Alphabet soup of preemie problems MBM & NEC
|
|
|
- Jody Robinson
- 5 years ago
- Views:
Transcription

1 Alphabet soup of preemie problems MBM & NEC Tanya Kamka, MSN, RNC-NIC Neonatal Outreach Educator Samantha Wynn, RN, BSN, Cynthia Jensen, MS Objectives Upon completion of this presentation the participant should be able to: Describe fetal GI development Differentiate between the term and preterm GI system Describe nutritional goals for the preterm infant Identify risk factors for necrotizing enterocolitis (NEC) Identify signs and symptoms of NEC Describe medical and surgical treatment plans for NEC 2 1



2 Embryologic GI Development Fetal gut complete by weeks Functional development begins in utero and continues into infancy 3 Gastrointestinal Development By 4 weeks the embryo has a single tube intestine, liver bud, and hepatobiliary system At 5-9 weeks rapid small intestine growth causes herniation By 10 weeks, intestines reenter the abdomen. Villi and microvilli are formed 4 Medline Plus. (2017). Fetal development: MedlinePlus Medical Encyclopedia.Medlineplus.gov. Retrieved 15 April 2017, from 2



3 Gastrointestinal Development At 16 weeks the fetus begins sucking & swallowing, meconium is present By 24 weeks the intestines secrete digestive enzymes At 32 weeks the fetus begins normal gastric emptying. At weeks suck swallow coordination occurs, along with rapid peristalsis 5 Medline Plus. (2017). Fetal development: MedlinePlus Medical Encyclopedia.Medlineplus.gov. Retrieved 15 April 2017, from How long are the small intestines? The intestines are the largest part of our body that interact with the external environment 6 McElroy, S. (2017). Innate Immunity and NEC. Presentation, UC Davis. 3
.")


4 How long are the small intestines? 7 McElroy, S. (2017). Innate Immunity and NEC. Presentation, UC Davis. How long are the small intestines? 8 McElroy, S. (2017). Innate Immunity and NEC. Presentation, UC Davis. 4

5 Structure of the Small Intestines

")

6 Small Intestines Tight Junctions 11 Gastrointestinal Development Neonatal phase Exposure to enteral nutrition leads to rapid differentiation and development Development of GIT mucosal immunity due to dietary antigens (or lack of) Mucosal immune system begins to distinguish between safe nutrients and foreign pathogens What are we putting into our babies?? 12 6
. Charles-Michel Billard (1800-1832): pioneer of neonatal medicine.")
7 Case Study DOL 9 small and weak Copious green-stained diarrhea Intense perianal redness Swollen abdomen DOL 11 Large bloody stools Vomiting Cold, livid extremeties Tense belly Extremely slow heartbeat Intense perianal redness Swollen abdomen Dies that evening with a large liquid black stool 13 Dunn, P. (1990). Charles-Michel Billard ( ): pioneer of neonatal medicine.archives Of Disease In Childhood, 65(7 Spec No), Case Study Continued Upon autopsy Terminal ileum intensely red and swollen Mucosa friable, covered in blood Mucosa is so soft it turns to mash when scraped with the fingernail -Reported by Charles Billard in


8 When Good Guts Go Bad 15 Necrotizing Enterocolitis 16 8
9 What is NEC? Definition: an acquired disease that affects the GI system, particularly that of premature infants. It is characterized by inflammation of the bowel wall followed by areas of necrosis, most commonly in the terminal ileum and proximal colon, but may affect any or all of the small and large intestines. 17 Verklan, M., & Walden, M. (2015). Core curriculum for neonatal intensive care nursing (5th ed.). Incidence BW 501 to 750 g 12 percent risk, 42 percent mortality with NEC BW 751 to 1000 g 9 percent risk, 29 percent mortality with NEC BW 1001 to 1250 g 6 percent risk, 21 percent mortality with NEC BW 1251 to 1500 g 3 percent risk, 16 percent mortality with NEC 18 Verklan, M., & Walden, M. (2015). Core curriculum for neonatal intensive care nursing (5th ed.). 9
. We have to redefine NEC.")
10 What is or isn t NEC? 19 Gordon, P. (2017). We have to redefine NEC. Presented at, UC Davis Which baby has NEC? 20 Gordon, P. (2017). We have to redefine NEC. Presented at, UC Davis 10
. We have to redefine NEC.")
11 Which baby has NEC? Many cases of NEC and SIP can be differentiated by an x-ray but unfortunately not all 21 Gordon, P. (2017). We have to redefine NEC. Presented at, UC Davis NEC vs SIP 22 Gordon, P. (2017). We have to redefine NEC. Presented at, UC Davis 11
12 NEC vs SIP NEC SIP Incidence < 1500 grams 7 10% 2 3% Age of onset 2-6 weeks 0-14 days Pneumatosis Yes No Enteral feedings Yes No Histologic evidence of villus necrosis Yes Mortality 10-30% above baseline 5-10% above baseline SIP Can occur in the absence of NEC Compared to NEC: less hemodynamic instability, less metabolic acidosis, improved survival rate, lack of coagulation necrosis seen in NEC More common in patients with: UAC, administration of indomethacin or ibuprofen No 23 Gordon, P. (2017). We have to redefine NEC. Presented at, UC Davis Early vs Late onset Early onset Usually term First 7 days Critically ill Never fed Vascular cause of intestinal injury Late onset > 7 days Growing preemie Has been fed Luminal cause of intestinal injury 12
13 NEC in Term Infants Gut vs gut immaturity Early onset perinatal events plausible Cannot rely on metabolic acidosis, hemodynamic instability. May have few systemic symptoms due to greater reserve Improved survival probably related to lack of associated problems of prematurity May be that NEC results from two different disease processes in premature and term infants Most have some risk factor What is or isn t NEC? 26 Gordon, P. (2017). We have to redefine NEC. Presented at, UC Davis 13


14 NEC Pathogenesis Prematurity Propensity towards gut inflammation Impaired intestinal barrier function Decreased intestinal motility Deficient mucosal enzymes, hormones, pepsin, and gastric acid Immature autoregulation of microcirculation Lack of amniotic fluid Immature mucin layer 27 NEC Pathogenesis Enteral Feeds Formula feeding Fortification Abnormal intestinal microbiota Decreased commensal flora Increased pathogenic bacteria Prolonged antibiotic therapy Acid suppression medications 28 14
15 NEC Pathogenesis Gut Ischemia Abnormal gut vascular regulation More prone to hypoxic events Inflammatory response Genetic factors? TLR4? 29 NEC Pathogenesis TLR4 Toll-like receptor 30 15
 Intestines become colonized Bacteria bind to injured mucosa Inflammatory response Increased permeability of")

16 Etiology Common final pathway the endogenous production of inflammatory mediators that precipitate intestinal injury Model of Pathogenesis Subclinical event (hypoxia, ischemia) Intestines become colonized Bacteria bind to injured mucosa Inflammatory response Increased permeability of mucosa Translocation of bacteria Inflammatory response accelerates Inflammatory mediators, reactive oxygen species further injure mucosa Maladaptive vasoconstrictive response leads to ongoing ischemia/reperfusion injury End result cycle of feedback mechanisms ultimately causing necrosis and perforation 16
 Hypoxemia/ Hypovolemia = Natural Disaster If persists can destroy the wall and")

.")


17 Gastrointestinal In the adult intestine Development Fats = Seagulls (complacent, harmless, unhelpful) Hypoxemia/ Hypovolemia = Natural Disaster If persists can destroy the wall and overfill the bay allowing unrestricted access to the town! In medical terms, it can lead to damage inflammation and shock. Bacteria = Sharks Commensal Biofilm = The Barges Mucin = The Moat Epithelium = The Wall TLR-4, Immune Cells, etc = sentries 33 Medline Plus. (2017). Fetal development: MedlinePlus Medical Encyclopedia.Medlineplus.gov. Retrieved 15 April 2017, from Rest of the body = town Gastrointestinal Breast In the premature Milk intestine Development Walls aren t as strong Moat isn t as wide Lots more sentries Not as many barges 34 Medline Plus. (2017). Fetal development: MedlinePlus Medical Encyclopedia.Medlineplus.gov. Retrieved 15 April 2017, from 17


 sends out")
 35 Medline Plus. (2017).")

