Stuart Murdoch Consultant Intensive Care St. James s University Hospital March 2010
|
|
|
- April Chambers
- 5 years ago
- Views:
Transcription
1 Stuart Murdoch Consultant Intensive Care St. James s University Hospital March 2010
2 Background- Critical Care Critical Care originated in Denmark with Polio epidemic 1950s respiratory support alone Rapid advances in organ support and monitoring Ability to use inotropes to support the heart Ability to offer renal replacement therapy for AKI
3 Background Critical Care Developed in ad- hoc way in UK Comprehensive Critical Care DOH 2000 Aimed to introduce a better assessment of need Hospital wide approach to critically ill patients Early warning score & Outreach services Quality Critical Care 2005 Recognised limited expansion (mostly HDU) and remaining unmet need Still significant number of inter hospital transfers
4 31 March January January January January January January January January January January January 2010 Number of beds Critical Care Beds in the UK Number of open and staffed adult critical care beds 4,000 3,500 3,000 2,500 2,000 1,500 1, High dependency Intensive care Census date
5 Background Critical Care UK fewer critical care beds than many other countries Sicker patients Greater level of nursing numbers (because of sicker patients- greater dependency) Makes comparison between countries difficult What may count as critical care in one country would not in another (HDU/advanced ward care etc)
6 Background Levels of Care Level 0: Patient s needs met on normal general ward Level 1: Patient at risk of deteriorating, needs can be met on the acute general ward with support Level 2 (HDU): Patient requires more detailed observation and monitoring including single organ support or post-major surgery or stepped down from level 3 Level 3 (ICU): Patient requires advanced respiratory support with invasive ventilation or basic respiratory support together with at least two organ supports
7 Why does this Matter? Limited Bed Numbers Goldilocks phenomenon patients not sick enough too well for critical care - therefore cannot come into limited beds available. If they do get into critical care discharged early Or too sick unlikely to survive? Is care appropriate? Patient has to be just sick enough to get into critical care.
8 Too Sick Early experience and reporting in oncology and haematology patients demonstrated high mortality rates and raised questions about the benefits of critical care for this group of patients. A lot of this is anecdote case series, from specialist centres etc. This informed views of appropriateness of admission to Critical Care (?still prevalent today)
9 Early data Cancer 1976 Turnbull et.al (Sloan Kettering Memorial New York) Report of 1035 consecutive admissions to cancer ITU between 1971 and 1974 (surgical, med onc and haem) Mortality in ICU 22.3% Mortality In Hospital 16.3% No indication of severity of illness or the underlying diagnosis Despite good results distinct note of caution in discussion
10 Haematology Patients Papers in the 1980 s describe mortality 80% and higher Mayo Clinic Data 1988 ( ) 116 patient 82% mortality Median survival of remaining 18% 12months Little published data on medical Oncology Patients (Chest 1988 Peters et al)
11 Too Sick 60 patients with haematological malignancy 13 left hospital alive. Data collected over 5 years at Barts In those who had relapsed 21/22 died The mortality of patients admitted to intensive care units with haematological malignancy is high. A humane approach to the management of the critically ill as well as efficient use of limited resources requires careful selection of those patients who are most likely to benefit from intensive care. Br Med J 1988;296: (9 April)
12 Too Sick JAMA 1993 Florida Cancer Centre 162 beds retrospective study 147 patients admitted Intensive care unit mortality 41 % 80% of patients with solid tumours survived less than 6 months The majority of patients with solid tumors and hematologic cancers admitted to the intensive care unit die before discharge, or, if they survive the hospital admission, they spend a minimal amount of time at home before dying
13 Too Sick patients in 5 centres in America- 190 had solid tumours 78 % hospital mortality 20% of cancer patients die of respiratory failure (excluding pneumonia and pulmonary emboli). Patients with cancer who require mechanical ventilation for respiratory failure have a grim prognosis.1-16 Respiratory failure in cancer patients is typically a manifestation of advanced lung disease that does not, in general, respond to supportive care. The decision to mechanically ventilate a cancer patient with respiratory failure is often contentious. The cost in terms of dollars, emotional suffering, and failed expectations is extraordinarily high. Journal of Clinical Oncology, Vol 17, Issue 3 (March), 1999: 991
14 UK data BJA 1999 Review of 22 patients admitted in regional centre (solid tumours 55%) Mortality 81% - associated with need for ventilation, renal support, neutropenia No survivors in the group who needed renal support, inotropes and ventilation Questioned discussing with patients prior to admission a view not supported in commentry
15 Better Results Intensive Care Medicine patients admitted to unit in Paris with solid tumours 30 day mortality was 58.7% Organ dysfunction and the need for ventilation strongly associated with poor outcome (not underlying malignancy)
16 Better?? In the last decade some data has suggested improvements in patient survival in patients with haematological malignancy Associated with use of Non-invasive ventilation Use of growth factors Usually from single centre specialist units However May be due to case selection- very sick patient not going to critical care

17 Longitudinal trends in sepsis among cancer patients from 1979 through 2001Danai P A et al. Chest 2006;129:
18 NIV Avoiding intubation is a major goal in the management of respiratory failure What can be done instead? Non invasive ventilation 52 patients 2 groups (one given NIV via face mask) Results 12 vs. 20, required endotracheal intubationp= vs. 21, had serious complications P=0.02, 10 vs. 18, died in the intensive care unit P= vs. 21, died in the hospital P=0.02 (N Engl J Med 2001;344:481-7.)
