What if it s not Alzheimer s? Update on Lewy body dementia and frontotemporal dementia
|
|
|
- Stephen White
- 6 years ago
- Views:
Transcription
1 What if it s not Alzheimer s? Update on Lewy body dementia and frontotemporal dementia
2 Dementia: broad term for any acquired brain condition impairing mental function such that ADLs are impaired. Includes: Alzheimer s disease Multi-infarct dementia (due to strokes) Lewy body dementia Frontotemporal dementia many others
3 Outline for tonight Lewy body dementia Frontotemporal dementia Treatment Research Support programs
4 Outline for tonight Lewy body dementia PDD (Parkinson s Disease Dementia) LBD (Lewy body dementia) Frontotemporal dementia Behavioral variants Language variants Genetic variants Treatment Research Support programs
5 Some definitions : Dementia = any acquired brain condition that interferes with the ability to think and to carry out routine daily functions
6 Some definitions : Dementia = any acquired brain condition that interferes with the ability to think and to carry out routine daily functions Alzheimer s disease = the most common cause of dementia, characterized by plaques and tangles in brain
7 Some definitions : Dementia = any acquired brain condition that interferes with the ability to think and to carry out routine daily functions Alzheimer s disease = the most common cause of dementia, characterized by plaques and tangles in brain
8 Some definitions : Dementia = any acquired brain condition that interferes with the ability to think and to carry out routine daily functions Alzheimer s disease = the most common cause of dementia, characterized by plaques and tangles in brain Parkinson s disease = A disease of movement With dementia occurring Years after diagnosis
9 Some definitions : Dementia = any acquired brain condition that interferes with the ability to think and to carry out routine daily functions Alzheimer s disease = the most common cause of dementia, characterized by plaques and tangles in brain Parkinson s disease = A disease of movement with dementia occurring years after diagnosis
10 Parkinson s: Classical view: Tremor Rigidity Bradykinesia Gait disorder
11 Cognitive Function in PD a motor disease without a significant cognitive component: Classical View: by the absence of any injury to the senses and to the intellect, (we conclude) that the morbid state does not involve the encephalon. ---James Parkinson, An Essay on the Shaking Palsy (1817)
12 Revised View: Cognitive impairment is a common feature of PD Cognitive impairment is a significant source of distress and disability
13 Dementia Prevalence of Cognitive Impairment in PD 20% of PD have mild cognitive impairment (MCI) at time of PD diagnosis 30-40% of all PD have dementia Up to 80% by 15 years into disease 4-6x greater than elderly without PD
14 What domains of mental function are affected in Parkinson s? Attention* Memory Executive function* Visuospatial function* Language function
15 Alzheimer s vs Parkinson s: Alzheimer s PD Dementia Attention Memory Executive Visuospatial Language
16 What causes cognitive decline in Parkinson s? Many causes Changes in neurotransmitters are part of the problem---but it s not the same neurotransmitters that cause the movement disorder
17 Motor Symptoms are Dopamine Responsive
18 Motor Symptoms are Dopamine Responsive
19 Motor Symptoms are Dopamine Responsive

20 Motor Symptoms are Dopamine Responsive
21 Cognitive symptoms are due to impairment in a different neurotransmitter: acetylcholine: Bohnen, Arch Neurol, 60:1745-8, 2003.

22 Bohnen, Arch Neurol, 60:1745-8, 2003.
23 Bohnen, Arch Neurol, 60:1745-8, 2003.
24 Bohnen, Arch Neurol, 60:1745-8, 2003.
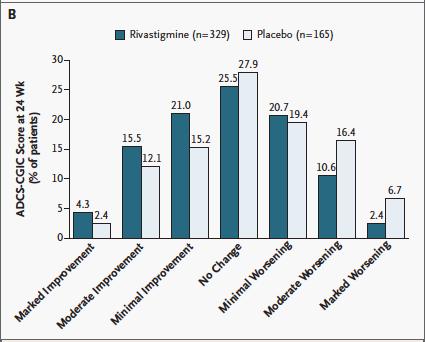
25 Drugs to boost acetylcholine help in PD dementia:
26
27
28 Conclusions: Parkinson s dementia is distinct from Alzheimer s Neurotransmitters involved in dementia are distinct from the ones involved in impaired movements.
29 What is Lewy body dementia? A dementia characterized by: Parkinsonism Hallucinations Sensitivity to anti-psychotic medications Fluctuations Brain autopsy shows lewy bodies in the brain
30 What is Lewy body dementia? The cognitive profile looks like parkinson s dementia Brain autopsy shows lewy bodies in the brain
31 How is Lewy body dementia different from Parkinson s disease? In Parkinson s disease, the dementia appears several years after diagnosis of movement problems. In Lewy body dementia, the movement problems and the dementia come on together.
32 How is Lewy body dementia different from Parkinson s disease? Tremor is less common Slowness and stiffness are more symmetric Motor symptoms are less responsive to medication in lewy body dementia than in parkinson s disease
33 How is Lewy body dementia different from Parkinson s disease? In Parkinson s disease, hallucinations are promoted by the drugs used to treat Parkinson s disease. In Lewy body dementia, hallucinations appear without being triggered by any drugs.
34 What is Lewy body dementia? Sensitivity to antipsychotic medications is part of Lewy body dementia. Patients can become frozen from low doses of these medications Fluctuations in level of consciousness are also common in Lewy body dementia.
35 How is Lewy body dementia treated? Need to be careful with Parkinson s medicines, because they will increase hallucinations. Need to be careful with medicine for hallucinations, because it worsens parkinsonian motor symptoms. Some patients do well with medicines that increase acetylcholine.
36 The ability to increase brain acetylcholine is limited: Because acetylcholine also works on the stomach and intestines Most of the drugs that boost acetylcholine in brain also boost it in GI tract and cause nausea, vomiting, loose stools, diarrhea If only there was a way to boost acetylcholine in the brain without affecting the gut.
37

38 Research on Lewy body dementia 28 studies currently recruiting world-wide 1 study recruiting in Oregon
39
40
41
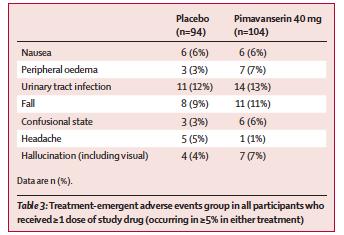
42 What can we do about hallucinations in Parkinson s dementia and Lewy body dementia The medications usually used for hallucinations make parkinsonism worse. One exception is clozapine, but there are risks with that drug which require weekly blood tests to monitor. A new approach to hallucinations in this population is needed.