18 Gastrointestinal Breast Milk Development Formula Has growth factors to increase mucin production Has HMOs that distract pathogens and feed commensals Both are still at risk for natural disasters but hopefully the breast fed infant can weather the storm a little better Less protection against pathogen invasions Over expressed TLR-4 (sentries) sends out alarm causing excessive inflammatory response (town panic & wall damage) 35 Medline Plus. (2017). Fetal development: MedlinePlus Medical Encyclopedia.Medlineplus.gov. Retrieved 15 April 2017, from Diagnosing NEC 18
19 Bell s Staging for NEC Most commonly used in practice Staging based on severity of systemic, intestinal, and radiographic findings Treatment is directed at the clinical signs rather than the particular stage of NEC Each advancing stage includes the characteristics of the previous stage plus additional findings due to increasing severity of the disease Stage 1-Suspected NEC Gastric residuals Abdominal distension Heme positive stools X-ray normal to mild distension Temp instability A s and B s 19

20 Stage 2- Proven NEC Absent bowel sounds Abdominal tenderness Pneumatosis intestinalis Portal venous gas Mild metabolic acidosis Platelets Radiograph findings include intestinal dilation, ileus, pneumatosis intestinalis, and ascites Stage IIA mildly ill, stage IIB moderately ill Stage 3-Advanced NEC Severely ill Marked distension Signs of peritonitis Hypotension Bradycardia Severe apnea Metabolic and respiratory acidosis Disseminated intravascular coagulation (DIC) Stage IIIA intact bowel, stage IIIB perforated bowel visualized as a pneumoperitoneum 20

21 Diagnosing NEC Khailova, L., Dvorak, K., Arganbright, K., Halpern, M., Kinouchi, T., Yajima, M., & Dvorak, B. (2017). Bifidobacterium bifidum improves intestinal integrity in a rat model of necrotizing enterocolitis. Retrieved 16 April 2017, from Diagnosing NEC Based on the presence of the characteristic clinical features of: Abdominal distention Rectal bleeding Abdominal radiographic finding of pneumatosis intestinalis. Assessment of infants with suspected NEC includes: abdominal imaging, blood studies, stool analysis, and sepsis evaluation Future Biomarkers? ifabp? PAF? 21


22 Presentation clinical findings Abdominal distension Feeding residuals, often bilious Gross or occult blood in stool Abdominal tenderness Erythema or bluish discoloration of abdominal wall Absent bowel sounds Non-specific signs (temp. instability, glucose instability, lethargy, apnea/bradycardia, hypotension) 22


23 Visual Exam 23

24 Abdominal Distension/ Increased AG What is the distension from? What has been the baseline abdominal exam Last stool Is he on CPAP or been recently bag/mask ventilated? Does he have an OGT in place and vented? Are there any other concerning signs? glucose instability, lethargy, temp. instability, apnea, etc. Is the infant hungry and eager to nipple feed? 24
 Is the physical exam benign? Could there be an ileus?")
25 Residuals Is the residual bilious? Is the baby stooling at least q12h, moderate amounts? Has the infant been recently bag/mask ventilated? What position has the baby been in? Has the last few hours been stressful for the infant? (blood draws, lots of handling, procedures) Is the physical exam benign? Could there be an ileus? morphine, infection, post-op Refeed residual if non-bilious, partially digested milk. Heme Positive Stools Is the stool meconium? Is the infant receiving glycerin suppositories? Does the infant have a fissure? Has the infant had abdominal surgery? 25

26 Presentation Laboratory Findings Glucose instability Abnormally high or low WBC Left shift of WBC Thrombocytopenia Metabolic acidosis DIC CRP Radiologic Findings 26


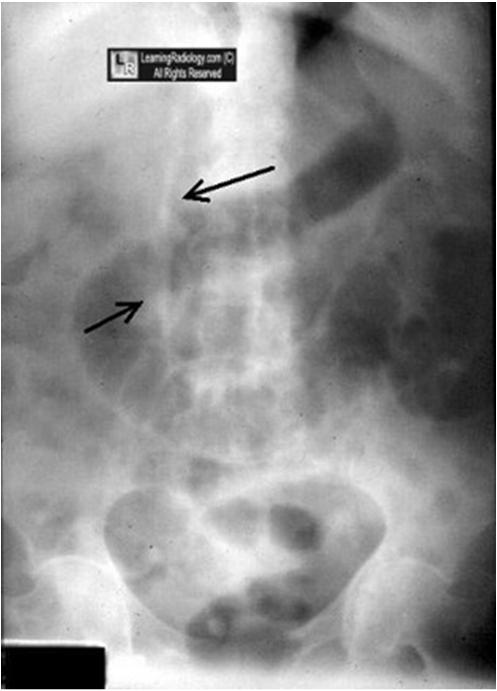
27 Normal Abdominal Xray Uniform size and shape of loops Diameter approximates vertebra Gas throughout entire bowel tract Gas pattern should vary on subsequent x rays No free air in abdomen and liver is opaque Presentation Radiographic Findings Non-specific bowel dilatation Thickening of bowel wall Fixed, dilated loop unchanged on >1 radiograph Pneumatosis intestinalis Portal venous gas Pneumoperitoneum Falciform ligament may be outlined Football sign 27


28 28

29 58 29


30 59 Ultrasound Used to look for bowel wall thickening Free air Portal Venous gas 30
31 Management- Suspected NEC NPO Fluid/electrolyte and parenteral nutrition management Gastric decompression Labs Antibiotics (Ampicillin and Gentamicin, Vancomycin, Cefotaxime, Flagyl?) Correct metabolic acidosis Serial xrays Respiratory & Circulatory support Rule out other causes of distension Transfusions? Close monitoring Management Definite NEC Obtain consult with surgical team Serial KUB s NPO 7-10 days Careful I/O s maintain bowel perfusion, may require fluid resuscitation Circulatory support Respiratory support PT, PTT, fibrinogen, platelets Frequent abg s, electrolytes Antibiotics 7-14 days 31

32 Surgical Treatment Medical management is appropriate in most cases Operative intervention indications: Perforation, evidence of necrotic bowel (fixed loop, metabolic acidosis, DIC, shock), or progressively worsening clinical condition despite intensive medical management Surgical Options: Peritoneal drain Exploratory laparotomy for resection of necrotic bowel Surgical Considerations Peritoneal drain +/- irrigation Allows time for baby to stabilize Better able to delineate viable gut when do operate Borderline bowel segments may recover Intestinal perforation may be definitively treated Laparotomy indicated if not improving in hrs 32


33 Surgical Considerations Exploratory laparotomy for resection of necrotic bowel Primary Anastomoses Ostomy & Mucous Fistula Clip & Drop 33

34 Prevention Human milk pasteurized MBM is not as protective Intestinal priming (gut stimulation feedings) Promotes structural and functional maturation Promotes acquisition of normal flora Stimulate release of gastric hormones Slow, but not too slow, feed advance Minimize prolonged antibiotic use Antenatal glucocorticoids for lung maturation also accelerate intestinal maturation Prebiotics, probiotics, postbiotics 34



35 How can Human Milk Prevent NEC? eaflet.html 69 Oligosaccharides & the Gut Human Milk Oligosaccharides 3 rd most abundant biomolecule in human milk Un-digestible by humans It s All About the Breast Milk Sugars, Baby 70 German, B. (2017). The Evolution of Lactation as a Guide to Understanding Nourishment and Prevention in the 21 st Century. Presentation, UC Davis. 35


36 Microbiota Modern life has stopped microbial transfer So what are we left with? Microbial Dysbiosis Long term consequences 71 Milk-Oriented Microbiota 72 36

37 Probiotics The Golden Age of Probiotics: A Systematic Review and Meta-Analysis of Randomized and Observational Studies in Preterm Infants Probiotics potentially prevent severe NEC and late-onset sepsis, and reduce mortality in preterm infants Prophylactic Probiotics for Preterm Infants: A Systematic Review and Meta-Analysis of Observational Studies. Probiotic supplementation reduces the risk of NEC and mortality in preterm infants. The effect sizes are similar to findings in meta-analyses of RCTs. However, the optimal strain, dose and timing need further investigation. 73 Colostrum Care Oropharyngeal administration Use syringe to place directly onto the oral mucosa in the buccal cavity for absorption via the mucosa Allows for systemic absorption of the cytokines and pancreatic secretory trypsin inhibitor (PSTI) Rich source of Oligosaccharides May reduce time to full feeds 74 37

38 Trophic feeds Improved feeding tolerance More rapid advancement to full feeds Improved weight gain Shortened duration of TPN Less phototherapy Reduction in direct bilirubin Decreased length of stay Does not increase risk of NEC! May be considered for an infant who is hemodynamically stable on a low dose of dopamine and/or with an Umbilical Arterial Line in place 75 Feeding Protocol for Preterm Infants Goal Preterm: ml/kg/day of 24cal/oz; fortify when feed volume is 60ml/kg/day Term: ml/kg/day of 20cal/oz Consider increasing concentration of feeds if poor weight gain, volume intolerance or fluid restriction, or increased energy requirements. Preterm infants should receive 24cal/oz for at least one week before increasing to 27cal/oz Consider hind milk 38

39 UCSF BCH Feeding Protocol Birth GA (wks) 1st day (ml/kg/d) Advance on Day # Amount (ml/kg/d) >60 ml/kg/d Advance by Achieve Goal Feeds by < Day to 27-6/ Day to 29-6/ Day to 31-6/7 20 Daily Day 8 32 to 34-6/7 20 Daily Day 5-8 >35 50 or ad lib Daily >20-40 or ad lib >20-40 or ad lib Day 4-6 Signs of intolerance No <2 ml or <⅓ of feeding volume, whichever is greater Yes Refeed aspirate as part of total volume and continue feeding No Yes NPO with MD order and evaluation 2. Refeed aspirate. Hold feed with MD order 3. Recheck residuals before next feeding time

40 Prevention - Disadvantages of NPO The wisdom of stopping all enteral intake is counterintuitive to the ontologic processes that started in utero Edmund Gamma, Lyle Browne, State Univ. NV Has not uniformly provided protection, may simply delay the onset of NEC Predisposes to injury when finally fed Gut atrophy Decreased mucin production and enzyme activity Decreased secretion of IgA Increased transmural penetration of bacteria, and antigens Increased susceptibility to infection Autodigestion Enteral Nutrition Breast milk is best Donor breast when MBM not available Use of standardized feeding guideline Reduced risk of NEC Less variability Achieve full feeds earlier 80 40
: an antioxidant Epidermal Growth Factor (EGF): matures intestinal mucosa Gut Check NEC (Gephart et al, 2014)")
41 Prevention experimental approaches Enteral IgG/IgA Formula acidification to prevent bacterial overgrowth Probiotics supplementation (bifidobacteria) L-arginine supplementation: precursor of NO Oral antibiotics PAF-acetylhydrolase: degrades the inflammatory mediator PAF Glutathione (GSH): an antioxidant Epidermal Growth Factor (EGF): matures intestinal mucosa Gut Check NEC (Gephart et al, 2014) 41

