Hepatitis C: Newest Treatment Options and What To Do When We Cure It!
|
|
|
- Sharyl Anderson
- 6 years ago
- Views:
Transcription
1 Hepatitis C: Newest Treatment Options and What To Do When We Cure It! Richard Kalman, MD Division of Hepatology Department of Transplantation Einstein Medical Center Learning Objectives Scope of HCV How far we have come Choosing individual therapy today (near) future therapies Post SVR monitoring 1

2 Learning Objectives Scope of HCV How far we have come Choosing individual therapy today (near) future therapies Post SVR monitoring Asia, Africa Have Highest HCV Burden million infections worldwide 3 4 million new infections every year 700,000 die every year from complications related to HCV Still fewer than the 240 million infected with HBV who.gov Thomas DL. Nature Medicine Lozano R. Lancet

 population The number chronically infected with HCV in the US may be even higher")
3 Regional Differences in Genotype Genotype 1 (79%), the most common in the U.S. Followed by 2,3 Antiviral choice, duration and efficacy affected by HCV genotype / subtype who.gov Messina JP. Hepatology US HCV Prevalence Difficult to Estimate 3.2 million people are chronically infected with HCV based on NHANES ( ) population The number chronically infected with HCV in the US may be even higher Accounting for high risk populations not sampled in NHANES 45 60% of people with HCV are unaware of the infection 360, ,000 are homeless or incarcerated Armgstrong G. Ann Intern Med cdc.gov Chak E. Liver Int Denniston M. Ann Intern Med
 Household")
4 Screening for Hepatitis C Most important risk factor is past or current injection drug use Additional risk factors include: Receiving a blood transfusion before 1992 Long term hemodialysis Being born to an HCV infected mother Incarceration Intranasal drug use Getting an unregulated tattoo, and other percutaneous exposures Heterosexual sexual transmission rare (HIV + MSM highest risk) Household transmission is possible Adults born between 1945 and 1965 ( Baby Boomers ) Account for ~70% HCV in the US 35% have F3/4 fibrosis Grade B recommendation by USPSTF in 2013 to screen this population Armgstrong G. Ann Intern Med Yaphe S. Sex Transm Infect McGarty LJ. Hepatology Natural History of HCV Acute hepatitis C 55-85% Clearance of HCV RNA 15% 45% Fulminant Hepatitis < 1% Chronic infection Extrahepatic Disease 70% Chronic hepatitis Cirrhosis 20% 0.8% per year 1-4%/yr HCC Time (yr) 4-5%/yr Decompensation Massoumy B. Best Pract Res Clin Gastroenterol
5 HCV Impacts Morbidity and Mortality 73.4% of HCV related deaths occur between years of age Median age was 57 ~20 years less than average person in US HCV is the leading cause of liver transplant in US Several extra hepatic morbid conditions are also linked to HCV infection Cryoglobulinemia, vasculitis, lymphoproliferative disorders, MPGN, depression Davis GL. Gastroenterology Smith BD. MMWR Recomm Rep Ali A. Cleve Clin J Med Learning Objectives Scope of HCV How far we have come Choosing individual therapy today (near) future therapies Post SVR monitoring 5

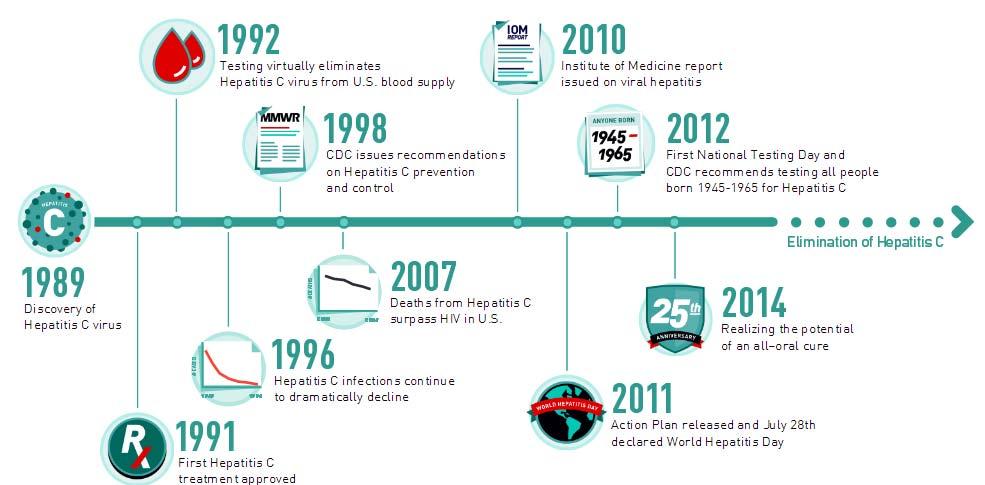
6 How Far We Have Come How Far We Have Come cdc.gov 6
")
7 How Far We Have Come Manns MP. Nature Reviews Drug Discovery Learning Objectives Scope of HCV How far we have come Choosing individual therapy today (near) future therapies Post SVR monitoring 7
8 SVR is the Goal of Treating HCV Primary goal is virus eradication Clinical Trial definition is Sustained Virologic Response (SVR) SVR12: Undetectable HCV RNA 12 weeks after treatment (newer studies) SVR24: Undetectable HCV RNA 24 weeks after treatment (older studies) SVR associated with high likelihood long term cure In phase III Sofosbuvir trials, 7/12 pts with SVR 12 but not SVR 24 found to have reinfection Secondary goal is improving outcomes Prevent progression to cirrhosis and incidence of HCC Reduce need for liver transplantation Improve / enhance survival HCV RNA 4 years after SVR 0.9% Negative 99.1% Positive Swain MG. Gastroenterology Sarrazin C. EASL abstract Van Der Meer AJ. JAMA SVR Associated with Improved Outcomes Lee MH. J Infect Dis

9 Treatment Options Asselah T. Liver International Antiviral Class Characteristics NS3 Protease Inhibitors NS5B nucleoside/ tide NS5B nonnucleoside NS5A Inhibitors Antiviral effect Genotype Resistance barrier Examples +++ to and 4 Moderate Simeprevir Grazoprevir ++ to High Sofosbuvir ++ to Low Dasabuvir Low Ledipasvir Elbasvir Velpatasvir 9
10 Current Approved HCV regimens (abbreviated) Genotype 1 SOF/LDV +/ RBV for 8 24 weeks OBV/PTV/RTV + DSV +/ RBV for weeks GZR/EBV +/ RBV for weeks DCV + SOF +/ RBV for weeks SMV + SOF +/ RBV for 12 weeks SOF/VEL for 12 weeks Genotype 3 SOF/VEL for 12 weeks DCV + SOF +/ RBV weeks SOF + RBV + PEG for 12 weeks Genotype 4 SOF/VEL for 12 weeks GZR/EBV +/ RBV for weeks OBV(Pro)/PTV/RTV +/ RBV for weeks SOF/LDV +/ RBV for weeks Genotype 2 SOF/VEL for 12 weeks SOF + RBV for weeks DCV + SOF +/ RBV weeks SOF + RBV + PEG for 12 weeks for full guidance please refer to Genotype 5 or 6 SOF/LDV +/ RBV 12 weeks SOF/VEL for 12 weeks SOF + RBV + PEG for 12 weeks RAVs Alter Some Treatment Regimens Resistance associated variants (RAV) occur during viral breakthrough and after treatment The approach to RAV treatment is rapidly changing NS5A reduces SVR in GZP/EBR x 12 weeks, but negated by extension to weeks NS3 RAVS are rare, routine baseline testing not indicated but may consider if using NS3 again soon after failure 10
11 Not all RAVs persist after treatment After 3D regimen (OBV/PTV/RTV + DSV) not all RAVs remain NS3/4A (all) 46% at 24 weeks, 9% at 48 weeks NS5A (all) 97% at 24 weeks, 96% at 48 weeks NS5B (all) 75% at 24 weeks, 57% at 48 weeks After GZR/EBV 85% NS5A persist SOF + GZR/EBR 37% NS5A persist SOF/LDV 65% NS5A persist Krishnan P. EASL Sulkowski M. Lancet Zeuzem S. Ann Intern Med Sarrazin C. AASLD 2014 Implications: SOF/VEL SOF/VEL has high SVR rates in GT 1 6 SOF/VEL is superior to SOF/RBV x 12 weeks for GT2 SOF/VEL is superior to SOF/RBV x 24 weeks in GT3 Baseline RAVs do not appear to influence SVR Well tolerated, good safety profile Not approved in post transplant setting Not safe in renal insufficiency 11
 29 (12) 80 (29) 27 (23) 5 (14) 6 (15) 220 (21) Platelets <100 x 10 3 /µl 21 (6) 4 (2) 25 (9) 8 (7) 1 (3) 3 (7) 62 (6) Albumin <3.")
