Hemorrhoids. Carlos R. Alvarez-Allende PGY-III Colorectal Surgery
|
|
|
- Marion Conley
- 5 years ago
- Views:
Transcription
1 Hemorrhoids Carlos R. Alvarez-Allende PGY-III Colorectal Surgery
2 Overview Anatomy Classification Etiology Incidence Symptoms Differential Diagnosis Medical Management Surgical Management
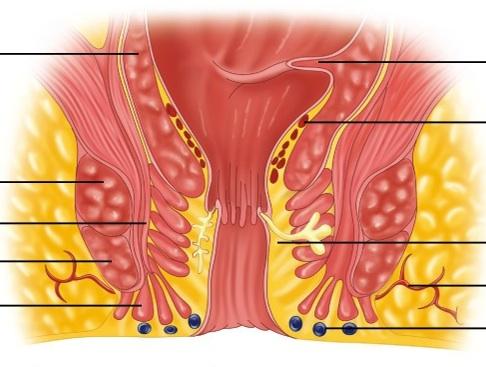
3 Anatomy Anal canal has 3 regions of fibrovascular cushions Located in the left lateral, right posterior and right anterior regions of the canal Contain submucosa, blood vessels, smooth muscle and connective tissue Contribute 15% to 20% of the resting anal pressure Prevent fecal incontinence by filling with blood during times of increased abdominal pressure and decreased anal tone
4 Anatomy
5 Anatomy The term hemorrhoid is used when one of these cushions enlarges and produces symptoms. Internal hemorrhoids Located above dentate line Covered with mucosa No sensory innervation - painless External hemorrhoids Located below dentate line Covered with anoderm Sensory innervation - painful
6 Classification Internal Hemorrhoids Grade I Grade II No prolapse, bleeding Prolapse with spontaneous reduction Grade III Prolapse requiring manual reduction Grade IV Prolapse not amenable to reduction secondary to thrombosis/incarceration
7 Etiology Etiology of hemorrhoids remains uncertain Pathophysiology includes: Elevated anal sphincter pressures Abnormal dilation of the internal hemorrhoid venous plexus Distention of the arteriovenous anastomosis Prolapse of the cushion and surrounding tissue
8 Etiology Risk factors: Constant straining with defecation Prolonged efforts at defecation History of constipation Inadequate fiber intake Long periods on the commode Conditions associated with increased intraabdominal pressure
9 Incidence Unknown incidence of hemorrhoids. Reported prevalence of 4.4% in the United States Approximately 10 million people affected Whites more likely affected than African Americans Peak incidence between 45 and 60 years of age for both genders Pregnant women and elderly patients at increased risk
10 Symptoms Painless bleeding is the most frequent complaint Other symptoms include swelling, prolapse, pruritus, hygiene problems and pain Prolapse of internal hemorrhoids occurs with straining Fecal leakage and pruritus Pain is associated with incarceration and strangularion Pain associated with external hemorrhoids associated with thrombosis Diminishes after 48 to 72 hours
11 Differential Diagnosis Evaluation should include digital rectal exam and anoscopy Hemorrhoids and rectal varices are not the same Located more proximal in the anal canal and rectum Treated with procedures that reduce portal hypertension No increased incidence of hemorrhoids in patients with portal hypertension
12 Differential Diagnosis Symptoms Pain and bleeding after bowel movement Forceful straining to have bowel movement Blood mixed with stools Drainage of pus Constant moisture Mucous drainage and incontinence Cause Ulcer/fissure disease Pelvic floor abnormalities Neoplasm Abscess/fistula, IBD Condyloma Rectal prolapse
13 Medical Management Lifestyle modifications Dietary changes Increased fluid and fiber intake 6 to 8 glasses of fluid daily 25 to 30 grams of fiber per day Dietary supplements Psyllum Improved anal hygiene Avoid excessive scrubbing Frequent sitz baths Use facial and baby wipes
14 Medical Management Strict toilet regimen Avoid reading in the toilet Avoid sitting on the toilet for long periods of time Do not defer the urge to defecate Over the counter topical treatments improve hygiene and alleviate associated symptoms Grade I, II and III internal hemorrhoids usually respond to these modifications
15 Rubber band ligation Best suited for Grade I internal hemorrhoids Bleeding with minimal prolapse Can be used to treat Grade II and III hemorrhoids Not indicated for External Hemorrhoids Somatic innervation Rubber band promotes inflammation that leads to ulcer formation, scarring and fixation to the rectal wall. Band is retained for 2 to 10 days

16 Rubber band ligation
17 Rubber band ligation Repeat banding should be performed after 4 weeks Allows inflammation to resolve Bands placed too close to the dentate line should be removed Discomfort after banding is managed with sitz baths, analgesics and avoidance of constipation
18 Rubber band ligation Complication rate of 0.5% to 8% Vasovagal reaction Bleeding 1 to 2 weeks after procedure Pelvic sepsis Fever, perianal pain, perineal cellulitis, watery discharge and urinary retention Relatively contraindicated in patients chronically anticoagulated Success rate over 75% in patients with Grade I and II hemorrhoids
19 Sclerotherapy Injection of irritant at the base of the hemorrhoid 1 to 2 ml of an oil based irritant containing 5% phenol 1 to 2 ml of an aqueous irritant (ethanolamine oleate) Causes an inflammatory reaction, edema and intravascular thrombosis leading to scarring. Indicated for Grade I and II internal hemorrhoids and grade III internal hemorrhoids in immunocompromised patients
20 Sclerotherapy Complications Upper abdominal pain if injected into the hemorrhoidal vessel Erectile dysfunction if injected in the periprostatic parasympathetic nerves Pelvic sepsis can occur up to 5 days after procedure Sclerotherapy improves symptoms in up to 75% of patients with Grade II internal hemorrhoids
21 Surgical Management Indications Large Grade III and Grade IV internal hemorrhoids Mixed hemorrhoids Large external hemorrhoids Failure of medical management
22 Surgical Management Preoperative preparation Stopping anticoagulation If patient is incontinent Anal manometry Ultrasound Enema Prophylactic antibiotics for patients at high risk for endocarditis Prone jackknife or lithotomy position Perianal block with local anesthetic 30 ml of 0.25% bupivicaine
23 Surgical Management Acute thrombosis of external hemorrhoids Worsens within 24 hours Managed with sitz baths and analgesics Surgical intervention due to pain should occur within the first 24 hours Clot is evacuated and overlying skin removed to avoid recurrence Not indicated after 24 hours due to cumulative pain Topical application of 0.3% nifedipine cream Antiinflammatory Smooth muscle relaxant
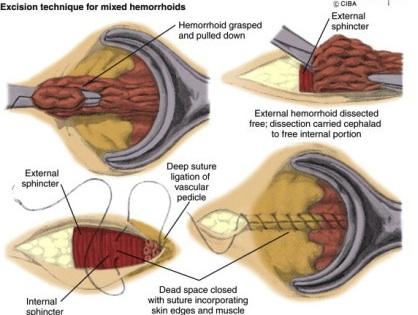
24 Surgical Hemorrhoidectomy
25 Surgical Hemorrhoidectomy Complications Most common complication is urinary retention Minimize intravenous fluids Voiding before discharge Resolves after swelling subsides Anal incontinence Anal stenosis Operate on the largest hemorrhoid first 1 cm of normal anoderm between suture lines Hemorrhage 1 to 2 weeks after procedure Reported rate of 0.9%
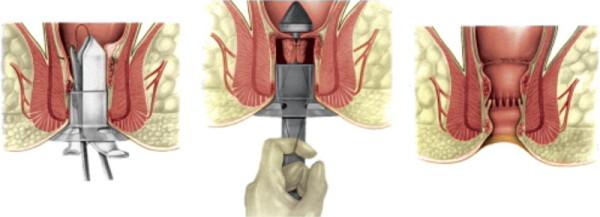
26 Surgical Hemorrhoidopexy
27 Surgical Hemorrhoidopexy Complications Urinary retention Bleeding Pain Rare complications Rectal perforation Rectovaginal fistula Pelvic sepsis Increased recurrence rate when compared with hemorrhoidectomy
Office Management of Anorectal Disease. Waqar Qureshi, MD, FRCP, FACG, FASGE Professor Baylor College of Medicine Houston Texas
 Office Management of Anorectal Disease Waqar Qureshi, MD, FRCP, FACG, FASGE Professor Baylor College of Medicine Houston Texas Commonly seen Anorectal Disease Hemorrhoids Anal fissures Pruritus Abscesses
Office Management of Anorectal Disease Waqar Qureshi, MD, FRCP, FACG, FASGE Professor Baylor College of Medicine Houston Texas Commonly seen Anorectal Disease Hemorrhoids Anal fissures Pruritus Abscesses
Benign anorectal diseases
 Benign anorectal diseases Symptoms Bleeding Pruritus Discharge Fecal incontinence Diarrhea Constipation False need to defecate Examinations Clinical exam Anuscopy Rectosigmoidoscopy Endosonography MRI
Benign anorectal diseases Symptoms Bleeding Pruritus Discharge Fecal incontinence Diarrhea Constipation False need to defecate Examinations Clinical exam Anuscopy Rectosigmoidoscopy Endosonography MRI
Anterior anal fissure is much more common in women and may arise following vaginal delivery.
