Cervical Case Study. M. Benson, A. Felts, S. Kibiloski, J. Mowen, A. Rijhwani
|
|
|
- Bruno O’Neal’
- 5 years ago
- Views:
Transcription
1 Cervical Case Study M. Benson, A. Felts, S. Kibiloski, J. Mowen, A. Rijhwani
2 Medical Dx 35 y.o. female with myofascial pain No significant radiological findings other than reported flattened cervical spine, mild scoliosis by chiropractor No precautions given by physician
3 Subjective History CC: Unrelenting L neck and shoulder pain with paresthesia into L third finger L arm weakness MOI: 2 months prior: - high stress - increased neck discomfort and neck muscle tightness One week ago: - pt. made a sudden movement to catch son - felt sudden lock down in neck afterwards
4 Subjective History Current symptoms: L neck & mid scap pain Intermittent parasthesias into 3rd finger. Pain: Current - 8/10, Low - 5/10, High - 10/10 PMH Anxiety Depression Mild scoliosis Birth of 2 children
5 Subjective History Medications Name Dosage Indication Wellbutrin 150 mg, 24 hr. tablet Antidepressant Citalopram 40 mg Antidepressant (SSRI) Diazepam 4 mg, 4x/day as needed Anti-anxiety (Benzo) Naproxen 500 mg, 2x/day NSAID
6 Objective Exam Posture Tall and thin R handed Elevated L shoulder, scapula, and 1st rib L thoracic convexity Forward head and mild increased thoracic kyphosis Normal lordosis
7 Objective Exam Cervical ROM: Flexion: 55º, discomfort, concordant symptoms (normal: 50º) Extension: 60º, pinching on L (normal: 60º) Rotation: L - 60º, pinch on L; R - 68º (normal: 80º) Sidebend: L - 40º, pain; R - 45º (normal: 45º) UE ROM: WNL B in: Flexion, ER, IR Strength: 4/5 in L Shoulder: Flexion, Abduction, Biceps, Triceps, Brachioradialis, Wrist extensors 5/5 in RUE mm
8 Objective Exam Palpation Tenderness with trigger points in: - L scalenes - L levator scapula - L upper and middle trap - L upper cervical region Joint Mobility Hypermobile body type Hypomobility on L C 2/3, 5/6, 6/7, & T1 L rotation in L upper thoracic region Hypomobility in L thoracic to PA spring
9 Special Tests ULTT Positive for median and radial nerve Cervical Distraction Positive for symptom relief Spurlings Positive with symptom reproduction
10 Outcome Measures NDI 25/50 MDC: 5 points 0-4 = no disability 5-14 = mild = moderate = severe above 34 = complete SPADI Pain - 66% Disability - 55% Total disability for L shoulder - 59% MDC: 10% No disability= 0
11 Patient Problems CCU nurse: heavy lifting, reaching, shifting of patients, 12 hour long shifts 2 small children: carrying, lifting, and care of children PMH Anxiety and depression exacerbate symptoms of pain and limit ability to relax upper quarter heightening muscle tension
12 Patient Goals 1. Pt. wants to return to work and work at computer without pain 2. Pt. wants to be able to pick up children without weakness or pain 3. Pt. wants to have L UE strength return to normal
13 ICF Model
14 Differential Dx Cervical Radiculopathy Cervical Facet Syndrome Thoracic Outlet Syndrome - Deep stabbing, burning neck pain - Pain, numbness, or tingling in UE - UE weakness - AGGs: prolonged sitting/reading, external or lateral rotation of spine - EASEs: supine with head and neck supported - Pain with extension and rotation, often bilateral - Pain can be gradual or acute following a traumatic incident - Posterior neck stiffness - Cervicogenic headache - Possible pain referral to shoulder, scapular regions, and UE - Often also complain of lumbar facet problems - Pain and heaviness in the cervical region and arms - Paresthesias (medial side of arm) - Aggravated by overhead positioning of the arms - Intrinsic muscle deficit/atrophy of hand - Easy fatigability, paleness, or coldness of hand - Pain with activity - Deep, boring, toothache-like pain - Cold intolerance - Loss of dexterity - Waking from sleep with pain and numbness

15 PT Evaluation C7 Cervical Radiculopathy Irritation of the nerve root caused by compression or inflammation Symptoms can radiate into the arm and hand C7 - causes pain &/or weakness to hand, can include: - Triceps - middle finger
16 Diagnostic Question What combination of tests is most accurate for diagnosing cervical radiculopathy in a 35 year-old woman with neck pain and radiating symptoms?
17 A systematic review of the diagnostic accuracy of provocative tests of the neck for diagnosing cervical radiculopathy Rubinstein et. al, European Spine Journal, 2007
18 A Systematic Review of Cohort Studies: Level 2a Evidence Purpose To determine diagnostic accuracy of clinical provocative tests of the neck that are commonly used in clinical practice for patients suspected cervical radiculopathy Methodological criteria Evaluated using QUADAS to determine any bias in diagnostic research such as spectrum bias, disease progression bias, review bias, etc.
19 Methods Inclusion Criteria Inclusion of any provocative test of neck for diagnosing cervical radiculopathy, use of reference standard, sensitivity and specificity reported or could be (re)calculated, full report Exclusion Criteria Case series or case reports, any animal, surgical, and cadaveric studies
20 Results Sensitivity (rule out) Specificity (rule in) Low Moderate High Low Moderate High Spurling s Traction/ distraction Valsalva ULTT Shoulder abduction
21 Conclusions Conclusions: A positive Spurling's, traction/distraction, and Valsalva might suggest cervical radiculopathy (high specificity) A negative ULTT might rule out (high sensitivity) Values of tests should be interpreted with caution if no other clinical info or evidence Limitations: Only 6 studies No study used optimal reference standard Lack of standardization or performance of tests
22 Reliability and diagnostic accuracy of the clinical examination and patient self-report measures for cervical radiculopathy Wainner et al. SPINE, 2003
23 A Blinded, Prospective Diagnostic Test Study: Level 2b Evidence Purpose: Assess individual items and identify optimum test-item cluster 82 patients recruited from four medical facilities Inclusion Criteria: electrophysiologic lab testing suggests CR or CTS Exclusion Criteria: systemic disease, bilateral pain, surgical procedures, history adversely affecting function of UE, previous testing on symptomatic limb NCS and EMG - reference standard Standardized clinical assessment of 34 items Performed by two therapists blinded to EMG/NCS results to test reliability

24 Analysis 11 variables with acceptable diagnostic accuracy ULTT A, Cervical rotation < 60, Cervical flexion < 55, Biceps MSR, Distraction test, Bicep MMT, Valsalva test, Spurling test A, Shoulder abduction test, C5 sensation, asking where symptoms are most bothersome, and asking if moving or positioning neck improves symptoms Regression model determined the best CR test item cluster
25 Conclusion Conclusions Test Item Cluster identified that provides higher posttest probability changes than individual items Limitations Reference standard required minimum EMG findings to establish diagnosis Large number of examiners and locations Study sample represented mild cases of almost exclusively C6 and C7 root level Further Research Tool requires validation with larger sample size
26 Conclusion What combination of tests is most accurate for diagnosing cervical radiculopathy in a 35-year old woman with neck pain and radiating symptoms? Cervical Distraction, Spurling s, Cervical Rotation, ULTT 1
27 Intervention Question For a 35-year old woman with cervical radiculopathy, is therapeutic exercise in conjunction with manual therapy more effective at reducing disability and symptoms compared to manual therapy alone?
28 Effectiveness of manual physical therapy in the treatment of cervical radiculopathy: a systematic review Boyles et al. Journal of Manual and Manipulative Therapy, 2011
29 A Systematic review: Level 2a evidence Purpose No systematic reviews have investigated the use of manual physical therapy for treatment of cervical radiculopathy. Objective To review current literature regarding the effectiveness of manual therapy in the treatment of cervical radiculopathy.
30 Methods Inclusion Criteria English language, PEDro score > 5 RCTs level I through case series (level IV) in peer reviewed journals between 1995 and Feb 2011 Patient under care of PT treated w/ manual therapy Diagnosed w/ CR based on MRI, CT Myelography, or a positive finding according to Wainner et al. CPR with 3 of 4 items present Included at least one of the following outcome measures AROM, PROM, functional outcome measure specific to neck (NDI), a quality of life measure (GROC) and a pain measure. Exclusion Criteria Surgical intervention within 1 year Non PT manual procedures Use of cervical collars and mechanical traction
31 Article Intervention Result Mobilization Manipulation Neural Mob MET Ragonese et al. Manual + Therapeutic exercise lowest pain and disability scores. Young et al. Significant improvements in pain and disability. Cleland et al. 53% surpassed MCIC Persson et al. No btw group difference
32 Conclusion Manual + Therapeutic Exercise = BEST Which intervention is responsible?? Future high quality RCTs featuring control groups needed.
33 Limitations 1. Only one article specifically prescribed the performed intervention. The other three articles allowed the PT to determine appropriate treatment. 2. None of the included studies were RCTs, so determining cause and effect relationship between manual therapy and the relief of CR symptoms is difficult. 3. Only articles published in English were reviewed leading to possible exclusion of other relevant articles.
