Drug Eluting Stents: The only SFA Advance with 5-year Outcomes
|
|
|
- Hilary Houston
- 6 years ago
- Views:
Transcription

 3.95 2.84 (1.00 10.00) 0.96 2.05 (-3.00 3.72) SMART without Abciximab 2.65 2.07 (0.50 7.03) 4.43 2.49 (0.50 10.00) 1.78 2.85 (-4.62 8.")
1 Drug Eluting Stents: The only SFA Advance with 5-year Outcomes Gary M. Ansel, MD System Medical Chief: Vascular OHioHealth/Riverside Methodist Hospital Columbus, Ohio Self-expanding Stents Pro Simple Safe Quick Randomized superiority data to PTA Stent fractures Con Cost Restenosis difficult to treat Inferior to DES in randomized trial data Stents Improve Ambulation: BLASTER 9 month Treadmill Results Measured in Time/minutes Parameter Baseline 9 Month Change SMART with Abciximab ( ) ( ) ( ) SMART without Abciximab ( ) ( ) ( ) All Patients ( ) ( ) ( ) Ansel et al;cath cardiovasc Interven
* Freedom from TLR* Clinical success Laird et al Circ Cardiovasc Interv. 2010 Jun 1;3(3):267-76 Laird et al. J Endovasc Ther.")
 Stent graft 50 Surgical bypass 50 Mean stent graft treatment length = 25.")
2 Randomized Stent Results: (Resilient: 12 and 36-Month(TLR) Results) 100% 80% 60% 40% 86% p=.91 86% 38% 80% 46% 87% PTA PTA+LifeStent 3-yr 75.5% vs. 41.8%, 34% 72% 20% p<.0001 p<.0001 p< % Freedom from MACE* Prim. Patency (duplex)* Freedom from TLR* Clinical success Laird et al Circ Cardiovasc Interv Jun 1;3(3): Laird et al. J Endovasc Ther Feb;19(1):1-9 Intimal vs subintimal stenting? Retrospective analysis of > 900 pts intraluminal subintimal Patency primary 3 year 55% 53% Patency secondary 3 year 80% 85% Soga et. al. J Vasc Surg 2013:58; Stent Grafts: Randomized Comparison to Surgical Prosthetic Bypass N = 86 pts (100 limbs) Stent graft 50 Surgical bypass 50 Mean stent graft treatment length = 25.6 cm SG Bypass 1-year patency Primary 73.5% 74.2% Secondary 83.9% 83.7% 2-year patency Primary 62% 65% Secondary 73% 75% Kedora et al J Vasc Surg 2007;45:10-16 McQuade et al. J Vasc Surg Jan;49(1):
 0.87 Mean (Std Dev) 19 (8) 18 (7) Median (Range) 20 (8 40) 16 (8 36) LESION CALCIFICATION 0.01 None Mild 37.5% 57.9% Moderate Severe 62.5% 42.")
 3 year Data 100% * Percentage of Patients (%) 80% 60% 40% 20% * 0% Primary Primary Secondary Freedom Primary Primary Secondary Freedom Patency Assisted Patency from")
3 Error bars = 95% confidence interval VIBRANT 1-YR Interim Results: Lesion Characteristics: Diffuse and complex LESION CHARACTERISTICS GORE VIABAHN Endoprosthesis Bare Nitinol Stent p-value TREATED OCCLUSIONS 59.7% 56.6% 0.74 TARGET LESION LENGTH (cm) 0.87 Mean (Std Dev) 19 (8) 18 (7) Median (Range) 20 (8 40) 16 (8 36) LESION CALCIFICATION 0.01 None Mild 37.5% 57.9% Moderate Severe 62.5% 42.1% TIBIAL RUNOFF Vessel 15.3% 22.4% 2 Vessel 50.0% 32.9% 3 Vessel 34.7% 44.7% Geraghty et al. J Vasc Surg May 13 VIBRANT (SG vs PMS) 3 year Data 100% * Percentage of Patients (%) 80% 60% 40% 20% * 0% Primary Primary Secondary Freedom Primary Primary Secondary Freedom Patency Assisted Patency from TLR Patency Assisted Patency from TLR Patency Patency GORE VIABAHN Endoprosthesis Bare Nitinol Stent End of 12 month F/U Window * p < 0.05 End of 36 month F/U Window Comment on cross-over: Sixteen Bare Nitinol Stent patients received the VIABAHN Endoprosthesis during subsequent reinterventions, which complicates secondary endpoint comparisons. Geraghty et al. J Vasc Surg May 13 Future Stent Designs 3
: One-Year Patency 92% 87% 74% 12 month duplex follow-up available for 103 /")
4 SUPERB TRIAL Freedom from Loss of Primary Patency at 1 Year (PSVR < 2.0) 98.4% 6 month patency N = 264 Mean lesion 8cm 86.1% primary patency Freedom from TLR = 90% TCT 2012 Survival Analysis conducted by HCRI VIPER Registry (Heparin/Contoured): One-Year Patency 92% 87% 74% 12 month duplex follow-up available for 103 / 120 patients Saxon et al. J Vasc Interv Radiol Feb;24(2): VIASTAR:Primary Patency VIPER: Effects of Device Sizing: Proximal Per Protocol Analysis, End-of-window patency 78% 78% 91% 73% p < % 53.5% 70% p = % VIABAHN, n = 66 BMS, n = 63 VIABAHN, n = 37 BMS, n = 23 p < 0.05 All Lesions n= 38 n= 57 Lesions 20 cm Now need longer term data Device oversizing assessed by independent Core Lab, data on file 4


5 Drug Coated Balloons Fempop: DCB vs PTA Levant 2 Fempop:InPactTrial DCB vs PTA Inpact 1 year 5



6 Fempop: DCB vs PTA InPact Trial: 1 year Polymer Based DES Results SIROCCO STRIDES 68.5% Zilver PTX Study Design Primary Randomization Enrollment PTA Zilver PTX Provisional BMS Suboptimal PTA Optimal PTA Secondary Randomization Provisional Zilver PTX 6
 1 78 ± 17 80 ± 17 0.38 Total occlusions 27% 33% 0.20 De novo lesions 94% 95% 0.")

7 Baseline Lesion Characteristics PTA Zilver PTX p-value Lesions Normal-to-normal lesion length (mm) 63 ± ± Stenosed lesion length (mm) 1,2 53 ± ± Diameter stenosis (%) 1 78 ± ± Total occlusions 27% 33% 0.20 De novo lesions 94% 95% 0.68 Lesion calcification 1 None 5% 2% 1 Angiographic core lab assessment 2 Region with > 20% diameter stenosis * Statistically significant Little 38% 26% Moderate 22% 35% Severe 35% 37% < 0.01* 5-year Stent Integrity Study Period Number of New Events Fracture Rate 1 Enrollment 0 0.0% 1-year 4 0.9% 3-year 3 1.9% 5-year 0 1.9% 1 Kaplan-Meier estimates Zilver PTX has excellent durability in challenging SFA environment 3-Year Freedom from TLR Zilver PTX vs. Standard Care 83.7% 70.2% Zilver PTX 240 patients Optimal PTA + Bare Zilver 139 patients p < 0.01 log-rank 3-year TLR Group Rate Reduction Zilver PTX 16.3% Optimal PTA % 45% Provisional Bare Zilver 7
8 5-year Freedom from TLR Zilver PTX vs. Standard Care 83.1% Zilver PTX p < 0.01 log-rank 67.6% Optimal PTA + BMS Years (PATIENTS) At Risk Zilver PTX Failed At Risk Standard Care Failed At 5 years, Zilver PTX demonstrates a 48% reduction in reintervention compared to standard care 5-year Primary Patency (PSVR < 2.0) Zilver PTX vs. Standard Care 66.4% Zilver PTX 43.4% Optimal PTA + BMS p < 0.01 log-rank Years (LESIONS) Zilver PTX Standard Care At Risk Failed At Risk Failed At 5 years, Zilver PTX demonstrates a 41% reduction in restenosis compared to standard care 5-year Primary Patency (PSVR < 2.0) Zilver PTX vs. Standard Care 66.4% Zilver PTX 43.4% Optimal PTA + BMS From 1-5 years, the relative separation increases by 35% 8
 0 1 2 3 4 5 At Risk 301 247 206 179 158 129 Zilver PTX Failed 0 38 52 56 57 57 At Risk 170 109 94 76 67 60 Standard Care Failed 0 48 56 61 64 64 At 5 years,")
9 5-year Clinical Benefit Index Zilver PTX vs. Standard Care 79.8% Zilver PTX p < 0.01 log-rank 59.3% Optimal PTA + BMS Years (PATIENTS) At Risk Zilver PTX Failed At Risk Standard Care Failed At 5 years, Zilver PTX has a superior rate of freedom from persistent or worsening claudication, rest pain, ulcer, or tissue loss 5-year Freedom from TLR Provisional Zilver PTX vs. BMS Provisional 84.9% Zilver PTX p = 0.06 log-rank 71.6% Provisional BMS Years (PATIENTS) Provisional Zilver PTX Provisional BMS At Risk Failed At Risk Failed At 5 years, Zilver PTX demonstrates a 47% reduction in reintervention compared to BMS 5-year Primary Patency (PSVR < 2.0) Provisional Zilver PTX vs. BMS Provisional 72.4% Zilver PTX p = 0.03 log-rank 53.0% Provisional BMS Years (LESIONS) Provisional Zilver PTX Provisional BMS At Risk Failed At Risk Failed At 5 years, Zilver PTX demonstrates a 41% reduction in restenosis compared to BMS 9
10 5-year Clinical Benefit Index Provisional xzilver PTX vs. BMS 81.8% Provisional Zilver PTX p = 0.02 log-rank 63.8% Provisional BMS Years (PATIENTS) Provisional Zilver PTX Provisional BMS At Risk Failed At Risk Failed At 5 years, Zilver PTX has a superior rate of freedom from persistent or worsening claudication, rest pain, ulcer, or tissue loss Can Results be Generalized OUS Registry: Subgroups Freedom from TLR Subgroup 12 Months 24 Months Overall 89% (n = 818) 82% (n = 427) De novo (all) 91% 88% < 7 cm Lesions 94% 91% > 7 cm to 15 cm Lesions 92% 86% > 15 cm Lesions 84% 80% TASC C and D* 87% 78% Occlusions 86% 77% Stenosis 90% 85% Restenosis (all) 81% 70% Restenosis (not ISR) 87% 73% In-stent Restenosis (ISR) 78% 69% *TASC 2000 Conxclusions for 5-year Zilver PTX RCT As the first randomized controlled SFA device trial with 5-year follow-up, these results with the Zilver PTX stent provide important insights regarding long-term outcomes for endovascular treatment 5-year data for Zilver PTX versus standard care Greater than 40% reduction in reintervention and restenosis Superior clinical benefit These benefits increase with time results with Zilver PTX continue to diverge from standard care over 5 years with no late catch-up 5-year results confirm long-term superiority of Zilver PTX versus bare metal stents 10
11 1/19/2015 DCB: Should You Add Them to Your Arsenal? Mahmood Razavi, MD, FSIR, FSVM Director Center for Clinical Trials Heart & Vascular Center Vasc & Interv Specialists of Orange Disclosures (2014/15) Advisor/consultant 480 Biomedical Abbott Vascular Bard Peripheral Vasc Boston Scientific Cagent Vasc Codman/ J&J Covidien Microvention/Terumo Reflow Trivascular Veniti Yawa Med Training/speaking/hon. Penumbra Covidien Gore Stocks 480 Biomedical Embo Medical Embomedics Neuravi Reflow Medical Trivascular Yawa Med Current Endo-Technologies Are Suboptimal Limitations of traditional endovascular technologies (POBA, BMS, & simple debulking) are well known & mechanisms of failure are better understood Need to move beyond simple mechanical approaches Do DCBs offer any advantage? How should they optimally be used? 1
12 1/19/2015 Current Solutions: Drug-Device Combinations Drug-eluting stents (DES) Drug-coated balloons (DCB) Adjunctive adventitial drug delivery Bioabsorbable drug eluting scaffolds (BVS) Debulking + drug delivery Drug-Coated Balloons Do DCBs offer any advantage over the traditional approaches? How should they optimally be used? DCB: Advantages Short learning curve Issues: Pre-dilation & geographic miss No implants No stent fx issues No stimulus for chronic inflammation (COF) Potentially more options for re-treatment?? May reduce need for long term antiplatelet tx May be a better option for no stent zones 2
 Drug: Paclitaxel 2 μg/mm 2 1 μ thick uniform non-flaking coating Balloon inflation")


