COPD exacerbation. Dr. med. Frank Rassouli
|
|
|
- Sydney Patterson
- 5 years ago
- Views:
Transcription
1
2 Definition according to GOLD report: - «An acute event - characterized by a worsening of the patients respiratory symptoms - that is beyond normal day-to-day variations - and leads to a change in medication»
3 - No biomarker and no diagnostic test to prove this diagnosis Clinical diagnosis of exclusion - Lead to acceleration of lung function decline! - Underreported / underrecognized - Seasonality

4 Cardinal symptoms (one or more fulfilled) - More dyspnea key symptom - More cough - More sputum - Changed sputum character / purulence

 - Severe:")
5 Classification - Mild: intensified inhalation only - Moderate: + corticosteroids (antibiotics) - Severe: hospitalisation
6 Risk factors - Age - Productive cough / chronic bronchitis - Duration of COPD - History of antibiotic therapy - COPD-related hospitalization previous year - Chronic mucous hypersecretion - Eosinophils > 0.34 x 10 9 cells per liter - Comorbidities - Low FEV1 - GERD - probably - Strongest predictor: history of prior exacerbations
7 Triggers/etiology - 70% respiratory tract infections: mostly viral and bacterial, atypical bacteria uncommon - 30% environmental pollution or unknown etiology
,")
8 Triggers/etiology viruses - Detected in up to 2/3 of exacerbations - Rhinovirus most common - Other: Influenza, parainfluenza, coronavirus, adenovirus, RSV, human metapneumovirus - Identification not proving cause (15% in stable COPD), except Influenza

9 Triggers/etiology bacteria % cause of exacerbation - Exacerbations: strongly associated with acquisition of new strain!
10 Triggers/etiology atypical bacteria - Chlamydia pneumoniae - Mycoplasma pneumoniae - Legionella spp rare causes!
11 Triggers/etiology viral and bacterial coinfection - Common - Increases severity - «Sequential infection» = bacterial infection after preceeding viral infection

12 Clinical manifestations - Extremely broad spectrum! - Mild increase of symptoms - respiratory failure
13 Physical examination - Wheezing - Tachypnea - Difficulty speaking - Use of accessory respiratory muscles - Paradoxical chest wall/abdominal movements - Decreased mental status hypercapnia/hypoxemia?
14 Goals of initial evaluation - Confirm diagnosis (exclude DD) - Identify cause (when possible) - Assess severity - Respect comorbidities
: clinical")



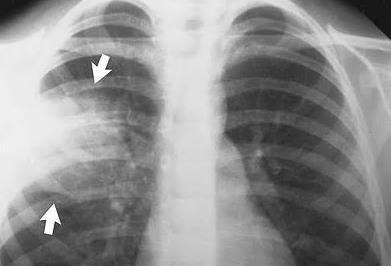
15 Initial evaluation Mild exacerbation (no ED admission): clinical assessment, maybe SpO 2 ED admission: - SpO 2 - Chest radiograph (pneumonia? pneumothorax? pulmonary edema? pleural effusion?) - Laboratory studies - ABGA - Additional tests depend. on clinical evaluation, e.g. ECG, troponin, BNP, D-dimer
16 Initial evaluation for infection Clinical indicators of bacterial infection: - More severe COPD - Sputum purulence Sputum studies (Gram stain, culture) when? - Risk factors for Pseudomonas - Failure to improve on initial empiric antibiotics - Acute respiratory failure
17 Initial evaluation for infection Detection of viruses: - Goal: detect influenza during season - Use of detection of other viruses not clear no specific treatment Procalcitonin (PCT) and CRP: - CRP: not recommended to differentiate between viral and bacterial etiology - PCT: more specific for bacterial infection still expensive and not readily available (globally) PCT-guidance: reduces antibiotic exposure and side effects, same clinical efficacy

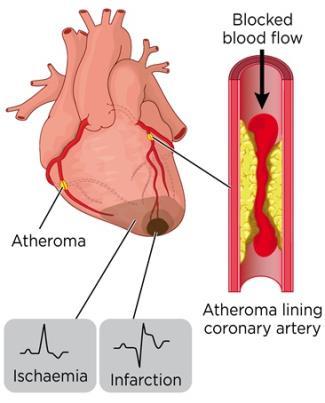


18 Differential diagnosis (main) - Heart failure - Acute coronary syndrome - Pulmonary embolism - Pneumonia - Pneumothorax
19 Triage Immediate intubation necessary? Intubation, ICU Yes No Severe dyspnea with clinical signs of respiratory failure? No Yes Yes ABGA: ph < 7.35 AND PaCO 2 > 6 kpa? Yes Contraindication for NIV? Yes No Other indication for ICU? No Start NIV, close monitoring. NIV-failure? No ICU Yes No Insufficient response to initial office/ed care? No Continue NIV, close monitoring Yes Other indication for hospitalization? Yes No Medical ward Outpatient management (>80%)
20 Goals of treatment 1. Minimize the negative impact of current exacerbation 2. Prevent subsequent events
21 Outpatient management 1. Intensification of bronchodilator therapy (SABA/SAMA; nebulized or MDI)
22 Outpatient management 1. Intensification of bronchodilator therapy (SABA/SAMA; nebulized or MDI) 2. Oral glucocorticoid therapy (Prednisone 40 mg/d for 5 days) Less dyspnea Greater improvement of FEV1
23 Outpatient management 3. Antibiotics?
24 Hospital management 1. Same measures as outpatient + 2. ABGA 3. Supplemental oxygen: target SpO % 4. Close monitoring (respiratory rate/effort, wheezing, SpO 2, HR, fluid status) 5. Maybe mechanical ventilation 6. Prevent complications of immobility (thromboembolism, deconditioning) 7. Improve nutritional status 8. Smokers: aid with smoking cessation
25 Hospital management systemic glucocorticoids - Improve symptoms - Improve lung function - Improve oxygenation - Decrease LOS - Reduce treatment failure - Reduce relapse
26 Hospital management systemic glucocorticoids Main side effect: Route: Dose: hyperglycemia mostly oral optimal dose unknown; GOLD: 40 mg prednisone equivalent/d; clinical practice: higher doses/i.v. in more severe cases (data limited)
27 Hospital management systemic glucocorticoids Duration: - Optimal duration not known - Depends on severity and response to therapy - GOLD: 5 days ( REDUCE trial, Leuppi et al., JAMA 2013) - ERS/ATS: 5-14 days - Tapering not necessary if < 2 weeks
28 Antibacterial therapy When? Recommendation of GOLD: All 3 cardinal symptoms fulfilled (more dyspnea, more sputum, increased sputum purulence) or 2 cardinal symptoms incl. increased sputum purulence or Procalcitonin-guided or Respiratory failure (NIV or IV)

29 Antibacterial therapy Choice of antibiotic: Guidelines.ch

30 Antiviral therapy - Influenza should be treated
31 Prognosis poor! - In-hospital mortality: 3-24% - 1-year mortality: 22-43% - 5-year mortality: 50-55%
32 Prognosis poor! - Persisting impact on health status, contribution to disease progression - Usual duration of symptoms 7-10 d - At 8 weeks, 20% not recovered to pre-exacerbation state - Re-admission: 24% within 30 d 43% within 90 d
33 «Frequent exacerbator» - 2 or more exacerbations in past 12 months Worse health status Higher mortality Faster decline in lung function
