Optimal Perioperative Management of the Geriatric Patient: A Best Practices Guideline from the ACS NSQIP/American Geriatrics Society
|
|
|
- Osborn Bryant
- 5 years ago
- Views:
Transcription
1 Optimal Perioperative Management of the Geriatric Patient: A Best Practices Guideline from the ACS NSQIP/American Geriatrics Society Sanjay Mohanty, MD; Ronnie A. Rosenthal, MS,MD; Marcia M. Russell, MD; Mark D. Neuman, MD, MSc; Clifford Y Ko, MD, MS, MSHS; Nestor F. Esnaola, MD, MPH, MBA
2 Disclosures I have no disclosures
3 Establishing Guidelines for Geriatric Surgical Care Preoperative Assessment Intraoperative Management Postoperative Care Discharge Planning Developing Quality Indicators for Elderly Surgical Patients. McGory (Russell) & Ko, Ann Surg 2009
4 Establishing Guidelines for Geriatric Surgical Care Preoperative Assessment Intraoperative Management Postoperative Care Discharge Planning Developing Quality Indicators for Elderly Surgical Patients. McGory (Russell) & Ko, Ann Surg 2009

5 Chow et al JACS, 2012
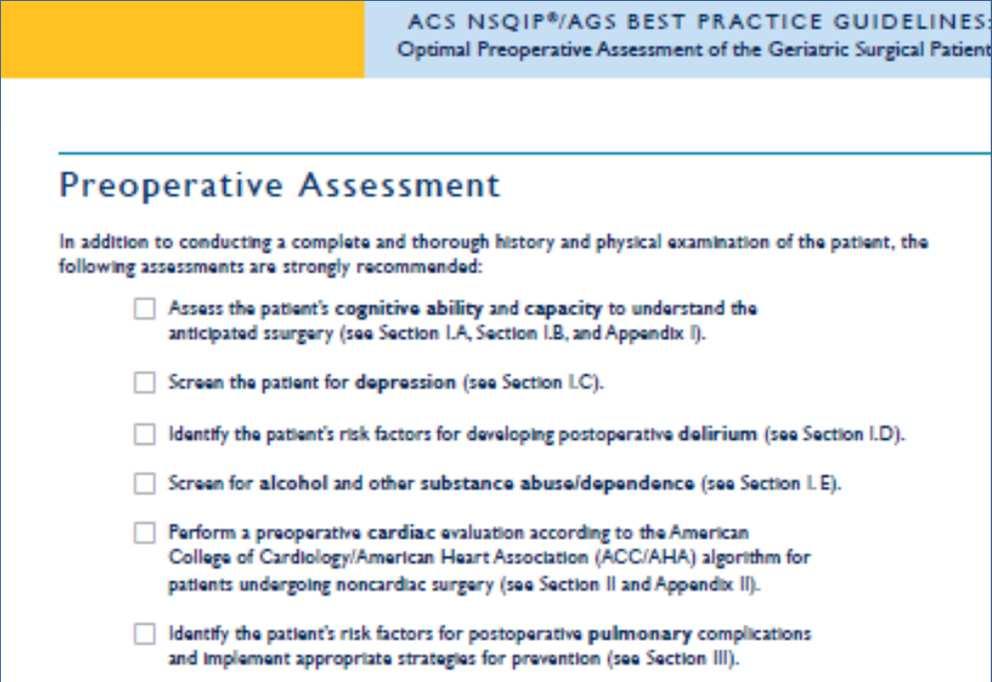
6 Preoperative Assessment Cognition, Function, Nutrition and Frailty Comorbidity Assessment Medication Use Provider and Patient Discussions Discharge Planning
7 Establishing Guidelines for Geriatric Surgical Care Preoperative Assessment Intraoperative Management Postoperative Care Discharge Planning

 AGS Geriatrics for Specialists Initiative")
8 Methods Focused, structured search of MEDLINE( ) to identify systematic reviews meta-analyses practice guidelines clinical trials 28-member, multidisciplinary expert panel: American College of Surgeons (ACS) ACS Geriatric Surgery Task Force American Society of Anesthesiologists American Geriatrics Society (AGS) AGS Geriatrics for Specialists Initiative Mohanty et al, JACS 2016
9


10 Perioperative Geriatric Care Immediate Preoperative Period Intraoperative Management Postoperative Care Care Transitions

11 Immediate Preoperative Goals / Advanced Care Planning Preoperative Preparations
12 Treatment Goals and Expectations Patient expectations are influenced by their treatment preferences. Older patients are less likely to want a treatment (even if it results in cure) that may result in severe functional or cognitive impairment. Fried TR, Bradley EH, Towle VR, Allore H. N Engl J Med. 2002;346:
13 Percent of Patients Who Want the Treatment Return to Current Health Functional Impairment Cognitive Impairment Low Burden Treatment High Burden Treatment 98.7% 88.8% Fried TR, Bradley EH, Towle VR, Allore H. N Engl J Med. 2002;346:
14 What percent of older adults do you think would accept a low burden treatment (possibly for cure) if there was a chance it might result in a severe functional deficit? A. 85% B. 65% C. 45% D. 25%
15 Percent of Patients Who Want the Treatment Return to Current Health Functional Impairment Cognitive Impairment Low Burden Treatment High Burden Treatment 98.7% 25.6% 11.2% 88.8% Fried TR, Bradley EH, Towle VR, Allore H. N Engl J Med. 2002;346:
16 For Patients with Pre-existing Advance Directives: Required Reconsideration New risks, benefits, and alternatives of procedure should be discussed Ensure that approach to potential lifethreatening problems is consistent with values American College of Surgeons, 2014; American Nurses Association, 2012; American Society of Anesthesiologists, 2008
17 From: BPG Preoperative Assessment 2012

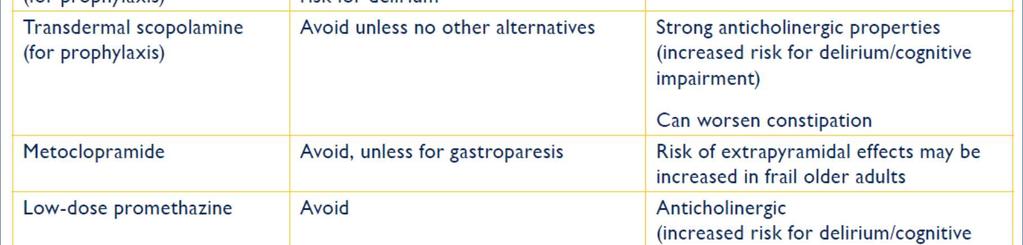
18 Discontinue Potentially Inappropriate Medications J Am Geriatr Soc Nov;63(11):
19 Intraoperative Management Anesthetic Approach Perioperative Analgesia Plan Preventing Postop Nausea and Vomiting Patient Safety in the OR Preventing Complications Fluid Management
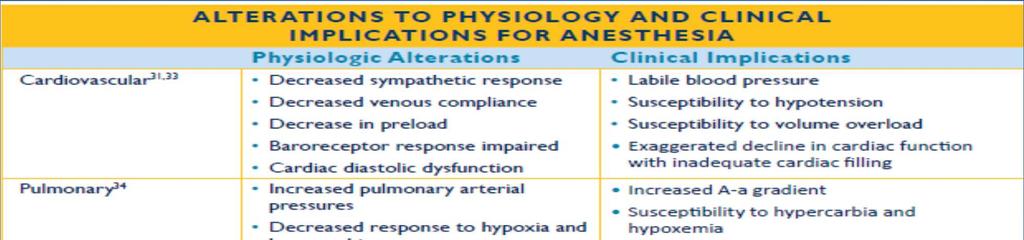
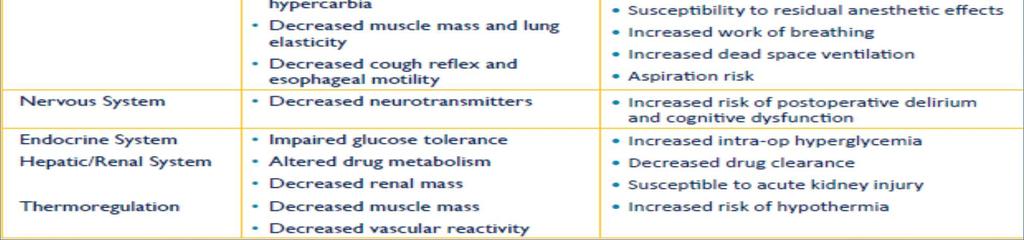
20 Physiologic Effects of Anesthesia Medications Changes in: Systemic Vascular Resistance Cardiac Preload Baroreceptors Responses Lung Mechanics Oxygen Diffusion Neurotransmitter Function End Organ Blood Flow
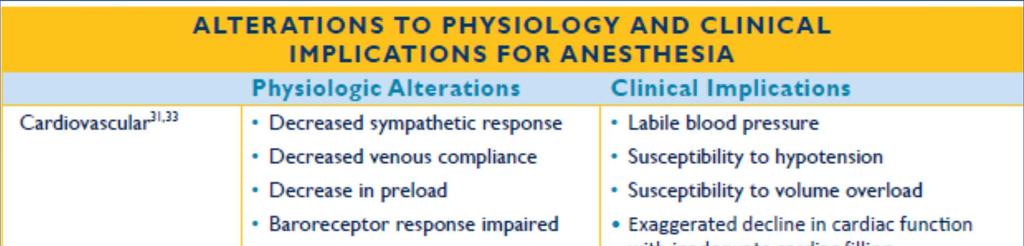
21 Physiologic Changes of Aging
22 Anesthesia in the Older Adult There is insufficient evidence to recommend a single best anesthetic plan for all older adults.

