Care of older people in surgery (COPS)
|
|
|
- Beverly Joanna Singleton
- 5 years ago
- Views:
Transcription





1 Care of older people in surgery (COPS) Who, what, and does it make a difference Professor Jacqueline Close Geriatrician - POWH Clinical Director Falls, Balance and Injury Research Centre

2 Early Mobilisation Devas M, BMJ, 1974
3 Orthogeriatrics
4 Orthogeriatrics Reduction in complications Reduction in LOS Reduction in mortality Better functional outcomes?benefits beyond hip fracture
5 (PAC -1.8%) (PAC -7.6%) Neuburger et al. Medical Care: 2015; 53:

6 Neuburger et al Age and Ageing 2017; 46:

7 The Holy Trinity



8 25 hospitals 3519 patients 34 hospitals 5178 patients 57 hospitals 9408 patients
9 The Population Mean age 84yrs 70% female 71% from home 41% have known cognitive impairment 55% used an assistive device before the fracture

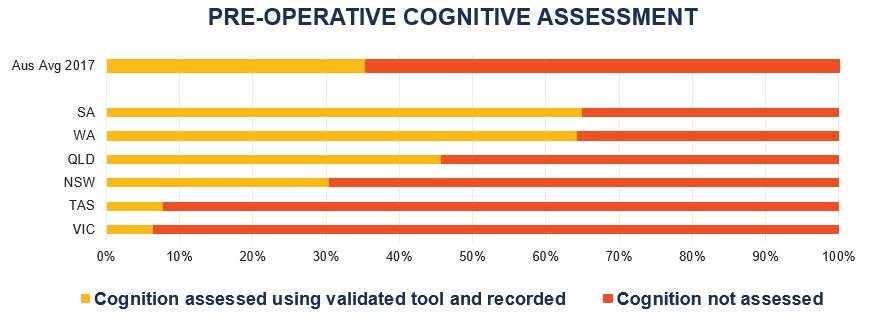
10 Pre-operative cognitive assessment
11

12 Nerve Blocks
13
14

15 Time to Surgery
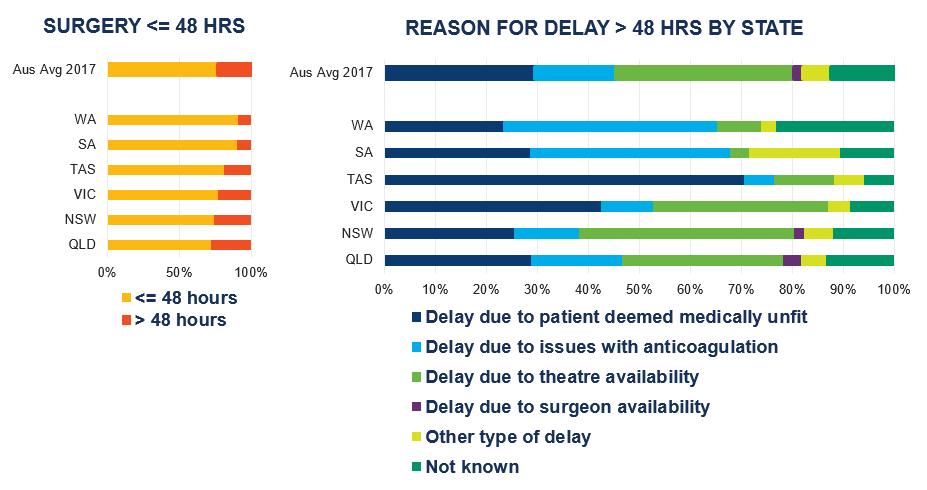
16
17 PJ Devereaux et al, CMAJ doi10:1503/cmaj
18 HIP ATTACK HIP Fracture Accelerated Surgical TreaTment And Care track Trial International randomized controlled trial of 3000 patients with a hip fracture that requires a surgical intervention. Rapid medical clearance with targeted arrival to the operating room within 6 hours of diagnosis of a hip fracture requiring surgical repair. Primary endpoints - 90 days Composite - mortality, nonfatal myocardial infarction, nonfatal pulmonary embolism, nonfatal pneumonia, nonfatal sepsis, nonfatal stroke, and nonfatal life-threatening and major bleeding All-cause mortality ClinicalTrials.gov Identifier: NCT

19 Mortality Pain Antipsychotic use Physical restraint use Pressure ulcers

20 Outcomes at 6 months If you survive 6 months and had surgery, you are less likely to have pain or a pressure injury but more likely to be physically restrained
21 31% dead at 6mths 54% dead at 6mths Berry et al, JAMA 2018, doi: /jamainternmed
22 Comfort Care After Fracture 21% utilized any form of palliative care service in the last 6 months Of those who survived 6 months, only 1.1% had a do not hospitalize order
23 Venturing beyond orthogeriatrics Why Will we add value Which patients Which specialties What will success look like
24 Geriatric Patient Not defined by age Partially defined by comorbidity Better defined by function physical and cognitive

25 Frailty associated with everything that matters

26
27 Impact of age, CCI and Frailty in the Surgical Setting All Surgical Patients Christina Norris, unpublished data
28 What to do with Frailty Screening Prognostication Decision making Intervention this is where we need more evidence
29 2018 There is evidence that CGA can improve outcomes in people with hip fracture. There are not enough studies to determine when CGA is most effective in relation to surgical intervention or if CGA is effective in surgical patients presenting with conditions other than hip fracture.
30 Multidisciplinary CGA using agreed protocols & guidelines. Tailored intervention and management plan - documented in the electronic medical record Primary outcome - LOS Surgical intervention AAA repair Lower limb by pass surgery Post-operative care delivered by the surgical team Secondary outcomes - new comorbidities, complications, dependency, delay in discharge BJS, 2017
31 Multidisciplinary CGA using agreed protocols & guidelines. Tailored intervention and management plan - documented in the electronic medical record Primary outcome - LOS Surgical intervention AAA repair Lower limb by pass surgery Post-operative care delivered by the surgical team Secondary outcomes - new comorbidities, complications, dependency, delay in discharge BJS, 2017
32 BJS, 2017


