Early Identification and Reduction of Patient Risk: The Cedars-Sinai Frail Elders Program
|
|
|
- Ethel Wright
- 5 years ago
- Views:
Transcription
1 Early Identification and Reduction of Patient Risk: The Cedars-Sinai Frail Elders Program Jeff Borenstein, MD, Medical Director Applied Health Services Research Harriet Aronow, Ph.D., Research Scientist, Nursing Research & Development June 20, 2013

2 2
3 Growing Challenge/Converging Storms Increasing population combined with aging population More people survive life-threatening illness/injury with resulting burden of chronic illness and/or disability By 2050 over 20 million people in U.S. aged Male Female <5 <5 <
4 The Hospital Experience by Age Discharges FY 2012 Age Group Length of Stay All Cause 30d Readmission Case Mix Index All Discharges 18+ (N = 46,470) % (n = 14,195; 30.5%) % (n = 13,533; 29.1%) % (n = 13,786; 29.7%) % (n = 4,956; 10.7%) % Focus on 85+ Average age 89.5 years; n=594 aged 95 or older (12.1% of the 85+) 58.6% Female 56.6% Major or Extreme Admission Severity 94.8% Discharged Alive; 33.1% Home/Self-Care; 29.4% Home/Home Health Care; 27.5% Skilled or Acute Rehab 82.2% with NO days in Intensive Care; Average LOS in ICU = 0.66 days (3.72 days for those with any days) 4
5 What do we know about vulnerable, older patients? Adverse events during hospital stays increase with age 1 Rates were markedly higher in the elderly Approximately 12% of patients 70 years and older lost independence in one or more ADLs during hospitalization 2 Permanent loss in ADL function was associated with older ages Older age is a risk factor for delirium, associated with Higher rates of death, medical complications and prolongation of hospital stay 3,4 Greater risk of re-hospitalization and institutionalization 1 Brennan TA et al. NEJM 1991;324(6): Inouye SK. et al. Ann Int Med 1990;113: Covinsky KE et al. JAGS 2003; 51(4): Podrazik PM Med Clin N Am 92 (2008) *Excluding Rehabilitation, Ob-Gyn, Pediatrics. 5
6 Delivery Model Redesign Engagement Best Practices Inpatient Clinical Decision Support Transparency COPD Pneumonia Hip & Knee Replacement Non-Malignant Gyn Stroke ACS/AMI A Fib Chest Pain Sepsis Spine Surgery Cellulitis Gastroenteritis/Diverticulitis ICU/Monitored Beds/LOC Urology (Male) Stability Criteria for Discharge Respiratory Therapy CS Medicine Best Practices As part of Cedars-Sinai Medicine, evidence-based medicine is applied to all care. Aim is to improve the utilization profile without sacrificing quality. Over 50 teams with more than 300 physicians have been convened to establish these best practices that consider appropriateness, efficiency, effectiveness, progression and outcomes across the entire continuum. Best practices development and implementation are Continuum of Care Preventing early inductions PTCA appropriateness End of Life including a comprehensive Human Caring Strategy Frailty Headaches Hypertension Heart Failure Back Pain Diabetes Pre-procedure testing guidelines Chronic Pain Cancer Referral appropriateness from PMD to Specialists Appropriateness of Utilization Imaging Ambulatory Surgery and Procedures Physical Therapy Pharmacy (high cost therapeutics and greater use of generics) Pathology/High Cost Lab Tests/Duplicate testing Transfusion of Blood Products focused at high volume and/or high impact conditions or services. We look for opportunities to reduce utilization and therefore cost by eliminating aspects of diagnosis, treatment and care that are not supported by evidence. Sometimes doing the right thing for patients takes more resources rather than fewer but often, the same or better outcomes Within the Medical Center, over 80% of the discharges are impacted by best practices.

7 Nurses are the primary caregivers for older patients in hospitals Nurses are generally not fully prepared to care for older patients Central Role of Nursing Nursing models can improve older patients care and decrease hospital costs Nursing can be a focal point for stimulating interprofessional care 7
8 Our Work at CSMC Steps to Improve System of Care Prepare Nursing Leaders and Champions UCLA research collaboration Gerontological Nursing Certification class NICHE Leadership Training Program Become NICHE hospital Collaborative, Interprofessional, Cross-cutting and Cross-setting Improvement Projects 8
9 Research/Quality Improvement Question Can an interprofessional team improve patient outcomes by identifying frail older adults and implementing preventive care plans in hospitalized older adults? 9
10 Team Based Design V.P. & Chief Nursing Officer Chairman Department of Medicine Research Scientist Nurse Managers Data analyst Medical Director, Health Services Research Nurse Education Coordinators Palliative Care Practitioner Nursing Directors (3) Private Physicians Staff nurses Pharmacy leadership Psychiatric Liaison Acute Rehabilitation services Acute (PT/OT/SLP) therapy Respiratory therapy Information specialists in EHR HID Clinical Social Worker Case Management 10
11 Dual Project Tracks 1. Clinical Practice Enhancement / Improvement Early identification of frailty Prompt provision of care Follow-along and discharge hand-off Spread and sustainability of assessment and interventions 2. Evidence Based Research / Evaluation Epidemiology of Frailty Evaluation of interventions / patient outcomes Evaluation of organizational outcomes Training, culture, infrastructure i.e. workflow 11
12 Project Aim Develop a preventive approach to frailty in acute care settings that would result in improved patient outcomes for at risk adults Reliable identification of risk factors and frailty criteria Design of clinical care and supportive care interventions based on individualized needs Improved care team communication, patient/family communication and coordination Desired outcomes 12 Decreased adverse events Decreased unplanned readmissions Improved progression of care and patient status Improved care transitions Improved patient/family satisfaction
13 Prospective Cohort Study of Frailty in Acute Hospital Care Patient Risks and Adverse Outcomes Purpose Create local evidence of the cross-cutting frailty factor Demonstrate that we could assess frailty risk in a timely manner Identify specific associations of risk factors and adverse hospital outcomes Is the prevalence of these patients sufficient to support a unit-based TOC? 13
14 Mixed Methods Derivation of risk factors/ literature + consensus process Patient screening and interviews Three weeks Prospective admissions Within 48 hours of admission Chart review 14
15 15 Baseline Risk Factors Age 80+ Admitted from SNF Prior unplanned admission w/in 30 days 2+ unplanned admissions w/in 6 months 4+ active, chronic conditions with one or more not well controlled 7+ prescription meds POA Unintentional recent weight loss PEG tube POA Decubitus ulcer(s) POA Katz Index of ADL Independence PHQ-2 screen for depression Cognitive impairment (per BIMS or interviewer) and the 13 questions of the Vulnerable Elders Survey
16 Other Chart-based Measures RN Assessments PT mobility protocol OT ADL protocol SLP Communication protocol Dysphagia (swallowing) protocol DC Planning screen Social Work/Case Management referral Modified Beers List Medications* Analgesics Antidepressants Urinary prescriptions Muscle relaxants Major tranquilizers GI prescriptions Antihypertensives Cardiac prescriptions Antihistamines Total number of MBL meds 1+ MBL medication * medications with known risks among older adults, listed by drug category Co-morbid Conditions Present on Admission CharlsonComorbidity Index Other co-morbid conditions associated with Frailty Anemia Deconditioning Dehydration Delirium (per chart, CAM data not reliable) Hemorrhagic CVA Hyponatremia Altered mental status 16
17 Outcome Measures Hospital-acquired infections pneumonia catheter-associated UTI iv catheter infection bacteremia or sepsis cellulitis MRSA/VRE Clostridium difficile colitis Hospital-acquired pressure ulcers Falls Procedure-associated complication Transfer to a higher level of care (e.g., wards to ICU) Death Readmission by 7, 14, and 30 days post-discharge 17
