Leeds, Grenville & Lanark Community Health Profile: Healthy Living, Chronic Diseases and Injury
|
|
|
- Ethelbert Daniels
- 5 years ago
- Views:
Transcription

1 Leeds, Grenville & Lanark Community Health Profile: Healthy Living, Chronic Diseases and Injury Executive Summary Contents: Defining income 2 Defining the data 3 Indicator summary 4 Glossary of indicators 8 Alcohol use 11 Community belonging 12 Dental insurance 13 Flu shot past 2-years 14 Folic acid 15 Food insecurity 16 Fruit & vegetable 17 High blood pressure 18 Life stress 19 Mammogram 20 Marijuana use 21 PAP test 22 Physical inactivity 23 Regular medical doctor 24 Smoking cigarettes 25 Work stress 26 Health 28 Mental health 29 Anxiety diagnosis 30 Asthma diagnosis 31 Diabetes diagnosis 32 Heart disease diagnosis 33 Mood disorder diagnosis 34 Injury 35 Injury (Fall) 36 Appendix 37 Data & Methodology 41 References 41 The focus of this report is to provide population level information about the healthrelated behaviours of the residents of Leeds, Grenville and Lanark (LGL), and the prevalence of associated chronic diseases and injury. These behaviours include: keeping physically fit, eating healthy foods, maintaining physical and mental health, maintaining oral health, managing life stress, and many others. These, in turn, can influence the risks for injuries, infections and chronic diseases. This report also presents health-related behaviours through the lens of health equity. The residents of LGL have differing opportunities to be healthy; at times due to their socio-economic situation. There is consistent evidence that people with the lowest incomes bear a heavier burden of illness and mortality 1,2. The report also explores the extent to which gender, age and urban/rural living are associated with health-related behaviours. Report data was collected from 2506 LGL residents aged 12+ years between 2009 and 2014 using combined cycles of the Canadian Community Health Survey (CCHS) 3. The results presented in the report indicate that individuals in the lowest income group were markedly different from individuals in the highest income group for 15 of the health indicators examined. Diagnoses of chronic diseases, smoking cigarettes, a weak sense of community belonging, a lack of dental insurance, food insecurity, and selfreported poor physical and mental health were all higher among individuals with low income. Women were more likely than men to be physically inactive, food insecure, report moderate to extreme life and work stress, and be injured due to a fall in the past 12- months. Men were more likely than women to report drinking in excess of low risk drinking guidelines, use of marijuana, smoke cigarettes, be injured in the past 12- months and be diagnosed with either diabetes and/or heart disease. Younger residents of LGL were more likely than older residents to report drinking in excess of low risk drinking guidelines, use of marijuana, be food insecure, have a weak sense of community belonging, and have suffered from an injury in the past 12- months. Older residents were more likely to report being physically inactive, not have dental insurance, smoke cigarettes, be diagnosed with a chronic disease such as diabetes, high blood pressure or heart disease, be injured from a fall in the past 12- months, and report fair or poor physical and mental health.
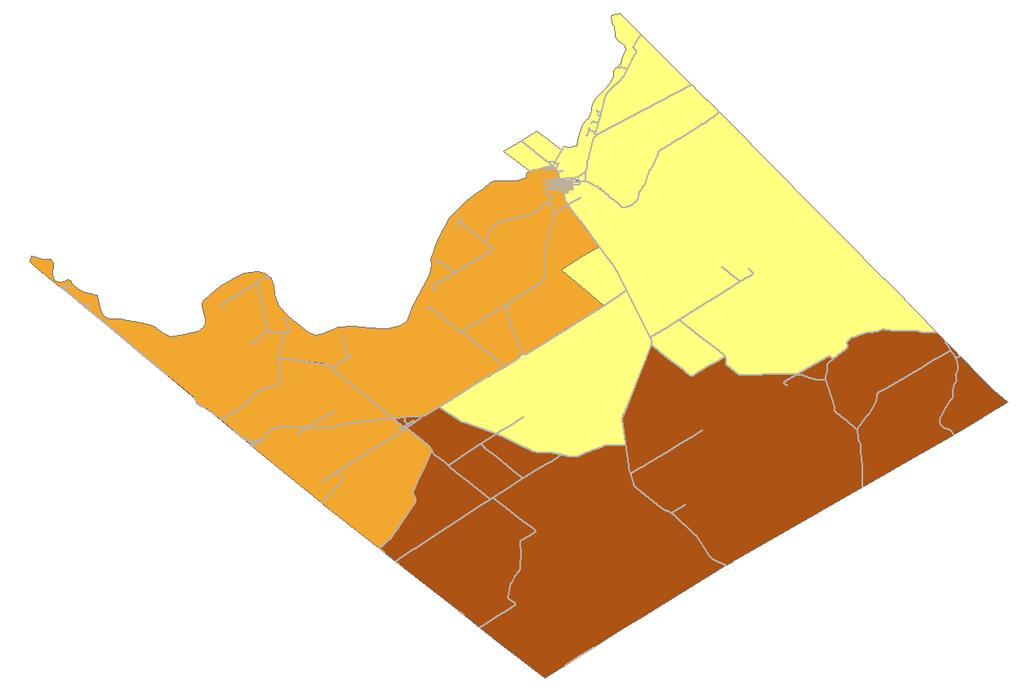
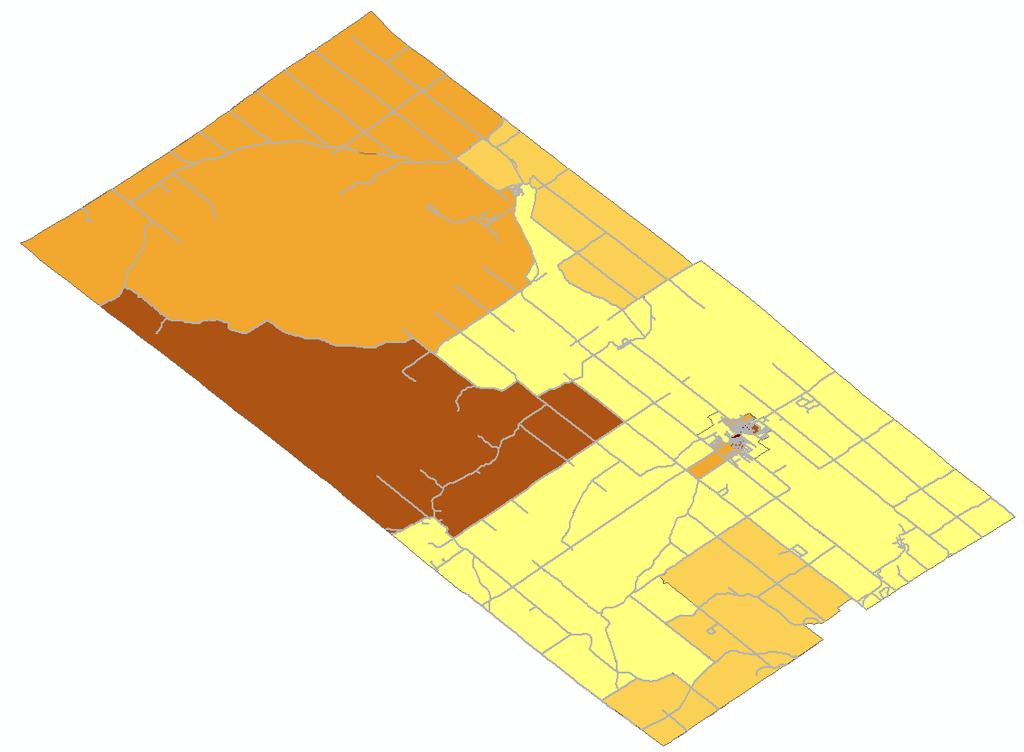
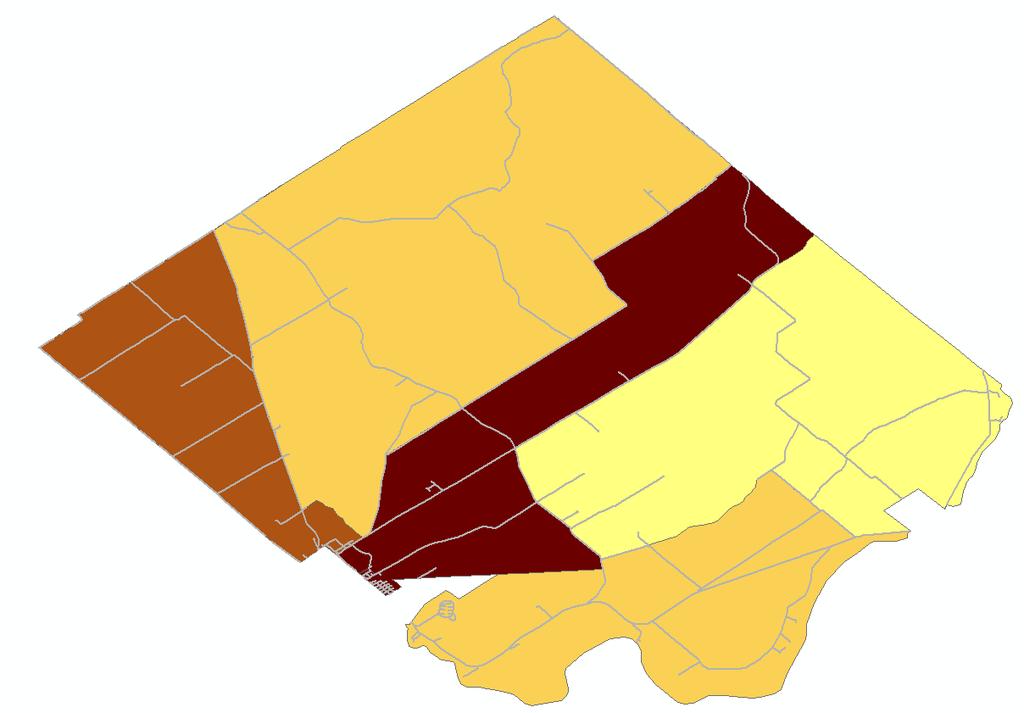
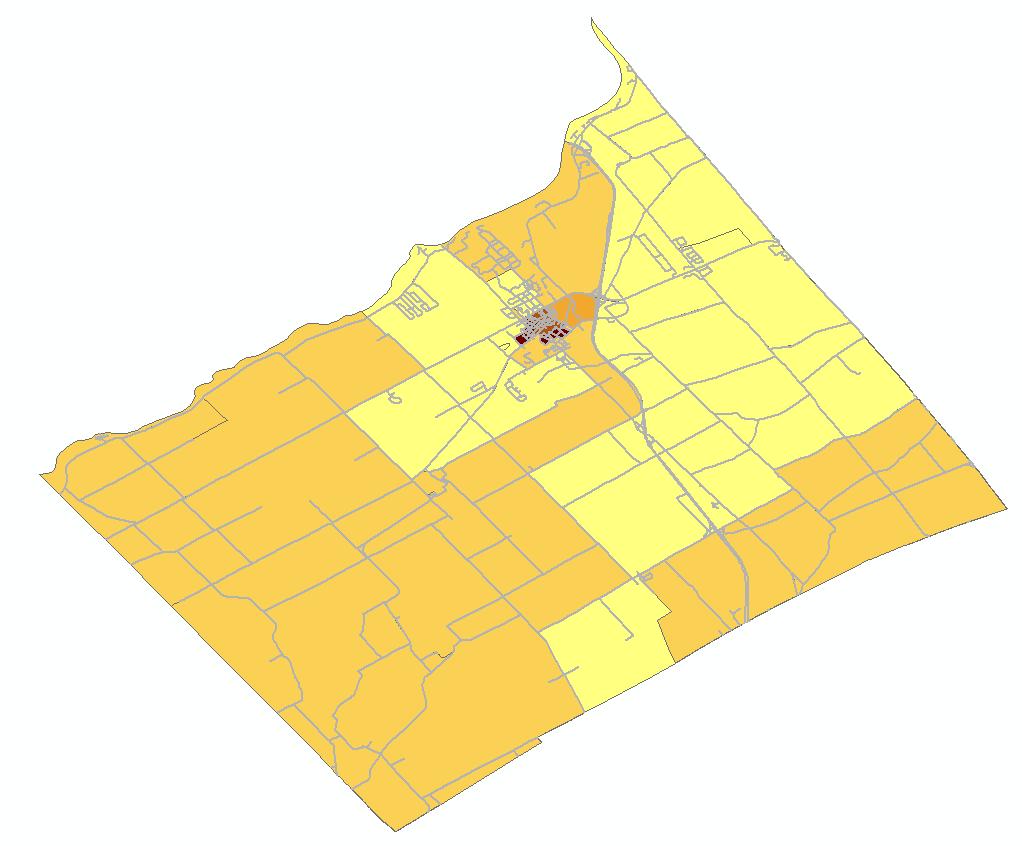
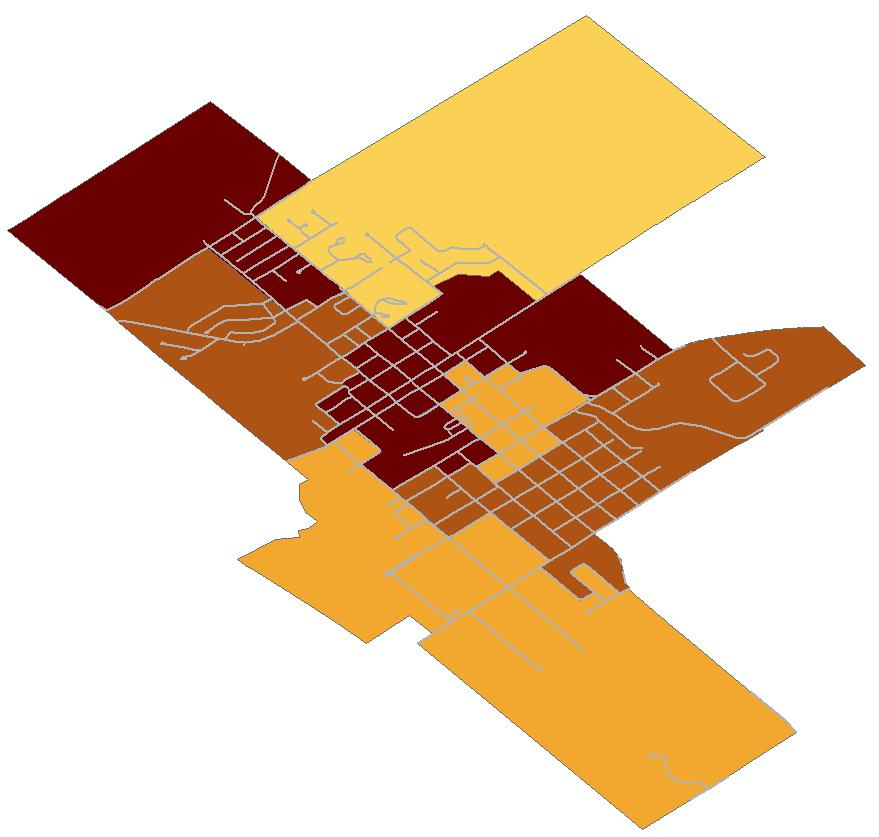
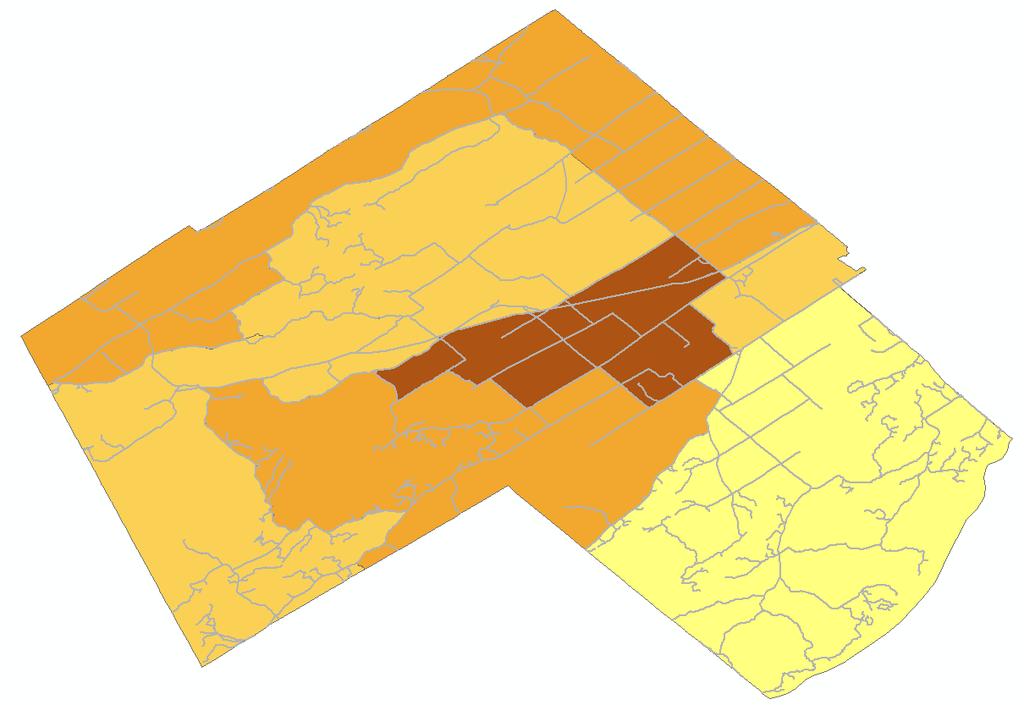
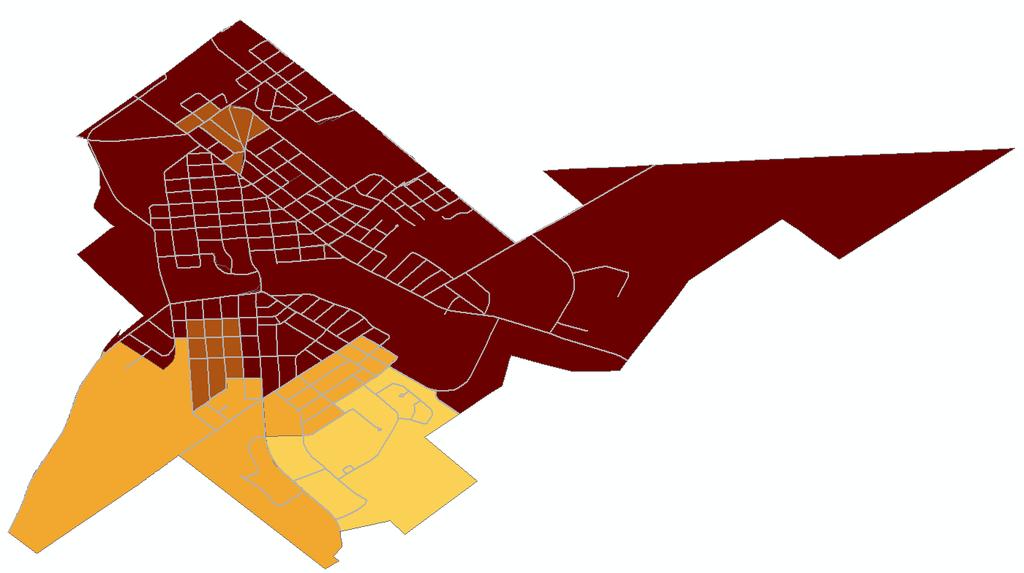
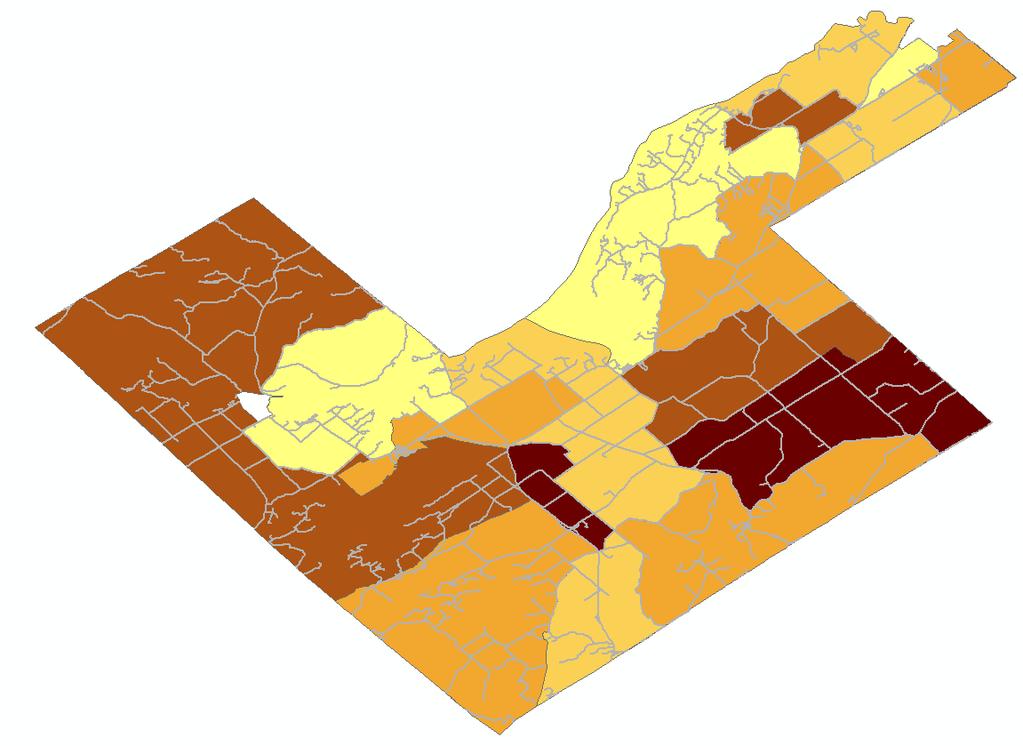
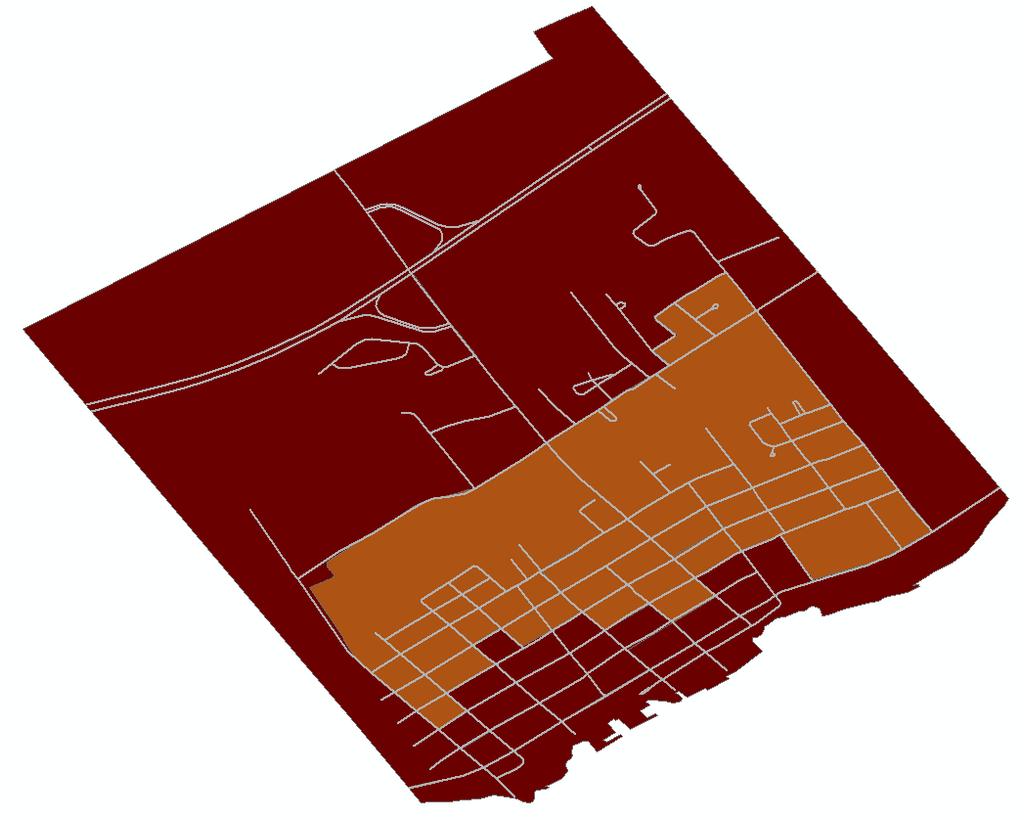
2 Defining Income Categories for the Analysis Income was provided as a variable in the CCHS database. The income variable was in Dissemination Area or DA format. The DA is a geographic measure created by Statistics Canada that represents a geographic area containing between 400 and 700 persons. The size of the DA can vary geographically depending upon the population density. An urban DA may only be a couple of city blocks in size, whereas a DA in a rural area may be hundreds of square kilometers in size. Mapping income by DA is the best measure we have to represent an actual neighbourhood. Figure 1 below represents income divided into five groups by DA for each neighbourhood in LGL (Please see the appendix for the five income groups by municipality). The five income groups were then collapsed to provide three income groups to increase the sample size in each. The groups represent the lowest ($0 $39,999), intermediate ($40,000 $79,999) and highest ($80,000+) income categorizations used for comparison purposes in the analysis. The number of individuals in each income group varied slightly for each variable analyzed as some of the individuals surveyed did not answer all survey questions. Figure 1: Income groups in LGL by Dissemination Area which is a proxy for neighbourhood. Page 2
3 Defining the Data Used in this Report Inequity and Inequality Leeds, Grenville & Lanark Community Health Profile: Healthy Living, Chronic Diseases and Injury Inequality and inequity are two different concepts and are well defined here 4 : The World Health Organization (WHO) defines a health inequality as any difference in the distribution of health status or health determinants between different population groups. Health inequalities can be attributed to free choice, biological variations, the physical environment, and factors beyond the control of the individuals concerned. For example, differences in physical capabilities between elderly and younger people in the population would be considered an inequality. In contrast, inequity is an ethical concept which reflects principles of social justice. Health inequities are defined as inequalities in which the outcome is unnecessary and avoidable as well as unjust and unfair. For example, differences in health care accessibility between socio-economic groups may be interpreted as an inequality as well as an inequity, while some differences in physical capabilities between elderly and younger people would not be considered an inequity as it is unavoidable. In general, differences due to biological variations, fully informed decisions to participate in higher risk behaviours, and chance are not considered inequities. Many would describe health inequalities across socioeconomic groups as unjust because they often reflect an unfair distribution of the social determinants of health. Health inequalities can be measured quantitatively while health inequities cannot. This is because identifying health inequities requires the use of judgment regarding the social justice of an inequality, which may depend on the causes of the inequality and the context of the local community. Better understanding of the causes and context of health inequalities can also help PHUs to better target interventions and advocate for necessary changes. This report will focus on quantitative measures of health inequalities. Identifying inequalities is a first and important step in the identification of inequities. Canadian Community Health Survey (CCHS) Data from the CCHS combined cycles provided the individual-level health information, for example: household income, alcohol use, smoking status, age, geography, etc. The CCHS is a national self reported survey of the Canadian population aged 12 and over at the health unit level. The CCHS makes use of a complex stratified and cluster sampling design to achieve representativeness. Excluded from the CCHS sampling frame are individuals living on Native Reserves and on Crown Lands, institutional residents, full-time members of the Canadian Forces, and residents of certain remote regions 5. Page 3
4 Summary of Health Inequality Related to Income The analysis presented in this report determined that some income, gender, age group and urban/rural health inequalities appear to exist within the Leeds, Grenville & Lanark District Health Unit s geographic boundaries (Tables 1, 2, 3 & 4). Table 1: The following self-reported indicators were associated with income. Indicator Low Income > High Income High Income > Low Income No Difference Diagnosis of an anxiety disorder Diagnosis of asthma Self-reported weak sense of community belonging Not having dental insurance Diagnosis of diabetes Not taking folic acid supplementation before last pregnancy Food insecurity Self rated fair to poor health Diagnosis of heart disease Diagnosis of high blood pressure Self rated fair to poor mental health Diagnosis of a mood disorder Physical Inactivity Not having a regular medical doctor Daily or occasional smoking Alcohol use above low risk drinking guidelines Never having a mammogram Never having a PAP test Not having a flu shot in past 2-years Less than 5 servings of daily fruit & vegetables Injury in past 12-months Injury due to fall in past 12-months Self rated moderate to extreme life stress Marijuana use in past 12-months Self rated moderate to extreme work stress Page 4
