HCV Infection: EASL Clinical Practice Guidelines Francesco Negro University Hospital Geneva Switzerland
|
|
|
- Lora Curtis
- 6 years ago
- Views:
Transcription
1 HCV Infection: EASL Clinical Practice Guidelines 2016 Francesco Negro University Hospital Geneva Switzerland
2 Panel Codinat: Jean-Michel Pawlotsky Panel: Alessio Aghemo David Back Geoffrey Dusheiko Xavier Fns Francesco Negro (EASL GB) Massimo Puoti Christoph Sarrazin
3 Goal of Therapy The goal of therapy is to cure HCV infection to prevent hepatic cirrhosis, decompensation of cirrhosis, HCC, severe extra-hepatic manifestations and death The endpoint of therapy is undetectable in a sensitive assay (LOD <15 IU/mL) 12 weeks (SVR12) and/ 24 weeks (SVR24) after the end of treatment Undetectable HCV ce antigen 12 weeks (SVR12) and/ 24 weeks (SVR24) after the end of treatment is an alternative endpoint of therapy in patients with detectable HCV ce antigen pri to therapy if assays are not available not affdable
4 Relationship Between HCV Ce Ag and Levels Analytical sensitivity equivalent to IU/mL Rare false-negatives (ce Ag-negative, -positive) (Chevaliez et al., J Clin Virol 2014;61:145-8)
5 Treatment Indications
6 Treatment Indications All treatment-naïve and treatment-experienced patients with compensated decompensated chronic liver disease due to HCV must be considered f therapy => UNIVERSAL ACCESS TO THERAPY
7 Patients Who Should be Treated Without Delay Significant fibrosis cirrhosis (METAVIR sce F2, F3, F4), including decompensated cirrhosis Clinically significant extra-hepatic manifestations HCV recurrence after liver transplantation Individuals at risk of transmitting HCV Active injection drug users MSM with high-risk sexual practices Women of child-bearing age who wish to get pregnant Hemodialysis patients Prison inmates
8 Available therapies
9 DAAs Approved in 2014 Sofosbuvir All genotypes Simeprevir Gen 1, 4 Daclatasvir All genotypes
10 DAAs Approved in 2015 Sofosbuvir/ Ledipasvir Gen 1, 4, 5, 6 Ombitasvir/ Paritaprevir/ Ritonavir Gen 1, 4 Dasabuvir Gen 1
11 DAAs Approved in 2016 Sofosbuvir/ Velpatasvir All genotypes Grazoprevir/ Elbasvir Gen 1, 4

12 General Considerations IFN-free regimens are the best options in HCVmonoinfected and in HIV-coinfected patients without cirrhosis with compensated (Child-Pugh A) cirrhosis, because of their virological efficacy, ease of use and tolerability The same IFN-free treatment regimens can be used in HIV-coinfected patients as in patients without HIV infection, as the virological results of therapy are identical



13 Drug-Drug Interactions
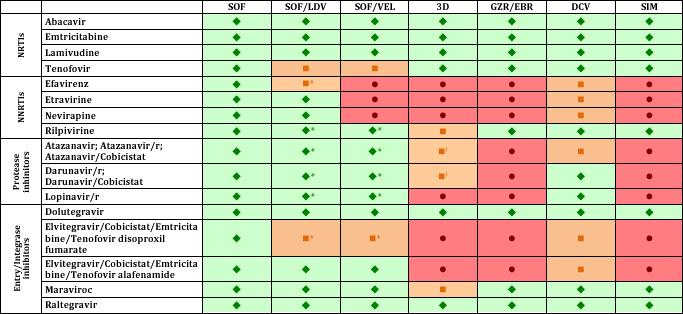
14 DDIs: HIV Antiretrovirals
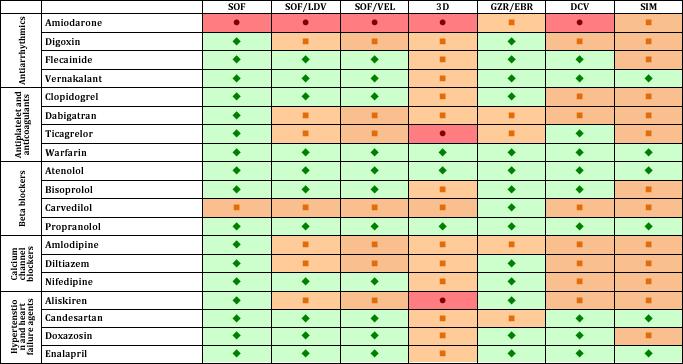
15 DDIs: Cardiovascular Drugs
16 IFN-Free Treatment Options Combination regimen GT1 GT2 GT3 GT4 GT5-6 SOF + RBV No Suboptimal Suboptimal No No SOF/LDV ± RBV Yes No No Yes Yes SOF/VEL ± RBV Yes Yes Yes Yes Yes OBV/PTV/r + DSV (3D) ± RBV Yes No No No No OBV/PTV/r (2D) ± RBV No No No Yes No GZR/EBR ± RBV Yes No No Yes No SOF + DCV ± RBV Yes Yes Yes Yes Yes SOF + SIM ± RBV Suboptimal No No Yes No
17 IFN-Free Treatment Options These options are considered equivalent f a given genotype, and their der of presentation does not indicate any superiity of preference, unless specified so By convention, the combination regimens listed start with fixed-dose, single-pill combinations (sofosbuvir-based followed by sofosbuvir-free), followed by combinations of sofosbuvir with another drug in a different pill
18 Characteristics that Infm Treatment Option Selection Pri treatment experience Drug-drug interactions HCV genotype/s ubtype Treatment selection PK profile of treatment Severity of liver disease Patient combidities
19 Genotype 1
20 Genotype 1a Options Combination regimen No cirrhosis Compensated cirrhosis Rx-naïve Rx-exp d Rx-naïve Rx-exp d SOF/LDV ± RBV 8-12 wk 12 wk + RBV* 12 wk 12 wk + RBV* SOF/VEL ± RBV 12 wk 12 wk 12 wk 12 wk OBV/PTV/r + DSV (3D) ± RBV 12 wk + RBV 12 wk + RBV 24 wk + RBV 24 wk + RBV GZR/EBR ± RBV >800,000 >800,000 >800,000 >800,000 SOF + DCV ± RBV 12 wk 12 wk + RBV* 12 wk 12 wk + RBV* *24 wk without RBV if RBV contraindicated poly tolerated Only if presence of NS5A RASs at baseline, if resistance testing available
21 Genotype 1a Options Combination regimen No cirrhosis Compensated cirrhosis Rx-naïve Rx-exp d Rx-naïve Rx-exp d SOF/LDV ± RBV 8-12 wk 12 wk + RBV* 12 wk 12 wk + RBV* SOF/VEL ± RBV 12 wk 12 wk 12 wk 12 wk OBV/PTV/r + DSV (3D) ± RBV 12 wk + RBV 12 wk + RBV 24 wk + RBV 24 wk + RBV GZR/EBR ± RBV >800,000 >800,000 >800,000 >800,000 SOF + DCV ± RBV 12 wk 12 wk + RBV* 12 wk 12 wk + RBV* *24 wk without RBV if RBV contraindicated poly tolerated Only if presence of NS5A RASs at baseline, if resistance testing available
22 Genotype 1a Options Combination regimen No cirrhosis Compensated cirrhosis Rx-naïve Rx-exp d Rx-naïve Rx-exp d SOF/LDV ± RBV 8-12 wk 12 wk + RBV* 12 wk 12 wk + RBV* SOF/VEL ± RBV 12 wk 12 wk 12 wk 12 wk OBV/PTV/r + DSV (3D) ± RBV 12 wk + RBV 12 wk + RBV 24 wk + RBV 24 wk + RBV GZR/EBR ± RBV >800,000 >800,000 >800,000 >800,000 SOF + DCV ± RBV 12 wk 12 wk + RBV* 12 wk 12 wk + RBV* *24 wk without RBV if RBV contraindicated poly tolerated Only if presence of NS5A RASs at baseline, if resistance testing available
23 Genotype 1a Options Combination regimen No cirrhosis Compensated cirrhosis Rx-naïve Rx-exp d Rx-naïve Rx-exp d SOF/LDV ± RBV 8-12 wk 12 wk + RBV* 12 wk 12 wk + RBV* SOF/VEL ± RBV 12 wk 12 wk 12 wk 12 wk OBV/PTV/r + DSV (3D) ± RBV 12 wk + RBV 12 wk + RBV 24 wk + RBV 24 wk + RBV GZR/EBR ± RBV >800,000 >800,000 >800,000 >800,000 SOF + DCV ± RBV 12 wk 12 wk + RBV* 12 wk 12 wk + RBV* *24 wk without RBV if RBV contraindicated poly tolerated Only if presence of NS5A RASs at baseline, if resistance testing available
24 Genotype 1a Options Combination regimen No cirrhosis Compensated cirrhosis Rx-naïve Rx-exp d Rx-naïve Rx-exp d SOF/LDV ± RBV 8-12 wk 12 wk + RBV* 12 wk 12 wk + RBV* SOF/VEL ± RBV 12 wk 12 wk 12 wk 12 wk OBV/PTV/r + DSV (3D) ± RBV 12 wk + RBV 12 wk + RBV 24 wk + RBV 24 wk + RBV GZR/EBR ± RBV >800,000 >800,000 >800,000 >800,000 SOF + DCV ± RBV 12 wk 12 wk + RBV* 12 wk 12 wk + RBV* *24 wk without RBV if RBV contraindicated poly tolerated Only if presence of NS5A RASs at baseline, if resistance testing available

25 SOF/LDV Trials vs Real-Wld ION-3 vs Real-wld, Rx-naive, No cirrhosis, VL <6 M IU/mL (Curry et al., EASL 2016)
26 SVR12 rate (%) Sofosbuvir + Velpatasvir ASTRAL-1 Phase III, TN and TE (32%), Gt 1,2,4,5,6, 19% cirrhosis, 12 wks 99% 99% 99% 99% % N=624 N=501 N=121 N=423 N=201 0 Overall No Yes Naïve Experienced Cirrhosis Treatment histy (Feld et al., N Engl J Med 2015;373: )