43
44
45
46
47 Conclusions: New strategies for increasing acetylcholine in the brain may permit more effective treatment of Lewy body dementia. A new strategy for treating hallucinations in the setting of Parkinson s disease may eventually be applied to Lewy body dementia

48 Future directions for Lewy body dementia: Aimed at underlying pathology: Lewy bodies, the chief component of which is alpha synuclein:

49 Spread of Lewy bodies to thinking centers of the brain:
50 Experimental therapies trageting synuclein include: small molecule (ie, a pill) Immunotherapy (ie, antibodies, delivered by injection) Gene therapy
51 Support for Lewy body dementia: Alzheimer s Association Lewy Body Dementia Association
52 Frontotemporal dementia: Behavioral variant Language variant
53 Behavioral variant: disinhibited: 52 year old man: Trouble learning new tasks at work Gradual onset of disinhibited statements there is no filter Over-spends, over-tips Eats impulsively: Stuffs mouth full without swallowing, episodes of choking Acts impulsively: eg, jumped in white water with dog while out hiking
54 Behavioral variant: disinhibited: 52 year old man: Mmse =29/30 EXIT-25 =14/50 Normal neuro exam Bilateral frontotemporal atrophy on MRI scan

55 MRI in FTD:
56 Language variant: Primary progressive aphasia (PPA) 53 year old woman referred for declining language function Worked as a traveling motel clerk until one year prior to evaluation. Telephone calls to husband and sister became flat about years prior to eval. Laid off from work one year prior to eval.
57 Language variant-ppa She was referred to a local neurologist, who found normal EEG, normal MRI, and thought neurodegenerative disease unlikely. Social security examiner thought she was depressed and recommended ECT. Psychiatrist thought her language was impaired, doubted depression as the primary diagnosis, and referred her to another neurologist Chief complaint was difficulty with expressive language
58 Mental status exam mmse = 21/30 Orientation = 6/10 Attention = 2/5 ( DLORY ) Repetition = 0/1 obvious trouble with word-finding during spontaneous speech, to the point where even simple sentences were rarely fluent
59 labs Neuro exam: normal Brain MRI normal
60 Brain autopsy Frontotemporal dementia confirmed in both instances Note: Younger than Alzheimer s patients Memory is relatively preserved Behavior or language are markedly impaired With time, impairment generalizes and function declines
61 Brain autopsy Some variants of frontotemporal dementia, defined by brain autopsy: Pick s disease FTDP-17 Progressive supranuclear palsy Corticobasal degeneration
62 Genetics: FTDP-17 (rare) Progranulin (rare) C9ORF72: fairly common in familial FTD, also seen in sporadic cases
63 Genetics: FTDP-17 (rare) Progranulin (rare) C9ORF72: fairly common in familial FTD, also seen in sporadic cases The genetics does not predict the particular symptoms
64 Treatment of FTD SSRI s are recommended by most experts Otherwise symptomatic treatment on a caseby-case basis

65 Research on FTD 45 studies worldwide none in Oregon 7 in California, none are treatments
66 Support for FTD Association for Frontotemporal Dementia Cure PSP Alzheimer s Association
67 conclusions Lewy body dementia and frontotemporal dementia are distinct from Alzheimer s disease Ongoing research is under way to develop disease-modifying treatments. In the meantime, treatment is tailored to symptoms. Support for caregivers is available through a number of non-profit groups.

68 Thank you for your attention Questions?
Improving diagnosis of Alzheimer s disease and lewy body dementia. Brain TLC October 2018
 Improving diagnosis of Alzheimer s disease and lewy body dementia Brain TLC October 2018 Plan for this discussion: Introduction to AD and LBD Why do we need to improve diagnosis? What progress has been
Improving diagnosis of Alzheimer s disease and lewy body dementia Brain TLC October 2018 Plan for this discussion: Introduction to AD and LBD Why do we need to improve diagnosis? What progress has been
DEMENTIA 101: WHAT IS HAPPENING IN THE BRAIN? Philip L. Rambo, PhD
 DEMENTIA 101: WHAT IS HAPPENING IN THE BRAIN? Philip L. Rambo, PhD OBJECTIVES Terminology/Dementia Basics Most Common Types Defining features Neuro-anatomical/pathological underpinnings Neuro-cognitive
DEMENTIA 101: WHAT IS HAPPENING IN THE BRAIN? Philip L. Rambo, PhD OBJECTIVES Terminology/Dementia Basics Most Common Types Defining features Neuro-anatomical/pathological underpinnings Neuro-cognitive
FRONTOTEMPORAL DEGENERATION: OVERVIEW, TRENDS AND DEVELOPMENTS
 FRONTOTEMPORAL DEGENERATION: OVERVIEW, TRENDS AND DEVELOPMENTS Norman L. Foster, M.D. Director, Center for Alzheimer s Care, Imaging and Research Chief, Division of Cognitive Neurology, Department of Neurology
FRONTOTEMPORAL DEGENERATION: OVERVIEW, TRENDS AND DEVELOPMENTS Norman L. Foster, M.D. Director, Center for Alzheimer s Care, Imaging and Research Chief, Division of Cognitive Neurology, Department of Neurology
Common Forms of Dementia Handout Package
 Common Forms of Dementia Handout Package Common Forms of Dementia 1 Learning Objectives As a result of working through this module, you should be better able to: 1. Describe clinical features of 4 major
Common Forms of Dementia Handout Package Common Forms of Dementia 1 Learning Objectives As a result of working through this module, you should be better able to: 1. Describe clinical features of 4 major
Non Alzheimer Dementias
 Non Alzheimer Dementias Randolph B Schiffer Department of Neuropsychiatry and Behavioral Science Texas Tech University Health Sciences Center 9/11/2007 Statement of Financial Disclosure Randolph B Schiffer,,
Non Alzheimer Dementias Randolph B Schiffer Department of Neuropsychiatry and Behavioral Science Texas Tech University Health Sciences Center 9/11/2007 Statement of Financial Disclosure Randolph B Schiffer,,
Clinical Differences Among Four Common Dementia Syndromes. a program of Morningside Ministries
 Clinical Differences Among Four Common Dementia Syndromes a program of Morningside Ministries Introduction Four clinical dementia syndromes account for 90% of all cases after excluding reversible causes
Clinical Differences Among Four Common Dementia Syndromes a program of Morningside Ministries Introduction Four clinical dementia syndromes account for 90% of all cases after excluding reversible causes
The ABCs of Dementia Diagnosis
 The ABCs of Dementia Diagnosis Dr. Robin Heinrichs, Ph.D., ABPP Board Certified Clinical Neuropsychologist Associate Professor, Psychiatry & Behavioral Sciences Director of Neuropsychology Training What
The ABCs of Dementia Diagnosis Dr. Robin Heinrichs, Ph.D., ABPP Board Certified Clinical Neuropsychologist Associate Professor, Psychiatry & Behavioral Sciences Director of Neuropsychology Training What
Overview. Overview. Parkinson s disease. Secondary Parkinsonism. Parkinsonism: Motor symptoms associated with impairment in basal ganglia circuits
 Overview Overview Parkinsonism: Motor symptoms associated with impairment in basal ganglia circuits The differential diagnosis of Parkinson s disease Primary vs. Secondary Parkinsonism Proteinopathies:
Overview Overview Parkinsonism: Motor symptoms associated with impairment in basal ganglia circuits The differential diagnosis of Parkinson s disease Primary vs. Secondary Parkinsonism Proteinopathies:
Dementia Update. October 1, 2013 Dylan Wint, M.D. Cleveland Clinic Lou Ruvo Center for Brain Health Las Vegas, Nevada
 Dementia Update October 1, 2013 Dylan Wint, M.D. Cleveland Clinic Lou Ruvo Center for Brain Health Las Vegas, Nevada Outline New concepts in Alzheimer disease Biomarkers and in vivo diagnosis Future trends
Dementia Update October 1, 2013 Dylan Wint, M.D. Cleveland Clinic Lou Ruvo Center for Brain Health Las Vegas, Nevada Outline New concepts in Alzheimer disease Biomarkers and in vivo diagnosis Future trends
Differential Diagnosis of Hypokinetic Movement Disorders
 Differential Diagnosis of Hypokinetic Movement Disorders Dr Donald Grosset Consultant Neurologist - Honorary Professor Institute of Neurological Sciences - Glasgow University Hypokinetic Parkinson's Disease
Differential Diagnosis of Hypokinetic Movement Disorders Dr Donald Grosset Consultant Neurologist - Honorary Professor Institute of Neurological Sciences - Glasgow University Hypokinetic Parkinson's Disease
Form D1: Clinician Diagnosis
 Initial Visit Packet Form D: Clinician Diagnosis NACC Uniform Data Set (UDS) ADC name: Subject ID: Form date: / / Visit #: Examiner s initials: INSTRUCTIONS: This form is to be completed by the clinician.