5 Summary of Inequality Related to Gender Table 2: The following self-reported indicators were associated with gender. Indicator Women > Men Men > Women No Difference Physical Inactivity Diagnosis of an anxiety disorder Diagnosis of asthma Self-reported weak sense of community belonging Food insecurity Alcohol use above low risk drinking guidelines Not having a flu shot in past 2- years Less than 5 servings of daily fruit & vegetables Marijuana use in past 12-months Not having a regular medical doctor Not having dental insurance Diagnosis of high blood pressure Self rated fair to poor mental health Self rated fair to poor health Injury due to fall in past 12- months Self rated moderate to extreme life stress Diagnosis of a mood disorder Self rated moderate to extreme work stress Daily or occasional smoking Diagnosis of diabetes Diagnosis of heart disease Injury in past 12-months Page 5
6 Summary of Inequality Related to Urban/Rural Living Table 3: The following self-reported indicators were associated with urban/rural living. Indicator Urban > Rural Rural > Urban No Difference Not having dental insurance Not taking folic acid supplementation before last pregnancy Alcohol use above low risk drinking guidelines Marijuana use in past 12-months Not having a flu shot in past 2-years Less than 5 servings of daily fruit & vegetables Never having a mammogram Never having a PAP test Diagnosis of high blood pressure Daily or occasional smoking Diagnosis of an anxiety disorder Self-reported weak sense of community belonging Diagnosis of diabetes Food insecurity Self rated fair to poor health Diagnosis of heart disease Self rated moderate to extreme life stress Self rated fair to poor mental health Diagnosis of a mood disorder Self rated moderate to extreme work stress Injury due to fall in past 12- months Physical Inactivity Not having a regular medical doctor Diagnosis of asthma Injury in past 12-months Page 6
7 Summary of Inequality Related to Age Table 4: The following self-reported indicators were associated age based on the trend by age group. Indicator Older > Younger Younger > Older No Difference Not having dental insurance Diagnosis of high blood pressure Physical Inactivity Not having a regular medical doctor Self rated moderate to extreme work stress Alcohol use above low risk drinking guidelines Self-reported weak sense of community belonging Not taking folic acid supplementation before last pregnancy Food insecurity Not having a flu shot in past 2- years Less than 5 servings of daily fruit & vegetables Diagnosis of an anxiety disorder Self rated moderate to extreme life stress Daily or occasional smoking Diagnosis of diabetes Self rated fair to poor health Diagnosis of heart disease Injury due to fall in past 12- months Self rated fair to poor mental health Diagnosis of a mood disorder Marijuana use in past 12-months Never having a mammogram Never having a PAP test Diagnosis of asthma Injury in past 12-months Page 7
8 Glossary of Indicators Alcohol use: Survey respondents were asked the average number of drinks consumed per day during the week prior to the interview. This variable was then calculated to determine if drinking behaviour was above low risk drinking guidelines set out by the Centre for Addiction and Mental Health (CAMH) 6. Anxiety disorder: Survey respondent were asked if they had been diagnosed with a phobia, obsessivecompulsive disorder or panic disorder by a health care professional, and if the diagnosis was expected to last for at least 6-months or had already lasted for 6-months or more. Asthma: Survey respondent were asked if they had been diagnosed with asthma by a health care professional, and if the diagnosis was expected to last for at least 6-months or had already lasted for 6- months or more. Community Belonging: This question dealt with aspects of social relationships and social well being. The respondent was asked to rate their sense of community belonging between very strong and very weak. The response categories of somewhat to very weak were combined to demonstrate a weak sense of community belonging. Dental Insurance: Survey respondents were asked if they had insurance that covered all or part of the cost of dental expenses. This could include government sponsored, employer sponsored or private plans. Diabetes: Survey respondents were asked if they had been diagnosed with diabetes by a health care professional, and if the diagnosis was expected to last for at least 6-months or had already lasted for 6- months or more. Excludes pre-diabetes responses. Flu Shot: Survey respondents were asked if they had ever had a flu shot and, if so, when the last one was. For the purposes of this report the interest was whether a respondent had a flu shot in the past 2-years. This question was part of a series around the use of health care services. Folic Acid Supplementation: This question was for recent mothers. Respondents were asked if they had taken a vitamin supplement containing folic acid prior to their last pregnancy and before they knew they were pregnant. Food Insecurity: This variable was based on a set of 18 questions and described the food security situation of the household in the previous 12 months. It captured three kinds of situations: 1- Food secure: No, or one, indication of difficulty with income-related food access. 2- Moderately food insecure: Indication of compromise in quality and/or quantity of food consumed. 3- Severely food insecure: Indication of reduced food intake and disrupted eating patterns. The response categories of moderate and severe were combined to demonstrate food insecurity. Fruit & Vegetable Consumption: This question classified the respondent based on the total number of times per day he/she ate fruits and vegetables but not the amount consumed. This indicator was used as a proxy for a healthy diet, which is related to the risk for chronic disease. Health Self Rated: This question dealt with health status. The respondent was asked to rate their health on a 5-point scale as being between excellent to poor. The response categories of fair and poor were combined to demonstrate poor self-rated health. Page 8 Leeds, Grenville & Lanark Community Health Profile: Healthy Living, Chronic Diseases and Injury
9 Glossary of Indicators (continued) Heart Disease: Survey respondent were asked if they had been diagnosed with heart disease by a health care professional, and if the diagnosis was expected to last for at least 6-months or had already lasted for 6-months or more. High Blood Pressure: Survey respondent were asked if they had been diagnosed with high blood pressure by a health care professional, and if the diagnosis was expected to last for at least 6-months or had already lasted for 6 -months or more. Injury: Survey respondents asked if they had sustained an injury in the past 12-months which was serious enough to limit their normal activities the day after the injury occurred. Injury From a Fall: Survey respondents asked if they had sustained an injury in the past 12-months which was serious enough to limit their normal activities the day after the injury occurred and if the injury was the result of a fall. Life Stress: This question dealt with the amount of perceived stress in a person s life. The respondent was asked to rate their life stress on a 5-point scale as being between not at all stressful and extremely stressful. The response categories of quite a bit and extreme were combined to demonstrate life stress. Mammogram: Female survey respondents aged 45+ years were asked if they had ever had a mammogram (breast x-ray). Marijuana Use: Survey respondents were asked if they had tried or used marijuana, cannabis or hashish in the 12 -months prior to the survey. Mental Health: This question dealt with mental health status. The respondent was asked to rate their mental health on a 5-point scale as being between excellent to poor. The response categories of fair and poor were combined to demonstrate poor mental health. Mood disorder: Survey respondents were asked if they had been diagnosed with depression, bipolar, mania or dysthymia by a health care professional, and if the diagnosis was expected to last for at least 6-months or had already lasted for 6-months or more. PAP Test: Female survey respondents aged 25+ years were asked if they had ever had a PAP smear test. Physical Activity: This variable classified respondents according to their pattern or regularity of leisure time physical activity lasting more than 15-minutes. The variable used physical activity not related to work. The variable categorized respondents as being active, moderately active or inactive based on their calculated total daily energy expenditure values. Regular MD: Survey respondents were asked if they had a regular medical doctor that they would go to when they were sick or needed advice about their health. Smoking status: Survey respondents were asked if they currently smoke daily, occasionally or not at all. Both daily and occasionally constituted smoking for the purposes of this report. Work Stress: This question dealt with the amount of perceived stress in a person s work life. The respondent was asked to rate their work stress on a 5-point scale as being between not at all stressful and extremely stressful. The response categories of quite a bit and extreme were combined to demonstrate work stress. Page 9 Leeds, Grenville & Lanark Community Health Profile: Healthy Living, Chronic Diseases and Injury