 44 (18) 71 (26) 52 (45) 11 (31) 3 (7) 291 (28) Black race 25 (8) 19 (8) 3 (1) 14 (12) 0 0 61 (6) Age 65 years 36 (11) 53 (22) 7 (3) 11 (10) 16 (46) 0 123 (12) BMI 35")
12 SOF/VEL x 12 weeks, All GTs Retrospective integrated analysis of data from 1,035 SOF/VEL patients in ASTRAL-1, -2, and -3 Patients, n (%) GT1 n=328 Baseline Demographics GT2 n=238 GT3 n=277 GT4 n=116 GT5 n=35 GT6 n=41 Total N=1035 Cirrhosis 73 (22) 29 (12) 80 (29) 27 (23) 5 (14) 6 (15) 220 (21) Platelets <100 x 10 3 /µl 21 (6) 4 (2) 25 (9) 8 (7) 1 (3) 3 (7) 62 (6) Albumin <3.5 mg/dl 6 (2) 1 (<1) 8 (3) 6 (5) (2) Fibroscan 15 kpa 30 (16) 9 (7) 40 (20) 17 (19) 4 (17) 5 (19) 105 (16) HCV RNA 800,000 IU/mL 255 (78) 186 (78) 191 (69) 74 (64) 26 (74) 31 (76) 763 (74) Treatment experienced 110 (34) 44 (18) 71 (26) 52 (45) 11 (31) 3 (7) 291 (28) Black race 25 (8) 19 (8) 3 (1) 14 (12) (6) Age 65 years 36 (11) 53 (22) 7 (3) 11 (10) 16 (46) (12) BMI 35 kg/m 2 20 (6) 18 (8) 21 (8) 8 (7) 3 (9) 0 70 (7) HbA1c 6.5% 21 (6) 9 (4) 13 (5) 10 (9) 3 (9) 4 (10) 60 (6) NS5A RAVs (15% cut off) 50 (15) 146 (61) 31 (11) 69 (59) 3 (9) 19 (46) 318 (31) Agarwal K. EASL SAT 195 SOF/VEL x 12 weeks, All GTs Agarwal K. EASL SAT 195 Jacobson I. EASL SAT
13 AASLD Guidelines Recommended GT 1, Treatment Naïve GT1a w/o cirrhosis GT1b w/o cirrhosis GT1a w/cirrhosis GT1b w/cirrhosis SOF/LDV 12 weeks 12 weeks 12 weeks 12 weeks OBV/PTV/RTV + DSV 12 weeks (+RBV) 12 weeks 12 weeks GZR/EBV 12 weeks (if no NS5A RAV, otherwise 16 with RBV) DCV + SOF 12 weeks 12 weeks 12 weeks 12 weeks (if no NS5A RAV, otherwise 16 with RBV) 12 weeks SMV + SOF 12 weeks (if no Q80K) 12 weeks SOF/VEL 12 weeks 12 weeks 12 weeks 12 weeks for full guidance please refer to AASLD guidelines Recommended GT 2 6, Treatment Naïve GT2 w/o cirrhosis GT2 w/ cirrhosis GT3, w/o cirrhosis GT3 w/ cirrhosis GT4 GT 5/6 SOF/VEL 12 weeks 12 weeks 12 weeks 12 weeks 12 weeks 12 weeks DCV + SOF 12 weeks 24 weeks (+/ RBV) SOF/LDV 12 weeks 12 weeks GZR/EBV 12 weeks OBV/PTV/ RTV + DSV +RBV 12 weeks for full guidance please refer to 13
14 Hard to Treat Populations Disappearing Decompensated cirrhosis SOF/VEL + RBV x 12 wk or SOF/VEL x 24 weeks Post liver transplant All approved combinations include ribavirin PTV increases Tacrolimus and Sirolimus levels HIV/HCV coinfection Beware DDI CKD No Sofosbuvir regimens if CrCl < 30 Can use 3D if not on HD Can use GZR/EBV regardless of HD Treatment experienced Interferon DAA DAA Failures GZP/EBR + SOF + RBV x 12 weeks (n=25) C SWIFT retreatment 100% SVR12 (including 9/9 with NS3+NS5A RAVs) OBV/PTV/r + DSV+ SOF (n=22) SVR12 21/22 overall (6/6 in cirrhosis) SOF/VEL + RBV x 24 weeks SVR12 59/65 overall in GT1 3 SOF/VEL + GS 9857(PI) x 12 weeks (n=128) SVR12 127/128 Overall in GT1 6 Lawitz E. EASL SAT 148 Poordad F. EASL SAT 156 Gane EJ EASL PS024 Lawitz E. EASL 2016.PS008 14
15 Acute HCV Classically advised waiting to see if patient develops persistent infection HEPNET Acute HCV study Single arm, prospective, multicenter 20 patients (no HIV, 11 GT1a) with acute HCV Known exposure < 4 mo, documented seroconversion, ALT > 10 x ULN Mean ALT 463, Mean bilirubin 24 mg/dl All 20 patients achieved SVR12 Detarding K. EASL 2016 LB08 Daily PPI Did NOT Effect SVR in Real World TRIO Cohort PPI use may decrease absorption of LDV 2,034 treated with DAA for 8, 12 or 24 weeks with our without RBV SVR rate 96% without PPI and 94% with PPI Type of PPI, dose, and duration had no effect on SVR BID PPI reduced SVR to 91.7% on univariate but not multivariate analysis Authors advise caution when using BID PPI Afdhal N. EASL LBP519 15
 future therapies Post SVR")
16 Learning Objectives Scope of HCV How far we have come Choosing individual therapy today (near) future therapies Post SVR monitoring 16
17 Phase 2 C Crest 1 and 2 Trial of Merck triple therapy PI/NS5A/Nuc GZR/MK 8408/MK 3682 x 8 weeks Non cirrhotic patients, GT1, 2 and 3 (combined 2 dosing groups for MK 3682) GT1 SVR24 44/47 GT2 SVR24 25/30 GT3 SVR24 40/ GT1 GT2 GT3 SVR No SVR Gane E. EASL SAT 139 SURVEYOR 1 and 2: Phase 2, non cirrhotic for 8 (GT1/2/3) and 12 weeks (4/5/6) ABT 493 (NS3/4A PI) + ABT 530 (NS5A inhibitor) High barrier to resistance, potent against common RAVs, and <1% renal excretion Genotype 1 and 2 (Surveyor 1 and 2) SVR12 33/34 GT1 and 53/54 GT2 Genotype 4, 5 and 6 (Surveyor 1 Part 2) 100% SVR12 for all genotypes; regardless of prior treatment Hx or baseline variants Genotype 3 28/29 SVR12 including 7/29 with F3 fibrosis GT1 GT2 GT3 SVR No SVR Gane E. EASL SAT 137 Poordad EASL SAT 157 Muir A. EASL PS098 17
18 RG 101 with 4 weeks of Oral DAA treatment x 4 weeks, Phase 2 study RG 101 targets mir 122 microrna abundant in the liver that HCV requires for replication Acts earlier in viral life cycle, before nonstructural proteins are even built on which traditional DAAs act N=79, 77% GT1 and 23%G4 DAA included LDV/SOF, SMV, or DCV Received 2mg/kg SQ on Day and Day patients with 8 weeks of follow up 97% with undetectable viral load 14 patients with 12 weeks of follow up SVR12 100% Horvath G. EASL GS08 Learning Objectives Scope of HCV How far we have come Choosing individual therapy today (near) future therapies Post SVR monitoring 18
19 Rechecking HCV RNA After SVR After SVR24, no indication to recheck HCV RNA May reconsider if liver enzymes become abnormal or if risk of reinfection Do not repeat HCV AB Advise patients AB will remain positive in case erroneously checked by another provider A Path Divided Early (F0 F2) Fibrosis Stage Pre Treatment Advanced (F3 F4) 19



20 Measuring Fibrosis Post SVR With Early Fibrosis Consider annual liver tests and CBC No indication for HCC surveillance No indication for variceal surveillance Remain vigilant against other causes of chronic liver disease Risk factors for NAFLD Risk factors of alcohol mediated injury Social alcohol use may be acceptable Check Hepatitis B status Consider hemochromatosis if labs remain abnormal 20
21 Post SVR With Advanced Fibrosis Monitor for signs of decompensation Perform screening for varices and HCC HCC risk persists at least 8 years after SVR Some data may suggest early HCC recurrent after DAA Monitor MELD and refer to transplant center for MELD > 15 Advocate strict alcohol sobriety If risk factors for NAFLD are present, attempt BMI < 25, and tight control of DM and hyperlipidemia Aleman S. Clin Infect Dis Reig M. Journal of Hepatol Summary Screening at risk population, including Baby Boomers, for HCV is recommended (Grade B, USPSTF) SVR is associated with improved outcomes including reduced all cause mortality, liver cancer and cirrhosis Every GT now has multiple recommended treatment options by AASLD (aside from GT2) SOF/VEL is a powerful new agent with high SVR rates in all genotypes DAA failures have treatment options that can be used, but limited tremendously by cost of these regimens Triplet regimens will be expected next year with high SVR rates in as little as 8 weeks Post SVR monitoring relies on assessing for advanced fibrosis, performing routine cirrhotic care when indicated and limiting other risk factors for advanced fibrosis 21
