A Case of Vascular MCI
|
|
|
- Beverley Golden
- 5 years ago
- Views:
Transcription



1 A Case of Vascular MCI Charles DeCarli, MD Victor and Genevieve Orsi Chair in Alzheimer s Research Director Alzheimer s Disease Center University of California at Davis
2 Initial Evaluation 78 y.o. Rt. Handed Male Memory decline starting ~ Mild problems with language; including comprehension CVA- dragging L foot; stroke dxd. Residual L hemiparesis and L arm dysaethesias Concerns regarding driving- since not staying in his lane, drifting towards incoming traffic. Not getting lost. Chronic problems with irritability and anger. Hx of depression, personality problems.
3 Initial Evaluation (cont d) Late hands shaking, difficulty with yard work and painting Hx falls and minor incontinence for a couple of yrs. Cane for 5 yrs, occasional walker Recent difficulties with organization and taking medications Can handle money and operate home appliances MMSE= 26 (06/2005) 25 (4/2006); started on Aricept (5 mg), MCI vs. mild dementia?, increased to 10 mg (8/2006).

4 Initial Evaluation PMH: CVA 2000, mild hypertension increased cholesterol Meds: amitriptyline (25 mg), Gabapentin (800 TiD), HCTZ, Simvastatin SH: retired mechanic, 12 yrs. Educ., Smoked 100 pkyrs then quit in 2002, no current ETOH FH: Mother had LO-AD
5 Physical Exam (IE) PE: Cor- frequent PVCs. Ext- decreased pulses in the LEs. Neuro Exam: MMSE = 29/30 (-1 season) BIMC = 32/33 CNS: decreased sensation lower L face, decreased hearing bilaterally Motor: slightly spastic L arm; decrease in strength L arm and leg; L intention tremor; decreased RAMs on L more than R. DTRS: 3+ L KJ; 2+ R side except absent AJs bilaterally; L plantar responses equivocal. No Frontal Release Signs.