18 Results: Demographics and Hospital Care 214 patients interviewed in three weeks 58% female Mean age = 75 (±13) years 31% non-caucasian Majority (74%) discharged home 22% with home health care referral Average length of stay = 6 (±6) days
19 Prevalence of Risk Factors Feeding Tube POA Decubitus Ulcer(s) POA Admitted from a Skilled Nursing Evidence of Recent Unintended 2+ Hospital Admissions with 180 days Cognitive Impairment by BIMS score or 1+ Unplanned Hospital Admission PHQ-2 Depression Screen Positive Katz Activities of Daily Living (ADL) Age 80 years or older 7+ Prescription Medications Present 4+ Active Chronic Conditions, with 1+ 0% 10% 20% 30% 40% 50% 60% 70% 80% 19
20 Risk Factor Frailty Risk Factors and Outcomes Direction Outcome Cluster Recent Unintentional Weight Loss Falls, HAPU, Procedural Potentially Inappropriate Medications Complications, Transfer to ICU Cognitive Impairment 4 active co-morbid conditions Anemia Cognitive Impairment Decubitus ulcer present on admission Functional Impairment Malnutrition Recent Unintentional Weight Loss Anemia Decubitus ulcer present at admission Functional impairment Hyponatremia 20 Hospital Acquired Infections, Adverse Drug Events, LOS >7 days Readmission within 30 days
21 Incidence of Adverse Events and Number of Patient Frailty Characteristics % Adverse Hospital Events % Readmission within 30 days Number of frailty characteristics Number of frailty characteristics 21
22 Conclusions No unified theory of frailty Outcome clusters suggest specific team interventions Ample evidence on which to design a test of change 22
23 SPICES 1988; Terry Fulmer PhD, RN, FAAN Framework for assessing older adults S = Sleep disorders P= Problems with eating I= Incontinence C= Confusion E= Evidence of falls S = Skin breakdown 23
24 Frailty Inpatient Intervention Overview 24
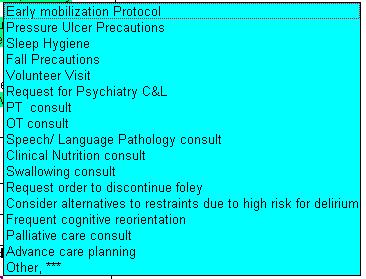
25 Table of Assessments and Interventions TEAM ASSESSMENT Delirium Risks Sweet-16 score <14 = cognitive impairment Hearing or vision problems Pain that is intolerable or greatly bothers Nausea that is intolerable or greatly bothers Problems sleeping Foley / restraints present CAM (delirium screen) positive Risks for Adverse Hospital Outcomes Braden score <=18, recent weight loss, Beers List medications Morse score >=45,, Beers List medications Lack of Social Support Lack of ADL s Katz Nutritional triggers met PT and/or OT triggers met Communication triggers met Swallowing triggers met Pharmacy assessment Beers List medication Non-Beer s list medication SUGGESTED INTERVENTIONS Delirium prevention protocol Sleep hygiene Early mobilization protocol Mealtime mates, Volunteer visit Management of Beers List medications Frequent cognitive reorientation by Nursing Unit staff Discontinue Foley, use restraint alternatives, if possible Treatment for unremitting symptoms (e.g., pain management) Psychiatry Consultation/Delirium Prevention Protocol Tailored care plan Pressure ulcer prevention protocol Fall prevention protocol Chaplaincy Physical and Occupational therapy consult Nutrition consult Physical and/or Occupational Therapy consult Speech Language Pathology consult Dysphagia evaluation Medication management Discontinuation, equivalent substitution, dose reduction Dosing adjustment or other recommendations as appropriate Continued
26 Continued Social work assessment Evidence of downward health trajectory Caregiver burden, cultural accommodation, community resource underutilization 4 active co-morbid conditions, anemia, cognitive impairment, decubitus ulcer present on admission, functional impairment, malnutrition, recent unintentional weight Loss Interprofessional, post-acute care recommendations Anemia, decubitus ulcer present at admission, functional impairment, hyponatremia Social work interventions Advanced care planning, palliative care referral, as appropriate Case management referral, patient/caregiver education Early discharge planning; establish goals of therapy if not clear or agreed among patient, family, and caregivers Frailty post-acute care plan Emphasis on coordination with primary care physician for close follow-up, evaluation and management of underlying health and psychosocial issues


27 Frailty Assessment SmartText Screenshot 27


28 SmartList 28


29 29 Frailty Completed Note
30 Risks Identified Frequently occurring risks identified among patients seen by Frailty Team through May 2012 included: Frailty Risk n % Physical Therapy Trigger % Occupational Therapy Trigger % Psychosocial % Medication-Related % Problem Sleeping % Cognitive Impairment % Nutrition Trigger % Lack Independence in ADLs (Katz) % Decline in Function % 30
31 Recommendations Frequently occurring recommendations among patients seen by Frailty Team through May 2012 included: Recommendation N % Sleep Hygiene % Physical Therapy Evaluation % Medication-Related % Volunteer Services % Occupational Therapy Evaluation % Palliative Care % May occur in clusters addressing a specific risk, e.g., Delirium risk Sleep Hygiene, Volunteer Services, Frequent rounding, Discontinue Foley/restraints, etc. Average number of recommendations = 4.9 (median = 4, range = 1 12) 31
32 Identifying Vulnerable Health States Most Common Discharge Diagnoses( >3% prevalence) Patients in the Frailty Pilot Evaluation Base MS-DRG Cases (n,%) Renal Failure 20 (5.8%) Heart Failure/shock 18 (5.2%) Septicemia w/o mechanical ventilation 96+ hrs 17 (5.%) Kidney/Urinary tract infections 15 (4.4%) Intracranial hemorrhage/cerebral infection 12 (3.5%) Respiratory infection/inflammation 12 (3.5%) Esophagitis, gastroenteritis/miscellaneous digestive disease 12 (3.5%) 32
33 33 Pilot Program Demographics
34 34 Pilot SPICE Demographics
35 Severity of Illness % of Cases 60% 50% 40% 30% 20% 10% 0% Intervention Control Minor Moderate Major Extreme APR-DRG Severity of Illness on Admission 35
36 Severity of Illness 50% 40% Intervention Control % of Cases 30% 20% 10% 0% Numbers of SPICES Present within 24 Hours of Admission 36
37 Preliminary Pilot Results Group Outcomes of Hospitalization By Treatment Group Cases (n) Average # of SPICES on Admission Length of Stay Expected (days) Length of Stay Observed (days) Average ICU Days Intervention Control *SPICES = Skin breakdown, Problems eating, Incontinence, Confusion, Evidence of falls, Sleeping disorder recorded within 24 hours of hospital admission by Nursing Average Difference in Expected and Observed LOS in Intervention versus Control Groups = -1.7 days (p=0.011) 37
38 Building Systems to Achieve Greater Efficiency and Reliability Internal stakeholder engagement, evolution of team-based, interprofessional care Streamlining and augmenting inpatient processes Revising Frailty assessment note Building a follow-up note and post-acute care plan Examining effectiveness and sustainability through a rigorous program evaluation Cluster, randomized controlled trial of 10 Nursing units to study impact on adverse inpatient events, adjusted length of stay, and readmissions Implementing the post-acute frailty care plan as part of a transitional model including advanced practice nurses and postdischarge follow-up Partnering with community-based service providers and other community resources 38
39
Potential disruption from private exchanges and narrow networks. In 2011, less than 10% of companies used High Performing Networks (narrow networks)
") 1 3 2 Potential disruption from private exchanges and narrow networks. In 2011, less than 10% of companies used High Performing Networks (narrow networks) and in 2014 estimated to be 40%. By 2018, that
1 3 2 Potential disruption from private exchanges and narrow networks. In 2011, less than 10% of companies used High Performing Networks (narrow networks) and in 2014 estimated to be 40%. By 2018, that
