By Kevin Solinsky, CPC, CPC-I, CEDC, CEMC
|
|
|
- Kelly Casey
- 5 years ago
- Views:
Transcription


1 By Kevin Solinsky, CPC, CPC-I, CEDC, CEMC


2 Learn components of the ED E&M Medical Necessity vs MDM Critical Care coding Procedure coding Orthopedic coding
3 Emergency Room Services Critical Care & Observation ,
4 There are 7 components to define the levels of E/M services: History Examination Medical Decision Making Counseling Coordination of Care Nature of Presenting Problem Time (CC)
5 History Exam Medical Decision Making
6 Chief Complaint (CC) required on all charts History of Present Illness (HPI) (4 of 8 should be on every chart) Review of Systems (ROS) ( 2-9, 10 OR MORE) Past Medical, Family and Social History (PMFSH) ( 2 of the 3 should be documented)
7 The ROS and or PFSH may be recorded by ancillary staff or on a form completed by the pt. To document that the physician reviewed the information, there must be a notation supplementing or confirming the information recorded by others

8 HPI is a chronological description of the development of the patient s present illness from the first sign and/or symptom or from the previous encounter to the present.
9 Location Context Quality Timing Severity Duration Modifying Factors Associated Signs and Symptoms
10 Location RUQ Left Upper Lower Anterior Distal 3 rd digit Context (allows for e codes) Sharpening a knife Occurred at. During. While. Bit by rat
11 Duration For 3 hours Started this morning For a month Since yesterday Timing In the afternoons Daily Intermittent Constant 20 minutes after..

12 Quality Sharp Throbbing Stabbing Crushing burning Severity Rated a out of 10 Severe Improving moderate
13 Modifying Factors Took Motrin Tried massage Exacerbated by Relieved by Not affected by Associated Signs and Symptoms No nausea or vomiting Also with cough Also complains of
14 Brief HPI 1-3 elements from above Extended HPI at least 4 elements Charts that you could bill as 4-5 get down coded if HPI does not have 4 elements
15 Quality over Quantity Cc: Chest Pain HPI: This is a 10 year old boy who presented to the ED complaining of throbbing posterior chest pain over the past 5 hours. Pt rates pain a 7 out of 10. duration Quality Location Severity
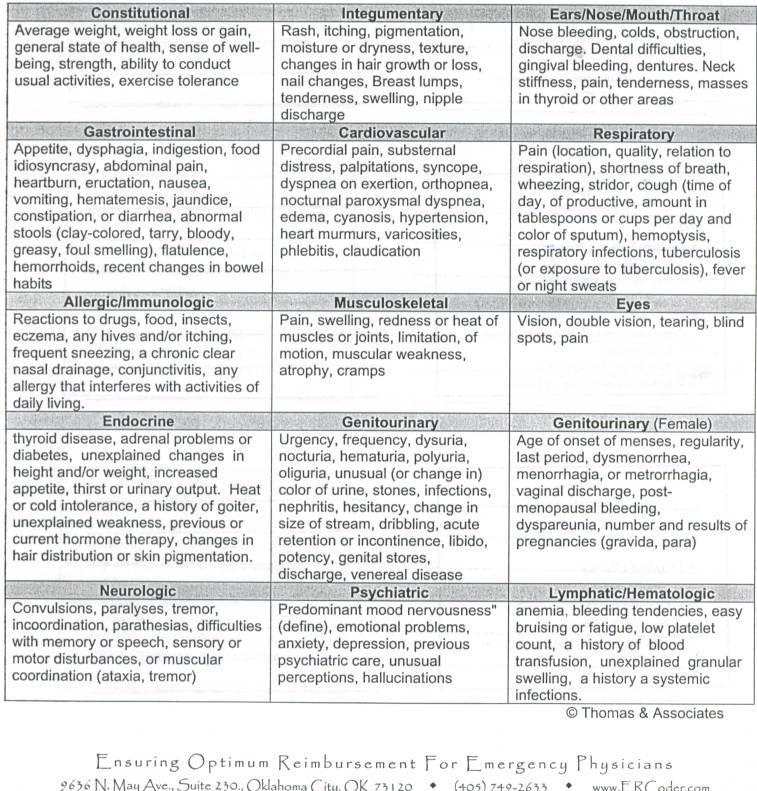
16 Allergic/Immunologic Cardiovascular Constitutional Ears, Nose, Mouth, Throat Endocrine Eye Gastrointestinal Genitourinary Hematologic/Lymph Integumentary Musculoskeletal Neurologic Psychiatric Respiratory
17 99282/99283 Problem pertinent ROS = 1 system Extended ROS 2-9 systems Complete ROS at least 10 symptoms May make statement all other systems reviewed and are negative means you reviewed all 14 systems!!
18
19 A pertinent PFS consists of any 1 element from the PFS = pertinent A complete PFS consists of 2 elements from 2 of the PFS areas Complete need 2
20 99281 Problem Focused History CC Brief History of Present Illness 99282/99283 Expanded Problem Focused History CC Brief History of Present Illness/Problem Pertinent ROS
21 99284 Detailed History CC Extended History of Present Illness Extended Review of Systems Problem pertinent past, family social history.

22 99285 Comprehensive History CC Extended History of present illness Complete review of systems Complete past, family, social history

23 99284 or downcoded to a Only brief HPI documented. A brief HPI limits code to downcoded to requires a complete ROS requires a complete PFS History

24 If unable to get a history from pt or source You must document the reason history is not obtained and documented in the record State specifically where the documented history was obtained Indicate what other sources for history were unavailable
25 7 body areas Head including face Neck Chest including breasts and axilla Abdomen Back Genitalia, groin, buttocks Each extremity 11 organ systems Eyes ENT Cardiovascular Respiratory Genitourinary Musculoskeletal Skin Neurologic Psychiatric Hematologic/lymphatic It s just as important to document negative findings as positives.
26 99281 Problem Focused 1 body area or system Detailed 2-7 body areas or systems 1 in detail 99282/99283 Expanded problem focused 2-7 BODY AREAS Comprehensive 8 or more Organ Systems
27 Medical decision making refers to the complexity of establishing a diagnosis and/or selecting a management option as measured by: The number of possible diagnosis and/or or the number of management options that must be considered. The amount and/or complexity of medical records, diagnostic tests, and/or other info. That must be obtained, reviewed and analyzed. The risk of significant complications, morbidity and/or mortality, as well as co-morbidities, associated with the patient s presenting problem(s), the diagnostic procedure(s) and /or the possible management options.
28 Must meet or exceed 2 out of 3 Straight Forward Low Complex Moderate Complexity High Complexity # of diagnosis or TX options (total points) 1 = minimal 2 = Limited 3 = Multiple** 4 or more = Extensive** Amt or complexit y or Data (total points) 1 = minimal 2 = Limited 3 = Multiple** 4 or more = Extensive** Level of risk Minimal Low Moderate High
 No additional workup needed 3 points **New problem (to examiner) 4 points Additional workup")
29 Problems to Examining Physician_ Points Self Limited or Minor 1 point Est problem (to examiner) stable 1 point Est problem (to examiner) worsening 2 point **New problem (to examiner) No additional workup needed 3 points **New problem (to examiner) 4 points Additional workup needed/planned