 and CD-TLR Primary Safety Endpoint: Composite of 30-day all cause POD and 1- yr freedom")
13 1/19/2015 Lutonix Peripheral DCB (Lutonix/ C.R. Bard Inc) Drug: Paclitaxel 2 μg/mm 2 1 μ thick uniform non-flaking coating Balloon inflation transfers the drug to the endoluminal surface of the vessel PTX diffuses into the vessel wall Drug LEVANT-2 Trial Global prospective, multicenter, single blind, randomized study of Lutonix DCB vs PTA (2:1 randomization) Duplex & angiographic core labs with CEC & independent DSMB 543 subjects enrolled at 54 US & EU sites LEVANT-2 Trial Design Primary Efficacy Endpoint: Primary patency through 12 months defined as absence of binary restenosis (PSVR 2.5) and CD-TLR Primary Safety Endpoint: Composite of 30-day all cause POD and 1- yr freedom from index limb amputation, re-intervention, and limb-related death 3
14 1/19/2015 Efficacy Endpoint of Primary Patency Levant-2 Achieved Primary Patency CO 80 = 12.6% p=0.015 Percent (%) n= Lutonix DCB N=264 n= Standard PTA N=135 CO-6 Primary Primary Patency Patency (Kaplan-Meier) % Free from Primary Patency Event Lutonix DCB (N) 291 Standard PTA (N) Months from Randomization Date DCB PTA p<0.001 Primary Efficacy Endpoint Through 24-Months Primary Efficacy (Preliminary Through Data) 24-Months CO-18 % Free from Primary Patency Event Lutonix DCB (N) 291 Standard PTA (N) 146 Survival % Time Lutonix DCB Standard PTA p-value 730 days 53.7% 48.4% DCB PTA p= Months from Randomization Date
 Index Limb Related death at 12 months 0.0% (0/285) 0.0% (0/140) Amputation at 12 months 0.3% (1/286) 0.0% (0/140) AV fistula surgery at 12 months 0.4% (1/285) 0.")
 Index limb interventions in non-target vessels at 12 months 2.1% (6/285) 2.9% (4/140) IN.PACT DCB Balloon (Medtronic Inc.")
, single blinded, randomized study of IN.")
15 1/19/2015 CO-23 Primary Safety Primary Events Safety Events Safety Event (Patients may have > 1 event) Lutonix DCB %(n/n) Standard PTA %(n/n) Perioperative ( 30) death 0.0% (0/308) 0.0% (0/155) Index Limb Related death at 12 months 0.0% (0/285) 0.0% (0/140) Amputation at 12 months 0.3% (1/286) 0.0% (0/140) AV fistula surgery at 12 months 0.4% (1/285) 0.0% (0/140) Surgical bypass at 12 months 0.7% (2/285) 0.7% (1/140) Total TLR at 12 months 12.3% (35/285) 16.8% (24/143) Non-TLR TVR at 12 months 1.1% (3/285) 1.4% (2/143) Index limb interventions in non-target vessels at 12 months 2.1% (6/285) 2.9% (4/140) IN.PACT DCB Balloon (Medtronic Inc.) Drug: Paclitaxel Excipient: Urea Urea hydrates upon contact with blood & drug released Paclitaxel binds to the vessel wall Paclitaxel penetrates into media & adventitia Can remain there for over 180 days at therapeutic levels IN.PACT SFA Trial Prospective, multicenter (EU & US), single blinded, randomized study of IN.PACT DCB vs PTA (2:1) Blinded Duplex & angiographic core labs with CEC Independent DSMB Primary endpoints at 12 months with 5-yr follow up 5
16 1/19/2015 Trial Design Screen Failure (treat per std practice) Trial design RC [1] Clinical and Anatomic Inclusion / Exclusion Criteria SUCCESSFUL PRE-DILATATION [2] Pre-screening Screening NO 331 Randomization Randomized 2:1 IN.PACT (220) PTA (111) Provisional Stenting? NO Secondary Analysis (331 ITT ALL Subjects) Primary Analysis (301 ITT NON-Stented Subjects) Laird J. TCT With symptoms of claudication and/or rest pain and angiographic evidence of SFA/PPA stenosis Trial Design Primary Efficacy Endpoint: Primary patency through 12-months, defined as freedom from clinically-driven TLR and Duplex restenosis (PSVR 2.4) Primary Safety Endpoint: Procedure related 30-d and freedom from clinically driven TVR & major amputation of index limb through 12-months Baseline Clinical Characteristics Charecteristics IN.PACT DCB PTA p N Age (Y) 67.5 ± ± Male Gender (%) 65.0% (143/220) 67.6% (75/111) Diabetes (%) 40.5% (89/220) 48.6% (54/111) Hypertension (%) 91.4% (201/220) 88.3% (98/111) Hyperlipidemia (%) 84.5% (186/220) 82.0% (91/111) Current Smoker (%) 38.6% (85/220) 36.0% (40/111) Coronary Artery Disease (%) 57.0% (122/214) 55.0% (60/109) Carotid Artery Disease (%) 34.9% (73/209) 31.7% (32/101) Laird J. TCT 2014 Rutherford Stage (%) ABI / TBI [1] ± ± % (83/220) 57.3% (126/220) 5.0% (11/220) 0.0% (0/220) All ITT subjects (stented and non-stented) 37.8% (42/111) 55.9% (62/111) 5.4% (6/111) 0.9% (1/111)
![1/19/2015 Baseline Angiographic Characteristics Lesion Type [1] De novo Restenotic IN.PACT DCB PTA p (N=220 Subjects, N=221 Lesions) 95.0% (209/220) 5.](/docs-images/78/77662511/images/17-0.jpg "0% (11/220) All ITT subjects (stented and non-stented) (N=111 Subjects, N=113 Lesions) 94.6% (105/111) 5.4% (6/111) # Patent Runoff Vessels 0 3.3% (7/212) 4.5% (5/112) 1 13.7% (29/212) 26.")
17 1/19/2015 Baseline Angiographic Characteristics Lesion Type [1] De novo Restenotic IN.PACT DCB PTA p (N=220 Subjects, N=221 Lesions) 95.0% (209/220) 5.0% (11/220) All ITT subjects (stented and non-stented) (N=111 Subjects, N=113 Lesions) 94.6% (105/111) 5.4% (6/111) # Patent Runoff Vessels 0 3.3% (7/212) 4.5% (5/112) % (29/212) 26.8% (30/112) % (88/212) 33.0% (37/112) % (88/212) 35.7% (40/112) Prox. Popliteal Involvement (%) 6.8% (15/221) 7.1% (8/113) Lesion Length (cm) [2] 8.94 ± ± Total Occlusions (%) 25.8% (57/221) 19.5% (22/113) Severe Calcification (%) 8.1% (18/221) 6.2% (7/113) RVD (mm) ± ± MLD pre (mm) ± ± Diameter Stenosis pre (%) 81.1 ± ± Laird J. TCT Months Results: IN.PACT SFA Randomized Controlled Trial Per Protocol, 12-month Outcomes 1. Primary patency is defined as freedom from clinically-driven TLR and freedom from restenosis as determined by duplex ultrasound (DUS) Peak Systolic Velocity Ratio (PSVR) Primary patency comparative statistics imputed missing data and non-stented ITT were adjusted for Propensity Score 3. Primary safety composite is defined as freedom from device and procedure-related 30-day death and freedom from target limb major amputation and clinically-driven TVR through 12 months 4. Non-inferiority margi 10% 5. Non-stented ITT cohort difference adjusted for (3) Propensity freedom Score 6. from p-value TVR, associated TLR with & sequential increase superiority in RB test 1 yr Laird J. TCT 2014 ALL ITT, 12-month Effectiveness Outcomes IN.PACT DCB PTA p PrimaryPate cy(psvr 2.4) 82.2% (157/191) 52.4% (54/103) <0.001 Clinically-driven TLR [1] 2.4% (5/207) 20.6% (22/107) <0.001 All TLR [2] 2.9% (6/207) 20.6% (22/107) <0.001 Primary Sustained Clinical Improv. [3] 85.2% (167/196) 68.9% (73/106) <0.001 ABI / TBI [4] ± ± ALL ITT, 12-month 12-Month Primary Patency Patency [1] (All Patients ITT Analysis) (p<0.001 by log-rank test) Laird J. TCT
 Laird J. TCT 2014 1.")

 SFA N=220 (DCB Arm) N=220 2.4% Global IN.PACT N=655 Global N=655 8.7% CD-TLR CD-TVR 2.4% 4.3% 8.7% 9.")
 Target Limb Major Amputation 0.0% (0) 0.3% (2) Ansel G. TCT 2014 IN.PACT SFA IN.PACT Global IN.PACT SFA IN.PACT Global Lesion Length 8.")
18 1/19/2015 ALL ITT, 12-month Clinically-driven TLR 12-Month Clinically Driven TLR (All Patients ITT Analysis) IN.PACT PTA p Clinically-driven TLR [1] 2.4% 20.6% <0.001 [2] (p<0.001 by log-rank test) Laird J. TCT Clinically-driven TLR defined as any re-intervention due to symptoms or drop of ABI/TBI of >20% or >0.15 compared to post-procedure ABI/TBI IN.PACT SFA IN.PACT Global and SFA and Registry IN.PACT Global IN.PACT (n=1483) Global 12-months Results Summary ~ 12-months 45% of data analyzed Results & adjudicated Summary by CEC IN.PACT SFA IN.PACT CD-TLR (DCB IN.PACT Arm) SFA N=220 (DCB Arm) N= % Global IN.PACT N=655 Global N= % CD-TLR CD-TVR 2.4% 4.3% 8.7% 9.5% CD-TVR Thrombosis 4.3% 1.4% 9.5% 3.8% Thrombosis Target Limb Major Amputation 1.4% 0.0% (0) 3.8% 0.3% (2) Target Limb Major Amputation 0.0% (0) 0.3% (2) Ansel G. TCT 2014 IN.PACT SFA IN.PACT Global IN.PACT SFA IN.PACT Global Lesion Length 8.9 cm 12.2 cm Lesion CTO Length 25.8% 8.9 cm 35.8% 12.2 cm ISR CTO 0.0% 25.8% 21.4% 35.8% Baseline RC ISR > 3 5% 0.0% 15% 21.4% Baseline RC > 3 5% 15% What about ISR? 8
19 1/19/2015 DCB in ISR Author/yr Therapy Number Lesion length (mm) 1-yr 1 patency 1-yr TLR Stabile/ 12 DCB ± 39 92% 8% Gandini/ 13 Laser + DCB ± % 17% Gandini/ 13 DCB ± 91 38% 50% Sixt/ 13 Excisional + DCB VanDenBerg ± 93 85% NR Laser+ DCB ± 92 79% 19% Liistro 14 DCB ± 86 80% 14% Patency appears better than PTA alone Applications of DCB De novo fempop lesions in sx pts In combination with debulking Outcome v. DES or BMS not well established ISR Failed/failing dialysis access BTK lesions (?) One failed trial, 2 nd enrolling, 3 rd will begin enrollment in 2016 Conclusion Answer: definitive YES! 9
20 1/20/2015 VuMedi Webinar - Current Advances in SFA Interventions Cases and Applications of Bare Metal Stents and Vascular Mimetic Implants: Growing Data & Equal Results January 20, 2015 Sahil A. Parikh, M.D. Assistant Professor of Medicine Director, Center for Research and Innovation Director, Experimental Interventional Cardiology Laboratory Director, Interventional Cardiology Fellowship Program Harrington Heart & Vascular Institute University Hospitals Case Medical Center Case Western Reserve University School of Medicine Cleveland, Ohio Disclosures Consulting/Speakers Bureau: Medtronic, Boston Scientific, Abbott Vascular, St. Jude Medical, Astra Zeneca, Edwards, Cordis, Janssen, CR Bard, Abiomed Research: Medtronic, Boston Scientific, IDEV Technologies/Abbott Vascular, Daiichi Sankyo, Lutonix/CR Bard, TriReme Medical I will be discussing off label applications of approved medical devices The Typical Claudicant 45 yo male with DM2, Dyslipidemia, HTN and Rutherford 2-3 symptoms for 3 months Works as a janitor in a large downtown office building unable to perform work Diminished pulses noted on physical examination in his podiatrist s office ABI: 0.6R and 0.8L Referred for evaluation 1