42 Gut Check NEC (Gephart et al, 2014) You are a better monitor than Hewlett Packard ever made (NICU nurse) Educate yourself in the signs/symptoms of NEC. Know your infant s history. Is this infant at risk? Know your infant s baseline exam. Be alert to subtle changes. Watch for patterns/clusters of concerning symptoms. Respect your intuition. It is grounded in expertise. If you are worried, assess, obtain a KUB, blood gas, CBC. Remember that these can be normal in the early phase of NEC. Nurses by their vigilance and expertise can substantially influence the incidence and outcome of NEC. 42


43 Neonatal nurses go beyond the numbers to take in the entire baby. Their nursing is particular, contextual, and holistic. It is an art. Xrays and lab values pale in comparison with the vigilance and commitment of an expert nurse
44 References American Academy of Pediatrics, Section on Breastfeeding. (2005). Breastfeeding and the use of human milk. Pediatrics, 115(2), Bisquera JA, Cooper TR, Berseth CL. Impact of necrotizing enterocolitis on length of stay and hospital charges in very low birth weight infants. Pediatrics.2002;109(3): Cochrane Library 2001, CPQCC/CAN; McClure, 2000; Peter, et al, 2002; Ziegler, 2002; Kuzman O Reily, 2003; Berseth Yu, et al, 2005; Tyson & Kennedy Cochrane review, 2005 Dasgupta, S., Arya, S., Choudhary, S., & Jain, S. K. (2016). Amniotic fluid: Source of trophic factors for the developing intestine. World journal of gastrointestinal pathophysiology, 7(1), 38. Dermyshi, E., Wang, Y., Yan, C., Hong, W., Qiu, G., Gong, X., & Zhang, T. (2017). The Golden Age of Probiotics: A Systematic Review and Meta-Analysis of Randomized and Observational Studies in Preterm Infants. Neonatology, Gephart, S., Spitzer, A., Effken, J., Dodd, E., Halpern, M., & McGrath, J. (2014). Discrimination of GutCheckNEC: a clinical risk index for necrotizing enterocolitis. Journal Of Perinatology, 34(6), References Morgan, J., Young, L., & McGuire, W. (2014). Delayed introduction of progressive enteral feeds to prevent necrotising enterocolitis in very low birth weight infants. Cochrane Database Of Systematic Reviews. Mulvihill, S. J., Stone, M. M., Debas, H. T., & Fonkalsrud, E. W. (1985). The role of amniotic fluid in fetal nutrition. Journal of pediatric surgery, 20(6), Rodriguez, N., Meier, P., Groer, M., Zeller, J., Engstrom, J., & Fogg, L. (2010). A Pilot Study to Determine the Safety and Feasibility of Oropharyngeal Administra on of Own Motherʼs Colostrum to Extremely Low-Birth- Weight Infants. Advances In Neonatal Care, 10(4), Underwood, M. (2017). Probiotics and the Prevention of Necrotizing Enterocolitis. Presentation, UC Davis. Vohr, B., Poindexter, B., Dusick, A., McKinley, L., Wright, L., Langer, J., & Poole, W. (2006). Beneficial Effects of Breast Milk in the Neonatal Intensive Care Unit on the Developmental Outcome of Extremely Low Birth Weight Infants at 18 Months of Age. PEDIATRICS, 118(1), e115-e
45 Questions? Thank you!! 89 45
Our Journey Toward Elimination of. Necrotizing Enterocolitis 4/16/2018. Disclosure. Presentation Outline. Clinical Presentation of NEC
 Our Journey Toward Elimination of Necrotizing Enterocolitis RAY SATO, M.D. TACOMA GENERAL HOSPITAL NICU APRIL 2018 Disclosure Ray Sato, MD has no financial relationship to disclose or conflicts of interest
Our Journey Toward Elimination of Necrotizing Enterocolitis RAY SATO, M.D. TACOMA GENERAL HOSPITAL NICU APRIL 2018 Disclosure Ray Sato, MD has no financial relationship to disclose or conflicts of interest
The Case Begins. The case continued. Necrotizing Enterocolitis
 Bugs, Drugs and Things that go Bump in the Night From ghoulies to ghosties and long leggety beasties & things that go bump in the night, good lord deliver us Old Cornish Prayer Caring for premature infant
Bugs, Drugs and Things that go Bump in the Night From ghoulies to ghosties and long leggety beasties & things that go bump in the night, good lord deliver us Old Cornish Prayer Caring for premature infant
Necrotizing Enterocolitis: The Role of the Immune System
 Necrotizing Enterocolitis: The Role of the Immune System Patricia Denning, M.D. Associate Professor in Pediatrics Division of Neonatology Emory University School of Medicine What is NEC? What is NEC? Necrotizing
Necrotizing Enterocolitis: The Role of the Immune System Patricia Denning, M.D. Associate Professor in Pediatrics Division of Neonatology Emory University School of Medicine What is NEC? What is NEC? Necrotizing
Ashley Robson Canyon Creek Dr. Mckinney, TX 75070
 1 Ashley Robson 2212 Canyon Creek Dr. Mckinney, TX 75070 September 2 nd 2014 Debra Brandon PhD, RN, CCNS, FAAN Duke University School of Nursing Durham, NC Dear Mrs. Brandon- I would like the opportunity
1 Ashley Robson 2212 Canyon Creek Dr. Mckinney, TX 75070 September 2 nd 2014 Debra Brandon PhD, RN, CCNS, FAAN Duke University School of Nursing Durham, NC Dear Mrs. Brandon- I would like the opportunity
Minimal Enteral Nutrition
 Abstract Minimal Enteral Nutrition Although parenteral nutrition has been used widely in the management of sick very low birth weight infants, a smooth transition to the enteral route is most desirable.
Abstract Minimal Enteral Nutrition Although parenteral nutrition has been used widely in the management of sick very low birth weight infants, a smooth transition to the enteral route is most desirable.
Gastric Residuals in Preterm Infants
 Neonatal Nursing Education Brief: Gastric Residuals in the Preterm Infant https://www.seattlechildrens.org/healthcareprofessionals/education/continuing-medical-nursing-education/neonatalnursing-education-briefs/
Neonatal Nursing Education Brief: Gastric Residuals in the Preterm Infant https://www.seattlechildrens.org/healthcareprofessionals/education/continuing-medical-nursing-education/neonatalnursing-education-briefs/
NEC. cathy e. shin childrens hospital los angeles department of surgery university of southern california keck school of medicine
 NEC cathy e. shin childrens hospital los angeles department of surgery university of southern california keck school of medicine Necrotizing enterocolitis (NEC) the most common and most lethal disease
NEC cathy e. shin childrens hospital los angeles department of surgery university of southern california keck school of medicine Necrotizing enterocolitis (NEC) the most common and most lethal disease
RD s In Practice: Advancing Pediatric Nutrition
 RD s In Practice: Advancing Pediatric Nutrition A Strong Beginning Mindy Morris, DNP, NNP-BC, CNS Extremely Low Birth Weight Program Coordinator Objectives Understand the challenges associated with the
RD s In Practice: Advancing Pediatric Nutrition A Strong Beginning Mindy Morris, DNP, NNP-BC, CNS Extremely Low Birth Weight Program Coordinator Objectives Understand the challenges associated with the
SWISS SOCIETY OF NEONATOLOGY. Spontaneous intestinal perforation or necrotizing enterocolitis?
 SWISS SOCIETY OF NEONATOLOGY Spontaneous intestinal perforation or necrotizing enterocolitis? June 2004 2 Stocker M, Berger TM, Neonatal and Pediatric Intensive Care Unit, Children s Hospital of Lucerne,
SWISS SOCIETY OF NEONATOLOGY Spontaneous intestinal perforation or necrotizing enterocolitis? June 2004 2 Stocker M, Berger TM, Neonatal and Pediatric Intensive Care Unit, Children s Hospital of Lucerne,
4/15/2014. Nurses Take the Lead to Improve Overall Infant Growth. Improving early nutrition. Problem Identification
 Nurses Take the Lead to Improve Overall Infant Growth Cathy Lee Leon, RN, BSN, MBA, NE-BC California Pacific Medical Center-San Francisco Improving early nutrition Standardized feeding protocol Problem
Nurses Take the Lead to Improve Overall Infant Growth Cathy Lee Leon, RN, BSN, MBA, NE-BC California Pacific Medical Center-San Francisco Improving early nutrition Standardized feeding protocol Problem
The Use of Simulated Amniotic Fluid in Preventing Feeding Intolerance and Necrotizing Enterocolitis
 St. Catherine University SOPHIA Master of Arts in Nursing Theses Nursing 12-2011 The Use of Simulated Amniotic Fluid in Preventing Feeding Intolerance and Necrotizing Enterocolitis Grethe Mortensen St.
St. Catherine University SOPHIA Master of Arts in Nursing Theses Nursing 12-2011 The Use of Simulated Amniotic Fluid in Preventing Feeding Intolerance and Necrotizing Enterocolitis Grethe Mortensen St.
Necrotizing Enterocolitis: the role of ultrasound in the assessment of bowel viability
 Necrotizing Enterocolitis: the role of ultrasound in the assessment of bowel viability Ricardo Faingold, MD. Department of Medical Imaging The Montreal Children s Hospital McGill University SPR Vancouver