30 Level of risk Presenting problem Diagnostic Procedures Ordered Management options Selected Minimal 1 self limited or minor problem Lab tests via venipuncture, xrays, ua, EKG, US Rest, gargle, bandages dressings Low 2 or more self limited or minor problems, 1 stable chronic disease, acute uncomplicated illness/injury Physiological w/o stress, lab via art puncture, superficial biopsy, noncv imaging w/contrast Minor surgery no risk factors, OTC drugs, IV therapy no additives, PT & OT Moderate Chronic illness w/exacerbation, 2 stable chronic illnesses, acute illness w/ systemic sxs, complicated acute injury Physiological w/stress, deep biopsies, obtain fluid from body cavity, endoscopy or cv imaging no risk factors Minor surgery w/risk factors, RX drug, IV w/additives, closed tx fx or dislocation High Chronic illness w/ severe exacerbation, illness/injury that pose a threat to life or bodyily fxn, abrupt in neuro status Endoscopies or cv imaging w/ risk factors Elective minor surgery w/risk factors, emergency surgery, RX w/monitoring, DNR decision, Parental
31 History Exam MDM Problem Focused Expanded Problem Focused Expanded Problem Focused Problem Focused Expanded Problem Focused Expanded Problem Focused Straightfor ward Low Complexity Moderate Complexity Detailed Detailed Moderate Complexity Comprehensive Comprehensive High
32 99281 Self Limited or minor Low to moderate severity Moderate severity High severity, and require urgent evaluation by the doc but do not pose an immediate significant threat to life or physiologic function high severity and pose an immediate significant threat to life or physiologic function.
33 Medical Necessity verses Medical Decision Making
34 It would not be medically necessary or appropriate to bill a higher level of evaluation and management service when a lower level of service is warranted. The volume of documentation should not be the primary influence upon which a specific level of service is billed. Documentation should support the level of service reported.
35 Discussion
36 Critical Care: Evaluation and management of the critically ill or critically injured pt, requiring the constant attendance of the physician.
37 Critical care services include but are not limited to the treatment or prevention of further deterioration of CNS failure, circulatory failure, shock-like conditions, renal, hepatic, metabolic, or respiratory failure, postop complications or overwhelming infection.
38 There is a high probability of sudden, clinically significant, or life threatening deterioration in the pts condition that requires the highest level of physician preparedness to intervene urgently. Withdrawal of or failure to initiate these interventions on an urgent basis would likely result in sudden, clinically significant or life threatening deterioration in the pts condition.
39 Critical Care services are billed based on the total physician attendance time at the bed side, Time entered does need to be at bedside. Time reported does not need to be continuous. The time can be totaled from multiple encounters on the same day. Must document critical care time of greater than 30 minutes.
40 Documented Critical Care time should include: Time at bedside with the pt Conversations with other personnel regarding pt Clinically necessary conversations with family when pt is unable to participate in decisions Review of test results Documentation of encounter

41 Documented Critical Care time should not include: Time performing separate billable procedures Time spent by residents managing the pt Time spent in teaching sessions with the residents
42 The interpretation of cardiac output measurements CXRT Pulse ox Blood gases Information data stored in computers Gastric intubation Transcutaneous pacing Ventilator management Vascular access procedures

43 Endotracheal intubation Periocardiocentesis Central Venous Catheter Chest Tube CPR The docs progress note must document that time involved in the performance of separately billable procedures was not counted toward critical care time.
44 Document procedures step by step and not as a whole Identify location of injury Document who performed minor procedures
45 3 levels Simple, intermediate, complex Document Number of layers closed Location of injury Length of wound Extra cleaning or debridement beyond normal
46 Procedure 3.0 cm right cheek laceration was anesthetized with 3.0ml LET Solution and subsequently Lidocaine 1% without Epinephrine 2ml via small gauge needle into the margin. The wound was copiously irrigated and 1 small foreign body was removed. 5-0 Prolene sutures simple interrupted x 4 were placed with excellent apposition of the wound edges. Pt tolerated procedure.
47 Splinting a fracture that will require reduction or other treatment at a subsequent time is considered supportive or temporary If the fx is definitively treated by splinting or other care provided in the E, the treatment is considered restorative or definitive
48 The exact location of the fracture or dislocation must be noted. Clear documentation of care provided in the Emergency Department is required. Reduction, stabilization, devices and materials utilized as well as who provided the care should be noted.
49 For non-medicare pts in the ed the doc must either apply the splint/cast or perform a post-placement check of the application in order to bill for the service

50

51

52
53 Many providers do not understand that Medical Necessity is the driving force for picking the appropriate E&M service.

54 This diagnosis is a clear example that the patient age, tests ordered and treatment plan are what drive the level of service that should be coded.

