Assessment & Management of Executive Dysfunction in an Occupational Context
|
|
|
- Holly Higgins
- 5 years ago
- Views:
Transcription
 Senior Scientist, Rotman Research Institute Associate Professor, Occupational Science & Occupational Therapy, University of Toronto")
1 Assessment & Management of Executive Dysfunction in an Occupational Context Deirdre Dawson, PhD, OT Reg. (Ont.) Senior Scientist, Rotman Research Institute Associate Professor, Occupational Science & Occupational Therapy, University of Toronto Ottawa, Ont.: March 1, 2018
2 Disclosures Received and hold research grants to investigating the Multiple Errands Test and the Cognitive Orientation to daily Occupational Performance: The CO-OP Approach TM Received income from published book on the CO-OP Approach TM CO-OP Certified Instructor Multiple Errands Test Instructor
3 Schedule Content 8:30 Introductions Overview of 3 Days Goals & Objectives 9:00 Foundational concepts, models and current cognitive neuroscience of executive function 9:30 Considerations for choosing assessments; Overview of Assessment Options ~ 10:30 BREAK 10:45 Multiple Errands Test: Overview, Scoring, Interpretation, MET-Home 11:45 Assessment Wrap-Up Take-home messages Check-in Regarding Objectives related to Asessment 12:00 LUNCH 1:00 Principles for occupational rehabilitation Evidence-based recommendations for rehabilitation of executive function Decision algorithm Overview of Management Approaches 2:00 Introduction to the CO-OP Approach TM & Discussion of active ingredients 2:30 BREAK 3:45 Application to participants clinical cases Check-in regarding Objectives related to Intervention Final questions / comments Wrap-up 4:30 End of Day
4 Learning Objectives By the end of this workshop, attending OTs will: Ø Have knowledge of foundational concepts and current cognitive neuroscience thinking about executive functions; Ø Be able to identify key considerations in choosing assessments including the differences between differences between occupational performance and cognitive assessment; Ø Be able to apply algorithms related to choosing assessments and rehabilitation approaches; Ø Have familiarity with a repertoire of evidence-based approaches and how these might be tailored to clients in different practice settings.
5 Foundational Concepts Executive Dysfunction through an Occupational Lens
6 Occupational Performance the ability to choose, organize and satisfactorily perform meaningful occupations (p. 30, Townsend, 1997)
 assessing &")



7 What are we / should we be (as OTs) assessing & treating? Impairment Level Activity / Task Level Everyday life Participation / Occupational Performance International Classification of Functioning, Disability & Health, WHO, 2000
8 Principles for Using an Occupational Approach 1. Occupational performance arises from a complex interaction of elements; 2. Contextual factors are accounted for in the context within which the occupation is performed; 3. Using an occupational approach requires a sound theoretical understanding of cognition; 4. Observing occupation allows clinicians to identify barriers and facilitators to performance.

9 Foundational Concepts Executive Function
10 Characteristics of Executive Functions Complex processes that integrate and are superordinate over lower-level processes Require cognitive effort Mediated through multiple networks involving frontal lobes, particularly the pre-frontal cortex and brain networks involving frontal and parietal cortices, and subcortical structures including the cerebellum No consensus on one set of domains
11 Theories of Executive Dysfunction Mesulam: the default mode Stuss: attentional fractionation
12 The default mode * (Mesulam, 2002) Actions are driven by immediate gratification and / or environmental triggers Behaviour is poorly modulated by context / experience There is a need for a buffer between stimulus and action To overcome this, executive control needs to be reestablished: ü Use of bottom-up strategies (externally-based cueing systems) ü Use of top-down approaches (internally driven, metacognitive strategies)
13 Think of a situation in which You need to place a buffer between a stimulus and an action
14 Frontal Functions Terms such as EF, the dysexecutive syndrome, the supervisory system, and frontal lobe functions are challenging to define and measure. The following schema divides what has been loosely termed executive functions into four more clearly defined and circumscribed domains that follow anatomy and evolutionary development: (1) executive cognitive functions, (2) behavioral self-regulatory functions, (3) activation regulating functions, (4) metacognitive processes. Cicerone, Levin, Malec, Stuss & Wyte, 2006, J Cog Neurosci

15 Energization Process of initiation and sustaining any response Linked to superior medial cortex Observed deficits may include; Slower response time Failure to sustain attention Dynamic relationship between sustained attention & inhibition Involves arousal and goal representation 15 Energization SUPERIOR MEDIAL Stuss, 2006, JINS
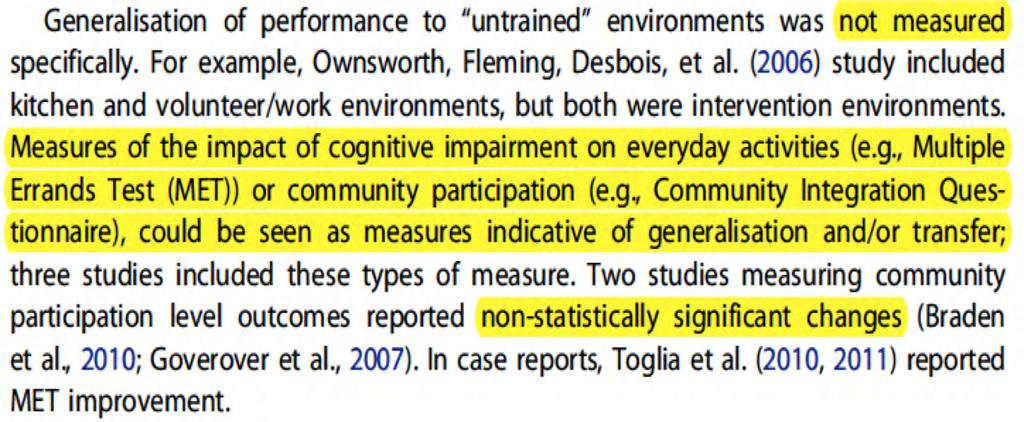
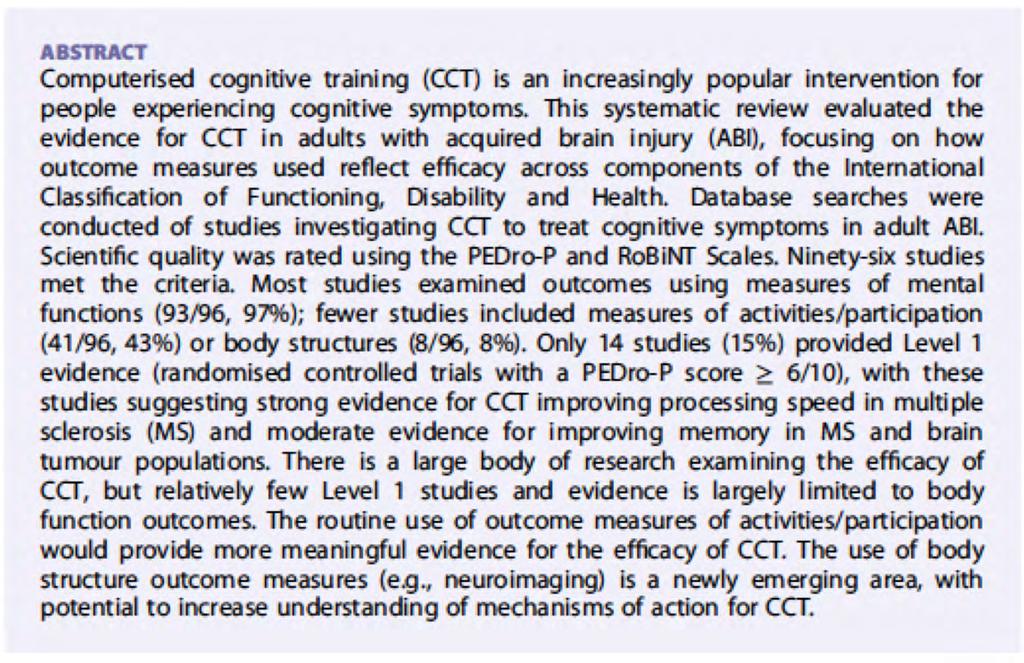
![Executive Cognitive Functions Control and direction of lower level cognitive functions Monitoring (right lateral prefrontal cortex [PFC]) Task setting (left lateral PFC)](/docs-images/93/112738181/images/16-3.jpg "Involves skills such as goal selection, flexibility, impulse control, planning, organisation and decision making LEFT LATERAL Task Setting RIGHT LATERAL 16 Stuss, 2006, JINS")
16 Executive Cognitive Functions Control and direction of lower level cognitive functions Monitoring (right lateral prefrontal cortex [PFC]) Task setting (left lateral PFC) Involves skills such as goal selection, flexibility, impulse control, planning, organisation and decision making LEFT LATERAL Task Setting RIGHT LATERAL 16 Stuss, 2006, JINS Monitoring
17 Self-Regulation Self-regulation of behaviour Automatic routine situations vs. novel and complex situations Linked to ventral medial PFC Involves planning, self-reflection, risk vs. reward assessment, inhibition 17 Stuss, 2006, JINS

18 Executive Attention Networks (Dopamine & Seratonin) Competing theories exist Commonalities - Widespread cortical connections - Anterior cingulate cortex - Prefrontal cortex - Dorsal and ventral - Medial - Orbitofrontal areas
19 Executive Attention Networks (dopamine & seratonin) - Allows for high level attentional tasks selection, alternating, dual-tasking - Involved in regulation of thoughts, feelings and behaviours - Includes processes for detection, inhibition, switching & conflict processing all important for error detection and correction - Allows for trial by trial adjustments and maintenance of a stable background for whole task performance
20 Metacognition Awareness of one s thought processes Integration of energization, emotional or motivational information and executive skills Self-awareness, personality, social cognition Linked to frontal poles 20 Stuss, 2006, JINS



21 Functions of the Frontal Lobes: Relation to Executive Functioning (Stuss, 2011)
22 Foundational Concepts Executive Function & Memory


23 C /figure/F1/
24 A Proposed Framework 1. Energization & Initiation 2. Fluency & flexibility 3. Organization 4. Control 5. Decision Making & Problem Solving 6. Meta-cognition
25 Energization & Initiation ENERGIZATION The process of initiating and sustaining a response.
26 Fluency & Flexibility WORKING MEMORY (verbal & non-verbal) COGNITIVE FLEXIBILITY TASK SWITCHING SET-SHIFTING Limited capacity memory held on line for manipulation Changing perspective spatially or interpersonally. Theorized to rely on inhibition, attention and working memory (inhibiting one stimuli, shifting one s attention to a new stimulus and re-focusing. Switching between tasks or sets such as on the Stroop task.
27 TASK SETTING: Includes: goal-setting goal formation plan formation Organization Forming a connection between a stimulus and response (if-then logic) such that a criterion for response is established. Determining a response is needed. PLANNING Making and executing plans in the sequence needed to achieve a goal.
28 INHIBITORY CONTROL Attentional Control Volitional attention Higher-level attention Control Suppression of an automatic, habitual or impulsive response to an environmental stimulus, internal thought or emotion in order to make a more relevant response TASK MONITORING Keeping track of performance over time to avoid making errors. SELF-REGULATION Top down control of attention toward goalrelevant information Suppression of ruminative thoughts Inhibition of unwanted affect, desires, craving
29 DECISION MAKING Decision Making & divergent and convergent reasoning PROBLEM SOLVING involves cognitive flexibility planning and organization decision making working memory Problem-Solving Generating multiple solutions to a problem (divergent) Considering multiple factors and deriving a solution (convergent) Identifying the problem, searching for a solution, determining what the solution will involve, choosing and executing the solution.
30 Meta-cognition & Self-Awareness SELF-AWARENESS Ability to recognize impairments, understand their functional consequences and anticipate possible future difficulties related to these META-COGNITION Includes self-awareness Ability to think about one s thinking Integrates all other executive functions
31 Assessment
32 Objectives By the end of the assessment section, attendees will be able to: Understand how to select an assessment for a particular therapeutic context; Identify a variety of assessment options for evaluating cognitive impairments and their effects in the context of everyday activities; Consider three specific assessments for use in clinical practice.
33 Overall Process I: Should a cognitive assessment be undertaken? 1. Has client or decision maker consented? 2. Who is asking for the information? What information is required? 3. What is the benefit of determining whether there is cognitive impairment? 4. Has any cognitive testing been done by others? What were the findings? Is further testing needed / required? 5. Are there occupational performance difficulties? If not, why is OT involved? 6. Are there other factors that could be influencing cognition e.g., sleep, mental health, medication, medical history, substance abuse, other, timing?
34 CSBPR 2015 (Eskes et al., 2015) 1. All patients with clinically evident stroke or TIA should be considered at risk for vascular cognitive impairment (Evidence Level A); 2. Patients with stroke and TIA should be considered for screening for VCI using a validated screening tool such as the MoCA (Evidence Level C); 3. Patients with demonstrate cognitive impairments when screened should be managed by healthcare professionals with expertise in the assessment and management of neurocognitive functioning. If required a referral could be made to an appropriate cognitive specialist (Evidence Level C).
35 After deciding a cognitive assessment should be undertaken II: Planning & Preparation 1. What is the assessment purpose? Discharge planning? Treatment planning? Returning to work / school? 2. What kind of assessment is client able to participate in? Consider level of awareness, physical tolerance, language, motor skills, education. 3. What are the pragmatic issues? Availability of space, time, assessment materials Personal expertise / training 4. What background information is available and relevant? Past medical history Information on client s cognitive and functional status from other assessments, team members, family
36 III: Initial Interview 1. What are the client s occupational difficulties and priorities? Canadian Occupational Performance Measure Activity Card Sort Pre-morbid / current daily log Occupational Repertoire 2. Is there a need to measure capacity and/or performance? 3. Is the goal to identify a problem and/or measure change after intervention?
37 Process of choosing an assessment 1. Determining whether a cognitive assessment should be done; 2. Planning and preparing for the assessment; 3. Undertaking the initial interview and occupational needs assessment; 4. Decision point