19 NIV in haematological patients with Acute Respiratory Failure 166 patients reviewed compared with small group 26 who received NIV 62% ICU mortality 71% hospital mortality Suggestion of improved outcome if avoid IPPV Depuydt et alchest 2004; 126:
20 Improved Outcomes? European study of cancer patients in ICU units in 24 countries 3147 patients enrolled 473 had a malignancy 85% solid tumours (15% haematological) Cancer patients older; likely to have had surgery and higher frequency of sepsis Increased incidence of ARDS/AKI Mortality 58% vs 27% for non-cancer population In patients with 3 or more organ system failure 75 % mortality cf 50% in non-cancer population Taccone et al Critical Care 2009, 13:R15
21 e Maximum Number of Organ Dysfunction during ICU stay White = No Cancer; Black=Solid Tumour; Grey=Haematological

22 Organ Dysfunction and Mortality White = No Cancer; Black=Solid Tumour; Grey=Haematological
23 Current UK data Haematological Malignancy Review of UK data entered into ICNARC 7689 admissions ( ) (1.5% of cases in database) ICU mortality 43%, hospital mortality 59.2% In patients with 3 organ system failure ICU mortality 83.9% Mortality associated with LOS prior to ICU and severe sepsis No time effect observed (Hampshire et al Critical Care 2009, 13 R137)
24 What can we do Early recognition and treatment Timely institution of appropriate care can reduce morbidity, mortality and length of stay Observations still poorly done Appropriate antibiotics- reduced mortality if cover Fluid resucitation Acting on Results Lack of knowledge widespread (NCEPOD report)
25 What can we do Good communication between oncology and critical care important Review of patients not just M&M but survivors
26 Outreach and Mews Aims to assist in early recognition of patients at risk and automatically trigger review and treatment Based on routine observations- variation from norm generates a score Escalation to more experienced staff Variable implementation nationwide Outreach service recommended to be 24/7 Not evidence based
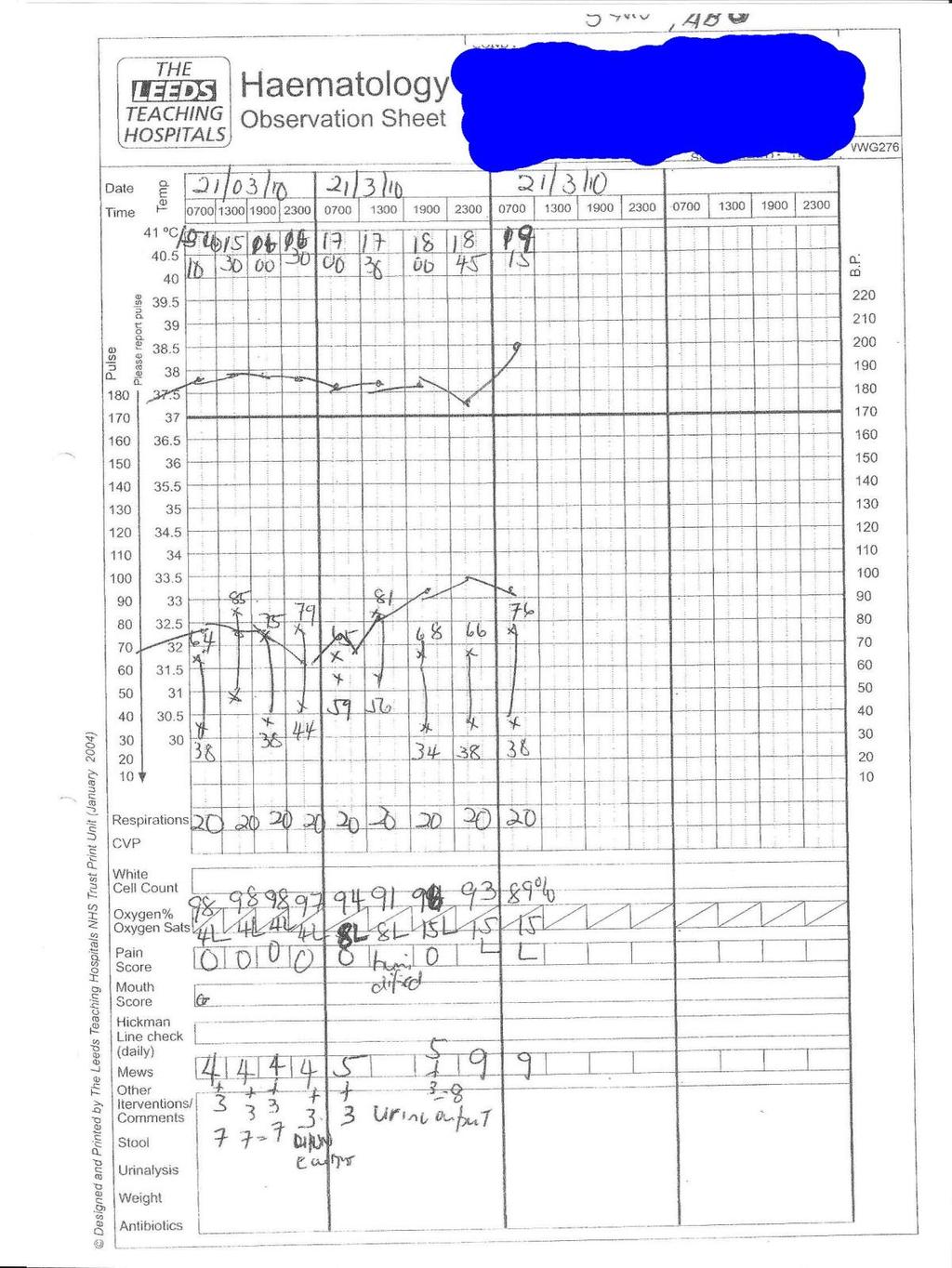
27 2 Patients 1 st patient 71 y old Non-Hodgkins lymphoma Septic at home- increased SOB, pyrexial, Admitted hypxoc; increased respiratory rate Signs of pneumonia on CXR Hypotensive admitted to ICU/HDU Lines fluids/inotropes CPAP- not intubated Appropriate antibiotic Got better after 48 hours discharged to HDU
28 2 nd Patient 73 y myeloma Neutropenic sepsis Pyrexial/Rigors at home? Pneumonia /hypoxic On ward deteriorated Eventually transferred to critical care Arrested/Intubated Now ventilated; cardiac impairment on inotropes and developing renal failure
29
30 Conclusion Admission to Critical Care in Oncology patients is associated with a high mortality In some patients admission may not be appropriate It is likely that early recognition and intervention into critically ill patients improves outcome and prevents deterioration Whilst data suggests improvements in outcome in oncology patients in critical care it is unclear if this is the same population as previously reported
31 Any Questions?
BTS/ICS Guidelines for the ventilatory management of acute hypercapnic respiratory failure in adults
 BTS/ICS Guidelines for the ventilatory management of acute hypercapnic respiratory failure in adults British Thoracic Society Intensive Care Society Introduction Acute Hypercapnic Respiratory Failure (AHRF)
BTS/ICS Guidelines for the ventilatory management of acute hypercapnic respiratory failure in adults British Thoracic Society Intensive Care Society Introduction Acute Hypercapnic Respiratory Failure (AHRF)
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Jain S, Kamimoto L, Bramley AM, et al. Hospitalized patients
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Jain S, Kamimoto L, Bramley AM, et al. Hospitalized patients
Outcome of patients with hematologic malignancy admitted to the ICU
 Outcome of patients with hematologic malignancy admitted to the ICU Geeta Mehta MD, FRCPC Mount Sinai Hospital Toronto, Canada CCCF November 2, 2016 Disclosures Hematologic Malignancy Advances in diagnostics,
Outcome of patients with hematologic malignancy admitted to the ICU Geeta Mehta MD, FRCPC Mount Sinai Hospital Toronto, Canada CCCF November 2, 2016 Disclosures Hematologic Malignancy Advances in diagnostics,
A Care Pathway exists for the management of neutropenic fever. Copies of the care pathway document are available in EAU, A&E, Deanesly and CHU.
 Subject: Neutropenic Fever Guideline for Junior Doctors Date of Implementation: January 2010 Date of Review: January 2012 Director Responsible for Implementation and Review: Policy location: Consultant
Subject: Neutropenic Fever Guideline for Junior Doctors Date of Implementation: January 2010 Date of Review: January 2012 Director Responsible for Implementation and Review: Policy location: Consultant
The paper provides an update for the Trust Board on hospital mortality and presents the updated Trust Mortality Action Plan.