22 Thank You! 22
Baseline and acquired viral resistance to DAAs: how to test and manage
 Baseline and acquired viral resistance to DAAs: how to test and manage Round table discussion by Marc Bourliere, Robert Flisiak, Vasily Isakov, Mark Sulkowsky & Konstantin Zhdanov Prevalence of baseline
Baseline and acquired viral resistance to DAAs: how to test and manage Round table discussion by Marc Bourliere, Robert Flisiak, Vasily Isakov, Mark Sulkowsky & Konstantin Zhdanov Prevalence of baseline
Genotype 1 HCV in 2016: Clinical Decision Making in a Time of Plenty
 Genotype 1 HCV in 216: Clinical Decision Making in a Time of Plenty Ira M. Jacobson, MD Chair, Department of Medicine Mount Sinai Beth Israel Senior Faculty and Vice-Chair, Department of Medicine Icahn
Genotype 1 HCV in 216: Clinical Decision Making in a Time of Plenty Ira M. Jacobson, MD Chair, Department of Medicine Mount Sinai Beth Israel Senior Faculty and Vice-Chair, Department of Medicine Icahn
Hepatitis C in Special Populations
 Hepatitis C in Special Populations David E. Bernstein, MD, FACG Vice Chairman of Medicine for Clinical Trials Chief, Division of Hepatology and Sandra Atlas Bass Center for Liver Diseases Northwell Health
Hepatitis C in Special Populations David E. Bernstein, MD, FACG Vice Chairman of Medicine for Clinical Trials Chief, Division of Hepatology and Sandra Atlas Bass Center for Liver Diseases Northwell Health
How to optimize treatment in G3 patients? Jérôme GOURNAY, MD Hépatologie Centre Hospitalier Universitaire de Nantes France
 How to optimize treatment in G3 patients? Jérôme GOURNAY, MD Hépatologie Centre Hospitalier Universitaire de Nantes France Paris Hepatitis Conference, January 12, 2016 Disclosures I have received funding
How to optimize treatment in G3 patients? Jérôme GOURNAY, MD Hépatologie Centre Hospitalier Universitaire de Nantes France Paris Hepatitis Conference, January 12, 2016 Disclosures I have received funding
2017 Bruce Lucas Hepatology and Liver Transplant Symposium October 13th 2017 Management of Hepatitis C in Pre- and Post-Transplant Patients
 2017 Bruce Lucas Hepatology and Liver Transplant Symposium October 13th 2017 Management of Hepatitis C in Pre- and Post-Transplant Patients Jens Rosenau, MD Associate Professor of Medicine Acting Director
2017 Bruce Lucas Hepatology and Liver Transplant Symposium October 13th 2017 Management of Hepatitis C in Pre- and Post-Transplant Patients Jens Rosenau, MD Associate Professor of Medicine Acting Director
HCV Resistance Clinical Aspects. Sanjay Bhagani Royal Free Hospital/UCL London
 HCV Resistance Clinical Aspects Sanjay Bhagani Royal Free Hospital/UCL London DAAs in 2018, and beyond % patients % patients Changing characteristics of patients treated with DAA over time Prospective,
HCV Resistance Clinical Aspects Sanjay Bhagani Royal Free Hospital/UCL London DAAs in 2018, and beyond % patients % patients Changing characteristics of patients treated with DAA over time Prospective,
HCV Infection: EASL Clinical Practice Guidelines Francesco Negro University Hospital Geneva Switzerland
 HCV Infection: EASL Clinical Practice Guidelines 2016 Francesco Negro University Hospital Geneva Switzerland Panel Codinat: Jean-Michel Pawlotsky Panel: Alessio Aghemo David Back Geoffrey Dusheiko Xavier
HCV Infection: EASL Clinical Practice Guidelines 2016 Francesco Negro University Hospital Geneva Switzerland Panel Codinat: Jean-Michel Pawlotsky Panel: Alessio Aghemo David Back Geoffrey Dusheiko Xavier
Viva La Revolución: Options to Combat Hepatitis C
 Viva La Revolución: Options to Combat Hepatitis C David L. Wyles, MD Professor of Medicine University of Colorado Chief, Division of Infectious Disease Denver Health Learning Objectives After attending
Viva La Revolución: Options to Combat Hepatitis C David L. Wyles, MD Professor of Medicine University of Colorado Chief, Division of Infectious Disease Denver Health Learning Objectives After attending
Treatment of HCV infection in daily clinical practice. Which are the optimal options for Genotypes 2 and 3? Jiannis Vlachogiannakos
 Treatment of HCV infection in daily clinical practice. Which are the optimal options for Genotypes 2 and 3? Jiannis Vlachogiannakos Associate Professor of Gastroenterology Academic Department of Gastroenterology
Treatment of HCV infection in daily clinical practice. Which are the optimal options for Genotypes 2 and 3? Jiannis Vlachogiannakos Associate Professor of Gastroenterology Academic Department of Gastroenterology
HCV Treatment of Genotype 1: Now and in the Future
 HCV Treatment of Genotype 1: Now and in the Future Bruce R. Bacon, MD, FACG James F. King, MD Endowed Chair in Gastroenterology Professor of Internal Medicine Co-Director of the Abdominal Transplant Program
HCV Treatment of Genotype 1: Now and in the Future Bruce R. Bacon, MD, FACG James F. King, MD Endowed Chair in Gastroenterology Professor of Internal Medicine Co-Director of the Abdominal Transplant Program
Hepatitis C Resistance Associated Variants (RAVs)
") Hepatitis C Resistance Associated Variants (RAVs) Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Nothing to disclose Disclosure
Hepatitis C Resistance Associated Variants (RAVs) Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Nothing to disclose Disclosure
Saeed Hamid, MD Alex Thompson, MD, PhD
 Saeed Hamid, MD Alex Thompson, MD, PhD 1 We will review some top line data from EASL Majority of the time discussing how the data affects daily practice 2 Grazoprevir (GZR; MK-5172) + Elbasvir (EBR; MK-
Saeed Hamid, MD Alex Thompson, MD, PhD 1 We will review some top line data from EASL Majority of the time discussing how the data affects daily practice 2 Grazoprevir (GZR; MK-5172) + Elbasvir (EBR; MK-
HCV Treatment Failure: What Next? Dr Ashley Brown, Imperial College Healthcare NHS Trust, London
 HCV Treatment Failure: What Next? Dr Ashley Brown, Imperial College Healthcare NHS Trust, London European HIV Hepatitis Co-infection Conference QEII Conference Centre 10 th December 2015 Dr Ashley Brown
HCV Treatment Failure: What Next? Dr Ashley Brown, Imperial College Healthcare NHS Trust, London European HIV Hepatitis Co-infection Conference QEII Conference Centre 10 th December 2015 Dr Ashley Brown
Why make this statement?
