Contents: Benign Diseases of the Uterus
|
|
|
- Justin Terry
- 5 years ago
- Views:
Transcription

1 COLLEGE OF MEDICINE DEPT. OF OBSTETRICS AND GYNECOLOGY Benign Diseases of the Uterus Dr.Ayman Hussien Shaamash MBBCH, MSc., MD. (Egypt) Professor of OB./Gyn. Faculty of Medicine. King khalid University 1 Contents: Congenital Anomalies Uterine Polypi Adenomyosis Uterine Fibroids Endometriosis 2 1
 or unicornuate uterus Fusion: [lateral fusion ] the lower segments of the paired müllerian ducts fuse to form the uterus,")
2 I- Congenital Anomalies The Complete formation and differentiation of the müllerian ducts depend on completion of 3 phases of development as follows: Organogenesis: One or both müllerian ducts may not develop fully, resulting in uterine agenesis or hypoplasia (bilateral) or unicornuate uterus Fusion: [lateral fusion ] the lower segments of the paired müllerian ducts fuse to form the uterus, cervix, and upper vagina. Failure of fusion results in anomalies such as bicornuate or didelphys uterus. [Vertical fusion] : fusion of the ascending sinovaginal bulb with the descending müllerian system forms a normal patent vagina, while incomplete vertical fusion results in an imperforate hymen or septum. Septal resorption: After fusion, a central septum is present, is resorbed to form a single uterine cavity and cervix. Failure of resorption is the 3 cause of septate uterus. The 3 phases of Mullerian Development 4 2
3 Prevalence of Mullerian Anomalies Müllerian duct anomalies are estimated to occur in 0.5-3% of women. The true prevalence is unknown because the anomalies usually are discovered in patients presenting with infertility. Full-term pregnancies have occurred in patients with forms of bicornuate, septate, or didelphys uteri; therefore, true prevalence may be slightly higher than currently estimated
4 Morbidity of Mullerian Anomalies Patients with müllerian duct anomalies have a higher incidence of infertility, repeated first-trimester spontaneous abortions, fetal intrauterine growth retardation, fetal malposition, preterm labor, and retained placenta Certain types of the anomaly can increase morbidity, such as in patients with obstructed or partially obstructed müllerian systems who present with hematosalpinx, hematocolpos, retrograde menses, and endometriosis In addition, a fairly high association exists between müllerian duct anomalies and renal anomalies such as unilateral agenesis 7 Diagnosis of Mullerian Anomalies History Clinical Examination Investigation: 1- HSG 2-3 D U/S 2- Laparoscopy 4-Hysteroscopy 5- MRI 8 4



5 9 3 Ds U/S Vs MRI for Mullerian Anomalies 10 5
6 Bicornuate VS Spetate The role of reconstructive surgery is difficult to assess esp in infertility Consideration should be confined to women with recurrent pregnancy loss * cerclage *Hysteroscopic resection of the septum *? Metroplasty 11 II- Endometrial Polypi Is the most common endometrial benign tumor at any age especially at premenopausal time Presentation: - Irregular bleeding - Menorrhagia - Protrusion through the cervix 12 6




7 Diagnosis; TVUS show very thick endometrium /Saline sonohysterogram Diagnostic hysteroscopy Treatment D&C and using polyp forcepes Or hysteroscopic resection 13 III- Adenomyosis Invasion of endometrial glands and stroma into myometrium Adenomyosis is thought to affect 1% of women and is typically diagnosed in the 4th and 5th decades of life The aetiology is unclear, and until recently a diagnosis was made only after invasive and Hysterectomy 14 7




8 Adenomyosis cont. The cause of is unknown, it has been associated with any sort of uterine trauma that may break the barrier between the endometrium and myometrium, such as C.S, D& C, Pregnancy, 15 Adenomyosis cont. Symptoms and Signs Menorrhagia,Dysmenorrhoea On exam : Symmetrical a asymmetrical enlarged tender uterus Diagnosis Ultrasound, MRI Treatment: -Hysterectomy is definitive - NSAI/ progestins 8 16
9 III- LEIOMYOMATA (FIBROIDS) Epidemiology - Diagnosed in approximately 40-50% of reproductive age women >35 years - More common, larger, and occur at earlier age in black women - Most common indication for major surgery in females - Minimal malignant potential (1:1000) - Tend to regress after menopause 17 Pathogenesis arise from smooth muscle (Estrogen stimulates monoclonal- proliferation starts from a single cell) and Progesterone inhibits apoptosisis most responsible for fibroid growth. Degenerative changes(if tumour outgrows blood supply) Hyaline degeneration (most common degenerative change) Cystic degeneration (from breakdown of hyaline) Red degeneration (hemorrhage into tumour, may occur with pregnancy) Fatty degeneration Calcification Sarcomatous degeneration (extremely rare) parasitic myoma - tumour becomes attached to omentum or small bowel mesentery, develops new blood supply, and loses connection to uterus 18 9
 pelvic pressure/heaviness increased abdominal girth urinary frequency and urgency acute urinary")
 constipation, bloating (rare) 3- Acute pelvic pain if: fibroid degeneration fibroid torsion (subserosal pedunculated) 4-")
10 Clinical Features Majority asymptomatic (60%), often discovered on TVS 1- abnormal uterine bleeding (30%) Dysmenorrhea, menorrhagia 2- Pressure/bulk symptoms (20-50%) pelvic pressure/heaviness increased abdominal girth urinary frequency and urgency acute urinary retention (rare but surgical emergency!) constipation, bloating (rare) 3- Acute pelvic pain if: fibroid degeneration fibroid torsion (subserosal pedunculated) 4- infertility (submucosal) 5-Pregnancy complications and difficult C-section 19 Types / Location: 20 10


11 Diagnosis 1. Pelvic / abdominal exam 2. Ultrasound / saline sonohysterography 3. Laparoscopy 4. MRI / CT scan 5. Rule out endometrial pathology 21 Pelvic / abdominal exam 22 11

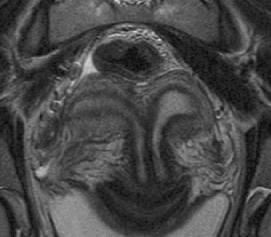
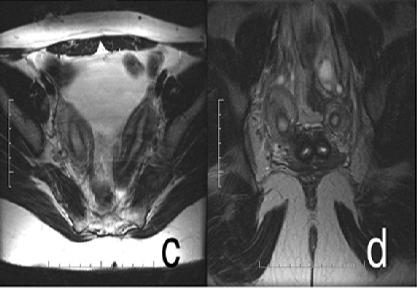
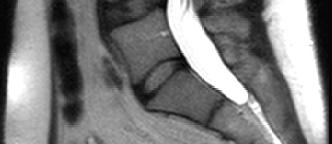
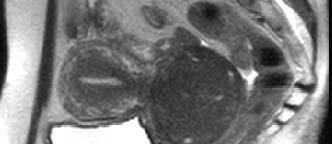
12 LAPAROSCOPY 23 MRI of Uterine Fibroid 24 12
 virtually all postmenopausal patients fall into this category (no increase in size or")
13 MRI of Uterine Fibroid 25 Treatment of fibroids Only if symptomatic, rapidly enlarging, or menorrhagia ( treat anemia if present) I- Conservative approach (watch and wait) if symptoms absent or minimal fibroids <6-8 em or stable in size not submucosal (submucosal fibroids are more likely to be symptomatic) virtually all postmenopausal patients fall into this category (no increase in size or bleeding) 26 13
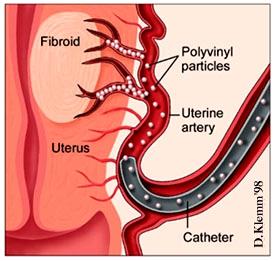
14 Treatment of fibroids cont. II-Medical approach Antiprostaglandins (ibuprofen) Tranexamic acid (Cyklokapron ) OCP/Depo-Provera GnRH agonist - leuprolide (Lupron@), or Androgen derivative danazol (Danocrine ). Short-term use only (6 months). Often used pre-myomectomy to facilitate surgery (reduces fibroid size) Selective progesterone receptor modulators -- currently in clinical trials. Prototype is RU486 which reduces fibroid volume by 50% after 3 months without side effects of GnRH agonists 27 Treatment of fibroids cont. III- Interventional radiology approach uterine artery embolization occludes both uterine arteries. Shrinks fibroids by 50% at 6 months. Improves menorrhagia in 70-90% within 1-2 months (not an option in women considering childbearing)) 28 14

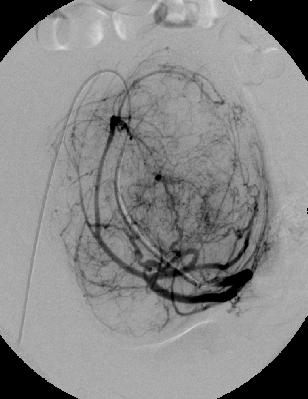

15 Uterine Artery Embolization 29 Pre Post 30 15




16 Pre Post 31 Uterine Fibroid Embolization (UFE) 32 16
17 Advantages of UFE Minimally invasive, complications rare Treats all fibroids simultaneously low recurrence rate Short recovery period No blood loss Avoids general anesthesia Preserves uterus 33 Limitations &Complications ONLY for interstitial myoma NOT for very huge myoma NOT for women desire fertility NOT if malignancy is suspected Very rarely uterine necrosis Very rarely ovarian failure 34 17