Initial Visit Packet Form D: Clinician Diagnosis NACC Uniform Data Set (UDS) ADC name: Subject ID: Form date: / / Visit #: Examiner s initials: INSTRUCTIONS: This form is to be completed by the clinician.
FTD basics! Etienne de Villers-Sidani, MD!
 FTD basics! Etienne de Villers-Sidani, MD! Frontotemporal lobar degeneration (FTLD) comprises 3 clinical syndromes! Frontotemporal dementia (behavioral variant FTD)! Semantic dementia (temporal variant
FTD basics! Etienne de Villers-Sidani, MD! Frontotemporal lobar degeneration (FTLD) comprises 3 clinical syndromes! Frontotemporal dementia (behavioral variant FTD)! Semantic dementia (temporal variant
Dementia Update. Daniel Drubach, M.D. Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota
 Dementia Update Daniel Drubach, M.D. Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota Nothing to disclose Dementia Progressive deterioration in mental function
Dementia Update Daniel Drubach, M.D. Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota Nothing to disclose Dementia Progressive deterioration in mental function
Objectives. RAIN Difficult Diagnosis 2014: A 75 year old woman with falls. Case History: First visit. Case History: First Visit
 Objectives RAIN Difficult Diagnosis 2014: A 75 year old woman with falls Alexandra Nelson MD, PhD UCSF Memory and Aging Center/Gladstone Institute of Neurological Disease Recognize important clinical features
Objectives RAIN Difficult Diagnosis 2014: A 75 year old woman with falls Alexandra Nelson MD, PhD UCSF Memory and Aging Center/Gladstone Institute of Neurological Disease Recognize important clinical features
III./3.1. Movement disorders with akinetic rigid symptoms
 III./3.1. Movement disorders with akinetic rigid symptoms III./3.1.1. Parkinson s disease Parkinson s disease (PD) is the second most common neurodegenerative disorder worldwide after Alzheimer s disease.
III./3.1. Movement disorders with akinetic rigid symptoms III./3.1.1. Parkinson s disease Parkinson s disease (PD) is the second most common neurodegenerative disorder worldwide after Alzheimer s disease.
Assessing and Managing the Patient with Cognitive Decline
 Assessing and Managing the Patient with Cognitive Decline Center of Excellence For Alzheimer s Disease for State of NY Capital Region Alzheimer s Center of Albany Medical Center Earl A. Zimmerman, MD Professor
Assessing and Managing the Patient with Cognitive Decline Center of Excellence For Alzheimer s Disease for State of NY Capital Region Alzheimer s Center of Albany Medical Center Earl A. Zimmerman, MD Professor
What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias
 What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias Presenter: Kim Bailey, MS Gerontology, Program & Education Specialist, Alzheimer s Orange County 1 1 Facts About Our
What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias Presenter: Kim Bailey, MS Gerontology, Program & Education Specialist, Alzheimer s Orange County 1 1 Facts About Our
2016 Programs & Information
 Mayo Alzheimer s Disease Research Clinic Education Center 2016 Programs & Information BROCHURE TITLE FLUSH RIGHT for Persons & Families impacted by Mild Cognitive Impairment Alzheimer s Disease Dementia
Mayo Alzheimer s Disease Research Clinic Education Center 2016 Programs & Information BROCHURE TITLE FLUSH RIGHT for Persons & Families impacted by Mild Cognitive Impairment Alzheimer s Disease Dementia
I do not have any disclosures
 Alzheimer s Disease: Update on Research, Treatment & Care Clinicopathological Classifications of FTD and Related Disorders Keith A. Josephs, MST, MD, MS Associate Professor & Consultant of Neurology Mayo
Alzheimer s Disease: Update on Research, Treatment & Care Clinicopathological Classifications of FTD and Related Disorders Keith A. Josephs, MST, MD, MS Associate Professor & Consultant of Neurology Mayo
Dementia. Stephen S. Flitman, MD Medical Director 21st Century Neurology
 Dementia Stephen S. Flitman, MD Medical Director 21st Century Neurology www.neurozone.org Dementia is a syndrome Progressive memory loss, plus Progressive loss of one or more cognitive functions: Language
Dementia Stephen S. Flitman, MD Medical Director 21st Century Neurology www.neurozone.org Dementia is a syndrome Progressive memory loss, plus Progressive loss of one or more cognitive functions: Language
Delirium & Dementia. Nicholas J. Silvestri, MD
 Delirium & Dementia Nicholas J. Silvestri, MD Outline Delirium vs. Dementia Neural pathways relating to consciousness Encephalopathy Stupor Coma Dementia Delirium vs. Dementia Delirium Abrupt onset Lasts
Delirium & Dementia Nicholas J. Silvestri, MD Outline Delirium vs. Dementia Neural pathways relating to consciousness Encephalopathy Stupor Coma Dementia Delirium vs. Dementia Delirium Abrupt onset Lasts
Parkinson Disease. Lorraine Kalia, MD, PhD, FRCPC. Presented by: Ontario s Geriatric Steering Committee
 Parkinson Disease Lorraine Kalia, MD, PhD, FRCPC Key Learnings Parkinson Disease (L. Kalia) Key Learnings Parkinson disease is the most common but not the only cause of parkinsonism Parkinson disease is
Parkinson Disease Lorraine Kalia, MD, PhD, FRCPC Key Learnings Parkinson Disease (L. Kalia) Key Learnings Parkinson disease is the most common but not the only cause of parkinsonism Parkinson disease is
Perspectives on Frontotemporal Dementia and Primary Progressive Aphasia
 Perspectives on Frontotemporal Dementia and Primary Progressive Aphasia Bradley F. Boeve, M.D. Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota Alzheimer s Disease
Perspectives on Frontotemporal Dementia and Primary Progressive Aphasia Bradley F. Boeve, M.D. Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota Alzheimer s Disease
Form A3: Subject Family History
 Initial Visit Packet NACC Uniform Data Set (UDS) Form A: Subject Family History ADC name: Subject ID: Form date: / / Visit #: Examiner s initials: INSTRUCTIONS: This form is to be completed by a clinician
Initial Visit Packet NACC Uniform Data Set (UDS) Form A: Subject Family History ADC name: Subject ID: Form date: / / Visit #: Examiner s initials: INSTRUCTIONS: This form is to be completed by a clinician
Medications and Non-Pharma Approaches to Treatment. David J. Irwin, MD Penn Frontotemporal Degeneration Center
 Medications and Non-Pharma Approaches to Treatment David J. Irwin, MD Penn Frontotemporal Degeneration Center Outline Non-Pharmacological Treatment Strategies Behavior Language Motor Supportive Care Check-points
Medications and Non-Pharma Approaches to Treatment David J. Irwin, MD Penn Frontotemporal Degeneration Center Outline Non-Pharmacological Treatment Strategies Behavior Language Motor Supportive Care Check-points
SECTION 1: as each other, or as me. THE BRAIN AND DEMENTIA. C. Boden *
 I read all the available books by other [people with] Alzheimer s disease but they never had quite the same problems as each other, or as me. I t s not like other diseases, where there is a standard set