38 * If more in-depth assessment required after doing step 4 proceed to step 5. IV: Decision Point
39 Cognitive Assessments cognitive, affective impairments STROKE Real-world measures ICF, WHO, 2000
40 IV: Screening Assessment Screening at activity / task performance / occupational level Unstructured observation Standardized tools (e.g., Cognitive Performance Test) Screening at the impairment level Quick Screen (e.g., MoCA) Profile Screen (e.g., LOTCA) IV: Decision Point V: In-depth Assessment In-depth assessment at level of activity / task performance / occupational level Unstructured observation Structured observation (e.g., Multiple Errands Test) Standardized assessment (e.g., ADL/IADL Profile) In-depth assessment at the impairment level Standardized cognitive assessments used by OT (e.g., BADS) Refer to neuropsychologist Questionnaires (self / other report) home-made Standardized (e.g., BRIEF-A; DEX)
41 Principles for Assessment with an Occupational Lens* The assessment should: 1. Be developed from the basis of theory. 2. Focus on the effects of the executive function impairment on occupational performance; 3. Provide the opportunity to understand the effects of real-world contextualization on performance; 4. Allow for observation of clients strategy use and determination of whether generated strategies assist with test performance. Dawson, Bottari, Nalder & Hébert. (forthcoming). Assessment and management of executive dysfunction through an occupational lens.
42 If your job is to assess at the performance level also consider the following 1. Does the client have the necessary executive function to manage the occupational demands of their current situation? 2. Does the client have the necessary executive function to allow them to manage the occupational demands of novel or non-routine situations? 3. Are the strategies the client is using moving them towards attaining their desired occupational performance goal and/ or is assistance needed? 4. If the client does not have the necessary executive function, where is performance breaking down? 5. If assistance is needed, what type of assistance best optimizes the clients abilities?
43 Informal Assessment Observation in naturalistic settings Pay attention to the amount of scaffolding (cues, prompts, structure) required for client to initiate and sustain action Useful for informally identifying a problem and guiding treatment.
.")
44 Useful resources for choosing an assessment 1. The Occupational Therapy Cognitive Assessment Inventory (04/2014). Available at nventory.pdf


45 2. Review Papers & Texts
46 3. Professionally developed and mediated websites Funding: Heart & Stroke Foundation Canadian Partnership for Stroke Recovery Funding: Heart & Stroke Foundation Canadian Partnership for Stroke Recovery Funding: Shirley Ryan Ability Lab Funding: Ontario Neurotrauma Foundation Funding: National Institute on Disability, Independent Living and Rehabilitation Research: Santa Clara Valley Medical Center
47 17 Performance-based Assessments 1. ADL Profile 10. Naturalistic Action Test 2. Behavioural Assessment of the Dysexecutive Syndrome 11. Observed Tasks of daily living-revised 3. Complex Task Performance Assessment 12. Rabideau Kitchen Evaluation 4. Cooking Task 13. Virtual action planning supermarket 5. Executive Function Performance Test* 14. Assessment of Motor & Process Skills 6. Executive Secretarial Task 15. Functional Assessment of Verbal Reasoning and Executive Strategies 7. Making a cake 16. Kettle Test 8. Multiple Errands Test* 17. Virtual Environment Technology 9. Virtual Multiple Errands Test *Strongest psychometric data
48 Comments about specific assessments Of 17 performance tests reviewed (Poulin et al., 2013), strongest reliability and validity had been demonstrated for: 1. Executive Function Performance Test (EFPT) 2. Multiple Errands Test (MET)
49 Executive Function Performance Test Manual & Test Available at: Purpose: To determine: which executive functions are impaired An individual s capacity for independent functioning The amount of assistance necessary for task completion. Example of Adminstration: Description: 5 tasks: (hand washing), simple cooking, telephone use, medication management, bill payment each scored on initiation, execution, organization, sequencing, judgement & safety, completion

50 I want you to make oatmeal. Here is an enlarged version of the instructions. Follows these directions and when you are done put the oatmeal in the bowl. The items you need are in the box.
 4 raters, 17 patients acute (lowest agreement on paying bills) Internal Consistency: Excellent (Baum et al.")
51 EFPT Psychometric Data in Stroke Reliability: Test-retest: Unknown Inter-rater: Moderate to Excellent Excellent: (Baum et al., 2008) 3 raters, 10 patients chronic Moderate (Cederfeldt et al., 2015) 4 raters, 17 patients acute (lowest agreement on paying bills) Internal Consistency: Excellent (Baum et al., 2008) Validity: (Discriminative): Significant but effect sizes are not reported
52 Baum et al., 2008 Effect sizes calculated post-hoc Control - Mild Stroke: Cohen s d=1.03 Control-Moderate Stroke Cohen s d=5.48
53 EFPT Psychometric Data in Stroke Validity: (Baum et al., 2008; Cederfelt et al., 2011; Wolf et al., 2010) Concurrent: moderate relationships with working memory, verbal fluency, attention (r> 0.39) in those with chronic stroke moderate to large relationships with Delis-Kaplan Executive Function System (r= to ) in those with mild, chronic stroke Moderate to large relationships with FIM scores (r= ) Moderate relationships with AMPS process scores (r= 0.65)
 Poncet et al., 2017, p.")
54 Formal Assessment Multiple possibilities (see Poncet et al., 2017, Neuropsych Rehabil) Poncet et al., 2017, p. 630


55 The Multiple Errands Test
56 Objectives By the end of this section of the workshop, participants will have: Gained familiarity with the development and construction of the Multiple Errands Test (MET); Understand the administration and scoring of the MET; Gained knowledge about psychometric properties of the MET; Considered the clinical utility of the MET. 2
57 Origins of the MET Frontal lobe lesions can produce a gross effect in the performance of everyday life activities other than the most routine, even though neuropsychological tests suggest that the cognitive changes that have occurred are at most minor (Shallice & Burgess, 1991, p. 727) NEED: a quantifiable analogue of open-ended multiple goal situations in a setting where minor unforeseen events can occur RESPONSE: Multiple Errands Test 3

58 Knight, Alderman, & Burgess, Hospital Version,

59 Knight, Alderman, & Burgess, Hospital Version,
60 Some of the Published Versions Natural environment 1. Knight et al., Multiple Errands Test for use in hospital settings. Neuropsych Rehab. 2. Alderman et al., 2003 simplified Multiple Errands shopping Test. J Intl Neuropsych Soc. 3. Dawson et al., Multiple Errands Test: Baycrest version. Arch Phys Med & Rehab. 4. Maeir et al., Ecological validity of the 1. Multiple Rand Errands et Test. al., OTJR. 2009, Virtual MET, Revised, Neuropsych AJOT. Rehab 5. Morrison et al., Multiple Errands Test- 6. Clark et al., 2015 Revised Baycrest Multiple Errands Test, Neuropsych Rehab. 7. Lancely, S. (2015). A new approach to the assessment of drivers: Applying the MET for use in a simple parking exercise. BJOT. 8. Burns et al. (in press). MET-HOME. Neuropsych Rehab & AJOT. Virtual environment 1. Parsons et al., (2008). Assessment of Executive Functioning Using Virtual Reality: Virtual Environment Grocery Store. Gerontechnology. 2. Rand et al., 2009, Virtual MET. Neuropsych Rehab. 3. Raspelli et al., 2011, Neuro VR MET. Stud Health Technol Inform. 4. Logie et al., Edinburgh VET. Mem Cognit. 5. Jovanovski et al., 2012, Multitasking in the City. Appl Neuropsych: Adult. 6. And others 6
61 The MET and Ecological Validity Representativeness (verisimilitude) ü corresponds to the form and context of the everyday environment üreflects the cognitive processes necessary to complete the everyday activity; Generalisability (veridicality) ücorresponds to and/or predicts realworld performance. 7
62 MET s & EFPT s characteristics in relation to principles of assessment Principle MET EFPT 1. Based on theory Based on the Supervisory? Not stated Attentional System 2. Focuses on the effects of executive dysfunction on occupational performance Tasks and rules are drawn from everyday life activities. -- To some extent, controlled test administration and environment 3. Real-world contextualization Versions have been developed for hospitals, shopping malls, home. -- Simulated tasks and environment 4. Allows for observation of Although no structure --To some extent but cues clients strategy use. for observation has been published. provided to ensure success. 8

63 Scoring the MET: Recommended Workflow During performance of the MET Participants / clients are observed (and recorded if possible) by therapist Therapist makes thorough notes on observations An additional person may video-record Scoring specific items occurs after performance 9
64 Administering the MET Refer to: 10
65 Preliminary Scoring: Task completion and Rule Adherence 1. Tasks completed accurately, tasks completed partially, tasks omitted. 2. Rule breaks: where a specified rule is broken. 11
66 12 Interruption task Please pick up a Baycrest Matters flyer and give it to your experimenter at the end of the task.
67 13
68 14

69 What about strategies used? 15
70
71 Considerations regarding strategy use* 1. Is the strategy directed internally (towards the person) or externally (towards the task or environment? 2. Is the strategy being used to enhance skill or performance, to cope with a challenge and/or to self-regulate behaviour? 3. Is the strategy being used before, during or after the activity? 4. Is the strategy specific to a particular task or domain and/or does it have the potential to be used in a more general manner? * Adopted from Toglia et al.,

72 Strategy Selection Process* 18
73 What is standardization? Any test that: 1. Requires all test takers to answer the same questions or selection of questions from a common bank 2. Requires all testees to take the test in the same way; 3. Is scored in a standard or consistent manner. 19
74 Psychometric Evidence 20
75 Studies Reviewed & Samples Knight et al n=20 pts; -12 TBI, 5 CVA, 3 others; - all severe 20 hospital staff matched on age, gender, IQ Alderman et al., 2003 n=50 pts, 36 inpts; - 39 TBI, 9 CVA; - 90% severe 46 hospital staff and associates Dawson et al., 2009 n=27 community dwelling; -13 TBI, 14 CVA; ~ 60% modsevere 25 friends, family, volunteers individually matched age, educ, gender Maier et al., 2011 n=30 rehab pts; - 19 CVA, 8 TBI, 3 others Morrison et al., 2013 n=25 pts; - all acute mild CVA n/a n=21 volunteers, matched 21 Clark et al., 2015 n=15 community dwelling; - all ABI / CVA with ED on neuropsych testing 16 friends, family, volunteers individually matched on age, educ, gender
76 Psychometrics Reliability Internal consistency: Cronbach s α = 0.77, MET-HV (Knight et al., 2002) Inter-rater reliability: ICC , MET-HV & BMET (Knight et al., 2002; Dawson et al., 2009; Morrison et al., 2013) Test-retest reliability: significant, strong correlations between two versions (r= ) (Clark et al., 2015) Responsivity No published data available 22
77 Validity Concurrent executive dysfunction: Associations between sub-scores and perseverative errors on MCST, BADS (profile score & Zoo map), DEX, and EFPT: r= (Alderman et al., 2003; Knight et al., 2002; Dawson et al., 2009; Morrison et al., 2013; Rand et al., 2009) Concurrent everyday life: Associations between rule breaks and errors and Sickness Impact Profile, MPAI participation index, Assessment of Motor and Process Skills (AMPS) and IADL: (Dawson et al., 2009; Rand et al., 2013) Negative associations between frequency of strategy use and AMPS: -.46 to-.53 (Dawson et al., in prep) Predictive everyday life at 3 mos post-d/c associations between rule break, errors, inefficiencies and MPAI Participant Index, r= (Maier et al., 2011) 23
78 Sensitivity A test with 100% sensitivity correctly identifies all of the people with the problem. Using a cut-off of 7 or more overall errors: ² Clark et al. (2015): 73.3% sensitivity (11/15 participants made 7+ errors) (Baycrest MET Version A) ² Knight et al. (2002): 85% sensitivity (17/20 participants made 7+ errors) *Sensitivity of breast screening ranges from 75% to 90%. 24
79 Specificity A test with 100% specificity correctly identifies all people without the problem. Using a cut-off of 7 or more overall errors: ² Clark et al. (2015): 81.3% specificity (3/16 controls made 7+ errors) (Baycrest MET Version A) ² Knight et al. (2002): 95% specificity (1/20 controls made 7+errors) *Specificity of breast screening ranges from 90 to 95%. 25
80 In summary The MET is a highly reliable, ecologically valid assessment used to characterize how executive function difficulties influence performance in everyday life. Abnormal performance is suggested by 7 or more errors. Ms. XX had 14 errors suggesting her executive function difficulties are impacting in a significantly negative way on her everyday life. Examples of this are. 26