18 Myomectomy IV- Surgical approach Myomectomy (hysteroscopic, transabdominal or laparoscopic approach) preserves childbearing capabilities Hysterectomy (abdominal or vaginal, depending on fibroid size) Avoid operating on fibroids during pregnancy (due to +++ vascularity); expectant management only 35 Myomectomy 36 18
19 IV-Endometriosis Etiology Not fully understood Proposed mechanisms (combination likely involved) 1. Retrograde menstruation theory of Sampson transtubal regurgitation during menstruation endometrial cells most often found in dependent sites of the pelvis 2. immunologic theory - altered immunity may limit clearance of transplanted endometrial cells from pelvic cavity (~ NK cell activity?) 3. Metaplasia of coelomic epithelium undefined endogenous biochemical factor may induce undifferentiated peritoneal cells to develop into endometrial tissue 4. Lymphatic flow from uterus to ovary may lead to ovarian endometriosis 5. Extrapelvic disease : due to vascular or lymphatic dissemination of cells 37 Endometriosis cont. Epidemiology Incidence: 15-30% of premenopausal women Mean age at presentation: years Regresses after menopause Risk Factors Family history (7-10 fold increased risk if affected 1st degree relative) Obstructive anomalies of the genital tract (earlier onset) Nulliparity Age >25 years 38 19
20 Endometriosis cont. Frequency Endometriosis occurs in 7-10% of women in the general population Endometriosis has a prevalence rate of 20-50% in infertile women And as high as 80% in women with chronic pelvic pain Evidence of endometriosis was found during laparoscopy in 20-50% of asymptomatic women 39 Endometriosis cont. Sites of Occurrence Ovaries - 60% patients have ovarian involvement Broad ligament Peritoneal surface of the cul-de-sac (uterosacral ligaments) Rectosigmoid colon Appendix 40 20


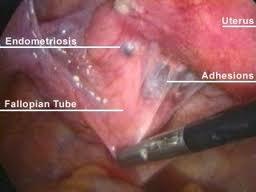

21 Ovarian Endometriosis (Endometrioma) 41 Peritoneal Endometriosis 42 21
22 Clinical Features My be asymptomatic Cyclic symptoms due to swelling and bleeding of ectopic endometrium, secondary dysmenorrhea deep dyspareunia sacral backache with menses pain may become constant but remains worse perimenstrually Premenstrual and postrnenstrual spotting Infertility 30-40% of patients with endometriosis will be infertile 15-30% of those who are infertile will have endometriosis Bowel and bladder symptoms Frequency, dysuna, hematuria Diarrhea, constipation, hematochezia, dyschezia Tender nodularity of uterine ligaments and cul-de-sac Fixed retroversion of uterus Firm, fixed adnexal mass (endometrioma) 43 Endometriosis cont. Investigations: definitive diagnosis requires direct visualization of lesions typical at laparoscopy biopsy and histologic exam of specimens LAPAROSCOPY dark blue or brownish-black implants on the uterosacral ligaments, cul-de-sac, or anywhere in the pelvis endometrioma: chocolate cysts in the ovaries "powder-bum" lesions on the peritoneal surface early white lesions and blebs CA-125 may be used as marker of response to medical therapy 22 44
23 Grading of Endometriosis (American Society of Reproductive Medicine) It Takes into account: 1- Location: peritoneal,ovarian and DP 2-Size:<1 cm,1-3 cm and > 3cm 3-Infilteration:Superficial and Deep 4-Adhesion:filmy or dense- extent : (< 1/3,2/3 or >2/3 of pelvis ) 45 Laparoscopic Staging: Stage Stage Stage Stage I: Minimal (1-5 points) II: Mild (6-15 points) III: Moderate (16-40 points) IV: Severe (> 40 points) 46 23
24 Endometriosis cont. Treatment depends on the severity of symptoms, extent of disease, desire for future fertility, and threat to GI/GU systems Medical NSAIDs (e.g, naproxen sodium) 2-pseudopregnancy cyclic/continuous estrogen-progestin (OCP) medroxyprogesterone (Depo-Provera ) 3- pseudomenopause [2nd line: only short-term «6 months) due to osteoporotic potential with prolonged use] danazol (Danocrine ) side effects:weight gain,fluid retention, acne, hirsutism,voice change GnRH agonist (suppresses pituitary GnRH leuprolide (Lupron ) =) - side effects: hot flashes, vaginal dryness, reduced libido - can use up to 12 months with add-back progestin or estrogen 1-47 Endometriosis cont. Surgical Laparoscopy using laser, electrocautery ablation/resection of implants, lysis of adhesions, ovarian cystectomy of endometriomas ± laparotomy for cytoreduction of pelvic endometriosis ± follow-up with medical treatment for pain control NOT fertility Radical surgery This involves total hysterectomy with bilateral oophorectomy and cytoreduction of visible endometriosis 48 24
25 49 25
Endometriosis د. نجمه محمود كلية الطب جامعة بغداد فرع النسائية والتوليد
 Endometriosis د. نجمه محمود كلية الطب جامعة بغداد فرع النسائية والتوليد Objectives:- To know what is endometriosis The sites where it occur To explain its itiology & pathogenesis To know the clinical features
Endometriosis د. نجمه محمود كلية الطب جامعة بغداد فرع النسائية والتوليد Objectives:- To know what is endometriosis The sites where it occur To explain its itiology & pathogenesis To know the clinical features
Endometriosis. Assoc.Prof.Pawin Puapornpong, Faculty of Medicine, Srinakharinwirot University.
 Endometriosis Assoc.Prof.Pawin Puapornpong, Faculty of Medicine, Srinakharinwirot University. Endometriosis Definition: Ectopic Endometrial Tissue True Incidence Unknown:? 1-5% Does NOT Discriminate by
Endometriosis Assoc.Prof.Pawin Puapornpong, Faculty of Medicine, Srinakharinwirot University. Endometriosis Definition: Ectopic Endometrial Tissue True Incidence Unknown:? 1-5% Does NOT Discriminate by
Definition Endometriosis is the presence of functioning endometrial tissue outside the cavity of the uterus.
 Dept. of Obstetrics t and Gynecology Faculty of Medicine University of Sumatera Utara Endometriosis Definition Endometriosis is the presence of functioning endometrial tissue outside the cavity of the
Dept. of Obstetrics t and Gynecology Faculty of Medicine University of Sumatera Utara Endometriosis Definition Endometriosis is the presence of functioning endometrial tissue outside the cavity of the
CLEAR COVERAGE HYSTERECTOMY CHECKLISTS
 CLEAR COVERAGE HYSTERECTOMY CHECKLISTS Click on the link below to access the checklist sheet. Abnormal Uterine Bleeding Adenomyosis Chronic Abdominal or Pelvic Pain Endometriosis Fibroids General Guidelines
CLEAR COVERAGE HYSTERECTOMY CHECKLISTS Click on the link below to access the checklist sheet. Abnormal Uterine Bleeding Adenomyosis Chronic Abdominal or Pelvic Pain Endometriosis Fibroids General Guidelines
Grand Rounds Mullerian Anomalies. Sara Schaenzer, PGY-3 9/26/18
 Grand Rounds Mullerian Anomalies Sara Schaenzer, PGY-3 9/26/18 Background Congenital uterine anomalies occur in 2-4% of women Three times more common in women with recurrent pregnancy loss True incidence
Grand Rounds Mullerian Anomalies Sara Schaenzer, PGY-3 9/26/18 Background Congenital uterine anomalies occur in 2-4% of women Three times more common in women with recurrent pregnancy loss True incidence
Sexual differentiation:
 Abnormal Development of Female Genitalia Dr. Maryam Fetal development of gonads, external genitalia, Mullerian ducts and Wolffian ducts can be disrupted at a variety of points, leading to a wide range
Abnormal Development of Female Genitalia Dr. Maryam Fetal development of gonads, external genitalia, Mullerian ducts and Wolffian ducts can be disrupted at a variety of points, leading to a wide range
MYOMA of UTERUS. By Zhengyu Li M.D. GYN/OB Department West China Second Univ. Hospital, S.U.