I read all the available books by other [people with] Alzheimer s disease but they never had quite the same problems as each other, or as me. I t s not like other diseases, where there is a standard set
P20.2. Characteristics of different types of dementia and challenges for the clinician
 P20.2. Characteristics of different types of dementia and challenges for the clinician, professor Danish Dementia Research Center Rigshospitalet, University of Copenhagen (Denmark) This project has received
P20.2. Characteristics of different types of dementia and challenges for the clinician, professor Danish Dementia Research Center Rigshospitalet, University of Copenhagen (Denmark) This project has received
Evaluations. Alzheimer s Disease A Public Health Response. Viewer Call-In. July 19, Guest Speakers. Thanks to our Sponsors:
 Alzheimer s Disease A Public Health Response July 19, 2007 1 2 Guest Speakers Thanks to our Sponsors: Earl A. Zimmerman, M.D. Bender Endowed Chair of Neurology and Director of the Alzheimer s Center at
Alzheimer s Disease A Public Health Response July 19, 2007 1 2 Guest Speakers Thanks to our Sponsors: Earl A. Zimmerman, M.D. Bender Endowed Chair of Neurology and Director of the Alzheimer s Center at
Dementia. Assessing Brain Damage. Mental Status Examination
 Dementia Assessing Brain Damage Mental status examination Information about current behavior and thought including orientation to reality, memory, and ability to follow instructions Neuropsychological
Dementia Assessing Brain Damage Mental status examination Information about current behavior and thought including orientation to reality, memory, and ability to follow instructions Neuropsychological
Diagnosis and Treatment of Alzhiemer s Disease
 Diagnosis and Treatment of Alzhiemer s Disease Roy Yaari, MD, MAS Director, Memory Disorders Clinic, Banner Alzheimer s Institute 602-839-6900 Outline Introduction Alzheimer s disease (AD)Guidelines -revised
Diagnosis and Treatment of Alzhiemer s Disease Roy Yaari, MD, MAS Director, Memory Disorders Clinic, Banner Alzheimer s Institute 602-839-6900 Outline Introduction Alzheimer s disease (AD)Guidelines -revised
Caring Sheet #11: Alzheimer s Disease:
 CARING SHEETS: Caring Sheet #11: Alzheimer s Disease: A Summary of Information and Intervention Suggestions with an Emphasis on Cognition By Shelly E. Weaverdyck, PhD Introduction This caring sheet focuses
CARING SHEETS: Caring Sheet #11: Alzheimer s Disease: A Summary of Information and Intervention Suggestions with an Emphasis on Cognition By Shelly E. Weaverdyck, PhD Introduction This caring sheet focuses
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017.
 DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
! slow, progressive, permanent loss of neurologic function.
 UBC ! slow, progressive, permanent loss of neurologic function.! cause unknown.! sporadic, familial or inherited.! degeneration of specific brain region! clinical syndrome.! pathology: abnormal accumulation
UBC ! slow, progressive, permanent loss of neurologic function.! cause unknown.! sporadic, familial or inherited.! degeneration of specific brain region! clinical syndrome.! pathology: abnormal accumulation
Update on functional brain imaging in Movement Disorders
 Update on functional brain imaging in Movement Disorders Mario Masellis, MSc, MD, FRCPC, PhD Assistant Professor & Clinician-Scientist Sunnybrook Health Sciences Centre University of Toronto 53 rd CNSF
Update on functional brain imaging in Movement Disorders Mario Masellis, MSc, MD, FRCPC, PhD Assistant Professor & Clinician-Scientist Sunnybrook Health Sciences Centre University of Toronto 53 rd CNSF
Pathogenesis of Degenerative Diseases and Dementias. D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria)
. M. Path (U. of Alexandria)") Pathogenesis of Degenerative Diseases and Dementias D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria) Dementias Defined: as the development of memory impairment and other cognitive deficits
Pathogenesis of Degenerative Diseases and Dementias D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria) Dementias Defined: as the development of memory impairment and other cognitive deficits
Objectives. Objectives continued: 3/24/2012. Copyright Do not distribute or replicate without permission 1
 Frontotemporal Degeneration and Primary Progressive Aphasia Caregiver and Professional Education Conference Diana R. Kerwin, MD Assistant Professor of Medicine-Geriatrics Cognitive Neurology and Alzheimer
Frontotemporal Degeneration and Primary Progressive Aphasia Caregiver and Professional Education Conference Diana R. Kerwin, MD Assistant Professor of Medicine-Geriatrics Cognitive Neurology and Alzheimer
Dementia. Aetiology, pathophysiology and the role of neuropsychological testing. Dr Sheng Ling Low Geriatrician
 Dementia Aetiology, pathophysiology and the role of neuropsychological testing Dr Sheng Ling Low Geriatrician Topics to cover Why is dementia important What is dementia Differentiate between dementia,
Dementia Aetiology, pathophysiology and the role of neuropsychological testing Dr Sheng Ling Low Geriatrician Topics to cover Why is dementia important What is dementia Differentiate between dementia,
DISCLOSURES. Objectives. THE EPIDEMIC of 21 st Century. Clinical Assessment of Cognition: New & Emerging Tools for Diagnosing Dementia NONE TO REPORT
 Clinical Assessment of Cognition: New & Emerging Tools for Diagnosing Dementia DISCLOSURES NONE TO REPORT Freddi Segal Gidan, PA, PhD USC Keck School of Medicine Rancho/USC California Alzheimers Disease
Clinical Assessment of Cognition: New & Emerging Tools for Diagnosing Dementia DISCLOSURES NONE TO REPORT Freddi Segal Gidan, PA, PhD USC Keck School of Medicine Rancho/USC California Alzheimers Disease
Memory Loss, Dementia and Alzheimer's Disease: The Basics
 Memory Loss, Dementia and Alzheimer's Disease: The Basics What is memory loss? What is age-related memory loss? Typical changes Typical age-related changes involve: Making a bad decision once in a while
Memory Loss, Dementia and Alzheimer's Disease: The Basics What is memory loss? What is age-related memory loss? Typical changes Typical age-related changes involve: Making a bad decision once in a while
MOVEMENT DISORDERS AND DEMENTIA
 MOVEMENT DISORDERS AND DEMENTIA FOCUS ON DEMENTIA WITH LEWY BODIES MADHAVI THOMAS MD NORTH TEXAS MOVEMENT DISORDERS INSTITUTE, INC DEMENTIA de men tia dəˈmen(t)sh(ē)ə/ nounmedicine noun: dementia a chronic
MOVEMENT DISORDERS AND DEMENTIA FOCUS ON DEMENTIA WITH LEWY BODIES MADHAVI THOMAS MD NORTH TEXAS MOVEMENT DISORDERS INSTITUTE, INC DEMENTIA de men tia dəˈmen(t)sh(ē)ə/ nounmedicine noun: dementia a chronic
Dementia Facts and Resources Dementia Warning Signs Getting a Diagnosis Dementia Communication Tips Dementia Risk Reduction.