6 Consensus Diagnosis Multi-domain amnestic MCI; vascular etiology likely, AD somewhat likely
7 1 year later. No decline in cognitive function Wears pad for some urinary incontinence, No bowel incont. Wife continues to dispense meds Mood good, but occasionally crabby, sleeps 12 hrs/night Uses a cane to support knees No longer drives, but has license No difficulty with basic ADL s Goes to church, bowls weekly (scores ~ 135), watches TV, plays dominoes

8 Neuro Exam: 1 year later MMSE= 26 (-1 year, day, date, place) STM: 2/5 on name and address 4/5 with cue 1.5/3 nonsense shapes after delay, intact recognition Motor: slight L arm spasticity, strength 5- R side; L WE, BC, TC 4+; deltoid 4; FE, FF 4-; L leg 4+ except dorsiflexors and plantar flexors 5-; RAMs moderately reduced on L, mildly reduced on R; No limb ataxia, Couldn t do HTS on L. DTRs: 2 upper extremities and sym., 2+ KJs, trace AJs. L toe equivocal. Gait: need to push off to arise. Neg. Romberg & Pull test.
9 Additional F/U visits 2 years later MMSE 24/30 & BDS 23/33 5 years later MMSE 16/30 & BDS 13/33 CDR = 2
10 End-of-life History Died 05/22/1010 Due to Pulmonary embolism. No Hx of additional strokes.
11 Longitudinal Cognitve Performance Executive Memory



12 MRI Results

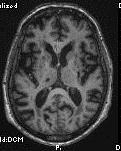
13 MRI Results

14 PiB Imaging
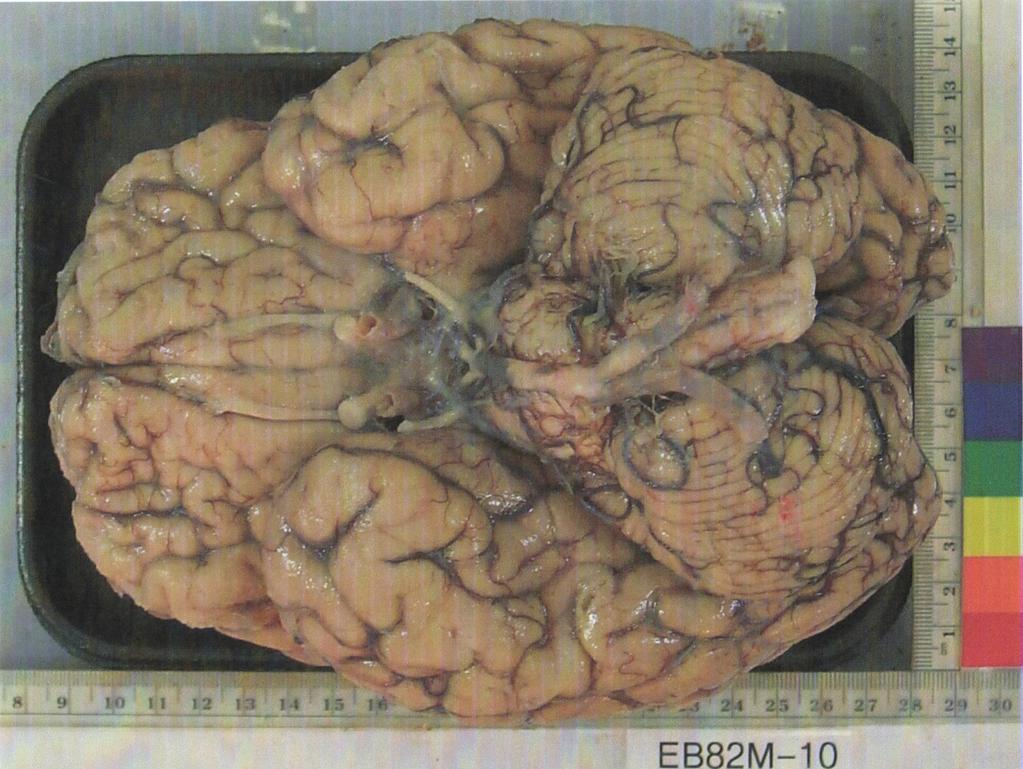
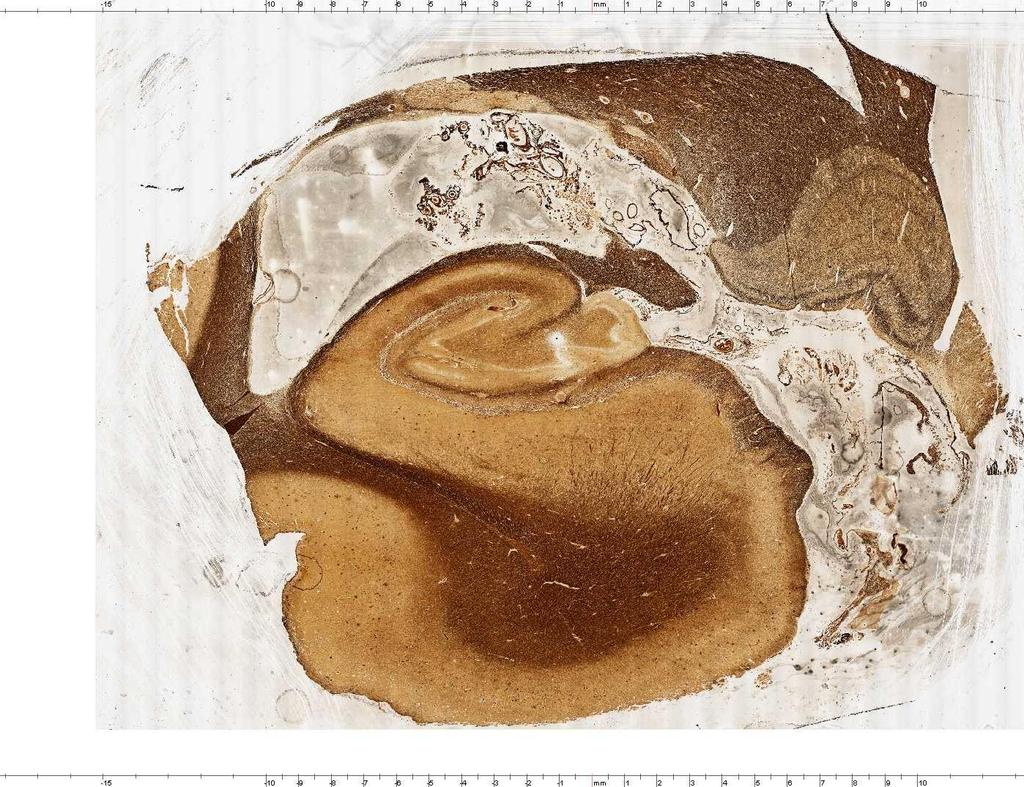
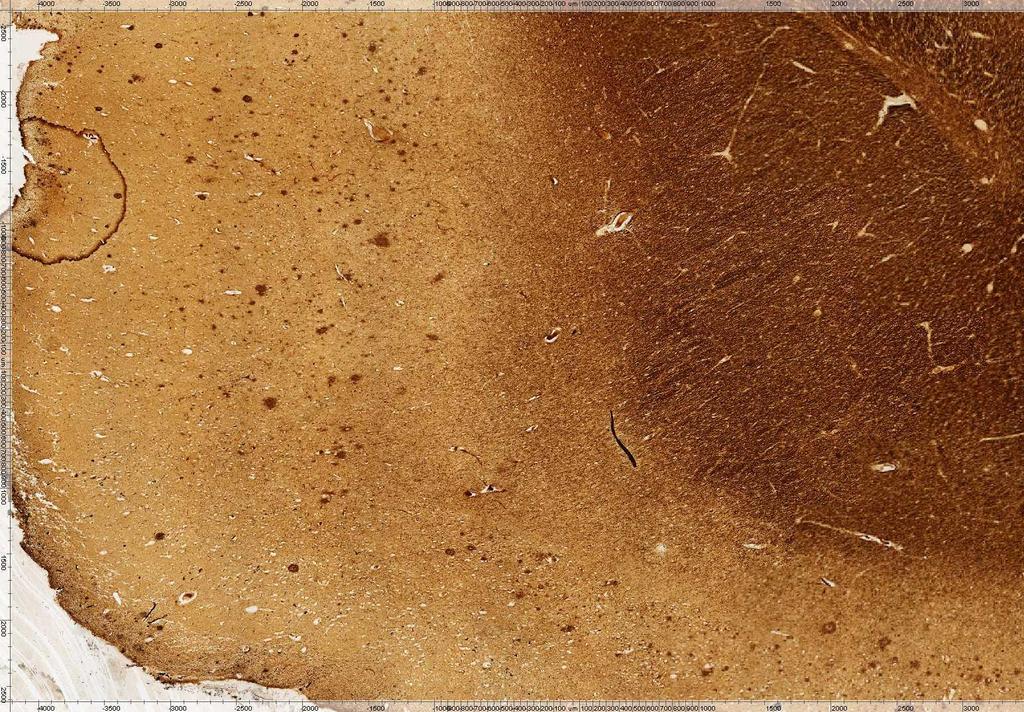
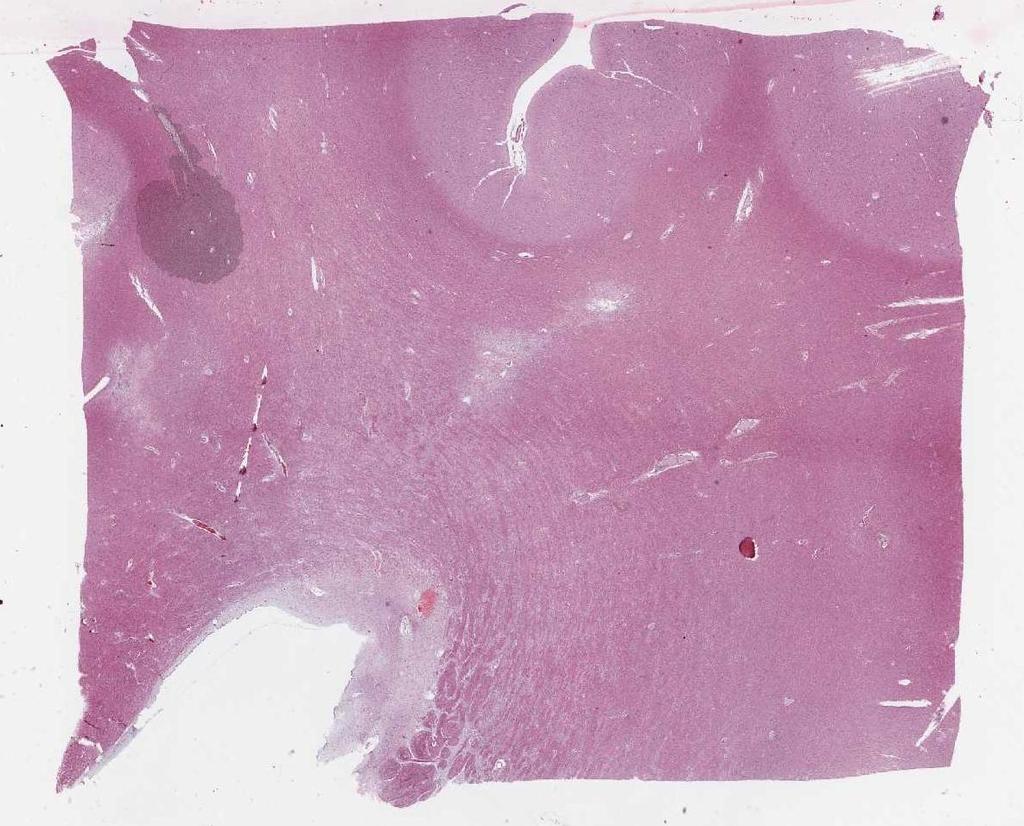
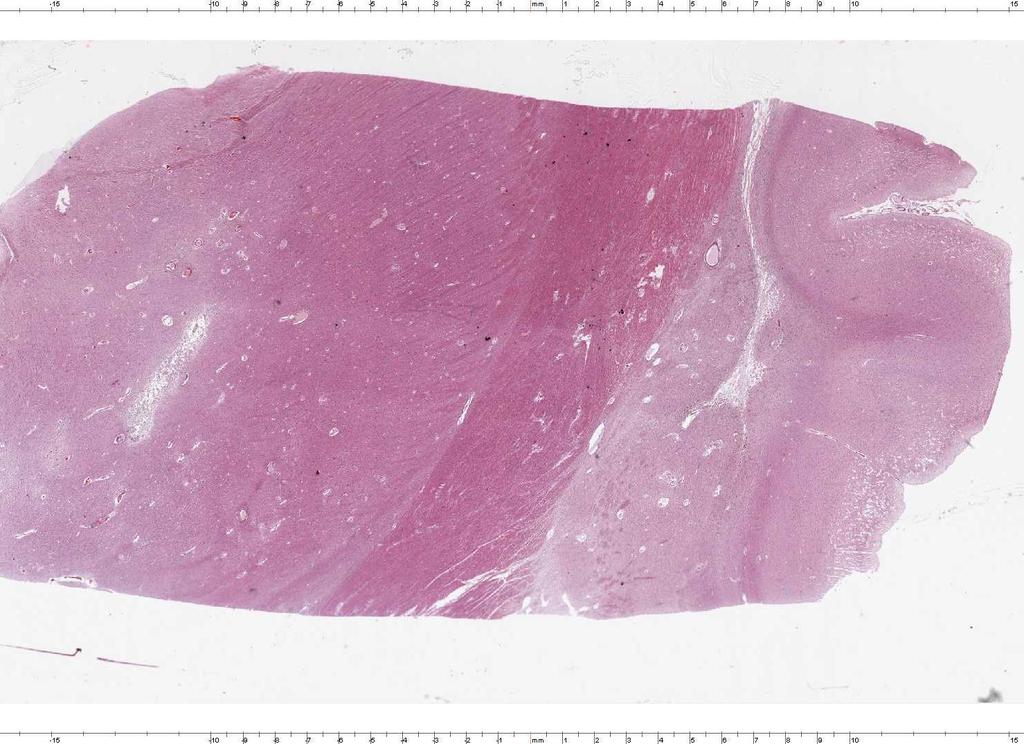
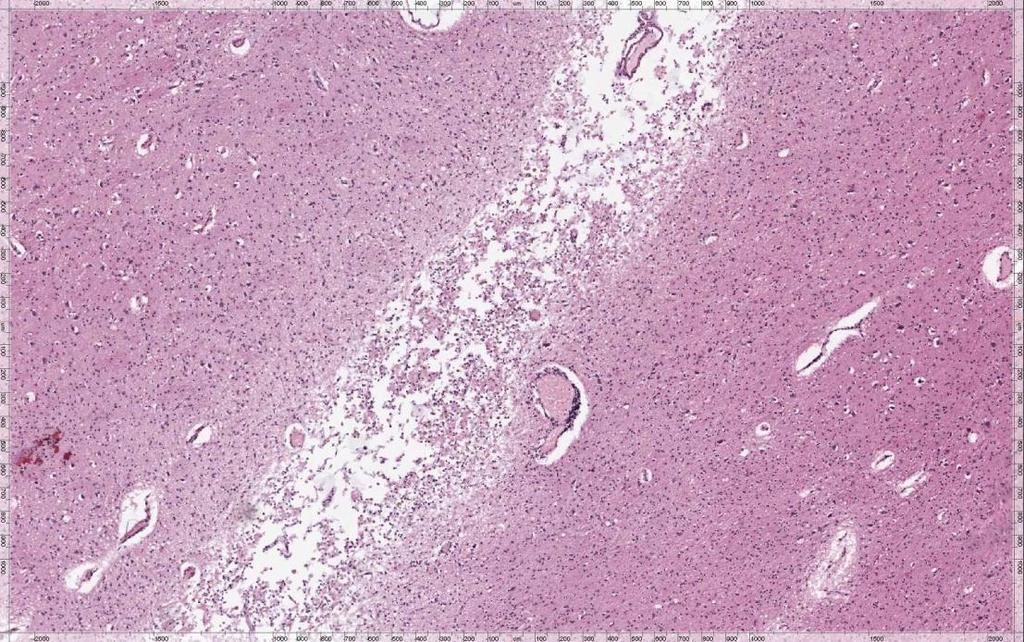
15 GROSS BRAIN EXAM Brain weight (fixed): 1333 grams. Moderate to severe atherosclerosis of the circle of Willis. Bilateral and multifocal cystic, non-cavitary, and lacunar infarcts in subcortical white matter and basal ganglia. Old lacunar infarct basis pontis.