Necrotizing Enterocolitis: the role of ultrasound in the assessment of bowel viability Ricardo Faingold, MD. Department of Medical Imaging The Montreal Children s Hospital McGill University SPR Vancouver
Neonatal Nutrition Management Guidelines
 Neonatal Nutrition Management Guidelines Nutrition Committee March 2018 Overall Aim 2 Provision of appropriate nutrition to neonates in a timely and safe manner to facilitate adequate growth and development
Neonatal Nutrition Management Guidelines Nutrition Committee March 2018 Overall Aim 2 Provision of appropriate nutrition to neonates in a timely and safe manner to facilitate adequate growth and development
Resuscitating neonatal and infant organs and preserving function. GI Tract and Kidneys
 Resuscitating neonatal and infant organs and preserving function GI Tract and Kidneys Australian and New Zealand Resuscitation Council Joint Guidelines Outline Emphasis on the infant - PICU Kidney Gastrointestinal
Resuscitating neonatal and infant organs and preserving function GI Tract and Kidneys Australian and New Zealand Resuscitation Council Joint Guidelines Outline Emphasis on the infant - PICU Kidney Gastrointestinal
Neonatal Perforated Gut: Etiology and Risk Factors
 Cronicon OPEN ACCESS EC PAEDIATRICS Research Article Mostafa Kotb 1 * and Marwa Beyaly 2 1 Pediatric Surgery Department, Alexandria Faculty of Medicine, Egypt. 2 Human Genetics Department, Medical Research
Cronicon OPEN ACCESS EC PAEDIATRICS Research Article Mostafa Kotb 1 * and Marwa Beyaly 2 1 Pediatric Surgery Department, Alexandria Faculty of Medicine, Egypt. 2 Human Genetics Department, Medical Research
Necrotizing Enterocolitis Update Muneef AL-Hathal, MD
 Necrotizing Enterocolitis Update Muneef AL-Hathal, MD Neonatal Department Maternity Hospital Kuwait Incidence There is almost fourfolds difference in the rate of NEC in babies < 1500 gm (from 2-7%) The
Necrotizing Enterocolitis Update Muneef AL-Hathal, MD Neonatal Department Maternity Hospital Kuwait Incidence There is almost fourfolds difference in the rate of NEC in babies < 1500 gm (from 2-7%) The
Necrotizing Enterocolitis
 CHAPTER 1 CHAPTER Necrotizing Enterocolitis Fawn C. Lewis and Daniel A. Bambini Incidence The incidence of necrotizing enterocolitis (NEC) in the United States is 1-3 cases per thousand live births, or
CHAPTER 1 CHAPTER Necrotizing Enterocolitis Fawn C. Lewis and Daniel A. Bambini Incidence The incidence of necrotizing enterocolitis (NEC) in the United States is 1-3 cases per thousand live births, or
NEC- What Lies Under the Big Umbrella?
 NEC- What Lies Under the Big Umbrella? Instructor in Surgery Associate Surgical Director, Center for Advanced Intestinal Rehabilitation Department of Surgery, Boston Children's Hospital Harvard Medical
NEC- What Lies Under the Big Umbrella? Instructor in Surgery Associate Surgical Director, Center for Advanced Intestinal Rehabilitation Department of Surgery, Boston Children's Hospital Harvard Medical
Managing Residuals, WakeMed 2008 Guidelines
 Managing Residuals, WakeMed 2008 Guidelines Management of Aspirates: Background Early in life, gastric motility and muscle tone are decreased, possibly due to several reasons: increased gastrin, poorly
Managing Residuals, WakeMed 2008 Guidelines Management of Aspirates: Background Early in life, gastric motility and muscle tone are decreased, possibly due to several reasons: increased gastrin, poorly
SWISS SOCIETY OF NEONATOLOGY. Neonatal pneumatosis coli a mild form of classical necrotizing enterocolitis?
 SWISS SOCIETY OF NEONATOLOGY Neonatal pneumatosis coli a mild form of classical necrotizing enterocolitis? August 2008 2 Steurer M, Stocker M, Caduff JH, Neonatal and Pediatric Intensive Care Unit (SM,
SWISS SOCIETY OF NEONATOLOGY Neonatal pneumatosis coli a mild form of classical necrotizing enterocolitis? August 2008 2 Steurer M, Stocker M, Caduff JH, Neonatal and Pediatric Intensive Care Unit (SM,
North Trent Neonatal Network Clinical Guideline
 North Trent Neonatal Network Clinical Guideline Title: Management of Necrotising Enterocolitis Index Number/other identifier: Author: Aiwyne Foo Date written: October 2011 Review date: October 2014 This
North Trent Neonatal Network Clinical Guideline Title: Management of Necrotising Enterocolitis Index Number/other identifier: Author: Aiwyne Foo Date written: October 2011 Review date: October 2014 This
Daniel Hirsch, MD Director of Neonatology Somerset Medical Center Assistant Professor of Pediatrics UMDNJ RWJMS
 Daniel Hirsch, MD Director of Neonatology Somerset Medical Center Assistant Professor of Pediatrics UMDNJ RWJMS Daniel Hirsch, MD Director of Neonatology Somerset Medical Center Assistant Professor of
Daniel Hirsch, MD Director of Neonatology Somerset Medical Center Assistant Professor of Pediatrics UMDNJ RWJMS Daniel Hirsch, MD Director of Neonatology Somerset Medical Center Assistant Professor of
INTRODUCING YOUR GUT BACTERIA
 INTRODUCING YOUR GUT BACTERIA Microflora Intestinal flora 1.5 kg We would die with 5 years of birth if we did not have them as we would not develop a proper immune system 1000 species and 5000 strains
INTRODUCING YOUR GUT BACTERIA Microflora Intestinal flora 1.5 kg We would die with 5 years of birth if we did not have them as we would not develop a proper immune system 1000 species and 5000 strains
Surgical decision making in NEC
 Surgical decision making in NEC (the role of ultrasound) Nigel Hall Associate Professor of Paediatric Surgery University of Southampton Consultant Paediatric and Neonatal Surgeon Southampton Children s
Surgical decision making in NEC (the role of ultrasound) Nigel Hall Associate Professor of Paediatric Surgery University of Southampton Consultant Paediatric and Neonatal Surgeon Southampton Children s
Nutrition in the premie World
 SURVIVAL AND GROWTH NUTRITION ESSENTIALS Nutrition in the premie World DR VISH SUBRAMANIAN MD MRCP (UK) FAAP NEONATAL CRITICAL CARE MERCY CHILDRENS HOSPITAL., SPRINGFIELD MO Prematurity Nutritional Requirements
SURVIVAL AND GROWTH NUTRITION ESSENTIALS Nutrition in the premie World DR VISH SUBRAMANIAN MD MRCP (UK) FAAP NEONATAL CRITICAL CARE MERCY CHILDRENS HOSPITAL., SPRINGFIELD MO Prematurity Nutritional Requirements
3/22/2011. Inflammatory Bowel Disease. Inflammatory Bowel Disease Objectives: Appendicitis. Lemone and Burke Chapter 26
 Inflammatory Bowel Disease Lemone and Burke Chapter 26 Inflammatory Bowel Disease Objectives: Discuss etiology, patho and clinical manifestations of Appendicitis Peritonitis Ulcerative Colitis Crohn s
Inflammatory Bowel Disease Lemone and Burke Chapter 26 Inflammatory Bowel Disease Objectives: Discuss etiology, patho and clinical manifestations of Appendicitis Peritonitis Ulcerative Colitis Crohn s
Is NEC requiring surgery precipitated by a change in feeds? Observations from 50 consecutive cases. David Burge SIGNEC September 2015
 Is NEC requiring surgery precipitated by a change in feeds? Observations from 50 consecutive cases. David Burge SIGNEC September 2015 Clinical series Specific cases Other scenarios Published experience
Is NEC requiring surgery precipitated by a change in feeds? Observations from 50 consecutive cases. David Burge SIGNEC September 2015 Clinical series Specific cases Other scenarios Published experience
Is It Possible to Prevent Necrotizing Enterocolitis?
 Is It Possible to Prevent Necrotizing Enterocolitis? Ravi Mangal Patel, MD MSc Associate Professor of Pediatrics Emory University School of Medicine, Atlanta, GA, USA @institutopgg @ravimpatelmd Disclosures
Is It Possible to Prevent Necrotizing Enterocolitis? Ravi Mangal Patel, MD MSc Associate Professor of Pediatrics Emory University School of Medicine, Atlanta, GA, USA @institutopgg @ravimpatelmd Disclosures
SHORT GUT SYNDROME (SGS) : A MANAGEMENT CHALLENGE!
 : A MANAGEMENT CHALLENGE!") SHORT GUT SYNDROME (SGS) : A MANAGEMENT CHALLENGE! Muhammad Saaiq DEPARTMENT OF SURGERY,PIMS, ISLAMABAD. Surgical Grand Round, Pakistan Institute of Medical Sciences (PIMS), Islamabad. September 23, 2005.
SHORT GUT SYNDROME (SGS) : A MANAGEMENT CHALLENGE! Muhammad Saaiq DEPARTMENT OF SURGERY,PIMS, ISLAMABAD. Surgical Grand Round, Pakistan Institute of Medical Sciences (PIMS), Islamabad. September 23, 2005.
Small Bowel Obstruction after operation in a severely malnourished man. By: Ms Bounmark Phoumesy
 Small Bowel Obstruction after operation in a severely malnourished man By: Ms Bounmark Phoumesy Normal length of GI tract Normal length(achieved by age 9) Small bowel 600cm (Men: 630 cm; Women: 592 cm)