55 99282:no tests or treatment sent home to take Tylenol :You order blood, and urine no medications, home on Tylenol or Motrin 99284: Blood work, urine, IV fluids, IV or IM medications may go home on antibiotics or not : Blood work, urine, IV fluids, Spinal Tap, IV antibiotics and administration to the hospital for R/o sepsis.
56 Chest Pain or abdominal pain always generate a higher level of medical necessity due to the possibilities with regards to diagnoses.
57 This also can drive the level you bill.
58 We are going to look at charts and review all the components and determine E&M and procedures that can and should be coded.
59 Disclaimer: You can put 5 certified coders in a room together and give them the same charts. They can all code them just a little different and still have the same outcome. Coding is not a science we are not perfect and can learn from each other..
60 Questions
61 Kevin Solinsky, CPC, CPC-I, CEDC, CEMC Healthcare Coding Consultants, LLC
Documentation- Overview. Coding for Emergency Department Services. Documentation Guidelines
 Documentation- Overview Coding for Emergency Department Services Sarah Todt, RN, CPC, CPMA, CEDC Documentation Guidelines CMS 1995 CMS 1997 May choose guidelines that are most favorable to the provider
Documentation- Overview Coding for Emergency Department Services Sarah Todt, RN, CPC, CPMA, CEDC Documentation Guidelines CMS 1995 CMS 1997 May choose guidelines that are most favorable to the provider
Optional Session: Intro to Emergency Department Coding And Advanced Procedure Coding for Emergency Medicine. February 22, 2017 Palm Springs, CA
 Optional Session: Intro to Emergency Department Coding And Advanced Procedure Coding for Emergency Medicine (*)Todd Thomas, CCS-P President, ERcoder, Inc; Oklahoma City, Oklahoma; Past-President, Oklahoma
Optional Session: Intro to Emergency Department Coding And Advanced Procedure Coding for Emergency Medicine (*)Todd Thomas, CCS-P President, ERcoder, Inc; Oklahoma City, Oklahoma; Past-President, Oklahoma
How to Code Correctly for E/M Services (1997 Guidelines)
") How to Code Correctly for E/M Services (1997 Guidelines) Phillip Ward, DPM CPT Editorial Board Advisor for Foot and Ankle Former CPT Assistant Editorial Board Member Past President, APMA General Principles
How to Code Correctly for E/M Services (1997 Guidelines) Phillip Ward, DPM CPT Editorial Board Advisor for Foot and Ankle Former CPT Assistant Editorial Board Member Past President, APMA General Principles
COA Advanced Practice Provider Call
 COA Advanced Practice Provider Call Tuesday, September, 19 th, 12:30 pm ET 2015 Community Oncology Alliance 1 CAPP Co-Chairs: Sara Pearce, NP-C, Cancer Care of WNC spearce@cancercareofwnc.com Diana Youngs,
COA Advanced Practice Provider Call Tuesday, September, 19 th, 12:30 pm ET 2015 Community Oncology Alliance 1 CAPP Co-Chairs: Sara Pearce, NP-C, Cancer Care of WNC spearce@cancercareofwnc.com Diana Youngs,
CONSULTATION REFRESHER
 060310 BLAST CONSULTATION REFRESHER We have had many requests from clients recently asking how to correctly code Medicare consultations utilizing the new CMS requirements. Attached is a mini refresher
060310 BLAST CONSULTATION REFRESHER We have had many requests from clients recently asking how to correctly code Medicare consultations utilizing the new CMS requirements. Attached is a mini refresher
2
 1 2 3 4 5 Elements: Location, Timing, Associated Sign and Symptom, Duration Type of History HPI Problem Focused (99201, 99213) Brief (1-3) Expanded Focused (99202, 99213 Brief (1-3) Detailed (99203, 99214)
1 2 3 4 5 Elements: Location, Timing, Associated Sign and Symptom, Duration Type of History HPI Problem Focused (99201, 99213) Brief (1-3) Expanded Focused (99202, 99213 Brief (1-3) Detailed (99203, 99214)
Practical E/M Audit Form: Initial Outpatient Visit (p.1)
") Patient: Name: Chart #: Date of visit: / / Reviewed by: Date of review: / / Practical E/M Audit Form: Initial Outpatient Visit (p.1) Medical History Review Select the level corresponding to lowest of the
Patient: Name: Chart #: Date of visit: / / Reviewed by: Date of review: / / Practical E/M Audit Form: Initial Outpatient Visit (p.1) Medical History Review Select the level corresponding to lowest of the
10/17/2013. Billing and Coding in Long Term Care: Keeping the Wolves at Bay. Disclosure
 Billing and Coding in Long Term Care: Keeping the Wolves at Bay Maine Medical Directors Association Annual Conference October 11, 2013 Alva S Baker, MD, CMD-R Disclosure Dr. Baker has indicated that he
Billing and Coding in Long Term Care: Keeping the Wolves at Bay Maine Medical Directors Association Annual Conference October 11, 2013 Alva S Baker, MD, CMD-R Disclosure Dr. Baker has indicated that he
CPT DOCUMENTATION REQUIREMENTS FOR EMERGENCY MEDICINE 2009 RELATIVE VALUE UNIT (RVU)
") CPT DOCUMENTATION REQUIREMENTS FOR EMERGENCY MEDICINE 2009 RELATIVE VALUE UNIT (RVU) Three components comprise the initial RVU calculation for each CPT code: Work - the estimated value of the time, effort,
CPT DOCUMENTATION REQUIREMENTS FOR EMERGENCY MEDICINE 2009 RELATIVE VALUE UNIT (RVU) Three components comprise the initial RVU calculation for each CPT code: Work - the estimated value of the time, effort,
HIV/AIDS Care: The Service (CPT) Code Evaluation and Management Series 1
 Code Evaluation and Management Series 1") HIV/AIDS Care: The Service (CPT) Code Evaluation and Management Series 1 Prepared By: Stacey L. Murphy, MPA, RHIA, CPC AHIMA Approved ICD-10-CM/ICD-10-CM Trainer Learning Outcomes Explain the importance
HIV/AIDS Care: The Service (CPT) Code Evaluation and Management Series 1 Prepared By: Stacey L. Murphy, MPA, RHIA, CPC AHIMA Approved ICD-10-CM/ICD-10-CM Trainer Learning Outcomes Explain the importance
Appendix I: E/M CodeBuilder
 Appendix I: E/M CodeBuilder For use with CMS 1997 Documentation Guidelines for Evaluation & Management Coding, which is located on the Student Companion Web Site at www.cengagebrain.com. CMS also published
Appendix I: E/M CodeBuilder For use with CMS 1997 Documentation Guidelines for Evaluation & Management Coding, which is located on the Student Companion Web Site at www.cengagebrain.com. CMS also published
Evaluation & Mangement ( E & M) Visits Adapted from 1997 CMS Guidance Using Single Organ System
 Visits Adapted from 1997 CMS Guidance Using Single Organ System") 5/7/15 University of Rochester Center for Health & Behavioral Training 1 Evaluation & Mangement ( E & M) Visits Adapted from 1997 CMS Guidance Using Single Organ System New Patient Office Visit [Patient
5/7/15 University of Rochester Center for Health & Behavioral Training 1 Evaluation & Mangement ( E & M) Visits Adapted from 1997 CMS Guidance Using Single Organ System New Patient Office Visit [Patient
Evaluation and Management (E/M) Training. Module 12
 Training. Module 12") Evaluation and Management (E/M) Training Module 12 AMA Disclaimer CPT copyright 2011 American Medical Association. All rights reserved. Fee schedules, relative value units, conversion factors and/or related
Evaluation and Management (E/M) Training Module 12 AMA Disclaimer CPT copyright 2011 American Medical Association. All rights reserved. Fee schedules, relative value units, conversion factors and/or related
ChiroCredit.com / OnlineCE.com presents Documentation 101 Part 5 of 10 Instructor: Paul Sherman, DC
 Online Continuing Education Courses www.onlinece.com www.chirocredit.com ChiroCredit.com / OnlineCE.com presents Documentation 101 Part 5 of 10 Instructor: Paul Sherman, DC Important Notice: This download
Online Continuing Education Courses www.onlinece.com www.chirocredit.com ChiroCredit.com / OnlineCE.com presents Documentation 101 Part 5 of 10 Instructor: Paul Sherman, DC Important Notice: This download
Fundamental E&M for Primary Care Risk Adjustment 2010
 2-hr Fundamental E&M for Primary Care Risk Adjustment 2010 E/M Relevance to Diagnosis Coding Presented by: Liz Jeremia Market Consultant Toni Toone, CPC, CPMA Sr. Provider Training & Development Consultant
2-hr Fundamental E&M for Primary Care Risk Adjustment 2010 E/M Relevance to Diagnosis Coding Presented by: Liz Jeremia Market Consultant Toni Toone, CPC, CPMA Sr. Provider Training & Development Consultant
