview only Please refer to the INSTRUCTIONS FOR USE included with this device for indications, contraindications, warnings, precautions and other important information
This information is intended as an overview only Please refer to the INSTRUCTIONS FOR USE included with this device for indications, contraindications, warnings, precautions and other important information
Incontinence. When I was given this topic in urology to discuss with you today I
 Incontinence When I was given this topic in urology to discuss with you today I was slightly disappointed. I personally see mostly men for problems such as stones, benign prostatic hyperplasia, prostate
Incontinence When I was given this topic in urology to discuss with you today I was slightly disappointed. I personally see mostly men for problems such as stones, benign prostatic hyperplasia, prostate
EAU GUIDELINES ON URINARY INCONTINENCE
 EU GUIDELINES ON URINRY INONTINENE (Limited text update March 2017) F.. urkhard (hair), J.L.H.R. osch, F. ruz, G.E. Lemack,.K. Nambiar, N. Thiruchelvam,. Tubaro Guidelines ssociates: D. mbühl, D. edretdinova,
EU GUIDELINES ON URINRY INONTINENE (Limited text update March 2017) F.. urkhard (hair), J.L.H.R. osch, F. ruz, G.E. Lemack,.K. Nambiar, N. Thiruchelvam,. Tubaro Guidelines ssociates: D. mbühl, D. edretdinova,
NON-Neurogenic Chronic Urinary Retention AUA White Paper
 NON-Neurogenic Chronic Urinary Retention AUA White Paper Great Lakes SUNA Inside Urology March 16, 2018 Michelle J. Lajiness FNP-BC Nurse Practitioner DMC Urology Incidence Really unknown Lack consensus
NON-Neurogenic Chronic Urinary Retention AUA White Paper Great Lakes SUNA Inside Urology March 16, 2018 Michelle J. Lajiness FNP-BC Nurse Practitioner DMC Urology Incidence Really unknown Lack consensus
Interventional procedures guidance Published: 12 October 2016 nice.org.uk/guidance/ipg566
 Single-incision short sling mesh insertion for stress urinary incontinence in women Interventional procedures guidance Published: 12 October 2016 nice.org.uk/guidance/ipg566 Your responsibility This guidance
Single-incision short sling mesh insertion for stress urinary incontinence in women Interventional procedures guidance Published: 12 October 2016 nice.org.uk/guidance/ipg566 Your responsibility This guidance
When Laughing is No Longer Funny Managing Transient Urinary Incontinence in Hospitalized Elderly Women
 When Laughing is No Longer Funny Managing Transient Urinary Incontinence in Hospitalized Elderly Women Grace Umejei, BSN, RN, CWOC. Texas Health Presbyterian Hospital Dallas NICHE Online Connect Webinars
When Laughing is No Longer Funny Managing Transient Urinary Incontinence in Hospitalized Elderly Women Grace Umejei, BSN, RN, CWOC. Texas Health Presbyterian Hospital Dallas NICHE Online Connect Webinars
Imaging of Pelvic Floor Weakness. Dr Susan Kouloyan-Ilic Radiologist Epworth Medical Imaging The Women s, Melbourne
 Imaging of Pelvic Floor Weakness Dr Susan Kouloyan-Ilic Radiologist Epworth Medical Imaging The Women s, Melbourne Outline Overview and Epidemiology Risk Factors, Causes and Results Review of Relevant
Imaging of Pelvic Floor Weakness Dr Susan Kouloyan-Ilic Radiologist Epworth Medical Imaging The Women s, Melbourne Outline Overview and Epidemiology Risk Factors, Causes and Results Review of Relevant
21/03/2016. The urogynaecologist approach. Urinary continence management in women: a multidisciplinary approach. Dr Anna Rosamillia
 Urinary continence management in women: a multidisciplinary approach The urogynaecologist approach Dr Anna Rosamillia What is normal bladder function? Incontinence is not normal Normal voiding is 7-8 times
Urinary continence management in women: a multidisciplinary approach The urogynaecologist approach Dr Anna Rosamillia What is normal bladder function? Incontinence is not normal Normal voiding is 7-8 times
Treatment Outcomes of Tension-free Vaginal Tape Insertion
 Are the Treatment Outcomes of Tension-free Vaginal Tape Insertion the Same for Patients with Stress Urinary Incontinence with or without Intrinsic Sphincter Deficiency? A Retrospective Study in Hong Kong
Are the Treatment Outcomes of Tension-free Vaginal Tape Insertion the Same for Patients with Stress Urinary Incontinence with or without Intrinsic Sphincter Deficiency? A Retrospective Study in Hong Kong
AGENDA. 8:00 AM 8:30 AM Pelvic Anatomy of the Lower Urinary Tract and the Anatomy and Physiology of Continence/Incontinence Mickey M.