 HCV Council 2014 10 clinical practice statements were evaluated by the Council A review of the available literature was conducted The level of support and level of evidence for the statements were discussed
HCV Council 2014 10 clinical practice statements were evaluated by the Council A review of the available literature was conducted The level of support and level of evidence for the statements were discussed
The Changing World of Hepatitis C
 The Changing World of Hepatitis C Alnoor Ramji Gastroenterology & Hepatology Clinical Associate Professor Division of Gastroenterology University Of British Columbia St. Paul s Hospital Site Disclosures
The Changing World of Hepatitis C Alnoor Ramji Gastroenterology & Hepatology Clinical Associate Professor Division of Gastroenterology University Of British Columbia St. Paul s Hospital Site Disclosures
Initial Treatment of HCV G Hugo E. Vargas, MD Professor of Medicine Medical, Director Office of Clinical Research Mayo Clinic Arizona
 Initial Treatment of HCV G1 2016 Hugo E. Vargas, MD Professor of Medicine Medical, Director Office of Clinical Research Mayo Clinic Arizona Disclosure Information Disclosure Information Dr. Vargas receives
Initial Treatment of HCV G1 2016 Hugo E. Vargas, MD Professor of Medicine Medical, Director Office of Clinical Research Mayo Clinic Arizona Disclosure Information Disclosure Information Dr. Vargas receives
Case 4: A 61-year-old man with HCV genotype 3 with cirrhosis. Ira M. Jacobson, M.D. Weill Cornell Medical College New York, New York USA
 Case 4: A 61-year-old man with HCV genotype 3 with cirrhosis Ira M. Jacobson, M.D. Weill Cornell Medical College New York, New York USA 1 Genotype 3 case 61-year-old man with HCV genotype 3 Cirrhosis on
Case 4: A 61-year-old man with HCV genotype 3 with cirrhosis Ira M. Jacobson, M.D. Weill Cornell Medical College New York, New York USA 1 Genotype 3 case 61-year-old man with HCV genotype 3 Cirrhosis on
4/30/2015. Interactive Case-Based Presentations and Audience Discussion. Debika Bhattacharya, MD, MSc. Learning Objectives
 4/3/215 Interactive Case-Based Presentations and Audience Discussion Debika Bhattacharya, MD, MSc Assistant Clinical Professor University of California Los Angeles Los Angeles, California Formatted:4-27-215
4/3/215 Interactive Case-Based Presentations and Audience Discussion Debika Bhattacharya, MD, MSc Assistant Clinical Professor University of California Los Angeles Los Angeles, California Formatted:4-27-215
Hepatitis C in Disclosures
 Hepatitis C in 2018 Sandeep Mukherjee, MD CHI Health and Creighton University Medical Center Division of Gastroenterology Grant support: Abbvie Disclosures Speaker: Abbvie, Gilead, Merck Section editor
Hepatitis C in 2018 Sandeep Mukherjee, MD CHI Health and Creighton University Medical Center Division of Gastroenterology Grant support: Abbvie Disclosures Speaker: Abbvie, Gilead, Merck Section editor
A One-day Scientific Conference: Updates on Hepatitis C Treatments along with Consensus on Management of Hepatitis C in Iran
 A One-day Scientific Conference: Updates on Hepatitis C Treatments along with Consensus on Management of Hepatitis C in Iran Teheran, 22 July 2016 Massimo Colombo Treatment of HCV genotype 1 & 4 with DAAs
A One-day Scientific Conference: Updates on Hepatitis C Treatments along with Consensus on Management of Hepatitis C in Iran Teheran, 22 July 2016 Massimo Colombo Treatment of HCV genotype 1 & 4 with DAAs
Direct-acting Antiviral (DAA) Regimens in Late-stage Development: Which Patients Should Wait? Fred Poordad, MD
 Regimens in Late-stage Development: Which Patients Should Wait? Fred Poordad, MD") Direct-acting Antiviral (DAA) Regimens in Late-stage Development: Which Patients Should Wait? Fred Poordad, MD The HCV Lifecycle: Multiple Targets Polymerase Inhibitors Protease Inhibitors NS5A Inhibitors
Direct-acting Antiviral (DAA) Regimens in Late-stage Development: Which Patients Should Wait? Fred Poordad, MD The HCV Lifecycle: Multiple Targets Polymerase Inhibitors Protease Inhibitors NS5A Inhibitors
HCV Treatment in 2016
 HCV Treatment in 2016 Hugo E. Vargas, MD Professor of Medicine Mayo College of Medicine Medical Director, Clinical Trials Office Vice Chair, Department of Research Educational Goals Caveats: Cannot cover
HCV Treatment in 2016 Hugo E. Vargas, MD Professor of Medicine Mayo College of Medicine Medical Director, Clinical Trials Office Vice Chair, Department of Research Educational Goals Caveats: Cannot cover
Update on the Treatment of HCV
 Update on the Treatment of HCV K. Rajender Reddy, MD Professor of Medicine Director of Hepatology Director, Viral Hepatitis Center University of Pennsylvania Philadelphia, USA 1 K. Rajender Reddy, MD Disclosure
Update on the Treatment of HCV K. Rajender Reddy, MD Professor of Medicine Director of Hepatology Director, Viral Hepatitis Center University of Pennsylvania Philadelphia, USA 1 K. Rajender Reddy, MD Disclosure
Associate Professor of Medicine University of Chicago
 Nancy Reau, MD Associate Professor of Medicine University of Chicago Management of Hepatitis C: New Drugs and New Paradigms HCV is More Lethal than HIV Infection HCV superseded HIV as a cause of death
Nancy Reau, MD Associate Professor of Medicine University of Chicago Management of Hepatitis C: New Drugs and New Paradigms HCV is More Lethal than HIV Infection HCV superseded HIV as a cause of death
HCV In 2015: Maximizing SVR
 HCV In 2015: Maximizing SVR Alnoor Ramji Gastroenterology & Hepatology Clinical Associate Professor Division of Gastroenterology University Of British Columbia ramji_a@hotmail.com Disclosures (within Last
HCV In 2015: Maximizing SVR Alnoor Ramji Gastroenterology & Hepatology Clinical Associate Professor Division of Gastroenterology University Of British Columbia ramji_a@hotmail.com Disclosures (within Last
Learning Objective. After completing this educational activity, participants should be able to:
 Learning Objective After completing this educational activity, participants should be able to: Use patient characteristics and preferences to select HCV treatment strategies that maximize the potential
Learning Objective After completing this educational activity, participants should be able to: Use patient characteristics and preferences to select HCV treatment strategies that maximize the potential
Expert Perspectives: Best of HCV from EASL 2015
 Best of HCV from EASL 2015 Expert Perspectives: Best of HCV from EASL 2015 Saeed Hamid, MD Alex Thompson, MD, PhD This activity is supported by educational grants from AbbVie, Bristol-Myers Squibb, and
Best of HCV from EASL 2015 Expert Perspectives: Best of HCV from EASL 2015 Saeed Hamid, MD Alex Thompson, MD, PhD This activity is supported by educational grants from AbbVie, Bristol-Myers Squibb, and
VIRAL LIVER DISEASE. OAG Post DDW Course Westin Prince, Toronto, June 13-14, 2015
 VIRAL LIVER DISEASE OAG Post DDW Course Westin Prince, Toronto, June 13-14, 2015 Financial Interest Disclosure (over the past 24 months) Dr. Paul Marotta Relationships related to this presentation! Research
VIRAL LIVER DISEASE OAG Post DDW Course Westin Prince, Toronto, June 13-14, 2015 Financial Interest Disclosure (over the past 24 months) Dr. Paul Marotta Relationships related to this presentation! Research
The Dawn of a New Era: Hepatitis C
 The Dawn of a New Era: Hepatitis C Naudia L. Jonassaint Assistant Professor of Medicine and Surgery University Pittsburgh School of Medicine December 1, 2015 Objectives After presentation the learner should
The Dawn of a New Era: Hepatitis C Naudia L. Jonassaint Assistant Professor of Medicine and Surgery University Pittsburgh School of Medicine December 1, 2015 Objectives After presentation the learner should
6/2/2015. Interactive Case-Based Presentations and Audience Discussion
 6/2/215 Interactive Case-Based Presentations and Audience Discussion Andrew Aronsohn, MD Assistant Professor of Medicine University of Chicago Medical Center Chicago, Illinois Formatted:5-6-215 Washington,
6/2/215 Interactive Case-Based Presentations and Audience Discussion Andrew Aronsohn, MD Assistant Professor of Medicine University of Chicago Medical Center Chicago, Illinois Formatted:5-6-215 Washington,
Update in the Management of Hepatitis C: What Does the Future Hold
 Update in the Management of Hepatitis C: What Does the Future Hold Paul Y Kwo, MD, FACG Professor of Medicine Mdi Medical ldirector, Liver Transplantation tti Gastroenterology/Hepatology Division Indiana
Update in the Management of Hepatitis C: What Does the Future Hold Paul Y Kwo, MD, FACG Professor of Medicine Mdi Medical ldirector, Liver Transplantation tti Gastroenterology/Hepatology Division Indiana
HCV care after cure. This program is supported by educational grants from
 HCV care after cure This program is supported by educational grants from Raffaele Bruno,MD Department of Infectious Diseases, Hepatology Outpatients Unit University of Pavia Fondazione IRCCS Policlinico
HCV care after cure This program is supported by educational grants from Raffaele Bruno,MD Department of Infectious Diseases, Hepatology Outpatients Unit University of Pavia Fondazione IRCCS Policlinico
Ari Bunim, M.D. Director of Hepatology New York Hospital Queens Assistant Professor of Clinical Medicine Weill Cornell Medical College
 Ari Bunim, M.D. Director of Hepatology New York Hospital Queens Assistant Professor of Clinical Medicine Weill Cornell Medical College New York State Law Goes into Effect January 1, 2014 Hepatitis C Virus
Ari Bunim, M.D. Director of Hepatology New York Hospital Queens Assistant Professor of Clinical Medicine Weill Cornell Medical College New York State Law Goes into Effect January 1, 2014 Hepatitis C Virus
Outline. HCV Disease Outcomes in the US. Hepatitis C: The New Landscape 5/24/16. Advances in Internal Medicine May 24, I have no disclosures
 5/24/16 Hepatitis C: The New Landscape Advances in Internal Medicine May 24, 2016 I have no disclosures Rena K. Fo, MD Professor of Clinical Medicine, UCSF Outline I. Current HCV outcomes in the US II.
