Behaviour Units: Understanding what they can offer Older Patients with Dementia
|
|
|
- Evan Conley
- 6 years ago
- Views:
Transcription

1 Behaviour Units: Understanding what they can offer Older Patients with Dementia David K. Conn Baycrest Centre and University of Toronto 2013 Mount Sinai Geriatrics institute
2
3 Outline Alice s journey continues BPSD in LTC brief overview Definition of Behaviour Support Units Studies of specialized units Optimal elements for success in these units
4 Alice s Journey Despite treatment of her pneumonia and CHF she remained agitated at times with episodic physical aggression towards staff and labile emotions. Symptoms of delirium improved but she did not return to baseline. After another week in hospital arrangements were made for a transfer to a Behaviour Support Unit in a local LTC Home

5 Neuropsychiatric Clusters in Dementia Aggression Agitation Apathy Aggressive resistance Physical aggression Verbal aggression Withdrawn Lack of interest Sad Amotivation Tearful Hopeless Low self-esteem Anxiety Guilt Depression Hallucinations Delusions Misidentifications Walking aimlessly Pacing Trailing Restlessness Repetitive actions Dressing/undressing Sleep disturbance Psychosis Adapted from McShane R. Int Rsychogeriatr 2000, 12(Suppl 1):147-54
6 AD patients with behaviours present (%) Neuropsychiatric Symptoms by Severity of AD 100 Mild (MMSE scores 21 30) Severe (MMSE scores 0 10) Moderate (MMSE scores 11 20) Adapted from Cummings and Back, 1998
7 A total of 74 studies examining the prevalence of psychiatric disorders and psychological symptoms in LTC populations were identified including: 30 studies on prevalence of dementia 9 studies on behavioural symptoms in dementia 26 studies on depression Int Psychogeriatrics, Nov. 2010
8 Prevalence of Dementia 30 studies 13 from N. America 12 from Europe 2 from Middle East 1 from Africa 1 from Asia 1 from Australia/ NZ 16 different diagnostic instruments
9 Range The estimated prevalence of dementia in nursing homes varied between 12.0% (Van den Berg, Spijker et al. 1995) and 95% (Serby, Chou et al. 1987) with a median prevalence of dementia of 58% from all the studies.
10 Prevalence of BPSD A total of 9 studies reporting the prevalence of behavioural symptoms in LTC resident with dementia or cognitive impairment were identified 6 from Europe, 2 from N. America, 1 from Australia
11 Range The prevalence of any behavioural symptom in LTC residents with dementia varied between 38% (Wancata, Benda et al. 2003) and 92% (Brodaty, Draper et al. 2001). The median prevalence of any behaviour symptom in dementia in LTC residents from the 9 studies was 78%.
12 Range. The prevalence of major depression in LTC ranged from 4% (Teresi, Abrams et al. 2001) to 25% (McSweeney and O'Connor 2008) the prevalence of depressive symptoms varied between 29% (McSweeney and O'Connor 2008) to 82% (Lin, Wang et al. 2007).
13 Prevalence of BPSD in Community and Nursing Home (Lyketsos et al, Brodaty et al, 2001) Overall Prevalence Clinically Significant Community (%) Delusions Hallucinations Nursing Home (%) Depressed Mood Aggression / Agitation
14 Possible Etiologies of Aggression / Agitation Caregiver related Environment related Manifestation of a medical disorder r/o pain / discomfort Psychiatric comorbidity Delirium Medication side effects Neurotransmitter changes Cohen-Mansfield J et al. Int Psychogeriatr. 1992;4(2): Mintzer JE, Brawman-Mintzer O. J Clin Psychiatry. 1996;57(7):55-63.
15
) Brodaty et al, MJA, 2003:")
16 Brodaty et al, MJA, in press (2003;178(4)) Brodaty et al, MJA, 2003: 178:

17
18
19
20
21
22 Principles that promote and support mental health for all LTC residents (CCSMH, 2006) individualized, person-centred care; respect for family ties; a biopsychosocial care planning framework; a culture of caring that prioritizes quality of life; a social and physical environment that is responsive to changing needs; a focus on early intervention and prevention as well as treatment; and staff training and development
23
24

25 Behavioural Support System: Essential Elements
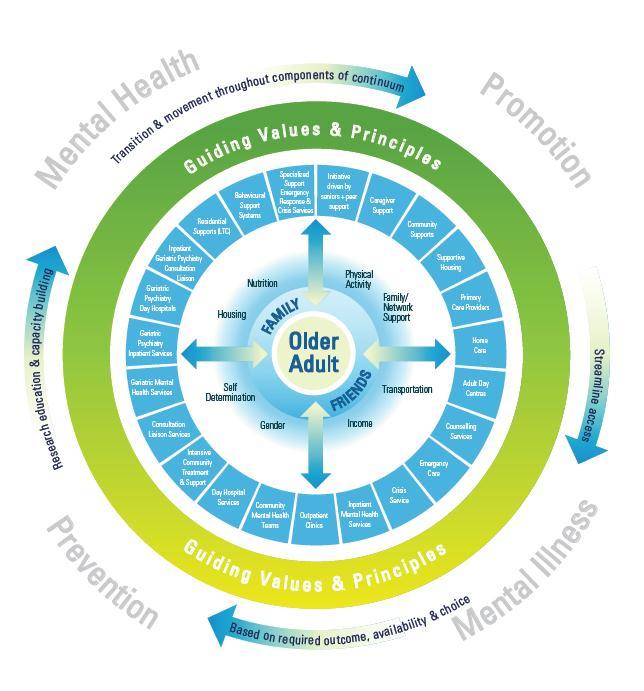
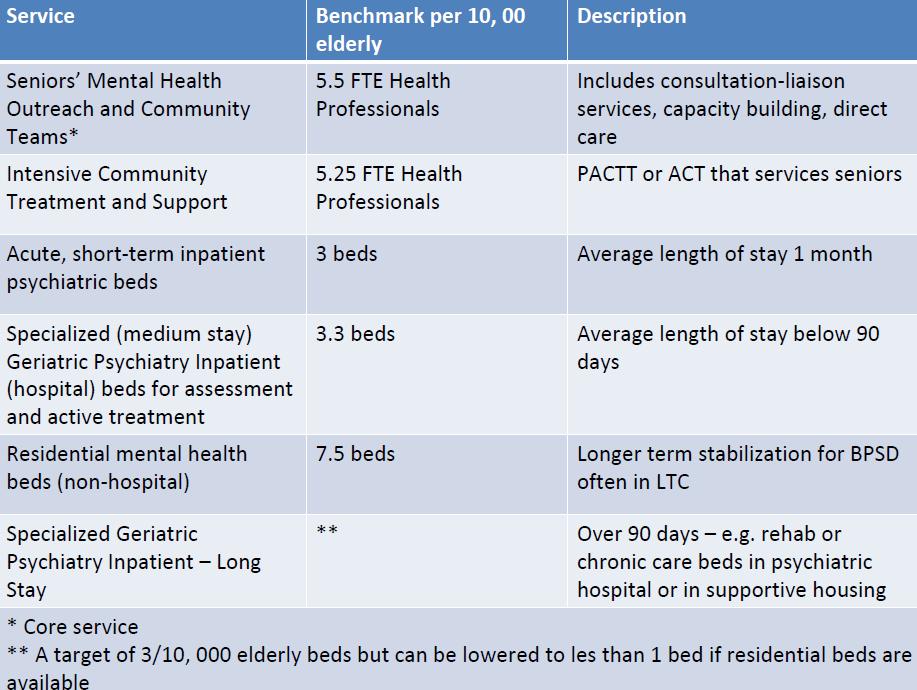
26 Behavioural Support Units (MOHLTC, 2007) Specialized treatment units located in selected LTC homes that focus on the treatment and stabilization of individuals with aggressive behaviours Do not rquire a hospital inpatient unit but they are not ready to return to a normal LTC home environment Transitional - a LHIN resource
27 Behavioural Support Unit (BSU) Recommendations (2007) BSUs be created as a regional resource Staffing ratio of regulated to unregulated ranging from 40:60 to 50:50 rather than 20:80 Staffing levels of allied HPs be increased to include a range of providers. Regular access to pharmacist Maximum of 15 to 20 residents
28 Behavioural Support Unit (BSU) Recommendations - cont. (2007) Support patient choice BSUs should be affiliated with a LTC home or another facility Admissions managed by CCAC in cooperation with PG team Regular priority review of admissions & discharges Highly specific admission & discharge criteria
29 Behavioural Support Unit (BSU) Recommendations - cont. (2007) Residents being transferred to a LTC setting should have assistance from a PG Outreach team BSUs must be funded from outside the current resident classification system Referrals to PG Outreach team mandatory if resident has potential for aggression
30 Longitudinal study comparing residents of SCUs versus those in traditional NHs Nobili et al Alz Dis Assoc Disord (2008) 349 res in 35 SCUs vs. 81 res in 9 NHs Res admitted to SCUs were younger, less cognitively and functionally impaired but had more behavioural problems Over 18 months SCU residents had less hospitalization, less use of physical restraints and had a higher rate of withdrawal from antipsychotics
31 Cross-sectional study of 28 SCUs compared with traditional care in Germany Weyerer et al. Int J Ger Psych (2010) 594 res in SCUs vs. 573 res in usual care After controlling for confounding variables: In SCUs. - More social contact to staff - More involvement in activities - More volunteer involvement - Fewer physical restraints - More use of psychiatrists - Less antipsychotics, more antidepressants
32 Special Care Units & Outcomes: National NH Survey 2004 Luo et al The Gerontologist Residents of SCUs more likely to receive specialized dementia care and behavioural management vs. residents in regular units or in NHs without an SCU. They were less likely to have bed rails, use catheters, more likely to have toilet plans, bladder training Less likely to have pressure ulcers, be hospitalized, or have weight loss More likely to have falls. In general residents in SCUs had better care processes.