27 Genotype 1b Options Combination regimen No cirrhosis Compensated cirrhosis Rx-naïve Rx-exp d Rx-naïve Rx-exp d SOF/LDV ± RBV 8-12 wk 12 wk 12 wk 12 wk SOF/VEL ± RBV 12 wk 12 wk 12 wk 12 wk OBV/PTV/r + DSV (3D) ± RBV 8-12 wk 12 wk 12 wk 12 wk GZR/EBR ± RBV 12 wk 12 wk 12 wk 12 wk SOF + DCV ± RBV 12 wk 12 wk 12 wk 12 wk
28 Genotype 1b Options Combination regimen No cirrhosis Compensated cirrhosis Rx-naïve Rx-exp d Rx-naïve Rx-exp d SOF/LDV ± RBV 8-12 wk 12 wk 12 wk 12 wk SOF/VEL ± RBV 12 wk 12 wk 12 wk 12 wk OBV/PTV/r + DSV (3D) ± RBV 8-12 wk 12 wk 12 wk 12 wk GZR/EBR ± RBV 12 wk 12 wk 12 wk 12 wk SOF + DCV ± RBV 12 wk 12 wk 12 wk 12 wk
29 SVR12 rate (%) 8 weeks of OBV/PTV/r + DSV in Genotype 1b Treatment-Naïves % GARNET study Genotype 1b Treatment-naïve No cirrhosis (F0-F3) SVR: 13/15 F3 patients 10 0 N=166 (Abbvie, presented at the EASL/AASLD Special Conference on Hepatitis C)
30 Genotype 2 Options Combination regimen No cirrhosis Compensated cirrhosis Rx-naïve Rx-exp d Rx-naïve Rx-exp d SOF/VEL ± RBV 12 wk 12 wk 12 wk 12 wk SOF + DCV ± RBV 12 wk 12 wk 12 wk 12 wk
31 SVR12 rate (%) Sofosbuvir + Velpatasvir ASTRAL-2 Phase III, TN and TE (14%), Gt 2, 14% cirrhosis, 12 weeks SOF/VEL SOF/RBV % 96% 100% 93% 100% 81% 100% 100% N=100 N=96 N=15 N=15 N=15 N=16 N=4 N=4 0 No cirrhosis Cirrhosis No cirrhosis Cirrhosis Treatment-naïve Treatment-experienced (Foster et al., N Engl J Med 2015;373: )
32 Genotype 3 Options Combination regimen No cirrhosis Compensated cirrhosis Rx-naïve Rx-exp d Rx-naïve Rx-exp d SOF/VEL ± RBV 12 wk 12 wk + RBV* 12 wk + RBV* 12 wk + RBV* SOF + DCV ± RBV 12 wk 12 wk + RBV* 24 wk + RBV 24 wk + RBV *24 wk without RBV if RBV contraindicated poly tolerated Only if presence of NS5A RAS Y93H at baseline, if resistance testing available
33 Genotype 3 Options Combination regimen No cirrhosis Compensated cirrhosis Rx-naïve Rx-exp d Rx-naïve Rx-exp d SOF/VEL ± RBV 12 wk 12 wk + RBV* 12 wk + RBV* 12 wk + RBV* SOF + DCV ± RBV 12 wk 12 wk + RBV* 24 wk + RBV 24 wk + RBV *24 wk without RBV if RBV contraindicated poly tolerated Only if presence of NS5A RAS Y93H at baseline, if resistance testing available
34 SVR12 rate (%) Sofosbuvir + Velpatasvir ASTRAL-3 Phase III, TN and TE (26%), Gt 3, 30% cirrhosis, 12 weeks % 90% SOF/VEL 12 wk 93% SOF/RBV 24 wk 91% 89% 80 73% 71% % N=163 N=156 N=43 N=45 N=34 N=31 N=37 N=38 0 No cirrhosis Treatment-naïve Cirrhosis No cirrhosis Cirrhosis Treatment-experienced (Foster et al., N Engl J Med 2015;373: )
35 Sofosbuvir + Velpatasvir ASTRAL-3 Phase III, TN and TE (26%), Gt 3, 30% cirrhosis, 12 weeks Resistance analysis (1% cutoff, deep sequencing) Total, n=274 Total, n=274 97% SVR12 84% No BL NS5A RASs n=231 16% BL NS5A RASs n=43 88% SVR12 225/231 38/43 SVR12 was 84% (21/25) in patients with Y93H (Foster et al., N Engl J Med 2015;373: )
36 Genotype 4 Options Combination regimen No cirrhosis Compensated cirrhosis Rx-naïve Rx-exp d Rx-naïve Rx-exp d SOF/LDV ± RBV 12 wk 12 wk + RBV* 12 wk 12 wk + RBV* SOF/VEL ± RBV 12 wk 12 wk 12 wk 12 wk OBV/PTV/r (2D) ± RBV 12 wk + RBV 12 wk + RBV 12 wk + RBV 12 wk + RBV GZR/EBR ± RBV 12 wk >800, wk >800,000 SOF + DCV ± RBV 12 wk 12 wk + RBV* 12 wk 12 wk + RBV* SOF + SIM ±RBV 12 wk 12 wk + RBV* 12 wk 12 wk + RBV* *24 wk without RBV if RBV contraindicated poly tolerated
37 Genotype 4 Options Combination regimen No cirrhosis Compensated cirrhosis Rx-naïve Rx-exp d Rx-naïve Rx-exp d SOF/LDV ± RBV 12 wk 12 wk + RBV* 12 wk 12 wk + RBV* SOF/VEL ± RBV 12 wk 12 wk 12 wk 12 wk OBV/PTV/r (2D) ± RBV 12 wk + RBV 12 wk + RBV 12 wk + RBV 12 wk + RBV GZR/EBR ± RBV 12 wk >800, wk >800,000 SOF + DCV ± RBV 12 wk 12 wk + RBV* 12 wk 12 wk + RBV* SOF + SIM ±RBV 12 wk 12 wk + RBV* 12 wk 12 wk + RBV* *24 wk without RBV if RBV contraindicated poly tolerated
38 Genotype 4 Options Combination regimen No cirrhosis Compensated cirrhosis Rx-naïve Rx-exp d Rx-naïve Rx-exp d SOF/LDV ± RBV 12 wk 12 wk + RBV* 12 wk 12 wk + RBV* SOF/VEL ± RBV 12 wk 12 wk 12 wk 12 wk OBV/PTV/r (2D) ± RBV 12 wk + RBV 12 wk + RBV 12 wk + RBV 12 wk + RBV GZR/EBR ± RBV 12 wk >800, wk >800,000 SOF + DCV ± RBV 12 wk 12 wk + RBV* 12 wk 12 wk + RBV* SOF + SIM ±RBV 12 wk 12 wk + RBV* 12 wk 12 wk + RBV* *24 wk without RBV if RBV contraindicated poly tolerated
39 SVR12 rate (%) Sofosbuvir + Velpatasvir ASTRAL-1 Phase III, TN and TE (32%), Gt 4, 19% cirrhosis, 12 wks % N=116 GT4 (Feld et al., N Engl J Med 2015;373: )
40 SVR12 rate (%) Grazoprevir + Elbasvir Integrated analysis of Phase II and III trials, Gt 4, w/o cirrhosis Treatment-naïve Treatment-experienced % 100% 93% 100% % % 10 0 N=56 N=10 N=9 N=15 No RBV 12 weeks + RBV 12 weeks No RBV 12 weeks + RBV 12 weeks N=5 N=8 No RBV 16 weeks + RBV 16 weeks (Asselah et al., AASLD 2015)
41 Genotype 5-6 Options Combination regimen No cirrhosis Compensated cirrhosis Rx-naïve Rx-exp d Rx-naïve Rx-exp d SOF/LDV ± RBV 12 wk 12 wk + RBV* 12 wk 12 wk + RBV* SOF/VEL ± RBV 12 wk 12 wk 12 wk 12 wk SOF + DCV ± RBV 12 wk 12 wk + RBV* 12 wk 12 wk + RBV* *24 wk without RBV if RBV contraindicated poly tolerated
42 Genotype 5-6 Options Combination regimen No cirrhosis Compensated cirrhosis Rx-naïve Rx-exp d Rx-naïve Rx-exp d SOF/LDV ± RBV 12 wk 12 wk + RBV* 12 wk 12 wk + RBV* SOF/VEL ± RBV 12 wk 12 wk 12 wk 12 wk SOF + DCV ± RBV 12 wk 12 wk + RBV* 12 wk 12 wk + RBV* *24 wk without RBV if RBV contraindicated poly tolerated
43 SVR12 rate (%) Sofosbuvir + Velpatasvir ASTRAL-1 Phase III, TN and TE (32%), Gt 1,2,4,5,6, 19% cirrhosis, 12 wks % 100% N=35 GT5 N=41 GT6 (Feld et al., N Engl J Med 2015;373: )

44 Utility of HCV resistance testing pri to first-line therapy

45 HCV RAS Testing Pri to First-line Therapy Systematic testing f HCV resistance pri to treatment is NOT recommended. Indeed, this obligation would seriously limit access to care and treatment regimens can be optimized without this infmation Physicians who have easy access to a reliable test assessing HCV resistance to NS5A inhibits (spanning amino acids 24 to 93) can use these results to guide their decisions The test should be based on population sequencing (repting RASs as present absent ) deep sequencing with a cutoff of 15% (only RASs that are present in me than 15% of the sequences generated must be considered)


46 HCV Resistance Testing Pri to First-Line DAA Therapy Not available Available, reliable, interpretable, understandable* *recommended f GZR/EBR f US patients with GT1a Optimize therapy to avoid treatment failure Presence of NS5As RASs conferring high-level resistance (pop seq >15%) SOF/LDV, SOF/DCV, SOF/SIM: Add RBV in G1a TE SOF/VEL: Add RBV in G3 TE patients and cirrhotics GZR/EBR: use 16 weeks with RBV in GT1a Add ribavirin and/ increase treatment duration in patients with NS5A RASs