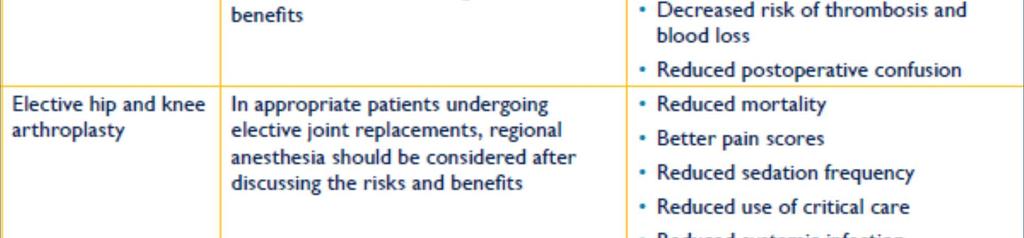
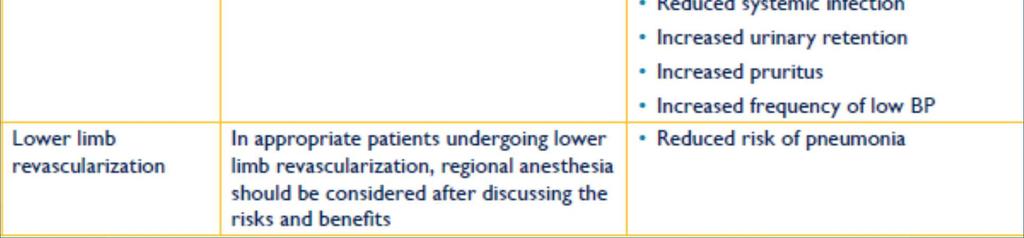
23 Role of Regional Techniques for Anesthesia
24 Perioperative Analgesia in the Older Adult Directed pain history and physical Appropriately titrated for increased sensitivity Include a prophylactic bowel regimen Avoid inappropriate medications (benozos, meperidine, benadryl, Beers list,) Multimodal Use opioid-sparing and regional techniques


25 Role of Regional Techniques for Perioperative Pain
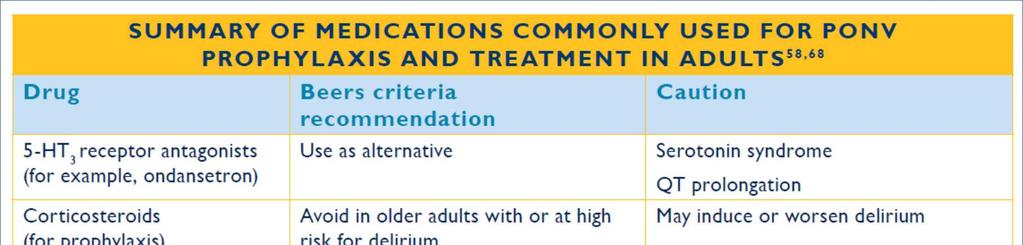
26 Preventing Postoperative Nausea and Vomiting
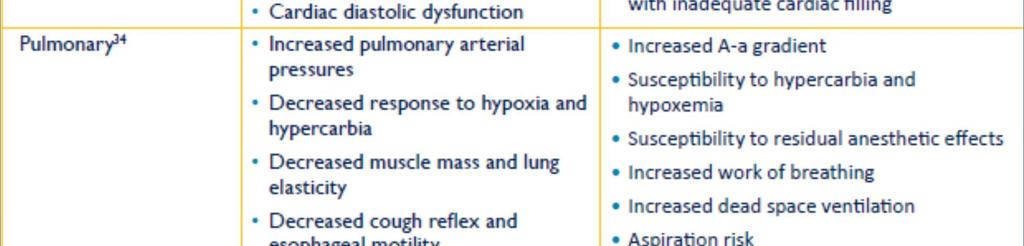
27 Pulmonary Considerations


28
29 Fluid Management in the Older Adult There is insufficient evidence to recommend a single best intraoperative fluid management plan for all older adults.

30 Fluid Management
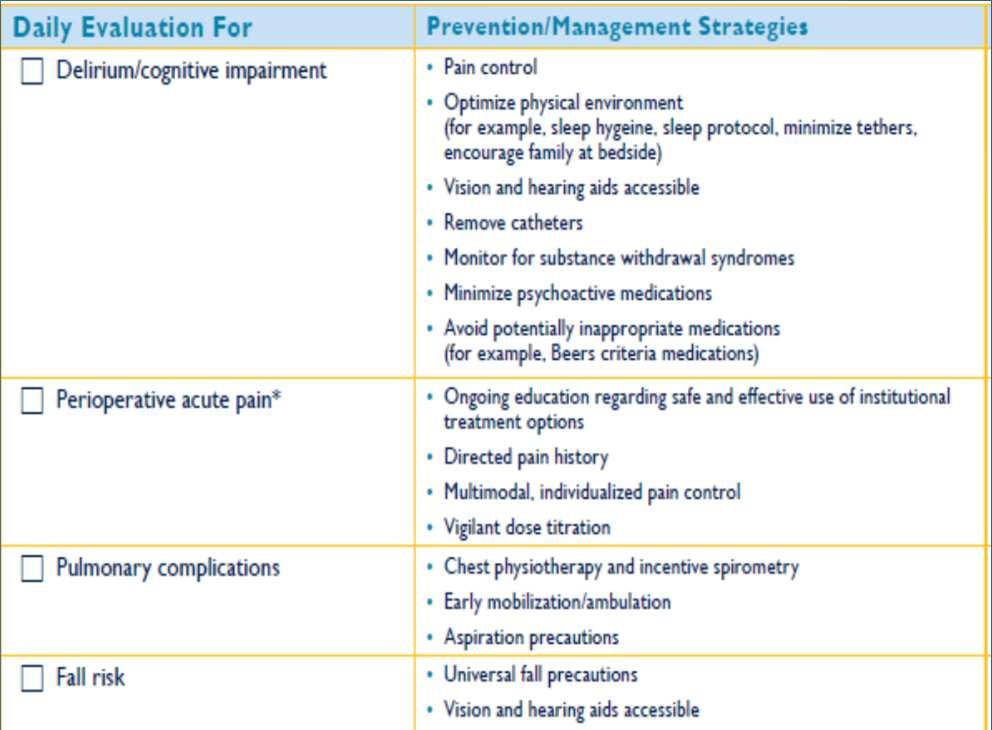
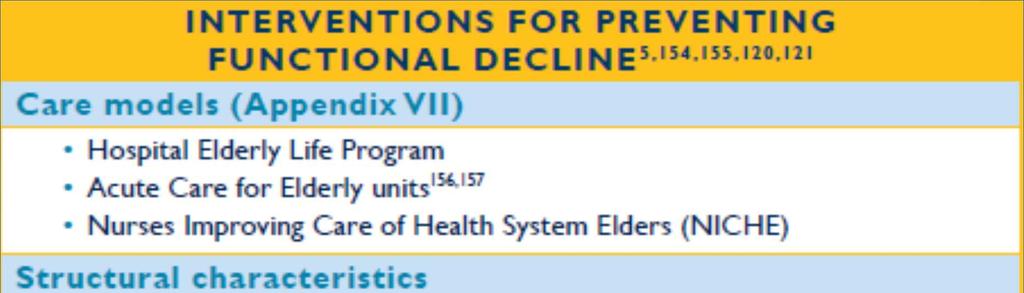
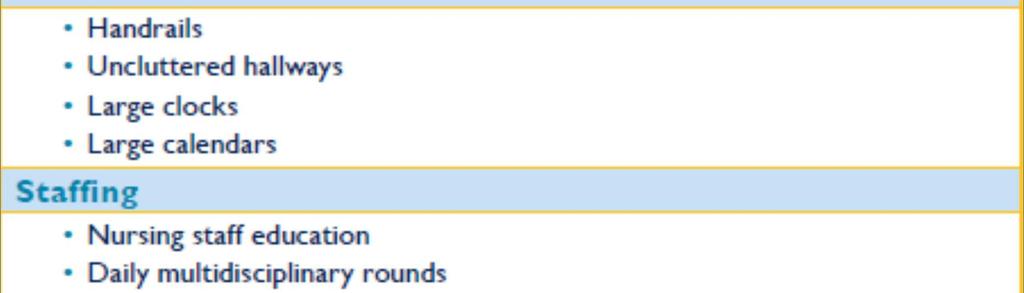
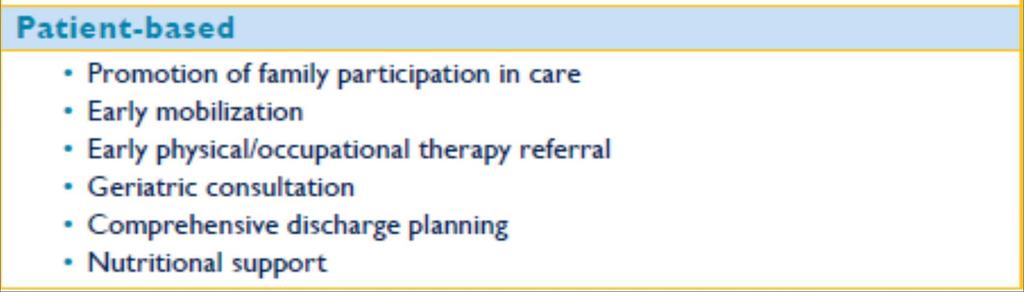
31 Postoperative Care Controlling Perioperative Acute Pain Delirium/ Cognitive Issues Functional Decline Fall Risk Pressure Ulcer and UTI Prevention Adequate Nutrition Pulmonary Complications
32 Perioperative Analgesia in the Older Adult Directed pain history and physical Appropriately titrated for increased sensitivity Include a prophylactic bowel regimen Avoid inappropriate medications (benozos, meperidine, benadryl, Beers list,) Multimodal Use opioid-sparing and regional techniques


33
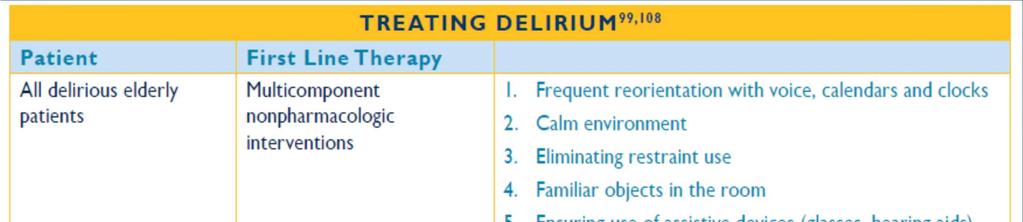
34 Precipitating Factors for Delirium Pain Medications Dehydration Under-nutrition Unfamiliar environment Sleep disruption Sensory deprivation Restraints Catheters & other devices Constipation Urinary retention Physiolgic stress of surgery Infection Hypoxemia Electrolyte imbalance Neurological events Major organ dysfunction
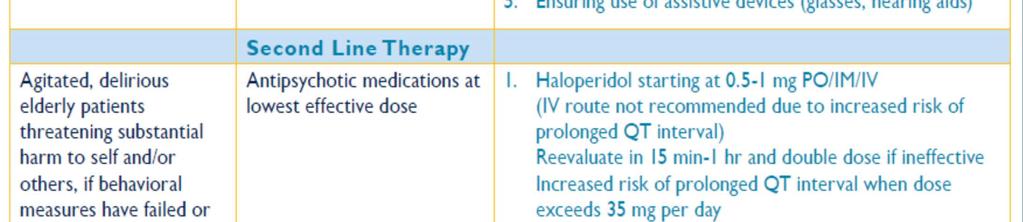
35 Which of the following drugs is the best first line treatment for delirium in the postoperative period? A. Lorazepam B. Diphenhydramine C. Haloperidol (low dose) D. None of the above
36
37 Perverse Incentives Definition: an incentive that has an unintended and undesirable result which is contrary to the interests of the incentive makers. Fall in hospital = Never Event Prevent falls = Keep patient in bed




38
39 Functional Decline and Deconditioning For every day an older adult is immobilized, it takes at least three days to regain lost function. For older adult surgical patients, one in four experiences a significant decline in function by hospital discharge and 60% experience some loss of independence* *Berian et al. JAMA Surg preprint on line July 2016
40
41 Nutritional Status of Older Adults Living in the Community or in Nursing Homes Community dwelling elders: 40 % are either malnourished or at risk Nursing home residents: Two thirds are either malnourished or at risk Kaiser MJ, 2010


42
43
44 Factors Associated with Swallowing Dysfunction and Aspiration Pneumonia Disease Related Factors Prior Stroke Neuromuscular disease GERD Incidence of Postop Aspiration Pneumonia with Age Iatrogenic Factors ET tubes Esophageal temp probes NG tubes TEE probes Medications KozlowJH, et al. Epidemiology and impact of aspiration pneumonia in patients undergoing surgery in Maryland, Crit Care Med 31: , 2003.



45

46 Transitions of Care Assess Social Support /Home Health Needs Complete Medication Review Pre-Discharge Geriatric Assessment Formal Written Discharge Instructions Communication with Primary Physician
47 Pre-Discharge Geriatric Assessment Cognition Status Presence of delirium Functional Status Mobility Fall Risk Nutritional Status Including access
48
49 Acknowledgements Sanjay Mohanty, MD (James C Thompson Geriatric Fellow at ACS) John A. Hartford Foundation American Geriatrics Society Geriatrics for Specialists Initiative American Society of Anesthesiologists American College of Surgeons NSQIP Google ACS Perioperative Guidelines.
Perioperative Care of Older Adults
 Perioperative Care of Older Adults SARAH A. WINGFIELD, MD AND THOMAS O. DALTON, MD UNIVERSITY OF TEXAS SOUTHWESTERN MEDICAL CENTER DIVISION OF GERIATRIC MEDICINE We have no disclosures. Objectives -Recognize
Perioperative Care of Older Adults SARAH A. WINGFIELD, MD AND THOMAS O. DALTON, MD UNIVERSITY OF TEXAS SOUTHWESTERN MEDICAL CENTER DIVISION OF GERIATRIC MEDICINE We have no disclosures. Objectives -Recognize
Perioperative Care of Older Adults