Frailty and Rehabilitation: How We Utilized FIM Data to Develop Risk Models
 Frailty and Rehabilitation: How We Utilized FIM Data to Develop Risk Models User Groups 2015 Orlando, Florida March 19, 2015 Las Vegas, Nevada May 7, 2015 Pam Roberts, PhD, OTR/L, SCFES, FAOTA, CPHQ, FNAP
Frailty and Rehabilitation: How We Utilized FIM Data to Develop Risk Models User Groups 2015 Orlando, Florida March 19, 2015 Las Vegas, Nevada May 7, 2015 Pam Roberts, PhD, OTR/L, SCFES, FAOTA, CPHQ, FNAP
Why New Thinking is Needed for Older Adults across the Rehabilitation Continuum
 Why New Thinking is Needed for Older Adults across the Rehabilitation Continuum Samir K. Sinha MD, DPhil, FRCPC Director of Geriatrics Mount Sinai and the University Health Network Hospitals Assistant
Why New Thinking is Needed for Older Adults across the Rehabilitation Continuum Samir K. Sinha MD, DPhil, FRCPC Director of Geriatrics Mount Sinai and the University Health Network Hospitals Assistant
Improving Healthcare Utilization in Injured Older Adults
 Improving Healthcare Utilization in Injured Older Adults G ERIATRIC T R A U MA I N I T I AT I V E S AT S TA N F O R D H E A LT H C A R E J U LY 12, 2018 Objectives Background on Geriatric Trauma Population
Improving Healthcare Utilization in Injured Older Adults G ERIATRIC T R A U MA I N I T I AT I V E S AT S TA N F O R D H E A LT H C A R E J U LY 12, 2018 Objectives Background on Geriatric Trauma Population
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative
 Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Hospital at Home. Frailty and Hospital at Home. 17 th March Pam Livingstone and Gwyneth Thom
 Hospital at Home Frailty and Hospital at Home 17 th March 2016 Pam Livingstone and Gwyneth Thom National Definition of Hospital at Home December 2013 An episode of specialist care delivered at home as
Hospital at Home Frailty and Hospital at Home 17 th March 2016 Pam Livingstone and Gwyneth Thom National Definition of Hospital at Home December 2013 An episode of specialist care delivered at home as
Geriatrics and Cancer Care
 Geriatrics and Cancer Care Roger Wong, BMSc, MD, FRCPC, FACP Postgraduate Dean of Medical Education Clinical Professor, Division of Geriatric Medicine UBC Faculty of Medicine Disclosure No competing interests
Geriatrics and Cancer Care Roger Wong, BMSc, MD, FRCPC, FACP Postgraduate Dean of Medical Education Clinical Professor, Division of Geriatric Medicine UBC Faculty of Medicine Disclosure No competing interests
Evolutions in Geriatric Fracture Care Preparing for the Silver Tsunami
 Evolutions in Geriatric Fracture Care Preparing for the Silver Tsunami James Holstine, DO Medical Director for the Joint Replacement Center, Geriatric Fracture Center, Orthopedic Surgeon PeaceHealth Whatcom
Evolutions in Geriatric Fracture Care Preparing for the Silver Tsunami James Holstine, DO Medical Director for the Joint Replacement Center, Geriatric Fracture Center, Orthopedic Surgeon PeaceHealth Whatcom
Proprietary Acute Care Indicators
 Proprietary Acute Care Indicators Indicator 1a: Device-Associated Infections in the Intensive Care Unit Central Line-Associated Bloodstream Infections in the APICU, CCU, MICU, M/S ICU, & SICU Ventilator-Associated
Proprietary Acute Care Indicators Indicator 1a: Device-Associated Infections in the Intensive Care Unit Central Line-Associated Bloodstream Infections in the APICU, CCU, MICU, M/S ICU, & SICU Ventilator-Associated
Sharp HealthCare Hospice and Palliative Care
 Sharp HealthCare Hospice and Palliative Care The Continuum for Advanced Illness and End Stage Disease Management (AAC) Daniel R. Hoefer, MD CMO, Outpatient Palliative Care and Hospice Suzi K. Johnson,
Sharp HealthCare Hospice and Palliative Care The Continuum for Advanced Illness and End Stage Disease Management (AAC) Daniel R. Hoefer, MD CMO, Outpatient Palliative Care and Hospice Suzi K. Johnson,
Quality Care for the Hospitalized Older Adult
 Quality Care for the Hospitalized Older Adult Quality Care for the Hospitalized Older Adult Shelley R McDonald, DO, PhD May 19 th, 2018 Objectives To define why the hospital is a dangerous place for older
Quality Care for the Hospitalized Older Adult Quality Care for the Hospitalized Older Adult Shelley R McDonald, DO, PhD May 19 th, 2018 Objectives To define why the hospital is a dangerous place for older
Delirium. A Geriatric Syndrome. Jonathan McCaleb, MD, CMD, HMDC UNSOM, Assistant Professor of Medicine Geriatrics / Hospice & Palliative Medicine
 Delirium A Geriatric Syndrome Jonathan McCaleb, MD, CMD, HMDC UNSOM, Assistant Professor of Medicine Geriatrics / Hospice & Palliative Medicine Introduction Common Serious Unrecognized: a medical emergency
Delirium A Geriatric Syndrome Jonathan McCaleb, MD, CMD, HMDC UNSOM, Assistant Professor of Medicine Geriatrics / Hospice & Palliative Medicine Introduction Common Serious Unrecognized: a medical emergency
ACEing Age Old Issues in the Care of Older Canadians
 ACEing Age Old Issues in the Care of Older Canadians Dr. Samir K. Sinha MD, DPhil, FRCPC Peter and Shelagh Godsoe Chair in Geriatrics and Director of Geriatrics Sinai Health System and the University Health
ACEing Age Old Issues in the Care of Older Canadians Dr. Samir K. Sinha MD, DPhil, FRCPC Peter and Shelagh Godsoe Chair in Geriatrics and Director of Geriatrics Sinai Health System and the University Health
Health Services & High Risk Admissions Registries. David Carnahan, MD MSCE DHA CEI Branch Chief 12 June 2014
 Health Services & High Risk Admissions Registries David Carnahan, MD MSCE DHA CEI Branch Chief 12 June 2014 Introduction Background Information Variables of Interest (potential markers) ACG Use case Readmissions
Health Services & High Risk Admissions Registries David Carnahan, MD MSCE DHA CEI Branch Chief 12 June 2014 Introduction Background Information Variables of Interest (potential markers) ACG Use case Readmissions
UNTHSC TCOM Geriatric Competencies Curriculum Mapping Document
 INSTRUCTIONS: Place a "B" (Basic), "I" (Intermediate), or "A" (Advanced) in the box next to the Geriatric Competency to indicate the Geraitaric Competency being taught, the corresponding Method of Subject
INSTRUCTIONS: Place a "B" (Basic), "I" (Intermediate), or "A" (Advanced) in the box next to the Geriatric Competency to indicate the Geraitaric Competency being taught, the corresponding Method of Subject
Accelero Identifies Opportunities to Provide Greater Value in Hip Fracture Care
 Accelero Health Partners, 2015 WHITE PAPER Accelero Identifies Opportunities to Provide Greater Value in Hip Fracture Care Jason Pry, Senior Director ABSTRACT Every year more than a quarter of a million
Accelero Health Partners, 2015 WHITE PAPER Accelero Identifies Opportunities to Provide Greater Value in Hip Fracture Care Jason Pry, Senior Director ABSTRACT Every year more than a quarter of a million
PURPOSE OF THE SELF-ASSESSMENT TOOLS:
 Pulmonary Rehab s Framework Self-Assessment Tool Inpatient Rehab Survey for Pulmonary Rehab INTRODUCTION: In response to a changing rehab landscape in which rehabilitation is offered in many different
Pulmonary Rehab s Framework Self-Assessment Tool Inpatient Rehab Survey for Pulmonary Rehab INTRODUCTION: In response to a changing rehab landscape in which rehabilitation is offered in many different
Integrating Medical and Social Support for Elderly System & Technology Enabled Service Innovations. Dr Christina MAW Hospital Authority, Hong Kong
 Integrating Medical and Social Support for Elderly System & Technology Enabled Service Innovations Dr Christina MAW Hospital Authority, Hong Kong Hospital Authority (HA) of Hong Kong A statutory body responsible
Integrating Medical and Social Support for Elderly System & Technology Enabled Service Innovations Dr Christina MAW Hospital Authority, Hong Kong Hospital Authority (HA) of Hong Kong A statutory body responsible
Dementia in the acute hospital setting what should we be doing and who should be doing it?
