A Tale of two specialties Merging Palliative care into Critical Care
|
|
|
- Peregrine Fields
- 5 years ago
- Views:
Transcription


1 A Tale of two specialties Merging Palliative care into Critical Care Dr. Cora WS Yau ICU Journal presentation 30/8/2011
2 Introduction Death in the Intensive Care Unit (ICU) is often inevitable ~ 20% (ranged from 6 to 41%) of patients die before discharge Unsuccessful intensive care Maximized medical support with advanced technology Maximizing comfort Discussion of medical futility of treatment and end-of-life issue is given less attention
3 Introduction Family conferences, spiritual care, social worker interview were not well-recorded in the ICU medical record Decisions to withhold/ withdraw treatments are variably documented and largely subtle that are difficult or impossible to capture in chart review One would have to agree on which patients needed these interventions before one could agree that they had been withheld Few guidelines/ practices for terminal weaning of ventilator

4 Introduction The ICU may not be an ideal place to die: Patients are isolated from their families Neurologically depressed to make communication NOT feasible Uncertainty about medical directives Problem associated with assessment of pain and other symptom control Care by different specialty teams

5 Introduction What are the barriers to end-of-life care in ICU? What are the attitudes of health care staff? What is quality end-of-life care in ICU? How to measure success of intervention? Any role of palliative care services in ICU?

6 What are the barriers to end-of-life care in ICU?
7 Barriers to End-of-life care in ICU 1. Difficulty in identifying who should receive EOL care in ICU Patients with a predicted length of stay longer than 5 days, predicted mortality > 25% as estimated by the attending physician, or change in functional status that was potentially irreversible 2. Prognostic uncertainty Gordon D. Rubenfeld, J. Randall Curtis. Improving care for patients dying in the intensive care unit. Clinical Chest Medicine 2003; 24: Judith E. Nelson. Identifying and overcoming the barriers to high-quality palliative care in the intensive care unit. Critical Care Medicine 2006; 34: S324-S331.
8 Barriers to End-of-life care in ICU 3. < 5% patients are communicable for decision-making? patients preferences for resuscitation (know only moderately better than chance) In one study, 78% of patients stated that if their previous preferences differed from a decision made by their family and physician 4. Poor decision making arises from conflict and inadequate information between physician-staff-family triad J. Randall Curtis, Sarah E. Shannon. Transcending the silos: toward an interdisciplinary approach to end-of-life care in the ICU. Intensive Care Medicine 2006; 32:15 17.
9 Barriers to End-of-life care in ICU Mean duration of a family meeting was 10 mins The families reported not understanding the diagnosis, prognosis or care plan ~ 54% Clinicians spoke most of the time ~ 71% No association between the duration of the conference and family satisfaction Mitchell M. Levy, Deborah L. McBride. End-of-life care in the intensive care unit: State of the art in Critical Care Medicine 2006; 34: S306-S308.
10 Barriers to End-of-life care in ICU Semi-structured interviews on a sample of 21 nurses from two community hospitals: Nurses stated that it was important for the physician to give the patient and family member a clear, accurate and realistic prognosis Nurses also thought that physicians were much more optimistic than the nurses, or presented things to the family with more optimism Kathleen A. Puntillo, Jennifer L. McAdam. Communication between physicians and nurses as a target for improving end-of-life care in the intensive care unit: Challenges and opportunities for moving forward. Critical Care Medicine 2006; 34(11): S332-S340
11 Barriers to End-of-life care in ICU 5. Insufficient training of ICU physicians in palliative medicine 6. Inflated expectations for critical care therapies (which are shared by many clinicians, patients and families) Death-denying society Lack of education or knowledge about critical care Judith E. Nelson. Identifying and overcoming the barriers to high-quality palliative care in the intensive care unit. Critical Care Medicine 2006; 34: S324-S331.

12 Barriers to End-of-life care in ICU A survey involving nationally representative sample of nursing and physician directors in 600 adult ICUs in the United States Judith E. Nelson, Derek C. Angus, Lisa A. Weissfeld. End-of-life care for the critically ill: A national intensive care unit survey. Critical Care Medicine 2006; 34:
13 Barriers to End-of-life care in ICU 7. Distrust of the healthcare system Fear that palliative care will provide lower quality care 8. Inadequate financing and insurance coverage for palliative care 9. Lack of diversity in hospice and palliative care teams to the cultural values of diverse communities

14 What are the attitudes of health care staff?
15 With regard to the practice of withholding and withdrawing treatment Studies reported wide variations in individual ICUs and groups of ICUs in Spain, Europe, and the United States Withdrawal of all active treatment was widespread in ICUs in the United Kingdom. However, there was considerable variation by unit, even after accounting for patient factors and differences in size and type of ICU Hannah Wunsch, David A. Harrison, Sheila Harvey, et al. End-of-life decisions: a cohort study of the withdrawal of all active treatment in intensive care units in the United Kingdom. Intensive Care Medicine 2005; 31: Charles L. Sprung, Simon L. Cohen, Peter Sjokvist, et al. End-of-Life Practices in European Intensive Care Unit. JAMA 2003; 290(6):
16 Factors independently associated with the decision to withdraw active treatment Older age Pre-existing severe medical conditions Emergency surgery or medical admission Cardiopulmonary resuscitation in the 24 h prior to admission Ventilation or sedation/paralysis in the first 24 h after admission
17 Withholding or placing an upper limit on treatment and partial withdrawal of treatment are common practice in ICUs Hannah Wunsch, David A. Harrison, Sheila Harvey, et al. End-of-life decisions: a cohort study of the withdrawal of all active treatment in intensive care units in the United Kingdom. Intensive Care Medicine 2005; 31:

18 The withholding and withdrawal of therapy from patients with no chance of recovery to a meaningful life is common in Hong Kong (99% and 89%, respectively) When the family wanted aggressive life-support despite recommendations to limit therapy, 62% of the respondents would still withhold therapy while only 9% would withdraw therapy

19 What is quality end-of-life care in ICU?
20 Defining the Scope of Palliative and End-of-Life Care No consensus definition of the end of life exists in the literature to guide investigation of quality (In ICU setting, the formulation of a definition for the end-of-life period will depend on the aspect of quality end-of-life care grounded in discussions of goals of care, to attempt to maintain a patient family perspective) Richard A. Mularski. Defining and measuring quality palliative and end-of-life care in the intensive care unit. Critical Care Medicine 2006; 34: S309-S316
21 Defining the Scope of Palliative and End-of-Life Care Four schemas have been applied in specifying the end-of-life period: 1) Active dying 2) Acceptance of treatment limitations 3) Severity of illness 4) Poor prognosis Study to Understand Prognoses and Preferences for Outcomes and Risks of Treatments showed that, even very near to death, much uncertainty exists in prognostication; median prognoses within the last week of life were often 50% to survive 6 months Richard A. Mularski. Defining and measuring quality palliative and end-of-life care in the intensive care unit. Critical Care Medicine 2006; 34: S309-S316.
22 Defining the Scope of Palliative and End-of-Life Care WHO defines palliative care as an approach that improves the quality of life... of patients and their families... [for] problems associated with life-threatening illness... through the prevention and relief of suffering by...early identification,... assessment, and...treatment of pain and other problems, physical, psychosocial and spiritual
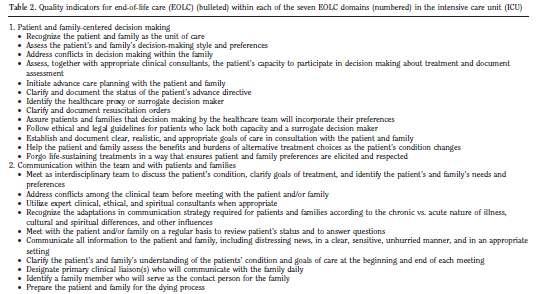
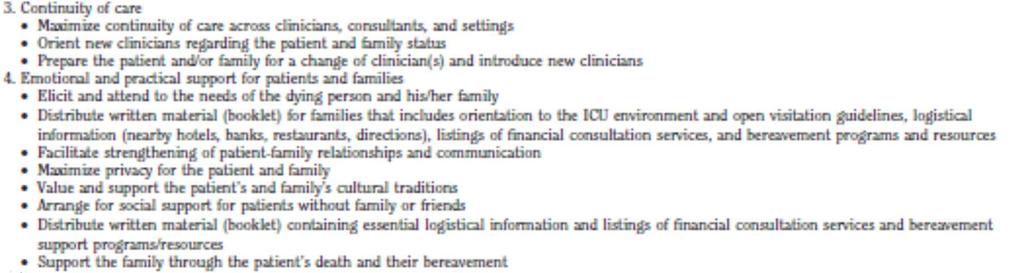
23 Measures of the quality of end-of-life care in the ICU Robert Wood Johnson Foundation (RWJF) Critical Care End-of-life Peer Workgroup In-depth literature review and consensus process to identify the key EOL care and related quality indicator, a number of quality-of-care domains were proposed: 1) Patient- and family-centered decision making 2) Communication with patients and family 3) Continuity of care 4) Emotional and practical support for patients and family members 5) Symptom management and comfort care 6) Spiritual support 7) Emotional and organizational support for ICU clinicians Ellen B. Clarke, J. Randall Curtis, John M. Luce, et al. Quality indicators for end-of-life care in the intensive care unit. Critical Care Medicine 2003; 31:
24


25 The Workgroup proposed 53 quality indicators within those domains and identified 100 examples of clinician and organizational behaviors that could address the end-of-life care quality indicators in the intensive care unit setting
26 Interventions to improve quality of End-of-life care in the ICU Value end-of-life care and routinely include it on rounds and in notes Schedule formal family conferences with specific talking points early in ICU course Use protocols for withholding and withdrawing life-sustaining treatments Provide nurses with documentation standards for withholding and withdrawing life-sustaining treatments Communicate decisions clearly about which treatments should be withheld Address exaggerated concerns over legal and ethical barriers to providing care to dying patients Convene multi-disciplinary rounds to review deaths that cover the medical and emotional aspects of caring for dying patients Liberalize family visiting hours Provide educational pamphlets for families of critically ill patients