 Perioperative Care of Older Adults SARAH A. WINGFIELD, MD AND THOMAS O. DALTON, MD UNIVERSITY OF TEXAS SOUTHWESTERN MEDICAL CENTER DIVISION OF GERIATRIC MEDICINE We have no disclosures. Objectives -Recognize
Perioperative Care of Older Adults SARAH A. WINGFIELD, MD AND THOMAS O. DALTON, MD UNIVERSITY OF TEXAS SOUTHWESTERN MEDICAL CENTER DIVISION OF GERIATRIC MEDICINE We have no disclosures. Objectives -Recognize
Building a Standards and Verification Program for Older Adults. Melissa Hornor, MD GSI/SEGUE Session: American Geriatric Society May 20, 2017
 Building a Standards and Verification Program for Older Adults Melissa Hornor, MD GSI/SEGUE Session: American Geriatric Society May 20, 2017 Disclosures 2016-2018 ACS/JAHF James C. Thompson Geriatric Surgery
Building a Standards and Verification Program for Older Adults Melissa Hornor, MD GSI/SEGUE Session: American Geriatric Society May 20, 2017 Disclosures 2016-2018 ACS/JAHF James C. Thompson Geriatric Surgery
Why Target Delirium for Surgical Quality Improvement?
 Why Target Delirium for Surgical Quality Improvement? Tom Robinson MD FACS thomas.robinson@ucdenver.edu July 22, 2018 Disclosures Tom Robinson has no disclosures. Who Cares About the Brain? Acute Organ
Why Target Delirium for Surgical Quality Improvement? Tom Robinson MD FACS thomas.robinson@ucdenver.edu July 22, 2018 Disclosures Tom Robinson has no disclosures. Who Cares About the Brain? Acute Organ
ACS NSQIP Coalition for Quality in Geriatric Surgery Project
 ACS NSQIP Coalition for Quality in Geriatric Surgery Project Julia BerianMD, MS; Marcia McGory-Russell MD; JoAnn Coleman, DNP, ANP, ACNP, AOCN; Emily Finlayson MD, MS; Mark Katlic, MD; Sandhya Lagoo-DeenadayalanMD,
ACS NSQIP Coalition for Quality in Geriatric Surgery Project Julia BerianMD, MS; Marcia McGory-Russell MD; JoAnn Coleman, DNP, ANP, ACNP, AOCN; Emily Finlayson MD, MS; Mark Katlic, MD; Sandhya Lagoo-DeenadayalanMD,
Surgery in Frail Elders. Emily Finlayson, MD, MS Department of Surgery University of California, San Francisco September, 2011
 Surgery in Frail Elders Emily Finlayson, MD, MS Department of Surgery University of California, San Francisco September, 2011 What we re going to cover Mortality after surgery in the elderly Fact v Fantasy
Surgery in Frail Elders Emily Finlayson, MD, MS Department of Surgery University of California, San Francisco September, 2011 What we re going to cover Mortality after surgery in the elderly Fact v Fantasy
Three years of NSQIP Pilot Data What We Learned. Julia R. Berian, MD, MS
 Three years of NSQIP Pilot Data What We Learned Julia R. Berian, MD, MS Developing a Geriatric Surgery Program at Your Hospital Three years of NSQIP Pilot Data (4:30 4:40 PM) Building a Standards and Verification
Three years of NSQIP Pilot Data What We Learned Julia R. Berian, MD, MS Developing a Geriatric Surgery Program at Your Hospital Three years of NSQIP Pilot Data (4:30 4:40 PM) Building a Standards and Verification
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative
 Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Loss of Independence is associated with readmission and delayed death in older surgical patients
 Loss of Independence is associated with readmission and delayed death in older surgical patients @BerianJulia July 18, 2016 ACS NSQIP 2016 Annual Meeting Julia R. Berian MD,MS; Clifford Y. Ko MD,MS,MSHS;
Loss of Independence is associated with readmission and delayed death in older surgical patients @BerianJulia July 18, 2016 ACS NSQIP 2016 Annual Meeting Julia R. Berian MD,MS; Clifford Y. Ko MD,MS,MSHS;
New York City Development of the Geriatric Collaborative
 New York City - 2014 Development of the Geriatric Collaborative The Clinical Problem More than 50% persons age 65 years will have some surgical procedure in the remainder of his or her lifetime Outcome
New York City - 2014 Development of the Geriatric Collaborative The Clinical Problem More than 50% persons age 65 years will have some surgical procedure in the remainder of his or her lifetime Outcome
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acetaminophen, for geriatric surgical patients, 569 570 Acute kidney injury, critical care issues in geriatric patients with, 555 556
Index Note: Page numbers of article titles are in boldface type. A Acetaminophen, for geriatric surgical patients, 569 570 Acute kidney injury, critical care issues in geriatric patients with, 555 556
How to Address an Inappropriately high Readmission Rate?