34 Follow-up GOLD 2018
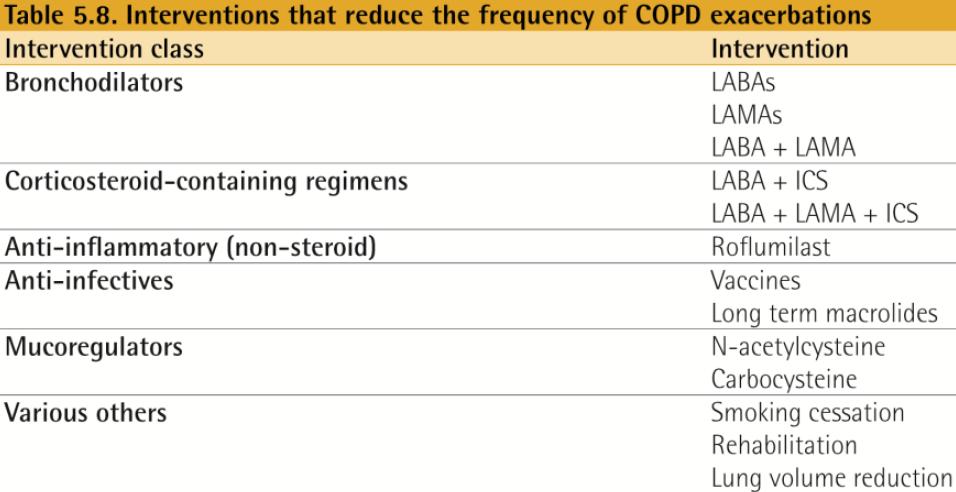
35 Prevention GOLD 2018
36 Early detection unmet goal!

37 Early detection unmet goal! Telemedicine as possible aid? 2016, Respiration
38 Goal: to test feasibility and patient acceptance Methods Daily entry of symptoms via Internet Daily check by study team (pulmonologist and study nurse) Phone call, when exacerbation suspected Further measures according to phone call
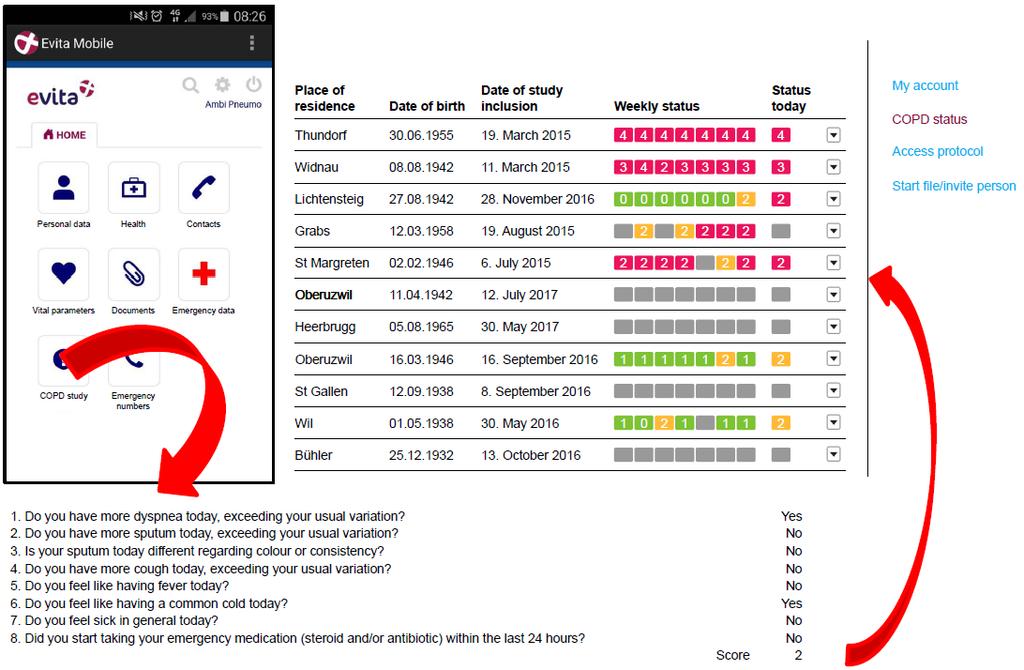
39 2016, Respiration
40 Results Data completeness: 88% Patient acceptance: 94% Improved satisfaction with care 60/63 exacerbations early detected Out of these, none hospitalised

41 2017, Int J COPD

42 2018, ERS Congress, Paris
43 Summary (1) - Important but underrecognized events - Persisting impact on health status, contribution to disease progression - Lead to acceleration of lung function decline - Strongest predictor of future events: history of prior exacerbations - Main etiology: LRTI, rather viral than bacterial - Broad clinical spectrum: mild increase of symptoms - respiratory failure
 - Prevention = important goal - Early recognition = major challenge - Telemedicine as possible aid studies ongoing CAT as longitudinal risk")
44 Summary (2) - Exclusion of DDs and correct triage important - Mainstay of therapy: corticosteroids - Antibiotics: clinically- (Anthonisen) or PCT-guided - Prognosis: poor (high mortality, high readmission) - Prevention = important goal - Early recognition = major challenge - Telemedicine as possible aid studies ongoing CAT as longitudinal risk marker

45 Thank you for your attention!
Management of Acute Exacerbations
 15 Management of Acute Exacerbations Cenk Kirakli Izmir Dr. Suat Seren Chest Diseases and Surgery Training Hospital Turkey 1. Introduction American Thoracic Society (ATS) and European Respiratory Society
15 Management of Acute Exacerbations Cenk Kirakli Izmir Dr. Suat Seren Chest Diseases and Surgery Training Hospital Turkey 1. Introduction American Thoracic Society (ATS) and European Respiratory Society
Management of Acute Exacerbations of COPD
 MiCMRC Educational Webinar Management of Acute Exacerbations of COPD August 22, 2018 MiCMRC Educational Webinar Management of Acute Exacerbations of COPD Expert Presenter: Catherine A. Meldrum PhD RN MS
MiCMRC Educational Webinar Management of Acute Exacerbations of COPD August 22, 2018 MiCMRC Educational Webinar Management of Acute Exacerbations of COPD Expert Presenter: Catherine A. Meldrum PhD RN MS
COPD: From Hospital to Home October 5, 2015 Derek Linderman, MD Associate Professor COPD Center Pulmonary Nodule Clinic
 COPD: From Hospital to Home October 5, 2015 Derek Linderman, MD Associate Professor COPD Center Pulmonary Nodule Clinic Learning Objectives Know the adverse effects of COPD exacerbations Know mainstays
COPD: From Hospital to Home October 5, 2015 Derek Linderman, MD Associate Professor COPD Center Pulmonary Nodule Clinic Learning Objectives Know the adverse effects of COPD exacerbations Know mainstays
an inflammation of the bronchial tubes
 BRONCHITIS DEFINITION Bronchitis is an inflammation of the bronchial tubes (or bronchi), which are the air passages that extend from the trachea into the small airways and alveoli. Triggers may be infectious
BRONCHITIS DEFINITION Bronchitis is an inflammation of the bronchial tubes (or bronchi), which are the air passages that extend from the trachea into the small airways and alveoli. Triggers may be infectious
AECOPD: Management and Prevention
 Neil MacIntyre MD Duke University Medical Center Durham NC Professor P.J. Barnes, MD, National Heart and Lung Institute, London UK Professor Peter J. Barnes, MD National Heart and Lung Institute, London
Neil MacIntyre MD Duke University Medical Center Durham NC Professor P.J. Barnes, MD, National Heart and Lung Institute, London UK Professor Peter J. Barnes, MD National Heart and Lung Institute, London
Community Acquired Pneumonia. Abdullah Alharbi, MD, FCCP
 Community Acquired Pneumonia Abdullah Alharbi, MD, FCCP A 68 y/ male presented to the ED with SOB and productive coughing for 2 days. Reports poor oral intake since onset due to nausea and intermittent
Community Acquired Pneumonia Abdullah Alharbi, MD, FCCP A 68 y/ male presented to the ED with SOB and productive coughing for 2 days. Reports poor oral intake since onset due to nausea and intermittent
Exacerbations of COPD. Dr J Cullen
 Exacerbations of COPD Dr J Cullen Definition An AECOPD is a sustained worsening of the patient s clinical condition from their stable state that is beyond their usual day-to-day variation is acute in onset
Exacerbations of COPD Dr J Cullen Definition An AECOPD is a sustained worsening of the patient s clinical condition from their stable state that is beyond their usual day-to-day variation is acute in onset
Acute Respiratory Infection. Dr Anthony Gibson
 Acute Respiratory Infection Dr Anthony Gibson Range of Conditions Upper tract Common Cold coryza Sore Throat- Pharyngitis Sinusitis Epiglottitis Range of Conditions Lower Acute Bronchitis Acute Exacerbation
Acute Respiratory Infection Dr Anthony Gibson Range of Conditions Upper tract Common Cold coryza Sore Throat- Pharyngitis Sinusitis Epiglottitis Range of Conditions Lower Acute Bronchitis Acute Exacerbation
Advances in the management of chronic obstructive lung diseases (COPD) David CL Lam Department of Medicine University of Hong Kong October, 2015
 David CL Lam Department of Medicine University of Hong Kong October, 2015") Advances in the management of chronic obstructive lung diseases (COPD) David CL Lam Department of Medicine University of Hong Kong October, 2015 Chronic obstructive pulmonary disease (COPD) COPD in Hong
Advances in the management of chronic obstructive lung diseases (COPD) David CL Lam Department of Medicine University of Hong Kong October, 2015 Chronic obstructive pulmonary disease (COPD) COPD in Hong
2/4/2019. GOLD Objectives. GOLD 2019 Report: Chapters
 GOLD Objectives To provide a non biased review of the current evidence for the assessment, diagnosis and treatment of patients with COPD. To highlight short term and long term treatment objectives organized
GOLD Objectives To provide a non biased review of the current evidence for the assessment, diagnosis and treatment of patients with COPD. To highlight short term and long term treatment objectives organized
Lecture Notes. Chapter 16: Bacterial Pneumonia