27 How to measure success of intervention?
28 Measure success of intervention A number of outcome measures used to evaluate endof-life care in the ICU 1) ICU length of stay and intensity of care 2) Patients symptoms 3) Family members symptoms associated with end-of-life care for the patient 4) Families and clinicians ratings of the quality of satisfaction with care J. Randall Curtis, Ruth A. Engelberg. Measuring success of interventions to improve the quality of end-of-life care in the intensive care unit. Critical Care Medicine 2006; 34: S341-S347
29 Measure success of intervention 1. ICU length of stay and intensity of care Examining the length of stay for patients who die either with or without an intervention This outcome assumes that prolongation of dying is a marker of poor-quality care 2. Surrogates assessments substituted for patients assessments may not accurately reflect the patient s experience Some scales employed: NRS/ Short form of the McGill Pain Questionnaire/ Edmonton Symptom Assessment Scale J. Randall Curtis, Ruth A. Engelberg. Measuring success of interventions to improve the quality of end-of-life care in the intensive care unit. Critical Care Medicine 2006; 34: S341-S347
30 Measure success of intervention 3. Family members symptoms associated with end-oflife care for the patient High levels of anxiety and depression among family members associated with aspects of ICU care Azoulay et al. in France and found that 33% of family members had significant symptoms of PTSD at 3 months No studies of complicated grief among J. Randall Curtis, Ruth A. Engelberg. Measuring success of interventions to improve the quality of end-of-life care in the intensive care unit. Critical Care Medicine 2006; 34: S341-S347 Élie Azoulay, Charles L. Sprung. Family-physician interactions in the intensive care unit. Critical Care Medicine 2004; 32(11):
31 Measure success of intervention 4. Families and clinicians ratings of the quality of satisfaction with care Few instruments have been adapted or have been evaluated for psychometric performance in ICU 90% of dying ICU patients have altered cognition, most evaluations will need to involve proxy reports and validity challenges Examples consist of multiple domains: Palliative Care Outcome Scale Quality of Dying and Death Quality of End-of-Life Care and Satisfaction with Treatment Quality of Life at End of Life Family Satisfaction in the Intensive Care Unit Toolkit After-Death Bereaved Family Member Interview Richard A. Mularski. Defining and measuring quality palliative and end-of-life care in the intensive care unit. Critical Care Medicine 2006; 34: S309-S316.
32 Measure success of intervention 4. Families and clinicians ratings of the quality of satisfaction with care Measures of the quality of end-of-life care in the ICU Family Satisfaction in the ICU questionnaire (developed and validated by Heyland et al. 24 items using Likert scales, 14 describe family satisfaction with care and ten describe family satisfaction with decision making) Quality of Patients Dying Experiences (QODD) questionnaire Levy et al. reported that nurses and resident physicians gave more negative ratings than family members Hodde et al. ICU nurse-assessed QODD demonstrated significantly higher quality of dying among patients who did not receive cardiopulmonary resuscitation in the last 8 hrs of life and for patients who had someone present at the time of their death Responsiveness to interventions is not yet known Measuring success of interventions to improve the quality of end-of-life care in the intensive care unit. J. Randall Curtis, Ruth A. Engelberg. Et al Critical Care Medicine 2006; 34: S341-S347

33 Any role of palliative care services in ICU?


34 Integration of palliative care team into an intensive care unit
35 Convenience sample of 157 consecutive patients served by a palliative care team which from August 2005 until August 2007 Interviews were conducted with a sample of family members Education on the death process in 85% of families Following consultation with the Palliative Care Service, patients were: Disconnected from mechanical ventilators 29% Discontinued inotropic support % Stopped artificial nutrition % Stopped dialysis 6.4% Discontinued artificial hydration - 2.5% Increase in the rate of the formalization of advance directives 83.4% of patients had do not resuscitate orders after the intervention Sean O Mahony, Janet McHenry, Arthur E Blank, et al. Preliminary report of the integration of a palliative care team into an intensive care unit. Palliative Medicine 2010; 24:
36 A separate case control study in 22 persons who died with and 43 who died without a palliative care consultation at the intervention campus ICU Sean O Mahony, Janet McHenry, Arthur E Blank, et al. Preliminary report of the integration of a palliative care team into an intensive care unit. Palliative Medicine 2010
37 Median survival times from admission were not significantly different when stratified by palliative care consultation status: 12 days for the control group (95% CI 8 18) and 13.5 days for the intervention group (95% CI 8 20)
38 Median charges for the use of opioid medications were higher (p=0.01) for the intervention group but lower for use of laboratory (p=0.004) and radiology tests (p=0.027) Integration of palliative care experts into the operation of critical care units is of benefit to patients, families and critical care clinicians Preliminary report of the integration of a palliative care team into an intensive care unit. Sean O Mahony et al. Palliative Medicine 2010
39 Any role of palliative care services in ICU? ICU-focused palliative care consultation service at Detroit Receiving Hospital (USA) since 1986 Comparison of patient with global cerebral ischemia after cardiac arrest or multiple organ system failure and a matched historical control group Identification of advance directive or preferences, if any; communication of prognosis and treatment options with patients or their surrogates; and implementation of palliative care strategies Decreased use of non-beneficial interventions, lag time between identification of poor prognosis and palliative care, reductions in hospital length of stay and hospital charges, with no difference in patient mortality Margaret L. Campbell. Palliative care consultation in the intensive care unit Critical Care Med 2006

40 Merging cultures: Palliative care specialists in the medical intensive care unit J. Andrew Billings et al. Critical Care Medicine 2006
41
42 Truog et al. Critical Care Medicine 2008
43 Conclusion Palliative and end-of-life care in the ICU is an appropriate and underdeveloped area With regard to the practice of withholding and withdrawing treatment, variations in individual ICUs Preliminary evidence suggest that integration of palliative care into the operation of critical care units may be associated with Improved quality Higher rates of formalization of advance directives and utilization of hospice Lower use of certain non-beneficial life-prolonging treatments
44 Conclusion There is increasing consensus within the field of critical care on shared decision making and the importance of caring for patients families Communication is consistently identified as the most important and least accomplished factor in quality of care
45 Conclusion Increasing interest in identifying and testing patient- and family-centered outcomes of end-of-life care in the ICU Further research is needed to develop a valid and responsive measures of the effectiveness of interventions designed to improve end-of-life care in the ICU
46 Reference J. Randall Curtis, Ruth A. Engelberg. Measuring success of interventions to improve the quality of end-of-life care in the intensive care unit. Critical Care Medicine 2006; 34: S341-S347. Sean O Mahony, Janet McHenry, Arthur E Blank, et al. Preliminary report of the integration of a palliative care team into an intensive care unit. Palliative Medicine 2010; 24: Robert Sibbald, James Downar, Laura Hawryluck. Perceptions of futile care among caregivers in intensive care unit. Canadian Medical Association Journal 2007; 10: Robert D. Truog, Margaret L. Campbell, J. Randall Curtis, et al. Recommendations for end-of-life care in the intensive care unit: A consensus statement by the American College of Critical Care Medicine. Critical Care Medicine. Critical Care Medicine 2008; 36: Mitchell M. Levy, Deborah L. McBride. End-of-life care in the intensive care unit: State of the art in Critical Care Medicine 2006; 34: S306-S308. Gordon D Rubenfeld, J Randall Curtis. Beyond ethical dilemmas: improving the quality of end-of-life care in the intensive care unit. Critical Care 2003; 7:
47 Reference Mitchell M. Levy. End-of-life care in the intensive care unit: Can we do better? Critical Care Medicine 2001; 29: N51-N61. Cari R. Levy, E. Wesley Ely, Kate Payne, et al. Quality of Dying and Death in Two Medical ICUs - Perceptions of Family and Clinicians. Chest 2005; 5: Gordon D. Rubenfeld, J. Randall Curtis. Improving care for patients dying in the intensive care unit. Clinical Chest Medicine 2003; 24: Judith E. Nelson. Identifying and overcoming the barriers to high-quality palliative care in the intensive care unit. Critical Care Medicine 2006; 34: S324-S331. Ellen B. Clarke, J. Randall Curtis, John M. Luce, et al. Quality indicators for end-of-life care in the intensive care unit. Critical Care Medicine 2003; 31: Richard A. Mularski. Defining and measuring quality palliative and end-of-life care in the intensive care unit. Critical Care Medicine 2006; 34: S309-S316. Élie Azoulay, Charles L. Sprung. Family-physician interactions in the intensive care unit. Critical Care Medicine 2004; 32(11): J. Randall Curtis, Sarah E. Shannon. Transcending the silos: toward an interdisciplinary approach to end-of-life care in the ICU. Intensive Care Medicine 2006; 32: Kwok M. Ho, Sonya English, Jeanette Bell. The involvement of intensive care nurse in end-of-life decisions: a nationwide survey. Intensive Care Medicine 2005; 31:

48 The End Thank you
Palliative Care: A Place on the Quality Scorecard?