Small Bowel Obstruction after operation in a severely malnourished man By: Ms Bounmark Phoumesy Normal length of GI tract Normal length(achieved by age 9) Small bowel 600cm (Men: 630 cm; Women: 592 cm)
NUTRITIONAL REQUIREMENTS
 NUTRITION AIMS To achieve growth and nutrient accretion similar to intrauterine rates To achieve best possible neurodevelopmental outcome To prevent specific nutritional deficiencies Target population
NUTRITION AIMS To achieve growth and nutrient accretion similar to intrauterine rates To achieve best possible neurodevelopmental outcome To prevent specific nutritional deficiencies Target population
8/20/12. Discuss the importance of thermoregulation in the neonate.
 Sharon Rush MSN NNP-BC Discuss the importance of thermoregulation in the neonate. To maintain correct body temperature range in order to: Reduce oxygen consumption Reduce calorie expenditure Maximize metabolic
Sharon Rush MSN NNP-BC Discuss the importance of thermoregulation in the neonate. To maintain correct body temperature range in order to: Reduce oxygen consumption Reduce calorie expenditure Maximize metabolic
BACTERIAL TRANSLOCATION AND INTESTINAL PERMEABILITY IN PRETERM INFANTS
 BACTERIAL TRANSLOCATION AND INTESTINAL PERMEABILITY IN PRETERM INFANTS Dr Paul Fleming Consultant Neonatal Medicine Homerton University Hospital Honorary Research Fellow Barts and the London School of
BACTERIAL TRANSLOCATION AND INTESTINAL PERMEABILITY IN PRETERM INFANTS Dr Paul Fleming Consultant Neonatal Medicine Homerton University Hospital Honorary Research Fellow Barts and the London School of
2015 Prolacta Bioscience
 Housekeeping Items 1 Presentation will be available on-demand http://www.prolacta.com/webinars/feeding-protocols 2 Turn up your speaker volume 3 Use the Ask a Question feature 4 Use the full screen feature
Housekeeping Items 1 Presentation will be available on-demand http://www.prolacta.com/webinars/feeding-protocols 2 Turn up your speaker volume 3 Use the Ask a Question feature 4 Use the full screen feature
Slow versus Fast Enteral Feed Advancements in Very Low Birth Weight Infants: A Randomized Controlled Trial. A. Salhotra and S.
 Original Article Slow versus Fast Enteral Feed Advancements in Very Low Birth Weight Infants: A Randomized Controlled Trial A. Salhotra and S. Ramji From the Neonatal Division, Department of Pediatrics,
Original Article Slow versus Fast Enteral Feed Advancements in Very Low Birth Weight Infants: A Randomized Controlled Trial A. Salhotra and S. Ramji From the Neonatal Division, Department of Pediatrics,
WHAT IS THE EVIDENCE FOR PROBIOTIC SUPPLEMENTATION?
 WHAT IS THE EVIDENCE FOR PROBIOTIC SUPPLEMENTATION? Roger F. Soll, MD H. Wallace Professor of Neonatology University of Vermont President Vermont Oxford Network 19 th International Symposium on Neonatology
WHAT IS THE EVIDENCE FOR PROBIOTIC SUPPLEMENTATION? Roger F. Soll, MD H. Wallace Professor of Neonatology University of Vermont President Vermont Oxford Network 19 th International Symposium on Neonatology
Melinda Elliott, MD Senior Director, Clinical Education and Professional Development, Prolacta Bioscience Neonatologist, Pediatrix Medical Group of
 Melinda Elliott, MD Senior Director, Clinical Education and Professional Development, Prolacta Bioscience Neonatologist, Pediatrix Medical Group of Maryland Breast Milk is for Babies, Cows Milk is for
Melinda Elliott, MD Senior Director, Clinical Education and Professional Development, Prolacta Bioscience Neonatologist, Pediatrix Medical Group of Maryland Breast Milk is for Babies, Cows Milk is for
Prenatal and neonatal gut maturation
 Department of Veterinary Clinical and Animal Sciences Prenatal and neonatal gut maturation Thomas Thymann Comparative Pediatrics and Nutrition Dept. Vet. and Animal Science P.W. Nathanielsz Whom signals
Department of Veterinary Clinical and Animal Sciences Prenatal and neonatal gut maturation Thomas Thymann Comparative Pediatrics and Nutrition Dept. Vet. and Animal Science P.W. Nathanielsz Whom signals
Gut Microbiota and IBD. Vahedi. H M.D Associate Professor of Medicine DDRI
 Gut Microbiota and IBD Vahedi. H M.D Associate Professor of Medicine DDRI 1393.3.1 2 GUT MICROBIOTA 100 Trillion Microbes - 10 times more than cells in our body Collective weight of about 1kg in human
Gut Microbiota and IBD Vahedi. H M.D Associate Professor of Medicine DDRI 1393.3.1 2 GUT MICROBIOTA 100 Trillion Microbes - 10 times more than cells in our body Collective weight of about 1kg in human
NECROTIZING ENTEROCOLITIS
 Necrotising Enterocolitis (NEC) NECROTIZING ENTEROCOLITIS Atan Baas Sinuhaji Department of Childhealth,School of Medicine,University of North Sumatera Medan Affects 0.5 to 1 per 1000 live births Incidence
Necrotising Enterocolitis (NEC) NECROTIZING ENTEROCOLITIS Atan Baas Sinuhaji Department of Childhealth,School of Medicine,University of North Sumatera Medan Affects 0.5 to 1 per 1000 live births Incidence
A Multi center Randomized Trial of Laparotomy vs. Drainage
 A Multi center Randomized Trial of Laparotomy vs. Drainage as the Initial Surgical Therapy for ELBW Infants with Necrotizing Enterocolitis (NEC) or Isolated Intestinal Perforation (IP): Outcomes at 18
A Multi center Randomized Trial of Laparotomy vs. Drainage as the Initial Surgical Therapy for ELBW Infants with Necrotizing Enterocolitis (NEC) or Isolated Intestinal Perforation (IP): Outcomes at 18
Presented by Megan R. Sanctuary, MS University of California at Davis
 Effects of supplementation with Bifidobacterium infantis in combination with bioactive milk components on gastrointestinal symptoms in children with autism Presented by Megan R. Sanctuary, MS University
Effects of supplementation with Bifidobacterium infantis in combination with bioactive milk components on gastrointestinal symptoms in children with autism Presented by Megan R. Sanctuary, MS University
The pathophysiology of necrotizing enterocolitis in preterm infants Heida, Fardou
 University of Groningen The pathophysiology of necrotizing enterocolitis in preterm infants Heida, Fardou IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish
University of Groningen The pathophysiology of necrotizing enterocolitis in preterm infants Heida, Fardou IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish
The Patent Ductus Arteriosus (PDA) and the Preterm Baby. Tanya Hatfield, RNC-NIC, MSN Neonatal Outreach Educator
 and the Preterm Baby. Tanya Hatfield, RNC-NIC, MSN Neonatal Outreach Educator") The Patent Ductus Arteriosus (PDA) and the Preterm Baby Tanya Hatfield, RNC-NIC, MSN Neonatal Outreach Educator Objectives Describe normal cardiac physiology and development Understand the unique physiologic
The Patent Ductus Arteriosus (PDA) and the Preterm Baby Tanya Hatfield, RNC-NIC, MSN Neonatal Outreach Educator Objectives Describe normal cardiac physiology and development Understand the unique physiologic
Bringing Synbiotic Interventions in Cancer to Practice: from bench to bedside The UC Davis Foods for Health Institute
 Bringing Synbiotic Interventions in Cancer to Practice: from bench to bedside The UC Davis Foods for Health Institute Jennifer T. Smilowitz, PhD Associate Director, Human Studies Research jensm@ucdavis.edu
Bringing Synbiotic Interventions in Cancer to Practice: from bench to bedside The UC Davis Foods for Health Institute Jennifer T. Smilowitz, PhD Associate Director, Human Studies Research jensm@ucdavis.edu
ENTERAL NUTRITION IN THE CRITICALLY ILL
 ENTERAL NUTRITION IN THE CRITICALLY ILL 1 Ebb phase Flow phase acute response (catabolic) adoptive response (anabolic) 2 3 Metabolic Response to Stress (catabolic phase) Glucose and Protein Metabolism
ENTERAL NUTRITION IN THE CRITICALLY ILL 1 Ebb phase Flow phase acute response (catabolic) adoptive response (anabolic) 2 3 Metabolic Response to Stress (catabolic phase) Glucose and Protein Metabolism
NEONATAL CLINICAL PRACTICE GUIDELINE
 NEONATAL CLINICAL PRACTICE GUIDELINE Approval Date: January 2015 Approved by: Neonatal Patient Care Teams, HSC & SBH Child Health Standards Committee Pages: 1 of 9 Supercedes: HSC #80.210.440 SBH#118 1.0
NEONATAL CLINICAL PRACTICE GUIDELINE Approval Date: January 2015 Approved by: Neonatal Patient Care Teams, HSC & SBH Child Health Standards Committee Pages: 1 of 9 Supercedes: HSC #80.210.440 SBH#118 1.0
Short Bowel Syndrome: Medical management
 Short Bowel Syndrome: Medical management La Sindrome dell'intestino Corto in età pediatrica Brescia 18 marzo 2011 Jon A.Vanderhoof, M.D. Division of Pediatric GI Harvard Medical School Children s Hospital,