33 Are Special Care Units better for individuals with behavioural problems? Cochrane Review 2009, Lai CK et al. No RCTs 4 studies available with extractable data Studies suggested a small improvement in NPI scores favouring SCUs & less use of physical restraints Authors concluded that there is no strong evidence of benefit from a SCU. They suggest the implementation of Best Practices is most important!
34 Principles that promote and support mental health for all LTC residents (CCSMH, 2006) individualized, person-centred care; respect for family ties; a biopsychosocial care planning framework; a culture of caring that prioritizes quality of life; a social and physical environment that is responsive to changing needs; a focus on early intervention and prevention as well as treatment; and staff training and development
35 Environmental design Fleming and Purandare (2010) recently reviewed 57 studies and synthesized the evidence with respect to environmental design in LTC Recommendations Re: - Spaces - Security - Single Rooms - Sight lines - Stimulation - Small, homelike, engage in ADLs, outside spaces

36 CCSMH: Assessment & Detailed Investigation We recommend Core elements of a detailed investigation should include history and physical exam, with follow up laboratory and psychological investigations, investigations of the social and physical environment, and diagnostic tests as indicated by the results of the history and physical exam, and treatment history and response. [C] It is important to consider all contributing factors. Investigation of potentially contributing factors (e.g., delirium, chronic pain) should refer to clinical practice guidelines for these conditions where available. [D]
37
38
39 Assessment Scales The Cohen-Mansfield Agitation Inventory (CMAI) Long Form 2 Assesses frequency of 29 agitated behaviours rated by the caregivers on a 7 point scale The Neuropsychiatric Inventory (NPI) and NPI-NH assesses 12 items: frequency (1-4) multiplied by severity (1-3) delusions hallucinations agitation/aggression depression anxiety elation/euphoria apathy disinhibition irritability aberrant motor beh nighttime beh appetite/eating 2. Cohen-Mansfield J. J Am Geriatr Soc 1986; 34: 722 7
40 Behavioural Symptoms: Psychological and Social Interventions We recommend Social contact interventions should always be considered, especially where the goal is to minimize sensory deprivation and social isolation, provide distraction and physical contact, and induce relaxation. [C] Sensory/relaxation interventions (e.g., music, snoezelen, aromatherapy, bright light) should be considered where the goal is to reduce behavioural symptoms, stimulate the senses and enhance relaxation. [B/D] Consider the need for promoting structured activities that engage the resident. [C] Individualized behaviour therapy should be considered where the goal is to manage behaviour symptoms (e.g., contextually inappropriate, disturbing, disruptive or potentially harmful behaviours). [C]
41 Non-Pharmacological Interventions (Beck & Shue, 1994) Behavioural techniques / staff training Environmental modifications Group programs (e.g. exercise, dancing ) Light Therapy Music Therapy Social Interaction / Psychosocial activities Multimodal Approaches Pet Therapy
42
43
44 Included Studies Total number of studies N=40 Total number of participants: 3,519 Sample size: median 80 (range ) Median age participants: 84 years Gender distribution: 78% female Cognitive impairment: MMSE = 5 10 Study duration: median 12 weeks (range of 1 52 weeks)
45 Efficacy of Interventions 16 of 40 (40%) studies reported statistically significant benefits for nonpharmacological intervention : Staff training N=3 (McCaillion, 1999; Chenoweth, 2009; Testad, 2010) Mental health assessment N= 2 (Rovner, 1996; Cohen- Mansfield, 2007) Psychosocial activities N=2 (Toseland, 1997; Lichtenberg, 2005) Exercise N=3 (Alessi, 1999; Landi, 2005; Williams, 2007) Music N=2 (Sung, 2006; Raglio, 2008) Other sensory stimulation N=4 (Ballard, 2002; van Weert, 2005; Woods, 2005; Hawranik, 2008)

46 Montessori Approach Cameron Camp, Gail Elliot Places emphasis on the environment, including activities designed for each individual s level of ability, based on interests and needs AND provides necessary cueing to support memory loss Emphasis is placed on assigning meaningful roles & routines When fully engaged behavioural challenges are eliminated


47 Memory Boxes Aids in the recollection of details about someone's life. Can prevent anxiety, frustration and agitation. Memory boxes need information about items displayed in the case to support declarative memory loss. Before After

48 Memory Boards: Let s Know our Residents


49 Washrooms (BSU) Contrast: Walls are now a different colour than the items hung on the wall Before After Where is the paper towel dispenser?? Where is the paper towel dispenser?? Contrast


50 Shower Room Where would you prefer to Before shower? After
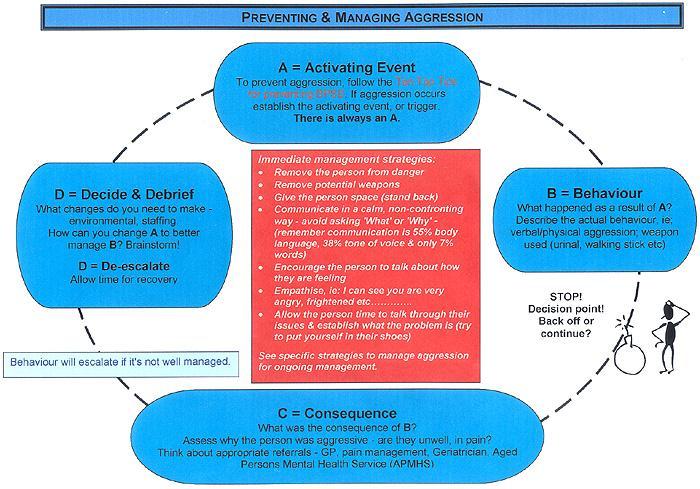
51 Behavioural Management Approach Cognitive Assessment Behavioural Assessment (ABC Analysis) Staff Perceptions Utilize Extinction, Reinforcement, Prompting Staff Stress Innoculation Rewilak, 2001
52
53 Remembering the forgotten: psychotherapy groups for the nursing home resident. Ken Schwartz Int J Group Psychother Oct;57(4): Weekly groups Co-facilitated by social worker from the unit An integrated model utilizing developmental, cognitive-behavioral, and psychodynamic approaches
54
55 Questions to be asked in evaluating any drug use in a NH Avorn & Gurwitz, 1995 What is the target problem being treated? Is the drug necessary? Are nonpharmacologic therapies available? Is this the lowest practical dose? Could discontinuing therapy with a medicine help to reduce symptoms? Does this drug have adverse effects that are more likely to occur in an older pt.? Is this the most cost-effective choice? By what criteria, and at what time, will the effects of therapy be assessed?