16

17
18
19
20

21
22
23
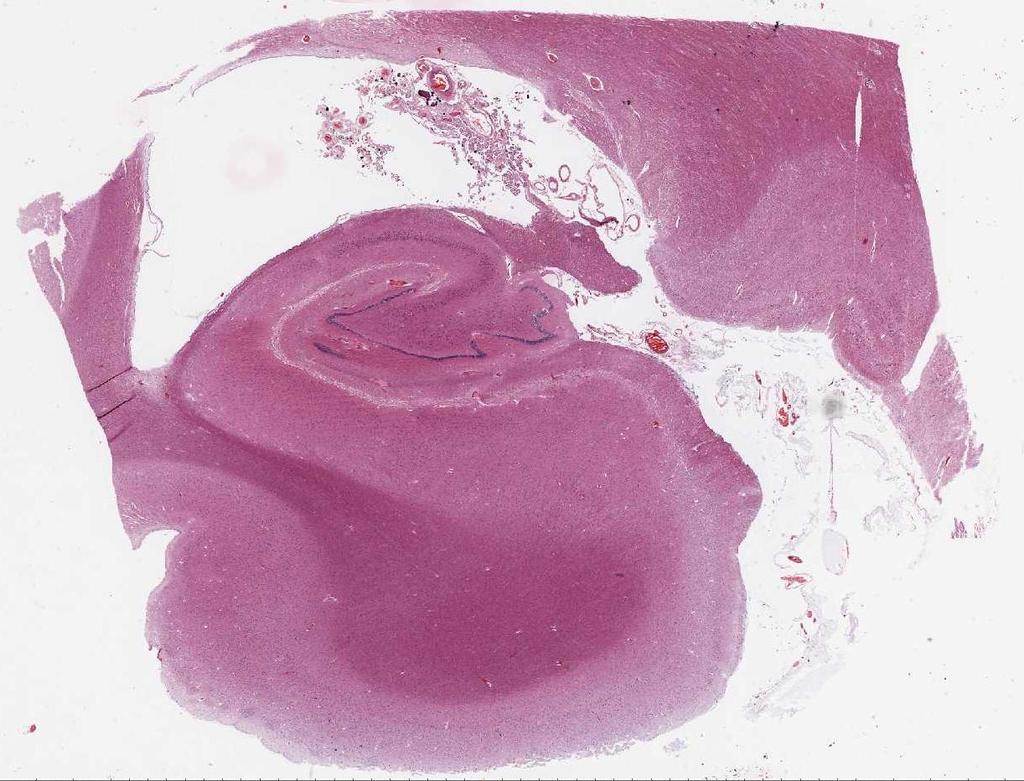
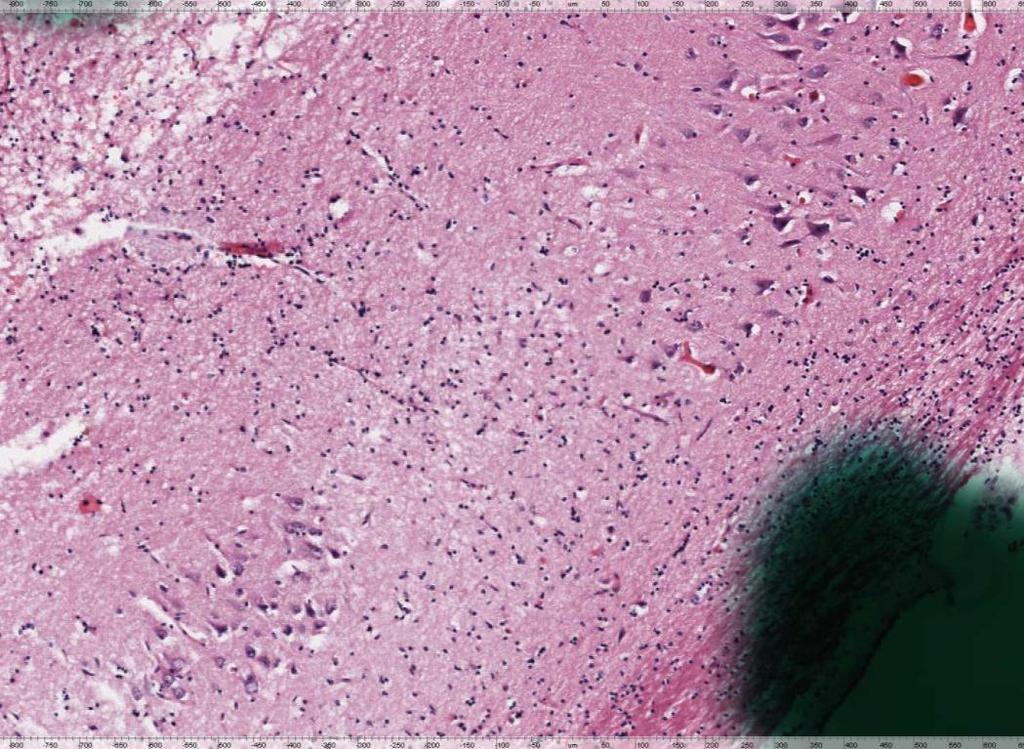
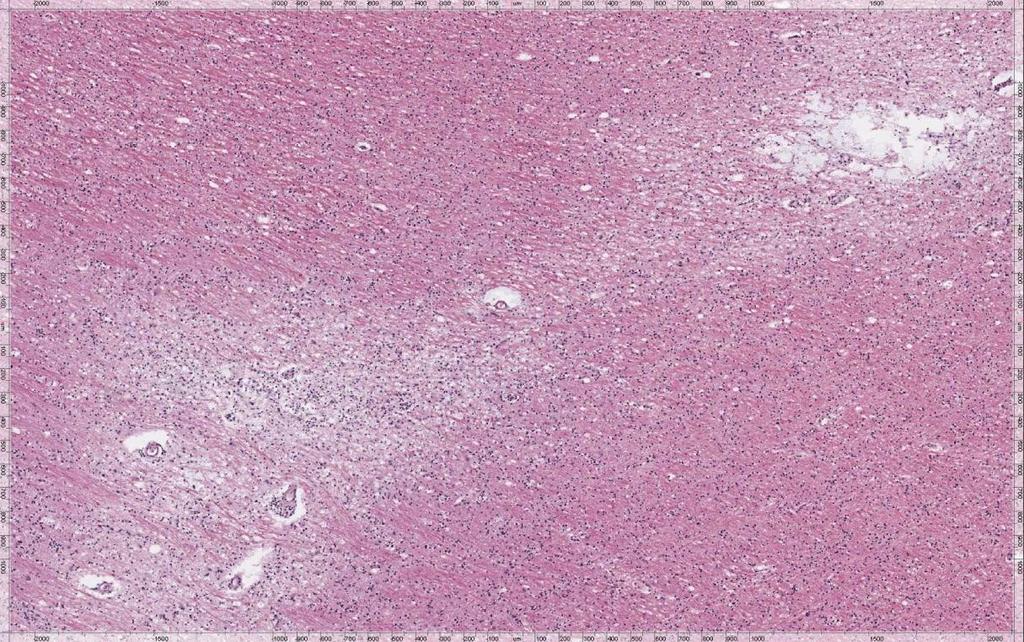
24 NEUROPATHOLOGIC DIAGNOSIS Cerebrovascular disease: Atherosclerosis, moderately severe in major branches of the circle of Willis, extending focally into many leptomeningeal arteries Arteriolosclerosis/ lipohyalinosis, variably severe throughout the brain, in many parenchymal arteries Vascular calcinosis, severe and extensive, in ganglionic arteries
25 NEUROPATHOLOGIC DIAGNOSIS Alzheimer s disease changes, Braak stage III: Neurofibrillary tangles confined to the hippocampi/parahippocampal regions Senile plaques, sparse to moderate, in cortex and hippocampi No amyloid angiopathy
26 Key Findings History of stroke Focal findings on clinical examination consistent with history of stroke Imaging features of substantial CVD Lack of severe cognitive impairment at initial assessment despite functional impairment
Clinical Differences Among Four Common Dementia Syndromes. a program of Morningside Ministries
 Clinical Differences Among Four Common Dementia Syndromes a program of Morningside Ministries Introduction Four clinical dementia syndromes account for 90% of all cases after excluding reversible causes
Clinical Differences Among Four Common Dementia Syndromes a program of Morningside Ministries Introduction Four clinical dementia syndromes account for 90% of all cases after excluding reversible causes
The Person: Dementia Basics
 The Person: Dementia Basics Objectives 1. Discuss how expected age related changes in the brain might affect an individual's cognition and functioning 2. Discuss how changes in the brain due to Alzheimer
The Person: Dementia Basics Objectives 1. Discuss how expected age related changes in the brain might affect an individual's cognition and functioning 2. Discuss how changes in the brain due to Alzheimer
Dementia. Assessing Brain Damage. Mental Status Examination
 Dementia Assessing Brain Damage Mental status examination Information about current behavior and thought including orientation to reality, memory, and ability to follow instructions Neuropsychological
Dementia Assessing Brain Damage Mental status examination Information about current behavior and thought including orientation to reality, memory, and ability to follow instructions Neuropsychological
Form D1: Clinician Diagnosis
 Initial Visit Packet Form D: Clinician Diagnosis NACC Uniform Data Set (UDS) ADC name: Subject ID: Form date: / / Visit #: Examiner s initials: INSTRUCTIONS: This form is to be completed by the clinician.
Initial Visit Packet Form D: Clinician Diagnosis NACC Uniform Data Set (UDS) ADC name: Subject ID: Form date: / / Visit #: Examiner s initials: INSTRUCTIONS: This form is to be completed by the clinician.