81 Score Interpretation & Clinical Reasoning: 27
82 MET Data which Guides Clinical Reasoning Overall consistency & organisation of performance 1. Functional skills important in everyday life 2. Observations of executive functions 3. Quantitative MET data 4. Strategy use (Bottari et al., 2014; Nalder et al., 2015) 28
83 1. Functional Skills for Everyday Life Money management & calculations Social interactions Navigational skills Ability to work under pressure Finding information (Bottari et al., 2014; Nalder et al., 2015) 29
 30")
84 Clinical Reasoning & Error Interpretation Qualitative analyses revealed 8 clinical signs: 1. Excessive time to execute task 2. Task omitted 3. Atypical behaviour (e.g., forgets bag and doesn't retrieve it) 4. Rule broken 5. Task completed only partially 6. Request for help 7. Interpretation failure 8. Inefficiency (Bottari & Dawson, 2011; Bottari, Iliopoulos, Shun, & Dawson, 2014) 30
85 When Interpreting Errors, Draw On... Scoring templates & test structure Psychometric evidence sensitivity & specificity Theories of EF Clinical experience and familiarity with the MET Debrief interview Referring back to client s therapy goals 31
. Development, Reliability, and Validity of the MET-Home. AJOT, 73(3).")
86 The MET-Home Burns*, S.P., Dawson, D.R., et al. (2018). Inhome contextual reality: A qualitative analysis using the Multiple-Errands Test Home Version (MET-Home). Neuropsychological Rehabilitation, Online first. Burns*, S.P., Dawson, D.R., et al. (in press). Development, Reliability, and Validity of the MET-Home. AJOT, 73(3). *sburns3@twu.edu) 32
87 33



88 Questions about the MET? 34
89 Workshop Part II Evidence-based Intervention
90 Objectives Participants in Part II of the workshop will: Know the principles of occupationally-focused intervention; Be able to follow and algorithm to assist with treatment decisions; Gain several new ideas / techniques to add to their intervention toolkit and understand the evidence supporting this technique; Understand the key elements of the CO-OP Approach TM and their application in clinical practice; Apply at least one new technique to a personal clinical problem.
91 Principles of Intervention The primary goal of therapy is to enable occupation, thus to focus on task acquisition (or improvement) and goal attainment. Thus, occupational goals must be identified. Clients should be provided with the resources that are necessary to support the maintenance of gains made in therapy. Whenever possible, intervention strategies should be selected that promote generalization and transfer of learning to situations and tasks that have not been included in the treatment context. Clients should be provided with the necessary resources to be able to meet new occupational challenges following their rehabilitation.


92 Criteria for Successful Rehabilitation ª clinically significant improvements in performance of and participation in everyday roles and activities; ª maintenance of gains over time; ª generalization of effects to untrained roles and activities.

93 Classifying interventions in relation to transfer distance Wilson, Giles & Baxter, 2014, Brain Injury
94 Stages of (Motor) Learning (Fitts & Posner, 1967; Magill, 1998) Cognitive cognition guides behavior individual gets the general idea of the movement Individual reflects on prior knowledge of task and attends to information from the environment



95 Cognitive phase I have to turn my head to check my blind spot when I change lanes At a curve in the road, I have to brake as I start into the curve and halfway through the turn, I have to begin accelerating Hand at 2 o clock, hand at 10 o clock 7 Look in front To stop, I have to brake gradually


96 Cognitive stage of transfer learning the plans
97 Cognitive Stages of Motor Learning Associative (Fitts & Posner; 1967; Magill, 1998) individual learns to perform movement with some degree of accuracy individual uses feedback to correct movement patterns Autonomous skill is performed fluently and automatically

98 I have to slow down at the nets exit Associative The Associative and Autonomous Stages I have to take the highway to get to the theatre Autonomous 10

99 The Associative and Autonomous Stages of Motor Learning The Plans Associative I m in the tub I didn t fall. Autonomous I m going to have a bath. Polatajko and Mandich 11
100 Stage of Treatment: Acquisition Application Adaptation Goals: Ensure objectives are clear; Connect to prior knowledge where possible and relevant; Introduce new knowledge; Provide cues, guidance, opportunity for practice. Facilitate improved performance and independence; Promote internalization of cues & strategies; Provide opportunities for generalization of skills from the structured therapy setting to clients realworld environments (home, community, work); Promote transfer of underlying strategies to new occupational performance problems.
101 Class I/Ia Class II Class III Levels of Evidence Studies with well designed, prospective, randomized controlled trials Prospective, nonrandomized cohort studies; or clinical series with well-designed controls that permitted between subject comparisons of treatment conditions; well designed single-case experimental design Clinical series w/o concurrent controls, or studies with results from 1 or more single cases w/ appropriate methods
102 Practice Standard / Level A Recommendation Practice Guideline/ Level B Recommendation Practice Option / Level C Recommendation LEVELS OF EVIDENCE (Haskin et al., 2012; INCOG, 2014) Based on at least 1 well-designed class I study with an adequate sample, with support from class II/III evidence; providing substantive evidence to support a recommendation. Based on 1 or more class I studies with methodologic limitations (e.g., small sample), or well-designed class II studies. Based on class II or class III studies that directly address the efficacy of a treatment; for Level C, recommendations supported by expert opinion.

103 CSBPR Levels of Evidence
104 Selected Sources of Evidence Eskes, G. A. (2015). Canadian stroke best practice recommendations: Mood, cognition and fatigue: Following stroke practice guidelines update International Journal of Stroke, 10(7), Gillen, G. et al. (2015). Effectiveness of interventions to improve occupational performance in people with cognitive impairments after stroke: A systematic review. AJOT, 69 (1), Haskins, et al., (2012). Cognitive rehabilitation manual: Translating evidence-based recommendations into practice. Reston, Virginia: ACRM. (TBI & Stroke) INCOG guidelines for cognitive rehabilitation following traumatic brain injury (2014). Journal of Head Trauma Rehabilitation, 29 (4). Poulin, V., Korner-Bitensky, N., Dawson, D., & Bherer, L. (2012). Efficacy of executive function interventions after stroke: A systematic review. Topics in Stroke Rehabilitation, 19(2), Radomski, M. et al. (2016). Effectiveness of interventions to address cognitive impairments and improve occupational performance after traumatic brain injury: A systematic review. AJOT, 70(3), Stroke best practice recommendations.
105 Practice Standard: Level A Evidence Strategies to improve the capacity to analyze and synthesize information should be used with adults with TBI who have impaired reasoning skills (problem-solving training). Direct corrective feedback should be used with adults with impaired self-awareness should be delivered in therapeutic, multi-contextual program.
106 Practice Guideline: Level B Evidence Group-based interventions may be considered for remediation of executive and problem-solving deficits
107 CSBP Recommendations (Eskes et al., 2015) Interventions for cognitive impairment should be tailored a) Goals should be patient-centred (Level B) b) Goals & interventions should take into account the cognitive and communication profile (Level C) c) Interventions should be individualized, based on best available evidence and have the long-term goal to facilitate resumption of desired activities (e.g., leisure, financial management); d) Compensation strategy training should focus on teaching strategies to manage impairments and is often directed at specific activity limitations to promote independence (Level B); e) It is reasonable to treat attention impairments with computerized skill training under the supervision of a therapist (Level B).
108 Can they understand the parts of the approach Is something is happening, does the client recognize it, and do something about it? Can the person generalize and transfer? What supports are needed in order for people use a problem-solving approach We are particularly concerned about online awareness in the moment & anticipatory Haskins et al., 2012 if awareness if very poor might need some experiential stuff second question would be goal setting or relating to everyday tasks so have new experience of themselves With an occupational focus. Create supportive environment, environmental supports NB: Awareness is an ongoing issue so have to keep coming back to this.
109 Self-awareness may ultimately be understood as the result of a complex combination of psychological and neuropsychological factors, which are affected by the (pathology) and by the individual s personality and previous experiences (Hart et al., JHTR, 2005)
110 Crosson s Model (1989) Anticipatory Emergent Intellectual
111 Intervene when. Ownsworth & Clare, The likelihood of heightened emotional distress is relatively low* AD represent a probable barrier to client's own goals 3. AD pose a significant safety risk which cannot managed effectively in other ways 4. Resources are available closely monitoring the individual's emotional well-being and coping reactions. *Rarely measured: Engel, Chui, Goverover & Dawson, 2017, Neuropsych Rehabil
112 Addressing Deficits in Awareness (Fleming & Ownsworth, 2006) Build a collaborative alliance Select personally relevant tasks engage in goal setting Structure opportunities to identify errors and correct performance Compare performance to the person s own expectations (predict/perform) Provide clear & tailored feedback Engage in goal setting
113 Awareness interventions that optimize occupational performance outcomes Engel, Chui, Goverover & Dawson, 2017, Neuropsych Rehab
114 But
115 1. Therapist introduces task Predict-Perform 2. Clients asked to Define performance goals including task completion time Predict performance Anticipate and pre-plan for errors / obstacles Choose a strategy to circumvent difficulties Assess amount of assistance needed 3. Perform task (experiential participation in everyday life task) 4. Self-estimate performance / self-evaluate 5. Discussion / feedback with therapist 6. Client records the experience including tips for success the next time
116 Perceive Predict - Perform Paradigm Perceive Predict Perform (Ap)Prove
117 What kind of feedback? Schmidt, Fleming et al. (2013). Neurorehabil & Neural Rep RCT Participants were videotaped doing a meal preparation task four times Pause, prompt, praise feedback throughout Primary outcome was error count during task Feedback session after every meal prep Watched video together and discussed Verbal feedback and discussion only Self-rating of independence on meal prep / experiential feedback
118 Feedback to enhance error awareness (Ownsworth et al., 2006) PAUSE to provide an opportunity for client to self-correct PROMPT - Non-specific: What is happening? - Specific: Check the recipe and find the first ingredient. Put it in the mixing bowl. PRAISE
119 Meta-cognitive & Problem-Solving Training
120 Self-instructional techniques ª Woman with bilateral parietal strokes ª Able to follow single step commands ª Dependent in many ADLs, behaviours were erratic ª Visual cue cards and routine therapy ineffective
121
122 Basic occupational example
123
124 A General Algorithm for Training of Executive Function Awareness (of problem to be addressed or goal to be attained) Anticipation and planning Execution and self-monitoring Self-evaluation
125 Comparison of some rubrics Problem-Solving (Ben-Yishay & Diller, 1983 ) ORIENT to problem FORMULATE problem ANALYZE conditions of problem Formulate STRATEGY & PLAN of Action Choose relevant TACTICS EXECUTE plan COMPARE solution to problem GPDR (Ylvisaker & Feeney, 1998) Goal Plan Do Review Levine 2000, 2011 Stop Define List Learn Do Check CO-OP (Polatajko & Mandich, 2001) Goal Plan Do Check Executive Plus (Gordon et al., 2006) Stop What is the problem? Alternative? Pick, Plan Satisfied? SWAPS
126 Common Elements in Formal Problem-Solving Training Awareness: Is there a problem? Acquisition: Therapist trains patient in the rationale and procedures of the model being used. Application: Client begins to use the model on various tasks in the clinic. Adaptation: Client applies the skills learned in the first two stages to problems and tasks outside the clinic.