21 1/20/2015 Examination 150/70, 66, 16, 98% JVP 6, Carotids 2+, soft L bruit CTA &P RRR S4 S1 S2 and no murmur No abd bruit Fem: 2+, 2+ Pop: Tr, 1+ DP: Monophasic, Biphasic PT: Monophasic, Biphasic What next? Risk factors treated to target Supervised Exercise Therapy recommended Patient continues to be vocationally limited No improvement with Cilostazol ACC/AHA Guidelines for the Management of Patients with Peripheral Arterial Disease Hirsch AT, et al. J Am Coll Cardiol. 2006;47:e1-e192. 2

")

22 1/20/2015 Aortography Runoff Angiography Bilateral SFA disease with focal L SFA stenosis and CTO R SFA (~15cm) BTK: 2V runoff bilaterally Up and Over SFA Selective DSA of the R SFA 3


23 1/20/2015 Questions Treatment Options: 1. Fem-Pop bypass with autogenous vein 2. Fem-Pop bypass with eptfe 3. SFA CTO endovascular revascularization antegrade 4. SFA CTO endovascular revascularization retrograde 5. Stem Cell Therapy TASC II Lesion Descriptions and Recommended Therapy of Femoral Artery Stenosis/Occlusion Norgren L et al. JVS. 2007:S5A S67A Femoropopliteal Disease: Open vs Endovascular Approaches OPEN SURGICAL 40%-75% 5 year patency rate depending on conduit Limb salvage rates are 70% at 5 years 1%-3% mortality rate Torsion Extension / Contraction ENDOVASCULAR Excellent procedural success Reported patency varies widely 30% 85% at 1 year Very little comparative Flexion effectiveness data exist comparing different therapies including stents, drug coated balloons and drug eluting stents Compression 4


24 1/20/2015 ABOVE-knee femoral popliteal bypass 5-year patency Table PTA/stents 3. The 5-year patency of Femoral-popliteal 55-75% different types of conduits Surgical reconstruction Femoral-popliteal 65-80% Vein Femoral-tibial 74 76% 60-75% eptfe Graft 39 52% AbuRahma et al, 1999; Green et al, 2000; Johnson and Lee, 2000; Klinkert et al, 2003 SFA Stenting is Superior to PTA Alone 32% Crossover due to inadequate PTA result Schillinger et al., NEJM 2006 After Endovascular Intervention, SFA Patency Decreases with Lesion Length for PTA and Conventional Stenting Conventional PTA Nitinol Stents Slope of relationship between length and restenosis is steeper for PTA compared to stenting Gray B. CCI
 2.")
25 1/20/2015 A Risk Stratification Score Predicts Patency in TASC C/D Lesions Risk Factor Points Female 1 Diabetes 1 Dialysis 1 CLI 1 Lesion >150mm 2 Poor Runoff 1 Risk Score Category 0-2 Low 3-4 Moderate 5-7 High Soga, et al. JVS 2011 Question: CTO Crossing Technique Options: 1. Wire and Catheter Intraluminal (Antegrade or Retrograde) 2. Wire and Catheter Subintimal (Antegrade or Retrograde) 3. CTO Crossing Device CTO Crossing 6


26 Angio image courtesy of Dr. Hans Biemans, Rivas Hospital Gorinchem, the Netherlands. 1. Scheinert, et al., Real world perspectives of treating complex SFA-Pop lesions, Results from the SUPERA-500 Registry, LINC Characteristically round lumens supported by Arena, F.J., Arena, F.A. Intravascular Ultrasound Evaluation of Interwoven Nitinol Stents at Implant. J Vasc Med Surg. 2013:1;116. Data on file at Abbott Vascular. 1/20/2015 Question: SFA Treatment Choices PTA alone Nitinol Stent Conventional Nitinol Stent Vascular Mimetic Implant Drug Eluting Stent Drug Coated Balloon Stent Graft Atherectomy Alone Orbital vs Directional vs Aspiration vs Laser Atherectomy + Stent Drug Coated Balloon + Stent The Supera Vascular Mimetic Implant (VMI) Provides Flexibility, Radial Strength and Kink Resistance The Supera implant mimics the natural structure and movement of the anatomy An interwoven nitinol design creates an implant that supports rather than resists the vessel Resists kinking and fracture with minimal chronic outward force Maintains a round, open lumen for normal, healthy blood flow in challenging anatomy 2 7
 experienced a Type III fracture at 24 months. The patient had a revascularization with directional atherectomy for in-stent restenosis at 9 months post index procedure.")

27 Source: Supera Peripheral Stent System Instructions for Use. 1. PSVR < Garcia, L., SUPERB Pivotal IDE Trial, 12-Month Results, TCT 2012 for Ankle-Brachial Index improvements. 3. One patient (1/200, 0.5%) experienced a Type III fracture at 24 months. The patient had a revascularization with directional atherectomy for in-stent restenosis at 9 months post index procedure. At 12-month follow up there was no evidence of a stent fracture. Additional in-stent restenoses were treated twice more with directional atherectomy between the 12- and 24-month evaluations. At 24 months, a type III fracture was noted in x- ray in the region of the earlier restenoses. There was no report of a major adverse event at 24 months. 1/20/2015 Vascular Mimetic Implants have Superior Kink Resistance Compared to Nitinol Stents Standard Nitinol Stents Supera implant AP View Lateral View Courtesy Abbott Vascular. SUPERB Trial SFA and proximal popliteal trial including complex patients Study Overview: 264 subjects (ITT), 34 sites Prospective, multi-center, un-blinded, single-arm versus PTA performance goal Stenotic, restenotic (non-stented) or occluded lesions Core laboratory used Primary safety endpoint: 99.2% free from composite death, TLR and amputation at 37 days Primary effectiveness endpoint (VIVA): 78.9% primary patency at 12 months 3 Patency (K-M): 86.3% primary patency at 12 months % severe/moderate calcification 1 78 mm mean lesion length 2 86% mid/distal SFA 1 Source: Supera Peripheral Stent System Instructions for Use. Data on file at Abbott Vascular. 1. Percent of lesions , Core Lab assessed. 3. Defined as freedom from >50% restenosis (Peak Systolic Velocity (PSV) ratio 2.0 as measured by duplex ultrasound) and no TLR.) SUPERB Results Safety and efficacy demonstrated with the Supera implant 1-year Results: Primary Patency (K-M) of 86.3% 1 Zero fractures 86.3% Significant improvement in ABI at 12 months versus baseline 2 and 89% of patients have improved more than 1 Rutherford- Becker clinical category at 12 months 2-year Results: 84% Freedom from TLR 0.5% fracture 3 8
 Courtesy: Lawrence Garcia, MD, VIVA 2014 Supera Patency Rates DO NOT Appear to Decrease with Lesion Length 100% Percent Percent of Lesions of without Lesions Restenosis without by")
28 Freedom From TLR 1/20/2015 Freedom From Clinically Driven TLR Through 3 Years 100% 80% 60% 40% 12 Months 89% 24 Months 84% Δ 3 years 7% 36 Months 82% 20% 0% Time Post Index Procedure (Days) Courtesy: Lawrence Garcia, MD, VIVA 2014 Supera Patency Rates DO NOT Appear to Decrease with Lesion Length 100% Percent Percent of Lesions of without Lesions Restenosis without by Lesion Restenosis Length (12 months SUPERB IDE Trial) by Lesion Length (12 months SUPERB TRIAL) 88% 88% 85% 50% 0% Shortest Lesions Middle Lesions Longest Lesions Shortest (35.4 ±12.3 Lesionsmm) Middle (73.5 Lesions ±10.8 (73.5±10.8cm) mm) (126.1 Longest ±33.4 Lesions mm) (35.4±12.3cm) (126.1±33.4cm) n=87 n=88 n=87 Courtesy: Lawrence Garcia, MD, VIVA 2014 SUPERB: Freedom From TLR Across Lesion Lengths is Fairly Constant 12 Months 24 Months 36 Months 100% % % 70% 60% 50% 40% 30% 20% 10% 0% Shortest Lesions Middle Lesions Longest Lesions Mean Lesion Length 35.4 mm 73.5mm mm Min, Max Lesion Length 8.5, 55.0 mm 55.5, 91.5 mm 96.1, mm Courtesy: Lawrence Garcia, MD, VIVA
 100% 94.5 91.6 90% 87.")
29 1/20/2015 SFA Patency Decreases with Lesion Length for PTA and Conventional Stenting but less so for Vascular Mimetic Implants Conventional PTA Nitinol Stents VMI/Supera Adapted from: Gray B. CCI SUPERB: Outcomes in Severe Calcification Freedom From TLR (K-M) 100% % % 70% 60% 50% 40% 30% 20% 10% 0% 12 Months 24 Months 36 Months Superb Severe Calcification Subset Severe calcification 45% Patency (VIVA 1 year) 89% Severe Ca++ defined as1cm both sides vessel Courtesy: Lawrence Garcia, MD, VIVA 2014 SUPERB: Deployment Technique Impact on Freedom From TLR is Significant 100% 80% Months 24 Months 36 Months % 63 40% 42 20% 0% Moderate Compression Minimal Compression Nominal Minimal Elongation Moderate Elongation Severe Elongation (21-40%) (11-20%) (±10%) (11-20%) (21-40%) (>40%) Courtesy: Lawrence Garcia, MD, VIVA

30 1/20/2015 SUPERB: Essentially ZERO Stent Fracture Stent Fracture 12 Months 0.0% (0/236) 24 Months 0.5% (1/196) 36 Months 0.6% (1/162) Single Strut 0.0% 0.0% 0.0% Multiple Strut 0.0% 0.0% 0.0% Complete Fracture/Fragments 0.0% 0.5%* 0.6%* Aligned Complete Fracture/Fragments 0.0% 0.0% 0.0% Malaligned Spiral Fracture 0.0% 0.0% 0.0% * One subject experienced a Type III fracture at 24 months after 3 directional atherectomy procedures to treat in-stent restenosis. Courtesy: Lawrence Garcia, MD, VIVA 2014 In.Pact SFA Tepe, et al. Charing Cross 2014 DCB in SFA A New Therapy IN.PACT PTA p Paclitaxel DCB vs PTA Primary Patency (PSVR 2.4) 82.2% (157/191) 52.4% (54/103) <0.001 Clinically-driven TLR [1] 2.4% (5/207) 20.6% (22/107) <0.001 All TLR [2] 2.9% (6/207) 20.6% (22/107) <0.001 Primary Sustained Clinical Improv. [3] 85.2% (167/196) 68.9% (73/106) <0.001 ABI / TBI [4] ± ± THUNDER: 5-Year Freedom from TLR Tepe, Zeller TCT 2011 Drug Eluting Stents Have Excellent Long Term Patency Approaching Bypass Patency(PSVR < 2.0): Provisional Zilver PTX vs BMS Courtesy: G. Ansel, MD 11
 Secondary Endpoint: Orbital Atherectomy Primary Patency at 12 Months (PSVR < 2.")