 ANAL FISSURE Definition An anal fissure (synonym: fissure-in-ano) is a longitudinal split in the anoderm of the distal anal canal which extends from the anal verge proximally towards, but not beyond, the
ANAL FISSURE Definition An anal fissure (synonym: fissure-in-ano) is a longitudinal split in the anoderm of the distal anal canal which extends from the anal verge proximally towards, but not beyond, the
Although disparate topics, these two different pathologic
 34 H E M O R R H O I D S A N D R E C T A L P R O L A P S E CHARLES N. HEADRICK MICHAEL J. STAMOS Although disparate topics, these two different pathologic entities are commonly misdiagnosed by both layperson
34 H E M O R R H O I D S A N D R E C T A L P R O L A P S E CHARLES N. HEADRICK MICHAEL J. STAMOS Although disparate topics, these two different pathologic entities are commonly misdiagnosed by both layperson
Hemorrhoidal Disease: A Comprehensive Review
 COLLECTIVE REVIEWS Hemorrhoidal Disease: A Comprehensive Review Orit Kaidar-Person, MD, Benjamin Person, MD, Steven D Wexner, MD, FACS, FRCS, FRCS (Ed) Hemorrhoids are one of the most common conditions
COLLECTIVE REVIEWS Hemorrhoidal Disease: A Comprehensive Review Orit Kaidar-Person, MD, Benjamin Person, MD, Steven D Wexner, MD, FACS, FRCS, FRCS (Ed) Hemorrhoids are one of the most common conditions
Dr Stephanie Ulmer General Surgeon Middlemore Hospital Auckland
 Dr Stephanie Ulmer General Surgeon Middlemore Hospital Auckland 16:30-17:25 WS #168: Modern Treatment of Haemorrhoids 17:35-18:30 WS #180: Modern Treatment of Haemorrhoids (Repeated) BOTTOMS Science and
Dr Stephanie Ulmer General Surgeon Middlemore Hospital Auckland 16:30-17:25 WS #168: Modern Treatment of Haemorrhoids 17:35-18:30 WS #180: Modern Treatment of Haemorrhoids (Repeated) BOTTOMS Science and
A painful problem. Symptoms of haemorrhoids. Causes of haemorrhoids. Your evaluation
 A painful problem Haemorrhoids, cushions of swollen veins in the anal canal, are often a source of embarrassment. They shouldn t be they re a very common problem that affects all kinds of people, including
A painful problem Haemorrhoids, cushions of swollen veins in the anal canal, are often a source of embarrassment. They shouldn t be they re a very common problem that affects all kinds of people, including
Anal Fissure: Finding the Root Cause
 Anal Fissure: Finding the Root Cause Michael A. Jobst, MD, FACS, FASCRS Surgical Associates, PC -- Lincoln, NE 27 th Annual Management of Colon and Rectal Diseases February 23, 2019 Objectives Differentiate
Anal Fissure: Finding the Root Cause Michael A. Jobst, MD, FACS, FASCRS Surgical Associates, PC -- Lincoln, NE 27 th Annual Management of Colon and Rectal Diseases February 23, 2019 Objectives Differentiate
Common Office Anorectal Problems
 Common Office Anorectal Problems Sandra J. Beck, M.D., FACS, FASCRS Associate Professor of Colon and Rectal Surgery University of Kentucky Medical Center l None Disclosures Benign Anal Rectal Disease l
Common Office Anorectal Problems Sandra J. Beck, M.D., FACS, FASCRS Associate Professor of Colon and Rectal Surgery University of Kentucky Medical Center l None Disclosures Benign Anal Rectal Disease l
Treatment of haemorrhoids. Mr Rowan Collinson FRACS Colorectal and General Surgeon Auckland
 Treatment of haemorrhoids Mr Rowan Collinson FRACS Colorectal and General Surgeon Auckland Much overlap of haemorrhoidal symptoms with other conditions Is it just the haemorrhoids? what type of haemorrhoidal
Treatment of haemorrhoids Mr Rowan Collinson FRACS Colorectal and General Surgeon Auckland Much overlap of haemorrhoidal symptoms with other conditions Is it just the haemorrhoids? what type of haemorrhoidal
Pelvic Prolapse. A Patient Guide to Pelvic Floor Reconstruction
 Pelvic Prolapse A Patient Guide to Pelvic Floor Reconstruction Pelvic Prolapse When an organ becomes displaced, or slips down in the body, it is referred to as a prolapse. Your physician has diagnosed
Pelvic Prolapse A Patient Guide to Pelvic Floor Reconstruction Pelvic Prolapse When an organ becomes displaced, or slips down in the body, it is referred to as a prolapse. Your physician has diagnosed
GI Physiology - Investigating and treating patients with pelvic floor dysfunction. Lynne Smith Department of GI Physiology NGH Sheffield
 GI Physiology - Investigating and treating patients with pelvic floor dysfunction Lynne Smith Department of GI Physiology NGH Sheffield Aims o o o To give an overview of lower GI investigations To demonstrate
GI Physiology - Investigating and treating patients with pelvic floor dysfunction Lynne Smith Department of GI Physiology NGH Sheffield Aims o o o To give an overview of lower GI investigations To demonstrate
Rectal Prolapse: A 10-Year Experience
 24 The Ochsner Journal Volume 7, Number 1, Spring 2007 25 Rectal Prolapse: A 10-Year Experience Figure 2. Physical examination. A. Concentric folds of prolapsed rectum. B. Radial folds of hemorrhoids (mucosal
24 The Ochsner Journal Volume 7, Number 1, Spring 2007 25 Rectal Prolapse: A 10-Year Experience Figure 2. Physical examination. A. Concentric folds of prolapsed rectum. B. Radial folds of hemorrhoids (mucosal
Fecal Incontinence. What is fecal incontinence?