47 SVR12 (%) SVR Accding to Baseline NS5A RASs GT1, SOF/LDV, guidelines-recommended With NS5A RASs No NS5A RASs Without cirrhosis With cirrhosis Rx-Naive Rx-Exp d Rx-Naive Rx-Exp d % 99% 99% 99% 90% 99% 96% 96% 100%100% 88% 100% 89% 96% 87% 100% N=32 N=108 N=189 N=509 N=88 N=300 N=27 N=68 N=10 N=27 N=9 N=19 N=66 N=214 N=15 N=84 8 Wks* 12 Wks 12 Wks 12 Wks 12 Wks + RBV * < 6 million IU/mL 24 Wks 12 Wks + RBV 24 Wks (Zeuzem et al., AASLD 2015)
48 SVR12 rate (%) Grazoprevir/Elbasvir Pooled efficacy population-phase II and III trials, GT1a, 12 weeks, no RBV No NS5A RASs With NS5A RASs % 100% 97% 100% 97% % % N=119 N=624 N=273 N=21 N=14 N=69 N= ,000 IU/mL >800,000 IU/mL Treatment-naïve (Merck, communicated to the panel) 800,000 IU/mL >800,000 IU/mL Treatment-experienced

49 SVR12 rate (%) Sofosbuvir/Ledipasvir FDC + RBV SOLAR-1- Genotype 1, decompensated cirrhosis LDV/SOF + RBV 12 Weeks LDV/SOF + RBV 24 Weeks % 89% 87% 89% 86% 90% N=52 N=47 Overall N=30 N=27 N=22 N=20 CPT B CPT C (Charlton et al., Gastroenterology 2015;149:649-59)
50 SOF/LDV SOF+DCV ± RBV Real-life UK EAP, Decompensated cirrhosis (CPT 7), All GTs Change in MELD sce (Foster et al., J Hepatol 2016;64: )
51 Patients with Decompensated Cirrhosis Without an Indication f LT Patients with decompensated cirrhosis (CPT-B CPT- C) not on the waiting list f liver transplantation and without concomitant combidities that could impact their survival should be treated urgently Protease inhibits should not be used in patients with Child-Pugh B and are contraindicated in patients with Child-Pugh C decompensated cirrhosis Frequent clinical and labaty assessment is necessary
A One-day Scientific Conference: Updates on Hepatitis C Treatments along with Consensus on Management of Hepatitis C in Iran
 A One-day Scientific Conference: Updates on Hepatitis C Treatments along with Consensus on Management of Hepatitis C in Iran Teheran, 22 July 2016 Massimo Colombo Treatment of HCV genotype 1 & 4 with DAAs
A One-day Scientific Conference: Updates on Hepatitis C Treatments along with Consensus on Management of Hepatitis C in Iran Teheran, 22 July 2016 Massimo Colombo Treatment of HCV genotype 1 & 4 with DAAs
Utility of Virological Assays at the DAA Era
 Utility of Virological Assays at the DAA Era Prof. Jean-Michel Pawlotsky, MD, PhD National Reference Center for Viral Hepatitis B, C and delta Department of Virology & INSERM U955 Henri Mondor Hospital
Utility of Virological Assays at the DAA Era Prof. Jean-Michel Pawlotsky, MD, PhD National Reference Center for Viral Hepatitis B, C and delta Department of Virology & INSERM U955 Henri Mondor Hospital
Hepatitis C in Special Populations
 Hepatitis C in Special Populations David E. Bernstein, MD, FACG Vice Chairman of Medicine for Clinical Trials Chief, Division of Hepatology and Sandra Atlas Bass Center for Liver Diseases Northwell Health
Hepatitis C in Special Populations David E. Bernstein, MD, FACG Vice Chairman of Medicine for Clinical Trials Chief, Division of Hepatology and Sandra Atlas Bass Center for Liver Diseases Northwell Health
HCV Treatment Failure: What Next? Dr Ashley Brown, Imperial College Healthcare NHS Trust, London
 HCV Treatment Failure: What Next? Dr Ashley Brown, Imperial College Healthcare NHS Trust, London European HIV Hepatitis Co-infection Conference QEII Conference Centre 10 th December 2015 Dr Ashley Brown
HCV Treatment Failure: What Next? Dr Ashley Brown, Imperial College Healthcare NHS Trust, London European HIV Hepatitis Co-infection Conference QEII Conference Centre 10 th December 2015 Dr Ashley Brown
How to optimize treatment in G3 patients? Jérôme GOURNAY, MD Hépatologie Centre Hospitalier Universitaire de Nantes France
 How to optimize treatment in G3 patients? Jérôme GOURNAY, MD Hépatologie Centre Hospitalier Universitaire de Nantes France Paris Hepatitis Conference, January 12, 2016 Disclosures I have received funding
How to optimize treatment in G3 patients? Jérôme GOURNAY, MD Hépatologie Centre Hospitalier Universitaire de Nantes France Paris Hepatitis Conference, January 12, 2016 Disclosures I have received funding
Need to Assess HCV Resistance to DAAs: Is it Useful and When?
 Need to Assess HCV Resistance to DAAs: Is it Useful and When? Stéphane Chevaliez French National Reference Center for Viral Hepatitis B, C and delta Department of Virology & INSERM U955 Henri Mondor Hospital
Need to Assess HCV Resistance to DAAs: Is it Useful and When? Stéphane Chevaliez French National Reference Center for Viral Hepatitis B, C and delta Department of Virology & INSERM U955 Henri Mondor Hospital
Treatment of HCV infection in daily clinical practice. Which are the optimal options for Genotypes 2 and 3? Jiannis Vlachogiannakos
 Treatment of HCV infection in daily clinical practice. Which are the optimal options for Genotypes 2 and 3? Jiannis Vlachogiannakos Associate Professor of Gastroenterology Academic Department of Gastroenterology
Treatment of HCV infection in daily clinical practice. Which are the optimal options for Genotypes 2 and 3? Jiannis Vlachogiannakos Associate Professor of Gastroenterology Academic Department of Gastroenterology
Treating HCV Prior to Liver Transplantation. What Are the Treatment Options? Xavier Forns Liver Unit Hospital Clinic, CIBEREHD, IDIBAPS Barcelona
 Treating HCV Prior to Liver Transplantation What Are the Treatment Options? Xavier Forns Liver Unit Hospital Clinic, CIBEREHD, IDIBAPS Barcelona Disclosures Unrestricted Grant Support: Janssen and Abbvie
Treating HCV Prior to Liver Transplantation What Are the Treatment Options? Xavier Forns Liver Unit Hospital Clinic, CIBEREHD, IDIBAPS Barcelona Disclosures Unrestricted Grant Support: Janssen and Abbvie
Saeed Hamid, MD Alex Thompson, MD, PhD
 Saeed Hamid, MD Alex Thompson, MD, PhD 1 We will review some top line data from EASL Majority of the time discussing how the data affects daily practice 2 Grazoprevir (GZR; MK-5172) + Elbasvir (EBR; MK-
Saeed Hamid, MD Alex Thompson, MD, PhD 1 We will review some top line data from EASL Majority of the time discussing how the data affects daily practice 2 Grazoprevir (GZR; MK-5172) + Elbasvir (EBR; MK-
TREATING HEPATITIS C TODAY
 TREATING HEPATITIS C TODAY Nikolaos K. Gatselis Department of Medicine& Research Laboratory of Internal Medicine, Larissa Medical School, Thessaly University Disclosure Research Support: Gilead, Janssen,
TREATING HEPATITIS C TODAY Nikolaos K. Gatselis Department of Medicine& Research Laboratory of Internal Medicine, Larissa Medical School, Thessaly University Disclosure Research Support: Gilead, Janssen,
Transformation of Chronic Hepatitis C Treatment
 Transformation of Chronic Hepatitis C Treatment UVHS, Adana, 22 May 2015 Christoph Sarrazin Goethe-University Hospital Frankfurt am Main Germany Epidemiology of HCV Infection Global Global HCV Prevalence