8/3/2011. Presented by: Brenda Edwards, CPC, CPMA, CPC I, CEMC AAPCCA Board of Directors. Documentation. Results ? 2
 Presented by: Brenda Edwards, CPC, CPMA, CPC I, CEMC AAPCCA Board of Directors 1 Documentation Auditing Results? 2 1 HANDWRITTEN Legibility Personalized DICTATED Concise Personalized Timely? EMR Lengthy,
Presented by: Brenda Edwards, CPC, CPMA, CPC I, CEMC AAPCCA Board of Directors 1 Documentation Auditing Results? 2 1 HANDWRITTEN Legibility Personalized DICTATED Concise Personalized Timely? EMR Lengthy,
Guideline Request Form Instructions
 Guideline Instructions We at Office Ally realize that the process of creating Guidelines can be time consuming. In an effort to help speed up the process we have implemented a new solution. Now, instead
Guideline Instructions We at Office Ally realize that the process of creating Guidelines can be time consuming. In an effort to help speed up the process we have implemented a new solution. Now, instead
E & M Chart Audit for the Allergy Practice
 E & M Chart Audit for the Allergy Practice Teresa Thompson, CPC, CCC TM Consulting, Inc. P O Box 267 Carlsborg, WA 98324 360-683-8293 Physician Documentation Verification that the coding is appropriate
E & M Chart Audit for the Allergy Practice Teresa Thompson, CPC, CCC TM Consulting, Inc. P O Box 267 Carlsborg, WA 98324 360-683-8293 Physician Documentation Verification that the coding is appropriate
Charting Smarter, not Longer: Basic Concepts in Outpatient Coding
 Charting Smarter, not Longer: Basic Concepts in Outpatient Coding Workshop WA01 SGIM 29 th Annual Meeting April 27, 2006 Sponsored by the SGIM Clinical Practice Task Force (CPTF) Faculty: Jeannine Engel,
Charting Smarter, not Longer: Basic Concepts in Outpatient Coding Workshop WA01 SGIM 29 th Annual Meeting April 27, 2006 Sponsored by the SGIM Clinical Practice Task Force (CPTF) Faculty: Jeannine Engel,
The 1995 and 1997 AMA HCFA E/M Guidelines describes three levels of ROS:
 The Most Common Cause of Down-Coded E & M Encounters The review of systems component must be adequately documented. By Ken Malkin, D.P.M. Dr. Malkin is a diplomate of the American Board of Quality Assurance
The Most Common Cause of Down-Coded E & M Encounters The review of systems component must be adequately documented. By Ken Malkin, D.P.M. Dr. Malkin is a diplomate of the American Board of Quality Assurance
ICD-10 Documentation Differences in E/M Services. Suzan Berman, CPC, CEMC, CEDC, HRAA
 ICD-10 Documentation Differences in E/M Services Suzan Berman, CPC, CEMC, CEDC, HRAA Publisher Notice Although we have tried to include accurate and comprehensive information in this presentation, please
ICD-10 Documentation Differences in E/M Services Suzan Berman, CPC, CEMC, CEDC, HRAA Publisher Notice Although we have tried to include accurate and comprehensive information in this presentation, please
Evaluation and Management Services
 DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services Open a Text-Only Version Evaluation and Management Services ICN 006764 August 2017 A review of this product in August 2017
DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services Open a Text-Only Version Evaluation and Management Services ICN 006764 August 2017 A review of this product in August 2017
E/M Chart Auditing. Presentation should be given by a knowledgeable chapter member who is comfortable with the subject content
 Presentation should be given by a knowledgeable chapter member who is comfortable with the subject content E/M Chart Auditing Developed by Pam Brooks, CPC, CPC-H, PCS 2013 AAPCCA Board of Directors Why
Presentation should be given by a knowledgeable chapter member who is comfortable with the subject content E/M Chart Auditing Developed by Pam Brooks, CPC, CPC-H, PCS 2013 AAPCCA Board of Directors Why
2016 Behavioral Medicine Resident Chart Documentation. Laura Sullivan, MSW, CPC Compliance Auditor
 2016 Behavioral Medicine Resident Chart Documentation Laura Sullivan, MSW, CPC Compliance Auditor 1 Legal Stuff The information provided here is being provided by a nonlawyer and should not be construed
2016 Behavioral Medicine Resident Chart Documentation Laura Sullivan, MSW, CPC Compliance Auditor 1 Legal Stuff The information provided here is being provided by a nonlawyer and should not be construed
Evaluation and Management Services
 DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services Click Here to Print a Text-Only Version Evaluation and Management Services ICN 006764 August 2015 This educational product
DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services Click Here to Print a Text-Only Version Evaluation and Management Services ICN 006764 August 2015 This educational product
The Coding Network, LLC
 1 1.1.2015 Course Agenda Components of E&M Services History Examination Medical Decision-Making Coding using Time Categories of E/M services and Documentation Requirements Documentation requirements for
1 1.1.2015 Course Agenda Components of E&M Services History Examination Medical Decision-Making Coding using Time Categories of E/M services and Documentation Requirements Documentation requirements for
CODING REVIEW FOR ACCESS2MD PROVIDERS
 CODING REVIEW FOR ACCESS2MD PROVIDERS May 27, 2015 Tricia Stanley, DNP, RN, ANP-BC, FNP-BC TYPES OF CODES CPT What was done during the visit Two Types CPT Evaluation and Management ICD Why it was done
CODING REVIEW FOR ACCESS2MD PROVIDERS May 27, 2015 Tricia Stanley, DNP, RN, ANP-BC, FNP-BC TYPES OF CODES CPT What was done during the visit Two Types CPT Evaluation and Management ICD Why it was done
E&M Nuts and Bolts Part I History and Exam. Presented by Kerin Draak, MSN, WHNP-BC, CPC, CEMC, COBGC
 E&M Nuts and Bolts Part I History and Exam Presented by Kerin Draak, MSN, WHNP-BC, CPC, CEMC, COBGC 1 Disclaimer The Wisconsin Medical Society continuing education publications and seminars are presented
E&M Nuts and Bolts Part I History and Exam Presented by Kerin Draak, MSN, WHNP-BC, CPC, CEMC, COBGC 1 Disclaimer The Wisconsin Medical Society continuing education publications and seminars are presented
Compare and Contrast health data and information. List Factors that lead to improvement in patient care healthcare quality and outcomes
 Developing World Class Health Information What Are the Factors That Lead To Improvement in Patient Care, Healthcare Quality and Outcomes? The Role of Electronic Health Records, Teamwork and Coordination
Developing World Class Health Information What Are the Factors That Lead To Improvement in Patient Care, Healthcare Quality and Outcomes? The Role of Electronic Health Records, Teamwork and Coordination
Physician Practice Compliance Conference
 Slide 1 E/M Coding and Documentation Why does it matter? Janet Himmelreich, Senior Vice President CHC Healthcare Solutions, LLC jhimmelreich@chchealthcare.com October 7, 2004 Slide 2 Discussion Points
Slide 1 E/M Coding and Documentation Why does it matter? Janet Himmelreich, Senior Vice President CHC Healthcare Solutions, LLC jhimmelreich@chchealthcare.com October 7, 2004 Slide 2 Discussion Points
2015 Behavioral Medicine Resident Chart Documentation. Laura Sullivan, MSW, CPC Compliance Auditor
 2015 Behavioral Medicine Resident Chart Documentation Laura Sullivan, MSW, CPC Compliance Auditor 1 Legal Stuff The information provided here is being provided by a nonlawyer and should not be construed
2015 Behavioral Medicine Resident Chart Documentation Laura Sullivan, MSW, CPC Compliance Auditor 1 Legal Stuff The information provided here is being provided by a nonlawyer and should not be construed
John Sanchez, D.O. August 18, 2013
 John Sanchez, D.O. August 18, 2013 Ø Coding Caps Ø Relevance to Clinical Practice Ø Current Guidelines 1995 (organ systems) 1997 (bullets) Ø Definitions ICD- 9 CPT E/M ( 99 _ ) Ø Who Should Determine the
John Sanchez, D.O. August 18, 2013 Ø Coding Caps Ø Relevance to Clinical Practice Ø Current Guidelines 1995 (organ systems) 1997 (bullets) Ø Definitions ICD- 9 CPT E/M ( 99 _ ) Ø Who Should Determine the
Emergency Room Skills Checklist