 Scan for mobile link. Fecal Incontinence Fecal incontinence is the inability to control the passage of waste material from the body. It may be associated with constipation or diarrhea and typically occurs
Scan for mobile link. Fecal Incontinence Fecal incontinence is the inability to control the passage of waste material from the body. It may be associated with constipation or diarrhea and typically occurs
The Non-Operative Treatment of Hemorrhoids and Anal Fissures
 Hemorrhoids Current non-surgical treatments The Non-Operative Treatment of Hemorrhoids and Anal Fissures Presented by Mitchel Guttenplan, MD, FACS mitchguttenplan@yahoo.com 2007, Alan L. Goldman, M.D.,
Hemorrhoids Current non-surgical treatments The Non-Operative Treatment of Hemorrhoids and Anal Fissures Presented by Mitchel Guttenplan, MD, FACS mitchguttenplan@yahoo.com 2007, Alan L. Goldman, M.D.,
1/3/2008. Karen Burke Priscilla LeMone Elaine Mohn-Brown. Medical-Surgical Nursing Care, 2e Karen Burke, Priscilla LeMone, and Elaine Mohn-Brown
 Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 20 Caring for Clients with Bowel Disorders Diarrhea Pathophysiology Result from impaired water absorption
Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 20 Caring for Clients with Bowel Disorders Diarrhea Pathophysiology Result from impaired water absorption
Piles / Sclerosing. Endoscopy Department. Patient information leaflet
 Piles / Sclerosing Endoscopy Department Patient information leaflet You will only be given this leaflet if you have been diagnosed with piles / sclerosing. The information below outlines the condition,
Piles / Sclerosing Endoscopy Department Patient information leaflet You will only be given this leaflet if you have been diagnosed with piles / sclerosing. The information below outlines the condition,
Hemorrhoids. What are hemorrhoids? What is the cause? What are the symptoms?
 What are hemorrhoids? Hemorrhoids Hemorrhoids are swollen veins in the lower end of your intestine (rectum) or the anus. The anus is the opening where bowel movements pass out of your body. Hemorrhoids
What are hemorrhoids? Hemorrhoids Hemorrhoids are swollen veins in the lower end of your intestine (rectum) or the anus. The anus is the opening where bowel movements pass out of your body. Hemorrhoids
Anorectal Diagnostic Overview
 Anorectal Diagnostic Overview 11-25-09 3.11.2010 2009 2010 Anorectal Manometry Overview Measurement of pressures and the annotation of rectal sensation throughout the rectum and anal canal to determine:
Anorectal Diagnostic Overview 11-25-09 3.11.2010 2009 2010 Anorectal Manometry Overview Measurement of pressures and the annotation of rectal sensation throughout the rectum and anal canal to determine:
General Surgery. Haemorrhoids
 General Surgery Haemorrhoids Hemorrhoids_PRINT.indd 1 5/9/2016 5:50:45 PM A painful problem Haemorrhoids, cushions of swollen veins in the anal canal, are often a source of embarrassment. They shouldn
General Surgery Haemorrhoids Hemorrhoids_PRINT.indd 1 5/9/2016 5:50:45 PM A painful problem Haemorrhoids, cushions of swollen veins in the anal canal, are often a source of embarrassment. They shouldn
World Journal of Pharmaceutical Research SJIF Impact Factor 5.990
 SJIF Impact Factor 5.990 Volume 4, Issue 9, 608-613. Review Article ISSN 2277 7105 AYURVEDIC MANAGEMENT OF HEMORRHOIDS *Dr Sunil Kumar Pandey Lecturer, Deptt. of Shalya Tantra, A & U Tibbia College & Hospital,
SJIF Impact Factor 5.990 Volume 4, Issue 9, 608-613. Review Article ISSN 2277 7105 AYURVEDIC MANAGEMENT OF HEMORRHOIDS *Dr Sunil Kumar Pandey Lecturer, Deptt. of Shalya Tantra, A & U Tibbia College & Hospital,
PAUL E. SAVOCA, MD, FACS, FASCRS Consent Form for Hemorrhoidectomy
 PAUL E. SAVOCA, MD, FACS, FASCRS Consent Form for Hemorrhoidectomy The doctor has explained that I have the following condition: Hemorrhoids- abnormally enlarged anal veins. The following procedure will
PAUL E. SAVOCA, MD, FACS, FASCRS Consent Form for Hemorrhoidectomy The doctor has explained that I have the following condition: Hemorrhoids- abnormally enlarged anal veins. The following procedure will
ACG Clinical Guideline: Management of Benign Anorectal Disorders
 ACG Clinical Guideline: Management of Benign Anorectal Disorders Arnold Wald, MD, MACG 1, Adil E. Bharucha, MBBS, MD 2, Bard C. Cosman, MD, MPH, FASCRS 3 and William E. Whitehead, PhD, MACG 4 1 Division
ACG Clinical Guideline: Management of Benign Anorectal Disorders Arnold Wald, MD, MACG 1, Adil E. Bharucha, MBBS, MD 2, Bard C. Cosman, MD, MPH, FASCRS 3 and William E. Whitehead, PhD, MACG 4 1 Division
Haemorrhoidal artery ligation
 Haemorrhoidal artery ligation Issued: May 2010 NICE interventional procedure guidance 342 www.nice.org.uk/ipg342 NHS Evidence has accredited the process used by the NICE Interventional Procedures Programme
Haemorrhoidal artery ligation Issued: May 2010 NICE interventional procedure guidance 342 www.nice.org.uk/ipg342 NHS Evidence has accredited the process used by the NICE Interventional Procedures Programme
15. Prevention of UTI and lifestyle modifications
 15. Prevention of UTI and lifestyle modifications Key questions: Does improving poor voiding habits help prevent UTI recurrence? Does improving constipation help prevent UTI recurrence? Does increasing
15. Prevention of UTI and lifestyle modifications Key questions: Does improving poor voiding habits help prevent UTI recurrence? Does improving constipation help prevent UTI recurrence? Does increasing
Approach to the Repair of Chronic Perineal Lacerations and Rectovaginal Fistula (RVF)
") Approach to the Repair of Chronic Perineal Lacerations and Rectovaginal Fistula (RVF) Blair B. Washington MD, MHA Urogynecology & Reconstructive Pelvic Surgery Virginia Mason Medical Center Disclosures
Approach to the Repair of Chronic Perineal Lacerations and Rectovaginal Fistula (RVF) Blair B. Washington MD, MHA Urogynecology & Reconstructive Pelvic Surgery Virginia Mason Medical Center Disclosures
Case Presentation and Discussion on GI Bleeding Nolan Ortega Aludino, M.D.