 ENC No 13 Meeting Trust Board Date 28 th November 2013 Title of Paper Lead Director Author Hospital Mortality Update Mr Amir Khan, Medical Director Mr Amir Khan, Medical Director PURPOSE OF THE PAPER The
ENC No 13 Meeting Trust Board Date 28 th November 2013 Title of Paper Lead Director Author Hospital Mortality Update Mr Amir Khan, Medical Director Mr Amir Khan, Medical Director PURPOSE OF THE PAPER The
Debate: Do Rapid Response Systems Dumb Down Floor Staff? YES (or at least a qualified yes) Randy Wax, MD, MEd, FRCPC, FCCM
 Randy Wax, MD, MEd, FRCPC, FCCM") Debate: Do Rapid Response Systems Dumb Down Floor Staff? YES (or at least a qualified yes) Randy Wax, MD, MEd, FRCPC, FCCM Chief of Critical Care, Department of Emergency Medicine and Critical Care, Lakeridge
Debate: Do Rapid Response Systems Dumb Down Floor Staff? YES (or at least a qualified yes) Randy Wax, MD, MEd, FRCPC, FCCM Chief of Critical Care, Department of Emergency Medicine and Critical Care, Lakeridge
Early and Structured Rehabilitation Team Collaboration. David McWilliams Clinical Specialist Physiotherapist - UHB
 Early and Structured Rehabilitation Team Collaboration David McWilliams Clinical Specialist Physiotherapist - UHB Start early Moving through milestones Schweikert et al (2009) Increase frequency of higher
Early and Structured Rehabilitation Team Collaboration David McWilliams Clinical Specialist Physiotherapist - UHB Start early Moving through milestones Schweikert et al (2009) Increase frequency of higher
Supplementary Online Content
 Supplementary Online Content Gershengorn HB, Scales DC, Kramer A, Wunsch H. Association between overnight extubations and outcomes in the intensive care unit. JAMA Intern Med. Published online September
Supplementary Online Content Gershengorn HB, Scales DC, Kramer A, Wunsch H. Association between overnight extubations and outcomes in the intensive care unit. JAMA Intern Med. Published online September
Neutropenic Sepsis Acute General Management and Support. Ernie Marshall Macmillan Consultant in Medical Oncology Clatterbridge Centre for Oncology
 Neutropenic Sepsis Acute General Management and Support Ernie Marshall Macmillan Consultant in Medical Oncology Clatterbridge Centre for Oncology Who Am I? I am A Medical Oncologist (MCCN) Site specialist
Neutropenic Sepsis Acute General Management and Support Ernie Marshall Macmillan Consultant in Medical Oncology Clatterbridge Centre for Oncology Who Am I? I am A Medical Oncologist (MCCN) Site specialist
Data and the MET What to measure and why. Dr Daryl Jones
 Data and the MET What to measure and why Dr Daryl Jones Overview Background to, and principles of MET The afferent limb Cardiac arrests Missed and delayed METS The efferent limb Repeat MET calls The overall
Data and the MET What to measure and why Dr Daryl Jones Overview Background to, and principles of MET The afferent limb Cardiac arrests Missed and delayed METS The efferent limb Repeat MET calls The overall
Increased female mortality after ICU admission and its potential causes.
 Increased female mortality after ICU admission and its potential causes. L. Mardini, J. Lipes, D. Jayaraman McGill University CCCF 2012 Oral presentations session October 29 th 2012 Increased female mortality
Increased female mortality after ICU admission and its potential causes. L. Mardini, J. Lipes, D. Jayaraman McGill University CCCF 2012 Oral presentations session October 29 th 2012 Increased female mortality
NIV in hypoxemic patients
 NIV in hypoxemic patients Massimo Antonelli, MD Dept. of Intensive Care & Anesthesiology Università Cattolica del Sacro Cuore Rome - Italy Conflict of interest (research grants and consultations): Maquet
NIV in hypoxemic patients Massimo Antonelli, MD Dept. of Intensive Care & Anesthesiology Università Cattolica del Sacro Cuore Rome - Italy Conflict of interest (research grants and consultations): Maquet
Critical care resources are often provided to the too well and as well as. to the too sick. The former include the patients admitted to an ICU
 Literature Review Critical care resources are often provided to the too well and as well as to the too sick. The former include the patients admitted to an ICU following major elective surgery for overnight
Literature Review Critical care resources are often provided to the too well and as well as to the too sick. The former include the patients admitted to an ICU following major elective surgery for overnight
END OF LIFE CARE FOR THE FRAIL ELDERLY
 Intensive Care Unit END OF LIFE CARE FOR THE FRAIL ELDERLY Ken Hillman Interface of Palliative Care and ICU/Critical Care. Palliative Care South Australia. 19 March 2018. Adelaide. THE CHALLENGE Increasing
Intensive Care Unit END OF LIFE CARE FOR THE FRAIL ELDERLY Ken Hillman Interface of Palliative Care and ICU/Critical Care. Palliative Care South Australia. 19 March 2018. Adelaide. THE CHALLENGE Increasing
Steroids for ARDS. Clinical Problem. Management
 Steroids for ARDS James Beck Clinical Problem A 60 year old lady re-presented to ICU with respiratory failure. She had previously been admitted for fluid management and electrolyte correction having presented
Steroids for ARDS James Beck Clinical Problem A 60 year old lady re-presented to ICU with respiratory failure. She had previously been admitted for fluid management and electrolyte correction having presented
PILOT STUDY PROPOSAL FOR EARLY DISCHARGE OF LOW-RISK NEUTROPENIC PATIENTS
 PILOT STUDY PROPOSAL FOR EARLY DISCHARGE OF LOW-RISK NEUTROPENIC PATIENTS RATIONALE: It is increasingly being recognised that not all neutropenic patients have the same risk of complications during episodes
PILOT STUDY PROPOSAL FOR EARLY DISCHARGE OF LOW-RISK NEUTROPENIC PATIENTS RATIONALE: It is increasingly being recognised that not all neutropenic patients have the same risk of complications during episodes
CARE PATHWAY FOR CHILDREN AND YOUNG PERSONS WITH FEBRILE NEUTROPENIA, NEUTROPENIC SEPSIS OR SUSPECTED CENTRAL VENOUS LINE INFECTIONS
 CARE PATHWAY FOR CHILDREN AND YOUNG PERSONS WITH FEBRILE NEUTROPENIA, NEUTROPENIC SEPSIS OR SUSPECTED CENTRAL VENOUS LINE INFECTIONS This Care Pathway has been developed by a multidisciplinary team. It
CARE PATHWAY FOR CHILDREN AND YOUNG PERSONS WITH FEBRILE NEUTROPENIA, NEUTROPENIC SEPSIS OR SUSPECTED CENTRAL VENOUS LINE INFECTIONS This Care Pathway has been developed by a multidisciplinary team. It
Ventilatory support in cancer patients
 Ventilatory support in cancer patients D. Benoit, MD, PhD Department of Intensive Care Medicine Ghent University Hospital La ventilation non-invasive (VNI) réduit le risque d intubation et la mortalité
Ventilatory support in cancer patients D. Benoit, MD, PhD Department of Intensive Care Medicine Ghent University Hospital La ventilation non-invasive (VNI) réduit le risque d intubation et la mortalité
Severe Dengue Infection in ICU. Shirish Prayag MD, FCCM Pune, India
 Severe Dengue Infection in ICU Shirish Prayag MD, FCCM Pune, India Greetings from India Declaration Honararia from MSD, Astra Zenecea, Fresenius Kabi, Pfizer, Intas, Glenmark for conducting lectures. No
Severe Dengue Infection in ICU Shirish Prayag MD, FCCM Pune, India Greetings from India Declaration Honararia from MSD, Astra Zenecea, Fresenius Kabi, Pfizer, Intas, Glenmark for conducting lectures. No
End of Life Care in IJN Our journey. Dato Dr. David Chew Soon Ping Consultant Cardiologist National Heart Institute Malaysia
 End of Life Care in IJN Our journey Dato Dr. David Chew Soon Ping Consultant Cardiologist National Heart Institute Malaysia End of Life Dying is final part of everyone journey in life Deaths used to occur
End of Life Care in IJN Our journey Dato Dr. David Chew Soon Ping Consultant Cardiologist National Heart Institute Malaysia End of Life Dying is final part of everyone journey in life Deaths used to occur
What s New in Acute COPD? Dr Nick Scriven Consultant AIM President SAM
 What s New in Acute COPD? Dr Nick Scriven Consultant AIM President SAM Covering: Basic Definition New assessment criteria Some newer treatments BiPAP Not Covering: Definitions: Chronic Obstructive Pulmonary