 Dementia in the acute hospital setting what should we be doing and who should be doing it? Sarah Pendlebury Consultant Physician and Associate Professor NIHR Oxford Biomedical Research Centre Departments
Dementia in the acute hospital setting what should we be doing and who should be doing it? Sarah Pendlebury Consultant Physician and Associate Professor NIHR Oxford Biomedical Research Centre Departments
Aging Research Day March 8, 2012
 Aging Research Day March 8, 2012 Heidi R. Wierman, MD Mane Medical Center Division Director, Geriatrics Assistant Professor, Tufts School of Medicine Overview 1.Brief Delirium Review 2.Describe HELP function
Aging Research Day March 8, 2012 Heidi R. Wierman, MD Mane Medical Center Division Director, Geriatrics Assistant Professor, Tufts School of Medicine Overview 1.Brief Delirium Review 2.Describe HELP function
Stroke Rehab Definitions Framework Self-Assessment Tool Acute Integrated Stroke Unit
 rth & East GTA Stroke Network Stroke Rehab Definitions Framework Self-Assessment Tool Acute Integrated Stroke Unit Purpose of the Self-Assessment Tool: The GTA Rehab Network and the GTA regions of the
rth & East GTA Stroke Network Stroke Rehab Definitions Framework Self-Assessment Tool Acute Integrated Stroke Unit Purpose of the Self-Assessment Tool: The GTA Rehab Network and the GTA regions of the
Delirium in the hospitalized patient
 Delirium in the hospitalized patient Jennifer A. Tarin, M.D. Department of Hospital Medicine Geriatric Health Safety Chair Colorado Permanente Medical Group UCLA Reynolds Scholar Delirium Preventing delirium
Delirium in the hospitalized patient Jennifer A. Tarin, M.D. Department of Hospital Medicine Geriatric Health Safety Chair Colorado Permanente Medical Group UCLA Reynolds Scholar Delirium Preventing delirium
nicheprogram.org 2016 Annual NICHE Conference Care Across the Continuum 1
 NICHE 101: Resources & Tools: The NICHE Knowledge Center Eugenia Bachaleda, MA Assistant Director, Education and Resources Deirdre M. Carolan, PhD, ANP, BC, GNP, BC Nurse Practitioner, Geriatrics, Clinical
NICHE 101: Resources & Tools: The NICHE Knowledge Center Eugenia Bachaleda, MA Assistant Director, Education and Resources Deirdre M. Carolan, PhD, ANP, BC, GNP, BC Nurse Practitioner, Geriatrics, Clinical
Evaluating Functional Status in Hospitalized Geriatric Patients. UCLA-Santa Monica Geriatric Medicine Didactic Lecture Series
 Evaluating Functional Status in Hospitalized Geriatric Patients UCLA-Santa Monica Geriatric Medicine Didactic Lecture Series Case 88 y.o. woman was admitted for a fall onto her hip. She is having trouble
Evaluating Functional Status in Hospitalized Geriatric Patients UCLA-Santa Monica Geriatric Medicine Didactic Lecture Series Case 88 y.o. woman was admitted for a fall onto her hip. She is having trouble
HEALTHSTREAM LIVING LABS IN ACTION
 HEALTHSTREAM LIVING LABS IN ACTION A CONVERSATION WITH: Mitchel T. Heflin MD, MHS Associate Professor of Medicine, Duke University School of Medicine Eleanor McConnell PhD, RN, GCNS-BC Associate Professor,
HEALTHSTREAM LIVING LABS IN ACTION A CONVERSATION WITH: Mitchel T. Heflin MD, MHS Associate Professor of Medicine, Duke University School of Medicine Eleanor McConnell PhD, RN, GCNS-BC Associate Professor,
Accelero Identifies Opportunities to Provide Greater Value in Hip Fracture Care
 Accelero Identifies Opportunities to Provide Greater Value in Hip Fracture Care Every year more than a quarter of a million people over the age of 65 are admitted to a hospital with a hip fracture. Mortality
Accelero Identifies Opportunities to Provide Greater Value in Hip Fracture Care Every year more than a quarter of a million people over the age of 65 are admitted to a hospital with a hip fracture. Mortality
Rehabilitation - Reducing costs and hospital stay. Dr Elizabeth Aitken Consultant Physician
 Rehabilitation - Reducing costs and hospital stay Dr Elizabeth Aitken Consultant Physician What factors affect outcome? Comorbidities Cardiac Respiratory Neurological Nutritional issues Diabetes Anaemia
Rehabilitation - Reducing costs and hospital stay Dr Elizabeth Aitken Consultant Physician What factors affect outcome? Comorbidities Cardiac Respiratory Neurological Nutritional issues Diabetes Anaemia
Hospital Transition Management. Barbara Wood, BSN, MBA
 Hospital Transition Management Barbara Wood, BSN, MBA Director, Embedded Care Management Programs OBJECTIVES Improve health care quality for our patients by streamlining care transitions Reduce avoidable
Hospital Transition Management Barbara Wood, BSN, MBA Director, Embedded Care Management Programs OBJECTIVES Improve health care quality for our patients by streamlining care transitions Reduce avoidable
Geriatric Medicine I) OBJECTIVES
 OBJECTIVES") Geriatric Medicine I) OBJECTIVES 1 To provide a broad training and in-depth experience at a level sufficient for trainees to acquire competence and professionalism required of a specialist in Geriatric
Geriatric Medicine I) OBJECTIVES 1 To provide a broad training and in-depth experience at a level sufficient for trainees to acquire competence and professionalism required of a specialist in Geriatric
2010 National Audit of Dementia (Care in General Hospitals)
") Royal College of Psychiatrists 2010 National Audit of Dementia (Care in General Hospitals) Organisational checklist results and commentary for: Barking, Havering and Redbridge Hospitals NHS Trust The 2010
Royal College of Psychiatrists 2010 National Audit of Dementia (Care in General Hospitals) Organisational checklist results and commentary for: Barking, Havering and Redbridge Hospitals NHS Trust The 2010
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acute coronary syndrome (ACS), burden of condition, 83 diagnosis of, 82 83 evaluation of, 83, 87 major complications of, 86 risk for,
Index Note: Page numbers of article titles are in boldface type. A Acute coronary syndrome (ACS), burden of condition, 83 diagnosis of, 82 83 evaluation of, 83, 87 major complications of, 86 risk for,
Standards of excellence
 The Accreditation Canada Stroke Distinction program was launched in March 2010 to offer a rigorous and highly specialized process above and beyond the requirements of Qmentum. The comprehensive Stroke
The Accreditation Canada Stroke Distinction program was launched in March 2010 to offer a rigorous and highly specialized process above and beyond the requirements of Qmentum. The comprehensive Stroke
Hospitalization- Associated Disability
 Hospitalization- Associated Disability Deborah Villarreal, MD Assistant Professor Geriatric and Palliative Medicine An Unfortunately Common Scenario Mrs.G 70 y/o BF DM type II, HTN, s/p CVA, OA, OP admitted
Hospitalization- Associated Disability Deborah Villarreal, MD Assistant Professor Geriatric and Palliative Medicine An Unfortunately Common Scenario Mrs.G 70 y/o BF DM type II, HTN, s/p CVA, OA, OP admitted
nicheprogram.org 2016 Annual NICHE Conference Care Across the Continuum 1 Dissemination of Geriatrics Guidelines in the Emergency Department:
 Dissemination of Geriatrics Guidelines in the Emergency Department: The Intersection of Geriatric Experts, National Guidelines, and Quality Improvement in 3 Midwestern Hospitals. Aaron Malsch MS, RN, GCNS-BC
Dissemination of Geriatrics Guidelines in the Emergency Department: The Intersection of Geriatric Experts, National Guidelines, and Quality Improvement in 3 Midwestern Hospitals. Aaron Malsch MS, RN, GCNS-BC
