Hospice 101: A Primer for the PCP/Hospitalist. John Thompson, II DO, DABFM, HMDC
|
|
|
- Muriel Cannon
- 5 years ago
- Views:
Transcription

1 Hospice 101: A Primer for the PCP/Hospitalist John Thompson, II DO, DABFM, HMDC
2 Objectives: Understand the difference between Hospice and Palliative Medicine. Have a general understanding of hospice criteria for various disease states and when to refer to hospice. Review of commonly used pain medicines in hospice care. Introduction to prognostication. Review of Hospice levels of care.
3 Hospice To neither hasten nor delay an inevitable death. From our friends at Wikipedia: Hospice care is a type of care and philosophy of care that focuses on the palliation of a chronically ill, terminally ill or seriously ill patient's pain and symptoms, while attending to their emotional and spiritual needs. Patients not seeking/no longer seeking curative treatment. An interdisciplinary, not a multidisciplinary, approach involving Physicians, RNs, Social Workers, Chaplains, and Volunteers. Guidelines i.e. regulations are set by Medicare.
4 Hospice Is a home based program! Unless a patient has straight Medi-Cal or is VA affiliated hospice does not pay for care in a SNF (except Respite Care). It is NOT 24 hour care (with certain exceptions), but it IS 24/7 nursing availability. Is reimbursed on a per-diem/day rate model, so any treatments related to the terminal diagnosis come out of the hospice per diem bucket. Treatments that are not related to the terminal diagnosis are still covered by Medicare/insurance. All hospice expenses come out of that bucket; RN visits, Hospice Aides, Chaplain visits, meds, etc. Example: Patient on service for liver failure with comorbid COPD, we pay for lasix, aldactone, lactulose, and anything related to liver disease. Medicare pays for Combivent, Advair, etc.

5 Palliative Medicine An approach to medicine that focuses on relieving symptoms, not necessarily attempting to cure, the underlying disease process. NOT the same as Hospice! Many Palliative Care docs/clinics follow oncology, CHF, COPD, etc. patients that are seeking curative/life prolonging treatments.

6 Continuum of Care
7 Hospice Criteria Generally, life expectancy of 6 months or less. Guidelines are set by Medicare. Though the guidelines are set by CMS/Medicare, they are still generally guidelines and for the most part we have some latitude to use our clinical judgement. However, if the patient doesn t meet any specific disease criteria we as Medical Directors still need to make a convincing case that the life expectancy is 6 months or less.
8 Disease Specific Criteria Cancer - progressed despite treatment or metastatic at time of presentation and not, or no longer, seeking curative treatment. Dementia - What? No longer allowed (except specific diagnoses such as Alzheimer s, Lewey Body, Frontotemporal). Cerebrovascular Disease is our new Dementia &/or Debility and Decline.
9 Criteria - cont. Liver Disease, need criteria from 1 & 2: 1. INR >/=1.5 & </=Albumin Ascites refractory to treatment (or patient noncompliant), SBP, HRS, Hepatic encephalopathy refractory to treatment (or pt noncompliant), Recurrent variceal bleeding. Patients seeking liver transplant can be on hospice.
10 Criteria - cont. Renal Disease, need 1 AND 2 or 3: 1. Not seeking dialysis or transplant (or discontinuing dialysis). 2. Creatinine clearance <10mL/min (<15mL/min in diabetics) or <15mL/min (<20mL/min in diabetics) if pt has comorbid CHF. 3. Serum creatinine >8.0 mg/dl (>6.0 mg/dl in diabetics).

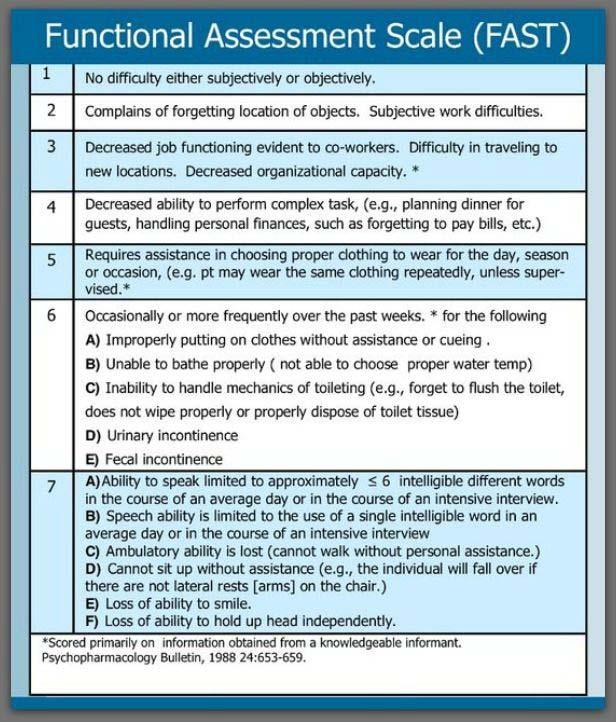
11 FAST Score


12 Criteria - cont. Alzheimer s Disease - FAST 7C with recent (last 12 months) sepsis, recurrent pneumonia/uti s, etc. or FAST worse than 7C. Parkinson s - Stage 5: Patients fall when standing or turning, falling or freezing when walking, hallucinations or delusions. ALS - significant breathing impairment and not using or going off of a vent, significant dysphagia and no artificial hydration/nutrition, etc. COPD/CHF - SOB at rest worse with minimal exertion creating a bed to chair existence, ie Class IV CHF.
13 Certification Initial certification can be done by a phone call. Requires a Certification of Terminal Illness (CTI) from a PCP and the Hospice Medical Director. If you are asked to follow a patient on hospice, it generally means that you are willing to remain the PCP for the patient and will continue to manage the nonhospice related issues (although we usually manage most issues on our hospice patients). It usually DOES NOT mean that you are managing the day to day aspects of the hospice patient. This can be anything from getting simple updates to taking the first call on pain issues. First 2 certification periods are for two 90 day periods (180 days).
14 Re-Certification Each recertification period is for 60 days. Each recertification after the initial two 90 day periods requires a face to face visit by a physician/np. Need to show decline in the patient. Commonly used symptoms of decline: Weight loss/muscle wasting (decrease in mid arm circumference). Decreased intake, usually measured objectively in cups per meal/day. Skin break down! Has the patient started to develop pressure sores, deep tissue injuries, etc? Are they healing, staying the same or getting worse? Increased sleeping/social withdrawal.


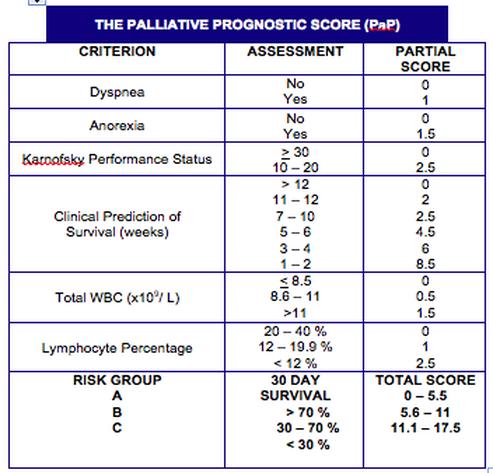
15 Prognostication Palliative Prognostic Score (PaP) - relies heavily on the clinical estimation of life expectancy, has been validated in adult and pediatric oncology populations, has been validated in oncology and non-oncology patients, and has been validated in large prospective studies. COPD - BODE score, based on BMI, exercise tolerance, FEV1, dyspnea rating. Alzheimer s Disease - Mortality Risk Index (validated for Nursing Home residents only).