What s New in Acute COPD? Dr Nick Scriven Consultant AIM President SAM Covering: Basic Definition New assessment criteria Some newer treatments BiPAP Not Covering: Definitions: Chronic Obstructive Pulmonary
TACO CASE STUDIES RTC JUNE Kerry Dowling Blood Transfusion Laboratory Manager Jonathan Ricks Blood Transfusion Nurse Practitioner
 TACO CASE STUDIES RTC JUNE 2017 Kerry Dowling Blood Transfusion Laboratory Manager Jonathan Ricks Blood Transfusion Nurse Practitioner RISK FACTORS - TACO Age over 70 years although also seen in younger
TACO CASE STUDIES RTC JUNE 2017 Kerry Dowling Blood Transfusion Laboratory Manager Jonathan Ricks Blood Transfusion Nurse Practitioner RISK FACTORS - TACO Age over 70 years although also seen in younger
Acute NIV in COPD and what happens next. Dr Rachael Evans PhD Associate Professor, Respiratory Medicine, Glenfield Hospital
 Acute NIV in COPD and what happens next Dr Rachael Evans PhD Associate Professor, Respiratory Medicine, Glenfield Hospital Content Scenarios Evidence based medicine for the first 24 hrs Who should we refer
Acute NIV in COPD and what happens next Dr Rachael Evans PhD Associate Professor, Respiratory Medicine, Glenfield Hospital Content Scenarios Evidence based medicine for the first 24 hrs Who should we refer
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdomen, acute, in oncological surgery patients, critical care issues in, 101 102 Acquired factor VIII inhibitors, in critically ill cancer
Index Note: Page numbers of article titles are in boldface type. A Abdomen, acute, in oncological surgery patients, critical care issues in, 101 102 Acquired factor VIII inhibitors, in critically ill cancer
Approach to type 2 Respiratory Failure
 Approach to type 2 Respiratory Failure Changing Nature of NIV Not longer just the traditional COPD patients Increasingly Obesity Neuromuscular Pneumonias 3 fold increase in patients with Ph 7.25 and below
Approach to type 2 Respiratory Failure Changing Nature of NIV Not longer just the traditional COPD patients Increasingly Obesity Neuromuscular Pneumonias 3 fold increase in patients with Ph 7.25 and below
Should we admit these patients to the ICU? Triage, boundaries and outcomes
 1 Triage, boundaries and outcomes Filomena Faria filomena.faria@ipoporto.min-saude.pt Serviço de Cuidados Intensivos, IPO Porto FG EPE 2 Topics: #1 Introduction; #2 Epidemiology; #3 Triage; #4 Boundaries;
1 Triage, boundaries and outcomes Filomena Faria filomena.faria@ipoporto.min-saude.pt Serviço de Cuidados Intensivos, IPO Porto FG EPE 2 Topics: #1 Introduction; #2 Epidemiology; #3 Triage; #4 Boundaries;
Reducing the Door to Needle Time for Antibiotics in Suspected Neutropenic Sepsis using a Dedicated Clinical Pathway
 Reducing the Door to Needle Time for Antibiotics in Suspected Neutropenic Sepsis using a Dedicated Clinical Pathway Dr Alex Williams, Oncology Specialty Doctor. Cheltenham General Hospital Oncology Centre
Reducing the Door to Needle Time for Antibiotics in Suspected Neutropenic Sepsis using a Dedicated Clinical Pathway Dr Alex Williams, Oncology Specialty Doctor. Cheltenham General Hospital Oncology Centre
National Emergency Laparotomy Audit. Help Box Text
 National Emergency Laparotomy Audit Help Box Text Version Control Version 1.1 06/12/13 1.2 13/12/13 1.3 20/12/13 1.4 20/01/14 1.5 30/01/14 1.6 13/03/14 1.7 07/04/14 1.8 01/12/14 1.9 05/05/15 1.10 02/07/15
National Emergency Laparotomy Audit Help Box Text Version Control Version 1.1 06/12/13 1.2 13/12/13 1.3 20/12/13 1.4 20/01/14 1.5 30/01/14 1.6 13/03/14 1.7 07/04/14 1.8 01/12/14 1.9 05/05/15 1.10 02/07/15
MAKING SENSE OF IT ALL AUGUST 17
 MAKING SENSE OF IT ALL AUGUST 17 @SepsisUK Dr Ron Daniels B.E.M. CEO, UK Sepsis Trust CEO, Global Sepsis Alliance Special Adviser to WHO SCALE AND BURDEN @sepsisuk Dr Ron Daniels B.E.M. CEO, UK Sepsis
MAKING SENSE OF IT ALL AUGUST 17 @SepsisUK Dr Ron Daniels B.E.M. CEO, UK Sepsis Trust CEO, Global Sepsis Alliance Special Adviser to WHO SCALE AND BURDEN @sepsisuk Dr Ron Daniels B.E.M. CEO, UK Sepsis
Rapid Response Teams and End-of-Life Care. James Downar, MDCM, MHSc, FRCPC Critical Care and Palliative Care, University Health Network, Toronto
 Rapid Response Teams and End-of-Life Care James Downar, MDCM, MHSc, FRCPC Critical Care and Palliative Care, University Health Network, Toronto Conflicts of Interest To place your ad here, please call
Rapid Response Teams and End-of-Life Care James Downar, MDCM, MHSc, FRCPC Critical Care and Palliative Care, University Health Network, Toronto Conflicts of Interest To place your ad here, please call
Patient Experience Research in Malignant Hematology: describing the lived experience of illness with acute myeloid leukemia
 Patient Experience Research in Malignant Hematology: describing the lived experience of illness with acute myeloid leukemia Thomas W. LeBlanc, MD, MA, MHS, FAAHPM Associate Professor of Medicine Division
Patient Experience Research in Malignant Hematology: describing the lived experience of illness with acute myeloid leukemia Thomas W. LeBlanc, MD, MA, MHS, FAAHPM Associate Professor of Medicine Division
Large observational study to UNderstand the Global impact of Severe Acute respiratory FailurE (LUNG-SAFE)
") Large observational study to UNderstand the Global impact of Severe Acute respiratory FailurE (LUNG-SAFE) John Laffey, Giacomo Bellani, Tai Pham, Eddy Fan, Antonio Pesenti on behalf of the LUNG SAFE Investigators
Large observational study to UNderstand the Global impact of Severe Acute respiratory FailurE (LUNG-SAFE) John Laffey, Giacomo Bellani, Tai Pham, Eddy Fan, Antonio Pesenti on behalf of the LUNG SAFE Investigators
The use of proning in the management of Acute Respiratory Distress Syndrome
 Case 3 The use of proning in the management of Acute Respiratory Distress Syndrome Clinical Problem This expanded case summary has been chosen to explore the rationale and evidence behind the use of proning
Case 3 The use of proning in the management of Acute Respiratory Distress Syndrome Clinical Problem This expanded case summary has been chosen to explore the rationale and evidence behind the use of proning
Acute Oncology: Service Provision in Smaller Cancer Centres Ernie Marshall Clatterbridge Centre for Oncology
 Acute Oncology: Service Provision in Smaller Cancer Centres Ernie Marshall Clatterbridge Centre for Oncology Whiston Hospital St Helen s Hospital 350,000 population ~1000 beds Regional Plastics Unit DGH
Acute Oncology: Service Provision in Smaller Cancer Centres Ernie Marshall Clatterbridge Centre for Oncology Whiston Hospital St Helen s Hospital 350,000 population ~1000 beds Regional Plastics Unit DGH
Key statistics from the National Cardiac Arrest Audit: Paediatric arrests April 2012 to March 2017
 Key statistics from the National Cardiac Arrest Audit: Paediatric arrests April 12 to March 17 Supported by Resuscitation Council (UK) and Intensive Care National Audit & Research Centre (ICNARC) Data
Key statistics from the National Cardiac Arrest Audit: Paediatric arrests April 12 to March 17 Supported by Resuscitation Council (UK) and Intensive Care National Audit & Research Centre (ICNARC) Data
Adding Insult to Injury. Marlies Ostermann Consultant in Nephrology & Critical Care Guy s & St Thomas Hospital, London
 Acute Kidney Injury Adding Insult to Injury Marlies Ostermann Consultant in Nephrology & Critical Care Guy s & St Thomas Hospital, London Content 1. Brief review of AKI and its impact 2. Comments on the
Acute Kidney Injury Adding Insult to Injury Marlies Ostermann Consultant in Nephrology & Critical Care Guy s & St Thomas Hospital, London Content 1. Brief review of AKI and its impact 2. Comments on the
Is Bigger Better? Does PICU Volume Impact Volume
 Is Bigger Better? Does PICU Volume Impact Volume Brad Poss, MD, MMM Professor of Pediatrics Associate Dean for Graduate Medical Education University of Utah School of Medicine PICU Attending Physician
Is Bigger Better? Does PICU Volume Impact Volume Brad Poss, MD, MMM Professor of Pediatrics Associate Dean for Graduate Medical Education University of Utah School of Medicine PICU Attending Physician
Transfusion for the sickest ICU patients: Are there unanswered questions?