127 Manualized Theoretically based primary objective is to train patients to stop ongoing behaviour in order to define goal hierarchies and monitor performance (Levine et al., 2011) 9 modules, 2 hours each STOP, mindfulness, task splitting
128 Evidence for Benefits Has been studied in relation to aging, TBI, stroke, spina bifida, multiple sclerosis, abstinent polysubstance abuse, post-critical patients
129


130 Goal Management Training (Levine et al,. 2011)
131 Task-Specific Training
132 What about those with more severe cognitive impairments? Direct corrective feedback should be used with adults with impaired self-awareness should be delivered in therapeutic, multi-contextual program.
133 The Neurofunctional Approach Giles, 2005; Wilson, Giles & Baxter, Development of therapeutic alliance focus on client s value and goals; 2. Gather and assimilate information to understand client s current functioning in their own environment and to identify their likely responses to intervention; 3. Task Analysis task, client, environment; 4. Reconcile client s goals with available resources divide task into relevant units that can be learned. 5. Create specific skill-retraining programmes incorporating aids and supports as needed including errorless learning during acquisition if necessary; 6. Repetition keeping in mind principles of motor learning; 7. Generalize to client s context and facilitate maintenance of skill consider ongoing supports that will be necessary; 8. Provide feedback to encourage progress and engagement.
134 Vanderploeg et al., 2008, Arch Phys Med Rehab: Benefits Evidence (independence in everyday life) for more severely injured individuals (possibly for older, less education individuals) Rotenberg et al., 2012, Neuropsych Rehabil: Benefits for community dwelling severely impaired adults with chronic stroke
135 Cognitive Process-Specific Training? CSBPR: Direct remediation/cognitive skill training should focus on providing intensive specific training to directly improve the cognitive domain. It can include drill & practice exercises or computer-based tools directed at specific deficits (Level B evidence). Evidence for impact on activity or participation limitations is limited and requires more research (Level C). However, sole reliance on repeated exposure and practice on computer-based tasks without some involvement and intervention by a therapist is not recommended.

136 Recent review results
137 Sigmundsdottir et al., 2016
138 Recent review results

139 CogMed* Study Design Results Akerulnd et al., 2013 Bjorkdahl et al., 2012 Johannson et al., 2012 RCT, PeDRO 5, n-47 RCT, PeDRO 3, n=45 Case series No OP changes Sign but small changes on AMPS Imp on COPM Lundqvist et al., 212 RCT, PeDRO 4, n=21 Imp on satisfaction (COPM) not performance *Bogdanova et al., 2015
140 Exercise


141 Don t forget to exercise! CSBPG: Aerobic exercise can improve EF although evidence for transfer to participation is limited. (Level B)

142 Managing the manifestation of executive dysfunction in everyday life: The CO-OP Approach TM GOAL CHECK PLAN DO
143 Learning objectives At the end of this mini-workshop you will have: 1.An understanding of how and why CO-OP is used with adults and older adults with executive cognitive dysfunction (ED); 2.An understanding of the key elements of CO-OP and their application for individuals with ED. 3.Knowledge regarding the evidence relating to the use of CO-OP with adults with ABI and stroke. 4.Practiced techniques of dynamic performance analysis and guided discovery. 5.Considered how these techniques can be applied to personal clinical practice.




144 Cognitive Orientation to daily Occupational Performance (CO-OP) a client-centred, performance-based, problem solving, approach that enables skill acquisition through a process of strategy use and guided discovery. (Polatajko & Mandich, 2004, p. 2).

145 CO-OP engages the client at a metacognitive level in an iterative process of dynamic performance analysis and solution creation and evaluation. -International CO-OP Academy Executive,
146 Four major objectives 1. Skill acquisition 2. Strategy use 3. Generalization 4. Transfer Polatajko and Mandich 58 CO-OP: Goal
147 Theory for use with Impairments in We hypothesize that: Frontal Processes üglobal strategy use compensates for executive cognitive impairments and for impairments in the integrative functions in the frontal poles; üimpairments in self-regulation may be partially addressed through the use of this strategy, which by its very nature encourages people to monitor their behaviours; ühaving clients actively involved in identifying problems in their daily lives is engaging - they want to change and set goals accordingly.
148 Evidence (in adults with cognitive impairments) Adults with ABI 1. Dawson et al. (2009). Using the cognitive orientation to occupational performance (CO-OP) with adults with traumatic brain injury. Canadian Journal of Occupational Therapy, 76, Dawson et al. (2013). Occupation-based strategy training for adults with traumatic brain injury: A pilot study. Archives of Physical Medicine & Rehabilitation, 94(10), Dawson et al. (2013). Managing executive dysfunction following acquired brain injury and stroke using an ecologically valid rehabilitation approach: A protocol for a randomized, controlled trial. Trials, Ng, E., Dawson, D. (2013). Telerehabilitation for addressing executive dysfunction after traumatic brain injury. Brain Injury, 27(5), Adults with Stroke 5. Skidmore Dawson, D. et al. (2011). The feasibility of meta-cognitive strategy training in acute inpatient stroke rehabilitation: A case report. Neuropsychological Rehabilitation, 21, Skidmore, E. R., Dawson, D. R., et al. (2014). Developing complex interventions: Lessons learned from a pilot study examining strategy training in acute rehabilitation. Clinical Rehabilitation, 28(4), Skidmore, E., Dawson, D., et al. (Dec. 2015). Strategy training may reduce disability in the first six months post-stroke. Neurorehabilitation and Neural Repair. 8. Poulin, V., Dawson, D. (2016). Comparison of two cognitive interventions for adults experiencing executive dysfunction post-stroke: A pilot study. Disability & Rehabilitation. Older Adults with Age-related Executive Changes 9. Dawson, et al. (2014). An occupation-based strategy training approach to managing age-related executive changes: A pilot randomized controlled trial. Clinical Rehabilitation, 28(2),
149
150
151
152 CO-OP Key Features
153 Client Chosen Goals COGNITIVE ORIENTATION to daily OCCUPATIONAL PERFORMANCE CO-OP Dynamic Performance Analysis Cognitive Strategy Use Essential Elements Guided Discovery Enabling Principles Parent Significant other involvement Structural Elements Intervention Format
154 Establish goal Establish baseline performance Do the DPA (iteratively) Use GPDC (throughout) Plan DSS The CO-OP Process Goal DPA GD Use Guided Discovery (throughout) Identify DSS s (throughout) Use Enabling Principles (throughout) Post-test No Check Do Skill Acquisition Yes Polatajko and Mandich
155 Pre-requisites Client Polatajko and Mandich 67 CO-OP: Getting Started Able to identify at least 3 occupational performance difficulties. Sufficient language fluency Behavioural responsiveness
156 Pre-requisites Therapist Polatajko and Mandich 68 CO-OP: Getting Started Client-centred philosophy Understanding of disability Behavioural management Effective communication Activity analysis Learning theory Working with parents
157 Goal Setting 1. The COPM 2. The Activity Card Sort 3. Daily Log
158 Establish Baseline Performance
159 Establishing Baseline Performance Performance Quality Rating Scale - Observational, performance measure - 10 point Likert-type scale - 1=no activity criteria are met - 10=all activity criteria are met with good quality
160 Dawson, Establishing baseline with goals you cannot observe
161 Dynamic Performance Analysis
162 DYNAMIC PERFORMANCE Objectives ANALYSIS to identify performance problems to begin hypothesizing about potential strategies to enable performance Refers to ongoing analysis with client of their performance. Use of activity analysis to identify performance problems or areas of breakdown, use of guided discovery to assist client in problem-solving regarding where performance is breaking down Iterative process Intervention is then guided accordingly.
163 DPA What s going wrong with: individual environment task? behavioral analysis CO-OP: DPA Task analysis What s the underlying problem: neurodevelopmental sensory-motor visual perceptual? component analysis Polatajko and Mandich 75
164 Key Feature: Cognitive Strategy Use
165 Polatajko and Mandich 77 CO-OP: Skill Acquisition Through Strategy Use Cognitive Strategy: a cognitive tool put into place to help learn, memorize and problem solve a goal directed, cognitive operation used to facilitate learning and problem solving a skill under consideration (Paris 1989)
166 Polatajko and Mandich 78 Why use strategies? Learners should know more about how to manage their own cognitive strategies, and how to analyse themselves and the situational demands in order to improve learning and performance.
167 Types Global Strategy Polatajko and Mandich 79 CO-OP: Cognitive Strategies Domain Specific Strategy (DSS)
168 Introducing the global strategy Introduce the strategy Go over definitions for each part of the strategy Check participant s understanding using examples GOAL PLAN DO CHECK

169 What are Domain Specific Strategies? Strategies that are specific to a particular task & situation (cognitive and/or other strategies). They are introduced to solve specific performance issues as they arise. Domain specific strategies may differ between people performing the same task. DPA is used in CO-OP to determine the need for DSS. Used only when needed! (Polatajko & Mandich, 2004)
170 V E R B A L G U I D A N C E Domain Specific Strategies Body position Attention to task Task specification/modification Supplementing task knowledge Feeling the movement 2V s Verbal motor mnemonic / Verbal rote script Polatajko and Mandich 82
171 Body Position Verbalization of attention to or shift of the body, whole or part relative to the task Therapist: Is that the foot you usually start with?
172 Attention to Doing Verbalization to cue attending to the doing of the task Therapist: The kettle is boiling. Polatajko and Mandich 84
173 Task Modification Discussions regarding the modification of the task or parts of the task that facilitate performance Decrease speed to accomplish task Use non-impaired hand to do task Provision of any adapted equipment, such as modified cutting board Polatajko and Mandich
174 Supplementing Task Knowledge Verbalization of the specifics of a task -things - things that cannot be discovered or that are not central to the focus of attention. Therapist To save the file, click on file and then on save. Polatajko and Mandich
175 Circumstance Polatajko and Mandich 87 Strategies as Solutions When the Client does not have enough information to specify the GOAL or PLAN When the Client does not DO the plan When the Client can do the task but required verbal guidance to practice Strategies Used Supplementing task knowledge Task specification Mnemonic Attention to doing Task modification Body position Feeling the movement Verbal Guidance Verbal self-guidance Verbal Rote Script

176 Bottari et al., Consider cognitive demand related to strategy use
177 Key Feature: Guided Discovery
178 Guided Discovery Guided discovery is a way of using language to guide the participant to discover strategies and make plans to solve their problems or to make plans to work toward their goals.
179 Figure it out on your own! Low: Discovery Learning Instructor Control Try to do it out on your own but I will help you if you get stuck. Continuum Mid: Guided Discovery High: Explicit Instruction I will tell you what to do! 91
180 Ask, don t tell! Guided Discovery Coach, don t adjust! Guided Discovery Make it obvious! One thing at a time!

181 How much guided discovery do we usually do in our practice? Urquhart & Skidmore, OTJR, 2014
182 Purpose Study on Guided Discovery Brennan, Morrison, Bottari, Hunt, LeDorze & Dawson, in prep. 1. To describe the verbalizations utilized by the therapist in the context of guided discovery; 2. To determine if some verbalizations were more effective than others at promoting plan formulation.



183 Results: Effectiveness of strategy for promotion of goal attainment Frequency of progress
184 Guided Discovery: Hierarchy Asking broadly Coaching (e.g., Can you tell me more about that? ) One thing at a time (e.g., I m hearing a few different things in the plan can you tell it to me one part at a time?) Describing alternatives (e.g., from another client or self) Suggesting alternatives Dawson & Hunt, 2013
185 Guided Discovery Cues ü What do you usually do? (What have you done in the past?) ü How did that work? ü How are you doing? (How is it going?) ü Tell me more about that. ü What s next? ü That s the good thing about plans, if one doesn t work you can always make another one. ü I think we re a little off track here, let s bring it back to G-P-D-C. ü Okay, let s stick with the plan. ü How will you know that plan worked? ü You said your plan didn t work, but your plan actually did work. ü So let me understand what you are saying ü Sometimes a plan will be that we can do it together. ü Affirmations (good, great idea, etc.) Dawson & Hunt, 2013
186 Scenario: Guided Discovery David is trying to find a phone number in his daytimer. Mary said where do you keep your phone numbers? What other GD verbalizations might you use?
187 Scenario: Guided Discovery A participant s goal is to stop burning food on the stove. Rather than directly telling the participant how to solve the problem (e.g. by setting a timer) the facilitator guides the participant to discover a solution on their own.
188 Guided Discovery Examples
189 Key Feature: Enabling Principles
190 ü Make it fun ü Promote learning Polatajko and Mandich 102 Enabling Principles ü Work towards independence ü Promote generalization and transfer

