MANUAL MEDICAL DIRECTOR RESPIRATORY BOB MILLER, BS, RRT, RCP RESPIRATORY SERVICES DIRECTOR APPROVED BY
|
|
|
- Evelyn Snow
- 5 years ago
- Views:
Transcription
1 HOSPITAL RESPIRATORY SERVICES RESPIRATORY SERVICES TITLE: NON-INVASIVE CAPNOGRAPHY MONITORING POLICY # PAGES 1 OF 10 MANUAL RESPIRATORY SERVICES ATTACHMENTS: RESPIRATORY COMPROMISE RISK LEVELS RESPIRATORY COMPROMISE EVALUATION. RESPIRATORY CAPNOGRAPHY COMPOSITE SCORE ASSESSMENT. DEVELOPED BY: RESPIRATORY SERVICES MEDICAL DIRECTOR RESPIRATORY DATE IMPLEMENTED: DATE REVIEWED: DATE REVISED: BOB MILLER, BS, RRT, RCP RESPIRATORY SERVICES DIRECTOR APPROVED BY POLICY/PURPOSE Post-operative respiratory failure & respiratory compromise from opioid-induced respiratory depression is associated with increased morbidity & mortality 1. Capnography monitoring can help to prevent or reduce adverse events such as undetected respiratory depression and hypoxia 2. Some experts believe that monitoring ventilation with ETCO2 measurement in addition to pulse oximetry could improve patient safety and postoperative clinical outcomes 3-4 Opioid-induced respiratory compromise can be reduced with appropriate screening and monitoring of patients receiving multiple forms of opioid therapy. The purpose of this policy is to provide guidance for patient selection/inclusion and capnography monitoring for non-mechanically ventilated (intubated) patients admitted to Non-ICU nursing units. General Information/ Definitions: End-tidal carbon dioxide (ETCO2) is the level of carbon dioxide that is released at the end of an exhaled breath. ETCO2 levels reflect the adequacy with which CO2 is carried in the blood back to the lungs and exhaled. Available evidence has established that ETCO2 measurement can provide an indication of cardiac output and pulmonary blood flow. Non-invasive methods for ETCO2 measurement include capnometry and capnography. Capnometry provides a numerical value for ETCO2. In contrast, capnography delivers a more comprehensive measurement that is displayed in both graphical (waveform) and numerical value.
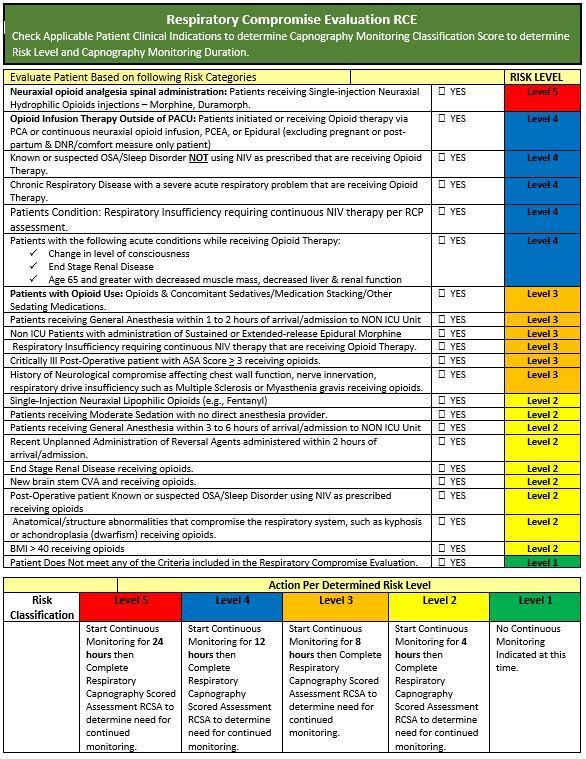
2 IPI Integrated Pulmonary Index: The IPI algorithm incorporates four real-time respiratory measurements into a single number that represents an inclusive respiratory profile: end-tidal CO2 (etco2), respiratory rate, pulse rate and SpO2 (pulse oximetry). IPI is displayed on a scale from 1 to 10, with 10 indicating a normal cardiopulmonary/respiratory status. IPI provides a real-time indication of changes in the patient s respiratory status that may not be reflected by the current values of any of the four individual parameters. To aid in monitoring patients over time, IPI is captured and analyzed to show upward and downward trends. Respiratory Compromise Evaluation (RCE): Assessment tool used to determine risk level for Respiratory Compromise. Respiratory Compromise Scored Assessment (RCA): Assessment tool used to determine safe liberation from non-invasive capnography monitoring. SCOPE OF RESPONSIBILITY Respiratory Care Practitioner (RCP), Registered Nurse (RN) GENERAL GUIDELINES This policy covers all patient populations requiring NON-Invasive capnography monitoring. There are two methods for initiating patient monitoring. Method 1 Direct Provider orders, Method 2 Respiratory Consult & Treat per policy protocol. Patients < 18 years of age will require a direct Provider order as outlined in program order process and will be excluded by Respiratory Consult and Treat protocols per policy. Method:1 Direct provider order consisting of standard order set with specific monitoring duration indicated with four pre-determined time choices of 4 hours, 8 hours, 12 hours, & 24 hours, at the end of first 24-hour monitoring period the provider will be required to extend the order every 24 hours per Provider discretion. Method: 2 RCP or RN patient driven protocol order for Respiratory Consult and Treat per policy for Capnography monitoring. This order will trigger initiation of Respiratory Compromise Evaluation (RCE) by RCP to determine patient inclusion for non-invasive capnography monitoring & duration (real-time) of monitoring based on Risk Evaluation & Respiratory Compromise Scored Assessment. 1) Respiratory Compromise Evaluation (RCE), RCP will complete bedside evaluation assessment of patient by starting at the highest risk level and continuing to the lowest risk level to complete the evaluation. When the highest risk level has been determined, the RCP will start continuous monitoring for the time duration associated with the matching risk level. Example: Patient meets Risk Level 3. The patient would be monitored for 8 hours continuously then after 8 hours the RCP would complete a Respiratory Capnography Composite Score assessment to determine if patient can be removed safely from monitoring.
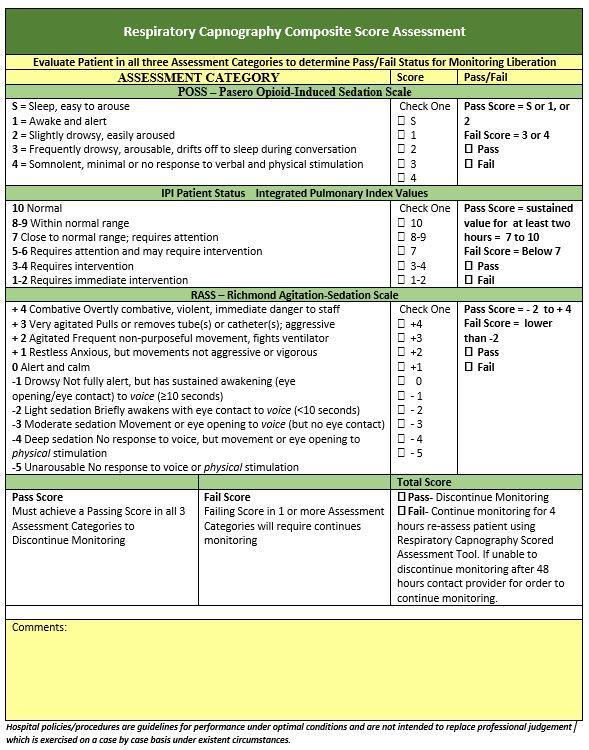
3 2) Respiratory Compromise Scored Assessment (RCA) determines monitoring discontinuation post initial RCE established assessment. Discontinuation is based on three pass/fail assessment categories to include POSS Pasero Opioid induced Sedation scale 5, sustained IPI Integrated Pulmonary Index values taken from Capnography Capnocheck monitor and RASS Richmond Agitation Sedation Scale. Only RCP staff can discontinue monitoring based on Respiratory Compromise Assessment (RCA) scored assessment. If the patient passes all three categories of the RCA assessment, the monitoring is discontinued. Respiratory Compromise Scored Assessment is a 3-category assessment that evaluates the following Criteria: 1. POSS Pasero Opioid Sedation Scale: Pass/Fail a) Pass Score = S or 1, or 2 b) Fail Score = 3 or 4 2. IPI Integrated Pulmonary Index Score- Algorithm score based on RR, SpO2, HR. ETCO2 a) Pass Score = sustained value for at least two hours = 7 to 10 b) Fail Score = Below 7 3. RASS Richmond Agitation-Sedation Scale a) Pass Score = - 2 to + 4 b) Fail Score = lower than -2 If the patient fails any or all three categories, the monitoring continues for four hours and the patient is re-assessed using the same composite scored assessment methodology until the patient is liberated from the monitoring. In the event the patient cannot be liberated per assessment within 24 hours of monitoring start time, the Provider is contacted for consultation of care. In the event a provider requests discontinuation of monitoring without completion of RCA assessment, provider must place discontinuation order in EHR, no monitoring will be discontinued without executed Provider EHR order or RCP assessment to discontinue monitoring. Patient Selection & Assessment: 1. All patients receiving Opioid Therapy including procedural sedation admitted to a NON-ICU unit will receive a RCE evaluation to determine Respiratory Compromise Risk Level (listed below) per protocol policy. OR 2. Direct Provider order including short term procedural sedation in the Emergency Department and monitoring initiated by direct provider orders can be started and discontinued at any time per Provider consultation.

4 ORDER PROCEDURE PACU OPIOID THERAPY PATIENTS In the PACU, PACU RN will initiate Respiratory Services consultation request for RCE evaluation assessment to include all post-operative patients admitted to inpatient status to a Non-ICU nursing unit. Any patients who meets risk criteria outlined in this policy will be placed on non-invasive capnography monitoring. At time of PACU RN consultation request, Respiratory Services will immediately report to PACU to complete bedside RCE Evaluation in PACU. All patients requiring monitoring based on RCE evaluation will be placed on bedside capnography monitoring in PACU prior to inpatient transfer. The patient will remain on monitoring in PACU until
5 transfer to inpatient unit. At time of transfer, the PACU RN will transport the patient on the bedside monitor to inpatient room and will be responsible to resume monitoring set up at new room location. The PACU RN will immediately contact Respiratory Services for notification of arrival to inpatient unit. Notification will include hand-off report of patient status and room location. Respiratory Services will report to bedside to verify patient monitoring set-up and perform a monitor check. PACU RCE Inclusion Criteria Summary The following criteria shall also be a consideration for RCE consultation: a) Patients with STOP BANG/Sleep Apnea Score greater than 5. b) Patients who have received neuraxial opioid analgesia spinal medication administration (aka. Duramorph) in the Operating Room or postoperatively in PACU. (If admitted, monitoring will continue for 24 hours by the RCP). c) Patients who received operative General Anesthesia and then receive additional Opioid medications while in PACU (aka. stacking medications) for pain. d) Any patient with diagnosed OSA (Obstructive Sleep Apnea) will receive CPAP therapy by the RCP and EtCO2 monitoring if applicable based on the patient interface utilization capabilities. Respiratory Services consultation notifications will be processed via RT communication order entry into EHR as Respiratory Evaluate & Treat for Capnography Monitoring. Order will be entered at time of patient arriving to the inpatient unit from PACU. Non-Opioid Obstructive Sleep Apnea (OSA) Patients Patients admitted to a NON-ICU nursing unit identified at risk for Obstructive Sleep Apnea (OSA) based on the following criteria will receive a Respiratory Services consultation by nursing services for OSA risk prevention interventions. Respiratory Services will complete a bedside assessment to confirm OSA risks and if patient is confirmed at Risk for Undiagnosed or Diagnosed untreated OSA the patient will receive one of the following patient safety Interventions: Non-Invasive Positive Pressure therapy or Non-Invasive Capnography monitoring interventions determined by the following criteria:
6 Clinical Criteria for Monitoring/Interventions a) Undiagnosed Untreated OSA Defined as: Any patient with Obstructive Sleep Apnea Score (aka Stop Bang Score) of greater than 4 on risk scale of 1 thru 8 that has not had a diagnostic sleep study or and does not currently utilize supportive Non-Invasive Positive Pressure therapy. b) Diagnosed Untreated OSA Defined as: Any patient with Obstructive Sleep Apnea Score (aka Stop Bang Score) of greater than 4 on risk scale of 1 thru 8 that has had a diagnostic sleep study with positive diagnosis of OSA and does not currently utilize supportive Non-Invasive Positive Pressure therapy. OSA Risk Prevention Interventions Patients determined high risk Undiagnosed OSA will receive Respiratory Consult and Treat order for Non-Invasive Positive Pressure Therapy via auto titrating PAP therapy for sleeping or resting periods or Non- Invasive Capnography monitoring. These patients will be placed on auto-titrating CPAP (Auto-PAP) while sleeping to reduce risk of respiratory compromise while in facility care. If patient refuses Auto-PAP therapy for sleep periods while in the facility, patient will be placed on Non-Invasive Capnography Monitoring during sleep periods in the facility. These patients will be referred to Outpatient sleep center at time of discharge for a diagnostic sleep study to confirm OSA diagnosis. In the event patient refuses both safety interventions Provider must be notified of patient refusal of risk prevention interventions. RCP will document refusal and Provider notification in clinical progress notes of EHR. Equipment Set-up and Initiation of patient monitoring Interface Selection: Obtain EtCO2 monitor and Smart CapnoLine from patient supply rooms. Primary starting line is the Smart Capnoline Plus (adult intermediate O2 #9822) oral nasal sampling line that provides short-term 24-hour coverage and supplemental oxygen line. Select appropriate specialty sampling line if needed based on patient s respiratory pattern and need for supplemental oxygen. Starting interface choices include; 1) Pediatric Smart Capnoline Oral/Nasal Sampling Line # 7269 (for patients with a smaller facial area) with oxygen supply capabilities) 2) FilterLine H set (trach patients or patients on NIV that require inline circuit set up)
7 3) Nasal Only Filterline #7739 for patients with intolerance to oral nasal filterline. 4) Capnoline H Plus oral/nasal filterline for patients with high humidity concerns NOTE: Non-ventilator tracheostomy patients will require FilterLine H Set attached directly to distal end of trach tube. Patients on NIV bilevel or CPAP therapy via oral/nasal mask interface will require FilterLine H Set to be placed inline distal to the NIV mask in-line with the circuit. Exceptions/Special Circumstance: In the event a patient is utilizing a respiratory modality where monitoring cannot be inter-phased in conjunction with capnography line, the patient will be placed on continuous oximetry monitoring via capnography monitor until the patient can be transitioned to another modality or has intermittent use of that modality. Example patient wearing home NIV therapy with Nasal pillow interphase or patient with high flow oxygen modality and cannot be weaned i.e. Vapotherm or high flow oxygen mask. Monitor Initiation: Insert Smart CapnoLine into the EtCO2 monitor port Educate patient and family on the purpose of EtCO2 monitor, alarm feature, and patient interventions if the monitor alarms Apply Smart CapnoLine to patient to allow sampling from the nose and mouth Place pulse ox sensor on the patient Administer supply oxygen as needed to maintain SpO2 greater than 89%. Turn the monitor on and allow 30 seconds for waveform tracings to appear Enter patient type for IPI is correctly set: Adult Patients or Pediatric Patients (1-3 yrs, 3-6 yrs., and 6-12 yrs.). Evaluate End-tidal waveform to ensure accurate tracing and reading. IPI reading will be used to give you a summary of the patient status. IPI reading equal to 8 or greater is considered normal Document in EHR, ETCO2, SpO2, RR, and IPI score at set up then return start 1- hour to perform first Q4-hour check. Complete Q-4-hour checks until discontinued.
8 Alarm Set Up: Alarm parameters are patient specific based on the patient s starting baseline and chronic disease status. Patients with specific respiratory difficulties (in contrast to normally healthy patients who are being monitored during sedation or pain management) may require a lower IPI Low Alert threshold to reflect their impaired respiratory capacity. The following are recommended default alarms: EtC02 High -60 mmhg EtC02 Low 10 mmhg IPI 7 Respiratory rate High 35 breaths per minute Respiratory rate Low 6 breaths per minute No breath delay 30 seconds FiCo2-8 mmhg Pulse oximetry less than 90% Patients with Chronic CO2 Retention: Patients with known or suspected chronic CO2 retention, as confirmed by current or previous blood gas analysis will require modification of alarm settings, set high EtCO2 alarm limit at 10 above baseline value and set low alarm limit at 10 below baseline value. Set IPI at 6. ETCO2 Values Normal Adults ETCO2 35 to 45mmHg (in normal, healthy adults) Device troubleshooting and Abnormal ETCO2 Values potential causes An EtCO2 less than 35 mmhg indicates an increased respiratory rate or Hyperventilation/ Hypo-capnia" An EtCO2 more than 45 mmhg indicates respiratory depression or Hypoventilation/ Hypercapnia" A sudden loss of EtCO2 indicates no respiratory activity (apnea). Medical conditions that affect reliability of ETCO2 values include: COPD (causing incomplete alveolar emptying) ARDS (causing a ventilation-perfusion mismatch) Pulmonary embolism and hypovolemia (causing un-perfused, but ventilated alveoli) Capnography monitoring evaluates trends of the RR and ETCO2 values, and should be assessed together. In the event the RR and ETCO2 or IPI Index are changing the patient should be assessed and interventions considered as needed.
9 Indications for Interventions If ETC02 is mmhg (Non-Chronic CO2 retainer) for Chronic CO2 retainers EtCO2 that exceeds 15 Torr above patients established baseline value IPI Index of less than 7 Abnormal (SP02 saturation, ETCO2 Reading, HR, RR resulting in monitor alarms Interventions: Attempt to stimulate and arouse the patient. If patient is immediately aroused and breathing normally, monitor until ETCO2 level returns to baseline. Assure the airway is patient and patient position is optimal for ventilatory effort. Assess vital signs for decompensation (SP02 saturation, BP, HR, RR, and loss of consciousness (LOC). Assess pain, level of sedation, and consider decreasing narcotic dose and/or frequency. Reposition patient head and neck to assure adequate respirations. Reposition the Smart CapnoLine if necessary. Replace the Smart CapnoLine if excessive moisture is suspected as excessive moisture may require high humidity line. Activate Rapid Response Team Protocol. Administer Naloxone Therapy to reverse Opioid effects. Consider obtaining ABG (RRT can also be consulted during this process). Application of NIV therapy with settings per RCP assessment to stabilize the patient followed by ABG analysis and provider notification within 45 minutes of initiation. Transfer patient to higher level of care until patient is stable. Interpretation of Monitoring Trends When utilizing capnography monitoring during sedation, the emphasis should be placed on significant changes from the baseline waveform and numeric EtC02 value rather than an absolute number. Device must be placed at a minimum of 3 min prior to administration of sedation to obtain accurate baseline data.
 to determine safe discontinuation of monitoring.")
10 IPI INDEX SCORE SCALE DOCUMENTION RCP is responsible for checking and documenting monitoring checks every four hours until monitoring is discontinued. DISCONTINUATION OF MONITORING RCP shall complete Respiratory Compromise Scored Assessment (RCA) to determine safe discontinuation of monitoring. If the patient passes all three categories of the RCA assessment, the monitoring is discontinued by RCP per policy. RCP will notify RN responsible for patient that monitoring has been discontinued and document in clinical progress notes RCA score detail and time of discontinuation. In the event the patient cannot be liberated per assessment within 24 hours of monitoring initiation time, RCP will contact Provider for consultation of care. In the event a Provider requests discontinuation of monitoring without completion of RCP assessment, provider must place discontinuation order in HER. No monitoring will be discontinued without executed Provider EHR order or RCP RCA assessment to discontinue monitoring.
11 Other Considerations: PRN Medication Change in Opioid Therapy Regimen: In the event monitoring, has been discontinued by RCP assessment and patient has a change in Opioid pain regimen management that could result in new risk for Respiratory Compromise per RN assessment, RN should initiate a new RT Consult and Treat request for new RCE evaluation for capnography monitoring to Respiratory Services.
12 REFERENCES: 1. Brueckmann et al. Development and validation of a Score for Prediction of Postoperative Respiratory Complications: Anesthesiology 2013; 118: Deitch K, Miner J, Chudnofsky CR, Dominici P, Latta D. Does end tidal CO2 monitoring during emergency department procedural sedation and analgesia with propofol decrease the incidence of hypoxic events? A randomized, controlled trial. Ann Emerg Med Mar; 55(3): Hutchison R, Rodriguez L. Capnography and respiratory depression. Am J Nurs Feb; 108(2): Weinger M, Lee LA. No patient shall be harmed by opioid-induced respiratory depression: proceedings of "Essential monitoring strategies to detect clinically significant drug-induced respiratory depression in the postoperative period" conference. APSF Newsletter [Internet] [cited 2015 Aug 5]; 26 (2):21, Available from: 5. Pasero, Chris, and Margo McCaffery. "Monitoring Sedation: It's the key to preventing opioid-induced respiratory depression." AJN The American Journal of Nursing (2002): Canet, Jaume, et al. "Development and validation of a score to predict postoperative respiratory failure in a multicentre European cohort: a prospective, observational study." European Journal of Anaesthesiology (EJA) 32.7 (2015): Gallart, Lluís, and Jaume Canet. "Post-operative pulmonary complications: Understanding definitions and risk assessment." Best Practice & Research Clinical Anaesthesiology 29.3 (2015): Berkenstadt, H., et al., An evaluation of the Integrated Pulmonary Index (IPI) for the detection of respiratory events in sedated patients undergoing colonoscopy. J Clin Monit Comput Jun; 26(3): , (3): p Bloom, J., et al., Postoperative naloxone rescue following parenteral opioids after abdominal surgery: Incidence and cohort morbidity and mortality. Intensive Care Medicine. 2010: 36 (Suppl 2): S283.: p. S Burke, J., et al., Implementing Microstream end tidal CO2 in the PACU. Journal of PeriAnesthesia Nursing. 2014: 29 (5): e28: p. e Adams, L., S. Butas, and D. Spurlock, Capnography (ETCO2), respiratory depression, and nursing interventions in moderately sedated adults undergoing transesophageal echocardiography (TEE). J Perianesth Nurs Feb;30(1):14-22., (1): p Nisbet AT, Mooney-Cotter F. Comparison of selected sedation scales for reporting opioid- induced sedation assessment. Pain Manag Nurs Sep;10(3): Gupta, P. K., Fang, X., Miller, W. J., Cemaj, S., Forse, R. A., & Morrow, L. E. Development and Vaildation of a Risk Calculator Predicting Postoperative Respiratory Failure. Chest, 2011:140(5),
13 14. Practice Guidelines for the Prevention, Detection, and Management of Respiratory Depression Associated with Neuraxial Opioid Administration: Anesthesiology 2016; 124: Patient safety council San Diego 2013 Respiratory monitoring of patients outside the ICU tool kit. 16. Capnostream 20 p Operators manual ATTACHMENTS:
14
15
HOSPITAL PROCEDURE Collaborative Practice Committee
 Title: Capnography (ETC0 2 ) Monitoring Code: CPC-2012AUG-1.C.35 HOSPITAL PROCEDURE Collaborative Practice Committee Title of Responsible Party: Director of Medical-Surgical Services Origination Date:
Title: Capnography (ETC0 2 ) Monitoring Code: CPC-2012AUG-1.C.35 HOSPITAL PROCEDURE Collaborative Practice Committee Title of Responsible Party: Director of Medical-Surgical Services Origination Date:
Julie Zimmerman, MSN, RN, CCRN Clinical Nurse Specialist
 Julie Zimmerman, MSN, RN, CCRN Clinical Nurse Specialist Objectives Define capnography vs. end tidal CO2 (EtCO 2 ) Identify what normal vs. abnormal EtCO2 values mean and what to do Understand when to
Julie Zimmerman, MSN, RN, CCRN Clinical Nurse Specialist Objectives Define capnography vs. end tidal CO2 (EtCO 2 ) Identify what normal vs. abnormal EtCO2 values mean and what to do Understand when to
ASPIRUS WAUSAU HOSPITAL, INC. Passion for excellence. Compassion for people. SUBJECT: END TIDAL CARBON DIOXIDE MONITORING (CAPNOGRAPHY)
") Passion for excellence. Compassion for people. P&P REF : NEW 7-2011 ONBASE POLICY ID: 13363 REPLACES: POLICY STATUS : FINAL DOCUMENT TYPE: Policy EFFECTIVE DATE: 4/15/2014 PROPOSED BY: Respiratory Therapy
Passion for excellence. Compassion for people. P&P REF : NEW 7-2011 ONBASE POLICY ID: 13363 REPLACES: POLICY STATUS : FINAL DOCUMENT TYPE: Policy EFFECTIVE DATE: 4/15/2014 PROPOSED BY: Respiratory Therapy
Maria Tracey, Director-Perioperative and Elaine Warren, Directory-Surgery Level. III (Three)
") PAGE 1/6 MANAGEMENT OF ADULT SURGICAL CLIENTS WITH KNOWN OR SUSPECTED OBSTRUCTIVE SLEEP APNEA (OSA) Patient Care Issuing Authority Dr. James Flynn, Clinical Chief Surgical Services (Perioperative) Signed
PAGE 1/6 MANAGEMENT OF ADULT SURGICAL CLIENTS WITH KNOWN OR SUSPECTED OBSTRUCTIVE SLEEP APNEA (OSA) Patient Care Issuing Authority Dr. James Flynn, Clinical Chief Surgical Services (Perioperative) Signed
Capnography: The Most Vital of Vital Signs. Tom Ahrens, PhD, RN, FAAN Research Scientist, Barnes-Jewish Hospital, St. Louis, MO May, 2017
 Capnography: The Most Vital of Vital Signs Tom Ahrens, PhD, RN, FAAN Research Scientist, Barnes-Jewish Hospital, St. Louis, MO May, 2017 Assessing Ventilation and Blood Flow with Capnography Capnography
Capnography: The Most Vital of Vital Signs Tom Ahrens, PhD, RN, FAAN Research Scientist, Barnes-Jewish Hospital, St. Louis, MO May, 2017 Assessing Ventilation and Blood Flow with Capnography Capnography
ETCO2 MONITORING NON-INTUBATED PATIENTS
 Although the standard of care in ETC02 is well established for intubated patients, there has been little emphasis on the use of capnography in nonintubated patients till now. In addition to confirming
Although the standard of care in ETC02 is well established for intubated patients, there has been little emphasis on the use of capnography in nonintubated patients till now. In addition to confirming
Monitoring Patients for Respiratory Depression: outside of the ICU. James D. Harrell, RCP San Diego Patient Safety Council November 14, 2014
 Monitoring Patients for Respiratory Depression: outside of the ICU James D. Harrell, RCP San Diego Patient Safety Council November 14, 2014 1 What is the San Diego Patient Safety Council? SDPSC consists
Monitoring Patients for Respiratory Depression: outside of the ICU James D. Harrell, RCP San Diego Patient Safety Council November 14, 2014 1 What is the San Diego Patient Safety Council? SDPSC consists
Pain Module. Opioid-RelatedRespiratory Depression (ORRD)
") Pain Module Opioid-RelatedRespiratory Depression (ORRD) Characteristics of patients who are at higher risk for Opioid- Related Respiratory Depression (ORRD) Sleep apnea or sleep disorder diagnosis : typically
Pain Module Opioid-RelatedRespiratory Depression (ORRD) Characteristics of patients who are at higher risk for Opioid- Related Respiratory Depression (ORRD) Sleep apnea or sleep disorder diagnosis : typically
By Mark Bachand, RRT-NPS, RPFT. I have no actual or potential conflict of interest in relation to this presentation.
 By Mark Bachand, RRT-NPS, RPFT I have no actual or potential conflict of interest in relation to this presentation. Objectives Review state protocols regarding CPAP use. Touch on the different modes that
By Mark Bachand, RRT-NPS, RPFT I have no actual or potential conflict of interest in relation to this presentation. Objectives Review state protocols regarding CPAP use. Touch on the different modes that
Capnography for Pediatric Procedural Sedation Learning Module Last revised: February 18, 2014
 Capnography for Pediatric Procedural Sedation Learning Module Last revised: February 18, 2014 Capnography 40 Non-invasive device that continually monitors EtCO 2 While pulse oximetry measures oxygen saturation,
Capnography for Pediatric Procedural Sedation Learning Module Last revised: February 18, 2014 Capnography 40 Non-invasive device that continually monitors EtCO 2 While pulse oximetry measures oxygen saturation,
Interfacility Protocol Protocol Title:
 Interfacility Protocol Protocol Title: Mechanical Ventilator Monitoring & Management Original Adoption Date: 05/2009 Past Protocol Updates 05/2009, 12/2013 Date of Most Recent Update: March 23, 2015 Medical
Interfacility Protocol Protocol Title: Mechanical Ventilator Monitoring & Management Original Adoption Date: 05/2009 Past Protocol Updates 05/2009, 12/2013 Date of Most Recent Update: March 23, 2015 Medical
Nihon Kohden America. Capnography Monitoring with the CapONE CO2 Sensor For use with the BSM 2300/4100/5100 and the BSM 6000 Series Bedside Monitors
 Nihon Kohden America Capnography Monitoring with the CapONE CO2 Sensor For use with the BSM 2300/4100/5100 and the BSM 6000 Series Bedside Monitors Self Study Training Packet August 2011 Table of Contents
Nihon Kohden America Capnography Monitoring with the CapONE CO2 Sensor For use with the BSM 2300/4100/5100 and the BSM 6000 Series Bedside Monitors Self Study Training Packet August 2011 Table of Contents
Safe Use of Opioids in Hospitals: Addressing The Joint Commission Sentinel Event Alert
 Safe Use of Opioids in Hospitals: Addressing The Joint Commission Sentinel Event Alert Physician-Patient Alliance for Health & Safety (PPAHS) www.ppahs.org Panelists Michael Wong, JD - Physician-Patient
Safe Use of Opioids in Hospitals: Addressing The Joint Commission Sentinel Event Alert Physician-Patient Alliance for Health & Safety (PPAHS) www.ppahs.org Panelists Michael Wong, JD - Physician-Patient
Spontaneous Breathing Trial and Mechanical Ventilation Weaning Process
 Page 1 of 5 ASSESSMENT INTERVENTION Patient receiving mechanical ventilation Baseline ventilatory mode/ settings RT and RN to assess criteria 1 for SBT Does patient meet criteria? RT to initiate SBT Does
Page 1 of 5 ASSESSMENT INTERVENTION Patient receiving mechanical ventilation Baseline ventilatory mode/ settings RT and RN to assess criteria 1 for SBT Does patient meet criteria? RT to initiate SBT Does
Capnography Connections Guide
 Capnography Connections Guide Patient Monitoring Contents I Section 1: Capnography Introduction...1 I Section 2: Capnography & PCA...3 I Section 3: Capnography & Critical Care...7 I Section 4: Capnography
Capnography Connections Guide Patient Monitoring Contents I Section 1: Capnography Introduction...1 I Section 2: Capnography & PCA...3 I Section 3: Capnography & Critical Care...7 I Section 4: Capnography
Capnography: The Most Vital Sign
 Capnography: The Most Vital Sign Mike McEvoy, PhD, NRP, RN, CCRN Cardiac Surgical ICU RN & Chair Resuscitation Committee Albany Medical Center EMS Coordinator Saratoga County, NY www.mikemcevoy.com CO
Capnography: The Most Vital Sign Mike McEvoy, PhD, NRP, RN, CCRN Cardiac Surgical ICU RN & Chair Resuscitation Committee Albany Medical Center EMS Coordinator Saratoga County, NY www.mikemcevoy.com CO
Identification of patients at risk for Opioid-Induced Respiratory Depression
 Identification of patients at risk for Opioid-Induced Respiratory Depression 2015 Objectives: Discuss the significance of Opioid Induced Respiratory depression (OIRD) Review the patient characteristics/risk
Identification of patients at risk for Opioid-Induced Respiratory Depression 2015 Objectives: Discuss the significance of Opioid Induced Respiratory depression (OIRD) Review the patient characteristics/risk
Capnography. Capnography. Oxygenation. Pulmonary Physiology 4/15/2018. non invasive monitor for ventilation. Edward C. Adlesic, DMD.
 Capnography Edward C. Adlesic, DMD University of Pittsburgh School of Dental Medicine 2018 North Carolina Program Capnography non invasive monitor for ventilation measures end tidal CO2 early detection
Capnography Edward C. Adlesic, DMD University of Pittsburgh School of Dental Medicine 2018 North Carolina Program Capnography non invasive monitor for ventilation measures end tidal CO2 early detection
Capnography (ILS/ALS)
") Capnography (ILS/ALS) Clinical Indications: 1. Capnography shall be used as soon as possible in conjunction with any airway management adjunct, including endotracheal, Blind Insertion Airway Devices (BIAD)
Capnography (ILS/ALS) Clinical Indications: 1. Capnography shall be used as soon as possible in conjunction with any airway management adjunct, including endotracheal, Blind Insertion Airway Devices (BIAD)
A Business & Clinical Case for Continuous Surveillance
 A Business & Clinical Case for Continuous Surveillance Session 209, February 14, 2019 Leah Baron, MD, Anesthesiologist John Zaleski, PhD, CAP, CPHIMS, Chief Analytics Officer, Bernoulli Health 1 Conflict
A Business & Clinical Case for Continuous Surveillance Session 209, February 14, 2019 Leah Baron, MD, Anesthesiologist John Zaleski, PhD, CAP, CPHIMS, Chief Analytics Officer, Bernoulli Health 1 Conflict
Conflict of Interest Disclosure Authors Conflicts of Interest:
 MONITORING FOR OPIOID- INDUCED RESPIRATORY DEPRESSION: REVIEW OF NEW EVIDENCE Carla R. Jungquist, ANP-BC, PhD Assistant Professor School of Nursing 1 Conflict of Interest Disclosure Authors Conflicts of
MONITORING FOR OPIOID- INDUCED RESPIRATORY DEPRESSION: REVIEW OF NEW EVIDENCE Carla R. Jungquist, ANP-BC, PhD Assistant Professor School of Nursing 1 Conflict of Interest Disclosure Authors Conflicts of
8/26/2011. Disclosures. Objectives. None
 Ann Holmes RN, MS Director Munson Healthcare Traverse City, MI Lisa Biehl, RN, MSN Patient Care Coordinator Munson Healthcare Traverse City, MI Disclosures None Objectives Identify factors that place patients
Ann Holmes RN, MS Director Munson Healthcare Traverse City, MI Lisa Biehl, RN, MSN Patient Care Coordinator Munson Healthcare Traverse City, MI Disclosures None Objectives Identify factors that place patients
WRHA Surgery Program. Obstructive Sleep Apnea (OSA)
") WRHA Surgery Program Obstructive Sleep Apnea (OSA) March 2010 Prepared by WRHA Surgery & Anesthesiology Programs Objectives 1. Define obstructive sleep apnea (OSA). 2. Purpose of the guidelines. 3. Identify
WRHA Surgery Program Obstructive Sleep Apnea (OSA) March 2010 Prepared by WRHA Surgery & Anesthesiology Programs Objectives 1. Define obstructive sleep apnea (OSA). 2. Purpose of the guidelines. 3. Identify
Association for Radiologic & Imaging Nursing
 Overview: Radiology and Imaging Nurses provide procedural sedation to a variety of patients. The administration of procedural sedation in the interventional radiology and diagnostic imaging suites presents
Overview: Radiology and Imaging Nurses provide procedural sedation to a variety of patients. The administration of procedural sedation in the interventional radiology and diagnostic imaging suites presents
CAPNOGRAPHY. 1.1 To set forth the policy and procedure for performing continuous end-tidal waveform capnography.
 OFFICE OF MEDICAL AFFAIRS DIRECTIVE 2009-02 CAPNOGRAPHY 1. PURPOSE 1.1 To set forth the policy and procedure for performing continuous end-tidal waveform capnography. 2. SCOPE 2.1 This procedure applies
OFFICE OF MEDICAL AFFAIRS DIRECTIVE 2009-02 CAPNOGRAPHY 1. PURPOSE 1.1 To set forth the policy and procedure for performing continuous end-tidal waveform capnography. 2. SCOPE 2.1 This procedure applies
Optimize vent weaning and SBT outcomes. Identify underlying causes for SBT failures. Role SBT and weaning protocol have in respiratory care
 Optimize vent weaning and SBT outcomes Identify underlying causes for SBT failures Role SBT and weaning protocol have in respiratory care Lower risk of developing complications Lower risk of VAP, other
Optimize vent weaning and SBT outcomes Identify underlying causes for SBT failures Role SBT and weaning protocol have in respiratory care Lower risk of developing complications Lower risk of VAP, other
POLICY. Number: Title: APPLICATION OF NON INVASIVE VENTILATION FOR ACUTE RESPIRATORY FAILURE. Authorization
 POLICY Number: 7311-60-024 Title: APPLICATION OF NON INVASIVE VENTILATION FOR ACUTE RESPIRATORY FAILURE Authorization [ ] President and CEO [ x ] Vice President, Finance and Corporate Services Source:
POLICY Number: 7311-60-024 Title: APPLICATION OF NON INVASIVE VENTILATION FOR ACUTE RESPIRATORY FAILURE Authorization [ ] President and CEO [ x ] Vice President, Finance and Corporate Services Source:
End Tidal CO2 Not All Its Cracked Up To Be The Limitations of PETCO2 In Sedation Analgesia
 End Tidal CO2 Not All Its Cracked Up To Be The Limitations of PETCO2 In Sedation Analgesia Tidal Volume Noninvasive monitoring of ventilation and exhaled carbon dioxide of a patient End Tidal CO2 Produces
End Tidal CO2 Not All Its Cracked Up To Be The Limitations of PETCO2 In Sedation Analgesia Tidal Volume Noninvasive monitoring of ventilation and exhaled carbon dioxide of a patient End Tidal CO2 Produces
Resuscitation Patient Management Tool May 2015 MET Event
 OPTIONAL: Local Event ID: Date/Time MET was activated: Time Not Documented MET 2.1 Pre-Event Pre-Event Tab Was patient discharged from an Intensive Care Unit (ICU) at any point during this admission and
OPTIONAL: Local Event ID: Date/Time MET was activated: Time Not Documented MET 2.1 Pre-Event Pre-Event Tab Was patient discharged from an Intensive Care Unit (ICU) at any point during this admission and
Capnography 101. James A Temple BA, NRP, CCP
 Capnography 101 James A Temple BA, NRP, CCP Expected Outcomes 1. Gain a working knowledge of the physiology and science behind End-Tidal CO2. 2.Relate End-Tidal CO2 to ventilation, perfusion, and metabolism.
Capnography 101 James A Temple BA, NRP, CCP Expected Outcomes 1. Gain a working knowledge of the physiology and science behind End-Tidal CO2. 2.Relate End-Tidal CO2 to ventilation, perfusion, and metabolism.
How it Works. CO 2 is the smoke from the flames of metabolism 10/21/18. -Ray Fowler, MD. Metabolism creates ETC0 2 for excretion
 CO 2 is the smoke from the flames of metabolism -Ray Fowler, MD How it Works Metabolism creates ETC0 2 for excretion ETC02 and Oxygen are exchanged at the alveolar level in the lungs with each breath.
CO 2 is the smoke from the flames of metabolism -Ray Fowler, MD How it Works Metabolism creates ETC0 2 for excretion ETC02 and Oxygen are exchanged at the alveolar level in the lungs with each breath.
June 2011 Bill Streett-Training Section Chief
 Capnography 102 June 2011 Bill Streett-Training Section Chief Terminology Capnography: the measurement and numerical display of end-tidal CO2 concentration, at the patient s airway, during a respiratory
Capnography 102 June 2011 Bill Streett-Training Section Chief Terminology Capnography: the measurement and numerical display of end-tidal CO2 concentration, at the patient s airway, during a respiratory
3/30/12. Luke J. Gasowski BS, BSRT, NREMT-P, FP-C, CCP-C, RRT-NPS
 Luke J. Gasowski BS, BSRT, NREMT-P, FP-C, CCP-C, RRT-NPS 1) Define and describe ETCO 2 2) Explain methods of measuring ETCO 2 3) Describe various clinical applications of ETCO 2 4) Describe the relationship
Luke J. Gasowski BS, BSRT, NREMT-P, FP-C, CCP-C, RRT-NPS 1) Define and describe ETCO 2 2) Explain methods of measuring ETCO 2 3) Describe various clinical applications of ETCO 2 4) Describe the relationship
POLICY All patients will be assessed for risk factors associated with OSA prior to any surgical procedures.
 Revised Date: Page: 1 of 7 SCOPE All Pre-Admission Testing (PAT) and Same Day Surgery (SDS) nurses at HRMC. PURPOSE The purpose of this policy is to provide guidelines for identifying surgical patients
Revised Date: Page: 1 of 7 SCOPE All Pre-Admission Testing (PAT) and Same Day Surgery (SDS) nurses at HRMC. PURPOSE The purpose of this policy is to provide guidelines for identifying surgical patients
NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP)
") Introduction NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP) Noninvasive ventilation (NIV) is a method of delivering oxygen by positive pressure mask that allows for the prevention or postponement of invasive
Introduction NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP) Noninvasive ventilation (NIV) is a method of delivering oxygen by positive pressure mask that allows for the prevention or postponement of invasive
Sleep Apnea and ifficulty in Extubation. Jean Louis BOURGAIN May 15, 2016
 Sleep Apnea and ifficulty in Extubation Jean Louis BOURGAIN May 15, 2016 Introduction Repetitive collapse of the upper airway > sleep fragmentation, > hypoxemia, hypercapnia, > marked variations in intrathoracic
Sleep Apnea and ifficulty in Extubation Jean Louis BOURGAIN May 15, 2016 Introduction Repetitive collapse of the upper airway > sleep fragmentation, > hypoxemia, hypercapnia, > marked variations in intrathoracic
Don t let your patients turn blue! Isn t it about time you used etco 2?
 Don t let your patients turn blue! Isn t it about time you used etco 2? American Association of Critical Care Nurses National Teaching Institute Expo Ed 2013 Susan Thibeault MS, CRNA, APRN, CCRN, EMT-P
Don t let your patients turn blue! Isn t it about time you used etco 2? American Association of Critical Care Nurses National Teaching Institute Expo Ed 2013 Susan Thibeault MS, CRNA, APRN, CCRN, EMT-P
CAPNOGRAPHY in the SLEEP CENTER Julie DeWitte, RCP, RPSGT, RST Assistant Department Administrator Kaiser Permanente Fontana Sleep Center
 FOCUS Fall 2018 CAPNOGRAPHY in the SLEEP CENTER Julie DeWitte, RCP, RPSGT, RST Assistant Department Administrator Kaiser Permanente Fontana Sleep Center 1 Learning Objectives The future of in laboratory
FOCUS Fall 2018 CAPNOGRAPHY in the SLEEP CENTER Julie DeWitte, RCP, RPSGT, RST Assistant Department Administrator Kaiser Permanente Fontana Sleep Center 1 Learning Objectives The future of in laboratory
Overcoming Opioid-Induced Oversedation: More Than Meets the Eye
 Overcoming Opioid-Induced Oversedation: More Than Meets the Eye ANCC National Magnet Conference 2013 Jeannine M. Brant, PhD, APRN, AOCN Lisa Peterson, RN-BC, BSN Health Care, Education and Research www.billingsclinic.com
Overcoming Opioid-Induced Oversedation: More Than Meets the Eye ANCC National Magnet Conference 2013 Jeannine M. Brant, PhD, APRN, AOCN Lisa Peterson, RN-BC, BSN Health Care, Education and Research www.billingsclinic.com
Transcutaneous Monitoring and Case Studies
 Transcutaneous Monitoring and Case Studies Objectives General concept, applications and principles of operation Role of TCM in clinical settings Role of TCM in home care settings Need for continuous TCM
Transcutaneous Monitoring and Case Studies Objectives General concept, applications and principles of operation Role of TCM in clinical settings Role of TCM in home care settings Need for continuous TCM
Bi-Level Therapy: Boosting Comfort & Compliance in Apnea Patients
 Bi-Level Therapy: Boosting Comfort & Compliance in Apnea Patients Objectives Describe nocturnal ventilation characteristics that may indicate underlying conditions and benefits of bilevel therapy for specific
Bi-Level Therapy: Boosting Comfort & Compliance in Apnea Patients Objectives Describe nocturnal ventilation characteristics that may indicate underlying conditions and benefits of bilevel therapy for specific
Non-invasive Ventilation protocol For COPD
 NHS LANARKSHIRE MONKLANDS HOSPITAL Non-invasive Ventilation protocol For COPD April 2017 S Baird Review Date: Oct 2019 Approved by Medical Directorate Indications for Non-Invasive Ventilation (NIV) NIV
NHS LANARKSHIRE MONKLANDS HOSPITAL Non-invasive Ventilation protocol For COPD April 2017 S Baird Review Date: Oct 2019 Approved by Medical Directorate Indications for Non-Invasive Ventilation (NIV) NIV
Responding to The Joint Commission Alert on Safe Use of Opioids in Hospitals
 Responding to The Joint Commission Alert on Safe Use of Opioids in Hospitals Suzanne A Nesbit, PharmD, CPE Clinical Pharmacy Specialist, Pain Management The Johns Hopkins Hospital Objectives and Disclosures
Responding to The Joint Commission Alert on Safe Use of Opioids in Hospitals Suzanne A Nesbit, PharmD, CPE Clinical Pharmacy Specialist, Pain Management The Johns Hopkins Hospital Objectives and Disclosures
Disclosures. Objectives. OSA Death and Near Miss Registry The path to creation.
 OSA Death and Near Miss Registry The path to creation. October 23, 2015 Norman Bolden, M.D. Vice-Chairman, Department of Anesthesiology Associate Professor, Case Western Reserve University n None Disclosures
OSA Death and Near Miss Registry The path to creation. October 23, 2015 Norman Bolden, M.D. Vice-Chairman, Department of Anesthesiology Associate Professor, Case Western Reserve University n None Disclosures
IFT1 Interfacility Transfer of STEMI Patients. IFT2 Interfacility Transfer of Intubated Patients. IFT3 Interfacility Transfer of Stroke Patients
 IFT1 Interfacility Transfer of STEMI Patients IFT2 Interfacility Transfer of Intubated Patients IFT3 Interfacility Transfer of Stroke Patients Interfacility Transfer Guidelines IFT 1 TRANSFER INTERFACILITY
IFT1 Interfacility Transfer of STEMI Patients IFT2 Interfacility Transfer of Intubated Patients IFT3 Interfacility Transfer of Stroke Patients Interfacility Transfer Guidelines IFT 1 TRANSFER INTERFACILITY
10/17/2016 OXYGEN DELIVERY: INDICATIONS AND USE OF EQUIPMENT COURSE OBJECTIVES COMMON CAUSES OF RESPIRATORY FAILURE
 OXYGEN DELIVERY: INDICATIONS AND USE OF EQUIPMENT J U L I E Z I M M E R M A N, R N, M S N C L I N I C A L N U R S E S P E C I A L I S T E L O I S A C U T L E R, R R T, B S R C C L I N I C A L / E D U C
OXYGEN DELIVERY: INDICATIONS AND USE OF EQUIPMENT J U L I E Z I M M E R M A N, R N, M S N C L I N I C A L N U R S E S P E C I A L I S T E L O I S A C U T L E R, R R T, B S R C C L I N I C A L / E D U C
Non-Invasive Assessment of Respiratory Function. Chapter 11
 Non-Invasive Assessment of Respiratory Function Chapter 11 Pulse Oximetry Laboratory measurements of ABG s are the gold standard for measuring levels of hypoxemia, however since these are performed intermittently
Non-Invasive Assessment of Respiratory Function Chapter 11 Pulse Oximetry Laboratory measurements of ABG s are the gold standard for measuring levels of hypoxemia, however since these are performed intermittently
Interesting Capnography Cases
 Interesting Capnography Cases Mike McEvoy, PhD, NRP, RN, CCRN Cardiac Surgical ICU RN & Chair Resuscitation Committee Albany Medical Center EMS Coordinator Saratoga County, NY www.mikemcevoy.com Outline
Interesting Capnography Cases Mike McEvoy, PhD, NRP, RN, CCRN Cardiac Surgical ICU RN & Chair Resuscitation Committee Albany Medical Center EMS Coordinator Saratoga County, NY www.mikemcevoy.com Outline
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES
 DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
Transcutaneous CO2 Monitoring: Alerting the Anesthesia Provider to Impending Respiratory Depression
 Transcutaneous CO2 Monitoring: Alerting the Anesthesia Provider to Impending Respiratory Depression JEANETTE R BAUCHAT, MD, MS ASSOCIATE PROFESSOR OF ANESTHESIOLOGY DIVISION CHIEF, OBSTETRIC ANESTHESIOLOGY
Transcutaneous CO2 Monitoring: Alerting the Anesthesia Provider to Impending Respiratory Depression JEANETTE R BAUCHAT, MD, MS ASSOCIATE PROFESSOR OF ANESTHESIOLOGY DIVISION CHIEF, OBSTETRIC ANESTHESIOLOGY
Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor
 Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
Guidelines Administrative Practice X Clinical Practice Professional Practice
 Guidelines Administrative Practice X Clinical Practice Professional Practice End Tidal CO 2 (EtCO2) Monitoring Using the Zoll Monitor/Defibrillator Page 1 of 4 Scope: Outcome: Respiratory Therapists (RT),
Guidelines Administrative Practice X Clinical Practice Professional Practice End Tidal CO 2 (EtCO2) Monitoring Using the Zoll Monitor/Defibrillator Page 1 of 4 Scope: Outcome: Respiratory Therapists (RT),
The case for capnography in patients receiving opioids
 The case for capnography in patients receiving opioids Learn why capnography is essential for detecting respiratory depression. By Heather Carlisle, PhD, DNP, FNP-BC, RN-BC IT S YOUR WORST NIGHTMARE: At
The case for capnography in patients receiving opioids Learn why capnography is essential for detecting respiratory depression. By Heather Carlisle, PhD, DNP, FNP-BC, RN-BC IT S YOUR WORST NIGHTMARE: At
2 hospital system, tertiary care, community, referral centers
 2 hospital system, tertiary care, community, referral centers! Two of the oldest continuously operating hospitals in the nation! Largest healthcare system in SE Georgia; 675 beds! Approximately 25,000
2 hospital system, tertiary care, community, referral centers! Two of the oldest continuously operating hospitals in the nation! Largest healthcare system in SE Georgia; 675 beds! Approximately 25,000
Conflict of Interest Disclosure
 Monitoring for Opioid Induced Respiratory Depression: Paradigm Shift from Threshold Monitoring to Trend Monitoring Carla R. Jungquist, ANP BC, PhD Assistant Professor University at Buffalo J. Paul Curry,
Monitoring for Opioid Induced Respiratory Depression: Paradigm Shift from Threshold Monitoring to Trend Monitoring Carla R. Jungquist, ANP BC, PhD Assistant Professor University at Buffalo J. Paul Curry,
James Paul MD MSc FRCPC
 SCIENCE VIGILANCE COMPASSION VIGILANCE Study: VItal sign monitoring with continuous pulse oximetry And wireless clinician notification after surgery James Paul MD MSc FRCPC Outline Background Rationale
SCIENCE VIGILANCE COMPASSION VIGILANCE Study: VItal sign monitoring with continuous pulse oximetry And wireless clinician notification after surgery James Paul MD MSc FRCPC Outline Background Rationale
Critical Review Form Therapy
 Critical Review Form Therapy Does End-tidal Carbon Dioxide Monitoring Detect Respiratory Events Prior to Current Sedation Monitoring Practices, Acad Emerg Med 2006; 13:500-504 Objective: To determine the
Critical Review Form Therapy Does End-tidal Carbon Dioxide Monitoring Detect Respiratory Events Prior to Current Sedation Monitoring Practices, Acad Emerg Med 2006; 13:500-504 Objective: To determine the
Emergency Department Guideline. Procedural Sedation and Analgesia Policy for the Registered Nurse
 Emergency Department Guideline Purpose: To ensure safe, consistent patient monitoring and documentation standards when procedure related sedation and analgesia is indicated. Definitions: Minimal Sedation
Emergency Department Guideline Purpose: To ensure safe, consistent patient monitoring and documentation standards when procedure related sedation and analgesia is indicated. Definitions: Minimal Sedation
County of Santa Clara Emergency Medical Services System
 County of Santa Clara Emergency Medical Services System Policy #700-M12: Continuous Positive Airway Pressure CONTINUOUS POSITIVE AIRWAY PRESSURE Effective: February 8, 2013TBD Replaces: NewFebruary 8,
County of Santa Clara Emergency Medical Services System Policy #700-M12: Continuous Positive Airway Pressure CONTINUOUS POSITIVE AIRWAY PRESSURE Effective: February 8, 2013TBD Replaces: NewFebruary 8,
Identification and Treatment of the Patient with Sleep Related Hypoventilation
 Identification and Treatment of the Patient with Sleep Related Hypoventilation Hillary Loomis-King, MD Pulmonary and Critical Care of NW MI Munson Sleep Disorders Center X Conflict of Interest Disclosures
Identification and Treatment of the Patient with Sleep Related Hypoventilation Hillary Loomis-King, MD Pulmonary and Critical Care of NW MI Munson Sleep Disorders Center X Conflict of Interest Disclosures
What is the next best step?
 Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
Capnography: Creating a Culture of Safety! An Interview With Peggy Lange, RT!
 Capnography: Creating a Culture of Safety An Interview With Peggy Lange, RT Pat Iyer Hi, this is a podcast from the Physician-Patient Alliance for Health & Safety. The podcast that we're presenting today
Capnography: Creating a Culture of Safety An Interview With Peggy Lange, RT Pat Iyer Hi, this is a podcast from the Physician-Patient Alliance for Health & Safety. The podcast that we're presenting today
BiLevel Pressure Device
 PROCEDURE - Page 1 of 7 Purpose Scope Classes/ Goals Define indications and care settings for acute and chronic initiation of Noninvasive Positive Pressure Ventilation. Identify the role of Respiratory
PROCEDURE - Page 1 of 7 Purpose Scope Classes/ Goals Define indications and care settings for acute and chronic initiation of Noninvasive Positive Pressure Ventilation. Identify the role of Respiratory
NON INVASIVE LIFE SAVERS. Non Invasive Ventilation (NIV)
") Table 1. NIV: Mechanisms Of Action Decreases work of breathing Increases functional residual capacity Recruits collapsed alveoli Improves respiratory gas exchange Reverses hypoventilation Maintains upper
Table 1. NIV: Mechanisms Of Action Decreases work of breathing Increases functional residual capacity Recruits collapsed alveoli Improves respiratory gas exchange Reverses hypoventilation Maintains upper
Respiratory Depression and Considerations for Monitoring Following Ophthalmologic Surgery
 Respiratory Depression and Considerations for Monitoring Following Ophthalmologic Surgery Athir Morad, M.D. Division of Neurocritical care Departments of Anesthesiology/ Critical Care Medicine and Neurology
Respiratory Depression and Considerations for Monitoring Following Ophthalmologic Surgery Athir Morad, M.D. Division of Neurocritical care Departments of Anesthesiology/ Critical Care Medicine and Neurology
Reducing Adverse Drug Events Related to Opioids: An Interview with Thomas W. Frederickson MD, FACP, SFHM, MBA
 Reducing Adverse Drug Events Related to Opioids: An Interview with Thomas W. Frederickson MD, FACP, SFHM, MBA The following is a transcript of part two of an interview with Dr. Thomas Frederickson. For
Reducing Adverse Drug Events Related to Opioids: An Interview with Thomas W. Frederickson MD, FACP, SFHM, MBA The following is a transcript of part two of an interview with Dr. Thomas Frederickson. For
11/20/2015. Beyond CPAP. No relevant financial conflicts of interest. Kristie R Ross, M.D. November 12, Describe advanced ventilation options
 Beyond CPAP Kristie R Ross, M.D. November 12, 2015 No relevant financial conflicts of interest Sponsored by The Warren Alpert Medical School of Brown University Describe advanced ventilation options Compare
Beyond CPAP Kristie R Ross, M.D. November 12, 2015 No relevant financial conflicts of interest Sponsored by The Warren Alpert Medical School of Brown University Describe advanced ventilation options Compare
(To be filled by the treating physician)
") CERTIFICATE OF MEDICAL NECESSITY TO BE ISSUED TO CGHS BENEFICIAREIS BEING PRESCRIBED BILEVEL CONTINUOUS POSITIVE AIRWAY PRESSURE (BI-LEVEL CPAP) / BI-LEVEL VENTILATORY SUPPORT SYSTEM Certification Type
CERTIFICATE OF MEDICAL NECESSITY TO BE ISSUED TO CGHS BENEFICIAREIS BEING PRESCRIBED BILEVEL CONTINUOUS POSITIVE AIRWAY PRESSURE (BI-LEVEL CPAP) / BI-LEVEL VENTILATORY SUPPORT SYSTEM Certification Type
I. Subject. Moderate Sedation
 I. Subject II. III. Moderate Sedation Purpose To establish criteria for the monitoring and management of patients receiving moderate throughout the hospital Definitions A. Definitions of three levels of
I. Subject II. III. Moderate Sedation Purpose To establish criteria for the monitoring and management of patients receiving moderate throughout the hospital Definitions A. Definitions of three levels of
Date 8/95; Rev.12/97; 7/98; 2/99; 5/01, 3/03, 9/03; 5/04; 8/05; 3/07; 10/08; 10/09; 10/10 Manual of Administrative Policy Source Sedation Committee
 Code No. 711 Section Subject Moderate Sedation (formerly termed Conscious Sedation ) Date 8/95; Rev.12/97; 7/98; 2/99; 5/01, 3/03, 9/03; 5/04; 8/05; 3/07; 10/08; Manual of Administrative Policy Source
Code No. 711 Section Subject Moderate Sedation (formerly termed Conscious Sedation ) Date 8/95; Rev.12/97; 7/98; 2/99; 5/01, 3/03, 9/03; 5/04; 8/05; 3/07; 10/08; Manual of Administrative Policy Source
Anaesthetic considerations for laparoscopic surgery in canines
 Vet Times The website for the veterinary profession https://www.vettimes.co.uk Anaesthetic considerations for laparoscopic surgery in canines Author : Chris Miller Categories : Canine, Companion animal,
Vet Times The website for the veterinary profession https://www.vettimes.co.uk Anaesthetic considerations for laparoscopic surgery in canines Author : Chris Miller Categories : Canine, Companion animal,
Hypoventilation? Obstructive Sleep Apnea? Different Tests, Different Treatment
 Hypoventilation? Obstructive Sleep Apnea? Different Tests, Different Treatment Judith R. Fischer, MSLS, Editor, Ventilator-Assisted Living (fischer.judith@sbcglobal.net) Thanks to Josh Benditt, MD, University
Hypoventilation? Obstructive Sleep Apnea? Different Tests, Different Treatment Judith R. Fischer, MSLS, Editor, Ventilator-Assisted Living (fischer.judith@sbcglobal.net) Thanks to Josh Benditt, MD, University
Respiratory Rate. Disclosure: Research grants and honoraria from Masimo Corp
 Respiratory Rate Acoustic Monitoring Michael Ramsay MD Chairman, Department of Anesthesia Baylor University Medical Center President, Baylor Research Institute Professor, Texas A&M Health Science Center
Respiratory Rate Acoustic Monitoring Michael Ramsay MD Chairman, Department of Anesthesia Baylor University Medical Center President, Baylor Research Institute Professor, Texas A&M Health Science Center
7 Initial Ventilator Settings, ~05
 Abbreviations (inside front cover and back cover) PART 1 Basic Concepts and Core Knowledge in Mechanical -- -- -- -- 1 Oxygenation and Acid-Base Evaluation, 1 Review 01Arterial Blood Gases, 2 Evaluating
Abbreviations (inside front cover and back cover) PART 1 Basic Concepts and Core Knowledge in Mechanical -- -- -- -- 1 Oxygenation and Acid-Base Evaluation, 1 Review 01Arterial Blood Gases, 2 Evaluating
Respiratory Depression in the Early Postoperative Period. Toby N Weingarten, MD Mayo Clinic Professor Anesthesiology
 Respiratory Depression in the Early Postoperative Period Toby N Weingarten, MD Mayo Clinic Professor Anesthesiology Conflicts of Interest Medtronic Chair of CEC Committee for PRODIGY Trial Merck Investigator
Respiratory Depression in the Early Postoperative Period Toby N Weingarten, MD Mayo Clinic Professor Anesthesiology Conflicts of Interest Medtronic Chair of CEC Committee for PRODIGY Trial Merck Investigator
Overview. Introduction. Opioids and Respiratory Monitoring Technology WHITE PAPER
 WHITE PAPER Opioids and Respiratory Monitoring Technology JW Beard, MD, MBA Overview Opioids play a central role in postoperative multimodal analgesic therapy but are considered high-alert medications
WHITE PAPER Opioids and Respiratory Monitoring Technology JW Beard, MD, MBA Overview Opioids play a central role in postoperative multimodal analgesic therapy but are considered high-alert medications
Noninvasive Mechanical Ventilation in Children ศ.พญ.อร ณวรรณ พฤทธ พ นธ หน วยโรคระบบหายใจเด ก ภาคว ชาก มารเวชศาสตร คณะแพทยศาสตร โรงพยาบาลรามาธ บด
 Noninvasive Mechanical Ventilation in Children ศ.พญ.อร ณวรรณ พฤทธ พ นธ หน วยโรคระบบหายใจเด ก ภาคว ชาก มารเวชศาสตร คณะแพทยศาสตร โรงพยาบาลรามาธ บด Noninvasive Mechanical Ventilation Provide support without
Noninvasive Mechanical Ventilation in Children ศ.พญ.อร ณวรรณ พฤทธ พ นธ หน วยโรคระบบหายใจเด ก ภาคว ชาก มารเวชศาสตร คณะแพทยศาสตร โรงพยาบาลรามาธ บด Noninvasive Mechanical Ventilation Provide support without
Addendum D. Procedural Sedation Test MERCY MEDICAL CENTER- SIOUX CITY. Procedural Sedation Questions
 Addendum D. Procedural Sedation Test MERCY MEDICAL CENTER- SIOUX CITY Procedural Sedation Questions Individuals applying for moderate sedation privileges must achieve a score of 80%. PRACTITIONER NAME
Addendum D. Procedural Sedation Test MERCY MEDICAL CENTER- SIOUX CITY Procedural Sedation Questions Individuals applying for moderate sedation privileges must achieve a score of 80%. PRACTITIONER NAME
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES
 DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
OXYGEN USE IN PHYSICAL THERAPY PRACTICE. Rebecca H. Crouch, PT,DPT,MS,CCS,FAACVPR
 OXYGEN USE IN PHYSICAL THERAPY PRACTICE Rebecca H. Crouch, PT,DPT,MS,CCS,FAACVPR Supplemental Oxygen Advantages British Medical Research Council Clinical Trial Improved survival using oxygen 15 hrs/day
OXYGEN USE IN PHYSICAL THERAPY PRACTICE Rebecca H. Crouch, PT,DPT,MS,CCS,FAACVPR Supplemental Oxygen Advantages British Medical Research Council Clinical Trial Improved survival using oxygen 15 hrs/day
Foundation in Critical Care Nursing. Airway / Respiratory / Workbook
 Foundation in Critical Care Nursing Airway / Respiratory / Workbook Airway Anatomy: Please label the following: Tongue Larynx Epiglottis Pharynx Trachea Vertebrae Oesophagus Where is the ET (endotracheal)
Foundation in Critical Care Nursing Airway / Respiratory / Workbook Airway Anatomy: Please label the following: Tongue Larynx Epiglottis Pharynx Trachea Vertebrae Oesophagus Where is the ET (endotracheal)
Correlation Between Partial Pressure of Arterial Carbon Dioxide and End Tidal Carbon Dioxide in Patients with Severe Alcohol Withdrawal
 ORIGINAL RESEARCH The Ochsner Journal 15:418 422, 2015 Ó Academic Division of Ochsner Clinic Foundation Correlation Between Partial Pressure of Arterial Carbon Dioxide and End Tidal Carbon Dioxide in Patients
ORIGINAL RESEARCH The Ochsner Journal 15:418 422, 2015 Ó Academic Division of Ochsner Clinic Foundation Correlation Between Partial Pressure of Arterial Carbon Dioxide and End Tidal Carbon Dioxide in Patients
Opioids and Respiratory Depression
 Opioids and Respiratory Depression Clinical Committee Society of Anesthesia and Sleep Medicine https://commons.wikimedia.org/wiki/file:mu_opioid_receptor.svg Introduction Opioid-induced respiratory depression
Opioids and Respiratory Depression Clinical Committee Society of Anesthesia and Sleep Medicine https://commons.wikimedia.org/wiki/file:mu_opioid_receptor.svg Introduction Opioid-induced respiratory depression
Dr Alireza Yarahmadi and Dr Arvind Perathur Mercy Medical Center - Winter Retreat Des Moines February 2012
 Dr Alireza Yarahmadi and Dr Arvind Perathur Mercy Medical Center - Winter Retreat Des Moines February 2012 Why screen of OSA prior to surgery? What factors increase the risk? When due to anticipate problems?
Dr Alireza Yarahmadi and Dr Arvind Perathur Mercy Medical Center - Winter Retreat Des Moines February 2012 Why screen of OSA prior to surgery? What factors increase the risk? When due to anticipate problems?
Airway Clearance Devices
 Print Page 1 of 11 Wisconsin.gov home state agencies subject directory department of health services Search Welcome» August 2, 2018 5:18 PM Program Name: BadgerCare Plus and Medicaid Handbook Area: Durable
Print Page 1 of 11 Wisconsin.gov home state agencies subject directory department of health services Search Welcome» August 2, 2018 5:18 PM Program Name: BadgerCare Plus and Medicaid Handbook Area: Durable
Objectives. Health care significance of ARF 9/10/15 TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION
 TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION Louisa Chika Ikpeama, DNP, CCRN, ACNP-BC Objectives Identify health care significance of acute respiratory
TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION Louisa Chika Ikpeama, DNP, CCRN, ACNP-BC Objectives Identify health care significance of acute respiratory
1/27/2017 RECOGNITION AND MANAGEMENT OF OBSTRUCTIVE SLEEP APNEA: STRATEGIES TO PREVENT POST-OPERATIVE RESPIRATORY FAILURE DEFINITION PATHOPHYSIOLOGY
 RECOGNITION AND MANAGEMENT OF OBSTRUCTIVE SLEEP APNEA: STRATEGIES TO PREVENT POST-OPERATIVE RESPIRATORY FAILURE Peggy Hollis MSN, RN, ACNS-BC March 9, 2017 DEFINITION Obstructive sleep apnea is a disorder
RECOGNITION AND MANAGEMENT OF OBSTRUCTIVE SLEEP APNEA: STRATEGIES TO PREVENT POST-OPERATIVE RESPIRATORY FAILURE Peggy Hollis MSN, RN, ACNS-BC March 9, 2017 DEFINITION Obstructive sleep apnea is a disorder
NON-INVASIVE VENTILATION. Lijun Ding 23 Jan 2018
 NON-INVASIVE VENTILATION Lijun Ding 23 Jan 2018 Learning objectives What is NIV The difference between CPAP and BiPAP The indication of the use of NIV Complication of NIV application Patient monitoring
NON-INVASIVE VENTILATION Lijun Ding 23 Jan 2018 Learning objectives What is NIV The difference between CPAP and BiPAP The indication of the use of NIV Complication of NIV application Patient monitoring
STATE OF OKLAHOMA 2014 EMERGENCY MEDICAL SERVICES PROTOCOLS
 3K NON-INVASIVE POSITIVE PRESSURE VENTILATION (NIPPV) ADULT EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC Indications: 1. Dyspnea Uncertain Etiology Adult. 2. Dyspnea Asthma Adult. 3. Dyspnea Chronic
3K NON-INVASIVE POSITIVE PRESSURE VENTILATION (NIPPV) ADULT EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC Indications: 1. Dyspnea Uncertain Etiology Adult. 2. Dyspnea Asthma Adult. 3. Dyspnea Chronic
OSA and COPD: What happens when the two OVERLAP?
 2011 ISRC Seminar 1 COPD OSA OSA and COPD: What happens when the two OVERLAP? Overlap Syndrome 1 OSA and COPD: What happens when the two OVERLAP? ResMed 10 JAN Global leaders in sleep and respiratory medicine
2011 ISRC Seminar 1 COPD OSA OSA and COPD: What happens when the two OVERLAP? Overlap Syndrome 1 OSA and COPD: What happens when the two OVERLAP? ResMed 10 JAN Global leaders in sleep and respiratory medicine
MASTER SYLLABUS
 MASTER SYLLABUS 2018-2019 A. Academic Division: Health Science B. Discipline: Respiratory Care C. Course Number and Title: RESP 2490 Practicum IV D. Course Coordinator: Tricia Winters, BBA, RRT, RCP Assistant
MASTER SYLLABUS 2018-2019 A. Academic Division: Health Science B. Discipline: Respiratory Care C. Course Number and Title: RESP 2490 Practicum IV D. Course Coordinator: Tricia Winters, BBA, RRT, RCP Assistant
Bergen Community College Division of Health Professions Department of Respiratory Care Fundamentals of Respiratory Critical Care
 Bergen Community College Division of Health Professions Department of Respiratory Care Fundamentals of Respiratory Critical Care Date Revised: January 2015 Course Description Student Learning Objectives:
Bergen Community College Division of Health Professions Department of Respiratory Care Fundamentals of Respiratory Critical Care Date Revised: January 2015 Course Description Student Learning Objectives:
NAVIGATING THE HEALTHCARE LANDSCAPE TOGETHER JENNIFER FRUITTICHER, RN CLINICAL PRODUCT SPECIALIST
 NAVIGATING THE HEALTHCARE LANDSCAPE TOGETHER JENNIFER FRUITTICHER, RN CLINICAL PRODUCT SPECIALIST PRESENTATION OBJECTIVES: Provide a better understanding of Capnography vs. Pulse Oximetry Define Respiratory
NAVIGATING THE HEALTHCARE LANDSCAPE TOGETHER JENNIFER FRUITTICHER, RN CLINICAL PRODUCT SPECIALIST PRESENTATION OBJECTIVES: Provide a better understanding of Capnography vs. Pulse Oximetry Define Respiratory
Obstructive Sleep Apnea and the use of Capnometry
 Obstructive Sleep Apnea and the use of Capnometry 1230-1330 Obstructive Sleep Apnea and Use of End Tidal CO₂ in the PACU Objectives: Define Obstructive Sleep Apnea (OSA) Define End Tidal CO₂. Describe
Obstructive Sleep Apnea and the use of Capnometry 1230-1330 Obstructive Sleep Apnea and Use of End Tidal CO₂ in the PACU Objectives: Define Obstructive Sleep Apnea (OSA) Define End Tidal CO₂. Describe
Test Bank Pilbeam's Mechanical Ventilation Physiological and Clinical Applications 6th Edition Cairo
 Instant dowload and all chapters Test Bank Pilbeam's Mechanical Ventilation Physiological and Clinical Applications 6th Edition Cairo https://testbanklab.com/download/test-bank-pilbeams-mechanical-ventilation-physiologicalclinical-applications-6th-edition-cairo/
Instant dowload and all chapters Test Bank Pilbeam's Mechanical Ventilation Physiological and Clinical Applications 6th Edition Cairo https://testbanklab.com/download/test-bank-pilbeams-mechanical-ventilation-physiologicalclinical-applications-6th-edition-cairo/
Web Appendix 1: Literature search strategy. BTS Acute Hypercapnic Respiratory Failure (AHRF) write-up. Sources to be searched for the guidelines;
 write-up. Sources to be searched for the guidelines;") Web Appendix 1: Literature search strategy BTS Acute Hypercapnic Respiratory Failure (AHRF) write-up Sources to be searched for the guidelines; Cochrane Database of Systematic Reviews (CDSR) Database of
Web Appendix 1: Literature search strategy BTS Acute Hypercapnic Respiratory Failure (AHRF) write-up Sources to be searched for the guidelines; Cochrane Database of Systematic Reviews (CDSR) Database of
NYSPFP Kickoff. Reducing Adverse Drug Events from Opioids. April 6, 2017
 NYSPFP Kickoff Reducing Adverse Drug Events from Opioids April 6, 2017 I have no financial relationships with drug companies, durable medical equipment companies or other for profit entities related to
NYSPFP Kickoff Reducing Adverse Drug Events from Opioids April 6, 2017 I have no financial relationships with drug companies, durable medical equipment companies or other for profit entities related to
Frederic J., Gerges MD. Ghassan E. Kanazi MD., Sama, I. Jabbour-Khoury MD. Review article from Journal of clinical anesthesia 2006.
 Frederic J., Gerges MD. Ghassan E. Kanazi MD., Sama, I. Jabbour-Khoury MD. Review article from Journal of clinical anesthesia 2006 Introduction Laparoscopic surgery started in the mid 1950s. In recent
Frederic J., Gerges MD. Ghassan E. Kanazi MD., Sama, I. Jabbour-Khoury MD. Review article from Journal of clinical anesthesia 2006 Introduction Laparoscopic surgery started in the mid 1950s. In recent
1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation.
 Chapter 1: Principles of Mechanical Ventilation TRUE/FALSE 1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation. F
Chapter 1: Principles of Mechanical Ventilation TRUE/FALSE 1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation. F
1.1.2 CPAP therapy is used for patients who are suffering from an acute type 1 respiratory failure (Pa02 <8kPa with a normal or low Pac02).
.") Guidelines for initiating and managing CPAP (Continuous Positive Airway Pressure) on a general ward. B25/2006 1.Introduction and Who Guideline applies to 1.1.1 This document provides guidance for Healthcare
Guidelines for initiating and managing CPAP (Continuous Positive Airway Pressure) on a general ward. B25/2006 1.Introduction and Who Guideline applies to 1.1.1 This document provides guidance for Healthcare