 _ XXX-XX- Print Name Last 4 of SS # Date Completed Directions Please circle a value for each question to provide us and the interested facilities with an assessment of your clinical experience. These values
_ XXX-XX- Print Name Last 4 of SS # Date Completed Directions Please circle a value for each question to provide us and the interested facilities with an assessment of your clinical experience. These values
04/11/2014. Retina Coding and Reimbursement 101. Financial Disclosure. Chief Complaint
 Retina Coding and Reimbursement 101 William T. Koch, COA, COE, CPC Administrative Director Director of Billing Operations The Retina Institute St. Louis, Missouri Advisory Boards Allergan Genentech Regeneron
Retina Coding and Reimbursement 101 William T. Koch, COA, COE, CPC Administrative Director Director of Billing Operations The Retina Institute St. Louis, Missouri Advisory Boards Allergan Genentech Regeneron
A Common Sense Approach to Emergency Department E&M
 A Common Sense Approach to Emergency Department E&M Common Sense it don t make no Sense, It don t Make no sense no More John Prine We all Know the Drill CPT and CMS Guidelines History Physical Medical
A Common Sense Approach to Emergency Department E&M Common Sense it don t make no Sense, It don t Make no sense no More John Prine We all Know the Drill CPT and CMS Guidelines History Physical Medical
URBAN RESIDENCY PROGRAM PROCEDURAL SKILLS LOG BOOK NAME: DIVISION:
 URBAN RESIDENCY PROGRAM PROCEDURAL SKILLS LOG BOOK NAME: DIVISION: Procedures This list is provided as a guide to most of the procedures you might be exposed to during your training. There is no expectation
URBAN RESIDENCY PROGRAM PROCEDURAL SKILLS LOG BOOK NAME: DIVISION: Procedures This list is provided as a guide to most of the procedures you might be exposed to during your training. There is no expectation
Ritecode.com Physician Coding Audit Report - Summary Statistics
 Clinic Name: 1111 Manager: 1111 OB/GYN Physician: 1111 Encounters Correct (%): 80.00% Medical Decision Making Correct (%): 80.00% Exam Correct (%): 80.00% History Correct (%): 100.00% Documentation Needs
Clinic Name: 1111 Manager: 1111 OB/GYN Physician: 1111 Encounters Correct (%): 80.00% Medical Decision Making Correct (%): 80.00% Exam Correct (%): 80.00% History Correct (%): 100.00% Documentation Needs
ER Skills Checklist. Frequency Scale: 1 = Never Observed 2 = Less than 6 times a year 3 = 1 or 2 Times a Month 4 = Daily or Weekly
 ER Skills Checklist This assessment is for determining your experience in the below outlined clinical areas. This checklist will not be used as a determining factor in accepting your application for employment
ER Skills Checklist This assessment is for determining your experience in the below outlined clinical areas. This checklist will not be used as a determining factor in accepting your application for employment
Volume 2. Issue 3. March 2013 Cristy Donaldson, CPC, CPMA Coding Specialist
 Volume 2. Issue 3. March 203 Cristy Donaldson, CPC, CPMA Coding Specialist 865-670-677 CDonaldson@utmck.edu Are you struggling with knowing how to document and code for a Preventive and Problem visit on
Volume 2. Issue 3. March 203 Cristy Donaldson, CPC, CPMA Coding Specialist 865-670-677 CDonaldson@utmck.edu Are you struggling with knowing how to document and code for a Preventive and Problem visit on
Practical Approaches to Medical Necessity
 Practical Approaches to Medical Necessity CAROLYN AVERY, CPC, CEMC CAROLYN AVERY & ASSOCIATES, PC ROBERT OSSOFF DMD, MD, CHC ASSISTANT VICE CHANCELLOR FOR COMPLIANCE &CORPORATE INTEGRITY VANDERBILT MEDICAL
Practical Approaches to Medical Necessity CAROLYN AVERY, CPC, CEMC CAROLYN AVERY & ASSOCIATES, PC ROBERT OSSOFF DMD, MD, CHC ASSISTANT VICE CHANCELLOR FOR COMPLIANCE &CORPORATE INTEGRITY VANDERBILT MEDICAL
Rational Physician Coding for Emergency Department E/M Services and Critical Care. Redacted Version. Peter R. Jensen, MD, CPC
 Rational Physician Coding for Emergency Department E/M Services and Critical Care Peter R. Jensen, MD, CPC www.emuniversity.com Rational Physician Coding for Emergency E/M Services Peter R. Jensen, MD,
Rational Physician Coding for Emergency Department E/M Services and Critical Care Peter R. Jensen, MD, CPC www.emuniversity.com Rational Physician Coding for Emergency E/M Services Peter R. Jensen, MD,
CPT is a registered trademark of the American Medical Association.
 Welcome to s Webinar and Audio Conference Training. We hope that the information contained herein will give you valuable tips that you can use to improve your skills and performance on the job. Each year,
Welcome to s Webinar and Audio Conference Training. We hope that the information contained herein will give you valuable tips that you can use to improve your skills and performance on the job. Each year,
Procedures in the ED. MCEP Straight Talk Most $$$ ED CPT Codes (not including E&M codes) EKGs X-rays Ultrasounds.
 EKGs X-rays Ultrasounds.") Procedures in the ED Most $$$ ED CPT Codes (not including E&M codes) 93010 Electrocardiogram report 31500 Insert emergency airway 36556 Insert non-tunnel CV cath 92950 Heart/lung resuscitation CPR 12001
Procedures in the ED Most $$$ ED CPT Codes (not including E&M codes) 93010 Electrocardiogram report 31500 Insert emergency airway 36556 Insert non-tunnel CV cath 92950 Heart/lung resuscitation CPR 12001
Student Guide Module 4: Pediatric Trauma
 Student Guide Module 4: Pediatric Trauma Problem based learning exercise objectives Understand how to manage traumatic injuries in mass casualty events. Discuss the features and the approach to pediatric
Student Guide Module 4: Pediatric Trauma Problem based learning exercise objectives Understand how to manage traumatic injuries in mass casualty events. Discuss the features and the approach to pediatric
Effective Case Presentations
 Effective Case Presentations Alan Lefor MD MPH Department of Surgery Jichi Medical University 4 4 Alan Lefor 1. History The complete medical history always should have six parts It begins with the Chief
Effective Case Presentations Alan Lefor MD MPH Department of Surgery Jichi Medical University 4 4 Alan Lefor 1. History The complete medical history always should have six parts It begins with the Chief
Logo Placement *######*
 INPATIENT ADMITTING HISTORY AND PHYSICAL Page 1 of 8 Date of Service / / Time of Service : AM PM CHIEF COMPLAINT(S): HISTORY UNOBTAINABLE -- Patient was admitted UNACCOMPANIED, and no history could be
INPATIENT ADMITTING HISTORY AND PHYSICAL Page 1 of 8 Date of Service / / Time of Service : AM PM CHIEF COMPLAINT(S): HISTORY UNOBTAINABLE -- Patient was admitted UNACCOMPANIED, and no history could be
Rational Physician Coding for E/M Services
 Rational Physician Coding for E/M Services CO-NM-OK-TX-VA Peter R. Jensen, MD, CPC www.emuniversity.com Rational Physician Coding for E/M Services Peter R. Jensen, MD, CPC Goals ) Improve physician E/M
Rational Physician Coding for E/M Services CO-NM-OK-TX-VA Peter R. Jensen, MD, CPC www.emuniversity.com Rational Physician Coding for E/M Services Peter R. Jensen, MD, CPC Goals ) Improve physician E/M
By Laureen Jandroep, CPC, CPC-I, CMSCS, CHCI ~ Instructor (888)
") UNDERSTANDING E&M STEP BY STEP Step 1 - Determine the E/M Category/Subcategory (location/service type) Step 2 - Determine Level of History Step 3 - Determine Level of Exam Step 4 - Determine Level of Medical
UNDERSTANDING E&M STEP BY STEP Step 1 - Determine the E/M Category/Subcategory (location/service type) Step 2 - Determine Level of History Step 3 - Determine Level of Exam Step 4 - Determine Level of Medical
Coding for Clinicians Are you Ready??? By Donelle Holle, R.N. Pediatric Coding Consultant
 Coding for Clinicians Are you Ready??? By Donelle Holle, R.N. Pediatric Coding Consultant Coding Office Visits Each visit is dependent on history/physical and Medical Decision Making Consequently not every
Coding for Clinicians Are you Ready??? By Donelle Holle, R.N. Pediatric Coding Consultant Coding Office Visits Each visit is dependent on history/physical and Medical Decision Making Consequently not every
Assignments for SUM Program Beginning Medical Transcription, 2nd edition