34 A Randomized Control Trial Comparing Manual Therapy to Therapeutic Exercises, to a Combination of Therapies, for the Treatment of Cervical Radiculopathy Ragonese, Orthopedic Practice, 2009
35 A Randomized Control Trial: Level 1b Evidence Purpose: To determine which treatment method will produce superior outcomes for patients with cervical radiculopathy: manual physical therapy, therapeutic exercises, or a combination of manual physical therapy and therapeutic exercises
36 Methods: 30 patients with cervical radiculopathy 3 treatment groups: Only manual therapy Only therapeutic exercises Both manual therapy and therapeutic exercises 3 sessions/week for 3 weeks
37 Methods: Outcome Measures: Assessed at initial session, once per week, and at final session Numeric Pain Rating Scale (NPRS) Neck Disability Index (NDI) Cervical rotation AROM Results analyzed using independent groups ANOVA
38 Participant Characteristics 30 patients who were referred to the Outpatient Physical Therapy Department at Loyola University Medical Center with a chief complaint of neck and/or UE symptoms Inclusion Criteria: 4 positive exam findings on CPR of clinical radiculopathy Exclusion Criteria: If patient had any current medical condition that placed their rehab outside of routine practice
39 Intervention: Manual group: Cervical lateral glides Thoracic mobilizations Median nerve gliding Exercise group: Deep neck flexor strengthening Lower and middle trapezius strengthening Serratus anterior strengthening Combination group: Both manual therapy and therapeutic exercises
40 Results All 3 groups demonstrated significant improvements in pain, with the combination group showing greatest results All 3 groups demonstrated significant improvements in function, with the combination group again showing the greatest results All 3 groups demonstrated equal improvements in cervical rotation
41 Conclusion A multimodal treatment approach is superior than either intervention alone Combination of manual therapy and strengthening exercises
42 Limitations Small sample size Although only one evaluator, different therapists providing treatment (although were trained on each of manual techniques) There was no long-term follow-up to see how long patients improvement lasted The combination group essentially received 2x the amount of therapy
43 Conclusion For a 35-year old woman with cervical radiculopathy, is therapeutic exercise in conjunction with manual therapy more effective at reducing disability and symptoms compared to manual therapy alone? YES

44 Class Goal & Intervention
45 Physical Therapy Goals Short Term (3 weeks) Pt will demonstrate full active cervical flexion and rotation with pain < 3/10 to return to functional ADLs. Pt will score 15/50 on NDI for decreased perceived disability. Pt will report ability to work at computer for 15 minutes asymptomatically with proper body mechanics in order to return to function and work activities.
46 Physical Therapy Goals Long term (6 weeks) Pt will demonstrate ability to lift 40 lbs asymptomatically with proper body mechanics in order to return to childcare activities. Pt will demonstrate the ability to reach behind back asymptomatically in order to perform ADLs independently. Pt will score 5/50 on NDI for decreased perceived disability.


47 Pain Relief
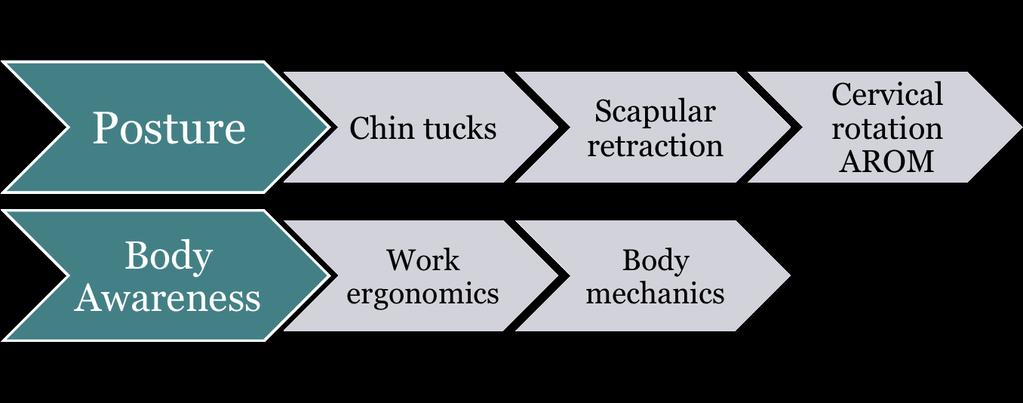
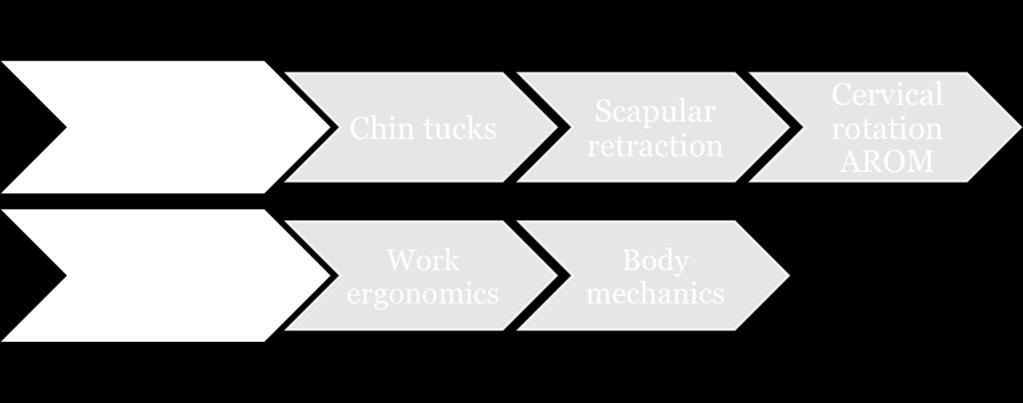
48 Education
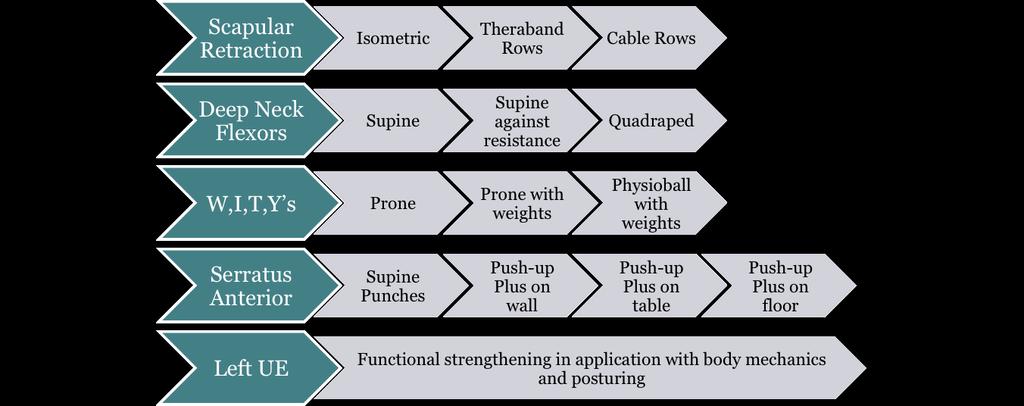
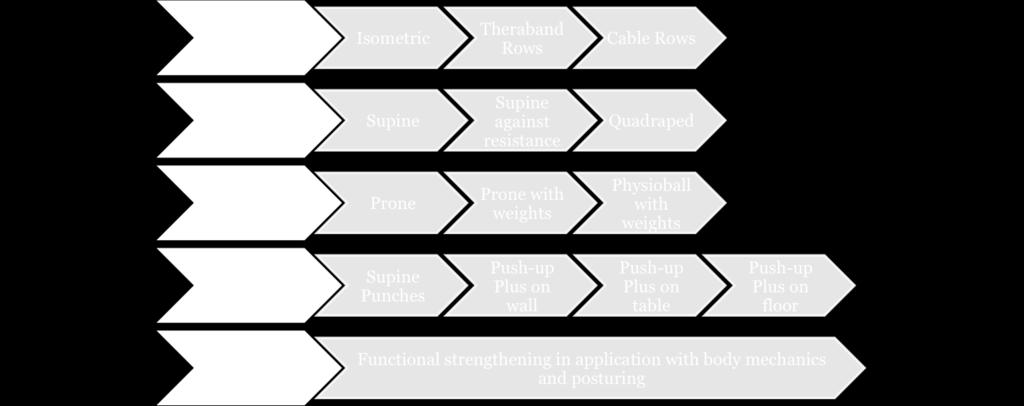
49 Strengthening

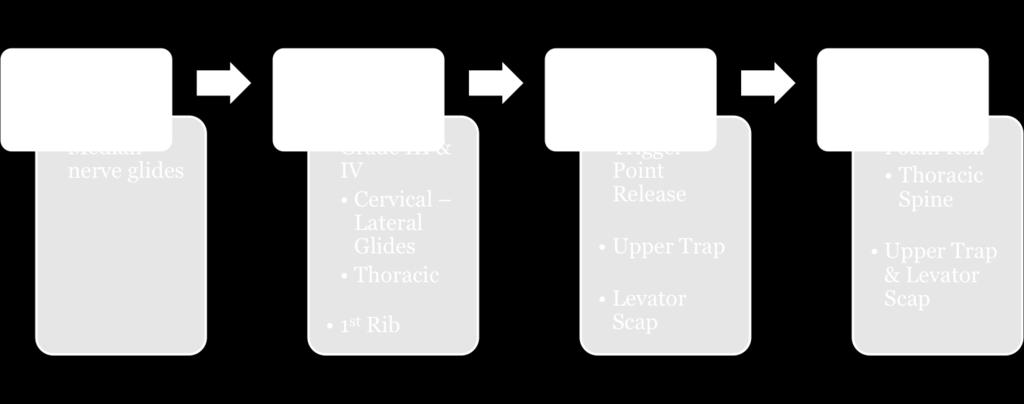
50 Manual & Stretching
51 References 1. Boyles, R. et al Effectiveness of manual physical therapy in the treatment of cervical radiculopathy: a systematic review. Journal of Manual and Manipulative Therapy, Ragonese, J. et al A Randomized Control Trial Comparing Manual Therapy to Therapeutic Exercises, to a Combination of Therapies, for the Treatment of Cervical Radiculopathy. Orthopedic Practice, Rubinstein, S, M. et al A systematic review of the diagnostic accuracy of provocative tests of the neck for diagnosing cervical radiculopathy. European Spine Journal, Wainer, R. S. et al.,2003. Reliability and diagnostic accuracy of the clinical examination and patient self-report measures for cervical radiculopathy. SPINE,