 How to Address an Inappropriately high Readmission Rate? Joe Sharma, MD Associate Professor of Surgery NSQIP Surgical Champion Medical Officer CDC/DHPQ Disclosure Slide No COI and no disclosures. OBJECTIVES
How to Address an Inappropriately high Readmission Rate? Joe Sharma, MD Associate Professor of Surgery NSQIP Surgical Champion Medical Officer CDC/DHPQ Disclosure Slide No COI and no disclosures. OBJECTIVES
Quality Care for the Hospitalized Older Adult
 Quality Care for the Hospitalized Older Adult Quality Care for the Hospitalized Older Adult Shelley R McDonald, DO, PhD May 19 th, 2018 Objectives To define why the hospital is a dangerous place for older
Quality Care for the Hospitalized Older Adult Quality Care for the Hospitalized Older Adult Shelley R McDonald, DO, PhD May 19 th, 2018 Objectives To define why the hospital is a dangerous place for older
Multidisciplinary Geriatric Trauma Care Guideline
 Multidisciplinary Geriatric Trauma Care Background Traumatic injury in the geriatric population is increasing in prevalence and is associated with higher mortality and complication rates comparted to younger
Multidisciplinary Geriatric Trauma Care Background Traumatic injury in the geriatric population is increasing in prevalence and is associated with higher mortality and complication rates comparted to younger
Saman Arbabi M.D., M.P.H., F.A.C.S. Kathleen O'Connell M.D. Bryce Robinson M.D., M.S., F.A.C.S., F.C.C.M
 Form "EAST Multicenter Study Proposal" Study Title Primary investigator / Senior researcher Email of Primary investigator / Senior researcher Co-primary investigator Are you a current member of EAST? If
Form "EAST Multicenter Study Proposal" Study Title Primary investigator / Senior researcher Email of Primary investigator / Senior researcher Co-primary investigator Are you a current member of EAST? If
Guidelines for Management and Prevention of Delirium In Geriatric Trauma Patients
 Guidelines for Management and Prevention of Delirium In Geriatric Trauma Patients Objectives: Provide a guideline for recognizing and managing delirium in geriatric trauma patients. Provide a template
Guidelines for Management and Prevention of Delirium In Geriatric Trauma Patients Objectives: Provide a guideline for recognizing and managing delirium in geriatric trauma patients. Provide a template
The Coalition for Quality in Geriatric Surgery. Ronnie A. Rosenthal, MS, MD, FACS
 The Coalition for Quality in Geriatric Surgery Ronnie A. Rosenthal, MS, MD, FACS Disclosures I receive an honorarium from the Coalition for Quality in Geriatric Surgery grant The Aging U.S. Population
The Coalition for Quality in Geriatric Surgery Ronnie A. Rosenthal, MS, MD, FACS Disclosures I receive an honorarium from the Coalition for Quality in Geriatric Surgery grant The Aging U.S. Population
Delirium. Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta
 Delirium Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta Overview A. Delirium - the nature of the beast B. Significance of delirium C. An approach
Delirium Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta Overview A. Delirium - the nature of the beast B. Significance of delirium C. An approach
Enhanced Perioperative Management of Older Adults
 Enhanced Perioperative Management of Older Adults Bernardo Reyes, MD Assistant Professor of Geriatrics Charles E. Schmidt College of Medicine Disclosures None Interesting Facts Warhol was a sickly child,
Enhanced Perioperative Management of Older Adults Bernardo Reyes, MD Assistant Professor of Geriatrics Charles E. Schmidt College of Medicine Disclosures None Interesting Facts Warhol was a sickly child,
Senior Visceral Surgery Fast-Track in Colorectal Surgery The anesthetist s point of view
 Senior Visceral Surgery Fast-Track in Colorectal Surgery The anesthetist s point of view 1st Geneva International SCIENTIFIC DAY February 3 rd 2010 E. Schiffer Dept APSI, HUG 1 Fast-Track in colorectal
Senior Visceral Surgery Fast-Track in Colorectal Surgery The anesthetist s point of view 1st Geneva International SCIENTIFIC DAY February 3 rd 2010 E. Schiffer Dept APSI, HUG 1 Fast-Track in colorectal
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Adverse drug events, polypharmacy and perioperative considerations in elderly patients, 377 389 Age, and risk of postoperative urinary retention,
Note: Page numbers of article titles are in boldface type. A Adverse drug events, polypharmacy and perioperative considerations in elderly patients, 377 389 Age, and risk of postoperative urinary retention,
ACS Leadership Cliff Ko MD Ronnie Rosenthal MD. ACS Staff Kat Christensen
 ACS Leadership Cliff Ko MD Ronnie Rosenthal MD ACS Staff Kat Christensen Team Members JoAnn Coleman NP Emily Finlayson MD Mark Katlic MD Sandhya Lagoo-Deenadayalan MD Tom Robinson MD Marcia Russell MD
ACS Leadership Cliff Ko MD Ronnie Rosenthal MD ACS Staff Kat Christensen Team Members JoAnn Coleman NP Emily Finlayson MD Mark Katlic MD Sandhya Lagoo-Deenadayalan MD Tom Robinson MD Marcia Russell MD
9/19/2018. Common Medical Issues and Management in the Geriatric Trauma Patient. Disclosures. Objectives. I have no financial disclosures
 Common Medical Issues and Management in the Geriatric Trauma Patient 2018 UW Medicine EMS & Trauma Conference September 17, 2018 Joe C. Huang, M.D. Clinical Instructor Medical Director, Geriatrics-Palliative
Common Medical Issues and Management in the Geriatric Trauma Patient 2018 UW Medicine EMS & Trauma Conference September 17, 2018 Joe C. Huang, M.D. Clinical Instructor Medical Director, Geriatrics-Palliative
Delirium in the hospitalized patient
 Delirium in the hospitalized patient Jennifer A. Tarin, M.D. Department of Hospital Medicine Geriatric Health Safety Chair Colorado Permanente Medical Group UCLA Reynolds Scholar Delirium Preventing delirium
Delirium in the hospitalized patient Jennifer A. Tarin, M.D. Department of Hospital Medicine Geriatric Health Safety Chair Colorado Permanente Medical Group UCLA Reynolds Scholar Delirium Preventing delirium
Implications of Education and Prehabilitation on the Geriatric Surgical Patient
 Implications of Education and Prehabilitation on the Geriatric Surgical Patient Hufford, Theadore MD 1 ; Rubin, Jonathan MD 1 ; Al-Qudah, Ghaith 1 ; Prendergast, Michael MD 2 1 University of Illinois,
Implications of Education and Prehabilitation on the Geriatric Surgical Patient Hufford, Theadore MD 1 ; Rubin, Jonathan MD 1 ; Al-Qudah, Ghaith 1 ; Prendergast, Michael MD 2 1 University of Illinois,
Strategies to minimize delirium for hip fracture patients
 Strategies to minimize delirium for hip fracture patients Stephen L Kates, M.D. Professor and Chairman Department Date of Orthopaedic Surgery Delirium incidence Up to 61% of hip fracture patients get delirium
Strategies to minimize delirium for hip fracture patients Stephen L Kates, M.D. Professor and Chairman Department Date of Orthopaedic Surgery Delirium incidence Up to 61% of hip fracture patients get delirium
Practical Management of the Delirious Patient with Mental Retardation by the Nurse Anesthetist
 Practical Management of the Delirious Patient with Mental Retardation by the Nurse Anesthetist 1. Basic Facts on Delirium The nurse anesthetist plays an important role in prevention of delirium among surgical
Practical Management of the Delirious Patient with Mental Retardation by the Nurse Anesthetist 1. Basic Facts on Delirium The nurse anesthetist plays an important role in prevention of delirium among surgical