 Assignments for SUM Program Beginning, 2nd edition SECTION 1 Introduction, Dermatology/ Plastics Body () Unit 1, Body as a Whole, Ch. 1, Organization of the Body; Ch. 4, Tissues, Glands, etc., Ch. 5, Integumentary
Assignments for SUM Program Beginning, 2nd edition SECTION 1 Introduction, Dermatology/ Plastics Body () Unit 1, Body as a Whole, Ch. 1, Organization of the Body; Ch. 4, Tissues, Glands, etc., Ch. 5, Integumentary
Evaluation and Management Services
 Advanced E/M Auditing Evaluation and Management Services Disclaimer area Evaluation and Management Services History Exam Medical Decision Making Select the E/M Code Subjective portion of the visit where
Advanced E/M Auditing Evaluation and Management Services Disclaimer area Evaluation and Management Services History Exam Medical Decision Making Select the E/M Code Subjective portion of the visit where
Alix Casler, M.D., F.A.A.P. Orlando, FL
 Alix Casler, M.D., F.A.A.P. Orlando, FL Emergencies in the School Setting Initial triage Basics of History and Exam Specific Scenarios Initial Assessment and Triage First steps in evaluating a potential
Alix Casler, M.D., F.A.A.P. Orlando, FL Emergencies in the School Setting Initial triage Basics of History and Exam Specific Scenarios Initial Assessment and Triage First steps in evaluating a potential
E/M for Orthopaedics
 E/M for Orthopaedics Julie A. Leu, CPC, CPMA, CPC-I 2009-2011 NAB Member, Region 7 1 Objectives Review of Evaluation and Management Guidelines Comparison of the 1995 and 1997 Exam Guidelines Reporting
E/M for Orthopaedics Julie A. Leu, CPC, CPMA, CPC-I 2009-2011 NAB Member, Region 7 1 Objectives Review of Evaluation and Management Guidelines Comparison of the 1995 and 1997 Exam Guidelines Reporting
Step 1 - Determine the Category/Subcategory (Location/Service Type)
") UNDERSTANDING E&M STEP BY STEP Step 1 - Determine the E/M Category/Subcategory (location/service type) Step 2 - Determine Level of History Step 3 - Determine Level of Exam Step 4 - Determine Level of Medical
UNDERSTANDING E&M STEP BY STEP Step 1 - Determine the E/M Category/Subcategory (location/service type) Step 2 - Determine Level of History Step 3 - Determine Level of Exam Step 4 - Determine Level of Medical
The Surgical Patient. Objectives:
 The Surgical Patient Objectives: 1. Discuss the effect of surgery on the body systems. 2. Explain the etiological factors, nursing assessment, and management of potential problems during the postoperative
The Surgical Patient Objectives: 1. Discuss the effect of surgery on the body systems. 2. Explain the etiological factors, nursing assessment, and management of potential problems during the postoperative
Sutter Medical Center, Sacramento Department of Emergency Medicine - Delineation of Privileges NAME: INITIAL: [ ] RENEWED: [ ] ADDITIONAL: [ ]
![Sutter Medical Center, Sacramento Department of Emergency Medicine - Delineation of Privileges NAME: INITIAL: [ ] RENEWED: [ ] ADDITIONAL: [ ]](/thumbs/85/91875103.jpg "Sutter Medical Center, Sacramento Department of Emergency Medicine - Delineation of Privileges NAME: INITIAL: [ ] RENEWED: [ ] ADDITIONAL: [ ]") Privileges are granted for Sutter Medical Center, Sacramento and exercise of privileges is based on the type of care, treatment and services provided at each facility. Privileges are granted for Sutter
Privileges are granted for Sutter Medical Center, Sacramento and exercise of privileges is based on the type of care, treatment and services provided at each facility. Privileges are granted for Sutter
APPLY FIRST AID ONLINE WORKBOOK
 APPLY FIRST AID ONLINE WORKBOOK STUDENT NAME: ADDRESS: PHONE CONTACT: DATE OF COURSE: Welcome to CYNERGEX GROUP pre-learning package for the APPLY FIRST AID course. This workbook is to be completed in
APPLY FIRST AID ONLINE WORKBOOK STUDENT NAME: ADDRESS: PHONE CONTACT: DATE OF COURSE: Welcome to CYNERGEX GROUP pre-learning package for the APPLY FIRST AID course. This workbook is to be completed in
It is for this reason that we have upgraded our HPI button for the review of chronic conditions.
 Chronic Conditions The chronic condition review has changed. On the Master GP template the chronic conditions are listed in the first column. Beside the list of Chronic Conditions there are a number of
Chronic Conditions The chronic condition review has changed. On the Master GP template the chronic conditions are listed in the first column. Beside the list of Chronic Conditions there are a number of
Focus On Signs and Symptoms
 Focus On Signs and Symptoms Decreasing Primary Care Access Help Your Patients with Their Insurance Benefits Risk Management and Reimbursement Align Don t Forget to Document Abnormal Vitals and Labs Document
Focus On Signs and Symptoms Decreasing Primary Care Access Help Your Patients with Their Insurance Benefits Risk Management and Reimbursement Align Don t Forget to Document Abnormal Vitals and Labs Document
(Based on Presenting Problem) Joe Barton, MD, MHMS Oct 30, 2012
 Joe Barton, MD, MHMS Oct 30, 2012") (Based on Presenting Problem) Joe Barton, MD, MHMS Oct 30, 2012 Review specific critical care clinical presentations Outline which scenarios may NOT be appropriate for CC time Identify documentation and
(Based on Presenting Problem) Joe Barton, MD, MHMS Oct 30, 2012 Review specific critical care clinical presentations Outline which scenarios may NOT be appropriate for CC time Identify documentation and
The ABC s of Chest Trauma
 The ABC s of Chest Trauma J Bradley Pickhardt MD, FACS Providence St Patrick Hospital What s the Problem? 2/3 of trauma patients have chest trauma Responsible for 25% of all trauma deaths Most injuries
The ABC s of Chest Trauma J Bradley Pickhardt MD, FACS Providence St Patrick Hospital What s the Problem? 2/3 of trauma patients have chest trauma Responsible for 25% of all trauma deaths Most injuries
Sutter Medical Center, Sacramento Department of Emergency Medicine - Delineation of Privileges
 INITIAL: [ ] RENEWED: [ ] ADDITIONAL: [ ] Privileges are granted for Sutter Medical Center, Sacramento and exercise of privileges is based on the type of care, treatment and services provided at each facility.
INITIAL: [ ] RENEWED: [ ] ADDITIONAL: [ ] Privileges are granted for Sutter Medical Center, Sacramento and exercise of privileges is based on the type of care, treatment and services provided at each facility.
Pain Management Questionnaire
 In order to make the most of your visit, we require this form to be completed to the best of your ability and sent to the Pain Management Clinic a copy should be shared with your Primary Care Provider
In order to make the most of your visit, we require this form to be completed to the best of your ability and sent to the Pain Management Clinic a copy should be shared with your Primary Care Provider
Skin Deep. Agenda. Burns Wounds Debridement Evaluation and Management Services. Presented by: Mike Strong, SFM The Work Comp Experts.
 Presented by: Mike Strong, SFM The Work Comp Experts Agenda Wounds Debridement Evaluation and Management Services 2 1 Types of First Degree Second Degree Third Degree Rule of 9 Adults Infants Burn Coding
Presented by: Mike Strong, SFM The Work Comp Experts Agenda Wounds Debridement Evaluation and Management Services 2 1 Types of First Degree Second Degree Third Degree Rule of 9 Adults Infants Burn Coding
Introduction to ICD-10-CM
 Chapter 3 Introduction to ICD-10-CM Exercise 1 Directions: Using the ICD-10-CM codebook locate the diagnosis codes for the following conditions. 1. Fever 2. Chronic non-intractable common migraine headache
Chapter 3 Introduction to ICD-10-CM Exercise 1 Directions: Using the ICD-10-CM codebook locate the diagnosis codes for the following conditions. 1. Fever 2. Chronic non-intractable common migraine headache
PARAMEDIC COURSE OBJECTIVES
 ELEMENT TITLE PARAMEDIC COURSE OBJECTIVES 100000 INTRODUCTION TO PARAMEDICINE 101000 Introduction to Paramedicine 101000T Discuss the characteristics of the profession of paramedicine. 102000 EMS Systems
ELEMENT TITLE PARAMEDIC COURSE OBJECTIVES 100000 INTRODUCTION TO PARAMEDICINE 101000 Introduction to Paramedicine 101000T Discuss the characteristics of the profession of paramedicine. 102000 EMS Systems