 Lecture Notes Chapter 16: Bacterial Pneumonia Objectives Explain the epidemiology Identify the common causes Explain the pathological changes in the lung Identify clinical features Explain the treatment
Lecture Notes Chapter 16: Bacterial Pneumonia Objectives Explain the epidemiology Identify the common causes Explain the pathological changes in the lung Identify clinical features Explain the treatment
Best of Pulmonary Jennifer R. Hucks, MD University of South Carolina School of Medicine
 Best of Pulmonary 2012-2013 Jennifer R. Hucks, MD University of South Carolina School of Medicine Topics ARDS- Berlin Definition Prone Positioning For ARDS Lung Protective Ventilation In Patients Without
Best of Pulmonary 2012-2013 Jennifer R. Hucks, MD University of South Carolina School of Medicine Topics ARDS- Berlin Definition Prone Positioning For ARDS Lung Protective Ventilation In Patients Without
2/12/2015. ASTHMA & COPD The Yin &Yang. Asthma General Information. Asthma General Information
 ASTHMA & COPD The Yin &Yang Arizona State Association of Physician Assistants March 6, 2015 Sedona, Arizona Randy D. Danielsen, PhD, PA-C, DFAAPA Dean & Professor A.T. Still University Asthma General Information
ASTHMA & COPD The Yin &Yang Arizona State Association of Physician Assistants March 6, 2015 Sedona, Arizona Randy D. Danielsen, PhD, PA-C, DFAAPA Dean & Professor A.T. Still University Asthma General Information
HQO s Episode of Care for Chronic Obstructive Pulmonary Disease
 HQO s Episode of Care for Chronic Obstructive Pulmonary Disease Dr. Chaim Bell, MD PhD FRCPC Ontario Hospital Association Webcast October 23, 2013 Objectives 1. Describe the rationale and methodology for
HQO s Episode of Care for Chronic Obstructive Pulmonary Disease Dr. Chaim Bell, MD PhD FRCPC Ontario Hospital Association Webcast October 23, 2013 Objectives 1. Describe the rationale and methodology for
Upper...and Lower Respiratory Tract Infections
 Upper...and Lower Respiratory Tract Infections Robin Jump, MD, PhD Cleveland Geriatric Research Education and Clinical Center (GRECC) Louis Stokes Cleveland VA Medical Center Case Western Reserve University
Upper...and Lower Respiratory Tract Infections Robin Jump, MD, PhD Cleveland Geriatric Research Education and Clinical Center (GRECC) Louis Stokes Cleveland VA Medical Center Case Western Reserve University
Author(s): Frank Madore (Hennepin County Medical Center), MD 2012
: Frank Madore (Hennepin County Medical Center), MD 2012") Project: Ghana Emergency Medicine Collaborative Document Title: COPD in the Emergency Department Author(s): Frank Madore (Hennepin County Medical Center), MD 2012 License: Unless otherwise noted, this
Project: Ghana Emergency Medicine Collaborative Document Title: COPD in the Emergency Department Author(s): Frank Madore (Hennepin County Medical Center), MD 2012 License: Unless otherwise noted, this
COPD Update. Muhammad Talha Khan MD. COPD Exacerbations. COPD Clinical Importance. COPD Pathophysiology. Overview/Objectives
 Overview/Objectives COPD Update Muhammad Talha Khan MD Pulmonologist St Croix Regional Medical Center, St Croix Falls, WI. Overview of COPD and disease impact Classification of COPD Severity Treatment
Overview/Objectives COPD Update Muhammad Talha Khan MD Pulmonologist St Croix Regional Medical Center, St Croix Falls, WI. Overview of COPD and disease impact Classification of COPD Severity Treatment
EXACERBATION ASSESSMENT FORM
 EXACERBATION ASSESSMENT FORM ID NUMBER: 0a) Form Completion Date... 0b) Staff Code... Administrative Information 1) Date of clinic visit: 2) What type of Event is this?... Participant/HCU-triggered...
EXACERBATION ASSESSMENT FORM ID NUMBER: 0a) Form Completion Date... 0b) Staff Code... Administrative Information 1) Date of clinic visit: 2) What type of Event is this?... Participant/HCU-triggered...
CLINICAL PATHWAY. Acute Medicine. Chronic Obstructive Pulmonary Disease
 CLINICAL PATHWAY Acute Medicine Chronic Obstructive Pulmonary Disease Chronic Obstructive Pulmonary Disease Table of Contents (tap to jump to page) INTRODUCTION 1 Scope of this Pathway 1 Pathway Contacts
CLINICAL PATHWAY Acute Medicine Chronic Obstructive Pulmonary Disease Chronic Obstructive Pulmonary Disease Table of Contents (tap to jump to page) INTRODUCTION 1 Scope of this Pathway 1 Pathway Contacts
EXACERBATION ASSESSMENT FORM
 EXACERBATION ASSESSMENT FORM ID NUMBER: VERSION: 1.0 05/27/14 0a) Form Completion Date... 0b) Staff Code... Instructions: This form should be completed when a participant comes to the clinical center for
EXACERBATION ASSESSMENT FORM ID NUMBER: VERSION: 1.0 05/27/14 0a) Form Completion Date... 0b) Staff Code... Instructions: This form should be completed when a participant comes to the clinical center for
Chronic Obstructive Pulmonary Disease (COPD) Clinical Guideline
 Clinical Guideline") Chronic Obstructive Pulmonary Disease (COPD) Clinical These clinical guidelines are designed to assist clinicians by providing an analytical framework for the evaluation and treatment of patients. They
Chronic Obstructive Pulmonary Disease (COPD) Clinical These clinical guidelines are designed to assist clinicians by providing an analytical framework for the evaluation and treatment of patients. They
Chapter 10 Respiratory System J00-J99. Presented by: Jesicca Andrews
 Chapter 10 Respiratory System J00-J99 Presented by: Jesicca Andrews 1 Respiratory System 2 Respiratory Infections A respiratory infection cannot be assumed from a laboratory report alone; physician concurrence
Chapter 10 Respiratory System J00-J99 Presented by: Jesicca Andrews 1 Respiratory System 2 Respiratory Infections A respiratory infection cannot be assumed from a laboratory report alone; physician concurrence
Deep discoveries: the ED. Brian H. Rowe, MD, MSc, CCFP(EM) Canada Research Chair in Emergency Airway Diseases Department of Emergency Medicine
 Canada Research Chair in Emergency Airway Diseases Department of Emergency Medicine") Deep discoveries: Treating respiratory infections in the ED. Brian H. Rowe, MD, MSc, CCFP(EM) Canada Research Chair in Emergency Airway Diseases Department of Emergency Medicine University of Alberta Respiratory
Deep discoveries: Treating respiratory infections in the ED. Brian H. Rowe, MD, MSc, CCFP(EM) Canada Research Chair in Emergency Airway Diseases Department of Emergency Medicine University of Alberta Respiratory
COPD Treatable. Preventable.