Improving the quality of care of patients with delirium
 Improving the quality of care of patients with delirium Alasdair MacLullich MRCP(UK), PhD Professor of Geriatric Medicine University of Edinburgh Scotland How are we doing now? We are doing badly. Difficult
Improving the quality of care of patients with delirium Alasdair MacLullich MRCP(UK), PhD Professor of Geriatric Medicine University of Edinburgh Scotland How are we doing now? We are doing badly. Difficult
Pre-operative Assessment of the Frail Elderly Person at Addenbrookes Hospital. Dr Fay J Gilder Consultant Anaesthetist
 Pre-operative Assessment of the Frail Elderly Person at Addenbrookes Hospital Dr Fay J Gilder Consultant Anaesthetist Frailty Models A multidimensional state of increased vulnerability Phenotype model
Pre-operative Assessment of the Frail Elderly Person at Addenbrookes Hospital Dr Fay J Gilder Consultant Anaesthetist Frailty Models A multidimensional state of increased vulnerability Phenotype model
Public Dissemination Effective: January 2018
 Board of Pharmacy Specialties Board Certified Geriatric Pharmacist (BCGP) Detailed Content Outline 1. GENERAL PRINCIPLES OF AGING (20%) A. Apply the knowledge of physiologic changes associated with aging
Board of Pharmacy Specialties Board Certified Geriatric Pharmacist (BCGP) Detailed Content Outline 1. GENERAL PRINCIPLES OF AGING (20%) A. Apply the knowledge of physiologic changes associated with aging
If you reduce variability in volume administration, HOW. you can reduce post-surgical complications, LOS and associated costs 1-4
 A large body of clinical evidence* demonstrates If you reduce variability in volume administration, you can reduce post-surgical complications, LOS and associated costs 1-4 Complications Too Dry Too Wet
A large body of clinical evidence* demonstrates If you reduce variability in volume administration, you can reduce post-surgical complications, LOS and associated costs 1-4 Complications Too Dry Too Wet
Designing Clinical Trials in Perioperative Sleep Medicine
 Designing Clinical Trials in Perioperative Sleep Medicine A Rationale and Pragmatic Approach Daniel J. Gottlieb, MD, MPH Director, Sleep Disorders Center, VA Boston Healthcare System Program in Sleep and
Designing Clinical Trials in Perioperative Sleep Medicine A Rationale and Pragmatic Approach Daniel J. Gottlieb, MD, MPH Director, Sleep Disorders Center, VA Boston Healthcare System Program in Sleep and
UND GERIATRIC MEDICINE FELLOWSHIP CURRICULUM ACUTE CARE
 LOCATION SITE Sanford Medical Center Fargo 5225 23rd Avenue S Fargo, ND 58104 CONTACT LEAD FACULTY MEMBER Dr. Darin Lang Darin.lang@sanfordhealth.org PROGRAM CONTACT Dr. Gunjan Manocha gunjan.dhawan@und.edu
LOCATION SITE Sanford Medical Center Fargo 5225 23rd Avenue S Fargo, ND 58104 CONTACT LEAD FACULTY MEMBER Dr. Darin Lang Darin.lang@sanfordhealth.org PROGRAM CONTACT Dr. Gunjan Manocha gunjan.dhawan@und.edu
Geriatric Hip Fracture Co-Management. Pannida Wattanapanom, M.D., FACP.
 Geriatric Hip Fracture Co-Management Pannida Wattanapanom, M.D., FACP. An 80 year old man with a hip fracture The General Medicine approach: Medical clearance for surgery Role of Geriatrician Assess caused
Geriatric Hip Fracture Co-Management Pannida Wattanapanom, M.D., FACP. An 80 year old man with a hip fracture The General Medicine approach: Medical clearance for surgery Role of Geriatrician Assess caused
The role of the Geriatrician
 Post-operative management of the older adults with cancer The role of the Geriatrician Sofia Duque Hospital Beatriz Ângelo Geriatric University Unit Faculty of Medicine of Lisbon Geriatrics Study Group
Post-operative management of the older adults with cancer The role of the Geriatrician Sofia Duque Hospital Beatriz Ângelo Geriatric University Unit Faculty of Medicine of Lisbon Geriatrics Study Group
Quality Outcomes and Financial Benefits of Nutrition Intervention. Tracy R. Smith, PhD, RD, LD Senior Clinical Manager, Abbott Nutrition
 Quality Outcomes and Financial Benefits of Nutrition Intervention Tracy R. Smith, PhD, RD, LD Senior Clinical Manager, Abbott Nutrition January 28, 2016 SHIFTING MARKET DYNAMICS PROVIDE AN OPPORTUNITY
Quality Outcomes and Financial Benefits of Nutrition Intervention Tracy R. Smith, PhD, RD, LD Senior Clinical Manager, Abbott Nutrition January 28, 2016 SHIFTING MARKET DYNAMICS PROVIDE AN OPPORTUNITY
Perso An. Geri-O. Objectives: fragility fracture. AL SUPPORT. presentation.
 10 th Annual Spring Conference Arizona Geriatrics Society Perso on-centered Care: An Interprofessional Panel Ana Sanguineti, MD Geri-O Ortho Hip Fracture Consult Service Banner Univer rsity Medical Center
10 th Annual Spring Conference Arizona Geriatrics Society Perso on-centered Care: An Interprofessional Panel Ana Sanguineti, MD Geri-O Ortho Hip Fracture Consult Service Banner Univer rsity Medical Center
Coalition for Quality in Geriatric Surgery: Creating Standards for Geriatric Surgical Care
 Coalition for Quality in Geriatric Surgery: Creating Standards for Geriatric Surgical Care Melissa Hornor, MD John A Hartford Foundation/American College of Surgeons James C. Thompson Clinical Scholar
Coalition for Quality in Geriatric Surgery: Creating Standards for Geriatric Surgical Care Melissa Hornor, MD John A Hartford Foundation/American College of Surgeons James C. Thompson Clinical Scholar
Continence, falls and the frailty syndrome. Anne Foley - BGS Bladders and Bowel Health 2012
 Continence, falls and the frailty syndrome Outline Frailty Geriatric syndromes and giants Aetiology What can be done? The future Frailty Frailty Frailty (noun): The state of being weak in health or body
Continence, falls and the frailty syndrome Outline Frailty Geriatric syndromes and giants Aetiology What can be done? The future Frailty Frailty Frailty (noun): The state of being weak in health or body
EMERGING EVIDENCE AND BEST PRACTICES TO PREVENT SSI IN COLON PROCEDURES
 EMERGING EVIDENCE AND BEST PRACTICES TO PREVENT SSI IN COLON PROCEDURES Clifford Ko, MD, MS, MSHS, FACS, FASCRS Professor of Surgery UCLA Director, ACS NSQIP, American College of Surgeons EVIDENCE Ban
EMERGING EVIDENCE AND BEST PRACTICES TO PREVENT SSI IN COLON PROCEDURES Clifford Ko, MD, MS, MSHS, FACS, FASCRS Professor of Surgery UCLA Director, ACS NSQIP, American College of Surgeons EVIDENCE Ban
Examination of Hospital-Level Variation in Preventing Post-Operative Sepsis
 Examination of Hospital-Level Variation in Preventing Post-Operative Sepsis Elizabeth Berger, MD; Sanjay Mohanty MD MS; Lynn Zhou PhD; Mark Cohen, PhD; Bruce Hall MD PhD MBA; Cliff Ko, MD MS MSHS; Karl
Examination of Hospital-Level Variation in Preventing Post-Operative Sepsis Elizabeth Berger, MD; Sanjay Mohanty MD MS; Lynn Zhou PhD; Mark Cohen, PhD; Bruce Hall MD PhD MBA; Cliff Ko, MD MS MSHS; Karl
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acute pain, outcomes assessment of evidence-based guidelines and registries, 124 125 Adverse event tracking, improved, with anesthesia
Index Note: Page numbers of article titles are in boldface type. A Acute pain, outcomes assessment of evidence-based guidelines and registries, 124 125 Adverse event tracking, improved, with anesthesia
Pain Management Protocol in Adolescent Idiopathic Spinal Fusion Reduces Length of Stay and Complications
 Pain Management Protocol in Adolescent Idiopathic Spinal Fusion Reduces Length of Stay and Complications Abstract Authors: Karen Martin, RHIT, CPHQ - Surgical Clinical Reviewer - Quality Management Analyst,