 MYOMA of UTERUS By Zhengyu Li M.D GYN/OB Department West China Second Univ. Hospital, S.U. zhengyuli@scu.edu.cn General Consideration Benign neoplasms composed primarily of smooth muscle. Most common solid
MYOMA of UTERUS By Zhengyu Li M.D GYN/OB Department West China Second Univ. Hospital, S.U. zhengyuli@scu.edu.cn General Consideration Benign neoplasms composed primarily of smooth muscle. Most common solid
Fibroid mapping. Haitham Hamoda MD FRCOG Consultant Gynaecologist, Subspecialist in Reproductive Medicine & Surgery King s College Hospital
 Fibroid mapping Haitham Hamoda MD FRCOG Consultant Gynaecologist, Subspecialist in Reproductive Medicine & Surgery King s College Hospital Fibroids Common condition >70% of women by onset of menopause.
Fibroid mapping Haitham Hamoda MD FRCOG Consultant Gynaecologist, Subspecialist in Reproductive Medicine & Surgery King s College Hospital Fibroids Common condition >70% of women by onset of menopause.
Endometriosis. *Chocolate cyst in the ovary
 Endometriosis What is endometriosis? Endometriosis is a common condition in young women. It's chronic, painful, and it often progressively gets worse over the time. *Chocolate cyst in the ovary Normally,
Endometriosis What is endometriosis? Endometriosis is a common condition in young women. It's chronic, painful, and it often progressively gets worse over the time. *Chocolate cyst in the ovary Normally,
Aulia Rahman, S. Ked Endang Sri Wahyuni, S. Ked Nova Faradilla, S. Ked
 Authors : Aulia Rahman, S. Ked Endang Sri Wahyuni, S. Ked Nova Faradilla, S. Ked Faculty of Medicine University of Riau Pekanbaru, Riau 2009 Files of DrsMed FK UR (http://www.files-of-drsmed.tk 0 INTTRODUCTION
Authors : Aulia Rahman, S. Ked Endang Sri Wahyuni, S. Ked Nova Faradilla, S. Ked Faculty of Medicine University of Riau Pekanbaru, Riau 2009 Files of DrsMed FK UR (http://www.files-of-drsmed.tk 0 INTTRODUCTION
PELVIC PAIN IN GYNECOLOGY
 PELVIC PAIN IN GYNECOLOGY Pelvic pain is an important part of clinical practice for who any clinician who provides health care for women. It can be acute, recurrent or chronic. Differential Diagnosis:
PELVIC PAIN IN GYNECOLOGY Pelvic pain is an important part of clinical practice for who any clinician who provides health care for women. It can be acute, recurrent or chronic. Differential Diagnosis:
Moneli Golara Consultant Obstetrician and Gynaecologist Barnet Hospital Royal Free NHS Trust
 Moneli Golara Consultant Obstetrician and Gynaecologist Barnet Hospital Royal Free NHS Trust Endometriosis one of the most common conditions requiring treatment Growth of endometrial like tissue outside
Moneli Golara Consultant Obstetrician and Gynaecologist Barnet Hospital Royal Free NHS Trust Endometriosis one of the most common conditions requiring treatment Growth of endometrial like tissue outside
ADENOMYOSIS CHRONIC PELVIC PAIN IN WOMEN IMAGING CHRONIC PELVIC PAIN IN WOMEN CHRONIC PELVIC PAIN IN WOMEN ADENOMYOSIS: PATHOLOGY ADENOMYOSIS
 CHRONIC PELVIC PAIN IN WOMEN IMAGING CHRONIC PELVIC PAIN IN WOMEN MOSTAFA ATRI, MD Dipl. Epid. UNIVERSITY OF TORONTO Non-menstrual pain of 6 months Prevalence 15%: 18-50 years of age 10-40% of gynecology
CHRONIC PELVIC PAIN IN WOMEN IMAGING CHRONIC PELVIC PAIN IN WOMEN MOSTAFA ATRI, MD Dipl. Epid. UNIVERSITY OF TORONTO Non-menstrual pain of 6 months Prevalence 15%: 18-50 years of age 10-40% of gynecology
Palm Beach Obstetrics & Gynecology, PA
 Palm Beach Obstetrics & Gynecology, PA 4671 S. Congress Avenue, Lake Worth, FL 33461 561.434.0111 4631 N. Congress Avenue, Suite 102, West Palm Beach, FL 33407 Endometriosis The lining of the uterus is
Palm Beach Obstetrics & Gynecology, PA 4671 S. Congress Avenue, Lake Worth, FL 33461 561.434.0111 4631 N. Congress Avenue, Suite 102, West Palm Beach, FL 33407 Endometriosis The lining of the uterus is
CNGOF Guidelines for the Management of Endometriosis
 CNGOF Guidelines for the Management of Endometriosis Anatomoclinical forms of endometriosis Definitions Endometriosis is defined as the presence of endometrial tissue containing both glands and stroma
CNGOF Guidelines for the Management of Endometriosis Anatomoclinical forms of endometriosis Definitions Endometriosis is defined as the presence of endometrial tissue containing both glands and stroma
CLINICAL PRESENTATION AND RADIOLOGY QUIZ QUESTION
 Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 2/12/2011 Radiology Quiz of the Week # 7 Page 1 CLINICAL PRESENTATION AND RADIOLOGY QUIZ
Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 2/12/2011 Radiology Quiz of the Week # 7 Page 1 CLINICAL PRESENTATION AND RADIOLOGY QUIZ
Dysmenorrhea. Erin Eppsteiner, M.D. Department of Ob/Gyn The University of Iowa Roy J & Lucille A Carver College of Medicine
 Dysmenorrhea Erin Eppsteiner, M.D. Department of Ob/Gyn The University of Iowa Roy J & Lucille A Carver College of Medicine Objectives Be able to recognize primary and secondary dysmenorrhea Be familiar
Dysmenorrhea Erin Eppsteiner, M.D. Department of Ob/Gyn The University of Iowa Roy J & Lucille A Carver College of Medicine Objectives Be able to recognize primary and secondary dysmenorrhea Be familiar
The many faces of Endometriosis
 The many faces of Endometriosis Beryl Benacerraf M.D Harvard Medical School What is Endometriosis? Endometriosis is defined as the presence of normal endometrial tissue occurring outside of the endometrial
The many faces of Endometriosis Beryl Benacerraf M.D Harvard Medical School What is Endometriosis? Endometriosis is defined as the presence of normal endometrial tissue occurring outside of the endometrial
Management of Gynae Problems in Primary Care David Griffiths FRCOG The Great Western Hospital Swindon. A brief overview
 Management of Gynae Problems in Primary Care David Griffiths FRCOG The Great Western Hospital Swindon A brief overview Pelvic Pain Challenge to the physician In UK 1 Million sufferers 20% of all gynae
Management of Gynae Problems in Primary Care David Griffiths FRCOG The Great Western Hospital Swindon A brief overview Pelvic Pain Challenge to the physician In UK 1 Million sufferers 20% of all gynae
Gynecologic Decision Making Based on Sonographic Findings
 Gynecologic Decision Making Based on Sonographic Findings Mindy Goldman, MD Department of Obstetrics & Gynecology & Vickie A. Feldstein, MD Department of Radiology University of California, San Francisco
Gynecologic Decision Making Based on Sonographic Findings Mindy Goldman, MD Department of Obstetrics & Gynecology & Vickie A. Feldstein, MD Department of Radiology University of California, San Francisco
Frequency of menses. Duration of menses 3 days to 7 days. Flow/amount of menses Average blood loss with menstruation is 60-80cc.