Assessing and Managing the Patient with Cognitive Decline
 Assessing and Managing the Patient with Cognitive Decline Center of Excellence For Alzheimer s Disease for State of NY Capital Region Alzheimer s Center of Albany Medical Center Earl A. Zimmerman, MD Professor
Assessing and Managing the Patient with Cognitive Decline Center of Excellence For Alzheimer s Disease for State of NY Capital Region Alzheimer s Center of Albany Medical Center Earl A. Zimmerman, MD Professor
DEMENTIA 101: WHAT IS HAPPENING IN THE BRAIN? Philip L. Rambo, PhD
 DEMENTIA 101: WHAT IS HAPPENING IN THE BRAIN? Philip L. Rambo, PhD OBJECTIVES Terminology/Dementia Basics Most Common Types Defining features Neuro-anatomical/pathological underpinnings Neuro-cognitive
DEMENTIA 101: WHAT IS HAPPENING IN THE BRAIN? Philip L. Rambo, PhD OBJECTIVES Terminology/Dementia Basics Most Common Types Defining features Neuro-anatomical/pathological underpinnings Neuro-cognitive
Vascular Dementia. Laura Pedelty, PhD MD The University of Illinois at Chicago and Jesse Brown VA Medical Center
 Vascular Dementia Laura Pedelty, PhD MD The University of Illinois at Chicago and Jesse Brown VA Medical Center none Disclosures Objectives To review the definition of Vascular Cognitive Impairment (VCI);
Vascular Dementia Laura Pedelty, PhD MD The University of Illinois at Chicago and Jesse Brown VA Medical Center none Disclosures Objectives To review the definition of Vascular Cognitive Impairment (VCI);
The ABCs of Dementia Diagnosis
 The ABCs of Dementia Diagnosis Dr. Robin Heinrichs, Ph.D., ABPP Board Certified Clinical Neuropsychologist Associate Professor, Psychiatry & Behavioral Sciences Director of Neuropsychology Training What
The ABCs of Dementia Diagnosis Dr. Robin Heinrichs, Ph.D., ABPP Board Certified Clinical Neuropsychologist Associate Professor, Psychiatry & Behavioral Sciences Director of Neuropsychology Training What
Caring Sheet #11: Alzheimer s Disease:
 CARING SHEETS: Caring Sheet #11: Alzheimer s Disease: A Summary of Information and Intervention Suggestions with an Emphasis on Cognition By Shelly E. Weaverdyck, PhD Introduction This caring sheet focuses
CARING SHEETS: Caring Sheet #11: Alzheimer s Disease: A Summary of Information and Intervention Suggestions with an Emphasis on Cognition By Shelly E. Weaverdyck, PhD Introduction This caring sheet focuses
Cesarean section for breech presentation. Jonathan H. Waters, M.D.
 Cesarean section for breech presentation Jonathan H. Waters, M.D. 1 26 y.o. G1P0 presented to triage in labor at 38 weeks. Patient was a known breech with a failed version 5 days before presentation. PMH
Cesarean section for breech presentation Jonathan H. Waters, M.D. 1 26 y.o. G1P0 presented to triage in labor at 38 weeks. Patient was a known breech with a failed version 5 days before presentation. PMH
A Hypothesis Driven Approach to the Neurological Exam
 A Hypothesis Driven Approach to the Neurological Exam Vanja Douglas, MD Assistant Clinical Professor UCSF Department of Neurology Disclosures None 1 Purpose of Neuro Exam Screen asymptomatic patients Screen
A Hypothesis Driven Approach to the Neurological Exam Vanja Douglas, MD Assistant Clinical Professor UCSF Department of Neurology Disclosures None 1 Purpose of Neuro Exam Screen asymptomatic patients Screen
How to Think like a Neurologist Review of Exam Process and Assessment Findings
 Lehigh Valley Health Network LVHN Scholarly Works Neurology Update for the Non-Neurologist 2013 Neurology Update for the Non-Neurologist Feb 20th, 5:10 PM - 5:40 PM How to Think like a Neurologist Review
Lehigh Valley Health Network LVHN Scholarly Works Neurology Update for the Non-Neurologist 2013 Neurology Update for the Non-Neurologist Feb 20th, 5:10 PM - 5:40 PM How to Think like a Neurologist Review
Evolution of a concept: Apraxia/higher level gait disorder. ataxia v. apraxia gait = limb apraxia. low, middle, high gait disturbance levels
 Case #1 81-year-old woman Gait Imbalance: Two Unusual Cases in Older Patients February 2008: 3 years of gradually progressive gait imbalance no vertigo, dizziness or paresthesias etiology unclear on examination
Case #1 81-year-old woman Gait Imbalance: Two Unusual Cases in Older Patients February 2008: 3 years of gradually progressive gait imbalance no vertigo, dizziness or paresthesias etiology unclear on examination
Early Intervention the Key to Geriatric Assessment: Geriatric Assessment Outreach Teams
 Early Intervention the Key to Geriatric Assessment: Geriatric Assessment Outreach Teams Regional Geriatric Program of Eastern Ontario Outpatient Clinics Geriatric Rehabilitation Unit Community Referrals
Early Intervention the Key to Geriatric Assessment: Geriatric Assessment Outreach Teams Regional Geriatric Program of Eastern Ontario Outpatient Clinics Geriatric Rehabilitation Unit Community Referrals
Patterns of Cognitive Impairment in Dementia
 Patterns of Cognitive Impairment in Dementia Lindsay R. Clark, PhD Assistant professor (CHS) Department of Medicine - Division of Geriatrics & Gerontology UW-Madison School of Medicine & Public Health
Patterns of Cognitive Impairment in Dementia Lindsay R. Clark, PhD Assistant professor (CHS) Department of Medicine - Division of Geriatrics & Gerontology UW-Madison School of Medicine & Public Health
Dementia. Stephen S. Flitman, MD Medical Director 21st Century Neurology
 Dementia Stephen S. Flitman, MD Medical Director 21st Century Neurology www.neurozone.org Dementia is a syndrome Progressive memory loss, plus Progressive loss of one or more cognitive functions: Language
Dementia Stephen S. Flitman, MD Medical Director 21st Century Neurology www.neurozone.org Dementia is a syndrome Progressive memory loss, plus Progressive loss of one or more cognitive functions: Language
Objectives. My Patient: The story 10/6/2017
 Objectives Our Grey Matter Matters: A Case in Point Vivien Brown MDCM, CCFP,FCFP, NCMP Assistant Professor, University of Toronto Vice President, Medical Affairs, Medisys Healthy Group Past President,
Objectives Our Grey Matter Matters: A Case in Point Vivien Brown MDCM, CCFP,FCFP, NCMP Assistant Professor, University of Toronto Vice President, Medical Affairs, Medisys Healthy Group Past President,
Patterns of Cognitive Impairment in Dementia
 Patterns of Cognitive Impairment in Dementia Lindsay R. Clark, PhD Assistant professor (CHS) Department of Medicine - Division of Geriatrics & Gerontology UW-Madison School of Medicine & Public Health
Patterns of Cognitive Impairment in Dementia Lindsay R. Clark, PhD Assistant professor (CHS) Department of Medicine - Division of Geriatrics & Gerontology UW-Madison School of Medicine & Public Health
High Yield Neurological Examination
 High Yield Neurological Examination Vanja Douglas, MD Sara & Evan Williams Foundation Endowed Neurohospitalist Chair Director, Neurohospitalist Division Associate Professor of Clinical Neurology UCSF Department
High Yield Neurological Examination Vanja Douglas, MD Sara & Evan Williams Foundation Endowed Neurohospitalist Chair Director, Neurohospitalist Division Associate Professor of Clinical Neurology UCSF Department
Neuroanatomy of a Stroke. Joni Clark, MD Professor of Neurology Barrow Neurologic Institute
 Neuroanatomy of a Stroke Joni Clark, MD Professor of Neurology Barrow Neurologic Institute No disclosures Stroke case presentations Review signs and symptoms Review pertinent exam findings Identify the
Neuroanatomy of a Stroke Joni Clark, MD Professor of Neurology Barrow Neurologic Institute No disclosures Stroke case presentations Review signs and symptoms Review pertinent exam findings Identify the
Alzheimer s Disease without Dementia
 Alzheimer s Disease without Dementia Dr Emer MacSweeney CEO & Consultant Neuroradiologist Re:Cognition Health London Osteopathic Society 13 September 2016 Early diagnosis of Alzheimer s Disease How and
Alzheimer s Disease without Dementia Dr Emer MacSweeney CEO & Consultant Neuroradiologist Re:Cognition Health London Osteopathic Society 13 September 2016 Early diagnosis of Alzheimer s Disease How and
UNIVERSITY OF WESTERN ONTARIO
 UNIVERSITY OF WESTERN ONTARIO Vladimir Hachinski, CM, MD, FRCPC, DSc Department of Clinical Neurological Sciences University of Western Ontario London, Ontario, Canada Vladimir.hachinski@lhsc.on.ca ALZHEIMER
UNIVERSITY OF WESTERN ONTARIO Vladimir Hachinski, CM, MD, FRCPC, DSc Department of Clinical Neurological Sciences University of Western Ontario London, Ontario, Canada Vladimir.hachinski@lhsc.on.ca ALZHEIMER
Carol Manning, PhD, ABPP-CN Director, Memory Disorders Clinic University of Virginia
 Carol Manning, PhD, ABPP-CN Director, Memory Disorders Clinic University of Virginia Case Study Mr. S. is a 74 year old man who has smoked for 20 years. He is overweight, has high cholesterol and high
Carol Manning, PhD, ABPP-CN Director, Memory Disorders Clinic University of Virginia Case Study Mr. S. is a 74 year old man who has smoked for 20 years. He is overweight, has high cholesterol and high
Moving Targets: An Update on Diagnosing Dementia in the Clinic
 Moving Targets: An Update on Diagnosing Dementia in the Clinic Eric McDade DO Department of Neurology School of Medicine Alzheimer Disease Research Center Disclosures No relevant financial disclosures
Moving Targets: An Update on Diagnosing Dementia in the Clinic Eric McDade DO Department of Neurology School of Medicine Alzheimer Disease Research Center Disclosures No relevant financial disclosures
Alzheimer s disease dementia: a neuropsychological approach
 Alzheimer s disease dementia: a neuropsychological approach Dr. Roberta Biundo, PhD Neuropsychology Coordinator at Parkinson s disease and movement disorders unit of San Camillo rehabilitation hospital