10 Healthy Living Indicators Page 10
. 8.2% within the lowest income group compared to 9.")
11 Alcohol Use Above Low Risk Drinking Guidelines 91.4% of the overall population in LGL that consumes alcohol reported drinking within the low risk drinking guidelines. 8.6% of the overall population reported having exceeded low risk drinking guidelines in the week prior to the survey (Figure 1). 8.2% within the lowest income group compared to 9.5% within the highest income group reported having exceeded low risk drinking guidelines (Figure 2). Men were more likely than women to report having exceeded low risk drinking guidelines in all income groups. However, women in the highest income group were more likely to engage in high risk alcohol use than women in the lowest income group (Figure 3). A higher proportion of individuals in the and year age group were more likely to report having exceeded low risk drinking guidelines (11.0%) than those in older age groups (6.8% - 7.4%) (Figure 4). Reports of exceeding low risk drinking guidelines were more common among men than women, among individuals in younger age groups and among those living in rural rather than urban settings. Individuals living in rural settings were more likely to report exceeding low risk drinking guidelines than those in urban settings (10.2% vs. 6.9%). Figure 1: Population distribution of individuals reporting having exceeded low risk drinking guidelines in LGL. Figure 2: Reporting having exceeded low risk drinking guidelines within each income group in LGL. Figure 3: Reporting having exceeded low risk drinking guidelines by income group and gender in LGL. Figure 4: Reporting having exceeded low risk drinking guidelines by age group in LGL. Page 11
12 Community Belonging 71.8% of the overall population in LGL reported having a somewhat strong to very strong sense of community belonging. 28.2% of the overall population reported having a somewhat weak to very weak sense of community belonging (Figure 5). 31.9% within the lowest income group compared to 23.4% within the highest income group reported having a somewhat to very weak sense of community belonging (Figure 6). Women were more likely than men to report having a somewhat to very weak sense of community belonging in the lowest and highest income groups (Figure 7). A higher proportion of individuals in the year age group (32.9%) reported having a somewhat to very weak sense of community belonging than those in the 65+ year age group (22.3%) (Figure 8). A higher proportion of individuals living in urban settings reported having a somewhat to very weak sense of community belonging than those in rural settings (28.9% vs. 26.3%). A higher proportion of individuals within the lowest income group reported having a somewhat to very weak sense of community belonging than individuals within the highest income group. A somewhat to very weak sense of community belonging was more common for younger populations and those living in urban rather than rural settings. Figure 5: Population distribution of individuals reporting having a weak sense of community belonging in LGL. Figure 6: Reporting having a weak sense of community belonging within each income group in LGL. Figure 7: Reporting having a weak sense of community belonging by income group and gender in LGL. Figure 8: Reporting having a weak sense of community belonging by age group in LGL. Page 12
.")
13 Dental Insurance 64.6% of the overall population in LGL reported having dental insurance. 35.4% of the overall population in LGL reported not having dental insurance (Figure 9). 65.1% of individuals within the lowest income group compared to 15.7% within the highest income group reported not having dental insurance (Figure 10). Men and women had an equal likelihood of reporting not having dental insurance in all income groups (Figure 11). A higher proportion of individuals in the 65+ year age group (55.5%) reported not having dental insurance than those in younger age groups (26.9% %) (Figure 12). A higher proportion of individuals living in urban settings reported not having dental insurance than those in rural settings (39.8% vs. 32.6%). A higher proportion of individuals within the lowest income group reported not having dental insurance than individuals within the highest income group. Reports of not having dental insurance were higher among individuals in older age groups and those living in urban compared to rural settings. Figure 9: Population distribution of individuals reporting not having dental insurance in LGL. Figure 10: Reporting not having dental insurance within each income group in LGL. Figure 11: Reporting not having dental insurance by income group and gender in LGL. Figure 12: Reporting not having dental insurance by age group in LGL. Page 13
14 Flu Shot (Past 2-Years) 70.3% of the overall population in LGL reported having a flu shot in the past 2-years. 29.7% of the overall population reported not having a flu shot in past 2-years (Figure 13). 26.3% within the lowest income group compared to 29.6% within the highest income group reported not having a flu shot in the past 2- years (Figure 14). Men were more likely than women to report not having a flu shot in the past 2-years in all income groups (Figure 15). A lower proportion of individuals in the 65+ year age group reported not having a flu shot in the past 2-years (8.9%) than those in the younger age groups (27.2% %) (Figure 16). Similar proportions of individuals living in rural and urban settings reported not having a flu shot in past 2-years (30.5% vs. 29.9%). Similar proportions of individuals within all income groups reported not having a flu shot in past 2-years. Reports of not having a flu shot in past 2- years were more common among men. Reports of not having a flu shot in the past 2 -years were higher for younger age groups and similar among individuals living in urban and rural settings. Figure 13: Population distribution of individuals reporting not having a flu shot in LGL. Figure 14: Reporting not having a flu shot within each income group in LGL. Figure 15: Reporting not having a flu shot by income group and gender in LGL. Figure 16: Reporting not having a flu shot by age group in LGL. Page 14
. 64.2% within the lowest income group compared to 39.")
15 Folic Acid Supplementation 56.1% of the overall female population aged 18 to 44 years in LGL reported taking folic acid before their last pregnancy. 43.9% of the overall female population reported not taking folic acid before their last pregnancy (Figure 17). 64.2% within the lowest income group compared to 39.9% within the highest income group reported not taking folic acid before their last pregnancy (Figure 18). A higher proportion of individuals in the year age group (85.6%) reported not taking folic acid supplementation before their last pregnancy than those in the year age group (40.2%) (Figure 19). A higher proportion of individuals living in urban settings reported not taking folic acid before their last pregnancy than those in rural settings (47.2% vs. 40.9%). A higher proportion of women within the lowest income group reported not taking folic acid than individuals within the highest income group. Reports of not taking folic acid were higher in the youngest age group. Reports of not taking folic acid were higher among individuals living in urban compared to rural settings. Figure 17: Population distribution of women reporting not taking folic acid in LGL. Figure 18: Reporting not taking folic acid within each income group in LGL. Figure 19: Reporting not taking folic acid by age group in LGL. Page 15
. Women were more likely than men to report being food insecure in the lowest and intermediate income groups (Figure 22).")
