Optimizing Safety in Patients with Addictions
|
|
|
- Darlene Gallagher
- 5 years ago
- Views:
Transcription

1 Optimizing Safety in Patients with Addictions CRIT/FIT program May 2015 Alex Walley, MD, MSc Assistant Professor of Medicine
2 Learning objectives At the end of this session, you should be able to: 1. Define harm reduction and apply it to patient care 2. Teach overdose prevention strategies 3. Minimize the risk of polypharmacy among patients
3 Case You are called to admit a 29 yo woman with polydrug overdose, complicated by aspiration, and a left arm cellulitis. She was found unresponsive in the bathroom of a restaurant with a syringe, cooker and filters. Works as a waiter Injecting heroin daily since age 23. Uses cocaine on the weekends and drinks alcohol after work Trades sex for drugs, when money is short Prescribed clonazepam, clonidine and gabapentin for panic disorder and mood stabilization Treated with methadone and buprenorphine in the past when pregnant Intends to use again on discharge Despite your best brief intervention and motivational interviewing She is not interested in treatment at this time.
4 How do you optimize safety for people who continue to use (or who may relapse)? First assess risks: Infection risk behaviors Injection New needle and syringe every time Filters and Cooking Clean solvent Sex Without a condom? With multiple partners While using drugs In exchange for money or drugs bad date sheet Overdose risk behaviors Using alone Mixing substances - POLYPHARMACY Abstinence Unknown source Chronic illness Second: Make a safety plan
5 Optimizing safety (aka Harm Reduction)

6 What is Harm Reduction? Practical strategies and ideas to reduce substance use consequences A movement for social justice built on a belief in, and respect for, the rights of people who use substances. Harmreduction.org Interventions guided by risk-benefit analysis Abstinence is not a prerequisite to care

7 Harm Reduction Interventions Opioid agonist treatment to reduce HIV and mortality Treatment continuity post-incarceration Needle and syringe programs to reduce HIV and injection risk Pharmacy access needles and syringes Drug consumption rooms for injection risk and overdose mortality Naloxone rescue kits for opioid overdose mortality Pre and Post exposure prophylaxis Housing first programs Shelter-based alcohol administration Bad date sheets



8 Vascular Access


9 Filters Used to trap particulate matter Cotton balls, Q tip, tampon, cigarette filter Require manipulation with fingers Contamination with skin flora Ideal filter small, preformed (dental pellet)

10 To Cook or not to Cook Strang J et al. Different forms of heroin and their relationship to cook-up techniques: data on, and explanation of, use of lemon juice and other acids. Subst Use Misuse Apr;36(5):

11 Syringes and needles New needle and syringe each injection Needle dulls with each use Bleach is option Don t use syringe to divide dose or mix heroin
12 Change in HIV seroprevalence with and without needle-syringe programs Cities with NSPs Cities without NSPs All cities -5.8% per year +5.9% per year Cities with seroprevalence <10% -1.1% per year +16.2% per year Hurley et al. Lancet 1997:349; David Satcher, Surgeon General 2000 After reviewing all of the research to date, the senior scientists of the Department and I have unanimously agreed that there is conclusive scientific evidence that syringe exchange programs, as part of a comprehensive HIV prevention strategy, are an effective public health intervention that reduces the transmission of HIV and does not encourage the use of illegal drugs. In many cases, a decrease in injection frequency has been observed among those attending these programs. In addition, when properly structured, syringe exchange programs provide a unique opportunity for communities to reach out to the active drug injecting population and provide for the referral and retention of individuals in local substance abuse treatment and counseling programs and other important health services. -
13
 infections in community of 4200 Jan-April 2015 55% male, age range 18-57 80% acknowledge IDU, 3% deny IDU All PWIDs report oxymorphone tablets as drug of choice Other")
14 MMWR / May 1, 2015 / Vol. 64 / No (129 confirmed, 6 prelim) infections in community of 4200 Jan-April % male, age range % acknowledge IDU, 3% deny IDU All PWIDs report oxymorphone tablets as drug of choice Other injection drugs include methamphetamine and heroin 84% co-infected with HCV Up to three generations injecting together Crushing and cooking 40mg tablets with frequent sharing of injection equipment Number of injections per day range from 4-15 Injection partners range from 1 to 6