Alzheimer s disease dementia: a neuropsychological approach Dr. Roberta Biundo, PhD Neuropsychology Coordinator at Parkinson s disease and movement disorders unit of San Camillo rehabilitation hospital
Spinal Cord: Clinical Applications. Dr. Stuart Inglis
 Spinal Cord: Clinical Applications Dr. Stuart Inglis Tabes dorsalis, also known as syphilitic myelopathy, is a slow degeneration (specifically, demyelination) of the nerves in the dorsal funiculus of the
Spinal Cord: Clinical Applications Dr. Stuart Inglis Tabes dorsalis, also known as syphilitic myelopathy, is a slow degeneration (specifically, demyelination) of the nerves in the dorsal funiculus of the
MOS SF-36 health survey (Ware &
 Biomedical and Physical Functioning General Health Height Weight Waist Circumfernece % Body Fat Tanita scale BMI Self-rated Health - overall clinical protocol Self-rated Health - rel. to age clinical protocol
Biomedical and Physical Functioning General Health Height Weight Waist Circumfernece % Body Fat Tanita scale BMI Self-rated Health - overall clinical protocol Self-rated Health - rel. to age clinical protocol
Dementia. Aetiology, pathophysiology and the role of neuropsychological testing. Dr Sheng Ling Low Geriatrician
 Dementia Aetiology, pathophysiology and the role of neuropsychological testing Dr Sheng Ling Low Geriatrician Topics to cover Why is dementia important What is dementia Differentiate between dementia,
Dementia Aetiology, pathophysiology and the role of neuropsychological testing Dr Sheng Ling Low Geriatrician Topics to cover Why is dementia important What is dementia Differentiate between dementia,
What if it s not Alzheimer s? Update on Lewy body dementia and frontotemporal dementia
 What if it s not Alzheimer s? Update on Lewy body dementia and frontotemporal dementia Dementia: broad term for any acquired brain condition impairing mental function such that ADLs are impaired. Includes:
What if it s not Alzheimer s? Update on Lewy body dementia and frontotemporal dementia Dementia: broad term for any acquired brain condition impairing mental function such that ADLs are impaired. Includes:
Diagnosis and management of non-alzheimer dementias. Melissa Yu, M.D. Department of Neurology
 Diagnosis and management of non-alzheimer dementias Melissa Yu, M.D. Department of Neurology AGENDA Introduction When to think of alternate diagnoses Other forms of dementia Other reasons for confusion
Diagnosis and management of non-alzheimer dementias Melissa Yu, M.D. Department of Neurology AGENDA Introduction When to think of alternate diagnoses Other forms of dementia Other reasons for confusion
ICR SYMPOSIUM ON HOMOEOPATHIC PRESCRIBING DECEMBER 2018, MUMBAI EXPLORING DR. C. M. BOGER S PHILOSOPHY & ITS APPLICATION IN CLINICAL PRACTICE
 DR.SUNIT NIKUMH - CSE-3 OGER SYMPOSIUM/DECEMER 2018 Objectives : 1. Importance of study of Structure-Function-Form-Time axis (SFFT) in lcohol withdrawal cases 2. Illustrating the Value of pathological
DR.SUNIT NIKUMH - CSE-3 OGER SYMPOSIUM/DECEMER 2018 Objectives : 1. Importance of study of Structure-Function-Form-Time axis (SFFT) in lcohol withdrawal cases 2. Illustrating the Value of pathological
The Neurological System. Neurological Exam 5 Components. Mental Status Examination
 The Neurological System 1 Neurological Exam 5 Components Mental status Cranial nerves Reflexes Motor- includes Cerebellar function Sensory 2 Mental Status Examination Examination - ABCT Appearance Behavior
The Neurological System 1 Neurological Exam 5 Components Mental status Cranial nerves Reflexes Motor- includes Cerebellar function Sensory 2 Mental Status Examination Examination - ABCT Appearance Behavior
This presentation is the intellectual property of the author. Contact them for permission to reprint and/or distribute.
 Medically Refractory Epilepsy with a Temporal Lobe Lesion Steven Ellis, MD Neurophysiology Fellow, PGY-5 UT Health San Antonio History No history of febrile seizures, meningitis, encephalitis, or head
Medically Refractory Epilepsy with a Temporal Lobe Lesion Steven Ellis, MD Neurophysiology Fellow, PGY-5 UT Health San Antonio History No history of febrile seizures, meningitis, encephalitis, or head
Delirium & Dementia. Nicholas J. Silvestri, MD
 Delirium & Dementia Nicholas J. Silvestri, MD Outline Delirium vs. Dementia Neural pathways relating to consciousness Encephalopathy Stupor Coma Dementia Delirium vs. Dementia Delirium Abrupt onset Lasts
Delirium & Dementia Nicholas J. Silvestri, MD Outline Delirium vs. Dementia Neural pathways relating to consciousness Encephalopathy Stupor Coma Dementia Delirium vs. Dementia Delirium Abrupt onset Lasts
Dementia is not normal aging!
 The Future of Alzheimer s Disease Treatment Adam L. Boxer, MD, PhD Director, Alzheimer s Disease Clinical Trials Program Memory and Aging Center Assistant Professor of Neurology University of California,
The Future of Alzheimer s Disease Treatment Adam L. Boxer, MD, PhD Director, Alzheimer s Disease Clinical Trials Program Memory and Aging Center Assistant Professor of Neurology University of California,
Acute stroke. Ischaemic stroke. Characteristics. Temporal classification. Clinical features. Interpretation of Emergency Head CT
 Ischaemic stroke Characteristics Stroke is the third most common cause of death in the UK, and the leading cause of disability. 80% of strokes are ischaemic Large vessel occlusive atheromatous disease
Ischaemic stroke Characteristics Stroke is the third most common cause of death in the UK, and the leading cause of disability. 80% of strokes are ischaemic Large vessel occlusive atheromatous disease
Mental Health Counseling for mood, aging, and coping with life transitions and chronic illness.
 Mental Health Counseling for mood, aging, and coping with life transitions and chronic illness. Silver Linings for Seniors Silver Linings for Seniors, Inc. offers on-site confidential Mental Health Counseling
Mental Health Counseling for mood, aging, and coping with life transitions and chronic illness. Silver Linings for Seniors Silver Linings for Seniors, Inc. offers on-site confidential Mental Health Counseling
PROJECTION: Worlds dementia population is expected to triple by 2050
 DEMENTIA C L I S K C O N S U LTA N T P H Y S I C I A N I N A C U T E M E D I C I N E A N D G E R I AT R I C M E D I C I N E, B A R N E T H O S P I TA L, R O YA L F R E E N H S F O U N D AT I O N T R U
DEMENTIA C L I S K C O N S U LTA N T P H Y S I C I A N I N A C U T E M E D I C I N E A N D G E R I AT R I C M E D I C I N E, B A R N E T H O S P I TA L, R O YA L F R E E N H S F O U N D AT I O N T R U
Memory Loss, Dementia and Alzheimer's Disease: The Basics
 Memory Loss, Dementia and Alzheimer's Disease: The Basics What is memory loss? What is age-related memory loss? Typical changes Typical age-related changes involve: Making a bad decision once in a while
Memory Loss, Dementia and Alzheimer's Disease: The Basics What is memory loss? What is age-related memory loss? Typical changes Typical age-related changes involve: Making a bad decision once in a while
Disorders of the Nervous System. Disorders of the Neurological System. General Endpoints of CNS Disease. General Endpoints of CNS Disease
 HD in Nursing-Pathophysiology Disorders of the Nervous System What are some disorders of the nervous system? Disorders of the Neurological System Dr. C.H. Lai The nervous system is vulnerable to various
HD in Nursing-Pathophysiology Disorders of the Nervous System What are some disorders of the nervous system? Disorders of the Neurological System Dr. C.H. Lai The nervous system is vulnerable to various
1st interactive course in MS advanced managment
 6-7 December - Toronto, Canada 1st interactive course in MS advanced managment IMPROVING THE PATIENT S LIFE THROUGH MEDICAL EDUCATION www.excemed.org Liesly Lee Sunnybrook Health Sciences Centre. Department
6-7 December - Toronto, Canada 1st interactive course in MS advanced managment IMPROVING THE PATIENT S LIFE THROUGH MEDICAL EDUCATION www.excemed.org Liesly Lee Sunnybrook Health Sciences Centre. Department
Type 2 Diabetes and Brain Disease in Older Adults. Erin L. Abner, PhD, MPH Asst. Professor University Of Kentucky
 Type 2 Diabetes and Brain Disease in Older Adults Erin L. Abner, PhD, MPH Asst. Professor University Of Kentucky Disclosures to Participants Requirements for Successful Completion: For successful completion,
Type 2 Diabetes and Brain Disease in Older Adults Erin L. Abner, PhD, MPH Asst. Professor University Of Kentucky Disclosures to Participants Requirements for Successful Completion: For successful completion,
ALZHEIMER S DISEASE. Mary-Letitia Timiras M.D. Overlook Hospital Summit, New Jersey
 ALZHEIMER S DISEASE Mary-Letitia Timiras M.D. Overlook Hospital Summit, New Jersey Topics Covered Demography Clinical manifestations Pathophysiology Diagnosis Treatment Future trends Prevalence and Impact
ALZHEIMER S DISEASE Mary-Letitia Timiras M.D. Overlook Hospital Summit, New Jersey Topics Covered Demography Clinical manifestations Pathophysiology Diagnosis Treatment Future trends Prevalence and Impact
Mild Cognitive Impairment (MCI)
") October 19, 2018 Mild Cognitive Impairment (MCI) Yonas E. Geda, MD, MSc Professor of Neurology and Psychiatry Consultant, Departments of Psychiatry & Psychology, and Neurology Mayo Clinic College of Medicine
October 19, 2018 Mild Cognitive Impairment (MCI) Yonas E. Geda, MD, MSc Professor of Neurology and Psychiatry Consultant, Departments of Psychiatry & Psychology, and Neurology Mayo Clinic College of Medicine
Dementia is an overall term for a set of symptoms that is caused by disorders affecting the brain.