 Transfusion for the sickest ICU patients: Are there unanswered questions? Tim Walsh Professor of Critical Care Edinburgh University None Conflict of Interest Guidelines on the management of anaemia and
Transfusion for the sickest ICU patients: Are there unanswered questions? Tim Walsh Professor of Critical Care Edinburgh University None Conflict of Interest Guidelines on the management of anaemia and
Is nosocomial infection the major cause of death in sepsis?
 Is nosocomial infection the major cause of death in sepsis? Warren L. Lee, MD PhD, FRCPC Department of Medicine University of Toronto There are no specific therapies for sepsis the graveyard for pharmaceutical
Is nosocomial infection the major cause of death in sepsis? Warren L. Lee, MD PhD, FRCPC Department of Medicine University of Toronto There are no specific therapies for sepsis the graveyard for pharmaceutical
Alister Jones Patient Blood Management Practitioner NHS Blood and Transplant
 Alister Jones Patient Blood Management Practitioner NHS Blood and Transplant All medical RCC transfusions (but only 1 in 3 haematology or oncology cases) in 3 x one week periods Medical specialties include:
Alister Jones Patient Blood Management Practitioner NHS Blood and Transplant All medical RCC transfusions (but only 1 in 3 haematology or oncology cases) in 3 x one week periods Medical specialties include:
Sepsis 3.0: The Impact on Quality Improvement Programs
 Sepsis 3.0: The Impact on Quality Improvement Programs Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care Warren Alpert Medical School of Brown University
Sepsis 3.0: The Impact on Quality Improvement Programs Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care Warren Alpert Medical School of Brown University
COPD exacerbation. Dr. med. Frank Rassouli
 Definition according to GOLD report: - «An acute event - characterized by a worsening of the patients respiratory symptoms - that is beyond normal day-to-day variations - and leads to a change in medication»
Definition according to GOLD report: - «An acute event - characterized by a worsening of the patients respiratory symptoms - that is beyond normal day-to-day variations - and leads to a change in medication»
Update in Hospital Medicine
 Update in Hospital Medicine 2017-2018 Brad Sharpe, MD SFHM UCSF Division of Hospital Medicine 2017-2018 Updated literature March 2017 March 2018 Process: CME collaborative review of journals Including
Update in Hospital Medicine 2017-2018 Brad Sharpe, MD SFHM UCSF Division of Hospital Medicine 2017-2018 Updated literature March 2017 March 2018 Process: CME collaborative review of journals Including
What is Acute Oncology? Kay McCallum Acute Oncology Advanced Nurse Practitioner John Radcliffe Hospital Oxford September 2015
 What is Acute Oncology? Kay McCallum Acute Oncology Advanced Nurse Practitioner John Radcliffe Hospital Oxford September 2015 What is Acute Oncology? Outline of Talk Concept of Acute Oncology Service (AOS)
What is Acute Oncology? Kay McCallum Acute Oncology Advanced Nurse Practitioner John Radcliffe Hospital Oxford September 2015 What is Acute Oncology? Outline of Talk Concept of Acute Oncology Service (AOS)
Approach to Severe Sepsis. Jan Hau Lee, MBBS, MRCPCH. MCI Children s Intensive Care Unit KK Women s and Children's Hospital, Singapore
 Approach to Severe Sepsis Jan Hau Lee, MBBS, MRCPCH. MCI Children s Intensive Care Unit KK Women s and Children's Hospital, Singapore 1 2 No conflict of interest Overview Epidemiology of Pediatric Severe
Approach to Severe Sepsis Jan Hau Lee, MBBS, MRCPCH. MCI Children s Intensive Care Unit KK Women s and Children's Hospital, Singapore 1 2 No conflict of interest Overview Epidemiology of Pediatric Severe
ARDS during Neutropenia. D Mokart DAR IPC GRRRRROH 2010
 ARDS during Neutropenia D Mokart DAR IPC GRRRRROH 2010 Definitions Neutropenia is a decrease in circulating neutrophil white cells in the peripheral blood. neutrophil count of 1,000 1,500 cells/ml = mild
ARDS during Neutropenia D Mokart DAR IPC GRRRRROH 2010 Definitions Neutropenia is a decrease in circulating neutrophil white cells in the peripheral blood. neutrophil count of 1,000 1,500 cells/ml = mild
Emergency Department Overcrowding: Is Ambulatory Care the solution?
 Emergency Department Overcrowding: Is Ambulatory Care the solution? Tim Cooksley Consultant in Acute Medicine, UHSM and Honorary Consultant, The Christie @acutemed2 Overview ED Overcrowding The benefit
Emergency Department Overcrowding: Is Ambulatory Care the solution? Tim Cooksley Consultant in Acute Medicine, UHSM and Honorary Consultant, The Christie @acutemed2 Overview ED Overcrowding The benefit
Acute noninvasive ventilation what s the evidence? Respiratory Medicine Update: Royal College of Physicians & BTS Thu 28 th January 2016
 Acute noninvasive ventilation what s the evidence? Respiratory Medicine Update: Royal College of Physicians & BTS Thu 28 th January 2016 Annabel Nickol Consultant in Respiratory Medicine, Sleep & Ventilation
Acute noninvasive ventilation what s the evidence? Respiratory Medicine Update: Royal College of Physicians & BTS Thu 28 th January 2016 Annabel Nickol Consultant in Respiratory Medicine, Sleep & Ventilation
Assessing perioperative risk
 Assessing perioperative risk Chronic Obstructive Pulmonary Disease Dr. Michelle Caldecott Respiratory & Sleep Physician Epworth Healthcare Austin Health Impact of COPD on Postoperative Outcomes: Results
Assessing perioperative risk Chronic Obstructive Pulmonary Disease Dr. Michelle Caldecott Respiratory & Sleep Physician Epworth Healthcare Austin Health Impact of COPD on Postoperative Outcomes: Results
SAH READMISSIONS TO NCCU
 SAH READMISSIONS TO NCCU Are they preventable? João Amaral Rebecca Gorf Critical Care Outreach Team - NHNN 2015 Total admissions to NCCU =862 Total SAH admitted to NCCU= 104 (93e) (12.0%) Total SAH readmissions=
SAH READMISSIONS TO NCCU Are they preventable? João Amaral Rebecca Gorf Critical Care Outreach Team - NHNN 2015 Total admissions to NCCU =862 Total SAH admitted to NCCU= 104 (93e) (12.0%) Total SAH readmissions=
Use of surrogate inflammatory markers in the diagnosis & monitoring of patients with severe sepsis
 Thursday 11 th June 2015 Use of surrogate inflammatory markers in the diagnosis & monitoring of patients with severe sepsis Dr Duncan Wyncoll Guy s & St Thomas NHS Trust, London Conflicts of Interest In
Thursday 11 th June 2015 Use of surrogate inflammatory markers in the diagnosis & monitoring of patients with severe sepsis Dr Duncan Wyncoll Guy s & St Thomas NHS Trust, London Conflicts of Interest In
NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP)
") Introduction NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP) Noninvasive ventilation (NIV) is a method of delivering oxygen by positive pressure mask that allows for the prevention or postponement of invasive
Introduction NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP) Noninvasive ventilation (NIV) is a method of delivering oxygen by positive pressure mask that allows for the prevention or postponement of invasive
Escalations of Care The Impact of Delayed Diagnosis of Sepsis and Pneumonia
 #MakingEveryBreathCount Escalations of Care The Impact of Delayed Diagnosis of and Improving patient flow, improved healthcare economics Your hospital could be measuring respiratory rate incorrectly and
#MakingEveryBreathCount Escalations of Care The Impact of Delayed Diagnosis of and Improving patient flow, improved healthcare economics Your hospital could be measuring respiratory rate incorrectly and
The role of the Nephrologist in Acute Kidney Injury. Rebecca Brown Consultant Nephrologist Royal Liverpool University Hospital
 The role of the Nephrologist in Acute Kidney Injury Rebecca Brown Consultant Nephrologist Royal Liverpool University Hospital Overview Impact of AKI Need for change Who needs a Nephrologist Are we making
The role of the Nephrologist in Acute Kidney Injury Rebecca Brown Consultant Nephrologist Royal Liverpool University Hospital Overview Impact of AKI Need for change Who needs a Nephrologist Are we making
1.1.2 CPAP therapy is used for patients who are suffering from an acute type 1 respiratory failure (Pa02 <8kPa with a normal or low Pac02).