33 Cognition MOCA 30/30 Now a certified genius according to his doctor!!
34

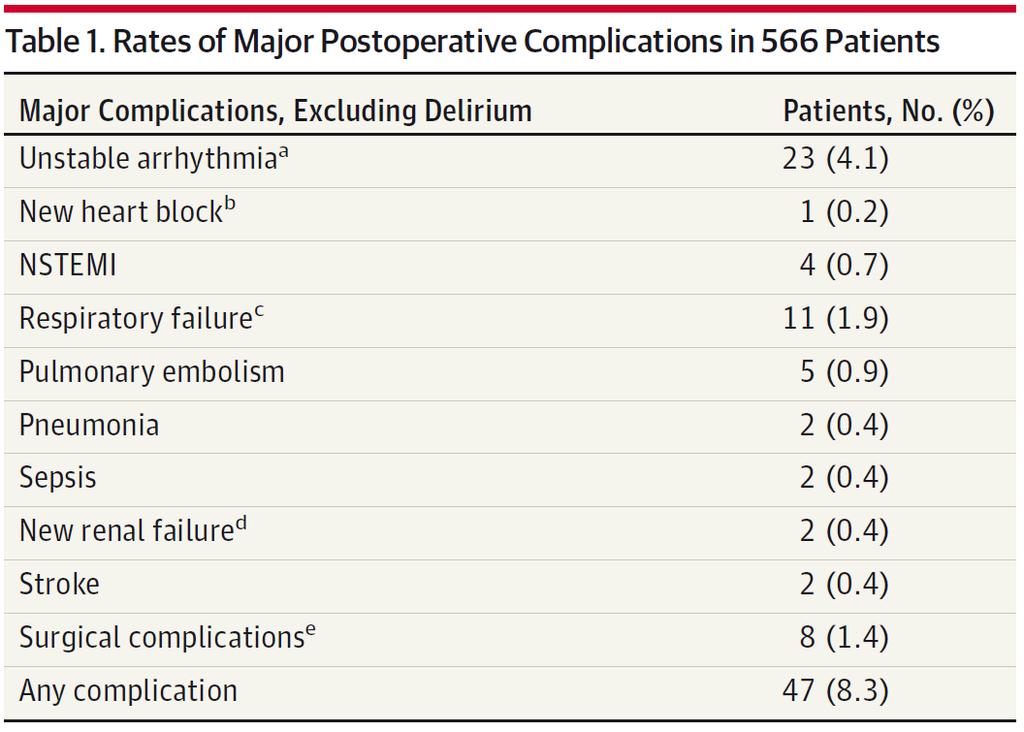
35 24% develop a delirium
36

37 Intervention 3 nursing protocols Orienting / communication Oral and nutritional assistance Early mobilisation

38
39
40 To assess the effectiveness of interventions for preventing delirium in hospitalised non-intensive Care Unit (ICU) patients. RCTs of single and multicomponent pharmacological and non-pharmacological interventions 39 trials (32 in surgical patients) 16,082 participants 22 different interventions
41 Intervention Studies Participants Quality RR Multicomponent intervention Cholinesterase inhibitors Moderate RR 0.69 ( ) Very low RR 0.68 ( ) Antipsychotics Very low RR 0.73 ( ) Haloperidol Very low RR 1.05 ( ) Olanzapine Moderate RR 0.36 ( ) Melatonin Low RR 0.41 ( ) BIS guided anaesthesia Moderate RR 0.71 ( )
42 Which Patients Age Comorbidity Function physical and cognitive Elective v Emergent Only surgical intervention Which speciality
43 COPS Observational Cohort Study Apr-Aug 2016 Delivery of Shared Care Model Sep 16-Apr 18 Evaluation of new model Ongoing

44 COPS 303 patients (140 elective, 163 emergency) Age 75+, mean age 81, 41% female 91% community dwelling 59% mobilized independently 14% cognitively impaired Christina Norris
45 Observational Cohort Study Surgery undertaken in 65% 30% in General Surgery vs 81% in Plastic Surgery Median ALOS 4.0 days Emergency admissions 5.0 days Elective 2.5 days Most patients return directly home (86%) Rehabilitation in 7% (11% vs 3% in emergency vs elective)
46 Observational Cohort Study Complication rate 40% Higher in emergency admissions (50% vs 31%) No significant difference between those who undergo surgery and those who do not (47% vs 38%) Most common complications Delirium 18% Cardiovascular (AF, CCF, ACS) 15% AKI 14% Infection 13%

47 Surgical Specialties Less than 50% screen for CI A third screened for malnutrition Less than half reviewed by physiotherapist High rates of functional decline Communication Care coordination
48 Delivery of Shared Care Model Partly pragmatic / partly informed People aged 75+ Emergency admissions Acute & general surgery Colorectal surgery Upper GI surgery Oncological surgery
49 Models of care Consult Service Invited to review Issue specific Time limited Intermittent No onus to make changes Often driven at junior level Shared Care Joint responsibility Joint accountability Shared decision making Must come from the top Mutual understanding, trust and respect
50 Models of care Consult Service Invited to review Issue specific Time limited Intermittent No onus to make changes Often driven at junior level Shared Care Joint responsibility Joint accountability Shared decision making Must come from the top Mutual understanding, trust and respect
51 INTENSIVE PHYSIO PROGRAM MULTIDISCIPLINARY CARE COORDINATION FRAIL OR UNDERGOING SURGERY COMPREHENSIVE GERIATRIC ASSESSMENT FIT VULNERABLE FRAIL END OF LIFE Clinical Frailty Scale



52 Nepean Hospital - Partners


53 799 patients seen over the study period Analysis in progress
54 Key Process and Outcome Measures Clinical Outcomes PROMs and PREMS Process Measures Complications Mortality Functional Status Experience Satisfaction LOS Cost of Care
55 Reduction in complications since the introduction of the COPS service 60% Reduction in Complications 50% 40% 30% 20% 10% 0% PRECOPS POSTCOPS

56 LOS 7.6 days to 6.9 days

57 Rate of Falls Reduced
58 Better Documentation - Nepean 80 Co-Morbidities % 40 Pre-COPS Post-COPS HT AF IHD Cog Imp Depression COPD
59 Reduced Medical Complications - Nepean 14 Complication % 8 6 Pre-COPS Post-COPS HAP AKI Arrhythmias ACS CCF Delirium