5/24/16 Hepatitis C: The New Landscape Advances in Internal Medicine May 24, 2016 I have no disclosures Rena K. Fo, MD Professor of Clinical Medicine, UCSF Outline I. Current HCV outcomes in the US II.
Current Treatment Options for HCV Patients. Michael Manns Dept. of Gastroenterology, Hepatology and Endocrinology Hannover Germany
 Current Treatment Options for HCV Patients Michael Manns Dept. of Gastroenterology, Hepatology and Endocrinology Hannover Germany 7th International Congress of Internal Medicine of Central Greece, Larissa,
Current Treatment Options for HCV Patients Michael Manns Dept. of Gastroenterology, Hepatology and Endocrinology Hannover Germany 7th International Congress of Internal Medicine of Central Greece, Larissa,
David L. Wyles, MD Chief, Division of Infectious Disease Denver Health Medical Center Denver, Colorado
 FORMATTED: 1/3/16 Drug Resistance-Associated Variants in Hepatitis C Virus Infection: Hype or Help? Atlanta, Georgia: October 2, 216 David L. Wyles, MD Chief, Division of Infectious Disease Denver Health
FORMATTED: 1/3/16 Drug Resistance-Associated Variants in Hepatitis C Virus Infection: Hype or Help? Atlanta, Georgia: October 2, 216 David L. Wyles, MD Chief, Division of Infectious Disease Denver Health
Rome, February nd Riunione Annuale AISF th AISF ANNUAL MEETING
 Rome, February 20-21 nd 2014 Riunione Annuale AISF 2014 14 th AISF ANNUAL MEETING Present and future treatment strategies for patients with HCV infection: chronic hepatitis and special populations IFN
Rome, February 20-21 nd 2014 Riunione Annuale AISF 2014 14 th AISF ANNUAL MEETING Present and future treatment strategies for patients with HCV infection: chronic hepatitis and special populations IFN
Disclosures. Advanced HCV management. Overview. Renal failure 1/10/2018. Research Grant support to UCSF from AbbVie Gilead Merck Proteus NIH
 Disclosures Advanced HCV management Annie Luetkemeyer, MD Division of HIV, ID and Global Medicine ZSFG, UCSF Research Grant support to UCSF from AbbVie Gilead Merck Proteus NIH Overview Renal failure Acute
Disclosures Advanced HCV management Annie Luetkemeyer, MD Division of HIV, ID and Global Medicine ZSFG, UCSF Research Grant support to UCSF from AbbVie Gilead Merck Proteus NIH Overview Renal failure Acute
HCV Management in Decompensated Cirrhosis: Current Therapies
 Treatment of Patients with Decompensated Cirrhosis and Liver Transplant Recipients Paul Y. Kwo, MD, FACG Professor of Medicine Gastroenterology/Hepatology Division Stanford University email pkwo@stanford.edu
Treatment of Patients with Decompensated Cirrhosis and Liver Transplant Recipients Paul Y. Kwo, MD, FACG Professor of Medicine Gastroenterology/Hepatology Division Stanford University email pkwo@stanford.edu
Antiviral treatment in HCV cirrhotic patients on waiting list
 Antiviral treatment in HCV cirrhotic patients on waiting list Krzysztof Tomasiewicz Department of Hepatology and Infectious Diseases Medical University of Lublin, Poland Disclosures Consultancy/Advisory
Antiviral treatment in HCV cirrhotic patients on waiting list Krzysztof Tomasiewicz Department of Hepatology and Infectious Diseases Medical University of Lublin, Poland Disclosures Consultancy/Advisory
Treatment of HCV in 2016
 5/1/16 Treatment of HCV in 16 Graham R Foster Professor of Hepatology QMUL Conflicts of Interest Speaker and consultancy fees received from AbbVie, BI, BMS, Gilead, Janssen, Roche, Merck, Novartis, Springbank,
5/1/16 Treatment of HCV in 16 Graham R Foster Professor of Hepatology QMUL Conflicts of Interest Speaker and consultancy fees received from AbbVie, BI, BMS, Gilead, Janssen, Roche, Merck, Novartis, Springbank,
IFN-free therapy in naïve HCV GT1 patients
 IFN-free therapy in naïve HCV GT1 patients Paris Hepatitis Conference Paris, 12th January, 2015 Pr Tarik Asselah MD, PhD; Service d Hépatologie & INSERM U773 University Paris Diderot, Hôpital Beaujon,
IFN-free therapy in naïve HCV GT1 patients Paris Hepatitis Conference Paris, 12th January, 2015 Pr Tarik Asselah MD, PhD; Service d Hépatologie & INSERM U773 University Paris Diderot, Hôpital Beaujon,
10/21/2016. David L. Wyles, MD Chief, Division of Infectious Disease Denver Health Medical Center Denver, Colorado
 Drug Resistance-Associated Variants in Hepatitis C Virus Infection: Hype or Help? David L. Wyles, MD Chief, Division of Infectious Disease Denver Health Medical Center Denver, Colorado FORMATTED: 1/3/16
Drug Resistance-Associated Variants in Hepatitis C Virus Infection: Hype or Help? David L. Wyles, MD Chief, Division of Infectious Disease Denver Health Medical Center Denver, Colorado FORMATTED: 1/3/16
CCO Official Conference Coverage: Clinical Impact of New Data From AASLD 2015
 CCO Official Conference Coverage: Clinical Impact of New Data From AASLD 2015 CCO Official Conference Coverage of the 2015 Annual Meeting of the American Association for the Study of Liver Diseases, November
CCO Official Conference Coverage: Clinical Impact of New Data From AASLD 2015 CCO Official Conference Coverage of the 2015 Annual Meeting of the American Association for the Study of Liver Diseases, November
Need to Assess HCV Resistance to DAAs: Is it Useful and When?
 Need to Assess HCV Resistance to DAAs: Is it Useful and When? Stéphane Chevaliez French National Reference Center for Viral Hepatitis B, C and delta Department of Virology & INSERM U955 Henri Mondor Hospital
Need to Assess HCV Resistance to DAAs: Is it Useful and When? Stéphane Chevaliez French National Reference Center for Viral Hepatitis B, C and delta Department of Virology & INSERM U955 Henri Mondor Hospital
Tough Cases in HIV/HCV Coinfection
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER Tough Cases in HIV/HCV Coinfection John Scott, MD, MSc Assistant Professor University of Washington Presentation prepared by: J Scott Last Updated: Jun 5, 2014
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Tough Cases in HIV/HCV Coinfection John Scott, MD, MSc Assistant Professor University of Washington Presentation prepared by: J Scott Last Updated: Jun 5, 2014
What Should We Do With Difficult to Treat HCV Populations?