 Frequency of menses 24 days (0.5%) to 35 days (0.9%) Age 25, 40% are between 25 and 28 days Age 25-35, 60% are between 25 and 28 days Teens and women over 40 s cycles may be longer apart Duration of menses
Frequency of menses 24 days (0.5%) to 35 days (0.9%) Age 25, 40% are between 25 and 28 days Age 25-35, 60% are between 25 and 28 days Teens and women over 40 s cycles may be longer apart Duration of menses
Endometriosis. What you need to know. 139 Dumaresq Street Campbelltown Phone Fax
 Endometriosis What you need to know 139 Dumaresq Street Campbelltown Phone 4628 5292 Fax 4628 0349 www.nureva.com.au September 2015 What is Endometriosis? Endometriosis is a condition whereby the lining
Endometriosis What you need to know 139 Dumaresq Street Campbelltown Phone 4628 5292 Fax 4628 0349 www.nureva.com.au September 2015 What is Endometriosis? Endometriosis is a condition whereby the lining
Difference Between PCOS and Endometriosis
 Difference Between PCOS and Endometriosis www.differencebetween.com Key Difference PCOS vs Endometriosis Ovaries play an important role in the reproduction and the maintenance of the female body. They
Difference Between PCOS and Endometriosis www.differencebetween.com Key Difference PCOS vs Endometriosis Ovaries play an important role in the reproduction and the maintenance of the female body. They
Endometriosis BRADEN COLEMAN, MD PGY-3
 Endometriosis BRADEN COLEMAN, MD PGY-3 Case 1: 30 y/o F PMH Borderline personality disorder, anxiety, depression, presents with complaints of LLQ abdominal pain and palpable abdominal nodules. She reports
Endometriosis BRADEN COLEMAN, MD PGY-3 Case 1: 30 y/o F PMH Borderline personality disorder, anxiety, depression, presents with complaints of LLQ abdominal pain and palpable abdominal nodules. She reports
Freedom of Information
 ND ref. FOI/16/309 Freedom of Information Thank you for your 19/10/16 request for the following information: Under the Freedom of Information Act, please could you fill out the following Freedom of Information
ND ref. FOI/16/309 Freedom of Information Thank you for your 19/10/16 request for the following information: Under the Freedom of Information Act, please could you fill out the following Freedom of Information
Chapter 100 Gynecologic Disorders
 Chapter 100 Gynecologic Disorders Episode Overview: 1. Describe the presentation and RF for Adnexal torsion 2. List the imaging findings of adnexal torsion (US vs CT) 3. What is the management of adnexal
Chapter 100 Gynecologic Disorders Episode Overview: 1. Describe the presentation and RF for Adnexal torsion 2. List the imaging findings of adnexal torsion (US vs CT) 3. What is the management of adnexal
Ovaries: In Sickness and Health. Mr N Pisal Consultant Gynaecologist The Portland Hospital
 Ovaries: In Sickness and Health Mr N Pisal Consultant Gynaecologist The Portland Hospital Topics for discussion How to assess ovarian function? AMH PCOS Ovarian pain Ovarian cysts Ovarian screening Menopause
Ovaries: In Sickness and Health Mr N Pisal Consultant Gynaecologist The Portland Hospital Topics for discussion How to assess ovarian function? AMH PCOS Ovarian pain Ovarian cysts Ovarian screening Menopause
Pelvic Pain: Diagnosis and Management
 Pelvic Pain: Diagnosis and Management Mr N Pisal Consultant Gynaecologist Advanced Laparoscopic Surgeon www.london-gynaecology.com History LMP Dysmenorrhoea / Dyspareunia Cyclical pain related to menstrual
Pelvic Pain: Diagnosis and Management Mr N Pisal Consultant Gynaecologist Advanced Laparoscopic Surgeon www.london-gynaecology.com History LMP Dysmenorrhoea / Dyspareunia Cyclical pain related to menstrual
My Patient Has Pelvic Pain. David A. Kenny DO
 My Patient Has Pelvic Pain David A. Kenny DO Definition Of apparent pelvic origin Present most of the time for at least six months Severe enough to cause functional disability Requiring surgical or medical
My Patient Has Pelvic Pain David A. Kenny DO Definition Of apparent pelvic origin Present most of the time for at least six months Severe enough to cause functional disability Requiring surgical or medical
2/24/19. Myometrial evaluation. Size Echotexture. Homogeneous Heterogeneous. Adenomyosis Fibroids. Adenomyosis. MUSA guidelines
 Content Adenomyosis and MUSA guidelines for myometrial disorders Adenomyosis MUSA guidelines Dr Lufee Wong FRANZCOG, MPH, DDU Recommended reporting guidelines Fibroids Adenomyosis Myometrial evaluation
Content Adenomyosis and MUSA guidelines for myometrial disorders Adenomyosis MUSA guidelines Dr Lufee Wong FRANZCOG, MPH, DDU Recommended reporting guidelines Fibroids Adenomyosis Myometrial evaluation
Modern Management of Fibroids
 Modern Management of Fibroids Mr Narendra Pisal The Portland Hospital Fibroids Very common 20-40% of all women Up to 80% of black women by 50y Most fibroids are asymptomatic 50% will have significant symptoms
Modern Management of Fibroids Mr Narendra Pisal The Portland Hospital Fibroids Very common 20-40% of all women Up to 80% of black women by 50y Most fibroids are asymptomatic 50% will have significant symptoms
Dysmenorrhoea Gynaecology د.شيماءعبداالميرالجميلي. Aetiology of secondary dysmenorrhea
 30-11-2014 Gynaecology Dysmenorrhoea د.شيماءعبداالميرالجميلي Dysmenorrhoea is defined as painful menstruation. It is experienced by 45 95 per cent of women of reproductive age.primary Spasmodic Dysmenorrhea
30-11-2014 Gynaecology Dysmenorrhoea د.شيماءعبداالميرالجميلي Dysmenorrhoea is defined as painful menstruation. It is experienced by 45 95 per cent of women of reproductive age.primary Spasmodic Dysmenorrhea
Log Title: OBRES Gynecologic Case Log
 Log Title: OBRES Gynecologic Case Log Hospital/Institution: (Lookup) Attending Physician (Lookup) Is Patient Pregnant? ( Y or N) MEDRECNO: (text) Date (encounter) (Date) Diagnosis DX GYN Acute Pelvic Pain
Log Title: OBRES Gynecologic Case Log Hospital/Institution: (Lookup) Attending Physician (Lookup) Is Patient Pregnant? ( Y or N) MEDRECNO: (text) Date (encounter) (Date) Diagnosis DX GYN Acute Pelvic Pain
Pelvic Pain: Overlooked
 EDUCATION EXHIBIT 3 Pelvic Pain: Overlooked and Underdiagnosed Gynecologic Conditions 1 CME FEATURE See accompanying test at http:// www.rsna.org /education /rg_cme.html LEARNING OBJECTIVES FOR TEST 1
EDUCATION EXHIBIT 3 Pelvic Pain: Overlooked and Underdiagnosed Gynecologic Conditions 1 CME FEATURE See accompanying test at http:// www.rsna.org /education /rg_cme.html LEARNING OBJECTIVES FOR TEST 1
Endometriosis. A Guide for Patients PATIENT INFORMATION SERIES
 Endometriosis A Guide for Patients PATIENT INFORMATION SERIES Published by the American Society for Reproductive Medicine under the direction of the Patient Education Committee and the Publications Committee.
Endometriosis A Guide for Patients PATIENT INFORMATION SERIES Published by the American Society for Reproductive Medicine under the direction of the Patient Education Committee and the Publications Committee.
 1 2 Infertile women are seven to ten times more likely to have endometriosis than their fertile 3 The mechanism by which endometriosis develops is unknown Theories for the histogenesis of endometriosis
1 2 Infertile women are seven to ten times more likely to have endometriosis than their fertile 3 The mechanism by which endometriosis develops is unknown Theories for the histogenesis of endometriosis
What is endometrial cancer?