.") Guidelines for initiating and managing CPAP (Continuous Positive Airway Pressure) on a general ward. B25/2006 1.Introduction and Who Guideline applies to 1.1.1 This document provides guidance for Healthcare
Guidelines for initiating and managing CPAP (Continuous Positive Airway Pressure) on a general ward. B25/2006 1.Introduction and Who Guideline applies to 1.1.1 This document provides guidance for Healthcare
Hospice and Palliative Care An Essential Component of the Aging Services Network
 Hospice and Palliative Care An Essential Component of the Aging Services Network Howard Tuch, MD, MS American Academy of Hospice and Palliative Medicine Physician Advocate, American Academy of Hospice
Hospice and Palliative Care An Essential Component of the Aging Services Network Howard Tuch, MD, MS American Academy of Hospice and Palliative Medicine Physician Advocate, American Academy of Hospice
CareFirst Hospice. Health care for the end of life. CareFirst
 Hospice Health care for the end of life 1 What is Hospice? Hospice is a philosophy- When a person in end stages of an illness can no longer receive, or wants to receive, life sustaining treatment, he or
Hospice Health care for the end of life 1 What is Hospice? Hospice is a philosophy- When a person in end stages of an illness can no longer receive, or wants to receive, life sustaining treatment, he or
The Role of Observation Care in the Evaluation and Management of Cancer Emergencies
 The Role of Observation Care in the Evaluation and Management of Cancer Emergencies Adam Klotz, MD Associate Attending Physician Memorial Sloan Kettering Cancer Center FACULTY DISCLOSURE Nothing to disclose
The Role of Observation Care in the Evaluation and Management of Cancer Emergencies Adam Klotz, MD Associate Attending Physician Memorial Sloan Kettering Cancer Center FACULTY DISCLOSURE Nothing to disclose
Intensive care in the very old. Hans Flaatten
 Intensive care in the very old Hans Flaatten What is considered old and very old? WHO definition Old 60, suggested 65 in developed countries Very old No accepted definition 75 and 80 are often used as
Intensive care in the very old Hans Flaatten What is considered old and very old? WHO definition Old 60, suggested 65 in developed countries Very old No accepted definition 75 and 80 are often used as
Retrospective analysis of outcome of women with breast or gynaecological cancer in the intensive care unit
 RESEARCH Retrospective analysis of outcome of women with breast or gynaecological cancer in the intensive care unit Marlies Ostermann 1 Mario Raimundo 1,2 Anna Williams 1 Craig Whiteley 1 Richard Beale
RESEARCH Retrospective analysis of outcome of women with breast or gynaecological cancer in the intensive care unit Marlies Ostermann 1 Mario Raimundo 1,2 Anna Williams 1 Craig Whiteley 1 Richard Beale
Sleep Apnea and ifficulty in Extubation. Jean Louis BOURGAIN May 15, 2016
 Sleep Apnea and ifficulty in Extubation Jean Louis BOURGAIN May 15, 2016 Introduction Repetitive collapse of the upper airway > sleep fragmentation, > hypoxemia, hypercapnia, > marked variations in intrathoracic
Sleep Apnea and ifficulty in Extubation Jean Louis BOURGAIN May 15, 2016 Introduction Repetitive collapse of the upper airway > sleep fragmentation, > hypoxemia, hypercapnia, > marked variations in intrathoracic
Non-invasive Positive Pressure Mechanical Ventilation: NIPPV: CPAP BPAP IPAP EPAP. My Real Goals. What s new in 2018? OMG PAP?
 Non-invasive Positive Pressure Mechanical Ventilation: What s new in 2018? Geoffrey R. Connors, MD, FACP Associate Professor of Medicine University of Colorado School of Medicine Division of Pulmonary
Non-invasive Positive Pressure Mechanical Ventilation: What s new in 2018? Geoffrey R. Connors, MD, FACP Associate Professor of Medicine University of Colorado School of Medicine Division of Pulmonary
What is sepsis? RECOGNITION. Sepsis I Know It When I See It 9/21/2017
 Sepsis I Know It When I See It September 15, 2017 Matthew Exline, MD MPH Medical Director, Medical ICU What is sepsis? I shall not today attempt further to define the kinds of material [b]ut I know it
Sepsis I Know It When I See It September 15, 2017 Matthew Exline, MD MPH Medical Director, Medical ICU What is sepsis? I shall not today attempt further to define the kinds of material [b]ut I know it
6. Endovascular aneurysm repair
 Introduction The standard treatment for aortic aneurysm, open repair, involves a large abdominal incision and cross-clamping of the aorta. In recent years, a minimally invasive technique, endovascular
Introduction The standard treatment for aortic aneurysm, open repair, involves a large abdominal incision and cross-clamping of the aorta. In recent years, a minimally invasive technique, endovascular
How hematologists perceive critical care- Acute myeloid leukemia
 How hematologists perceive critical care- Acute myeloid leukemia Groupe de Recherche Respiratoire en Réanimation Onco-Hématologique Research Meeting June 30 th 2011 Peter Schellongowski Intensive Care
How hematologists perceive critical care- Acute myeloid leukemia Groupe de Recherche Respiratoire en Réanimation Onco-Hématologique Research Meeting June 30 th 2011 Peter Schellongowski Intensive Care
Ischemic Stroke in Critically Ill Patients with Malignancy
 Ischemic Stroke in Critically Ill Patients with Malignancy Jeong-Am Ryu 1, Oh Young Bang 2, Daesang Lee 1, Jinkyeong Park 1, Jeong Hoon Yang 1, Gee Young Suh 1, Joongbum Cho 1, Chi Ryang Chung 1, Chi-Min
Ischemic Stroke in Critically Ill Patients with Malignancy Jeong-Am Ryu 1, Oh Young Bang 2, Daesang Lee 1, Jinkyeong Park 1, Jeong Hoon Yang 1, Gee Young Suh 1, Joongbum Cho 1, Chi Ryang Chung 1, Chi-Min
Supplementary Online Content
 Supplementary Online Content Yunos NM, Bellomo R, Hegarty C, Story D, Ho L, Bailey M. Association between a chloride-liberal vs chloride-restrictive intravenous fluid administration strategy and kidney
Supplementary Online Content Yunos NM, Bellomo R, Hegarty C, Story D, Ho L, Bailey M. Association between a chloride-liberal vs chloride-restrictive intravenous fluid administration strategy and kidney