 What Should We Do With Difficult to Treat HCV Populations? Norah Terrault, MD Professor of Medicine and Surgery Director, Viral Hepatitis Center University of California San Francisco Disclosures Norah
What Should We Do With Difficult to Treat HCV Populations? Norah Terrault, MD Professor of Medicine and Surgery Director, Viral Hepatitis Center University of California San Francisco Disclosures Norah
HEPATITIS C: UPDATE AND MANAGEMENT
 HEPATITIS C: UPDATE AND MANAGEMENT José Franco, MD Professor of Medicine Associate Dean for Educational Improvement Associate Director, Kern Institute STAR Center Director José Franco, MD Disclosures I
HEPATITIS C: UPDATE AND MANAGEMENT José Franco, MD Professor of Medicine Associate Dean for Educational Improvement Associate Director, Kern Institute STAR Center Director José Franco, MD Disclosures I
5/12/2016. Learning Objectives. Management of Hepatitis C Virus Genotype 2 or 3 Infected Treatment-Naive or Experienced Patients
 5/12/216 Management of Hepatitis C Virus Genotype 2 or 3 Infected Treatment-Naive or Experienced Patients Alexander Monto, MD Professor of Clinical Medicine University of California San Francisco San Francisco,
5/12/216 Management of Hepatitis C Virus Genotype 2 or 3 Infected Treatment-Naive or Experienced Patients Alexander Monto, MD Professor of Clinical Medicine University of California San Francisco San Francisco,
TREATING HEPATITIS C TODAY
 TREATING HEPATITIS C TODAY Nikolaos K. Gatselis Department of Medicine& Research Laboratory of Internal Medicine, Larissa Medical School, Thessaly University Disclosure Research Support: Gilead, Janssen,
TREATING HEPATITIS C TODAY Nikolaos K. Gatselis Department of Medicine& Research Laboratory of Internal Medicine, Larissa Medical School, Thessaly University Disclosure Research Support: Gilead, Janssen,
New Hepatitis C Antivirals
 New Hepatitis C Antivirals Kris Stewart, BSP, MD, FRCPC Drug Therapy Conference College of Medicine, University of Saskatchewan September 23, 2016 Disclosures I have received research and program support
New Hepatitis C Antivirals Kris Stewart, BSP, MD, FRCPC Drug Therapy Conference College of Medicine, University of Saskatchewan September 23, 2016 Disclosures I have received research and program support
HCV therapy : Clinical case
 HCV therapy : Clinical case PHC 2018 Paris January 14th, 2018 Tarik Asselah (MD, PhD) Professor of Medicine Hepatology, Chief INSERM UMR 1149, Hôpital Beaujon, Clichy, France. Disclosures Professor Asselah
HCV therapy : Clinical case PHC 2018 Paris January 14th, 2018 Tarik Asselah (MD, PhD) Professor of Medicine Hepatology, Chief INSERM UMR 1149, Hôpital Beaujon, Clichy, France. Disclosures Professor Asselah
Rapid Response from San Francisco: The Latest in the HCV Treatment Revolution
 Activity presentations are considered intellectual property. These slides may not be published or posted online without permission from Vindico Medical Education (cme@vindicocme.com). Please be respectful
Activity presentations are considered intellectual property. These slides may not be published or posted online without permission from Vindico Medical Education (cme@vindicocme.com). Please be respectful
Management of Chronic HCV 2017 and Beyond
 Management of Chronic HCV 2017 and Beyond Blaire E Burman, MD Virginia Mason Gastroenterology & Hepatology Relevant Disclosures No financial disclosures to report Leaning Objectives Burden of HCV Prevalence
Management of Chronic HCV 2017 and Beyond Blaire E Burman, MD Virginia Mason Gastroenterology & Hepatology Relevant Disclosures No financial disclosures to report Leaning Objectives Burden of HCV Prevalence
TREATMENT OF GENOTYPE 2
 Treatment of Genotype 2, 3,and 4 David E. Bernstein, MD, FACG Advisory Committee/Board Member: AbbVie Pharmaceuticals, Gilead, Merck, Janssen Consultant: AbbVie Pharmaceuticals, Bristol-Myers Squibb, Gilead,
Treatment of Genotype 2, 3,and 4 David E. Bernstein, MD, FACG Advisory Committee/Board Member: AbbVie Pharmaceuticals, Gilead, Merck, Janssen Consultant: AbbVie Pharmaceuticals, Bristol-Myers Squibb, Gilead,
Hepatitis C: Difficult-to-treat Patients 11th Paris Hepatology Conference 16th January 2018 Stefan Zeuzem, MD University Hospital, Frankfurt, Germany
 Hepatitis C: Difficult-to-treat Patients 11th Paris Hepatology Conference 16th January 2018 Stefan Zeuzem, MD University Hospital, Frankfurt, Germany PHC 2018 - www.aphc.info Disclosures Advisory boards:
Hepatitis C: Difficult-to-treat Patients 11th Paris Hepatology Conference 16th January 2018 Stefan Zeuzem, MD University Hospital, Frankfurt, Germany PHC 2018 - www.aphc.info Disclosures Advisory boards:
A treatment revolution: current management for chronic HCV
 A treatment revolution: current management for chronic HCV Ray Chung, M.D. Director of Hepatology and Liver Center Kevin and Polly Maroni Research Scholar Massachusetts General Hospital Disclosures Research
A treatment revolution: current management for chronic HCV Ray Chung, M.D. Director of Hepatology and Liver Center Kevin and Polly Maroni Research Scholar Massachusetts General Hospital Disclosures Research
Treatment of Unique Populations Raymond T. Chung, MD
 Treatment of Unique Populations Raymond T. Chung, MD Director of Hepatology and Liver Center Vice Chief, Gastroenterology Kevin and Polly Maroni Research Scholar Mass General Hospital Disclosures Research
Treatment of Unique Populations Raymond T. Chung, MD Director of Hepatology and Liver Center Vice Chief, Gastroenterology Kevin and Polly Maroni Research Scholar Mass General Hospital Disclosures Research
Hepatitis C Emerging Treatment Paradigms
 Hepatitis C Emerging Treatment Paradigms David R Nelson MD Assistant Vice President for Research Professor of Medicine Director, Clinical and Translational Science Institute University of Florida Gainesville,
Hepatitis C Emerging Treatment Paradigms David R Nelson MD Assistant Vice President for Research Professor of Medicine Director, Clinical and Translational Science Institute University of Florida Gainesville,
What is the Optimized Treatment Duration? To Overtreat versus Undertreat. Nancy Reau, MD Associate Professor of Medicine University of Chicago
 What is the Optimized Treatment Duration? To Overtreat versus Undertreat Nancy Reau, MD Associate Professor of Medicine University of Chicago Learning Objectives: 1. Discuss patient populations appropriate
What is the Optimized Treatment Duration? To Overtreat versus Undertreat Nancy Reau, MD Associate Professor of Medicine University of Chicago Learning Objectives: 1. Discuss patient populations appropriate
Evolution of Therapy in HCV
 Hepatitis C: Update on New Therapies and AASLD 13 David Bernstein, MD, FACP, AGAF, FACP Professor of Medicine Hofstra North Shore-LIJ School of Medicine Evolution of Therapy in HCV 199 1999 1 13 (%) SVR
Hepatitis C: Update on New Therapies and AASLD 13 David Bernstein, MD, FACP, AGAF, FACP Professor of Medicine Hofstra North Shore-LIJ School of Medicine Evolution of Therapy in HCV 199 1999 1 13 (%) SVR
Treating HCV After Liver Transplantation: What are the Treatment Options?
 4 th OPTIMIZE WORKSHOP USING DAAs IN PATIENTS WITH CIRRHOSIS AND LIVER RECIPIENTS Treating HCV After Liver Transplantation: What are the Treatment Options? Maria Carlota Londoño, MD Liver Unit, Hospital
4 th OPTIMIZE WORKSHOP USING DAAs IN PATIENTS WITH CIRRHOSIS AND LIVER RECIPIENTS Treating HCV After Liver Transplantation: What are the Treatment Options? Maria Carlota Londoño, MD Liver Unit, Hospital
EASL 2013 Interferon Free, All Oral Regimens for Hepatitis C. Maria Buti Hospital Universitario Valle Hebron Barcelona Spain
 EASL 2013 Interferon Free, All Oral Regimens for Hepatitis C Maria Buti Hospital Universitario Valle Hebron Barcelona Spain The first Results with Oral therapy: a Protease Inhibitor and NS5A inhibitor
EASL 2013 Interferon Free, All Oral Regimens for Hepatitis C Maria Buti Hospital Universitario Valle Hebron Barcelona Spain The first Results with Oral therapy: a Protease Inhibitor and NS5A inhibitor
Future strategies with new DAAs