 Uterine cancer What is endometrial cancer? Endometrial cancer is the growth of abnormal cells in the lining of the uterus. The lining is called the endometrium. Endometrial cancer usually occurs in women
Uterine cancer What is endometrial cancer? Endometrial cancer is the growth of abnormal cells in the lining of the uterus. The lining is called the endometrium. Endometrial cancer usually occurs in women
Laparoscopy and Hysteroscopy
 AMERICAN SOCIETY FOR REPRODUCTIVE MEDICINE Laparoscopy and Hysteroscopy A Guide for Patients PATIENT INFORMATION SERIES Published by the American Society for Reproductive Medicine under the direction of
AMERICAN SOCIETY FOR REPRODUCTIVE MEDICINE Laparoscopy and Hysteroscopy A Guide for Patients PATIENT INFORMATION SERIES Published by the American Society for Reproductive Medicine under the direction of
Normal and Abnormal Development of the Genital Tract. Dr.Raghad Abdul-Halim
 Normal and Abnormal Development of the Genital Tract Dr.Raghad Abdul-Halim objectives: Revision of embryology. Clinical presentation, investigations and clinical significance of most common developmental
Normal and Abnormal Development of the Genital Tract Dr.Raghad Abdul-Halim objectives: Revision of embryology. Clinical presentation, investigations and clinical significance of most common developmental
Endometrial Stromal Sarcoma
 May 26, 2011 By Sushila Ladumor, MD [1] Endometrial stromal sarcoma (ESS) is a rare malignant tumor of the endometrium, occurring in the age group of 40-50 years. History The 50-year-old, female patient
May 26, 2011 By Sushila Ladumor, MD [1] Endometrial stromal sarcoma (ESS) is a rare malignant tumor of the endometrium, occurring in the age group of 40-50 years. History The 50-year-old, female patient
MANAGEMENT OF REFRACTORY ENDOMETRIOSIS
 (339) MANAGEMENT OF REFRACTORY ENDOMETRIOSIS Serdar Bulun, MD JJ Sciarra Professor and Chair Department of Ob/Gyn Northwestern University ENDOMETRIOSIS OCs Teenager: severe dysmenorrhea often starting
(339) MANAGEMENT OF REFRACTORY ENDOMETRIOSIS Serdar Bulun, MD JJ Sciarra Professor and Chair Department of Ob/Gyn Northwestern University ENDOMETRIOSIS OCs Teenager: severe dysmenorrhea often starting
Endometriosis - MRI findings with anatomic-pathologic correlation
 Endometriosis - MRI findings with anatomic-pathologic correlation Poster No.: C-2551 Congress: ECR 2015 Type: Educational Exhibit Authors: E. Matos, A. T. Almeida, A. Sanches; Vila Nova de Gaia/PT Keywords:
Endometriosis - MRI findings with anatomic-pathologic correlation Poster No.: C-2551 Congress: ECR 2015 Type: Educational Exhibit Authors: E. Matos, A. T. Almeida, A. Sanches; Vila Nova de Gaia/PT Keywords:
Introduction to GYN Specialties
 Outline Introduction to GYN Specialties Gynecologic Oncology* Female Pelvic Medicine and Reconstructive Surgery* Reproductive Endocrinology and Infertility* Pediatric and Adolescent Gynecology** Family
Outline Introduction to GYN Specialties Gynecologic Oncology* Female Pelvic Medicine and Reconstructive Surgery* Reproductive Endocrinology and Infertility* Pediatric and Adolescent Gynecology** Family
MPH Quiz. 1. How many primaries are present based on this pathology report? 2. What rule is this based on?
 MPH Quiz Case 1 Surgical Pathology from hysterectomy performed July 11, 2007 Final Diagnosis: Uterus, resection: Endometrioid adenocarcinoma, Grade 1 involving most of endometrium, myometrial invasion
MPH Quiz Case 1 Surgical Pathology from hysterectomy performed July 11, 2007 Final Diagnosis: Uterus, resection: Endometrioid adenocarcinoma, Grade 1 involving most of endometrium, myometrial invasion
Pelvic Pain/Endometriosis Year 3 Updated April 2017 By Dr. J. N. Kirby
 Pelvic Pain/Endometriosis Year 3 Updated April 2017 By Dr. J. N. Kirby Objectives (At the end of this session ) Causes of acute and chronic pelvic pain will be more clear to you Investigations to determine
Pelvic Pain/Endometriosis Year 3 Updated April 2017 By Dr. J. N. Kirby Objectives (At the end of this session ) Causes of acute and chronic pelvic pain will be more clear to you Investigations to determine
CLINICAL PRESENTATION AND RADIOLOGY QUIZ QUESTION
 Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 8/20/2011 Radiology Quiz of the Week # 34 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 8/20/2011 Radiology Quiz of the Week # 34 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Laparoscopic Morcellation of Didelphic Uterus With Cervical and Renal Aplasia
 CASE REPORT Laparoscopic Morcellation of Didelphic Uterus With Cervical and Renal Aplasia Albert Altchek, MD, Michael Brodman, MD, Peter Schlosshauer, MD, Liane Deligdisch, MD ABSTRACT This is a case report
CASE REPORT Laparoscopic Morcellation of Didelphic Uterus With Cervical and Renal Aplasia Albert Altchek, MD, Michael Brodman, MD, Peter Schlosshauer, MD, Liane Deligdisch, MD ABSTRACT This is a case report
Dr Devashana Gupta. Repromed Auckland. 17:30-18:00 Fibroids, Endometriosis and DUB
 Dr Devashana Gupta Repromed Auckland 17:30-18:00 Fibroids, Endometriosis and DUB Fibroids, Endometriosis and AUB Dr Devashana Gupta 9 th June 2018 Abnormal uterine bleeding PALM-COEIN 3 What is abnormal
Dr Devashana Gupta Repromed Auckland 17:30-18:00 Fibroids, Endometriosis and DUB Fibroids, Endometriosis and AUB Dr Devashana Gupta 9 th June 2018 Abnormal uterine bleeding PALM-COEIN 3 What is abnormal
Endometriosis Information Leaflet
 Endometriosis Information Leaflet What is Endometriosis? Endometriosis is a condition where tissue similar to the lining of the womb (endometrium) is found outside the womb. About 1 out of 10 women of
Endometriosis Information Leaflet What is Endometriosis? Endometriosis is a condition where tissue similar to the lining of the womb (endometrium) is found outside the womb. About 1 out of 10 women of
Endometriosis. A Guide for Patients PATIENT INFORMATION SERIES
 Endometriosis A Guide for Patients PATIENT INFORMATION SERIES Published by the American Society for Reproductive Medicine under the direction of the Patient Education Committee and the Publications Committee.
Endometriosis A Guide for Patients PATIENT INFORMATION SERIES Published by the American Society for Reproductive Medicine under the direction of the Patient Education Committee and the Publications Committee.
Pelvic Pain. What you need to know. 139 Dumaresq Street Campbelltown Phone Fax
 Pelvic Pain What you need to know 139 Dumaresq Street Campbelltown Phone 4628 5292 Fax 4628 0349 www.nureva.com.au September 2015 PELVIC PAIN This is a common problem and most women experience some form
Pelvic Pain What you need to know 139 Dumaresq Street Campbelltown Phone 4628 5292 Fax 4628 0349 www.nureva.com.au September 2015 PELVIC PAIN This is a common problem and most women experience some form
Radiological assessment of infertility: A pictorial review
 Radiological assessment of infertility: A pictorial review Poster No.: C-1681 Congress: ECR 2015 Type: Educational Exhibit Authors: J. P. Walsh, N. Healy, M. O'sullivan, S. Harte, M. T. Knox; Dublin/ IE
Radiological assessment of infertility: A pictorial review Poster No.: C-1681 Congress: ECR 2015 Type: Educational Exhibit Authors: J. P. Walsh, N. Healy, M. O'sullivan, S. Harte, M. T. Knox; Dublin/ IE
5 Mousa Al-Abbadi. Ola Al-juneidi & Obada Zalat. Ahmad Al-Tarefe
 5 Mousa Al-Abbadi Ola Al-juneidi & Obada Zalat Ahmad Al-Tarefe Abnormal Uterine Bleeding (AUB) AUB is a very common scenario or symptom where women complain of menorrhagia (heavy and/or for long periods),
5 Mousa Al-Abbadi Ola Al-juneidi & Obada Zalat Ahmad Al-Tarefe Abnormal Uterine Bleeding (AUB) AUB is a very common scenario or symptom where women complain of menorrhagia (heavy and/or for long periods),
ORILISSA (elagolix) oral tablet
 oral tablet") ORILISSA (elagolix) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage
ORILISSA (elagolix) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage
General history. Basic Data : Age :62y/o Date of admitted: Married status : Married
 General history Basic Data : Age :62y/o Date of admitted:940510 Married status : Married General history Chief Complain : bilateral ovarian cyst incidentally being found out during pap smear. Present Illness
General history Basic Data : Age :62y/o Date of admitted:940510 Married status : Married General history Chief Complain : bilateral ovarian cyst incidentally being found out during pap smear. Present Illness
Endometriosis: An Overview
 Endometriosis: An Overview www.bcwomens.ca Welcome to the BC Women s Centre for Pelvic Pain and Endometriosis. This handout will give you some basic information about endometriosis. It will also explain
Endometriosis: An Overview www.bcwomens.ca Welcome to the BC Women s Centre for Pelvic Pain and Endometriosis. This handout will give you some basic information about endometriosis. It will also explain
Question Bank III - BHMS
 Question Bank III - BHMS Sub:- Ob/Gy -Paper-II 1. Give the definition of Puberty. 2. Enumerate five important physical changes evident during puberty. 3. Write down the vaginal changes during puberty.