16

: 1 year survival 85-90% Class")
17 Prognostication - cont. Congestive Heart Failure: NYHA Class II (dyspnea w/ normal activity): 1 year survival 90-95% Class III (dyspnea w/ mild activity): 1 year survival 85-90% Class IV (dyspnea at rest): 1 year survival 30-40%!

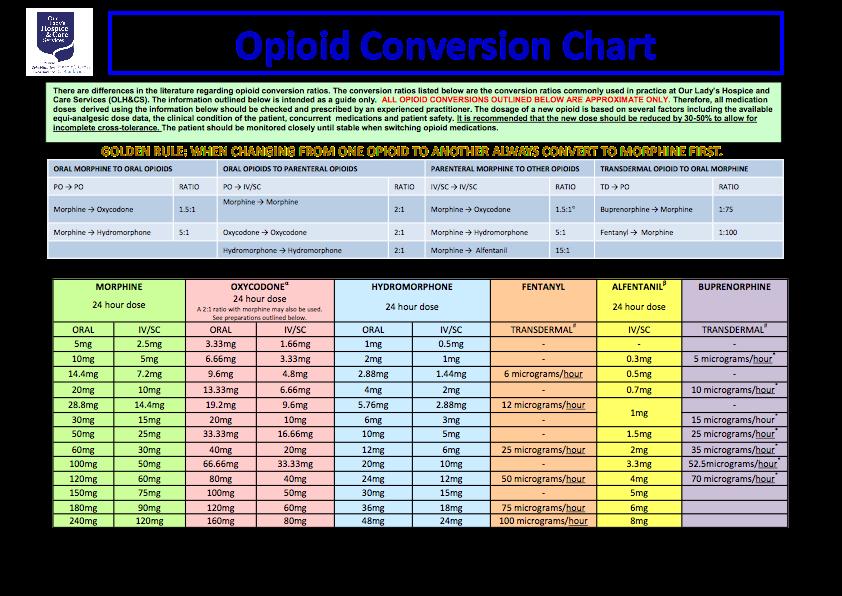
18 Pain Medications Morphine - Oral Morphine Equivalent (OME) the gold standard of pain meds, right? 1mg oral morphine = 1mg hydrocodone 1mg IV morphine = 3mg oral morphine/hydrocodone This means 2mg of IV morphine is the equivalent of 6mg of oral hydrocodone which means 2mg of IV morphine is roughly equivalent to taking a Vicodin after a procedure!
19 Pain Meds - cont. Equivalencies: 1.5 OME = 1mg oxycodone (Percocet) 5 OME = 1mg oral hydromorphone (Dilaudid) 25mcg/hr fentanyl patch = OME/day 50mcg/hr = OME/day 100mcg/hr = OME/day 150mcg/hr = OME/day, etc.
20 Pain Meds - cont. Methadone - dosing too complicated to get into here, but you do NOT need special licensing to prescribe it unless you are prescribing for maintenance therapy for opioid addiction! Start low and go slow; we commonly start patients out at 2.5mg one to two times a day, depending on their opioid usage and history. Affects QT interval, so caution in cardiac patients. Numerous potential drug-drug interactions. The only long acting opioid available in a liquid formulation.
21
. $156.06/day.")
22 Levels of Care Routine Home Care - what most folks are familiar with, a hospice patient at home, or a SNF, getting routine hospice care provided by the family (usually) with the support of hospice staff (CNA, LVN, RN, SW, Chaplain). $156.06/day. Continuous Care - for hospice patients in crisis (pain crisis, uncontrolled delirium, terminal agitation, etc) an RN for at least 8 out of 24 hours at the patients bedside in the home/snf to help control symptoms. Most expensive level of care: $910.78/day. Respite Care - usually provided in a SNF or inpatient hospice unit and provides for up to 5 days respite for care givers. $161.42/day.
23 Levels of Care - cont. General Inpatient - provided in a medicare approved inpatient hospice, hospital, or SNF and is for symptom management that requires 24 hour nursing attention/intervention that cannot be provided at a lower level of care. It is not a default status for patients that are actively dying, or for patients whose caregiving situation has broken down. $694.19/day. Per diem rates quoted are the national base rates for 2014, they are regionally adjusted based on the Wage Index for various geographic regions.
24 Take Home Points Medicare guidelines set the standard. Palliative Care and Hospice are not the same thing. Let your Palliative Care Team, if you have one, help you! If you don t have one, don t be afraid to start the conversation. If you are the one giving the bad news ask the patient and/or family what they heard regarding what was said not unusual for people to hear something different than what we think we said. There are validated models for prognostication for most disease states, but they are still only an estimate: Remember, People plan, and God laughs! Morphine, not quite as potent as we all think, but still the Gold Standard.
25 Take Home - cont. Please don t under medicate patients with legitimate sources of pain: I m not saying let s go back to pain is what the patient says it is, but my understanding is metastatic cancer can be painful and 2mg of IV morphine every 4 hours might be under treating. Hospice is a home based program, please don t tell patients they can go to a SNF with hospice without consulting your case managers/discharge planners. If you have a patient with class III-IV NYHA CHF, or O2 dependent COPD, consider a Palliative Care discussion/referral regarding goals of care. If they are truly class IV &/or O2 dependent you can refer for help with symptom management too!

26 Resources Oxford American Handbook of Hospice and Palliative Medicine and Supportive Care, 2nd Edition, Yennurajalingam & Bruera, Oxford University Press, 2016 Hospice Quickflips: A Guide for Hospice Clinicians, The Corridor Group, 2006/Reviewed 2015 Scottish Palliative Care Guidelines, The American Academy of Hospice and Palliative Medicine,
Objectives 2/11/2016 HOSPICE 101
 HOSPICE 101 Overview Hospice History and Statistics What is Hospice? Who qualifies for services? Levels of Service The Admission Process Why Not to Wait Objectives Understand how to determine hospice eligibility
HOSPICE 101 Overview Hospice History and Statistics What is Hospice? Who qualifies for services? Levels of Service The Admission Process Why Not to Wait Objectives Understand how to determine hospice eligibility
Medicare hospice benefit. Katherine Dietrich, DO HMDC FACP CPE
 Medicare hospice benefit Katherine Dietrich, DO HMDC FACP CPE Disclosures Hospice Compassus Medical Director Billings MT Which of the following is correct about the Medicare Hospice Benefit? A. Once a
Medicare hospice benefit Katherine Dietrich, DO HMDC FACP CPE Disclosures Hospice Compassus Medical Director Billings MT Which of the following is correct about the Medicare Hospice Benefit? A. Once a
Hospice Eligibility August 2018
 Hospice Eligibility August 2018 Objectives Identify who can make a hospice referral Review hospice eligibility and disease-specific prognostic indicators Review Open Access philosophy Who Can Make A Referral
Hospice Eligibility August 2018 Objectives Identify who can make a hospice referral Review hospice eligibility and disease-specific prognostic indicators Review Open Access philosophy Who Can Make A Referral
Life is pleasant. Death is peaceful. It s the transition that s troublesome. Isaac Asimov ( )
") Life is pleasant. Death is peaceful. It s the transition that s troublesome. Isaac Asimov (1920-1992) Objectives Palliative care versus hospice care. Admission guidelines to hospice services. Having the
Life is pleasant. Death is peaceful. It s the transition that s troublesome. Isaac Asimov (1920-1992) Objectives Palliative care versus hospice care. Admission guidelines to hospice services. Having the
Determining Eligibility for Hospice Care
 Determining Eligibility for Hospice Care Main Number: 203 739-8300 Toll Free Number: 888 357-3334 www.regionalhospicect.org Many people may not understand all that Regional Hospice can offer or they are
Determining Eligibility for Hospice Care Main Number: 203 739-8300 Toll Free Number: 888 357-3334 www.regionalhospicect.org Many people may not understand all that Regional Hospice can offer or they are
There For You. Your Compassionate Guide. World-Class Hospice Care Since 1979
 There For You Your Compassionate Guide World-Class Hospice Care Since 1979 What Is Hospice? Hospice is a type of care designed to provide support during an advanced illness. Hospice care focuses on comfort
There For You Your Compassionate Guide World-Class Hospice Care Since 1979 What Is Hospice? Hospice is a type of care designed to provide support during an advanced illness. Hospice care focuses on comfort