52 Questions?
Dynamic Neural Mobilization as an Adjunct Intervention for a Patient with Cervical Radiculopathy: A Case Report.
 Dynamic Neural Mobilization as an Adjunct Intervention for a Patient with Cervical Radiculopathy: A. Kara Delie, SPT Kristine Erickson, PT, MS, NCS 1 Abstract: Title: Dynamic Neural Mobilization as an
Dynamic Neural Mobilization as an Adjunct Intervention for a Patient with Cervical Radiculopathy: A. Kara Delie, SPT Kristine Erickson, PT, MS, NCS 1 Abstract: Title: Dynamic Neural Mobilization as an
Regional Review of Musculoskeletal System: Head, Neck, and Cervical Spine Presented by Michael L. Fink, PT, DSc, SCS, OCS Pre- Chapter Case Study
 Regional Review of Musculoskeletal System: Presented by Michael L. Fink, PT, DSc, SCS, OCS (20 minutes CEU Time) Subjective A 43-year-old male, reported a sudden onset of left-sided neck and upper extremity
Regional Review of Musculoskeletal System: Presented by Michael L. Fink, PT, DSc, SCS, OCS (20 minutes CEU Time) Subjective A 43-year-old male, reported a sudden onset of left-sided neck and upper extremity
TREATMENT OF CHRONIC MECHANICAL NECK PAIN IN AN OUTPATIENT ORTHOPEDIC SETTING
 TREATMENT OF CHRONIC MECHANICAL NECK PAIN IN AN OUTPATIENT ORTHOPEDIC SETTING Clinical Problem Solving II Allison Walsh PATIENT OVERVIEW Age: 22 years Gender: Female Chief Complaint: Cervical pain, cervicogenic
TREATMENT OF CHRONIC MECHANICAL NECK PAIN IN AN OUTPATIENT ORTHOPEDIC SETTING Clinical Problem Solving II Allison Walsh PATIENT OVERVIEW Age: 22 years Gender: Female Chief Complaint: Cervical pain, cervicogenic
Dynamic Neuromobilization for the Treatment of Thoracic Outlet Syndrome Courtney Convey and Dr. Erickson
 Dynamic Neuromobilization for the Treatment of Thoracic Outlet Syndrome Courtney Convey and Dr. Erickson Abstract Title: Dynamic Neuromobilization for the Treatment of Thoracic Outlet Syndrome Background:
Dynamic Neuromobilization for the Treatment of Thoracic Outlet Syndrome Courtney Convey and Dr. Erickson Abstract Title: Dynamic Neuromobilization for the Treatment of Thoracic Outlet Syndrome Background:
HISTORY AND CHIEF COMPLAINT:
 submitted by Keith M. Bartley, D.C. Jasper, IN 07/21/11 presented at Cox Seminar in Nashville, TN, on October 8 9, 2011 HISTORY AND CHIEF COMPLAINT: 01/21/11 55 year old male press operator for Jasper
submitted by Keith M. Bartley, D.C. Jasper, IN 07/21/11 presented at Cox Seminar in Nashville, TN, on October 8 9, 2011 HISTORY AND CHIEF COMPLAINT: 01/21/11 55 year old male press operator for Jasper
What do we want? Cervicothoracic Workgroup. ICF Scheme. start with end in mind. What do consumers want?
 Cervicothoracic Workgroup Use of the International Classification of Functioning to Develop Evidence-Based Treatment Guidelines for the Management of Cervicothoracic Conditions John D. Childs, PT, PhD,
Cervicothoracic Workgroup Use of the International Classification of Functioning to Develop Evidence-Based Treatment Guidelines for the Management of Cervicothoracic Conditions John D. Childs, PT, PhD,
Pain Assessment Patient Interview (location/nature of symptoms), Body Diagram. Observation and Examination: Tests and Measures
, Body Diagram. Observation and Examination: Tests and Measures") Examination of Upper Quarter Neurogenic Pain Jane Fedorczyk, PT, PhD, CHT Thomas Jefferson University, Philadelphia, PA Center of Excellence for Hand and Upper Limb Rehabilitation I. History Mechanism
Examination of Upper Quarter Neurogenic Pain Jane Fedorczyk, PT, PhD, CHT Thomas Jefferson University, Philadelphia, PA Center of Excellence for Hand and Upper Limb Rehabilitation I. History Mechanism
WEEKEND 1 CERVICAL SPINE
 Virginia Orthopedic Manual Physical Therapy Institute - Technique Manual WEEKEND 1 CERVICAL SPINE Cervical Active Range of Motion Testing Rotation CT Flexion Mid Cervical Flexion Extension Side-Bending
Virginia Orthopedic Manual Physical Therapy Institute - Technique Manual WEEKEND 1 CERVICAL SPINE Cervical Active Range of Motion Testing Rotation CT Flexion Mid Cervical Flexion Extension Side-Bending
The Utilization of the Clinical Practice Guideline: Neck Pain in
 The Utilization of the Clinical Practice Guideline: Neck Pain in Diagnosis and Treatment of a Patient with Neck Pain: A Case Report A case report submitted for the degree of Doctor of Physical Therapy
The Utilization of the Clinical Practice Guideline: Neck Pain in Diagnosis and Treatment of a Patient with Neck Pain: A Case Report A case report submitted for the degree of Doctor of Physical Therapy
Lab Workbook. ANATOMY Manual Muscle Testing Lower Trapezius Patient: prone
 ANATOMY Manual Muscle Testing Lower Trapezius Patient: prone Lab Workbook Fixation: place on hand below the scapula on the opposite side Test: adduction and depression of the scapula with lateral rotation
ANATOMY Manual Muscle Testing Lower Trapezius Patient: prone Lab Workbook Fixation: place on hand below the scapula on the opposite side Test: adduction and depression of the scapula with lateral rotation
CERVICAL SPINE TIPS A
 CERVICAL SPINE TIPS A Musculoskeletal Approach to managing Neck Pain An ALGORITHM, as a management guide Rick Bernau & Ian Wallbridge June 2010 THE PROCESS An interactive approach to the management of
CERVICAL SPINE TIPS A Musculoskeletal Approach to managing Neck Pain An ALGORITHM, as a management guide Rick Bernau & Ian Wallbridge June 2010 THE PROCESS An interactive approach to the management of
EVALUATION AND MANAGEMENT OF CERVICAL SPINE DISORDERS
 CERVICAL SPINE EVALUATION AND MANAGEMENT OF CERVICAL SPINE DISORDERS Gregory M Yoshida MD Supports the skull Allows movement of the head Houses the spinal cord CERVICAL SPINE Unique anatomy Upper C spine
CERVICAL SPINE EVALUATION AND MANAGEMENT OF CERVICAL SPINE DISORDERS Gregory M Yoshida MD Supports the skull Allows movement of the head Houses the spinal cord CERVICAL SPINE Unique anatomy Upper C spine
Alternative Therapies for Adhesive Capsulitis: A Case Study LANIE ALPHIN
 Alternative Therapies for Adhesive Capsulitis: A Case Study LANIE ALPHIN Case Background 53 year old female Chief Complaint: Right shoulder pain for 6 months Diagnosis: Adhesive Capsulitis Imagining indicated
Alternative Therapies for Adhesive Capsulitis: A Case Study LANIE ALPHIN Case Background 53 year old female Chief Complaint: Right shoulder pain for 6 months Diagnosis: Adhesive Capsulitis Imagining indicated
Evaluation of Tingling and Numbness in the Upper Extremities
 Evaluation of Tingling and Numbness in the Upper Extremities DR. W. ANTHONY FRISELLA M.D. ADVANCED BONE & JOINT, ST CHARLES MO MONA 2018 Overview Polyneuropathy Compressive nerve lesions Carpal tunnel
Evaluation of Tingling and Numbness in the Upper Extremities DR. W. ANTHONY FRISELLA M.D. ADVANCED BONE & JOINT, ST CHARLES MO MONA 2018 Overview Polyneuropathy Compressive nerve lesions Carpal tunnel
Upledger Institute Case Study CranioSacral Therapy Pain/Numbness/Limited Mobility By Amy Sanders, O.T.R., LMT, CST T
 Upledger Institute Case Study CranioSacral Therapy Pain/Numbness/Limited Mobility By Amy Sanders, O.T.R., LMT, CST T The purpose of this case report is to describe treatment for a client with cervical
Upledger Institute Case Study CranioSacral Therapy Pain/Numbness/Limited Mobility By Amy Sanders, O.T.R., LMT, CST T The purpose of this case report is to describe treatment for a client with cervical