Question Bank III - BHMS Sub:- Ob/Gy -Paper-II 1. Give the definition of Puberty. 2. Enumerate five important physical changes evident during puberty. 3. Write down the vaginal changes during puberty.
intractable dysmenorrhea are diagnosed with endometriosis. 5
 Endometriosis From Identification to Management Endometriosis, a gynecologic disorder that typically affects women of childbearing age, can result in dysmenorrhea, deep dyspareunia, chronic pelvic pain,
Endometriosis From Identification to Management Endometriosis, a gynecologic disorder that typically affects women of childbearing age, can result in dysmenorrhea, deep dyspareunia, chronic pelvic pain,
Endometrial line thickness in different conditions.
 Endometrial line thickness in different conditions 1 Endometrial thickens in response to Rising estrogen levels during the menstrual cycle and then shedding endometrial at the times of menses 2 The thickens
Endometrial line thickness in different conditions 1 Endometrial thickens in response to Rising estrogen levels during the menstrual cycle and then shedding endometrial at the times of menses 2 The thickens
Endometriosis an Enigma- Review Article
 Volume 2 Issue 1 2018 Page 212 to 217 Editorial Gynaecology and Perinatology ISSN: 2576-8301 Endometriosis an Enigma- Review Article Dr. Sreelatha S 1 *, Dr. Shruthi A 2, Dr. Vandana Ambastha 2, Dr. Asha
Volume 2 Issue 1 2018 Page 212 to 217 Editorial Gynaecology and Perinatology ISSN: 2576-8301 Endometriosis an Enigma- Review Article Dr. Sreelatha S 1 *, Dr. Shruthi A 2, Dr. Vandana Ambastha 2, Dr. Asha
SURGICAL PROBLEMS IN FERTILITY- FIBROIDS. Dr.Māris Arājs gyn-ob specialist Cell phone:
 SURGICAL PROBLEMS IN FERTILITY- FIBROIDS Dr.Māris Arājs gyn-ob specialist maris@myclinicriga.lv Cell phone: +371 26556466 There is NO Industry Sponsorship and Financial Conflict of Interest for this presentation
SURGICAL PROBLEMS IN FERTILITY- FIBROIDS Dr.Māris Arājs gyn-ob specialist maris@myclinicriga.lv Cell phone: +371 26556466 There is NO Industry Sponsorship and Financial Conflict of Interest for this presentation
Coexistence of Endometriosis and Uterine Dysfunction in Infertile Women
 Coexistence of Endometriosis and Uterine Dysfunction in Infertile Women Ludwig Kiesel University of Münster Department of Gynecology and Obstetrics Münster, Germany Symptoms: Risk of Endometriosis Compared
Coexistence of Endometriosis and Uterine Dysfunction in Infertile Women Ludwig Kiesel University of Münster Department of Gynecology and Obstetrics Münster, Germany Symptoms: Risk of Endometriosis Compared
Endometriosis and Infertility - FAQs
 Published on: 8 Apr 2013 Endometriosis and Infertility - FAQs Introduction The inner lining of the uterus is called the endometrium and it responds to changes that take place during a woman's monthly menstrual
Published on: 8 Apr 2013 Endometriosis and Infertility - FAQs Introduction The inner lining of the uterus is called the endometrium and it responds to changes that take place during a woman's monthly menstrual
INFERTILITY CAUSES. Basic evaluation of the female
 INFERTILITY Infertility is the inability to conceive after 12 months of unprotected intercourse. There are multiple causes of infertility and a systematic way to evaluate the condition. Let s look at some
INFERTILITY Infertility is the inability to conceive after 12 months of unprotected intercourse. There are multiple causes of infertility and a systematic way to evaluate the condition. Let s look at some
At the conclusion of the first two year, the resident should be able to:
 Reproductive Endocrinology/Infertility Rotations PGY-I COMPETENCY 1. Patient Care, Provide patient centered care that is compassionate, appropriate, and effective for the treatment of health problems and
Reproductive Endocrinology/Infertility Rotations PGY-I COMPETENCY 1. Patient Care, Provide patient centered care that is compassionate, appropriate, and effective for the treatment of health problems and
ENDOMETRIOSIS WITH LYMPHATIC SPREAD P. Narmadha 1, P. Viswanathan 2, Rehana Tippoo 3, U. Manohar 4, Lavanya Kumari 5
 ENDOMETRIOSIS WITH LYMPHATIC SPREAD P. Narmadha 1, P. Viswanathan 2, Rehana Tippoo 3, U. Manohar 4, Lavanya Kumari 5 HOW TO CITE THIS ARTICLE: P. Narmadha, P. Viswanathan, Rehana Tippoo, U. Manohar, Lavanya
ENDOMETRIOSIS WITH LYMPHATIC SPREAD P. Narmadha 1, P. Viswanathan 2, Rehana Tippoo 3, U. Manohar 4, Lavanya Kumari 5 HOW TO CITE THIS ARTICLE: P. Narmadha, P. Viswanathan, Rehana Tippoo, U. Manohar, Lavanya
Please complete prior to the webinar. HOSPITAL REGISTRY WEBINAR FEMALE REPRODUCTIVE SYSTEM EXERCISES CASE 1: FEMALE REPRODUCTIVE
 Please complete prior to the webinar. HOSPITAL REGISTRY WEBINAR FEMALE REPRODUCTIVE SYSTEM EXERCISES PHYSICAL EXAMINATION CASE 1: FEMALE REPRODUCTIVE 3/5 Patient presents through the emergency room with
Please complete prior to the webinar. HOSPITAL REGISTRY WEBINAR FEMALE REPRODUCTIVE SYSTEM EXERCISES PHYSICAL EXAMINATION CASE 1: FEMALE REPRODUCTIVE 3/5 Patient presents through the emergency room with
Conflicts 10/5/2016. Abnormal Uterine Bleeding. Objectives Review diagnosis and updated nomenclature. Management options for acute and chronic AUB.
 Abnormal Uterine Bleeding Barbara L. Keller, MD JD Naval Hospital Oak Harbor OB/GYN Physician Conflicts I have no conflicts or financial interests to disclose. Objectives Review diagnosis and updated nomenclature.
Abnormal Uterine Bleeding Barbara L. Keller, MD JD Naval Hospital Oak Harbor OB/GYN Physician Conflicts I have no conflicts or financial interests to disclose. Objectives Review diagnosis and updated nomenclature.