ECMO in oncology and immunosupressed patients. Peter Schellongowski Department of Medicine I Intensive Care Unit 13.i2 Medical University of Vienna
 ECMO in oncology and immunosupressed patients Peter Schellongowski Department of Medicine I Intensive Care Unit 13.i2 Medical University of Vienna ECMO in immunocompromised patients? Is it feasible? Is
ECMO in oncology and immunosupressed patients Peter Schellongowski Department of Medicine I Intensive Care Unit 13.i2 Medical University of Vienna ECMO in immunocompromised patients? Is it feasible? Is
OHSU. Update in Sepsis
 Update in Sepsis Jonathan Pak, MD June 1, 2017 Structure of Talk 1. Sepsis-3: The latest definition 2. Clinical Management - Is EGDT dead? - Surviving Sepsis Campaign Guidelines 3. A novel therapy: Vitamin
Update in Sepsis Jonathan Pak, MD June 1, 2017 Structure of Talk 1. Sepsis-3: The latest definition 2. Clinical Management - Is EGDT dead? - Surviving Sepsis Campaign Guidelines 3. A novel therapy: Vitamin
Landmark articles on ventilation
 Landmark articles on ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity ARDS AECC DEFINITION-1994 ALI Acute onset Bilateral chest infiltrates PCWP
Landmark articles on ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity ARDS AECC DEFINITION-1994 ALI Acute onset Bilateral chest infiltrates PCWP
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Suntharalingam G, Perry MR, Ward S, et al. Cytokine storm in
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Suntharalingam G, Perry MR, Ward S, et al. Cytokine storm in
Physiotherapy on the Intensive Care Unit. Information for patients, their family and carers
 Physiotherapy on the Intensive Care Unit Information for patients, their family and carers A team of Specialist Physiotherapists works in the Intensive Care Units within the Oxford University Hospitals
Physiotherapy on the Intensive Care Unit Information for patients, their family and carers A team of Specialist Physiotherapists works in the Intensive Care Units within the Oxford University Hospitals
Transfusion & Mortality. Philippe Van der Linden MD, PhD
 Transfusion & Mortality Philippe Van der Linden MD, PhD Conflict of Interest Disclosure In the past 5 years, I have received honoraria or travel support for consulting or lecturing from the following companies:
Transfusion & Mortality Philippe Van der Linden MD, PhD Conflict of Interest Disclosure In the past 5 years, I have received honoraria or travel support for consulting or lecturing from the following companies:
Mortality Rate was unsightly!!! 4/24/2013. Sepsis Quality Improvement Project
 Libby, MT Sepsis Quality Improvement Project Barb Dumont RN, Director of Quality and Risk Management Mike Julius RN, ED Manager Cathy Wolfe RN, Chief Nursing Officer. Mortality Rate was unsightly!!! percent
Libby, MT Sepsis Quality Improvement Project Barb Dumont RN, Director of Quality and Risk Management Mike Julius RN, ED Manager Cathy Wolfe RN, Chief Nursing Officer. Mortality Rate was unsightly!!! percent
PALLIATIVE MEDICINE Nigel Sykes St Christopher s Hospice London UK
 Guttmann Conference June 2013 PALLIATIVE MEDICINE Nigel Sykes St Christopher s Hospice London UK Palliative Medicine What is Palliative Medicine and where did it come from? The extent and organisation
Guttmann Conference June 2013 PALLIATIVE MEDICINE Nigel Sykes St Christopher s Hospice London UK Palliative Medicine What is Palliative Medicine and where did it come from? The extent and organisation
Management of the Cirrhotic Patient in the ICU
 Management of the Cirrhotic Patient in the ICU Peter E. Morris, MD Professor & Chief, Pulmonary, Critical Care and Sleep Medicine University of Kentucky Conflict of Interest Funding US National Institutes
Management of the Cirrhotic Patient in the ICU Peter E. Morris, MD Professor & Chief, Pulmonary, Critical Care and Sleep Medicine University of Kentucky Conflict of Interest Funding US National Institutes
Palliative Care & Haematology: Known Unknowns or Unknown Unknowns? Working towards a better collaboration.
 Palliative Care & Haematology: Known Unknowns or Unknown Unknowns? Working towards a better collaboration. Dr Michelle Gold Director, Palliative Care Alfred Health ANZSPM Update June 2013 % Epidemiology
Palliative Care & Haematology: Known Unknowns or Unknown Unknowns? Working towards a better collaboration. Dr Michelle Gold Director, Palliative Care Alfred Health ANZSPM Update June 2013 % Epidemiology
The Sepsis Timebomb. James Wigfull Critical Care and Anaesthesia Sheffield Teaching Hospitals
 The Sepsis Timebomb James Wigfull Critical Care and Anaesthesia Sheffield Teaching Hospitals Relationship of SIRS, Sepsis and Infection BACTEREMIA PANCREATITIS INFECTION FUNGEMIA PARASITEMIA VIREMIA SEPSIS
The Sepsis Timebomb James Wigfull Critical Care and Anaesthesia Sheffield Teaching Hospitals Relationship of SIRS, Sepsis and Infection BACTEREMIA PANCREATITIS INFECTION FUNGEMIA PARASITEMIA VIREMIA SEPSIS
Andrea Blotsky MDCM FRCPC General Internal Medicine, McGill University Thursday, October 15, 2015
 The TIMES Project: (Time to Initiation of Antibiotic Therapy in Medical Patients Presenting to the Emergency Department with Sepsis) - Preliminary Findings Andrea Blotsky MDCM FRCPC General Internal Medicine,
The TIMES Project: (Time to Initiation of Antibiotic Therapy in Medical Patients Presenting to the Emergency Department with Sepsis) - Preliminary Findings Andrea Blotsky MDCM FRCPC General Internal Medicine,
Year in Review: Critical Care Medicine
 Year in Review: Critical Care Medicine No disclosures Eric J. Seeley, M.D. Assistant Professor of Medicine Division of Pulmonary and Critical Care Medicine Why I Selected These Studies High quality studies
Year in Review: Critical Care Medicine No disclosures Eric J. Seeley, M.D. Assistant Professor of Medicine Division of Pulmonary and Critical Care Medicine Why I Selected These Studies High quality studies
King s College Hospital NHS Foundation Trust. Acute on Chronic Liver Failure: Practical management outside the tertiary centre.