Palliative and Hospice Care of the Terminally Ill Introduction
 Palliative and Hospice Care of the Terminally Ill Introduction There has been an increase in life expectancy for men and women of all races to 77.6 years Leading causes of death in older patients are chronic
Palliative and Hospice Care of the Terminally Ill Introduction There has been an increase in life expectancy for men and women of all races to 77.6 years Leading causes of death in older patients are chronic
Primary Palliative Care
 Primary Palliative Care Amanda Overstreet, DO October 20, 2017 No financial disclosures Objectives Discuss palliative care and how it differs from hospice Explore how to manage patients goals and expectations
Primary Palliative Care Amanda Overstreet, DO October 20, 2017 No financial disclosures Objectives Discuss palliative care and how it differs from hospice Explore how to manage patients goals and expectations
Hospice Basics and Benefits
 Hospice Basics and Benefits Goal To educate health care professionals about hospice basics and the benefits for the patient and family. 2 Objectives Describe the history and philosophy of the hospice movement
Hospice Basics and Benefits Goal To educate health care professionals about hospice basics and the benefits for the patient and family. 2 Objectives Describe the history and philosophy of the hospice movement
BACK TO THE FUTURE: Palliative Care in the 21 st Century
 BACK TO THE FUTURE: Palliative Care in the 21 st Century Section 3: Hospice 101 I m not afraid of death; I just don t want to be there when it happens. -Woody Allen A Century of Change 1900 2000 Age at
BACK TO THE FUTURE: Palliative Care in the 21 st Century Section 3: Hospice 101 I m not afraid of death; I just don t want to be there when it happens. -Woody Allen A Century of Change 1900 2000 Age at
How Can Palliative Care Help Your Patient Get Home Sooner?
 How Can Palliative Care Help Your Patient Get Home Sooner? Annette T. Carron, D.O. Director Geriatrics and Palliative Care Botsford Hospital OMED 2014 Patient Care Issues That Can Delay Your Day/ Pain
How Can Palliative Care Help Your Patient Get Home Sooner? Annette T. Carron, D.O. Director Geriatrics and Palliative Care Botsford Hospital OMED 2014 Patient Care Issues That Can Delay Your Day/ Pain
Palliative Care and Hospice. Silver Linings: Reflecting on Our Past & Transitioning into our Future
 Palliative Care and Hospice Silver Linings: Reflecting on Our Past & Transitioning into our Future Objectives: 1. What is Palliative Care? What is Hospice? What is the difference? 2. What are the trending
Palliative Care and Hospice Silver Linings: Reflecting on Our Past & Transitioning into our Future Objectives: 1. What is Palliative Care? What is Hospice? What is the difference? 2. What are the trending
CareFirst Hospice. Health care for the end of life. CareFirst
 Hospice Health care for the end of life 1 What is Hospice? Hospice is a philosophy- When a person in end stages of an illness can no longer receive, or wants to receive, life sustaining treatment, he or
Hospice Health care for the end of life 1 What is Hospice? Hospice is a philosophy- When a person in end stages of an illness can no longer receive, or wants to receive, life sustaining treatment, he or
Hospice Approach to Caring Ellen M. Brown M.D.
 Hospice Approach to Caring Ellen M. Brown M.D. bjectives By the conclusion of this session, attendees will be able to: Explain the hospice philosophy and goals Understand what is covered by the hospice
Hospice Approach to Caring Ellen M. Brown M.D. bjectives By the conclusion of this session, attendees will be able to: Explain the hospice philosophy and goals Understand what is covered by the hospice
Three triggers that suggest that patients could benefit from a hospice palliative care approach
 Why is it important to identify people nearing the end of life? About 1% of the population dies each year. Although some deaths are unexpected, many more in fact can be predicted. This is inherently difficult,
Why is it important to identify people nearing the end of life? About 1% of the population dies each year. Although some deaths are unexpected, many more in fact can be predicted. This is inherently difficult,
August 16, Healthy Living Conference For Seniors and Caregivers VITAS 1. What we Know. Defining Palliative Care: Comfort. Symptom Management.
 Comfort. Symptom Management. Respect. & Hospice Care Pam Wright, LCSW Licensed Clinical Social Worker pamela.wright@vitas.com 626-918-2273 What we Know Defining : Palliative care is medical care that relieves
Comfort. Symptom Management. Respect. & Hospice Care Pam Wright, LCSW Licensed Clinical Social Worker pamela.wright@vitas.com 626-918-2273 What we Know Defining : Palliative care is medical care that relieves
Objectives. ORC Definition. Definitions of Palliative Care. CMS and National Quality Forum Definition (2013) CAPC 9/7/2017
 CAPC 9/7/2017") Objectives General overview of palliative care Define the role of palliative care Palliative Care Management and Transition Joan Hanson, Director of WRN Palliative Care, RN, CHPCA Jennifer Martnick, Team
Objectives General overview of palliative care Define the role of palliative care Palliative Care Management and Transition Joan Hanson, Director of WRN Palliative Care, RN, CHPCA Jennifer Martnick, Team
Module 1: Principles of Palliative Care. Part I: Dying Well. A Good Death Defined
 E L N E C End-of-Life Nursing Education Consortium Geriatric Curriculum Module 1: Principles of Palliative Care Part I: Dying Well A natural part of life Opportunity for growth Profoundly personal experience
E L N E C End-of-Life Nursing Education Consortium Geriatric Curriculum Module 1: Principles of Palliative Care Part I: Dying Well A natural part of life Opportunity for growth Profoundly personal experience
End of Life with Dementia Sue Quist RN, CHPN
 End of Life with Dementia Sue Quist RN, CHPN Objectives: Describe the Medicare hospice benefit and services. Discuss the Medicare admission criteria for hospice patients with dementia due to Alzheimer
End of Life with Dementia Sue Quist RN, CHPN Objectives: Describe the Medicare hospice benefit and services. Discuss the Medicare admission criteria for hospice patients with dementia due to Alzheimer
Alzheimer s Disease, Dementia, Related Disorders
 Alzheimer s Disease, Dementia, Related Disorders Stage 7 on the FAST Scale signifies the threshold of activity limitation that would support a six-month prognosis. The FAST Scale does not address the impact
Alzheimer s Disease, Dementia, Related Disorders Stage 7 on the FAST Scale signifies the threshold of activity limitation that would support a six-month prognosis. The FAST Scale does not address the impact
Partnership HealthPlan s Implementation of SB Robert Moore, MD MPH MBA. Chief Medical Officer, Partnership HealthPlan of California
 Partnership HealthPlan s Implementation of SB 1004 Robert Moore, MD MPH MBA Chief Medical Officer, Partnership HealthPlan of California Medi-Cal Managed Care Model: County Organized Health System Mission:
Partnership HealthPlan s Implementation of SB 1004 Robert Moore, MD MPH MBA Chief Medical Officer, Partnership HealthPlan of California Medi-Cal Managed Care Model: County Organized Health System Mission:
HOSPICE My lecture outline
 Objectives: o Describe a brief history of the development of hospice care o Describe the hospice philosophy of care o Describe the referral process o Describe hospice services o Describe reimbursement
Objectives: o Describe a brief history of the development of hospice care o Describe the hospice philosophy of care o Describe the referral process o Describe hospice services o Describe reimbursement
Hospice & Palliative Care
 Patient-centered Medical Neighborhood Hospice & Palliative Care Our Hospice of South Central Indiana 2626 East 17th Street Columbus, IN 47201 812-314-8089 Schneck Medical Center Hospice & Palliative Care
Patient-centered Medical Neighborhood Hospice & Palliative Care Our Hospice of South Central Indiana 2626 East 17th Street Columbus, IN 47201 812-314-8089 Schneck Medical Center Hospice & Palliative Care
Palliative Care, Hospice, and the Medical Home. Rob Stone MD Director, Palliative Care Indiana Health Bloomington
 Palliative Care, Hospice, and the Medical Home Rob Stone MD Director, Palliative Care Indiana Health Bloomington The Patient Centered Medical Home (1) A personal physician (2) Physician-directed medical
Palliative Care, Hospice, and the Medical Home Rob Stone MD Director, Palliative Care Indiana Health Bloomington The Patient Centered Medical Home (1) A personal physician (2) Physician-directed medical
Clinical Policy: Hospice Services Reference Number: PA.CP.MP.54
 Clinical Policy: Reference Number: PA.CP.MP.54 Effective Date: 01/18 Last Review Date: 10/17 Coding Implications Revision Log Description Medical necessity for hospice services. Policy It is the policy
Clinical Policy: Reference Number: PA.CP.MP.54 Effective Date: 01/18 Last Review Date: 10/17 Coding Implications Revision Log Description Medical necessity for hospice services. Policy It is the policy
A Quick Talk About Hospice As a Local Community Resource
 A Quick Talk About Hospice As a Local Community Resource 1 Agenda A Very Brief Overview of Hospice Care Your Local Hospice as a Greif & Bereavement Resource 2 David Stone, LCSW, ACSW, CAE Chief Executive
A Quick Talk About Hospice As a Local Community Resource 1 Agenda A Very Brief Overview of Hospice Care Your Local Hospice as a Greif & Bereavement Resource 2 David Stone, LCSW, ACSW, CAE Chief Executive
Palliative Care: Improving quality of life when you re seriously ill.
 Palliative Care The Relief You Need When You re Experiencing the Symptoms of Serious Illness Palliative Care: Improving quality of life when you re seriously ill. Dealing with the symptoms of any painful
Palliative Care The Relief You Need When You re Experiencing the Symptoms of Serious Illness Palliative Care: Improving quality of life when you re seriously ill. Dealing with the symptoms of any painful
5/3/2012 PRESENTATION GOALS RESPIRATORY THERAPISTS ROLE IN END OF LIFE CARE FOR THE PULMONARY PATIENT
 RESPIRATORY THERAPISTS ROLE IN END OF LIFE CARE FOR THE PULMONARY PATIENT Presented by Carrie Black Bourassa, LRT, RRT PRESENTATION GOALS Define palliative care Define hospice care Discuss pulmonary hospice
RESPIRATORY THERAPISTS ROLE IN END OF LIFE CARE FOR THE PULMONARY PATIENT Presented by Carrie Black Bourassa, LRT, RRT PRESENTATION GOALS Define palliative care Define hospice care Discuss pulmonary hospice
Palliative Care for Older Adults in the United States
 Palliative Care for Older Adults in the United States Nathan Goldstein, MD Associate Professor Hertzberg Palliative Care Institute Brookdale Department of Geriatrics and Palliative Medicine Icahn School
Palliative Care for Older Adults in the United States Nathan Goldstein, MD Associate Professor Hertzberg Palliative Care Institute Brookdale Department of Geriatrics and Palliative Medicine Icahn School
Department of Health Care Services SB 1004 Medi-Cal Palliative Care Policy September 1, 2016 Update
 Department of Health Care Services SB 1004 Medi-Cal Palliative Care Policy September 1, 2016 Update This document provides an update on the Department of Health Care Services (DHCS) Medi-Cal palliative
Department of Health Care Services SB 1004 Medi-Cal Palliative Care Policy September 1, 2016 Update This document provides an update on the Department of Health Care Services (DHCS) Medi-Cal palliative
Road Blocks in Non-Cancer Palliative Care Obstacles observed from outpatient non-cancer palliative practice.
 Road Blocks in Non-Cancer Palliative Care Obstacles observed from outpatient non-cancer palliative practice. 25th Annual Palliative Education and Research Days, West Edmonton Mall. Edmonton. 2014 Amanda
Road Blocks in Non-Cancer Palliative Care Obstacles observed from outpatient non-cancer palliative practice. 25th Annual Palliative Education and Research Days, West Edmonton Mall. Edmonton. 2014 Amanda
There Is Something More We Can Do: An Introduction to Hospice and Palliative Care
 There Is Something More We Can Do: An Introduction to Hospice and Palliative Care presented to the Washington Patient Safety Coalition July 28, 2010 Hope Wechkin, MD Medical Director Evergreen Hospice
There Is Something More We Can Do: An Introduction to Hospice and Palliative Care presented to the Washington Patient Safety Coalition July 28, 2010 Hope Wechkin, MD Medical Director Evergreen Hospice
James W. Castillo II, MD Medical Director of the Palliative Care Consultation Service Valley Baptist Health System
 End of Life Issues in Stroke James W. Castillo II, MD Medical Director of the Palliative Care Consultation Service Valley Baptist Health System Conflict Disclosure Information James W. Castillo II, MD
End of Life Issues in Stroke James W. Castillo II, MD Medical Director of the Palliative Care Consultation Service Valley Baptist Health System Conflict Disclosure Information James W. Castillo II, MD
Transitions Guidelines: Chronic Illness Management. Revised 2016
 Transitions Guidelines: Chronic Illness Management Revised 2016 1 Table of Contents Introduction Transitions Program Pillars General Principles Regarding Admission Cancer Cirrhosis Congestive Heart Failure
Transitions Guidelines: Chronic Illness Management Revised 2016 1 Table of Contents Introduction Transitions Program Pillars General Principles Regarding Admission Cancer Cirrhosis Congestive Heart Failure
Palliative Care and Hospice. University of Illinois at Chicago College of Nursing
 Palliative Care and Hospice University of Illinois at Chicago College of Nursing 1 Learning Objectives Upon completion of this module, participants will be better able to: 1. Describe Palliative Care 2.
Palliative Care and Hospice University of Illinois at Chicago College of Nursing 1 Learning Objectives Upon completion of this module, participants will be better able to: 1. Describe Palliative Care 2.