2010 National Audit of Dementia (Care in General Hospitals) North West London Hospitals NHS Trust
 North West London Hospitals NHS Trust") Royal College of Psychiatrists 2010 National Audit of Dementia (Care in General Hospitals) Organisational checklist results and commentary for: rth West London Hospitals NHS Trust The 2010 national audit
Royal College of Psychiatrists 2010 National Audit of Dementia (Care in General Hospitals) Organisational checklist results and commentary for: rth West London Hospitals NHS Trust The 2010 national audit
Comprehensive Assessment with Rapid Evaluation and Treatment: Integrating palliative care into the care of patients with advanced cancer Leslie J
 Comprehensive Assessment with Rapid Evaluation and Treatment: Integrating palliative care into the care of patients with advanced cancer Leslie J Blackhall MD MTS Section Head, Palliative Care University
Comprehensive Assessment with Rapid Evaluation and Treatment: Integrating palliative care into the care of patients with advanced cancer Leslie J Blackhall MD MTS Section Head, Palliative Care University
There s No Place like Home
 THERE S NO PLACE LIKE HOME There s No Place like Home Regional Advisory Committee for Excellence in Care of Older Adults Elements of the Program TAKE AWAY SERVICES R & G PROGRAM CONSULTATION O SERVICES
THERE S NO PLACE LIKE HOME There s No Place like Home Regional Advisory Committee for Excellence in Care of Older Adults Elements of the Program TAKE AWAY SERVICES R & G PROGRAM CONSULTATION O SERVICES
Delirium in the Elderly
 Delirium in the Elderly ELITE 2015 Mamata Yanamadala M.B.B.S, MS Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity
Delirium in the Elderly ELITE 2015 Mamata Yanamadala M.B.B.S, MS Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity
UND GERIATRIC MEDICINE FELLOWSHIP CURRICULUM ACUTE CARE
 LOCATION SITE Sanford Medical Center Fargo 5225 23rd Avenue S Fargo, ND 58104 CONTACT LEAD FACULTY MEMBER Dr. Darin Lang Darin.lang@sanfordhealth.org PROGRAM CONTACT Dr. Gunjan Manocha gunjan.dhawan@und.edu
LOCATION SITE Sanford Medical Center Fargo 5225 23rd Avenue S Fargo, ND 58104 CONTACT LEAD FACULTY MEMBER Dr. Darin Lang Darin.lang@sanfordhealth.org PROGRAM CONTACT Dr. Gunjan Manocha gunjan.dhawan@und.edu
Objectives 2/11/2016 HOSPICE 101
 HOSPICE 101 Overview Hospice History and Statistics What is Hospice? Who qualifies for services? Levels of Service The Admission Process Why Not to Wait Objectives Understand how to determine hospice eligibility
HOSPICE 101 Overview Hospice History and Statistics What is Hospice? Who qualifies for services? Levels of Service The Admission Process Why Not to Wait Objectives Understand how to determine hospice eligibility
End of Life Care in Dementia. Dr Rosie Lockwood Consultant Geriatrician Sheffield Teaching Hospitals
 End of Life Care in Dementia Dr Rosie Lockwood Consultant Geriatrician Sheffield Teaching Hospitals Rosie.Lockwood@sth.nhs.uk Agenda Some facts and figures What are the challenges? What is good care? How
End of Life Care in Dementia Dr Rosie Lockwood Consultant Geriatrician Sheffield Teaching Hospitals Rosie.Lockwood@sth.nhs.uk Agenda Some facts and figures What are the challenges? What is good care? How
2010 National Audit of Dementia (Care in General Hospitals) Chelsea and Westminster Hospital NHS Foundation Trust
 Chelsea and Westminster Hospital NHS Foundation Trust") Royal College of Psychiatrists 2010 National Audit of Dementia (Care in General Hospitals) Organisational checklist results and commentary for: NHS Foundation Trust The 2010 national audit of dementia
Royal College of Psychiatrists 2010 National Audit of Dementia (Care in General Hospitals) Organisational checklist results and commentary for: NHS Foundation Trust The 2010 national audit of dementia
How to disseminate the Acute Care for Elders (ACE) model of care beyond one unit
 model of care beyond one unit") How to disseminate the Acute Care for Elders (ACE) model of care beyond one unit Roger Wong, BMSc, MD, FRCPC, FACP Clinical Professor, Division of Geriatric Medicine Associate Dean, Postgraduate Medical
How to disseminate the Acute Care for Elders (ACE) model of care beyond one unit Roger Wong, BMSc, MD, FRCPC, FACP Clinical Professor, Division of Geriatric Medicine Associate Dean, Postgraduate Medical
Care of older people in surgery (COPS)
") Care of older people in surgery (COPS) Who, what, and does it make a difference Professor Jacqueline Close Geriatrician - POWH Clinical Director Falls, Balance and Injury Research Centre Early Mobilisation
Care of older people in surgery (COPS) Who, what, and does it make a difference Professor Jacqueline Close Geriatrician - POWH Clinical Director Falls, Balance and Injury Research Centre Early Mobilisation
LEVELS OF NICHE IMPLEMENTATION. Stage 2: Progressive Implementation
 LEVELS OF NICHE IMPLEMENTATION *Required element Stage 1: Early Stage 2: Progressive Stage 3: Senior Friendly Stage 4: Exemplar Dimensions Guiding Principles The institution has a mission statement that
LEVELS OF NICHE IMPLEMENTATION *Required element Stage 1: Early Stage 2: Progressive Stage 3: Senior Friendly Stage 4: Exemplar Dimensions Guiding Principles The institution has a mission statement that
Geriatric Medicine Clerkship Orientation. Aval-Na Ree Green (modified by Huai Cheng)
") Geriatric Medicine Clerkship Orientation Aval-Na Ree Green (modified by Huai Cheng) Welcome! Goals The geriatric clerkship is designed to prepare medical students to provide evidence-based, competent,
Geriatric Medicine Clerkship Orientation Aval-Na Ree Green (modified by Huai Cheng) Welcome! Goals The geriatric clerkship is designed to prepare medical students to provide evidence-based, competent,
Measure Applications Partnership. Hospital Workgroup In-Person Meeting Follow- Up Call
 Measure Applications Partnership Hospital Workgroup In-Person Meeting Follow- Up Call December 21, 2016 Feedback on Current Measure Sets for IQR, HACs, Readmissions, and VBP 2 Previously Identified Crosscutting
Measure Applications Partnership Hospital Workgroup In-Person Meeting Follow- Up Call December 21, 2016 Feedback on Current Measure Sets for IQR, HACs, Readmissions, and VBP 2 Previously Identified Crosscutting
Delirium in the Elderly
 Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
Please make sure that you complete a self-assessment survey for each type of rehab program that your organization provides.
 Oncology Rehab s Framework Self-Assessment Tool Inpatient Rehab Survey for Oncology Rehab INTRODUCTION: In response to a changing rehab landscape in which rehabilitation is offered in many different settings
Oncology Rehab s Framework Self-Assessment Tool Inpatient Rehab Survey for Oncology Rehab INTRODUCTION: In response to a changing rehab landscape in which rehabilitation is offered in many different settings
Understanding and Assessing for Frailty
 Understanding and Assessing for Frailty Dr Gloria Yu Clinical Head of Bexley Integrated Care Consultant Physician in Elderly, General and Stroke Medicine 8 July 2015 Learning objectives What is frailty?
Understanding and Assessing for Frailty Dr Gloria Yu Clinical Head of Bexley Integrated Care Consultant Physician in Elderly, General and Stroke Medicine 8 July 2015 Learning objectives What is frailty?