191 Promoting Learning?
I have no financial disclosures.
 Performance-Based Cognitive Assessment Glen Gillen, EdD, OTR, FAOTA Programs in Occupational Therapy College of Physicians and Surgeons Columbia University I have no financial disclosures. Outline Approaches
Performance-Based Cognitive Assessment Glen Gillen, EdD, OTR, FAOTA Programs in Occupational Therapy College of Physicians and Surgeons Columbia University I have no financial disclosures. Outline Approaches
The Role of Self- Awareness in the Use of Strategy Training. Jessica Kersey, MOT, OTR/L, CBIS
 The Role of Self- Awareness in the Use of Strategy Training Jessica Kersey, MOT, OTR/L, CBIS Objectives 1. Understand the implications of self-awareness impairments 2. Identify the active ingredients of
The Role of Self- Awareness in the Use of Strategy Training Jessica Kersey, MOT, OTR/L, CBIS Objectives 1. Understand the implications of self-awareness impairments 2. Identify the active ingredients of
COGNITION PART TWO HIGHER LEVEL ASSESSMENT FUNCTIONAL ASSESSMENT
 COGNITION PART TWO HIGHER LEVEL ASSESSMENT FUNCTIONAL ASSESSMENT RECAP ON PART ONE BASIC ASSESSMENT Cognitive screening tests are one component of the cognitive assessment process and NOT equivalent to
COGNITION PART TWO HIGHER LEVEL ASSESSMENT FUNCTIONAL ASSESSMENT RECAP ON PART ONE BASIC ASSESSMENT Cognitive screening tests are one component of the cognitive assessment process and NOT equivalent to
by Peter K. Isquith, PhD, Robert M. Roth, PhD, Gerard A. Gioia, PhD, and PAR Staff
 by Peter K. Isquith, PhD, Robert M. Roth, PhD, Gerard A. Gioia, PhD, and PAR Staff Client name : Sample Client Client ID : 321 Gender : Female Age : 27 Test date : Test form : BRIEF-A Informant Report
by Peter K. Isquith, PhD, Robert M. Roth, PhD, Gerard A. Gioia, PhD, and PAR Staff Client name : Sample Client Client ID : 321 Gender : Female Age : 27 Test date : Test form : BRIEF-A Informant Report
Complex Task Performance Assessment. Timothy J. Wolf, OTD, MSCI, OTR/L Assistant Professor Program in Occupational Therapy Department of Neurology
 Complex Task Performance Assessment Timothy J. Wolf, OTD, MSCI, OTR/L Assistant Professor Executive Function Definitions Executive function is the ability to integrate various component cognitive abilities
Complex Task Performance Assessment Timothy J. Wolf, OTD, MSCI, OTR/L Assistant Professor Executive Function Definitions Executive function is the ability to integrate various component cognitive abilities
Tutorial: Cognition See Tutorials on Attention, Memory, Retrieval, Organization, Problem Solving, Reasoning, Self- Regulation/Executive Functions
 Tutorial: Cognition See Tutorials on Attention, Memory, Retrieval, Organization, Problem Solving, Reasoning, Self- Regulation/Executive Functions WHAT IS COGNITION? comprehending it, storing it, retrieving
Tutorial: Cognition See Tutorials on Attention, Memory, Retrieval, Organization, Problem Solving, Reasoning, Self- Regulation/Executive Functions WHAT IS COGNITION? comprehending it, storing it, retrieving
The ultimate outcome of TBI rehabilitation: Successful and satisfying community participation (McCabe, 2007)
") Steven Wheeler, Ph.D., OTR/L Associate Professor, Occupational Therapy West Virginia University School of Medicine 1. Understand the effect of impaired cognitive functioning on successful and satisfying
Steven Wheeler, Ph.D., OTR/L Associate Professor, Occupational Therapy West Virginia University School of Medicine 1. Understand the effect of impaired cognitive functioning on successful and satisfying
LOTCA Assessment review. Georgina Wrack. University of the Sunshine Coast
 Assessment review 1 LOTCA Assessment review Georgina Wrack University of the Sunshine Coast Assessment review 2 LOTCA Summary Page The Loewenstein Occupational Therapy Cognitive Assessment (LOTCA) is a
Assessment review 1 LOTCA Assessment review Georgina Wrack University of the Sunshine Coast Assessment review 2 LOTCA Summary Page The Loewenstein Occupational Therapy Cognitive Assessment (LOTCA) is a
Process of a neuropsychological assessment
 Test selection Process of a neuropsychological assessment Gather information Review of information provided by referrer and if possible review of medical records Interview with client and his/her relative
Test selection Process of a neuropsychological assessment Gather information Review of information provided by referrer and if possible review of medical records Interview with client and his/her relative
The Measurement of Everyday Life Executive Functioning in Adults with FASD: A Pilot Study
 The Measurement of Everyday Life Executive Functioning in Adults with FASD: A Pilot Study 11/15/2013 Dr. M. Tracy Morrison, OTD R/L Clinical Scientist and Manager of Clinical Programs and Services, Courage
The Measurement of Everyday Life Executive Functioning in Adults with FASD: A Pilot Study 11/15/2013 Dr. M. Tracy Morrison, OTD R/L Clinical Scientist and Manager of Clinical Programs and Services, Courage
Changes, Challenges and Solutions: Overcoming Cognitive Deficits after TBI Sarah West, Ph.D. Hollee Stamper, LCSW, CBIS
 Changes, Challenges and Solutions: Overcoming Cognitive Deficits after TBI Sarah West, Ph.D. Hollee Stamper, LCSW, CBIS Learning Objectives 1. Be able to describe the characteristics of brain injury 2.
Changes, Challenges and Solutions: Overcoming Cognitive Deficits after TBI Sarah West, Ph.D. Hollee Stamper, LCSW, CBIS Learning Objectives 1. Be able to describe the characteristics of brain injury 2.
Executive Functioning
 Executive Functioning What is executive functioning? Executive functioning is a process of higher brain functioning that is involved in goal directed activities. It is the part of the brain that enables
Executive Functioning What is executive functioning? Executive functioning is a process of higher brain functioning that is involved in goal directed activities. It is the part of the brain that enables
Note: The trainings below represent a foundational list, and may be adapted based on audience and need.
 MOTIVATIONAL INTERVIEWING Introduction to Motivational Interviewing (offered in English and Spanish) 2-day Course (12-14 credit hours) This course is designed to introduce clinicians and staff members
MOTIVATIONAL INTERVIEWING Introduction to Motivational Interviewing (offered in English and Spanish) 2-day Course (12-14 credit hours) This course is designed to introduce clinicians and staff members
Understanding and improving attention and information processing in MS
 Understanding and improving attention and information processing in MS Ben Harris Clinical Neuropsychologist Overview A follow up to previous presentation on memory strategies Aim is to provide explanation
Understanding and improving attention and information processing in MS Ben Harris Clinical Neuropsychologist Overview A follow up to previous presentation on memory strategies Aim is to provide explanation
Reliability and construct validity of a revised Baycrest Multiple Errands Test
 Neuropsychological Rehabilitation An International Journal ISSN: 0960-2011 (Print) 1464-0694 (Online) Journal homepage: http://www.tandfonline.com/loi/pnrh20 Reliability and construct validity of a revised
Neuropsychological Rehabilitation An International Journal ISSN: 0960-2011 (Print) 1464-0694 (Online) Journal homepage: http://www.tandfonline.com/loi/pnrh20 Reliability and construct validity of a revised
Disclosure : Financial No relevant financial relationship exists. Nonfinancial received partial support for my research from BioGen
 Innovative assessments and treatments in cognitive rehabilitation with persons with MS Yael Goverover Disclosure : Financial No relevant financial relationship exists. Nonfinancial received partial support
Innovative assessments and treatments in cognitive rehabilitation with persons with MS Yael Goverover Disclosure : Financial No relevant financial relationship exists. Nonfinancial received partial support
Everyday Strategies to Manage Thinking and Memory Changes Associated with MS
 Everyday Strategies to Manage Thinking and Memory Changes Associated with MS Ben Harris (MPsych, PhD) Clinical Neuropsychologist Overview Brief summary of areas of cognitive function commonly affected
Everyday Strategies to Manage Thinking and Memory Changes Associated with MS Ben Harris (MPsych, PhD) Clinical Neuropsychologist Overview Brief summary of areas of cognitive function commonly affected
Cognitive Remediation Therapy (CRT)
") Cognitive Remediation Therapy (CRT) Experiences of implementation in inpatient rehabilitation services Dr Ian-Mark Kevan (Consultant Clinical Psychologist) BPS PCMHF Event 24 th March 2017 - Stirling Plan
Cognitive Remediation Therapy (CRT) Experiences of implementation in inpatient rehabilitation services Dr Ian-Mark Kevan (Consultant Clinical Psychologist) BPS PCMHF Event 24 th March 2017 - Stirling Plan
Traumatic Brain Injury for VR Counselors Margaret A. Struchen, Ph.D. and Laura M. Ritter, Ph.D., M.P.H.
 Training Session 3a: Understanding Roles of Members of the Interdisciplinary Treatment Team, Evaluations by Team Members and the Utility of Evaluations Conducted by such Team Members. The Interdisciplinary
Training Session 3a: Understanding Roles of Members of the Interdisciplinary Treatment Team, Evaluations by Team Members and the Utility of Evaluations Conducted by such Team Members. The Interdisciplinary
Thinking and Memory in MS
 Thinking and Memory in MS Ben Harris (MPsych, PhD) Clinical Neuropsychologist Overview Basic structure of the brain and how signals are communicated between different areas Changes to the brain associated
Thinking and Memory in MS Ben Harris (MPsych, PhD) Clinical Neuropsychologist Overview Basic structure of the brain and how signals are communicated between different areas Changes to the brain associated
Champlain Assessment/Outcome Measures Forum February 22, 2010
 Champlain Assessment/Outcome Measures Forum February 22, 2010 Welcome Table Configurations Each table has a card with the name of the discipline(s) and the mix of professions Select the discipline of interest
Champlain Assessment/Outcome Measures Forum February 22, 2010 Welcome Table Configurations Each table has a card with the name of the discipline(s) and the mix of professions Select the discipline of interest
THE ESSENTIAL BRAIN INJURY GUIDE
 THE ESSENTIAL BRAIN INJURY GUIDE Outcomes Section 9 Measurements & Participation Presented by: Rene Carfi, LCSW, CBIST Senior Brain Injury Specialist Brain Injury Alliance of Connecticut Contributors Kimberly
THE ESSENTIAL BRAIN INJURY GUIDE Outcomes Section 9 Measurements & Participation Presented by: Rene Carfi, LCSW, CBIST Senior Brain Injury Specialist Brain Injury Alliance of Connecticut Contributors Kimberly
support support support STAND BY ENCOURAGE AFFIRM STRENGTHEN PROMOTE JOIN IN SOLIDARITY Phase 3 ASSIST of the SASA! Community Mobilization Approach
 support support support Phase 3 of the SASA! Community Mobilization Approach STAND BY STRENGTHEN ENCOURAGE PROMOTE ASSIST AFFIRM JOIN IN SOLIDARITY support_ts.indd 1 11/6/08 6:55:34 PM support Phase 3
support support support Phase 3 of the SASA! Community Mobilization Approach STAND BY STRENGTHEN ENCOURAGE PROMOTE ASSIST AFFIRM JOIN IN SOLIDARITY support_ts.indd 1 11/6/08 6:55:34 PM support Phase 3
Cancer and Cognitive Functioning
 Cancer and Cognitive Functioning Myron Goldberg, PhD, ABPP-CN Clinical Neuropsychologist Department of Rehabilitation Medicine University of Washington Medical Center Cognitive Functioning after Cancer
Cancer and Cognitive Functioning Myron Goldberg, PhD, ABPP-CN Clinical Neuropsychologist Department of Rehabilitation Medicine University of Washington Medical Center Cognitive Functioning after Cancer
How to Impact Initiation in Brain Injury Recovery Fall 2017 NeuroInstitute. Gordon J. Horn, PhD National Deputy Director Analytics & Outcomes
 How to Impact Initiation in Brain Injury Recovery Fall 2017 NeuroInstitute Gordon J. Horn, PhD National Deputy Director Analytics & Outcomes Objectives Participants will learn about the role of the frontal
How to Impact Initiation in Brain Injury Recovery Fall 2017 NeuroInstitute Gordon J. Horn, PhD National Deputy Director Analytics & Outcomes Objectives Participants will learn about the role of the frontal