56 Good Drugs or Bad Drugs? (more good than harm or more harm than good) Let s Vote re: older adults in LTC Antidepressants Benzodiazepines with a long half life (e.g. diazepam) Benzodiazepines with a short half life (e.g lorazepam) Antipsychotics Cholinesterase Inhibitors (e.g. Aricept)
57
58 Medication Use in 2004 National Nursing Home Survey Participants and Estimates in U.S. Nursing Home Population NNHS Sample Estimates for U.S. Nursing Home Population Total Number Age 65 years 11,940 1,317,292 Any Antidepressant, N (%) 5,567 (46.6) 603,691 (45.8) Any Antipsychotic, N (%) 2,890 (24.2) 324,771 (24.7) Any Benzodiazepine, N (%) 1,498 (12.5) 158,147 (12.0)
59 Medication Use in 2004 National Nursing Home Survey participants: rates of use of cholinesterase inhibitors National Nursing Home Survey (n=5866) U.S Nursing Home Population (N=665,217) Any ChEI No ChEI Any ChEI No ChEI Total Number of Individuals with Dementia (%) 1696* (28.9) 4170 (71.1) 199,296* (30.0) 465,921 (70.0) Total Num Receiving ChEIs (%) Donepezil Rivastigmine Galantamine 1192 (20.3) 237 (4.0) 268 (4.5) ,649 (21.3) 26,986 (4.1) 30,833 (4.6) Seitz et al. JAGS, 2009
60 Mental Health Care System in LTC Facilities Intrinsic Provided by the frontline staff of the facility Extrinsic Mental Health and other professionals (usually visiting consultants or outreach teams)
61
62

63 Quality of the educational input Individual motivation Nature, complexity and acceptability of the proposed change initiative Receptivity of the care environment and its organizational context
64 Conclusions Literature on the effectiveness of Behavioural Support Units / SCUs is sparce. No RCTs. Some studies suggest less use of physical restraints and more optimal use of medications in SCUs vs usual care. Little data on staffing levels. Clear need for significantly higher levels with a full complement of health disciplines. Several models for mental health service provision exist. Clear need for involvement of staff with high levels of expertise. Education & training of staff is essential.
How I Treat Aggression in Outpatients With Dementia. C. Omelan MD, FRCP(C)
") How I Treat Aggression in Outpatients With Dementia C. Omelan MD, FRCP(C) Conflict of Interest I have no potential conflicts of interest to declare Overview Outline the prevalence of aggression Review
How I Treat Aggression in Outpatients With Dementia C. Omelan MD, FRCP(C) Conflict of Interest I have no potential conflicts of interest to declare Overview Outline the prevalence of aggression Review
Across the Spectrum of Dementia. Keys to Understanding Behaviours & Anticipating Needs
 Across the Spectrum of Dementia Keys to Understanding Behaviours & Anticipating Needs Outline Review current predictions for dementia prevalence, & the implications for future needs Discuss retrogenesis
Across the Spectrum of Dementia Keys to Understanding Behaviours & Anticipating Needs Outline Review current predictions for dementia prevalence, & the implications for future needs Discuss retrogenesis
MANAGEMENT OF NEUROPSYCHIATRIC SYMPTOMS OF DEMENTIA
 MANAGEMENT OF NEUROPSYCHIATRIC SYMPTOMS OF DEMENTIA Dr. Dallas Seitz MD PhD FRCPC Associate Professor and Division Chair, Division of Geriatric Psychiatry Department of Psychiatry, Queen s University President,
MANAGEMENT OF NEUROPSYCHIATRIC SYMPTOMS OF DEMENTIA Dr. Dallas Seitz MD PhD FRCPC Associate Professor and Division Chair, Division of Geriatric Psychiatry Department of Psychiatry, Queen s University President,
Recognition and Management of Behavioral Disturbances in Dementia
 Recognition and Management of Behavioral Disturbances in Dementia Danielle Hansen, DO, MS (Med Ed), MHSA INTRODUCTION 80% 90% of patients with dementia develop at least one behavioral disturbances or psychotic
Recognition and Management of Behavioral Disturbances in Dementia Danielle Hansen, DO, MS (Med Ed), MHSA INTRODUCTION 80% 90% of patients with dementia develop at least one behavioral disturbances or psychotic
Psychiatric and Behavioral Symptoms in Alzheimer s and Other Dementias. Aaron H. Kaufman, MD
 Psychiatric and Behavioral Symptoms in Alzheimer s and Other Dementias Aaron H. Kaufman, MD Psychiatric and Behavioral Symptoms in Alzheimer s and Other Dementias Aaron H. Kaufman, M.D. Health Sciences
Psychiatric and Behavioral Symptoms in Alzheimer s and Other Dementias Aaron H. Kaufman, MD Psychiatric and Behavioral Symptoms in Alzheimer s and Other Dementias Aaron H. Kaufman, M.D. Health Sciences
Behavioral and Psychological Symptoms of dementia (BPSD)
") Behavioral and Psychological Symptoms of dementia (BPSD) Chris Collins - Old Age Psychiatrist, Christchurch chris.collins@cdhb.health.nz Approaching BPSD: the right mindset Assessment Non-drug management
Behavioral and Psychological Symptoms of dementia (BPSD) Chris Collins - Old Age Psychiatrist, Christchurch chris.collins@cdhb.health.nz Approaching BPSD: the right mindset Assessment Non-drug management
Optimal Management of Challenging Behaviours in Dementia: An Update on Pharmacologic and Non-Pharmacologic Approaches
 Optimal Management of Challenging Behaviours in Dementia: An Update on Pharmacologic and Non-Pharmacologic Approaches Andrea Iaboni, MD, DPhil, FRCPC Toronto Rehab Institute, UHN Learning objectives Recognize
Optimal Management of Challenging Behaviours in Dementia: An Update on Pharmacologic and Non-Pharmacologic Approaches Andrea Iaboni, MD, DPhil, FRCPC Toronto Rehab Institute, UHN Learning objectives Recognize
Management of the Acutely Agitated Long Term Care Patient
 Management of the Acutely Agitated Long Term Care Patient 80 60 Graying of the Population US Population Over Age 65 Millions of Persons 40 20 0 1900 1920 1940 1960 1980 1990 2010 2030 Year Defining Dementia
Management of the Acutely Agitated Long Term Care Patient 80 60 Graying of the Population US Population Over Age 65 Millions of Persons 40 20 0 1900 1920 1940 1960 1980 1990 2010 2030 Year Defining Dementia
Neuropsychiatric Syndromes
 Neuropsychiatric Syndromes Susan Czapiewski,MD VAHCS December 10, 2015 Dr. Czapiewski has indicated no potential conflict of interest to this presentation. She does intend to discuss the off-label use
Neuropsychiatric Syndromes Susan Czapiewski,MD VAHCS December 10, 2015 Dr. Czapiewski has indicated no potential conflict of interest to this presentation. She does intend to discuss the off-label use
Screening and Management of Behavioral and Psychiatric Symptoms Associated with Dementia
 Screening and Management of Behavioral and Psychiatric Symptoms Associated with Dementia Measure Description Percentage of patients with dementia for whom there was a documented screening* for behavioral
Screening and Management of Behavioral and Psychiatric Symptoms Associated with Dementia Measure Description Percentage of patients with dementia for whom there was a documented screening* for behavioral
Appropriate Use of Psychotropic Medication in the Seniors Population
 Appropriate Use of Psychotropic Medication in the Seniors Population Finding the Right balance David Conn Baycrest & University of Toronto Symposium on Excellence in Aging Care Fredericton, N.B. Sept 25
Appropriate Use of Psychotropic Medication in the Seniors Population Finding the Right balance David Conn Baycrest & University of Toronto Symposium on Excellence in Aging Care Fredericton, N.B. Sept 25