Pain Management Protocol in Adolescent Idiopathic Spinal Fusion Reduces Length of Stay and Complications Abstract Authors: Karen Martin, RHIT, CPHQ - Surgical Clinical Reviewer - Quality Management Analyst,
Efficacy of postoperative epidural analgesia Block B M, Liu S S, Rowlingson A J, Cowan A R, Cowan J A, Wu C L
 Efficacy of postoperative epidural analgesia Block B M, Liu S S, Rowlingson A J, Cowan A R, Cowan J A, Wu C L CRD summary This review evaluated the efficacy of post-operative epidural analgesia. The authors
Efficacy of postoperative epidural analgesia Block B M, Liu S S, Rowlingson A J, Cowan A R, Cowan J A, Wu C L CRD summary This review evaluated the efficacy of post-operative epidural analgesia. The authors
Delirium in the Elderly
 Delirium in the Elderly ELITE 2015 Mamata Yanamadala M.B.B.S, MS Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity
Delirium in the Elderly ELITE 2015 Mamata Yanamadala M.B.B.S, MS Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity
Sleep Apnea and ifficulty in Extubation. Jean Louis BOURGAIN May 15, 2016
 Sleep Apnea and ifficulty in Extubation Jean Louis BOURGAIN May 15, 2016 Introduction Repetitive collapse of the upper airway > sleep fragmentation, > hypoxemia, hypercapnia, > marked variations in intrathoracic
Sleep Apnea and ifficulty in Extubation Jean Louis BOURGAIN May 15, 2016 Introduction Repetitive collapse of the upper airway > sleep fragmentation, > hypoxemia, hypercapnia, > marked variations in intrathoracic
Update in Geriatrics: Choosing Wisely Primum Non Nocere
 Joseph G. Ouslander, M.D. Professor of Clinical Biomedical Science Senior Associate Dean for Geriatric Programs Chair, Department of Integrated Medical Science Charles E. Schmidt College of Medicine Professor
Joseph G. Ouslander, M.D. Professor of Clinical Biomedical Science Senior Associate Dean for Geriatric Programs Chair, Department of Integrated Medical Science Charles E. Schmidt College of Medicine Professor
Delirium. Delirium. Delirium Etiology and Pathophysiology. Fall 2018
 Three most common cognitive problems in adults 1. (acute confusion) 2. Dementia 3. Depression These problems often occur together Can you think of common stimuli for each? 1 1 State of temporary but acute
Three most common cognitive problems in adults 1. (acute confusion) 2. Dementia 3. Depression These problems often occur together Can you think of common stimuli for each? 1 1 State of temporary but acute
Multimodal Approach for Managing Postoperative Ileus: Role of Health- System Pharmacists (ACPE program H01P)
") 1. In the normal gastrointestinal tract, what percent of nutrient absorption occurs in the jejunum? a. 20%. b. 40%. c. 70%. d. 90%. 2. According to Dr. Erstad, the four components of gastrointestinal control
1. In the normal gastrointestinal tract, what percent of nutrient absorption occurs in the jejunum? a. 20%. b. 40%. c. 70%. d. 90%. 2. According to Dr. Erstad, the four components of gastrointestinal control
Delirium and Dementia
 Delirium and Dementia Elder Friendly Care in Acute Care Seniors Health Strategic Clinical Network Acute Care Stress Blender Poor Poor sleep At-Risk Older Adult TREAT CAUSE immediately & aggressively. Increased
Delirium and Dementia Elder Friendly Care in Acute Care Seniors Health Strategic Clinical Network Acute Care Stress Blender Poor Poor sleep At-Risk Older Adult TREAT CAUSE immediately & aggressively. Increased
Geriatric Grand Rounds
 Geriatric Grand Rounds Prevalence and Risk Factors of Delirium in Older Patients Admitted to a Community Based Acute Care Hospital Tuesday, October 27, 2009 12:00 noon Dr. Bill Black Auditorium Glenrose
Geriatric Grand Rounds Prevalence and Risk Factors of Delirium in Older Patients Admitted to a Community Based Acute Care Hospital Tuesday, October 27, 2009 12:00 noon Dr. Bill Black Auditorium Glenrose
Charles Bernick, MD, MPH Cleveland Clinic Lou Ruvo Center for Brain Health June 2, 2018
 Charles Bernick, MD, MPH Cleveland Clinic Lou Ruvo Center for Brain Health June 2, 2018 Delirium common Prolongs hospitalization Worsens dementia ( if you survive) Increased risk of institutionalization
Charles Bernick, MD, MPH Cleveland Clinic Lou Ruvo Center for Brain Health June 2, 2018 Delirium common Prolongs hospitalization Worsens dementia ( if you survive) Increased risk of institutionalization
7/18/2014 به نام خداوند جان و خرد
 1 به نام خداوند جان و خرد NURSING CARE in GERIATRIC SURGERY A. Shahrokhi Qazvin Nursing & Midwifery School 3 Natural, progressive & irreversible alterations in aged people result in significant physiological
1 به نام خداوند جان و خرد NURSING CARE in GERIATRIC SURGERY A. Shahrokhi Qazvin Nursing & Midwifery School 3 Natural, progressive & irreversible alterations in aged people result in significant physiological
Improving Colectomy Outcomes in the Enhanced Recovery In NSQIP (ERIN) Pilot
 Pilot") Improving Colectomy Outcomes in the Enhanced Recovery In NSQIP (ERIN) Pilot Julia R. BerianMD; Kristen A. Ban MD; Sanjay MohantyMD,MS; Jennifer L. ParuchMD,MS; Clifford Y. KoMD,MS,MSHS; Julie K. Thacker
Improving Colectomy Outcomes in the Enhanced Recovery In NSQIP (ERIN) Pilot Julia R. BerianMD; Kristen A. Ban MD; Sanjay MohantyMD,MS; Jennifer L. ParuchMD,MS; Clifford Y. KoMD,MS,MSHS; Julie K. Thacker
Is Readmission a Good Quality Measure for Surgical Care? Examining the Underlying Reasons for Readmissions after Surgery at ACS NSQIP Hospitals
 Is Readmission a Good Quality Measure for Surgical Care? Examining the Underlying Reasons for Readmissions after Surgery at ACS NSQIP Hospitals Mila H. Ju, MD, MS Ryan P. Merkow, MD, MS Jeanette W. Chung,
Is Readmission a Good Quality Measure for Surgical Care? Examining the Underlying Reasons for Readmissions after Surgery at ACS NSQIP Hospitals Mila H. Ju, MD, MS Ryan P. Merkow, MD, MS Jeanette W. Chung,
Delirium in the Elderly
 Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
Enhanced Recovery after Surgery - A Colorectal Perspective. R Sim Centre for Advanced Laparoscopic Surgery, TTSH
 Enhanced Recovery after Surgery - A Colorectal Perspective R Sim Centre for Advanced Laparoscopic Surgery, TTSH Conventional Surgery Postop care Nasogastric tube Enteral feeds when ileus resolves Opioid
Enhanced Recovery after Surgery - A Colorectal Perspective R Sim Centre for Advanced Laparoscopic Surgery, TTSH Conventional Surgery Postop care Nasogastric tube Enteral feeds when ileus resolves Opioid
譫妄症 (Delirium) Objectives. Epidemiology. Delirium. DSM-5 Diagnostic Criteria. Prognosis 台大醫院老年醫學部陳人豪 2016/8/28
 Objectives. Epidemiology. Delirium. DSM-5 Diagnostic Criteria. Prognosis 台大醫院老年醫學部陳人豪 2016/8/28") 譫妄症 (Delirium) 台大醫院老年醫學部陳人豪 2016/8/28 Objectives Delirium Epidemiology Etiology Diagnosis Evaluation and Management Postoperative delirium Delirium (and acute problematic behavior) in the longterm care
譫妄症 (Delirium) 台大醫院老年醫學部陳人豪 2016/8/28 Objectives Delirium Epidemiology Etiology Diagnosis Evaluation and Management Postoperative delirium Delirium (and acute problematic behavior) in the longterm care
LINKS OF INTEREST DISCLOSURE
 LINKS OF INTEREST DISCLOSURE Name of the speaker: Sarah L. Krein I have no link of interest. www.sf2h.net 7, 8 et 9 juin 2017 And what about getting rid of catheter-associated urinary tract infections?
LINKS OF INTEREST DISCLOSURE Name of the speaker: Sarah L. Krein I have no link of interest. www.sf2h.net 7, 8 et 9 juin 2017 And what about getting rid of catheter-associated urinary tract infections?