 Palliative Care: A Place on the Quality Scorecard? J. Randall Curtis, MD, MPH Professor of Medicine Director, Palliative Care Center of Excellence www.uwpalliativecarecenter.com Disclosures and Funding
Palliative Care: A Place on the Quality Scorecard? J. Randall Curtis, MD, MPH Professor of Medicine Director, Palliative Care Center of Excellence www.uwpalliativecarecenter.com Disclosures and Funding
Élie AZOULAY Hôpital Saint-Louis, Service de Réanimation Médicale Université Paris-Diderot, Sorbonne Paris-Cité
 Élie AZOULAY Hôpital Saint-Louis, Service de Réanimation Médicale Université Paris-Diderot, Sorbonne Paris-Cité Groupe de Recherche Respiratoire en Réanimation Onco-Hématologique (GRRR-OH) Thank you for
Élie AZOULAY Hôpital Saint-Louis, Service de Réanimation Médicale Université Paris-Diderot, Sorbonne Paris-Cité Groupe de Recherche Respiratoire en Réanimation Onco-Hématologique (GRRR-OH) Thank you for
A Practical Approach to Palliative Care in the ICU
 A Practical Approach to Palliative Care in the ICU Wendy Anderson, MD MS Critical Care Medicine and Trauma May 31, 2013 Disclosure Statement Dr. Anderson has no relevant financial relationships to disclose.
A Practical Approach to Palliative Care in the ICU Wendy Anderson, MD MS Critical Care Medicine and Trauma May 31, 2013 Disclosure Statement Dr. Anderson has no relevant financial relationships to disclose.
Gestione degli ICD/CRT a fine vita dei pazienti. Prof. Luigi Padeletti Università degli Studi di Firenze
 Gestione degli ICD/CRT a fine vita dei pazienti Prof. Luigi Padeletti Università degli Studi di Firenze What would you do if you knew you had 6 months to live? How would you choose to spend your time?
Gestione degli ICD/CRT a fine vita dei pazienti Prof. Luigi Padeletti Università degli Studi di Firenze What would you do if you knew you had 6 months to live? How would you choose to spend your time?
When to think about palliation
 When to think about palliation Hannah Wunsch, MD MSc Department of Critical Care Medicine, Sunnybrook Health Sciences Centre Associate Professor of Anesthesiology, University of Toronto Visiting Assistant
When to think about palliation Hannah Wunsch, MD MSc Department of Critical Care Medicine, Sunnybrook Health Sciences Centre Associate Professor of Anesthesiology, University of Toronto Visiting Assistant
Communication with relatives of critically ill patients. Dr WAN Wing Lun Specialist in Critical Care Medicine Yan Chai Hospital
 Communication with relatives of critically ill patients Dr WAN Wing Lun Specialist in Critical Care Medicine Yan Chai Hospital Why is communication with relatives important? Relatives of ICU patients suffer
Communication with relatives of critically ill patients Dr WAN Wing Lun Specialist in Critical Care Medicine Yan Chai Hospital Why is communication with relatives important? Relatives of ICU patients suffer
Quality of Life (F309 End of Life) Interpretive Guidance Investigative Protocol
 Interpretive Guidance Investigative Protocol") 483.25 Quality of Life (F309 End of Life) Interpretive Guidance Investigative Protocol 2 483.25 End of Life Each resident must receive and the facility must provide the necessary care and services to attain
483.25 Quality of Life (F309 End of Life) Interpretive Guidance Investigative Protocol 2 483.25 End of Life Each resident must receive and the facility must provide the necessary care and services to attain
Protocol euroq2; European Quality Questionnaire. Families experiences of ICU quality of care. Development and validation of a European questionnaire
 Protocol euroq2; European Quality Questionnaire Hanne Irene Jensen Rik Gerritsen Matty Koopmans Families experiences of ICU quality of care. Development and validation of a European questionnaire Background
Protocol euroq2; European Quality Questionnaire Hanne Irene Jensen Rik Gerritsen Matty Koopmans Families experiences of ICU quality of care. Development and validation of a European questionnaire Background
Pediatric Palliative Care
 Pediatric Palliative Care { Andrew K. Gormley, M.D. Director, Cardiac Intensive Care Assistant Medical Director, PICU Critical Care Medicine Department of Pediatrics The Children's Hospital at OU Medical
Pediatric Palliative Care { Andrew K. Gormley, M.D. Director, Cardiac Intensive Care Assistant Medical Director, PICU Critical Care Medicine Department of Pediatrics The Children's Hospital at OU Medical
Quality and Fiscal Metrics: What Proves Success?
 Quality and Fiscal Metrics: What Proves Success? 1 Quality and Fiscal Metrics: What Proves Success? Kathleen Kerr Kerr Healthcare Analytics Creating the Future of Palliative Care NHPCO Virtual Event February
Quality and Fiscal Metrics: What Proves Success? 1 Quality and Fiscal Metrics: What Proves Success? Kathleen Kerr Kerr Healthcare Analytics Creating the Future of Palliative Care NHPCO Virtual Event February
Palliative Care In PICU
 Palliative Care In PICU Professor Lucy Lum University Malaya Annual Scientific Meeting on Intensive Care 15 August 2015 2 Defining Palliative Care: Mistaken perception: For patients whom curative care
Palliative Care In PICU Professor Lucy Lum University Malaya Annual Scientific Meeting on Intensive Care 15 August 2015 2 Defining Palliative Care: Mistaken perception: For patients whom curative care
At the. End of Life. difficult conversations about. organ donation
 At the End of Life difficult conversations about organ donation Hope is the power of being cheerful in circumstances we know to be desperate. Hope is an attachment to something I believe that I do not
At the End of Life difficult conversations about organ donation Hope is the power of being cheerful in circumstances we know to be desperate. Hope is an attachment to something I believe that I do not
Physician Attitudes Towards Death and Pain and Their Effects on Care Keith LeBlanc, Jr.