31 1/20/2015 Other Evolving Techniques: Atherectomy Devices DEFINITIVE LE Largest independently-adjudicated study of peripheral atherectomy performed to date (>800 patients) Claudicants Directional Atherectomy Primary Endpoint: Primary Patency at 12 Months (PSVR < 3.5) Secondary Endpoint: Orbital Atherectomy Primary Patency at 12 Months (PSVR < 2.4) Patency LL (cm) Patency LL (cm) All (n=743) 82% % 7.5 Diabetic (n=345) 80% % 7.6 Non-Diabetic (n=398) 83% % 7.4 Diabetics perform equally well when treated with directional atherectomy to non-diabetics for claudicants LASER Excisional/Aspiration McKinsey, JF, et al. JACC Cardiovasc Interv Aug;7(8): Are we approaching equipoise in SFA revascularization? The 5-year primary patency of different types of conduits for the SFA Vein PTA/stents ~75% Femoral-popliteal 55-75% eptfe Graft 40-50% Surgical reconstruction Nitinol Stent Femoral-popliteal 60% (3-5year) 65-80% Femoral-tibial 60-75% Stent Graft 74% (1yr); 25% (3yr) VMI (Supera) >80% (1yr&3yr TLR) DES ~65-75% (5yr) DCB >70% (5yr) Atherectomy ~80% (1yr) AbuRahma et al, 1999; Green et al, 2000; Johnson and Lee, 2000; Klinkert et al, 2003; Saxon, JVIR 2013; McKinsey, JACC CI 2013; Ansel, TCT 2014; Zeller, TCT
32 1/20/2015 Followup ABI 0.8 no symptoms ASA 81mg daily Plavix 75mg daily for 3 months (?) LLE asymptomatic Surveillance Duplex at 30d, 6mo, and 12 months and then annually Patent now out to 3 years Case 2: Bilateral Claudicant 66 yo salesman with Rutherford 3 claudication bilaterally R SFA heavily calcified subtotal occlusion requiring orbital atherectomy/pta/stent (overlapping 6x100 SE stents) L SFA CTO Occlusion treated next 13
33 1/20/


34 1/20/

35 1/20/


36 1/20/

37 1/20/
38 1/20/2015 Followup That patient has done well with stable and nearly normal ABI over 24 months We serial duplex surveillance demonstrates widely patent stents He is maintained on ASA Summary PTA and Conventional Nitinol Stents have relatively poor long term primary patency that worsens with lesion length Vascular Mimetic Implants are designed to resist the rigors of implantation within the SFA and have demonstrably improved primary patency and clinically driven TLR. Vascular Mimetic Implants are likely best suited to treat the majority of SFA lesions, particularly when calcification is present. Other emerging techniques including DES, DCB, and Atherectomy may have important roles in SFA Intervention VuMedi Webinar - Current Advances in SFA Interventions Cases and Applications of Bare Metal Stents and Vascular Mimetic Implants January 20, 2015 Sahil A. Parikh, M.D. Assistant Professor of Medicine Director, Research and Innovation Center Director, Experimental Interventional Cardiology Laboratory Director, Interventional Cardiology Fellowship Program Harrington Heart & Vascular Institute University Hospitals Case Medical Center Case Western Reserve University School of Medicine Cleveland, Ohio 19

39 Atherectomy for lower limb revascularization Lawrence A. Garcia, MD Chief, Section Interventional Cardiology and Vascular Interventions Director, Vascular Medicine St. Elizabeth s Medical Center Tufts University School of Medicine Boston, MA Case JC year old male with history HTN, HLP, CAD s/p PCI in the past and PVD with claudication Non-invasive work-up included ABI/duplex with ABI on the RLE 0.62 and duplex with serial lesions in the CFA/SFA and popliteal. Outflow appears preserved Angiography planned and images taken 1