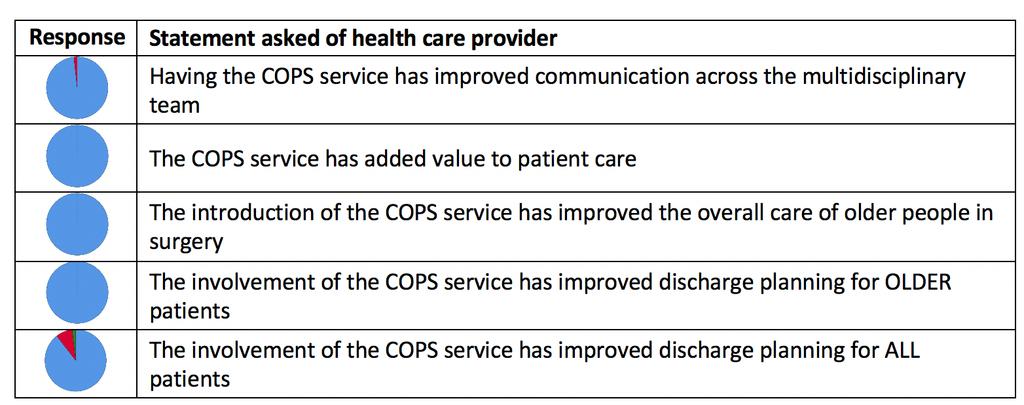
60 Patient and Staff experiences

61 3 words to describe COPS Service
62 Conclusions Orthopaedic care model well established altho still room to improve delivery / outcomes Evidence in other surgical specialties emerging Geriatric medicine needs to be clear who is its target population Do we need large RCTs?
Rehabilitation - Reducing costs and hospital stay. Dr Elizabeth Aitken Consultant Physician
 Rehabilitation - Reducing costs and hospital stay Dr Elizabeth Aitken Consultant Physician What factors affect outcome? Comorbidities Cardiac Respiratory Neurological Nutritional issues Diabetes Anaemia
Rehabilitation - Reducing costs and hospital stay Dr Elizabeth Aitken Consultant Physician What factors affect outcome? Comorbidities Cardiac Respiratory Neurological Nutritional issues Diabetes Anaemia
HIP ATTACK Trial: Can we improve outcomes after a hip fracture with accelerated surgery? PJ Devereaux, MD, PhD
 HIP ATTACK Trial: Can we improve outcomes after a hip fracture with accelerated surgery? PJ Devereaux, MD, PhD Disclosure Member of research group with policy of not accepting honorariums or other payments
HIP ATTACK Trial: Can we improve outcomes after a hip fracture with accelerated surgery? PJ Devereaux, MD, PhD Disclosure Member of research group with policy of not accepting honorariums or other payments
SAFE HIP FRACTURES. Dr Karthik Kayan MD FRCP Consultant Physician and Orthogeriatrician Stockport NHS Foundation Trust
 SAFE HIP FRACTURES Dr Karthik Kayan MD FRCP Consultant Physician and Orthogeriatrician Stockport NHS Foundation Trust Why hip fracture? Common in older adult (~84 years) UK current incidence : 70000 (Stockport
SAFE HIP FRACTURES Dr Karthik Kayan MD FRCP Consultant Physician and Orthogeriatrician Stockport NHS Foundation Trust Why hip fracture? Common in older adult (~84 years) UK current incidence : 70000 (Stockport
Breast cancer in the elderly - is there a role for the geriatrician?
 Breast cancer in the elderly - is there a role for the geriatrician? Workshop in Breast Cancer Surgery Aarhus 18 May 2016 Lone Winther Lietzen MD, PhD Department of Geriatrics, Geriatricians? Internal
Breast cancer in the elderly - is there a role for the geriatrician? Workshop in Breast Cancer Surgery Aarhus 18 May 2016 Lone Winther Lietzen MD, PhD Department of Geriatrics, Geriatricians? Internal
Hospital at Home. Frailty and Hospital at Home. 17 th March Pam Livingstone and Gwyneth Thom
 Hospital at Home Frailty and Hospital at Home 17 th March 2016 Pam Livingstone and Gwyneth Thom National Definition of Hospital at Home December 2013 An episode of specialist care delivered at home as
Hospital at Home Frailty and Hospital at Home 17 th March 2016 Pam Livingstone and Gwyneth Thom National Definition of Hospital at Home December 2013 An episode of specialist care delivered at home as
The role of the Geriatrician
 Post-operative management of the older adults with cancer The role of the Geriatrician Sofia Duque Hospital Beatriz Ângelo Geriatric University Unit Faculty of Medicine of Lisbon Geriatrics Study Group
Post-operative management of the older adults with cancer The role of the Geriatrician Sofia Duque Hospital Beatriz Ângelo Geriatric University Unit Faculty of Medicine of Lisbon Geriatrics Study Group
Aged Care and Health Services Research. A/Prof Kwang Lim Sep 2016
 Aged Care and Health Services Research A/Prof Kwang Lim Sep 2016 Accumulating evidence 20% of health care interventions is based on hard evidence. Feasibility of doing randomised controlled trials on all
Aged Care and Health Services Research A/Prof Kwang Lim Sep 2016 Accumulating evidence 20% of health care interventions is based on hard evidence. Feasibility of doing randomised controlled trials on all
Geriatric Hip Fracture Co-Management. Pannida Wattanapanom, M.D., FACP.
 Geriatric Hip Fracture Co-Management Pannida Wattanapanom, M.D., FACP. An 80 year old man with a hip fracture The General Medicine approach: Medical clearance for surgery Role of Geriatrician Assess caused
Geriatric Hip Fracture Co-Management Pannida Wattanapanom, M.D., FACP. An 80 year old man with a hip fracture The General Medicine approach: Medical clearance for surgery Role of Geriatrician Assess caused
Delirium assessment and management. Dr Kim Jeffs Northern Health
 Delirium assessment and management Dr Kim Jeffs Northern Health What do you need to know? Epidemiology How big is the problem? Who is at risk? Assessment Tools for diagnosis Prevention Evidence base Management
Delirium assessment and management Dr Kim Jeffs Northern Health What do you need to know? Epidemiology How big is the problem? Who is at risk? Assessment Tools for diagnosis Prevention Evidence base Management
Geriatric Medicine I) OBJECTIVES
 OBJECTIVES") Geriatric Medicine I) OBJECTIVES 1 To provide a broad training and in-depth experience at a level sufficient for trainees to acquire competence and professionalism required of a specialist in Geriatric
Geriatric Medicine I) OBJECTIVES 1 To provide a broad training and in-depth experience at a level sufficient for trainees to acquire competence and professionalism required of a specialist in Geriatric
Assessment and management of dementia in relation to falls risk: Tools and tips for community, hospital and residential care
 Assessment and management of dementia in relation to falls risk: Tools and tips for community, hospital and residential care Professor Jacqueline CT Close Neuroscience Research Australia Prince of Wales
Assessment and management of dementia in relation to falls risk: Tools and tips for community, hospital and residential care Professor Jacqueline CT Close Neuroscience Research Australia Prince of Wales
The Geriatrician in the Trauma Service. Trauma Quality Improvement Program (TQIP) Annual Scientific Meeting and Training 2013
 Annual Scientific Meeting and Training 2013") The Geriatrician in the Trauma Service Trauma Quality Improvement Program (TQIP) Annual Scientific Meeting and Training 2013 Challenges of the Geriatric Trauma Patient Challenges of the Geriatric Patient
The Geriatrician in the Trauma Service Trauma Quality Improvement Program (TQIP) Annual Scientific Meeting and Training 2013 Challenges of the Geriatric Trauma Patient Challenges of the Geriatric Patient
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative
 Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Role and impact of orthogeriatric service in the hip fracture care pathway: 15-year experience
 Role and impact of orthogeriatric service in the hip fracture care pathway: 15-year experience AA Fisher, MW Davis Department of Geriatric Medicine, The Canberra Hospital, and Australian National University
Role and impact of orthogeriatric service in the hip fracture care pathway: 15-year experience AA Fisher, MW Davis Department of Geriatric Medicine, The Canberra Hospital, and Australian National University
Acute care for older people with frailty
 Acute care for older people with frailty Professor Simon Conroy Clinical lead, Acute Frailty Network, England Geriatrician, University Hospitals of Leicester Worldview that will colour this talk Demography
Acute care for older people with frailty Professor Simon Conroy Clinical lead, Acute Frailty Network, England Geriatrician, University Hospitals of Leicester Worldview that will colour this talk Demography
Hip Fracture (HFR) Measures Document
 Measures Document") Hip Fracture (HFR) Measures Document HFR Version: 2 - covering patients discharged between 01/10/2017 and present. Programme Lead: Sam Doddridge Clinical Leads: Ms Phil Thorpe Dr John Tsang Number of Measures
Hip Fracture (HFR) Measures Document HFR Version: 2 - covering patients discharged between 01/10/2017 and present. Programme Lead: Sam Doddridge Clinical Leads: Ms Phil Thorpe Dr John Tsang Number of Measures
National Hip Fracture Database North West Regional Meeting 13th March 2013 Planning patient care and achieving Best Practice Tariff