Elaina Sexton, MD, MSc Obstetrics and Gynecology St. Vincent s Hospital. Objectives
 Elaina Sexton, MD, MSc Obstetrics and Gynecology St. Vincent s Hospital Objectives Definition of normal menstrual cycle and abnormal uterine bleeding (AUB) Evaluation of AUB Medical options for AUB Surgical
Elaina Sexton, MD, MSc Obstetrics and Gynecology St. Vincent s Hospital Objectives Definition of normal menstrual cycle and abnormal uterine bleeding (AUB) Evaluation of AUB Medical options for AUB Surgical
Perimenopausal DUB. Mary Anne Jamieson, MD Associate Professor, OB/GYN Queen s University Kingston, Ontario
 Perimenopausal DUB Mary Anne Jamieson, MD Associate Professor, OB/GYN Queen s University Kingston, Ontario Objectives Clinicians will: Make a confident diagnosis for Perimenopausal DUB (know how/when to
Perimenopausal DUB Mary Anne Jamieson, MD Associate Professor, OB/GYN Queen s University Kingston, Ontario Objectives Clinicians will: Make a confident diagnosis for Perimenopausal DUB (know how/when to
PALM-COEIN: Your AUB Counseling Guide
 PALM-COEIN: Your AUB Counseling Guide 10 million+ Treat the cause, not the symptom In the U.S, more than 10 million women between the ages of 35 and 49 are affected by AUB 1 Diagnosis Cause Structural
PALM-COEIN: Your AUB Counseling Guide 10 million+ Treat the cause, not the symptom In the U.S, more than 10 million women between the ages of 35 and 49 are affected by AUB 1 Diagnosis Cause Structural
A Rare Presentation of Endometriosis with Recurrent Massive Hemorrhagic Ascites which Can Mislead
 Case Report INTERNATIONAL JOURNAL OF WOMEN'S HEALTH AND REPRODUCTION SCIENCES http://www.ijwhr.net A Rare Presentation of Endometriosis with Recurrent Massive Hemorrhagic Ascites which Can Mislead Article
Case Report INTERNATIONAL JOURNAL OF WOMEN'S HEALTH AND REPRODUCTION SCIENCES http://www.ijwhr.net A Rare Presentation of Endometriosis with Recurrent Massive Hemorrhagic Ascites which Can Mislead Article
Female Genital Tract Lab. Dr. Nisreen Abu Shahin Assistant Professor of Pathology University of Jordan
 Female Genital Tract Lab Dr. Nisreen Abu Shahin Assistant Professor of Pathology University of Jordan Ovarian Pathology A 20-year-old female presented with vague left pelvic pain. Pelvic exam revealed
Female Genital Tract Lab Dr. Nisreen Abu Shahin Assistant Professor of Pathology University of Jordan Ovarian Pathology A 20-year-old female presented with vague left pelvic pain. Pelvic exam revealed
Molly A. Brewer DVM, MD, MS Chair and Professor Department of Obstetrics and Gynecology University of Connecticut School of Medicine
 Molly A. Brewer DVM, MD, MS Chair and Professor Department of Obstetrics and Gynecology University of Connecticut School of Medicine Review causes of abnormal uterine bleeding: Adolescent Reproductive
Molly A. Brewer DVM, MD, MS Chair and Professor Department of Obstetrics and Gynecology University of Connecticut School of Medicine Review causes of abnormal uterine bleeding: Adolescent Reproductive
Endometriosis Treatment & Management Medscape
 Endometriosis Treatment & Management Medscape Updated: Apr 25, 2016 Author: G Willy Davila, MD; Chief Editor: Michel E Rivlin, MD more... Approach Considerations The dependence of endometriosis on the
Endometriosis Treatment & Management Medscape Updated: Apr 25, 2016 Author: G Willy Davila, MD; Chief Editor: Michel E Rivlin, MD more... Approach Considerations The dependence of endometriosis on the
understanding endometriosis Authored by Dr KT Subrayen Sponsored by
 understanding endometriosis Authored by Dr KT Subrayen Sponsored by in this booklet What is Endometriosis? 1 What causes Endometriosis? 3 What does Endometriosis look like? 4 Common symptoms of Endometriosis
understanding endometriosis Authored by Dr KT Subrayen Sponsored by in this booklet What is Endometriosis? 1 What causes Endometriosis? 3 What does Endometriosis look like? 4 Common symptoms of Endometriosis
Investigations and management of severe endometriosis
 Investigations and management of severe endometriosis Dr Jim Tsaltas Head of Gynaecological Endoscopy and Endometriosis Surgery Monash Health Monash University Dept of O&G Melbourne IVF Freemasons Hospital
Investigations and management of severe endometriosis Dr Jim Tsaltas Head of Gynaecological Endoscopy and Endometriosis Surgery Monash Health Monash University Dept of O&G Melbourne IVF Freemasons Hospital
MULLERIAN DUCT ANOMALY: A CASE REPORT
 MULLERIAN DUCT ANOMALY: A Sunny Goyal 1, Ankur Aggarwal 2, Hemant Kumar Mishra 3, Tushar Prabha 4, Vipin kumar Bakshi 5 HOW TO CITE THIS ARTICLE: Sunny Goyal, Ankur Aggarwal, Hemant Kumar Mishra, Tushar
MULLERIAN DUCT ANOMALY: A Sunny Goyal 1, Ankur Aggarwal 2, Hemant Kumar Mishra 3, Tushar Prabha 4, Vipin kumar Bakshi 5 HOW TO CITE THIS ARTICLE: Sunny Goyal, Ankur Aggarwal, Hemant Kumar Mishra, Tushar
Menstrual Disorders & Ambulatory Gynaecology
 Menstrual Disorders & Ambulatory Gynaecology Mr. Nagui Lewis Aziz M B, CH B, FRCOG Consultant Gynaecologist The Royal Oldham Hospital 01/09/2018 Heavy menstrual bleeding (HMB ) is a common problem responsible
Menstrual Disorders & Ambulatory Gynaecology Mr. Nagui Lewis Aziz M B, CH B, FRCOG Consultant Gynaecologist The Royal Oldham Hospital 01/09/2018 Heavy menstrual bleeding (HMB ) is a common problem responsible
Pathology of the female genital tract
 Pathology of the female genital tract Common illnesses of the female genital tract Before menarche Developmental anomalies Tumors (ovarial teratoma) Amenorrhea Fertile years PCOS, ovarian cysts Endometriosis
Pathology of the female genital tract Common illnesses of the female genital tract Before menarche Developmental anomalies Tumors (ovarial teratoma) Amenorrhea Fertile years PCOS, ovarian cysts Endometriosis
Posterior Deep Endometriosis. What is the best approach? Posterior Deep Endometriosis. Should we perform a routine excision of the vagina??
 Posterior Deep Endometriosis What is the best approach? Dept Gyn Obst Polyclinique Hotel Dieu CHU Clermont Ferrand France Posterior Deep Endometriosis Organs involved - Peritoneum - Uterine cervix -Rectum
Posterior Deep Endometriosis What is the best approach? Dept Gyn Obst Polyclinique Hotel Dieu CHU Clermont Ferrand France Posterior Deep Endometriosis Organs involved - Peritoneum - Uterine cervix -Rectum
Not all roads point to hysterectomy: treatment options for fibroids
 Not all roads point to hysterectomy: treatment options for fibroids MAUREEN KOHI, MD DEPARTMENT OF RADIOLOGY JEANNETTE LAGER, MD DEPARTMENT OF OBSTETRICS, GYNECOLOGY AND REPRODUCTIVE SCIENCES A lady, recently
Not all roads point to hysterectomy: treatment options for fibroids MAUREEN KOHI, MD DEPARTMENT OF RADIOLOGY JEANNETTE LAGER, MD DEPARTMENT OF OBSTETRICS, GYNECOLOGY AND REPRODUCTIVE SCIENCES A lady, recently
FDG-PET value in deep endometriosis
 Gynecol Surg (2011) 8:305 309 DOI 10.1007/s10397-010-0652-6 ORIGINAL ARTICLE FDG-PET value in deep endometriosis A. Setubal & S. Maia & C. Lowenthal & Z. Sidiropoulou Received: 3 December 2010 / Accepted:
Gynecol Surg (2011) 8:305 309 DOI 10.1007/s10397-010-0652-6 ORIGINAL ARTICLE FDG-PET value in deep endometriosis A. Setubal & S. Maia & C. Lowenthal & Z. Sidiropoulou Received: 3 December 2010 / Accepted:
Gynaecological Oncology Cases
 Gynaecological Oncology Cases 1. Tamoxifen and the endometrium 2. Cancer and the older woman Dr Julie M Lamont Consultant Gynaecological Oncologist Epworth Freemasons Hospital 21 st April 2015 Mrs FS 66
Gynaecological Oncology Cases 1. Tamoxifen and the endometrium 2. Cancer and the older woman Dr Julie M Lamont Consultant Gynaecological Oncologist Epworth Freemasons Hospital 21 st April 2015 Mrs FS 66