 Future strategies with new DAAs Ola Weiland professor New direct antiviral drugs Case no 1 male with genotype 2b Male with gt 2b chronic HCV Male with gt 2b relapse afer peg-ifn + RBV during 24 weeks
Future strategies with new DAAs Ola Weiland professor New direct antiviral drugs Case no 1 male with genotype 2b Male with gt 2b chronic HCV Male with gt 2b relapse afer peg-ifn + RBV during 24 weeks
Hepatitis C Elimination: Screening, Linkage and Treatment. Eric Lawitz, MD The Texas Liver Institute San Antonio, Texas
 Hepatitis C Elimination: Screening, Linkage and Treatment Eric Lawitz, MD The Texas Liver Institute San Antonio, Texas Hepatitis C: Worldwide Presence Worldwide prevalence: 130-150 million Viral hepatitis
Hepatitis C Elimination: Screening, Linkage and Treatment Eric Lawitz, MD The Texas Liver Institute San Antonio, Texas Hepatitis C: Worldwide Presence Worldwide prevalence: 130-150 million Viral hepatitis
Meet the Professor: HIV/HCV Coinfection
 Meet the Professor: HIV/HCV Coinfection Vincent Lo Re, MD, MSCE Assistant Professor of Medicine and Epidemiology Division of Infectious Diseases Center for Clinical Epidemiology and Biostatistics University
Meet the Professor: HIV/HCV Coinfection Vincent Lo Re, MD, MSCE Assistant Professor of Medicine and Epidemiology Division of Infectious Diseases Center for Clinical Epidemiology and Biostatistics University
Hepatitis C in Correctional Facilities: Big Problem, Bigger Opportunity. Cody A. Chastain, MD
 Hepatitis C in Correctional Facilities: Big Problem, Bigger Opportunity Cody A. Chastain, MD Disclosures Research supported by Gilead Sciences Inc.: Site investigator for HIV/HCV SWITCH Registry Study
Hepatitis C in Correctional Facilities: Big Problem, Bigger Opportunity Cody A. Chastain, MD Disclosures Research supported by Gilead Sciences Inc.: Site investigator for HIV/HCV SWITCH Registry Study
The HCV Pipeline Ira M. Jacobson, MD, FACP, FACG, AGAF. Slide Presentation. IFN-free DAA combinations (G1)
") Slide Presentation The HCV Pipeline Vincent Astor Distinguished Professor of Medicine Chief, Division of Gastroenterology and Hepatology Medical Director, Center for the Study of Hepatitis C Weill Cornell
Slide Presentation The HCV Pipeline Vincent Astor Distinguished Professor of Medicine Chief, Division of Gastroenterology and Hepatology Medical Director, Center for the Study of Hepatitis C Weill Cornell
SURVEYOR-II Part 2 Study Design
 HIGH SVR RATES WITH + CO-ADMINISTERED FOR 8 WEEKS IN NON-CIRRHOTIC PATIENTS WITH HCV GENOTYPE 3 INFECTION A.J. Muir, S. Strasser, S. Wang, S. Shafran, M. Bonacini, P. Kwo, D. Wyles, E. Gane, S.S. Lovell,
HIGH SVR RATES WITH + CO-ADMINISTERED FOR 8 WEEKS IN NON-CIRRHOTIC PATIENTS WITH HCV GENOTYPE 3 INFECTION A.J. Muir, S. Strasser, S. Wang, S. Shafran, M. Bonacini, P. Kwo, D. Wyles, E. Gane, S.S. Lovell,
Hepatitis C Treatment 2014
 Hepatitis C Treatment 214 Brendan M. McGuire, MD UAB Liver Center Outline Epidemiology/National History Terminology for Treatment Treatment Considerations Current Treatment Options Genotype 1 (GT 1) Genotype
Hepatitis C Treatment 214 Brendan M. McGuire, MD UAB Liver Center Outline Epidemiology/National History Terminology for Treatment Treatment Considerations Current Treatment Options Genotype 1 (GT 1) Genotype
Failure after treatment with DAAs: What to do? Marseille France 2-3 th June 2016
 Failure after treatment with DAAs: What to do? Marc Bourliere, MD White Nights of Hepatology Hôpital Saint Joseph Saint Petersburg Marseille France 2-3 th June 16 Disclosures Board member for : Schering-Plough,
Failure after treatment with DAAs: What to do? Marc Bourliere, MD White Nights of Hepatology Hôpital Saint Joseph Saint Petersburg Marseille France 2-3 th June 16 Disclosures Board member for : Schering-Plough,
10/21/2016. Susanna Naggie, MD, MHS Associate Professor of Medicine Duke University Durham, North Carolina. Learning Objectives
 A Crash Course on the AASLD/IDSA Hepatitis C Virus Infection Treatment Guidelines: What s New Susanna Naggie, MD, MHS Associate Professor of Medicine Duke University Durham, North Carolina FORMATTED: 1/3/16
A Crash Course on the AASLD/IDSA Hepatitis C Virus Infection Treatment Guidelines: What s New Susanna Naggie, MD, MHS Associate Professor of Medicine Duke University Durham, North Carolina FORMATTED: 1/3/16
DAAs in the era of decompensated liver disease. Piero L. Almasio University of Palermo
 DAAs in the era of decompensated liver disease Piero L. Almasio University of Palermo piero.almasio@unipa.it HCV therapy in the era of interferon based therapy Priority Compensated cirrhosis Decompensated
DAAs in the era of decompensated liver disease Piero L. Almasio University of Palermo piero.almasio@unipa.it HCV therapy in the era of interferon based therapy Priority Compensated cirrhosis Decompensated
HCV-G3: Sofosbuvir with ledipasvir or daclatasvir?
 HCV-G3: Sofosbuvir with ledipasvir or daclatasvir? Ioannis Goulis, MD Aristotelian University of Thessaloniki XXIII International Hepatitis B & C Meeting of Athens Hadziyannis HCV genotype 3 therapy Chronic
HCV-G3: Sofosbuvir with ledipasvir or daclatasvir? Ioannis Goulis, MD Aristotelian University of Thessaloniki XXIII International Hepatitis B & C Meeting of Athens Hadziyannis HCV genotype 3 therapy Chronic
Patients with compensated cirrhosis: how to treat and follow-up
 Patients with compensated cirrhosis: how to treat and follow-up Thomas Berg Sektion Hepatologie Klinik und Poliklinik für Gastroenterologie und Rheumatologie Universitätsklinikum Leipzig Leber- und Studienzentrum
Patients with compensated cirrhosis: how to treat and follow-up Thomas Berg Sektion Hepatologie Klinik und Poliklinik für Gastroenterologie und Rheumatologie Universitätsklinikum Leipzig Leber- und Studienzentrum
Case 1: Chronic Hepatitis C
 Case 1: Chronic Hepatitis C Moderator Dawn Pease, MSN, RN, ANP-BC Seton Healthcare Family University Medical Center Brackenridge Brackenridge Specialty Clinics - Gastroenterology and Endocrinology Austin,
Case 1: Chronic Hepatitis C Moderator Dawn Pease, MSN, RN, ANP-BC Seton Healthcare Family University Medical Center Brackenridge Brackenridge Specialty Clinics - Gastroenterology and Endocrinology Austin,
Current HCV Treatment by Genotype
 Current HCV Treatment by Genotype Ari Bunim, MD Assistant Professor Clinical Medicine Weill Cornell Medical College Clinical Director of Hepatology New York-Presbyterian/Queens Objectives To understand
Current HCV Treatment by Genotype Ari Bunim, MD Assistant Professor Clinical Medicine Weill Cornell Medical College Clinical Director of Hepatology New York-Presbyterian/Queens Objectives To understand
Program Disclosure. A maximum of 1.5 contact hours may be earned for successful completion of this activity.
 Program Disclosure This activity has been planned and implemented in accordance with the accreditation requirements and policies of the Accreditation Council for Continuing Medical Education (ACCME) through
Program Disclosure This activity has been planned and implemented in accordance with the accreditation requirements and policies of the Accreditation Council for Continuing Medical Education (ACCME) through
Management of HCV in Prior Treatment Failure
 Management of HCV in Prior Treatment Failure Arthur Y. Kim, MD Associate Professor of Medicine Harvard Medical School Boston, Massachusetts Learning Objectives After attending this presentation, learners
Management of HCV in Prior Treatment Failure Arthur Y. Kim, MD Associate Professor of Medicine Harvard Medical School Boston, Massachusetts Learning Objectives After attending this presentation, learners
Phase 3. Treatment Experienced. Ledipasvir-Sofosbuvir +/- Ribavirin in HCV Genotype 1 ION-2. Afdhal N, et al. N Engl J Med. 2014;370:
 Phase 3 Treatment Experienced Ledipasvir-Sofosbuvir +/- Ribavirin in HCV Genotype 1 ION-2 Afdhal N, et al. N Engl J Med. 2014;370:1483-93. Ledipasvir-Sofosbuvir +/- Ribavirin in Treatment-Experienced HCV
Phase 3 Treatment Experienced Ledipasvir-Sofosbuvir +/- Ribavirin in HCV Genotype 1 ION-2 Afdhal N, et al. N Engl J Med. 2014;370:1483-93. Ledipasvir-Sofosbuvir +/- Ribavirin in Treatment-Experienced HCV
THE CHANGING LANDSCAPE OF HEPATITIS INFECTION. Michael E. Herman D.O.