 National Hip Fracture Database North West Regional Meeting 13th March 2013 Planning patient care and achieving Best Practice Tariff Dr John Tsang MB ChB, FRCP Consultant Orthogeriatrician Lead clinician
National Hip Fracture Database North West Regional Meeting 13th March 2013 Planning patient care and achieving Best Practice Tariff Dr John Tsang MB ChB, FRCP Consultant Orthogeriatrician Lead clinician
The paper provides an update for the Trust Board on hospital mortality and presents the updated Trust Mortality Action Plan.
 ENC No 13 Meeting Trust Board Date 28 th November 2013 Title of Paper Lead Director Author Hospital Mortality Update Mr Amir Khan, Medical Director Mr Amir Khan, Medical Director PURPOSE OF THE PAPER The
ENC No 13 Meeting Trust Board Date 28 th November 2013 Title of Paper Lead Director Author Hospital Mortality Update Mr Amir Khan, Medical Director Mr Amir Khan, Medical Director PURPOSE OF THE PAPER The
Management of the Frail Older Patients: What Are the Outcomes
 Management of the Frail Older Patients: What Are the Outcomes Professor Edwina Brown Imperial College Renal and Transplant Centre Hammersmith Hospital, London Increasing prevalence of old old on RRT RRT
Management of the Frail Older Patients: What Are the Outcomes Professor Edwina Brown Imperial College Renal and Transplant Centre Hammersmith Hospital, London Increasing prevalence of old old on RRT RRT
Geriatrics and Cancer Care
 Geriatrics and Cancer Care Roger Wong, BMSc, MD, FRCPC, FACP Postgraduate Dean of Medical Education Clinical Professor, Division of Geriatric Medicine UBC Faculty of Medicine Disclosure No competing interests
Geriatrics and Cancer Care Roger Wong, BMSc, MD, FRCPC, FACP Postgraduate Dean of Medical Education Clinical Professor, Division of Geriatric Medicine UBC Faculty of Medicine Disclosure No competing interests
Pre-operative Assessment of the Frail Elderly Person at Addenbrookes Hospital. Dr Fay J Gilder Consultant Anaesthetist
 Pre-operative Assessment of the Frail Elderly Person at Addenbrookes Hospital Dr Fay J Gilder Consultant Anaesthetist Frailty Models A multidimensional state of increased vulnerability Phenotype model
Pre-operative Assessment of the Frail Elderly Person at Addenbrookes Hospital Dr Fay J Gilder Consultant Anaesthetist Frailty Models A multidimensional state of increased vulnerability Phenotype model
What is the shared care model for the Hip fracture patient The Ortho-geriatric Model of Care at St Vincent s Public Hospital Our team and how we make
 What is the shared care model for the Hip fracture patient The Ortho-geriatric Model of Care at St Vincent s Public Hospital Our team and how we make it work! Benefits of a Shared Care Model The Shared
What is the shared care model for the Hip fracture patient The Ortho-geriatric Model of Care at St Vincent s Public Hospital Our team and how we make it work! Benefits of a Shared Care Model The Shared
Why New Thinking is Needed for Older Adults across the Rehabilitation Continuum
 Why New Thinking is Needed for Older Adults across the Rehabilitation Continuum Samir K. Sinha MD, DPhil, FRCPC Director of Geriatrics Mount Sinai and the University Health Network Hospitals Assistant
Why New Thinking is Needed for Older Adults across the Rehabilitation Continuum Samir K. Sinha MD, DPhil, FRCPC Director of Geriatrics Mount Sinai and the University Health Network Hospitals Assistant
Perso An. Geri-O. Objectives: fragility fracture. AL SUPPORT. presentation.
 10 th Annual Spring Conference Arizona Geriatrics Society Perso on-centered Care: An Interprofessional Panel Ana Sanguineti, MD Geri-O Ortho Hip Fracture Consult Service Banner Univer rsity Medical Center
10 th Annual Spring Conference Arizona Geriatrics Society Perso on-centered Care: An Interprofessional Panel Ana Sanguineti, MD Geri-O Ortho Hip Fracture Consult Service Banner Univer rsity Medical Center
Perioperative Care of Older People
 Perioperative Care of Older People Philip Braude, Consultant Geriatrician POPS Proactive care of Older People undergoing Surgery Guy s and St Thomas Hospital @DrPhilipBraude #AGM17conf Prevalence surgical
Perioperative Care of Older People Philip Braude, Consultant Geriatrician POPS Proactive care of Older People undergoing Surgery Guy s and St Thomas Hospital @DrPhilipBraude #AGM17conf Prevalence surgical
Understanding and Assessing for Frailty
 Understanding and Assessing for Frailty Dr Gloria Yu Clinical Head of Bexley Integrated Care Consultant Physician in Elderly, General and Stroke Medicine 8 July 2015 Learning objectives What is frailty?
Understanding and Assessing for Frailty Dr Gloria Yu Clinical Head of Bexley Integrated Care Consultant Physician in Elderly, General and Stroke Medicine 8 July 2015 Learning objectives What is frailty?
Acute front door care of frail older people. Simon Conroy Professor of Geriatric Medicine
 Acute front door care of frail older people Simon Conroy Professor of Geriatric Medicine Why is this important for physicians? Type 1 A&E attendances 11% Total Activity (Leicester) Elective admissions
Acute front door care of frail older people Simon Conroy Professor of Geriatric Medicine Why is this important for physicians? Type 1 A&E attendances 11% Total Activity (Leicester) Elective admissions
Introduction of Early Supported Discharge to Intermediate Care Pathway for Hip Fracture
 Introduction of Early Supported Discharge to Intermediate Care Pathway for Hip Fracture Neil Pendleton, Mark Brown, Heather Spence Salford Royal NHS Hospital Introduction of Early Supported Discharge to
Introduction of Early Supported Discharge to Intermediate Care Pathway for Hip Fracture Neil Pendleton, Mark Brown, Heather Spence Salford Royal NHS Hospital Introduction of Early Supported Discharge to
Lorraine Montoya, BSN, MAdEd APN / Coordinator TAVI Program. 7 April
 Using Frailty Measurement to Assist With Patient Assessment and Discharge Planning in Patients Undergoing Transcatheter Aortic Valve Implant Results of a Pilot Project Lorraine Montoya, BSN, MAdEd APN
Using Frailty Measurement to Assist With Patient Assessment and Discharge Planning in Patients Undergoing Transcatheter Aortic Valve Implant Results of a Pilot Project Lorraine Montoya, BSN, MAdEd APN
Komorbiditet og ortopædkirugi - erfaringer og viden. Benn Rønnow Duus, Ledende overlæge, Ortopædkirurgisk afdeling Bispebjerg Hospital
 Komorbiditet og ortopædkirugi - erfaringer og viden Benn Rønnow Duus, Ledende overlæge, Ortopædkirurgisk afdeling Bispebjerg Hospital Kræft og komorbiditet alle skal have del i de gode resultater 1 Kræftens
Komorbiditet og ortopædkirugi - erfaringer og viden Benn Rønnow Duus, Ledende overlæge, Ortopædkirurgisk afdeling Bispebjerg Hospital Kræft og komorbiditet alle skal have del i de gode resultater 1 Kræftens
Acute Care of Older Surgical Patients. Dr Shane O Hanlon Consultant Geriatrician St Vincent s University Hospital IHFM 8 th Nov 2017
 Acute Care of Older Surgical Patients Dr Shane O Hanlon Consultant Geriatrician St Vincent s University Hospital IHFM 8 th Nov 2017 NCEPOD 2010 overall care % 50 45 40 35 30 25 20 15 10 5 0 Good practice
Acute Care of Older Surgical Patients Dr Shane O Hanlon Consultant Geriatrician St Vincent s University Hospital IHFM 8 th Nov 2017 NCEPOD 2010 overall care % 50 45 40 35 30 25 20 15 10 5 0 Good practice
Identifying patients at risk of delirium: a project for patients undergoing elective orthopedic surgery. The next steps in orthogeriatrics
 Identifying patients at risk of delirium: a project for patients undergoing elective orthopedic surgery Dr. John Joanisse, Chantal Chabot NP The next steps in orthogeriatrics Background More than 8 years
Identifying patients at risk of delirium: a project for patients undergoing elective orthopedic surgery Dr. John Joanisse, Chantal Chabot NP The next steps in orthogeriatrics Background More than 8 years
Nutrition in the critically ill elderly (geriatric) patient CHRISTINA NIEUWOUDT RD(SA) SASPEN/CCSSA CONGRESS 2017