40 2



41 How would you treat this lesion? 3





 1 year primary patency (%)")
 RESILIENT 137 Stent 6.3 81 (2.")
 VIPER 119 Stent graft 19.0 73(2.")
42 Stenting? To date the current default technology is stenting To date the meaningful studies have evaluated 5-6 cm lesions and only 2 studies have tested long lesions closer to 20 cms that we consider real world cases The gorilla in the room is restenosis In-stent restenosis vs de-novo restenosis Focal vs diffuse Recurrent vs recurrent Alternative therapies have been shown to be just as durable and safe as DES/BMS and combination therapy appears very appealing B A Calcium C D Current endovascular data Patients (n) Device Lesion length (cm) 1 year primary patency (%) (PSVR) MIMIC 81 PTA NA NA ABSOLUTE 104 Stent (2.5) RESILIENT 137 Stent (2.4) VIBRANT 76 Stent graft (2.5) VIPER 119 Stent graft (2.5) ZilverPTX 240 DES-SES (2.0) THUNDER 54 DCB (2.4) LEVANT 50 DCB (2.5) IN-PACT 301/220 DCB (2.4) 4
 IN-PACT PTA P n=220 subjects (221")
43 IN-PACT 2:1 randomized single blinded study DCB vs PTA alone 1 year results presented of 5 year study Lesions under 18 cm Occlusions under 10 cm RB 2-4 enrolled 331 randomized (all subjects) ITT 301 patients Provisional stenting listed in all subjects Baseline characteristics Lesion Type De-novo Restenotic Run off vessels Prox popliteal involvement (%) IN-PACT PTA P n=220 subjects (221 lesions) 95.0% (209/220) 5.0% (11/220) 3.3% (7/212) 13.7% (29/212) 41.5% (88/212) 41.5% (88/212) n=111 subjects (113 lesions) 94.6% (105/11) 5.4% (6/111) 4.5% (5/112) 26.8% (30/112) 33.0% )37/112) 35.7% (40/112) < % (15/221) 7.1% (8/113) 1.00 Lesion length (cm) 8.94± ± Total occlusions (%) 25.8% (57/221) 19.5% (22/113) 0.22 Severe calcification (%) 8.1% (18/221) 6.2% (7/113) 0.66 RVD (mm) 4.65± ± MLD pre (mm) 0.90± ± Diameter stenosis pre (%) 81.1± ± All ITT, 12 month patency 5
44 Directional atherectomy SilverHawk Key Study Design Elements Study Design and Oversight: Prospective, non-randomized, global study 800 subjects enrolled at 47 centers CEC and Steering Committee oversight and CEC adjudicaiton Angiographic and Duplex core laboratory analyses Inclusion Criteria RCC % stenosis Lesion lengths up to 20cm Reference Vessel 1.5 mm and 7.0 mm Exclusion Criteria Severe calcification In-stent restenosis Aneurysmal target vessel Primary Patency in Subgroups Subgroup Claudicants (n=743) Patency (PSVR < 2.4) Lesion Length (cm) All (n=1022) 78% 7.5 By Lesion Length < 4 cm (n=318) 81% cm (n=418) 83% cm (n=283) 67% 14.4 SFA Only By Lesion Length < 4 cm (n=184) 78% cm (n=253) 83% cm (n=232) 65%
45 Effective treatment for all lesion lengths 12 Month Primary Patency Rates from DEFINITIVE LE 100% 90% 80% 70% 60% 81% 83% 67% 50% 40% PSVR < % 20% 10% 0% < 4 cm cm 10 cm Mean length : 2.2 cm 6.5 cm 14.4 cm Number of lesions: DEFINITIVE AR Study Design Purpose: assess and estimate the effect of treating a vessel with directional atherectomy + DCB (DAART) compared to treatment with DCB alone Registry arm for severely calcified lesions created to limit bail-out stenting (and therefore variables) in randomized arm. DAART* General and Angiographic Criteria Assessment Lesion severely calcified? No Yes Guidewire passage, enrollment & Randomization Guidewire Passage & Enrollment * Directional Atherectomy + Anti-Restenotic Therapy (N = 48) DCB (N = 54) DAART* (N=19) Baseline Lesion Characteristics Per Core Lab Baseline Characteristics DAART (N= 48) DCB (N = 54) p-value* DAART Severe Ca++ Arm (N=19) Lesion Length (cm) Diameter Stenosis 82% 85% % Reference vessel diameter (mm) Minimum lumen diameter (mm) Calcification 70.8% 74.1% % Severe calcification 25.0% 18.5% % * p-value for DAART and DCB groups 7
46 Primary Patency Key Study Outcome at 12 Months Angiographic Patency shows similar pattern All Patients Lesions > 10 cm All Severe Ca++ N = 34 N = 39 N = 22 N = 16 N = 24 N = 7 DAART DCB Results for all patients who returned for angiographic follow-up 12-Month Patency: DAART RCT Patients Is it Important to Achieve 30% Residual Stenosis with Directional Atherectomy Post-Procedure? MLD = DAART Arm ~15.1 mm 2 lumen p = MLD = 3.78 DCB Arm ~11.8 mm 2 lumen area DCB DA Pre-Dilatation Baseline DAART resulted in a significantly larger area minimum lumen diameter (MLD) following the protocol-defined treatment in DEFINITIVE AR DUS Patency Angiographic Patency N = 20 N = 18 N = 17 N = 16 30% Residual Stenosis Post-DA >30% Residual Stenosis Post-DA Comparing non-stent technologies at 12 months 100% 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% Durability II IMPACT Fem-Pac Resilient Durability Levant 1 Supera Viper ZilverPTX Absolute Durability II Thunder Vibrant 78% 83% 68% DEFINITIVE LE Durability II Lesion Length (cm) 8
47 Long lesion atherectomy Drug coated balloon technology is safe and effective IN-Pact has shown benefit at 1 year higher than any other trial to date in a level 1 randomized protocol at near 9 cm LL. DEFINITIVE LE proved atherectomy safe & effective at 12 months Effective for short, medium and long lesions in claudicants & CLI patients DEFINTIVE AR pilot study demonstrated a signal of benefit for combined therapy Initial signal suggests an potential role for DCB with atherectomy that may obviate the need for stenting as an upfront need for our patients with complex peripheral vascular disease Opportunity for re-therapy remains open to the operator and patient if no endoprosthesis is left behind at the index procedure. Overall cost benefit needs assessment but remember repeat revascularization for ISRS may not benign and only once 9
Which Stent Is Best for Various Femoropopliteal Anatomy? 2018 Pacific Northwest Endovascular Conference June 15-26, 2018 Seattle, WA
 Which Stent Is Best for Various Femoropopliteal Anatomy? 2018 Pacific Northwest Endovascular Conference June 15-26, 2018 Seattle, WA Brian DeRubertis, MD, FACS Associate Professor of Surgery UCLA Division
Which Stent Is Best for Various Femoropopliteal Anatomy? 2018 Pacific Northwest Endovascular Conference June 15-26, 2018 Seattle, WA Brian DeRubertis, MD, FACS Associate Professor of Surgery UCLA Division
Is a Stent or Scaffold Necessary in The SFA?
 1 2 3 Is a Stent or Scaffold Necessary in The SFA? Stents were developed to optimize acute results after angioplasty Specifically, stents are universally accepted to manage flow limiting dissections and
1 2 3 Is a Stent or Scaffold Necessary in The SFA? Stents were developed to optimize acute results after angioplasty Specifically, stents are universally accepted to manage flow limiting dissections and
Long Lesions: Primary stenting or DCB first? John Laird MD Adventist Heart and Vascular Institute, St. Helena, CA
 Long Lesions: Primary stenting or DCB first? John Laird MD Adventist Heart and Vascular Institute, St. Helena, CA Disclosures John R. Laird Within the past 12 months, I or my spouse/partner have had a
Long Lesions: Primary stenting or DCB first? John Laird MD Adventist Heart and Vascular Institute, St. Helena, CA Disclosures John R. Laird Within the past 12 months, I or my spouse/partner have had a
Disclosures. In the DCB Era, How Do I Choose To Use a Stent? When to Stent and What Devices to Use in the SFA
 In the DCB Era, How Do I Choose To Use a Stent? When to Stent and What Devices to Use in the SFA Disclosures No financial disclosures. Cameron M. Akbari, MD, MBA, FACS Site Director, Vascular Surgery Medstar
In the DCB Era, How Do I Choose To Use a Stent? When to Stent and What Devices to Use in the SFA Disclosures No financial disclosures. Cameron M. Akbari, MD, MBA, FACS Site Director, Vascular Surgery Medstar
Clinical Data Update for Drug Coated Balloons (DCB) Seung-Whan Lee, MD, PhD
 Seung-Whan Lee, MD, PhD") Clinical Data Update for Drug Coated Balloons (DCB) Seung-Whan Lee, MD, PhD Asan Medical Center, Heart Institute, University of Ulsan College of Medicine, Werk et al. Circulation Cardiovasc Intervent 2012
Clinical Data Update for Drug Coated Balloons (DCB) Seung-Whan Lee, MD, PhD Asan Medical Center, Heart Institute, University of Ulsan College of Medicine, Werk et al. Circulation Cardiovasc Intervent 2012
4/14/2016. Faculty Disclosure. Drug-eluting technology in the SFA and Popliteal. Typical SFA Disease Pattern. Why Peripheral Artery Disease Matters
 Drug-eluting technology in the SFA and Popliteal David Paul Slovut, MD, PhD Associate Professor of Medicine and Surgery Co-director of TAVR program Director of Advanced Intervention Faculty Disclosure
Drug-eluting technology in the SFA and Popliteal David Paul Slovut, MD, PhD Associate Professor of Medicine and Surgery Co-director of TAVR program Director of Advanced Intervention Faculty Disclosure
Disclosures. Rational Selection of Endovascular Options for the SFA and Popliteal: What Works Where and for How Long?
 Rational Selection of Endovascular Options for the SFA and Popliteal: What Works Where and for How Long? UCSF Vascular Symposium 2017 April 6-8, 2017 San Francisco, CA Disclosures Consulting, Speakers
Rational Selection of Endovascular Options for the SFA and Popliteal: What Works Where and for How Long? UCSF Vascular Symposium 2017 April 6-8, 2017 San Francisco, CA Disclosures Consulting, Speakers
Christian Wissgott MD, PhD Assistant Director, Radiology Westküstenkliniken Heide
 2-Year Results Of The Tack Optimized Balloon Angioplasty (TOBA) Trial For Fem- Pop Lesions Demonstrates Safety and Efficacy Of The Tack Endovascular System In Repairing Focal Post-PTA Dissections Christian
2-Year Results Of The Tack Optimized Balloon Angioplasty (TOBA) Trial For Fem- Pop Lesions Demonstrates Safety and Efficacy Of The Tack Endovascular System In Repairing Focal Post-PTA Dissections Christian
Outcomes Of DCB Use In Real World Registries: 2 Year Results From The INPACT Global Registry
 Outcomes Of DCB Use In Real World Registries: 2 Year Results From The INPACT Global Registry Marianne Brodmann, MD Head of the Clinical Division of Angiology Department of Internal Medicine Medical University
Outcomes Of DCB Use In Real World Registries: 2 Year Results From The INPACT Global Registry Marianne Brodmann, MD Head of the Clinical Division of Angiology Department of Internal Medicine Medical University
Atherectomy is Still Live and Effective. John R. Laird, MD Professor of Medicine Medical Director of the Vascular Center UC Davis Health System
 Atherectomy is Still Live and Effective John R. Laird, MD Professor of Medicine Medical Director of the Vascular Center UC Davis Health System Why is Atherectomy Still Alive? Improved devices Better data
Atherectomy is Still Live and Effective John R. Laird, MD Professor of Medicine Medical Director of the Vascular Center UC Davis Health System Why is Atherectomy Still Alive? Improved devices Better data
Drug-Coated Balloon Treatment for Patients with Intermittent Claudication: Insights from the IN.PACT Global Full Clinical Cohort
 Drug-Coated Balloon Treatment for Patients with Intermittent Claudication: Insights from the IN.PACT Global Full Clinical Cohort a.o. Univ. Prof. Dr. Marianne Brodmann Medical University of Graz Graz,
Drug-Coated Balloon Treatment for Patients with Intermittent Claudication: Insights from the IN.PACT Global Full Clinical Cohort a.o. Univ. Prof. Dr. Marianne Brodmann Medical University of Graz Graz,
Merits and demerits of DES, DEB or covered stent in lower extremity arterial occlusive disease 성균관의과대학삼성서울병원순환기내과최승혁
 Merits and demerits of DES, DEB or covered stent in lower extremity arterial occlusive disease 성균관의과대학삼성서울병원순환기내과최승혁 Contents DES in SFA DES in BTK DEB in SFA DEB in BTK Current status of covered stent
Merits and demerits of DES, DEB or covered stent in lower extremity arterial occlusive disease 성균관의과대학삼성서울병원순환기내과최승혁 Contents DES in SFA DES in BTK DEB in SFA DEB in BTK Current status of covered stent
Is combination therapy with directional atherectomy followed by DCB the answer to challenges in treating SFA disease?
 Is combination therapy with directional atherectomy followed by DCB the answer to challenges in treating SFA disease? The REALITY trial G. Torsello Münster Disclosure Speaker name: G. Torsello... I have
Is combination therapy with directional atherectomy followed by DCB the answer to challenges in treating SFA disease? The REALITY trial G. Torsello Münster Disclosure Speaker name: G. Torsello... I have
Drug- Coated Balloons for the SFA: Overview of Technology and Results
 Drug- Coated Balloons for the SFA: Overview of Technology and Results NCVH Latin American 2015 Bogota, Colombia April 9-11, 2015 Brian G. DeRubertis, M.D. Associate Professor of Surgery Division of Vascular
Drug- Coated Balloons for the SFA: Overview of Technology and Results NCVH Latin American 2015 Bogota, Colombia April 9-11, 2015 Brian G. DeRubertis, M.D. Associate Professor of Surgery Division of Vascular
Cutting/scoring balloon Cryoplasty Drug-eluting balloon Brachytherapy Debulking Restent (BMS or DES) John R. Laird, MD
 John R. Laird, MD") Current Treatment of Femoropopliteal Instent Restenosis Professor of Medicine Medical Director of the Vascular Center UC Davis Medical Center SFA In-stent Restenosis Common: 18%- 40% at 12 months in recent
Current Treatment of Femoropopliteal Instent Restenosis Professor of Medicine Medical Director of the Vascular Center UC Davis Medical Center SFA In-stent Restenosis Common: 18%- 40% at 12 months in recent
DCB use in fem-pop lesions of patients with CLI (RCC 4-5): subgroup analysis of IN.PACT Global 12-month outcomes
: subgroup analysis of IN.PACT Global 12-month outcomes") DCB use in fem-pop lesions of patients with CLI (RCC 4-5): subgroup analysis of IN.PACT Global 12-month outcomes Carlos Mena, MD FACC FSCAI Associate Professor of Medicine - Cardiology Director Cardiac