Death by Bedrest: The Perils of The Hospital
 Death by Bedrest: The Perils of The Hospital Mindy Fain, MD Professor of Clinical Medicine Director, Arizona Reynolds Program of Applied Geriatrics Section Head, Geriatrics & Gerontology University of
Death by Bedrest: The Perils of The Hospital Mindy Fain, MD Professor of Clinical Medicine Director, Arizona Reynolds Program of Applied Geriatrics Section Head, Geriatrics & Gerontology University of
HOMES AND SENIORS SERVICES. APPROVAL DATE: February 2011 REVISION DATE: January 2015; July 2018
 POLICY: Page 1 of 6 A resident requiring enteral (tube) feeding as a sole source or adjunctive nutrition support have access to a comprehensive enteral feeding program and receive appropriate support from
POLICY: Page 1 of 6 A resident requiring enteral (tube) feeding as a sole source or adjunctive nutrition support have access to a comprehensive enteral feeding program and receive appropriate support from
Intro Who should read this document 2 Key practice points 2 What is new in this version 3 Background 3 Guideline Subsection headings
 Enhanced Recovery for Major Urology and Gynaecological Classification: Clinical Guideline Lead Author: Dr Dominic O Connor Additional author(s): Jane Kingham Authors Division: Anaesthesia Unique ID: DDCAna3(12)
Enhanced Recovery for Major Urology and Gynaecological Classification: Clinical Guideline Lead Author: Dr Dominic O Connor Additional author(s): Jane Kingham Authors Division: Anaesthesia Unique ID: DDCAna3(12)
Aging Research Day March 8, 2012
 Aging Research Day March 8, 2012 Heidi R. Wierman, MD Mane Medical Center Division Director, Geriatrics Assistant Professor, Tufts School of Medicine Overview 1.Brief Delirium Review 2.Describe HELP function
Aging Research Day March 8, 2012 Heidi R. Wierman, MD Mane Medical Center Division Director, Geriatrics Assistant Professor, Tufts School of Medicine Overview 1.Brief Delirium Review 2.Describe HELP function
5 older patients become. What is delirium? (Acute confusional state) Where We ve Been and
 Where We ve Been and") Update on Delirium: Where We ve Been and Where We re Going Sharon K. Inouye, M.D., M.P.H. M PH Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley F. Levy
Update on Delirium: Where We ve Been and Where We re Going Sharon K. Inouye, M.D., M.P.H. M PH Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley F. Levy
Pre-op Clinical Triad - Pulmonary. Sammy Pedram, MD FCCP Assistant Professor of Medicine Pulmonary & Critical Care Medicine March 16, 2018
 Pre-op Clinical Triad - Pulmonary Sammy Pedram, MD FCCP Assistant Professor of Medicine Pulmonary & Critical Care Medicine March 16, 2018 Disclosures none Case Mr. G is a 64 year-old man who presents to
Pre-op Clinical Triad - Pulmonary Sammy Pedram, MD FCCP Assistant Professor of Medicine Pulmonary & Critical Care Medicine March 16, 2018 Disclosures none Case Mr. G is a 64 year-old man who presents to
2018 ABG QCDR Measure Specifications. (changes to old measures from 2017 in red font)
") 2018 ABG QCDR Measure Specifications (changes to old measures from 2017 in red font) Calculations Reporting Rate = Performance Met + Performance Not Met + Denominator Exceptions + Denominator Exclusions
2018 ABG QCDR Measure Specifications (changes to old measures from 2017 in red font) Calculations Reporting Rate = Performance Met + Performance Not Met + Denominator Exceptions + Denominator Exclusions
Updates in Geriatrics. Christopher R. Carpenter, MD, FACEP, AGSF October 24, 2018
 Updates in Geriatrics Christopher R. Carpenter, MD, FACEP, AGSF October 24, 2018 Disclosure of Relationships Deputy Editor-in-Chief Academic Emergency Medicine Editorial Board ACP Journal Club Journal
Updates in Geriatrics Christopher R. Carpenter, MD, FACEP, AGSF October 24, 2018 Disclosure of Relationships Deputy Editor-in-Chief Academic Emergency Medicine Editorial Board ACP Journal Club Journal
Faculty/Presenter Disclosure
 Faculty/Presenter Disclosure Faculty: Dr. Anthony Kerigan Relationships with commercial interests:* Grants/Research Support: NONE Speakers Bureau/Honoraria: NONE Consulting Fees: NONE Other: NONE Meeting
Faculty/Presenter Disclosure Faculty: Dr. Anthony Kerigan Relationships with commercial interests:* Grants/Research Support: NONE Speakers Bureau/Honoraria: NONE Consulting Fees: NONE Other: NONE Meeting
Laparoscopic Colorectal Surgery
 Laparoscopic Colorectal Surgery 20 th November 2015 Dr Adam Cichowitz General Surgeon Laparoscopic Colorectal Surgery Introduced in early 1990s Uptake slow Steep learning curve Requirement for equipment
Laparoscopic Colorectal Surgery 20 th November 2015 Dr Adam Cichowitz General Surgeon Laparoscopic Colorectal Surgery Introduced in early 1990s Uptake slow Steep learning curve Requirement for equipment
JAMA, January 11, 2012 Vol 307, No. 2
 JAMA, January 11, 2012 Vol 307, No. 2 Dementia is associated with increased rates and often poorer outcomes of hospitalization Worsening cognitive status Adequate chronic disease management is more difficult
JAMA, January 11, 2012 Vol 307, No. 2 Dementia is associated with increased rates and often poorer outcomes of hospitalization Worsening cognitive status Adequate chronic disease management is more difficult
Gastrointestinal Feedings Post Op: What s the deal on beginning oral feedings?
 Gastrointestinal Feedings Post Op: What s the deal on beginning oral feedings? Kate Willcutts, DCN, RD, CNSC University of Virginia Health System Charlottesville, VA kfw3w@virginia.edu Objectives 1. Discuss
Gastrointestinal Feedings Post Op: What s the deal on beginning oral feedings? Kate Willcutts, DCN, RD, CNSC University of Virginia Health System Charlottesville, VA kfw3w@virginia.edu Objectives 1. Discuss
Effect of Ortho-Geriatric Co-Management on Hip Fractures
 Effect of Ortho-Geriatric Co-Management on Hip Fractures Kenji Shigemoto Takeshi Sawaguchi Daigo Sakagoshi Kenichi Goshima Yu Hatsuchi Dept. Orthop. Surg. Toyama Municipal Hospital, Toyama, Japan Purpose
Effect of Ortho-Geriatric Co-Management on Hip Fractures Kenji Shigemoto Takeshi Sawaguchi Daigo Sakagoshi Kenichi Goshima Yu Hatsuchi Dept. Orthop. Surg. Toyama Municipal Hospital, Toyama, Japan Purpose
Delirium. Dr. John Puxty
 Delirium Dr. John Puxty Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors, causes and main
Delirium Dr. John Puxty Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors, causes and main
Background Information
 Background Information Age plays an important role in patients selection for spinal surgeries as it is associated with increased morbidity and mortality Consequences of suffering postoperative complications
Background Information Age plays an important role in patients selection for spinal surgeries as it is associated with increased morbidity and mortality Consequences of suffering postoperative complications
How to Address an Inappropriately high Mortality Rate? Joe Sharma, MD Associate Professor of Surgery NSQIP Surgical Champion
 How to Address an Inappropriately high Mortality Rate? Joe Sharma, MD Associate Professor of Surgery NSQIP Surgical Champion Disclosure Slide No COI and no disclosures. Hospital Mortality rate : is it
How to Address an Inappropriately high Mortality Rate? Joe Sharma, MD Associate Professor of Surgery NSQIP Surgical Champion Disclosure Slide No COI and no disclosures. Hospital Mortality rate : is it
Identifying patients at risk of delirium: a project for patients undergoing elective orthopedic surgery. The next steps in orthogeriatrics
 Identifying patients at risk of delirium: a project for patients undergoing elective orthopedic surgery Dr. John Joanisse, Chantal Chabot NP The next steps in orthogeriatrics Background More than 8 years
Identifying patients at risk of delirium: a project for patients undergoing elective orthopedic surgery Dr. John Joanisse, Chantal Chabot NP The next steps in orthogeriatrics Background More than 8 years
Geriatric Medicine Clerkship Orientation. Aval-Na Ree Green (modified by Huai Cheng)
") Geriatric Medicine Clerkship Orientation Aval-Na Ree Green (modified by Huai Cheng) Welcome! Goals The geriatric clerkship is designed to prepare medical students to provide evidence-based, competent,
Geriatric Medicine Clerkship Orientation Aval-Na Ree Green (modified by Huai Cheng) Welcome! Goals The geriatric clerkship is designed to prepare medical students to provide evidence-based, competent,
Anesthesia For The Elderly. Yasser Sakawi, M.D. Associate Professor Anesthesiology Department
 Anesthesia For The Elderly Yasser Sakawi, M.D. Associate Professor Anesthesiology Department Topics of Discussion General concepts and definitions Aging and general organ function Cardiopulmonary function
Anesthesia For The Elderly Yasser Sakawi, M.D. Associate Professor Anesthesiology Department Topics of Discussion General concepts and definitions Aging and general organ function Cardiopulmonary function
General anesthetics. Dr. Shamil AL-Noaimy Lecturer of Pharmacology Dept. of Pharmacology College of Medicine
 General anesthetics Dr. Shamil AL-Noaimy Lecturer of Pharmacology Dept. of Pharmacology College of Medicine Rationale General anesthesia is essential to surgical practice, because it renders patients analgesic,
General anesthetics Dr. Shamil AL-Noaimy Lecturer of Pharmacology Dept. of Pharmacology College of Medicine Rationale General anesthesia is essential to surgical practice, because it renders patients analgesic,
The Geriatrician in the Trauma Service. Trauma Quality Improvement Program (TQIP) Annual Scientific Meeting and Training 2013