 My COPD Action Plan Patient s Copy (Patient s Name) Date Canadian Respiratory COPD Treatable. Preventable. This is to tell me how I will take care of myself when I have a COPD flare-up. My goals are My
My COPD Action Plan Patient s Copy (Patient s Name) Date Canadian Respiratory COPD Treatable. Preventable. This is to tell me how I will take care of myself when I have a COPD flare-up. My goals are My
Chronic Obstructive Pulmonary Disease (COPD) Copyright 2014 by Mosby, an imprint of Elsevier Inc.
 Copyright 2014 by Mosby, an imprint of Elsevier Inc.") Chronic Obstructive Pulmonary Disease () 8.18.18 Copyright 2014 by Mosby, an imprint of Elsevier Inc. Description Airflow limitation not fully reversible progressive Abnormal inflammatory response of lungs
Chronic Obstructive Pulmonary Disease () 8.18.18 Copyright 2014 by Mosby, an imprint of Elsevier Inc. Description Airflow limitation not fully reversible progressive Abnormal inflammatory response of lungs
RESPIRATORY FAILURE - CAUSES, CLINICAL INFORMATION, TREATMENT AND CODING CONVENTIONS
 RESPIRATORY FAILURE - CAUSES, CLINICAL INFORMATION, TREATMENT AND CODING CONVENTIONS QUIZ REVIEW The correct answer is in bold font. 1. Hypoxic respiratory failure involves: a. Low oxygen b. High oxygen
RESPIRATORY FAILURE - CAUSES, CLINICAL INFORMATION, TREATMENT AND CODING CONVENTIONS QUIZ REVIEW The correct answer is in bold font. 1. Hypoxic respiratory failure involves: a. Low oxygen b. High oxygen
Epiglottitis. Bronchitis. Bronchiolitis. Pneumonia. Croup syndrome. Miss. kamlah 2
 Miss. kamlah 1 Epiglottitis. Bronchitis. Bronchiolitis. Pneumonia. Croup syndrome. Miss. kamlah 2 Acute Epiglottitis Is an infection of the epiglottis, the long narrow structure that closes off the glottis
Miss. kamlah 1 Epiglottitis. Bronchitis. Bronchiolitis. Pneumonia. Croup syndrome. Miss. kamlah 2 Acute Epiglottitis Is an infection of the epiglottis, the long narrow structure that closes off the glottis
Guideline for the Diagnosis and Management of COPD
 Guideline for the Diagnosis and Management of COPD Introduction Chronic obstructive pulmonary disease (COPD) is a respiratory disorder largely caused by smoking. It is characterized by progressive, partially
Guideline for the Diagnosis and Management of COPD Introduction Chronic obstructive pulmonary disease (COPD) is a respiratory disorder largely caused by smoking. It is characterized by progressive, partially
COPD: A Renewed Focus. Disclosures
 COPD: A Renewed Focus Heath Latham, MD Assistant Professor Division of Pulmonary and Critical Care Medicine Disclosures No Business Interests No Consulting No Speakers Bureau No Off Label Use to Discuss
COPD: A Renewed Focus Heath Latham, MD Assistant Professor Division of Pulmonary and Critical Care Medicine Disclosures No Business Interests No Consulting No Speakers Bureau No Off Label Use to Discuss
PNEUMONIA IN CHILDREN. IAP UG Teaching slides
 PNEUMONIA IN CHILDREN 1 INTRODUCTION 156 million new episodes / yr. worldwide 151 million episodes developing world 95% in developing countries 19% of all deaths in children
PNEUMONIA IN CHILDREN 1 INTRODUCTION 156 million new episodes / yr. worldwide 151 million episodes developing world 95% in developing countries 19% of all deaths in children
PBL RESPIRATORY SYSTEM DR. NATHEER OBAIDAT
 PBL RESPIRATORY SYSTEM DR. NATHEER OBAIDAT Dr started to talk about his specialty at the hospital which is (ICU-Pulmonary-Internal Medicine). Pulmonary medical branch is a subspecialty of internal medicine.
PBL RESPIRATORY SYSTEM DR. NATHEER OBAIDAT Dr started to talk about his specialty at the hospital which is (ICU-Pulmonary-Internal Medicine). Pulmonary medical branch is a subspecialty of internal medicine.
Respiratory Medicine. Some pet peeves and other random topics. Kyle Perrin
 Respiratory Medicine Some pet peeves and other random topics Kyle Perrin Overview 1. Acute asthma Severity assessment and management 2. Acute COPD NIV and other management 3. Respiratory problems in the
Respiratory Medicine Some pet peeves and other random topics Kyle Perrin Overview 1. Acute asthma Severity assessment and management 2. Acute COPD NIV and other management 3. Respiratory problems in the
Lecture Notes. Chapter 3: Asthma
 Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
Chronic Obstructive Pulmonary Disease
 Chronic Obstructive Pulmonary Disease 07 Contributor Dr David Tan Hsien Yung Definition, Diagnosis and Risk Factors for (COPD) Differential Diagnoses Goals of Management Management of COPD THERAPY AT EACH
Chronic Obstructive Pulmonary Disease 07 Contributor Dr David Tan Hsien Yung Definition, Diagnosis and Risk Factors for (COPD) Differential Diagnoses Goals of Management Management of COPD THERAPY AT EACH
Pneumonia 2017 OMAR PIRZADA
 Pneumonia 2017 OMAR PIRZADA Pneumonia Pneumonia is common 0.5-1% of adults per year, 5-12% presenting to GP with LRTi 22-42% will be admitted to hospital Symptoms and signs Case 1 26 year old man Sudden
Pneumonia 2017 OMAR PIRZADA Pneumonia Pneumonia is common 0.5-1% of adults per year, 5-12% presenting to GP with LRTi 22-42% will be admitted to hospital Symptoms and signs Case 1 26 year old man Sudden
COPD exacerbation. Chiara Maruggi, PGY2
 COPD exacerbation Chiara Maruggi, PGY2 Learning objectives At the end of this lecture students will be able to: 1) Critically assess patients for COPD and design a management plan. 2) Develop a step-wise
COPD exacerbation Chiara Maruggi, PGY2 Learning objectives At the end of this lecture students will be able to: 1) Critically assess patients for COPD and design a management plan. 2) Develop a step-wise
COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis.