TECHNOLOGY AND HOW WE USE IT TO DAMAGE OURSELVES WILLIAM A. DELP, DO ASSISTANT PROFESSOR OF OMM GA PCOM
 TECHNOLOGY AND HOW WE USE IT TO DAMAGE OURSELVES WILLIAM A. DELP, DO ASSISTANT PROFESSOR OF OMM GA PCOM OBJECTIVES Understand how we interact with technology new and old Understand how injury occurs Texting
TECHNOLOGY AND HOW WE USE IT TO DAMAGE OURSELVES WILLIAM A. DELP, DO ASSISTANT PROFESSOR OF OMM GA PCOM OBJECTIVES Understand how we interact with technology new and old Understand how injury occurs Texting
Arm Pain, Numbness, and Tingling: Etiologies and Treatment
 Arm Pain, Numbness, and Tingling: Etiologies and Treatment Steve Fowler MD Confluence Health Department of Physiatry Education Medical School: University of Utah Residency: Mayo Clinic Work Confluence
Arm Pain, Numbness, and Tingling: Etiologies and Treatment Steve Fowler MD Confluence Health Department of Physiatry Education Medical School: University of Utah Residency: Mayo Clinic Work Confluence
Documentation and Billing For Myofacial Disruption Treatment
 Documentation and Billing For Myofacial Disruption Treatment Page 1 of 7 Documentation Requirements The following information comes directly from the American Medical Association CPT coding Committee:
Documentation and Billing For Myofacial Disruption Treatment Page 1 of 7 Documentation Requirements The following information comes directly from the American Medical Association CPT coding Committee:
Thoracic Spine Management. Jason Zafereo, PT, OCS, FAAOMPT
 Thoracic Spine Management Jason Zafereo, PT, OCS, FAAOMPT Clinical i l Orthopedic Rehabilitation ti Education Objectives Describe the treatment interventions used for the management of pain from contractile
Thoracic Spine Management Jason Zafereo, PT, OCS, FAAOMPT Clinical i l Orthopedic Rehabilitation ti Education Objectives Describe the treatment interventions used for the management of pain from contractile
Physical Examination of the Shoulder
 General setup Patient will be examined in both the seated and supine position so exam table needed 360 degree access to patient Expose neck and both shoulders (for comparison); female in gown or sports
General setup Patient will be examined in both the seated and supine position so exam table needed 360 degree access to patient Expose neck and both shoulders (for comparison); female in gown or sports
UPPER EXTREMITY NEURODYAMICS
 UPPER EXTREMITY NEURODYAMICS Kristin Kelley, PT, DPT, OCS, FAAOMPT Orthopaedic Manual Physical Therapy Series Charlottesville 2017-2018 Body Chart Initial Hypothesis? Subjective Exam Medial epicondylalgia
UPPER EXTREMITY NEURODYAMICS Kristin Kelley, PT, DPT, OCS, FAAOMPT Orthopaedic Manual Physical Therapy Series Charlottesville 2017-2018 Body Chart Initial Hypothesis? Subjective Exam Medial epicondylalgia
Thoracic Spine Mobilization for Shoulder Pain. Scott Tauferner PT, ATC
 Thoracic Spine Mobilization for Shoulder Pain Scott Tauferner PT, ATC Conflicts of Interest None 1 2 3 Participants will be able to select thoracic mobilization strategies in patients with shoulder pain.
Thoracic Spine Mobilization for Shoulder Pain Scott Tauferner PT, ATC Conflicts of Interest None 1 2 3 Participants will be able to select thoracic mobilization strategies in patients with shoulder pain.
DPT 772 Spine Notebook Matt Kubalski, SPT
 DPT 772 Spine Notebook Matt Kubalski, SPT Table of Contents: IMPAIRMENTS/CLASSIFICATIONS PAGES Neck Pain with Mobility Deficit: Cervicalgia, Pain in thoracic spine - JOSPT 3-6 Neck Pain with Headache:
DPT 772 Spine Notebook Matt Kubalski, SPT Table of Contents: IMPAIRMENTS/CLASSIFICATIONS PAGES Neck Pain with Mobility Deficit: Cervicalgia, Pain in thoracic spine - JOSPT 3-6 Neck Pain with Headache:
Cervical Spine: Pearls and Pitfalls
 Cervical Spine: Pearls and Pitfalls Presenters Dr. Rob Donkin Functional Anatomy Current research Cervical Radiculopathy Dr. Gert Ferreira Red flags Case Study Kinesio Taping Chris Neethling Gonstead adjusting
Cervical Spine: Pearls and Pitfalls Presenters Dr. Rob Donkin Functional Anatomy Current research Cervical Radiculopathy Dr. Gert Ferreira Red flags Case Study Kinesio Taping Chris Neethling Gonstead adjusting
SHOULDER PAIN. A Real Pain in the Neck. Michael Wolk, MD Northeastern Rehabilitation Associates October 31, 2017
 SHOULDER PAIN A Real Pain in the Neck Michael Wolk, MD Northeastern Rehabilitation Associates October 31, 2017 THE SHOULDER JOINT (S) 1. glenohumeral 2. suprahumeral 3. acromioclavicular 4. scapulocostal
SHOULDER PAIN A Real Pain in the Neck Michael Wolk, MD Northeastern Rehabilitation Associates October 31, 2017 THE SHOULDER JOINT (S) 1. glenohumeral 2. suprahumeral 3. acromioclavicular 4. scapulocostal
Symptoms and Referred Pain from Myofascial Trigger Points in the Anterior Scalene Muscle or Scalenus Anterior
 Symptoms and Referred Pain from Myofascial Trigger Points in the Anterior Scalene Muscle or Scalenus Anterior picture Symptoms and signs Aching or throbbing in the lateral forearm extending to thumb and
Symptoms and Referred Pain from Myofascial Trigger Points in the Anterior Scalene Muscle or Scalenus Anterior picture Symptoms and signs Aching or throbbing in the lateral forearm extending to thumb and
Official Definition. Carpal tunnel syndrome, the most common focal peripheral neuropathy, results from compression of the median nerve at the wrist.
 Mod 2 MMT Course Official Definition Carpal tunnel syndrome, the most common focal peripheral neuropathy, results from compression of the median nerve at the wrist. epidemiology Affects an estimated 3
Mod 2 MMT Course Official Definition Carpal tunnel syndrome, the most common focal peripheral neuropathy, results from compression of the median nerve at the wrist. epidemiology Affects an estimated 3
Application of Classification Systems and Multimodal Interventions for a 69-yearold
 Application of Classification Systems and Multimodal Interventions for a 69-yearold Patient with Cervical Disc Degeneration and Radicular Pain: A Case Report Ben Miers, SPT Lauren Fackler, PT, DPT Christopher
Application of Classification Systems and Multimodal Interventions for a 69-yearold Patient with Cervical Disc Degeneration and Radicular Pain: A Case Report Ben Miers, SPT Lauren Fackler, PT, DPT Christopher
Latarjet Repair Rehabilitation Protocol
 General Notes: As tolerated should be understood to include with safety for the reconstruction/repair; a sudden increase in pain, swelling, or other undesirable factors are indicators that you are doing
General Notes: As tolerated should be understood to include with safety for the reconstruction/repair; a sudden increase in pain, swelling, or other undesirable factors are indicators that you are doing
Nonoperative Treatment For Rotator Cuff Tendinitis/ Partial Thickness Tear Dr. Trueblood
 Nonoperative Treatment For Rotator Cuff Tendinitis/ Partial Thickness Tear Dr. Trueblood Relieving Pain Patients who present with SIS will have shoulder pain that is exacerbated with overhead activities.
Nonoperative Treatment For Rotator Cuff Tendinitis/ Partial Thickness Tear Dr. Trueblood Relieving Pain Patients who present with SIS will have shoulder pain that is exacerbated with overhead activities.