 Case Presentation and Discussion on GI Bleeding Nolan Ortega Aludino, M.D. General Data R.L. R.L. 4343 years old MaleMale PacoPaco Manila Chief Complaint Anal Anal bleeding History of Present Illness 3
Case Presentation and Discussion on GI Bleeding Nolan Ortega Aludino, M.D. General Data R.L. R.L. 4343 years old MaleMale PacoPaco Manila Chief Complaint Anal Anal bleeding History of Present Illness 3
Patient information leaflet. Royal Surrey County Hospital. NHS Foundation Trust. Haemorrhoids. Day Surgery Unit
 Patient information leaflet Royal Surrey County Hospital NHS Foundation Trust Haemorrhoids Day Surgery Unit What are haemorrhoids? The anal canal (back passage) contains cushions of tissue at the top of
Patient information leaflet Royal Surrey County Hospital NHS Foundation Trust Haemorrhoids Day Surgery Unit What are haemorrhoids? The anal canal (back passage) contains cushions of tissue at the top of
Comparative Study of Outcome of Open Vs Closed Hemorrhoidectomy Vs Rubber Band Ligation in Third Degree Haemorrhoids
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 16, Issue 3 Ver. IX (March. 2017), PP 29-34 www.iosrjournals.org Comparative Study of Outcome of Vs Closed
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 16, Issue 3 Ver. IX (March. 2017), PP 29-34 www.iosrjournals.org Comparative Study of Outcome of Vs Closed
Accidental Bowel Leakage (Fecal Incontinence)
") Accidental Bowel Leakage (Fecal Incontinence) What is Accidental Bowel Leakage (ABL)? Accidental bowel leakage is the inability to control solid or liquid stool. This is the inability to control gas and
Accidental Bowel Leakage (Fecal Incontinence) What is Accidental Bowel Leakage (ABL)? Accidental bowel leakage is the inability to control solid or liquid stool. This is the inability to control gas and
THE RATIONAL TREATMENT OF INTERNAL HEMORRHOID BASED ON ITS PATHOGENESIS
 THE RATIONAL TREATMENT OF INTERNAL HEMORRHOID BASED ON ITS PATHOGENESIS Ignatius Riwanto Dept. of Surgery, Digestive div. Diponegoro Medical Faculty ACUTE CARE SURGERY BANDUNG FEBRUARY 2018 HEMORRHOID
THE RATIONAL TREATMENT OF INTERNAL HEMORRHOID BASED ON ITS PATHOGENESIS Ignatius Riwanto Dept. of Surgery, Digestive div. Diponegoro Medical Faculty ACUTE CARE SURGERY BANDUNG FEBRUARY 2018 HEMORRHOID
Surgical Management for Defecation Dysfunction
 Defecatory Dysfunction Surgical Management for Defecation Dysfunction JMAJ 46(9): 378 383, 2003 Tatsuo TERAMOTO Professor, 1st Department of Surgery, School of Medicine, Toho University Abstract: Typical
Defecatory Dysfunction Surgical Management for Defecation Dysfunction JMAJ 46(9): 378 383, 2003 Tatsuo TERAMOTO Professor, 1st Department of Surgery, School of Medicine, Toho University Abstract: Typical
MCOMPASS ANAL MANOMETRY AN OVERVIEW
 MCOMPASS ANAL MANOMETRY AN OVERVIEW ANAL MANOMETRY MEASURES PRESSURE ALLOWS INTERPRITATION SENSATION RAIR RECTAL COMPLIANCE MOTIVATION OF THE PATIENT FUNCTION OF THE PUDENDAL NERVE WHEN TO USE ANAL MANOMETRY
MCOMPASS ANAL MANOMETRY AN OVERVIEW ANAL MANOMETRY MEASURES PRESSURE ALLOWS INTERPRITATION SENSATION RAIR RECTAL COMPLIANCE MOTIVATION OF THE PATIENT FUNCTION OF THE PUDENDAL NERVE WHEN TO USE ANAL MANOMETRY
MCOMPASS ANAL MANOMETRY AN OVERVIEW
 MCOMPASS ANAL MANOMETRY AN OVERVIEW ANAL MANOMETRY MEASURES PRESSURE ALLOWS INTERPRITATION SENSATION RAIR RECTAL COMPLIANCE MOTIVATION OF THE PATIENT FUNCTION OF THE PUDENDAL NERVE WHEN TO USE ANAL MANOMETRY
MCOMPASS ANAL MANOMETRY AN OVERVIEW ANAL MANOMETRY MEASURES PRESSURE ALLOWS INTERPRITATION SENSATION RAIR RECTAL COMPLIANCE MOTIVATION OF THE PATIENT FUNCTION OF THE PUDENDAL NERVE WHEN TO USE ANAL MANOMETRY
Diagnosis of Impaired Defecatory Function with Special Reference to Physiological Tests
 Defecatory Dysfunction Diagnosis of Impaired Defecatory Function with Special Reference to Physiological Tests JMAJ 46(9): 373 377, 2003 Masatoshi OYA, Masashi UENO, and Tetsuichiro MUTO Department of
Defecatory Dysfunction Diagnosis of Impaired Defecatory Function with Special Reference to Physiological Tests JMAJ 46(9): 373 377, 2003 Masatoshi OYA, Masashi UENO, and Tetsuichiro MUTO Department of
Duc M. Vo, MD, FACS Northwest Surgical Specialists
 Duc M. Vo, MD, FACS Northwest Surgical Specialists Disclosures none Outline Definition Etiologies Exam findings Additional testing Medical management Surgical options What is fecal incontinence? Recurrent
Duc M. Vo, MD, FACS Northwest Surgical Specialists Disclosures none Outline Definition Etiologies Exam findings Additional testing Medical management Surgical options What is fecal incontinence? Recurrent
POST-OPERATIVE INSTRUCTIONS FOLLOWING RECTAL OFFICE SURGERY
 POST-OPERATIVE INSTRUCTIONS FOLLOWING RECTAL OFFICE SURGERY 1. KEEP THE RECTAL AREA CLEAN AND DRY. After a bowel movement, clean your bottom with peri-anal cleansing pads (i.e. Tucks or baby-wipes), followed
POST-OPERATIVE INSTRUCTIONS FOLLOWING RECTAL OFFICE SURGERY 1. KEEP THE RECTAL AREA CLEAN AND DRY. After a bowel movement, clean your bottom with peri-anal cleansing pads (i.e. Tucks or baby-wipes), followed
HREE Questions. Setting 3: Inpatient Facilities. Block
 Block HREE Questions Setting 3: Inpatient Facilities You have general admitting privileges to the hospital. You may see patients in the critical care unit, the pediatrics unit, the maternity unit, or recovery
Block HREE Questions Setting 3: Inpatient Facilities You have general admitting privileges to the hospital. You may see patients in the critical care unit, the pediatrics unit, the maternity unit, or recovery
EFFICAY OF RUBBER BAND LIGATION VS HEMORHOIDECTOMY IN 2 ND AND 3 RD DEGREE HEMORHOIDS
 EFFICAY OF RUBBER BAND LIGATION VS HEMORHOIDECTOMY IN 2 ND AND 3 RD DEGREE HEMORHOIDS Muhammad Kalim, Barka Sajjad, Muhammad Adnan Saeed, Saad Sajjad, Zahid Aman ABSTRACT Background: Hemorrhoids are dilatation
EFFICAY OF RUBBER BAND LIGATION VS HEMORHOIDECTOMY IN 2 ND AND 3 RD DEGREE HEMORHOIDS Muhammad Kalim, Barka Sajjad, Muhammad Adnan Saeed, Saad Sajjad, Zahid Aman ABSTRACT Background: Hemorrhoids are dilatation
Bright-red bleeding: If you have piles, you might see bright-red bleeding on the toilet paper, in the toilet bowl or on the surface of the faeces.