 THE CHANGING LANDSCAPE OF HEPATITIS INFECTION Michael E. Herman D.O. What s New? For Primary Care Providers Importance of diagnosing HCV For HCV Treaters How can we improve current therapies? For everyone
THE CHANGING LANDSCAPE OF HEPATITIS INFECTION Michael E. Herman D.O. What s New? For Primary Care Providers Importance of diagnosing HCV For HCV Treaters How can we improve current therapies? For everyone
Hepatitis C: New Therapies in
 Hepatitis C: New Therapies in 216-217 Mark Sulkowski, MD Professor of Medicine Johns Hopkins University School of Medicine Medical Director, Viral Hepatitis Center Divisions of Infectious Diseases and
Hepatitis C: New Therapies in 216-217 Mark Sulkowski, MD Professor of Medicine Johns Hopkins University School of Medicine Medical Director, Viral Hepatitis Center Divisions of Infectious Diseases and
Hepatitis C Update: A Growing Challenge With Evolving Management Solutions
 Pts (%) Hepatitis C Update: A Growing Challenge With Evolving Management Solutions A Growing Challenge With Evolving Management Solutions Introduction Magda Houlberg, MD Chief Clinical Officer Howard Brown
Pts (%) Hepatitis C Update: A Growing Challenge With Evolving Management Solutions A Growing Challenge With Evolving Management Solutions Introduction Magda Houlberg, MD Chief Clinical Officer Howard Brown
Eliminating Hepatitis C from New Zealand
 Eliminating Hepatitis C from New Zealand Catherine Stedman Associate Professor of Medicine, University of Otago, Christchurch Gastroenterology Department, Christchurch Hospital Disclosures I have the following
Eliminating Hepatitis C from New Zealand Catherine Stedman Associate Professor of Medicine, University of Otago, Christchurch Gastroenterology Department, Christchurch Hospital Disclosures I have the following
Treating HCV Prior to Liver Transplantation. What Are the Treatment Options? Xavier Forns Liver Unit Hospital Clinic, CIBEREHD, IDIBAPS Barcelona
 Treating HCV Prior to Liver Transplantation What Are the Treatment Options? Xavier Forns Liver Unit Hospital Clinic, CIBEREHD, IDIBAPS Barcelona Disclosures Unrestricted Grant Support: Janssen and Abbvie
Treating HCV Prior to Liver Transplantation What Are the Treatment Options? Xavier Forns Liver Unit Hospital Clinic, CIBEREHD, IDIBAPS Barcelona Disclosures Unrestricted Grant Support: Janssen and Abbvie
Hepatitis C: the 2015 Perspective for the Family Medicine Practitioner
 Hepatitis C: the 2015 Perspective for the Family Medicine Practitioner Annie Luetkemeyer, MD Division of HIV,ID & Global Medicine San Francisco General Hospital Disclosures I have received research grant
Hepatitis C: the 2015 Perspective for the Family Medicine Practitioner Annie Luetkemeyer, MD Division of HIV,ID & Global Medicine San Francisco General Hospital Disclosures I have received research grant
HIV-HCV Co-Infection in Shobha Swaminathan, MD Associate Professor of Medicine Rutgers New Jersey Medical School
 HIV-HCV Co-Infection in 2018 Shobha Swaminathan, MD Associate Professor of Medicine Rutgers New Jersey Medical School AASLD/IDSA and DHHS Guidance: HIV/HCV Coinfection All pts with HIV should be screened
HIV-HCV Co-Infection in 2018 Shobha Swaminathan, MD Associate Professor of Medicine Rutgers New Jersey Medical School AASLD/IDSA and DHHS Guidance: HIV/HCV Coinfection All pts with HIV should be screened
Approved regimens for cirrhotic patients
 5th Workshop on HCV THERAPY ADVANCES New antivirals in clinical practice Approved regimens for cirrhotic patients Amsterdam, 4-5 december 2015 Disease burden in Spain 400000 350000 300000 F0 Peak cirrhosis
5th Workshop on HCV THERAPY ADVANCES New antivirals in clinical practice Approved regimens for cirrhotic patients Amsterdam, 4-5 december 2015 Disease burden in Spain 400000 350000 300000 F0 Peak cirrhosis
THE THERAPEUTIC REVOLUTION THAT TRANSFORMED CHRONIC HEPATITIS C TO A CURABLE DISEASE
 THE THERAPEUTIC REVOLUTION THAT TRANSFORMED CHRONIC HEPATITIS C TO A CURABLE DISEASE MARIA SCHINA CONSULTANT PHYSICIAN INTERNAL MEDICINE AND HEPATOLOGY ATHENS EUROCLINIC 10 th INTERNATIONAL CONGRESS OF
THE THERAPEUTIC REVOLUTION THAT TRANSFORMED CHRONIC HEPATITIS C TO A CURABLE DISEASE MARIA SCHINA CONSULTANT PHYSICIAN INTERNAL MEDICINE AND HEPATOLOGY ATHENS EUROCLINIC 10 th INTERNATIONAL CONGRESS OF
47 th Annual Meeting AISF
 47 th Annual Meeting AISF Rome, 21 February 2014 Present and future treatment strategies for patients with HCV infection: chronic hepatitis and special populations (HCV/HIV coinfection, advanced cirrhosis,
47 th Annual Meeting AISF Rome, 21 February 2014 Present and future treatment strategies for patients with HCV infection: chronic hepatitis and special populations (HCV/HIV coinfection, advanced cirrhosis,
HCV TREATMENT PRE- AND POST TRANSPLANTATION
 HCV TREATMENT PRE- AND POST TRANSPLANTATION Mitchell L. Shiffman, MD, FACG Medical Director Liver Institute of Virginia Bon Secours Health System Richmond and Newport News, VA, USA IVer Liver Institute
HCV TREATMENT PRE- AND POST TRANSPLANTATION Mitchell L. Shiffman, MD, FACG Medical Director Liver Institute of Virginia Bon Secours Health System Richmond and Newport News, VA, USA IVer Liver Institute
Hepatitis C Update: Screening, Diagnosis, and Treatment
 Mountain West AIDS Education and Training Center Hepatitis C Update: Screening, Diagnosis, and Treatment Brian R. Wood, MD (bwood2@uw.edu) Assistant Professor of Medicine, University of Washington Medical
Mountain West AIDS Education and Training Center Hepatitis C Update: Screening, Diagnosis, and Treatment Brian R. Wood, MD (bwood2@uw.edu) Assistant Professor of Medicine, University of Washington Medical
HIV and Hepatitis C Have we finally slayed the beast?
 HIV and Hepatitis C Have we finally slayed the beast? Mark W. Sonderup Division of Hepatology Department of Medicine University of Cape Town & Groote Schuur Hospital Accelerated Fibrosis in HIV-HCV co-infected
HIV and Hepatitis C Have we finally slayed the beast? Mark W. Sonderup Division of Hepatology Department of Medicine University of Cape Town & Groote Schuur Hospital Accelerated Fibrosis in HIV-HCV co-infected
Special developments in the management of Hepatitis C. Disclosures
 Special developments in the management of Hepatitis C Sandeep Mukherjee,MD Division of Gastroenterology CHI Health and Creighton University Medical Center Omaha, NE 68154 Sandeep.Mukherjee@alegent.org
Special developments in the management of Hepatitis C Sandeep Mukherjee,MD Division of Gastroenterology CHI Health and Creighton University Medical Center Omaha, NE 68154 Sandeep.Mukherjee@alegent.org
Hepatitis C ew Medications, New Hope and New. V. Opportunities for Primary Care. Outline. HCV Disease Outcomes in the US 9/21/2016
 Hepatitis C ew Medications, New Hope and New Opportunities for Primary Care Primary Care Principles and Practice October 14, 2016 Disclosures: Grant support Gilead Sciences, Inc Quality improvement Systematized
Hepatitis C ew Medications, New Hope and New Opportunities for Primary Care Primary Care Principles and Practice October 14, 2016 Disclosures: Grant support Gilead Sciences, Inc Quality improvement Systematized
STATE OF THE ART Update: Treatment Options 2016 Mark Sulkowski, MD
 Housekeeping Please turn off or silence cell phones. Restrooms are located on this floor. Make a left out of the ballroom foyer and the men s room is on your left. The ladies room is across from the elevators
Housekeeping Please turn off or silence cell phones. Restrooms are located on this floor. Make a left out of the ballroom foyer and the men s room is on your left. The ladies room is across from the elevators
HIV/HCV Coinfection: Why It Matters and What To Do About It. Cody A. Chastain, MD 10/26/16
 HIV/HCV Coinfection: Why It Matters and What To Do About It Cody A. Chastain, MD 10/26/16 Disclosures I have no relevant financial disclosures. Objectives At the end of this lecture, the learner will be
HIV/HCV Coinfection: Why It Matters and What To Do About It Cody A. Chastain, MD 10/26/16 Disclosures I have no relevant financial disclosures. Objectives At the end of this lecture, the learner will be
What do we need to know about RAVs clinically?
 14 th European HIV & Hepatitis Workshop Rome, 25-27 May, 2016 What do we need to know about RAVs clinically? Stefan Zeuzem, MD University of Frankfurt Germany Background Resistance associated variants
14 th European HIV & Hepatitis Workshop Rome, 25-27 May, 2016 What do we need to know about RAVs clinically? Stefan Zeuzem, MD University of Frankfurt Germany Background Resistance associated variants
Cases: Management of Hepatitis C in Prior Treatment Failure
 Cases: Management of Hepatitis C in Prior Treatment Failure David L. Wyles, MD Professor of Medicine University of Colorado Chief, Division of Infectious Disease Denver Health Learning Objectives After
Cases: Management of Hepatitis C in Prior Treatment Failure David L. Wyles, MD Professor of Medicine University of Colorado Chief, Division of Infectious Disease Denver Health Learning Objectives After
Terapie attuali. Eradicazione di HCV e nuove prospettive:
 Eradicazione di HCV e nuove prospettive: Terapie attuali Luisa Pasulo U.S.C. Gastroenterologia Epatologia e Trapiantologia Ospedale Papa Giovanni XXIII - Bergamo From Infection to liver disease Infezione
Eradicazione di HCV e nuove prospettive: Terapie attuali Luisa Pasulo U.S.C. Gastroenterologia Epatologia e Trapiantologia Ospedale Papa Giovanni XXIII - Bergamo From Infection to liver disease Infezione