Avon Office 2 Simsbury Rd. Avon, CT Office: (860) Fax: (860) REHABILITATION AFTER REVERSE SHOULDER ARTHROPLASTY
 Fax: (860) REHABILITATION AFTER REVERSE SHOULDER ARTHROPLASTY") Katherine J. Coyner, MD UCONN Musculoskeletal Institute Medical Arts & Research Building 263 Farmington Ave. Farmington, CT 06030 Office: (860) 679-6600 Fax: (860) 679-6649 www.drcoyner.com Avon Office
Katherine J. Coyner, MD UCONN Musculoskeletal Institute Medical Arts & Research Building 263 Farmington Ave. Farmington, CT 06030 Office: (860) 679-6600 Fax: (860) 679-6649 www.drcoyner.com Avon Office
S p o r t s & O r t h o p a e d i c S p e c i a l i s t s A n t e r i o r I n s t a b i l i t y P r o t o c o l
 S p o r t s & O r t h o p a e d i c S p e c i a l i s t s This protocol provides appropriate guidelines for the rehabilitation of patients with anterior instability. The protocol draws evidence from the
S p o r t s & O r t h o p a e d i c S p e c i a l i s t s This protocol provides appropriate guidelines for the rehabilitation of patients with anterior instability. The protocol draws evidence from the
Thoracic Spine Applied Anatomy. Jason Zafereo, PT, OCS, FAAOMPT
 Thoracic Spine Applied Anatomy Jason Zafereo, PT, OCS, FAAOMPT Clinical i l Orthopedic Rehabilitation ti Education Objectives Discuss concepts relevant to thoracic pain of red flag origin Discuss concepts
Thoracic Spine Applied Anatomy Jason Zafereo, PT, OCS, FAAOMPT Clinical i l Orthopedic Rehabilitation ti Education Objectives Discuss concepts relevant to thoracic pain of red flag origin Discuss concepts
Osteopathic Considerations in Shoulder Pain. Kristen Brusky DO February 22, 2018
 Osteopathic Considerations in Shoulder Pain Kristen Brusky DO February 22, 2018 Overview Importance of pectoral girdle Ligaments, ligaments tensegrity Bones, joints, muscles Neurovasculature Innervation
Osteopathic Considerations in Shoulder Pain Kristen Brusky DO February 22, 2018 Overview Importance of pectoral girdle Ligaments, ligaments tensegrity Bones, joints, muscles Neurovasculature Innervation
The Straw that Broke the Child s Back SPORTS Symposium E. John Stanley PT,SCS
 The Straw that Broke the Child s Back 2017 SPORTS Symposium E. John Stanley PT,SCS Learning Objectives: 1.Identify 3 characteristics of kids at risk for back injuries. 2.Describe the impact of flexibility,
The Straw that Broke the Child s Back 2017 SPORTS Symposium E. John Stanley PT,SCS Learning Objectives: 1.Identify 3 characteristics of kids at risk for back injuries. 2.Describe the impact of flexibility,
Clinical Examination. of the. Cervicothoracic Region. Neck Disability Index. Serious Pathological Conditions. Medical Screening Questionnaire
 Clinical Examination Clinical Examination of the Cervicothoracic Region Screening for associated serious pathological conditions Neck disability index Physical Exam Serious Pathological Conditions Cervical
Clinical Examination Clinical Examination of the Cervicothoracic Region Screening for associated serious pathological conditions Neck disability index Physical Exam Serious Pathological Conditions Cervical
TALLGRASS ORTHOPEDIC & SPORTS MEDICINE. Phase I Immediate Post-Surgical Phase (Weeks 0-2) Date: Maintain/protect integrity of the repair
 Date: Maintain/protect integrity of the repair") TALLGRASS ORTHOPEDIC & SPORTS MEDICINE Name: Date of Surgery: Patient Flow Sheet Arthroscopic Rotator Cuff Repair Small to Medium Tears Benedict Figuerres, MD Phase I Immediate Post-Surgical Phase (Weeks
TALLGRASS ORTHOPEDIC & SPORTS MEDICINE Name: Date of Surgery: Patient Flow Sheet Arthroscopic Rotator Cuff Repair Small to Medium Tears Benedict Figuerres, MD Phase I Immediate Post-Surgical Phase (Weeks
LUMBAR SPINE CASE 3. Property of VOMPTI, LLC. For Use of Participants Only. No Use or Reproduction Without Consent 1. L4-5, 5-S1 disc, facet (somatic)
") LUMBAR SPINE CASE 3 A.J. Lievre, PT, DPT, OCS, CMPT Aaron Hartstein, PT, DPT, OCS, FAAOMPT Orthopaedic Manual Physical Therapy Series Richmond 2018-2019 L4-5, 5-S1 disc, facet (somatic) L5/S1 Radiculopathy
LUMBAR SPINE CASE 3 A.J. Lievre, PT, DPT, OCS, CMPT Aaron Hartstein, PT, DPT, OCS, FAAOMPT Orthopaedic Manual Physical Therapy Series Richmond 2018-2019 L4-5, 5-S1 disc, facet (somatic) L5/S1 Radiculopathy
A.J. Lievre, PT, DPT, OCS, CMPT Aaron Hartstein, PT, DPT, OCS, FAAOMPT
 LUMBAR SPINE CASE #3 A.J. Lievre, PT, DPT, OCS, CMPT Aaron Hartstein, PT, DPT, OCS, FAAOMPT Orthopaedic Manual Physical Therapy Series Charlottesville 2017-2018 L4-5, 5-S1 disc, facet (somatic) L5/S1 Radiculopathy
LUMBAR SPINE CASE #3 A.J. Lievre, PT, DPT, OCS, CMPT Aaron Hartstein, PT, DPT, OCS, FAAOMPT Orthopaedic Manual Physical Therapy Series Charlottesville 2017-2018 L4-5, 5-S1 disc, facet (somatic) L5/S1 Radiculopathy
Cervical and Thoracic Spinal Conditions Chapter 11
 Cervical and Thoracic Spinal Conditions Chapter 11 Anatomy Spinal column Vertebrae Cervical (7) convex anteriorly Thoracic (12) concave anteriorly Lumbar (5) convex anteriorly Sacral (5 fused) concave
Cervical and Thoracic Spinal Conditions Chapter 11 Anatomy Spinal column Vertebrae Cervical (7) convex anteriorly Thoracic (12) concave anteriorly Lumbar (5) convex anteriorly Sacral (5 fused) concave
10/5/2017. Cervical Manual Evaluation and Mobilizations. Upper Cervical Stability Testing Alar Ligament
 Cervical Manual Evaluation and Mobilizations Upper Cervical Stability Testing Alar Ligament Upper Cervical Stability Testing Transverse Ligament 1 Upper Cervical Stability Testing Transverse Plane Positive
Cervical Manual Evaluation and Mobilizations Upper Cervical Stability Testing Alar Ligament Upper Cervical Stability Testing Transverse Ligament 1 Upper Cervical Stability Testing Transverse Plane Positive
NECK PAIN WORKSHOP A Musculoskeletal Approach to managing Neck Pain An ALGORITHM, as a management guide
 NECK PAIN WORKSHOP A Musculoskeletal Approach to managing Neck Pain An ALGORITHM, as a management guide Rick Bernau & Ian Wallbridge June 2010 THE PROCESS An interactive approach to the management of neck
NECK PAIN WORKSHOP A Musculoskeletal Approach to managing Neck Pain An ALGORITHM, as a management guide Rick Bernau & Ian Wallbridge June 2010 THE PROCESS An interactive approach to the management of neck
Treatment of a 41 Year Old Male Status/Post MVA with Radicular Symptoms in the Left Arm and Scapula: A Case Report
 Governors State University OPUS Open Portal to University Scholarship All Capstone Projects Student Capstone Projects Spring 2015 Treatment of a 41 Year Old Male Status/Post MVA with Radicular Symptoms
Governors State University OPUS Open Portal to University Scholarship All Capstone Projects Student Capstone Projects Spring 2015 Treatment of a 41 Year Old Male Status/Post MVA with Radicular Symptoms
Diagnostic and Management Approach to the Painful Shoulder
 Diagnostic and Management Approach to the Painful Shoulder Introduction What conditions causing shoulder pain commonly present in General Practice? Subacromial impingement Rotator cuff tears AC joint pathology
Diagnostic and Management Approach to the Painful Shoulder Introduction What conditions causing shoulder pain commonly present in General Practice? Subacromial impingement Rotator cuff tears AC joint pathology
Shoulder Impingement Rehabilitation Recommendations
 Shoulder Impingement Rehabilitation Recommendations The following protocol can be utilized for conservative care of shoulder impingement as well as post- operative subacromial decompression (SAD) surgery.
Shoulder Impingement Rehabilitation Recommendations The following protocol can be utilized for conservative care of shoulder impingement as well as post- operative subacromial decompression (SAD) surgery.
Premier Orthopedic Spine Center
 Premier Orthopedic Spine Center Atrium Medical Center Professional Buliding 200 Medical Center Dr., Ste. 375 Middletown, Ohio 45005 Neck Questionnaire Patient Date Family Physician The onset of my neck
Premier Orthopedic Spine Center Atrium Medical Center Professional Buliding 200 Medical Center Dr., Ste. 375 Middletown, Ohio 45005 Neck Questionnaire Patient Date Family Physician The onset of my neck
Upper Cross Syndrome: Assessment & Management in Family Practice HKDU Symposium Dec 2014
 Upper Cross Syndrome: Assessment & Management in Family Practice HKDU Symposium Dec 2014 Dr. Ngai Ho Yin Allen Family Medicine Specialist PGDipMusculoskeletal Medicine MBBS(HK), DCH(London), DFM(CUHK),
Upper Cross Syndrome: Assessment & Management in Family Practice HKDU Symposium Dec 2014 Dr. Ngai Ho Yin Allen Family Medicine Specialist PGDipMusculoskeletal Medicine MBBS(HK), DCH(London), DFM(CUHK),
ACTIVE AGING.