 Physician Attitudes Towards Death and Pain and Their Effects on Care Keith LeBlanc, Jr. Palliative care is a medical specialty derived from the hospice movement which began in 1967, and was realized as
Physician Attitudes Towards Death and Pain and Their Effects on Care Keith LeBlanc, Jr. Palliative care is a medical specialty derived from the hospice movement which began in 1967, and was realized as
RE: Draft CMS Quality Measure Development Plan: Supporting the Transition to the Merit-based Incentive Payment System and Alternative Payment Models
 March 1, 2016 Centers for Medicare & Medicaid Services Department of Health and Human Services P.O. Box 8016 Baltimore, MD 21244 Submitted electronically via MACRA-MDP@hsag.com. RE: Draft CMS Quality Measure
March 1, 2016 Centers for Medicare & Medicaid Services Department of Health and Human Services P.O. Box 8016 Baltimore, MD 21244 Submitted electronically via MACRA-MDP@hsag.com. RE: Draft CMS Quality Measure
END OF LIFE ISSUES. 41 st Semi-Annual Family Practice Review Course Lewis Katz School of Medicine at Temple University
 END OF LIFE ISSUES 41 st Semi-Annual Family Practice Review Course Lewis Katz School of Medicine at Temple University Stanley J. Savinese DO FAAHPM HMDC Medical Director VNA Hospice of Philadelphia Co-Director
END OF LIFE ISSUES 41 st Semi-Annual Family Practice Review Course Lewis Katz School of Medicine at Temple University Stanley J. Savinese DO FAAHPM HMDC Medical Director VNA Hospice of Philadelphia Co-Director
BETTER CONVERSATIONS, BETTER CARE : HOW MEANINGFUL CONVERSATIONS IMPROVE PATIENT EXPERIENCE AND QUALITY OF LIFE
 Teva Pharmaceuticals Europe BV, Piet Heinkade 107, 1019 GM Amsterdam, Netherlands Date of preparation: March 2017. HQ/ONCO/17/0001 BETTER CONVERSATIONS, BETTER CARE : HOW MEANINGFUL CONVERSATIONS IMPROVE
Teva Pharmaceuticals Europe BV, Piet Heinkade 107, 1019 GM Amsterdam, Netherlands Date of preparation: March 2017. HQ/ONCO/17/0001 BETTER CONVERSATIONS, BETTER CARE : HOW MEANINGFUL CONVERSATIONS IMPROVE
Early Involvement of Palliative Care. Jessica Heestand, PGY2 5/14/2014
 Early Involvement of Palliative Care Jessica Heestand, PGY2 5/14/2014 Why is this important? Palliative care is frequently misconstrued as synonymous with end-of-life care Palliative care is important
Early Involvement of Palliative Care Jessica Heestand, PGY2 5/14/2014 Why is this important? Palliative care is frequently misconstrued as synonymous with end-of-life care Palliative care is important
The Influence of Race and Ethnicity on End-of-Life Care in the Intensive Care Unit
 The Influence of Race and Ethnicity on End-of-Life Care in the Intensive Care Unit Sarah Muni, MD Department of Medicine Chair s Rounds November 10, 2009 Health Disparities Research Clinical appropriateness
The Influence of Race and Ethnicity on End-of-Life Care in the Intensive Care Unit Sarah Muni, MD Department of Medicine Chair s Rounds November 10, 2009 Health Disparities Research Clinical appropriateness
Palliative Medicine Boot Camp: Ethical Issues
 Palliative Medicine Boot Camp: Ethical Issues Rev. Thomas F. Bracken, Jr. D Min - Community LIFE, Pittsburgh, PA David Wensel, DO - Midland Care PACE, Topeka, KS Learning Objectives Address ethical questions
Palliative Medicine Boot Camp: Ethical Issues Rev. Thomas F. Bracken, Jr. D Min - Community LIFE, Pittsburgh, PA David Wensel, DO - Midland Care PACE, Topeka, KS Learning Objectives Address ethical questions
NeuroPI Case Study: Palliative Care Counseling and Advance Care Planning
 Case: An 86 year-old man presents to your office after recently being diagnosed as having mild dementia due to Alzheimer s disease, accompanied by his son who now runs the family business. At baseline
Case: An 86 year-old man presents to your office after recently being diagnosed as having mild dementia due to Alzheimer s disease, accompanied by his son who now runs the family business. At baseline
PALLIATIVE CARE IN NEW YORK STATE
 Collaborative for Palliative Care In collaboration with its partners End of Life Choices New York Finger Lakes Geriatric Education Center at the University of Rochester COLLABORATIVE FOR PALLIATIVE CARE
Collaborative for Palliative Care In collaboration with its partners End of Life Choices New York Finger Lakes Geriatric Education Center at the University of Rochester COLLABORATIVE FOR PALLIATIVE CARE
BACK TO THE FUTURE: Palliative Care in the 21 st Century
 BACK TO THE FUTURE: Palliative Care in the 21 st Century Section 3: Hospice 101 I m not afraid of death; I just don t want to be there when it happens. -Woody Allen A Century of Change 1900 2000 Age at
BACK TO THE FUTURE: Palliative Care in the 21 st Century Section 3: Hospice 101 I m not afraid of death; I just don t want to be there when it happens. -Woody Allen A Century of Change 1900 2000 Age at
Module 1: Principles of Palliative Care. Part I: Dying Well. A Good Death Defined
 E L N E C End-of-Life Nursing Education Consortium Geriatric Curriculum Module 1: Principles of Palliative Care Part I: Dying Well A natural part of life Opportunity for growth Profoundly personal experience
E L N E C End-of-Life Nursing Education Consortium Geriatric Curriculum Module 1: Principles of Palliative Care Part I: Dying Well A natural part of life Opportunity for growth Profoundly personal experience
END-OF-LIFE DECISIONS HONORING THE WISHES OF A PERSON WITH ALZHEIMER S DISEASE
 END-OF-LIFE DECISIONS HONORING THE WISHES OF A PERSON WITH ALZHEIMER S DISEASE PREPARING FOR THE END OF LIFE When a person with late-stage Alzheimer s a degenerative brain disease nears the end of life
END-OF-LIFE DECISIONS HONORING THE WISHES OF A PERSON WITH ALZHEIMER S DISEASE PREPARING FOR THE END OF LIFE When a person with late-stage Alzheimer s a degenerative brain disease nears the end of life
End of Life Care in IJN Our journey. Dato Dr. David Chew Soon Ping Consultant Cardiologist National Heart Institute Malaysia
 End of Life Care in IJN Our journey Dato Dr. David Chew Soon Ping Consultant Cardiologist National Heart Institute Malaysia End of Life Dying is final part of everyone journey in life Deaths used to occur
End of Life Care in IJN Our journey Dato Dr. David Chew Soon Ping Consultant Cardiologist National Heart Institute Malaysia End of Life Dying is final part of everyone journey in life Deaths used to occur
There Is Something More We Can Do: An Introduction to Hospice and Palliative Care
 There Is Something More We Can Do: An Introduction to Hospice and Palliative Care presented to the Washington Patient Safety Coalition July 28, 2010 Hope Wechkin, MD Medical Director Evergreen Hospice
There Is Something More We Can Do: An Introduction to Hospice and Palliative Care presented to the Washington Patient Safety Coalition July 28, 2010 Hope Wechkin, MD Medical Director Evergreen Hospice
The quality of dying and death: a systematic review of measures
 Review The quality of dying and death: a systematic review of s Palliative Medicine 24(2) 127 144! The Author(s) 2010 Reprints and permissions: sagepub.co.uk/journalspermissions.nav DOI: 10.1177/0269216309351783
Review The quality of dying and death: a systematic review of s Palliative Medicine 24(2) 127 144! The Author(s) 2010 Reprints and permissions: sagepub.co.uk/journalspermissions.nav DOI: 10.1177/0269216309351783
Advances in Palliative Care
 Steven Pantilat, MD Professor of Clinical Medicine Alan M. Kates and John M. Burnard Endowed Chair in Palliative Care Director, Palliative Care Program and Palliative Care Leadership Center Division of
Steven Pantilat, MD Professor of Clinical Medicine Alan M. Kates and John M. Burnard Endowed Chair in Palliative Care Director, Palliative Care Program and Palliative Care Leadership Center Division of
Quality of Life (F309 End of Life) Surveyor Train the Trainer: Interpretive Guidance Investigative Protocol
 Surveyor Train the Trainer: Interpretive Guidance Investigative Protocol") 483.25 Quality of Life (F309 End of Life) Surveyor Train the Trainer: Interpretive Guidance Investigative Protocol 2 483.25 End of Life Each resident must receive and the facility must provide the necessary
483.25 Quality of Life (F309 End of Life) Surveyor Train the Trainer: Interpretive Guidance Investigative Protocol 2 483.25 End of Life Each resident must receive and the facility must provide the necessary
Essential Palliative Care Skills For Every Clinician
 Essential Palliative Care Skills For Every Clinician Tools for Assessment and Management of Serious Illness for Primary Care Providers Comprehensive Curriculum Self-Paced Fully Online 03012018 Online,
Essential Palliative Care Skills For Every Clinician Tools for Assessment and Management of Serious Illness for Primary Care Providers Comprehensive Curriculum Self-Paced Fully Online 03012018 Online,
Palliative Care in the Community
 Palliative Care in the Community Carol Babcock, MFT Director Palliative Care, Navicent Health American College of Surgeons Commission on Cancer (CoC) Standard 2.4 Palliative care services are available
Palliative Care in the Community Carol Babcock, MFT Director Palliative Care, Navicent Health American College of Surgeons Commission on Cancer (CoC) Standard 2.4 Palliative care services are available
Accurate prognostic awareness facilitates, whereas better quality of life and more anxiety symptoms hinder end-of-life discussions
 Accurate prognostic awareness facilitates, whereas better quality of life and more anxiety symptoms hinder end-of-life discussions Siew Tzuh Tang, DNSc Chang Gung University, School of Nursing Importance
Accurate prognostic awareness facilitates, whereas better quality of life and more anxiety symptoms hinder end-of-life discussions Siew Tzuh Tang, DNSc Chang Gung University, School of Nursing Importance
Transformative Social Work Practice, Schott & Weiss. Test Bank
 Test Bank Chapter 2: Palliative and Hospice Care Settings (Dawn Joosten) Multiple Choice 1. Based on their definition and function, what are the two similar factors associated with both palliative and
Test Bank Chapter 2: Palliative and Hospice Care Settings (Dawn Joosten) Multiple Choice 1. Based on their definition and function, what are the two similar factors associated with both palliative and
Road Blocks in Non-Cancer Palliative Care Obstacles observed from outpatient non-cancer palliative practice.
 Road Blocks in Non-Cancer Palliative Care Obstacles observed from outpatient non-cancer palliative practice. 25th Annual Palliative Education and Research Days, West Edmonton Mall. Edmonton. 2014 Amanda
Road Blocks in Non-Cancer Palliative Care Obstacles observed from outpatient non-cancer palliative practice. 25th Annual Palliative Education and Research Days, West Edmonton Mall. Edmonton. 2014 Amanda
Family Member Satisfaction With End-of-Life Decision Making in the ICU*
 Original Research CRITICAL CARE MEDICINE Family Member Satisfaction With End-of-Life Decision Making in the ICU* Cynthia J. Gries, MD, MSc; J. Randall Curtis, MD, MPH, FCCP; Richard J. Wall, MD, MPH; and
Original Research CRITICAL CARE MEDICINE Family Member Satisfaction With End-of-Life Decision Making in the ICU* Cynthia J. Gries, MD, MSc; J. Randall Curtis, MD, MPH, FCCP; Richard J. Wall, MD, MPH; and
Chapter 6. Hospice: A Team Approach to Care
 Chapter 6 Hospice: A Team Approach to Care Chapter 6: Hospice: A Team Approach to Care Comfort, Respect and Dignity in Dying Hospice care provides patients and family members with hope, comfort, respect,
Chapter 6 Hospice: A Team Approach to Care Chapter 6: Hospice: A Team Approach to Care Comfort, Respect and Dignity in Dying Hospice care provides patients and family members with hope, comfort, respect,
IMPLEMENTING STANDARDS FOR QUALITY PALLIATIVE CARE. Monica Malec, MD University of Chicago
 IMPLEMENTING STANDARDS FOR QUALITY PALLIATIVE CARE Monica Malec, MD University of Chicago Nothing to disclose OBJECTIVES Utilize the eight domains of palliative care as the structure for palliative care
IMPLEMENTING STANDARDS FOR QUALITY PALLIATIVE CARE Monica Malec, MD University of Chicago Nothing to disclose OBJECTIVES Utilize the eight domains of palliative care as the structure for palliative care
The impact of a palliative care unit on mortality rate and length of stay for medical intensive care unit patients
 Palliative and Supportive Care (2011), 9, 387 392. # Cambridge University Press, 2011 1478-9515/11 $20.00 doi:10.1017/s147895151100040x The impact of a palliative care unit on mortality rate and length
Palliative and Supportive Care (2011), 9, 387 392. # Cambridge University Press, 2011 1478-9515/11 $20.00 doi:10.1017/s147895151100040x The impact of a palliative care unit on mortality rate and length
Geriatric Grand Rounds
 Geriatric Grand Rounds Tuesday, April 15, 2008 12:00 noon Dr. Bill Black Auditorium Glenrose Rehabilitation Hospital Visit web sites: for handouts, poster, schedule, subscription: http://www.ualberta.ca/~geriatri/ggr/.
Geriatric Grand Rounds Tuesday, April 15, 2008 12:00 noon Dr. Bill Black Auditorium Glenrose Rehabilitation Hospital Visit web sites: for handouts, poster, schedule, subscription: http://www.ualberta.ca/~geriatri/ggr/.
Dementia & Palliative Care
 Dementia & Palliative Care Aspiration, Myth or Reality? A Clinicians Perspective... Lesley Jones Advanced Practitioner Dementia Care Dementia Dementia is a chronic progressive mental disorder that adversely
Dementia & Palliative Care Aspiration, Myth or Reality? A Clinicians Perspective... Lesley Jones Advanced Practitioner Dementia Care Dementia Dementia is a chronic progressive mental disorder that adversely
How Many Times? Result: an Unsatisfactory Outcome That Can Be Avoided
 Removing Obstacles to a Peaceful Death by Revising Health Professional Training and Payment Systems Professor Kathy L. Cerminara Nova Southeastern University Shepard Broad College of Law October 24, 2018
Removing Obstacles to a Peaceful Death by Revising Health Professional Training and Payment Systems Professor Kathy L. Cerminara Nova Southeastern University Shepard Broad College of Law October 24, 2018
Primary Palliative Care Skills
 Primary Palliative Care Skills Tools for Assessment and Management of Serious Illness for Primary Care Providers Comprehensive Curriculum Self-Paced Fully Online 03012018 Online, On-Demand Education for
Primary Palliative Care Skills Tools for Assessment and Management of Serious Illness for Primary Care Providers Comprehensive Curriculum Self-Paced Fully Online 03012018 Online, On-Demand Education for
What You Need To Know About Palliative Care. Natalie Wu Moy, LCSW, MSPA RUHS Medical Center Hospital Social Services Director
 What You Need To Know About Palliative Care Natalie Wu Moy, LCSW, MSPA RUHS Medical Center Hospital Social Services Director None of the faculty, planners, speakers, providers, nor CME committee members
What You Need To Know About Palliative Care Natalie Wu Moy, LCSW, MSPA RUHS Medical Center Hospital Social Services Director None of the faculty, planners, speakers, providers, nor CME committee members
Feasibility of Implementing Advance Directive in Hong Kong Chinese Elderly People
 Asia Pacific Regional Conference in End-of-Life and Palliative Care in Long Term Care Settings Feasibility of Implementing Advance Directive in Hong Kong Chinese Elderly People Dr. Patrick CHIU MBBS (HK),
Asia Pacific Regional Conference in End-of-Life and Palliative Care in Long Term Care Settings Feasibility of Implementing Advance Directive in Hong Kong Chinese Elderly People Dr. Patrick CHIU MBBS (HK),
12/6/2016. Objective PALLIATIVE CARE IN THE NURSING HOME. Medical Care in the US. Palliative Care
 Objective PALLIATIVE CARE IN THE NURSING HOME Deborah Morris, M.D., M.H.S. Assistant Professor of Medicine The Glennan Center for Geriatrics and Gerontology Eastern Virginia Medical School Describe program
Objective PALLIATIVE CARE IN THE NURSING HOME Deborah Morris, M.D., M.H.S. Assistant Professor of Medicine The Glennan Center for Geriatrics and Gerontology Eastern Virginia Medical School Describe program
The Next Generation of Advance Directives. Carol Wilson, MSHA Director of Palliative Care and Advance Care Planning Riverside Health System
 The Next Generation of Advance Directives Carol Wilson, MSHA Director of Palliative Care and Advance Care Planning Riverside Health System Need for a Better System Only 25% of all adults have Advance Directives
The Next Generation of Advance Directives Carol Wilson, MSHA Director of Palliative Care and Advance Care Planning Riverside Health System Need for a Better System Only 25% of all adults have Advance Directives
The needs for palliative care in HIV/AIDS care setting. Linlin Lindayani
 The needs for palliative care in HIV/AIDS care setting Linlin Lindayani HIV is important indicator in SDGs Target: By 2030, end the epidemics of AIDS HIV: THE FACTS Increase in people receiving ART over
The needs for palliative care in HIV/AIDS care setting Linlin Lindayani HIV is important indicator in SDGs Target: By 2030, end the epidemics of AIDS HIV: THE FACTS Increase in people receiving ART over
Pediatric Palliative Care and Having Difficult Conversations
 Pediatric Palliative Care and Having Difficult Conversations UCSF Pediatric Neurology and Palliative Care Audrey Foster-Barber, MD, PhD Pediatric Hospital Medicine Boot Camp 6/14 Palliative Care A philosophy
Pediatric Palliative Care and Having Difficult Conversations UCSF Pediatric Neurology and Palliative Care Audrey Foster-Barber, MD, PhD Pediatric Hospital Medicine Boot Camp 6/14 Palliative Care A philosophy
Dr. Andrea Johnson Saskatoon Health Region/Saskatoon Cancer Centre September 30, 2016
 Dr. Andrea Johnson Saskatoon Health Region/Saskatoon Cancer Centre September 30, 2016 Conflicts of Interest None... Our drugs are old and cheap (for the most part) so big pharma isn t really interested
Dr. Andrea Johnson Saskatoon Health Region/Saskatoon Cancer Centre September 30, 2016 Conflicts of Interest None... Our drugs are old and cheap (for the most part) so big pharma isn t really interested
Communicating with Patients with Heart Failure and their Families
 Communicating with Patients with Heart Failure and their Families Nathan Goldstein, MD Associate Professor Hertzberg Palliative Care Institute Brookdale Department of Geriatrics and Palliative Medicine
Communicating with Patients with Heart Failure and their Families Nathan Goldstein, MD Associate Professor Hertzberg Palliative Care Institute Brookdale Department of Geriatrics and Palliative Medicine
Palliative Care under a Value Based Reimbursement Model. Janet Bull MD, MBA, FAAHPM CMO Four Seasons
 Palliative Care under a Value Based Reimbursement Model Janet Bull MD, MBA, FAAHPM CMO Four Seasons Objectives o Describe palliative care o Discuss benefits of palliative care o Understand differences
Palliative Care under a Value Based Reimbursement Model Janet Bull MD, MBA, FAAHPM CMO Four Seasons Objectives o Describe palliative care o Discuss benefits of palliative care o Understand differences
Palliative Care Standards & Models
 Palliative Care Standards & Models Ian Anderson Continuing Education Program in End-of of-life Care End-of of-life Care! 222,000 Canadians die each year! 75% die in institutions! 90% want to die at home
Palliative Care Standards & Models Ian Anderson Continuing Education Program in End-of of-life Care End-of of-life Care! 222,000 Canadians die each year! 75% die in institutions! 90% want to die at home
Palliative Care in the ICU
 Palliative Care in the ICU David M. Fedor, DO, FACP, HMDC Intermountain Health Care Physician Intensivist-Critical Care Medicine: MckayDee Hospital; Medical Director - Palliative Care at Mckay Dee Hospital;
Palliative Care in the ICU David M. Fedor, DO, FACP, HMDC Intermountain Health Care Physician Intensivist-Critical Care Medicine: MckayDee Hospital; Medical Director - Palliative Care at Mckay Dee Hospital;
2017 National Association of Social Workers. All Rights Reserved. 1
 2017 National Association of Social Workers. All Rights Reserved. 1 Palliative Care 101 for Social Workers in Aging Karen Bullock, PhD, LCSW June 15, 2017 NASW Virtual Conference Learning Objectives Overview
2017 National Association of Social Workers. All Rights Reserved. 1 Palliative Care 101 for Social Workers in Aging Karen Bullock, PhD, LCSW June 15, 2017 NASW Virtual Conference Learning Objectives Overview
Founded in 1978 as Hospice of the North Shore. Know Your Choices. A Guide for People with Serious Illness
 Founded in 1978 as Hospice of the North Shore Know Your Choices A Guide for People with Serious Illness Advance Care Planning: Expressing Your Wishes In Massachusetts, all patients with serious advancing
Founded in 1978 as Hospice of the North Shore Know Your Choices A Guide for People with Serious Illness Advance Care Planning: Expressing Your Wishes In Massachusetts, all patients with serious advancing
Approximately one in five U.S.
 Using the medical record to evaluate the quality of end-of-life care in the intensive care unit* Bradford J. Glavan, MD; Ruth A. Engelberg, PhD; Lois Downey, MA; J. Randall Curtis, MD, MPH Rationale: We
Using the medical record to evaluate the quality of end-of-life care in the intensive care unit* Bradford J. Glavan, MD; Ruth A. Engelberg, PhD; Lois Downey, MA; J. Randall Curtis, MD, MPH Rationale: We
Palliative Medicine Overview. Francine Arneson, MD Palliative Medicine
 Palliative Medicine Overview Francine Arneson, MD Palliative Medicine Palliative Medicine: Definition Palliative care: An approach that improves the quality of life of patients and their families facing
Palliative Medicine Overview Francine Arneson, MD Palliative Medicine Palliative Medicine: Definition Palliative care: An approach that improves the quality of life of patients and their families facing
2/12/2016. Disclosure. Objectives. The Hospice Medical Director: What Should They Be Doing?
 The Hospice Medical Director: What Should They Be Doing? Tommie W. Farrell, MD HMDCB FAAHPM Pathways at Hendrick Hospital Palliative and Supportive and Hospice Care Abilene Texas Disclosure Governing Board
The Hospice Medical Director: What Should They Be Doing? Tommie W. Farrell, MD HMDCB FAAHPM Pathways at Hendrick Hospital Palliative and Supportive and Hospice Care Abilene Texas Disclosure Governing Board
Donation after Circulatory Determination of Death: Ethical Tensions
 Donation after Circulatory Determination of Death: Ethical Tensions Robert D. Truog, MD Frances Glessner Lee Professor of Medical Ethics, Anaesthesia, & Pediatrics, Harvard Medical School Director, Center
Donation after Circulatory Determination of Death: Ethical Tensions Robert D. Truog, MD Frances Glessner Lee Professor of Medical Ethics, Anaesthesia, & Pediatrics, Harvard Medical School Director, Center
Achieving earlier entry to hospice care: Issues and strategies. Sonia Lee, APN, GCNS-BC
 Achieving earlier entry to hospice care: Issues and strategies Sonia Lee, APN, GCNS-BC Objectives The learner will: Describe the benefits of hospice List at least barriers to early hospice care List at
Achieving earlier entry to hospice care: Issues and strategies Sonia Lee, APN, GCNS-BC Objectives The learner will: Describe the benefits of hospice List at least barriers to early hospice care List at
Palliative Care Consultative Service in Acute Hospital - Impact & Challenges
 Palliative Care Consultative Service in Acute Hospital - Impact & Challenges Dr. Annie Kwok Consultant Palliative Care Unit Department of Medicine & Geriatrics Caritas Medical Centre Contents Aging population
Palliative Care Consultative Service in Acute Hospital - Impact & Challenges Dr. Annie Kwok Consultant Palliative Care Unit Department of Medicine & Geriatrics Caritas Medical Centre Contents Aging population
Palliative Care. Jennifer K. Clark, MD. Something Old, Something New, Something Borrowed, Something Blue
 Palliative Care Something Old, Something New, Something Borrowed, Something Blue Osteopathic Founders Foundation Richard C. Staab, DO Memorial Symposium April 6-7, 2018 Jennifer K. Clark, MD Disclosures
Palliative Care Something Old, Something New, Something Borrowed, Something Blue Osteopathic Founders Foundation Richard C. Staab, DO Memorial Symposium April 6-7, 2018 Jennifer K. Clark, MD Disclosures
Palliative Care in the Community Setting. David Mandelbaum, MD Melissa Rockhill, MSN, GNP-BC Lorie Hacker, MSN, NP-C, CNE
 Palliative Care in the Community Setting David Mandelbaum, MD Melissa Rockhill, MSN, GNP-BC Lorie Hacker, MSN, NP-C, CNE Objectives 1. Discuss the framework for building a palliative care program in the
Palliative Care in the Community Setting David Mandelbaum, MD Melissa Rockhill, MSN, GNP-BC Lorie Hacker, MSN, NP-C, CNE Objectives 1. Discuss the framework for building a palliative care program in the
Romayne Gallagher MD, CCFP Divisions of Residential and Palliative Care Providence Health Care Vancouver, BC
 Romayne Gallagher MD, CCFP Divisions of Residential and Palliative Care Providence Health Care Vancouver, BC My father s memory may be gone but otherwise he is all there Daughter of 92 yr old in wheelchair,
Romayne Gallagher MD, CCFP Divisions of Residential and Palliative Care Providence Health Care Vancouver, BC My father s memory may be gone but otherwise he is all there Daughter of 92 yr old in wheelchair,
Immediate Past President American Association of Critical-Care Nurses Clareen Wiencek, PhD, RN, ACHPN, ACNP
 Clareen Wiencek, PhD, RN, ACHPN, ACNP Immediate Past President American Association of Critical-Care Nurses Clareen.Wiencek@aacn.org Palliative Care and Critical Care: A New Decade The purpose of this
Clareen Wiencek, PhD, RN, ACHPN, ACNP Immediate Past President American Association of Critical-Care Nurses Clareen.Wiencek@aacn.org Palliative Care and Critical Care: A New Decade The purpose of this
Learning Objectives. Hospice Size. CoPs (cont d) The Problem: Pertinent Medicare CoPs related to Hospice Medical Directors
 The Problem: Pertinent Medicare CoPs related to Hospice Medical Directors") Session 7D NHPCO 29th Management and Leadership Conference March 28, 2014 Competency Evaluation for the Hospice Physician in Smaller or Rural Hospices Cheryl Arenella MD, MPH Associate, The Corridor Group
Session 7D NHPCO 29th Management and Leadership Conference March 28, 2014 Competency Evaluation for the Hospice Physician in Smaller or Rural Hospices Cheryl Arenella MD, MPH Associate, The Corridor Group
Palliative Care in Adolescents and Young Adults Needs, Obstacles and Opportunities
 Palliative Care in Adolescents and Young Adults Needs, Obstacles and Opportunities Justin N Baker, MD, FAAP, FAAHPM Chief, Division of Quality of Life and Palliative Care Attending Physician, Quality of
Palliative Care in Adolescents and Young Adults Needs, Obstacles and Opportunities Justin N Baker, MD, FAAP, FAAHPM Chief, Division of Quality of Life and Palliative Care Attending Physician, Quality of
Managing Conflicts Around Medical Futility
 Managing Conflicts Around Medical Futility Robert M. Taylor, MD Medical Director, OSUMC Center for Palliative Care Associate Professor of Neurology The Ohio State University James Cancer Hospital Objectives
Managing Conflicts Around Medical Futility Robert M. Taylor, MD Medical Director, OSUMC Center for Palliative Care Associate Professor of Neurology The Ohio State University James Cancer Hospital Objectives
Hospice and Palliative Care An Essential Component of the Aging Services Network
 Hospice and Palliative Care An Essential Component of the Aging Services Network Howard Tuch, MD, MS American Academy of Hospice and Palliative Medicine Physician Advocate, American Academy of Hospice
Hospice and Palliative Care An Essential Component of the Aging Services Network Howard Tuch, MD, MS American Academy of Hospice and Palliative Medicine Physician Advocate, American Academy of Hospice
Integrating Palliative and Oncology Care in Patients with Advanced Cancer
 Integrating Palliative and Oncology Care in Patients with Advanced Cancer Jennifer Temel, MD Massachusetts General Hospital Cancer Center Director, Cancer Outcomes Research Overview 1. Why should we be
Integrating Palliative and Oncology Care in Patients with Advanced Cancer Jennifer Temel, MD Massachusetts General Hospital Cancer Center Director, Cancer Outcomes Research Overview 1. Why should we be
2514 Stenson Dr Cedar Park TX Fax
 END OF LIFE DEFINITIONS Advance Directive ~ legal document stating a patient's preferences for end-of-life treatment and care Amenity ~ something intended to make circumstances more pleasant Chronic ~
END OF LIFE DEFINITIONS Advance Directive ~ legal document stating a patient's preferences for end-of-life treatment and care Amenity ~ something intended to make circumstances more pleasant Chronic ~
Adam D. Marks, MD MPH Assistant Professor of Medicine University of Michigan Health System
 Adam D. Marks, MD MPH Assistant Professor of Medicine University of Michigan Health System The truth will set you free but first it will piss you off - Gloria Steinem Life expectancy is up dramatically
Adam D. Marks, MD MPH Assistant Professor of Medicine University of Michigan Health System The truth will set you free but first it will piss you off - Gloria Steinem Life expectancy is up dramatically
Early Integration of Palliative Care
 Early Integration of Palliative Care Dr. Camilla Zimmermann Head, Palliative Care Program University Health Network Toronto November 1, 2014 www.fpon.ca Early Integration of Palliative Care: Evidence and
Early Integration of Palliative Care Dr. Camilla Zimmermann Head, Palliative Care Program University Health Network Toronto November 1, 2014 www.fpon.ca Early Integration of Palliative Care: Evidence and
Identify essential primary palliative care (PPC) communication skills that every provider needs AND clinical triggers for PPC conversations
 communication skills that every provider needs AND clinical triggers for PPC conversations") Identify essential primary palliative care (PPC) communication skills that every provider needs AND clinical triggers for PPC conversations Esmé Finlay, MD Division of Palliative Medicine University of
Identify essential primary palliative care (PPC) communication skills that every provider needs AND clinical triggers for PPC conversations Esmé Finlay, MD Division of Palliative Medicine University of
Withdrawal of Care in the ICU
 Withdrawal of Care in the ICU Arlene Bobonich, MD Director, Inpatient Palliative Medicine PinnacleHealth System WHO IS DRIVING THE BUS? WHERE IS THE BUS GOING? HOW DO YOU GET OFF THE BUS? WHO GETS THROWN
Withdrawal of Care in the ICU Arlene Bobonich, MD Director, Inpatient Palliative Medicine PinnacleHealth System WHO IS DRIVING THE BUS? WHERE IS THE BUS GOING? HOW DO YOU GET OFF THE BUS? WHO GETS THROWN
PALLIATIVE CARE GOALS of CARE: DNR. Debra Luczkiewicz MD Kelly Denall ANP Supportive Medical Partners
 PALLIATIVE CARE GOALS of CARE: DNR Debra Luczkiewicz MD Kelly Denall ANP Supportive Medical Partners OBJECTIVES Understand the scope of palliative care. Describe the differences between Hospice and palliative
PALLIATIVE CARE GOALS of CARE: DNR Debra Luczkiewicz MD Kelly Denall ANP Supportive Medical Partners OBJECTIVES Understand the scope of palliative care. Describe the differences between Hospice and palliative
Brought to you by the Massachusetts Medical Society and its Committee on Geriatric Medicine
 Brought to you by the Massachusetts Medical Society and its Committee on Geriatric Medicine What is palliative care? Care focused on helping support and guide patients who have life limiting and serious
Brought to you by the Massachusetts Medical Society and its Committee on Geriatric Medicine What is palliative care? Care focused on helping support and guide patients who have life limiting and serious
NURSING S ROLE IN ICU PALLIATIVE ACCESS 2. emotional, intellectual, and spiritual needs (Dahlin, 2013). Palliative care can be
. Palliative care can be") NURSING S ROLE IN ICU PALLIATIVE ACCESS 2 Palliative care is health care provided by an interdisciplinary team with the primary goal of relieving patient and family suffering through treatment of a patient
NURSING S ROLE IN ICU PALLIATIVE ACCESS 2 Palliative care is health care provided by an interdisciplinary team with the primary goal of relieving patient and family suffering through treatment of a patient
Donation After Cardiac Death
 Donation After Cardiac Death Barriers to increasing organ donations after cardiac death Key lessons learned from previous and ongoing efforts/next steps Uncontrolled Category II DCD Kenneth E. Wood, DO
Donation After Cardiac Death Barriers to increasing organ donations after cardiac death Key lessons learned from previous and ongoing efforts/next steps Uncontrolled Category II DCD Kenneth E. Wood, DO
Palliative Care & Hospice
 Palliative Care & Hospice Kenneth Brummel-Smith, M.D. Charlotte Edwards Maguire Professor, Department of Geriatrics Florida State University College of Medicine 1 Diane Meier, MD Director, Center to Advance
Palliative Care & Hospice Kenneth Brummel-Smith, M.D. Charlotte Edwards Maguire Professor, Department of Geriatrics Florida State University College of Medicine 1 Diane Meier, MD Director, Center to Advance
Update on the Cambia Palliative Care Center of Excellence at UW
 Update on the Cambia Palliative Care Center of Excellence at UW J. Randall Curtis, MD, MPH Director, Cambia Palliative Care Center of Excellence Harborview Medical Center, University of Washington www.uwpalliativecarecenter.com
Update on the Cambia Palliative Care Center of Excellence at UW J. Randall Curtis, MD, MPH Director, Cambia Palliative Care Center of Excellence Harborview Medical Center, University of Washington www.uwpalliativecarecenter.com
The Role of Palliative Care in Readmission Reduction Steven Z. Pantilat, MD
 The Role of Palliative Care in Readmission Reduction Steven Z. Pantilat, MD Professor of Clinical Medicine Alan M. Kates and John M. Burnard Endowed Chair in Palliative Care Director, Palliative Care Program
The Role of Palliative Care in Readmission Reduction Steven Z. Pantilat, MD Professor of Clinical Medicine Alan M. Kates and John M. Burnard Endowed Chair in Palliative Care Director, Palliative Care Program
Objectives. Chronic Care Management (CCM) 9/13/2018 INCREASING EARLIER HOSPICE REFERRALS THROUGH CHRONIC CARE MANAGEMENT
 9/13/2018 INCREASING EARLIER HOSPICE REFERRALS THROUGH CHRONIC CARE MANAGEMENT") INCREASING EARLIER HOSPICE REFERRALS THROUGH CHRONIC CARE MANAGEMENT Jill Wilke, MS, RN Director of Lake Regional Home Health, Hospice, & Palliative Chronic Care Management Objectives Describe the Chronic
INCREASING EARLIER HOSPICE REFERRALS THROUGH CHRONIC CARE MANAGEMENT Jill Wilke, MS, RN Director of Lake Regional Home Health, Hospice, & Palliative Chronic Care Management Objectives Describe the Chronic
Research and Innovation in Aging Forum December 15, 2015
 Palliative Care: Evaluating Regional Initiatives to Reduce Hospital Utilization Ray Viola, MD Division of Palliative Medicine Department of Medicine Research and Innovation in Aging Forum December 15,
Palliative Care: Evaluating Regional Initiatives to Reduce Hospital Utilization Ray Viola, MD Division of Palliative Medicine Department of Medicine Research and Innovation in Aging Forum December 15,
Ventilator Withdrawal: Procedures and Outcomes. Report of a Collaboration Between a Critical Care Division and a Palliative Care Service
 954 Journal of Pain and Symptom Management Vol. 26 No. 4 October 2003 Clinical Note Ventilator Withdrawal: Procedures and Outcomes. Report of a Collaboration Between a Critical Care Division and a Palliative
954 Journal of Pain and Symptom Management Vol. 26 No. 4 October 2003 Clinical Note Ventilator Withdrawal: Procedures and Outcomes. Report of a Collaboration Between a Critical Care Division and a Palliative
The Impact of Death Anxiety on Communication and Care Delivery for Patients with Advanced Illness
 The Impact of Death Anxiety on Communication and Care Delivery for Patients with Advanced Illness Liz Elmquist, LMSW, New York Presbyterian/Weill Cornell Medical Center Carolyn Fulton, LCSW-R, Memorial
The Impact of Death Anxiety on Communication and Care Delivery for Patients with Advanced Illness Liz Elmquist, LMSW, New York Presbyterian/Weill Cornell Medical Center Carolyn Fulton, LCSW-R, Memorial
Focused on the Big picture
 Focused on the Big picture Tamara M. Shearrow, MSN, NP-C, ACHPN Palliative Care Services Winchester Medical Center The presenter has no conflicts of interest to disclose. Objectives Understand how palliative
Focused on the Big picture Tamara M. Shearrow, MSN, NP-C, ACHPN Palliative Care Services Winchester Medical Center The presenter has no conflicts of interest to disclose. Objectives Understand how palliative
Temiskaming Hospital Hospice Palliative Care. Presented by: Dr. Don Davies January 31, 2017
 Temiskaming Hospital Hospice Palliative Care Presented by: Dr. Don Davies January 31, 2017 Objectives Talk a little about Palliative Care. In general A quick look at Temiskaming District and Hospice Model
Temiskaming Hospital Hospice Palliative Care Presented by: Dr. Don Davies January 31, 2017 Objectives Talk a little about Palliative Care. In general A quick look at Temiskaming District and Hospice Model
Objectives. Sometimes We Get Ahead of Ourselves 3/6/2015
 Withholding and Withdrawing No Longer Beneficial Medical Interventions: Historical, Ethical and Practical Issues Marcia Levetown, MD FAAHPM HealthCare Communication Assocs Houston, TX mlevetown@earthlink.net
Withholding and Withdrawing No Longer Beneficial Medical Interventions: Historical, Ethical and Practical Issues Marcia Levetown, MD FAAHPM HealthCare Communication Assocs Houston, TX mlevetown@earthlink.net
What is palliative care? What is palliative care? Dr Claire L Hookey
 What is palliative care? What is palliative care? Dr Claire L Hookey Palliative Care an approach that improves the quality of life of patients and their families facing the problems associated with life-threatening
What is palliative care? What is palliative care? Dr Claire L Hookey Palliative Care an approach that improves the quality of life of patients and their families facing the problems associated with life-threatening
Cambia Palliative Care Metrics: Where are we and where are we going?
 Cambia Palliative Care Metrics: Where are we and where are we going? J. Randall Curtis, MD, MPH Director, Cambia Palliative Care Center of Excellence www.uwpalliativecarecenter.com Overview of System-Wide
Cambia Palliative Care Metrics: Where are we and where are we going? J. Randall Curtis, MD, MPH Director, Cambia Palliative Care Center of Excellence www.uwpalliativecarecenter.com Overview of System-Wide
Palliative Care Impact on Patients with Breast Cancer. Sigy Chathanatt, D.O. Board Certified in Hospice and Palliative Care September 17, 2016
 Palliative Care Impact on Patients with Breast Cancer Sigy Chathanatt, D.O. Board Certified in Hospice and Palliative Care September 17, 2016 What do We Know? Cancer as a Disease Experience Survival rates
Palliative Care Impact on Patients with Breast Cancer Sigy Chathanatt, D.O. Board Certified in Hospice and Palliative Care September 17, 2016 What do We Know? Cancer as a Disease Experience Survival rates
Changing the Face of Palliative Care in Oncology Practice
 Changing the Face of Palliative Care in Oncology Practice Karin Porter-Williamson MD Associate Professor of Medicine Medical Director Palliative Care Services KU Hospital Amy Velasquez RN BSN OCN Allen
Changing the Face of Palliative Care in Oncology Practice Karin Porter-Williamson MD Associate Professor of Medicine Medical Director Palliative Care Services KU Hospital Amy Velasquez RN BSN OCN Allen
Understanding Hospice, Palliative Care and of-life Issues
 Understanding Hospice, Palliative Care and End-of of-life Issues Huntington's Disease Society of America June 2009 Roseanne Berry, MS, RN RBC Consulting, LLC roseanne@rbcconsultingllc.com The information
Understanding Hospice, Palliative Care and End-of of-life Issues Huntington's Disease Society of America June 2009 Roseanne Berry, MS, RN RBC Consulting, LLC roseanne@rbcconsultingllc.com The information
Integration of a Palliative Approach:
 Integration of a Palliative Approach: A Look at Serious Illness 2018 CHPCA Learning Institute June 2018 Objectives 1. Explore what is meant by a palliative approach 2. Describe different conceptual models
Integration of a Palliative Approach: A Look at Serious Illness 2018 CHPCA Learning Institute June 2018 Objectives 1. Explore what is meant by a palliative approach 2. Describe different conceptual models
THE ROLE OF PALLIATIVE CARE IN TREATMENT OF PATIENTS WITH CHRONIC, INFECTIOUS DISEASE
 THE ROLE OF PALLIATIVE CARE IN TREATMENT OF PATIENTS WITH CHRONIC, INFECTIOUS DISEASE JESSICA MCFARLIN MD ASSISTANT PROFESSOR OF NEUROLOGY DIVISION CHIEF, PALLIATIVE AND SUPPORTIVE CARE I HAVE NO COI OR
THE ROLE OF PALLIATIVE CARE IN TREATMENT OF PATIENTS WITH CHRONIC, INFECTIOUS DISEASE JESSICA MCFARLIN MD ASSISTANT PROFESSOR OF NEUROLOGY DIVISION CHIEF, PALLIATIVE AND SUPPORTIVE CARE I HAVE NO COI OR
Community and Mental Health Services. Palliative Care. Criteria and
 Community and Mental Health Services Specialist Palliative Care Service Referral Criteria and Guidance November 2018 Specialist Palliative Care Service Referrals These guidelines cover referrals for patients
Community and Mental Health Services Specialist Palliative Care Service Referral Criteria and Guidance November 2018 Specialist Palliative Care Service Referrals These guidelines cover referrals for patients
To prevent and relieve suffering, and promote quality of life at every stage of life
 To prevent and relieve suffering, and promote quality of life at every stage of life The views expressed in this presentation are those of the author and do not necessarily reflect the official policy
To prevent and relieve suffering, and promote quality of life at every stage of life The views expressed in this presentation are those of the author and do not necessarily reflect the official policy
Death as Great Equalizer? Recognizing & Reducing Disparities in End-Stage Cancer Care
 Death as Great Equalizer? Recognizing & Reducing Disparities in End-Stage Cancer Care Holly G. Prigerson, PhD Irving Sherwood Wright Professor of Geriatrics Professor of Sociology in Medicine Director,
Death as Great Equalizer? Recognizing & Reducing Disparities in End-Stage Cancer Care Holly G. Prigerson, PhD Irving Sherwood Wright Professor of Geriatrics Professor of Sociology in Medicine Director,
Transitioning to palliative care: How early is early palliative care?
 Transitioning to palliative care: How early is early palliative care? Cancer: a growing problem Cancer is an increasing health care problem It is estimated that by 2020, there will be 20 million new cases
Transitioning to palliative care: How early is early palliative care? Cancer: a growing problem Cancer is an increasing health care problem It is estimated that by 2020, there will be 20 million new cases