Transformation of Chronic Hepatitis C Treatment UVHS, Adana, 22 May 2015 Christoph Sarrazin Goethe-University Hospital Frankfurt am Main Germany Epidemiology of HCV Infection Global Global HCV Prevalence
Viva La Revolución: Options to Combat Hepatitis C
 Viva La Revolución: Options to Combat Hepatitis C David L. Wyles, MD Professor of Medicine University of Colorado Chief, Division of Infectious Disease Denver Health Learning Objectives After attending
Viva La Revolución: Options to Combat Hepatitis C David L. Wyles, MD Professor of Medicine University of Colorado Chief, Division of Infectious Disease Denver Health Learning Objectives After attending
Current HCV Treatment by Genotype
 Current HCV Treatment by Genotype Ari Bunim, MD Assistant Professor Clinical Medicine Weill Cornell Medical College Clinical Director of Hepatology New York-Presbyterian/Queens Objectives To understand
Current HCV Treatment by Genotype Ari Bunim, MD Assistant Professor Clinical Medicine Weill Cornell Medical College Clinical Director of Hepatology New York-Presbyterian/Queens Objectives To understand
2017 Bruce Lucas Hepatology and Liver Transplant Symposium October 13th 2017 Management of Hepatitis C in Pre- and Post-Transplant Patients
 2017 Bruce Lucas Hepatology and Liver Transplant Symposium October 13th 2017 Management of Hepatitis C in Pre- and Post-Transplant Patients Jens Rosenau, MD Associate Professor of Medicine Acting Director
2017 Bruce Lucas Hepatology and Liver Transplant Symposium October 13th 2017 Management of Hepatitis C in Pre- and Post-Transplant Patients Jens Rosenau, MD Associate Professor of Medicine Acting Director
Hepatitis C: Difficult-to-treat Patients 11th Paris Hepatology Conference 16th January 2018 Stefan Zeuzem, MD University Hospital, Frankfurt, Germany
 Hepatitis C: Difficult-to-treat Patients 11th Paris Hepatology Conference 16th January 2018 Stefan Zeuzem, MD University Hospital, Frankfurt, Germany PHC 2018 - www.aphc.info Disclosures Advisory boards:
Hepatitis C: Difficult-to-treat Patients 11th Paris Hepatology Conference 16th January 2018 Stefan Zeuzem, MD University Hospital, Frankfurt, Germany PHC 2018 - www.aphc.info Disclosures Advisory boards:
Treatment of HCV in 2016
 5/1/16 Treatment of HCV in 16 Graham R Foster Professor of Hepatology QMUL Conflicts of Interest Speaker and consultancy fees received from AbbVie, BI, BMS, Gilead, Janssen, Roche, Merck, Novartis, Springbank,
5/1/16 Treatment of HCV in 16 Graham R Foster Professor of Hepatology QMUL Conflicts of Interest Speaker and consultancy fees received from AbbVie, BI, BMS, Gilead, Janssen, Roche, Merck, Novartis, Springbank,
A treatment revolution: current management for chronic HCV
 A treatment revolution: current management for chronic HCV Ray Chung, M.D. Director of Hepatology and Liver Center Kevin and Polly Maroni Research Scholar Massachusetts General Hospital Disclosures Research
A treatment revolution: current management for chronic HCV Ray Chung, M.D. Director of Hepatology and Liver Center Kevin and Polly Maroni Research Scholar Massachusetts General Hospital Disclosures Research
Tough Cases in HIV/HCV Coinfection
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER Tough Cases in HIV/HCV Coinfection John Scott, MD, MSc Assistant Professor University of Washington Presentation prepared by: J Scott Last Updated: Jun 5, 2014
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Tough Cases in HIV/HCV Coinfection John Scott, MD, MSc Assistant Professor University of Washington Presentation prepared by: J Scott Last Updated: Jun 5, 2014
HCV Management in Decompensated Cirrhosis: Current Therapies
 Treatment of Patients with Decompensated Cirrhosis and Liver Transplant Recipients Paul Y. Kwo, MD, FACG Professor of Medicine Gastroenterology/Hepatology Division Stanford University email pkwo@stanford.edu
Treatment of Patients with Decompensated Cirrhosis and Liver Transplant Recipients Paul Y. Kwo, MD, FACG Professor of Medicine Gastroenterology/Hepatology Division Stanford University email pkwo@stanford.edu
Expert Perspectives: Best of HCV from EASL 2015
 Best of HCV from EASL 2015 Expert Perspectives: Best of HCV from EASL 2015 Saeed Hamid, MD Alex Thompson, MD, PhD This activity is supported by educational grants from AbbVie, Bristol-Myers Squibb, and
Best of HCV from EASL 2015 Expert Perspectives: Best of HCV from EASL 2015 Saeed Hamid, MD Alex Thompson, MD, PhD This activity is supported by educational grants from AbbVie, Bristol-Myers Squibb, and
Wonder pills, breakthroughs and continuing challenges HIV and Hepatitis C antiviral treatments revisited
 Wonder pills, breakthroughs and continuing challenges HIV and Hepatitis C antiviral treatments revisited Harald Hofer Department of Internal Medicine III Division of Gastroenterology and Hepatology Medical
Wonder pills, breakthroughs and continuing challenges HIV and Hepatitis C antiviral treatments revisited Harald Hofer Department of Internal Medicine III Division of Gastroenterology and Hepatology Medical
Treatment of Unique Populations Raymond T. Chung, MD
 Treatment of Unique Populations Raymond T. Chung, MD Director of Hepatology and Liver Center Vice Chief, Gastroenterology Kevin and Polly Maroni Research Scholar Mass General Hospital Disclosures Research
Treatment of Unique Populations Raymond T. Chung, MD Director of Hepatology and Liver Center Vice Chief, Gastroenterology Kevin and Polly Maroni Research Scholar Mass General Hospital Disclosures Research
Initial Treatment of HCV G Hugo E. Vargas, MD Professor of Medicine Medical, Director Office of Clinical Research Mayo Clinic Arizona
 Initial Treatment of HCV G1 2016 Hugo E. Vargas, MD Professor of Medicine Medical, Director Office of Clinical Research Mayo Clinic Arizona Disclosure Information Disclosure Information Dr. Vargas receives
Initial Treatment of HCV G1 2016 Hugo E. Vargas, MD Professor of Medicine Medical, Director Office of Clinical Research Mayo Clinic Arizona Disclosure Information Disclosure Information Dr. Vargas receives
Disclosures. Advanced HCV management. Overview. Renal failure 1/10/2018. Research Grant support to UCSF from AbbVie Gilead Merck Proteus NIH
 Disclosures Advanced HCV management Annie Luetkemeyer, MD Division of HIV, ID and Global Medicine ZSFG, UCSF Research Grant support to UCSF from AbbVie Gilead Merck Proteus NIH Overview Renal failure Acute
Disclosures Advanced HCV management Annie Luetkemeyer, MD Division of HIV, ID and Global Medicine ZSFG, UCSF Research Grant support to UCSF from AbbVie Gilead Merck Proteus NIH Overview Renal failure Acute
Hepatitis C: Newest Treatment Options and What To Do When We Cure It!