History: Going the Distance. Suzan Berman, CPC, CEMC, CEDC
 History: Going the Distance Suzan Berman, CPC, CEMC, CEDC Publisher Notice Although we have tried to include accurate and comprehensive information in this presentation, please remember it is not intended
History: Going the Distance Suzan Berman, CPC, CEMC, CEDC Publisher Notice Although we have tried to include accurate and comprehensive information in this presentation, please remember it is not intended
Face and Throat Injuries. Chapter 26
 Face and Throat Injuries Chapter 26 Anatomy of the Head Landmarks of the Neck Injuries to the Face Injuries around the face can lead to upper airway obstructions. Bleeding from the face can be profuse.
Face and Throat Injuries Chapter 26 Anatomy of the Head Landmarks of the Neck Injuries to the Face Injuries around the face can lead to upper airway obstructions. Bleeding from the face can be profuse.
Dear Mercy Cancer Center Radiation Oncology Patient
 Dear Mercy Cancer Center Radiation Oncology Patient Welcome to our Department. In order to complete our records, and enable our physicians to ensure that your questions are fully addressed, we appreciate
Dear Mercy Cancer Center Radiation Oncology Patient Welcome to our Department. In order to complete our records, and enable our physicians to ensure that your questions are fully addressed, we appreciate
Emergency Care Progress Log
 Emergency Care Progress Log For further details on the National Occupational Competencies for EMRs, please visit www.paramedic.ca. Check off each skill once successfully demonstrated the Instructor. All
Emergency Care Progress Log For further details on the National Occupational Competencies for EMRs, please visit www.paramedic.ca. Check off each skill once successfully demonstrated the Instructor. All
Accurate Documentation and Billing Evaluation & Management
 Accurate Documentation and Billing Evaluation & Management Luis S. Marsano, M.D. Professor of Medicine Director of Clinical Hepatology University of Louisville & Louisville VAMC 2012 Documentation Requirements
Accurate Documentation and Billing Evaluation & Management Luis S. Marsano, M.D. Professor of Medicine Director of Clinical Hepatology University of Louisville & Louisville VAMC 2012 Documentation Requirements
Medicare & Dual Options Annual Comprehensive Exam FAX COMPLETED FORM TO: Patient Personal Information
 FAX COMPLETED FM TO: 877-682-2216 All fields marked with an * are required to be completed in order to receive payment for the ACE Form, unless indicated otherwise. Please refer to the document titled
FAX COMPLETED FM TO: 877-682-2216 All fields marked with an * are required to be completed in order to receive payment for the ACE Form, unless indicated otherwise. Please refer to the document titled
Applicant s Name First Middle Last
 Delineation of Privileges Internal Medicine Effective from (date) to (date) at (hospital name) Applicant s Name First Middle Last Instructions 1. Review Basic Minimum Requirements to make sure you qualify
Delineation of Privileges Internal Medicine Effective from (date) to (date) at (hospital name) Applicant s Name First Middle Last Instructions 1. Review Basic Minimum Requirements to make sure you qualify
New Patient History. Name: DOB: Sex: Date: If yes, give the name of the physician who did your evaluation or ordered your tests:
 New Patient History Name: DOB: Sex: Date: Chief Complaint: 1. Give a brief description of the problem you are seeking treatment for today: 2. Have you been evaluated for this problem or had any tests for
New Patient History Name: DOB: Sex: Date: Chief Complaint: 1. Give a brief description of the problem you are seeking treatment for today: 2. Have you been evaluated for this problem or had any tests for
Subject Ch Hours Date Preparatory Intro to Course 4 9/4. Safety and Wellness 2 2 9/11 Public Health 3 2. Medical, Legal and Ethical Issues 4 4 9/13
 Subject Ch Hours Date Preparatory Intro to Course 4 9/4 Intro to Course (continued) 2 9/6 EMS Systems 1 2 Safety and Wellness 2 2 9/11 Public Health 3 2 Medical, Legal and Ethical Issues 4 4 9/13 Medical,
Subject Ch Hours Date Preparatory Intro to Course 4 9/4 Intro to Course (continued) 2 9/6 EMS Systems 1 2 Safety and Wellness 2 2 9/11 Public Health 3 2 Medical, Legal and Ethical Issues 4 4 9/13 Medical,
Writing with purpose. Make IT real and simple. On the Medicine Wards for Medical Students, Interns, and Residents
 Writing with purpose Make IT real and simple On the Medicine Wards 2017-2018 for Medical Students, Interns, and Residents Omar S. Darwish, MS, DO Health Science Assistant Professor Coordinator of the M&M
Writing with purpose Make IT real and simple On the Medicine Wards 2017-2018 for Medical Students, Interns, and Residents Omar S. Darwish, MS, DO Health Science Assistant Professor Coordinator of the M&M
"No FUNDS Left Behind": Maximizing Inpatient Revenue Capture Through Better Understanding and Use of Documentation and Coding Guidelines
 "No FUNDS Left Behind": Maximizing Inpatient Revenue Capture Through Better Understanding and Use of Documentation and Coding Guidelines Workshop A01: SGIM 31 st Annual National Meeting Thursday April
"No FUNDS Left Behind": Maximizing Inpatient Revenue Capture Through Better Understanding and Use of Documentation and Coding Guidelines Workshop A01: SGIM 31 st Annual National Meeting Thursday April
WPS Medicare Part B - Quarterly CERT Error Findings Report ~ MICHIGAN ~
 WPS Medicare Part B - Quarterly CERT Error Findings Report ~ MICHIGAN ~ This report provides details of Comprehensive Error Rate Testing (CERT) errors assessed July 2014 through September 2014 for Michigan
WPS Medicare Part B - Quarterly CERT Error Findings Report ~ MICHIGAN ~ This report provides details of Comprehensive Error Rate Testing (CERT) errors assessed July 2014 through September 2014 for Michigan
E/M Auditing. Today s Session
 E/M Auditing Shannon O. Smith, CPC, CPC-I, CEMC, CMSCS, CPMA DoctorsManagement/NAMAS 1 Today s Session Auditing Basics Teaching the Provider E&M Documentation Guidelines Documentation Components Difference
E/M Auditing Shannon O. Smith, CPC, CPC-I, CEMC, CMSCS, CPMA DoctorsManagement/NAMAS 1 Today s Session Auditing Basics Teaching the Provider E&M Documentation Guidelines Documentation Components Difference
Emergency Medicine Scope of Practice
 Emergency Medicine Scope of Practice All Physician Assistants working in Emergency Medicine will encounter a wide variety of non acute, urgent and emergent patient complaints and conditions. Given the
Emergency Medicine Scope of Practice All Physician Assistants working in Emergency Medicine will encounter a wide variety of non acute, urgent and emergent patient complaints and conditions. Given the
Surgical Care at the District Hospital. EMERGENCY & ESSENTIAL SURGICAL CARE
 Surgical Care at the District Hospital 1 5 Basic Surgical Procedures Key Points 2 5.1 Wound Management Many important procedures can be performed under local anesthesia and do not require a surgical specialist
Surgical Care at the District Hospital 1 5 Basic Surgical Procedures Key Points 2 5.1 Wound Management Many important procedures can be performed under local anesthesia and do not require a surgical specialist
Skin Anatomy and Physiology
 Skin Anatomy and Physiology Body s largest organ Three layers: Epidermis Dermis Subcutaneous tissue 1 2 Skin Anatomy and Physiology Complex system, variety of functions Sensation Control of water loss
Skin Anatomy and Physiology Body s largest organ Three layers: Epidermis Dermis Subcutaneous tissue 1 2 Skin Anatomy and Physiology Complex system, variety of functions Sensation Control of water loss
EMS-192 EMT CURRICULUM
 Lesson Topic Content 1 Section #1 Welcome and Orientation MATC/EMS Orientation & Policies Student Packet 11th Edition AAOS 2 AHA - CPR AHA - CPR Basic Life Support Certification A. Management for Health
Lesson Topic Content 1 Section #1 Welcome and Orientation MATC/EMS Orientation & Policies Student Packet 11th Edition AAOS 2 AHA - CPR AHA - CPR Basic Life Support Certification A. Management for Health
You Are the Emergency Medical Responder