DCB use in fem-pop lesions of patients with CLI (RCC 4-5): subgroup analysis of IN.PACT Global 12-month outcomes Carlos Mena, MD FACC FSCAI Associate Professor of Medicine - Cardiology Director Cardiac
Promise and limitations of DCB in long lesions What Have we Learned from Clinical Trials? Ramon L. Varcoe, MBBS, MS, FRACS, PhD
 Promise and limitations of DCB in long lesions What Have we Learned from Clinical Trials? Ramon L. Varcoe, MBBS, MS, FRACS, PhD Associate Professor of Vascular Surgery University of New South Wales Sydney,
Promise and limitations of DCB in long lesions What Have we Learned from Clinical Trials? Ramon L. Varcoe, MBBS, MS, FRACS, PhD Associate Professor of Vascular Surgery University of New South Wales Sydney,
DCB level 1 evidence review
 DCB level 1 evidence review Raphaël COSCAS Vascular Surgery Department Ambroise Paré Hospital, AP-HP and Paris-Ouest University Boulogne-Billancourt, France Disclosure Speaker name: Raphael COSCAS I have
DCB level 1 evidence review Raphaël COSCAS Vascular Surgery Department Ambroise Paré Hospital, AP-HP and Paris-Ouest University Boulogne-Billancourt, France Disclosure Speaker name: Raphael COSCAS I have
Do we really need a stent in long SFA lesions? No: DEB is the answer
 Do we really need a stent in long SFA lesions? No: DEB is the answer Thomas Zeller, MD University Heart-Center Freiburg-Bad Krozingen Bad Krozingen Germany My Disclosures: Advisory Board: Medtronic-Invatec,
Do we really need a stent in long SFA lesions? No: DEB is the answer Thomas Zeller, MD University Heart-Center Freiburg-Bad Krozingen Bad Krozingen Germany My Disclosures: Advisory Board: Medtronic-Invatec,
TOBA II 12-Month Results Tack Optimized Balloon Angioplasty
 TOBA II 12-Month Results Tack Optimized Balloon Angioplasty William Gray, MD System Chief, Cardiovascular Division Main Line Health, Philadelphia, PA Dissection: The Primary Mechanism of Angioplasty Lesions
TOBA II 12-Month Results Tack Optimized Balloon Angioplasty William Gray, MD System Chief, Cardiovascular Division Main Line Health, Philadelphia, PA Dissection: The Primary Mechanism of Angioplasty Lesions
Clinical benefits on DES Patient s perspectives
 Clinical benefits on DES Patient s perspectives Dr. Skyi Pang Vascular Surgeon Department of Surgery Pamela Youde Nethersole Eastern Hospital Hong Kong Disclosure Speaker name: Skyi Pang... I have the
Clinical benefits on DES Patient s perspectives Dr. Skyi Pang Vascular Surgeon Department of Surgery Pamela Youde Nethersole Eastern Hospital Hong Kong Disclosure Speaker name: Skyi Pang... I have the
Making BTK Interventions more Durable: Are DES and DCB the answer? Thomas Zeller, MD
 Making BTK Interventions more Durable: Are DES and DCB the answer? Thomas Zeller, MD Faculty Disclosure Thomas Zeller, MD For the 12 months preceding this presentation, I disclose the following types of
Making BTK Interventions more Durable: Are DES and DCB the answer? Thomas Zeller, MD Faculty Disclosure Thomas Zeller, MD For the 12 months preceding this presentation, I disclose the following types of
A Data-driven Therapeutic Algorithm For Choosing Among Currently Available Tools For SFA Intervention
 A Data-driven Therapeutic Algorithm For Choosing Among Currently Available Tools For SFA Intervention William A. Gray MD Director of Endovascular Services Associate Professor of Clinical Medicine Columbia
A Data-driven Therapeutic Algorithm For Choosing Among Currently Available Tools For SFA Intervention William A. Gray MD Director of Endovascular Services Associate Professor of Clinical Medicine Columbia
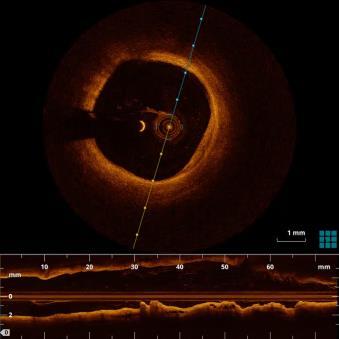
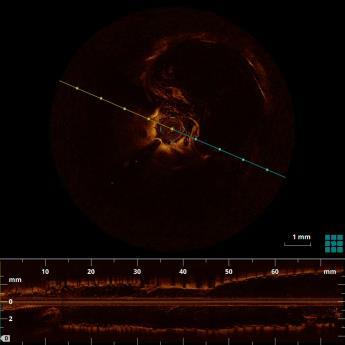
Accurate Vessel Sizing Drives Clinical Results. IVUS In the Periphery
 Accurate Vessel Sizing Drives Clinical Results IVUS In the Periphery Discussion Iida O, et. al. Study Efficacy of Intravascular Ultrasound in Femoropopliteal Stenting for Peripheral Artery Disease With
Accurate Vessel Sizing Drives Clinical Results IVUS In the Periphery Discussion Iida O, et. al. Study Efficacy of Intravascular Ultrasound in Femoropopliteal Stenting for Peripheral Artery Disease With
William A. Gray MD System Chief of Cardiovascular Services, Main Line Health President, Lankenau Heart Institute Wynnewood, PA USA
 William A. Gray MD System Chief of Cardiovascular Services, President, Wynnewood, PA USA Why atherectomy? Calcification is the norm not the exception Most trials do not include heavy calcification There
William A. Gray MD System Chief of Cardiovascular Services, President, Wynnewood, PA USA Why atherectomy? Calcification is the norm not the exception Most trials do not include heavy calcification There
Update on the Levant 2 Clinical Trial Programme. Dierk Scheinert, MD University Hospital Leipzig Leipzig, Germany
 Update on the Levant 2 Clinical Trial Programme Dierk Scheinert, MD University Hospital Leipzig Leipzig, Germany Disclosure Speaker name: Dierk Scheinert I have the following potential conflicts of interest
Update on the Levant 2 Clinical Trial Programme Dierk Scheinert, MD University Hospital Leipzig Leipzig, Germany Disclosure Speaker name: Dierk Scheinert I have the following potential conflicts of interest
12-month Outcomes of Post Dilatation in the IN.PACT Global CTO Cohort. Gunnar Tepe, MD RodMed Clinic Rosenheim Rosenheim, Germany
 12-month Outcomes of Post Dilatation in the IN.PACT Global CTO Cohort Gunnar Tepe, MD RodMed Clinic Rosenheim Rosenheim, Germany Disclosure Speaker name: Gunnar Tepe I have the following potential conflicts
12-month Outcomes of Post Dilatation in the IN.PACT Global CTO Cohort Gunnar Tepe, MD RodMed Clinic Rosenheim Rosenheim, Germany Disclosure Speaker name: Gunnar Tepe I have the following potential conflicts
Efficacy of DEB in Calcification and Subintimal Angioplasty
 Efficacy of DEB in Calcification and Subintimal Angioplasty Seung-Woon Rha, MD, PhD, FACC, FAHA, FSCAI, FESC, FAPSIC Div of Cardiovascular Intervention and Research Cardiovascular Center, Korea University
Efficacy of DEB in Calcification and Subintimal Angioplasty Seung-Woon Rha, MD, PhD, FACC, FAHA, FSCAI, FESC, FAPSIC Div of Cardiovascular Intervention and Research Cardiovascular Center, Korea University
The ZILVERPASS study a randomized study comparing ZILVER PTX stenting with Bypass in femoropopliteal lesions
 The ZILVERPASS study a randomized study comparing ZILVER PTX stenting with Bypass in femoropopliteal lesions Dr. Sven Bräunlich Department of Angiology University-Hospital Leipzig, Germany Disclosure Speaker
The ZILVERPASS study a randomized study comparing ZILVER PTX stenting with Bypass in femoropopliteal lesions Dr. Sven Bräunlich Department of Angiology University-Hospital Leipzig, Germany Disclosure Speaker
Vessel Preparation: What does it mean and what are the current tools? Lawrence Garcia, MD St. Elizabeth s Medical Center Boston, MA, USA
 Vessel Preparation: What does it mean and what are the current tools? Lawrence Garcia, MD St. Elizabeth s Medical Center Boston, MA, USA Disclosure Statement of Financial Interest Within the past 12 months,
Vessel Preparation: What does it mean and what are the current tools? Lawrence Garcia, MD St. Elizabeth s Medical Center Boston, MA, USA Disclosure Statement of Financial Interest Within the past 12 months,
BIOLUX P-III Passeo-18 Lux All-comers Registry: 12-month Results for the All-Comers Cohort
 BIOLUX P-III Passeo-18 Lux All-comers Registry: 12-month Results for the All-Comers Cohort Prof. Dr. Gunnar TEPE, Klinikum Rosenheim, Germany CCI on behalf of the BIOLUX P-III Investigators Disclosure
BIOLUX P-III Passeo-18 Lux All-comers Registry: 12-month Results for the All-Comers Cohort Prof. Dr. Gunnar TEPE, Klinikum Rosenheim, Germany CCI on behalf of the BIOLUX P-III Investigators Disclosure
Latest Insights from the LEVANT II study and sub-group analysis
 Latest Insights from the LEVANT II study and sub-group analysis Prof. Dr. med. Dierk Scheinert Division of Interventional Angiology University-Hospital Leipzig, Germany Conflicts of Interest Advisory Board
Latest Insights from the LEVANT II study and sub-group analysis Prof. Dr. med. Dierk Scheinert Division of Interventional Angiology University-Hospital Leipzig, Germany Conflicts of Interest Advisory Board
Robert W. Fincher, DO The Ritz-Carlton, Dove Mountain Marana, Arizona February 7th, 2015
 Robert W. Fincher, DO The Ritz-Carlton, Dove Mountain Marana, Arizona February 7th, 2015 Disclosure I have nothing to disclose Randomized Controlled Studies In SFA Technology: What s The Best Tool For
Robert W. Fincher, DO The Ritz-Carlton, Dove Mountain Marana, Arizona February 7th, 2015 Disclosure I have nothing to disclose Randomized Controlled Studies In SFA Technology: What s The Best Tool For
Final Results of the Feasibility Study for the Drug-coated Chocolate Touch PTA balloon. (The ENDURE Trial)
") Final results of the feasibility study for the drug-coated Chocolate Touch PTA balloon of of femoropopliteal Femoropopliteal lesions lesions: (The ENDURE Trial) Final Results of the Feasibility Study for
Final results of the feasibility study for the drug-coated Chocolate Touch PTA balloon of of femoropopliteal Femoropopliteal lesions lesions: (The ENDURE Trial) Final Results of the Feasibility Study for
Management of In-stent Restenosis after Lower Extremity Endovascular Procedures
 Management of In-stent Restenosis after Lower Extremity Endovascular Procedures Piotr Sobieszczyk, MD Associate Director, Cardiac Catheterization Laboratory Cardiovascular Division and Vascular Medicine
Management of In-stent Restenosis after Lower Extremity Endovascular Procedures Piotr Sobieszczyk, MD Associate Director, Cardiac Catheterization Laboratory Cardiovascular Division and Vascular Medicine
Treatment Strategies for Long Lesions of greater than 20 cm
 Treatment Strategies for Long Lesions of greater than 20 cm Donald L. Jacobs, MD C. Rollins Hanlon Professor and Chair Chair of the Department of Surgery Saint Louis University Disclosure Speaker name:
Treatment Strategies for Long Lesions of greater than 20 cm Donald L. Jacobs, MD C. Rollins Hanlon Professor and Chair Chair of the Department of Surgery Saint Louis University Disclosure Speaker name:
Final Results of the Feasibility Study for the Drug-coated Chocolate Touch PTA balloon. (The ENDURE Trial)
") Final results of the feasibility study for the drug-coated Chocolate Touch PTA balloon of of femoropopliteal Femoropopliteal lesions lesions: (The ENDURE Trial) Final Results of the Feasibility Study for
Final results of the feasibility study for the drug-coated Chocolate Touch PTA balloon of of femoropopliteal Femoropopliteal lesions lesions: (The ENDURE Trial) Final Results of the Feasibility Study for
Dierk Scheinert, MD. Department of Angiology University Hospital Leipzig, Germany
 The RANGER clinical trial programme: 12-month results from the RANGER RCT and first look at the COMARE I study of RANGER vs. IN.PACT for femoropopliteal lesions Dierk Scheinert, MD Department of Angiology
The RANGER clinical trial programme: 12-month results from the RANGER RCT and first look at the COMARE I study of RANGER vs. IN.PACT for femoropopliteal lesions Dierk Scheinert, MD Department of Angiology
Current Status and Limitations in the Treatment of Femoropopliteal In-Stent Restenosis
 Current Status and Limitations in the Treatment of Femoropopliteal In-Stent Restenosis Osamu Iida, MD From the Kansai Rosai Hospital Cardiovascular Center, Amagasaki City, Japan. ABSTRACT: Approximately
Current Status and Limitations in the Treatment of Femoropopliteal In-Stent Restenosis Osamu Iida, MD From the Kansai Rosai Hospital Cardiovascular Center, Amagasaki City, Japan. ABSTRACT: Approximately
Lessons learnt from DES in the SFA is there any ideal concept so far?
 Wednesday, January 25, 2017 - Time: 11:49-11:55 DEEP DIVE SESSION: Lower limb interventions (part II) Lessons learnt from DES in the SFA is there any ideal concept so far? S.Müller-Hülsbeck, MD, EBIR,
Wednesday, January 25, 2017 - Time: 11:49-11:55 DEEP DIVE SESSION: Lower limb interventions (part II) Lessons learnt from DES in the SFA is there any ideal concept so far? S.Müller-Hülsbeck, MD, EBIR,
The Final Triumph Of Endovascular Therapy In SFA Treatment
 The Final Triumph Of Endovascular Therapy In SFA Treatment MEET 07 Mark W. Mewissen, M.D. Director, St Lukes Vascular Center Milwaukee, WI Endovascular Therapy In SFA Treatment: Works In Progress! Mark
The Final Triumph Of Endovascular Therapy In SFA Treatment MEET 07 Mark W. Mewissen, M.D. Director, St Lukes Vascular Center Milwaukee, WI Endovascular Therapy In SFA Treatment: Works In Progress! Mark
MEET M. Bosiers K. Deloose P. Peeters. SFA stenting in 2009 : The good and the ugly What factors influence patency?
 MEET 2009 SFA stenting in 2009 : The good and the ugly What factors influence patency? M. Bosiers K. Deloose P. Peeters 1 TASC II 2007 vs TASC 2000 Type A Type B Type C Type D 2000 < 3 cm 3-5 cm < 3 cm
MEET 2009 SFA stenting in 2009 : The good and the ugly What factors influence patency? M. Bosiers K. Deloose P. Peeters 1 TASC II 2007 vs TASC 2000 Type A Type B Type C Type D 2000 < 3 cm 3-5 cm < 3 cm
Update on the role of drug eluting balloons
 Update on the role of drug eluting balloons William A. Gray MD Director of Endovascular Services Associate Professor of Clinical Medicine Columbia University Medical Center The Cardiovascular Research
Update on the role of drug eluting balloons William A. Gray MD Director of Endovascular Services Associate Professor of Clinical Medicine Columbia University Medical Center The Cardiovascular Research
SFA lesion treatment: China experience. Wei Liang, MD