 Hepatitis C: Newest Treatment Options and What To Do When We Cure It! Richard Kalman, MD Division of Hepatology Department of Transplantation Einstein Medical Center Learning Objectives Scope of HCV How
Hepatitis C: Newest Treatment Options and What To Do When We Cure It! Richard Kalman, MD Division of Hepatology Department of Transplantation Einstein Medical Center Learning Objectives Scope of HCV How
Current HCV Treatment by Genotype Ira M. Jacobson, MD
 Current HCV Treatment by Genotype Ira M. Jacobson, MD Director of Hepatology NYU School of Medicine Objectives To understand the prevalence of HCV and distribution of HCV genotypes Describe the HCV lifecycle
Current HCV Treatment by Genotype Ira M. Jacobson, MD Director of Hepatology NYU School of Medicine Objectives To understand the prevalence of HCV and distribution of HCV genotypes Describe the HCV lifecycle
4/30/2015. Interactive Case-Based Presentations and Audience Discussion. Debika Bhattacharya, MD, MSc. Learning Objectives
 4/3/215 Interactive Case-Based Presentations and Audience Discussion Debika Bhattacharya, MD, MSc Assistant Clinical Professor University of California Los Angeles Los Angeles, California Formatted:4-27-215
4/3/215 Interactive Case-Based Presentations and Audience Discussion Debika Bhattacharya, MD, MSc Assistant Clinical Professor University of California Los Angeles Los Angeles, California Formatted:4-27-215
HCV Treatment of Genotype 1: Now and in the Future
 HCV Treatment of Genotype 1: Now and in the Future Bruce R. Bacon, MD, FACG James F. King, MD Endowed Chair in Gastroenterology Professor of Internal Medicine Co-Director of the Abdominal Transplant Program
HCV Treatment of Genotype 1: Now and in the Future Bruce R. Bacon, MD, FACG James F. King, MD Endowed Chair in Gastroenterology Professor of Internal Medicine Co-Director of the Abdominal Transplant Program
TREATMENT OF GENOTYPE 2
 Treatment of Genotype 2, 3,and 4 David E. Bernstein, MD, FACG Advisory Committee/Board Member: AbbVie Pharmaceuticals, Gilead, Merck, Janssen Consultant: AbbVie Pharmaceuticals, Bristol-Myers Squibb, Gilead,
Treatment of Genotype 2, 3,and 4 David E. Bernstein, MD, FACG Advisory Committee/Board Member: AbbVie Pharmaceuticals, Gilead, Merck, Janssen Consultant: AbbVie Pharmaceuticals, Bristol-Myers Squibb, Gilead,
HCV Treatment in 2016
 HCV Treatment in 2016 Hugo E. Vargas, MD Professor of Medicine Mayo College of Medicine Medical Director, Clinical Trials Office Vice Chair, Department of Research Educational Goals Caveats: Cannot cover
HCV Treatment in 2016 Hugo E. Vargas, MD Professor of Medicine Mayo College of Medicine Medical Director, Clinical Trials Office Vice Chair, Department of Research Educational Goals Caveats: Cannot cover
HCV Resistance Clinical Aspects. Sanjay Bhagani Royal Free Hospital/UCL London
 HCV Resistance Clinical Aspects Sanjay Bhagani Royal Free Hospital/UCL London DAAs in 2018, and beyond % patients % patients Changing characteristics of patients treated with DAA over time Prospective,
HCV Resistance Clinical Aspects Sanjay Bhagani Royal Free Hospital/UCL London DAAs in 2018, and beyond % patients % patients Changing characteristics of patients treated with DAA over time Prospective,
HCV treatment options in clinical practice. Current treatment options for HCV-G4
 HCV treatment options in clinical practice Current treatment options for HCV-G4 C. Triantos Gastroenterology Department University Hospital of Patras Conflicts of interest Speaker and research/travel grants
HCV treatment options in clinical practice Current treatment options for HCV-G4 C. Triantos Gastroenterology Department University Hospital of Patras Conflicts of interest Speaker and research/travel grants
Genotype 1 HCV in 2016: Clinical Decision Making in a Time of Plenty
 Genotype 1 HCV in 216: Clinical Decision Making in a Time of Plenty Ira M. Jacobson, MD Chair, Department of Medicine Mount Sinai Beth Israel Senior Faculty and Vice-Chair, Department of Medicine Icahn
Genotype 1 HCV in 216: Clinical Decision Making in a Time of Plenty Ira M. Jacobson, MD Chair, Department of Medicine Mount Sinai Beth Israel Senior Faculty and Vice-Chair, Department of Medicine Icahn
Current trends in CHC 1st genotype treatment
 Current trends in CHC 1st genotype treatment Tarik Asselah MD, PhD Professor of Medicine Hepatology, Chief INSERM UMR 1149, Hôpital Beaujon, Clichy, France Disclosures Employee of Paris Public University
Current trends in CHC 1st genotype treatment Tarik Asselah MD, PhD Professor of Medicine Hepatology, Chief INSERM UMR 1149, Hôpital Beaujon, Clichy, France Disclosures Employee of Paris Public University
10/21/2016. Susanna Naggie, MD, MHS Associate Professor of Medicine Duke University Durham, North Carolina. Learning Objectives
 A Crash Course on the AASLD/IDSA Hepatitis C Virus Infection Treatment Guidelines: What s New Susanna Naggie, MD, MHS Associate Professor of Medicine Duke University Durham, North Carolina FORMATTED: 1/3/16
A Crash Course on the AASLD/IDSA Hepatitis C Virus Infection Treatment Guidelines: What s New Susanna Naggie, MD, MHS Associate Professor of Medicine Duke University Durham, North Carolina FORMATTED: 1/3/16
Treating now vs. post transplant
 Resistance with treatment failure Treating now vs. post transplant Pros (for treating pre transplant) If SVR efficacy means Better quality of life Removal from waiting list No post transplant recurrence
Resistance with treatment failure Treating now vs. post transplant Pros (for treating pre transplant) If SVR efficacy means Better quality of life Removal from waiting list No post transplant recurrence
Clinical guidelines for the treatment of hepatitis C in Iceland
 F the Treatment as Prevention f Hepatitis C in Iceland (TraP Hep C) A nationwide campaign f reducing disease burden using combination antiviral treatment Whom to treat All patients infected with the hepatitis
F the Treatment as Prevention f Hepatitis C in Iceland (TraP Hep C) A nationwide campaign f reducing disease burden using combination antiviral treatment Whom to treat All patients infected with the hepatitis
Patients with compensated cirrhosis: how to treat and follow-up
 Patients with compensated cirrhosis: how to treat and follow-up Thomas Berg Sektion Hepatologie Klinik und Poliklinik für Gastroenterologie und Rheumatologie Universitätsklinikum Leipzig Leber- und Studienzentrum
Patients with compensated cirrhosis: how to treat and follow-up Thomas Berg Sektion Hepatologie Klinik und Poliklinik für Gastroenterologie und Rheumatologie Universitätsklinikum Leipzig Leber- und Studienzentrum
New Hepatitis C Antivirals
 New Hepatitis C Antivirals Kris Stewart, BSP, MD, FRCPC Drug Therapy Conference College of Medicine, University of Saskatchewan September 23, 2016 Disclosures I have received research and program support
New Hepatitis C Antivirals Kris Stewart, BSP, MD, FRCPC Drug Therapy Conference College of Medicine, University of Saskatchewan September 23, 2016 Disclosures I have received research and program support
VIRAL LIVER DISEASE. OAG Post DDW Course Westin Prince, Toronto, June 13-14, 2015
 VIRAL LIVER DISEASE OAG Post DDW Course Westin Prince, Toronto, June 13-14, 2015 Financial Interest Disclosure (over the past 24 months) Dr. Paul Marotta Relationships related to this presentation! Research
VIRAL LIVER DISEASE OAG Post DDW Course Westin Prince, Toronto, June 13-14, 2015 Financial Interest Disclosure (over the past 24 months) Dr. Paul Marotta Relationships related to this presentation! Research
10/21/2016. David L. Wyles, MD Chief, Division of Infectious Disease Denver Health Medical Center Denver, Colorado
 Drug Resistance-Associated Variants in Hepatitis C Virus Infection: Hype or Help? David L. Wyles, MD Chief, Division of Infectious Disease Denver Health Medical Center Denver, Colorado FORMATTED: 1/3/16
Drug Resistance-Associated Variants in Hepatitis C Virus Infection: Hype or Help? David L. Wyles, MD Chief, Division of Infectious Disease Denver Health Medical Center Denver, Colorado FORMATTED: 1/3/16
David L. Wyles, MD Chief, Division of Infectious Disease Denver Health Medical Center Denver, Colorado
 FORMATTED: 1/3/16 Drug Resistance-Associated Variants in Hepatitis C Virus Infection: Hype or Help? Atlanta, Georgia: October 2, 216 David L. Wyles, MD Chief, Division of Infectious Disease Denver Health
FORMATTED: 1/3/16 Drug Resistance-Associated Variants in Hepatitis C Virus Infection: Hype or Help? Atlanta, Georgia: October 2, 216 David L. Wyles, MD Chief, Division of Infectious Disease Denver Health
Treating HCV After Liver Transplantation: What are the Treatment Options?
 4 th OPTIMIZE WORKSHOP USING DAAs IN PATIENTS WITH CIRRHOSIS AND LIVER RECIPIENTS Treating HCV After Liver Transplantation: What are the Treatment Options? Maria Carlota Londoño, MD Liver Unit, Hospital
4 th OPTIMIZE WORKSHOP USING DAAs IN PATIENTS WITH CIRRHOSIS AND LIVER RECIPIENTS Treating HCV After Liver Transplantation: What are the Treatment Options? Maria Carlota Londoño, MD Liver Unit, Hospital
What Should We Do With Difficult to Treat HCV Populations?
 What Should We Do With Difficult to Treat HCV Populations? Norah Terrault, MD Professor of Medicine and Surgery Director, Viral Hepatitis Center University of California San Francisco Disclosures Norah
What Should We Do With Difficult to Treat HCV Populations? Norah Terrault, MD Professor of Medicine and Surgery Director, Viral Hepatitis Center University of California San Francisco Disclosures Norah
Current Treatment Options for HCV Patients. Michael Manns Dept. of Gastroenterology, Hepatology and Endocrinology Hannover Germany
 Current Treatment Options for HCV Patients Michael Manns Dept. of Gastroenterology, Hepatology and Endocrinology Hannover Germany 7th International Congress of Internal Medicine of Central Greece, Larissa,
Current Treatment Options for HCV Patients Michael Manns Dept. of Gastroenterology, Hepatology and Endocrinology Hannover Germany 7th International Congress of Internal Medicine of Central Greece, Larissa,
HIV-HCV Co-Infection in Shobha Swaminathan, MD Associate Professor of Medicine Rutgers New Jersey Medical School
 HIV-HCV Co-Infection in 2018 Shobha Swaminathan, MD Associate Professor of Medicine Rutgers New Jersey Medical School AASLD/IDSA and DHHS Guidance: HIV/HCV Coinfection All pts with HIV should be screened
HIV-HCV Co-Infection in 2018 Shobha Swaminathan, MD Associate Professor of Medicine Rutgers New Jersey Medical School AASLD/IDSA and DHHS Guidance: HIV/HCV Coinfection All pts with HIV should be screened
Kristen M. Marks, MD Assistant Professor Weill Cornell Medical College New York, New York
 Newly Approved Hepatitis C Virus Drugs: Approach to Initial Therapy Kristen M. Marks, MD Assistant Professor Weill Cornell Medical College New York, New York Learning Objectives After attending this presentation,
Newly Approved Hepatitis C Virus Drugs: Approach to Initial Therapy Kristen M. Marks, MD Assistant Professor Weill Cornell Medical College New York, New York Learning Objectives After attending this presentation,
Why make this statement?