Implementing Best Practice Rehabilitative Care for Patients with Hip Fracture & Total Joint Replacement
 Implementing Best Practice Rehabilitative Care for Patients with Hip Fracture & Total Joint Replacement A Toolkit for Implementing the RCA s TJR and Hip Fracture Best Practice Frameworks January 2018 Purpose
Implementing Best Practice Rehabilitative Care for Patients with Hip Fracture & Total Joint Replacement A Toolkit for Implementing the RCA s TJR and Hip Fracture Best Practice Frameworks January 2018 Purpose
Palliative Care Consultative Service in Acute Hospital - Impact & Challenges
 Palliative Care Consultative Service in Acute Hospital - Impact & Challenges Dr. Annie Kwok Consultant Palliative Care Unit Department of Medicine & Geriatrics Caritas Medical Centre Contents Aging population
Palliative Care Consultative Service in Acute Hospital - Impact & Challenges Dr. Annie Kwok Consultant Palliative Care Unit Department of Medicine & Geriatrics Caritas Medical Centre Contents Aging population
4/26/2012. Laura Grooms, MD Assistant Professor Geriatric Medicine Department of Family and Geriatric Medicine University of Louisville April 20, 2012
 Laura Grooms, MD Assistant Professor Geriatric Medicine Department of Family and Geriatric Medicine University of Louisville April 20, 2012 Laura Grooms, MD Assistant Professor Geriatric Medicine Department
Laura Grooms, MD Assistant Professor Geriatric Medicine Department of Family and Geriatric Medicine University of Louisville April 20, 2012 Laura Grooms, MD Assistant Professor Geriatric Medicine Department
William Osler Health System
 William Osler Health System Implementation of a Standardized approach to Delirium Assessment, Prevention & Management Cohort 1: Stephanie Jarvis, CNS, Seniors Health System Kuldeep Chahal, ELS, Hospital
William Osler Health System Implementation of a Standardized approach to Delirium Assessment, Prevention & Management Cohort 1: Stephanie Jarvis, CNS, Seniors Health System Kuldeep Chahal, ELS, Hospital
Why Target Delirium for Surgical Quality Improvement?
 Why Target Delirium for Surgical Quality Improvement? Tom Robinson MD FACS thomas.robinson@ucdenver.edu July 22, 2018 Disclosures Tom Robinson has no disclosures. Who Cares About the Brain? Acute Organ
Why Target Delirium for Surgical Quality Improvement? Tom Robinson MD FACS thomas.robinson@ucdenver.edu July 22, 2018 Disclosures Tom Robinson has no disclosures. Who Cares About the Brain? Acute Organ
PROVIDING BETTER CARE FOR OLDER CANADIANS OBJECTIVES
 PROVIDING BETTER CARE FOR OLDER CANADIANS CGS/ SQG SYMPOSIUM MARIE-JEANNE KERGOAT MD, FRCPC,TORONTO, APRIL 19TH 2013 OBJECTIVES Debate with other clinicians responsible for delivering care to vulnerable
PROVIDING BETTER CARE FOR OLDER CANADIANS CGS/ SQG SYMPOSIUM MARIE-JEANNE KERGOAT MD, FRCPC,TORONTO, APRIL 19TH 2013 OBJECTIVES Debate with other clinicians responsible for delivering care to vulnerable
Delirium assessment and management. Dr Kim Jeffs Northern Health
 Delirium assessment and management Dr Kim Jeffs Northern Health What do you need to know? Epidemiology How big is the problem? Who is at risk? Assessment Tools for diagnosis Prevention Evidence base Management
Delirium assessment and management Dr Kim Jeffs Northern Health What do you need to know? Epidemiology How big is the problem? Who is at risk? Assessment Tools for diagnosis Prevention Evidence base Management
NATIONAL REHABILITATION HOSPITAL (NRH) THE SPINAL CORD SYSTEM OF CARE (SCSC) PROGRAMME INPATIENT SCOPE OF SERVICE
 THE SPINAL CORD SYSTEM OF CARE (SCSC) PROGRAMME INPATIENT SCOPE OF SERVICE") NATIONAL REHABILITATION HOSPITAL (NRH) THE SPINAL CORD SYSTEM OF CARE (SCSC) PROGRAMME INPATIENT SCOPE OF SERVICE NATIONAL REHABILITATION HOSPITAL SCOPE OF SERVICE FOR THE SPINAL CORD SYSTEM OF CARE PROGRAMME
NATIONAL REHABILITATION HOSPITAL (NRH) THE SPINAL CORD SYSTEM OF CARE (SCSC) PROGRAMME INPATIENT SCOPE OF SERVICE NATIONAL REHABILITATION HOSPITAL SCOPE OF SERVICE FOR THE SPINAL CORD SYSTEM OF CARE PROGRAMME
MSK Rehab Definitions Framework - hip fractures Self assessment Survey Outpatient Rehab
 MSK Rehab Definitions Framework - hip fractures Self assessment Survey Outpatient Rehab In response to a changing rehab landscape in which rehabilitation is offered in many different settings with variations
MSK Rehab Definitions Framework - hip fractures Self assessment Survey Outpatient Rehab In response to a changing rehab landscape in which rehabilitation is offered in many different settings with variations
CMS Hospital Inpatient Quality Reporting (IQR) Program Measures for the FY 2019 Payment Update
 Program Measures for the FY 2019 Payment Update") CMS Inpatient Quality Reporting (IQR) Program Measures for the Update Measures Required to Meet IQR Program APU Requirements NHSN Submission CAUTI National Healthcare Safety Network (NHSN) Catheter-Associated
CMS Inpatient Quality Reporting (IQR) Program Measures for the Update Measures Required to Meet IQR Program APU Requirements NHSN Submission CAUTI National Healthcare Safety Network (NHSN) Catheter-Associated
How to prevent delirium in nursing home. Dr. Sophie ALLEPAERTS Geriatric department CHU-Liège Belgium
 How to prevent delirium in nursing home Dr. Sophie ALLEPAERTS Geriatric department CHU-Liège Belgium 1 CONFLICT OF INTEREST DISCLOSURE I have no potential conflict of interest to report 2 Outline 1. Introduction
How to prevent delirium in nursing home Dr. Sophie ALLEPAERTS Geriatric department CHU-Liège Belgium 1 CONFLICT OF INTEREST DISCLOSURE I have no potential conflict of interest to report 2 Outline 1. Introduction
A snapshot of inpatient oncology rehabilitation: Patient profiles and rehab outcomes Rehabilitation Rounds, University of Toronto April 5, 2012
 A snapshot of inpatient oncology rehabilitation: Patient profiles and rehab outcomes Rehabilitation Rounds, University of Toronto April 5, 2012 Sara McEwen, PT, PhD Research Scientist, St. John s Rehab
A snapshot of inpatient oncology rehabilitation: Patient profiles and rehab outcomes Rehabilitation Rounds, University of Toronto April 5, 2012 Sara McEwen, PT, PhD Research Scientist, St. John s Rehab
Community and Mental Health Services. Palliative Care. Criteria and
 Community and Mental Health Services Specialist Palliative Care Service Referral Criteria and Guidance November 2018 Specialist Palliative Care Service Referrals These guidelines cover referrals for patients
Community and Mental Health Services Specialist Palliative Care Service Referral Criteria and Guidance November 2018 Specialist Palliative Care Service Referrals These guidelines cover referrals for patients
Comprehensive geriatric assessment (CGA)
") Comprehensive geriatric assessment (CGA) Mieke Deschodt, RN, PhD Lucky you, getting older in Europe - Multiplier event IC Dien Oostduinkerke, 5 June 2018 @mieke_deschodt 2 Outline Comprehensive geriatric
Comprehensive geriatric assessment (CGA) Mieke Deschodt, RN, PhD Lucky you, getting older in Europe - Multiplier event IC Dien Oostduinkerke, 5 June 2018 @mieke_deschodt 2 Outline Comprehensive geriatric
Update - Delirium in Elders
 Update - Delirium in Elders Impact Recognition Prevention, and Management Michael J. Lichtenstein, MD F. Carter Pannill, Jr. Professor of Medicine Chief, Division of Geriatrics, Gerontology and Palliative
Update - Delirium in Elders Impact Recognition Prevention, and Management Michael J. Lichtenstein, MD F. Carter Pannill, Jr. Professor of Medicine Chief, Division of Geriatrics, Gerontology and Palliative
2010 National Audit of Dementia (Care in General Hospitals) Guy's and St Thomas' NHS Foundation Trust