 Dementia Facts and Resources Dementia Warning Signs Getting a Diagnosis Dementia Communication Tips Dementia Risk Reduction Intermission Dementia Stages and Behaviors Caregiving and Self-Care Overview
Dementia Facts and Resources Dementia Warning Signs Getting a Diagnosis Dementia Communication Tips Dementia Risk Reduction Intermission Dementia Stages and Behaviors Caregiving and Self-Care Overview
Clinical Diagnosis. Step 1: Dementia or not? Diagnostic criteria for dementia (DSM-IV)
") Step 1: Dementia or not? Diagnostic criteria for dementia (DSM-IV) A. The development of multiple cognitive deficits manifested by both 1 and 2 1 1. Memory impairment 2. One (or more) of the following
Step 1: Dementia or not? Diagnostic criteria for dementia (DSM-IV) A. The development of multiple cognitive deficits manifested by both 1 and 2 1 1. Memory impairment 2. One (or more) of the following
7/3/2013 ABNORMAL PSYCHOLOGY SEVENTH EDITION CHAPTER FOURTEEN CHAPTER OUTLINE. Dementia, Delirium, and Amnestic Disorders. Oltmanns and Emery
 ABNORMAL PSYCHOLOGY SEVENTH EDITION Oltmanns and Emery PowerPoint Presentations Prepared by: Ashlea R. Smith, Ph.D. This multimedia and its contents are protected under copyright law. The following are
ABNORMAL PSYCHOLOGY SEVENTH EDITION Oltmanns and Emery PowerPoint Presentations Prepared by: Ashlea R. Smith, Ph.D. This multimedia and its contents are protected under copyright law. The following are
FTD/PPA Caregiver Education Conference March 11, 2011
 FTD/PPA Caregiver Education Conference March 11, 2011 Question and Answer Session Answered by Joseph Cooper, MD, Darby Morhardt, MSW, LCSW, Mary O Hara, AM, LCSW, Jaimie Robinson, MSW, LCSW, Emily Rogalski,
FTD/PPA Caregiver Education Conference March 11, 2011 Question and Answer Session Answered by Joseph Cooper, MD, Darby Morhardt, MSW, LCSW, Mary O Hara, AM, LCSW, Jaimie Robinson, MSW, LCSW, Emily Rogalski,
10th Medicine Review Course st July Prakash Kumar
 10th Medicine Review Course 2018 21 st July 2018 Drug Therapy for Parkinson's disease Prakash Kumar National Neuroscience Institute Singapore General Hospital Sengkang General Hospital Singhealth Duke-NUS
10th Medicine Review Course 2018 21 st July 2018 Drug Therapy for Parkinson's disease Prakash Kumar National Neuroscience Institute Singapore General Hospital Sengkang General Hospital Singhealth Duke-NUS
The frontotemporal dementia spectrum what the general physician needs to know Dr Jonathan Rohrer
 The frontotemporal dementia spectrum what the general physician needs to know Dr Jonathan Rohrer MRC Clinician Scientist Honorary Consultant Neurologist Dementia Research Centre, UCL Institute of Neurology
The frontotemporal dementia spectrum what the general physician needs to know Dr Jonathan Rohrer MRC Clinician Scientist Honorary Consultant Neurologist Dementia Research Centre, UCL Institute of Neurology
Dementia Past, Present and Future
 Dementia Past, Present and Future Morris Freedman MD, FRCPC Division of Neurology Baycrest and University of Toronto Rotman Research Institute, Baycrest CNSF 2015 Objectives By the end of this presentation,
Dementia Past, Present and Future Morris Freedman MD, FRCPC Division of Neurology Baycrest and University of Toronto Rotman Research Institute, Baycrest CNSF 2015 Objectives By the end of this presentation,
The Basics of Alzheimer s Disease
 2017 Memory Loss Conference The Basics of Alzheimer s Disease Tom Ala, MD Center for Alzheimer s Disease and Related Disorders Southern Illinois University School of Medicine Springfield, Illinois SIU
2017 Memory Loss Conference The Basics of Alzheimer s Disease Tom Ala, MD Center for Alzheimer s Disease and Related Disorders Southern Illinois University School of Medicine Springfield, Illinois SIU
What is frontotemporal dementia?
 What is frontotemporal dementia? Introduction Information in this introductory booklet is for anyone who wants to know more about frontotemporal dementia (FTD). This includes people living with FTD, their
What is frontotemporal dementia? Introduction Information in this introductory booklet is for anyone who wants to know more about frontotemporal dementia (FTD). This includes people living with FTD, their
Dementia: It s Not Always Alzheimer s
 Dementia: It s Not Always Alzheimer s A Caregiver s Perspective Diane E. Vance, Ph.D. Mid-America Institute on Aging and Wellness 2017 My Background Caregiver for my husband who had Lewy Body Dementia
Dementia: It s Not Always Alzheimer s A Caregiver s Perspective Diane E. Vance, Ph.D. Mid-America Institute on Aging and Wellness 2017 My Background Caregiver for my husband who had Lewy Body Dementia
DEMENTIA? 45 Million. What is. WHAT IS DEMENTIA Dementia is a disturbance in a group of mental processes including: 70% Dementia is not a disease
 What is PRESENTS DEMENTIA? WHAT IS DEMENTIA Dementia is a disturbance in a group of mental processes including: Memory Reasoning Planning Learning Attention Language Perception Behavior AS OF 2013 There
What is PRESENTS DEMENTIA? WHAT IS DEMENTIA Dementia is a disturbance in a group of mental processes including: Memory Reasoning Planning Learning Attention Language Perception Behavior AS OF 2013 There
Parkinson s Disease. Gillian Sare
 Parkinson s Disease Gillian Sare Outline Reminder about PD Parkinson s disease in the inpatient Surgical patients with PD Patients who cannot swallow End of life care Parkinson s disease PD is the second
Parkinson s Disease Gillian Sare Outline Reminder about PD Parkinson s disease in the inpatient Surgical patients with PD Patients who cannot swallow End of life care Parkinson s disease PD is the second
ALZHEIMER S DISEASE. Mary-Letitia Timiras M.D. Overlook Hospital Summit, New Jersey
 ALZHEIMER S DISEASE Mary-Letitia Timiras M.D. Overlook Hospital Summit, New Jersey Topics Covered Demography Clinical manifestations Pathophysiology Diagnosis Treatment Future trends Prevalence and Impact