For the OT2019 Class of MScOT students entering fall 2017: Occupational Therapy Year One Course Descriptions 44 credits
 For the OT2019 Class of MScOT students entering fall 2017: Occupational Therapy Year One Course Descriptions 44 credits OT 801 Conceptual Models in Occupational Therapy This course introduces students
For the OT2019 Class of MScOT students entering fall 2017: Occupational Therapy Year One Course Descriptions 44 credits OT 801 Conceptual Models in Occupational Therapy This course introduces students
PTSD Ehlers and Clark model
 Problem-specific competences describe the knowledge and skills needed when applying CBT principles to specific conditions. They are not a stand-alone description of competences, and should be read as part
Problem-specific competences describe the knowledge and skills needed when applying CBT principles to specific conditions. They are not a stand-alone description of competences, and should be read as part
Note: The trainings below represent a foundational list, and may be adapted based on audience and need.
 MOTIVATIONAL INTERVIEWING Introduction to Motivational Interviewing (offered in English and Spanish) 2-day Course (12-14 credit hours) This course is designed to introduce clinicians and staff members
MOTIVATIONAL INTERVIEWING Introduction to Motivational Interviewing (offered in English and Spanish) 2-day Course (12-14 credit hours) This course is designed to introduce clinicians and staff members
Objectives MCST CICI MCST CICI. Population & Background 4/1/2016
 Metacognitive Strategy Training for Breast Cancer Survivors with Chemobrain: Translating Research into Clinical Practice Meghan Doherty, MSOT, OTR/L, OTD/S Timothy Wolf, OTD, OTR/L, MSCI, FAOTA Objectives
Metacognitive Strategy Training for Breast Cancer Survivors with Chemobrain: Translating Research into Clinical Practice Meghan Doherty, MSOT, OTR/L, OTD/S Timothy Wolf, OTD, OTR/L, MSCI, FAOTA Objectives
Virginia s Autism Competencies for Direct Support Professionals and Supervisors who support individuals with Developmental Disabilities
 Autism Competencies Checklist (rev. 9.1.17) DMAS#P201 Virginia s Autism Competencies for Direct Support Professionals and Supervisors who support individuals with Developmental Disabilities The Autism
Autism Competencies Checklist (rev. 9.1.17) DMAS#P201 Virginia s Autism Competencies for Direct Support Professionals and Supervisors who support individuals with Developmental Disabilities The Autism
Views of autistic adults on assessment in the early years
 Views of autistic adults on what should be assessed and how assessment should be conducted on children with autism in the early years Summary of autistic adults views on assessment 1. Avoid drawing negative
Views of autistic adults on what should be assessed and how assessment should be conducted on children with autism in the early years Summary of autistic adults views on assessment 1. Avoid drawing negative
ARGUABLY ONE OF THE most devastating problems
 ORIGINAL ARTICLE Further Development of the Multiple Errands Test: Standardized Scoring, Reliability, and Ecological Validity for the Baycrest Version Deirdre R. Dawson, PhD, OT Reg (ON), Nicole D. Anderson,
ORIGINAL ARTICLE Further Development of the Multiple Errands Test: Standardized Scoring, Reliability, and Ecological Validity for the Baycrest Version Deirdre R. Dawson, PhD, OT Reg (ON), Nicole D. Anderson,
Chronic Fatigue Syndrome (CFS) / Myalgic Encephalomyelitis/Encephalopathy (ME)
 / Myalgic Encephalomyelitis/Encephalopathy (ME)") Chronic Fatigue Syndrome (CFS) / Myalgic Encephalomyelitis/Encephalopathy (ME) This intervention (and hence this listing of competences) assumes that practitioners are familiar with, and able to deploy,
Chronic Fatigue Syndrome (CFS) / Myalgic Encephalomyelitis/Encephalopathy (ME) This intervention (and hence this listing of competences) assumes that practitioners are familiar with, and able to deploy,
Course Descriptions for Courses in the Entry-Level Doctorate in Occupational Therapy Curriculum
 Course Descriptions for Courses in the Entry-Level Doctorate in Occupational Therapy Curriculum Course Name Therapeutic Interaction Skills Therapeutic Interaction Skills Lab Anatomy Surface Anatomy Introduction
Course Descriptions for Courses in the Entry-Level Doctorate in Occupational Therapy Curriculum Course Name Therapeutic Interaction Skills Therapeutic Interaction Skills Lab Anatomy Surface Anatomy Introduction
The development of a task applied executive function model to inform assessment and intervention in stroke rehabilitation
 Aphasia Research Unit - University College London 12 October 2016 The development of a task applied executive function model to inform assessment and intervention in stroke rehabilitation Charlie Chung
Aphasia Research Unit - University College London 12 October 2016 The development of a task applied executive function model to inform assessment and intervention in stroke rehabilitation Charlie Chung
Difference between ADHD and Executive Functioning. Dr. Josette Abdalla
 Difference between ADHD and Executive Functioning Dr. Josette Abdalla DSM-5 Definition of ADHD The DSM-5 diagnoses 3 types of ADHD: ADHD Predominantly Inattentive type ADHD Predominantly Hyperactive-Impulsive
Difference between ADHD and Executive Functioning Dr. Josette Abdalla DSM-5 Definition of ADHD The DSM-5 diagnoses 3 types of ADHD: ADHD Predominantly Inattentive type ADHD Predominantly Hyperactive-Impulsive
Slide Presentation 93rd AOTA Annual Conference & Expo, April 2013, San Diego, CA
 Slide Presentation 93rd AOTA Annual Conference & Expo, April 2013, San Diego, CA Preliminary Findings From the Systematic Review on Occupational Therapy Interventions for Stroke Focused question: What
Slide Presentation 93rd AOTA Annual Conference & Expo, April 2013, San Diego, CA Preliminary Findings From the Systematic Review on Occupational Therapy Interventions for Stroke Focused question: What
Test review. Comprehensive Trail Making Test (CTMT) By Cecil R. Reynolds. Austin, Texas: PRO-ED, Inc., Test description
 By Cecil R. Reynolds. Austin, Texas: PRO-ED, Inc., Test description") Archives of Clinical Neuropsychology 19 (2004) 703 708 Test review Comprehensive Trail Making Test (CTMT) By Cecil R. Reynolds. Austin, Texas: PRO-ED, Inc., 2002 1. Test description The Trail Making Test
Archives of Clinical Neuropsychology 19 (2004) 703 708 Test review Comprehensive Trail Making Test (CTMT) By Cecil R. Reynolds. Austin, Texas: PRO-ED, Inc., 2002 1. Test description The Trail Making Test
Increasing awareness following acquired brain injury: A quantative analysis of an outpatient education group
 Increasing awareness following acquired brain injury: A quantative analysis of an outpatient education group Lead Investigator: Orla McEvoy, Occupational Therapist, NRH Co-Facilitator: Joan Monahan, Speech
Increasing awareness following acquired brain injury: A quantative analysis of an outpatient education group Lead Investigator: Orla McEvoy, Occupational Therapist, NRH Co-Facilitator: Joan Monahan, Speech
The Role of Executive Functions in Attention Deficit Hyperactivity Disorder and Learning Disabilities
 Journal April 2000 Volume 10, No. 2 (Reprinted with permission of Editor) Attention Deficit Hyperactivity Disorder (ADHD) appears to be a disorder of self-control or executive functions. The executive
Journal April 2000 Volume 10, No. 2 (Reprinted with permission of Editor) Attention Deficit Hyperactivity Disorder (ADHD) appears to be a disorder of self-control or executive functions. The executive
Cancer and Cognitive Functioning: Strategies for Improvement
 Cancer and Cognitive Functioning: Strategies for Improvement Myron Goldberg, Ph.D., ABPP-CN Clinical Neuropsychologist Director, Neuro-Rehabilitation Program Department of Rehabilitation Medicine University
Cancer and Cognitive Functioning: Strategies for Improvement Myron Goldberg, Ph.D., ABPP-CN Clinical Neuropsychologist Director, Neuro-Rehabilitation Program Department of Rehabilitation Medicine University
Cognitive Rehabilitation with Current Research and Transition of Care
 Cognitive Rehabilitation with Current Research and Transition of Care Mike Dichiaro, MD Pediatric Rehabilitation Medicine Carin Rowan, MPT Pediatric Physical Therapy Financial Disclosures No relevant financial
Cognitive Rehabilitation with Current Research and Transition of Care Mike Dichiaro, MD Pediatric Rehabilitation Medicine Carin Rowan, MPT Pediatric Physical Therapy Financial Disclosures No relevant financial
COGNITIVE ENHANCEMENT:
 COGNITIVE ENHANCEMENT: Keeping Our Brains Fit and Healthy Debbie Gilmore Executive Director, Arrowsmith Program Established in Toronto, 1978 In over 100 public and private schools throughout Canada, USA,
COGNITIVE ENHANCEMENT: Keeping Our Brains Fit and Healthy Debbie Gilmore Executive Director, Arrowsmith Program Established in Toronto, 1978 In over 100 public and private schools throughout Canada, USA,
MANUAL FOR THE LIDCOMBE PROGRAM OF EARLY STUTTERING INTERVENTION 2008 CONTENTS
 MANUAL FOR THE LIDCOMBE PROGRAM OF EARLY STUTTERING INTERVENTION 2008 CONTENTS PART ONE: OVERVIEW OF THE LIDCOMBE PROGRAM... 2 PART TWO: ESSENTIAL COMPONENTS OF THE LIDCOMBE PROGRAM... 3 Parental Verbal
MANUAL FOR THE LIDCOMBE PROGRAM OF EARLY STUTTERING INTERVENTION 2008 CONTENTS PART ONE: OVERVIEW OF THE LIDCOMBE PROGRAM... 2 PART TWO: ESSENTIAL COMPONENTS OF THE LIDCOMBE PROGRAM... 3 Parental Verbal
Neuropsychology in Spina Bifida. Dr Ellen Northcott Clinical Neuropsychologist Kids Rehab, CHW
 Neuropsychology in Spina Bifida Dr Ellen Northcott Clinical Neuropsychologist Kids Rehab, CHW Who are neuropsychologists? Undergraduate Degree (eg. BPsych, BSc, BA) Honours in Psychology Master or Doctor
Neuropsychology in Spina Bifida Dr Ellen Northcott Clinical Neuropsychologist Kids Rehab, CHW Who are neuropsychologists? Undergraduate Degree (eg. BPsych, BSc, BA) Honours in Psychology Master or Doctor
CRITICALLY APPRAISED PAPER (CAP)
") CRITICALLY APPRAISED PAPER (CAP) Couillet, J., Soury, S., Lebornec, G., Asloun, S., Joseph, P., Mazaux, J., & Azouvi, P. (2010). Rehabilitation of divided attention after severe traumatic brain injury:
CRITICALLY APPRAISED PAPER (CAP) Couillet, J., Soury, S., Lebornec, G., Asloun, S., Joseph, P., Mazaux, J., & Azouvi, P. (2010). Rehabilitation of divided attention after severe traumatic brain injury:
Creating Better Lives for People with Dementia
 Creating Better Lives for People with Dementia PRESENTED BY: Kim Warchol, OTR/L Founder and President of Dementia Care Specialists LeadingAge/LALA Conference Objectives 1. Identify prevalence and characteristics
Creating Better Lives for People with Dementia PRESENTED BY: Kim Warchol, OTR/L Founder and President of Dementia Care Specialists LeadingAge/LALA Conference Objectives 1. Identify prevalence and characteristics
Beyond Lazy and Unmotivated
 Beyond Lazy and Unmotivated Why Parents and Teachers Need to Know About Executive Skills Peg Dawson Center for Learning and Attention Disorders Portsmouth, NH dawson.peg@gmail.com smartbutscatteredkids.com
Beyond Lazy and Unmotivated Why Parents and Teachers Need to Know About Executive Skills Peg Dawson Center for Learning and Attention Disorders Portsmouth, NH dawson.peg@gmail.com smartbutscatteredkids.com
Topics to Discuss. The Skeptic. The Human Brain. Right Brain! Left Brain! Hey, What About the Front Brain? Executive Functioning in the 21st Century
 Right Brain! Left Brain! Hey, What About the Front Brain? Executive Functioning in the 21st Century Adam J. Schwebach, Ph.D. Topics to Discuss Different Learning Styles Defining Executive Functioning Executive
Right Brain! Left Brain! Hey, What About the Front Brain? Executive Functioning in the 21st Century Adam J. Schwebach, Ph.D. Topics to Discuss Different Learning Styles Defining Executive Functioning Executive
A Framework for Optimal Cancer Care Pathways in Practice
 A to Guide Care Cancer Care A for Care in Practice SUPPORTING CONTINUOUS IMPROVEMENT IN CANCER CARE Developed by the National Cancer Expert Reference Group to support the early adoption of the A to Guide
A to Guide Care Cancer Care A for Care in Practice SUPPORTING CONTINUOUS IMPROVEMENT IN CANCER CARE Developed by the National Cancer Expert Reference Group to support the early adoption of the A to Guide