Endometriosis of the Appendix Resulting in Perforated Appendicitis
 27 Endometriosis of the Appendix Resulting in Perforated Appendicitis Toru Hasegawa a Koichi Yoshida b Kazuhiro Matsui c a Department of Obstetrics and Gynecology, Faculty of Medicine, University of Toyama,
27 Endometriosis of the Appendix Resulting in Perforated Appendicitis Toru Hasegawa a Koichi Yoshida b Kazuhiro Matsui c a Department of Obstetrics and Gynecology, Faculty of Medicine, University of Toyama,
5/5/2010. Infertility FINANCIAL DISCLOSURE. Infertility Definition. Objectives. Normal Human Fertility. Normal Menstrual Cycle
 Infertility FINANCIAL DISCLOSURE I HAVE NO FINANCIAL INTEREST IN ANY OF THE PRODUCTS MENTIONED IN MY PRESENTATION Bryan K. Rone, M.D. University of Kentucky Obstetrics and Gynecology I AM RECEIVING COMPENSATION
Infertility FINANCIAL DISCLOSURE I HAVE NO FINANCIAL INTEREST IN ANY OF THE PRODUCTS MENTIONED IN MY PRESENTATION Bryan K. Rone, M.D. University of Kentucky Obstetrics and Gynecology I AM RECEIVING COMPENSATION
Uterine-Sparing Treatment Options for Symptomatic Uterine Fibroids
 Uterine-Sparing Treatment Options for Symptomatic Uterine Fibroids Developed in collaboration Learning Objective Upon completion, participants should be able to: Review uterine-sparing fibroid therapies
Uterine-Sparing Treatment Options for Symptomatic Uterine Fibroids Developed in collaboration Learning Objective Upon completion, participants should be able to: Review uterine-sparing fibroid therapies
ENDOMETRIOSIS AS A COMMON CAUSE OF PELVIC PAIN
 ENDOMETRIOSIS AS A COMMON CAUSE OF PELVIC PAIN M.Basta Nikolić, S. Stojanović, O. Nikolić, T. Mrđanin, D. Donat, V. Žigić Center for Radiology, Clinical Center of Vojvodina Novi Sad Chronic pelvic pain
ENDOMETRIOSIS AS A COMMON CAUSE OF PELVIC PAIN M.Basta Nikolić, S. Stojanović, O. Nikolić, T. Mrđanin, D. Donat, V. Žigić Center for Radiology, Clinical Center of Vojvodina Novi Sad Chronic pelvic pain
Reproductive Endocrinology and Infertility Rotation Objectives. Reproductive Endocrinology and Infertility Specialists
 Reproductive Endocrinology and Infertility Rotation Objectives Reproductive Endocrinology and Infertility Specialists Terry O Grady M.D., FRCSC Sarah Healey M.D., FRCSC Deanna Murphy M.D., FRCSC Sean Murphy
Reproductive Endocrinology and Infertility Rotation Objectives Reproductive Endocrinology and Infertility Specialists Terry O Grady M.D., FRCSC Sarah Healey M.D., FRCSC Deanna Murphy M.D., FRCSC Sean Murphy
Chronic Pelvic Pain. AP099, December 2010
 AP099, December 2010 Chronic Pelvic Pain Pain in the pelvic area that lasts for 6 months or longer is called chronic pelvic pain. An estimated 15 20% of women aged 18 50 years have chronic pelvic pain
AP099, December 2010 Chronic Pelvic Pain Pain in the pelvic area that lasts for 6 months or longer is called chronic pelvic pain. An estimated 15 20% of women aged 18 50 years have chronic pelvic pain
5/5/2010 FINANCIAL DISCLOSURE. Abnormal Uterine Bleeding. Is This A Problem? About me % of visits to gynecologist
 Abnormal Uterine FINANCIAL DISCLOSURE I HAVE NO FINANCIAL INTEREST IN ANY OF THE PRODUCTS MENTIONED IN MY PRESENTATION Bryan K. Rone, M.D. University of Kentucky Obstetrics and Gynecology May 5, 2010 About
Abnormal Uterine FINANCIAL DISCLOSURE I HAVE NO FINANCIAL INTEREST IN ANY OF THE PRODUCTS MENTIONED IN MY PRESENTATION Bryan K. Rone, M.D. University of Kentucky Obstetrics and Gynecology May 5, 2010 About
Dr. Nancy Van Eyk Associate Professor, Dalhousie University Chief of Gynaecology, IWK Health Centre
 Dr. Nancy Van Eyk Associate Professor, Dalhousie University Chief of Gynaecology, IWK Health Centre AUB Outline Terminology Classification/Etiology Assessment Treatment Referral to Gynaecology U c pt 4
Dr. Nancy Van Eyk Associate Professor, Dalhousie University Chief of Gynaecology, IWK Health Centre AUB Outline Terminology Classification/Etiology Assessment Treatment Referral to Gynaecology U c pt 4
4 Mousa Al-abbadi. Ola Al-juneidi. Abdul-rahman Ibrahim
 4 Mousa Al-abbadi Ola Al-juneidi Abdul-rahman Ibrahim Cervical Cancer We previously talked about human papilloma virus (HPV). There are almost 140 serotypes of HPV so far. Certain serotypes (14 of them)
4 Mousa Al-abbadi Ola Al-juneidi Abdul-rahman Ibrahim Cervical Cancer We previously talked about human papilloma virus (HPV). There are almost 140 serotypes of HPV so far. Certain serotypes (14 of them)
Chronic Pelvic Pain. Bridget Kamen, MD Obstetrics and Gynecology, Confluence Health. I have no disclosures
 Chronic Pelvic Pain Bridget Kamen, MD Obstetrics and Gynecology, Confluence Health I have no disclosures Objectives A little epidemiology Understand there are both gynecologic and non-gynecologic causes
Chronic Pelvic Pain Bridget Kamen, MD Obstetrics and Gynecology, Confluence Health I have no disclosures Objectives A little epidemiology Understand there are both gynecologic and non-gynecologic causes
Minimal Access Surgery in Gynaecology
 Gynaecology & Fertility Information for GPs August 2014 Minimal Access Surgery in Gynaecology Today, laparoscopy is an alternative technique for carrying out many operations that have traditionally required
Gynaecology & Fertility Information for GPs August 2014 Minimal Access Surgery in Gynaecology Today, laparoscopy is an alternative technique for carrying out many operations that have traditionally required
ADENOMYOSIS. ETIOPHATOGENICAL, DIAGNOSTIC AND THERAPEUTICAL CONSIDERATIONS
 UNIVERSITY OF MEDICINE AND PHARMACY OF CRAIOVA FACULTY OF MEDICINE Ph.D. THESIS ADENOMYOSIS. ETIOPHATOGENICAL, DIAGNOSTIC AND THERAPEUTICAL CONSIDERATIONS ABSTRACT SCIENTIFIC COORDINATOR: PROF. DR. MIHAI
UNIVERSITY OF MEDICINE AND PHARMACY OF CRAIOVA FACULTY OF MEDICINE Ph.D. THESIS ADENOMYOSIS. ETIOPHATOGENICAL, DIAGNOSTIC AND THERAPEUTICAL CONSIDERATIONS ABSTRACT SCIENTIFIC COORDINATOR: PROF. DR. MIHAI
Laparoscopic approach to severe endometriosis
 Center for minimal access Surgery in Gynecology Department of Gynaecology and Obstetrics Hospital Sachsenhausen Frankfurt Academic Teaching hospital University of Frankfurt Laparoscopic approach to severe
Center for minimal access Surgery in Gynecology Department of Gynaecology and Obstetrics Hospital Sachsenhausen Frankfurt Academic Teaching hospital University of Frankfurt Laparoscopic approach to severe
Polycystic ovarian disease and Endometriosis
 Polycystic ovarian disease and Endometriosis Objectives: At the end of this lecture, the student should be able to: Know the clinicopathologic features of endometriosis with special emphasis on: definition,
Polycystic ovarian disease and Endometriosis Objectives: At the end of this lecture, the student should be able to: Know the clinicopathologic features of endometriosis with special emphasis on: definition,
41a Pathology: Reproductive System
 41a Pathology: Reproductive System 41a Pathology: Reproductive System! Class Outline" 5 minutes" "Attendance, Breath of Arrival, and Reminders " 10 minutes "Lecture:" 25 minutes "Lecture:" 15 minutes "Active
41a Pathology: Reproductive System 41a Pathology: Reproductive System! Class Outline" 5 minutes" "Attendance, Breath of Arrival, and Reminders " 10 minutes "Lecture:" 25 minutes "Lecture:" 15 minutes "Active
1) Intersexuality - Dr. Huda
 Intersexuality - Dr. Huda") 1) Intersexuality - Dr. Huda DSD (Disorders of sex development) occur when there is disruption of either: Gonadal differentiation Fetal sex steroid production or action Mullerian abnormalities and Wolffian
1) Intersexuality - Dr. Huda DSD (Disorders of sex development) occur when there is disruption of either: Gonadal differentiation Fetal sex steroid production or action Mullerian abnormalities and Wolffian