 What are haemorrhoids/piles? In the inner lining of the anus there are three haemorrhoidal cushions of tissue, which help to seal the anus and contribute to the control of the bowels (continence). Often,
What are haemorrhoids/piles? In the inner lining of the anus there are three haemorrhoidal cushions of tissue, which help to seal the anus and contribute to the control of the bowels (continence). Often,
Pelvic Organ Functions: Urinary, Sexual and Bowel Dysfunction after Rectal Surgery
 Pelvic Organ Functions: Urinary, Sexual and Bowel Dysfunction after Rectal Surgery Disclosure M ADHULIKA G. V ARMA M D PROFESSOR AND CHIEF S E CTION O F COLORECTAL S U R G ERY U N I V ERS ITY O F CALIFORNIA,
Pelvic Organ Functions: Urinary, Sexual and Bowel Dysfunction after Rectal Surgery Disclosure M ADHULIKA G. V ARMA M D PROFESSOR AND CHIEF S E CTION O F COLORECTAL S U R G ERY U N I V ERS ITY O F CALIFORNIA,
Principles of Surgery - Ano rectal region: Haemorrhoids
 Principles of Surgery - Ano rectal region: Haemorrhoids Maurice Brygel Director, Melbourne Hernia Clinic (www.hernia.net.au) Fellow, Royal Australian College of Surgeons (RACS) Correspondence Maurice Brygel
Principles of Surgery - Ano rectal region: Haemorrhoids Maurice Brygel Director, Melbourne Hernia Clinic (www.hernia.net.au) Fellow, Royal Australian College of Surgeons (RACS) Correspondence Maurice Brygel
Bowel and Bladder Dysfunction (BBD) Naida Kalloo, MD Pediatric Urology Children s National
 Naida Kalloo, MD Pediatric Urology Children s National") Bowel and Bladder Dysfunction (BBD) Naida Kalloo, MD Pediatric Urology Children s National What is Bowel and Bladder Dysfunction? Lower urinary tract symptoms (LUTS) and bowel movement disorders Majority
Bowel and Bladder Dysfunction (BBD) Naida Kalloo, MD Pediatric Urology Children s National What is Bowel and Bladder Dysfunction? Lower urinary tract symptoms (LUTS) and bowel movement disorders Majority
Management of Neurogenic Bowel Dysfunction. Fiona Paul, DNP, RN, CPNP Center for Motility and Functional Gastrointestinal Disorders
 Management of Neurogenic Bowel Dysfunction Fiona Paul, DNP, RN, CPNP Center for Motility and Functional Gastrointestinal Disorders DEFECATION Delivery of colon contents to the rectum Rectal compliance
Management of Neurogenic Bowel Dysfunction Fiona Paul, DNP, RN, CPNP Center for Motility and Functional Gastrointestinal Disorders DEFECATION Delivery of colon contents to the rectum Rectal compliance
2015 General Surgery Survival Guide
 2015 General Surgery Survival Guide Chapter 9: Hemorrhoids New codes in the block: 45350 & 45398 45350: Sigmoidoscopy, flexible; with band ligation(s) (eg, hemorrhoids) 45398: Colonoscopy, flexible; with
2015 General Surgery Survival Guide Chapter 9: Hemorrhoids New codes in the block: 45350 & 45398 45350: Sigmoidoscopy, flexible; with band ligation(s) (eg, hemorrhoids) 45398: Colonoscopy, flexible; with
A Nursing Assessment Tool for Adults With Fecal Incontinence
 Journal of Wound, Ostomy and Continence Nursing 2000, 279- A Nursing Assessment Tool for Adults With Fecal Incontinence Christine Norton, MA, RN, and Sonya Chelvanayagam, MSc, RN Abstract Fecal incontinence
Journal of Wound, Ostomy and Continence Nursing 2000, 279- A Nursing Assessment Tool for Adults With Fecal Incontinence Christine Norton, MA, RN, and Sonya Chelvanayagam, MSc, RN Abstract Fecal incontinence
Common Gastrointestinal Problems in the Elderly
 Common Gastrointestinal Problems in the Elderly Brian Viviano, D.O. Objectives Understand the pathophysiology, clinical manifestations, diagnosis and management of GI diseases of the elderly. Differentiate
Common Gastrointestinal Problems in the Elderly Brian Viviano, D.O. Objectives Understand the pathophysiology, clinical manifestations, diagnosis and management of GI diseases of the elderly. Differentiate
Constipation Information Leaflet THE DIGESTIVE SYSTEM. gutscharity.org.uk
 THE DIGESTIVE SYSTEM http://healthfavo.com/digestive-system-for-kids.html This factsheet is about Constipation Constipation is a symptom that can mean different things to different people but the usual
THE DIGESTIVE SYSTEM http://healthfavo.com/digestive-system-for-kids.html This factsheet is about Constipation Constipation is a symptom that can mean different things to different people but the usual
Fecal Incontinence. Inability to retain feces or bowel movements, resulting in involuntary passage of feces or bowel movements
 Fecal Incontinence (Involuntary Passage of Feces or Bowel Movements) Basics OVERVIEW Inability to retain feces or bowel movements, resulting in involuntary passage of feces or bowel movements GENETICS
Fecal Incontinence (Involuntary Passage of Feces or Bowel Movements) Basics OVERVIEW Inability to retain feces or bowel movements, resulting in involuntary passage of feces or bowel movements GENETICS
Treatments for Fecal Incontinence A Review of the Research for Adults
 Treatments for Fecal Incontinence A Review of the Research for Adults e Is This Information Right for Me? This information is right for you if: Your health care professional* said you or your loved one
Treatments for Fecal Incontinence A Review of the Research for Adults e Is This Information Right for Me? This information is right for you if: Your health care professional* said you or your loved one
Rectal Cancer. About the Colon and Rectum. Symptoms. Colorectal Cancer Screening
 Patient information regarding care and surgery associated with RECTAL CANCER by Robert K. Cleary, M.D., John C. Eggenberger, M.D., Amalia J. Stefanou., M.D. location: Michigan Heart and Vascular Institute,
Patient information regarding care and surgery associated with RECTAL CANCER by Robert K. Cleary, M.D., John C. Eggenberger, M.D., Amalia J. Stefanou., M.D. location: Michigan Heart and Vascular Institute,
Postpartum Complications
 ACOG Postpartum Toolkit Postpartum Complications Introduction The effects of pregnancy on many organ systems begin to resolve spontaneously after birth of the infant and delivery of the placenta. The timeline
ACOG Postpartum Toolkit Postpartum Complications Introduction The effects of pregnancy on many organ systems begin to resolve spontaneously after birth of the infant and delivery of the placenta. The timeline
Hyung Kyu Yang. Hemorrhoids
 Hyung Kyu Yang Hemorrhoids 123 Hemorrhoids Hyung Kyu Yang Hemorrhoids Hyung Kyu Yang Yang Hospital Seoul Republic of Korea Videos to this book can be accessed at http://www.springerimages.com/videos/978-3-642-41797-9
Hyung Kyu Yang Hemorrhoids 123 Hemorrhoids Hyung Kyu Yang Hemorrhoids Hyung Kyu Yang Yang Hospital Seoul Republic of Korea Videos to this book can be accessed at http://www.springerimages.com/videos/978-3-642-41797-9
LAPAROSCOPIC REPAIR OF PELVIC FLOOR
 LAPAROSCOPIC REPAIR OF PELVIC FLOOR Dr. R. K. Mishra Elements comprising the Pelvis Bones Ilium, ischium and pubis fusion Ligaments Muscles Obturator internis muscle Arcus tendineus levator ani or white
LAPAROSCOPIC REPAIR OF PELVIC FLOOR Dr. R. K. Mishra Elements comprising the Pelvis Bones Ilium, ischium and pubis fusion Ligaments Muscles Obturator internis muscle Arcus tendineus levator ani or white
Stapled transanal rectal resection for obstructed defaecation syndrome
 Stapled transanal rectal resection for obstructed Issued: June 2010 www.nice.org.uk/ipg351 NHS Evidence has accredited the process used by the NICE Interventional Procedures Programme to produce interventional
Stapled transanal rectal resection for obstructed Issued: June 2010 www.nice.org.uk/ipg351 NHS Evidence has accredited the process used by the NICE Interventional Procedures Programme to produce interventional
DISEASES OF THE COLON, RECTUM, & ANUS
 DISEASES OF THE COLON, RECTUM, & ANUS Rocco Ricciardi, MD, MPH Chief, Section of Colon & Rectal Surgery Massachusetts General Hospital Associate Professor of Surgery Harvard Medical School CASE 1 Hemorrhoid
DISEASES OF THE COLON, RECTUM, & ANUS Rocco Ricciardi, MD, MPH Chief, Section of Colon & Rectal Surgery Massachusetts General Hospital Associate Professor of Surgery Harvard Medical School CASE 1 Hemorrhoid
Aging Persons with Intellectual Developmental Disorders (IDD): Constipation KEYPOINTS OVERVIEW
: Constipation KEYPOINTS OVERVIEW") Aging Persons with Intellectual Developmental Disorders (IDD): Constipation KEYPOINTS A major medical conditions that commonly is seen among persons with IDD and may lead to serious complications is constipation.