 1 Definition of COPD: COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis. Airflow obstruction may be accompanied by airway hyper-responsiveness
1 Definition of COPD: COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis. Airflow obstruction may be accompanied by airway hyper-responsiveness
Running head: COMMON COLD AND BRONCHITIS 1
 Running head: COMMON COLD AND BRONCHITIS 1 Common Cold and Bronchitis Name: Institution: COMMON COLD AND BRONCHITIS 2 Common Cold and Bronchitis Bronchitis also labeled in medical terminology as acute
Running head: COMMON COLD AND BRONCHITIS 1 Common Cold and Bronchitis Name: Institution: COMMON COLD AND BRONCHITIS 2 Common Cold and Bronchitis Bronchitis also labeled in medical terminology as acute
Session Guidelines. This is a 15 minute webinar session for CNC physicians and staff
 Respiratory Disease Session Guidelines This is a 15 minute webinar session for CNC physicians and staff CNC holds webinars monthly to address topics related to risk adjustment documentation and coding
Respiratory Disease Session Guidelines This is a 15 minute webinar session for CNC physicians and staff CNC holds webinars monthly to address topics related to risk adjustment documentation and coding
62 year old man with a cough! Dr. Aflah Sadikeen Consultant Respiratory Physician Colombo
 62 year old man with a cough! Dr. Aflah Sadikeen Consultant Respiratory Physician Colombo History Mr.KS, a 62 year-old, has been feeling unwell - Worsening cough for the last 5 days - Feels out of breath
62 year old man with a cough! Dr. Aflah Sadikeen Consultant Respiratory Physician Colombo History Mr.KS, a 62 year-old, has been feeling unwell - Worsening cough for the last 5 days - Feels out of breath
Charles Krasner, M.D. University of NV, Reno School of Medicine Sierra NV Veterans Affairs Medical Center
 Charles Krasner, M.D. University of NV, Reno School of Medicine Sierra NV Veterans Affairs Medical Center Kathy Peters is a 63 y.o. patient that presents to your urgent care office today with a history
Charles Krasner, M.D. University of NV, Reno School of Medicine Sierra NV Veterans Affairs Medical Center Kathy Peters is a 63 y.o. patient that presents to your urgent care office today with a history
UPDATE IN HOSPITAL MEDICINE
 UPDATE IN HOSPITAL MEDICINE FLORIDA CHAPTER ACP MEETING 2016 Himangi Kaushal, M.D., F.A.C.P. Program Director Memorial Healthcare System Internal Medicine Residency DISCLOSURES None OBJECTIVES Review some
UPDATE IN HOSPITAL MEDICINE FLORIDA CHAPTER ACP MEETING 2016 Himangi Kaushal, M.D., F.A.C.P. Program Director Memorial Healthcare System Internal Medicine Residency DISCLOSURES None OBJECTIVES Review some
Update on heterogeneity of COPD, evaluation of COPD severity and exacerbation
 Update on heterogeneity of COPD, evaluation of COPD severity and exacerbation Yung-Yang Liu, MD Taipei Veterans General Hospital Aug 29, 2015 G O lobal Initiative for Chronic bstructive L D ung isease
Update on heterogeneity of COPD, evaluation of COPD severity and exacerbation Yung-Yang Liu, MD Taipei Veterans General Hospital Aug 29, 2015 G O lobal Initiative for Chronic bstructive L D ung isease
Chapter 22. Pulmonary Infections
 Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
Asthma and COPD in older people lumping or splitting? Christine Jenkins Concord Hospital Woolcock Institute of Medical Research
 Asthma and COPD in older people lumping or splitting? Christine Jenkins Concord Hospital Woolcock Institute of Medical Research Concord Hospital Woolcock Institute of Medical Research Joe has asthma What
Asthma and COPD in older people lumping or splitting? Christine Jenkins Concord Hospital Woolcock Institute of Medical Research Concord Hospital Woolcock Institute of Medical Research Joe has asthma What
CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MOUSTAPHA ABIDALI, DO CRITICAL CARE FELLOW UNIVERSITY OF ARIZONA- PHOENIX
 MOUSTAPHA ABIDALI, DO CRITICAL CARE FELLOW UNIVERSITY OF ARIZONA- PHOENIX") CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MOUSTAPHA ABIDALI, DO CRITICAL CARE FELLOW UNIVERSITY OF ARIZONA- PHOENIX COPD OUTLINE Definition and Overview Pathophysiology Diagnosis and Assessment Therapeutic
CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MOUSTAPHA ABIDALI, DO CRITICAL CARE FELLOW UNIVERSITY OF ARIZONA- PHOENIX COPD OUTLINE Definition and Overview Pathophysiology Diagnosis and Assessment Therapeutic
COPD Management in LTC: Presented By: Jessica Denney RRT
 COPD Management in LTC: Presented By: Jessica Denney RRT Sponsored by Z & D Medical Services, Diamond Sponsor Seizing Opportunities to Provide Individualized Treatment and Device Selection for your COPD
COPD Management in LTC: Presented By: Jessica Denney RRT Sponsored by Z & D Medical Services, Diamond Sponsor Seizing Opportunities to Provide Individualized Treatment and Device Selection for your COPD
ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss?
 ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss? Randall W. Brown, MD MPH AE-C Association of Asthma Educators Annual Conference July 20, 2018 Phoenix, Arizona FACULTY/DISCLOSURES Randall Brown,
ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss? Randall W. Brown, MD MPH AE-C Association of Asthma Educators Annual Conference July 20, 2018 Phoenix, Arizona FACULTY/DISCLOSURES Randall Brown,
Antimicrobial Stewardship in Community Acquired Pneumonia
 Antimicrobial Stewardship in Community Acquired Pneumonia Medicine Review Course 2018 Dr Lee Tau Hong Consultant Department of Infectious Diseases National Centre for Infectious Diseases Scope 1. Diagnosis
Antimicrobial Stewardship in Community Acquired Pneumonia Medicine Review Course 2018 Dr Lee Tau Hong Consultant Department of Infectious Diseases National Centre for Infectious Diseases Scope 1. Diagnosis
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE 1 Guideline title SCOPE Bronchiolitis: diagnosis and management of bronchiolitis in children. 1.1 Short title Bronchiolitis in children 2 The remit The
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE 1 Guideline title SCOPE Bronchiolitis: diagnosis and management of bronchiolitis in children. 1.1 Short title Bronchiolitis in children 2 The remit The
The McMaster at night Pediatric Curriculum
 The McMaster at night Pediatric Curriculum Community Acquired Pneumonia Based on CPS Practice Point Pneumonia in healthy Canadian children and youth and the British Thoracic Society Guidelines on CAP Objectives
The McMaster at night Pediatric Curriculum Community Acquired Pneumonia Based on CPS Practice Point Pneumonia in healthy Canadian children and youth and the British Thoracic Society Guidelines on CAP Objectives
Dr Conroy Wong. Professor Richard Beasley. Dr Sarah Mooney. Professor Innes Asher
 Professor Richard Beasley University of Otago Director Medical Research Institute of New Zealand Wellington Dr Sarah Mooney Physiotherapy Advanced Clinician Counties Manukau Health NZ Respiratory and Sleep
Professor Richard Beasley University of Otago Director Medical Research Institute of New Zealand Wellington Dr Sarah Mooney Physiotherapy Advanced Clinician Counties Manukau Health NZ Respiratory and Sleep
Integrated Cardiopulmonary Pharmacology Third Edition
 Integrated Cardiopulmonary Pharmacology Third Edition Chapter 13 Pharmacologic Management of Asthma, Chronic Bronchitis, and Emphysema Multimedia Directory Slide 7 Slide 12 Slide 60 COPD Video Passive
Integrated Cardiopulmonary Pharmacology Third Edition Chapter 13 Pharmacologic Management of Asthma, Chronic Bronchitis, and Emphysema Multimedia Directory Slide 7 Slide 12 Slide 60 COPD Video Passive
Over the last several years various national and
 Recommendations for the Management of COPD* Gary T. Ferguson, MD, FCCP Three sets of guidelines for the management of COPD that are widely recognized (from the European Respiratory Society [ERS], American