 Guy's and St Thomas' NHS Foundation Trust") Royal College of Psychiatrists 2010 National Audit of Dementia (Care in General Hospitals) Organisational checklist results and commentary for: Guy's and St Thomas' NHS Foundation Trust The 2010 national
Royal College of Psychiatrists 2010 National Audit of Dementia (Care in General Hospitals) Organisational checklist results and commentary for: Guy's and St Thomas' NHS Foundation Trust The 2010 national
Improving documentation and coding of malnutrition a five year journey
 Improving documentation and coding of malnutrition a five year journey Natalie Simmance, Chief Dietitian Clara Newsome Sally Bell Sonia Grundy St Vincent's Hospital Melbourne Patient Malnutrition common
Improving documentation and coding of malnutrition a five year journey Natalie Simmance, Chief Dietitian Clara Newsome Sally Bell Sonia Grundy St Vincent's Hospital Melbourne Patient Malnutrition common
SPINAL CORD INJURY Rehab Definitions Framework Self-Assessment Tool inpatient rehab Survey for Spinal Cord Injury (SCI)
") SPINAL CORD INJURY Rehab s Framework Self-Assessment Tool inpatient rehab Survey for Spinal Cord Injury (SCI) INTRODUCTION: In response to a changing rehab landscape in which rehabilitation is offered
SPINAL CORD INJURY Rehab s Framework Self-Assessment Tool inpatient rehab Survey for Spinal Cord Injury (SCI) INTRODUCTION: In response to a changing rehab landscape in which rehabilitation is offered
The Geriatrician in the Trauma Service. Trauma Quality Improvement Program (TQIP) Annual Scientific Meeting and Training 2013
 Annual Scientific Meeting and Training 2013") The Geriatrician in the Trauma Service Trauma Quality Improvement Program (TQIP) Annual Scientific Meeting and Training 2013 Challenges of the Geriatric Trauma Patient Challenges of the Geriatric Patient
The Geriatrician in the Trauma Service Trauma Quality Improvement Program (TQIP) Annual Scientific Meeting and Training 2013 Challenges of the Geriatric Trauma Patient Challenges of the Geriatric Patient
Upon completing this session, participates will be able to:
 C18 These presenters have nothing to disclose Methods for Identifying a High- Need, High-Cost Population Don Goldmann, MD Jose Figueroa, MD, MPH R. Corey Waller, MD, MS, DFASAM Christine Vogeli, PhD December
C18 These presenters have nothing to disclose Methods for Identifying a High- Need, High-Cost Population Don Goldmann, MD Jose Figueroa, MD, MPH R. Corey Waller, MD, MS, DFASAM Christine Vogeli, PhD December
Needs Assessment and Plan for Integrated Stroke Rehabilitation in the GTA February, 2002
 Funding for this project has been provided by the Ministry of Health and Long-Term Care as part of the Ontario Integrated Stroke Strategy 2000. It should be noted that the opinions expressed are those
Funding for this project has been provided by the Ministry of Health and Long-Term Care as part of the Ontario Integrated Stroke Strategy 2000. It should be noted that the opinions expressed are those
National Palliative Care Registry : Hospital Palliative Care Preview
 National Palliative Care Registry : Hospital Palliative Care Preview Maggie Rogers, MPH Senior Research Associate, CAPC Tamara Dumanovsky, PhD VP Research & Analytics, CAPC September 15, 2016 The National
National Palliative Care Registry : Hospital Palliative Care Preview Maggie Rogers, MPH Senior Research Associate, CAPC Tamara Dumanovsky, PhD VP Research & Analytics, CAPC September 15, 2016 The National
Delirium in Older Persons: An Investigative Journey
 Delirium in Older Persons: An Investigative Journey Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley F. Levy Family Chair
Delirium in Older Persons: An Investigative Journey Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley F. Levy Family Chair
New York City Development of the Geriatric Collaborative
 New York City - 2014 Development of the Geriatric Collaborative The Clinical Problem More than 50% persons age 65 years will have some surgical procedure in the remainder of his or her lifetime Outcome
New York City - 2014 Development of the Geriatric Collaborative The Clinical Problem More than 50% persons age 65 years will have some surgical procedure in the remainder of his or her lifetime Outcome
Surgery in Frail Elders. Emily Finlayson, MD, MS Department of Surgery University of California, San Francisco September, 2011
 Surgery in Frail Elders Emily Finlayson, MD, MS Department of Surgery University of California, San Francisco September, 2011 What we re going to cover Mortality after surgery in the elderly Fact v Fantasy
Surgery in Frail Elders Emily Finlayson, MD, MS Department of Surgery University of California, San Francisco September, 2011 What we re going to cover Mortality after surgery in the elderly Fact v Fantasy
With Respect to Old Age: Can We Do Better?
 With Respect to Old Age: Can We Do Better? Dr. Samir K. Sinha MD, DPhil, FRCPC Provincial Lead, Ontario s Seniors Care Strategy Director of Geriatrics Mount Sinai and the University Health Network Hospitals
With Respect to Old Age: Can We Do Better? Dr. Samir K. Sinha MD, DPhil, FRCPC Provincial Lead, Ontario s Seniors Care Strategy Director of Geriatrics Mount Sinai and the University Health Network Hospitals
Strategies for Enhancing Sepsis Survivorship
 Strategies for Enhancing Sepsis Survivorship Hallie Prescott, MD, MSc Ohio Hospital Association August 16, 2016 Disclosures I have no relevant financial conflicts of interest Key Funding NIH/NIGMS American
Strategies for Enhancing Sepsis Survivorship Hallie Prescott, MD, MSc Ohio Hospital Association August 16, 2016 Disclosures I have no relevant financial conflicts of interest Key Funding NIH/NIGMS American
Specialist Palliative Care Referral for Patients
 Specialist Palliative Care Referral for Patients This guideline covers referrals for patients with progressive terminal illness, whether due to cancer or other disease. For many patients in the late stages
Specialist Palliative Care Referral for Patients This guideline covers referrals for patients with progressive terminal illness, whether due to cancer or other disease. For many patients in the late stages
Session Objectives 11/27/2013
 Workshop A3 and B3 This presenter has nothing to disclose Clinical and Cost Improvement for Population Health Scott Weingarten, MD Senior Vice President and Chief Clinical Transformation Officer Cedars-Sinai
Workshop A3 and B3 This presenter has nothing to disclose Clinical and Cost Improvement for Population Health Scott Weingarten, MD Senior Vice President and Chief Clinical Transformation Officer Cedars-Sinai
Specialist Palliative Care Service Referral Criteria and Guidance
 Specialist Palliative Care Service Referral Criteria and Guidance Specialist Palliative Care Service Referrals These guidelines cover referrals for patients with progressive terminal illness, whether
Specialist Palliative Care Service Referral Criteria and Guidance Specialist Palliative Care Service Referrals These guidelines cover referrals for patients with progressive terminal illness, whether
Dave Ure, OT Reg. (Ont.), CPA, CMA Coordinator
, CPA, CMA Coordinator") Dave Ure, OT Reg. (Ont.), CPA, CMA Coordinator Development of the model In response to the request for proposal issued by the Ministry of Health and Long-Term Care in September 2001, the Southwestern Ontario
Dave Ure, OT Reg. (Ont.), CPA, CMA Coordinator Development of the model In response to the request for proposal issued by the Ministry of Health and Long-Term Care in September 2001, the Southwestern Ontario
Hospice and Palliative Care An Essential Component of the Aging Services Network