Aging Persons with Intellectual Developmental Disorders (IDD): Constipation KEYPOINTS A major medical conditions that commonly is seen among persons with IDD and may lead to serious complications is constipation.
INCONTINENCE & DEFAECATORY DISORDERS AFTER HAEMORRHOIDECTOMY - MINIMISING THE RISK
 INCONTINENCE & DEFAECATORY DISORDERS AFTER HAEMORRHOIDECTOMY - MINIMISING THE RISK SURGICAL CONTROVERSIES SYMPOSIUM OCTOBER 2015 Stephen Grobler Bloemfontein Haemorrhoidal Disease One of the most common
INCONTINENCE & DEFAECATORY DISORDERS AFTER HAEMORRHOIDECTOMY - MINIMISING THE RISK SURGICAL CONTROVERSIES SYMPOSIUM OCTOBER 2015 Stephen Grobler Bloemfontein Haemorrhoidal Disease One of the most common
To inject, to band or to excise? These were the alternatives for a colorectal surgeon
 CHAPTER 2 Hemorrhoids To inject, to band or to excise? These were the alternatives for a colorectal surgeon some 50 years ago, when sclerosant injection, rubber band ligation and hemorrhoidectomy were
CHAPTER 2 Hemorrhoids To inject, to band or to excise? These were the alternatives for a colorectal surgeon some 50 years ago, when sclerosant injection, rubber band ligation and hemorrhoidectomy were
Chapter 31 Bowel Elimination
 Chapter 31 Bowel Elimination Defecation Defecation: the act of expelling feces from the body Peristalsis: rhythmic contractions of intestinal smooth muscle to facilitate defecation Gastrocolic reflex:
Chapter 31 Bowel Elimination Defecation Defecation: the act of expelling feces from the body Peristalsis: rhythmic contractions of intestinal smooth muscle to facilitate defecation Gastrocolic reflex:
Pelvic Floor Disorders. Amir Darakhshan MD FRCS (Gen Surg) Consultant Colorectal and General Surgeon
 Consultant Colorectal and General Surgeon") Pelvic Floor Disorders Amir Darakhshan MD FRCS (Gen Surg) Consultant Colorectal and General Surgeon What is Pelvic Floor Disorder Surgical perspective symptoms of RED, FI or prolapse on the background
Pelvic Floor Disorders Amir Darakhshan MD FRCS (Gen Surg) Consultant Colorectal and General Surgeon What is Pelvic Floor Disorder Surgical perspective symptoms of RED, FI or prolapse on the background
Continence Promotion in
 Everybody s Business- Continence Promotion in Aged Care Melissa O Grady Clinical Nurse Consultant Continence Warning Some graphic images are contained in this presentation Objectives What is Old Age? What
Everybody s Business- Continence Promotion in Aged Care Melissa O Grady Clinical Nurse Consultant Continence Warning Some graphic images are contained in this presentation Objectives What is Old Age? What
Pelvic Floor Therapy for the Oncology Patient
 Therapy for the Oncology Patient CARINA SIRACUSA, PT, DPT, WCS OHIOHEALTH PELVIC FLOOR PHYSICAL THERAPIST ONCOLOGY REHABILITATION PROGRAM COORDINATOR What does a pelvic floor therapist treat? Muscles Muscles
Therapy for the Oncology Patient CARINA SIRACUSA, PT, DPT, WCS OHIOHEALTH PELVIC FLOOR PHYSICAL THERAPIST ONCOLOGY REHABILITATION PROGRAM COORDINATOR What does a pelvic floor therapist treat? Muscles Muscles
Management Of Rectal Bleeding In The Community: How A Shared Care Approach Can Benefit Dr. Daniel Lee
 Management Of Rectal Bleeding In The Community: How A Shared Care Approach Can Benefit Dr. Daniel Lee MD, MMed (S'pore), FRCS (Edin) Associate Consultant Department of Surgery 9 January 2016 Incidence
Management Of Rectal Bleeding In The Community: How A Shared Care Approach Can Benefit Dr. Daniel Lee MD, MMed (S'pore), FRCS (Edin) Associate Consultant Department of Surgery 9 January 2016 Incidence
An effective and minimally invasive bridge between conservative therapy and invasive surgery for BCD (bowel control disorder).
.") An effective and minimally invasive bridge between conservative therapy and invasive surgery for BCD (bowel control disorder). Mederi Therapeutics has developed this kit to help you raise awareness of
An effective and minimally invasive bridge between conservative therapy and invasive surgery for BCD (bowel control disorder). Mederi Therapeutics has developed this kit to help you raise awareness of
Stop Coping. Start Living. Talk to your doctor about pelvic organ prolapse and sacrocolpopexy
 Stop Coping. Start Living Talk to your doctor about pelvic organ prolapse and sacrocolpopexy Did you know? One in three women will suffer from a pelvic health condition in her lifetime. Four of the most
Stop Coping. Start Living Talk to your doctor about pelvic organ prolapse and sacrocolpopexy Did you know? One in three women will suffer from a pelvic health condition in her lifetime. Four of the most
Recent trends in management of haemorrhoids
 International Surgery Journal Ali SA et al. Int Surg J. 2017 Apr;4(4):1276-1280 http://www.ijsurgery.com pissn 2349-3305 eissn 2349-2902 Original Research Article DOI: http://dx.doi.org/10.18203/2349-2902.isj20171127
International Surgery Journal Ali SA et al. Int Surg J. 2017 Apr;4(4):1276-1280 http://www.ijsurgery.com pissn 2349-3305 eissn 2349-2902 Original Research Article DOI: http://dx.doi.org/10.18203/2349-2902.isj20171127
Department of General Surgery. Anus Benign. Lucy Yang PGY 2 Dr. Nawar Alkhamesi October 5, 2016
 Department of General Surgery Lucy Yang PGY 2 Dr. Nawar Alkhamesi October 5, 2016 Objectives Medical Expert: 1. Anal canal anatomy, histology, innervation and pelvic floor association 2. Etiology and management
Department of General Surgery Lucy Yang PGY 2 Dr. Nawar Alkhamesi October 5, 2016 Objectives Medical Expert: 1. Anal canal anatomy, histology, innervation and pelvic floor association 2. Etiology and management
INFORMED CONSENT FOR ANORECTAL PROCEDURES
 516-248-2422 www.crssny.com Locations in Nassau, Suffolk and Queens INFORMED CONSENT FOR ANORECTAL PROCEDURES You may undergo anoscopy or proctosigmoidoscopy as part of your rectal examination. These tests
516-248-2422 www.crssny.com Locations in Nassau, Suffolk and Queens INFORMED CONSENT FOR ANORECTAL PROCEDURES You may undergo anoscopy or proctosigmoidoscopy as part of your rectal examination. These tests
THE PELVIC FLOOR, EPISIOTOMY AND PERINEAL REPAIR AND VAGINAL/RECTAL MEDICATIONS
 THE PELVIC FLOOR, EPISIOTOMY AND PERINEAL REPAIR AND VAGINAL/RECTAL MEDICATIONS MID2010 LEARNING OBJECTIVE 1 - REVIEW THE ANATOMY OF THE PELVIC FLOOR Superficial layers cavernosus Deep layer Coccygeus
THE PELVIC FLOOR, EPISIOTOMY AND PERINEAL REPAIR AND VAGINAL/RECTAL MEDICATIONS MID2010 LEARNING OBJECTIVE 1 - REVIEW THE ANATOMY OF THE PELVIC FLOOR Superficial layers cavernosus Deep layer Coccygeus
Comparison of Electrotherapy, Rubber Band Ligation and Hemorrhoidectomy in the Treatment of Hemorrhoids: A Clinical and Manometric Study
 Original Article 9 Comparison of Electrotherapy, Rubber Band Ligation and Hemorrhoidectomy in the Treatment of Hemorrhoids: A Clinical and Manometric Study A Izadpanah 1*, SV Hosseini 2, M Mahjoob 1 1.