 Shoulder Pain Rehabilitation Protocol Rotator Cuff Syndrome Shoulder impingement The Resistance Chair Solution Shoulder Impingement a. Shoulder impingement is one of the most common causes of shoulder
Shoulder Pain Rehabilitation Protocol Rotator Cuff Syndrome Shoulder impingement The Resistance Chair Solution Shoulder Impingement a. Shoulder impingement is one of the most common causes of shoulder
Musculoskeletal Examination of the Pain Patient
 Musculoskeletal Examination of the Pain Patient Joseph F. Audette, M.A., M.D Assistant Clinical Professor, Harvard Medical School Chief, Department of Pain Medicine Harvard Vanguard Medical Associates
Musculoskeletal Examination of the Pain Patient Joseph F. Audette, M.A., M.D Assistant Clinical Professor, Harvard Medical School Chief, Department of Pain Medicine Harvard Vanguard Medical Associates
Anterior Stabilization of the Shoulder: Distal Tibial Allograft
 Anterior Stabilization of the Shoulder: Distal Tibial Allograft Name: Diagnosis: Date: Date of Surgery: Phase I Immediate Post Surgical Phase (approximately Weeks 1-3) Minimize shoulder pain and inflammatory
Anterior Stabilization of the Shoulder: Distal Tibial Allograft Name: Diagnosis: Date: Date of Surgery: Phase I Immediate Post Surgical Phase (approximately Weeks 1-3) Minimize shoulder pain and inflammatory
Brachial Plexopathy in a Division I Football Player
 www.fisiokinesiterapia.biz Brachial Plexopathy in a Division I Football Player Brachial Plexus Injuries in Sport Typically a transient neurapraxia - 70% of injured players said they did not always report
www.fisiokinesiterapia.biz Brachial Plexopathy in a Division I Football Player Brachial Plexus Injuries in Sport Typically a transient neurapraxia - 70% of injured players said they did not always report
Please Note: This is an Example Case Study Not to Be Reproduced, Copied or Shared
 Please Note: This is an Example Case Study Not to Be Reproduced, Copied or Shared Your Name Workshops Name and date Case Study For Level 3 FST History: a) Torn labrum R shoulder 2009 Complete rupture/tear
Please Note: This is an Example Case Study Not to Be Reproduced, Copied or Shared Your Name Workshops Name and date Case Study For Level 3 FST History: a) Torn labrum R shoulder 2009 Complete rupture/tear
Shoulder and Elbow ORTHOPAEDIC SYPMPOSIUM APRIL 8, 2017 DANIEL DOTY MD
 Shoulder and Elbow ORTHOPAEDIC SYPMPOSIUM APRIL 8, 2017 DANIEL DOTY MD Shoulder Articulations Glenohumeral Joint 2/3 total arc of motion Shallow Ball and Socket Joint Allows for excellent ROM Requires
Shoulder and Elbow ORTHOPAEDIC SYPMPOSIUM APRIL 8, 2017 DANIEL DOTY MD Shoulder Articulations Glenohumeral Joint 2/3 total arc of motion Shallow Ball and Socket Joint Allows for excellent ROM Requires
Restraints to Movement... 4 Restraints to flexion... 4 Primary restraint into Extension... 4
 CERVICAL SPINE... 4 Neck Pain Categories... 4 Kinematics... Error! Bookmark not defined. Ranges of Motion C2-7... 4 Coupled Movements... 4 Ranges of Motion C0-2... 4 Coupled Movements... 4 Restraints to
CERVICAL SPINE... 4 Neck Pain Categories... 4 Kinematics... Error! Bookmark not defined. Ranges of Motion C2-7... 4 Coupled Movements... 4 Ranges of Motion C0-2... 4 Coupled Movements... 4 Restraints to
Do you Treat Ribs? The Role Between the Axial and Appendicular Skeleton
 Do you Treat Ribs? The Role Between the Axial and Appendicular Skeleton Your Presenters: Eric S. Furto, PT, DPT, MTC, FAAOMPT Larry Yack, PT, DPT, MTC Ribs 2-9, 12 articulations 2 Intervertebral 10 Innervated
Do you Treat Ribs? The Role Between the Axial and Appendicular Skeleton Your Presenters: Eric S. Furto, PT, DPT, MTC, FAAOMPT Larry Yack, PT, DPT, MTC Ribs 2-9, 12 articulations 2 Intervertebral 10 Innervated
Shoulder Arthroscopy: Postop Instructions. Activites & Advice for in the Hospital and while at Home
 Dr. Mark Price MGH Sports Medicine Center 175 Cambridge Street, 4th floor Boston, MA 02114 www.massgeneral.org/ortho-sports-medicine/dr-price Shoulder Arthroscopy: Postop Instructions You will wake up
Dr. Mark Price MGH Sports Medicine Center 175 Cambridge Street, 4th floor Boston, MA 02114 www.massgeneral.org/ortho-sports-medicine/dr-price Shoulder Arthroscopy: Postop Instructions You will wake up
Cervical Radiculopathy: My 32 Year-Old Cyclist is Nervous What do I do on the initial visit?
 Cervical Radiculopathy: My 32 Year-Old Cyclist is Nervous What do I do on the initial visit? Scott D Boden, MD The Emory Spine Center Atlanta, Georgia History of Trauma? 2 History of Trauma? 3 Sometimes
Cervical Radiculopathy: My 32 Year-Old Cyclist is Nervous What do I do on the initial visit? Scott D Boden, MD The Emory Spine Center Atlanta, Georgia History of Trauma? 2 History of Trauma? 3 Sometimes
Diagnostic and Treatment Approach to the Active Patient with Complex Spine Pathology
 Physical Therapy Diagnostic and Treatment Approach to the Active Patient with Complex Spine Pathology Scott Behjani, DPT, OCS Introduction Prevalence 1-year incidence of first-episode LBP ranges from
Physical Therapy Diagnostic and Treatment Approach to the Active Patient with Complex Spine Pathology Scott Behjani, DPT, OCS Introduction Prevalence 1-year incidence of first-episode LBP ranges from
Missing figures - copyright restrictions
 Cervical alignment Consideration of Adjacent Regions Shirley Sahrmann, PT, PhD, FAPTA Mary Kate McDonnell PT,DPT,OCS Washington University School of Medicine -St. Louis Cervical movement Diagnoses with
Cervical alignment Consideration of Adjacent Regions Shirley Sahrmann, PT, PhD, FAPTA Mary Kate McDonnell PT,DPT,OCS Washington University School of Medicine -St. Louis Cervical movement Diagnoses with
Rotator Cuff Repair Therapy Protocol
 Bart Eastwood D.O. 825 Davis st Blacksburg, VA 24060 540-951-6000 All information contained in this protocol is to be used as general guidelines only. Specific variations may be appropriate for each patient
Bart Eastwood D.O. 825 Davis st Blacksburg, VA 24060 540-951-6000 All information contained in this protocol is to be used as general guidelines only. Specific variations may be appropriate for each patient
Anterior Stabilization of the Shoulder: Latarjet Protocol
 Robert K. Fullick, MD 6400 Fannin Street, Suite 1700 Houston, Texas 77030 Ph.: 713-486-7543 / Fx.: 713-486-5549 Anterior Stabilization of the Shoulder: Latarjet Protocol The intent of this protocol is
Robert K. Fullick, MD 6400 Fannin Street, Suite 1700 Houston, Texas 77030 Ph.: 713-486-7543 / Fx.: 713-486-5549 Anterior Stabilization of the Shoulder: Latarjet Protocol The intent of this protocol is
5 minutes: Attendance and Breath of Arrival. 50 minutes: Problem Solving Torso
 5 minutes: Attendance and Breath of Arrival 50 minutes: Problem Solving Torso Punctuality- everybody's time is precious: o o Be ready to learn by the start of class, we'll have you out of here on time
5 minutes: Attendance and Breath of Arrival 50 minutes: Problem Solving Torso Punctuality- everybody's time is precious: o o Be ready to learn by the start of class, we'll have you out of here on time
Total Shoulder Rehab Protocol Dr. Payne
 Total Shoulder Rehab Protocol Dr. Payne Phase I Immediate Post Surgical Phase (0-4 weeks): Allow healing of soft tissue Maintain integrity of replaced joint Gradually increase passive range of motion (PROM)
Total Shoulder Rehab Protocol Dr. Payne Phase I Immediate Post Surgical Phase (0-4 weeks): Allow healing of soft tissue Maintain integrity of replaced joint Gradually increase passive range of motion (PROM)
Christopher K. Jones, MD Colorado Springs Orthopaedic Group
 Christopher K. Jones, MD Colorado Springs Orthopaedic Group 719-632-7669 Total Shoulder Replacement You have undergone a shoulder replacement procedure. The performance of the procedure is complete, but
Christopher K. Jones, MD Colorado Springs Orthopaedic Group 719-632-7669 Total Shoulder Replacement You have undergone a shoulder replacement procedure. The performance of the procedure is complete, but
Thoracic Spine Applied Anatomy. Jason Zafereo, PT, OCS, FAAOMPT
 Thoracic Spine Applied Anatomy Jason Zafereo, PT, OCS, FAAOMPT Clinical i l Orthopedic Rehabilitation ti Education 1 Objectives Discuss red flag signs for the thoracic region Apply key concepts from the
Thoracic Spine Applied Anatomy Jason Zafereo, PT, OCS, FAAOMPT Clinical i l Orthopedic Rehabilitation ti Education 1 Objectives Discuss red flag signs for the thoracic region Apply key concepts from the
CENTER FOR ORTHOPAEDICS AND SPINE CARE PHYSICAL THERAPY PROTOCOL BENJAMIN J. DAVIS, MD Type Two Rotator Cuff Repair
 I. Phase I - Immediate Post-Surgical Phase (Day 1-10) Goals: Maintain Integrity of the Repair Gradually Increase Passive Range of Motion Diminish Pain and Inflammation Prevent Muscular Inhibition Passive
I. Phase I - Immediate Post-Surgical Phase (Day 1-10) Goals: Maintain Integrity of the Repair Gradually Increase Passive Range of Motion Diminish Pain and Inflammation Prevent Muscular Inhibition Passive
Pain: Who is Likely to Respond?