A new scale for the assessment of competences in Cognitive and Behavioural Therapy. Anthony D. Roth. University College London, UK
 A new scale for the assessment of competences in Cognitive and Behavioural Therapy Anthony D. Roth University College London, UK Abstract Background: Scales for assessing competence in CBT make an important
A new scale for the assessment of competences in Cognitive and Behavioural Therapy Anthony D. Roth University College London, UK Abstract Background: Scales for assessing competence in CBT make an important
Cognitive Impairment in AOD: Assessment and Treatment
 Cognitive Impairment in AOD: Assessment and Treatment A Presentation for the Addiction Leadership Day 23 rd November 2016 Dr Jamie Berry Clinical Neuropsychologist Advanced Neuropsychological Treatment
Cognitive Impairment in AOD: Assessment and Treatment A Presentation for the Addiction Leadership Day 23 rd November 2016 Dr Jamie Berry Clinical Neuropsychologist Advanced Neuropsychological Treatment
COGNITIVE REHABILITATION OF INDIVIDUALS WITH MS CMSC 2015
 COGNITIVE REHABILITATION OF INDIVIDUALS WITH MS CMSC 2015 Aaron Turner, Ph.D. (ABPP-RP) Director, Rehabilitation Psychology VA Puget Sound Health Care System Associate Professor Department of Rehabilitation
COGNITIVE REHABILITATION OF INDIVIDUALS WITH MS CMSC 2015 Aaron Turner, Ph.D. (ABPP-RP) Director, Rehabilitation Psychology VA Puget Sound Health Care System Associate Professor Department of Rehabilitation
After the Diagnosis: Rehabilitation & Support Options for Mild Dementia
 After the Diagnosis: Rehabilitation & Support Options for Mild Dementia Dr. Toni Nicholls, Clinical Neuropsychologist Peronne Village, cottage #20, Worthing, Christ Church 621-2022 Say these aloud Dog
After the Diagnosis: Rehabilitation & Support Options for Mild Dementia Dr. Toni Nicholls, Clinical Neuropsychologist Peronne Village, cottage #20, Worthing, Christ Church 621-2022 Say these aloud Dog
Interventions, Effects, and Outcomes in Occupational Therapy
 Interventions, Effects, and Outcomes in Occupational Therapy ADULTS AND OLDER ADULTS Instructor s Manual Learning Activities Mary Law, PhD, FCAOT Professor and Associate Dean Rehabilitation Science McMaster
Interventions, Effects, and Outcomes in Occupational Therapy ADULTS AND OLDER ADULTS Instructor s Manual Learning Activities Mary Law, PhD, FCAOT Professor and Associate Dean Rehabilitation Science McMaster
Behavior Rating Inventory of Executive Function BRIEF. Interpretive Report. Developed by SAMPLE
 Behavior Rating Inventory of Executive Function BRIEF Interpretive Report Developed by Peter K. Isquith, PhD, Gerard A. Gioia, PhD, and PAR Staff Client Information Client Name : Sample Client Client ID
Behavior Rating Inventory of Executive Function BRIEF Interpretive Report Developed by Peter K. Isquith, PhD, Gerard A. Gioia, PhD, and PAR Staff Client Information Client Name : Sample Client Client ID
PST-PC Appendix. Introducing PST-PC to the Patient in Session 1. Checklist
 PST-PC Appendix Introducing PST-PC to the Patient in Session 1 Checklist 1. Structure of PST-PC Treatment 6 Visits Today Visit: 1-hour; Visits 2-8: 30-minutes Weekly and Bi-weekly Visits Teach problem
PST-PC Appendix Introducing PST-PC to the Patient in Session 1 Checklist 1. Structure of PST-PC Treatment 6 Visits Today Visit: 1-hour; Visits 2-8: 30-minutes Weekly and Bi-weekly Visits Teach problem
How to Integrate Peer Support & Navigation into Care Delivery
 How to Integrate Peer Support & Navigation into Care Delivery Andrew Bertagnolli, PhD Care Management Institute Why Integrate Peer Support into the Care Delivery Pathway? Improved health Increased feelings
How to Integrate Peer Support & Navigation into Care Delivery Andrew Bertagnolli, PhD Care Management Institute Why Integrate Peer Support into the Care Delivery Pathway? Improved health Increased feelings
Final Consultation on the Neuropsychologist Scope of Practice: Core Competencies, and a Grand-parenting Pathway to Registration
 Final Consultation on the Neuropsychologist Scope of Practice: Core Competencies, and a Grand-parenting Pathway to Registration June 2017 SECTION A: BACKGROUND In December 2015 the Board consulted stakeholders
Final Consultation on the Neuropsychologist Scope of Practice: Core Competencies, and a Grand-parenting Pathway to Registration June 2017 SECTION A: BACKGROUND In December 2015 the Board consulted stakeholders
Developing Psychological Interventions for adults with high functioning autism spectrum disorders. Dr Neil Hammond Consultant Clinical Psychologist
 Developing Psychological Interventions for adults with high functioning autism spectrum disorders Dr Neil Hammond Consultant Clinical Psychologist Outline Current research psychological therapy Autism
Developing Psychological Interventions for adults with high functioning autism spectrum disorders Dr Neil Hammond Consultant Clinical Psychologist Outline Current research psychological therapy Autism
FRASER RIVER COUNSELLING Practicum Performance Evaluation Form
 FRASER RIVER COUNSELLING Practicum Performance Evaluation Form Semester 1 Semester 2 Other: Instructions: To be completed and reviewed in conjunction with the supervisor and the student, signed by both,
FRASER RIVER COUNSELLING Practicum Performance Evaluation Form Semester 1 Semester 2 Other: Instructions: To be completed and reviewed in conjunction with the supervisor and the student, signed by both,
Integrated Care for Depression, Anxiety and PTSD. Introduction: Overview of Clinical Roles and Ideas
 Integrated Care for Depression, Anxiety and PTSD University of Washington An Evidence-based d Approach for Behavioral Health Professionals (LCSWs, MFTs, and RNs) Alameda Health Consortium November 15-16,
Integrated Care for Depression, Anxiety and PTSD University of Washington An Evidence-based d Approach for Behavioral Health Professionals (LCSWs, MFTs, and RNs) Alameda Health Consortium November 15-16,
Brain Injury Behaviors or Symptoms. Zach Tubbs, LSW, CBIS Education and Community Outreach Specialist
 Brain Injury Behaviors or Symptoms Zach Tubbs, LSW, CBIS Education and Community Outreach Specialist Minnesota Brain Injury Alliance To raise awareness and enhance the quality of life for all people affected
Brain Injury Behaviors or Symptoms Zach Tubbs, LSW, CBIS Education and Community Outreach Specialist Minnesota Brain Injury Alliance To raise awareness and enhance the quality of life for all people affected
3/23/2017 ASSESSMENT AND TREATMENT NEEDS OF THE INDIVIDUAL WITH A TRAUMATIC BRAIN INJURY: A SPEECH-LANGUAGE PATHOLOGIST S PERSPECTIVE
 ASSESSMENT AND TREATMENT NEEDS OF THE INDIVIDUAL WITH A TRAUMATIC BRAIN INJURY: A SPEECH-LANGUAGE PATHOLOGIST S PERSPECTIVE MONICA STRAUSS HOUGH, PH.D, CCC/SLP CHAIRPERSON AND PROFESSOR COMMUNICATION SCIENCES
ASSESSMENT AND TREATMENT NEEDS OF THE INDIVIDUAL WITH A TRAUMATIC BRAIN INJURY: A SPEECH-LANGUAGE PATHOLOGIST S PERSPECTIVE MONICA STRAUSS HOUGH, PH.D, CCC/SLP CHAIRPERSON AND PROFESSOR COMMUNICATION SCIENCES
sammanchester Assessing Cognition in Emergency and Acute Medicine September 2015
 sammanchester 10 11 September 2015 Assessing Cognition in Emergency and Acute Medicine. Dr. Austin Claffey Senior Lecturer in Occupational Therapy London South Bank University. Assumptions Underlying neuropsychological
sammanchester 10 11 September 2015 Assessing Cognition in Emergency and Acute Medicine. Dr. Austin Claffey Senior Lecturer in Occupational Therapy London South Bank University. Assumptions Underlying neuropsychological
Cognitive Changes Workshop Outcomes
 HO 4.1 Cognitive Changes Workshop Outcomes At the end of this session, participants should be able to: define Neuropsychology and the role of the Neuropsychologist (optional) recognise normal difficulties
HO 4.1 Cognitive Changes Workshop Outcomes At the end of this session, participants should be able to: define Neuropsychology and the role of the Neuropsychologist (optional) recognise normal difficulties
Top Ten Things to Know About Motivational Interviewing
 Top Ten Things to Know About Motivational Interviewing Theresa Moyers, Ph.D. Department of Psychology, University of New Mexico Center on Alcoholism, Substance Abuse and Addictions (CASAA) Four Foundational
Top Ten Things to Know About Motivational Interviewing Theresa Moyers, Ph.D. Department of Psychology, University of New Mexico Center on Alcoholism, Substance Abuse and Addictions (CASAA) Four Foundational
Neuropsychological Assessment: Applications to the Work Setting
 : Applications to the Work Setting! Arlin Pachet, Ph.D, R.Psych., ABPP Board Certified Clinical Neuropsychologist! September 30, 2014 1 Presentation Objectives! (NPA) overview What is an NPA? What is a
: Applications to the Work Setting! Arlin Pachet, Ph.D, R.Psych., ABPP Board Certified Clinical Neuropsychologist! September 30, 2014 1 Presentation Objectives! (NPA) overview What is an NPA? What is a
Cognitive Rehabilitation: Tools for Living Better with Brain Injury
 Cognitive Rehabilitation: Tools for Living Better with Brain Injury Jessica Petersen, OTR/L Meeting Name Here And Date Here 2011 MFMER slide-1 Objectives Upon completion of this presentation, participants
Cognitive Rehabilitation: Tools for Living Better with Brain Injury Jessica Petersen, OTR/L Meeting Name Here And Date Here 2011 MFMER slide-1 Objectives Upon completion of this presentation, participants
Brain TLC: Supporting Brain Health with Cognitive Rehabilitation. Kristin Knight, MS, CCC-SLP Haley Landau, MS, CCC-SLP
 Brain TLC: Supporting Brain Health with Cognitive Rehabilitation Kristin Knight, MS, CCC-SLP Haley Landau, MS, CCC-SLP April 26, 2018 TODAY S PLAN Provide an overview of: The role of the speech-language
Brain TLC: Supporting Brain Health with Cognitive Rehabilitation Kristin Knight, MS, CCC-SLP Haley Landau, MS, CCC-SLP April 26, 2018 TODAY S PLAN Provide an overview of: The role of the speech-language
Low Tolerance Long Duration (LTLD) Stroke Demonstration Project
 Stroke Demonstration Project") Low Tolerance Long Duration (LTLD) Stroke Demonstration Project Interim Summary Report October 25 Table of Contents 1. INTRODUCTION 3 1.1 Background.. 3 2. APPROACH 4 2.1 LTLD Stroke Demonstration Project
Low Tolerance Long Duration (LTLD) Stroke Demonstration Project Interim Summary Report October 25 Table of Contents 1. INTRODUCTION 3 1.1 Background.. 3 2. APPROACH 4 2.1 LTLD Stroke Demonstration Project
Occupational Therapy (OTHR)
") Occupational Therapy (OTHR) 1 Occupational Therapy (OTHR) Courses OTHR 5001. Developmental Perspectives in Occupational Therapy. 2 Credit Hours. This course explores human development and the relation
Occupational Therapy (OTHR) 1 Occupational Therapy (OTHR) Courses OTHR 5001. Developmental Perspectives in Occupational Therapy. 2 Credit Hours. This course explores human development and the relation
Psychotherapists and Counsellors Professional Liaison Group (PLG) 15 December 2010
 15 December 2010") Psychotherapists and Counsellors Professional Liaison Group (PLG) 15 December 2010 Standards of proficiency for counsellors Executive summary and recommendations Introduction At the meeting on 19 October
Psychotherapists and Counsellors Professional Liaison Group (PLG) 15 December 2010 Standards of proficiency for counsellors Executive summary and recommendations Introduction At the meeting on 19 October
Mapping A Pathway For Embedding A Strengths-Based Approach In Public Health. By Resiliency Initiatives and Ontario Public Health
 + Mapping A Pathway For Embedding A Strengths-Based Approach In Public Health By Resiliency Initiatives and Ontario Public Health + Presentation Outline Introduction The Need for a Paradigm Shift Literature
+ Mapping A Pathway For Embedding A Strengths-Based Approach In Public Health By Resiliency Initiatives and Ontario Public Health + Presentation Outline Introduction The Need for a Paradigm Shift Literature
Continuing Care. Part 3 Telephone Monitoring
 Continuing Care Part 3 Telephone Monitoring The goal of telephone monitoring is to establish a consistent avenue for tracking a client s recovery process. Through telephone collaborations the addiction
Continuing Care Part 3 Telephone Monitoring The goal of telephone monitoring is to establish a consistent avenue for tracking a client s recovery process. Through telephone collaborations the addiction