 Lesson 32: Injuries to the Chest, Abdomen and Genitalia You Are the Emergency Medical Responder Your police unit responds to a call in a part of town plagued by violence. When you arrive, you find the
Lesson 32: Injuries to the Chest, Abdomen and Genitalia You Are the Emergency Medical Responder Your police unit responds to a call in a part of town plagued by violence. When you arrive, you find the
Chapter 29 - Chest_and_Abdominal_Trauma
 Introduction to Emergency Medical Care 1 OBJECTIVES 29.1 Define key terms introduced in this chapter. Slides 11, 15, 18, 27 29.2 Describe mechanisms of injury commonly associated with chest injuries. Slides
Introduction to Emergency Medical Care 1 OBJECTIVES 29.1 Define key terms introduced in this chapter. Slides 11, 15, 18, 27 29.2 Describe mechanisms of injury commonly associated with chest injuries. Slides
ADMINISTRATIVE REQUIREMENT MANUAL EFFECTIVE DATE
 PURPOSE: I. To establish the minimum requirements for a first responder training course in first aid, which all first responders must take, in order to meet the requirements of M.G.L. c. 111, 201 and 105
PURPOSE: I. To establish the minimum requirements for a first responder training course in first aid, which all first responders must take, in order to meet the requirements of M.G.L. c. 111, 201 and 105
Top Missed Coding Concepts
 Top Missed Coding Concepts Open vs Closed Fracture Care Open fracture care is reported when the provider creates an opening to expose the bone to treat a fracture. Not performed in the ED Patient is taken
Top Missed Coding Concepts Open vs Closed Fracture Care Open fracture care is reported when the provider creates an opening to expose the bone to treat a fracture. Not performed in the ED Patient is taken
Application for Clinical Privileges Physician Specialty: Family Medicine
 Application for Clinical Privileges Physician Specialty: Family Medicine Qualifications To be eligible to apply for clinical core privileges in family medicine, the initial applicant must meet the following
Application for Clinical Privileges Physician Specialty: Family Medicine Qualifications To be eligible to apply for clinical core privileges in family medicine, the initial applicant must meet the following
GENERAL MULTI-SYSTEM EXAMINATION WORKSHEET
 GENERAL MULTI-SYSTEM EXAMINATION WORKSHEET HPI ROS PFSH History Location Timing Allergic/Imm Eyes Musc/Sk el Past History Documentation of history of Problem Pertinent ROS = Related System Expanded General
GENERAL MULTI-SYSTEM EXAMINATION WORKSHEET HPI ROS PFSH History Location Timing Allergic/Imm Eyes Musc/Sk el Past History Documentation of history of Problem Pertinent ROS = Related System Expanded General
UMC HEALTH SYSTEM Lubbock, Texas :
 Consent for Commonly Performed Procedures in the Adult Critical Care Units I, the undersigned, understand that the adult intensive and intermediate care units ( critical care units ) are places where seriously
Consent for Commonly Performed Procedures in the Adult Critical Care Units I, the undersigned, understand that the adult intensive and intermediate care units ( critical care units ) are places where seriously
LABORATORY PROCEDURES IMAGING/RADIOLOGY PROCEDURES THERAPY GVH EMERGENCY DEPARTMENT PROCECURES
 PROCEDURE CHARGES / HOSPITAL may vary depending on circumstances. Prices subject to change. LABORATORY PROCEDURES Basic Metabolic Panel $112.00 80048 Comprehensive Metabolic Panel $140.00 80053 UA Micro
PROCEDURE CHARGES / HOSPITAL may vary depending on circumstances. Prices subject to change. LABORATORY PROCEDURES Basic Metabolic Panel $112.00 80048 Comprehensive Metabolic Panel $140.00 80053 UA Micro
Advanced Anesthesia. Presented by: Shelly Cronin, CPC, CPMA, CANPC, CGSC, CGIC. Agenda
 Advanced Anesthesia Presented by: Shelly Cronin, CPC, CPMA, CANPC, CGSC, CGIC 1 Agenda Understanding key terms Review coding concepts & modifiers Documentation standards How to avoid coding pitfalls New
Advanced Anesthesia Presented by: Shelly Cronin, CPC, CPMA, CANPC, CGSC, CGIC 1 Agenda Understanding key terms Review coding concepts & modifiers Documentation standards How to avoid coding pitfalls New
UBMD Internal Medicine
 UBMD Internal Medicine Clinical Documentation Example Established Outpatient Visit - 99215 Pat Kisiel-Neunder, Compliance Administrator Email: pkisieln@buffalo.edu Regulations The following information
UBMD Internal Medicine Clinical Documentation Example Established Outpatient Visit - 99215 Pat Kisiel-Neunder, Compliance Administrator Email: pkisieln@buffalo.edu Regulations The following information
QI. Read the following questions and choose the most correct answer (20 Marks):
:") Question One: QI. Read the following questions and choose the most correct answer (20 Marks): 1- Some people are very allergic to some drugs like penicillin. This condition is called: a) Septic shock.
Question One: QI. Read the following questions and choose the most correct answer (20 Marks): 1- Some people are very allergic to some drugs like penicillin. This condition is called: a) Septic shock.
The evaluation-and-management (E/M) codes in the 1992 CPT Book are entirely new. All
 codes in the 1992 CPT Book are entirely new. All") Printed in Plastic Surgery News - February 1992 Don't kill the messenger New evaluation/management codes announced By Raymond Janevicius, MD The evaluation-and-management (E/M) codes in the 1992 CPT Book
Printed in Plastic Surgery News - February 1992 Don't kill the messenger New evaluation/management codes announced By Raymond Janevicius, MD The evaluation-and-management (E/M) codes in the 1992 CPT Book
Decision-Making in the Acute Management of Blunt and Penetrating Wounds Mary Somerville, DVM, DACVS
 Decision-Making in the Acute Management of Blunt and Penetrating Wounds Mary Somerville, DVM, DACVS Providing the best quality care and service for the patient, the client, and the referring veterinarian.
Decision-Making in the Acute Management of Blunt and Penetrating Wounds Mary Somerville, DVM, DACVS Providing the best quality care and service for the patient, the client, and the referring veterinarian.
Prescribe appropriate immunizations for. Prescribe childhood immunization as per. Prescribe influenza vaccinations in high-risk
 Supplemental Digital Appendix 1 46 Health Care Problems and the Corresponding 59 Practice Indicators Expected of All Physicians Entering or in Practice Infectious and parasitic diseases Avoidable complications/death
Supplemental Digital Appendix 1 46 Health Care Problems and the Corresponding 59 Practice Indicators Expected of All Physicians Entering or in Practice Infectious and parasitic diseases Avoidable complications/death
CODING and RVU s: What AHLTA Can Do For You (and what it can t)! Edited 2015 from USAFP Conference March 2007 Mark Stackle, MD
! Edited 2015 from USAFP Conference March 2007 Mark Stackle, MD") CODING and RVU s: What AHLTA Can Do For You (and what it can t)! Edited 2015 from USAFP Conference March 2007 Mark Stackle, MD Coding Basics The Dry Stuff Evaluation and Management Coding 2/3 areas for
CODING and RVU s: What AHLTA Can Do For You (and what it can t)! Edited 2015 from USAFP Conference March 2007 Mark Stackle, MD Coding Basics The Dry Stuff Evaluation and Management Coding 2/3 areas for
DATE TOPIC INSTRUCTOR. MODULE I Preparatory. 08/21/ MILLER Course Overview (books, paperwork, etc.)
") Autumn 2018 EMT (Evening Class) August 21, 2018 December 15, 2018 Emergency Medical Technician Tuesdays & Thursdays 1800 2200 3-Wednesdays 1800 2200 as scheduled 2-Saturdays 0800 1700 as scheduled DATE
Autumn 2018 EMT (Evening Class) August 21, 2018 December 15, 2018 Emergency Medical Technician Tuesdays & Thursdays 1800 2200 3-Wednesdays 1800 2200 as scheduled 2-Saturdays 0800 1700 as scheduled DATE
Patient Interview Form
 Page 1 of 6 Patient Interview Form Patient Information First Name: MRN: Age: Last Name: Date Of Birth: Notes: Email Please check one as your preferred email for communications Personal: Work: Race Select
Page 1 of 6 Patient Interview Form Patient Information First Name: MRN: Age: Last Name: Date Of Birth: Notes: Email Please check one as your preferred email for communications Personal: Work: Race Select