 HCV Council 2014 10 clinical practice statements were evaluated by the Council A review of the available literature was conducted The level of support and level of evidence for the statements were discussed
HCV Council 2014 10 clinical practice statements were evaluated by the Council A review of the available literature was conducted The level of support and level of evidence for the statements were discussed
Hepatitis C Introduction and Overview
 Hepatitis C Introduction and Overview Michael S. Saag, MD Professor of Medicine Associate Dean of Global Health Director, Center for AIDS Research University of Alabama at Birmingham Birmingham, Alabama
Hepatitis C Introduction and Overview Michael S. Saag, MD Professor of Medicine Associate Dean of Global Health Director, Center for AIDS Research University of Alabama at Birmingham Birmingham, Alabama
Baseline and acquired viral resistance to DAAs: how to test and manage
 Baseline and acquired viral resistance to DAAs: how to test and manage Round table discussion by Marc Bourliere, Robert Flisiak, Vasily Isakov, Mark Sulkowsky & Konstantin Zhdanov Prevalence of baseline
Baseline and acquired viral resistance to DAAs: how to test and manage Round table discussion by Marc Bourliere, Robert Flisiak, Vasily Isakov, Mark Sulkowsky & Konstantin Zhdanov Prevalence of baseline
THE THERAPEUTIC REVOLUTION THAT TRANSFORMED CHRONIC HEPATITIS C TO A CURABLE DISEASE
 THE THERAPEUTIC REVOLUTION THAT TRANSFORMED CHRONIC HEPATITIS C TO A CURABLE DISEASE MARIA SCHINA CONSULTANT PHYSICIAN INTERNAL MEDICINE AND HEPATOLOGY ATHENS EUROCLINIC 10 th INTERNATIONAL CONGRESS OF
THE THERAPEUTIC REVOLUTION THAT TRANSFORMED CHRONIC HEPATITIS C TO A CURABLE DISEASE MARIA SCHINA CONSULTANT PHYSICIAN INTERNAL MEDICINE AND HEPATOLOGY ATHENS EUROCLINIC 10 th INTERNATIONAL CONGRESS OF
Hepatitis C Resistance Associated Variants (RAVs)
") Hepatitis C Resistance Associated Variants (RAVs) Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Nothing to disclose Disclosure
Hepatitis C Resistance Associated Variants (RAVs) Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Nothing to disclose Disclosure
Next generation DAAs: Combining efficacy and safety profile. Jiannis Vlachogiannakos
 Next generation DAAs: Combining efficacy and safety profile. Jiannis Vlachogiannakos Associate Professor of Gastroenterology, Academic Department of Gastroenterology, National and Kapodistrian University
Next generation DAAs: Combining efficacy and safety profile. Jiannis Vlachogiannakos Associate Professor of Gastroenterology, Academic Department of Gastroenterology, National and Kapodistrian University
Debate: Do We Need More HCV Drugs Con Standpoint
 Debate: Do We Need More HCV Drugs Con Standpoint 18 th Antivirals PK Workshop, Friday 16 th June 2017, Chicago Jürgen Rockstroh Department of Medicine I University Hospital Bonn, Bonn, Germany Conflict
Debate: Do We Need More HCV Drugs Con Standpoint 18 th Antivirals PK Workshop, Friday 16 th June 2017, Chicago Jürgen Rockstroh Department of Medicine I University Hospital Bonn, Bonn, Germany Conflict
HCV In 2015: Maximizing SVR
 HCV In 2015: Maximizing SVR Alnoor Ramji Gastroenterology & Hepatology Clinical Associate Professor Division of Gastroenterology University Of British Columbia ramji_a@hotmail.com Disclosures (within Last
HCV In 2015: Maximizing SVR Alnoor Ramji Gastroenterology & Hepatology Clinical Associate Professor Division of Gastroenterology University Of British Columbia ramji_a@hotmail.com Disclosures (within Last
Massimo Puoti SC Malattie Infettive AO Ospedale Niguarda Cà Granda, Milano. Eradicazione da HCV e nuove prospettive: Prospetive Terapeutiche future
 Massimo Puoti SC Malattie Infettive AO Ospedale Niguarda Cà Granda, Milano Eradicazione da HCV e nuove prospettive: Prospetive Terapeutiche future DAA classes and subclasses Drug Class Subclass Potency
Massimo Puoti SC Malattie Infettive AO Ospedale Niguarda Cà Granda, Milano Eradicazione da HCV e nuove prospettive: Prospetive Terapeutiche future DAA classes and subclasses Drug Class Subclass Potency
HCV Therapy in Liver Transplant Candidate
 PHC 216 HCV Therapy in Liver Professor Didier SAMUEL Transplant Candidate Dr Audrey COILLY Centre Hépato-Biliaire, Inserm 1193 Treat before orrearch afuniter? University Paris Sud A Villejuif u d r e yfrance
PHC 216 HCV Therapy in Liver Professor Didier SAMUEL Transplant Candidate Dr Audrey COILLY Centre Hépato-Biliaire, Inserm 1193 Treat before orrearch afuniter? University Paris Sud A Villejuif u d r e yfrance
Update on Hepatitis C. Francesco Negro Hôpitaux Universitaires de Genève Berne, November 15, 2017
 Update on Hepatitis C Francesco Negro Hôpitaux Universitaires de Genève Berne, November 15, 2017 The global prevalence of HCV was 1 0% (95% uncertainty interval 0 8 1 1) in 2015: 71 1 million (62 5 79
Update on Hepatitis C Francesco Negro Hôpitaux Universitaires de Genève Berne, November 15, 2017 The global prevalence of HCV was 1 0% (95% uncertainty interval 0 8 1 1) in 2015: 71 1 million (62 5 79
Future strategies with new DAAs
 Future strategies with new DAAs Ola Weiland professor New direct antiviral drugs Case no 1 male with genotype 2b Male with gt 2b chronic HCV Male with gt 2b relapse afer peg-ifn + RBV during 24 weeks
Future strategies with new DAAs Ola Weiland professor New direct antiviral drugs Case no 1 male with genotype 2b Male with gt 2b chronic HCV Male with gt 2b relapse afer peg-ifn + RBV during 24 weeks
5/12/2016. Learning Objectives. Management of Hepatitis C Virus Genotype 2 or 3 Infected Treatment-Naive or Experienced Patients
 5/12/216 Management of Hepatitis C Virus Genotype 2 or 3 Infected Treatment-Naive or Experienced Patients Alexander Monto, MD Professor of Clinical Medicine University of California San Francisco San Francisco,
5/12/216 Management of Hepatitis C Virus Genotype 2 or 3 Infected Treatment-Naive or Experienced Patients Alexander Monto, MD Professor of Clinical Medicine University of California San Francisco San Francisco,
Hepatitis C: The New World of Treatment
 Hepatitis C: The New World of Treatment Aban 1395, NIOC Hospital Shahin Merat, M.D. Professor of Medicine Digestive Disease Research Institute Tehran University of Medical Sciences 1 Drugs NS5B polymerase
Hepatitis C: The New World of Treatment Aban 1395, NIOC Hospital Shahin Merat, M.D. Professor of Medicine Digestive Disease Research Institute Tehran University of Medical Sciences 1 Drugs NS5B polymerase
Management of HIV/HCV Coinfection. Kristen M. Marks, MD Assistant Professor Weill Cornell Medical College New York, NY
 Management of HIV/HCV Coinfection Kristen M. Marks, MD Assistant Professor Weill Cornell Medical College New York, NY Disclosure Dr. Marks has received grants and research support from Gilead Sciences
Management of HIV/HCV Coinfection Kristen M. Marks, MD Assistant Professor Weill Cornell Medical College New York, NY Disclosure Dr. Marks has received grants and research support from Gilead Sciences
Virological tools for hepatitis C: re-treatment and resistance. Joop Arends Will Irving. by author
 Virological tools for hepatitis C: re-treatment and resistance Joop Arends Will Irving Disclosures Joop Arends Advisory board: Gilead, Abbvie, Janssen, MSD, BMS (research) grants: Abbvie, BMS, MSD and
Virological tools for hepatitis C: re-treatment and resistance Joop Arends Will Irving Disclosures Joop Arends Advisory board: Gilead, Abbvie, Janssen, MSD, BMS (research) grants: Abbvie, BMS, MSD and
IL TRAPIANTO DI FEGATO: QUALE FUTURO CON LE NUOVE TERAPIE PER LE MALATTIE EPATICHE?