 Vascular Dementia Vascular Dementia Other Dementias This information sheet provides an overview of a type of dementia known as vascular dementia. In this information sheet you will find: An overview of
Vascular Dementia Vascular Dementia Other Dementias This information sheet provides an overview of a type of dementia known as vascular dementia. In this information sheet you will find: An overview of
Gary Rea MD PhD Medical Director OSU Comprehensive Spine Center
 Gary Rea MD PhD Medical Director OSU Comprehensive Spine Center 1. The less specific the patient is about symptoms and pain, the less likely a specific diagnosis will be made and the less likely the patient
Gary Rea MD PhD Medical Director OSU Comprehensive Spine Center 1. The less specific the patient is about symptoms and pain, the less likely a specific diagnosis will be made and the less likely the patient
Active Learning Strategies for Mastering Geriatric Assessment Tools
 Active Learning Strategies for Mastering Geriatric Assessment Tools Sara McCumber, MS, RN, CNP, CNS Family Nurse Practitioner & Adult-Gerontological Primary Care NP The College of St. Scholastica Nursing
Active Learning Strategies for Mastering Geriatric Assessment Tools Sara McCumber, MS, RN, CNP, CNS Family Nurse Practitioner & Adult-Gerontological Primary Care NP The College of St. Scholastica Nursing
FRONTOTEMPORAL DEGENERATION: OVERVIEW, TRENDS AND DEVELOPMENTS
 FRONTOTEMPORAL DEGENERATION: OVERVIEW, TRENDS AND DEVELOPMENTS Norman L. Foster, M.D. Director, Center for Alzheimer s Care, Imaging and Research Chief, Division of Cognitive Neurology, Department of Neurology
FRONTOTEMPORAL DEGENERATION: OVERVIEW, TRENDS AND DEVELOPMENTS Norman L. Foster, M.D. Director, Center for Alzheimer s Care, Imaging and Research Chief, Division of Cognitive Neurology, Department of Neurology
ID # COMPLETED: YES.. 1 DATE NO... 5 NEUROLOGICAL EXAM
 ID # COMPLETED: YES.. 1 DATE NO... 5 NEUROLOGICAL EXAM VIDEOTAPED: YES.. 1 NO... 5 COMMENT: NEUROLOGICAL EXAM "Normal, Abnormal, Other, Can't execute or Missing for each question. Always complete specify
ID # COMPLETED: YES.. 1 DATE NO... 5 NEUROLOGICAL EXAM VIDEOTAPED: YES.. 1 NO... 5 COMMENT: NEUROLOGICAL EXAM "Normal, Abnormal, Other, Can't execute or Missing for each question. Always complete specify
Dementia: How to explain the diagnosis to patients and relatives
 GPHot Topics (April 2017): Dementia: How to explain the diagnosis to patients and relatives mohammad somauroo Consultant Physician with specialist interest in Community Geriatrics Royal Liverpool and Broadgreen
GPHot Topics (April 2017): Dementia: How to explain the diagnosis to patients and relatives mohammad somauroo Consultant Physician with specialist interest in Community Geriatrics Royal Liverpool and Broadgreen
Cerebrovascular Disorders. Blood, Brain, and Energy. Blood Supply to the Brain 2/14/11
 Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
Neuropsychiatric Manifestations in Vascular Cognitive Impairment Patients with and without Dementia
 86 Neuropsychiatric Manifestations in Vascular Cognitive Impairment Patients with and without Dementia Pai-Yi Chiu 1,3, Chung-Hsiang Liu 2, and Chon-Haw Tsai 2 Abstract- Background: Neuropsychiatric profile
86 Neuropsychiatric Manifestations in Vascular Cognitive Impairment Patients with and without Dementia Pai-Yi Chiu 1,3, Chung-Hsiang Liu 2, and Chon-Haw Tsai 2 Abstract- Background: Neuropsychiatric profile
Why should white matter changes be taken into account; the clinical dementia perspective
 Kista, Sept 15, 2016 Why should white matter changes be taken into account; the clinical dementia perspective Anders Wallin MD, PhD, Prof, Institute of Neuroscience and Physiology at Sahlgrenska Academy,
Kista, Sept 15, 2016 Why should white matter changes be taken into account; the clinical dementia perspective Anders Wallin MD, PhD, Prof, Institute of Neuroscience and Physiology at Sahlgrenska Academy,
Assessment at the bedside or in the clinic using the history, examination and laboratory tests to distinguish between different types of dementia
 Assessment at the bedside or in the clinic using the history, examination and laboratory tests to distinguish between different types of dementia AP Passmore Content Common dementia syndromes (older people)
Assessment at the bedside or in the clinic using the history, examination and laboratory tests to distinguish between different types of dementia AP Passmore Content Common dementia syndromes (older people)
SECTION 1: as each other, or as me. THE BRAIN AND DEMENTIA. C. Boden *
 I read all the available books by other [people with] Alzheimer s disease but they never had quite the same problems as each other, or as me. I t s not like other diseases, where there is a standard set
I read all the available books by other [people with] Alzheimer s disease but they never had quite the same problems as each other, or as me. I t s not like other diseases, where there is a standard set
Next patient please Dementia Clare Hawley 2018
 Next patient please Dementia Clare Hawley 2018 I have no conflict of interest to declare Dr Clare Hawley Associate Specialist Cardiology Chesterfield Royal Hospital GPwSI Refractory Angina Hon Clinical
Next patient please Dementia Clare Hawley 2018 I have no conflict of interest to declare Dr Clare Hawley Associate Specialist Cardiology Chesterfield Royal Hospital GPwSI Refractory Angina Hon Clinical
WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient
 DEMENTIA WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient Progressive and disabling Not an inherent aspect of
DEMENTIA WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient Progressive and disabling Not an inherent aspect of
Dementia and Healthy Ageing : is the pathology any different?
 Dementia and Healthy Ageing : is the pathology any different? Professor David Mann, Professor of Neuropathology, University of Manchester, Hope Hospital, Salford DEMENTIA Loss of connectivity within association
Dementia and Healthy Ageing : is the pathology any different? Professor David Mann, Professor of Neuropathology, University of Manchester, Hope Hospital, Salford DEMENTIA Loss of connectivity within association
3/6/2019 DIAGNOSIS OF DEMENTIA IN THE OUTPATIENT SETTING FINANCIAL DISCLOSURES LEARNING OBJECTIVES
 DIAGNOSIS OF DEMENTIA IN THE OUTPATIENT SETTING MILTA LITTLE, DO, CMD DUKE UNIVERSITY SCHOOL OF MEDICINE FINANCIAL DISCLOSURES Dr. Little has no relevant financial disclosures to report Dr. Little will
DIAGNOSIS OF DEMENTIA IN THE OUTPATIENT SETTING MILTA LITTLE, DO, CMD DUKE UNIVERSITY SCHOOL OF MEDICINE FINANCIAL DISCLOSURES Dr. Little has no relevant financial disclosures to report Dr. Little will
Getting Help for Patients with Dementia and their Caregivers. Erica Salamida Associate Director of Programs and Services Alzheimer s Association-NENY
 Getting Help for Patients with Dementia and their Caregivers Erica Salamida Associate Director of Programs and Services Alzheimer s Association-NENY In this session you will learn about: Symptoms of dementia,
Getting Help for Patients with Dementia and their Caregivers Erica Salamida Associate Director of Programs and Services Alzheimer s Association-NENY In this session you will learn about: Symptoms of dementia,
A Fresh View of Cognitive Disorders in Older Adults: New Classification and Screening Strategies
 A Fresh View of Cognitive Disorders in Older Adults: New Classification and Screening Strategies Lynda Mackin, PhD, AGPCNP-BC, CNS University of California San Francisco School of Nursing 1 Alzheimer s
A Fresh View of Cognitive Disorders in Older Adults: New Classification and Screening Strategies Lynda Mackin, PhD, AGPCNP-BC, CNS University of California San Francisco School of Nursing 1 Alzheimer s
Dementia the A,B,Cs. Dr. Frank Molnar. Associate Professor of Medicine, University of Ottawa Division of Geriatric Medicine, the Ottawa Hospital
 Dementia the A,B,Cs Dr. Frank Molnar Associate Professor of Medicine, University of Ottawa Division of Geriatric Medicine, the Ottawa Hospital Implications for Practice Dementia the A,B,Cs (Dr. Frank Molnar)
Dementia the A,B,Cs Dr. Frank Molnar Associate Professor of Medicine, University of Ottawa Division of Geriatric Medicine, the Ottawa Hospital Implications for Practice Dementia the A,B,Cs (Dr. Frank Molnar)