Recommendations for the Management of COPD* Gary T. Ferguson, MD, FCCP Three sets of guidelines for the management of COPD that are widely recognized (from the European Respiratory Society [ERS], American
Viral Threat on Respiratory Failure
 Viral Threat on Respiratory Failure Younsuck Koh, MD, PhD, FCCM Department of Pulmonary and Critical Care Medicine Asan Medical Center University of Ulsan College of Medicine Seoul, Korea No Conflict of
Viral Threat on Respiratory Failure Younsuck Koh, MD, PhD, FCCM Department of Pulmonary and Critical Care Medicine Asan Medical Center University of Ulsan College of Medicine Seoul, Korea No Conflict of
Lecture Notes. Chapter 4: Chronic Obstructive Pulmonary Disease (COPD)
") Lecture Notes Chapter 4: Chronic Obstructive Pulmonary Disease (COPD) Objectives Define COPD Estimate incidence of COPD in the US Define factors associated with onset of COPD Describe the clinical features
Lecture Notes Chapter 4: Chronic Obstructive Pulmonary Disease (COPD) Objectives Define COPD Estimate incidence of COPD in the US Define factors associated with onset of COPD Describe the clinical features
Epidemiology and Etiology of Community-Acquired Pneumonia 761 Lionel A. Mandell
 LOWER RESPIRATORY TRACT INFECTIONS Preface Thomas M. File, Jr xiii Community-Acquired Pneumonia: Pathophysiology and Host Factors with Focus on Possible New Approaches to Management of Lower Respiratory
LOWER RESPIRATORY TRACT INFECTIONS Preface Thomas M. File, Jr xiii Community-Acquired Pneumonia: Pathophysiology and Host Factors with Focus on Possible New Approaches to Management of Lower Respiratory
Chronic obstructive pulmonary disease
 0 Chronic obstructive pulmonary disease Implementing NICE guidance June 2010 NICE clinical guideline 101 What this presentation covers Background Scope Key priorities for implementation Discussion Find
0 Chronic obstructive pulmonary disease Implementing NICE guidance June 2010 NICE clinical guideline 101 What this presentation covers Background Scope Key priorities for implementation Discussion Find
Community Acquired & Nosocomial Pneumonias
 Community Acquired & Nosocomial Pneumonias IDSA/ATS 2007 & 2016 Guidelines José Luis González, MD Clinical Assistant Professor of Medicine Outline Intro - Definitions & Diagnosing CAP treatment VAP & HAP
Community Acquired & Nosocomial Pneumonias IDSA/ATS 2007 & 2016 Guidelines José Luis González, MD Clinical Assistant Professor of Medicine Outline Intro - Definitions & Diagnosing CAP treatment VAP & HAP
Respiratory Syncytial Virus (RSV) in Older Adults: A Hidden Annual Epidemic. Webinar Agenda
 in Older Adults: A Hidden Annual Epidemic. Webinar Agenda") Respiratory Syncytial Virus (RSV) in Older Adults: A Hidden Annual Epidemic Wednesday, November 2, 2016 12:00 PM ET Webinar Agenda Agenda Welcome and Introductions William Schaffner, MD, NFID Medical Director
Respiratory Syncytial Virus (RSV) in Older Adults: A Hidden Annual Epidemic Wednesday, November 2, 2016 12:00 PM ET Webinar Agenda Agenda Welcome and Introductions William Schaffner, MD, NFID Medical Director
66YM Chronic obstructive pulmonary disease annual review. H Chronic obstructive pulmonary disease
 Supplementary materials Table S1. Read codes to define COPD Read code Medical code Clinical event Read term 66YM.00 11287 382901 Chronic obstructive pulmonary disease annual review H3...00 1001 338812
Supplementary materials Table S1. Read codes to define COPD Read code Medical code Clinical event Read term 66YM.00 11287 382901 Chronic obstructive pulmonary disease annual review H3...00 1001 338812
Chronic Obstructive Pulmonary Disease (COPD).
.") Chronic Obstructive Pulmonary Disease (COPD). Linde: Living healthcare 02 03 Chronic Obstructive Pulmonary Disease (COPD). A pocket guide for healthcare professionals. COPD the facts Moderate to severe
Chronic Obstructive Pulmonary Disease (COPD). Linde: Living healthcare 02 03 Chronic Obstructive Pulmonary Disease (COPD). A pocket guide for healthcare professionals. COPD the facts Moderate to severe
A Previously Hospitalized Patient Who Is Having Frequent COPD Exacerbations Specialty House Calls Case 2
 The following is a transcript from a web-based CME-certified multimedia activity. This enduring activity is provided by Albert Einstein College of Medicine of Yeshiva University. This enduring activity
The following is a transcript from a web-based CME-certified multimedia activity. This enduring activity is provided by Albert Einstein College of Medicine of Yeshiva University. This enduring activity
Course Handouts & Disclosure
 COPD: Disease Trajectory and Hospice Eligibility Terri L. Maxwell PhD, APRN VP, Strategic Initiatives Weatherbee Resources Hospice Education Network Course Handouts & Disclosure To download presentation
COPD: Disease Trajectory and Hospice Eligibility Terri L. Maxwell PhD, APRN VP, Strategic Initiatives Weatherbee Resources Hospice Education Network Course Handouts & Disclosure To download presentation
COPD. Dr.O.Paknejad Pulmonologist Shariati Hospital TUMS
 IN THE NAME OF GOD COPD Dr.O.Paknejad Pulmonologist Shariati Hospital TUMS Definition of COPD* COPD is a preventable and treatable chronic lung disease characterized by airflow limitation that is not fully
IN THE NAME OF GOD COPD Dr.O.Paknejad Pulmonologist Shariati Hospital TUMS Definition of COPD* COPD is a preventable and treatable chronic lung disease characterized by airflow limitation that is not fully
THE CHALLENGES OF COPD MANAGEMENT IN PRIMARY CARE An Expert Roundtable
 THE CHALLENGES OF COPD MANAGEMENT IN PRIMARY CARE An Expert Roundtable This activity is supported by an educational grant from Sunovion Pharmaceuticals Inc. COPD in the United States Third leading cause
THE CHALLENGES OF COPD MANAGEMENT IN PRIMARY CARE An Expert Roundtable This activity is supported by an educational grant from Sunovion Pharmaceuticals Inc. COPD in the United States Third leading cause
Pneumonia. Dr. Rami M Adil Al-Hayali Assistant professor in medicine
 Pneumonia Dr. Rami M Adil Al-Hayali Assistant professor in medicine Definition Pneumonia is an acute respiratory illness caused by an infection of the lung parenchyma, associated with recently developed
Pneumonia Dr. Rami M Adil Al-Hayali Assistant professor in medicine Definition Pneumonia is an acute respiratory illness caused by an infection of the lung parenchyma, associated with recently developed
Pulmonary Pathophysiology
 Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
Early infection diagnosis
 Procalcitonin in the EMERGENCY DEPARTMENT Early infection diagnosis and risk assessment with Procalcitonin (PCT) Early differential diagnosis and therapy decision in the emergency department Antibiotic
Procalcitonin in the EMERGENCY DEPARTMENT Early infection diagnosis and risk assessment with Procalcitonin (PCT) Early differential diagnosis and therapy decision in the emergency department Antibiotic
GOALS AND INSTRUCTIONAL OBJECTIVES
 October 4-7, 2004 Respiratory GOALS: GOALS AND INSTRUCTIONAL OBJECTIVES By the end of the week, the first quarter student will have an in-depth understanding of the diagnoses listed under Primary Diagnoses
October 4-7, 2004 Respiratory GOALS: GOALS AND INSTRUCTIONAL OBJECTIVES By the end of the week, the first quarter student will have an in-depth understanding of the diagnoses listed under Primary Diagnoses
Chronic Obstructive Pulmonary Disease (COPD)
") Chronic Obstructive Pulmonary Disease (COPD) Definition of COPD Airflow obstruction that is: o Not fully reversible o Progressive o Does not change markedly over several months Combination of airway and
Chronic Obstructive Pulmonary Disease (COPD) Definition of COPD Airflow obstruction that is: o Not fully reversible o Progressive o Does not change markedly over several months Combination of airway and
Chronic obstructive pulmonary disease
 Chronic obstructive pulmonary disease By: Dr. Fatima Makee AL-Hakak () University of kerbala College of nursing Out lines What is the? Overview Causes of Symptoms of What's the difference between and asthma?