 patient CHRISTINA NIEUWOUDT RD(SA) SASPEN/CCSSA CONGRESS 2017") Nutrition in the critically ill elderly (geriatric) patient CHRISTINA NIEUWOUDT RD(SA) SASPEN/CCSSA CONGRESS 2017 CONTENT WHO is the critically ill elderly (geriatric) patient? WHY look at the critically
Nutrition in the critically ill elderly (geriatric) patient CHRISTINA NIEUWOUDT RD(SA) SASPEN/CCSSA CONGRESS 2017 CONTENT WHO is the critically ill elderly (geriatric) patient? WHY look at the critically
Trial clinici nell anziano: efficacy or effectiveness?
 LA SPERIMENTAZIONE FARMACOLOGICA CLINICA IN ETÀ GERIATRICA Trial clinici nell anziano: efficacy or effectiveness? Graziano Onder Fondazione Universitaria Policlinico A. Gemelli Università Cattolica del
LA SPERIMENTAZIONE FARMACOLOGICA CLINICA IN ETÀ GERIATRICA Trial clinici nell anziano: efficacy or effectiveness? Graziano Onder Fondazione Universitaria Policlinico A. Gemelli Università Cattolica del
Define frailty Recognise the consequences of frailty Know why CGA important and what are the main components of a CGA that can be done in an initial
 Dr Kyra Neubauer Define frailty Recognise the consequences of frailty Know why CGA important and what are the main components of a CGA that can be done in an initial assessment Understand what are potential
Dr Kyra Neubauer Define frailty Recognise the consequences of frailty Know why CGA important and what are the main components of a CGA that can be done in an initial assessment Understand what are potential
Chirurgie Ziekenhuisgroep Twente Locatie Almelo. Disclosure presenter
 Disclosure presenter The effectiveness of integrated orthogeriatric treatment on 1-year outcome in frail elderly withhip fracture E. Folbert, MANP, PhD Hospital Group, Almelo-Hengelo Rotterdam, 2018 august
Disclosure presenter The effectiveness of integrated orthogeriatric treatment on 1-year outcome in frail elderly withhip fracture E. Folbert, MANP, PhD Hospital Group, Almelo-Hengelo Rotterdam, 2018 august
The Experience in Exeter with. hip fracture care. Data For Change
 The Experience in Exeter with hip fracture care Data For Change John Charity Associate Specialist in T&O, Lead NHFD Clinician, Royal Devon and Exeter NHS Foundation Trust Respond Deliver & Enable People
The Experience in Exeter with hip fracture care Data For Change John Charity Associate Specialist in T&O, Lead NHFD Clinician, Royal Devon and Exeter NHS Foundation Trust Respond Deliver & Enable People
Hip Fracture from audit into action
 Hip Fracture from audit into action Antony Johansen Orthogeriatrician Trauma Unit University Hospital of Wales, Cardiff National Hip Fracture Database Royal College of Physicians, London Global projections
Hip Fracture from audit into action Antony Johansen Orthogeriatrician Trauma Unit University Hospital of Wales, Cardiff National Hip Fracture Database Royal College of Physicians, London Global projections
Improving the quality of care of patients with delirium
 Improving the quality of care of patients with delirium Alasdair MacLullich MRCP(UK), PhD Professor of Geriatric Medicine University of Edinburgh Scotland How are we doing now? We are doing badly. Difficult
Improving the quality of care of patients with delirium Alasdair MacLullich MRCP(UK), PhD Professor of Geriatric Medicine University of Edinburgh Scotland How are we doing now? We are doing badly. Difficult
Improving Healthcare Utilization in Injured Older Adults
 Improving Healthcare Utilization in Injured Older Adults G ERIATRIC T R A U MA I N I T I AT I V E S AT S TA N F O R D H E A LT H C A R E J U LY 12, 2018 Objectives Background on Geriatric Trauma Population
Improving Healthcare Utilization in Injured Older Adults G ERIATRIC T R A U MA I N I T I AT I V E S AT S TA N F O R D H E A LT H C A R E J U LY 12, 2018 Objectives Background on Geriatric Trauma Population
The Relationship between Multimorbidity and Concordant and Discordant Causes of Hospital Readmission at 30 Days and One Year
 The Relationship between Multimorbidity and Concordant and Discordant Causes of Hospital Readmission at 30 Days and One Year Arlene S. Bierman, M.D., M.S Professor, University of Toronto and Scientist,
The Relationship between Multimorbidity and Concordant and Discordant Causes of Hospital Readmission at 30 Days and One Year Arlene S. Bierman, M.D., M.S Professor, University of Toronto and Scientist,
There s No Place like Home
 THERE S NO PLACE LIKE HOME There s No Place like Home Regional Advisory Committee for Excellence in Care of Older Adults Elements of the Program TAKE AWAY SERVICES R & G PROGRAM CONSULTATION O SERVICES
THERE S NO PLACE LIKE HOME There s No Place like Home Regional Advisory Committee for Excellence in Care of Older Adults Elements of the Program TAKE AWAY SERVICES R & G PROGRAM CONSULTATION O SERVICES
Development of Guidelines to Manage Geriatric Trauma Patients. Kelly Czarnecki MS,FNP
 Development of Guidelines to Manage Geriatric Trauma Patients Kelly Czarnecki MS,FNP No Disclosures Disclosures Project Introduction According to best practice recommendations the geriatric trauma population
Development of Guidelines to Manage Geriatric Trauma Patients Kelly Czarnecki MS,FNP No Disclosures Disclosures Project Introduction According to best practice recommendations the geriatric trauma population
Vision for quality: A framework for action - technical document
 3. Frailty Vision for quality: A framework for action - technical document Contents 1.0 Introduction 1 2.0 The current situation in Warwickshire North 2 3.0 The case for change 4 4.0 Views and opinions
3. Frailty Vision for quality: A framework for action - technical document Contents 1.0 Introduction 1 2.0 The current situation in Warwickshire North 2 3.0 The case for change 4 4.0 Views and opinions
Integrating Medical and Social Support for Elderly System & Technology Enabled Service Innovations. Dr Christina MAW Hospital Authority, Hong Kong
 Integrating Medical and Social Support for Elderly System & Technology Enabled Service Innovations Dr Christina MAW Hospital Authority, Hong Kong Hospital Authority (HA) of Hong Kong A statutory body responsible
Integrating Medical and Social Support for Elderly System & Technology Enabled Service Innovations Dr Christina MAW Hospital Authority, Hong Kong Hospital Authority (HA) of Hong Kong A statutory body responsible
Medico-Social Impact of Fragility Fracture 11/2/2014. Dr David Dai Consultant Geriatrician Prince of Wales Hospital 24 th January, 2014
 Medico-Social Impact of Fragility Fracture Dr David Dai Consultant Geriatrician Prince of Wales Hospital 24 th January, 2014 2014 Policy Agenda As Hong Kong moves steadily to an ageing society (with the
Medico-Social Impact of Fragility Fracture Dr David Dai Consultant Geriatrician Prince of Wales Hospital 24 th January, 2014 2014 Policy Agenda As Hong Kong moves steadily to an ageing society (with the
Guidelines to standards. Orthogeriatrics How The UK Care For Fragility Fractures
 Guidelines to standards Orthogeriatrics How The UK Care For Fragility Fractures Karen Hertz-SOTN Advanced Nurse Practitioner The NHFD Project - jointly led by BOA and BGS with the involvement of the RCN
Guidelines to standards Orthogeriatrics How The UK Care For Fragility Fractures Karen Hertz-SOTN Advanced Nurse Practitioner The NHFD Project - jointly led by BOA and BGS with the involvement of the RCN
Blood transfusions in ICU: double-edged sword. Paul Hébert, MD MHSc(Epid) Physician-in-Chief, CHUM Professor, University of Montreal
 Physician-in-Chief, CHUM Professor, University of Montreal") Blood transfusions in ICU: double-edged sword Paul Hébert, MD MHSc(Epid) Physician-in-Chief, CHUM Professor, University of Montreal Canadian Critical Care Trials Group Collaborating for Impact Leading
Blood transfusions in ICU: double-edged sword Paul Hébert, MD MHSc(Epid) Physician-in-Chief, CHUM Professor, University of Montreal Canadian Critical Care Trials Group Collaborating for Impact Leading
Disclosures. Personalized Approaches to Gastrointestinal Cancers. Objectives. What is personalized cancer care. Go through some genomic studies