 Thursday, June 12, 2014 Juniper Ballroom 1: Exhibits AGENDA 6:30 AM 8:00 AM Breakfast and Exhibits EVALUATION AND MANAGEMENT OF LOWER URINARY TRACT SYMPTOMS 8:00 AM 8:30 AM Pelvic Anatomy of the Lower
Thursday, June 12, 2014 Juniper Ballroom 1: Exhibits AGENDA 6:30 AM 8:00 AM Breakfast and Exhibits EVALUATION AND MANAGEMENT OF LOWER URINARY TRACT SYMPTOMS 8:00 AM 8:30 AM Pelvic Anatomy of the Lower
Female Urinary Incontinence: What It Is and What You Can Do About It
 Female Urinary Incontinence: What It Is and What You Can Do About It Urogynecology Patient Information Sheet What is Urinary Incontinence? Stress Incontinence is a leakage of urine that occurs, for example,
Female Urinary Incontinence: What It Is and What You Can Do About It Urogynecology Patient Information Sheet What is Urinary Incontinence? Stress Incontinence is a leakage of urine that occurs, for example,
9/24/2015. Pelvic Floor Disorders. Agenda. What is the Pelvic Floor? Pelvic Floor Problems
 Management of Pelvic Floor Disorders Doctor, I don t want THAT mesh! Agenda What are pelvic floor disorders (PFDs)? What are the treatment options? Expectant. Conservative. Surgical. How and when are grafts
Management of Pelvic Floor Disorders Doctor, I don t want THAT mesh! Agenda What are pelvic floor disorders (PFDs)? What are the treatment options? Expectant. Conservative. Surgical. How and when are grafts
Incontinence. Anatomy The human body has two kidneys. The kidneys continuously filter the blood and make urine.
 Incontinence Introduction Urinary incontinence occurs when a person cannot control the emptying of his or her urinary bladder. It can happen to anyone, but is very common in older people. Urinary incontinence
Incontinence Introduction Urinary incontinence occurs when a person cannot control the emptying of his or her urinary bladder. It can happen to anyone, but is very common in older people. Urinary incontinence
Urinary Incontinence. Alison A Moore, MD, FACP
 Urinary Incontinence Alison A Moore, MD, FACP Professor of Medicine/Geriatric Medicine David Geffen School of Medicine at UCLA Department of Medicine, Division of Geriatrics Urinary Incontinence (UI) Involuntary
Urinary Incontinence Alison A Moore, MD, FACP Professor of Medicine/Geriatric Medicine David Geffen School of Medicine at UCLA Department of Medicine, Division of Geriatrics Urinary Incontinence (UI) Involuntary
Continence Promotion in
 Everybody s Business- Continence Promotion in Aged Care Melissa O Grady Clinical Nurse Consultant Continence Warning Some graphic images are contained in this presentation Objectives What is Old Age? What
Everybody s Business- Continence Promotion in Aged Care Melissa O Grady Clinical Nurse Consultant Continence Warning Some graphic images are contained in this presentation Objectives What is Old Age? What
INCONTINENCE What can Wee do about it?