Table of Contents: Amyotrophic Lateral Sclerosis (ALS)
") Guidelines for Hospice Admission Amyotrophic Lateral Sclerosis (ALS) Cancer Cerebral Vascular Accident / Stroke or Coma Dementia / Alzheimer s Failure to Thrive Adults Heart Disease / CHF HIV Disease Huntington
Guidelines for Hospice Admission Amyotrophic Lateral Sclerosis (ALS) Cancer Cerebral Vascular Accident / Stroke or Coma Dementia / Alzheimer s Failure to Thrive Adults Heart Disease / CHF HIV Disease Huntington
Opioid Pearls and Acute Pain Management
 Opioid Pearls and Acute Pain Management Jeanie Youngwerth, MD University of Colorado Denver Assistant Professor of Medicine, Hospitalist Associate Director, Colorado Palliative Medicine Fellowship Program
Opioid Pearls and Acute Pain Management Jeanie Youngwerth, MD University of Colorado Denver Assistant Professor of Medicine, Hospitalist Associate Director, Colorado Palliative Medicine Fellowship Program
12/6/2016. Objective PALLIATIVE CARE IN THE NURSING HOME. Medical Care in the US. Palliative Care
 Objective PALLIATIVE CARE IN THE NURSING HOME Deborah Morris, M.D., M.H.S. Assistant Professor of Medicine The Glennan Center for Geriatrics and Gerontology Eastern Virginia Medical School Describe program
Objective PALLIATIVE CARE IN THE NURSING HOME Deborah Morris, M.D., M.H.S. Assistant Professor of Medicine The Glennan Center for Geriatrics and Gerontology Eastern Virginia Medical School Describe program
Palliative Care & Hospice
 Palliative Care & Hospice Kenneth Brummel-Smith, M.D. Charlotte Edwards Maguire Professor, Department of Geriatrics Florida State University College of Medicine 1 Diane Meier, MD Director, Center to Advance
Palliative Care & Hospice Kenneth Brummel-Smith, M.D. Charlotte Edwards Maguire Professor, Department of Geriatrics Florida State University College of Medicine 1 Diane Meier, MD Director, Center to Advance
Palliative Care for Primary Care Providers QUYNH BUI, MD MPH DECEMBER 2015
 Palliative Care for Primary Care Providers QUYNH BUI, MD MPH DECEMBER 2015 Objectives Define palliative care and primary palliative care Describe the rationale for providing primary palliative care in
Palliative Care for Primary Care Providers QUYNH BUI, MD MPH DECEMBER 2015 Objectives Define palliative care and primary palliative care Describe the rationale for providing primary palliative care in
So let s go through each disease then and understand some of the established prognostic factors starting with COPD.
 Okay, I am Dr. David Hui from the Department of Palliative Care from The University of Texas MD Anderson Cancer Center and we are going to talk about Prognostication in Advanced Diseases, Part II. So in
Okay, I am Dr. David Hui from the Department of Palliative Care from The University of Texas MD Anderson Cancer Center and we are going to talk about Prognostication in Advanced Diseases, Part II. So in
Pain Management in Older Adults. Mary Shelkey, PhD, ARNP
 Pain Management in Older Adults Mary Shelkey, PhD, ARNP Cause of Death/ Demographic and Social Trends Early 1900s Current Medicine's Focus Comfort Cure Cause of Death Infectious Diseases/ Communicable
Pain Management in Older Adults Mary Shelkey, PhD, ARNP Cause of Death/ Demographic and Social Trends Early 1900s Current Medicine's Focus Comfort Cure Cause of Death Infectious Diseases/ Communicable
Course Handouts & Post Test
 End Stage Liver Disease (ESLD) End Stage Renal Disease (ESRD) Disease Trajectory and Hospice Eligibility Terri Maxwell PhD, APRN VP, Strategic Initiatives Weatherbee Resources Inc. & Hospice Education
End Stage Liver Disease (ESLD) End Stage Renal Disease (ESRD) Disease Trajectory and Hospice Eligibility Terri Maxwell PhD, APRN VP, Strategic Initiatives Weatherbee Resources Inc. & Hospice Education
Advocate Health Care Palliative Care Service Line
 Advocate Health Care Palliative Care Service Line Making the case for Palliative Care Approximately 90 million Americans are living with serious and life-threatening illness, and this number is expected
Advocate Health Care Palliative Care Service Line Making the case for Palliative Care Approximately 90 million Americans are living with serious and life-threatening illness, and this number is expected
Objectives. End-of-Life Exercise. Palliative Care Can Help Patients and Decrease 30-Day Hospital Readmissions.
 Palliative Care Can Help Patients and Decrease 30-Day Hospital Readmissions. Objectives Describe how palliative care meets the needs of the patient and family. Discuss how out-patient palliative care can
Palliative Care Can Help Patients and Decrease 30-Day Hospital Readmissions. Objectives Describe how palliative care meets the needs of the patient and family. Discuss how out-patient palliative care can
the sum of our parts. More than HOSPICE of the PIEDMONT
 More than the sum of our parts. HOSPICE of the PIEDMONT Hospice in-home care Hospice Home at high point grief counseling center kids path CARE CONNECTION Understanding your healthcare choices and talking
More than the sum of our parts. HOSPICE of the PIEDMONT Hospice in-home care Hospice Home at high point grief counseling center kids path CARE CONNECTION Understanding your healthcare choices and talking
Brought to you by the Massachusetts Medical Society and its Committee on Geriatric Medicine
 Brought to you by the Massachusetts Medical Society and its Committee on Geriatric Medicine What is palliative care? Care focused on helping support and guide patients who have life limiting and serious
Brought to you by the Massachusetts Medical Society and its Committee on Geriatric Medicine What is palliative care? Care focused on helping support and guide patients who have life limiting and serious
Hospice and Palliative Care An Essential Component of the Aging Services Network
 Hospice and Palliative Care An Essential Component of the Aging Services Network Howard Tuch, MD, MS American Academy of Hospice and Palliative Medicine Physician Advocate, American Academy of Hospice
Hospice and Palliative Care An Essential Component of the Aging Services Network Howard Tuch, MD, MS American Academy of Hospice and Palliative Medicine Physician Advocate, American Academy of Hospice
Analgesics: Management of Pain In the Elderly Handout Package
 Analgesics: Management of Pain In the Elderly Handout Package Analgesics: Management of Pain in the Elderly Each patient or resident and their pain problem is unique. A complete assessment should be performed
Analgesics: Management of Pain In the Elderly Handout Package Analgesics: Management of Pain in the Elderly Each patient or resident and their pain problem is unique. A complete assessment should be performed
PART one. The Palliative Care Spectrum: Providing Care Across Settings
 PART one The Palliative Care Spectrum: Providing Care Across Settings Chapter 1 An Introduction to Palliative Pharmacy Care Jennifer M. Strickland To palliate means to alleviate. Palliative care, as the
PART one The Palliative Care Spectrum: Providing Care Across Settings Chapter 1 An Introduction to Palliative Pharmacy Care Jennifer M. Strickland To palliate means to alleviate. Palliative care, as the
Understanding Hospice, Palliative Care and of-life Issues
 Understanding Hospice, Palliative Care and End-of of-life Issues Huntington's Disease Society of America June 2009 Roseanne Berry, MS, RN RBC Consulting, LLC roseanne@rbcconsultingllc.com The information
Understanding Hospice, Palliative Care and End-of of-life Issues Huntington's Disease Society of America June 2009 Roseanne Berry, MS, RN RBC Consulting, LLC roseanne@rbcconsultingllc.com The information
Clinical Policy: Hospice Services Reference Number: CP.MP.54
 Clinical Policy: Reference Number: CP.MP.54 Effective Date: 05/13 Last Review Date: 07/16 Coding Implications Revision Log See Important Reminder at the end of this policy for important regulatory and
Clinical Policy: Reference Number: CP.MP.54 Effective Date: 05/13 Last Review Date: 07/16 Coding Implications Revision Log See Important Reminder at the end of this policy for important regulatory and
End of Life Care Communication and Advance Illness Care Planning. Gideon Sughrue MD May 18, 2013
 End of Life Care Communication and Advance Illness Care Planning Gideon Sughrue MD May 18, 2013 Objectives End of life Care Communication Describe Palliative Care Place in therapy What is hospice? What
End of Life Care Communication and Advance Illness Care Planning Gideon Sughrue MD May 18, 2013 Objectives End of life Care Communication Describe Palliative Care Place in therapy What is hospice? What
Delivering personalised care to end of life patients. Jane Naismith Nurse Consultant in Palliative care St Joseph s Hospice London
 Delivering personalised care to end of life patients Jane Naismith Nurse Consultant in Palliative care St Joseph s Hospice London Over View This session will cover Supporting patients with long term conditions
Delivering personalised care to end of life patients Jane Naismith Nurse Consultant in Palliative care St Joseph s Hospice London Over View This session will cover Supporting patients with long term conditions
Frequently Asked Questions About Dementia
 Frequently Asked Questions About Dementia Disclaimer This is general information developed by The Ottawa Hospital. It is not intended to replace the advice of a qualified healthcare provider. Please consult
Frequently Asked Questions About Dementia Disclaimer This is general information developed by The Ottawa Hospital. It is not intended to replace the advice of a qualified healthcare provider. Please consult
HOSPICE 101. Another choice for patients facing a terminal prognosis. De Anna Looper, RN, CHPN, CHPCA. Carrefour Associates L.L.C.