ALZHEIMER S DISEASE Mary-Letitia Timiras M.D. Overlook Hospital Summit, New Jersey Topics Covered Demography Clinical manifestations Pathophysiology Diagnosis Treatment Future trends Prevalence and Impact
3/6/2019 DIAGNOSIS OF DEMENTIA IN THE OUTPATIENT SETTING FINANCIAL DISCLOSURES LEARNING OBJECTIVES
 DIAGNOSIS OF DEMENTIA IN THE OUTPATIENT SETTING MILTA LITTLE, DO, CMD DUKE UNIVERSITY SCHOOL OF MEDICINE FINANCIAL DISCLOSURES Dr. Little has no relevant financial disclosures to report Dr. Little will
DIAGNOSIS OF DEMENTIA IN THE OUTPATIENT SETTING MILTA LITTLE, DO, CMD DUKE UNIVERSITY SCHOOL OF MEDICINE FINANCIAL DISCLOSURES Dr. Little has no relevant financial disclosures to report Dr. Little will
Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE
 Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE Objectives At the conclusion of the session, participants will be
Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE Objectives At the conclusion of the session, participants will be
Rarer causes of dementia
 Rarer causes of dementia Factsheet 442LP March 2015 Alzheimer s disease is the most common cause of dementia, but there are many rarer diseases and conditions that can lead to dementia, dementialike symptoms
Rarer causes of dementia Factsheet 442LP March 2015 Alzheimer s disease is the most common cause of dementia, but there are many rarer diseases and conditions that can lead to dementia, dementialike symptoms
The Person: Dementia Basics
 The Person: Dementia Basics Objectives 1. Discuss how expected age related changes in the brain might affect an individual's cognition and functioning 2. Discuss how changes in the brain due to Alzheimer
The Person: Dementia Basics Objectives 1. Discuss how expected age related changes in the brain might affect an individual's cognition and functioning 2. Discuss how changes in the brain due to Alzheimer
For carers and relatives of people with frontotemporal dementia and semantic dementia. Newsletter
 For carers and relatives of people with frontotemporal dementia and semantic dementia Newsletter AUGUST 2008 1 Welcome Welcome to the August edition of our CFU Support Group Newsletter. Thanks to all of
For carers and relatives of people with frontotemporal dementia and semantic dementia Newsletter AUGUST 2008 1 Welcome Welcome to the August edition of our CFU Support Group Newsletter. Thanks to all of
Parkinson s for Care Staff
 Unit 28: Understand Parkinson s for Care Staff Unit reference number: A/616/7339 Level: 3 Unit type: Optional Credit value: 2 Guided learning hours: 14 Unit summary Parkinson s is a progressive neurological
Unit 28: Understand Parkinson s for Care Staff Unit reference number: A/616/7339 Level: 3 Unit type: Optional Credit value: 2 Guided learning hours: 14 Unit summary Parkinson s is a progressive neurological
WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient
 DEMENTIA WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient Progressive and disabling Not an inherent aspect of
DEMENTIA WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient Progressive and disabling Not an inherent aspect of
Dementia and Healthy Ageing : is the pathology any different?
 Dementia and Healthy Ageing : is the pathology any different? Professor David Mann, Professor of Neuropathology, University of Manchester, Hope Hospital, Salford DEMENTIA Loss of connectivity within association
Dementia and Healthy Ageing : is the pathology any different? Professor David Mann, Professor of Neuropathology, University of Manchester, Hope Hospital, Salford DEMENTIA Loss of connectivity within association
Parkinson s Disease in the Elderly A Physicians perspective. Dr John Coyle
 Parkinson s Disease in the Elderly A Physicians perspective Dr John Coyle Overview Introduction Epidemiology and aetiology Pathogenesis Diagnosis and clinical features Treatment Psychological issues/ non
Parkinson s Disease in the Elderly A Physicians perspective Dr John Coyle Overview Introduction Epidemiology and aetiology Pathogenesis Diagnosis and clinical features Treatment Psychological issues/ non
Resources: Types of dementia
 1/5 Dementia is an umbrella term for a number of progressive conditions affecting the functioning of the brain. Different types of dementia have different causes. There are a great number of rare forms.
1/5 Dementia is an umbrella term for a number of progressive conditions affecting the functioning of the brain. Different types of dementia have different causes. There are a great number of rare forms.
DEMENTIA. Stephanie Janka Spurlock and Mandy Nagy T&SDFT trainers and assessors
 DEMENTIA Stephanie Janka Spurlock and Mandy Nagy T&SDFT trainers and assessors amanda.nagy@nhs.net Definition Dementia is an umbrella term used to describe a set of symptoms that may include memory loss
DEMENTIA Stephanie Janka Spurlock and Mandy Nagy T&SDFT trainers and assessors amanda.nagy@nhs.net Definition Dementia is an umbrella term used to describe a set of symptoms that may include memory loss
MAXIMIZING FUNCTION IN PARKINSON S DISEASE
 1 MAXIMIZING FUNCTION IN PARKINSON S DISEASE September 13, 2016 End Falls This Falls Conference Jan Goldstein Elman One Step Ahead Mobility Toronto, Ontario Outline An overview of Parkinson s disease (PD):
1 MAXIMIZING FUNCTION IN PARKINSON S DISEASE September 13, 2016 End Falls This Falls Conference Jan Goldstein Elman One Step Ahead Mobility Toronto, Ontario Outline An overview of Parkinson s disease (PD):
100 billion neurons!
 100 billion neurons! Where s my car parked? Normal Memory Changes with Age Memory changes start even before 30 Harder to store new memories Sensory inputs aren't as sharp hear, see, taste Multi-tasking
100 billion neurons! Where s my car parked? Normal Memory Changes with Age Memory changes start even before 30 Harder to store new memories Sensory inputs aren't as sharp hear, see, taste Multi-tasking
What is. frontotemporal. address? dementia?