 Prevalence INCONTINENCE What can Wee do about it? High risk groups Myths Aetiology Assessment-History Assessment-Drugs Assessment- Examination & Tests INCONTINENCE What can wee do about it? Treatment-First
Prevalence INCONTINENCE What can Wee do about it? High risk groups Myths Aetiology Assessment-History Assessment-Drugs Assessment- Examination & Tests INCONTINENCE What can wee do about it? Treatment-First
Normal micturition involves complex
 NEW TARGET FOR INTERVENTION: THE NEUROUROLOGY CONNECTION * Donald R. Ostergard, MD, FACOG ABSTRACT Urine storage and release are under the control of the parasympathetic, sympathetic, and somatic nervous
NEW TARGET FOR INTERVENTION: THE NEUROUROLOGY CONNECTION * Donald R. Ostergard, MD, FACOG ABSTRACT Urine storage and release are under the control of the parasympathetic, sympathetic, and somatic nervous
Sep \8958 Appell Dmochowski.ppt LMF 1
 Surgical Outcomes (How did we get ourselves into this mess?) Roger R. Dmochowski, MD, FACS Department of Urologic Surgery Vanderbilt University School of Medicine Nashville, Tennessee Considerations Evaluation
Surgical Outcomes (How did we get ourselves into this mess?) Roger R. Dmochowski, MD, FACS Department of Urologic Surgery Vanderbilt University School of Medicine Nashville, Tennessee Considerations Evaluation
Continence. Who cares and does it matter? Dr Carl Hanger Geriatrician, CDHB SI Alliance Stroke Education Day 2/11/17
 Continence. Who cares and does it matter? Dr Carl Hanger Geriatrician, CDHB SI Alliance Stroke Education Day 2/11/17 1500 pages, leading stroke experts Does it Matter? Definitely! Patient Dignity / QOL
Continence. Who cares and does it matter? Dr Carl Hanger Geriatrician, CDHB SI Alliance Stroke Education Day 2/11/17 1500 pages, leading stroke experts Does it Matter? Definitely! Patient Dignity / QOL
Post operative voiding dysfunction and the Value of Urodynamics. Dr Salwan Al-Salihi Urogynaecologist Obstetrician and Gynaecologist
 Post operative voiding dysfunction and the Value of Urodynamics Dr Salwan Al-Salihi Urogynaecologist Obstetrician and Gynaecologist Learning objectives: v Pathophysiology of post op voiding dysfunction.
Post operative voiding dysfunction and the Value of Urodynamics Dr Salwan Al-Salihi Urogynaecologist Obstetrician and Gynaecologist Learning objectives: v Pathophysiology of post op voiding dysfunction.
FEMALE URINARY INCONTINENCE: WHAT IT IS AND WHAT YOU CAN DO ABOUT IT
 URO-GYNECOLOGY PATIIENT IINFORMATIION SHEET FEMALE URINARY INCONTINENCE: WHAT IT IS AND WHAT YOU CAN DO ABOUT IT What is Urinary Incontinence? Stress Incontinence is a leakage of urine that occurs, for
URO-GYNECOLOGY PATIIENT IINFORMATIION SHEET FEMALE URINARY INCONTINENCE: WHAT IT IS AND WHAT YOU CAN DO ABOUT IT What is Urinary Incontinence? Stress Incontinence is a leakage of urine that occurs, for
The Neurogenic Bladder
 The Neurogenic Bladder Outline Brandon Haynes, MD Resident Physician Department of Urology Jelena Svircev, MD Assistant Professor Department of Rehabilitation Medicine Anatomy and Bladder Physiology Bladder
The Neurogenic Bladder Outline Brandon Haynes, MD Resident Physician Department of Urology Jelena Svircev, MD Assistant Professor Department of Rehabilitation Medicine Anatomy and Bladder Physiology Bladder
Prolapse & Urogynaecology. Hester Mannion and Fabi Sica
 Prolapse & Urogynaecology Hester Mannion and Fabi Sica Take home messages Prolapse and associated incontinence is very common It has a devastating effect on the QoL of the patient and their partner Strategies
Prolapse & Urogynaecology Hester Mannion and Fabi Sica Take home messages Prolapse and associated incontinence is very common It has a devastating effect on the QoL of the patient and their partner Strategies
Pelvic Floor Therapy for the Oncology Patient
 Therapy for the Oncology Patient CARINA SIRACUSA, PT, DPT, WCS OHIOHEALTH PELVIC FLOOR PHYSICAL THERAPIST ONCOLOGY REHABILITATION PROGRAM COORDINATOR What does a pelvic floor therapist treat? Muscles Muscles
Therapy for the Oncology Patient CARINA SIRACUSA, PT, DPT, WCS OHIOHEALTH PELVIC FLOOR PHYSICAL THERAPIST ONCOLOGY REHABILITATION PROGRAM COORDINATOR What does a pelvic floor therapist treat? Muscles Muscles
Urodynamic study before and after radical porstatectomy 가톨릭의대성바오로병원김현우
 Urodynamic study before and after radical porstatectomy 가톨릭의대성바오로병원김현우 Introduction Radical prostatectomy - treatment of choice for patients with localized prostate cancer. Urinary incontinence and/or
Urodynamic study before and after radical porstatectomy 가톨릭의대성바오로병원김현우 Introduction Radical prostatectomy - treatment of choice for patients with localized prostate cancer. Urinary incontinence and/or