Short Bowel Syndrome: Medical management La Sindrome dell'intestino Corto in età pediatrica Brescia 18 marzo 2011 Jon A.Vanderhoof, M.D. Division of Pediatric GI Harvard Medical School Children s Hospital,
Efficacy of Breast Milk Gastric Lavage in Preterm Neonates. Archana B. Patel and Samiuddin Shaikh
 Research Papers Efficacy of Breast Milk Gastric Lavage in Preterm Neonates Archana B. Patel and Samiuddin Shaikh From the Department of Pediatrics and Clinical Epidemiology Unit, Indira Gandhi Medical
Research Papers Efficacy of Breast Milk Gastric Lavage in Preterm Neonates Archana B. Patel and Samiuddin Shaikh From the Department of Pediatrics and Clinical Epidemiology Unit, Indira Gandhi Medical
Exchange Transfusion
 Approved by: Exchange Transfusion Gail Cameron Director, Maternal, Neonatal & Child Health Programs Neonatal Nursery Policy & Procedures Manual : Next Review March 2016 Dr. Ensenat Medical Director, Neonatology
Approved by: Exchange Transfusion Gail Cameron Director, Maternal, Neonatal & Child Health Programs Neonatal Nursery Policy & Procedures Manual : Next Review March 2016 Dr. Ensenat Medical Director, Neonatology
SWISS SOCIETY OF NEONATOLOGY. Catastrophic gastrointestinal event in a 10-week-old extremely growth restricted preterm infant
 SWISS SOCIETY OF NEONATOLOGY Catastrophic gastrointestinal event in a 10-week-old extremely growth restricted preterm infant APRIL 2011 2 Häberli So, Hausladen Si, Hürlimann Sa, Caduff JH, Esslinger P,
SWISS SOCIETY OF NEONATOLOGY Catastrophic gastrointestinal event in a 10-week-old extremely growth restricted preterm infant APRIL 2011 2 Häberli So, Hausladen Si, Hürlimann Sa, Caduff JH, Esslinger P,
Nutrition Management in GI Diseases
 Nutrition Management in GI Diseases Aryono Hendarto MD Nutrition & Metabolic Diseases Division Department of Child Health Cipto Mangunkusumo Hospital University of Indonesia 1 Patient s Care 1. Drugs 2.
Nutrition Management in GI Diseases Aryono Hendarto MD Nutrition & Metabolic Diseases Division Department of Child Health Cipto Mangunkusumo Hospital University of Indonesia 1 Patient s Care 1. Drugs 2.
ENTERAL NUTRITION Identifying risk of patients for enteral feeding problems: Low risk: Moderate risk: High risk:
 ENTERAL NUTRITION Statement of best practice Feeding with mother s own breastmilk is protective against sepsis, NEC and death All mothers should be informed about this and strongly encouraged to express
ENTERAL NUTRITION Statement of best practice Feeding with mother s own breastmilk is protective against sepsis, NEC and death All mothers should be informed about this and strongly encouraged to express
Rebecca T Slagle, MN, APRN, NNP-BC. Speak up!!
 Rebecca T Slagle, MN, APRN, NNP-BC Speak up!! Objectives: Understand the incidence and prevalence of sepsis in the newborn period Identify the risk factors for neonatal sepsis List the most frequent causative
Rebecca T Slagle, MN, APRN, NNP-BC Speak up!! Objectives: Understand the incidence and prevalence of sepsis in the newborn period Identify the risk factors for neonatal sepsis List the most frequent causative
Clinical Management of Necrotizing Enterocolitis
 Article Clinical Management of Necrotizing Enterocolitis Reed A. Dimmitt, MD,* and R. Lawrence Moss, MD Objectives After completing this article, readers should be able to: 1. List the major risk factor
Article Clinical Management of Necrotizing Enterocolitis Reed A. Dimmitt, MD,* and R. Lawrence Moss, MD Objectives After completing this article, readers should be able to: 1. List the major risk factor
Hypothermia in Neonates with HIE TARA JENDZIO, DNP(C), RN, RNC-NIC
, RN, RNC-NIC") Hypothermia in Neonates with HIE TARA JENDZIO, DNP(C), RN, RNC-NIC Objectives 1. Define Hypoxic-Ischemic Encephalopathy (HIE) 2. Identify the criteria used to determine if an infant qualifies for therapeutic
Hypothermia in Neonates with HIE TARA JENDZIO, DNP(C), RN, RNC-NIC Objectives 1. Define Hypoxic-Ischemic Encephalopathy (HIE) 2. Identify the criteria used to determine if an infant qualifies for therapeutic
GENERAL SURGERY FOR SMART PEOPLE JOE NOLD MD, FACS WICHITA SURGICAL SPECIALISTS
 GENERAL SURGERY FOR SMART PEOPLE JOE NOLD MD, FACS WICHITA SURGICAL SPECIALISTS CONFLICTS/DECLARATIONS I have no financial conflicts or declarations I AM always willing to see a consult for you TEXT TOPICS
GENERAL SURGERY FOR SMART PEOPLE JOE NOLD MD, FACS WICHITA SURGICAL SPECIALISTS CONFLICTS/DECLARATIONS I have no financial conflicts or declarations I AM always willing to see a consult for you TEXT TOPICS
Small bowel atresia. Great Ormond Street Hospital for Children NHS Foundation Trust: Information for Families
 Great Ormond Street Hospital for Children NHS Foundation Trust: Information for Families Small bowel atresia This information sheet from Great Ormond Street Hospital explains the causes, symptoms and treatment
Great Ormond Street Hospital for Children NHS Foundation Trust: Information for Families Small bowel atresia This information sheet from Great Ormond Street Hospital explains the causes, symptoms and treatment
Guslihan Dasa Tjipta Division of Perinatology Department of Child Health Medical School University of Sumatera Utara
 Guslihan Dasa Tjipta Division of Perinatology Department of Child Health Medical School University of Sumatera Utara 1 Definition Perinatal asphyxia is a fetus/newborn, due to: is an insult to the Lack
Guslihan Dasa Tjipta Division of Perinatology Department of Child Health Medical School University of Sumatera Utara 1 Definition Perinatal asphyxia is a fetus/newborn, due to: is an insult to the Lack
The impact of the microbiome on brain and cognitive development
 The Gut-Brain Axis The impact of the microbiome on brain and cognitive development Diane Stadler, PhD, RD Oregon Health & Sciences University, Portland, Oregon Lao-American Nutrition Institute With acknowledgements
The Gut-Brain Axis The impact of the microbiome on brain and cognitive development Diane Stadler, PhD, RD Oregon Health & Sciences University, Portland, Oregon Lao-American Nutrition Institute With acknowledgements
... Inflammatory disorder of the colon that occurs as a complication of antibiotic treatment.
 Definition Inflammatory disorder of the colon that occurs as a complication of antibiotic treatment. " Epidemiology Humans represent the main reservoir of Clostridium difficile, which is not part of the
Definition Inflammatory disorder of the colon that occurs as a complication of antibiotic treatment. " Epidemiology Humans represent the main reservoir of Clostridium difficile, which is not part of the
Effects of Probiotics on the Reduction in Incidence of Necrotizing Enterocolitis in Premature (< 37 Weeks Gestation) Neonates
 Neonates") University of Central Florida Honors in the Major Theses Open Access Effects of Probiotics on the Reduction in Incidence of Necrotizing Enterocolitis in Premature (< 37 Weeks Gestation) Neonates 2016 Makenzie
University of Central Florida Honors in the Major Theses Open Access Effects of Probiotics on the Reduction in Incidence of Necrotizing Enterocolitis in Premature (< 37 Weeks Gestation) Neonates 2016 Makenzie
Malabsorption: etiology, pathogenesis and evaluation
 Malabsorption: etiology, pathogenesis and evaluation Peter HR Green NORMAL ABSORPTION Coordination of gastric, small intestinal, pancreatic and biliary function Multiple mechanisms Fat protein carbohydrate
Malabsorption: etiology, pathogenesis and evaluation Peter HR Green NORMAL ABSORPTION Coordination of gastric, small intestinal, pancreatic and biliary function Multiple mechanisms Fat protein carbohydrate
Objectives. Birth Depression Management. Birth Depression Terms
 Objectives Birth Depression Management Regional Perinatal Outreach Program 2016 Understand the terms and the clinical characteristics of birth depression. Be familiar with the evidence behind therapeutic
Objectives Birth Depression Management Regional Perinatal Outreach Program 2016 Understand the terms and the clinical characteristics of birth depression. Be familiar with the evidence behind therapeutic
HOW TO DO EARLY NUTRITION in VLBW INFANTS. David H Adamkin M.D. University of Louisville USA
 HOW TO DO EARLY NUTRITION in VLBW INFANTS David H Adamkin M.D. University of Louisville USA NUTRITIONAL CHALLENGES in EARLY NUTRITION Strategies to Prevent Postnatal Growth Failure Early Total Parenteral