Original Article 9 Comparison of Electrotherapy, Rubber Band Ligation and Hemorrhoidectomy in the Treatment of Hemorrhoids: A Clinical and Manometric Study A Izadpanah 1*, SV Hosseini 2, M Mahjoob 1 1.
Bowel dysfunctions following hysterectomy
 Bowel dysfunctions following hysterectomy Marco Scaglia Retrospective studies Retrospective studies 6% of patients developed new symptoms (Carlson 1994) Constipation is more common in women after hysterectomy
Bowel dysfunctions following hysterectomy Marco Scaglia Retrospective studies Retrospective studies 6% of patients developed new symptoms (Carlson 1994) Constipation is more common in women after hysterectomy
Human Anatomy rectum
 rectum The colon is also called the large intestine. The ileum (last part of the small intestine) connects to the cecum (first part of the colon) in the lower right abdomen. The rest of the colon is divided
rectum The colon is also called the large intestine. The ileum (last part of the small intestine) connects to the cecum (first part of the colon) in the lower right abdomen. The rest of the colon is divided
5/29/2015. Objectives. Functions of the PFM. Various phases of PFM. Evaluation of the PFM
 The Physical Therapist s Approach to the Female Pelvic Floor Musculature Examination and Treatment. Presented By: Evelyne Burtis, DPT Objectives Core and pelvic floor muscles (PFM) Functions of the PFM
The Physical Therapist s Approach to the Female Pelvic Floor Musculature Examination and Treatment. Presented By: Evelyne Burtis, DPT Objectives Core and pelvic floor muscles (PFM) Functions of the PFM
Chapter 34. Nursing Care of Patients with Lower Gastrointestinal Disorders
 Chapter 34 Nursing Care of Patients with Lower Gastrointestinal Disorders Lower Gastrointestinal System Small Intestines Large Intestines Rectum Anus Constipation Fecal Mass Held In Rectum Feces Become
Chapter 34 Nursing Care of Patients with Lower Gastrointestinal Disorders Lower Gastrointestinal System Small Intestines Large Intestines Rectum Anus Constipation Fecal Mass Held In Rectum Feces Become
Motility Disorders. Pelvic Floor. Colorectal Center for Functional Bowel Disorders (N = 701) January 2010 November 2011
 January 2010 November 2011") Motility Disorders Pelvic Floor Colorectal Center for Functional Bowel Disorders (N = 71) January 21 November 211 New Patients 35 3 25 2 15 1 5 Constipation Fecal Incontinence Rectal Prolapse Digestive-Genital
Motility Disorders Pelvic Floor Colorectal Center for Functional Bowel Disorders (N = 71) January 21 November 211 New Patients 35 3 25 2 15 1 5 Constipation Fecal Incontinence Rectal Prolapse Digestive-Genital
Long-Term Bowel Symptoms Following Corrective Surgery
 HIRSCHSPRUNG'S DISEASE Samuel Nurko MD MPH Center for Motility and Functional Gastrointestinal Disorders Children s Hospital Medical Center, Boston Ma Long-Term Bowel Symptoms Following Corrective Surgery
HIRSCHSPRUNG'S DISEASE Samuel Nurko MD MPH Center for Motility and Functional Gastrointestinal Disorders Children s Hospital Medical Center, Boston Ma Long-Term Bowel Symptoms Following Corrective Surgery
Today s Date: Pt Initials: PATIENT INFORMATION. First Name: Last Name: Middle Name: Date of Birth: Social Security #: Preferred Language:
 PATIENT INFORMATION First Name: Last Name: Middle Name: Suffix: Nickname: Male Female Date of Birth: Social Security #: Preferred Language: Race: Asian Native Hawaiian Other Pacific Islander Black / African
PATIENT INFORMATION First Name: Last Name: Middle Name: Suffix: Nickname: Male Female Date of Birth: Social Security #: Preferred Language: Race: Asian Native Hawaiian Other Pacific Islander Black / African
Constipation An Overview. Definition Physiology of GI tract Etiology Assessment Treatment
 CONSTIPATION Constipation An Overview Definition Physiology of GI tract Etiology Assessment Treatment Definition Constipation = the infrequent passage of hard feces Definition of Infrequent The meaning
CONSTIPATION Constipation An Overview Definition Physiology of GI tract Etiology Assessment Treatment Definition Constipation = the infrequent passage of hard feces Definition of Infrequent The meaning
PREPARING FOR ANORECTOAL MANOMETRY. ManoScan Anorectal Manometry System
 PREPARING FOR ANORECTOAL MANOMETRY ManoScan Anorectal Manometry System WHAT IS ANORECTAL MANOMETRY? Anorectal manometry is a test used to evaluate the function and coordination of the sphincter and pelvic
PREPARING FOR ANORECTOAL MANOMETRY ManoScan Anorectal Manometry System WHAT IS ANORECTAL MANOMETRY? Anorectal manometry is a test used to evaluate the function and coordination of the sphincter and pelvic
, may spread caudally to present as a perianal abscess, laterally across the external sphincter to form an ischiorectal abscess or, rarely,
 ANORECTAL ABSCESSES , may spread caudally to present as a perianal abscess, laterally across the external sphincter to form an ischiorectal abscess or, rarely, superiorly above the anorectal junction
ANORECTAL ABSCESSES , may spread caudally to present as a perianal abscess, laterally across the external sphincter to form an ischiorectal abscess or, rarely, superiorly above the anorectal junction
Surgical Management of IBD in the Age of Biologics
 Surgical Management of IBD in the Age of Biologics Lisa S. Poritz, M.D Associate Professor of Surgery Division of Colon and Rectal Surgery Objectives Discuss surgical management of IBD When to operate
Surgical Management of IBD in the Age of Biologics Lisa S. Poritz, M.D Associate Professor of Surgery Division of Colon and Rectal Surgery Objectives Discuss surgical management of IBD When to operate
Colorectal Surgery. Patient Care. Goals and Objectives
 Colorectal Surgery Patient Care 1) Interpret the results of clinical evaluations (history, physical examination) performed on patients with a) Hemorrhoids b) Perianal abscess/fistula c) Anal fissure d)
Colorectal Surgery Patient Care 1) Interpret the results of clinical evaluations (history, physical examination) performed on patients with a) Hemorrhoids b) Perianal abscess/fistula c) Anal fissure d)
Robotic Ventral Rectopexy
 Robotic Ventral Rectopexy What is a robotic ventral rectopexy? The term rectopexy refers to an operation in which the rectum (the part of the bowel nearest the anus) is put back into its normal position
Robotic Ventral Rectopexy What is a robotic ventral rectopexy? The term rectopexy refers to an operation in which the rectum (the part of the bowel nearest the anus) is put back into its normal position
DIAPPERS: Transient Causes of Urinary Incontinence and other contributing factors
 DIAPPERS: Transient Causes of Urinary Incontinence and other contributing factors D Delirium Acute confusion alters one s ability to anticipate and meet own needs. Delirium may occur from drugs, surgery,