 HOSPICE 101 Another choice for patients facing a terminal prognosis. De Anna Looper, RN, CHPN, CHPCA Senior Vice President of Clinical Operations Carrefour Associates L.L.C. HOSPICE 101 Patients and their
HOSPICE 101 Another choice for patients facing a terminal prognosis. De Anna Looper, RN, CHPN, CHPCA Senior Vice President of Clinical Operations Carrefour Associates L.L.C. HOSPICE 101 Patients and their
Quality of Life (F309 End of Life) Surveyor Train the Trainer: Interpretive Guidance Investigative Protocol
 Surveyor Train the Trainer: Interpretive Guidance Investigative Protocol") 483.25 Quality of Life (F309 End of Life) Surveyor Train the Trainer: Interpretive Guidance Investigative Protocol 2 483.25 End of Life Each resident must receive and the facility must provide the necessary
483.25 Quality of Life (F309 End of Life) Surveyor Train the Trainer: Interpretive Guidance Investigative Protocol 2 483.25 End of Life Each resident must receive and the facility must provide the necessary
What You Need To Know About Palliative Care. Natalie Wu Moy, LCSW, MSPA RUHS Medical Center Hospital Social Services Director
 What You Need To Know About Palliative Care Natalie Wu Moy, LCSW, MSPA RUHS Medical Center Hospital Social Services Director None of the faculty, planners, speakers, providers, nor CME committee members
What You Need To Know About Palliative Care Natalie Wu Moy, LCSW, MSPA RUHS Medical Center Hospital Social Services Director None of the faculty, planners, speakers, providers, nor CME committee members
HPS ALLIANCE MEMBERS ONLY HOSPICE WEBINAR SERIES
 HPS ALLIANCE MEMBERS ONLY HOSPICE WEBINAR SERIES - 2019 PRESENTER(S): LESLIE HEAGY, RN, COS-C & MELINDA A. GABOURY, COS-C Documenting to support the Hospice Terminal Prognosis February 15, 2019 DOCUMENTING
HPS ALLIANCE MEMBERS ONLY HOSPICE WEBINAR SERIES - 2019 PRESENTER(S): LESLIE HEAGY, RN, COS-C & MELINDA A. GABOURY, COS-C Documenting to support the Hospice Terminal Prognosis February 15, 2019 DOCUMENTING
Palliative Care and End of Life Care
 Palliative Care and End of Life Care 8/2012 Palliative Care Palliative care is specialized medical care for people with serious illness. This type of care is focused on providing patients with relief from
Palliative Care and End of Life Care 8/2012 Palliative Care Palliative care is specialized medical care for people with serious illness. This type of care is focused on providing patients with relief from
The Changing Landscape of Palliative Care
 The Changing Landscape of Palliative Care KAHPC 17th Annual Conference August 2015 Brian Jones Joe Rotella Elizabeth Wessels Turner West Kay Williams Why Home-based Palliative Care? Turner West, MPH, MTS
The Changing Landscape of Palliative Care KAHPC 17th Annual Conference August 2015 Brian Jones Joe Rotella Elizabeth Wessels Turner West Kay Williams Why Home-based Palliative Care? Turner West, MPH, MTS
Home Based Palliative Care Across The Age Spectrum
 Home Based Palliative Care Across The Age Spectrum Lessons learned in beginning development 2018 New England Home Health & Hospice Conference and Trade Show April 25, 2018 Greg Burns, BSN, RN, CHPPN MHCAH
Home Based Palliative Care Across The Age Spectrum Lessons learned in beginning development 2018 New England Home Health & Hospice Conference and Trade Show April 25, 2018 Greg Burns, BSN, RN, CHPPN MHCAH
Improving Health, Enriching Life. Pain Management. Altru HEALTH SYSTEM
 Improving Health, Enriching Life altru.org Pain Management Altru HEALTH SYSTEM There are many different causes and kinds of pain. Pain can be caused by injury, illness, sickness, disease or surgery. Treating
Improving Health, Enriching Life altru.org Pain Management Altru HEALTH SYSTEM There are many different causes and kinds of pain. Pain can be caused by injury, illness, sickness, disease or surgery. Treating
Palliative Care in the ED:
 Palliative Care in the ED: Don t Just Do Something Stand There Eric Isaacs, MD, FACEP Attending Physician, San Francisco General Hospital and Trauma Center Professor of Emergency Medicine, University of
Palliative Care in the ED: Don t Just Do Something Stand There Eric Isaacs, MD, FACEP Attending Physician, San Francisco General Hospital and Trauma Center Professor of Emergency Medicine, University of
Learning Goals: REMAP: Discussing Goals of Care. Reframe. 2. Expect emotion: respond empathically. 2. Expect emotion: respond empathically
 Practicing patient centered medicine in the 4th quarter Bob Arnold MD 2016 Learning Goals: To define the difference between goals and strategy To describe a goal focused method of talking with patients
Practicing patient centered medicine in the 4th quarter Bob Arnold MD 2016 Learning Goals: To define the difference between goals and strategy To describe a goal focused method of talking with patients
Exploring the Benefits of Both Palliative and Hospice Care
 Exploring the Benefits of Both Palliative and Hospice Care David Mandelbaum, M.D. Director, Palliative Care Services Co-Medical Director, Hospice Services Franciscan Health, Indianapolis, Mooresville,
Exploring the Benefits of Both Palliative and Hospice Care David Mandelbaum, M.D. Director, Palliative Care Services Co-Medical Director, Hospice Services Franciscan Health, Indianapolis, Mooresville,
Palliative Care in the Community Setting. David Mandelbaum, MD Melissa Rockhill, MSN, GNP-BC Lorie Hacker, MSN, NP-C, CNE
 Palliative Care in the Community Setting David Mandelbaum, MD Melissa Rockhill, MSN, GNP-BC Lorie Hacker, MSN, NP-C, CNE Objectives 1. Discuss the framework for building a palliative care program in the
Palliative Care in the Community Setting David Mandelbaum, MD Melissa Rockhill, MSN, GNP-BC Lorie Hacker, MSN, NP-C, CNE Objectives 1. Discuss the framework for building a palliative care program in the
Preventing harmful treatment
 Preventing harmful treatment How can Palliative Care prevent patients receiving overzealous or futile treatment? Antwerp, November 2010 Prof Scott A Murray, St Columba s Hospice Chair of Primary Palliative
Preventing harmful treatment How can Palliative Care prevent patients receiving overzealous or futile treatment? Antwerp, November 2010 Prof Scott A Murray, St Columba s Hospice Chair of Primary Palliative
4/2/2015. Palliative Care: Myths vs. Reality in the New Era of Healthcare. Purpose. Objectives. Session W38 April 29, Dr. Scott A.