HOW TO DO EARLY NUTRITION in VLBW INFANTS David H Adamkin M.D. University of Louisville USA NUTRITIONAL CHALLENGES in EARLY NUTRITION Strategies to Prevent Postnatal Growth Failure Early Total Parenteral
ROLE OF THE GUT BACTERIA
 ROLE OF THE GUT BACTERIA Our Good Bacteria In a perfect world, we would all have a proper ratio of good bacteria And what could this proper ratio do for us? The knowledge of the connections between our
ROLE OF THE GUT BACTERIA Our Good Bacteria In a perfect world, we would all have a proper ratio of good bacteria And what could this proper ratio do for us? The knowledge of the connections between our
ESPEN Congress The Hague 2017
 ESPEN Congress The Hague 2017 Meeting nutritional needs of acute care patients Feeding acute pancreatitis patients J. Luttikhold (NL) FEEDING ACUTE PANCREATITIS PATIENTS Joanna Luttikhold, MD PhD Registrar
ESPEN Congress The Hague 2017 Meeting nutritional needs of acute care patients Feeding acute pancreatitis patients J. Luttikhold (NL) FEEDING ACUTE PANCREATITIS PATIENTS Joanna Luttikhold, MD PhD Registrar
Functional Nutrition Approaches to Gut Health 20 CPEU Module accredited by Nutrition Mission
 Topics Covered 1. Good Health Starts in the Gut 2. Microbiome Part 1 3. Microbiome Part 2 4. What Can Go Wrong 5. FODMAP Intolerance 6. GERD 7. Celiac Disease 8. Non-Celiac Gluten Sensitivity 9. Intestinal
Topics Covered 1. Good Health Starts in the Gut 2. Microbiome Part 1 3. Microbiome Part 2 4. What Can Go Wrong 5. FODMAP Intolerance 6. GERD 7. Celiac Disease 8. Non-Celiac Gluten Sensitivity 9. Intestinal
3/30/18. Common Radiology Studies in Pediatric Surgery. Disclosure Information. Objectives
 Common Radiology Studies in Pediatric Surgery A Scenario Based Approach to Interpretation for the Pediatric Nurse and Provider presented by Elizabeth A. Paton, DNP, RN-BC, PNP-A, PPCNP-BC, CPEN, FAEN Disclosure
Common Radiology Studies in Pediatric Surgery A Scenario Based Approach to Interpretation for the Pediatric Nurse and Provider presented by Elizabeth A. Paton, DNP, RN-BC, PNP-A, PPCNP-BC, CPEN, FAEN Disclosure
The role of gut microbiome in IBS
 The role of gut microbiome in IBS Chung Owyang, MD H. Marvin Pollard Professor of Internal Medicine Professor of Molecular and Integrative Physiology Chief, Division of Gastroenterology Director, Pollard
The role of gut microbiome in IBS Chung Owyang, MD H. Marvin Pollard Professor of Internal Medicine Professor of Molecular and Integrative Physiology Chief, Division of Gastroenterology Director, Pollard
General Data. 王 X 村 78 y/o 男性
 General Data 王 X 村 78 y/o 男性 Chief Complaint Vomiting twice this early morning Fever up to 38.9ºC was noted Present Illness (1) Old CVA with left side weakness for more than 10 years and with bed ridden
General Data 王 X 村 78 y/o 男性 Chief Complaint Vomiting twice this early morning Fever up to 38.9ºC was noted Present Illness (1) Old CVA with left side weakness for more than 10 years and with bed ridden
Indian Pediatrics - Editorial
 Page 1 of 7 Home Past Issue About IP About IAP Feedback Links Author Info. Subscription Original Articles Indian Pediatrics 2004; 41:435-441 Slow versus Fast Enteral Feed Advancements in Very Low Birth
Page 1 of 7 Home Past Issue About IP About IAP Feedback Links Author Info. Subscription Original Articles Indian Pediatrics 2004; 41:435-441 Slow versus Fast Enteral Feed Advancements in Very Low Birth
SWISS SOCIETY OF NEONATOLOGY. Neonatal gastric perforation
 SWISS SOCIETY OF NEONATOLOGY Neonatal gastric perforation September 2002 2 Zankl A, Stähelin J, Roth K, Boudny P and Zeilinger G, Children s Hospital of Aarau (ZA, SJ, RK, ZG) and Institute of Pathology
SWISS SOCIETY OF NEONATOLOGY Neonatal gastric perforation September 2002 2 Zankl A, Stähelin J, Roth K, Boudny P and Zeilinger G, Children s Hospital of Aarau (ZA, SJ, RK, ZG) and Institute of Pathology
1/3/2008. Karen Burke Priscilla LeMone Elaine Mohn-Brown. Medical-Surgical Nursing Care, 2e Karen Burke, Priscilla LeMone, and Elaine Mohn-Brown
 Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 20 Caring for Clients with Bowel Disorders Diarrhea Pathophysiology Result from impaired water absorption
Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 20 Caring for Clients with Bowel Disorders Diarrhea Pathophysiology Result from impaired water absorption
7/18/13. Outline of Talk. Neonatal bowel injury: Diverting energy to avoid a nutritional crisis. The Developing Gut. Types of Bowel Injury
 Outline of Talk Neonatal bowel injury: Diverting energy to avoid a nutritional crisis Jae Kim MD PhD Neonatology & Pediatric Gastroenterology Hepatology and Nutrition May 13, 2013 SCANN meeting UCSD Auditorium
Outline of Talk Neonatal bowel injury: Diverting energy to avoid a nutritional crisis Jae Kim MD PhD Neonatology & Pediatric Gastroenterology Hepatology and Nutrition May 13, 2013 SCANN meeting UCSD Auditorium
Neonatal intestinal obstruction: how to make etiological diagnosis?
 Neonatal intestinal obstruction: how to make etiological diagnosis? Poster No.: C-1414 Congress: ECR 2013 Type: Educational Exhibit Authors: W. Mnari, M. Zguidi, A. Zrig, M. Maatouk, B. Hmida, R. Salem,
Neonatal intestinal obstruction: how to make etiological diagnosis? Poster No.: C-1414 Congress: ECR 2013 Type: Educational Exhibit Authors: W. Mnari, M. Zguidi, A. Zrig, M. Maatouk, B. Hmida, R. Salem,
Crohn's Disease. What causes Crohn s disease? What are the symptoms?
 Crohn's Disease Crohn s disease is an ongoing disorder that causes inflammation of the digestive tract, also referred to as the gastrointestinal (GI) tract. Crohn s disease can affect any area of the GI
Crohn's Disease Crohn s disease is an ongoing disorder that causes inflammation of the digestive tract, also referred to as the gastrointestinal (GI) tract. Crohn s disease can affect any area of the GI
Intestinal Microbiota in Health and Disease
 Intestinal Microbiota in Health and Disease February 27, 2015 Master s Course in Gastroenterology Prof. Kathy McCoy 1 Overview Overview of Gut Microbiota Microbiota in Health Microbiota in Disease 2 Gut
Intestinal Microbiota in Health and Disease February 27, 2015 Master s Course in Gastroenterology Prof. Kathy McCoy 1 Overview Overview of Gut Microbiota Microbiota in Health Microbiota in Disease 2 Gut
Neonatal intestinal obstruction: how to make etiological diagnosis?
 Neonatal intestinal obstruction: how to make etiological diagnosis? Poster No.: C-1414 Congress: ECR 2013 Type: Educational Exhibit Authors: W. MNARI, M. Zguidi, A. Zrig, M. MAATOUK, B. Hmida, R. Salem,
Neonatal intestinal obstruction: how to make etiological diagnosis? Poster No.: C-1414 Congress: ECR 2013 Type: Educational Exhibit Authors: W. MNARI, M. Zguidi, A. Zrig, M. MAATOUK, B. Hmida, R. Salem,
Scott A. Lynch, MD, MPH,FAAFP Assistant Professor
 Scott A. Lynch, MD, MPH,FAAFP Assistant Professor Lynch.Scott@mayo.edu 2015 MFMER 3543652-1 Nutrition in the Hospital Mayo School of Continuous Professional Development 2nd Annual Inpatient Medicine for
Scott A. Lynch, MD, MPH,FAAFP Assistant Professor Lynch.Scott@mayo.edu 2015 MFMER 3543652-1 Nutrition in the Hospital Mayo School of Continuous Professional Development 2nd Annual Inpatient Medicine for
Patent Ductus Arteriosus: Philosophy or Pathology?
 Patent Ductus Arteriosus: Philosophy or Pathology? Disclosure Ray Sato, MD is a speaker for Prolacta Biosciences, Inc. This presentation will discuss off-label uses of acetaminophen and ibuprofen. RAY
Patent Ductus Arteriosus: Philosophy or Pathology? Disclosure Ray Sato, MD is a speaker for Prolacta Biosciences, Inc. This presentation will discuss off-label uses of acetaminophen and ibuprofen. RAY
Studies on probiotics effects on innate immune functions in the gastrointestinal tract of broiler chicks (SUMMARY)
") Doctoral Thesis Studies on probiotics effects on innate immune functions in the gastrointestinal tract of broiler chicks (SUMMARY) ELSAYED SEDDEK IBRAHEM MOHAMMED Department of Bioresource Science Graduate
Doctoral Thesis Studies on probiotics effects on innate immune functions in the gastrointestinal tract of broiler chicks (SUMMARY) ELSAYED SEDDEK IBRAHEM MOHAMMED Department of Bioresource Science Graduate
Infant Nutrition & Growth to Optimize Outcome Fauzia Shakeel, MD
 Infant Nutrition & Growth to Optimize Outcome Fauzia Shakeel, MD Neonatologist All Children s Hospital / Johns Hopkins Medicine Affiliate Assistant Professor, University of South Florida September 2014
Infant Nutrition & Growth to Optimize Outcome Fauzia Shakeel, MD Neonatologist All Children s Hospital / Johns Hopkins Medicine Affiliate Assistant Professor, University of South Florida September 2014