16 Food Insecurity 92.7% of the overall population in LGL reported being food secure. 7.3% of the population reported being food insecure (Figure 20). 19.2% within the lowest income group compared to 0.8% within the highest income group reported being food insecure (Figure 21). Women were more likely than men to report being food insecure in the lowest and intermediate income groups (Figure 22). A lower proportion of individuals in the 65+ year age group reported being food insecure (2.2%) than those in the younger age groups (10.5% - 7.6%) (Figure 23). A higher proportion of individuals living in urban settings reported being food insecure than those in rural settings (8.3% vs. 6.2%). A higher proportion of individuals within the lowest income group reported being food insecure than individuals in the highest income group. Reports of being food insecure were more common among younger age groups and among women than men. Reports of being food insecure were higher among individuals living in urban compared to rural settings. Figure 20: Population distribution of individuals reporting food insecurity in LGL. Figure 21: Reporting food insecurity within each income group in LGL. Figure 22: Reporting food insecurity by income group and gender in LGL. Figure 23: Reporting food insecurity by age group in LGL. Page 16
. 61.3% within the lowest income group and 60.")
17 Fruit & Vegetable Consumption (< 5 Servings per Day) 39.8% of the overall population in LGL reported eating 5 servings or more of fruit and vegetables daily. 60.2% of the overall population reported eating less than 5 servings of fruit and vegetables daily (Figure 24). 61.3% within the lowest income group and 60.0% within the highest income group reported eating less than 5 servings of fruit and vegetables daily (Figure 25). Men were more likely than women to report eating less than 5 servings of fruit and vegetables daily in all income groups (Figure 26). Similar proportions of individuals in the two youngest age groups reported eating less than 5 servings of fruit and vegetables daily. The proportion was highest in the year age group (64.8%) and lowest in the 65+ year age group (51.5%) (Figure 27). Similar proportions of individuals living in urban and rural settings reported eating less than 5 servings of fruit and vegetables daily (60.4% vs. 59.8%). Figure 24: Population distribution of individuals reporting eating < 5 servings of fruit and vegetables daily in LGL. Similar proportions of individuals within all income groups reported eating less than 5 servings of fruit and vegetables daily. Reports of low fruit and vegetable consumption were more common among men than women and among the year age group. Figure 25: Reporting eating < 5 servings of fruit and vegetables daily within each income group in LGL. Figure 26: Reporting eating < 5 servings of fruit and vegetables daily by income group and gender in LGL. Figure 27: Reporting eating < 5 servings of fruit and vegetables daily by age group in LGL. Page 17
18 High Blood Pressure Diagnosis 78.9% of the overall population in LGL self-reported having a diagnosis of normal blood pressure. 20.8% of the overall population self-reported a diagnosis of high blood pressure (Figure 28). 30.0% within the lowest income group compared to 16.3% within the highest income group self-reported a diagnosis of high blood pressure (Figure 29). Having a diagnosis of high blood pressure was higher among men in the lowest income group than women and the reverse was seen for the intermediate income group (Figure 30). A higher proportion of individuals in the 65+ year age group (45.6%) reported a diagnosis of high blood pressure than those in younger age groups (2.2% %) (Figure 31). A slightly higher proportion of individuals living in urban settings reported a diagnosis of high blood pressure than those in rural settings (22.0% vs. 19.7%). A higher proportion of individuals within the lowest income group reported having a diagnosis of high blood pressure than individuals within the highest income group. Reports of high blood pressure were higher in older age groups and similar for those living in urban compared to rural settings. Figure 28: Population distribution of individuals reporting high blood pressure in LGL. Figure 29: Reporting having high blood pressure within each income group in LGL. Figure 30: Reporting having high blood pressure by income group and gender in LGL. Figure 31: Reporting high blood pressure by age group in LGL. Page 18
19 Life Stress (Self Rated) 77.9% of the overall population in LGL self-reported little to no life stress. 22.1% of the overall population self-reported quite a bit or extreme life stress (Figure 32). 31.5% within the highest income group compared to 38.7% within the intermediate income group and 33.9% within the lowest income group self-reported a quite a bit to extreme life stress (Figure 33). Men were more likely to self report quite a bit or extreme life stress than women in all income groups (Figure 34). Quite a bit to extreme life stress increased with age group (18.4% %) until dropping off at the 65+ year age group (11.4%) (Figure 35). A slightly higher proportion of individuals living in urban settings reported having quite a bit or extreme life stress than those in rural settings (23.6% vs. 21.2%). A higher proportion of individuals in the intermediate income group reported quite a bit or extreme life stress. Reports of life stress were more common among men than women. Reports of quite a bit to extreme life stress increased with age and then decreased in the 65+ year age group. Higher proportions of individuals living in urban settings reported quite a bit to extreme life stress. Figure 32: Population distribution of individuals reporting quite a bit or extreme life stress in LGL. Figure 33: Reporting quite a bit or extreme life stress within each income group in LGL. Figure 34: Reporting quite a bit or extreme life stress by income group and gender in LGL. Figure 35: Reporting quite a bit or extreme life stress by age group in LGL. Page 19
. 15.")
20 Mammogram Leeds, Grenville & Lanark Community Health Profile: Healthy Living, Chronic Diseases and Injury 81.5% of the overall population of women aged 45+ years in LGL reported ever having a mammogram. 18.5% of women aged 45+ years reported never having a mammogram (Figure 36). 15.1% within the lowest income group compared to 34.4% within the highest income group reported never having a mammogram (Figure 37). A higher proportion of women in the year age group (22.2%) reported never having a mammogram than those in the 65+ year age group (12.1%) (Figure 38). A higher proportion of individuals living in rural settings reported never having a mammogram than those living in urban settings (23.9% vs. 14.6%). A higher proportion of women within the highest income group reported never having had a mammogram than individuals within the intermediate and lowest income groups. Reports of never having a mammogram were higher among women in the younger age group and those living in rural compared to urban settings. Figure 36: Population distribution of women reporting never having a mammogram in LGL. Figure 37: Reporting never having a mammogram within each income group in LGL. Figure 38: Reporting never having a mammogram by age group in LGL. Page 20
21 Marijuana Use 77.0% of the overall population in LGL reported not using marijuana in the past 12-months. 23.0% of the overall population reported having used marijuana in the past 12-months (Figure 39). 28.3% of individuals within the intermediate income group compared to 19.4% within the lowest income group and 22.0% within the highest income group reported having used marijuana in the past 12-months (Figure 40). Men were more likely to report using marijuana in the past 12-months than women in all income groups (Figure 41). A higher proportion of individuals in the year age group (48.1%) reported having used marijuana in the past 12-months than other age groups (15.9% %) (Figure 42). A higher proportion of individuals living in rural settings reported having used marijuana in the past 12-months than those living in urban settings (25.4% vs. 20.4%). Almost one in four people reported marijuana use in the past 12-months. Marijuana use was reported in all age groups with the highest use reported in the youngest age group. Reports of marijuana use were more common among men than women. A higher proportion of individuals living in rural than urban settings reported marijuana use. Figure 39: Population distribution of individuals reporting marijuana use in LGL. Figure 40: Reporting marijuana use within each income group in LGL. Figure 41: Reporting marijuana use by income group and gender in LGL. Figure 42: Reporting marijuana use by age group in LGL. Page 21
22 PAP Test Leeds, Grenville & Lanark Community Health Profile: Healthy Living, Chronic Diseases and Injury 97.1% of women aged 25+ years in LGL reported having a PAP test. 2.9% of women overall reported not ever having had a PAP test (Figure 43). 2.9% within the lowest income group compared to 4.6% within the highest income group reported not ever having had a PAP test (Figure 44). A higher proportion of women in the 65+ year age group (8.0%) reported not ever having had a PAP test than those the younger age groups (0.3% - 1.8%) (Figure 45). A higher proportion of individuals living in rural settings were more likely to report not ever having had a PAP test than those in urban settings (4.5% vs. 1.9%). A higher proportion of women within the highest income group reported not ever having had a PAP test than those in the lowest income group. Reports of not ever having had a PAP test were highest in the 65+ year age group. Reports of not ever having had a PAP test were higher among women living in rural compared to urban settings. Figure 43: Population distribution of women reporting not ever having had a PAP test in LGL. Figure 44: Reporting not ever having had a PAP test within each income group in LGL. Figure 45: Reporting not ever having had a PAP test by age group in LGL. Page 22
. 50.5% within the lowest income group compared to 33.")
23 Physical Inactivity 59.4% of the overall population in LGL reported being physically active during their leisure time. 40.6% of the overall population reported being physically inactive during their leisure time (Figure 46). 50.5% within the lowest income group compared to 33.3% within the highest income group reported being physically inactive (Figure 47). Women were more likely than men to report being physically inactive in both the intermediate and highest income groups (Figure 48). Physical inactivity increased with age. A higher proportion of individuals in the 65+ year age group (49.0%) reported being physically inactive than the younger age groups (20.0% %) (Figure 49). A similar proportion of individuals living in urban and rural settings reported being physically inactive (40.8% vs. 40.6%). A higher proportion of individuals in the lowest income group reported being physically inactive than individuals in the highest income group. Reports of physical inactivity increased with age and were highest in the 65+ year age group. Women in both the intermediate and highest income groups were more likely to report being physically inactive compared to men. Figure 46: Population distribution of individuals reporting being physically inactive in LGL. Figure 47: Reporting being physically inactive within each income group in LGL. Figure 48: Reporting being physically inactive by income group and gender in LGL. Figure 49: Reporting being physically inactive by age group in LGL. Page 23
24 Regular Medical Doctor 94.9% of the overall population in LGL reported having a regular medical doctor. 5.1% of the overall population reported not having a regular medical doctor (Figure 50) 6.4% within the lowest income group compared to 3.2% within the highest income group reported not having a regular medical doctor (Figure 51). Men were more likely than women in all income groups to report not having a regular medical doctor (Figure 52). A higher proportion of individuals in the and year age groups (6.1% and 6.2%) reported not having a regular medical doctor than other age groups (3.1% - 4.7%) (Figure 53). A similar proportion of individuals living in urban and rural settings reported not having a regular medical doctor (5.7% vs. 4.1%). A higher proportion of individuals within the lowest income group reported not having a regular medical doctor than individuals within the highest income group. Reports of not having a regular medical doctor were higher among younger age groups, and among men than women. Figure 50: Population distribution of individuals reporting not having a regular medical doctor in LGL. Figure 51: Reporting not having a regular medical doctor within each income group in LGL. Figure 52: Reporting not having a regular medical doctor by income group and gender in LGL. Figure 53: Reporting not having a regular medical doctor by age group in LGL. Page 24
25 Smoking Cigarettes 75.6% of the overall population in LGL reported currently being a nonsmoker. 24.4% of the overall population reported currently smoking cigarettes (Figure 54). 37.8% within the lowest income group compared to 15.5% within the highest income group reporting being a current cigarette smoker (Figure 55). Men were more likely than women to report being a current cigarette smoker in all income groups (Figure 56). A higher proportion of individuals in the year age group (33.2%) and the year age group (28.9%) reported being a current cigarette smoker than both the younger and older age groups (17.0% %) (Figure 57). A higher proportion of individuals living in urban settings were more likely to report being a current cigarette smoker than those in rural settings (28.2% vs. 20.0%). A higher proportion of individuals within the lowest income group reported being a current cigarette smoker than individuals within the highest income group. Reports of being a current cigarette smoker were more common among men than women, and among individuals living in urban compared to rural settings. Figure 54: Population distribution of individuals reporting being a current cigarette smoker in LGL. Figure 55: Reporting being a current cigarette smoker within each income group in LGL. Figure 56: Reporting being a current cigarette smoker by income group and gender in LGL. Figure 57: Reporting being a current cigarette smoker by age group in LGL. Page 25
.")