BEHAVIOURAL AND PSYCHOLOGICAL SYMPTOMS IN DEMENTIA
 BEHAVIOURAL AND PSYCHOLOGICAL SYMPTOMS IN DEMENTIA Unmet needs What might be your behavioural response to this experience? Content Definition What are BPSD? Prevalence How common are they? Aetiological
BEHAVIOURAL AND PSYCHOLOGICAL SYMPTOMS IN DEMENTIA Unmet needs What might be your behavioural response to this experience? Content Definition What are BPSD? Prevalence How common are they? Aetiological
October 28, Geriatrics Update Course. Lesley Wiesenfeld, MD, MHCM, FRCPC. Managing BPSD. Geriatric Psychiatrist, Mount Sinai Hospital
 October 28, 2016 Geriatrics Update Course Managing BPSD Lesley Wiesenfeld, MD, MHCM, FRCPC Geriatric Psychiatrist, Mount Sinai Hospital Disclosures ~No Pharmaceutical or Industry Support ~ No Health Without
October 28, 2016 Geriatrics Update Course Managing BPSD Lesley Wiesenfeld, MD, MHCM, FRCPC Geriatric Psychiatrist, Mount Sinai Hospital Disclosures ~No Pharmaceutical or Industry Support ~ No Health Without
Guidelines for the Management of Behavioural and Psychological Symptoms of Dementia (BPSD) Summary document for Primary Care
 Summary document for Primary Care") Guidelines for the Management of Behavioural and Psychological Symptoms of Dementia (BPSD) Summary document for Primary Care Guidelines for the Management of Behavioural and Psychological Symptoms of Dementia
Guidelines for the Management of Behavioural and Psychological Symptoms of Dementia (BPSD) Summary document for Primary Care Guidelines for the Management of Behavioural and Psychological Symptoms of Dementia
BEHAVIORAL PROBLEMS IN DEMENTIA
 BEHAVIORAL PROBLEMS IN DEMENTIA CLINICAL FEATURES Particularly as dementia progresses, psychiatric symptoms may develop that resemble discrete mental disorders such as depression or mania The course and
BEHAVIORAL PROBLEMS IN DEMENTIA CLINICAL FEATURES Particularly as dementia progresses, psychiatric symptoms may develop that resemble discrete mental disorders such as depression or mania The course and
Management of Behavioral Problems in Dementia
 Management of Behavioral Problems in Dementia Ghulam M. Surti, MD Clinical Assistant Professor Department of Psychiatry and Human Behavior Warren Alpert Medical School of Brown University Definition of
Management of Behavioral Problems in Dementia Ghulam M. Surti, MD Clinical Assistant Professor Department of Psychiatry and Human Behavior Warren Alpert Medical School of Brown University Definition of
American Board of Psychiatry and Neurology, Inc. Geriatric Psychiatry Core Competencies Outline
 American Board of Psychiatry and Neurology, Inc. Geriatric Psychiatry Core Competencies Outline I. Geriatric Psychiatry Patient Care and Procedural Skills Core Competencies A. Geriatric psychiatrists shall
American Board of Psychiatry and Neurology, Inc. Geriatric Psychiatry Core Competencies Outline I. Geriatric Psychiatry Patient Care and Procedural Skills Core Competencies A. Geriatric psychiatrists shall
THE BEHAVIOURAL VITAL SIGNS (BVS) TOOL
 TOOL") DID YOU KNOW THE BEHAVIOURAL VITAL SIGNS (BVS) TOOL. Did you know that it is essential to know the target cluster(s)/symptom(s) one is treating to guide and monitor non-pharmacological approaches and pharmacological
DID YOU KNOW THE BEHAVIOURAL VITAL SIGNS (BVS) TOOL. Did you know that it is essential to know the target cluster(s)/symptom(s) one is treating to guide and monitor non-pharmacological approaches and pharmacological
The place for treatments of associated neuropsychiatric and other symptoms
 The place for treatments of associated neuropsychiatric and other symptoms Luca Pani dg@aifa.gov.it London, 25 th November 2014 Workshop on Alzheimer s Disease European Medicines Agency London, UK Public
The place for treatments of associated neuropsychiatric and other symptoms Luca Pani dg@aifa.gov.it London, 25 th November 2014 Workshop on Alzheimer s Disease European Medicines Agency London, UK Public
How Aging and Dementia Effect Resident Behaviors
 How Aging and Dementia Effect Resident Behaviors November 3, 2011 1:00 2:00 PM EST Webinar Presented by: Alfred W. Norwood, BS, MBA Education Arm of the Carmelite Sisters for the Aged and Infirm Webinar
How Aging and Dementia Effect Resident Behaviors November 3, 2011 1:00 2:00 PM EST Webinar Presented by: Alfred W. Norwood, BS, MBA Education Arm of the Carmelite Sisters for the Aged and Infirm Webinar
LTC Research Influencing Practice
 LTC Research Influencing Practice David A. Nace, MD, MPH Division of Geriatric Medicine naceda@upmc.edu PGS Clinical Update April 6, 2017 Conflicts of Interest Dr. Nace does not have any current conflicts
LTC Research Influencing Practice David A. Nace, MD, MPH Division of Geriatric Medicine naceda@upmc.edu PGS Clinical Update April 6, 2017 Conflicts of Interest Dr. Nace does not have any current conflicts
PSYCHOTROPIC SOLUTIONS
 PSYCHOTROPIC SOLUTIONS A proactive approach to antipsychotic medication management A Quality Use of Medicines initiative by Choice Aged Care Copyright 2018 Key Senate Committee Recommendations: All RACF
PSYCHOTROPIC SOLUTIONS A proactive approach to antipsychotic medication management A Quality Use of Medicines initiative by Choice Aged Care Copyright 2018 Key Senate Committee Recommendations: All RACF
Presented by Rengena Chan-Ting, DO, CMD, FACOI Jenna D. Toniatti, PharmD
 Presented by Rengena Chan-Ting, DO, CMD, FACOI Jenna D. Toniatti, PharmD Define BPSD and review the spectrum of associated symptoms Review pharmacologic and non-pharmacologic treatments for BPSD Evaluate
Presented by Rengena Chan-Ting, DO, CMD, FACOI Jenna D. Toniatti, PharmD Define BPSD and review the spectrum of associated symptoms Review pharmacologic and non-pharmacologic treatments for BPSD Evaluate
Responsiveness of the QUALID to Improved Neuropsychiatric Symptoms in Patients with Alzheimer s Disease
 ORIGINAL RESEARCH Responsiveness of the QUALID to Improved Neuropsychiatric Symptoms in Patients with Alzheimer s Disease Hadas Benhabib 1, Krista L. Lanctôt, PhD 1,2,4, Goran M. Eryavec, MD, FRCPC 3,4,
ORIGINAL RESEARCH Responsiveness of the QUALID to Improved Neuropsychiatric Symptoms in Patients with Alzheimer s Disease Hadas Benhabib 1, Krista L. Lanctôt, PhD 1,2,4, Goran M. Eryavec, MD, FRCPC 3,4,
11/11/2016. Disclosures. Natural history of BPSD. Objectives. Assessment of BPSD. Behavioral Management of Persons with Alzheimer s Disease
 Disclosures Behavioral Management of Persons with Alzheimer s Disease Wisconsin Association of Medical Directors November 17, 2016 Art Walaszek, M.D. Professor of Psychiatry UW School of Medicine & Public
Disclosures Behavioral Management of Persons with Alzheimer s Disease Wisconsin Association of Medical Directors November 17, 2016 Art Walaszek, M.D. Professor of Psychiatry UW School of Medicine & Public
QUESTIONNAIRE: Finland
 QUESTIONNAIRE: Finland To put the assessment and management of behavioural disorders into a broader context of social and health policy and services in Finland, some background information is presented.
QUESTIONNAIRE: Finland To put the assessment and management of behavioural disorders into a broader context of social and health policy and services in Finland, some background information is presented.