Surgical Management of IBD. Val Jefford Grand Rounds October 14, 2003
 Surgical Management of IBD Val Jefford Grand Rounds October 14, 2003 Introduction Important Features Clinical Presentation Evaluation Medical Treatment Surgical Treatment Cases Overview Introduction Two
Surgical Management of IBD Val Jefford Grand Rounds October 14, 2003 Introduction Important Features Clinical Presentation Evaluation Medical Treatment Surgical Treatment Cases Overview Introduction Two
Objectives: Resources:
 Objectives: Realize the impact of Age : - Where/who are the history sources Recognize and interpret the : - Important symptoms - Important signs Resources: Davidson s. Slides Surgical recall. Raslan s
Objectives: Realize the impact of Age : - Where/who are the history sources Recognize and interpret the : - Important symptoms - Important signs Resources: Davidson s. Slides Surgical recall. Raslan s
Mohamed EL-hemaly Gastro- intestinal surgical center, Mansoura University.
 Mohamed EL-hemaly Gastro- intestinal surgical center, Mansoura University. Chronic transmural inflammatory process of the bowel & affects any part of the gastro -intestinal tract from the mouth to the
Mohamed EL-hemaly Gastro- intestinal surgical center, Mansoura University. Chronic transmural inflammatory process of the bowel & affects any part of the gastro -intestinal tract from the mouth to the
Objectives. Apnea Definition and Pitfalls. Pathophysiology of Apnea. Apnea of Prematurity and hypoxemia episodes 5/18/2015
 Apnea of Prematurity and hypoxemia episodes Deepak Jain MD Care of Sick Newborn Conference May 2015 Objectives Differentiating between apnea and hypoxemia episodes. Pathophysiology Diagnosis of apnea and
Apnea of Prematurity and hypoxemia episodes Deepak Jain MD Care of Sick Newborn Conference May 2015 Objectives Differentiating between apnea and hypoxemia episodes. Pathophysiology Diagnosis of apnea and
Extremely well tolerated. Feeding shock
 Extremely well tolerated Feeding shock FEEDING DURING CIRCULATORY FAILURE Dr S Omar Chris Hani Baragwanath Hospital Hospital/University of Witwatersrand Introduction Circulatory shock lack of adequate
Extremely well tolerated Feeding shock FEEDING DURING CIRCULATORY FAILURE Dr S Omar Chris Hani Baragwanath Hospital Hospital/University of Witwatersrand Introduction Circulatory shock lack of adequate
The Intestinal Microbiota and the Developing Immune System
 The Intestinal Microbiota and the Developing Immune System 4 Feb 2016 The Intestinal Microbiota 10 fold more bacterial cells than human cells 100-1000 fold more bacterial genes than human genes Why does
The Intestinal Microbiota and the Developing Immune System 4 Feb 2016 The Intestinal Microbiota 10 fold more bacterial cells than human cells 100-1000 fold more bacterial genes than human genes Why does
Objectives. Pediatric Mortality. Another belly pain. Gastroenteritis. Spewing & Pooing Child 4/18/16
 Gastro-tastrophies A Review of Pediatric GI Emergencies Objectives Discuss common presentations of Pediatric Abdominal Pain complaints Discuss work up and physical exam findings Discuss care, management
Gastro-tastrophies A Review of Pediatric GI Emergencies Objectives Discuss common presentations of Pediatric Abdominal Pain complaints Discuss work up and physical exam findings Discuss care, management
FIBER HEALTH BENEFITS
 FIBER FIBER HEALTH BENEFITS Normal Laxation: Increase stool weight from fiber, water retained by fiber and bacterial mass Eases defecation and prevents or relieves constipation Cereal fibers are best;
FIBER FIBER HEALTH BENEFITS Normal Laxation: Increase stool weight from fiber, water retained by fiber and bacterial mass Eases defecation and prevents or relieves constipation Cereal fibers are best;
Human milk. The Gold Standard. Human milk. Human milk. Human milk. Human milk. 3 Types of Human Milk 4/23/2015
 The Gold Standard Defining characteristic of the class Mammalian Ability to produce designed specifically to nourish the young It is a unique complex fluid with a species specific composition It is the
The Gold Standard Defining characteristic of the class Mammalian Ability to produce designed specifically to nourish the young It is a unique complex fluid with a species specific composition It is the
INTESTINAL OBSTRUCTION ESCAPED SURGERY: MECONIUM PLUG
 7 INTESTINAL OBSTRUCTION ESCAPED SURGERY: MECONIUM PLUG Oluwayemi IO 1 *, Ade-Ojo IP 2, Olofinbiyi BA 2 1. Department of Paediatrics, Ekiti State University Teaching Hospital, Ado-Ekiti, Ekiti State, Nigeria
7 INTESTINAL OBSTRUCTION ESCAPED SURGERY: MECONIUM PLUG Oluwayemi IO 1 *, Ade-Ojo IP 2, Olofinbiyi BA 2 1. Department of Paediatrics, Ekiti State University Teaching Hospital, Ado-Ekiti, Ekiti State, Nigeria
OB Well Baby Nursery Admission (Term) [ ] For specialty focused order sets for your patient, refer to: General
![OB Well Baby Nursery Admission (Term) [ ] For specialty focused order sets for your patient, refer to: General](/thumbs/85/91909911.jpg "OB Well Baby Nursery Admission (Term) [ ] For specialty focused order sets for your patient, refer to: General") OB Well Baby Nursery Admission (Term) [3040000234] For specialty focused order sets for your patient, refer to: 3040000424 Neonatal Circumcision Order Set 3040000522 Neonatal Herpes Viral Order Set 3040000524
OB Well Baby Nursery Admission (Term) [3040000234] For specialty focused order sets for your patient, refer to: 3040000424 Neonatal Circumcision Order Set 3040000522 Neonatal Herpes Viral Order Set 3040000524
Principles of nutrition in the preterm infant. Importance of nutrition: Undernutrition is very common in VLBW infants
 Principles of nutrition in the preterm infant Dr. S. Navarro-Psihas Pädiatrie IV, Klinik für Neonatologie Medizinische Universität Innsbruck Importance of nutrition: Undernutrition is very common in VLBW
Principles of nutrition in the preterm infant Dr. S. Navarro-Psihas Pädiatrie IV, Klinik für Neonatologie Medizinische Universität Innsbruck Importance of nutrition: Undernutrition is very common in VLBW
Enteral Nutrition: Whom, Why, When, What and Where to Feed?
 Meier RF, Reddy BR, Soeters PB (eds): The Importance of Nutrition as an Integral Part of Disease Management. Nestlé Nutr Inst Workshop Ser, vol 82, pp 53 59, (DOI: 10.1159/000382002) Nestec Ltd., Vevey/S.
Meier RF, Reddy BR, Soeters PB (eds): The Importance of Nutrition as an Integral Part of Disease Management. Nestlé Nutr Inst Workshop Ser, vol 82, pp 53 59, (DOI: 10.1159/000382002) Nestec Ltd., Vevey/S.
Hyaline membrane disease. By : Dr. Ch Sarishma Peadiatric Pg
 Hyaline membrane disease By : Dr. Ch Sarishma Peadiatric Pg Also called Respiratory distress syndrome. It occurs primarily in premature infants; its incidence is inversely related to gestational age and
Hyaline membrane disease By : Dr. Ch Sarishma Peadiatric Pg Also called Respiratory distress syndrome. It occurs primarily in premature infants; its incidence is inversely related to gestational age and
220 SUBJECT INDEX. D Diarrhea and sodium balance, 74 weanling, 161,179,208,212; see also Infection
 Subject Index Acid balance, see ph Allergy, food, see also Immunity and beikost, 143-144 and breast milk, 91,143 and formula, 89-90 Antidiuretic hormone, 66 67 Antigens, see also Immunity determinants,
Subject Index Acid balance, see ph Allergy, food, see also Immunity and beikost, 143-144 and breast milk, 91,143 and formula, 89-90 Antidiuretic hormone, 66 67 Antigens, see also Immunity determinants,
LOOKING FOR AIR IN ALL THE WRONG PLACES Richard M. Gore, MD North Shore University Health System University of Chicago Evanston, IL
 SIGNIFICANCE OF EXTRALUMINAL ABDOMINAL GAS: LOOKING FOR AIR IN ALL THE WRONG PLACES Richard M. Gore, MD North Shore University Health System University of Chicago Evanston, IL SCBT/MR 2012 October 26,
SIGNIFICANCE OF EXTRALUMINAL ABDOMINAL GAS: LOOKING FOR AIR IN ALL THE WRONG PLACES Richard M. Gore, MD North Shore University Health System University of Chicago Evanston, IL SCBT/MR 2012 October 26,
Current concepts in Critical Care Nutrition
 Current concepts in Critical Care Nutrition Dr.N.Ramakrishnan AB (Int Med), AB (Crit Care), MMM, FACP, FCCP, FCCM Director, Critical Care Services Apollo Hospitals, Chennai Objectives Why? Enteral or Parenteral
Current concepts in Critical Care Nutrition Dr.N.Ramakrishnan AB (Int Med), AB (Crit Care), MMM, FACP, FCCP, FCCM Director, Critical Care Services Apollo Hospitals, Chennai Objectives Why? Enteral or Parenteral