 What is frontotemporal address? dementia? Contents 03 What is frontotemporal dementia? 04 Symptoms 05 Diagnosis 06 Treatments Information in this booklet is for anyone who wants to know more about frontotemporal
What is frontotemporal address? dementia? Contents 03 What is frontotemporal dementia? 04 Symptoms 05 Diagnosis 06 Treatments Information in this booklet is for anyone who wants to know more about frontotemporal
Palliative Approach to the Person with Advanced Dementia
 Mid North Coast Rural Palliative Care Project Link Nurse Education 2004 Palliative Approach to the Person with Advanced Dementia Anne Sneesby CNC - ACAT To care for the dying is a very human opportunity
Mid North Coast Rural Palliative Care Project Link Nurse Education 2004 Palliative Approach to the Person with Advanced Dementia Anne Sneesby CNC - ACAT To care for the dying is a very human opportunity
Multiple System Atrophy
 Multiple System Atrophy This document has been prepared to help you become more informed about Multiple System Atrophy. It is designed to answer questions about the condition and includes suggestions on
Multiple System Atrophy This document has been prepared to help you become more informed about Multiple System Atrophy. It is designed to answer questions about the condition and includes suggestions on
Parkinson s Disease Update. Presented by Joanna O Leary, MD Movement disorder neurologist Providence St. Vincent s
 Parkinson s Disease Update Presented by Joanna O Leary, MD Movement disorder neurologist Providence St. Vincent s What is a movement disorder? Neurological disorders that affect ability to move by causing
Parkinson s Disease Update Presented by Joanna O Leary, MD Movement disorder neurologist Providence St. Vincent s What is a movement disorder? Neurological disorders that affect ability to move by causing
PD ExpertBriefing: Cognition and PD: What You ve Always Wanted to Know But Were Too Afraid to Ask. Presented By: Tuesday, March 22, 2011 at 1:00 PM ET
 PD ExpertBriefing: Cognition and PD: What You ve Always Wanted to Know But Were Too Afraid to Ask Presented By: Alexander I. Tröster, PhD, ABPP University of North Carolina, Chapel Hill, NC Tuesday, March
PD ExpertBriefing: Cognition and PD: What You ve Always Wanted to Know But Were Too Afraid to Ask Presented By: Alexander I. Tröster, PhD, ABPP University of North Carolina, Chapel Hill, NC Tuesday, March
Old Age and Stress. Disorders of Aging and Cognition. Disorders of Aging and Cognition. Chapter 18
 Disorders of Aging and Cognition Chapter 18 Slides & Handouts by Karen Clay Rhines, Ph.D. Northampton Community College Comer, Abnormal Psychology, 8e Disorders of Aging and Cognition Dementia deterioration
Disorders of Aging and Cognition Chapter 18 Slides & Handouts by Karen Clay Rhines, Ph.D. Northampton Community College Comer, Abnormal Psychology, 8e Disorders of Aging and Cognition Dementia deterioration
Dementia Diagnosis Guidelines Primary Care
 Dementia Diagnosis Guidelines Primary Care Dementia Diagnosis Primary Care Guidelines Introduction Dementia is a long term condition, which primarily affects people over the age of 65 (late on-set dementia)
Dementia Diagnosis Guidelines Primary Care Dementia Diagnosis Primary Care Guidelines Introduction Dementia is a long term condition, which primarily affects people over the age of 65 (late on-set dementia)
Understanding Dementia
 Understanding Dementia Dr. Dallas Seitz MD FRCPC Assistant Professor, Department of Psychiatry, Queen s University, Kingston, Ontario, Canada What s Next Information about Dementia, Elder Care and Supports
Understanding Dementia Dr. Dallas Seitz MD FRCPC Assistant Professor, Department of Psychiatry, Queen s University, Kingston, Ontario, Canada What s Next Information about Dementia, Elder Care and Supports
Evaluation of Parkinson s Patients and Primary Care Providers
 Evaluation of Parkinson s Patients and Primary Care Providers 2018 Movement Disorders Half Day Symposium Elise Anderson MD Medical Co-Director, PBSI Movement Disorders 6/28/2018 1 Disclosures GE Speaker,
Evaluation of Parkinson s Patients and Primary Care Providers 2018 Movement Disorders Half Day Symposium Elise Anderson MD Medical Co-Director, PBSI Movement Disorders 6/28/2018 1 Disclosures GE Speaker,
Parkinson s Disease. Prevalence. Mark S. Baron, M.D. Cardinal Features. Clinical Characteristics. Not Just a Movement Disorder
 Prevalence Parkinson s Disease Mark S. Baron, M.D. Associate Professor of Neurology Movement Disorders Section VCU School of Medicine Common disorder Approaching 1% by 65 yrs of age, 2% by 80 yrs of age
Prevalence Parkinson s Disease Mark S. Baron, M.D. Associate Professor of Neurology Movement Disorders Section VCU School of Medicine Common disorder Approaching 1% by 65 yrs of age, 2% by 80 yrs of age
Do not copy or distribute without permission. S. Weintraub, CNADC, NUFSM, 2009
 Sandra Weintraub, Ph.D. Clinical Core Director, Cognitive Neurology and Alzheimer s Disease Center Northwestern University Feinberg School of Medicine Chicago, Illinois Dementia: a condition caused by
Sandra Weintraub, Ph.D. Clinical Core Director, Cognitive Neurology and Alzheimer s Disease Center Northwestern University Feinberg School of Medicine Chicago, Illinois Dementia: a condition caused by
Frontotemporal Dementia: Towards better diagnosis. Frontotemporal Dementia. John Hodges, NeuRA & University of New South Wales, Sydney.
 I.1 I.2 II.1 II.2 II.3 II.4 II.5 II.6 III.1 III.2 III.3 III.4 III.5 III.6 III.7 III.8 III.9 III.10 III.11 III.12 IV.1 IV.2 IV.3 IV.4 IV.5 Frontotemporal Dementia: Towards better diagnosis Frontotemporal
I.1 I.2 II.1 II.2 II.3 II.4 II.5 II.6 III.1 III.2 III.3 III.4 III.5 III.6 III.7 III.8 III.9 III.10 III.11 III.12 IV.1 IV.2 IV.3 IV.4 IV.5 Frontotemporal Dementia: Towards better diagnosis Frontotemporal
Differentiating Dementia Diagnoses
 Differentiating Dementia Diagnoses Waitemata PHO 21 October 2014 Dr Michal Boyd, RN, NP, ND Nurse Practitioner Older Adults School of Nursing & Freemasons Dept. of Geriatric Medicine The University of
Differentiating Dementia Diagnoses Waitemata PHO 21 October 2014 Dr Michal Boyd, RN, NP, ND Nurse Practitioner Older Adults School of Nursing & Freemasons Dept. of Geriatric Medicine The University of
White matter hyperintensities correlate with neuropsychiatric manifestations of Alzheimer s disease and frontotemporal lobar degeneration
 White matter hyperintensities correlate with neuropsychiatric manifestations of Alzheimer s disease and frontotemporal lobar degeneration Annual Scientific Meeting Canadian Geriatric Society Philippe Desmarais,
White matter hyperintensities correlate with neuropsychiatric manifestations of Alzheimer s disease and frontotemporal lobar degeneration Annual Scientific Meeting Canadian Geriatric Society Philippe Desmarais,
A BRIEF LOOK AT DEMENTIA
 Dementia A BRIEF LOOK AT DEMENTIA David Kaufman, MD Neurology Consultants of Bellin Health November 2, 2017 Defined as a progressive decline in cognitive function that impairs daily activities. Always
Dementia A BRIEF LOOK AT DEMENTIA David Kaufman, MD Neurology Consultants of Bellin Health November 2, 2017 Defined as a progressive decline in cognitive function that impairs daily activities. Always
Parkinsonian Disorders with Dementia
 Parkinsonian Disorders with Dementia George Tadros Consultant in Old Age Liaison Psychiatry, RAID, Heartlands Hospital Professor of Dementia and Liaison Psychiatry, Aston Medical School Aston University
Parkinsonian Disorders with Dementia George Tadros Consultant in Old Age Liaison Psychiatry, RAID, Heartlands Hospital Professor of Dementia and Liaison Psychiatry, Aston Medical School Aston University
Faculty. Joseph Friedman, MD
 Faculty Claire Henchcliffe, MD, DPhil Associate Professor of Neurology Weill Cornell Medical College Associate Attending Neurologist New York-Presbyterian Hospital Director of the Parkinson s Institute
Faculty Claire Henchcliffe, MD, DPhil Associate Professor of Neurology Weill Cornell Medical College Associate Attending Neurologist New York-Presbyterian Hospital Director of the Parkinson s Institute
Issues for Patient Discussion
 onmotor complications radykinesia Screening Tools asked PD micrographia eurodegeneration Designed for Use by Family Practitioners remor on-off opamine agonists tiffness depression ostural instability wearing
onmotor complications radykinesia Screening Tools asked PD micrographia eurodegeneration Designed for Use by Family Practitioners remor on-off opamine agonists tiffness depression ostural instability wearing
Diagnosis and management of non-alzheimer dementias. Melissa Yu, M.D. Department of Neurology
 Diagnosis and management of non-alzheimer dementias Melissa Yu, M.D. Department of Neurology AGENDA Introduction When to think of alternate diagnoses Other forms of dementia Other reasons for confusion
Diagnosis and management of non-alzheimer dementias Melissa Yu, M.D. Department of Neurology AGENDA Introduction When to think of alternate diagnoses Other forms of dementia Other reasons for confusion
What is dementia? Symptoms. alzheimers.org.uk
 alzheimers.org.uk What is dementia? This factsheet explains what dementia is, including the causes and symptoms, and how it is diagnosed and treated. It also looks at some of the different types of dementia.
alzheimers.org.uk What is dementia? This factsheet explains what dementia is, including the causes and symptoms, and how it is diagnosed and treated. It also looks at some of the different types of dementia.