 Annual Scientific Meeting and Training 2013") The Geriatrician in the Trauma Service Trauma Quality Improvement Program (TQIP) Annual Scientific Meeting and Training 2013 Challenges of the Geriatric Trauma Patient Challenges of the Geriatric Patient
The Geriatrician in the Trauma Service Trauma Quality Improvement Program (TQIP) Annual Scientific Meeting and Training 2013 Challenges of the Geriatric Trauma Patient Challenges of the Geriatric Patient
Preventing Postoperative Cognitive Decline in the Elderly
 Preventing Postoperative Cognitive Decline in the Elderly Alex Bekker, M.D., Ph.D Professor and Chair Department of Anesthesiology Rutgers New Jersey Medical School "My brain, that's my second favorite
Preventing Postoperative Cognitive Decline in the Elderly Alex Bekker, M.D., Ph.D Professor and Chair Department of Anesthesiology Rutgers New Jersey Medical School "My brain, that's my second favorite
Creating an Early Recovery Order Set for Colorectal Surgery-It s the Journey as well as the Destination
 Creating an Early Recovery Order Set for Colorectal Surgery-It s the Journey as well as the Destination Jason D. Sciarretta, MD, FACS Grand Strand Medical Center, Myrtle Beach, SC University of South Carolina
Creating an Early Recovery Order Set for Colorectal Surgery-It s the Journey as well as the Destination Jason D. Sciarretta, MD, FACS Grand Strand Medical Center, Myrtle Beach, SC University of South Carolina
Fast Track Surgery and Surgical Carepath in Optimising Colorectal Surgery. R Sim Centre for Advanced Laparoscopic Surgery, TTSH
 Fast Track Surgery and Surgical Carepath in Optimising Colorectal Surgery R Sim Centre for Advanced Laparoscopic Surgery, TTSH Conventional Surgery Postop care Nasogastric tube Enteral feeds when ileus
Fast Track Surgery and Surgical Carepath in Optimising Colorectal Surgery R Sim Centre for Advanced Laparoscopic Surgery, TTSH Conventional Surgery Postop care Nasogastric tube Enteral feeds when ileus
Chapter 01 Introduction
 Chapter 01 Introduction Defining the Elderly There is no universally accepted age cut-off defining elderly. This reflects the fact that chronological age itself is less important than biological events
Chapter 01 Introduction Defining the Elderly There is no universally accepted age cut-off defining elderly. This reflects the fact that chronological age itself is less important than biological events
Development and Utilization of Standardized Hip Fracture Guidelines
 Development and Utilization of Standardized Hip Fracture Guidelines Sally Knight RN Clinical Quality Nurse Lori Smith RN Clinical Quality Nurse Deborah Newall RN Orthopedic Program Coordinator Wallace
Development and Utilization of Standardized Hip Fracture Guidelines Sally Knight RN Clinical Quality Nurse Lori Smith RN Clinical Quality Nurse Deborah Newall RN Orthopedic Program Coordinator Wallace
Update - Delirium in Elders
 Update - Delirium in Elders Impact Recognition Prevention, and Management Michael J. Lichtenstein, MD F. Carter Pannill, Jr. Professor of Medicine Chief, Division of Geriatrics, Gerontology and Palliative
Update - Delirium in Elders Impact Recognition Prevention, and Management Michael J. Lichtenstein, MD F. Carter Pannill, Jr. Professor of Medicine Chief, Division of Geriatrics, Gerontology and Palliative
Day 1 10:50. Panel Discussions/Group Photo Coffee/Tea Break 11:15-11:30 (Networking) Different types of. Anesthesia. Day 2
 Different types of. Anesthesia. Day 2") Day 1 Evening Sessions Morning Sessions Reception/Registration 08:3009:30 General Session Time 09:3009:55 Inaugural Address 10:0010:25 Keynote/Plenary Talk 1 Least of 3 Keynote/Plenary 10:25Talks 10:50
Day 1 Evening Sessions Morning Sessions Reception/Registration 08:3009:30 General Session Time 09:3009:55 Inaugural Address 10:0010:25 Keynote/Plenary Talk 1 Least of 3 Keynote/Plenary 10:25Talks 10:50
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Activated partial thromboplastin time abnormality, perioperative approach to, 104 105 Acute kidney injury, perioperative, 89 99 early
Index Note: Page numbers of article titles are in boldface type. A Activated partial thromboplastin time abnormality, perioperative approach to, 104 105 Acute kidney injury, perioperative, 89 99 early
POLYPHARMACY IN OLDER ADULTS AND BEERS CRITERIA UPDATE
 POLYPHARMACY IN OLDER ADULTS AND BEERS CRITERIA UPDATE Jeannie Kim Lee, PharmD, BCPS, CGP Clinical Pharmacy Director College of Pharmacy The University of Arizona Learning Objectives: State the risks of
POLYPHARMACY IN OLDER ADULTS AND BEERS CRITERIA UPDATE Jeannie Kim Lee, PharmD, BCPS, CGP Clinical Pharmacy Director College of Pharmacy The University of Arizona Learning Objectives: State the risks of
Click to edit Master subtitle style
 Does Enhanced Recovery Improve Outcomes? Click to edit Master subtitle style Kaare Weber, MD Director of Surgery Associate Medical Director, Surgery A MEMBER OF THE MONTEFIORE HEALTH SYSTEM mes? Click
Does Enhanced Recovery Improve Outcomes? Click to edit Master subtitle style Kaare Weber, MD Director of Surgery Associate Medical Director, Surgery A MEMBER OF THE MONTEFIORE HEALTH SYSTEM mes? Click
In 2009, more than 37% of all interventional and
 CE 2.5 HOURS Continuing Education Postoperative Delirium in Elderly Patients A review of risk factors, assessment tools, and strategies to minimize this frequent surgical complication. OVERVIEW: Nearly
CE 2.5 HOURS Continuing Education Postoperative Delirium in Elderly Patients A review of risk factors, assessment tools, and strategies to minimize this frequent surgical complication. OVERVIEW: Nearly
Geriatric Pharmacology
 Geriatric Pharmacology Janice Scheufler R.Ph.,PharmD, FASCP Clinical Pharmacist Hospice of the Western Reserve Objectives List three risk factors for adverse drug events in the elderly Discuss two physiological
Geriatric Pharmacology Janice Scheufler R.Ph.,PharmD, FASCP Clinical Pharmacist Hospice of the Western Reserve Objectives List three risk factors for adverse drug events in the elderly Discuss two physiological
Perioperative Pain Management
 Perioperative Pain Management Overview and Update As defined by the Anesthesiologist's Task Force on Acute Pain Management are from the practice guidelines from the American Society of Anesthesiologists
Perioperative Pain Management Overview and Update As defined by the Anesthesiologist's Task Force on Acute Pain Management are from the practice guidelines from the American Society of Anesthesiologists
The following content was supplied by the author as supporting material and has not been copy-edited or verified by JBJS.
 Page 1 The following content was supplied by the author as supporting material and has not been copy-edited or verified by JBJS. Appendix TABLE E-1 Care-Module Trigger Events That May Indicate an Adverse
Page 1 The following content was supplied by the author as supporting material and has not been copy-edited or verified by JBJS. Appendix TABLE E-1 Care-Module Trigger Events That May Indicate an Adverse
PAAQS Reference Guide
 Q. 1 Patient's Date of Birth (DOB) *Required Enter patient's date of birth PAAQS Reference Guide Q. 2 Starting Anesthesiologist *Required Record the anesthesiologist that started the case Q. 3 Reporting
Q. 1 Patient's Date of Birth (DOB) *Required Enter patient's date of birth PAAQS Reference Guide Q. 2 Starting Anesthesiologist *Required Record the anesthesiologist that started the case Q. 3 Reporting
Delirium in Hospital Care
 Delirium in Hospital Care Dr John Puxty 1 Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors,
Delirium in Hospital Care Dr John Puxty 1 Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors,
Clinical Care Team approach to management of key conditions
 Clinical Care Team approach to management of key conditions BJD Ho Chi Minh City Nov 30, 2012 Kristina Åkesson, MD, PhD Dept of Orthopedics Malmö University Hospital Lund University Malmö, Sweden Multidisciplinary
Clinical Care Team approach to management of key conditions BJD Ho Chi Minh City Nov 30, 2012 Kristina Åkesson, MD, PhD Dept of Orthopedics Malmö University Hospital Lund University Malmö, Sweden Multidisciplinary
Delirium assessment and management. Dr Kim Jeffs Northern Health
 Delirium assessment and management Dr Kim Jeffs Northern Health What do you need to know? Epidemiology How big is the problem? Who is at risk? Assessment Tools for diagnosis Prevention Evidence base Management
Delirium assessment and management Dr Kim Jeffs Northern Health What do you need to know? Epidemiology How big is the problem? Who is at risk? Assessment Tools for diagnosis Prevention Evidence base Management
POLICY All patients will be assessed for risk factors associated with OSA prior to any surgical procedures.
 Revised Date: Page: 1 of 7 SCOPE All Pre-Admission Testing (PAT) and Same Day Surgery (SDS) nurses at HRMC. PURPOSE The purpose of this policy is to provide guidelines for identifying surgical patients
Revised Date: Page: 1 of 7 SCOPE All Pre-Admission Testing (PAT) and Same Day Surgery (SDS) nurses at HRMC. PURPOSE The purpose of this policy is to provide guidelines for identifying surgical patients
Objectives 9/7/2012. Optimizing Analgesia to Enhance the Recovery After Surgery CME FACULTY DISCLOSURE
 Optimizing Analgesia to Enhance the Recovery After Surgery Francesco Carli, M.D.. McGill University, Montreal, QC, Canada. ASPMN, Baltimore, 2012 CME FACULTY DISCLOSURE Francesco Carli has no affiliation
Optimizing Analgesia to Enhance the Recovery After Surgery Francesco Carli, M.D.. McGill University, Montreal, QC, Canada. ASPMN, Baltimore, 2012 CME FACULTY DISCLOSURE Francesco Carli has no affiliation