26 Work Stress (Self Rated) 72.7% of the overall population in LGL reported little to no work stress. 27.3% of the overall population reported having quite a bit or extreme work stress (Figure 58). A similar proportion of individuals within all income groups reported quite a bit or extreme work stress (Figure 59). Reporting quite a bit or extreme work stress was higher for women than men in the lowest and intermediate income groups (Figure 60). A higher proportion of individuals in the year age group (33.2%) reported having quite a bit to extreme work stress than other age groups (15.2% %) (Figure 61). A higher proportion of individuals living in urban settings reported quite a bit or extreme work stress than those in rural settings (31.7% vs. 27.3%). Reporting quite a bit or extreme work stress was similar within all income groups. More women than men reported quite a bit to extreme work stress in the lowest and intermediate income groups. Reports of quite a bit to extreme work stress was highest in the year age groups. Higher proportions of individuals reporting work stress lived in urban settings. Figure 58: Population distribution of individuals reporting quite a bit or extreme work stress in LGL. Figure 59: Reporting quite a bit or extreme work stress within each income group in LGL. Figure 60: Reporting quite a bit or extreme work stress by income group and gender in LGL. Figure 61: Reporting quite a bit or extreme work stress by age group in LGL. Page 26
27 Indicators of Health, Chronic Diseases and Injury Page 27
28 Health (Self Rated) 87.4% of the overall population in LGL reported having good to excellent health. 12.6% of the overall population reported fair to poor health (Figure 62). 24.8% within the lowest income group compared to 5.2% within the highest income group reported fair to poor health (Figure 63). Women were more likely than men to report fair to poor health in all income groups (Figure 64). A higher proportion of individuals in the (14.2%) and 65+ (18.9%) year age groups reported fair to poor health than other age groups (7.4% - 8.3%) (Figure 65). A higher proportion of individuals living in urban settings reported fair to poor health than those in rural settings (13.5% vs. 11.6%). A higher proportion of individuals within the lowest income group reported having fair to poor health than individuals within the highest income group. Reports of fair to poor health were more common in older age groups and more common among women than men. Figure 62: Population distribution of individuals reporting fair to poor health in LGL. Figure 63: Reporting having fair to poor health within each income group in LGL. Figure 64: Reporting having fair to poor health by income group and gender in LGL. Figure 65: Reporting fair to poor health by age group in LGL. Page 28
29 Mental Health (Self Rated) 92.5% of the overall population in LGL reported their mental health as being good to excellent. 7.5% of the overall population reported having fair to poor mental health (Figure 66). 10.7% of individuals within the lowest income group compared to 7.0% within the highest income group reported fair to poor mental health (Figure 67). More men than women in the lowest income group reported fair to poor mental health. This was reversed in the intermediate income group and there was no difference in the highest group (Figure 68). A higher proportion of individuals in the and year age groups (9.0% and 9.1%) reported fair to poor mental health than other age groups (3.0% - 5.9%) (Figure 69). A higher proportion of individuals living in urban settings reported having fair to poor mental health than those in rural settings (8.4% vs. 6.4%). A higher proportion of individuals within the lowest income group reported having fair to poor mental health than the highest income group. Higher proportions of individuals in the year age groups reported having fair to poor mental health. Higher proportions of individuals living in urban than rural settings reported fair to poor mental health. Figure 66: Population distribution of individuals reporting fair to poor mental health in LGL. Figure 67: Reporting fair to poor mental health within each income group in LGL. Figure 68: Reporting fair to poor mental health by income group and gender in LGL. Figure 69: Reporting fair to poor mental health by age group in LGL. Page 29
30 Anxiety Disorder Diagnosis 91.5% of the overall population in LGL reported not being diagnosed with an anxiety disorder. 8.5% of the overall population reported being diagnosed with an anxiety disorder (Figure 70). 12.4% within the lowest income group compared to 5.8% within the highest income group reported being diagnosed with an anxiety disorder (Figure 71). While both women and men reported a diagnosis of anxiety disorder, a higher proportion of women than men reported a diagnosis of an anxiety disorder in all income groups (Figure 72). A higher proportion of individuals in the year age group (10.9%) reported being diagnosed with an anxiety disorder than other age groups (5.2% - 7.6%) (Figure 73). A higher proportion of individuals living in urban settings reported being diagnosed with an anxiety disorder than those in rural settings (9.9% vs. 6.6%). A higher proportion of individuals within the lowest income group reported being diagnosed with an anxiety disorder than individuals within the highest income group. Reports of anxiety disorders were most common in the year age group. Reports of anxiety disorder were more common among women than men and among individuals living in urban settings. Figure 70: Population distribution of individuals reporting being diagnoses with an anxiety disorder in LGL. Figure 71: Reporting being diagnosed with an anxiety disorder within each income group in LGL. Figure 72: Reporting being diagnosed with an anxiety disorder by income group and gender in LGL. Figure 73: Reporting being diagnosed with an anxiety disorder by age group in LGL. Page 30
31 Asthma Diagnosis 89.9% of the overall population in LGL reported not being diagnosed with asthma. 10.1% of the overall population reported being diagnosed with asthma (Figure 74). 11.5% within the lowest income group compared to 9.2% within the highest income group reported being diagnosed with asthma (Figure 75). Women were more likely than men to report being diagnosed with asthma in all income groups (Figure 76). A higher proportion of individuals in the (12.5%) and the (11.8%) year age groups reported being diagnosed with asthma than the older age groups (8.3% - 8.9%) (Figure 77). A similar proportion of individuals living in urban and rural settings reported being diagnosed with asthma (10.4% vs. 9.7%). A slightly higher proportion of individuals within the highest income group reported being diagnosed with asthma than individuals within the lowest income group. A diagnosis of asthma was most common in the youngest age group. Reports of asthma were more common among women than men. Figure 74: Population distribution of individuals reporting being diagnosed with asthma in LGL. Figure 75: Reporting being diagnosed with asthma within each income group in LGL. Figure 76: Reporting being diagnosed with asthma by income group and gender in LGL. Figure 77: Reporting being diagnosed with asthma by age group in LGL. Page 31
.")
32 Diabetes Diagnosis 91.4% of the overall population in LGL reported not being diagnosed with diabetes. 8.6% of the overall population reported being diagnosed with diabetes (Figure 78). 12.1% within the lowest income group compared to 4.9% within the highest income group reported being diagnosed with diabetes (Figure 79). Men were more likely than women to report being diagnosed with diabetes in all income groups (Figure 80). A higher proportion of individuals in the (11.0%) and 65+ (16.6%) year age groups reported being diagnosed with diabetes than the younger age groups (0.5% - 3.1%) (Figure 81). A higher proportion of individuals living in urban settings reported being diagnosed with diabetes than those in rural settings (9.2% vs. 7.9%). A higher proportion of individuals within the lowest income group reported being diagnosed with diabetes than individuals in the highest income group. Reports of a diabetes diagnosis were more common in older age groups. Reports of diabetes were more common among men than women, and among individuals living in urban compared to rural settings. Figure 78: Population distribution of individuals reporting having diabetes in LGL. Figure 79: Reporting having diabetes within each income group in LGL. Figure 80: Reporting having diabetes by income group and gender in LGL. Figure 81: Reporting having diabetes by age group in LGL. Page 32
33 Heart Disease Diagnosis 93.9% of the overall population in LGL reported not being diagnosed with heart disease. 6.1% of the overall population reported a diagnosis of heart disease (Figure 82). 10.6% within the lowest income group compared to 3.5% within the highest income group reported being diagnosed with heart disease (Figure 83). Men were more likely than women to report being diagnosed with heart disease in all but the highest income group (Figure 84). A higher proportion of individuals in the 65+year age group (18.7%) reported a diagnosis of heart disease than other age groups (0.4% - 4.4%) (Figure 85). A higher proportion of individuals living in urban settings reported being diagnosed with heart disease than those in rural settings (7.0% vs. 4.8%). A higher proportion of individuals within the lowest income group reported being diagnosed with heart disease than individuals in the highest income group. Reports of having heart disease were more common among men than women, older age groups and among individuals living in urban compared to rural settings. Figure 82: Population distribution of individuals reporting being diagnosed with heart disease in LGL. Figure 83: Reporting being diagnosed with heart disease within each income group in LGL. Figure 84: Reporting being diagnosed with heart disease by income group and gender in LGL. Figure 85: Reporting being diagnosed with heart disease by age group in LGL. Page 33
34 Mood Disorder Diagnosis (Depression & Bipolar) 89.4% of the overall population in LGL reported not being diagnosed with a mood disorder. 10.6% of the overall population reported being diagnosed with a mood disorder (Figure 86). 20.2% within the lowest income group compared to 5.4% within the highest income group reported being diagnosed with a mood disorder (Figure 87). Women were more likely than men to report being diagnosed with a mood disorder in all income groups (Figure 88). A higher proportion of individuals in the year age group (15.0%) reported being diagnosed with a mood disorder than other age groups (6.6% - 9.6%) (Figure 89). A higher proportion of individuals living in urban settings were more likely to report being diagnosed with a mood disorder than those in rural settings (13.2% vs. 7.2%). A higher proportion of individuals within the lowest income group reported being diagnosed with a mood disorder than individuals in the highest income group. Reports of mood disorders were most common in the year age group. Reports of being diagnosed with a mood disorder were more common among women than men and among individuals living in urban compared to rural settings. Figure 86: Population distribution of individuals reporting being diagnosed with a mood disorder in LGL. Figure 87: Reporting being diagnosed with a mood disorder within each income group in LGL. Figure 88: Reporting being diagnosed with a mood disorder by income group and gender in LGL. Figure 89: Reporting being diagnosed with a mood disorder by age group in LGL. Page 34
35 Injury in Past 12-Months 80.5% of the overall population in LGL reported not being injured in the past 12-months. 19.5% of the overall population reported being injured in the past 12-months (Figure 90). 20.0% within the lowest income group compared to 21.4% within the highest income group reported being injured in past 12-months (Figure 91). Men were more likely than women to report being injured in past 12- months in all income groups (Figure 92). A higher proportion of individuals in the year age group (31.8%) reported being injured in the past 12-months than other age groups (11.8% %) (Figure 93). A similar proportion of individuals living in urban and rural settings reported being injured in the past 12-months (19.3% vs. 18.8%). Similar proportions of individuals within all income groups reported being injured in past 12-months. Reports of being injured in the past 12-months were most common in the youngest age group and decreased with age. Reports of being injured in past 12-months were more common among men than women. Figure 90: Population distribution of individuals reporting being injured in past 12-months in LGL. Figure 91: Reporting being injured in past 12-months within each income group in LGL. Figure 92: Reporting being injured in past 12-months by income group and gender in LGL. Figure 93: Reporting being injured in past 12-months by age group in LGL. Page 35
36 Injury From to a Fall in Past 12-Months 64.4% of the overall population in LGL reported not being injured due to a fall in the past 12-months. 35.6% of the overall population reported being injured due to a fall in the past 12-months (Figure 94). 42.1% within the intermediate income group compared to 31.7% within the highest and 35.0% in the lowest income groups reported being injured due to a fall in past 12-months (Figure 95). Women were more likely to report an injury due to a fall in the pastmonths than men in the intermediate and high income groups (Figure 96). A higher proportion of individuals in the 65+year age group (62.3%) and the year age group (45.5%) reported being injured from a fall in the past 12-months than other age groups (25.5% %) (Figure 97). A slightly higher proportion of individuals living in rural settings reported having sustained an injury due to a fall in the past 12-months than those in urban settings (36.1% vs. 33.8%). A greater proportion of individuals within the intermediate income group reported being injured due to a fall in the past 12-months compared to the lowest and highest income groups. Reports of being injured due to a fall in the past 12-months was most common in both the oldest and youngest age groups. Reports of being injured due to a fall were more common among women than men. Figure 94: Population distribution of individuals reporting being injured from a fall in past 12-months in LGL. Figure 95: Reporting being injured from a fall in past 12-months within each income group in LGL. Figure 96: Reporting being injured from a fall in past 12-months by income group and gender in LGL. Figure 97: Reporting being injured from a fall in past 12-months by age group in LGL. Page 36



37 Appendix 1: Mapping LGL Municipalities by Income Group Leeds, Grenville & Lanark Athens Augusta Beckwith Brockville Carleton Place Page 37




38 Appendix 1: Mapping LGL Municipalities by Income Group Drummond/North Elmsley Edwardsburg/Cardinal Elizabethtown-Kitley Front of Yonge Gananoque Lanark Highlands Page 38

39 Appendix 1: Mapping LGL Municipalities by Income Group Leeds & the Thousand Islands Merrickville/Wolford Mississippi Mills Montague North Grenville Perth Page 39

40 Appendix 1: Mapping LGL Municipalities by Income Group Rideau Lakes Smiths Falls Tay Valley Westport Prescott Page 40
Australian Longitudinal Study on Women's Health TRENDS IN WOMEN S HEALTH 2006 FOREWORD
 Australian Longitudinal Study on Women's Health TRENDS IN WOMEN S HEALTH 2006 FOREWORD The Longitudinal Study on Women's Health, funded by the Commonwealth Government, is the most comprehensive study ever
Australian Longitudinal Study on Women's Health TRENDS IN WOMEN S HEALTH 2006 FOREWORD The Longitudinal Study on Women's Health, funded by the Commonwealth Government, is the most comprehensive study ever
Seniors Health in York Region
 Seniors Health in York Region Seniors in York Region are generally healthy York Region is set to experience tremendous growth in its seniors population. A Profile of Baby Boomers and Seniors in York Region,