 Hospice and Palliative Care An Essential Component of the Aging Services Network Howard Tuch, MD, MS American Academy of Hospice and Palliative Medicine Physician Advocate, American Academy of Hospice
Hospice and Palliative Care An Essential Component of the Aging Services Network Howard Tuch, MD, MS American Academy of Hospice and Palliative Medicine Physician Advocate, American Academy of Hospice
Appendix 1: Service self-assessment
 Appendix 1: Service self-assessment Frailty Screening Are we delivering high-quality care for frail older people? We are assessing for frailty in people aged 65+ at every entry into the service using a
Appendix 1: Service self-assessment Frailty Screening Are we delivering high-quality care for frail older people? We are assessing for frailty in people aged 65+ at every entry into the service using a
Delirium Pilot Project
 CCU Nurses: Delirium Pilot Project Our unit has been selected to develop and implement a delirium assessment and intervention program. We are beginning Phase 1 with education and assessing for our baseline
CCU Nurses: Delirium Pilot Project Our unit has been selected to develop and implement a delirium assessment and intervention program. We are beginning Phase 1 with education and assessing for our baseline
Service Provider Department Phone Number
 Service Provider Department Phone Number A Activities of Daily Living Occupational Therapy Rehabilitation Services 734-593-5620 Adaptive Equipment - home Occupational Therapy Rehabilitation Services 734-593-5620
Service Provider Department Phone Number A Activities of Daily Living Occupational Therapy Rehabilitation Services 734-593-5620 Adaptive Equipment - home Occupational Therapy Rehabilitation Services 734-593-5620
The Challenges of Managing the Older Persons
 IAG Presidential Oration The Challenges of Managing the Older Persons G.S. Shanthi Professor & Head, Department of Geriatric Medicine, Madras Medical College, Chennai Globally, due to shifting demographics,
IAG Presidential Oration The Challenges of Managing the Older Persons G.S. Shanthi Professor & Head, Department of Geriatric Medicine, Madras Medical College, Chennai Globally, due to shifting demographics,
nicheprogram.org 2015 Annual NICHE Conference Innovation Through Leadership Background
 Wii Can Too! Using Gaming Technology with Hospital Elder Life Program Patients Megan Wheeler, MSN, RN, ACNS-BC Janice F. Moore, PhD, CFLE Background Grant Proposal Hospital Elder Life Program (HELP) proven
Wii Can Too! Using Gaming Technology with Hospital Elder Life Program Patients Megan Wheeler, MSN, RN, ACNS-BC Janice F. Moore, PhD, CFLE Background Grant Proposal Hospital Elder Life Program (HELP) proven
NURSES IMPROVING CARE FOR HEALTH SYSTEM ELDERS (NICHE) NICHE AND THE LONG TERM CARE COMMUNITY
 NICHE AND THE LONG TERM CARE COMMUNITY") 2 NURSES IMPROVING CARE FOR HEALTH SYSTEM ELDERS (NICHE) NICHE AND THE LONG TERM CARE COMMUNITY 215-218 Joanne Alderman, MS-N, APRN-CNS(C), RNBC,FNGNA Nita Dunbar, RN, GRN 1 A JOURNEY TO LEARNING 215-216
2 NURSES IMPROVING CARE FOR HEALTH SYSTEM ELDERS (NICHE) NICHE AND THE LONG TERM CARE COMMUNITY 215-218 Joanne Alderman, MS-N, APRN-CNS(C), RNBC,FNGNA Nita Dunbar, RN, GRN 1 A JOURNEY TO LEARNING 215-216
Delivering personalised care to end of life patients. Jane Naismith Nurse Consultant in Palliative care St Joseph s Hospice London
 Delivering personalised care to end of life patients Jane Naismith Nurse Consultant in Palliative care St Joseph s Hospice London Over View This session will cover Supporting patients with long term conditions
Delivering personalised care to end of life patients Jane Naismith Nurse Consultant in Palliative care St Joseph s Hospice London Over View This session will cover Supporting patients with long term conditions
Palliative Care for Older Adults in the United States
 Palliative Care for Older Adults in the United States Nathan Goldstein, MD Associate Professor Hertzberg Palliative Care Institute Brookdale Department of Geriatrics and Palliative Medicine Icahn School
Palliative Care for Older Adults in the United States Nathan Goldstein, MD Associate Professor Hertzberg Palliative Care Institute Brookdale Department of Geriatrics and Palliative Medicine Icahn School
Casa Colina Centers for Rehabilitation: A unique physician-directed model of care that works
 Casa Colina Centers for Rehabilitation: A unique physician-directed model of care that works Emily R. Rosario, PhD Why is Casa Colina unique? Continuum of care offering medical and rehabilitation services
Casa Colina Centers for Rehabilitation: A unique physician-directed model of care that works Emily R. Rosario, PhD Why is Casa Colina unique? Continuum of care offering medical and rehabilitation services
Charles Bernick, MD, MPH Cleveland Clinic Lou Ruvo Center for Brain Health June 2, 2018
 Charles Bernick, MD, MPH Cleveland Clinic Lou Ruvo Center for Brain Health June 2, 2018 Delirium common Prolongs hospitalization Worsens dementia ( if you survive) Increased risk of institutionalization
Charles Bernick, MD, MPH Cleveland Clinic Lou Ruvo Center for Brain Health June 2, 2018 Delirium common Prolongs hospitalization Worsens dementia ( if you survive) Increased risk of institutionalization
Do shared care wards work?
 Do shared care wards work? Prof Rowan H. Harwood Nottingham University Hospitals NHS Trust & University of Nottingham rowan.harwood@nuh.nhs.uk This presentation is on independent research funded by the
Do shared care wards work? Prof Rowan H. Harwood Nottingham University Hospitals NHS Trust & University of Nottingham rowan.harwood@nuh.nhs.uk This presentation is on independent research funded by the
What ASMBS Members Need to Know About: New Medicare Payment Policy Governing Bariatric Surgery and Hospital Acquired Conditions (HACs)
") What ASMBS Members Need to Know About: New Medicare Payment Policy Governing Bariatric Surgery and Hospital Acquired Conditions (HACs) Robin Blackstone, MD, FACS, FASMBS Beginning October 1, 2008, Medicare
What ASMBS Members Need to Know About: New Medicare Payment Policy Governing Bariatric Surgery and Hospital Acquired Conditions (HACs) Robin Blackstone, MD, FACS, FASMBS Beginning October 1, 2008, Medicare
Holy Cross Health Meeting the Needs of the Senior Population. Judith Rogers, RNC, MSN, PhD President, Holy Cross Hospital February, 2016
 Holy Cross Health Meeting the Needs of the Senior Population Judith Rogers, RNC, MSN, PhD President, Holy Cross Hospital February, 2016 Service Area Holy Cross Hospital s service area includes about 1.7
Holy Cross Health Meeting the Needs of the Senior Population Judith Rogers, RNC, MSN, PhD President, Holy Cross Hospital February, 2016 Service Area Holy Cross Hospital s service area includes about 1.7
Iatrogenesis in the frail elderly
 Iatrogenesis in the frail elderly Professor Michael Dooley Director of Pharmacy Alfred Health Professor of Clinical Pharmacy Centre for Medicine Use and Safety Monash University Iatrogenesis in the frail
Iatrogenesis in the frail elderly Professor Michael Dooley Director of Pharmacy Alfred Health Professor of Clinical Pharmacy Centre for Medicine Use and Safety Monash University Iatrogenesis in the frail
Executive Sponsorship of Delirium Initiatives Lessons from ICU Liberation
 Executive Sponsorship of Delirium Initiatives Lessons from ICU Liberation J. Matthew Aldrich, MD Co-Chair, SCCM ICU Liberation Committee Associate Professor Medical Director, Critical Care Medicine UCSF
Executive Sponsorship of Delirium Initiatives Lessons from ICU Liberation J. Matthew Aldrich, MD Co-Chair, SCCM ICU Liberation Committee Associate Professor Medical Director, Critical Care Medicine UCSF