Dementia and Fall Geriatric Interprofessional Training. Wael Hamade, MD, FAAFP
 Dementia and Fall Geriatric Interprofessional Training Wael Hamade, MD, FAAFP Prevalence of Dementia Age range 65-74 5% % affected 75-84 15-25% 85 and older 36-50% 5.4 Million American have AD Dementia
Dementia and Fall Geriatric Interprofessional Training Wael Hamade, MD, FAAFP Prevalence of Dementia Age range 65-74 5% % affected 75-84 15-25% 85 and older 36-50% 5.4 Million American have AD Dementia
5/17/2017. Conflicts of Interest. Key Takeaways
 Antipsychotic Medications: The Balance Between Quality of Care and Quality of Life Coleen M Kayden, RPh Medication Information Services A Division of Williams Apothecary Pennsylvania Restraint Reduction
Antipsychotic Medications: The Balance Between Quality of Care and Quality of Life Coleen M Kayden, RPh Medication Information Services A Division of Williams Apothecary Pennsylvania Restraint Reduction
Risks of Antipsychotics use In Dementia
 AHCA/NCAL Quality Initiative for Assisted Living Webinar Series: Safely Reducing the Off-Label Use of Antipsychotics Risks of Antipsychotics use In Dementia Sanjay P. Singh, MD Chairman & Professor, Department
AHCA/NCAL Quality Initiative for Assisted Living Webinar Series: Safely Reducing the Off-Label Use of Antipsychotics Risks of Antipsychotics use In Dementia Sanjay P. Singh, MD Chairman & Professor, Department
Behavioural Symptoms of Dementia
 Quality Standards Behavioural Symptoms of Dementia Care for Patients in Hospitals and Residents in Long-Term Care Homes Let s make our health system healthier Summary This quality standard addresses care
Quality Standards Behavioural Symptoms of Dementia Care for Patients in Hospitals and Residents in Long-Term Care Homes Let s make our health system healthier Summary This quality standard addresses care
Managing Behavioural Problems in Patients with Dementia in LTC and at Home
 Managing Behavioural Problems in Patients with Dementia in LTC and at Home Samuel D. Searle MD, FRCPC Assistant Professor Division of Geriatric Medicine Dalhousie University Disclosures I have received
Managing Behavioural Problems in Patients with Dementia in LTC and at Home Samuel D. Searle MD, FRCPC Assistant Professor Division of Geriatric Medicine Dalhousie University Disclosures I have received
Managing Behavioural Problems in Patients with Dementia in LTC and at Home
 Managing Behavioural Problems in Patients with Dementia in LTC and at Home Disclosures I have received various speaking honourarium Celgene NS Department of Transportation and Infrastructure Renewal Samuel
Managing Behavioural Problems in Patients with Dementia in LTC and at Home Disclosures I have received various speaking honourarium Celgene NS Department of Transportation and Infrastructure Renewal Samuel
Disclosure. Speaker Bureaus. Grant Support. Pfizer Forest Norvartis. Pan American Health Organization/WHO NIA HRSA
 Disclosure Speaker Bureaus Pfizer Forest Norvartis Grant Support Pan American Health Organization/WHO NIA HRSA How Common is Psychosis in Alzheimer s Disease? Review of 55 studies 41% of those with Alzheimer
Disclosure Speaker Bureaus Pfizer Forest Norvartis Grant Support Pan American Health Organization/WHO NIA HRSA How Common is Psychosis in Alzheimer s Disease? Review of 55 studies 41% of those with Alzheimer
Organization: Sheppard Pratt Health System Solution Title: Lean Methodology: Appropriate Antipsychotic Use on an Inpatient Dementia Unit
 Organization: Sheppard Pratt Health System Solution Title: Lean Methodology: Appropriate Antipsychotic Use on an Inpatient Dementia Unit Problem: For dementia patients, antipsychotic medications are prescribed
Organization: Sheppard Pratt Health System Solution Title: Lean Methodology: Appropriate Antipsychotic Use on an Inpatient Dementia Unit Problem: For dementia patients, antipsychotic medications are prescribed
The Agitated. Older Patient: old. What To Do? Michelle Gibson, MD, CCFP Presented at Brockville General Hospital Rounds, May 2003
 Focus on CME at Queen s University Focus on CME at Queen s University The Agitated The Older Patient: What To Do? Michelle Gibson, MD, CCFP Presented at Brockville General Hospital Rounds, May 2003 Both
Focus on CME at Queen s University Focus on CME at Queen s University The Agitated The Older Patient: What To Do? Michelle Gibson, MD, CCFP Presented at Brockville General Hospital Rounds, May 2003 Both
Pharmacological Treatment of Behavioural and Psychological Symptoms of Dementia (BPSD) Gurdeep K Major St. Charles Hospital
 Gurdeep K Major St. Charles Hospital") Pharmacological Treatment of Behavioural and Psychological Symptoms of Dementia (BPSD) Gurdeep K Major St. Charles Hospital with thanks to Jonathan Cavan for his input Aims Define BPSD and common symptoms
Pharmacological Treatment of Behavioural and Psychological Symptoms of Dementia (BPSD) Gurdeep K Major St. Charles Hospital with thanks to Jonathan Cavan for his input Aims Define BPSD and common symptoms
Psychosis and Agitation in Dementia
 Psychosis and Agitation in Dementia Dilip V. Jeste, MD Estelle & Edgar Levi Chair in Aging, Director, Stein Institute for Research on Aging, Distinguished Professor of Psychiatry & Neurosciences, University
Psychosis and Agitation in Dementia Dilip V. Jeste, MD Estelle & Edgar Levi Chair in Aging, Director, Stein Institute for Research on Aging, Distinguished Professor of Psychiatry & Neurosciences, University
Mental Health Issues in Nursing Homes. I m glad you asked.
 Mental Health Issues in Nursing Homes I m glad you asked. I m glad you asked Susan Wehry, M.D. Associate Professor of Psychiatry, College of Medicine, University of Vermont Consultant, State of Vermont
Mental Health Issues in Nursing Homes I m glad you asked. I m glad you asked Susan Wehry, M.D. Associate Professor of Psychiatry, College of Medicine, University of Vermont Consultant, State of Vermont
From Neurodevelopment to Neurodegeneration: Behavioral Issues
 From Neurodevelopment to Neurodegeneration: Behavioral Issues Amer M. Burhan, MBChB, FRCPC Associate Professor and Chair Geriatric Psychiatry at Western U Objectives Discuss factors that contribute to
From Neurodevelopment to Neurodegeneration: Behavioral Issues Amer M. Burhan, MBChB, FRCPC Associate Professor and Chair Geriatric Psychiatry at Western U Objectives Discuss factors that contribute to
Geriatric Grand Rounds. Managing Behavioural and Psychological Symptoms of Dementia (BPSD) in Patients with Alzheimer s Disease
 in Patients with Alzheimer s Disease") Geriatric Grand Rounds Visit web sites: Tuesday, April 14, 2009 12:00 noon Dr. Bill Black Auditorium Glenrose Rehabilitation Hospital In keeping with Glenrose Rehabilitation Hospital policy, speakers participating
Geriatric Grand Rounds Visit web sites: Tuesday, April 14, 2009 12:00 noon Dr. Bill Black Auditorium Glenrose Rehabilitation Hospital In keeping with Glenrose Rehabilitation Hospital policy, speakers participating
Managing agitation in dementia using non-pharmacological therapies
 Managing agitation in dementia using non-pharmacological therapies Gill Livingston Lynsey Kelly, Elanor Lewis-Holmes, Gianluca Baio, Rumana Omar, Stephen Morris, Nishma Patel, Cornelius Katona, Claudia
Managing agitation in dementia using non-pharmacological therapies Gill Livingston Lynsey Kelly, Elanor Lewis-Holmes, Gianluca Baio, Rumana Omar, Stephen Morris, Nishma Patel, Cornelius Katona, Claudia
2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY. MEASURE TYPE: Process
 Quality ID #283: Dementia Associated Behavioral and Psychiatric Symptoms Screening and Management National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY
Quality ID #283: Dementia Associated Behavioral and Psychiatric Symptoms Screening and Management National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY
Behavioral Interventions
 Behavioral Interventions Linda K. Shumaker, R.N.-BC, MA Pennsylvania Behavioral Health and Aging Coalition Behavioral Management is the key in taking care of anyone with a Dementia! Mental Health Issues
Behavioral Interventions Linda K. Shumaker, R.N.-BC, MA Pennsylvania Behavioral Health and Aging Coalition Behavioral Management is the key in taking care of anyone with a Dementia! Mental Health Issues
Addressing Difficult Behaviors in Dementia
 Addressing Difficult Behaviors in Dementia GEORGE SCHOEPHOERSTER, MD GERIATRICIAN GENEVIVE/CENTRACARE CLINIC Objectives By the end of the session, you will be able to: 1) Explain the role of pain management
Addressing Difficult Behaviors in Dementia GEORGE SCHOEPHOERSTER, MD GERIATRICIAN GENEVIVE/CENTRACARE CLINIC Objectives By the end of the session, you will be able to: 1) Explain the role of pain management
NEUROPSYCHOMETRIC TESTS
 NEUROPSYCHOMETRIC TESTS CAMCOG It is the Cognitive section of Cambridge Examination for Mental Disorders of the Elderly (CAMDEX) The measure assesses orientation, language, memory, praxis, attention, abstract
NEUROPSYCHOMETRIC TESTS CAMCOG It is the Cognitive section of Cambridge Examination for Mental Disorders of the Elderly (CAMDEX) The measure assesses orientation, language, memory, praxis, attention, abstract
Management of Agitation in Dementia. Kimberly Triplett Ferguson, MS4
 Management of Agitation in Dementia Kimberly Triplett Ferguson, MS4 Objectives 1. Review recommended evaluation of agitated patients with dementia. 2. Discuss evidence concerning nonpharmacologic management.
Management of Agitation in Dementia Kimberly Triplett Ferguson, MS4 Objectives 1. Review recommended evaluation of agitated patients with dementia. 2. Discuss evidence concerning nonpharmacologic management.
Sleep Apnea and Intellectual Disability
 Sleep Apnea and Intellectual Disability Presenters: Dr Colin Shapiro BSc, FRCP(C), MBBS, PhD Judi Hoskins DSW, B.A. Psych Nov 15, 2010 1 Sleep Apnea and Intellectual Disabilities: multidisciplinary assessment
Sleep Apnea and Intellectual Disability Presenters: Dr Colin Shapiro BSc, FRCP(C), MBBS, PhD Judi Hoskins DSW, B.A. Psych Nov 15, 2010 1 Sleep Apnea and Intellectual Disabilities: multidisciplinary assessment
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017.
 DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
Neuropsychiatric Inventory Nursing Home Version (NPI-NH)
") This is a Sample version of the Neuropsychiatric Inventory Nursing Home Version (NPI-NH) The full version of the Neuropsychiatric Inventory Nursing Home Version (NPI-NH) comes without sample watermark..