 Spinal Manipulation for Shoulder Pain: Who is Likely to Respond? Lori Michener, PhD, PT, ATC, FAPTA Professor Director of Clinical Outcomes and Research Director University of Southern California; Los
Spinal Manipulation for Shoulder Pain: Who is Likely to Respond? Lori Michener, PhD, PT, ATC, FAPTA Professor Director of Clinical Outcomes and Research Director University of Southern California; Los
Cervical Spine in Baseball
 Cervical Spine in Baseball Robert G Watkins, IV, MD Co-Director, Marina Spine Center Marina del Rey, CA Vice Chief of Staff Cedars-Marina del Rey Hospital Disclosures n Pioneer / RTI Consulting, Royalties
Cervical Spine in Baseball Robert G Watkins, IV, MD Co-Director, Marina Spine Center Marina del Rey, CA Vice Chief of Staff Cedars-Marina del Rey Hospital Disclosures n Pioneer / RTI Consulting, Royalties
Neck Pain & the Cervical Spine
 Neck Pain & the Cervical Spine At Loudoun Sports Therapy Center, we are specialists in treating all orthopedic conditions and injuries. It s our goal to help you live a healthy, active, pain-free lifestyle.
Neck Pain & the Cervical Spine At Loudoun Sports Therapy Center, we are specialists in treating all orthopedic conditions and injuries. It s our goal to help you live a healthy, active, pain-free lifestyle.
Ms. Ruth A. Delaney, MB BCh BAO, MMedSc, MRCS
 Ms. Ruth A. Delaney, MB BCh BAO, MMedSc, MRCS Consultant Orthopaedic Surgeon, Shoulder Specialist. +353 1 5262335 ruthdelaney@sportssurgeryclinic.com Modified from the protocol developed at Boston Shoulder
Ms. Ruth A. Delaney, MB BCh BAO, MMedSc, MRCS Consultant Orthopaedic Surgeon, Shoulder Specialist. +353 1 5262335 ruthdelaney@sportssurgeryclinic.com Modified from the protocol developed at Boston Shoulder
Cervical Spine Exercise and Manual Therapy for the Autonomous Practitioner
 Cervical Spine Exercise and Manual Therapy for the Autonomous Practitioner Eric Chaconas PT, PhD, DPT, FAAOMPT Assistant Professor and Assistant Program Director Doctor of Physical Therapy Program Eric
Cervical Spine Exercise and Manual Therapy for the Autonomous Practitioner Eric Chaconas PT, PhD, DPT, FAAOMPT Assistant Professor and Assistant Program Director Doctor of Physical Therapy Program Eric
Rehab protocol. Phase I: Immediate Post-Surgical Phase: Typically 0-4 weeks; 2 PT visits. Goals:
 Reverse Total shoulder arthroplasty Rehab protocol Phase I: Immediate Post-Surgical Phase: Typically 0-4 weeks; 2 PT visits Allow healing of soft tissue Maintain integrity of replaced joint Gradually increase
Reverse Total shoulder arthroplasty Rehab protocol Phase I: Immediate Post-Surgical Phase: Typically 0-4 weeks; 2 PT visits Allow healing of soft tissue Maintain integrity of replaced joint Gradually increase
Stand-Alone Technology. Reginald Davis, M.D., FAANS, FACS Director of Clinical Research
 Stand-Alone Technology Reginald Davis, M.D., FAANS, FACS Director of Clinical Research Disclosures Stand-Alone Devices Optio-C Stalif C Coalition Prevail ROI-C Technology Descriptions Optio-C A no profile,
Stand-Alone Technology Reginald Davis, M.D., FAANS, FACS Director of Clinical Research Disclosures Stand-Alone Devices Optio-C Stalif C Coalition Prevail ROI-C Technology Descriptions Optio-C A no profile,
82a Orthopedic Massage! Introduction - Thoracic Outlet"
 82a Orthopedic Massage! Introduction - Thoracic Outlet" 82a Orthopedic Massage! Introduction - Thoracic Outlet! Class Outline" 5 minutes" "Attendance, Breath of Arrival, and Reminders " 10 minutes "Lecture:"
82a Orthopedic Massage! Introduction - Thoracic Outlet" 82a Orthopedic Massage! Introduction - Thoracic Outlet! Class Outline" 5 minutes" "Attendance, Breath of Arrival, and Reminders " 10 minutes "Lecture:"
Phase I : Immediate Postoperative Phase- Protected Motion. (0-2 Weeks)
") Phase I : Immediate Postoperative Phase- Protected Motion (0-2 Weeks) Appointments Progression Criteria 2 weeks after surgery Rehabilitation appointments begin within 7-10 days of surgery, continue 1-2
Phase I : Immediate Postoperative Phase- Protected Motion (0-2 Weeks) Appointments Progression Criteria 2 weeks after surgery Rehabilitation appointments begin within 7-10 days of surgery, continue 1-2
Identification of Painful Tissue Orthopaedic Examination DX 612. James J. Lehman, DC, MBA, DABCO University of Bridgeport College of Chiropractic
 Identification of Painful Tissue Orthopaedic Examination DX 612 James J. Lehman, DC, MBA, DABCO University of Bridgeport College of Chiropractic Generalized Pain Description Joint pain may be constant
Identification of Painful Tissue Orthopaedic Examination DX 612 James J. Lehman, DC, MBA, DABCO University of Bridgeport College of Chiropractic Generalized Pain Description Joint pain may be constant
Efficient Examination Printable Templates
 Efficient Examination Printable Templates Seated Tests and Measures Sidelying Tests and Measures -Seated posture -Strength testing (gluteus medius) -Neurological examination (SLUMP test, dermatomes, -Sacroiliac
Efficient Examination Printable Templates Seated Tests and Measures Sidelying Tests and Measures -Seated posture -Strength testing (gluteus medius) -Neurological examination (SLUMP test, dermatomes, -Sacroiliac
Chapter 2 Diagnostic Algorithms. 4 Traumatic Neck Pain Algorithm
 Chapter 2 Diagnostic Algorithms 4 Traumatic Neck Pain Algorithm Patient presents with a traumatic onset of neck pain. In general, radiographs should be ordered with a history of recent, significant trauma.
Chapter 2 Diagnostic Algorithms 4 Traumatic Neck Pain Algorithm Patient presents with a traumatic onset of neck pain. In general, radiographs should be ordered with a history of recent, significant trauma.
Is This Really a Musculoskeletal Problem?
 Is This Really a Musculoskeletal Problem? UCSF Orthopedics Primary Care Sports Medicine Anthony Luke MD, MPH Annual Review in Family Medicine 2015 Disclosures Founder, RunSafe Founder & CEO, SportZPeak
Is This Really a Musculoskeletal Problem? UCSF Orthopedics Primary Care Sports Medicine Anthony Luke MD, MPH Annual Review in Family Medicine 2015 Disclosures Founder, RunSafe Founder & CEO, SportZPeak
Large/Massive Rotator Cuff Repair
 Large/Massive Rotator Cuff Repair 1. Defined a. Suturing of tears within the rotator cuff (most commonly supraspinatus muscle). Massive RCR usually involve more than the supraspinatus. b. May be done arthroscopically
Large/Massive Rotator Cuff Repair 1. Defined a. Suturing of tears within the rotator cuff (most commonly supraspinatus muscle). Massive RCR usually involve more than the supraspinatus. b. May be done arthroscopically
MLT Muscle(s) Patient Position Therapist position Stabilization Limb Position Picture Put biceps on slack by bending elbow.
 Patient Position Therapist position Stabilization Limb Position Picture Put biceps on slack by bending elbow.") MLT Muscle(s) Patient Position Therapist position Stabilization Limb Position Picture Put biceps on slack by bending elbow. Pectoralis Minor Supine, arm at side, elbows extended, supinated Head of Table
MLT Muscle(s) Patient Position Therapist position Stabilization Limb Position Picture Put biceps on slack by bending elbow. Pectoralis Minor Supine, arm at side, elbows extended, supinated Head of Table
ATRAUMATIC SHOULDER CONDITIONS. Matthew J. Landfried, MD Orthopaedic Surgeon Genesee Orthopaedics and Sports Medicine
 ATRAUMATIC SHOULDER CONDITIONS Matthew J. Landfried, MD Orthopaedic Surgeon Genesee Orthopaedics and Sports Medicine MATTHEW LANDFRIED MD Board Certified in Orthopedic Surgery and Sports Medicine Received
ATRAUMATIC SHOULDER CONDITIONS Matthew J. Landfried, MD Orthopaedic Surgeon Genesee Orthopaedics and Sports Medicine MATTHEW LANDFRIED MD Board Certified in Orthopedic Surgery and Sports Medicine Received
1-Apley scratch test.