Chronic obstructive pulmonary disease By: Dr. Fatima Makee AL-Hakak () University of kerbala College of nursing Out lines What is the? Overview Causes of Symptoms of What's the difference between and asthma?
COPD exacerbation and prevention
 HELVETICA CARDIOLOGICA SOCIETAS REVIEW ARTICLE SSC-CONGRESS 2016 38 Exacerbations of COPD should not be underestimated and should be prevented when possible COPD exacerbation and prevention Carlos Roberto
HELVETICA CARDIOLOGICA SOCIETAS REVIEW ARTICLE SSC-CONGRESS 2016 38 Exacerbations of COPD should not be underestimated and should be prevented when possible COPD exacerbation and prevention Carlos Roberto
Around-COPD Verona (Italy), January Highlights
, January Highlights") Introduction Around-COPD Verona (Italy), January 18 2017 Highlights Prof. Dal Negro chairman of the symposium, opened the congress by highlighting the burden of COPD as a chronic invalidating disease affecting
Introduction Around-COPD Verona (Italy), January 18 2017 Highlights Prof. Dal Negro chairman of the symposium, opened the congress by highlighting the burden of COPD as a chronic invalidating disease affecting
CLAIRE NOWLAN & SAM SEARLE. Pneumonia in the nursing home
 CLAIRE NOWLAN & SAM SEARLE Pneumonia in the nursing home No disclosures or conflicts of interest PMHX: A. FIB. GERD MIXED DEMENTIA MMSE 16/30 HTN Mr. Hack 86 years old RAMIPRIL 4 MG OD PARIET 20MG OD DONEPEZIL
CLAIRE NOWLAN & SAM SEARLE Pneumonia in the nursing home No disclosures or conflicts of interest PMHX: A. FIB. GERD MIXED DEMENTIA MMSE 16/30 HTN Mr. Hack 86 years old RAMIPRIL 4 MG OD PARIET 20MG OD DONEPEZIL
Community Acquired Pneumonia - Pediatric Clinical Practice Guideline MedStar Health Antibiotic Stewardship
 Community Acquired Pneumonia - Pediatric Clinical Practice Guideline MedStar Health Antibiotic Stewardship These guidelines are provided to assist physicians and other clinicians in making decisions regarding
Community Acquired Pneumonia - Pediatric Clinical Practice Guideline MedStar Health Antibiotic Stewardship These guidelines are provided to assist physicians and other clinicians in making decisions regarding
JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES
 MANAGEMENT GUIDELINES") JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES Authors Dr Ian Benton Respiratory Consultant COCH Penny Rideal Respiratory Nurse COCH Kirti Burgul Respiratory Pharmacist COCH Pam
JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES Authors Dr Ian Benton Respiratory Consultant COCH Penny Rideal Respiratory Nurse COCH Kirti Burgul Respiratory Pharmacist COCH Pam
Respiratory Diseases and Disorders
 Chapter 9 Respiratory Diseases and Disorders Anatomy and Physiology Chest, lungs, and conducting airways Two parts: Upper respiratory system consists of nose, mouth, sinuses, pharynx, and larynx Lower
Chapter 9 Respiratory Diseases and Disorders Anatomy and Physiology Chest, lungs, and conducting airways Two parts: Upper respiratory system consists of nose, mouth, sinuses, pharynx, and larynx Lower
11/19/2012. The spectrum of pulmonary diseases in HIV-infected persons is broad.
 The spectrum of pulmonary diseases in HIV-infected persons is broad. HIV-associated Opportunistic infections Neoplasms Miscellaneous conditions Non HIV-associated Antiretroviral therapy (ART)-associated
The spectrum of pulmonary diseases in HIV-infected persons is broad. HIV-associated Opportunistic infections Neoplasms Miscellaneous conditions Non HIV-associated Antiretroviral therapy (ART)-associated
Avian Influenza Clinical Picture, Risk profile & Treatment
 Avian Influenza Clinical Picture, Risk profile & Treatment Jantjie Taljaard Adult ID Unit Tygerberg Academic Hospital University of Stellenbosch jjt@sun.ac.za 083 419 1452 CLINICAL PICTURE The clinical
Avian Influenza Clinical Picture, Risk profile & Treatment Jantjie Taljaard Adult ID Unit Tygerberg Academic Hospital University of Stellenbosch jjt@sun.ac.za 083 419 1452 CLINICAL PICTURE The clinical
Guidelines/Guidance/CAP/ Hospitalized Child. PHM Boot Camp 2014 Jay Tureen, MD June 19, 2014
 Guidelines/Guidance/CAP/ Hospitalized Child PHM Boot Camp 2014 Jay Tureen, MD June 19, 2014 CAP in Children: Epi Greatest cause of death in children worldwide Estimated > 2 M deaths in children In developed
Guidelines/Guidance/CAP/ Hospitalized Child PHM Boot Camp 2014 Jay Tureen, MD June 19, 2014 CAP in Children: Epi Greatest cause of death in children worldwide Estimated > 2 M deaths in children In developed
Quality Care Innovation lead clinician for integrated respiratory service georges ng* man kwong
 Working in partnership Quality Care Innovation lead clinician for integrated respiratory service georges ng* man kwong chest physician pronounced ning qualified 1990 chief clinical information officer
Working in partnership Quality Care Innovation lead clinician for integrated respiratory service georges ng* man kwong chest physician pronounced ning qualified 1990 chief clinical information officer
Disclosure and Conflict of Interest 8/15/2017. Pharmacist Objectives. At the conclusion of this program, the pharmacist will be able to:
 Digging for GOLD Rebecca Young, PharmD, BCACP, Roosevelt University College of Pharmacy Assistant Professor of Clinical Sciences Practice Site Advocate Medical Group-Nesset Pavilion Disclosure and Conflict
Digging for GOLD Rebecca Young, PharmD, BCACP, Roosevelt University College of Pharmacy Assistant Professor of Clinical Sciences Practice Site Advocate Medical Group-Nesset Pavilion Disclosure and Conflict
KAISER PERMANENTE OHIO COMMUNITY ACQUIRED PNEUMONIA
 KAISER PERMANENTE OHIO COMMUNITY ACQUIRED PNEUMONIA Methodology: Expert opinion Issue Date: 8-97 Champion: Pulmonary Medicine Most Recent Update: 6-08, 7-10, 7-12 Key Stakeholders: Pulmonary Medicine,
KAISER PERMANENTE OHIO COMMUNITY ACQUIRED PNEUMONIA Methodology: Expert opinion Issue Date: 8-97 Champion: Pulmonary Medicine Most Recent Update: 6-08, 7-10, 7-12 Key Stakeholders: Pulmonary Medicine,
Francesco Blasi Head Respiratory Medicine Section Cardio-Thoracic Department University of Milan, Italy
 COPD EXACERBATIONS Francesco Blasi Head Respiratory Medicine Section Cardio-Thoracic Department University of Milan, Italy COPD OUTCOMES Cazzola M et al. ERJ 2008 COPD AND CARDIOVASCULAR DISEASE Cumulative
COPD EXACERBATIONS Francesco Blasi Head Respiratory Medicine Section Cardio-Thoracic Department University of Milan, Italy COPD OUTCOMES Cazzola M et al. ERJ 2008 COPD AND CARDIOVASCULAR DISEASE Cumulative
OPTIMIZING MANAGEMENT OF COPD IN THE PRACTICE SETTING 10/16/2018 DISCLOSURES I have no financial or other disclosures
 OPTIMIZING MANAGEMENT OF COPD IN THE PRACTICE SETTING J. Michael Fuller, MD, MEd, FACP, FCCP Associate Professor of Medicine University of South Carolina Greenville DISCLOSURES I have no financial or other