Seniors Health in York Region Seniors in York Region are generally healthy York Region is set to experience tremendous growth in its seniors population. A Profile of Baby Boomers and Seniors in York Region,
WASHINGTON COUNTY COMMUNITY HEALTH SURVEY 2016
 WASHINGTON COUNTY COMMUNITY HEALTH SURVEY 2016 Commissioned by: Aurora Health Care Children s Hospital of Wisconsin Froedtert & Medical College In Partnership with: Center for Urban Population Health Washington
WASHINGTON COUNTY COMMUNITY HEALTH SURVEY 2016 Commissioned by: Aurora Health Care Children s Hospital of Wisconsin Froedtert & Medical College In Partnership with: Center for Urban Population Health Washington
Colorado s Progress toward Year 2000 Objectives
 Colorado s Progress toward Year Objectives An update from the Survey Research Unit No. 26 November 1998 Two major roles of Public Health are to reduce preventable death and disability and to enhance quality
Colorado s Progress toward Year Objectives An update from the Survey Research Unit No. 26 November 1998 Two major roles of Public Health are to reduce preventable death and disability and to enhance quality
OZAUKEE COUNTY COMMUNITY HEALTH SURVEY 2016
 OZAUKEE COUNTY COMMUNITY HEALTH SURVEY 2016 Commissioned by: Aurora Health Care Children s Hospital of Wisconsin Columbia St. Mary s Health System In Partnership with: Center for Urban Population Health
OZAUKEE COUNTY COMMUNITY HEALTH SURVEY 2016 Commissioned by: Aurora Health Care Children s Hospital of Wisconsin Columbia St. Mary s Health System In Partnership with: Center for Urban Population Health
WAUKESHA COUNTY COMMUNITY HEALTH SURVEY 2017
 WAUKESHA COUNTY COMMUNITY HEALTH SURVEY 2017 Commissioned By: Aurora Health Care Children s Hospital of Wisconsin Froedtert & the Medical College of Wisconsin ProHealth Care Wheaton Franciscan Healthcare
WAUKESHA COUNTY COMMUNITY HEALTH SURVEY 2017 Commissioned By: Aurora Health Care Children s Hospital of Wisconsin Froedtert & the Medical College of Wisconsin ProHealth Care Wheaton Franciscan Healthcare
KENOSHA COUNTY COMMUNITY HEALTH SURVEY 2016
 KENOSHA COUNTY COMMUNITY HEALTH SURVEY 2016 Commissioned by: Aurora Health Care Children s Hospital of Wisconsin United Hospital Systems In Partnership with: Center for Urban Population Health Kenosha
KENOSHA COUNTY COMMUNITY HEALTH SURVEY 2016 Commissioned by: Aurora Health Care Children s Hospital of Wisconsin United Hospital Systems In Partnership with: Center for Urban Population Health Kenosha
Preliminary findings Sunshine Coast Community Dialogue Sechelt, September 11 th, 2014 Maritia Gully Regional Epidemiologist, Public Health
 Preliminary findings Sunshine Coast Community Dialogue Sechelt, September 11 th, 2014 Maritia Gully Regional Epidemiologist, Public Health Surveillance Unit, Vancouver Coastal Health email: phsu@vch.ca
Preliminary findings Sunshine Coast Community Dialogue Sechelt, September 11 th, 2014 Maritia Gully Regional Epidemiologist, Public Health Surveillance Unit, Vancouver Coastal Health email: phsu@vch.ca
WALWORTH COUNTY COMMUNITY HEALTH SURVEY 2016
 WALWORTH COUNTY COMMUNITY HEALTH SURVEY 2016 Commissioned by: Aurora Health Care Children s Hospital of Wisconsin Mercy Health System In Partnership with: Center for Urban Population Health Walworth County
WALWORTH COUNTY COMMUNITY HEALTH SURVEY 2016 Commissioned by: Aurora Health Care Children s Hospital of Wisconsin Mercy Health System In Partnership with: Center for Urban Population Health Walworth County
North Shore Community Health Survey Summary
 North Shore Community Health Survey Summary This research provides valuable behavioral data, lifestyle habits, and the prevalence of risk factors and disease conditions of North Shore residents. This summary
North Shore Community Health Survey Summary This research provides valuable behavioral data, lifestyle habits, and the prevalence of risk factors and disease conditions of North Shore residents. This summary
KENOSHA COUNTY COMMUNITY HEALTH SURVEY 2014
 KENOSHA COUNTY COMMUNITY HEALTH SURVEY 2014 Commissioned by: Aurora Health Care Children s Hospital of Wisconsin In Partnership with: Center for Urban Population Health Kenosha County Division of Health
KENOSHA COUNTY COMMUNITY HEALTH SURVEY 2014 Commissioned by: Aurora Health Care Children s Hospital of Wisconsin In Partnership with: Center for Urban Population Health Kenosha County Division of Health
Colorado Health Disparities Profiles
 Health Disparities Profiles includes: Larimer County Population Total Population Source: CDC/NCHS 2007-based, bridged-race population estimates, 2007. Social Determinants of Health 287,574 248,312 26,629
Health Disparities Profiles includes: Larimer County Population Total Population Source: CDC/NCHS 2007-based, bridged-race population estimates, 2007. Social Determinants of Health 287,574 248,312 26,629
Burden of Illness. Chapter 3 -- Highlights Document ONTARIO WOMEN'S HEALTH EQUITY REPORT
 Burden of Illness Chapter 3 -- Highlights Document A primary objective of the POWER (Project for an Ontario Women's Health Report) Study is to develop a tool that can be used to improve the health and
Burden of Illness Chapter 3 -- Highlights Document A primary objective of the POWER (Project for an Ontario Women's Health Report) Study is to develop a tool that can be used to improve the health and
Children in Household Year Because Trying to Quit 53% 55% 58% 66% Milwaukee 2012
 Men s Health (40 and Older) Alcohol Use in Past Month Milwaukee 2006 2009 2012 Milwaukee 2003 2006 2009 2012 Prostate Cancer Screening Binge Drinker 17% 20% 19% 32% Within Past 2 Years 61% 58% 45% Driver/Passenger
Men s Health (40 and Older) Alcohol Use in Past Month Milwaukee 2006 2009 2012 Milwaukee 2003 2006 2009 2012 Prostate Cancer Screening Binge Drinker 17% 20% 19% 32% Within Past 2 Years 61% 58% 45% Driver/Passenger
Colorado Health Disparities Profiles
 Health Disparities Profiles County includes: Jackson, Moffat, Rio Blanco, and Counties Population Total Population 22,382 43,638 4,861,515 21,015 39,473 3,508,736 904 3,224 909,833 140 263 228,718 210
Health Disparities Profiles County includes: Jackson, Moffat, Rio Blanco, and Counties Population Total Population 22,382 43,638 4,861,515 21,015 39,473 3,508,736 904 3,224 909,833 140 263 228,718 210
Hales Corners Community Health Survey Summary
 Hales Corners Community Health Survey Summary This research provides valuable behavioral data, lifestyle habits, and the prevalence of risk factors and disease conditions of Hales Corners residents. This
Hales Corners Community Health Survey Summary This research provides valuable behavioral data, lifestyle habits, and the prevalence of risk factors and disease conditions of Hales Corners residents. This
Vancouver Coastal Health & Fraser Health Data Summary Sheets: Alcohol Use. Purpose. Overview. Overall Alcohol Use. Overall Binge Drinking Prevalence
 Purpose The purpose of this data summary sheet is to provide an overview of binge drinking prevalence among different population groups across Vancouver Coastal Health (VCH) and Fraser Health (FH). The
Purpose The purpose of this data summary sheet is to provide an overview of binge drinking prevalence among different population groups across Vancouver Coastal Health (VCH) and Fraser Health (FH). The
Health Inequities in Renfrew County and District
 Authors Health Inequities in Renfrew County and District Data analysis, results and report prepared by the Knowledge Management Division, Kingston, Frontenac and Lennox & Addington Public Health: Evan
Authors Health Inequities in Renfrew County and District Data analysis, results and report prepared by the Knowledge Management Division, Kingston, Frontenac and Lennox & Addington Public Health: Evan
2016 Collier County Florida Health Assessment Executive Summary
 2016 Florida Health Assessment Executive Summary Prepared by: The Health Planning Council of Southwest Florida, Inc. www.hpcswf.com Executive Summary To access the report in its entirety, visit http://www.hpcswf.com/health-planning/health-planningprojects/.
2016 Florida Health Assessment Executive Summary Prepared by: The Health Planning Council of Southwest Florida, Inc. www.hpcswf.com Executive Summary To access the report in its entirety, visit http://www.hpcswf.com/health-planning/health-planningprojects/.
Children in Household Year Because Trying to Quit 43% 52% 43% 57% South Milwaukee 2012
 Men s Health (40 and Older) Alcohol Use in Past Month South Milwaukee 2006 2009 2012 South Milwaukee 2003 2006 2009 2012 Prostate Cancer Screening Binge Drinker 16% 20% 23% 38% Within Past 2 Years 70%
Men s Health (40 and Older) Alcohol Use in Past Month South Milwaukee 2006 2009 2012 South Milwaukee 2003 2006 2009 2012 Prostate Cancer Screening Binge Drinker 16% 20% 23% 38% Within Past 2 Years 70%
Children in Household Year Because Trying to Quit 30% 68% 51% 69% Hales Corners 2012
 Men s Health (40 and Older) Alcohol Use in Past Month Hales Corners 2006 2009 2012 Hales Corners 2003 2006 2009 2012 Prostate Cancer Screening Binge Drinker 13% 20% 20% 24% Within Past 2 Years 63% 70%
Men s Health (40 and Older) Alcohol Use in Past Month Hales Corners 2006 2009 2012 Hales Corners 2003 2006 2009 2012 Prostate Cancer Screening Binge Drinker 13% 20% 20% 24% Within Past 2 Years 63% 70%
GREENDALE COMMUNITY HEALTH SURVEY 2015
 GREENDALE COMMUNITY HEALTH SURVEY 2015 Commissioned by: Aurora Health Care Children s Hospital of Wisconsin Columbia St. Mary s Health System Froedtert Health Wheaton Franciscan Healthcare In Partnership
GREENDALE COMMUNITY HEALTH SURVEY 2015 Commissioned by: Aurora Health Care Children s Hospital of Wisconsin Columbia St. Mary s Health System Froedtert Health Wheaton Franciscan Healthcare In Partnership
CUDAHY COMMUNITY HEALTH SURVEY 2015
 CUDAHY COMMUNITY HEALTH SURVEY 2015 Commissioned by: Aurora Health Care Children s Hospital of Wisconsin Columbia St. Mary s Health System Froedtert Health Wheaton Franciscan Healthcare In Partnership
CUDAHY COMMUNITY HEALTH SURVEY 2015 Commissioned by: Aurora Health Care Children s Hospital of Wisconsin Columbia St. Mary s Health System Froedtert Health Wheaton Franciscan Healthcare In Partnership
Walworth County Community Health Survey Summary
 Walworth County Community Health Survey Summary This research provides valuable behavioral data, lifestyle habits, and the prevalence of risk factors and disease conditions of Walworth County residents.
Walworth County Community Health Survey Summary This research provides valuable behavioral data, lifestyle habits, and the prevalence of risk factors and disease conditions of Walworth County residents.
Children in Household Year Because Trying to Quit 45% 20% 45% 43% Greenfield 2012
 Men s Health (40 and Older) Alcohol Use in Past Month Greenfield 2006 2009 2012 Greenfield 2003 2006 2009 2012 Prostate Cancer Screening Binge Drinker 17% 25% 19% 28% Within Past 2 Years 59% 65% 68% Driver/Passenger
Men s Health (40 and Older) Alcohol Use in Past Month Greenfield 2006 2009 2012 Greenfield 2003 2006 2009 2012 Prostate Cancer Screening Binge Drinker 17% 25% 19% 28% Within Past 2 Years 59% 65% 68% Driver/Passenger
Children in Household Year Because Trying to Quit 47% 43% 47% 40% West Allis/West Milwaukee 2012
 Men s Health (40 and Older) Alcohol Use in Past Month West Allis/West Milwaukee 2006 2009 2012 West Allis/West Milwaukee 2003 2006 2009 2012 Prostate Cancer Screening Binge Drinker 18% 21% 24% 30% Within
Men s Health (40 and Older) Alcohol Use in Past Month West Allis/West Milwaukee 2006 2009 2012 West Allis/West Milwaukee 2003 2006 2009 2012 Prostate Cancer Screening Binge Drinker 18% 21% 24% 30% Within
Nutrition and Physical Activity Situational Analysis
 Nutrition and Physical Activity Situational Analysis A Resource to Guide Chronic Disease Prevention in Alberta Executive Summary December 2010 Prepared by: Alberta Health Services, AHS Overview Intrinsic
Nutrition and Physical Activity Situational Analysis A Resource to Guide Chronic Disease Prevention in Alberta Executive Summary December 2010 Prepared by: Alberta Health Services, AHS Overview Intrinsic
Daily Smoking Among BC Youth
 All results in this fact sheet are among students who had ever tried smoking. The 2013 BC Adolescent Health Survey (BC AHS) asked youth whether they had ever tried smoking and if they had, how many days
All results in this fact sheet are among students who had ever tried smoking. The 2013 BC Adolescent Health Survey (BC AHS) asked youth whether they had ever tried smoking and if they had, how many days
MILWAUKEE COUNTY COMMUNITY HEALTH SURVEY 2015
 MILWAUKEE COUNTY COMMUNITY HEALTH SURVEY 2015 Commissioned by: Aurora Health Care Children s Hospital of Wisconsin Columbia St. Mary s Health System Froedtert Health Wheaton Franciscan Healthcare In Partnership
MILWAUKEE COUNTY COMMUNITY HEALTH SURVEY 2015 Commissioned by: Aurora Health Care Children s Hospital of Wisconsin Columbia St. Mary s Health System Froedtert Health Wheaton Franciscan Healthcare In Partnership
DETERMINANTS OF HEALTH HHD Unit 3 AOS 1 Pg 61-76
 DETERMINANTS OF HEALTH HHD Unit 3 AOS 1 Pg 61-76 INTRODUCTION There are a different factors that impact on our health and development. These factors are called Determinants of Health because their impact
DETERMINANTS OF HEALTH HHD Unit 3 AOS 1 Pg 61-76 INTRODUCTION There are a different factors that impact on our health and development. These factors are called Determinants of Health because their impact
2017 Community Health Needs Assessment Report
 2017 Community Health Needs Assessment Report, Florida Prepared for: By: Professional Research Consultants, Inc. 11326 P Street Omaha, NE 68137-2316 www.prccustomresearch.com 2017-0313-02 June 2017 Table
2017 Community Health Needs Assessment Report, Florida Prepared for: By: Professional Research Consultants, Inc. 11326 P Street Omaha, NE 68137-2316 www.prccustomresearch.com 2017-0313-02 June 2017 Table
Washington County Community Health Survey Report 2014
 Washington County Community Health Survey Report 2014 Commissioned by: Aurora Health Care Children s Hospital of Wisconsin Froedtert & Medical College of Wisconsin In Partnership with: Center for Urban
Washington County Community Health Survey Report 2014 Commissioned by: Aurora Health Care Children s Hospital of Wisconsin Froedtert & Medical College of Wisconsin In Partnership with: Center for Urban
CANNABIS IN ONTARIO S COMMUNITIES
 CANNABIS IN ONTARIO S COMMUNITIES That municipal governments support their local Public Health Unit and encourage Develop a funded public health approach to cannabis legalization, regulation, restriction
CANNABIS IN ONTARIO S COMMUNITIES That municipal governments support their local Public Health Unit and encourage Develop a funded public health approach to cannabis legalization, regulation, restriction
CENTRAL RACINE COUNTY COMMUNITY HEALTH SURVEY July 2012
 CENTRAL RACINE COUNTY COMMUNITY HEALTH SURVEY July 2012 Commissioned by: Aurora Health Care Children s Hospital of Wisconsin Wheaton Franciscan Healthcare In Partnership with: Central Racine County Health
CENTRAL RACINE COUNTY COMMUNITY HEALTH SURVEY July 2012 Commissioned by: Aurora Health Care Children s Hospital of Wisconsin Wheaton Franciscan Healthcare In Partnership with: Central Racine County Health
Waukesha County Community Health Survey Report June 2012
 Waukesha County Community Health Survey Report June 2012 Commissioned by: Aurora Health Care Children s Hospital of Wisconsin Froedtert Health ProHealth Care Wheaton Franciscan Healthcare In Partnership
Waukesha County Community Health Survey Report June 2012 Commissioned by: Aurora Health Care Children s Hospital of Wisconsin Froedtert Health ProHealth Care Wheaton Franciscan Healthcare In Partnership
Healthy People, Healthy Communities
 Healthy People, Healthy Communities Public Health Policy Statements on Public Health Issues The provincial government plays an important role in shaping policies that impact both individual and community
Healthy People, Healthy Communities Public Health Policy Statements on Public Health Issues The provincial government plays an important role in shaping policies that impact both individual and community
Prostate cancer was the most commonly diagnosed type of cancer among Peel and Ontario male seniors in 2002.