Non Alzheimer Dementias
 Non Alzheimer Dementias Randolph B Schiffer Department of Neuropsychiatry and Behavioral Science Texas Tech University Health Sciences Center 9/11/2007 Statement of Financial Disclosure Randolph B Schiffer,,
Non Alzheimer Dementias Randolph B Schiffer Department of Neuropsychiatry and Behavioral Science Texas Tech University Health Sciences Center 9/11/2007 Statement of Financial Disclosure Randolph B Schiffer,,
Overview of neurological changes in Alzheimer s disease. Eric Karran
 Overview of neurological changes in Alzheimer s disease Eric Karran Alzheimer s disease Alois Alzheimer 1864-1915 Auguste D. 1850-1906 Case presented November 26 th 1906 Guildford Talk.ppt 20 th March,
Overview of neurological changes in Alzheimer s disease Eric Karran Alzheimer s disease Alois Alzheimer 1864-1915 Auguste D. 1850-1906 Case presented November 26 th 1906 Guildford Talk.ppt 20 th March,
How to Do the EDSS. Stephen S. Kamin, MD New Jersey Medical School
 How to Do the EDSS Stephen S. Kamin, MD New Jersey Medical School John F. Kurtzke, MD 1926-2015 EDSS Expanded Disability Status Scale Devised by John Kurtzke in the 1960s and modified in the 1980s EDSS
How to Do the EDSS Stephen S. Kamin, MD New Jersey Medical School John F. Kurtzke, MD 1926-2015 EDSS Expanded Disability Status Scale Devised by John Kurtzke in the 1960s and modified in the 1980s EDSS
LABs Albumin. (g/dl) Haemoglobin, (g/l) Creatinin, (mg/dl)
 Haemoglobin, (g/l) Creatinin, (mg/dl)") DATA COLLECTION SHEET CRF B Baseline evaluation Center ID: Patient code: Date of birth (dd/mm/yyyy): / / Sex: Male Female Living situation: home independent home with family/care giver residential care
DATA COLLECTION SHEET CRF B Baseline evaluation Center ID: Patient code: Date of birth (dd/mm/yyyy): / / Sex: Male Female Living situation: home independent home with family/care giver residential care
Imaging of Alzheimer s Disease: State of the Art
 July 2015 Imaging of Alzheimer s Disease: State of the Art Neir Eshel, Harvard Medical School Year IV Outline Our patient Definition of dementia Alzheimer s disease Epidemiology Diagnosis Stages of progression
July 2015 Imaging of Alzheimer s Disease: State of the Art Neir Eshel, Harvard Medical School Year IV Outline Our patient Definition of dementia Alzheimer s disease Epidemiology Diagnosis Stages of progression
Stroke School for Internists Part 1
 Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Reassessment: Neuroimaging in the Emergency Patient Presenting with Seizure
 Reassessment: Neuroimaging in the Emergency Patient Presenting with Seizure This evidence-based report provides clinicians with information to identify which seizure patients in the emergency department
Reassessment: Neuroimaging in the Emergency Patient Presenting with Seizure This evidence-based report provides clinicians with information to identify which seizure patients in the emergency department
Dementia Facts and Resources Dementia Warning Signs Getting a Diagnosis Dementia Communication Tips Dementia Risk Reduction.
 Dementia Facts and Resources Dementia Warning Signs Getting a Diagnosis Dementia Communication Tips Dementia Risk Reduction Intermission Dementia Stages and Behaviors Caregiving and Self-Care Overview
Dementia Facts and Resources Dementia Warning Signs Getting a Diagnosis Dementia Communication Tips Dementia Risk Reduction Intermission Dementia Stages and Behaviors Caregiving and Self-Care Overview
Dementia and Alzheimer s disease
 Since 1960 Medicine Korat โรงพยาบาลมหาราชนครราชส มา Dementia and Alzheimer s disease Concise Reviews PAWUT MEKAWICHAI MD DEPARTMENT of MEDICINE MAHARAT NAKHON RATCHASIMA HOSPITAL 1 Prevalence Increase
Since 1960 Medicine Korat โรงพยาบาลมหาราชนครราชส มา Dementia and Alzheimer s disease Concise Reviews PAWUT MEKAWICHAI MD DEPARTMENT of MEDICINE MAHARAT NAKHON RATCHASIMA HOSPITAL 1 Prevalence Increase
Neuro Exam Explained
 Neuro Exam Explained Michael Nelson M.D. Providence Neurological Specialties East Primary Care Conference October 26 rd, 2017 Michael Nelson M.D. Medical School: University of Missouri-Columbia Residency:
Neuro Exam Explained Michael Nelson M.D. Providence Neurological Specialties East Primary Care Conference October 26 rd, 2017 Michael Nelson M.D. Medical School: University of Missouri-Columbia Residency:
Silent Cerebral Strokes: Clinical Outcomes and Management
 Silent Cerebral Strokes: Clinical Outcomes and Management Nagaendran Kandiah Senior Consultant Neurologist, National Neuroscience Institute, Singapore Clinician Scientist, National Medical Research Council,
Silent Cerebral Strokes: Clinical Outcomes and Management Nagaendran Kandiah Senior Consultant Neurologist, National Neuroscience Institute, Singapore Clinician Scientist, National Medical Research Council,
The child with hemiplegic cerebral palsy thinking beyond the motor impairment. Dr Paul Eunson Edinburgh
 The child with hemiplegic cerebral palsy thinking beyond the motor impairment Dr Paul Eunson Edinburgh Content Coming to a diagnosis The importance of understanding the injury MRI scans Role of epilepsy
The child with hemiplegic cerebral palsy thinking beyond the motor impairment Dr Paul Eunson Edinburgh Content Coming to a diagnosis The importance of understanding the injury MRI scans Role of epilepsy
 CLINICAL FEATURES THAT SUPPORT ATHEROSCLEROTIC STROKE 1. cerebral cortical impairment (aphasia, neglect, restricted motor involvement, etc.) or brain stem or cerebellar dysfunction 2. lacunar clinical
CLINICAL FEATURES THAT SUPPORT ATHEROSCLEROTIC STROKE 1. cerebral cortical impairment (aphasia, neglect, restricted motor involvement, etc.) or brain stem or cerebellar dysfunction 2. lacunar clinical
Deprescribing. Living with Dementia: Staying at Home. Webinar #5 Webinar #1. Jessica Visco, PharmD, CGP. SeniorPharmAssist.
 Webinar #5 Webinar #1 Living with Dementia: Safety, Security Deprescribing and Staying at Home Mitchell Heflin, MD, MHS Cornelia Poer, MSW, LCSW Lisa Gwyther, MSW, LCSW Jessica Visco, PharmD, CGP SeniorPharmAssist
Webinar #5 Webinar #1 Living with Dementia: Safety, Security Deprescribing and Staying at Home Mitchell Heflin, MD, MHS Cornelia Poer, MSW, LCSW Lisa Gwyther, MSW, LCSW Jessica Visco, PharmD, CGP SeniorPharmAssist
PMH: No medications; Immunizations UTD No hospitalizations or surgeries Speech Delay. Birth Hx: 24 WGA, NICU x6 months
 HPI: 6 months of weakness and parathesias- originally in both feet x 2-3 months, then resolved. Now with parathesias and weakness in fingers x 1 week. Seen by podiatrist and given custom in-soles 1 month
HPI: 6 months of weakness and parathesias- originally in both feet x 2-3 months, then resolved. Now with parathesias and weakness in fingers x 1 week. Seen by podiatrist and given custom in-soles 1 month
Key Clinical Concepts
 Cerebrovascular Review and General Vascular Syndromes, Including Those That Impact Dizziness Key Clinical Concepts Basic Review of Cerebrovascular Circulation Circulation to the brain is divided into anterior
Cerebrovascular Review and General Vascular Syndromes, Including Those That Impact Dizziness Key Clinical Concepts Basic Review of Cerebrovascular Circulation Circulation to the brain is divided into anterior
The current state of healthcare for Normal Aging, Mild Cognitive Impairment, & Alzheimer s Disease
 The current state of healthcare for Normal Aging, g, Mild Cognitive Impairment, & Alzheimer s Disease William Rodman Shankle, MS MD FACP Director, Alzheimer s Program, Hoag Neurosciences Institute Neurologist,
The current state of healthcare for Normal Aging, g, Mild Cognitive Impairment, & Alzheimer s Disease William Rodman Shankle, MS MD FACP Director, Alzheimer s Program, Hoag Neurosciences Institute Neurologist,
What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias
 What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias Presenter: Kim Bailey, MS Gerontology, Program & Education Specialist, Alzheimer s Orange County 1 1 Facts About Our
What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias Presenter: Kim Bailey, MS Gerontology, Program & Education Specialist, Alzheimer s Orange County 1 1 Facts About Our
OLD AGE PSYCHIATRY. Dementia definition TYPES OF DEMENTIA. Other causes. Psychiatric disorders of the elderly. Dementia.