 1-Apley scratch test. The patient attempts to touch the opposite scapula to test range of motion of the shoulder. 1-Testing abduction and external rotation( +ve sign touch the opposite scapula, -ve sign
1-Apley scratch test. The patient attempts to touch the opposite scapula to test range of motion of the shoulder. 1-Testing abduction and external rotation( +ve sign touch the opposite scapula, -ve sign
Thoracic Manipulations and Mechanical Neck Pain: Exploring the CPR. By Greg Banks
 Thoracic Manipulations and Mechanical Neck Pain: Exploring the CPR By Greg Banks Theories of Thoracic Manipulation -Picker et. al: changes in mechanoreceptor discharge. -Analgesic response from descending
Thoracic Manipulations and Mechanical Neck Pain: Exploring the CPR By Greg Banks Theories of Thoracic Manipulation -Picker et. al: changes in mechanoreceptor discharge. -Analgesic response from descending
Thoracic Outlet Syndrome
 Thoracic Outlet Syndrome Part 1: The Scalene Triangle TOS: Vascular Symptom Presentation Venous persistent/intermittent edema heaviness and fatigue deep pain in neck/shoulder increased pain at night warm
Thoracic Outlet Syndrome Part 1: The Scalene Triangle TOS: Vascular Symptom Presentation Venous persistent/intermittent edema heaviness and fatigue deep pain in neck/shoulder increased pain at night warm
Andrew Scott MRSS MCSP. Postural Shoulder Pain
 Andrew Scott MRSS MCSP Postural Shoulder Pain Andrew Scott 25 years shiatsu experience 15 years shiatsu teacher with British School of Shiatsu-Do and in my own school in Liverpool Chartered Physiotherapist
Andrew Scott MRSS MCSP Postural Shoulder Pain Andrew Scott 25 years shiatsu experience 15 years shiatsu teacher with British School of Shiatsu-Do and in my own school in Liverpool Chartered Physiotherapist
Case Report: CASE REPORT OF FACET ARTHROPATHY INDUCED NERVE ROOT COMPRESSION RESULTING IN MOTOR WEAKNESS AND PAIN
 Cox Technic Case Report #100 published at www.coxtechnic.com (sent October 2011 on 10/11/11 ) 1 Case Report: CASE REPORT OF FACET ARTHROPATHY INDUCED NERVE ROOT COMPRESSION RESULTING IN MOTOR WEAKNESS
Cox Technic Case Report #100 published at www.coxtechnic.com (sent October 2011 on 10/11/11 ) 1 Case Report: CASE REPORT OF FACET ARTHROPATHY INDUCED NERVE ROOT COMPRESSION RESULTING IN MOTOR WEAKNESS
Rehabilitation Protocol: Arthroscopic Anterior Capsulolabral Repair of the Shoulder - Bankart Repair Rehabilitation Guidelines
 Rehabilitation Protocol: Arthroscopic Anterior Capsulolabral Repair of the Shoulder - Bankart Repair Rehabilitation Guidelines Department of Orthopaedic Surgery Lahey Hospital & Medical Center, Burlington
Rehabilitation Protocol: Arthroscopic Anterior Capsulolabral Repair of the Shoulder - Bankart Repair Rehabilitation Guidelines Department of Orthopaedic Surgery Lahey Hospital & Medical Center, Burlington
Planning the Objective Exam. Objective Examination of the Cervical Spine. Clearing Tests. Observation. Functional Demonstration.
 Objective Examination of the Cervical Spine Taking the complaint and identifying the damaged structure Planning the Objective Exam With a clear picture from the subjective exam, the objective exam should
Objective Examination of the Cervical Spine Taking the complaint and identifying the damaged structure Planning the Objective Exam With a clear picture from the subjective exam, the objective exam should
Rehabilitation Protocol: Massive Rotator Cuff Tear Repair
 Rehabilitation Protocol: Massive Rotator Cuff Tear Repair Department of Orthopaedic Surgery Lahey Hospital & Medical Center, Burlington 781-744-8650 Lahey Outpatient Center, Lexington 781-372-7020 Lahey
Rehabilitation Protocol: Massive Rotator Cuff Tear Repair Department of Orthopaedic Surgery Lahey Hospital & Medical Center, Burlington 781-744-8650 Lahey Outpatient Center, Lexington 781-372-7020 Lahey
Shoulder Arthroscopy with Posterior Labral Repair Rehabilitation Protocol
 General Notes: As tolerated should be understood to include with safety for the surgical procedure; a sudden increase in pain, swelling, or other undesirable factors are indicators that you are doing too
General Notes: As tolerated should be understood to include with safety for the surgical procedure; a sudden increase in pain, swelling, or other undesirable factors are indicators that you are doing too
Why choose Ottauquechee PT
 Why does your back hurt? Low back pain is one of the most common patient complaints affecting 80% of adults at some point in their lives. Generally the source of pain is in the spine and/or its supporting
Why does your back hurt? Low back pain is one of the most common patient complaints affecting 80% of adults at some point in their lives. Generally the source of pain is in the spine and/or its supporting
Arthroscopic Rotator Cuff Repair Protocol:
 Arthroscopic Rotator Cuff Repair Protocol: The intent of this protocol is to provide the therapist and patient with guidelines for the post-operative rehabilitation course after arthroscopic SLAP repair.
Arthroscopic Rotator Cuff Repair Protocol: The intent of this protocol is to provide the therapist and patient with guidelines for the post-operative rehabilitation course after arthroscopic SLAP repair.
A Patient s Guide to Ulnar Nerve Entrapment at the Wrist (Guyon s Canal Syndrome)
") A Patient s Guide to Ulnar Nerve Entrapment at the Wrist (Guyon s Canal Syndrome) Introduction The ulnar nerve is often called the funny bone at the elbow. However, there is little funny about injury to
A Patient s Guide to Ulnar Nerve Entrapment at the Wrist (Guyon s Canal Syndrome) Introduction The ulnar nerve is often called the funny bone at the elbow. However, there is little funny about injury to
WRITING SUB-TEST TEST BOOKLET
 PHYSAMPLE01 WRITING SUB-TEST TEST BOOKLET INSTRUCTIONS TO CANDIDATES You must write your answer for the Writing sub-test in the Writing Answer Booklet. You must NOT remove OET material from the test room.
PHYSAMPLE01 WRITING SUB-TEST TEST BOOKLET INSTRUCTIONS TO CANDIDATES You must write your answer for the Writing sub-test in the Writing Answer Booklet. You must NOT remove OET material from the test room.
Breakout Session #7: Manual therapy for shoulder pain and limited mobility
 Northwestern University Feinberg School of Medicine Breakout Session #7: Manual therapy for shoulder pain and limited mobility @Amee_S Objectives 1. Demonstrate the examination procedures and describe
Northwestern University Feinberg School of Medicine Breakout Session #7: Manual therapy for shoulder pain and limited mobility @Amee_S Objectives 1. Demonstrate the examination procedures and describe
Arthroscopic Anterior Stabilization Rehab
 Arthroscopic Anterior Stabilization Rehab Phase I (0-3weeks) Sling immobilization-md directed Codmans/Pendulum exercises Wrist/Elbow ROM Gripping exercises FF-AAROM (supine)-limit to 90 o ER to 0 o Sub
Arthroscopic Anterior Stabilization Rehab Phase I (0-3weeks) Sling immobilization-md directed Codmans/Pendulum exercises Wrist/Elbow ROM Gripping exercises FF-AAROM (supine)-limit to 90 o ER to 0 o Sub
FILED: RICHMOND COUNTY CLERK 01/17/ :45 PM INDEX NO /2015 NYSCEF DOC. NO. 65 RECEIVED NYSCEF: 01/17/2019
 BROOKLYN, N.Y. 11234 Kalant & Roytblat, PLLC January 3, 2019 9131 Queens Blyd., Ste. 313 Elmhurst, NY 11373 Attention: Alexander Roytblat, Esq. Re: Eran Taussi Date of Accident: January 30, 2014 Dear Mr.
BROOKLYN, N.Y. 11234 Kalant & Roytblat, PLLC January 3, 2019 9131 Queens Blyd., Ste. 313 Elmhurst, NY 11373 Attention: Alexander Roytblat, Esq. Re: Eran Taussi Date of Accident: January 30, 2014 Dear Mr.
Total Shoulder Arthroplasty / Hemiarthroplasty Protocol
 Adam N. Whatley, M.D. 6550 Main St., STE. 2300 Zachary, LA 70791 Phone(225)658-1808 Fax(225)658-5299 Total Shoulder Arthroplasty / Hemiarthroplasty Protocol The intent of this protocol is to provide the
Adam N. Whatley, M.D. 6550 Main St., STE. 2300 Zachary, LA 70791 Phone(225)658-1808 Fax(225)658-5299 Total Shoulder Arthroplasty / Hemiarthroplasty Protocol The intent of this protocol is to provide the