OPTIMIZING MANAGEMENT OF COPD IN THE PRACTICE SETTING J. Michael Fuller, MD, MEd, FACP, FCCP Associate Professor of Medicine University of South Carolina Greenville DISCLOSURES I have no financial or other
Antibiotic Guidance for Treatment of Acute Exacerbations of COPD (AECOPD) in Adults
 in Adults") Antibiotic Guidance for Treatment of Acute Exacerbations of COPD (AECOPD) in Adults Antibiotics are not recommended for all patients with AECOPD as bacterial infection is implicated in less than one-third
Antibiotic Guidance for Treatment of Acute Exacerbations of COPD (AECOPD) in Adults Antibiotics are not recommended for all patients with AECOPD as bacterial infection is implicated in less than one-third
HOSPITAL RECORD ABSTRACTION FORM
 HOSPITAL RECORD ABSTRACTION FORM ID NUMBER: VERSION: A 10/23/2015 0a. Form Completion Date... / / 0b. Staff Code... 0c. Event ID: 0d. Event Date: / / Instructions: Answers are derived from the medical
HOSPITAL RECORD ABSTRACTION FORM ID NUMBER: VERSION: A 10/23/2015 0a. Form Completion Date... / / 0b. Staff Code... 0c. Event ID: 0d. Event Date: / / Instructions: Answers are derived from the medical
IdentifyingRiskFactorsforAcuteExacerbationsofChronicObstructivePulmonaryDisease
 Global Journal of Medical Research: F Diseases Volume 18 Issue 5 Version 1.0 Type: Double Blind Peer Reviewed International Research Journal Publisher: Global Journals Online ISSN: 2249-4618 & Print ISSN:
Global Journal of Medical Research: F Diseases Volume 18 Issue 5 Version 1.0 Type: Double Blind Peer Reviewed International Research Journal Publisher: Global Journals Online ISSN: 2249-4618 & Print ISSN:
How to treat COPD? What is the mechanism of dyspnea? Smoking cessation
 : The Increasing Role of the FP Alan Kaplan, MD, CCFP(EM) Presented at the Primary Care Today: Education Conference and Medical Exposition, Toronto, Ontario, May 2006. Chronic obstructive pulmonary disease
: The Increasing Role of the FP Alan Kaplan, MD, CCFP(EM) Presented at the Primary Care Today: Education Conference and Medical Exposition, Toronto, Ontario, May 2006. Chronic obstructive pulmonary disease
COPD Challenge CASE PRESENTATION
 Chronic obstructive pulmonary disease (COPD) exacerbations may make up more than 10% of acute medical admissions [1], and they are increasingly recognised as a cause of significant morbidity and mortality
Chronic obstructive pulmonary disease (COPD) exacerbations may make up more than 10% of acute medical admissions [1], and they are increasingly recognised as a cause of significant morbidity and mortality
URIs and Pneumonia. Elena Bissell, MD 10/16/2013
 URIs and Pneumonia Elena Bissell, MD 10/16/2013 Objectives Recognize and treat community acquired PNA in children/adults Discern between inpatient and outpatient treatment of PNA Recognize special populations/cases
URIs and Pneumonia Elena Bissell, MD 10/16/2013 Objectives Recognize and treat community acquired PNA in children/adults Discern between inpatient and outpatient treatment of PNA Recognize special populations/cases
Brice Taylor Assistant Professor Division of Pulmonary and Critical Care Medicine
 Brice Taylor Assistant Professor Division of Pulmonary and Critical Care Medicine Discuss advances in predicting prognosis Understand dwhat we know (and don t know) about the Microbiology Recognize important
Brice Taylor Assistant Professor Division of Pulmonary and Critical Care Medicine Discuss advances in predicting prognosis Understand dwhat we know (and don t know) about the Microbiology Recognize important
HEALTH SERVICES POLICY & PROCEDURE MANUAL
 Page 1 of 9 PURPOSE To assure that DOP inmates with Pulmonary Diseases are receiving high quality Primary Care for their condition. POLICY All DOP Primary Care Providers and Chronic Disease Nurses are
Page 1 of 9 PURPOSE To assure that DOP inmates with Pulmonary Diseases are receiving high quality Primary Care for their condition. POLICY All DOP Primary Care Providers and Chronic Disease Nurses are
Chronic obstructive lung disease. Dr/Rehab F.Gwada
 Chronic obstructive lung disease Dr/Rehab F.Gwada Obstructive lung diseases Problem is in the expiratory phase Lung disease Restrictive lung disease Restriction may be with, or within the chest wall Problem
Chronic obstructive lung disease Dr/Rehab F.Gwada Obstructive lung diseases Problem is in the expiratory phase Lung disease Restrictive lung disease Restriction may be with, or within the chest wall Problem
COPD. Breathing Made Easier
 COPD Breathing Made Easier Catherine E. Cooke, PharmD, BCPS, PAHM Independent Consultant, PosiHleath Clinical Associate Professor, University of Maryland School of Pharmacy This program has been brought
COPD Breathing Made Easier Catherine E. Cooke, PharmD, BCPS, PAHM Independent Consultant, PosiHleath Clinical Associate Professor, University of Maryland School of Pharmacy This program has been brought
THE PHARMA INNOVATION - JOURNAL Acute exacerbation of chronic obstructive pulmonary disease, caused by viruses: the need of combined antiinfective
 Received: 19-11-2013 Accepted: 28-12-2013 ISSN: 2277-7695 CODEN Code: PIHNBQ ZDB-Number: 2663038-2 IC Journal No: 7725 Vol. 2 No. 11. 2014 Online Available at www.thepharmajournal.com THE PHARMA INNOVATION
Received: 19-11-2013 Accepted: 28-12-2013 ISSN: 2277-7695 CODEN Code: PIHNBQ ZDB-Number: 2663038-2 IC Journal No: 7725 Vol. 2 No. 11. 2014 Online Available at www.thepharmajournal.com THE PHARMA INNOVATION
Background. Background. Background 3/14/2014. Conflict of Interest Statement:
 Platform Presentations Comparison of zolpidem to other drugs associated with falls in hospitalized patients Ed Rainville, MSPharm. Conflict of Interest Statement: The speaker has no conflict of interest
Platform Presentations Comparison of zolpidem to other drugs associated with falls in hospitalized patients Ed Rainville, MSPharm. Conflict of Interest Statement: The speaker has no conflict of interest
Care Process Model. Chronic Obstructive Pulmonary Disease
 Chronic Obstructive Pulmonary Disease WHAT IS MULTIDISCIPLINARY CARE? Multidisciplinary care is agreed upon, interdisciplinary, patient-centered, disease-focused, care delivery systems that are informed
Chronic Obstructive Pulmonary Disease WHAT IS MULTIDISCIPLINARY CARE? Multidisciplinary care is agreed upon, interdisciplinary, patient-centered, disease-focused, care delivery systems that are informed
Acute exacerbation of. chronic obstructive pulmonary disease
 Nabil Al Lawati, MD, MRCP, J. Mark FitzGerald, MD, MB, FRCPC, FRCPCI Acute exacerbation of chronic obstructive pulmonary disease Bronchodilators, oral corticosteroids, and antibiotics may all be needed
Nabil Al Lawati, MD, MRCP, J. Mark FitzGerald, MD, MB, FRCPC, FRCPCI Acute exacerbation of chronic obstructive pulmonary disease Bronchodilators, oral corticosteroids, and antibiotics may all be needed