 IL TRAPIANTO DI FEGATO: QUALE FUTURO CON LE NUOVE TERAPIE PER LE MALATTIE EPATICHE? Francesco Paolo Russo Department of Surgery, Oncology and Gastroenterology Multivisceral/ Gastroenterology Section University
IL TRAPIANTO DI FEGATO: QUALE FUTURO CON LE NUOVE TERAPIE PER LE MALATTIE EPATICHE? Francesco Paolo Russo Department of Surgery, Oncology and Gastroenterology Multivisceral/ Gastroenterology Section University
Cases: Management of Hepatitis C in Prior Treatment Failure
 Cases: Management of Hepatitis C in Prior Treatment Failure David L. Wyles, MD Professor of Medicine University of Colorado Chief, Division of Infectious Disease Denver Health Learning Objectives After
Cases: Management of Hepatitis C in Prior Treatment Failure David L. Wyles, MD Professor of Medicine University of Colorado Chief, Division of Infectious Disease Denver Health Learning Objectives After
HIV/Hepatitis C in France: data from real life cohorts LIONEL PIROTH CHU DIJON UNIVERSITY OF BURGUNDY DECEMBER LONDON
 HIV/Hepatitis C in France: data from real life cohorts LIONEL PIROTH CHU DIJON UNIVERSITY OF BURGUNDY DECEMBER 2015 - LONDON The need Decreasing prevalence of chronic hepatitis C in French people living
HIV/Hepatitis C in France: data from real life cohorts LIONEL PIROTH CHU DIJON UNIVERSITY OF BURGUNDY DECEMBER 2015 - LONDON The need Decreasing prevalence of chronic hepatitis C in French people living
Terapie attuali. Eradicazione di HCV e nuove prospettive:
 Eradicazione di HCV e nuove prospettive: Terapie attuali Luisa Pasulo U.S.C. Gastroenterologia Epatologia e Trapiantologia Ospedale Papa Giovanni XXIII - Bergamo From Infection to liver disease Infezione
Eradicazione di HCV e nuove prospettive: Terapie attuali Luisa Pasulo U.S.C. Gastroenterologia Epatologia e Trapiantologia Ospedale Papa Giovanni XXIII - Bergamo From Infection to liver disease Infezione
Treatment of Hepatitis C Recurrence after Liver Transplantation. Maria Carlota Londoño Liver Unit Hospital Clínic Barcelona
 Treatment of Hepatitis C Recurrence after Liver Transplantation Maria Carlota Londoño Liver Unit Hospital Clínic Barcelona Agenda 1. Introduction 2. Treatment options for hepatitis C recurrence after transplantation
Treatment of Hepatitis C Recurrence after Liver Transplantation Maria Carlota Londoño Liver Unit Hospital Clínic Barcelona Agenda 1. Introduction 2. Treatment options for hepatitis C recurrence after transplantation
HCV in 2017: New Therapies and New Opportunities. Presentation prepared by: Date prepared: OBJECTIVES
 Project ECHO HCV Collaborative HCV in 217: New Therapies and New Opportunities Paulina Deming, PharmD Assistant Director Hepatitis C Programs, ECHO Institute Associate Professor College of Pharmacy University
Project ECHO HCV Collaborative HCV in 217: New Therapies and New Opportunities Paulina Deming, PharmD Assistant Director Hepatitis C Programs, ECHO Institute Associate Professor College of Pharmacy University
Norah Terrault, M.D. Professor of Medicine and Surgery Director, Viral Hepatitis Center University of California San Francisco
 Norah Terrault, MD Professor of Medicine and Surgery Director, Viral Hepatitis Center University of California San Francisco Disclosures Norah Terrault, M.D. Grants/Research Support AbbVie, Gilead, BMS,
Norah Terrault, MD Professor of Medicine and Surgery Director, Viral Hepatitis Center University of California San Francisco Disclosures Norah Terrault, M.D. Grants/Research Support AbbVie, Gilead, BMS,
HCV therapy : Clinical case
 HCV therapy : Clinical case PHC 2018 Paris January 14th, 2018 Tarik Asselah (MD, PhD) Professor of Medicine Hepatology, Chief INSERM UMR 1149, Hôpital Beaujon, Clichy, France. Disclosures Professor Asselah
HCV therapy : Clinical case PHC 2018 Paris January 14th, 2018 Tarik Asselah (MD, PhD) Professor of Medicine Hepatology, Chief INSERM UMR 1149, Hôpital Beaujon, Clichy, France. Disclosures Professor Asselah
Update in the Management of Hepatitis C: What Does the Future Hold
 Update in the Management of Hepatitis C: What Does the Future Hold Paul Y Kwo, MD, FACG Professor of Medicine Mdi Medical ldirector, Liver Transplantation tti Gastroenterology/Hepatology Division Indiana
Update in the Management of Hepatitis C: What Does the Future Hold Paul Y Kwo, MD, FACG Professor of Medicine Mdi Medical ldirector, Liver Transplantation tti Gastroenterology/Hepatology Division Indiana
HIV and Hepatitis C Have we finally slayed the beast?
 HIV and Hepatitis C Have we finally slayed the beast? Mark W. Sonderup Division of Hepatology Department of Medicine University of Cape Town & Groote Schuur Hospital Accelerated Fibrosis in HIV-HCV co-infected
HIV and Hepatitis C Have we finally slayed the beast? Mark W. Sonderup Division of Hepatology Department of Medicine University of Cape Town & Groote Schuur Hospital Accelerated Fibrosis in HIV-HCV co-infected
Special developments in the management of Hepatitis C. Disclosures
 Special developments in the management of Hepatitis C Sandeep Mukherjee,MD Division of Gastroenterology CHI Health and Creighton University Medical Center Omaha, NE 68154 Sandeep.Mukherjee@alegent.org
Special developments in the management of Hepatitis C Sandeep Mukherjee,MD Division of Gastroenterology CHI Health and Creighton University Medical Center Omaha, NE 68154 Sandeep.Mukherjee@alegent.org
IFN-free therapy in naïve HCV GT1 patients
 IFN-free therapy in naïve HCV GT1 patients Paris Hepatitis Conference Paris, 12th January, 2015 Pr Tarik Asselah MD, PhD; Service d Hépatologie & INSERM U773 University Paris Diderot, Hôpital Beaujon,
IFN-free therapy in naïve HCV GT1 patients Paris Hepatitis Conference Paris, 12th January, 2015 Pr Tarik Asselah MD, PhD; Service d Hépatologie & INSERM U773 University Paris Diderot, Hôpital Beaujon,
HEPATITIS C: UPDATE AND MANAGEMENT
 HEPATITIS C: UPDATE AND MANAGEMENT José Franco, MD Professor of Medicine Associate Dean for Educational Improvement Associate Director, Kern Institute STAR Center Director José Franco, MD Disclosures I
HEPATITIS C: UPDATE AND MANAGEMENT José Franco, MD Professor of Medicine Associate Dean for Educational Improvement Associate Director, Kern Institute STAR Center Director José Franco, MD Disclosures I
The Dawn of a New Era: Hepatitis C
 The Dawn of a New Era: Hepatitis C Naudia L. Jonassaint Assistant Professor of Medicine and Surgery University Pittsburgh School of Medicine December 1, 2015 Objectives After presentation the learner should
The Dawn of a New Era: Hepatitis C Naudia L. Jonassaint Assistant Professor of Medicine and Surgery University Pittsburgh School of Medicine December 1, 2015 Objectives After presentation the learner should
Shorter Durations and Pan-genotypic Regimens The Final Frontier. Professor Greg Dore
 Shorter Durations and Pan-genotypic Regimens The Final Frontier Professor Greg Dore Disclosures Funding and speaker fees from AbbVie, Bristol-Myers Squibb, Gilead Sciences and Merck Efficacy Evolution
Shorter Durations and Pan-genotypic Regimens The Final Frontier Professor Greg Dore Disclosures Funding and speaker fees from AbbVie, Bristol-Myers Squibb, Gilead Sciences and Merck Efficacy Evolution
6/2/2015. Interactive Case-Based Presentations and Audience Discussion
 6/2/215 Interactive Case-Based Presentations and Audience Discussion Andrew Aronsohn, MD Assistant Professor of Medicine University of Chicago Medical Center Chicago, Illinois Formatted:5-6-215 Washington,
6/2/215 Interactive Case-Based Presentations and Audience Discussion Andrew Aronsohn, MD Assistant Professor of Medicine University of Chicago Medical Center Chicago, Illinois Formatted:5-6-215 Washington,
Direct-acting Antiviral (DAA) Regimens in Late-stage Development: Which Patients Should Wait? Fred Poordad, MD
 Regimens in Late-stage Development: Which Patients Should Wait? Fred Poordad, MD") Direct-acting Antiviral (DAA) Regimens in Late-stage Development: Which Patients Should Wait? Fred Poordad, MD The HCV Lifecycle: Multiple Targets Polymerase Inhibitors Protease Inhibitors NS5A Inhibitors
Direct-acting Antiviral (DAA) Regimens in Late-stage Development: Which Patients Should Wait? Fred Poordad, MD The HCV Lifecycle: Multiple Targets Polymerase Inhibitors Protease Inhibitors NS5A Inhibitors
HCV-G3: Sofosbuvir with ledipasvir or daclatasvir?