 SFA lesion treatment: China experience Wei Liang, MD Disclosure I do not have any potential conflict of interest Background PAD: 14% - 20% in adults Aorta & Iliac A: 30% Femoral & Pop A: 80-90% Tibial
SFA lesion treatment: China experience Wei Liang, MD Disclosure I do not have any potential conflict of interest Background PAD: 14% - 20% in adults Aorta & Iliac A: 30% Femoral & Pop A: 80-90% Tibial
Vessel Preparation Prior to DCB and Stenting: How to Do It.
 Vessel Preparation Prior to DCB and Stenting: How to Do It. LINC 2018 January 30 February 2, 2018 Leipzig, Germany Brian DeRubertis, MD, FACS Associate Professor of Surgery UCLA Division of Vascular Surgery
Vessel Preparation Prior to DCB and Stenting: How to Do It. LINC 2018 January 30 February 2, 2018 Leipzig, Germany Brian DeRubertis, MD, FACS Associate Professor of Surgery UCLA Division of Vascular Surgery
DCB in my practice: How the evidence influences my strategy. Yang-Jin Park
 DCB in my practice: How the evidence influences my strategy Yang-Jin Park Associate Professor Division of Vascular Surgery, Department of Surgery Samsung Medical Center Sungkyunkwan University School of
DCB in my practice: How the evidence influences my strategy Yang-Jin Park Associate Professor Division of Vascular Surgery, Department of Surgery Samsung Medical Center Sungkyunkwan University School of
New Data to Shape the Era of Drug Elution in Peripheral Interventions
 New Data to Shape the Era of Drug Elution in Peripheral Interventions William A. Gray MD Director of Endovascular Services Columbia University Medical Center New York Lower Extremity Endovascular - Interventions
New Data to Shape the Era of Drug Elution in Peripheral Interventions William A. Gray MD Director of Endovascular Services Columbia University Medical Center New York Lower Extremity Endovascular - Interventions
Drug Elution, Data, and Decisions
 Drug Elution, Data, and Decisions What the data tell us about how to integrate drug-eluting technology into our daily practice. BY GARY ANSEL, MD, AND JOHN A. PHILLIPS, MD The use of drug-eluting technology
Drug Elution, Data, and Decisions What the data tell us about how to integrate drug-eluting technology into our daily practice. BY GARY ANSEL, MD, AND JOHN A. PHILLIPS, MD The use of drug-eluting technology
Update from Korea on the Lutonix SFA registry 12 month data
 Update from Korea on the Lutonix SFA registry 12 month data Prospective, Multicenter, Post-Market Registy Assessing the Clinical Use and Safety of the Lutonix Drug Coated Balloon in Femoropopliteal Arteries
Update from Korea on the Lutonix SFA registry 12 month data Prospective, Multicenter, Post-Market Registy Assessing the Clinical Use and Safety of the Lutonix Drug Coated Balloon in Femoropopliteal Arteries
COMPARE-Pilot RCT: 1-year results of a randomised comparison of RANGER DCB vs. IN.PACT DCB in complex SFA lesions. Dierk Scheinert
 COMPARE-Pilot RCT: 1-year results of a randomised comparison of RANGER DCB vs. IN.PACT DCB in complex SFA lesions Dierk Scheinert Department of Angiology University Hospital Leipzig, Germany Disclosure
COMPARE-Pilot RCT: 1-year results of a randomised comparison of RANGER DCB vs. IN.PACT DCB in complex SFA lesions Dierk Scheinert Department of Angiology University Hospital Leipzig, Germany Disclosure
Device Evolution. Atherectomy: Where Do We Stand After 12 Years Since FDA Clearance. Where Do We Stand? 4/18/2015
 Disclosure Statement of Financial Interest Atherectomy: Where Do We Stand After 12 Years Since FDA Clearance Within the past 12 months, I or my spouse/partner have had a financial interest/arrangement
Disclosure Statement of Financial Interest Atherectomy: Where Do We Stand After 12 Years Since FDA Clearance Within the past 12 months, I or my spouse/partner have had a financial interest/arrangement
Update on the Ranger clinical trial programme
 Update on the Ranger clinical trial programme Dierk Scheinert, MD Universitätsklinikum Leipzig, Leipzig, Germany on behalf of the RANGER SFA investigators Disclosure Speaker s name: Dierk Scheinert I have
Update on the Ranger clinical trial programme Dierk Scheinert, MD Universitätsklinikum Leipzig, Leipzig, Germany on behalf of the RANGER SFA investigators Disclosure Speaker s name: Dierk Scheinert I have
Neuestes aus der Therapie der pavk. beschichtete Stents + Ballons. Karls-University. Eberhard-Karls. of Tubingen Department of Diagnostic Radiology
 Eberhard-Karls Karls-University of Tubingen Department of Diagnostic Radiology Neuestes aus der Therapie der pavk Berlin Dezember 08 beschichtete Stents + Ballons Gunnar Tepe 1 Local Drug Delivery Basic
Eberhard-Karls Karls-University of Tubingen Department of Diagnostic Radiology Neuestes aus der Therapie der pavk Berlin Dezember 08 beschichtete Stents + Ballons Gunnar Tepe 1 Local Drug Delivery Basic
Evolving Role of Drug-Eluting Stents In Complex SFA - Majestic Trial Data
 Evolving Role of Drug-Eluting Stents In Complex SFA - Majestic Trial Data Ralf Langhoff, MD Center for Vascular Medicine Berlin-Wilmersdorf St. Gertrauden Hospital Charité, CC11 Academic Teaching Hospitals
Evolving Role of Drug-Eluting Stents In Complex SFA - Majestic Trial Data Ralf Langhoff, MD Center for Vascular Medicine Berlin-Wilmersdorf St. Gertrauden Hospital Charité, CC11 Academic Teaching Hospitals
Michael K.W. Lichtenberg, MD
 Ranger All-Comer Registry Treatment of femoropopliteal atherosclerotic lesions using the Drug eluting Balloon Ranger: An All Comers Registry Michael K.W. Lichtenberg, MD Klinikum Arnsberg Arnsberg, Germany
Ranger All-Comer Registry Treatment of femoropopliteal atherosclerotic lesions using the Drug eluting Balloon Ranger: An All Comers Registry Michael K.W. Lichtenberg, MD Klinikum Arnsberg Arnsberg, Germany
Could a combination of DCB + stent be the answer in complex SFA lesions
 Could a combination of DCB + stent be the answer in complex SFA lesions Sven Bräunlich, MD Division of Interventional Angiology University-Hospital Leipzig, Germany Disclosure Speaker name: Sven Bräunlich
Could a combination of DCB + stent be the answer in complex SFA lesions Sven Bräunlich, MD Division of Interventional Angiology University-Hospital Leipzig, Germany Disclosure Speaker name: Sven Bräunlich
Turbo-Power. Laser atherectomy catheter. The standard. for ISR
 Turbo-Power Laser atherectomy catheter The standard for ISR Vaporize the ISR challenge In-stent restenosis (ISR) Chance of recurring 7 115,000 + /year (U.S.) 1-6 Repeated narrowing of the arteries after
Turbo-Power Laser atherectomy catheter The standard for ISR Vaporize the ISR challenge In-stent restenosis (ISR) Chance of recurring 7 115,000 + /year (U.S.) 1-6 Repeated narrowing of the arteries after
Update on Tack Optimized Balloon Angioplasty (TOBA) Below the Knee. Marianne Brodmann, MD Medical University Graz Graz, Austria
 Below the Knee. Marianne Brodmann, MD Medical University Graz Graz, Austria") Update on Tack Optimized Balloon Angioplasty (TOBA) Below the Knee Marianne Brodmann, MD Medical University Graz Graz, Austria Critical Limb Ischemia Infrapopliteal arterial disease is a leading source
Update on Tack Optimized Balloon Angioplasty (TOBA) Below the Knee Marianne Brodmann, MD Medical University Graz Graz, Austria Critical Limb Ischemia Infrapopliteal arterial disease is a leading source
The BATTLE Trial Comparing Bare Metal to Drug Eluting Stents for Intermediate Length Lesions of the SFA
 The BATTLE Trial Comparing Bare Metal to Drug Eluting Stents for Intermediate Length Lesions of the SFA BATTLE RCT investigators: Y. Gouëffic, A. Sauguet, P. Desgranges, P. Feugier, E. Rosset, E. Ducasse,
The BATTLE Trial Comparing Bare Metal to Drug Eluting Stents for Intermediate Length Lesions of the SFA BATTLE RCT investigators: Y. Gouëffic, A. Sauguet, P. Desgranges, P. Feugier, E. Rosset, E. Ducasse,
Drug eluting stents and balloons in peripheral arterial disease A.T.O. ABDOOL-CARRIM UNIVERSITY OF WITWATERSRAND
 Drug eluting stents and balloons in peripheral arterial disease A.T.O. ABDOOL-CARRIM UNIVERSITY OF WITWATERSRAND Drug eluting stents and balloons Endovascular treatment now becoming more popular for treatment
Drug eluting stents and balloons in peripheral arterial disease A.T.O. ABDOOL-CARRIM UNIVERSITY OF WITWATERSRAND Drug eluting stents and balloons Endovascular treatment now becoming more popular for treatment
Disclosures: Stent-grafts for Long-Segment SFA Disease: Better than the Alternatives? SFA Treatment Overview: Longer Lesions 4/18/2013
 Stent-grafts for Long-Segment SFA Disease: Better than the Alternatives? Richard Saxon MD Director of Research San Diego Cardiac and Vascular Institute San Diego Imaging Medical Group San Diego, CA Disclosures:
Stent-grafts for Long-Segment SFA Disease: Better than the Alternatives? Richard Saxon MD Director of Research San Diego Cardiac and Vascular Institute San Diego Imaging Medical Group San Diego, CA Disclosures:
Lutonix DCB in BTK Update on the BTK real world registry and RCT
 Lutonix DCB in BTK Update on the BTK real world registry and RCT Prof. Dr. med. Dierk Scheinert Department of Interventional Angiology University Hospital Leipzig Disclosures Speaker: Prof. Dr. med. Dierk
Lutonix DCB in BTK Update on the BTK real world registry and RCT Prof. Dr. med. Dierk Scheinert Department of Interventional Angiology University Hospital Leipzig Disclosures Speaker: Prof. Dr. med. Dierk
SFA In-stent Restenosis
 Disclosure In-Stent Restenosis: Endo-Salvage Works for Most Patients Peter A. Schneider, MD Hawaii Permanente Medical Group and Kaiser Foundation Hospital Honolulu, Hawaii Peter A. Schneider Potential
Disclosure In-Stent Restenosis: Endo-Salvage Works for Most Patients Peter A. Schneider, MD Hawaii Permanente Medical Group and Kaiser Foundation Hospital Honolulu, Hawaii Peter A. Schneider Potential
The present status of selfexpanding. for CLI: Why and when to use. Sean P Lyden MD Cleveland Clinic Cleveland, Ohio
 The present status of selfexpanding and balloonexpandable tibial BMS and DES for CLI: Why and when to use Sean P Lyden MD Cleveland Clinic Cleveland, Ohio Disclosure Speaker name: Sean Lyden, MD I have
The present status of selfexpanding and balloonexpandable tibial BMS and DES for CLI: Why and when to use Sean P Lyden MD Cleveland Clinic Cleveland, Ohio Disclosure Speaker name: Sean Lyden, MD I have
Future Algorithm for Lower Extremity Revascularization: Where Does Vessel Prep Fit?
 Future Algorithm for Lower Extremity Revascularization: Where Does Vessel Prep Fit? John R. Laird Adventist Heart and Vascular Institute St. Helena, CA Disclosure Speaker name: John R. Laird... I have
Future Algorithm for Lower Extremity Revascularization: Where Does Vessel Prep Fit? John R. Laird Adventist Heart and Vascular Institute St. Helena, CA Disclosure Speaker name: John R. Laird... I have
Superficial Femoral Artery Intervention: The gift that keeps on giving! Wm. Britton Eaves,MD WKHSC Bossier City, LA
 : The gift that keeps on giving! Wm. Britton Eaves,MD WKHSC Bossier City, LA Peripheral arterial disease (PAD) of the superficial femoral artery (SFA) is the most common cause of intermittent claudication
: The gift that keeps on giving! Wm. Britton Eaves,MD WKHSC Bossier City, LA Peripheral arterial disease (PAD) of the superficial femoral artery (SFA) is the most common cause of intermittent claudication
Recent Advances in Peripheral Salvage
 Recent Advances in Peripheral Salvage Dr Shaiful Azmi Yahaya, MD, MMed, FNHAM, FAsCC, FAPSIC Consultant Cardiologist and Peripheral Interventionist, Institut Jantung Negara Disclosure I am proctoring for
Recent Advances in Peripheral Salvage Dr Shaiful Azmi Yahaya, MD, MMed, FNHAM, FAsCC, FAPSIC Consultant Cardiologist and Peripheral Interventionist, Institut Jantung Negara Disclosure I am proctoring for
The Role of Lithotripsy in Solving the Challenges of Vascular Calcium. Thomas Zeller, MD
 The Role of Lithotripsy in Solving the Challenges of Vascular Calcium Thomas Zeller, MD 1 1 Disclosure Speaker name: Thomas Zeller... I have the following potential conflicts of interest to report: X X
The Role of Lithotripsy in Solving the Challenges of Vascular Calcium Thomas Zeller, MD 1 1 Disclosure Speaker name: Thomas Zeller... I have the following potential conflicts of interest to report: X X
The ZILVERPASS study a randomized study comparing ZILVER PTX stenting with Bypass in femoropopliteal lesions Preliminary report
 The ZILVERPASS study a randomized study comparing ZILVER PTX stenting with Bypass in femoropopliteal lesions Preliminary report G. Biro, M. Bosiers on behalf of ZILVERPASS Study Group Disclosure Speaker
The ZILVERPASS study a randomized study comparing ZILVER PTX stenting with Bypass in femoropopliteal lesions Preliminary report G. Biro, M. Bosiers on behalf of ZILVERPASS Study Group Disclosure Speaker
Atherectomy: Jetstream and Directional. George S. Chrysant, M.D.
 Atherectomy: Jetstream and Directional George S. Chrysant, M.D. Disclosures Abbott Vascular: MAB, consultant, proctor Abiomed: consultant Boston Scientific: MAB, consultant, proctor Medicines Company:
Atherectomy: Jetstream and Directional George S. Chrysant, M.D. Disclosures Abbott Vascular: MAB, consultant, proctor Abiomed: consultant Boston Scientific: MAB, consultant, proctor Medicines Company:
The Lutonix BTK Clinical Trial Programme: Status Update and Real World Clinical Experience
 The Lutonix BTK Clinical Trial Programme: Status Update and Real World Clinical Experience Dierk Scheinert, MD University Hospital Leipzig Leipzig, Germany Disclosure Speaker name: Dierk Scheinert I have
The Lutonix BTK Clinical Trial Programme: Status Update and Real World Clinical Experience Dierk Scheinert, MD University Hospital Leipzig Leipzig, Germany Disclosure Speaker name: Dierk Scheinert I have