DIAPPERS: Transient Causes of Urinary Incontinence and other contributing factors D Delirium Acute confusion alters one s ability to anticipate and meet own needs. Delirium may occur from drugs, surgery,
Saratoga Schenectady Endoscopy Center, LLC Burnt Hills, N.Y Hemorrhoids. National Digestive Diseases Information Clearinghouse
 Hemorrhoids National Digestive Diseases Information Clearinghouse U.S. Department of Health and Human Services NATIONAL INSTITUTES OF HEALTH What are hemorrhoids? Hemorrhoids are swollen and inflamed veins
Hemorrhoids National Digestive Diseases Information Clearinghouse U.S. Department of Health and Human Services NATIONAL INSTITUTES OF HEALTH What are hemorrhoids? Hemorrhoids are swollen and inflamed veins
Incontinence Patient Information Form
 Incontinence Patient Information Form (To be completed by patient) Before talking with you, the doctor would like some information about your urine leakage. These questions are important for finding out
Incontinence Patient Information Form (To be completed by patient) Before talking with you, the doctor would like some information about your urine leakage. These questions are important for finding out
Hemorrhoids represent one of the most common
 THE JOURNAL OF FAMILY PRACTICE S U P P L E M E N T A new treatment option for grades III and IV hemorrhoids Glenn S. Parker, MD, FACS, FASCRS Chief, Division of Colon and Rectal Surgery, and Director,
THE JOURNAL OF FAMILY PRACTICE S U P P L E M E N T A new treatment option for grades III and IV hemorrhoids Glenn S. Parker, MD, FACS, FASCRS Chief, Division of Colon and Rectal Surgery, and Director,
Assessing rectal bleeding: A common symptom of haemorrhoids
 Assessing rectal bleeding: A common symptom of haemorrhoids Rectal bleeding is a red flag sign and one of the referral criteria for a 2-week wait to see a specialist. However, in most cases, it is commonly
Assessing rectal bleeding: A common symptom of haemorrhoids Rectal bleeding is a red flag sign and one of the referral criteria for a 2-week wait to see a specialist. However, in most cases, it is commonly
Hemorroids and pelvic venous congestion: venous embolization is it efficient and sufficient?
 Hemorroids and pelvic venous congestion: venous embolization is it efficient and sufficient? Milka GREINER MD American Hospital of Paris Hôpital Pitié-Salpêtrière Paris I do not have any potential conflict
Hemorroids and pelvic venous congestion: venous embolization is it efficient and sufficient? Milka GREINER MD American Hospital of Paris Hôpital Pitié-Salpêtrière Paris I do not have any potential conflict
DIAGNOSIS AND MANAGEMENT OF COMMON ANORECTAL DISORDERS. Lisa Coleman, DO, FASCRS, FACS Center for Colorectal Surgery TPMG Retreat 2017
 DIAGNOSIS AND MANAGEMENT OF COMMON ANORECTAL DISORDERS Lisa Coleman, DO, FASCRS, FACS Center for Colorectal Surgery TPMG Retreat 2017 The Heinous Anus Anal Abscess Anal Cancer Anal Fissure Anal Warts Cancer
DIAGNOSIS AND MANAGEMENT OF COMMON ANORECTAL DISORDERS Lisa Coleman, DO, FASCRS, FACS Center for Colorectal Surgery TPMG Retreat 2017 The Heinous Anus Anal Abscess Anal Cancer Anal Fissure Anal Warts Cancer
Instructions for Use
 CONTINENCE RESTORATION SYSTEM Instructions for Use Humanitarian Device Authorized by Federal (USA) Law for use in the treatment of fecal incontinence in patients who are not candidates for or have previously
CONTINENCE RESTORATION SYSTEM Instructions for Use Humanitarian Device Authorized by Federal (USA) Law for use in the treatment of fecal incontinence in patients who are not candidates for or have previously
ORIGINAL ARTICLE. a randomized study
 Int J Colorectal Dis (2004) 19:176 180 DOI 10.1007/s00384-003-0517-9 ORIGINAL ARTICLE Attila Bursics Krisztina Morvay Péter Kupcsulik Lajos Flautner Comparison of early and 1-year follow-up results of
Int J Colorectal Dis (2004) 19:176 180 DOI 10.1007/s00384-003-0517-9 ORIGINAL ARTICLE Attila Bursics Krisztina Morvay Péter Kupcsulik Lajos Flautner Comparison of early and 1-year follow-up results of
Women s and Men s Health Intake Form Comprehensive Physical Therapy Center
 Name: (Last, First) DOB: Date: Age: Referring Physician: Next Physician Appointment: Today s visit: What is the main reason you came to the office today? When did it start? What treatments have you had
Name: (Last, First) DOB: Date: Age: Referring Physician: Next Physician Appointment: Today s visit: What is the main reason you came to the office today? When did it start? What treatments have you had
"The Complete Guide to Hemorrhoids"
 Another ebookwholesaler Publication "The Complete Guide to Hemorrhoids" By Seymour Wells Understanding, Managing and Treating Hemorrhoids Proudly brought to you by WOW Enterprises Inc. Email Recommended
Another ebookwholesaler Publication "The Complete Guide to Hemorrhoids" By Seymour Wells Understanding, Managing and Treating Hemorrhoids Proudly brought to you by WOW Enterprises Inc. Email Recommended
Internationally Indexed Journal
 Internationally Indexed Journal Indexed in Chemical Abstract Services(USA),Index Coppernicus,Ulrichs Directory of Periodicals,Google scholar,cabi,doaj,psoar, EBSCO,SCOPUS, EMBASE etc. Rapid Publishing
Internationally Indexed Journal Indexed in Chemical Abstract Services(USA),Index Coppernicus,Ulrichs Directory of Periodicals,Google scholar,cabi,doaj,psoar, EBSCO,SCOPUS, EMBASE etc. Rapid Publishing
Perianal diseases. What causes pain in the bottom? What causes lumps around the bottom? What examination is likely?
 In association with: Primary Care Society for Gastroenterology INFORMATION ABOUT Perianal diseases www.corecharity.org.uk What are perianal diseases? What causes an itchy bottom? What causes pain in the
In association with: Primary Care Society for Gastroenterology INFORMATION ABOUT Perianal diseases www.corecharity.org.uk What are perianal diseases? What causes an itchy bottom? What causes pain in the
A Guide to Your Burning Questions
 The #1 Doctor Recommended Brand A Guide to Your Burning Questions Use products as directed. 2017 Pfizer Consumer Healthcare Put an End to Your Uncomfortable Questions We understand that talking about hemorrhoids
The #1 Doctor Recommended Brand A Guide to Your Burning Questions Use products as directed. 2017 Pfizer Consumer Healthcare Put an End to Your Uncomfortable Questions We understand that talking about hemorrhoids
Dr. Rick Shacket s Preferred Surgical Sites
 Dr. Rick Shacket s Preferred Surgical Sites Phoenix Baptist Hospital (PBH) 2000 W. Bethany Home Rd Phoenix, Arizona 85015 Phone (602) 249-0212 Laser Surgery Center (LSC) 10255 N. 32 nd Street Phoenix,
Dr. Rick Shacket s Preferred Surgical Sites Phoenix Baptist Hospital (PBH) 2000 W. Bethany Home Rd Phoenix, Arizona 85015 Phone (602) 249-0212 Laser Surgery Center (LSC) 10255 N. 32 nd Street Phoenix,