 Personalized Approaches to Gastrointestinal Cancers Emily Groves, MD Colorectal Surgery Assistant Professor, Division of Surgical Oncology Disclosures None Objectives What is personalized medicine and
Personalized Approaches to Gastrointestinal Cancers Emily Groves, MD Colorectal Surgery Assistant Professor, Division of Surgical Oncology Disclosures None Objectives What is personalized medicine and
Care & Support Planning/Advanced Care Planning for people living with frailty John Young
 Care & Support Planning/Advanced Care Planning for people living with frailty John Young Geriatrician, Bradford Hospitals Trust National Clinical Director for Integration & Frail Elderly, NHS England (john.young@bthft.nhs.uk)
Care & Support Planning/Advanced Care Planning for people living with frailty John Young Geriatrician, Bradford Hospitals Trust National Clinical Director for Integration & Frail Elderly, NHS England (john.young@bthft.nhs.uk)
Dementia in the acute hospital setting what should we be doing and who should be doing it?
 Dementia in the acute hospital setting what should we be doing and who should be doing it? Sarah Pendlebury Consultant Physician and Associate Professor NIHR Oxford Biomedical Research Centre Departments
Dementia in the acute hospital setting what should we be doing and who should be doing it? Sarah Pendlebury Consultant Physician and Associate Professor NIHR Oxford Biomedical Research Centre Departments
UND GERIATRIC MEDICINE FELLOWSHIP CURRICULUM ACUTE CARE
 LOCATION SITE Sanford Medical Center Fargo 5225 23rd Avenue S Fargo, ND 58104 CONTACT LEAD FACULTY MEMBER Dr. Darin Lang Darin.lang@sanfordhealth.org PROGRAM CONTACT Dr. Gunjan Manocha gunjan.dhawan@und.edu
LOCATION SITE Sanford Medical Center Fargo 5225 23rd Avenue S Fargo, ND 58104 CONTACT LEAD FACULTY MEMBER Dr. Darin Lang Darin.lang@sanfordhealth.org PROGRAM CONTACT Dr. Gunjan Manocha gunjan.dhawan@und.edu
Acute care for older people with frailty
 Acute care for older people with frailty Professor Simon Conroy Clinical lead, Acute Frailty Network, England Geriatrician, University Hospitals of Leicester CONFLICT OF INTEREST DISCLOSURE I have the
Acute care for older people with frailty Professor Simon Conroy Clinical lead, Acute Frailty Network, England Geriatrician, University Hospitals of Leicester CONFLICT OF INTEREST DISCLOSURE I have the
Acute care for older people with frailty
 Acute care for older people with frailty Professor Simon Conroy Clinical lead, Acute Frailty Network, England Geriatrician, University Hospitals of Leicester Why acute frailty? Demography Absence of immortality
Acute care for older people with frailty Professor Simon Conroy Clinical lead, Acute Frailty Network, England Geriatrician, University Hospitals of Leicester Why acute frailty? Demography Absence of immortality
Implementing a new Orthogeriatric model to improve patient care and outcomes Aiming for Excellence!
 Implementing a new Orthogeriatric model to improve patient care and outcomes Aiming for Excellence! Introduction Hip fractures effect 70,000 people in UK Central challenge for UK Trauma services- 560 in
Implementing a new Orthogeriatric model to improve patient care and outcomes Aiming for Excellence! Introduction Hip fractures effect 70,000 people in UK Central challenge for UK Trauma services- 560 in
Old age, polymorbidity and stroke, a new epidemy?
 Old age, polymorbidity and stroke, a new epidemy? Professor Gary Ford Chief Executive Officer, Oxford Academic Health Science Network Consultant Stroke Physician, Oxford University Hospitals Visiting Professor
Old age, polymorbidity and stroke, a new epidemy? Professor Gary Ford Chief Executive Officer, Oxford Academic Health Science Network Consultant Stroke Physician, Oxford University Hospitals Visiting Professor
The Community Assessment of Risk and Treatment Strategies (CARTS) Project. Professor D. William Molloy COLLAGE University College Cork, Ireland.
 Project. Professor D. William Molloy COLLAGE University College Cork, Ireland.") The Community Assessment of Risk and Treatment Strategies (CARTS) Project Professor D. William Molloy COLLAGE University College Cork, Ireland. Centre for Gerontology and Rehabilitation A time of limited
The Community Assessment of Risk and Treatment Strategies (CARTS) Project Professor D. William Molloy COLLAGE University College Cork, Ireland. Centre for Gerontology and Rehabilitation A time of limited
DELIRIUM. J. Sukanya 28.Jun.12
 DELIRIUM J. Sukanya 28.Jun.12 Outline Why? What? How? What s next? Delirium Introduction Delirium An acute decline in attention and cognition The most frequent neuropsychiatric syndrome A common, life-threatening,
DELIRIUM J. Sukanya 28.Jun.12 Outline Why? What? How? What s next? Delirium Introduction Delirium An acute decline in attention and cognition The most frequent neuropsychiatric syndrome A common, life-threatening,
The Healthy User Effect: Ubiquitous and Uncontrollable S. R. Majumdar, MD MPH FRCPC FACP
 The Healthy User Effect: Ubiquitous and Uncontrollable S. R. Majumdar, MD MPH FRCPC FACP Professor of Medicine, Endowed Chair in Patient Health Management, Health Scholar of the Alberta Heritage Foundation,
The Healthy User Effect: Ubiquitous and Uncontrollable S. R. Majumdar, MD MPH FRCPC FACP Professor of Medicine, Endowed Chair in Patient Health Management, Health Scholar of the Alberta Heritage Foundation,
Critical illness- A new co-morbidity?
 Critical illness- A new co-morbidity? Brian H Cuthbertson Chief, Department of Critical Care Medicine Sunnybrook Health Sciences Centre Professor of Anaesthesia University of Toronto Toronto, Canada Critical
Critical illness- A new co-morbidity? Brian H Cuthbertson Chief, Department of Critical Care Medicine Sunnybrook Health Sciences Centre Professor of Anaesthesia University of Toronto Toronto, Canada Critical
Delirium in the Elderly
 Delirium in the Elderly ELITE 2015 Mamata Yanamadala M.B.B.S, MS Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity
Delirium in the Elderly ELITE 2015 Mamata Yanamadala M.B.B.S, MS Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity
How to disseminate the Acute Care for Elders (ACE) model of care beyond one unit
 model of care beyond one unit") How to disseminate the Acute Care for Elders (ACE) model of care beyond one unit Roger Wong, BMSc, MD, FRCPC, FACP Clinical Professor, Division of Geriatric Medicine Associate Dean, Postgraduate Medical
How to disseminate the Acute Care for Elders (ACE) model of care beyond one unit Roger Wong, BMSc, MD, FRCPC, FACP Clinical Professor, Division of Geriatric Medicine Associate Dean, Postgraduate Medical
Preop risk stratification & postop management in elderly cancer patients
 Preop risk stratification & postop management in elderly cancer patients laudia Spies Klinik für Anästhesiologie und Intensivmedizin ampus Virchow-Klinikum und ampus harité Mitte U N I V E R S I T Ä T
Preop risk stratification & postop management in elderly cancer patients laudia Spies Klinik für Anästhesiologie und Intensivmedizin ampus Virchow-Klinikum und ampus harité Mitte U N I V E R S I T Ä T
Risk Factors for Falls in Cognitive Impairment
 Risk Factors for Falls in Cognitive Impairment A/Prof Jacqueline Close Falls and Injury Prevention Group NeuRA Prince of Wales Clinical School University of New South Wales Background Epidemiology of falls
Risk Factors for Falls in Cognitive Impairment A/Prof Jacqueline Close Falls and Injury Prevention Group NeuRA Prince of Wales Clinical School University of New South Wales Background Epidemiology of falls
PREVENTION AND MANAGEMENT OF FRAILTY. Christopher Patterson John Feightner for the Canadian Initiative on frailty and Aging 2006
 PREVENTION AND MANAGEMENT OF FRAILTY Christopher Patterson John Feightner for the Canadian Initiative on frailty and Aging 2006 Prevention & management Avoidance of definition of frailty SER of RCTs addressing
PREVENTION AND MANAGEMENT OF FRAILTY Christopher Patterson John Feightner for the Canadian Initiative on frailty and Aging 2006 Prevention & management Avoidance of definition of frailty SER of RCTs addressing