The latest evidences from the DES trials in peripheral arterial disease
 The latest evidences from the DES trials in peripheral arterial disease Michael D. Dake, MD Thelma and Henry Doelger Professor Stanford University School of Medicine Disclosure Speaker name: Michael D.
The latest evidences from the DES trials in peripheral arterial disease Michael D. Dake, MD Thelma and Henry Doelger Professor Stanford University School of Medicine Disclosure Speaker name: Michael D.
Are RCT always needed: Experience with objective performance criteria (OPC)
") Are RCT always needed: Experience with objective performance criteria (OPC) Peter A. Schneider, MD Krishna Rocha-Singh, MD Kaiser Foundation Hospital Honolulu, Hawaii Prarie Heart Institute Springfield,
Are RCT always needed: Experience with objective performance criteria (OPC) Peter A. Schneider, MD Krishna Rocha-Singh, MD Kaiser Foundation Hospital Honolulu, Hawaii Prarie Heart Institute Springfield,
BioMimics 3D in my Clinical Practice
 BioMimics 3D in my Clinical Practice M Lichtenberg M.D. Vascular Centre Arnsberg / German Venous Centre Arnsberg CAUTION: Investigational Device. Limited by Federal (or United States) Law to Investigational
BioMimics 3D in my Clinical Practice M Lichtenberg M.D. Vascular Centre Arnsberg / German Venous Centre Arnsberg CAUTION: Investigational Device. Limited by Federal (or United States) Law to Investigational
Are Drug-coated balloons Durable? Level 1 evidence review. Koen Keirse, MD Vascular Surgery, RZ Tienen Tienen, Belgium
 Are Drug-coated balloons Durable? Level 1 evidence review Koen Keirse, MD Vascular Surgery, RZ Tienen Tienen, Belgium Disclosure Speaker name: Koen Keirse, MD I have the following potential conflicts of
Are Drug-coated balloons Durable? Level 1 evidence review Koen Keirse, MD Vascular Surgery, RZ Tienen Tienen, Belgium Disclosure Speaker name: Koen Keirse, MD I have the following potential conflicts of
Nicolas W Shammas, MD, MS
 Rota%onal and Aspira%on Atherectomy in Trea%ng in- Stent Restenosis of Femoropopliteal Arteries: Final Results of the JETSTREAM- ISR Feasibility Study Nicolas W Shammas, MD, MS President and Research Director,
Rota%onal and Aspira%on Atherectomy in Trea%ng in- Stent Restenosis of Femoropopliteal Arteries: Final Results of the JETSTREAM- ISR Feasibility Study Nicolas W Shammas, MD, MS President and Research Director,
Evidence-Based Optimal Treatment for SFA Disease
 Evidence-Based Optimal Treatment for SFA Disease Endo first Don t burn surgical bridge Don t stent if possible Javairiah Fatima, MD Assistant Professor of Surgery Division of Vascular and Endovascular
Evidence-Based Optimal Treatment for SFA Disease Endo first Don t burn surgical bridge Don t stent if possible Javairiah Fatima, MD Assistant Professor of Surgery Division of Vascular and Endovascular
MICHAEL R. JAFF, DO MASSACHUSETTS, UNITED STATES. Medtronic Further. Together
 DRUG-COATED BALL0ON TREATMENT FOR PATIENTS WITH INTERMITTENT CLAUDICATION: INSIGHTS FROM THE IN.PACT GLOBAL FULL CLINICAL COHORT MICHAEL R. JAFF, DO MASSACHUSETTS, UNITED STATES Medtronic Further. Together
DRUG-COATED BALL0ON TREATMENT FOR PATIENTS WITH INTERMITTENT CLAUDICATION: INSIGHTS FROM THE IN.PACT GLOBAL FULL CLINICAL COHORT MICHAEL R. JAFF, DO MASSACHUSETTS, UNITED STATES Medtronic Further. Together
Surgical Bypass vs. Zilver PTX stent for long SFA lesions : Interim results of the ZilverPass Trial
 Surgical Bypass vs. Zilver PTX stent for long SFA lesions : Interim results of the ZilverPass Trial Dr. Koen Deloose Head of Vascular Surgery AZ Sint-Blasius Dendermonde Belgium Disclosure slide Speaker
Surgical Bypass vs. Zilver PTX stent for long SFA lesions : Interim results of the ZilverPass Trial Dr. Koen Deloose Head of Vascular Surgery AZ Sint-Blasius Dendermonde Belgium Disclosure slide Speaker
Importance of Thorough Vessel Preparation Followed By Anti- Restenotic Therapy: An Update from the DEFINITIVE AR Study
 Importance of Thorough Vessel Preparation Followed By Anti- Restenotic Therapy: An Update from the DEFINITIVE AR Study Gunnar Tepe, MD Romed Klinikum, Rosenheim, Germany On behalf of the DEFINITIVE AR
Importance of Thorough Vessel Preparation Followed By Anti- Restenotic Therapy: An Update from the DEFINITIVE AR Study Gunnar Tepe, MD Romed Klinikum, Rosenheim, Germany On behalf of the DEFINITIVE AR
Current Status of DCB Experience with Non- Femoropopliteal Applications (Dialysis, Tibial, Venous)
") Current Status of DCB Experience with Non- Femoropopliteal Applications (Dialysis, Tibial, Venous) Saher Sabri, MD University of Virginia Health System Charlottesville, Virginia Dialysis vascular access
Current Status of DCB Experience with Non- Femoropopliteal Applications (Dialysis, Tibial, Venous) Saher Sabri, MD University of Virginia Health System Charlottesville, Virginia Dialysis vascular access
REACT Treatment Rationale and Clinical Evidence. ICI Meeting 5th of December 2017
 REACT Treatment Rationale and Clinical Evidence ICI Meeting 5th of December 2017 The SFA is a challenging vessel to treat Shortening 23-25%1 Compression > 1kg2 Torsion 60 3 Bending 64 4 SFA, superficial
REACT Treatment Rationale and Clinical Evidence ICI Meeting 5th of December 2017 The SFA is a challenging vessel to treat Shortening 23-25%1 Compression > 1kg2 Torsion 60 3 Bending 64 4 SFA, superficial
Endovascular Therapy vs. Open Femoral Endarterectomy Rationale and Design of the Randomized PESTO Trial
 Endovascular Therapy vs. Open Femoral Endarterectomy Rationale and Design of the Randomized PESTO Trial Prof. Thomas Zeller, MD Department Angiology Clinic for Cardiology and Angiology II University Heart-Center
Endovascular Therapy vs. Open Femoral Endarterectomy Rationale and Design of the Randomized PESTO Trial Prof. Thomas Zeller, MD Department Angiology Clinic for Cardiology and Angiology II University Heart-Center
Patterns of Vessel Calcification and Clinical Relevance
 Patterns of Vessel Calcification and Clinical Relevance Michael R. Jaff, DO Paul and Phyllis Fireman Endowed Chair in Vascular Medicine Massachusetts General Hospital Professor of Medicine Harvard Medical
Patterns of Vessel Calcification and Clinical Relevance Michael R. Jaff, DO Paul and Phyllis Fireman Endowed Chair in Vascular Medicine Massachusetts General Hospital Professor of Medicine Harvard Medical
Contemporary use of DCBs, Ranger clinical trial and investigator sponsored research
 Contemporary use of DCBs, Ranger clinical trial and investigator sponsored research Dierk Scheinert, MD Division of Interventional Angiology University-Hospital, Leipzig, Germany IMPORTANT INFORMATION:
Contemporary use of DCBs, Ranger clinical trial and investigator sponsored research Dierk Scheinert, MD Division of Interventional Angiology University-Hospital, Leipzig, Germany IMPORTANT INFORMATION:
Disclosures. How many people have heard a talk on DCBs? By show of hands, how many people here have used a DCB?
 Disclosures Drug Coated Balloons: How they work and what s the evidence? Christopher D. Owens, MD, MSc UCSF vascular surgery I am paid to talk about peripheral interventional procedures by Medtronic and
Disclosures Drug Coated Balloons: How they work and what s the evidence? Christopher D. Owens, MD, MSc UCSF vascular surgery I am paid to talk about peripheral interventional procedures by Medtronic and
SFA CTO Lesion Management laser or directional atherectomy?
 SFA CTO Lesion Management laser or directional atherectomy? Kevin, Chung-Ho Hsu, M.D. Setion of Peripheral Vascular Disease, Division of Cardiology, China Medical University Hospital, Taichung, Taiwan
SFA CTO Lesion Management laser or directional atherectomy? Kevin, Chung-Ho Hsu, M.D. Setion of Peripheral Vascular Disease, Division of Cardiology, China Medical University Hospital, Taichung, Taiwan
ILLUMENATE Pivotal Stellarex DCB IDE Study 12-Month Results
 ILLUMENATE Pivotal Stellarex DCB IDE Study 12-Month Results Sean Lyden, MD On behalf of Co-PI Prakash Krishnan, MD and the ILLUMENATE Pivotal Investigators Cleveland Clinic Cleveland, Ohio Disclosure Statement
ILLUMENATE Pivotal Stellarex DCB IDE Study 12-Month Results Sean Lyden, MD On behalf of Co-PI Prakash Krishnan, MD and the ILLUMENATE Pivotal Investigators Cleveland Clinic Cleveland, Ohio Disclosure Statement
TOBA Trial 12 months Results
 Tack Optimized Balloon Angioplasty: TOBA Trial 12 months Results New Paradigm for Managing Post PTA Dissections Marc Bosiers, MD A.Z. St. Blasius Hospital, Belgium Disclosure Speaker name: Dr. Marc Bosiers
Tack Optimized Balloon Angioplasty: TOBA Trial 12 months Results New Paradigm for Managing Post PTA Dissections Marc Bosiers, MD A.Z. St. Blasius Hospital, Belgium Disclosure Speaker name: Dr. Marc Bosiers
The importance of scientific evidence. Prof. I. Baumgartner Head Clinical & Interventional Angiology University Hospital Bern
 The importance of scientific evidence Prof. I. Baumgartner Head Clinical & Interventional Angiology University Hospital Bern Disclosure Speaker name:...i. Baumgartner... I have the following potential
The importance of scientific evidence Prof. I. Baumgartner Head Clinical & Interventional Angiology University Hospital Bern Disclosure Speaker name:...i. Baumgartner... I have the following potential
John E. Campbell, MD Assistant Professor of Surgery and Medicine Department of Vascular Surgery West Virginia University, Charleston Division
 John E. Campbell, MD Assistant Professor of Surgery and Medicine Department of Vascular Surgery West Virginia University, Charleston Division John Campbell, MD For the 12 months preceding this CME activity,
John E. Campbell, MD Assistant Professor of Surgery and Medicine Department of Vascular Surgery West Virginia University, Charleston Division John Campbell, MD For the 12 months preceding this CME activity,
Hiroshi Ando, MD Kasukabe Chuo General Hospital Saitama, Japan
 Hiroshi Ando, MD Kasukabe Chuo General Hospital Saitama, Japan Disclosure Hiroshi Ando, MD Kasukabe Chuo General Hospital I have the following potential conflicts of interest to report: Consulting Employment
Hiroshi Ando, MD Kasukabe Chuo General Hospital Saitama, Japan Disclosure Hiroshi Ando, MD Kasukabe Chuo General Hospital I have the following potential conflicts of interest to report: Consulting Employment
Long-term results with interwoven nitinol stents vs. BMS vs. DCB
 Long-term results with interwoven nitinol stents vs. BMS vs. DCB Dierk Scheinert, MD Division of Interventional Angiology University Hospital Leipzig, Germany Disclosure Advisory Board /Consultant: Abbott,
Long-term results with interwoven nitinol stents vs. BMS vs. DCB Dierk Scheinert, MD Division of Interventional Angiology University Hospital Leipzig, Germany Disclosure Advisory Board /Consultant: Abbott,
Directional Atherectomy and Gender Outcomes in DEFINTIVE LE
 Directional Atherectomy and Gender Outcomes in DEFINTIVE LE Lawrence A. Garcia MD, on behalf of the DEFINITIVE LE Investigators Chief, Section Interventional Cardiology St. Elizabeth s Medical Center,
Directional Atherectomy and Gender Outcomes in DEFINTIVE LE Lawrence A. Garcia MD, on behalf of the DEFINITIVE LE Investigators Chief, Section Interventional Cardiology St. Elizabeth s Medical Center,
Alternative concepts for drug delivery in BTK arteries the LIMBO project
 Alternative concepts for drug delivery in BTK arteries the LIMBO project Dierk Scheinert, MD Division of Interventional Angiology University Hospital Leipzig, Germany 1 Disclosure Speaker s name: Dierk
Alternative concepts for drug delivery in BTK arteries the LIMBO project Dierk Scheinert, MD Division of Interventional Angiology University Hospital Leipzig, Germany 1 Disclosure Speaker s name: Dierk
PHARMACOLOGICAL TREATMENT OF ARTERIAL RESTENOSIS
 PHARMACOLOGICAL TREATMENT OF ARTERIAL RESTENOSIS PACLITAXEL VS RAPAMYCIN Paclitaxel essentially freezes the microtubules that are in place during cell division. The cells cannot complete cell division
PHARMACOLOGICAL TREATMENT OF ARTERIAL RESTENOSIS PACLITAXEL VS RAPAMYCIN Paclitaxel essentially freezes the microtubules that are in place during cell division. The cells cannot complete cell division
6-month 0utcomes of a Novel Sirolimus Coated DCB Technology Evaluated in SFA Thomas Zeller, MD University Heart Center Freiburg-Bad Krozingen
 First Report of the SELUTION Trial: 6-month 0utcomes of a Novel Sirolimus Coated DCB Technology Evaluated in SFA Thomas Zeller, MD University Heart Center Freiburg-Bad Krozingen On behalf of the SELUTION
First Report of the SELUTION Trial: 6-month 0utcomes of a Novel Sirolimus Coated DCB Technology Evaluated in SFA Thomas Zeller, MD University Heart Center Freiburg-Bad Krozingen On behalf of the SELUTION
Interventional Radiology in Peripheral Vascular Disease: How Far Can We Go? Dr. L. F. CHENG Department of Radiology Princess Margaret Hospital
 Interventional Radiology in Peripheral Vascular Disease: How Far Can We Go? Dr. L. F. CHENG Department of Radiology Princess Margaret Hospital History The era of innovation in image-guided intervention
Interventional Radiology in Peripheral Vascular Disease: How Far Can We Go? Dr. L. F. CHENG Department of Radiology Princess Margaret Hospital History The era of innovation in image-guided intervention
ESVB State of the art: DES, DCB and the role of debulking. Gunnar Tepe, Rosenheim
 ESVB 2013 State of the art: DES, DCB and the role of debulking Gunnar Tepe, Rosenheim DES I Sirocco Sirolimus coating, quick release Duda et al., J Vasc Surg 2002; 106: 1505-1509 20 DES II Strides Everolimus
ESVB 2013 State of the art: DES, DCB and the role of debulking Gunnar Tepe, Rosenheim DES I Sirocco Sirolimus coating, quick release Duda et al., J Vasc Surg 2002; 106: 1505-1509 20 DES II Strides Everolimus