 Cancer HIGHLIGHTS Prostate, colorectal, and lung cancers accounted for almost half of all newly diagnosed cancers among Peel seniors in 22. The incidence rates of lung cancer in Ontario and Peel have decreased
Cancer HIGHLIGHTS Prostate, colorectal, and lung cancers accounted for almost half of all newly diagnosed cancers among Peel seniors in 22. The incidence rates of lung cancer in Ontario and Peel have decreased
Our Health: A Community Health Assessment Survey. Eastern Shore Musquodoboit (ESM) Community Health Board Presentation
 Community Health Board Presentation") Our Health: A Community Health Assessment Survey Eastern Shore Musquodoboit (ESM) Community Health Board Presentation Purpose of this Evening Share information on the health of the citizens in our communities
Our Health: A Community Health Assessment Survey Eastern Shore Musquodoboit (ESM) Community Health Board Presentation Purpose of this Evening Share information on the health of the citizens in our communities
Despite substantial declines over the past decade,
 19 The journey to quitting smoking Margot Shields Abstract Objectives This article outlines smoking trends over the past 10 years among the population aged 18 or older. Factors associated with smoking
19 The journey to quitting smoking Margot Shields Abstract Objectives This article outlines smoking trends over the past 10 years among the population aged 18 or older. Factors associated with smoking
Facts on: Self Rated Oral Health
 Facts on: Self Rated Oral Health In Durham Region Highlights April 2016 In 2014, 61% of the Durham Region residents aged 12 and over rated their oral health as excellent or very good. Rates for both Durham
Facts on: Self Rated Oral Health In Durham Region Highlights April 2016 In 2014, 61% of the Durham Region residents aged 12 and over rated their oral health as excellent or very good. Rates for both Durham
WAUWATOSA COMMUNITY HEALTH SURVEY 2015
 WAUWATOSA COMMUNITY HEALTH SURVEY 2015 Commissioned by: Aurora Health Care Children s Hospital of Wisconsin Columbia St. Mary s Health System Froedtert Health Wheaton Franciscan Healthcare In Partnership
WAUWATOSA COMMUNITY HEALTH SURVEY 2015 Commissioned by: Aurora Health Care Children s Hospital of Wisconsin Columbia St. Mary s Health System Froedtert Health Wheaton Franciscan Healthcare In Partnership
Data Brief. Exploring Urban Environments and Inequalities in Health
 Data Brief Exploring Urban Environments and Inequalities in Health Halifax Census Metropolitan Area In 008, the Canadian Population Health Initiative (CPHI), a part of the Canadian Institute for Health
Data Brief Exploring Urban Environments and Inequalities in Health Halifax Census Metropolitan Area In 008, the Canadian Population Health Initiative (CPHI), a part of the Canadian Institute for Health
Adult overweight and obesity
 Facts on Adult overweight and obesity March 2017 in Durham Region Highlights In 2013/2014, 57 per cent of Durham Region adults 18 and older were overweight or obese. Rates for both Durham Region and Ontario
Facts on Adult overweight and obesity March 2017 in Durham Region Highlights In 2013/2014, 57 per cent of Durham Region adults 18 and older were overweight or obese. Rates for both Durham Region and Ontario
Socio-Demographic and Lifestyle Correlates of Obesity
 Socio-Demographic and Lifestyle Correlates of Obesity Technical Report on the Secondary Analyses Using the 2000 2001 Canadian Community Health Survey C a n a d i a n P o p u l a t i o n H e a l t h I n
Socio-Demographic and Lifestyle Correlates of Obesity Technical Report on the Secondary Analyses Using the 2000 2001 Canadian Community Health Survey C a n a d i a n P o p u l a t i o n H e a l t h I n
GREENDALE COMMUNITY HEALTH SURVEY December 2012
 GREENDALE COMMUNITY HEALTH SURVEY December 2012 Commissioned by: Aurora Health Care Children s Hospital of Wisconsin Columbia St. Mary s Health System Froedtert Health Wheaton Franciscan Healthcare In
GREENDALE COMMUNITY HEALTH SURVEY December 2012 Commissioned by: Aurora Health Care Children s Hospital of Wisconsin Columbia St. Mary s Health System Froedtert Health Wheaton Franciscan Healthcare In
Te Rau Hinengaro: The New Zealand Mental Health Survey
 Te Rau Hinengaro: The New Zealand Mental Health Survey Executive Summary Mark A Oakley Browne, J Elisabeth Wells, Kate M Scott Citation: Oakley Browne MA, Wells JE, Scott KM. 2006. Executive summary. In:
Te Rau Hinengaro: The New Zealand Mental Health Survey Executive Summary Mark A Oakley Browne, J Elisabeth Wells, Kate M Scott Citation: Oakley Browne MA, Wells JE, Scott KM. 2006. Executive summary. In:
CHAPTER 3: Modifiable risk factors and diabetes self-care
 CHAPTER 3: Modifiable risk factors and diabetes self-care Diabetes is caused by a number of genetic, environmental and biological factors, many of which are not within an individual s control, such as
CHAPTER 3: Modifiable risk factors and diabetes self-care Diabetes is caused by a number of genetic, environmental and biological factors, many of which are not within an individual s control, such as
Executive Summary To access the report in its entirety, visit
 Executive Summary To access the report in its entirety, visit http://www.hpcswf.com/health-planning/health-planningprojects/. Demographic and Socioeconomic Characteristics Population Demographics has a
Executive Summary To access the report in its entirety, visit http://www.hpcswf.com/health-planning/health-planningprojects/. Demographic and Socioeconomic Characteristics Population Demographics has a
The Community Health Data Base
 The Community Health Data Base 2017 The Community Health Data Base A population health resource Provides community-level health and social service data Has served the Southeastern PA region since 1991.
The Community Health Data Base 2017 The Community Health Data Base A population health resource Provides community-level health and social service data Has served the Southeastern PA region since 1991.
Community Health Needs Assessment. Implementation Strategy.. SAMPLE TEMPLATE
 Community Health Needs Assessment & Implementation Strategy SAMPLE TABLE OF CONTENTS Executive Summary I. Service Area and Population II. Community Health Needs Assessment Partners.. III. IV. Community
Community Health Needs Assessment & Implementation Strategy SAMPLE TABLE OF CONTENTS Executive Summary I. Service Area and Population II. Community Health Needs Assessment Partners.. III. IV. Community
WEST ALLIS/WEST MILWAUKEE COMMUNITY HEALTH SURVEY December 2012
 WEST ALLIS/WEST MILWAUKEE COMMUNITY HEALTH SURVEY December 2012 Commissioned by: Aurora Health Care Children s Hospital of Wisconsin Columbia St. Mary s Health System Froedtert Health Wheaton Franciscan
WEST ALLIS/WEST MILWAUKEE COMMUNITY HEALTH SURVEY December 2012 Commissioned by: Aurora Health Care Children s Hospital of Wisconsin Columbia St. Mary s Health System Froedtert Health Wheaton Franciscan
Community Needs Analysis Report
 Grampians Medicare Local Community Needs Analysis Report Summary October 2013 2 Contents Introduction 3 Snapshot of results 4 Stakeholder feedback 5 Health status of residents 6 Health behaviour of residents
Grampians Medicare Local Community Needs Analysis Report Summary October 2013 2 Contents Introduction 3 Snapshot of results 4 Stakeholder feedback 5 Health status of residents 6 Health behaviour of residents
SDHU Population Health Profile. Summary Report
 SDHU Population Health Profile Summary Report Sudbury & District Health Unit Revised: January 29, 2016 Authors Michael King, Epidemiologist Dar Malaviarachchi, Epidemiologist Alissa Palangio, Data Analyst
SDHU Population Health Profile Summary Report Sudbury & District Health Unit Revised: January 29, 2016 Authors Michael King, Epidemiologist Dar Malaviarachchi, Epidemiologist Alissa Palangio, Data Analyst
Trends in Pneumonia and Influenza Morbidity and Mortality
 Trends in Pneumonia and Influenza Morbidity and Mortality American Lung Association Epidemiology and Statistics Unit Research and Health Education Division November 2015 Page intentionally left blank Introduction
Trends in Pneumonia and Influenza Morbidity and Mortality American Lung Association Epidemiology and Statistics Unit Research and Health Education Division November 2015 Page intentionally left blank Introduction
SOUTH MILWAUKEE COMMUNITY HEALTH SURVEY 2012
 SOUTH MILWAUKEE COMMUNITY HEALTH SURVEY 2012 Commissioned by: Aurora Health Care Children s Hospital of Wisconsin Columbia St. Mary s Health System Froedtert Health Wheaton Franciscan Healthcare In Partnership
SOUTH MILWAUKEE COMMUNITY HEALTH SURVEY 2012 Commissioned by: Aurora Health Care Children s Hospital of Wisconsin Columbia St. Mary s Health System Froedtert Health Wheaton Franciscan Healthcare In Partnership
LOTHIAN HEALTH & LIFESTYLE SURVEY 2010 COMMUNITY HEALTH PARTNERSHIP FINDINGS: REPORT
 LOTHIAN HEALTH & LIFESTYLE SURVEY 2010 COMMUNITY HEALTH PARTNERSHIP FINDINGS: REPORT Directorate of Public Health & Health Policy NHS April 2013 1 AUTHORS Pat Boreham John Forbes Annette Gallimore Laura
LOTHIAN HEALTH & LIFESTYLE SURVEY 2010 COMMUNITY HEALTH PARTNERSHIP FINDINGS: REPORT Directorate of Public Health & Health Policy NHS April 2013 1 AUTHORS Pat Boreham John Forbes Annette Gallimore Laura
The Canadian Community Health Survey
 Canadian Community Health Survey Cycle 2.1 Report 2 Physical Activity in Nova Scotia January 2005 The Canadian Community Health Survey (CCHS) is a new series of health surveys being conducted by Statistics
Canadian Community Health Survey Cycle 2.1 Report 2 Physical Activity in Nova Scotia January 2005 The Canadian Community Health Survey (CCHS) is a new series of health surveys being conducted by Statistics
Factual Information Contained in this Report: PURPOSE. Health Perceptions. Health Insurance Coverage. Health Care Access. Preventive Health Care
 Factual Information Contained in this Report: Health Perceptions Health Insurance Coverage Health Care Access Preventive Health Care Maternal and Child Health Alcohol, Tobacco, and Other Drug Use PURPOSE
Factual Information Contained in this Report: Health Perceptions Health Insurance Coverage Health Care Access Preventive Health Care Maternal and Child Health Alcohol, Tobacco, and Other Drug Use PURPOSE
Oral Health in Perth County
 District Health Unit Oral Health in County PURPOSE The purpose of this report is to Examine oral health care and dental disease trends in County residents aged 12 and over, over a -year period To identify
District Health Unit Oral Health in County PURPOSE The purpose of this report is to Examine oral health care and dental disease trends in County residents aged 12 and over, over a -year period To identify
Pre-Conception & Pregnancy in Ohio
 Pre-Conception & Pregnancy in Ohio Elizabeth Conrey, PhD 1 January 217 1 State Maternal and Child Health Epidemiologist, Ohio Department of Health EXECUTIVE SUMMARY The primary objective of the analyses
Pre-Conception & Pregnancy in Ohio Elizabeth Conrey, PhD 1 January 217 1 State Maternal and Child Health Epidemiologist, Ohio Department of Health EXECUTIVE SUMMARY The primary objective of the analyses
Timiskaming Health Stats
 Health Stats Drug Use in the Health Unit Area Released ebruary Released 14 July 14 Introduction This report presents the percentage of residents aged 12 years and older who have ever used illicit drugs
Health Stats Drug Use in the Health Unit Area Released ebruary Released 14 July 14 Introduction This report presents the percentage of residents aged 12 years and older who have ever used illicit drugs
These are more than words. They are the principles and philosophy that drive every decision that ProMedica makes as an organization.
 Foreword Mission-driven. Community-based. Not-for-profit. These are more than words. They are the principles and philosophy that drive every decision that ProMedica makes as an organization. With people
Foreword Mission-driven. Community-based. Not-for-profit. These are more than words. They are the principles and philosophy that drive every decision that ProMedica makes as an organization. With people
Leveling the Playing Field
 Leveling the Playing Field Who s Using, Who s Not and How to Narrow the Gap Ilana M. Knopf, J.D. Albany Hilton, Kerry M. Snyder, J.D. January 28, 2015 Public Health Advocacy Institute at Northeastern University
Leveling the Playing Field Who s Using, Who s Not and How to Narrow the Gap Ilana M. Knopf, J.D. Albany Hilton, Kerry M. Snyder, J.D. January 28, 2015 Public Health Advocacy Institute at Northeastern University
Looking Toward State Health Assessment.
 CONNECTICUT DEPARTMENT OF PUBLIC HEALTH Policy, Planning and Analysis. Looking Toward 2000 - State Health Assessment. Table of Contents Glossary Maps Appendices Publications Public Health Code PP&A Main
CONNECTICUT DEPARTMENT OF PUBLIC HEALTH Policy, Planning and Analysis. Looking Toward 2000 - State Health Assessment. Table of Contents Glossary Maps Appendices Publications Public Health Code PP&A Main
Pennsylvania Department of Health 2003 Behavioral Risks of McKean County Adults Page 1
 2003 Behavioral Health Risks Of Adults Collaborative Board Pennsylvania Department of Health 2003 Behavioral Risks of Adults Page 1 Introduction The Centers for Disease Control and Prevention (CDC) and
2003 Behavioral Health Risks Of Adults Collaborative Board Pennsylvania Department of Health 2003 Behavioral Risks of Adults Page 1 Introduction The Centers for Disease Control and Prevention (CDC) and
Hull s Adult Health and Lifestyle Survey: Summary
 Hull s 211-212 Adult Health and Lifestyle Survey: Summary Public Health Sciences, Hull Public Health April 213 Front cover photographs of Hull are taken from the Hull City Council Flickr site (http://www.flickr.com/photos/hullcitycouncil/).
Hull s 211-212 Adult Health and Lifestyle Survey: Summary Public Health Sciences, Hull Public Health April 213 Front cover photographs of Hull are taken from the Hull City Council Flickr site (http://www.flickr.com/photos/hullcitycouncil/).