This is a Sample version of the Neuropsychiatric Inventory Nursing Home Version (NPI-NH) The full version of the Neuropsychiatric Inventory Nursing Home Version (NPI-NH) comes without sample watermark..
Supplementary Online Content
 Supplementary Online Content Porsteinsson AP, Drye LT, Pollock BG, et al. Effect of citalopram on agitation in Alzheimer disease: the CitAD randomized controlled trial. JAMA. doi:10.1001/jama.2014.93 eappendix.
Supplementary Online Content Porsteinsson AP, Drye LT, Pollock BG, et al. Effect of citalopram on agitation in Alzheimer disease: the CitAD randomized controlled trial. JAMA. doi:10.1001/jama.2014.93 eappendix.
Non-Pharmacological Interventions for Persons With Dementia. John Erpenbach, CNP Michele Snyders, LCSW, ACHP-SW
 Non-Pharmacological Interventions for Persons With Dementia John Erpenbach, CNP Michele Snyders, LCSW, ACHP-SW Prevalence3 5.5 million people in the United States are aging with dementia and complex comorbidities
Non-Pharmacological Interventions for Persons With Dementia John Erpenbach, CNP Michele Snyders, LCSW, ACHP-SW Prevalence3 5.5 million people in the United States are aging with dementia and complex comorbidities
Delirium, Depression and Dementia
 Delirium, Depression and Dementia Martha Watson, MS, APRN, GCNS Some material included in this presentation is adapted from: NICHE (2009). Geriatric Resource Nurse Core Curriculum [Power Point presentation].
Delirium, Depression and Dementia Martha Watson, MS, APRN, GCNS Some material included in this presentation is adapted from: NICHE (2009). Geriatric Resource Nurse Core Curriculum [Power Point presentation].
SECTION 1. Children and Adolescents with Depressive Disorder: Summary of Findings. from the Literature and Clinical Consultation in Ontario
 SECTION 1 Children and Adolescents with Depressive Disorder: Summary of Findings from the Literature and Clinical Consultation in Ontario Children's Mental Health Ontario Children and Adolescents with
SECTION 1 Children and Adolescents with Depressive Disorder: Summary of Findings from the Literature and Clinical Consultation in Ontario Children's Mental Health Ontario Children and Adolescents with
The Neuropsychiatric Inventory Questionnaire: Background and Administration
 The Neuropsychiatric Inventory Questionnaire: Background and Administration The Neuropsychiatric Inventory Questionnaire (NPI-Q) was developed and crossvalidated with the standard NPI to provide a brief
The Neuropsychiatric Inventory Questionnaire: Background and Administration The Neuropsychiatric Inventory Questionnaire (NPI-Q) was developed and crossvalidated with the standard NPI to provide a brief
Management of Behavioral Symptoms in Dementia. Brenda Jordan, MS, ARNP, BC- PCM Dartmouth-Hitchcock Kendal
 Management of Behavioral Symptoms in Dementia Brenda Jordan, MS, ARNP, BC- PCM Dartmouth-Hitchcock Kendal Behavioral Symptoms Common & troubling At least one will occur in 61-92% of those with any dementia
Management of Behavioral Symptoms in Dementia Brenda Jordan, MS, ARNP, BC- PCM Dartmouth-Hitchcock Kendal Behavioral Symptoms Common & troubling At least one will occur in 61-92% of those with any dementia
Antipsychotic Medications
 TRAIL: Team Review of EVIDENCE REVIEW & RECOMMENDATIONS FOR LTC Behavioural and psychological symptoms of dementia (BPSD) refer to the non-cognitive symptoms of disturbed perception, thought content, mood
TRAIL: Team Review of EVIDENCE REVIEW & RECOMMENDATIONS FOR LTC Behavioural and psychological symptoms of dementia (BPSD) refer to the non-cognitive symptoms of disturbed perception, thought content, mood
Pharmacological Treatment of Aggression in the Elderly
 Pharmacological Treatment of Aggression in the Elderly Howard Fenn, MD Adjunct Clinical Associate Professor Department of Psychiatry and Behavioral Sciences Stanford University Self-Assessment Question
Pharmacological Treatment of Aggression in the Elderly Howard Fenn, MD Adjunct Clinical Associate Professor Department of Psychiatry and Behavioral Sciences Stanford University Self-Assessment Question
Non-pharmacological Approaches in Dementia Care. Dr. Anna Fisher
 Non-pharmacological Approaches in Dementia Care Dr. Anna Fisher What is Dementia Dementia is a group of symptoms that may accompany certain diseases or conditions Symptoms many involve changes in personality,
Non-pharmacological Approaches in Dementia Care Dr. Anna Fisher What is Dementia Dementia is a group of symptoms that may accompany certain diseases or conditions Symptoms many involve changes in personality,
Assessing and Treating Agitation Associated with Alzheimer s Disease
 AXS-05 R&D Day April 24, 2018 Assessing and Treating Agitation Associated with Alzheimer s Disease Marc E. Agronin, MD VP, Behavioral Health and Clinical Research, Miami Jewish Health Affiliate Associate
AXS-05 R&D Day April 24, 2018 Assessing and Treating Agitation Associated with Alzheimer s Disease Marc E. Agronin, MD VP, Behavioral Health and Clinical Research, Miami Jewish Health Affiliate Associate
GERIATRIC WORKFORCE ENHANCEMENT PROGRAM (GWEP) FACULTY DEVELOPMENT MASTERWORKS SERIES
 FACULTY DEVELOPMENT MASTERWORKS SERIES") UNIVERSITY OF SOUTH FLORIDA GERIATRIC WORKFORCE ENHANCEMENT PROGRAM (GWEP) FACULTY DEVELOPMENT MASTERWORKS SERIES Kathryn Hyer, PhD, MPP Principal Investigator h Providers of Continuing Education For additional
UNIVERSITY OF SOUTH FLORIDA GERIATRIC WORKFORCE ENHANCEMENT PROGRAM (GWEP) FACULTY DEVELOPMENT MASTERWORKS SERIES Kathryn Hyer, PhD, MPP Principal Investigator h Providers of Continuing Education For additional
PSYCHOTROPIC SOLUTIONS
 PSYCHOTROPIC SOLUTIONS A proactive approach to antipsychotic medication management A Quality Use of Medicines initiative by Choice Aged Care Copyright 2018 Hello everyone. Today we will be discussing the
PSYCHOTROPIC SOLUTIONS A proactive approach to antipsychotic medication management A Quality Use of Medicines initiative by Choice Aged Care Copyright 2018 Hello everyone. Today we will be discussing the
Responsive Behaviours in the Dining Room
 How BSO and Dietary Can Work Together Responsive Behaviours in the Dining Room April 5, 2016 TWC Culinary and Nutrition Summit Teresa Tibbo RPN, Twinkle Patel RD Seasons Care Dietitian Network Carol Donovan,
How BSO and Dietary Can Work Together Responsive Behaviours in the Dining Room April 5, 2016 TWC Culinary and Nutrition Summit Teresa Tibbo RPN, Twinkle Patel RD Seasons Care Dietitian Network Carol Donovan,
Behavior Problems: in Long Term Care and Assisted Living
 Behavior Problems: Dementia and Mental Illness in Long Term Care and Assisted Living Module I Dr. David A. Smith, M.D., FAAFP, CMD mmlearn.org is a program of Morningside Ministries Cell Phones and Pagers
Behavior Problems: Dementia and Mental Illness in Long Term Care and Assisted Living Module I Dr. David A. Smith, M.D., FAAFP, CMD mmlearn.org is a program of Morningside Ministries Cell Phones and Pagers
Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE
 Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE Objectives At the conclusion of the session, participants will be
Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE Objectives At the conclusion of the session, participants will be
Treatment of behavioral and psychological symptoms of dementia: a systematic review
 Psychiatr. Pol. 2016; 50(4): 679 715 PL ISSN 0033-2674 (PRINT), ISSN 2391-5854 (ONLINE) www.psychiatriapolska.pl DOI: http://dx.doi.org/10.12740/pp/64477 Treatment of behavioral and psychological symptoms
Psychiatr. Pol. 2016; 50(4): 679 715 PL ISSN 0033-2674 (PRINT), ISSN 2391-5854 (ONLINE) www.psychiatriapolska.pl DOI: http://dx.doi.org/10.12740/pp/64477 Treatment of behavioral and psychological symptoms
Introduction to Dementia: Complications
 Introduction to Dementia: Complications Created in March 2005 Duration: about 15 minutes Axel Juan, MD The Geriatrics Institute axel.juan@med.va.gov 305-575-3388 Credits Principal medical contributor:
Introduction to Dementia: Complications Created in March 2005 Duration: about 15 minutes Axel Juan, MD The Geriatrics Institute axel.juan@med.va.gov 305-575-3388 Credits Principal medical contributor:
Pharmacological Treatments for Neuropsychiatric Symptoms in Dementia 3/22/2018
 Pharmacological Treatments for Neuropsychiatric Symptoms in Dementia 3/22/2018 Mary Ellen Quiceno, MD, FAAN Associate Professor of Neurology UNTHSC Center for Geriatrics 855 Montgomery Street, PCC 4, Ft.