What is dementia? What is dementia?
 What is dementia? What is dementia? What is dementia? Dementia is an umbrella term for a range of progressive conditions that affect the brain. There are over 200 subtypes of dementia, but the five most
What is dementia? What is dementia? What is dementia? Dementia is an umbrella term for a range of progressive conditions that affect the brain. There are over 200 subtypes of dementia, but the five most
The PD You Don t See: Cognitive and Non-motor Symptoms
 The PD You Don t See: Cognitive and Non-motor Symptoms Benzi M. Kluger, M.D., M.S. Associate Professor of Neurology and Psychiatry Director Movement Disorders Center University of Colorado Denver Goals
The PD You Don t See: Cognitive and Non-motor Symptoms Benzi M. Kluger, M.D., M.S. Associate Professor of Neurology and Psychiatry Director Movement Disorders Center University of Colorado Denver Goals
The prevalence of YOD increases almost exponentially with age (as does the prevalence of late onset dementia).
.") Factsheet 1 Young Onset Dementia (YOD) Dementia is commonly seen as a health and social problem of older adults. Nevertheless dementia can occur earlier in life. Young onset dementia is defined by an onset
Factsheet 1 Young Onset Dementia (YOD) Dementia is commonly seen as a health and social problem of older adults. Nevertheless dementia can occur earlier in life. Young onset dementia is defined by an onset
A Fresh View of Cognitive Disorders in Older Adults: New Classification and Screening Strategies
 A Fresh View of Cognitive Disorders in Older Adults: New Classification and Screening Strategies Lynda Mackin, PhD, AGPCNP-BC, CNS University of California San Francisco School of Nursing 1 Alzheimer s
A Fresh View of Cognitive Disorders in Older Adults: New Classification and Screening Strategies Lynda Mackin, PhD, AGPCNP-BC, CNS University of California San Francisco School of Nursing 1 Alzheimer s
Lecture 42: Final Review. Martin Wessendorf, Ph.D.
 Lecture 42: Final Review Martin Wessendorf, Ph.D. Lecture 33 cortex Heilbronner 5 lobes of the cortex Lateral view (left side) Mid-saggital view (right side) Cellular organization of cortex White matter
Lecture 42: Final Review Martin Wessendorf, Ph.D. Lecture 33 cortex Heilbronner 5 lobes of the cortex Lateral view (left side) Mid-saggital view (right side) Cellular organization of cortex White matter
Understanding Dementia & Symptoms:
 Understanding Dementia & Symptoms: What is Happening? & How to Help! Teepa Snow, MS, OTR/L, FAOTA Dementia Care & Training Specialist, Positive Approach, LLC Consulting Associate, Duke University School
Understanding Dementia & Symptoms: What is Happening? & How to Help! Teepa Snow, MS, OTR/L, FAOTA Dementia Care & Training Specialist, Positive Approach, LLC Consulting Associate, Duke University School
DEMENTIA ANDREA BERG, MD
 DEMENTIA ANDREA BERG, MD What Is Dementia? Decline in memory, language, problem-solving and other cognitive skills that affects a persons ability to perform everyday activities Progressive and disabling
DEMENTIA ANDREA BERG, MD What Is Dementia? Decline in memory, language, problem-solving and other cognitive skills that affects a persons ability to perform everyday activities Progressive and disabling
PARKINSON S PRIMER. Dr. Kathryn Giles MD, MSc, FRCPC Cambridge, Ontario, Canada
 PARKINSON S PRIMER Dr. Kathryn Giles MD, MSc, FRCPC Cambridge, Ontario, Canada COPYRIGHT 2017 BY SEA COURSES INC. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
PARKINSON S PRIMER Dr. Kathryn Giles MD, MSc, FRCPC Cambridge, Ontario, Canada COPYRIGHT 2017 BY SEA COURSES INC. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Understanding Dementia
 Dementia Handbook for Carers Essex Understanding Dementia What is dementia? 1 Summary of dementia symptoms 4 Medication and treatment 5 1 Dementia is the name for several conditions that lead to the progressive
Dementia Handbook for Carers Essex Understanding Dementia What is dementia? 1 Summary of dementia symptoms 4 Medication and treatment 5 1 Dementia is the name for several conditions that lead to the progressive
Movement Disorders- Parkinson s Disease. Fahed Saada, MD March 8 th, th Family Medicine Refresher Course St.
 Movement Disorders- Parkinson s Disease Fahed Saada, MD March 8 th, 2019 48 th Family Medicine Refresher Course St. Joseph s Health Disclosure ACADIA Pharmaceuticals Objectives Review the classification
Movement Disorders- Parkinson s Disease Fahed Saada, MD March 8 th, 2019 48 th Family Medicine Refresher Course St. Joseph s Health Disclosure ACADIA Pharmaceuticals Objectives Review the classification
Dementia. Dr Maria Foundas Consultant Physician. Training support Skills development Competency Assessment Scholarships Education
 Dementia Dr Maria Foundas Consultant Physician Training support Skills development Competency Assessment Scholarships Education Preamble and disclaimer These slides are made available by the Western Australian
Dementia Dr Maria Foundas Consultant Physician Training support Skills development Competency Assessment Scholarships Education Preamble and disclaimer These slides are made available by the Western Australian
Elizabeth Rhynold MD FRCPC Geriatric Medicine
 Elizabeth Rhynold MD FRCPC Geriatric Medicine erhynold@pmh-mb.ca Faculty: Elizabeth Rhynold Relationships with commercial interests: Grants/Research Support: Not applicable Speakers Bureau/Honoraria: Not
Elizabeth Rhynold MD FRCPC Geriatric Medicine erhynold@pmh-mb.ca Faculty: Elizabeth Rhynold Relationships with commercial interests: Grants/Research Support: Not applicable Speakers Bureau/Honoraria: Not
Dementia: Diagnosis and Treatment
 Dementia: Diagnosis and Treatment Outline 1. Risk factors and definition of dementia 2. Types of Dementias 3. MMSE and testing 4. Treatment options Cognitive decline with aging Mild changes in memory and
Dementia: Diagnosis and Treatment Outline 1. Risk factors and definition of dementia 2. Types of Dementias 3. MMSE and testing 4. Treatment options Cognitive decline with aging Mild changes in memory and
If you have dementia, you may have some or all of the following symptoms.
 About Dementia Dementia may be caused by a number of illnesses that affect the brain. Dementia typically leads to memory loss, inability to do everyday things, difficulty in communication, confusion, frustration,
About Dementia Dementia may be caused by a number of illnesses that affect the brain. Dementia typically leads to memory loss, inability to do everyday things, difficulty in communication, confusion, frustration,