Professor Brian Draper
 Understanding what s different for patients with dementia in acute care hospitals coalface implications Psychiatry Professor Brian Draper UNSW & Prince of Wales Hospital, Randwick Background Previous analyses
Understanding what s different for patients with dementia in acute care hospitals coalface implications Psychiatry Professor Brian Draper UNSW & Prince of Wales Hospital, Randwick Background Previous analyses
Delirium and cognitive impairment in the perioperative
 Delirium and cognitive impairment in the perioperative period Richard Sztramko Assistant Professor, McMaster University Divisions of Geriatrics and General Internal Medicine Disclosures Chief Medical Officer
Delirium and cognitive impairment in the perioperative period Richard Sztramko Assistant Professor, McMaster University Divisions of Geriatrics and General Internal Medicine Disclosures Chief Medical Officer
Wirral University Teaching Hospital NHS Foundation Trust. Advancing Quality Results October 2008 to June 2017
 Wirral University Teaching Hospital NHS Foundation Trust Advancing Quality Results October 2008 to June 2017 Wirral University Teaching Hospital NHS Foundation Trust Participation Summary Y1 Y2 Y3 Y4 Y5
Wirral University Teaching Hospital NHS Foundation Trust Advancing Quality Results October 2008 to June 2017 Wirral University Teaching Hospital NHS Foundation Trust Participation Summary Y1 Y2 Y3 Y4 Y5
COGNITIVE IMPAIRMENT IN
 COGNITIVE IMPAIRMENT IN THE HOSPITAL SETTING Professor Len Gray April 2014 Some key questions How common is cognitive impairment among hospitalised older patients? Which cognitive syndromes are associated
COGNITIVE IMPAIRMENT IN THE HOSPITAL SETTING Professor Len Gray April 2014 Some key questions How common is cognitive impairment among hospitalised older patients? Which cognitive syndromes are associated
New York City Development of the Geriatric Collaborative
 New York City - 2014 Development of the Geriatric Collaborative The Clinical Problem More than 50% persons age 65 years will have some surgical procedure in the remainder of his or her lifetime Outcome
New York City - 2014 Development of the Geriatric Collaborative The Clinical Problem More than 50% persons age 65 years will have some surgical procedure in the remainder of his or her lifetime Outcome
Falls & Injury Prevention Reflections and Projections Jacqueline CT Close
 Falls & Injury Prevention Reflections and Projections Jacqueline CT Close Orthogeriatrician Prince of Wales Hospital Director - Falls and Injury Prevention Group, NeuRA Conjoint Professor - Prince of Wales
Falls & Injury Prevention Reflections and Projections Jacqueline CT Close Orthogeriatrician Prince of Wales Hospital Director - Falls and Injury Prevention Group, NeuRA Conjoint Professor - Prince of Wales
Warrington And Halton Hospitals NHS Foundation Trust. Advancing Quality Results October 2008 to June 2017
 Warrington And Halton Hospitals NHS Foundation Trust Advancing Quality Results October 2008 to June 2017 Warrington And Halton Hospitals NHS Foundation Trust Participation Summary Y1 Y2 Y3 Y4 Y5 Y6 Acute
Warrington And Halton Hospitals NHS Foundation Trust Advancing Quality Results October 2008 to June 2017 Warrington And Halton Hospitals NHS Foundation Trust Participation Summary Y1 Y2 Y3 Y4 Y5 Y6 Acute
Aintree University Hospital NHS Foundation Trust. Advancing Quality Results October 2008 to June 2017
 Aintree University Hospital NHS Foundation Trust Advancing Quality Results October 2008 to June 2017 Aintree University Hospital NHS Foundation Trust Participation Summary Y1 Y2 Y3 Y4 Y5 Y6 Acute Kidney
Aintree University Hospital NHS Foundation Trust Advancing Quality Results October 2008 to June 2017 Aintree University Hospital NHS Foundation Trust Participation Summary Y1 Y2 Y3 Y4 Y5 Y6 Acute Kidney
Aintree University Hospital NHS Foundation Trust. Advancing Quality Results October 2008 to December 2017
 Aintree University Hospital NHS Foundation Trust Advancing Quality Results October 2008 to December 2017 Aintree University Hospital Participation Summary Y1 Y2 Y3 Y4 Y5 Y6 Acute Kidney Injury - - - -
Aintree University Hospital NHS Foundation Trust Advancing Quality Results October 2008 to December 2017 Aintree University Hospital Participation Summary Y1 Y2 Y3 Y4 Y5 Y6 Acute Kidney Injury - - - -
EMU A NEW MODEL OF EMERGENCY CARE FOR THE FRAIL & ELDERLY
 EMU A NEW MODEL OF EMERGENCY CARE FOR THE FRAIL & ELDERLY Geriatrics, General practice, Emergency medicine, Interface medicine SUMMARY An integrated, community emergency service specifically designed for
EMU A NEW MODEL OF EMERGENCY CARE FOR THE FRAIL & ELDERLY Geriatrics, General practice, Emergency medicine, Interface medicine SUMMARY An integrated, community emergency service specifically designed for
2O18 ANNUAL REPORT SUPPLEMENTARY REPORT
 2O18 ANNUAL REPORT SUPPLEMENTARY REPORT Enhancing Outcomes for Older People ABBREVIATIONS AND DEFINITIONS For the purposes of this report, the following interpretation of terms should be used. ACT Australian
2O18 ANNUAL REPORT SUPPLEMENTARY REPORT Enhancing Outcomes for Older People ABBREVIATIONS AND DEFINITIONS For the purposes of this report, the following interpretation of terms should be used. ACT Australian
Integrating Geriatrics into Oncology Care
 Integrating Geriatrics into Oncology Care William Dale, MD, PhD Chief, Geriatrics & Palliative Medicine Director, Specialized Oncology Care & Research in the Elderly (SOCARE) Clinic University of Chicago
Integrating Geriatrics into Oncology Care William Dale, MD, PhD Chief, Geriatrics & Palliative Medicine Director, Specialized Oncology Care & Research in the Elderly (SOCARE) Clinic University of Chicago
Delirium. Dr. John Puxty
 Delirium Dr. John Puxty Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors, causes and main
Delirium Dr. John Puxty Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors, causes and main
Acute NIV in COPD and what happens next. Dr Rachael Evans PhD Associate Professor, Respiratory Medicine, Glenfield Hospital
 Acute NIV in COPD and what happens next Dr Rachael Evans PhD Associate Professor, Respiratory Medicine, Glenfield Hospital Content Scenarios Evidence based medicine for the first 24 hrs Who should we refer
Acute NIV in COPD and what happens next Dr Rachael Evans PhD Associate Professor, Respiratory Medicine, Glenfield Hospital Content Scenarios Evidence based medicine for the first 24 hrs Who should we refer
Patient Blood Management: Enough is Enough
 Patient Blood Management: Enough is Enough Richard Benjamin, MBChB, PhD, FRCPath Professor of Pathology Georgetown University Medical Center Washington, D.C. Chief Medical Officer Cerus Corporation Concord,
Patient Blood Management: Enough is Enough Richard Benjamin, MBChB, PhD, FRCPath Professor of Pathology Georgetown University Medical Center Washington, D.C. Chief Medical Officer Cerus Corporation Concord,
Fall-related hip fracture in NSW Epidemiology, evidence, practice and the future
 Fall-related hip fracture in NSW Epidemiology, evidence, practice and the future Jacqueline CT Close Orthogeriatrician, Prince of Wales Hospital Director - Falls and Injury Prevention Group Neuroscience
Fall-related hip fracture in NSW Epidemiology, evidence, practice and the future Jacqueline CT Close Orthogeriatrician, Prince of Wales Hospital Director - Falls and Injury Prevention Group Neuroscience
5 older patients become delirious every minute
 Management of Delirium: Nonpharmacologic and Pharmacologic Approaches Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley
Management of Delirium: Nonpharmacologic and Pharmacologic Approaches Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley
Hips & Knees Priority Action Team
 Hips & Knees Priority Action Team Current State Data Refresh September 5, 27 Overview Population Profile Health Status Utilization of Hip & Knee Total Joint Services 1 1 Population Profile 2 SouthWest