Pharmacological Treatments for Neuropsychiatric Symptoms in Dementia 3/22/2018 Mary Ellen Quiceno, MD, FAAN Associate Professor of Neurology UNTHSC Center for Geriatrics 855 Montgomery Street, PCC 4, Ft.
Management of Behavioral and Psychological Symptoms in People with Dementia Living in Care Homes: A UK Perspective
 Management of Behavioral and Psychological Symptoms in People with Dementia Living in Care Homes: A UK Perspective Clive Ballard Professor of Age Related Diseases, King s College London And Director of
Management of Behavioral and Psychological Symptoms in People with Dementia Living in Care Homes: A UK Perspective Clive Ballard Professor of Age Related Diseases, King s College London And Director of
Clinical Trial Designs for RCTs focussing on the Treatment of Agitation in people with Alzheimer s disease
 Clinical Trial Designs for RCTs focussing on the Treatment of Agitation in people with Alzheimer s disease Professor Clive Ballard Dr Byron Creese University of Exeter, UK Guardian guide for 2018: Top
Clinical Trial Designs for RCTs focussing on the Treatment of Agitation in people with Alzheimer s disease Professor Clive Ballard Dr Byron Creese University of Exeter, UK Guardian guide for 2018: Top
Supporting people with dementia to live well in London care homes
 Supporting people with dementia to live well in London care homes London Dementia Clinical Network Date Dr Daniel Harwood; Clinical Director and Consultant Psychiatrist SLAM (Lewisham Care Home Intervention
Supporting people with dementia to live well in London care homes London Dementia Clinical Network Date Dr Daniel Harwood; Clinical Director and Consultant Psychiatrist SLAM (Lewisham Care Home Intervention
Cambridge University Press Effective Treatments in Psychiatry Peter Tyrer and Kenneth R. Silk Excerpt More information
 Organic disorders 1 Delirium Based on Delirium by Laura Gage and David K. Conn in Effective Treatments in Psychiatry, Cambridge University Press, 2008 Introduction Delirium needs treatment for both its
Organic disorders 1 Delirium Based on Delirium by Laura Gage and David K. Conn in Effective Treatments in Psychiatry, Cambridge University Press, 2008 Introduction Delirium needs treatment for both its
Specialist dementia care units
 Specialist dementia care units An Evidence Check rapid review brokered by the Sax Institute for the Commonwealth Department of Health. September 2017 An Evidence Check rapid review brokered by the Sax
Specialist dementia care units An Evidence Check rapid review brokered by the Sax Institute for the Commonwealth Department of Health. September 2017 An Evidence Check rapid review brokered by the Sax
Burden of behavioral and psychiatric symptoms in people screened positive for dementia in primary care results of the DelpHi-study René Thyrian
 Burden of behavioral and psychiatric symptoms in people screened positive for dementia in primary care results of the DelpHi-study René Thyrian German Center for Neurodegenerative Diseases (DZNE), site
Burden of behavioral and psychiatric symptoms in people screened positive for dementia in primary care results of the DelpHi-study René Thyrian German Center for Neurodegenerative Diseases (DZNE), site
An Evaluation of a Training Program in Restraint-Free Care for Individuals with Dementia Christina Garrison-Diehn, Clair Rummel, & Jane E.
 An Evaluation of a Training Program in Restraint-Free Care for Individuals with Dementia Christina Garrison-Diehn, Clair Rummel, & Jane E. Fisher Background Disease. (Xu, Kochanek & Tejada-Vera, 2009)
An Evaluation of a Training Program in Restraint-Free Care for Individuals with Dementia Christina Garrison-Diehn, Clair Rummel, & Jane E. Fisher Background Disease. (Xu, Kochanek & Tejada-Vera, 2009)
Delirium. Approach. Symptom Update Masterclass:
 Symptom Update Masterclass: Delirium Jason Boland Senior Clinical Lecturer and Honorary Consultant in Palliative Medicine Wolfson Centre for Palliative Care Research Hull York Medical School University
Symptom Update Masterclass: Delirium Jason Boland Senior Clinical Lecturer and Honorary Consultant in Palliative Medicine Wolfson Centre for Palliative Care Research Hull York Medical School University
Delirium: developing and implementing a multi-component intervention
 Delirium: developing and implementing a multi-component intervention Dr. Duncan Forsyth Consultant Geriatrician Addenbrooke s Hospital Cambridge University Hospitals NHS Foundation Trust Cambridge, England
Delirium: developing and implementing a multi-component intervention Dr. Duncan Forsyth Consultant Geriatrician Addenbrooke s Hospital Cambridge University Hospitals NHS Foundation Trust Cambridge, England
Drugs used to relieve behavioural and psychological symptoms in dementia
 alzheimers.org.uk Drugs used to relieve behavioural and psychological symptoms in dementia People with dementia may develop behavioural and psychological symptoms including restlessness, aggression, delusions,
alzheimers.org.uk Drugs used to relieve behavioural and psychological symptoms in dementia People with dementia may develop behavioural and psychological symptoms including restlessness, aggression, delusions,
ANTIPSYCHOTICS IN LONG TERM CARE: Are We Doing More Harm than Good?
 ANTIPSYCHOTICS IN LONG TERM CARE: Are We Doing More Harm than Good? STEPHANIE M. OZALAS, PHARMD, BCPS, BCGP VA MARYLAND HEALTH CARE SYSTEM BALTIMORE, MD DISCLOSURES Off-label use of medications will be
ANTIPSYCHOTICS IN LONG TERM CARE: Are We Doing More Harm than Good? STEPHANIE M. OZALAS, PHARMD, BCPS, BCGP VA MARYLAND HEALTH CARE SYSTEM BALTIMORE, MD DISCLOSURES Off-label use of medications will be
How to prevent delirium in nursing home. Dr. Sophie ALLEPAERTS Geriatric department CHU-Liège Belgium
 How to prevent delirium in nursing home Dr. Sophie ALLEPAERTS Geriatric department CHU-Liège Belgium 1 CONFLICT OF INTEREST DISCLOSURE I have no potential conflict of interest to report 2 Outline 1. Introduction
How to prevent delirium in nursing home Dr. Sophie ALLEPAERTS Geriatric department CHU-Liège Belgium 1 CONFLICT OF INTEREST DISCLOSURE I have no potential conflict of interest to report 2 Outline 1. Introduction
Caregiver Mediated Intervention. Trumps Pharmacotherapy for BPSD
 Caregiver Mediated Intervention DEMENTIA RESEARCH Trumps Pharmacotherapy for BPSD Henry Brodaty and Caroline Arasaratnam Dementia Collaborative Research Centre Assessment and Better Care Collaborative
Caregiver Mediated Intervention DEMENTIA RESEARCH Trumps Pharmacotherapy for BPSD Henry Brodaty and Caroline Arasaratnam Dementia Collaborative Research Centre Assessment and Better Care Collaborative
Agita&on/Aggression in Elderly: What works. G. Michael Allan Professor, Dept of Family, U of A. Director, Evidence & CPD Program, ACFP
 Agita&on/Aggression in Elderly: What works G. Michael Allan Professor, Dept of Family, U of A. Director, Evidence & CPD Program, ACFP Background: Agita6on in Demen6a Demen&a can > agita&on and violent
Agita&on/Aggression in Elderly: What works G. Michael Allan Professor, Dept of Family, U of A. Director, Evidence & CPD Program, ACFP Background: Agita6on in Demen6a Demen&a can > agita&on and violent
Delirium. A Plan to Reduce Use of Restraints. David Wensel DO, FAAHPM Medical Director Midland Care
 Delirium A Plan to Reduce Use of Restraints David Wensel DO, FAAHPM Medical Director Midland Care Objectives Define delirium Describe pathophysiology of delirium Understand most common etiologies Define
Delirium A Plan to Reduce Use of Restraints David Wensel DO, FAAHPM Medical Director Midland Care Objectives Define delirium Describe pathophysiology of delirium Understand most common etiologies Define
Number of Items. Response Categories. Part V: Specific Behavior Scales-Sleep Scales. Based on past month
 Part V: Specific Behavior Scales-Sleep Scales Based on past month First 4 items ask for time or amount of sleep 41. Pittsburgh Sleep Quality Index (PSQI) Sleep quality Sleep latency Sleep duration Habitual
Part V: Specific Behavior Scales-Sleep Scales Based on past month First 4 items ask for time or amount of sleep 41. Pittsburgh Sleep Quality Index (PSQI) Sleep quality Sleep latency Sleep duration Habitual
Parkinsonian Disorders with Dementia
 Parkinsonian Disorders with Dementia George Tadros Consultant in Old Age Liaison Psychiatry, RAID, Heartlands Hospital Professor of Dementia and Liaison Psychiatry, Aston Medical School Aston University
Parkinsonian Disorders with Dementia George Tadros Consultant in Old Age Liaison Psychiatry, RAID, Heartlands Hospital Professor of Dementia and Liaison Psychiatry, Aston Medical School Aston University
CHCS. Multimorbidity Pattern Analyses and Clinical Opportunities: Dementia. Center for Health Care Strategies, Inc. FACES OF MEDICAID DATA SERIES
 CHCS Center for Health Care Strategies, Inc. FACES OF MEDICAID DATA SERIES Multimorbidity Pattern Analyses and Clinical Opportunities: Dementia December 2010 Cynthia Boyd, MD, MPH* Bruce Leff, MD* Carlos
CHCS Center for Health Care Strategies, Inc. FACES OF MEDICAID DATA SERIES Multimorbidity Pattern Analyses and Clinical Opportunities: Dementia December 2010 Cynthia Boyd, MD, MPH* Bruce Leff, MD* Carlos
Dementia: Managing Difficult Behaviors. No conflicts of interest. Off-label medication use will be discussed during this talk.