 Palliative Care: Myths vs. Reality in the New Era of Healthcare Dr. Scott A. Paxton, DO Session W38 April 29, 2015 Purpose The participant will learn how palliative medical care services need to be explored
Palliative Care: Myths vs. Reality in the New Era of Healthcare Dr. Scott A. Paxton, DO Session W38 April 29, 2015 Purpose The participant will learn how palliative medical care services need to be explored
Guideline for Estimating Length of Survival in Palliative Patients
 http://pal 11 ative. into Cornelius Woelk MD, CCFP Medical Director of Palliative Care Regional Health Authority - Central Manitoba 385 Main Street Winkler, Manitoba, Canada R6W 1J2 Ph: 204-325-4312 Fax:
http://pal 11 ative. into Cornelius Woelk MD, CCFP Medical Director of Palliative Care Regional Health Authority - Central Manitoba 385 Main Street Winkler, Manitoba, Canada R6W 1J2 Ph: 204-325-4312 Fax:
PALLIATIVE CARE IN NEW YORK STATE
 Collaborative for Palliative Care In collaboration with its partners End of Life Choices New York Finger Lakes Geriatric Education Center at the University of Rochester COLLABORATIVE FOR PALLIATIVE CARE
Collaborative for Palliative Care In collaboration with its partners End of Life Choices New York Finger Lakes Geriatric Education Center at the University of Rochester COLLABORATIVE FOR PALLIATIVE CARE
10 mg hydrocodone equals how much oxycodone
 Cari untuk: Cari Cari 10 mg hydrocodone equals how much oxycodone Posts about dilaudid 8 vs oxycodone 30 written by buyprescriptionmedication. Can you help me with the conversion of Oxycodone IR (5mg tab)
Cari untuk: Cari Cari 10 mg hydrocodone equals how much oxycodone Posts about dilaudid 8 vs oxycodone 30 written by buyprescriptionmedication. Can you help me with the conversion of Oxycodone IR (5mg tab)
The Role of Palliative Care in the Management of Advanced Heart Failure
 Disclosure The Role of Palliative Care in the Management of Advanced Heart Failure I have no conflict of interest to disclose. Darrell Craig MD Medical Director, Palliative Care Services St. Joseph Mercy
Disclosure The Role of Palliative Care in the Management of Advanced Heart Failure I have no conflict of interest to disclose. Darrell Craig MD Medical Director, Palliative Care Services St. Joseph Mercy
DEFINITIONS. Generalist. e Palliative Care. Specialist. Palliative Care. Palliative care. Conceptual Shift for Palliative Care. Primary care. Old.
 DEFINITIONS Palliative Primary Palliative (
DEFINITIONS Palliative Primary Palliative (
Identify essential primary palliative care (PPC) communication skills that every provider needs AND clinical triggers for PPC conversations
 communication skills that every provider needs AND clinical triggers for PPC conversations") Identify essential primary palliative care (PPC) communication skills that every provider needs AND clinical triggers for PPC conversations Esmé Finlay, MD Division of Palliative Medicine University of
Identify essential primary palliative care (PPC) communication skills that every provider needs AND clinical triggers for PPC conversations Esmé Finlay, MD Division of Palliative Medicine University of
Changing the Face of Palliative Care in Oncology Practice
 Changing the Face of Palliative Care in Oncology Practice Karin Porter-Williamson MD Associate Professor of Medicine Medical Director Palliative Care Services KU Hospital Amy Velasquez RN BSN OCN Allen
Changing the Face of Palliative Care in Oncology Practice Karin Porter-Williamson MD Associate Professor of Medicine Medical Director Palliative Care Services KU Hospital Amy Velasquez RN BSN OCN Allen
Chapter 6. Hospice: A Team Approach to Care
 Chapter 6 Hospice: A Team Approach to Care Chapter 6: Hospice: A Team Approach to Care Comfort, Respect and Dignity in Dying Hospice care provides patients and family members with hope, comfort, respect,
Chapter 6 Hospice: A Team Approach to Care Chapter 6: Hospice: A Team Approach to Care Comfort, Respect and Dignity in Dying Hospice care provides patients and family members with hope, comfort, respect,
Symptoms Assess symptoms and needs across all domains. Screen using Edmonton Symptom Assessment System (ESAS) for: Pain Nausea Depression
 for: Pain Nausea Depression") A Palliative Care Approach for Primary Care Integrating a palliative care approach earlier in the disease trajectory improves the quality of living and dying, and relieves suffering for patients and families
A Palliative Care Approach for Primary Care Integrating a palliative care approach earlier in the disease trajectory improves the quality of living and dying, and relieves suffering for patients and families
Relatedness *, Terminal Prognosis and Multiple Diagnoses
 Relatedness *, Terminal Prognosis and Multiple Diagnoses *Is Relatedness a word? John C. Tangeman MD FACP The Center for Hospice and Palliative Care Buffalo, New York The Good ol Days Single Hospice Diagnosis
Relatedness *, Terminal Prognosis and Multiple Diagnoses *Is Relatedness a word? John C. Tangeman MD FACP The Center for Hospice and Palliative Care Buffalo, New York The Good ol Days Single Hospice Diagnosis
Chronic Hepatic Disease
 Chronic Hepatic Disease 10 th Leading Cause of Death Liver Functions Energy Metabolism Protein Synthesis Solubilization, Transport, and Storage Protects and Clears drugs, damaged cells Causes of Liver
Chronic Hepatic Disease 10 th Leading Cause of Death Liver Functions Energy Metabolism Protein Synthesis Solubilization, Transport, and Storage Protects and Clears drugs, damaged cells Causes of Liver
Improving End-of-Life Cardiac Care Case Studies. Alan T. Kono, MD Associate Professor of Medicine DHMC & Geisel School of Medicine
 Improving End-of-Life Cardiac Care Case Studies Alan T. Kono, MD Associate Professor of Medicine DHMC & Geisel School of Medicine Palliative Care provides relief from pain and other distressing symptoms
Improving End-of-Life Cardiac Care Case Studies Alan T. Kono, MD Associate Professor of Medicine DHMC & Geisel School of Medicine Palliative Care provides relief from pain and other distressing symptoms
Pain and the MGH Promise
 Pain is an unpleasant sensory & emotional experience associated with actual or potential tissue damage or described in terms of such damage Our promise to patients we will always: Work as a team to evaluate,
Pain is an unpleasant sensory & emotional experience associated with actual or potential tissue damage or described in terms of such damage Our promise to patients we will always: Work as a team to evaluate,
TRAJECTORY OF ILLNESS IN END OF LIFE CARE
 TRAJECTORY OF ILLNESS IN END OF LIFE CARE By Dr Helen Fryer OBJECTIVES To be aware of the three commonest trajectories of decline in the UK To understand the challenges faced in delivering effective Palliative
TRAJECTORY OF ILLNESS IN END OF LIFE CARE By Dr Helen Fryer OBJECTIVES To be aware of the three commonest trajectories of decline in the UK To understand the challenges faced in delivering effective Palliative
Palliative Care Impact Survey
 September 2018 Contents Introduction...3 Headlines...3 Approach...4 Findings...4 Which guideline are used...4 How and where the guidelines are used...6 Alternative sources of information...7 Use of the
September 2018 Contents Introduction...3 Headlines...3 Approach...4 Findings...4 Which guideline are used...4 How and where the guidelines are used...6 Alternative sources of information...7 Use of the
A Population Health Approach to Palliative Care
 A Population Health Approach to Palliative Care Steven Pantilat, MD Professor of Medicine Kates-Burnard and Hellman Distinguished Professor in Palliative Care Director, and Palliative Care Quality Network
A Population Health Approach to Palliative Care Steven Pantilat, MD Professor of Medicine Kates-Burnard and Hellman Distinguished Professor in Palliative Care Director, and Palliative Care Quality Network
Long-Acting Opioid Analgesics
 Market DC Long-Acting Opioid Analgesics Override(s) Prior Authorization Step Therapy Quantity Limit Approval Duration Initial request: 3 months Maintenance Therapy: Additional prior authorization required
Market DC Long-Acting Opioid Analgesics Override(s) Prior Authorization Step Therapy Quantity Limit Approval Duration Initial request: 3 months Maintenance Therapy: Additional prior authorization required
PAIN MANAGEMENT PGY-1. Aaron D. Storms, MD Carin van Zyl, MD Adult and Pediatric Palliative Care, LAC+USC Keck School of Medicine of USC
 PAIN MANAGEMENT PGY-1 Aaron D. Storms, MD Carin van Zyl, MD Adult and Pediatric Palliative Care, LAC+USC Keck School of Medicine of USC Perception Matters A builder aged 29 came to the accident and emergency
PAIN MANAGEMENT PGY-1 Aaron D. Storms, MD Carin van Zyl, MD Adult and Pediatric Palliative Care, LAC+USC Keck School of Medicine of USC Perception Matters A builder aged 29 came to the accident and emergency
Opioid Rotation. Dr Bruno Gagnon, M.D., M.Sc.