Hips & Knees Priority Action Team Current State Data Refresh September 5, 27 Overview Population Profile Health Status Utilization of Hip & Knee Total Joint Services 1 1 Population Profile 2 SouthWest
Update in Geriatrics: Choosing Wisely Primum Non Nocere
 Joseph G. Ouslander, M.D. Professor of Clinical Biomedical Science Senior Associate Dean for Geriatric Programs Chair, Department of Integrated Medical Science Charles E. Schmidt College of Medicine Professor
Joseph G. Ouslander, M.D. Professor of Clinical Biomedical Science Senior Associate Dean for Geriatric Programs Chair, Department of Integrated Medical Science Charles E. Schmidt College of Medicine Professor
01/07/2018 ISCHAEMIC PAIN IN NON-RECONSTRUCTABLE CRITICAL LIMB ISCHAEMIA PRESENTATION OUTLINE
 ISCHAEMIC PAIN IN NON-RECONSTRUCTABLE CRITICAL LIMB ISCHAEMIA Dr. Áine Ní Laoire The Oxford Advanced Pain & Symptom Management Course Nottingham 27 th June 2018 PRESENTATION OUTLINE A Typical Case Background
ISCHAEMIC PAIN IN NON-RECONSTRUCTABLE CRITICAL LIMB ISCHAEMIA Dr. Áine Ní Laoire The Oxford Advanced Pain & Symptom Management Course Nottingham 27 th June 2018 PRESENTATION OUTLINE A Typical Case Background
Delirium in the Elderly
 Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
JAMA, January 11, 2012 Vol 307, No. 2
 JAMA, January 11, 2012 Vol 307, No. 2 Dementia is associated with increased rates and often poorer outcomes of hospitalization Worsening cognitive status Adequate chronic disease management is more difficult
JAMA, January 11, 2012 Vol 307, No. 2 Dementia is associated with increased rates and often poorer outcomes of hospitalization Worsening cognitive status Adequate chronic disease management is more difficult
The Challenges of Managing the Older Persons
 IAG Presidential Oration The Challenges of Managing the Older Persons G.S. Shanthi Professor & Head, Department of Geriatric Medicine, Madras Medical College, Chennai Globally, due to shifting demographics,
IAG Presidential Oration The Challenges of Managing the Older Persons G.S. Shanthi Professor & Head, Department of Geriatric Medicine, Madras Medical College, Chennai Globally, due to shifting demographics,
Quality of Acute Care for Older Persons with Dementia
 Quality of Acute Care for Older Persons with Dementia A Hospital-Based Pilot Study Chien-Liang Liu Center for Geriatrics and Gerontology, Taipei Veterans General Hospital, Taiwan 2013/04/20 Outline Background
Quality of Acute Care for Older Persons with Dementia A Hospital-Based Pilot Study Chien-Liang Liu Center for Geriatrics and Gerontology, Taipei Veterans General Hospital, Taiwan 2013/04/20 Outline Background
Pennine Acute Hospitals NHS Trust. Advancing Quality Results October 2008 to December 2016
 Pennine Acute Hospitals NHS Trust Advancing Quality Results October 2008 to December 2016 Pennine Acute Hospitals NHS Trust Participation Summary Y1 Y2 Y3 Y4 Y5 Y6 Acute Kidney Injury - - - - - - - Alcohol
Pennine Acute Hospitals NHS Trust Advancing Quality Results October 2008 to December 2016 Pennine Acute Hospitals NHS Trust Participation Summary Y1 Y2 Y3 Y4 Y5 Y6 Acute Kidney Injury - - - - - - - Alcohol
Scottish Standards of Care for Hip Fracture Patients
 Scottish Standards of Care for Hip Fracture Patients This document has been prepared in collaboration with Healthcare Improvement Scotland to align with the forthcoming updated Older People in Hospitals
Scottish Standards of Care for Hip Fracture Patients This document has been prepared in collaboration with Healthcare Improvement Scotland to align with the forthcoming updated Older People in Hospitals
Royal Liverpool And Broadgreen University Hospitals NHS Trust. Advancing Quality Results October 2008 to June 2017
 Royal Liverpool And Broadgreen University Hospitals NHS Trust Advancing Quality Results October 2008 to June 2017 Royal Liverpool And Broadgreen University Hospitals NHS Trust Participation Summary Y1
Royal Liverpool And Broadgreen University Hospitals NHS Trust Advancing Quality Results October 2008 to June 2017 Royal Liverpool And Broadgreen University Hospitals NHS Trust Participation Summary Y1
Karl Sash, MD Board Certified: Internal Medicine, Geriatrics, and Hospice and Palliative Medicine Medical Director, St Mary s Palliative Care
 Karl Sash, MD Board Certified: Internal Medicine, Geriatrics, and Hospice and Palliative Medicine Medical Director, St Mary s Palliative Care (Inpatient) Medical Director, Aseracare Hospice Evansville
Karl Sash, MD Board Certified: Internal Medicine, Geriatrics, and Hospice and Palliative Medicine Medical Director, St Mary s Palliative Care (Inpatient) Medical Director, Aseracare Hospice Evansville
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acute coronary syndrome (ACS), burden of condition, 83 diagnosis of, 82 83 evaluation of, 83, 87 major complications of, 86 risk for,
Index Note: Page numbers of article titles are in boldface type. A Acute coronary syndrome (ACS), burden of condition, 83 diagnosis of, 82 83 evaluation of, 83, 87 major complications of, 86 risk for,
Healthcare, hospitals and the challenges of an ageing population
 Healthcare, hospitals and the challenges of an ageing population Prof David Oliver Vice President, RCP, London Past President, British Geriatrics Society Senior Visiting Fellow, King s Fund Consultant
Healthcare, hospitals and the challenges of an ageing population Prof David Oliver Vice President, RCP, London Past President, British Geriatrics Society Senior Visiting Fellow, King s Fund Consultant
Delirium: Prevention with Melatonin
 Delirium: Prevention with Melatonin Lisa Burry, PharmD Department of Pharmacy, Mount Sinai Hospital Leslie Dan Faculty of Pharmacy, University of Toronto Disclosures Centre for Collaborative Drug Research,
Delirium: Prevention with Melatonin Lisa Burry, PharmD Department of Pharmacy, Mount Sinai Hospital Leslie Dan Faculty of Pharmacy, University of Toronto Disclosures Centre for Collaborative Drug Research,
Interprofessional Care for Elders through 48/5
 Interprofessional Care for Elders through 48/5 Janet E. McElhaney, MD, FRCPC, FACP HSN Volunteer Association Chair in Geriatric Research Professor of Medicine, Northern Ontario School of Medicine Health
Interprofessional Care for Elders through 48/5 Janet E. McElhaney, MD, FRCPC, FACP HSN Volunteer Association Chair in Geriatric Research Professor of Medicine, Northern Ontario School of Medicine Health
Test and Learn Community Frailty Service for frail housebound patients and those living in care homes in South Gloucestershire
 Test and Learn Community Frailty Service for frail housebound patients and those living in care homes in South Gloucestershire Introduction This document introduces South Gloucestershire Clinical Commissioning
Test and Learn Community Frailty Service for frail housebound patients and those living in care homes in South Gloucestershire Introduction This document introduces South Gloucestershire Clinical Commissioning
Transfusion & Mortality. Philippe Van der Linden MD, PhD
 Transfusion & Mortality Philippe Van der Linden MD, PhD Conflict of Interest Disclosure In the past 5 years, I have received honoraria or travel support for consulting or lecturing from the following companies:
Transfusion & Mortality Philippe Van der Linden MD, PhD Conflict of Interest Disclosure In the past 5 years, I have received honoraria or travel support for consulting or lecturing from the following companies:
Mental Health in STH Mike Richmond, Medical Director Mark Cobb, Clinical Director of Professional Services Debate & Note
 SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST EXECUTIVE SUMMARY REPORT TO THE TRUST HEALTHCARE GOVERNANCE COMMITTEE E TO BE HELD ON 27 FEBRUARY 2012 Subject: Supporting Director: Author: Status 1 Mental
SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST EXECUTIVE SUMMARY REPORT TO THE TRUST HEALTHCARE GOVERNANCE COMMITTEE E TO BE HELD ON 27 FEBRUARY 2012 Subject: Supporting Director: Author: Status 1 Mental