 King s College Hospital NHS Foundation Trust NHS Acute on Chronic Liver Failure: Practical management outside the tertiary centre. William Bernal Professor of Liver Critical Care Liver Intensive Therapy
King s College Hospital NHS Foundation Trust NHS Acute on Chronic Liver Failure: Practical management outside the tertiary centre. William Bernal Professor of Liver Critical Care Liver Intensive Therapy
Anaesthesia for the Over 75s. Chris Edge
 Anaesthesia for the Over 75s Chris Edge Topics to be Covered Post-operative cognitive management Morbidity and mortality General anaesthesia a good idea or not? Multiple comorbidities and assessment of
Anaesthesia for the Over 75s Chris Edge Topics to be Covered Post-operative cognitive management Morbidity and mortality General anaesthesia a good idea or not? Multiple comorbidities and assessment of
(Non)-invasive ventilation: transition from PICU to home. Christian Dohna-Schwake
-invasive ventilation: transition from PICU to home. Christian Dohna-Schwake") (Non)-invasive ventilation: transition from PICU to home Christian Dohna-Schwake Increased use of NIV in PICUs over last 15 years First choice of respiratory support in many diseases Common temporary indications:
(Non)-invasive ventilation: transition from PICU to home Christian Dohna-Schwake Increased use of NIV in PICUs over last 15 years First choice of respiratory support in many diseases Common temporary indications:
Accelero Identifies Opportunities to Provide Greater Value in Hip Fracture Care
 Accelero Health Partners, 2015 WHITE PAPER Accelero Identifies Opportunities to Provide Greater Value in Hip Fracture Care Jason Pry, Senior Director ABSTRACT Every year more than a quarter of a million
Accelero Health Partners, 2015 WHITE PAPER Accelero Identifies Opportunities to Provide Greater Value in Hip Fracture Care Jason Pry, Senior Director ABSTRACT Every year more than a quarter of a million
End of life. care planning. in dementia. Dr Victor Pace St Christopher s Hospice February 2018
 Dr Victor Pace St Christopher s Hospice February 2018 It s making the headlines Why does advance matter in dementia? Why does this matter? Since 2015, dementia has become the leading cause of death in
Dr Victor Pace St Christopher s Hospice February 2018 It s making the headlines Why does advance matter in dementia? Why does this matter? Since 2015, dementia has become the leading cause of death in
9 Diabetes care. Back to contents
 Back to contents Diabetes is a major risk factor for the development of peripheral vascular disease and 349/628 (55.6%) of the patients in this study had diabetes. Hospital inpatients with diabetes are
Back to contents Diabetes is a major risk factor for the development of peripheral vascular disease and 349/628 (55.6%) of the patients in this study had diabetes. Hospital inpatients with diabetes are
Prioritasing services in hospital
 Prioritasing services in hospital Admission to, utilisation of and discharge from services Capacity in services can be created through the active management of admissions and discharges in conjunction
Prioritasing services in hospital Admission to, utilisation of and discharge from services Capacity in services can be created through the active management of admissions and discharges in conjunction
Best of Pulmonary Jennifer R. Hucks, MD University of South Carolina School of Medicine
 Best of Pulmonary 2012-2013 Jennifer R. Hucks, MD University of South Carolina School of Medicine Topics ARDS- Berlin Definition Prone Positioning For ARDS Lung Protective Ventilation In Patients Without
Best of Pulmonary 2012-2013 Jennifer R. Hucks, MD University of South Carolina School of Medicine Topics ARDS- Berlin Definition Prone Positioning For ARDS Lung Protective Ventilation In Patients Without
2016 Top Papers in Critical Care
 2016 Top Papers in Critical Care Briana Witherspoon DNP, APRN, ACNP-BC Assistant Director of Advanced Practice, Neuroscience Assistant in Division of Critical Care, Department of Anesthesiology Neuroscience
2016 Top Papers in Critical Care Briana Witherspoon DNP, APRN, ACNP-BC Assistant Director of Advanced Practice, Neuroscience Assistant in Division of Critical Care, Department of Anesthesiology Neuroscience
Recent Advances in Respiratory Medicine
 Recent Advances in Respiratory Medicine Dr. R KUMAR Pulmonologist Non Invasive Ventilation (NIV) NIV Noninvasive ventilation (NIV) refers to the administration of ventilatory support without using an invasive
Recent Advances in Respiratory Medicine Dr. R KUMAR Pulmonologist Non Invasive Ventilation (NIV) NIV Noninvasive ventilation (NIV) refers to the administration of ventilatory support without using an invasive
Palliative Care: A Place on the Quality Scorecard?
 Palliative Care: A Place on the Quality Scorecard? J. Randall Curtis, MD, MPH Professor of Medicine Director, Palliative Care Center of Excellence www.uwpalliativecarecenter.com Disclosures and Funding
Palliative Care: A Place on the Quality Scorecard? J. Randall Curtis, MD, MPH Professor of Medicine Director, Palliative Care Center of Excellence www.uwpalliativecarecenter.com Disclosures and Funding
Keeping Patients Off the Vent: Bilevel, HFNC, Neither?
 Keeping Patients Off the Vent: Bilevel, HFNC, Neither? Robert Kempainen, MD Pulmonary and Critical Care Medicine Hennepin County Medical Center University of Minnesota School of Medicine Objectives Summarize
Keeping Patients Off the Vent: Bilevel, HFNC, Neither? Robert Kempainen, MD Pulmonary and Critical Care Medicine Hennepin County Medical Center University of Minnesota School of Medicine Objectives Summarize
The role of palliative care in non-malignant disease
 The role of palliative care in non-malignant disease Dr. Tony O Brien Consultant Physician in Palliative Medicine Marymount Hospice & Cork University Hospital School of Medicine, University College, Cork
The role of palliative care in non-malignant disease Dr. Tony O Brien Consultant Physician in Palliative Medicine Marymount Hospice & Cork University Hospital School of Medicine, University College, Cork
Accelero Identifies Opportunities to Provide Greater Value in Hip Fracture Care
 Accelero Identifies Opportunities to Provide Greater Value in Hip Fracture Care Every year more than a quarter of a million people over the age of 65 are admitted to a hospital with a hip fracture. Mortality
Accelero Identifies Opportunities to Provide Greater Value in Hip Fracture Care Every year more than a quarter of a million people over the age of 65 are admitted to a hospital with a hip fracture. Mortality
Update in Critical Care Medicine
 Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
UPDATE IN HOSPITAL MEDICINE
 UPDATE IN HOSPITAL MEDICINE FLORIDA CHAPTER ACP MEETING 2016 Himangi Kaushal, M.D., F.A.C.P. Program Director Memorial Healthcare System Internal Medicine Residency DISCLOSURES None OBJECTIVES Review some
UPDATE IN HOSPITAL MEDICINE FLORIDA CHAPTER ACP MEETING 2016 Himangi Kaushal, M.D., F.A.C.P. Program Director Memorial Healthcare System Internal Medicine Residency DISCLOSURES None OBJECTIVES Review some
The MET reduces cardiac arrests. Dr Daryl Jones
 The MET reduces cardiac arrests Dr Daryl Jones Overview Epidemiology of in-hospital arrests Failings of traditional model of care Principles of the MET Evidence from single centre studies Meta-analysis
The MET reduces cardiac arrests Dr Daryl Jones Overview Epidemiology of in-hospital arrests Failings of traditional model of care Principles of the MET Evidence from single centre studies Meta-analysis
Critical Illness and Homelessness
 Critical Illness and Homelessness Jan O Friedrich, MD DPhil Associate Professor of Medicine, University of Toronto Medical Director, MSICU St. Michael s Hospital, Toronto, Canada Critical Care Canada Forum
Critical Illness and Homelessness Jan O Friedrich, MD DPhil Associate Professor of Medicine, University of Toronto Medical Director, MSICU St. Michael s Hospital, Toronto, Canada Critical Care Canada Forum
Inflammatory Statements
 Inflammatory Statements Using ETCO 2 Analysis in Sepsis Syndromes George A. Ralls M.D. Orange County EMS System Sepsis Sepsis Over 750,000 cases annually Expected growth of 1.5% per year Over 215,000 deaths
Inflammatory Statements Using ETCO 2 Analysis in Sepsis Syndromes George A. Ralls M.D. Orange County EMS System Sepsis Sepsis Over 750,000 cases annually Expected growth of 1.5% per year Over 215,000 deaths
SECTION 1: INCLUSION/EXCLUSION CRITERIA INCLUSION CRITERIA Please put a cross in the Yes or No box for each question
 Site Number Patient s Initials SECTION 1: INCLUSION/EXCLUSION CRITERIA INCLUSION CRITERIA Please put a cross in the Yes or No box for each question Yes No 1.1 Is the patient receiving invasive mechanical
Site Number Patient s Initials SECTION 1: INCLUSION/EXCLUSION CRITERIA INCLUSION CRITERIA Please put a cross in the Yes or No box for each question Yes No 1.1 Is the patient receiving invasive mechanical