 Psychiatric disorders of the elderly OLD AGE PSYCHIATRY Dementia Depression Delusional disorder/late onset schizophrenia Delirium Dementia definition LOCALISATION OF CEREBRAL FUNCTION Impairment of multiple
Psychiatric disorders of the elderly OLD AGE PSYCHIATRY Dementia Depression Delusional disorder/late onset schizophrenia Delirium Dementia definition LOCALISATION OF CEREBRAL FUNCTION Impairment of multiple
Non-lesional Medically-intractable Localization-related Epilepsy Case Presentation December 8, 2013
 Non-lesional Medically-intractable Localization-related Epilepsy Case Presentation December 8, 2013 Jennifer L. DeWolfe, DO Associate Professor of Neurology University of Alabama at Birmingham American
Non-lesional Medically-intractable Localization-related Epilepsy Case Presentation December 8, 2013 Jennifer L. DeWolfe, DO Associate Professor of Neurology University of Alabama at Birmingham American
62 yo F, RHD Epilepsy onset: 44 yo Seizure type: 1) Dyscognitive seizure 2) Somatosensory aura (abnormal feeling at both feet) Seizures disappeared
 Dyscognitive seizure 2) Somatosensory aura (abnormal feeling at both feet) Seizures disappeared") 62 yo F, RHD Epilepsy onset: 44 yo Seizure type: 1) Dyscognitive seizure 2) Somatosensory aura (abnormal feeling at both feet) Seizures disappeared since age 56 years Seizure period: 12 years (44 56 yrs)
62 yo F, RHD Epilepsy onset: 44 yo Seizure type: 1) Dyscognitive seizure 2) Somatosensory aura (abnormal feeling at both feet) Seizures disappeared since age 56 years Seizure period: 12 years (44 56 yrs)
Brain Health and Risk Factors for Dementia
 Welcome To Brain Health and Risk Factors for Dementia Presented by Kamal Masaki, MD Professor and Chair Department of Geriatric Medicine John A. Burns School of Medicine, UH Manoa April 4, 2018 10:00 11:00
Welcome To Brain Health and Risk Factors for Dementia Presented by Kamal Masaki, MD Professor and Chair Department of Geriatric Medicine John A. Burns School of Medicine, UH Manoa April 4, 2018 10:00 11:00
Mild Cognitive Impairment
 Mild Cognitive Impairment Victor W. Henderson, MD, MS Departments of Health Research & Policy (Epidemiology) and of Neurology & Neurological Sciences Stanford University Director, Stanford Alzheimer s
Mild Cognitive Impairment Victor W. Henderson, MD, MS Departments of Health Research & Policy (Epidemiology) and of Neurology & Neurological Sciences Stanford University Director, Stanford Alzheimer s
Divine Intervention Episode 59 Neurology Clerkship Shelf Review Part 8 (Final Part) Some PGY1
 Some PGY1") Divine Intervention Episode 59 Neurology Clerkship Shelf Review Part 8 (Final Part) Some PGY1 1 Paresthesias in a patient who is being treated for TB. Paresthesias/loss of joint and position sense/le hyperreflexia
Divine Intervention Episode 59 Neurology Clerkship Shelf Review Part 8 (Final Part) Some PGY1 1 Paresthesias in a patient who is being treated for TB. Paresthesias/loss of joint and position sense/le hyperreflexia
Sorting Out the Three D s:
 Sorting Out the Three D s: Delirium, Depression & Dementia Teepa Snow, Positive Approach, LLC to be reused only with permission. Dementia Delirium Depression What s What? What s What For Each D Onset Hx
Sorting Out the Three D s: Delirium, Depression & Dementia Teepa Snow, Positive Approach, LLC to be reused only with permission. Dementia Delirium Depression What s What? What s What For Each D Onset Hx
IMPAIRMENT OF THE NERVOUS SYSTEM
 IMPAIRMENT OF THE NERVOUS SYSTEM The following information provides criteria for the evaluation of permanent impairment resulting from dysfunction brain, spinal cord and cranial nerves and certain peripheral
IMPAIRMENT OF THE NERVOUS SYSTEM The following information provides criteria for the evaluation of permanent impairment resulting from dysfunction brain, spinal cord and cranial nerves and certain peripheral
Exploration of a weighed cognitive composite score for measuring decline in amnestic MCI
 Exploration of a weighed cognitive composite score for measuring decline in amnestic MCI Sarah Monsell NACC biostatistician smonsell@uw.edu October 6, 2012 Background Neuropsychological batteries used
Exploration of a weighed cognitive composite score for measuring decline in amnestic MCI Sarah Monsell NACC biostatistician smonsell@uw.edu October 6, 2012 Background Neuropsychological batteries used
Dr. Michael Lobatz Dr. Michael Jackson Dr. James Brewer Dr. Paul Aisen. Dr. Michael Plopper. Dr. Guerry Peavy
 1 Anne State 2 3 Dr. Michael Lobatz Dr. Michael Jackson Dr. James Brewer Dr. Paul Aisen Dr. Michael Plopper Dr. Guerry Peavy 4 Michael Lobatz, MD Medical Director, Neurosciences Medical Director, Rehabilitation
1 Anne State 2 3 Dr. Michael Lobatz Dr. Michael Jackson Dr. James Brewer Dr. Paul Aisen Dr. Michael Plopper Dr. Guerry Peavy 4 Michael Lobatz, MD Medical Director, Neurosciences Medical Director, Rehabilitation
BANISH BRAIN FOG: Chapter 5 workbook Copyright 2016 by datis kharrazian published by elephant press Page 1
 The Brain Function Assessment Form (BFAF) will help you see which symptoms relate to specific areas of your brain. I suggest printing out a few copies so you can take the test several times as you go along
The Brain Function Assessment Form (BFAF) will help you see which symptoms relate to specific areas of your brain. I suggest printing out a few copies so you can take the test several times as you go along
CNS VASCULAR DISEASE. Reid R. Heffner, M.D. Department of Pathology/Anatomy UB Jacobs School of Medicine January 15, 2019
 CNS VASCULAR DISEASE Reid R. Heffner, M.D. Department of Pathology/Anatomy UB Jacobs School of Medicine January 15, 2019 I HAVE NO CONFLICTS OF INTEREST OR ANY DISCLOSURES TO DECLARE. I HAVE NO FINANCIAL
CNS VASCULAR DISEASE Reid R. Heffner, M.D. Department of Pathology/Anatomy UB Jacobs School of Medicine January 15, 2019 I HAVE NO CONFLICTS OF INTEREST OR ANY DISCLOSURES TO DECLARE. I HAVE NO FINANCIAL
CHAPTER 5 NEUROPSYCHOLOGICAL PROFILE OF ALZHEIMER S DISEASE
 CHAPTER 5 NEUROPSYCHOLOGICAL PROFILE OF ALZHEIMER S DISEASE 5.1 GENERAL BACKGROUND Neuropsychological assessment plays a crucial role in the assessment of cognitive decline in older age. In India, there
CHAPTER 5 NEUROPSYCHOLOGICAL PROFILE OF ALZHEIMER S DISEASE 5.1 GENERAL BACKGROUND Neuropsychological assessment plays a crucial role in the assessment of cognitive decline in older age. In India, there
Risk Factors for Dementia and MCI in the Oldest Old The 90+ Study
 Risk Factors for Dementia and MCI in the Oldest Old The 90+ Study Claudia H. Kawas, M.D. January 18, 2015 Department of Neurology Department of Neurobiology & Behavior Institute for Memory Impairment &
Risk Factors for Dementia and MCI in the Oldest Old The 90+ Study Claudia H. Kawas, M.D. January 18, 2015 Department of Neurology Department of Neurobiology & Behavior Institute for Memory Impairment &
Dementia. Jeanette Norden, Ph.D. Professor Emerita Vanderbilt University School of Medicine
 Dementia Jeanette Norden, Ph.D. Professor Emerita Vanderbilt University School of Medicine What is Dementia? Dementia is a general term referring to a decline in cognitive/mental functioning; this decline
Dementia Jeanette Norden, Ph.D. Professor Emerita Vanderbilt University School of Medicine What is Dementia? Dementia is a general term referring to a decline in cognitive/mental functioning; this decline
o Normal Balanced Diet for your Age o High in Carbohydrates o High in Fats o High in Protein o Other Diet
 HEALTH ASSESSMENT SCREENING FORM GO402 Welcome to G0438 First Annual G0439 Subsequent Other Code PATIENTS NAME: DATE OF BIRTH: DATE OF SERVICE: PLEASE LIST CURRENT MEDICATION, ALSO OVER THE COUNTER MEDICATIONS
HEALTH ASSESSMENT SCREENING FORM GO402 Welcome to G0438 First Annual G0439 Subsequent Other Code PATIENTS NAME: DATE OF BIRTH: DATE OF SERVICE: PLEASE LIST CURRENT MEDICATION, ALSO OVER THE COUNTER MEDICATIONS
Approach to a Neurologic Diagnosis
 Approach to a Neurologic Diagnosis Neurologic Diagnosis History Physical & Neurological Examination Ancillary Procedures 3 Questions Asked Focal neurologic deficits Increased intracranial pressure Signs
Approach to a Neurologic Diagnosis Neurologic Diagnosis History Physical & Neurological Examination Ancillary Procedures 3 Questions Asked Focal neurologic deficits Increased intracranial pressure Signs
Frailty. Nicholas Butler MD, MBA Department of Family Medicine University of Iowa
 Frailty Nicholas Butler MD, MBA Department of Family Medicine University of Iowa Doris 84 yo female who comes into your clinic with her daughter. She complains of feeling increasingly fatigued and just
Frailty Nicholas Butler MD, MBA Department of Family Medicine University of Iowa Doris 84 yo female who comes into your clinic with her daughter. She complains of feeling increasingly fatigued and just
The Australian Imaging Biomarkers and Lifestyle Flagship Study of Ageing
 The Australian Imaging Biomarkers and Lifestyle Flagship Study of Ageing. (AUSTRALIAN ADNI) July 2012 UPDATE Imaging Christopher Rowe MD Neuroimaging stream leader October 2011 The Australian Imaging Biomarkers
The Australian Imaging Biomarkers and Lifestyle Flagship Study of Ageing. (AUSTRALIAN ADNI) July 2012 UPDATE Imaging Christopher Rowe MD Neuroimaging stream leader October 2011 The Australian Imaging Biomarkers
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal