Optimizing Patient Selection, Organ Allocation, and Outcomes in Liver Transplant (LT) Candidates with Hepatocellular Carcinoma (HCC)
|
|
|
- Osborn Cole
- 5 years ago
- Views:
Transcription
 Neil Mehta, MD University of California, San Francisco Division of")
1 XXVI SETH Congress- 30 November 2017 Optimizing Patient Selection, Organ Allocation, and Outcomes in Liver Transplant (LT) Candidates with Hepatocellular Carcinoma (HCC) Neil Mehta, MD University of California, San Francisco Division of GI/Hepatology

2 OVERVIEW Current state of LT for HCC worldwide Pushing beyond Milan criteria Down-staging and All-comers results Identifying important recurrence risk factors Does the donor matter? Assessing individualized post-lt HCC recurrence risk Novel risk scores using explant pathology Standardize surveillance regimens Tailor post-lt immunosuppression

3 Liver Transplant for HCC Milan Criteria 1 lesion 5 cm 2 to 3, none > 3 cm + Absence of Macroscopic Vascular Invasion Absence of Extra-hepatic Spread Mazzaferro, et al. N Engl J Med 1996;334:
4 LT FOR HCC: EXPANDED CRITERIA Sapisochin, G. & Bruix, J Nat. Rev. Gastroenterol. Hepatol.
5 LT FOR HCC: EXPANDED CRITERIA XX XX XX XX Sapisochin, G. & Bruix, J Nat. Rev. Gastroenterol. Hepatol.

6 Extended Toronto Criteria Milan >Milan 5-yr post-transplant survival 68% ETC; 78% Milan 5-yr recurrence probability 30% ETC; 13% Milan >Milan Milan Sapisochin G et al. Hepatology 2016;64:

7 LT FOR HCC: EXPANDED CRITERIA XX XX XX XX Sapisochin, G. & Bruix, J Nat. Rev. Gastroenterol. Hepatol.
8 Extended Criteria & FDG PET/CT The National Cancer Korea Criteria Total tumor diameter < 10 cm Negative 18 F-FDG PET/ CT 84% 85% Within NCCK Within NCCK > NCCK > NCCK Preoperative P < Pathology P < Lee SD, et al. World J Transpl 2016;6:

9 HCC MELD EXCEPTION WORLDWIDE Sapisochin, G. & Bruix, J Nat. Rev. Gastroenterol. Hepatol.



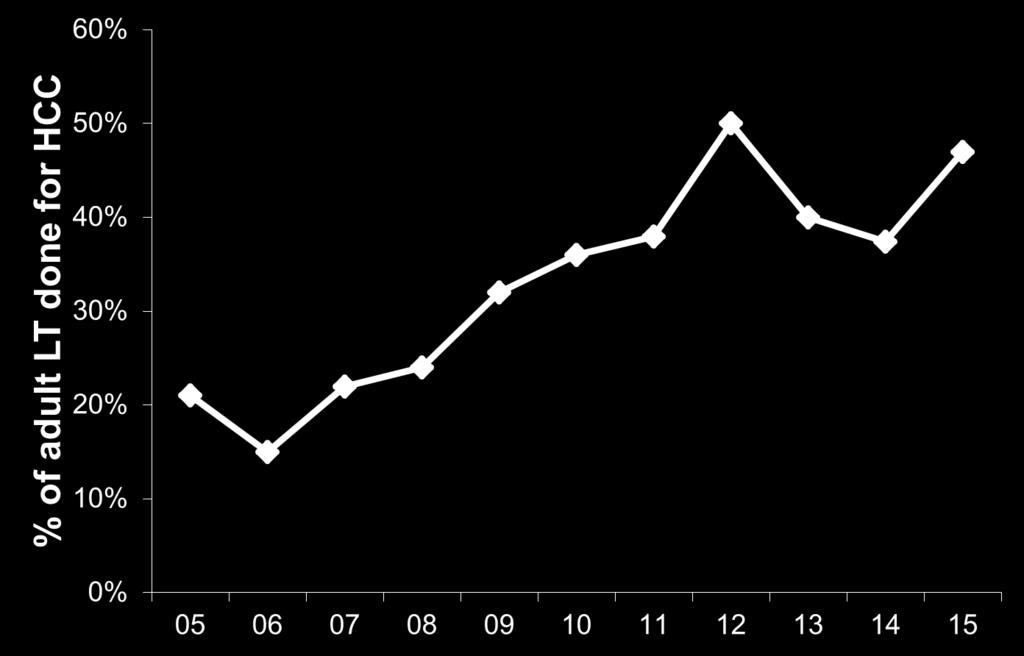
10 RISING INCIDENCE OF LIVER TRANSPLANT FOR HCC AT UCSF Year
11 RISING INCIDENCE OF LIVER TRANSPLANT FOR HCC AT UCSF 22 LT for HCC in % Year
12 RISING INCIDENCE OF LIVER TRANSPLANT FOR HCC AT UCSF 84 LT for HCC in % 22 LT for HCC in % Year
13 LIVER TRANSPLANTATION FOR HCC: OPTIMIZING SELECTION CRITERIA Scenario: Your patient with a 3.5 cm HCC is at the top of the wait list and is expecting a liver offer at any time. Today in clinic he asks you what his expected outcomes are after transplant.
14 LIVER TRANSPLANTATION FOR HCC: OPTIMIZING SELECTION CRITERIA Scenario: Your patient with a 3.5 cm HCC is at the top of the wait list and is expecting a liver offer at any time. Today in clinic he asks you what his expected outcomes are after transplant. 5 yr post-lt survival: 75-80% 5 yr HCC recurrence: ~15%
15 LIVER TRANSPLANTATION FOR HCC: OPTIMIZING SELECTION CRITERIA Scenario: Your patient with a 3.5 cm HCC is at the top of the wait list and is expecting a liver offer at any time. Today in clinic he asks you what his expected outcomes are after transplant. 5 yr post-lt survival:??? 5 yr HCC recurrence:???
16 LIVER TRANSPLANTATION FOR HCC: OPTIMIZING SELECTION CRITERIA Response to LRT 3.5 cm
17 LIVER TRANSPLANTATION FOR HCC: OPTIMIZING SELECTION CRITERIA Response to LRT AFP 3.5 cm
18 LIVER TRANSPLANTATION FOR HCC: OPTIMIZING SELECTION CRITERIA Response to LRT AFP 7.5 cm 3.5 cm
19 LIVER TRANSPLANTATION FOR HCC: OPTIMIZING SELECTION CRITERIA Response to LRT AFP Wait Time to LT 7.5 cm 3.5 cm
20 LIVER TRANSPLANTATION FOR HCC: OPTIMIZING SELECTION CRITERIA Response to LRT AFP Wait Time to LT 7.5 cm Donor Factors 3.5 cm

21 LIVER TRANSPLANTATION FOR HCC: OPTIMIZING SELECTION CRITERIA Response to LRT AFP Wait Time to LT 7.5 cm Donor Factors 3.5 cm 5 yr post-lt survival: % 5 yr HCC recurrence: %
22 LIVER TRANSPLANTATION FOR HCC: DOWNSTAGING 7.5 cm 3.5 cm 5 yr post-lt survival: % 5 yr HCC recurrence: %


23 Down-staging of HCC for Transplant Definition: Reduction in the size of tumor using local regional therapy to meet acceptable criteria for liver transplant 1 Tumor response: Based on radiographic measurement of the size of all viable tumors, not including the area of necrosis from local regional therapy 2 A selection tool for tumors with more favorable biology that respond to down-staging treatment and also do well after liver transplant 1 1. Yao & Fidelman. Hepatology 2016;63: EASL Guidelines - Briux J. et al. J Hepatol 2001;35:



24 Tumor Down-staging Before Liver Transplant Beyond Milan Within Milan Complete necrosis EASL and mrecist Yao & Fidelman. Hepatology 2016;63:
25 Eligibility criteria Dropout LRT for tumor down-staging Exclusion criteria End-point of Down-staging (Milan or other criteria) Dropout Minimum observation period LRT for maintaining tumors within LT listing criteria Deceased donor Liver Transplant 5-yr survival the same as those meeting criteria without down-staging International Consensus Conference on OLT and HCC. Clavien PA, et al. Lancet Oncology 2012:13;11-22
26 HCC Transplant UCSF MILAN CRITERIA DOWNSTAGING CRITERIA ALL-COMERS CRITERIA 1 lesion < 5 cm 2-3 lesions < 3 cm No extra-hepatic dz 1 lesion 5.1-8cm 2-3 lesions 5 cm 4-5 lesions 3 cm TTD 8 cm No extra-hepatic dz Any number of tumors Total tumor burden beyond DS criteria No extra-hepatic dz
27 Down-staging of HCC Updated UCSF Data (n=41) Dropout Meeting Milan criteria Median f/u 3.8 years 78% 5-yr survival post-transplant Down-staging (n=118) UCSF Criteria for Down-staging 1 tumor 8 cm 2-3 tumor 5 cm + total diameter 8 cm 4-5 tumor 3 cm + total diameter 8 cm Transplant (n=64) 91% 5-yr recurrence- free probability Yao et al. Hepatology 2015;61:
28 Post-Transplant Survival Milan group 81% Down-staged group 78% p=0.69 Yao FY, et al. Hepatology 2015;61:
29 Region 5 Multi-center Experience 187 consecutive adult patients with HCC treated under Region 5 down-staging protocol from 3 centers (UCSF, CPMC, Scripps) between 2002 and 2012 Uniform eligibility criteria, criteria for successful down-staging (within Milan criteria) and minimal observation period of 3 months Median time from down-staging to liver transplant of 12.6 months (IQR 6-19) Median post-transplant follow-up of 4.3 years Mehta N et al. Clinical Gastroenterology and Hepatology 2017 (in press)
30 Probability of Survival Post-Transplant Survival % 95% 80% 56.2% Years Post-Transplant Mehta N et al. Clinical Gastroenterology and Hepatology 2017 (in press)
31 Probability of Survival Post-Transplant Survival 1.0 Center 1 (n=75) 0.8 Center (n=34) P= Years Post-Transplant Center Center 2/ Mehta N et al. Clinical Gastroenterology and Hepatology 2017 (in press)
32 Region 5 Multi-center Experience Explant Tumor Characteristics n (%) Pathologic Tumor Stage (n=109) Complete necrosis (no viable tumor) 38 (35%) Within Milan criteria 50 (46%) Beyond Milan criteria 21 (19%) Vascular Invasion Micro-vascular/ Macro-vascular 7 (6%)/ 1 (1%) Histologic Grade of Differentiation (n=71) Well differentiated 25 (35%) Moderately differentiated 45 (63%) Poorly differentiated 1 (1%) Mehta N et al. Clinical Gastroenterology and Hepatology 2017 (in press)
 Vascular Invasion Micro-vascular/ Macro-vascular 7 (6%)/ 1 (1%) Histologic Grade of Differentiation (n=71) Well differentiated 25 (35%) Moderately differentiated 45 (63%) Poorly")
33 Region 5 Multi-center Experience Explant Tumor Characteristics n (%) Pathologic Tumor Stage (n=109) Complete necrosis (no viable tumor) 38 (35%) Within Milan criteria 50 (46%) Beyond Milan criteria 21 (19%) Vascular Invasion Micro-vascular/ Macro-vascular 7 (6%)/ 1 (1%) Histologic Grade of Differentiation (n=71) Well differentiated 25 (35%) Moderately differentiated 45 (63%) Poorly differentiated 1 (1%) Mehta N et al. Clinical Gastroenterology and Hepatology 2017 (in press)
34 - 1 tumor 8 cm tumor 5 cm + total diameter 8 cm tumor 3 cm + total diameter 8 cm Exclusion criteria Dropout UCSF/ Region 5 Down-staging criteria End-point of Down-staging = Milan Criteria LRT for tumor down-staging Dropout Observation period > 3 months LRT for maintaining tumors within LT listing criteria Liver Transplant 5-yr survival same as Milan criteria without down-staging UCSF/ Region 5 Down-staging protocol recently accepted as national policy
35 BEYOND DOWN-STAGING CRITERIA? What about patients whose tumor burden exceeds even the Region 5 down-staging protocol? Is there an upper limit of tumor burden beyond which LT is a bad idea?
36 HCC Transplant UCSF MILAN CRITERIA DOWNSTAGING CRITERIA ALL-COMERS CRITERIA 1 lesion < 5 cm 2-3 lesions < 3 cm No extra-hepatic dz 1 lesion 5.1-8cm 2-3 lesions 5 cm 4-5 lesions 3 cm TTD 8 cm No extra-hepatic dz Any number of tumors Total tumor burden beyond DS criteria No extra-hepatic dz

37 All-comers Down-staging Protocol All-comers Dropout LRT for tumor down-staging End-point of Down-staging = Milan Criteria Dropout Observation period > 6 months LRT for maintaining tumors within LT criteria Liver Transplant
38 All-comers group Meeting All-Comer Criteria (N = 74) Down-staged to Milan (N = 48) (65%) Never Downstaged (N = 26) (35%) Rassiwala J et al. AASLD 2016
39 All-comers group Meeting All-Comer Criteria (N = 74) Never Downstaged (N = 26) Awaiting LT (N = 6) Down-staged to Milan (N = 48) Underwent LT (N = 10) (14%) Dropout after Down-staging (N = 32) Rassiwala J et al. AASLD 2016
40 Probability of Downstaging by Initial Tumor Burden Number of Lesions + Largest Tumor Diameter 68% 57% 47% 38% Rassiwala J et al. AASLD 2016
41 HCC Recurrence (All-comers group) Meeting All-Comer Criteria (N = 74) Down-staged to Milan (N = 48) Underwent LT (N = 10) Post LT Recurrence (N = 3) Median 21.4 months from LT to recurrence
42 Intention-to-Treat Survival UCSF-DS 56% All-Comers 21% P < 0.001
43 All-comers Summary An upper limit in tumor burden probably exists beyond which successful LT after down-staging becomes an unrealistic goal Patients with tumor burden exceeding the Region 5 down-staging criteria must be very carefully selected for consideration of LT

44 LIVER TRANSPLANTATION FOR HCC: AFP AFP 3.5 cm 5 yr post-lt survival: % 5 yr HCC recurrence: %
45 Survival rate (%) AFP and Post-transplant Outcome- France % % n=387 n=109 AFP <100 AFP P < % n=61 AFP > Months after Liver Transplantation Duvoux et al. Gastroenterology 2012;143:986-94
46 Prognostic Model: Tumor size, number and AFP Variables Points Largest tumor diameter, cm > 6 4 Number of tumor nodules AFP level, ng/ml > Duvoux et al. Gastroenterology 2012;143:986-94
47 Prognostic Model: Tumor size, number and AFP Variables Points Largest tumor diameter, cm > 6 4 Number of tumor nodules AFP level, ng/ml > Low risk 2 points Some HCC > Milan but AFP 100 = Low risk Duvoux et al. Gastroenterology 2012;143:986-94
48 AFP and Post-transplant Outcome - UCSF AFP <1000 AFP > % 52% p = 0.03 y Hameed B. et al. Liver Transplantation 2014;
49 AFP and Post-transplant Outcome - UCSF AFP <1000 AFP > % 52% Applying AFP cutoff of >1000 ng/ml to pts within Milan criteria results in exclusion of 5% and 20% reduction in post-lt HCC recurrence y Hameed B. et al. Liver Transplantation 2014;
50 REDUCING HIGH AFP PRIOR TO LT Yao F. et al. AASLD 2017
51 REDUCING HIGH AFP PRIOR TO LT Yao F. et al. AASLD 2017
52 UNOS POLICY CHANGE High AFP Threshold Candidates with lesions meeting T2 criteria but with an AFP >1000 are not eligible for a standardized MELD exception If AFP falls <500 after LRT, the candidate is eligible for a standardized MELD exception
53 UNOS POLICY CHANGE High AFP Threshold Candidates with lesions meeting T2 criteria but with an AFP >1000 are not eligible for a standardized MELD exception If AFP falls <500 after LRT, the candidate is eligible for a standardized MELD exception However, AFP reduction to <100 after LRT is ideal
54 LT FOR HCC: METROTICKET 2.0 HCC Specific Survival Mazzaferro V et al. Gastroenterology 2017 (in press)
55 LT FOR HCC: METROTICKET 2.0 HCC Specific Survival x Mazzaferro V et al. Gastroenterology 2017 (in press)

56 LT FOR HCC: METROTICKET 2.0 HCC Specific Survival x Mazzaferro V et al. Gastroenterology 2017 (in press)
57 LIVER TRANSPLANTATION FOR HCC: OPTIMIZING SELECTION CRITERIA Response to LRT 3.5 cm 5 yr post-lt survival: % 5 yr HCC recurrence: %
58 Recurrence Rate (%) RESPONSE TO LOCAL-REGIONAL THERAPY AS PROGNOSTIC FACTOR 18% 5% Kim DJ, et al. Am J Transpl 2014;
59 Recurrence Free Survival (%) Within Milan, no risk factors Beyond Milan, no risk factors Within Milan, (+) risk factors Beyond Milan, (+) risk factors Risk factors - Radiologic tumor progression - AFP slope > 15 ng/ml/month Months after liver transplantation Lai Q, et al. Liver Transpl 2013;19:
60 Recurrence Free Survival (%) 90% Within Milan, no risk factors Beyond Milan, no risk factors Within Milan, (+) risk factors Beyond Milan, (+) risk factors Risk factors - Radiologic tumor progression - AFP slope > 15 ng/ml/month Months after liver transplantation Lai Q, et al. Liver Transpl 2013;19:
61 Recurrence Free Survival (%) 90% 68% Within Milan, no risk factors Beyond Milan, no risk factors Within Milan, (+) risk factors 42% Beyond Milan, (+) risk factors Risk factors - Radiologic tumor progression - AFP slope > 15 ng/ml/month Months after liver transplantation Lai Q, et al. Liver Transpl 2013;19:
62 LIVER TRANSPLANTATION FOR HCC: OPTIMIZING SELECTION CRITERIA Wait Time to LT 3.5 cm 5 yr HCC recurrence: %



63 POST-LT HCC SURVIVAL IN UNOS DATABASE: IMPACT OF WAITING TIME Time from listing to LT > 3 months Schlansky et al, Liver Transplantation 2014;
64 U.S. MULTI-CENTER STUDY ON WAIT TIMES Multi-center cohort study of all adults with HCC within Milan criteria by imaging listed with MELD exception from (n=911) 3 study centers chosen to capture spectrum of wait times: Long (UCSF - Center 1) Medium (Mayo Clinic Rochester - Center 2) Short (Mayo Clinic Jacksonville - Center 3) Wait time started at HCC diagnosis Mehta N, et al. Transplantation 2017
65 PREDICTORS OF RECURRENCE KNOWN PRIOR TO LT Predictor Multivariable HR (95% CI) p- value Wait Time to LT <6 or >18 mo 1.6 ( ) 0.04 AFP at HCC dx >400 vs ( ) <0.001 Wait time of <6 or >18 mo associated w/ AFP >100 at LT (HR 1.6, 95% CI , p<0.03) Mehta N, et al. Transplantation 2017
66 THE WAIT TIME SWEET SPOT : 6-18 MONTHS p=0.049 <6 or >18 months 16% 6-18 months 10% Mehta N, et al. Transplantation 2017
 Avoid unnecessary dropout seen with very prolonged wait times Mehta N, et al.")
67 U.S. MULTI-CENTER STUDY ON WAIT TIMES The sweet spot wait time of 6-18 months from HCC diagnosis should be the target to: 1) Minimize HCC recurrence after LT 2) Avoid unnecessary dropout seen with very prolonged wait times Mehta N, et al. Transplantation 2017
68 LIVER TRANSPLANTATION FOR HCC: DONOR INFLUENCE ON OUTCOMES? Donor Factors 3.5 cm 5 yr post-lt survival: % 5 yr HCC recurrence: %
69 MARGINAL LIVERS INFLUENCE ON OUTCOMES (HCC AND NON-HCC) p=0.08 for Standard Liver vs Marginal Liver (DCD, split, steatosis >30%, CIT >12 hrs, donor age>70) 76% 70% Halazun K et al. Ann Surgery 2016:
 Marginal Livers more")

70 MARGINAL LIVERS INFLUENCE ON OUTCOMES (HCC AND NON-HCC) Marginal Livers more likely to have HCC (21% vs 10%) 76% 70% Halazun K et al. Ann Surgery 2017:
71 Orci LA, et al. Br J Surgery 2015: DONOR INFLUENCE ON HCC RECURRENCE?
72 COLD ISCHEMIA TIME INFLUENCE ON HCC RECURRENCE? Vagefi P, et al. Liver Txp 2015:


73 LIVER TRANSPLANTATION FOR HCC: DCD INFLUENCE ON OUTCOMES? Post-LT HCC Survival DBD and DCD Matched Cohorts with HCC Post-LT HCC Recurrence Croome KP, et al. Am J Transpl 2015;
74 LIVER TRANSPLANTATION FOR HCC: DONOR SUMMARY Donor age >60, donor steatosis/diabetes/ obesity, and increased cold ischemia time may lead to small increase in recurrence When using marginal livers for HCC, need to maximize chance of a good outcome whenever possible: E.g. Well-compensated patient with well treated tumor likely will not benefit from DCD donor Limit # of risk factors (e.g. if cold ischemia time >10 hours then hopefully donor age <60) Normothermic perfusion for DCD or steatotic livers Vining CC et al Liver Txp; Sapisochin, G. & Bruix, J Nat. Rev. Gastroenterol. Hepatol.
75 OVERVIEW Current state of LT for HCC worldwide Down-staging and All-comers results Pushing beyond Milan criteria Identifying important recurrence risk factors Does the donor matter? Assessing individualized post-lt recurrence risk using the explant to: Standardized surveillance regimens Tailor immunosuppression
76 ESTIMATING POST-LT HCC RECURRENCE Tumor recurrence is the most common cause of death after LT for HCC w/ median survival of ~1 year Explant provides a wealth of objective (?) data to better stratify recurrence risk Several post-lt models have been recently proposed to estimate post-transplant recurrence (and survival): Post- or Combo-MORAL score US Multicenter HCC Transplant Consortium nomogram RETREAT score Clavien PA, et al. Lancet Oncology 2012; 13:11-22; Halazun KJ et al. Ann Surg 2017; Mehta N et al. JAMA Oncology 2017; Agopian VG et al. ATC 2017


77 RETREAT SCORE Multi-center study, 1060 LT recipients w/ HCC meeting Milan criteria by imaging, developed + validated prediction index for HCC recurrence The Risk Estimation of Tumor Recurrence After Transplant (RETREAT) score incorporates 3 variables that independently predict recurrence - Last AFP prior to LT - Microvascular invasion - Largest viable tumor diameter + number of viable tumors on explant Mehta N, et al. JAMA Oncology 2017
78 RETREAT: EXPLANT TUMOR BURDEN Sum of the largest diameter of viable tumor + number of viable tumors on explant 1 viable lesion 4 cm = 5 2 viable lesions 4 cm & 2 cm = 6 2 completely necrotic lesions are not counted
79 RETREAT SCORE Predictor Points AFP at LT > Micro-vascular Invasion Yes 2 Largest Viable Tumor Size (cm) + Number of Viable Lesions >10 3 No RETREAT points scored for: AFP 0-20, no microvascular invasion, and explant pathology stage score of 0 Mehta N, et al. JAMA Oncology 2017
80 RETREAT SCORE: 1 YR RECURRENCE 50 % C Concordance Statistic % 39% 30 % % % 0 % 1% 3% 4% 5% _ >5 RETREAT Score 11% N=
81 RETREAT SCORE: 5 YR RECURRENCE 80 % 75% 60 % 40 % 29% 20 0 % % 14% 11% 8% 3% _ >5 RETREAT Score N=
82 RETREAT VALIDATION IN UNOS (N=3392) C Statistic 0.75 for HCC recurrence prediction in UNOS Mehta N, et al. Am J Transplant 2017 (in press)
83 RETREAT VALIDATION IN UNOS (N=3392) C Statistic 0.75 for HCC recurrence prediction in UNOS Log-rank p<0.001 RETREAT Mehta N, et al. Am J Transplant 2017 (in press)
84 RETREAT FOR HCC SURVEILLANCE 80 % 75% 60 % % % % 3% 29% 14% 11% 8% _ >5 RETREAT Score
85 RETREAT FOR HCC SURVEILLANCE RETREAT Proposed surveillance regimen 0 No surveillance (20-25% of the cohort) Mehta N, et al. JAMA Oncology 2017
86 RETREAT SCORE: 5 YR RECURRENCE 80 % 75% 60 % % % % 3% 11% 14% 8% 29% _ >5 RETREAT Score
87 RETREAT FOR HCC SURVEILLANCE RETREAT Proposed surveillance regimen 0 No surveillance (20-25% of the cohort) 1-3 HCC surveillance every 6 months for 2 years Mehta N, et al. JAMA Oncology 2017
88 RETREAT SCORE: 5 YR RECURRENCE 80 % 75% 60 % % % % 14% 11% 8% 3% 29% _ >5 RETREAT Score
89 RETREAT FOR HCC SURVEILLANCE RETREAT Proposed surveillance regimen 0 No surveillance (20-25% of the cohort) 1-3 HCC surveillance every 6 months for 2 years 4 HCC surveillance every 6 months for 5 years Mehta N, et al. JAMA Oncology 2017
90 RETREAT SCORE: 1 YR RECURRENCE 50 % 40 % 39% 30 % 20 % 10 % 0 % 11% 3% 4% 5% 1% >5 _ RETREAT Score
91 RETREAT FOR HCC SURVEILLANCE RETREAT Proposed surveillance regimen 0 No surveillance (20-25% of the cohort) 1-3 HCC surveillance every 6 months for 2 years 4 HCC surveillance every 6 months for 5 years 5+ HCC surveillance every 3-4 months for 2 years; then every 6 months for years 2-5 Mehta N, et al. JAMA Oncology 2017
92 RETREAT FOR HCC SURVEILLANCE RETREAT Proposed surveillance regimen 0 No surveillance (20-25% of the cohort) 1-3 HCC surveillance every 6 months for 2 years 4 HCC surveillance every 6 months for 5 years 5+ HCC surveillance every 3-4 months for 2 years; then every 6 months for years 2-5 Surveillance should be performed w/ multiphasic abdominal CT or MRI, chest CT, and AFP at the recommended interval
93 RETREAT FOR HCC SURVEILLANCE RETREAT Proposed surveillance regimen 0 No surveillance (20-25% of the cohort) 1-3 HCC surveillance every 6 months for 2 years 4 HCC surveillance every 6 months for 5 years 5+ HCC surveillance every 3-4 months for 2 years; then every 6 months for years 2-5 Consensus statement from participating centers in the multi-center cohort (UCSF, Mayo Clinic Rochester, Mayo Clinic Jacksonville, U. Toronto) Mehta N, et al. JAMA Oncology 2017
94 RETREAT: JBL 1/24/15 AFP at Transplant Explant - Evidence of HCC in explant: Necrotic nodule, no viable tumor. - Number of tumors: 1, well-circumscribed. - Largest Tumor: 3.6 cm, entirely necrosed. - Vascular invasion: Necrotic nodule abuts large vessel but does not invade it. - Local extension of tumor: Confined to liver.
95 RETREAT: JBL Risk Factors for HCC Recurrence Points AFP at LT > Microvascular Invasion No 0 Yes 2 Explant Largest Viable Tumor Size (cm) Plus Number of Viable Lesions >10 3
96 RETREAT: JBL HCC Recurrence at 1 and 5 Years after LT Total Points Scored Predicted HCC Recurrence at 1 yr Predicted HCC Recurrence at 5 yrs 0 1.0% 2.9% 1 2.9% 8.0% 2 4.0% 10.8% 3 5.1% 13.7% % 28.7% >5 39.3% 75.2%
97 RETREAT FOR HCC SURVEILLANCE RETREAT Proposed surveillance regimen 1-3 HCC surveillance every 6 months for 2 years Surveillance should be performed w/ multiphasic abdominal CT or MRI, chest CT, and AFP at the recommended interval.
98 RETREAT FOR HCC SURVEILLANCE RETREAT Proposed surveillance regimen 1-3 HCC surveillance every 6 months for 2 years Surveillance should be performed w/ multiphasic abdominal CT or MRI, chest CT, and AFP at the recommended interval. Ongoing prospective multi-center study evaluating this surveillance protocol
99 POST-LT IMS: CNIs Standard post-lt IMS is CNI (e.g tacrolimus) w/ mycophenolate and prednisone Postulated that CNIs may increase HCC recurrence risk Rodriguez-Peralvarez et al. J Hepatology 2013

100 POST-LT IMS: mtori mtor regulates cell growth, proliferation, metabolism, and aging mtor inhibitors have shown anticancer properties in in vitro and animal models Prevents angiogenesis by interfering with VEGF-mediated pathways, thus potentially limiting tumor growth Induces extensive microthrombi, thus potentially inhibiting tumor growth mtor pathway frequently up-regulated in HCC Many LT centers have shifted to using mtor based IMS in HCC pts undergoing LT Matter MS et al J Hepatology 2014


101 POST-LT IMS: MTORi Yanik et al: SRTR HCC LT recipients, sirolimus within 3 mo of LT vs 3702 never treated with sirolimus Linked w/ national pharmacy claims Sirolimus pts more likely to be outside Milan (11% vs 5%) but AFPs similar No significant differences between the groups in all-cause mortality, cancer-specific mortality, and HCC recurrence Yanik EL et al, Liver Txp 2016
102 SILVER TRIAL Prospective phase 3, multi-center international RCT Geissler EK et al, Transplantation 2016

103 SILVER TRIAL: RFS Prospective phase 3, multi-center international RCT Sirolimus No SIR Geissler EK et al, Transplantation 2016

104 SILVER TRIAL: OVERALL SURVIVAL Sirolimus No SIR Geissler EK et al, Transplantation 2016
105 POST-LT IMS Consider moving away from studying mtor inhibitors in all HCC LT recipients, but focus on those most likely to benefit Specifically target those with up-regulation of mtor pathways, which occurs in ~50% of HCC pts Molecular subtyping of explant tumor may prove important, especially w/ 2nd generation mtor inhibitors that more widely block downstream targets At UCSF, pts w/ RETREAT score >4 are converted to MTOR based IMS at 4-12 wks post LT Mehta N et al, Liver Txp 2016; Matter MS et al J Hepatology 2014
106 POST-LT HCC RECURRENCE SUMMARY Recent development of several risk scores to estimate individual HCC recurrence risk Tailor post-lt HCC surveillance regimens based on recurrence risk Ongoing prospective studies to determine if this translates into improved outcomes Mixed results using mtor inhibitors focus on those most likely to benefit


107 Thank You! UCSF Transplant Hepatology Team
9/10/2018. Liver Transplant for Hepatocellular Carcinoma (HCC): What is New? DISCLOSURES
: What is New? DISCLOSURES") UCSF Transplant 2018: Pioneering Advances in Transplantation DISCLOSURES Liver Transplant for Hepatocellular Carcinoma (HCC): What is New? I have no relevant commercial interests or relationships to report
UCSF Transplant 2018: Pioneering Advances in Transplantation DISCLOSURES Liver Transplant for Hepatocellular Carcinoma (HCC): What is New? I have no relevant commercial interests or relationships to report
Reconsidering Liver Transplantation for HCC in a Era of Organ shortage
 Reconsidering Liver Transplantation for HCC in a Era of Organ shortage Professor Didier Samuel Centre Hépatobiliaire Inserm-Paris Sud Research Unit 1193 Departement Hospitalo Universitaire Hepatinov Hôpital
Reconsidering Liver Transplantation for HCC in a Era of Organ shortage Professor Didier Samuel Centre Hépatobiliaire Inserm-Paris Sud Research Unit 1193 Departement Hospitalo Universitaire Hepatinov Hôpital
Liver Transplantation for HCC Which Criteria?
 Liver Transplantation for HCC Which Criteria? Jacques Belghiti - François Durand Claire Francoz Hepato-Biliary-Pancreatic Liver Surgery and Liver Transplantation Unit Hôpital Beaujon (AP-HP), Clichy -
Liver Transplantation for HCC Which Criteria? Jacques Belghiti - François Durand Claire Francoz Hepato-Biliary-Pancreatic Liver Surgery and Liver Transplantation Unit Hôpital Beaujon (AP-HP), Clichy -
Liver transplantation: Hepatocellular carcinoma
 Liver transplantation: Hepatocellular carcinoma Alejandro Forner BCLC Group. Liver Unit. Hospital Clínic. University of Barcelona 18 de marzo 2015 3r Curso Práctico de Transplante de Órganos Sólidos Barcelona
Liver transplantation: Hepatocellular carcinoma Alejandro Forner BCLC Group. Liver Unit. Hospital Clínic. University of Barcelona 18 de marzo 2015 3r Curso Práctico de Transplante de Órganos Sólidos Barcelona
Liver transplanta-on with extented Milan criteria
 Liver transplanta-on with extented Milan criteria Pr Olivier Detry Dpt of Abdominal Surgery & Transplanta-on CHU Liege, University of Liege Liver transplanta-on for HCC: do size & number really maher??
Liver transplanta-on with extented Milan criteria Pr Olivier Detry Dpt of Abdominal Surgery & Transplanta-on CHU Liege, University of Liege Liver transplanta-on for HCC: do size & number really maher??
Hepatocellular Carcinoma: Transplantation, Resection or Ablation?
 Hepatocellular Carcinoma: Transplantation, Resection or Ablation? Roberto Gedaly MD Chief, Abdominal Transplantation Transplant Service Line University of Kentucky Nothing to disclose Disclosure Objective
Hepatocellular Carcinoma: Transplantation, Resection or Ablation? Roberto Gedaly MD Chief, Abdominal Transplantation Transplant Service Line University of Kentucky Nothing to disclose Disclosure Objective
21/02/2014. Disclosures. HCC: predicting recurrence. Outline. Liver transplant: Beyond Milan?
 Disclosures HCC: predicting recurrence Peter Ghali, MD, FRCPC, MSc (epid) None relevant to this talk other than off-label use of sirolimus Toronto, February 2014 Outline Recurrence after what? Locoregional
Disclosures HCC: predicting recurrence Peter Ghali, MD, FRCPC, MSc (epid) None relevant to this talk other than off-label use of sirolimus Toronto, February 2014 Outline Recurrence after what? Locoregional
Living Donor Liver Transplantation for Hepatocellular Carcinoma: It Is All about Donors?
 Original Article Living Donor Liver Transplantation for Hepatocellular Carcinoma: It Is All about Donors? R. F. Saidi 1 *, Y. Li 2, S. A. Shah 2, N. Jabbour 2 1 Division of Organ Transplantation, Department
Original Article Living Donor Liver Transplantation for Hepatocellular Carcinoma: It Is All about Donors? R. F. Saidi 1 *, Y. Li 2, S. A. Shah 2, N. Jabbour 2 1 Division of Organ Transplantation, Department
NHS BLOOD AND TRANSPLANT ORGAN DONATION AND TRANSPLANTATION DIRECTORATE LIVER ADVISORY GROUP UPDATE ON THE HCC DOWN-STAGING SERVICE EVALUATION
 NHS BLOOD AND TRANSPLANT ORGAN DONATION AND TRANSPLANTATION DIRECTORATE LIVER ADVISORY GROUP UPDATE ON THE HCC DOWN-STAGING SERVICE EVALUATION 1. A service development evaluation to transplant down-staged
NHS BLOOD AND TRANSPLANT ORGAN DONATION AND TRANSPLANTATION DIRECTORATE LIVER ADVISORY GROUP UPDATE ON THE HCC DOWN-STAGING SERVICE EVALUATION 1. A service development evaluation to transplant down-staged
HCC RADIOLOGIC DIAGNOSIS
 UCSF Transplant 2010 THE BEFORE AND AFTER HEPATOCELLULAR CARCINOMA MANAGEMENT Francis Yao, M.D. Professor of Clinical Medicine and Surgery Medical Director, Liver Transplantation University of California,
UCSF Transplant 2010 THE BEFORE AND AFTER HEPATOCELLULAR CARCINOMA MANAGEMENT Francis Yao, M.D. Professor of Clinical Medicine and Surgery Medical Director, Liver Transplantation University of California,
WHAT IS THE BEST APPROACH FOR TRANS-ARTERIAL THERAPY IN HCC?
 WHAT IS THE BEST APPROACH FOR TRANS-ARTERIAL THERAPY IN HCC? Dr. Alexander Kim Chief, Vascular and Interventional Radiology, Medstar Georgetown University Hospital, USA DISCLAIMER Please note: The views
WHAT IS THE BEST APPROACH FOR TRANS-ARTERIAL THERAPY IN HCC? Dr. Alexander Kim Chief, Vascular and Interventional Radiology, Medstar Georgetown University Hospital, USA DISCLAIMER Please note: The views
Hepatocellular Carcinoma: Diagnosis and Management
 Hepatocellular Carcinoma: Diagnosis and Management Nizar A. Mukhtar, MD Co-director, SMC Liver Tumor Board April 30, 2016 1 Objectives Review screening/surveillance guidelines Discuss diagnostic algorithm
Hepatocellular Carcinoma: Diagnosis and Management Nizar A. Mukhtar, MD Co-director, SMC Liver Tumor Board April 30, 2016 1 Objectives Review screening/surveillance guidelines Discuss diagnostic algorithm
Increased hepatocellular carcinoma recurrence in women compared to men with high alpha fetoprotein at liver transplant
 ORIGINAL ARTICLE July-August, Vol. 15 No. 4, 2016: 545-549 545 The Official Journal of the Mexican Association of Hepatology, the Latin-American Association for Study of the Liver and the Canadian Association
ORIGINAL ARTICLE July-August, Vol. 15 No. 4, 2016: 545-549 545 The Official Journal of the Mexican Association of Hepatology, the Latin-American Association for Study of the Liver and the Canadian Association
9th Paris Hepatitis Conference
 9th Paris Hepatitis Conference Paris, 12 January 2016 Treatment of hepatocellular carcinoma: beyond international guidelines Massimo Colombo Chairman Department of Liver, Kidney, Lung and Bone Marrow Units
9th Paris Hepatitis Conference Paris, 12 January 2016 Treatment of hepatocellular carcinoma: beyond international guidelines Massimo Colombo Chairman Department of Liver, Kidney, Lung and Bone Marrow Units
Extending Indication: Role of Living Donor Liver Transplantation for Hepatocellular Carcinoma
 LIVER TRANSPLANTATION 13:S48-S54, 27 SUPPLEMENT Extending Indication: Role of Living Donor Liver Transplantation for Hepatocellular Carcinoma Satoru Todo, 1 Hiroyuki Furukawa, 2 Mitsuhiro Tada, 3 and the
LIVER TRANSPLANTATION 13:S48-S54, 27 SUPPLEMENT Extending Indication: Role of Living Donor Liver Transplantation for Hepatocellular Carcinoma Satoru Todo, 1 Hiroyuki Furukawa, 2 Mitsuhiro Tada, 3 and the
Liver transplantation for hepatocellular carcinoma - non-cancer factors and implications for improving outcome beyond standard tumor criteria
 Kornberg et al. Hepatoma Res 2018;4:60 DOI: 10.20517/2394-5079.2018.86 Hepatoma Research Review Open Access Liver transplantation for hepatocellular carcinoma - non-cancer factors and implications for
Kornberg et al. Hepatoma Res 2018;4:60 DOI: 10.20517/2394-5079.2018.86 Hepatoma Research Review Open Access Liver transplantation for hepatocellular carcinoma - non-cancer factors and implications for
Unmet needs in intermediate HCC. Korea University Guro Hospital Ji Hoon Kim
 Unmet needs in intermediate HCC Korea University Guro Hospital Ji Hoon Kim BCLC HCC Stage 0 PST 0, Child Pugh A Stage A C PST 0 2, Child Pugh A B Stage D PST > 2, Child Pugh C Very early stage (0) 1 HCC
Unmet needs in intermediate HCC Korea University Guro Hospital Ji Hoon Kim BCLC HCC Stage 0 PST 0, Child Pugh A Stage A C PST 0 2, Child Pugh A B Stage D PST > 2, Child Pugh C Very early stage (0) 1 HCC
Waitlist Priority for Hepatocellular Carcinoma Beyond Milan Criteria: A Potentially Appropriate Decision Without a Structured Approach
 American Journal of Transplantation 2014; 14: 79 87 Wiley Periodicals Inc. C Copyright 2013 The American Society of Transplantation and the American Society of Transplant Surgeons doi: 10.1111/ajt.12530
American Journal of Transplantation 2014; 14: 79 87 Wiley Periodicals Inc. C Copyright 2013 The American Society of Transplantation and the American Society of Transplant Surgeons doi: 10.1111/ajt.12530
Surveillance for Hepatocellular Carcinoma
 Surveillance for Hepatocellular Carcinoma Marion G. Peters, MD John V. Carbone, MD, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California San Francisco Recorded on April
Surveillance for Hepatocellular Carcinoma Marion G. Peters, MD John V. Carbone, MD, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California San Francisco Recorded on April
Hepatitis C: Difficult-to-treat Patients 11th Paris Hepatology Conference 16th January 2018 Stefan Zeuzem, MD University Hospital, Frankfurt, Germany
 Hepatitis C: Difficult-to-treat Patients 11th Paris Hepatology Conference 16th January 2018 Stefan Zeuzem, MD University Hospital, Frankfurt, Germany PHC 2018 - www.aphc.info Disclosures Advisory boards:
Hepatitis C: Difficult-to-treat Patients 11th Paris Hepatology Conference 16th January 2018 Stefan Zeuzem, MD University Hospital, Frankfurt, Germany PHC 2018 - www.aphc.info Disclosures Advisory boards:
Management of HepatoCellular Carcinoma
 9th Symposium GIC St Louis - 2010 Management of HepatoCellular Carcinoma Overview Pierre A. Clavien, MD, PhD Department of Surgery University Hospital Zurich Zurich, Switzerland Hepatocellular carcinoma
9th Symposium GIC St Louis - 2010 Management of HepatoCellular Carcinoma Overview Pierre A. Clavien, MD, PhD Department of Surgery University Hospital Zurich Zurich, Switzerland Hepatocellular carcinoma
6/16/2016. Treating Hepatocellular Carcinoma: Deciphering the Clinical Data. Liver Regeneration. Liver Regeneration
 Treating : Deciphering the Clinical Data Derek DuBay, MD Associate Professor of Surgery Director of Liver Transplant Liver Transplant and Hepatobiliary Surgery UAB Department of Surgery Liver Regeneration
Treating : Deciphering the Clinical Data Derek DuBay, MD Associate Professor of Surgery Director of Liver Transplant Liver Transplant and Hepatobiliary Surgery UAB Department of Surgery Liver Regeneration
AASLD Washington DC, USA Dr. Alexander Kim Chief Vascular and Interventional Radiology, Medstar Georgetown University Hospital
 AASLD 2017 - Washington DC, USA Dr. Alexander Kim Chief Vascular and Interventional Radiology, Medstar Georgetown University Hospital THE CHANGING LANDSCAPE IN THE TREATMENT OF HCC DISCLAIMER Please note:
AASLD 2017 - Washington DC, USA Dr. Alexander Kim Chief Vascular and Interventional Radiology, Medstar Georgetown University Hospital THE CHANGING LANDSCAPE IN THE TREATMENT OF HCC DISCLAIMER Please note:
Hepatocellular Carcinoma. Markus Heim Basel
 Hepatocellular Carcinoma Markus Heim Basel Outline 1. Epidemiology 2. Surveillance 3. (Diagnosis) 4. Staging 5. Treatment Epidemiology of HCC Worldwide, liver cancer is the sixth most common cancer (749
Hepatocellular Carcinoma Markus Heim Basel Outline 1. Epidemiology 2. Surveillance 3. (Diagnosis) 4. Staging 5. Treatment Epidemiology of HCC Worldwide, liver cancer is the sixth most common cancer (749
Living donor liver transplantation for hepatocellular carcinoma in Seoul National University
 Original Article on Liver Transplantation for Hepatocellular Carcinoma Living donor liver transplantation for hepatocellular carcinoma in Seoul National University Suk Kyun Hong, Kwang-Woong Lee, Hyo-Sin
Original Article on Liver Transplantation for Hepatocellular Carcinoma Living donor liver transplantation for hepatocellular carcinoma in Seoul National University Suk Kyun Hong, Kwang-Woong Lee, Hyo-Sin
Advances in percutaneous ablation for hepatocellular carcinoma
 Advances in percutaneous ablation for hepatocellular carcinoma P. Nahon1,2,3 1 Hepatology, Jean Verdier Hospital, APHP, Bondy, France 2 Paris 13 university, Sorbonne Paris Cité, UFRSMBH, Bobigny, France
Advances in percutaneous ablation for hepatocellular carcinoma P. Nahon1,2,3 1 Hepatology, Jean Verdier Hospital, APHP, Bondy, France 2 Paris 13 university, Sorbonne Paris Cité, UFRSMBH, Bobigny, France
Worldwide Causes of HCC
 Approach to HCV Treatment in Patients with HCC JORGE L. HERRERA, MD, MACG UNIVERSITY OF SOUTH ALABAMA COLLEGE OF MEDICINE Worldwide Causes of HCC 60% 50% 40% 54% 30% 20% 10% 31% 15% 0% Hepatitis B Hepatitis
Approach to HCV Treatment in Patients with HCC JORGE L. HERRERA, MD, MACG UNIVERSITY OF SOUTH ALABAMA COLLEGE OF MEDICINE Worldwide Causes of HCC 60% 50% 40% 54% 30% 20% 10% 31% 15% 0% Hepatitis B Hepatitis
Current Status of HBV and Liver Transplant
 Current Status of HBV and Liver HBV as Indication for Liver ation in U.S. Significant decrease in rate of wait listing for decompensated cirrhosis since 2003 (since s) No change in rate of wait listing
Current Status of HBV and Liver HBV as Indication for Liver ation in U.S. Significant decrease in rate of wait listing for decompensated cirrhosis since 2003 (since s) No change in rate of wait listing
Disparities in Liver Transplant Allocation: An Update on MELD Allocation System
 Disparities in Liver Transplant Allocation: An Update on MELD Allocation System Naudia L. Jonassaint, MD MHS Assistant Professor of Medicine and Surgery University of Pittsburgh School of Medicine Historical
Disparities in Liver Transplant Allocation: An Update on MELD Allocation System Naudia L. Jonassaint, MD MHS Assistant Professor of Medicine and Surgery University of Pittsburgh School of Medicine Historical
THE CHANGING LANDSCAPE IN THE TREATMENT OF HEPATOCELLULAR CARCINOMA (HCC)
") MEETING SUMMARY EASL 2017, AMSTERDAM, THE NETHERLANDS APRIL 19 TH TO 23 RD 2017 DR JEAN-CHARLES NAULT JEAN VERDIER HOSPITAL, BONDY, FRANCE THE CHANGING LANDSCAPE IN THE TREATMENT OF HEPATOCELLULAR CARCINOMA
MEETING SUMMARY EASL 2017, AMSTERDAM, THE NETHERLANDS APRIL 19 TH TO 23 RD 2017 DR JEAN-CHARLES NAULT JEAN VERDIER HOSPITAL, BONDY, FRANCE THE CHANGING LANDSCAPE IN THE TREATMENT OF HEPATOCELLULAR CARCINOMA
Liver Transplantation Evaluation: Objectives
 Liver Transplantation Evaluation: Essential Work-Up Curtis K. Argo, MD, MS VGS/ACG Regional Postgraduate Course Williamsburg, VA September 13, 2015 Objectives Discuss determining readiness for transplantation
Liver Transplantation Evaluation: Essential Work-Up Curtis K. Argo, MD, MS VGS/ACG Regional Postgraduate Course Williamsburg, VA September 13, 2015 Objectives Discuss determining readiness for transplantation
Despite recent advances in the care of patients with
 Liver Transplantation for Hepatocellular Carcinoma: Lessons from the First Year Under the Model of End- Stage Liver Disease (MELD) Organ Allocation Policy Francis Y. Yao, 1,2 Nathan M. Bass, 1 Nancy L.
Liver Transplantation for Hepatocellular Carcinoma: Lessons from the First Year Under the Model of End- Stage Liver Disease (MELD) Organ Allocation Policy Francis Y. Yao, 1,2 Nathan M. Bass, 1 Nancy L.
Radiofrequency Ablation of Primary or Metastatic Liver Tumors
 Radiofrequency Ablation of Primary or Metastatic Liver Tumors Policy Number: 7.01.91 Last Review: 9/2018 Origination: 2/1996 Next Review: 9/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC)
Radiofrequency Ablation of Primary or Metastatic Liver Tumors Policy Number: 7.01.91 Last Review: 9/2018 Origination: 2/1996 Next Review: 9/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC)
OHSU Digital Commons. Oregon Health & Science University. Barry Schlansky. Scholar Archive. July 2013
 Oregon Health & Science University OHSU Digital Commons Scholar Archive July 2013 Waitlist time predicts survival after liver transplantation for hepatocellular carcinoma : a cohort study in the United
Oregon Health & Science University OHSU Digital Commons Scholar Archive July 2013 Waitlist time predicts survival after liver transplantation for hepatocellular carcinoma : a cohort study in the United
Liver Transplantation for Hepatocellular Carcinoma: Validation of the UCSF-Expanded Criteria Based on Preoperative Imaging
 American Journal of Transplantation 2007; 7: 2587 2596 Blackwell Munksgaard C 2007 The Authors Journal compilation C 2007 The American Society of Transplantation and the American Society of Transplant
American Journal of Transplantation 2007; 7: 2587 2596 Blackwell Munksgaard C 2007 The Authors Journal compilation C 2007 The American Society of Transplantation and the American Society of Transplant
Living donor liver transplantation for hepatocellular carcinoma achieves better outcomes
 Review Article on Liver Transplantation for Hepatocellular Carcinoma Living donor liver transplantation for hepatocellular carcinoma achieves better outcomes Chih-Che Lin, Chao-Long Chen Liver Transplantation
Review Article on Liver Transplantation for Hepatocellular Carcinoma Living donor liver transplantation for hepatocellular carcinoma achieves better outcomes Chih-Che Lin, Chao-Long Chen Liver Transplantation
HCC: Is it an oncological disease? - No
 June 13-15, 2013 Berlin, Germany Prof. Oren Shibolet Head of the Liver Unit, Department of Gastroenterology Tel-Aviv Sourasky Medical Center and Tel-Aviv University HCC: Is it an oncological disease? -
June 13-15, 2013 Berlin, Germany Prof. Oren Shibolet Head of the Liver Unit, Department of Gastroenterology Tel-Aviv Sourasky Medical Center and Tel-Aviv University HCC: Is it an oncological disease? -
Selection Criteria and Insertion of SIRT into HCC Treatment Guidelines
 Selection Criteria and Insertion of SIRT into HCC Treatment Guidelines 2 nd Asia Pacific Symposium on Liver- Directed Y-90 Microspheres Therapy 1st November 2014, Singapore Pierce Chow FRCSE PhD SIRT in
Selection Criteria and Insertion of SIRT into HCC Treatment Guidelines 2 nd Asia Pacific Symposium on Liver- Directed Y-90 Microspheres Therapy 1st November 2014, Singapore Pierce Chow FRCSE PhD SIRT in
Hepatocellular carcinoma: when is liver transplantation oncologically futile?
 Review Article Hepatocellular carcinoma: when is liver transplantation oncologically futile? André Viveiros 1, Heinz Zoller 1, Armin Finkenstedt 2 1 Department of Medicine I, Medical University Innsbruck,
Review Article Hepatocellular carcinoma: when is liver transplantation oncologically futile? André Viveiros 1, Heinz Zoller 1, Armin Finkenstedt 2 1 Department of Medicine I, Medical University Innsbruck,
Hepatocellular Carcinoma: A major global health problem. David L. Wood, MD Interventional Radiology Banner Good Samaritan Medical Center
 Hepatocellular Carcinoma: A major global health problem David L. Wood, MD Interventional Radiology Banner Good Samaritan Medical Center Hepatocellular Carcinoma WORLDWIDE The #2 Cancer Killer Overall cancer
Hepatocellular Carcinoma: A major global health problem David L. Wood, MD Interventional Radiology Banner Good Samaritan Medical Center Hepatocellular Carcinoma WORLDWIDE The #2 Cancer Killer Overall cancer
Worldwide Causes of HCC
 Approach to HCV Treatment in Patients with HCC Mark W. Russo, MD, MPH, FACG Carolinas HealthCare System Charlotte Worldwide Causes of HCC 60% 50% 40% 30% 20% 10% 0% 54% 31% 15% Hepatitis B Hepatitis C
Approach to HCV Treatment in Patients with HCC Mark W. Russo, MD, MPH, FACG Carolinas HealthCare System Charlotte Worldwide Causes of HCC 60% 50% 40% 30% 20% 10% 0% 54% 31% 15% Hepatitis B Hepatitis C
TREATMENT FOR HCC AND CHOLANGIOCARCINOMA. Shawn Pelletier, MD
 TREATMENT FOR HCC AND CHOLANGIOCARCINOMA Shawn Pelletier, MD Treatment for HCC Treatment strategies Curative first line therapy Thermal ablation vs Resection vs Transplant Other first line therapies TACE
TREATMENT FOR HCC AND CHOLANGIOCARCINOMA Shawn Pelletier, MD Treatment for HCC Treatment strategies Curative first line therapy Thermal ablation vs Resection vs Transplant Other first line therapies TACE
Total Tumor Volume and Alpha Fetoprotein for selection of transplant candidates. with hepatocellular carcinoma: a prospective validation
 Total Tumor Volume and Alpha Fetoprotein for selection of transplant candidates with hepatocellular carcinoma: a prospective validation Christian Toso 1, Glenda Meeberg 2, Roberto Hernandez-Alejandro 3,
Total Tumor Volume and Alpha Fetoprotein for selection of transplant candidates with hepatocellular carcinoma: a prospective validation Christian Toso 1, Glenda Meeberg 2, Roberto Hernandez-Alejandro 3,
Hepatocellular carcinoma (HCC) is a growing
 is a growing") AMERICAN ASSOCIATION FOR THE STUDY OFLIVERD I S E ASES REVIEW HEPATOLOGY, VOL. 67, NO. 1, 2018 Therapies for Patients With Hepatocellular Carcinoma Awaiting Liver Transplantation: A Systematic Review and
AMERICAN ASSOCIATION FOR THE STUDY OFLIVERD I S E ASES REVIEW HEPATOLOGY, VOL. 67, NO. 1, 2018 Therapies for Patients With Hepatocellular Carcinoma Awaiting Liver Transplantation: A Systematic Review and
Liver resection for HCC
 8 th LIVER INTEREST GROUP Annual Meeting Cape Town 2017 Liver resection for HCC Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre The liver is almost unique in that treatment of the
8 th LIVER INTEREST GROUP Annual Meeting Cape Town 2017 Liver resection for HCC Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre The liver is almost unique in that treatment of the
Screening for HCCwho,
 Screening for HCCwho, how and how often? Catherine Stedman Associate Professor of Medicine, University of Otago, Christchurch Gastroenterology Department, Christchurch Hospital HCC Global Epidemiology
Screening for HCCwho, how and how often? Catherine Stedman Associate Professor of Medicine, University of Otago, Christchurch Gastroenterology Department, Christchurch Hospital HCC Global Epidemiology
Hepatocellular Carcinoma: Can We Slow the Rising Incidence?
 Hepatocellular Carcinoma: Can We Slow the Rising Incidence? K.Rajender Reddy M.D. Professor of Medicine Director of Hepatology Medical Director of Liver Transplantation University of Pennsylvania Outline
Hepatocellular Carcinoma: Can We Slow the Rising Incidence? K.Rajender Reddy M.D. Professor of Medicine Director of Hepatology Medical Director of Liver Transplantation University of Pennsylvania Outline
Once considered a relative contraindication to
 Downstaging of Hepatocellular Cancer Before Liver Transplant: Long-Term Outcome Compared to Tumors Within Milan Criteria Francis Y. Yao, 1,2 Neil Mehta, 1 Jennifer Flemming, 1 Jennifer Dodge, 2 Bilal Hameed,
Downstaging of Hepatocellular Cancer Before Liver Transplant: Long-Term Outcome Compared to Tumors Within Milan Criteria Francis Y. Yao, 1,2 Neil Mehta, 1 Jennifer Flemming, 1 Jennifer Dodge, 2 Bilal Hameed,
6 Riunione Monotematica A.I.S.F NASH malattia epatica, oncologica e cardiovascolare
 6 Riunione Monotematica A.I.S.F. 2015 NASH malattia epatica, oncologica e cardiovascolare Modena, 9 ottobre 2015 Massimo Colombo NAFLD e HCC: caratteristiche distintive Chairman Department of Liver, Kidney,
6 Riunione Monotematica A.I.S.F. 2015 NASH malattia epatica, oncologica e cardiovascolare Modena, 9 ottobre 2015 Massimo Colombo NAFLD e HCC: caratteristiche distintive Chairman Department of Liver, Kidney,
Surveillance for HCC Who, how Diagnosis of HCC Surveillance for HCC in Practice
 Surveillance for Hepatocellular Carcinoma Hashem B. El-Serag, MD, MPH Dan L. Duncan Professor of Medicine Chief, Gastroenterology and Hepatology Houston VA & Baylor College of Medicine Houston, TX Outline
Surveillance for Hepatocellular Carcinoma Hashem B. El-Serag, MD, MPH Dan L. Duncan Professor of Medicine Chief, Gastroenterology and Hepatology Houston VA & Baylor College of Medicine Houston, TX Outline
Delta-slope of alpha-fetoprotein improves the ability to select liver transplant patients with hepatocellular cancer
 DOI:10.1111/hpb.12486 HPB ORIGINAL ARTICLE Delta-slope of alpha-fetoprotein improves the ability to select liver transplant patients with hepatocellular cancer Quirino Lai 1,2, Milton Inostroza 3, Juan
DOI:10.1111/hpb.12486 HPB ORIGINAL ARTICLE Delta-slope of alpha-fetoprotein improves the ability to select liver transplant patients with hepatocellular cancer Quirino Lai 1,2, Milton Inostroza 3, Juan
Guidelines for SIRT in HCC An Evolution
 Guidelines for SIRT in HCC An Evolution 2 nd Asia Pacific Symposium on Liver- Directed Y-90 Microspheres Therapy 1st November 2014, Singapore The challenge of HCC Surgery is potentially curative in early
Guidelines for SIRT in HCC An Evolution 2 nd Asia Pacific Symposium on Liver- Directed Y-90 Microspheres Therapy 1st November 2014, Singapore The challenge of HCC Surgery is potentially curative in early
The Chronic Liver Disease Foundation (CLDF) and the International Coalition of Hepatology Education Providers (IC-HEP) present:
 and the International Coalition of Hepatology Education Providers (IC-HEP) present:") The Chronic Liver Disease Foundation (CLDF) and the International Coalition of Hepatology Education Providers (IC-HEP) present: Certified by: Provided by: Endorsed by: Hepatocellular Carcinoma HCC: Age
The Chronic Liver Disease Foundation (CLDF) and the International Coalition of Hepatology Education Providers (IC-HEP) present: Certified by: Provided by: Endorsed by: Hepatocellular Carcinoma HCC: Age
Liver Cancer: Diagnosis and Treatment Options
 Liver Cancer: Diagnosis and Treatment Options Fred Poordad, MD Chief, Hepatology University Transplant Center Professor of Medicine UT Health, San Antonio VP, Academic and Clinical Affairs, Texas Liver
Liver Cancer: Diagnosis and Treatment Options Fred Poordad, MD Chief, Hepatology University Transplant Center Professor of Medicine UT Health, San Antonio VP, Academic and Clinical Affairs, Texas Liver
Clinical Study Use of Adjuvant Sorafenib in Liver Transplant Recipients with High-Risk Hepatocellular Carcinoma
 Transplantation, Article ID 913634, 5 pages http://dx.doi.org/10.1155/2014/913634 Clinical Study Use of Adjuvant Sorafenib in Liver Transplant Recipients with High-Risk Hepatocellular Carcinoma Kirti Shetty,
Transplantation, Article ID 913634, 5 pages http://dx.doi.org/10.1155/2014/913634 Clinical Study Use of Adjuvant Sorafenib in Liver Transplant Recipients with High-Risk Hepatocellular Carcinoma Kirti Shetty,
Surgical management of HCC. Evangelos Prassas Hepatobiliary and Pancreatic Surgery / Liver Transplantation Kings College Hospital / London
 Surgical management of HCC Evangelos Prassas Hepatobiliary and Pancreatic Surgery / Liver Transplantation Kings College Hospital / London Global distribution of HCC and staging systems WEST 1. Italy (Milan,
Surgical management of HCC Evangelos Prassas Hepatobiliary and Pancreatic Surgery / Liver Transplantation Kings College Hospital / London Global distribution of HCC and staging systems WEST 1. Italy (Milan,
The Regulatory Alphabet: CMS, OPTN, HRSA, SRTR, UNOS And Monitoring of Transplant Outcomes
 The Regulatory Alphabet: CMS, OPTN, HRSA, SRTR, UNOS And Monitoring of Transplant Outcomes John Paul Roberts M.D. University of California San Francisco NONE Disclosures Outcome Monitoring Outcome monitoring
The Regulatory Alphabet: CMS, OPTN, HRSA, SRTR, UNOS And Monitoring of Transplant Outcomes John Paul Roberts M.D. University of California San Francisco NONE Disclosures Outcome Monitoring Outcome monitoring
Liver Transplantation
 Liver Transplantation Dr Mathew Jacob - MRCS FRCS CCT (UK) Lead Consultant HPB/Transplant Surgeon Aster Integrated Liver Care Program AsterMedcity, kochi, kerala, India mathew@transplantationliver.com
Liver Transplantation Dr Mathew Jacob - MRCS FRCS CCT (UK) Lead Consultant HPB/Transplant Surgeon Aster Integrated Liver Care Program AsterMedcity, kochi, kerala, India mathew@transplantationliver.com
Analysis of prognostic factors of more/equal to10 years of survival for liver cancer patients after liver transplantation
 Journal of Cancer Research and Clinical Oncology (2018) 144:2465 2474 https://doi.org/10.1007/s00432-018-2756-8 ORIGINAL ARTICLE CLINICAL ONCOLOGY Analysis of prognostic factors of more/equal to10 years
Journal of Cancer Research and Clinical Oncology (2018) 144:2465 2474 https://doi.org/10.1007/s00432-018-2756-8 ORIGINAL ARTICLE CLINICAL ONCOLOGY Analysis of prognostic factors of more/equal to10 years
Review Article Liver Transplantation for Hepatocellular Carcinoma beyond Milan Criteria: Multidisciplinary Approach to Improve Outcome
 ISRN Hepatology, Article ID 706945, 25 pages http://dx.doi.org/10.1155/2014/706945 Review Article Liver Transplantation for Hepatocellular Carcinoma beyond Milan Criteria: Multidisciplinary Approach to
ISRN Hepatology, Article ID 706945, 25 pages http://dx.doi.org/10.1155/2014/706945 Review Article Liver Transplantation for Hepatocellular Carcinoma beyond Milan Criteria: Multidisciplinary Approach to
POST TRANSPLANT OUTCOMES IN PSC
 POST TRANSPLANT OUTCOMES IN PSC Kidist K. Yimam, MD Medical Director, Autoimmune Liver Disease Program Division of Hepatology and Liver Transplantation California Pacific Medical Center (CPMC) PSC Partners
POST TRANSPLANT OUTCOMES IN PSC Kidist K. Yimam, MD Medical Director, Autoimmune Liver Disease Program Division of Hepatology and Liver Transplantation California Pacific Medical Center (CPMC) PSC Partners
Paul Martin MD FACG. University of Miami
 Paul Martin MD FACG University of Miami 1 Liver cirrhosis of any cause Chronic C o c hepatitis epat t s B Risk increases with Male gender Age Diabetes Smoking ~5% increase in HCV-related HCC between 1991-28
Paul Martin MD FACG University of Miami 1 Liver cirrhosis of any cause Chronic C o c hepatitis epat t s B Risk increases with Male gender Age Diabetes Smoking ~5% increase in HCV-related HCC between 1991-28
Liver Transplantation for Cholangiocarcinoma. John McCall Division of Surgery Dunedin School of Medicine University of Otago
 Liver Transplantation for Cholangiocarcinoma John McCall Division of Surgery Dunedin School of Medicine University of Otago Primary Liver Cancer Hepatocellular carcinoma Hepatoblastoma Cholangiocarcinoma
Liver Transplantation for Cholangiocarcinoma John McCall Division of Surgery Dunedin School of Medicine University of Otago Primary Liver Cancer Hepatocellular carcinoma Hepatoblastoma Cholangiocarcinoma
3 Workshop on HCV THERAPY ADVANCES New Antivirals in Clinical Practice
 3 Workshop on HCV THERAPY ADVANCES New Antivirals in Clinical Practice Rome, 13 December 2013 Management and monitoring of HCC in the future era of DAA s Prof. Massimo Colombo Chairman Department of Liver,
3 Workshop on HCV THERAPY ADVANCES New Antivirals in Clinical Practice Rome, 13 December 2013 Management and monitoring of HCC in the future era of DAA s Prof. Massimo Colombo Chairman Department of Liver,
Cases: Treatment of Hepatitis C in Patients with Cirrhosis and Advanced Liver Disease
 Slide 1 of 20 Cases: Treatment of Hepatitis C in Patients with Cirrhosis and Advanced Liver Disease Kenneth E. Sherman, MD, PhD Gould Professor of Medicine Director, Division of Digestive Diseases University
Slide 1 of 20 Cases: Treatment of Hepatitis C in Patients with Cirrhosis and Advanced Liver Disease Kenneth E. Sherman, MD, PhD Gould Professor of Medicine Director, Division of Digestive Diseases University
The impact of the treatment of HCV in developing Hepatocellular Carcinoma
 The impact of the treatment of HCV in developing Hepatocellular Carcinoma Paul Y Kwo, MD Professor of Medicine Medical Director, Liver Transplantation Gastroenterology/Hepatology Division Indiana University
The impact of the treatment of HCV in developing Hepatocellular Carcinoma Paul Y Kwo, MD Professor of Medicine Medical Director, Liver Transplantation Gastroenterology/Hepatology Division Indiana University
Hepatocellular Carcinoma Recurrence After Liver Transplantation: an Analysis of Risk Factors and Incidence from Oregon Health & Science University
 Portland State University PDXScholar University Honors Theses University Honors College 2016 Hepatocellular Carcinoma Recurrence After Liver Transplantation: an Analysis of Risk Factors and Incidence from
Portland State University PDXScholar University Honors Theses University Honors College 2016 Hepatocellular Carcinoma Recurrence After Liver Transplantation: an Analysis of Risk Factors and Incidence from
Department of Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
 ORIGINAL ARTICLE pissn -575 eissn -79 https://doi.org/1.17/astr.1.95..111 Annals of Surgical Treatment and Research Clinical usefulness of transarterial chemoembolization response prior to liver transplantation
ORIGINAL ARTICLE pissn -575 eissn -79 https://doi.org/1.17/astr.1.95..111 Annals of Surgical Treatment and Research Clinical usefulness of transarterial chemoembolization response prior to liver transplantation
HEPATOCELLULAR CARCINOMA: AN OVERVIEW
 HEPATOCELLULAR CARCINOMA: AN OVERVIEW John K. Olynyk Head, Department of Gastroenterology & Hepatology Fiona Stanley Fremantle Hospital Group Dean of Research, Edith Cowan University RISING MORTALITY OF
HEPATOCELLULAR CARCINOMA: AN OVERVIEW John K. Olynyk Head, Department of Gastroenterology & Hepatology Fiona Stanley Fremantle Hospital Group Dean of Research, Edith Cowan University RISING MORTALITY OF
Liver transplantation for hepatocellular carcinoma: pre-transplant considerations and post-transplant management
 Review Article Page 1 of 9 Liver transplantation for hepatocellular carcinoma: pre-transplant considerations and post-transplant management Vladimir Marquez Division of Gastroenterology, University of
Review Article Page 1 of 9 Liver transplantation for hepatocellular carcinoma: pre-transplant considerations and post-transplant management Vladimir Marquez Division of Gastroenterology, University of
Selection of patients of hepatocellular carcinoma beyond the Milan criteria for liver transplantation
 Title Selection of patients of hepatocellular carcinoma beyond the Milan criteria for liver transplantation Author(s) Chan, SC; Fan, ST Citation Hepatobiliary Surgery and Nutrition, 2013, v. 2 n. 2, p.
Title Selection of patients of hepatocellular carcinoma beyond the Milan criteria for liver transplantation Author(s) Chan, SC; Fan, ST Citation Hepatobiliary Surgery and Nutrition, 2013, v. 2 n. 2, p.
HCC surgical approach: resection and transplantation indications and outcome
 SAMO, Friday 15th April 2011 Workshop on Primary liver tumors HCC surgical approach: resection and transplantation indications and outcome Gilles Mentha University Hospital of Geneva Hepatocellular Carcinoma
SAMO, Friday 15th April 2011 Workshop on Primary liver tumors HCC surgical approach: resection and transplantation indications and outcome Gilles Mentha University Hospital of Geneva Hepatocellular Carcinoma
Hepatitis Alert: Management of Patients With HCV Who Have Achieved SVR
 Hepatitis Alert: Management of Patients With HCV Who Have Achieved SVR This program is supported by educational grants from AbbVie, Gilead Sciences, and Merck About These Slides Please feel free to use,
Hepatitis Alert: Management of Patients With HCV Who Have Achieved SVR This program is supported by educational grants from AbbVie, Gilead Sciences, and Merck About These Slides Please feel free to use,
An Update on Hepatocellular Carcinoma. Ed Gane NZ Liver Transplant Unit
 An Update on Hepatocellular Carcinoma Ed Gane NZ Liver Transplant Unit Hepatocellular Carcinoma has a High Burden of Disease APSCVIR March 2018 Lung Liver Colon/Rectal Stomach Breast Cervix Uteri Esophagus
An Update on Hepatocellular Carcinoma Ed Gane NZ Liver Transplant Unit Hepatocellular Carcinoma has a High Burden of Disease APSCVIR March 2018 Lung Liver Colon/Rectal Stomach Breast Cervix Uteri Esophagus
Hepatocellular Carcinoma (HCC): Who Should be Screened and How Do We Treat? Tom Vorpahl MSN, RN, ACNP-BC
: Who Should be Screened and How Do We Treat? Tom Vorpahl MSN, RN, ACNP-BC") Hepatocellular Carcinoma (HCC): Who Should be Screened and How Do We Treat? Tom Vorpahl MSN, RN, ACNP-BC Objectives Identify patient risk factors for hepatocellular carcinoma (HCC) Describe strategies
Hepatocellular Carcinoma (HCC): Who Should be Screened and How Do We Treat? Tom Vorpahl MSN, RN, ACNP-BC Objectives Identify patient risk factors for hepatocellular carcinoma (HCC) Describe strategies
Increasing Trends in Transplantation of HCV-positive Livers into Uninfected Recipients
 Accepted Manuscript Increasing Trends in Transplantation of HCV-positive Livers into Uninfected Recipients George Cholankeril, MD, Andrew A. Li, MD, Brittany B. Dennis, PhD, Alice E. Toll, MS, Donghee
Accepted Manuscript Increasing Trends in Transplantation of HCV-positive Livers into Uninfected Recipients George Cholankeril, MD, Andrew A. Li, MD, Brittany B. Dennis, PhD, Alice E. Toll, MS, Donghee
Long-term Clinical Outcomes and Risk of Hepatocellular Carcinoma in Chronic Hepatitis B Patients with HBsAg Seroclearance
 Long-term Clinical Outcomes and Risk of Hepatocellular Carcinoma in Chronic Hepatitis B Patients with HBsAg Seroclearance Gi-Ae Kim, Han Chu Lee *, Danbi Lee, Ju Hyun Shim, Kang Mo Kim, Young-Suk Lim,
Long-term Clinical Outcomes and Risk of Hepatocellular Carcinoma in Chronic Hepatitis B Patients with HBsAg Seroclearance Gi-Ae Kim, Han Chu Lee *, Danbi Lee, Ju Hyun Shim, Kang Mo Kim, Young-Suk Lim,
HCV care after cure. This program is supported by educational grants from
 HCV care after cure This program is supported by educational grants from Raffaele Bruno,MD Department of Infectious Diseases, Hepatology Outpatients Unit University of Pavia Fondazione IRCCS Policlinico
HCV care after cure This program is supported by educational grants from Raffaele Bruno,MD Department of Infectious Diseases, Hepatology Outpatients Unit University of Pavia Fondazione IRCCS Policlinico
PATIENTS AND METHODS. Data Source
 LIVER TRANSPLANTATION 20:1045 1056, 2014 ORIGINAL ARTICLE Waiting Time Predicts Survival After Liver Transplantation for Hepatocellular Carcinoma: A Cohort Study Using the United Network for Organ Sharing
LIVER TRANSPLANTATION 20:1045 1056, 2014 ORIGINAL ARTICLE Waiting Time Predicts Survival After Liver Transplantation for Hepatocellular Carcinoma: A Cohort Study Using the United Network for Organ Sharing
Treatment of Hepatocellular Carcinoma. Andrew J. Muir, MD MHS Division of Gastroenterology Duke University Medical Center
 Treatment of Hepatocellular Carcinoma Andrew J. Muir, MD MHS Division of Gastroenterology Duke University Medical Center Epidemiology of HCC: world The 5 th most common cancer worldwide > 500, 000 new
Treatment of Hepatocellular Carcinoma Andrew J. Muir, MD MHS Division of Gastroenterology Duke University Medical Center Epidemiology of HCC: world The 5 th most common cancer worldwide > 500, 000 new
Management. Chapter 11. Primary Author. Contributing Authors. University of Toronto & University of Ottawa. Illustrators & figure contributors
 Chapter 11 Primary Author Donald G. Mitchell Thomas Jefferson University Contributing Authors Victoria Chernyak Ania Z. Kielar Yuko Kono Claude B. Sirlin Montefiore Medical Center University of Toronto
Chapter 11 Primary Author Donald G. Mitchell Thomas Jefferson University Contributing Authors Victoria Chernyak Ania Z. Kielar Yuko Kono Claude B. Sirlin Montefiore Medical Center University of Toronto
Osseous Metastases Missed by Bone Scan in Hepatocellular Carcinoma: A Retrospective Analysis
 Osseous Metastases Missed by Bone Scan in Hepatocellular Carcinoma: A Retrospective Analysis Lauren Ferrante, MD ICCR rotation: IRB protocol November 26, 2008 A. Study Background, Rationale, and Objectives
Osseous Metastases Missed by Bone Scan in Hepatocellular Carcinoma: A Retrospective Analysis Lauren Ferrante, MD ICCR rotation: IRB protocol November 26, 2008 A. Study Background, Rationale, and Objectives
Patient Selection for Surgery in RCC with Thrombus. E. Jason Abel, M.D.
 Patient Selection for Surgery in RCC with Thrombus E. Jason Abel, M.D. RCC with venous invasion Venous invasion occurs in ~10% of RCC Surgery more complex Increased risk for morbidity Thrombus may be confined
Patient Selection for Surgery in RCC with Thrombus E. Jason Abel, M.D. RCC with venous invasion Venous invasion occurs in ~10% of RCC Surgery more complex Increased risk for morbidity Thrombus may be confined
Natural History and Treatment Trends in Hepatocellular Carcinoma Subtypes: Insights From a National Cancer Registry
 2015;112:872 876 Natural History and Treatment Trends in Hepatocellular Carcinoma Subtypes: Insights From a National Cancer Registry PETER L. JERNIGAN, MD, KOFFI WIMA, MS, DENNIS J. HANSEMAN, PhD, RICHARD
2015;112:872 876 Natural History and Treatment Trends in Hepatocellular Carcinoma Subtypes: Insights From a National Cancer Registry PETER L. JERNIGAN, MD, KOFFI WIMA, MS, DENNIS J. HANSEMAN, PhD, RICHARD
In-situ v Normothermic Regional Perfusion for Abdominal Organs
 In-situ v Normothermic Regional Perfusion for Abdominal Organs ANGEL RUIZ M.D. DONATION AND TRANSPLNAT COORDINATION UNIT MEDICAL DIRECTION HOSPITAL CLÍNIC DE BARCELONA Introduction Donation after circulatory
In-situ v Normothermic Regional Perfusion for Abdominal Organs ANGEL RUIZ M.D. DONATION AND TRANSPLNAT COORDINATION UNIT MEDICAL DIRECTION HOSPITAL CLÍNIC DE BARCELONA Introduction Donation after circulatory
Prognosis of Hepatocellular Carcinoma after Liver Transplantation: Comparative Analysis with Partial Hepatectomy
 Journal of Pathology and Translational Medicine 2017; 51: 79-86 ORIGINAL ARTICLE Prognosis of Hepatocellular Carcinoma after Liver Transplantation: Comparative Analysis with Partial Hepatectomy Kyuho Lee
Journal of Pathology and Translational Medicine 2017; 51: 79-86 ORIGINAL ARTICLE Prognosis of Hepatocellular Carcinoma after Liver Transplantation: Comparative Analysis with Partial Hepatectomy Kyuho Lee
How to apply HCC prediction models to practice?
 How to apply HCC prediction models to practice? Department of Internal Medicine, Keimyung University School of Medicine Woo Jin Chung HCC prediction models 독특하게간세포암환자들의생존은암의진행상태뿐아니라기저간기능의중증정도에영향을받는특성이있다.
How to apply HCC prediction models to practice? Department of Internal Medicine, Keimyung University School of Medicine Woo Jin Chung HCC prediction models 독특하게간세포암환자들의생존은암의진행상태뿐아니라기저간기능의중증정도에영향을받는특성이있다.
In early but unresectable hepatocellular carcinoma (HCC),
,") Journal of Nuclear Medicine, published on April 16, 2009 as doi:10.2967/jnumed.108.060574 Prediction of Tumor Recurrence by F-FDG PET in Liver Transplantation for Hepatocellular Carcinoma Jeong Won Lee
Journal of Nuclear Medicine, published on April 16, 2009 as doi:10.2967/jnumed.108.060574 Prediction of Tumor Recurrence by F-FDG PET in Liver Transplantation for Hepatocellular Carcinoma Jeong Won Lee
Michał Grąt Oskar Kornasiewicz Zbigniew Lewandowski Wacław Hołówko Karolina Grąt Konrad Kobryń Waldemar Patkowski Krzysztof Zieniewicz Marek Krawczyk
 World J Surg (2014) 38:2698 2707 DOI 10.1007/s00268-014-2647-3 Combination of Morphologic Criteria and a-fetoprotein in Selection of Patients With Hepatocellular Carcinoma for Liver Transplantation Minimizes
World J Surg (2014) 38:2698 2707 DOI 10.1007/s00268-014-2647-3 Combination of Morphologic Criteria and a-fetoprotein in Selection of Patients With Hepatocellular Carcinoma for Liver Transplantation Minimizes
Learning Objectives. After attending this presentation, participants will be able to:
 Learning Objectives After attending this presentation, participants will be able to: Describe HCV in 2015 Describe how to diagnose advanced liver disease and cirrhosis Identify the clinical presentation
Learning Objectives After attending this presentation, participants will be able to: Describe HCV in 2015 Describe how to diagnose advanced liver disease and cirrhosis Identify the clinical presentation
Hepatocellular Carcinoma Surveillance
 Amit G. Singal, MD, MS Hepatocellular Carcinoma Surveillance Postgraduate Course: Challenges in Management of Common Liver Diseases 308 1 Patient Case 69 year-old otherwise healthy male with compensated
Amit G. Singal, MD, MS Hepatocellular Carcinoma Surveillance Postgraduate Course: Challenges in Management of Common Liver Diseases 308 1 Patient Case 69 year-old otherwise healthy male with compensated
Geographic Differences in Event Rates by Model for End-Stage Liver Disease Score
 American Journal of Transplantation 2006; 6: 2470 2475 Blackwell Munksgaard C 2006 The Authors Journal compilation C 2006 The American Society of Transplantation and the American Society of Transplant
American Journal of Transplantation 2006; 6: 2470 2475 Blackwell Munksgaard C 2006 The Authors Journal compilation C 2006 The American Society of Transplantation and the American Society of Transplant
MRI for HCC surveillance and reporting: LI-RADS. Donald G. Mitchell, M.D. Thomas Jefferson University Philadelphia, PA
 MRI for HCC surveillance and reporting: LI-RADS Donald G. Mitchell, M.D. Thomas Jefferson University Philadelphia, PA Cirrhotic Nodules Regenerative Nodule Atypical Nodule Hyperplastic Nodule Dysplastic
MRI for HCC surveillance and reporting: LI-RADS Donald G. Mitchell, M.D. Thomas Jefferson University Philadelphia, PA Cirrhotic Nodules Regenerative Nodule Atypical Nodule Hyperplastic Nodule Dysplastic
LIVER TRANSPLANTATION SURVIVAL IN HEPATOCELLULAR CARCINOMA. FUNDENI CLINICAL INSTITUTE EXPERIENCE
 THE PUBLISHING HOUSE OF THE ROMANIAN ACADEMY MEDICINE Research article LIVER TRANSPLANTATION SURVIVAL IN HEPATOCELLULAR CARCINOMA. FUNDENI CLINICAL INSTITUTE EXPERIENCE Gabriela ȘMIRA¹, Vladislav BRASOVEANU²,
THE PUBLISHING HOUSE OF THE ROMANIAN ACADEMY MEDICINE Research article LIVER TRANSPLANTATION SURVIVAL IN HEPATOCELLULAR CARCINOMA. FUNDENI CLINICAL INSTITUTE EXPERIENCE Gabriela ȘMIRA¹, Vladislav BRASOVEANU²,
The incidence of hepatocellular carcinoma
 AMERICAN ASSOCIATION FOR THE STUDY OFLIVERD I S E ASES REVIEWS HEPATOLOGY, VOL. 63, NO. 3, 2016 Reassessing the Boundaries of Liver Transplantation for Hepatocellular Carcinoma: Where Do We Stand With
AMERICAN ASSOCIATION FOR THE STUDY OFLIVERD I S E ASES REVIEWS HEPATOLOGY, VOL. 63, NO. 3, 2016 Reassessing the Boundaries of Liver Transplantation for Hepatocellular Carcinoma: Where Do We Stand With
Liver Transplantation: The End of the Road in Chronic Hepatitis C Infection
 University of Massachusetts Medical School escholarship@umms UMass Center for Clinical and Translational Science Research Retreat 2012 UMass Center for Clinical and Translational Science Research Retreat
University of Massachusetts Medical School escholarship@umms UMass Center for Clinical and Translational Science Research Retreat 2012 UMass Center for Clinical and Translational Science Research Retreat
Study Objective and Design
 Randomized, Open Label, Multicenter, Phase II Trial of Transcatheter Arterial Chemoembolization (TACE) Therapy in Combination with Sorafenib as Compared With TACE Alone in Patients with Hepatocellular
Randomized, Open Label, Multicenter, Phase II Trial of Transcatheter Arterial Chemoembolization (TACE) Therapy in Combination with Sorafenib as Compared With TACE Alone in Patients with Hepatocellular
Risk stratification in PBC
 Risk stratification in PBC Christophe Corpechot Reference Center for Inflammatory Biliary Diseases Saint-Antoine hospital, Paris, France What is currently known (background) PBC : chronic, progressive
Risk stratification in PBC Christophe Corpechot Reference Center for Inflammatory Biliary Diseases Saint-Antoine hospital, Paris, France What is currently known (background) PBC : chronic, progressive
How to evaluate tumor response? Yonsei University College of Medicine Kim, Beom Kyung
 How to evaluate tumor response? Yonsei University College of Medicine Kim, Beom Kyung End points in research for solid cancers Overall survival (OS) The most ideal one, but requires long follow-up duration
How to evaluate tumor response? Yonsei University College of Medicine Kim, Beom Kyung End points in research for solid cancers Overall survival (OS) The most ideal one, but requires long follow-up duration
Peri-Transplant Change in AFP Level: A Useful Predictor of Hepatocellular Carcinoma Recurrence Following Liver Transplantation
 ORIGINAL ARTICLE Cell Therapy & Organ Transplantation http://dx.doi.org/1.3346/jkms.16.31.7.149 J Korean Med Sci 16; 31: 149-154 Peri-Transplant Change in AFP Level: A Useful Predictor of Hepatocellular
ORIGINAL ARTICLE Cell Therapy & Organ Transplantation http://dx.doi.org/1.3346/jkms.16.31.7.149 J Korean Med Sci 16; 31: 149-154 Peri-Transplant Change in AFP Level: A Useful Predictor of Hepatocellular