 Dementia: Managing Difficult Behaviors No conflicts of interest. Off-label medication use will be discussed during this talk. 1 Types of Neurocognitive Disorder Alzheimer s Disease Vascular Frontotemporal
Dementia: Managing Difficult Behaviors No conflicts of interest. Off-label medication use will be discussed during this talk. 1 Types of Neurocognitive Disorder Alzheimer s Disease Vascular Frontotemporal
Behavioral and psychological symptoms of dementia characteristic of mild Alzheimer patients
 Blackwell Science, LtdOxford, UKPCNPsychiatry and Clinical Neurosciences1323-13162005 Blackwell Publishing Pty Ltd593274279Original ArticleDementia and mild AlzheimersJ. Shimabukuro et al. Psychiatry and
Blackwell Science, LtdOxford, UKPCNPsychiatry and Clinical Neurosciences1323-13162005 Blackwell Publishing Pty Ltd593274279Original ArticleDementia and mild AlzheimersJ. Shimabukuro et al. Psychiatry and
WHEN THE GOING GETS TOUGH: Working Through the Challenges of Dementia Together. Presented by
 WHEN THE GOING GETS TOUGH: Working Through the Challenges of Dementia Together Presented by Our agenda for today Understanding behavioral symptoms in people living with dementia Briefly review key strategies
WHEN THE GOING GETS TOUGH: Working Through the Challenges of Dementia Together Presented by Our agenda for today Understanding behavioral symptoms in people living with dementia Briefly review key strategies
Depression in the Eldery Handout Package
 Depression in the Eldery Handout Package Depression in the Elderly 1 Learning Objectives Upon completion of this module, you should be able to: 1. State the prevalence and describe the consequences of
Depression in the Eldery Handout Package Depression in the Elderly 1 Learning Objectives Upon completion of this module, you should be able to: 1. State the prevalence and describe the consequences of
Palliative Care Consult Service
 Creating Program Elements to Improve the Care of the Dementia Patient in Palliative & Hospice Settings Carla Jolley MN, ARNP, ANP-BC, AOCN, ACHPN Palliative Care APN/Program Coordinator WhidbeyHealth Palliative
Creating Program Elements to Improve the Care of the Dementia Patient in Palliative & Hospice Settings Carla Jolley MN, ARNP, ANP-BC, AOCN, ACHPN Palliative Care APN/Program Coordinator WhidbeyHealth Palliative
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE. Health Technology Appraisal
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Health Technology Appraisal Donepezil, galantamine, rivastigmine and memantine for the treatment of Alzheimer's disease (Review of TA 111) Appraisal
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Health Technology Appraisal Donepezil, galantamine, rivastigmine and memantine for the treatment of Alzheimer's disease (Review of TA 111) Appraisal
Appendix K: Evidence review flow charts
 K.1 Dementia diagnosis K.1.1 Dementia diagnosis What are the most effective methods of primary assessment to decide whether a person with suspected dementia should be referred to a dementia service? What
K.1 Dementia diagnosis K.1.1 Dementia diagnosis What are the most effective methods of primary assessment to decide whether a person with suspected dementia should be referred to a dementia service? What
Rational Medication Use in Dementia
 Rational Medication Use in Dementia Stephen Thielke sthielke@u.washington.edu (206) 764 2815 I have no conflicts of interest to report. I am an employee of the federal government. The opinions in this
Rational Medication Use in Dementia Stephen Thielke sthielke@u.washington.edu (206) 764 2815 I have no conflicts of interest to report. I am an employee of the federal government. The opinions in this
Management of the Behavioral and Psychological Symptoms of Dementia (BPSD)
") Management of the Behavioral and Psychological Symptoms of Dementia (BPSD) Soheyla Mahdavian, PharmD, BCGP, TTS Associate Professor of Pharmacy Practice Florida A&M University College of Pharmacy and Pharmaceutical
Management of the Behavioral and Psychological Symptoms of Dementia (BPSD) Soheyla Mahdavian, PharmD, BCGP, TTS Associate Professor of Pharmacy Practice Florida A&M University College of Pharmacy and Pharmaceutical
Delirium in the Elderly
 Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
Behavioral Management in Dementia. a.k.a. Public Enemy Number One a.k.a. Proteins Gone Bad
 Behavioral Management in Dementia a.k.a. Public Enemy Number One a.k.a. Proteins Gone Bad Game Plan 1. Definition 2. Epidemiology 3. Assessment: IT S OVER 4. Nonpharmacologic Strategies: 4 S 5. Nonpharmacologic:
Behavioral Management in Dementia a.k.a. Public Enemy Number One a.k.a. Proteins Gone Bad Game Plan 1. Definition 2. Epidemiology 3. Assessment: IT S OVER 4. Nonpharmacologic Strategies: 4 S 5. Nonpharmacologic:
Charles Bernick, MD, MPH Cleveland Clinic Lou Ruvo Center for Brain Health June 2, 2018
 Charles Bernick, MD, MPH Cleveland Clinic Lou Ruvo Center for Brain Health June 2, 2018 Delirium common Prolongs hospitalization Worsens dementia ( if you survive) Increased risk of institutionalization
Charles Bernick, MD, MPH Cleveland Clinic Lou Ruvo Center for Brain Health June 2, 2018 Delirium common Prolongs hospitalization Worsens dementia ( if you survive) Increased risk of institutionalization
Session outline. Introduction to dementia Assessment of dementia Management of dementia Follow-up Review
 Dementia 1 Session outline Introduction to dementia Assessment of dementia Management of dementia Follow-up Review 2 Activity 1: Person s story Present a person s story of what it feels like to live with
Dementia 1 Session outline Introduction to dementia Assessment of dementia Management of dementia Follow-up Review 2 Activity 1: Person s story Present a person s story of what it feels like to live with
MENTAL HEALTH DISEASE CLASSIFICATIONS
 MENTAL HEALTH DISEASE CLASSIFICATIONS DIAGNOSIS OF MENTAL DISORDERS DSM-IV-TR Published by APA ( 2000 ) Multiaxial system 5 categories called axes Facilitate holistic assessment for care Is a great resource
MENTAL HEALTH DISEASE CLASSIFICATIONS DIAGNOSIS OF MENTAL DISORDERS DSM-IV-TR Published by APA ( 2000 ) Multiaxial system 5 categories called axes Facilitate holistic assessment for care Is a great resource
Basic Standards for Residency/Fellowship Training in Geriatric Psychiatry
 Basic Standards for Residency/Fellowship Training in Geriatric Psychiatry American Osteopathic Association and American College of Osteopathic Neurologists and Psychiatrists Approved 2/2005 Revised 2/2008,
Basic Standards for Residency/Fellowship Training in Geriatric Psychiatry American Osteopathic Association and American College of Osteopathic Neurologists and Psychiatrists Approved 2/2005 Revised 2/2008,