Community Health Needs Assessment
 Community Health Needs Assessment Scott County, Missouri This assessment will identify the health needs of the residents of Scott County, Missouri, and those needs will be prioritized and recommendations
Community Health Needs Assessment Scott County, Missouri This assessment will identify the health needs of the residents of Scott County, Missouri, and those needs will be prioritized and recommendations
Table 7.1 Summary information for lung cancer in Ireland,
 7 Lung cancer 7.1 Summary Lung cancer is the third most common cancer in Ireland, accounting for 15% of cancers in men and 9% in women, if non-melanoma skin cancer is excluded (table 7.1). Each year, approximately
7 Lung cancer 7.1 Summary Lung cancer is the third most common cancer in Ireland, accounting for 15% of cancers in men and 9% in women, if non-melanoma skin cancer is excluded (table 7.1). Each year, approximately
Burden of Illness Chapter 3
 Burden of Illness Chapter 3 Arlene S. Bierman, Farah Ahmad, Jan Angus, Richard H. Glazier, Mandana Vahabi, Cynthia Damba, Janice Dusek, Susan K. Shiller, Yingzi Li, Stephanie Ross, Gabriel Shapiro, Douglas
Burden of Illness Chapter 3 Arlene S. Bierman, Farah Ahmad, Jan Angus, Richard H. Glazier, Mandana Vahabi, Cynthia Damba, Janice Dusek, Susan K. Shiller, Yingzi Li, Stephanie Ross, Gabriel Shapiro, Douglas
CHS 2009 Baltimore City Community Health Survey: Summary Results Report
 CHS 2009 Baltimore City Community Health Survey: Summary Results Report About the Survey: A representative sample of 1,134 Baltimore residents participated in the Community Health Survey The survey reached
CHS 2009 Baltimore City Community Health Survey: Summary Results Report About the Survey: A representative sample of 1,134 Baltimore residents participated in the Community Health Survey The survey reached
2014 Butte County BUTTE COUNTY COMMUNITY HEALTH ASSESSMENT
 2014 Butte County BUTTE COUNTY COMMUNITY HEALTH ASSESSMENT EXECUTIVE SUMMARY 2015 2017 EXECUTIVE SUMMARY TOGETHER WE CAN! HEALTHY LIVING IN BUTTE COUNTY Hundreds of local agencies and community members
2014 Butte County BUTTE COUNTY COMMUNITY HEALTH ASSESSMENT EXECUTIVE SUMMARY 2015 2017 EXECUTIVE SUMMARY TOGETHER WE CAN! HEALTHY LIVING IN BUTTE COUNTY Hundreds of local agencies and community members
SMOKING STAGES OF CHANGE KEY MESSAGES
 KEY MESSAGES In Peel among current daily or occasional smokers: o 19% are not thinking are not thinking about quitting (pre-contemplation stage) in the next six months; o 21% are thinking about quitting
KEY MESSAGES In Peel among current daily or occasional smokers: o 19% are not thinking are not thinking about quitting (pre-contemplation stage) in the next six months; o 21% are thinking about quitting
Health System Members of the Milwaukee Health Care Partnership
 Health System Members of the Milwaukee Health Care Partnership Aurora Health Care Children s Hospital of Wisconsin Columbia St. Mary s Health System Froedtert Health Wheaton Franciscan Healthcare In Collaboration
Health System Members of the Milwaukee Health Care Partnership Aurora Health Care Children s Hospital of Wisconsin Columbia St. Mary s Health System Froedtert Health Wheaton Franciscan Healthcare In Collaboration
The following are recommendations to help public health better address seniors health.
 Public Health Mandate There is only one provincial requirement specifically targeted for seniors. It currently addresses falls in the elderly. Peel Public Health also addresses medication use through a
Public Health Mandate There is only one provincial requirement specifically targeted for seniors. It currently addresses falls in the elderly. Peel Public Health also addresses medication use through a
No one should be at risk of poor health because of their social and economic situations.
 HEALTH MATTERS No one should be at risk of poor health because of their social and economic situations. Members of municipal government play an important role in shaping policies that impact all aspects
HEALTH MATTERS No one should be at risk of poor health because of their social and economic situations. Members of municipal government play an important role in shaping policies that impact all aspects
The Canadian Community Health Survey: what s new in the 2015 cycle?
 CRDCN Webinar Series The Canadian Community Health Survey: what s new in the 2015 cycle? with Andrew MacKenzie Statistics Canada January 25, 2017 The Canadian Research Data Centre Network Improve access
CRDCN Webinar Series The Canadian Community Health Survey: what s new in the 2015 cycle? with Andrew MacKenzie Statistics Canada January 25, 2017 The Canadian Research Data Centre Network Improve access
Tobacco, Alcohol, and
 Healthier San Joaquin County Community Assessment 2011 Tobacco, Alcohol, and Drug Use Summary... 100 Indicators Tobacco Use... 101 Tobacco Use Among Pregnant Women... 103 Alcohol Consumption... 104 Adult
Healthier San Joaquin County Community Assessment 2011 Tobacco, Alcohol, and Drug Use Summary... 100 Indicators Tobacco Use... 101 Tobacco Use Among Pregnant Women... 103 Alcohol Consumption... 104 Adult
Cancer in Halton. Halton Region Cancer Incidence and Mortality Report
 Cancer in Halton Halton Region Cancer Incidence and Mortality Report 2008 2012 The Regional Municipality of Halton March 2017 Reference: Halton Region Health Department, Cancer in Halton: Halton Region
Cancer in Halton Halton Region Cancer Incidence and Mortality Report 2008 2012 The Regional Municipality of Halton March 2017 Reference: Halton Region Health Department, Cancer in Halton: Halton Region
Healthy Futures: 2014 Toronto Public Health Student Survey. Dr. David McKeown March 9, 2015
 Healthy Futures: 2014 Toronto Public Health Student Survey Dr. David McKeown March 9, 2015 Health Assessment and Surveillance Health assessment and surveillance is a foundation of public health Health
Healthy Futures: 2014 Toronto Public Health Student Survey Dr. David McKeown March 9, 2015 Health Assessment and Surveillance Health assessment and surveillance is a foundation of public health Health
Normalizing Conversation, Not Consumption
 Normalizing Conversation, Not Consumption A Public Health Approach to Cannabis Canadian Public Health Association A Public Health Approach to Cannabis Project Overview A public health approach emphasizes
Normalizing Conversation, Not Consumption A Public Health Approach to Cannabis Canadian Public Health Association A Public Health Approach to Cannabis Project Overview A public health approach emphasizes
Maternal and Infant Nutrition Briefs
 Maternal and Infant Nutrition Briefs January/February 2004 A research-based newsletter prepared by the University of California for professionals interested in maternal and infant nutrition What are Infants
Maternal and Infant Nutrition Briefs January/February 2004 A research-based newsletter prepared by the University of California for professionals interested in maternal and infant nutrition What are Infants
How does socio-economic status influence body weight? The mediating role of psychological distress and maladaptive eating behaviours
 How does socio-economic status influence body weight? The mediating role of psychological distress and maladaptive eating behaviours Charlotte A. Hardman, Paul Christiansen, Joanne Dickson & Jade Stewart
How does socio-economic status influence body weight? The mediating role of psychological distress and maladaptive eating behaviours Charlotte A. Hardman, Paul Christiansen, Joanne Dickson & Jade Stewart
The Cecil County Community Health Survey 2009 Report
 The Cecil County Community Health Survey 2009 Report May 2010 Cecil County Health Department 401 Bow Street Elkton, Maryland 21921 410-996-5113 www.cecilcountyhealth.org Acknowledgement Thank you again
The Cecil County Community Health Survey 2009 Report May 2010 Cecil County Health Department 401 Bow Street Elkton, Maryland 21921 410-996-5113 www.cecilcountyhealth.org Acknowledgement Thank you again
Influenza Vaccination Coverage in British Columbia Canadian Community Health Survey 2011 & 2012
 Background The Canadian Community Health Survey (CCHS) is a cross-sectional survey that collects information related to the health status, health care utilization and health determinants of the Canadian
Background The Canadian Community Health Survey (CCHS) is a cross-sectional survey that collects information related to the health status, health care utilization and health determinants of the Canadian
County Health Rankings Monroe County 2016
 Health Rankings Monroe 2016 Graphics of Health Rankings Include All Counties In the North Central Health District Public Health for Middle Georgia Serving Baldwin, Bibb, Crawford, Hancock, Houston, Jasper,
Health Rankings Monroe 2016 Graphics of Health Rankings Include All Counties In the North Central Health District Public Health for Middle Georgia Serving Baldwin, Bibb, Crawford, Hancock, Houston, Jasper,
CANCER. in north carolina Report. cancer and income with a special report on cancer, income, and racial differences
 CANCER in north carolina 2008 Report cancer and income with a special report on cancer, income, and racial differences purpose During 2007 cancer passed heart disease as the number one cause of death among
CANCER in north carolina 2008 Report cancer and income with a special report on cancer, income, and racial differences purpose During 2007 cancer passed heart disease as the number one cause of death among
Community Health Priority: Alcohol & Other Drug Misuse and Abuse
 Alcohol & Other Drug Misuse and Abuse Melissa Dotter, MS Drug Free Communities Coordinator 715.261.1962 melissa.dotter@co.marathon.wi.us Creating a culture in communities where alcohol is used responsibly
Alcohol & Other Drug Misuse and Abuse Melissa Dotter, MS Drug Free Communities Coordinator 715.261.1962 melissa.dotter@co.marathon.wi.us Creating a culture in communities where alcohol is used responsibly
2016 PRC Community Health Needs Assessment
 2016 PRC Community Health Needs Assessment Staunton City, Waynesboro City, and Augusta County, Virginia Prepared for: Augusta Health By Professional Research Consultants, Inc. The PRC Community Health
2016 PRC Community Health Needs Assessment Staunton City, Waynesboro City, and Augusta County, Virginia Prepared for: Augusta Health By Professional Research Consultants, Inc. The PRC Community Health
Primary Care Demographic and Medical History Form
 Primary Care Demographic and Medical History Form PATIENT DEMOGRAPHIC INFORMATION: Patient Name: Date of Birth: / / Street Address: City: State: Zip: Home Phone #: Work #: Cell #: Email: Preferred Method
Primary Care Demographic and Medical History Form PATIENT DEMOGRAPHIC INFORMATION: Patient Name: Date of Birth: / / Street Address: City: State: Zip: Home Phone #: Work #: Cell #: Email: Preferred Method
Susan Kaai, PhD University of Waterloo, Ontario, Canada NBATC Webinar Slides February 10, 2015
 Susan Kaai, PhD University of Waterloo, Ontario, Canada NBATC Webinar Slides February 10, 2015 Background Study question and rationale Literature review Methods Results and implications Strengths and limitations
Susan Kaai, PhD University of Waterloo, Ontario, Canada NBATC Webinar Slides February 10, 2015 Background Study question and rationale Literature review Methods Results and implications Strengths and limitations
Demand and Burden of Dental Care in Canadian Households. Mustafa Andkhoie, MPH PhD student, Epidemiology University of Saskatchewan May 27 th, 2015
 Demand and Burden of Dental Care in Canadian Households Mustafa Andkhoie, MPH PhD student, Epidemiology University of Saskatchewan May 27 th, 2015 Introduction Dental Health Expenditure In Canada second-largest
Demand and Burden of Dental Care in Canadian Households Mustafa Andkhoie, MPH PhD student, Epidemiology University of Saskatchewan May 27 th, 2015 Introduction Dental Health Expenditure In Canada second-largest
HEALTHY AGING IN TORONTO
 MARCH 2017 HEALTHY AGING IN TORONTO Seniors aged 65 and older represent a large and quickly growing population group in Toronto. This stage of life is a time when many begin to face increased health challenges,
MARCH 2017 HEALTHY AGING IN TORONTO Seniors aged 65 and older represent a large and quickly growing population group in Toronto. This stage of life is a time when many begin to face increased health challenges,
Statistics on Alcohol: England, 2010
 Statistics on Alcohol: England, 2010 Copyright 2010, The Health and Social Care Information Centre. All Rights Reserved. Copyright 2010, The Health and Social Care Information Centre. All Rights Reserved.
Statistics on Alcohol: England, 2010 Copyright 2010, The Health and Social Care Information Centre. All Rights Reserved. Copyright 2010, The Health and Social Care Information Centre. All Rights Reserved.
8 Key Findings from the 2018 Community Cannabis Survey
 8 Key Findings from the 2018 Community Cannabis Survey MARCH 2019 Author Auburn Larose, Epidemiologist Planning and Evaluation Services research@healthunit.ca 1 8 Key Findings from the 2018 Community Cannabis
8 Key Findings from the 2018 Community Cannabis Survey MARCH 2019 Author Auburn Larose, Epidemiologist Planning and Evaluation Services research@healthunit.ca 1 8 Key Findings from the 2018 Community Cannabis
Canadian Adult and Youth Opinions on the Sizing of Health Warning Messages HC H /001/CB
 Canadian Adult and Youth Opinions on the Sizing of Health Warning Messages HC-003-155-9925 H4097-9-0017/001/CB Prepared for Health Canada Office for Tobacco Control October 1999 Prepared by Environics
Canadian Adult and Youth Opinions on the Sizing of Health Warning Messages HC-003-155-9925 H4097-9-0017/001/CB Prepared for Health Canada Office for Tobacco Control October 1999 Prepared by Environics
Smoking-related Behaviour and Attitudes, 2007
 Omnibus Survey Report No. 36 Smoking-related Behaviour and Attitudes, 2007 A report on research using the National Statistics Omnibus Survey produced on behalf of the NHS Information Centre for health
Omnibus Survey Report No. 36 Smoking-related Behaviour and Attitudes, 2007 A report on research using the National Statistics Omnibus Survey produced on behalf of the NHS Information Centre for health
Analysis of Wirral Stop Smoking Service clients using Mosaic Public Sector. Produced by Wirral Council Performance & Public Health Intelligence Team
 Analysis of Wirral Stop Smoking Service clients using Mosaic Public Sector Produced by Wirral Council Performance & Public Health Intelligence Team February 2015 Introduction Mosaic is a geo-demographic
Analysis of Wirral Stop Smoking Service clients using Mosaic Public Sector Produced by Wirral Council Performance & Public Health Intelligence Team February 2015 Introduction Mosaic is a geo-demographic
Indian CHRNA (Community Health Resources and Needs Assessment)
") (Community Health Resources and Needs Assessment) Between 2014 and 2015, the Center for the Study of Asian American Health collected 113 surveys in the Indian community in NYC in partnership with community
(Community Health Resources and Needs Assessment) Between 2014 and 2015, the Center for the Study of Asian American Health collected 113 surveys in the Indian community in NYC in partnership with community
Cancer Risk Factors in Ontario. Alcohol
 Cancer Risk Factors in Ontario Alcohol Prepared by Stephanie Young, Elisa Candido, Beth Theis and Loraine Marrett, Prevention and Surveillance, Prevention and Cancer Control, Cancer Care Ontario. The authors
Cancer Risk Factors in Ontario Alcohol Prepared by Stephanie Young, Elisa Candido, Beth Theis and Loraine Marrett, Prevention and Surveillance, Prevention and Cancer Control, Cancer Care Ontario. The authors