Transitions in Mental Health
 Transitions in Mental Health Slide 1: This PowerPoint focuses on mental health and how the concepts are applicable across many different populations and life span transitions. Slide 2: There are many lifestyle
Transitions in Mental Health Slide 1: This PowerPoint focuses on mental health and how the concepts are applicable across many different populations and life span transitions. Slide 2: There are many lifestyle
Treating New Learning and Memory Deficits in Rehabilitation Populations: the modified Story Memory Technique (msmt)
") Treating New Learning and Memory Deficits in Rehabilitation Populations: the modified Story Memory Technique (msmt) Nancy D. Chiaravalloti, Ph.D. Nancy Moore, MA Objectives Understand techniques for memory
Treating New Learning and Memory Deficits in Rehabilitation Populations: the modified Story Memory Technique (msmt) Nancy D. Chiaravalloti, Ph.D. Nancy Moore, MA Objectives Understand techniques for memory
VPS PRACTICUM STUDENT COMPETENCIES: SUPERVISOR EVALUATION VPS PRACTICUM STUDENT CLINICAL COMPETENCIES
 VPS PRACTICUM STUDENT COMPETENCIES: SUPERVISOR EVALUATION VPS PRACTICUM STUDENT CLINICAL COMPETENCIES EXPECTED CLINICAL COMPETENCIES OF UVM PRACTICUM STUDENTS COMPETENCY #1: TO DEVELOP EFFECTIVE COMMUNICATION
VPS PRACTICUM STUDENT COMPETENCIES: SUPERVISOR EVALUATION VPS PRACTICUM STUDENT CLINICAL COMPETENCIES EXPECTED CLINICAL COMPETENCIES OF UVM PRACTICUM STUDENTS COMPETENCY #1: TO DEVELOP EFFECTIVE COMMUNICATION
Telerehabilitation Applications for Cognitive and Vocational Rehabilitation
 3/29/11 Telerehabilitation Applications for Cognitive and Vocational Rehabilitation Michael McCue, PhD, April 1, 2011 School of Health and Rehabilitation Sciences Department of Rehabilitation Science and
3/29/11 Telerehabilitation Applications for Cognitive and Vocational Rehabilitation Michael McCue, PhD, April 1, 2011 School of Health and Rehabilitation Sciences Department of Rehabilitation Science and
Cognitive Remediation Therapy. CIRCuiTS
 Cognitive Remediation Therapy CIRCuiTS Outline What is CRT and CIRCuiTS? Aims of the course Cognitive impairment in schizophrenia What is impaired? Why try to improve thinking skills? Research findings
Cognitive Remediation Therapy CIRCuiTS Outline What is CRT and CIRCuiTS? Aims of the course Cognitive impairment in schizophrenia What is impaired? Why try to improve thinking skills? Research findings
MSc Psychological Research Methods/ MPsych Advanced Psychology Module Catalogue / 2018
 MSc Psychological Research Methods/ MPsych Advanced Psychology Module Catalogue - 2017 / 2018 PSY555: Communication of Research for Psychology (Semester 2) 10 credits core PRM, option MPsych This module
MSc Psychological Research Methods/ MPsych Advanced Psychology Module Catalogue - 2017 / 2018 PSY555: Communication of Research for Psychology (Semester 2) 10 credits core PRM, option MPsych This module
Canadian Mental Health Association
 Canadian Mental Health Association Manitoba and Winnipeg Supports & Services Founded in 1918, CMHA National is a Canada-wide charitable organization with 87 branches in over 330 communities across the
Canadian Mental Health Association Manitoba and Winnipeg Supports & Services Founded in 1918, CMHA National is a Canada-wide charitable organization with 87 branches in over 330 communities across the
Practical measures for evaluating outcomes: Australian Therapy Outcome Measures (AusTOMs)
") Practical measures for evaluating outcomes: Australian Therapy Outcome Measures (AusTOMs) Jemma Skeat Evaluation and Analysis Coordinator Royal Children s Hospital, Melbourne Professor Alison Perry Professor
Practical measures for evaluating outcomes: Australian Therapy Outcome Measures (AusTOMs) Jemma Skeat Evaluation and Analysis Coordinator Royal Children s Hospital, Melbourne Professor Alison Perry Professor
LONGITUDINAL EVALUATION OF COGNITION AFTER STROKE A SCOPING REVIEW
 LONGITUDINAL EVALUATION OF COGNITION AFTER STROKE A SCOPING REVIEW Juan Pablo Saa Doctor of Occupational Therapy Master of Public Health Washington University in St. Louis. USA PhD Candidate La Trobe University,
LONGITUDINAL EVALUATION OF COGNITION AFTER STROKE A SCOPING REVIEW Juan Pablo Saa Doctor of Occupational Therapy Master of Public Health Washington University in St. Louis. USA PhD Candidate La Trobe University,
New Mexico TEAM Professional Development Module: Deaf-blindness
 [Slide 1] Welcome Welcome to the New Mexico TEAM technical assistance module on making eligibility determinations under the category of deaf-blindness. This module will review the guidance of the NM TEAM
[Slide 1] Welcome Welcome to the New Mexico TEAM technical assistance module on making eligibility determinations under the category of deaf-blindness. This module will review the guidance of the NM TEAM
MEDICAL POLICY SUBJECT: COGNITIVE REHABILITATION. POLICY NUMBER: CATEGORY: Therapy/Rehabilitation
 MEDICAL POLICY SUBJECT: COGNITIVE REHABILITATION PAGE: 1 OF: 5 If a product excludes coverage for a service, it is not covered, and medical policy criteria do not apply. If a commercial product (including
MEDICAL POLICY SUBJECT: COGNITIVE REHABILITATION PAGE: 1 OF: 5 If a product excludes coverage for a service, it is not covered, and medical policy criteria do not apply. If a commercial product (including
Behaviour Change Intervention Design and Evaluation: Process Evaluation
 Behaviour Change Intervention Design and Evaluation: Process Evaluation Charles Abraham 28 th May, 2014 Are We Creating Evidence-Based Interventions Relevant to Government Policy UK House of Lords Inquiry
Behaviour Change Intervention Design and Evaluation: Process Evaluation Charles Abraham 28 th May, 2014 Are We Creating Evidence-Based Interventions Relevant to Government Policy UK House of Lords Inquiry
Kapi'olani Community College Courses , O-P, page 1
 Kapi'olani Community College Courses 2016 2017, O-P, page 1 OCCUPATIONAL THERAPY ASSISTANT OTA 110 Introduction to Occupational Therapy (3) Comment: Letter grade only. OTA 110 may not be audited. OTA 110
Kapi'olani Community College Courses 2016 2017, O-P, page 1 OCCUPATIONAL THERAPY ASSISTANT OTA 110 Introduction to Occupational Therapy (3) Comment: Letter grade only. OTA 110 may not be audited. OTA 110
CRITICALLY APPRAISED PAPER (CAP)
") CRITICALLY APPRAISED PAPER (CAP) FOCUSED QUESTION For community-dwelling older adults with functional limitations, does an occupational therapy home modification intervention program that includes the
CRITICALLY APPRAISED PAPER (CAP) FOCUSED QUESTION For community-dwelling older adults with functional limitations, does an occupational therapy home modification intervention program that includes the
Education Options for Children with Autism
 Empowering children with Autism and their families through knowledge and support Education Options for Children with Autism Starting school is a major milestone in a child s life, and a big step for all
Empowering children with Autism and their families through knowledge and support Education Options for Children with Autism Starting school is a major milestone in a child s life, and a big step for all
Functional Approaches to Managing Memory and Cognitive Deficits in Individuals with Traumatic Brain Injury. Janice Osborne Dowdy, MS, CCC-SLP, CBIS
 Functional Approaches to Managing Memory and Cognitive Deficits in Individuals with Traumatic Brain Injury Janice Osborne Dowdy, MS, CCC-SLP, CBIS Objectives In this course, participants will 1. Understand
Functional Approaches to Managing Memory and Cognitive Deficits in Individuals with Traumatic Brain Injury Janice Osborne Dowdy, MS, CCC-SLP, CBIS Objectives In this course, participants will 1. Understand
Using Brain Science to Help Transitional Workers Attain Goals & Progress Toward Self-Sufficiency
 Using Brain Science to Help Transitional Workers Attain Goals & Progress Toward Self-Sufficiency Richard Guare, Ph.D. D-BCBA October 26, 2017 WWW..ORG 2015 Goals and Agenda Goals: Attendees grasp the rationale,
Using Brain Science to Help Transitional Workers Attain Goals & Progress Toward Self-Sufficiency Richard Guare, Ph.D. D-BCBA October 26, 2017 WWW..ORG 2015 Goals and Agenda Goals: Attendees grasp the rationale,
Dr Claire Evans-Williams Highly Specialist Clinical Psychologist NHS/STAG Psychological Services/ The Autism Academy U.K
 Dr Claire Evans-Williams Highly Specialist Clinical Psychologist NHS/STAG Psychological Services/ The Autism Academy U.K Intended Learning Outcomes Identify the ways in which an autism assessment may arise
Dr Claire Evans-Williams Highly Specialist Clinical Psychologist NHS/STAG Psychological Services/ The Autism Academy U.K Intended Learning Outcomes Identify the ways in which an autism assessment may arise
DESIGN TYPE AND LEVEL OF EVIDENCE: Level I: Pilot randomized controlled trial. Limitations (appropriateness of study design):
:") CRITICALLY APPRAISED PAPER (CAP) FOCUSED QUESTION Does the Cognitive Orientation to daily Occupational Performance (CO-OP) approach increase clients performance on goals more than a standard occupational
CRITICALLY APPRAISED PAPER (CAP) FOCUSED QUESTION Does the Cognitive Orientation to daily Occupational Performance (CO-OP) approach increase clients performance on goals more than a standard occupational
ESDM Early Start Denver Model Parent Coaching P-ESDM
 ESDM Early Start Denver Model Parent Coaching P-ESDM BCASLPA Conference October 22nd, 2016 ESDM Canada Mary McKenna Janet Harder Michaela Jelen ESDM ESDM draws on several different models as its foundation
ESDM Early Start Denver Model Parent Coaching P-ESDM BCASLPA Conference October 22nd, 2016 ESDM Canada Mary McKenna Janet Harder Michaela Jelen ESDM ESDM draws on several different models as its foundation
How our understanding of ADHD and mental health issues in youth and young adults is changing. T. Sigi Hale, Ph.D.
 How our understanding of ADHD and mental health issues in youth and young adults is changing. T. Sigi Hale, Ph.D. A Neuroscientist s Perspective... Philosophical Theoretical Conceptual A Psychiatrist s
How our understanding of ADHD and mental health issues in youth and young adults is changing. T. Sigi Hale, Ph.D. A Neuroscientist s Perspective... Philosophical Theoretical Conceptual A Psychiatrist s
Time Experiencing by Robotic Agents
 Time Experiencing by Robotic Agents Michail Maniadakis 1 and Marc Wittmann 2 and Panos Trahanias 1 1- Foundation for Research and Technology - Hellas, ICS, Greece 2- Institute for Frontier Areas of Psychology
Time Experiencing by Robotic Agents Michail Maniadakis 1 and Marc Wittmann 2 and Panos Trahanias 1 1- Foundation for Research and Technology - Hellas, ICS, Greece 2- Institute for Frontier Areas of Psychology
The knowledge and skills involved in clinical audit
 The knowledge and skills involved in clinical A list of possible knowledge and skills related to clinical is in the box. Knowledge and skills involved in clinical Knowledge Skills The clinical process
The knowledge and skills involved in clinical A list of possible knowledge and skills related to clinical is in the box. Knowledge and skills involved in clinical Knowledge Skills The clinical process
Dialectical Behaviour Therapy in Secure Services Calverton Hill & Priory Hospital East Midlands Priory Group
 Context Our Dialectical Behaviour Therapy (DBT) team is a large multi-site team offering a standard DBT programme to patients who present with complex, severe, and enduring mental illness, personality
Context Our Dialectical Behaviour Therapy (DBT) team is a large multi-site team offering a standard DBT programme to patients who present with complex, severe, and enduring mental illness, personality
Demystifying the Neuropsychological Evaluation Report. Clinical Neuropsychologist 17 March 2017 Program Director, Neurobehavioral Program
 Demystifying the Neuropsychological Evaluation Report Jennifer R. Cromer, PhD BIAC Annual Conference Clinical Neuropsychologist 17 March 2017 Program Director, Neurobehavioral Program 84% of neuropsychologists
Demystifying the Neuropsychological Evaluation Report Jennifer R. Cromer, PhD BIAC Annual Conference Clinical Neuropsychologist 17 March 2017 Program Director, Neurobehavioral Program 84% of neuropsychologists