 HCV-G3: Sofosbuvir with ledipasvir or daclatasvir? Ioannis Goulis, MD Aristotelian University of Thessaloniki XXIII International Hepatitis B & C Meeting of Athens Hadziyannis HCV genotype 3 therapy Chronic
HCV-G3: Sofosbuvir with ledipasvir or daclatasvir? Ioannis Goulis, MD Aristotelian University of Thessaloniki XXIII International Hepatitis B & C Meeting of Athens Hadziyannis HCV genotype 3 therapy Chronic
Hepatitis C Genotypes
 9/2/21 OBJECTIVES Project ECHO HCV Collaborative HCV in 21: New Therapies and New Opportunities Paulina Deming, PharmD Assistant Director Hepatitis C Programs, ECHO Institute Associate Professor College
9/2/21 OBJECTIVES Project ECHO HCV Collaborative HCV in 21: New Therapies and New Opportunities Paulina Deming, PharmD Assistant Director Hepatitis C Programs, ECHO Institute Associate Professor College
Hepatitis C ew Medications, New Hope and New. V. Opportunities for Primary Care. Outline. HCV Disease Outcomes in the US 9/21/2016
 Hepatitis C ew Medications, New Hope and New Opportunities for Primary Care Primary Care Principles and Practice October 14, 2016 Disclosures: Grant support Gilead Sciences, Inc Quality improvement Systematized
Hepatitis C ew Medications, New Hope and New Opportunities for Primary Care Primary Care Principles and Practice October 14, 2016 Disclosures: Grant support Gilead Sciences, Inc Quality improvement Systematized
Hepatitis C Virus Management
 Hepatitis C Virus Management FORMATTED: 04/20/17 New York, New York: February 24, 2017 Marion G. Peters, MD John V. Carbone, Endowed Chair Professor of Medicine University of California San Francisco San
Hepatitis C Virus Management FORMATTED: 04/20/17 New York, New York: February 24, 2017 Marion G. Peters, MD John V. Carbone, Endowed Chair Professor of Medicine University of California San Francisco San
Outline. HCV Disease Outcomes in the US. Hepatitis C: The New Landscape 5/24/16. Advances in Internal Medicine May 24, I have no disclosures
 5/24/16 Hepatitis C: The New Landscape Advances in Internal Medicine May 24, 2016 I have no disclosures Rena K. Fo, MD Professor of Clinical Medicine, UCSF Outline I. Current HCV outcomes in the US II.
5/24/16 Hepatitis C: The New Landscape Advances in Internal Medicine May 24, 2016 I have no disclosures Rena K. Fo, MD Professor of Clinical Medicine, UCSF Outline I. Current HCV outcomes in the US II.
Hepatitis C Virus: HIV/Hepatitis C Coinfection Wednesday, August 24, 2016
 Hepatitis C Virus: HIV/Hepatitis C Coinfection Debika Bhattacharya, MD, MSc Associate Clinical Professor University of California Los Angeles Los Angeles, California Washington, DC: August 24, 2016 Slide
Hepatitis C Virus: HIV/Hepatitis C Coinfection Debika Bhattacharya, MD, MSc Associate Clinical Professor University of California Los Angeles Los Angeles, California Washington, DC: August 24, 2016 Slide
Can we afford to Cure all HIV-HCV Co-infected Patients of HCV?
 Can we afford to Cure all HIV-HCV Co-infected Patients of HCV? Michael S. Saag, MD Professor of Medicine University of Alabama at Birmingham Birmingham, Alabama FINAL AU EDITED: 09-17-14 Disclosure Dr
Can we afford to Cure all HIV-HCV Co-infected Patients of HCV? Michael S. Saag, MD Professor of Medicine University of Alabama at Birmingham Birmingham, Alabama FINAL AU EDITED: 09-17-14 Disclosure Dr
What is the Optimized Treatment Duration? To Overtreat versus Undertreat. Nancy Reau, MD Associate Professor of Medicine University of Chicago
 What is the Optimized Treatment Duration? To Overtreat versus Undertreat Nancy Reau, MD Associate Professor of Medicine University of Chicago Learning Objectives: 1. Discuss patient populations appropriate
What is the Optimized Treatment Duration? To Overtreat versus Undertreat Nancy Reau, MD Associate Professor of Medicine University of Chicago Learning Objectives: 1. Discuss patient populations appropriate
STATE OF THE ART Update: Treatment Options 2016 Mark Sulkowski, MD
 Housekeeping Please turn off or silence cell phones. Restrooms are located on this floor. Make a left out of the ballroom foyer and the men s room is on your left. The ladies room is across from the elevators
Housekeeping Please turn off or silence cell phones. Restrooms are located on this floor. Make a left out of the ballroom foyer and the men s room is on your left. The ladies room is across from the elevators
5/10/2016. Management of Hepatitis C Virus Genotype 1 and 4 Treatment-Naive and Treatment-Experienced Patients. HCV life-cycle and antiviral targets
 5/1/216 Management of Hepatitis C Virus Genotype 1 and 4 Treatment-Naive and Treatment-Experienced Patients David L. Wyles, MD Associate Professor of Medicine University of California San Diego La Jolla,
5/1/216 Management of Hepatitis C Virus Genotype 1 and 4 Treatment-Naive and Treatment-Experienced Patients David L. Wyles, MD Associate Professor of Medicine University of California San Diego La Jolla,
HBV/HCV Eradication. Prof. Jean-Michel Pawlotsky, MD, PhD
 HBV/HCV Eradication Prof. Jean-Michel Pawlotsky, MD, PhD National Reference Center for Viral Hepatitis B, C and delta Department of Virology & INSERM U955 Henri Mondor Hospital University of Paris-Est
HBV/HCV Eradication Prof. Jean-Michel Pawlotsky, MD, PhD National Reference Center for Viral Hepatitis B, C and delta Department of Virology & INSERM U955 Henri Mondor Hospital University of Paris-Est
HEPATITIS WEB STUDY. Treatment of Hepatitis C following Liver Transplantation
 HEPATITIS WEB STUDY Treatment of Hepatitis C following Liver Transplantation Terry D. Box, MD Associate Professor of Medicine Division of Gastroenterology/Hepatology University of Utah Health Sciences
HEPATITIS WEB STUDY Treatment of Hepatitis C following Liver Transplantation Terry D. Box, MD Associate Professor of Medicine Division of Gastroenterology/Hepatology University of Utah Health Sciences
Rome, February nd Riunione Annuale AISF th AISF ANNUAL MEETING
 Rome, February 20-21 nd 2014 Riunione Annuale AISF 2014 14 th AISF ANNUAL MEETING Present and future treatment strategies for patients with HCV infection: chronic hepatitis and special populations IFN
Rome, February 20-21 nd 2014 Riunione Annuale AISF 2014 14 th AISF ANNUAL MEETING Present and future treatment strategies for patients with HCV infection: chronic hepatitis and special populations IFN
National Clinical Guidelines for the treatment of HCV in adults. Version 5
 National Clinical Guidelines for the treatment of HCV in adults Version 5 June 2018 Sponsors and Authorship The guidelines have been authored on behalf of the viral hepatitis clinical leads and MCN co-ordinators
National Clinical Guidelines for the treatment of HCV in adults Version 5 June 2018 Sponsors and Authorship The guidelines have been authored on behalf of the viral hepatitis clinical leads and MCN co-ordinators
TREATMENT OF HEPATITIS C IN THE LIVER TRANSPLANT SETTING. Dra. Zoe Mariño Liver Unit. Hospital Clinic Barcelona
 TREATMENT OF HEPATITIS C IN THE LIVER TRANSPLANT SETTING Dra. Zoe Mariño Liver Unit. Hospital Clinic Barcelona Hepatitis C after LT Survival (%) HCV negative HCV positive Time from LT (years) HCV treatment
TREATMENT OF HEPATITIS C IN THE LIVER TRANSPLANT SETTING Dra. Zoe Mariño Liver Unit. Hospital Clinic Barcelona Hepatitis C after LT Survival (%) HCV negative HCV positive Time from LT (years) HCV treatment
CCO Official Conference Coverage: Clinical Impact of New Data From AASLD 2015
 CCO Official Conference Coverage: Clinical Impact of New Data From AASLD 2015 CCO Official Conference Coverage of the 2015 Annual Meeting of the American Association for the Study of Liver Diseases, November
CCO Official Conference Coverage: Clinical Impact of New Data From AASLD 2015 CCO Official Conference Coverage of the 2015 Annual Meeting of the American Association for the Study of Liver Diseases, November
Disclosures. I have given sponsored lectures for the following pharmaceutical companies: Gilead, Abbvie and MSD. I own shares of Gilead Sciences.
 Disclosures I have given sponsored lectures for the following pharmaceutical companies: Gilead, Abbvie and MSD. I own shares of Gilead Sciences. Chronic Hepatitis C Prof CL Lai University Department of
Disclosures I have given sponsored lectures for the following pharmaceutical companies: Gilead, Abbvie and MSD. I own shares of Gilead Sciences. Chronic Hepatitis C Prof CL Lai University Department of
Learning Objective. After completing this educational activity, participants should be able to:
 Learning Objective After completing this educational activity, participants should be able to: Use patient characteristics and preferences to select HCV treatment strategies that maximize the potential
Learning Objective After completing this educational activity, participants should be able to: Use patient characteristics and preferences to select HCV treatment strategies that maximize the potential
Dogma: HCV treatment for eradication. Lisa Barrett MD PhD FRCPC Dept. of Infectious Diseases, Microbiology and Immunology April 18, 2015
 Dogma: HCV treatment for eradication Lisa Barrett MD PhD FRCPC Dept. of Infectious Diseases, Microbiology and Immunology April 18, 2015 Disclosures Some discussion of non-hc approved compounds Industry:
Dogma: HCV treatment for eradication Lisa Barrett MD PhD FRCPC Dept. of Infectious Diseases, Microbiology and Immunology April 18, 2015 Disclosures Some discussion of non-hc approved compounds Industry:
Hepatitis C Update: Screening, Diagnosis, and Treatment
 Mountain West AIDS Education and Training Center Hepatitis C Update: Screening, Diagnosis, and Treatment Brian R. Wood, MD (bwood2@uw.edu) Assistant Professor of Medicine, University of Washington Medical
Mountain West AIDS Education and Training Center Hepatitis C Update: Screening, Diagnosis, and Treatment Brian R. Wood, MD (bwood2@uw.edu) Assistant Professor of Medicine, University of Washington Medical