 Opioid Rotation Dr Bruno Gagnon, M.D., M.Sc. Associate Professor Department of Family Medicine and Emergency Medicine, Faculty of Medicine, Université Laval Consultant in Palliative Medicine CHU de Québec-Université
Opioid Rotation Dr Bruno Gagnon, M.D., M.Sc. Associate Professor Department of Family Medicine and Emergency Medicine, Faculty of Medicine, Université Laval Consultant in Palliative Medicine CHU de Québec-Université
Cambia Palliative Care Metrics: Where are we and where are we going?
 Cambia Palliative Care Metrics: Where are we and where are we going? J. Randall Curtis, MD, MPH Director, Cambia Palliative Care Center of Excellence www.uwpalliativecarecenter.com Overview of System-Wide
Cambia Palliative Care Metrics: Where are we and where are we going? J. Randall Curtis, MD, MPH Director, Cambia Palliative Care Center of Excellence www.uwpalliativecarecenter.com Overview of System-Wide
Renal Care and Liver Disease: Disease Trajectory and Hospice Eligibility
 Renal Care and Liver Disease: Disease Trajectory and Hospice Eligibility Terri L. Maxwell PhD, APRN VP, Strategic Initiatives Weatherbee Resources/HEN Course Materials & Disclosure Course materials including
Renal Care and Liver Disease: Disease Trajectory and Hospice Eligibility Terri L. Maxwell PhD, APRN VP, Strategic Initiatives Weatherbee Resources/HEN Course Materials & Disclosure Course materials including
END OF LIFE ISSUES. 41 st Semi-Annual Family Practice Review Course Lewis Katz School of Medicine at Temple University
 END OF LIFE ISSUES 41 st Semi-Annual Family Practice Review Course Lewis Katz School of Medicine at Temple University Stanley J. Savinese DO FAAHPM HMDC Medical Director VNA Hospice of Philadelphia Co-Director
END OF LIFE ISSUES 41 st Semi-Annual Family Practice Review Course Lewis Katz School of Medicine at Temple University Stanley J. Savinese DO FAAHPM HMDC Medical Director VNA Hospice of Philadelphia Co-Director
Clinical Policy: Hospice Services Reference Number: CA.CP.MP.54
 Clinical Policy: Reference Number: CA.CP.MP.54 Effective Date: 05/13 Last Review Date: 01/18 Coding Implications Revision Log See Important Reminder at the end of this policy for important regulatory and
Clinical Policy: Reference Number: CA.CP.MP.54 Effective Date: 05/13 Last Review Date: 01/18 Coding Implications Revision Log See Important Reminder at the end of this policy for important regulatory and
Hospice Care vs Palliative Care
 Hospice Care vs Palliative Care Easing the burden of illness, Improving quality of life Seasons Hospice and Palliative Care Cheryl Ledesma, FNP-BC Jacklyn Griffin, ACNP-BC Objectives After completing this
Hospice Care vs Palliative Care Easing the burden of illness, Improving quality of life Seasons Hospice and Palliative Care Cheryl Ledesma, FNP-BC Jacklyn Griffin, ACNP-BC Objectives After completing this
INDIANA HEALTH COVERAGE PROGRAMS
 INDIANA HEALTH COVERAGE PROGRAMS PROVIDER CODE TABLES Note: Due to possible changes in Indiana Health Coverage Programs (IHCP) policy or national coding updates, inclusion of a code on the code tables
INDIANA HEALTH COVERAGE PROGRAMS PROVIDER CODE TABLES Note: Due to possible changes in Indiana Health Coverage Programs (IHCP) policy or national coding updates, inclusion of a code on the code tables
Palliative Care: Myths vs. Reality in the New Era of Healthcare
 Palliative Care: Myths vs. Reality in the New Era of Healthcare Presented by: Purpose The participant will learn how palliative medical care services need to be explored as viable options in reducing re-hospitalizations
Palliative Care: Myths vs. Reality in the New Era of Healthcare Presented by: Purpose The participant will learn how palliative medical care services need to be explored as viable options in reducing re-hospitalizations
Community and Mental Health Services. Palliative Care. Criteria and
 Community and Mental Health Services Specialist Palliative Care Service Referral Criteria and Guidance November 2018 Specialist Palliative Care Service Referrals These guidelines cover referrals for patients
Community and Mental Health Services Specialist Palliative Care Service Referral Criteria and Guidance November 2018 Specialist Palliative Care Service Referrals These guidelines cover referrals for patients
National Council on Patient Information and Education
 National Council on Patient Information and Education You are not alone The type of pain that caused your doctor to prescribe a pain medicine for you can make you feel that you are different from everyone
National Council on Patient Information and Education You are not alone The type of pain that caused your doctor to prescribe a pain medicine for you can make you feel that you are different from everyone
Bring Palliative Care Into Your Office. Renee Baird, MSN, FNP-C, CHPN
 Bring Palliative Care Into Your Office Renee Baird, MSN, FNP-C, CHPN Pal-ee-uh-tiv Kair Palliative care is both a philosophy of care and an organized, highly structured system for delivering care. The
Bring Palliative Care Into Your Office Renee Baird, MSN, FNP-C, CHPN Pal-ee-uh-tiv Kair Palliative care is both a philosophy of care and an organized, highly structured system for delivering care. The
WRHA Clinical Practice Guideline: Sedation for Palliative Purposes (SPP)
") WRHA Clinical Practice Guideline: Sedation for Palliative Purposes (SPP) Developed by: WRHA Regional Working Group Mike Harlos MD, CCFP(PC), FCFP Professor and Section Head, Palliative Medicine, University
WRHA Clinical Practice Guideline: Sedation for Palliative Purposes (SPP) Developed by: WRHA Regional Working Group Mike Harlos MD, CCFP(PC), FCFP Professor and Section Head, Palliative Medicine, University