15 Overdose prevention
16
17 Intervention State legislation Pill Mills, Doctor Shopping, and Good Samaritan laws Prescription drug monitoring programs Insurance and pharmacy benefits manager Safe storage and disposal Clinical guidelines Findings Low evidence quality from 3 states where multiple efforts in place at the same time with inadequate controls No clear effects on total opioid prescribing or health outcomes. Data only up through 2008, Impact of proactive reporting or provider mandates not known Low evidence quality because lack of commparison groups, short-term follow-up and inadequate statistical testing Extremely low evidence quality from lack of baseline data and comparison groups, small sample size, short-term follow-up, health outcomes not assessed and inadequate controls Low evidence quality from lack of baseline data and comparison groups, small sample size, short-term follow-up and inadequate controls Education: Patient and Providers Moderate to low evidence quality. Few studies of patient education. Studies of providers find some adoption of safer prescribing, but less impact on patient outcomes Naloxone distribution Some evidence of effectiveness in reducing opioid overdose death rates, but overall low evidence quality. Data based on people who inject heroin The impact of state policy and systems-level interventions on prescription drug overdose Haegerich et al. Drug Alc Dep 2014: 145; 34-47

18 Intervention State legislation Pill Mills, Doctor Shopping, and Good Samaritan laws Prescription drug monitoring programs Insurance and pharmacy benefits manager Safe storage and disposal Clinical guidelines Findings Low evidence quality from 3 states where multiple efforts in place at the same time with inadequate controls No clear effects on total opioid prescribing or health outcomes. Data only up through 2008, Impact of proactive reporting or provider mandates not known Low evidence quality because lack of commparison groups, short-term follow-up and inadequate statistical testing Extremely low evidence quality from lack of baseline data and comparison groups, small sample size, short-term follow-up, health outcomes not assessed and inadequate controls Low evidence quality from lack of baseline data and comparison groups, small sample size, short-term follow-up and inadequate controls Education: Patient and Providers Moderate to low evidence quality. Few studies of patient education. Studies of providers find some adoption of safer prescribing, but less impact on patient outcomes Naloxone distribution Some evidence of effectiveness in reducing opioid overdose death rates, but overall low evidence quality. Data based on people who inject heroin The impact of state policy and systems-level interventions on prescription drug overdose Haegerich et al. Drug Alc Dep 2014: 145; 34-47

19 Intervention State legislation Pill Mills, Doctor Shopping, and Good Samaritan laws Prescription drug monitoring programs Insurance and pharmacy benefits manager Safe storage and disposal Clinical guidelines Findings Low evidence quality from 3 states where multiple efforts in place at the same time with inadequate controls No clear effects on total opioid prescribing or health outcomes. Data only up through 2008, Impact of proactive reporting or provider mandates not known Low evidence quality because lack of commparison groups, short-term follow-up and inadequate statistical testing Extremely low evidence quality from lack of baseline data and comparison groups, small sample size, short-term follow-up, health outcomes not assessed and inadequate controls Low evidence quality from lack of baseline data and comparison groups, small sample size, short-term follow-up and inadequate controls Education: Patient and Providers Moderate to low evidence quality. Few studies of patient education. Studies of providers find some adoption of safer prescribing, but less impact on patient outcomes Naloxone distribution Some evidence of effectiveness in reducing opioid overdose death rates, but overall low evidence quality. Data based on people who inject heroin The impact of state policy and systems-level interventions on prescription drug overdose Haegerich et al. Drug Alc Dep 2014: 145; 34-47

20 Intervention State legislation Pill Mills, Doctor Shopping, and Good Samaritan laws Prescription drug monitoring programs Insurance and pharmacy benefits manager Safe storage and disposal Clinical guidelines Education: Patient and Providers Naloxone distribution Findings Low evidence quality from 3 states where multiple efforts in place at the same time with inadequate controls No clear effects on total opioid prescribing or health outcomes. Data only up through 2008, Impact of proactive reporting or provider mandates not known Low evidence quality because lack of commparison groups, short-term follow-up and inadequate statistical testing Extremely low evidence quality from lack of baseline data and comparison groups, small sample size, short-term follow-up, health outcomes not assessed and inadequate controls Low evidence quality from lack of baseline data and comparison groups, small sample size, short-term follow-up and inadequate controls Moderate to low evidence quality. Few studies of patient education. Studies of providers find some adoption of safer prescribing, but less impact on patient outcomes Some evidence of effectiveness in reducing opioid overdose death rates, but overall low evidence quality. Data based on people who inject heroin The impact of state policy and systems-level interventions on prescription drug overdose Haegerich et al. Drug Alc Dep 2014: 145; 34-47

21 OD deaths per 100 pys Overdose deaths decrease when agonist Methadone and Buprenorphine in Baltimore: Schwartz et al. AJPH treatments increase



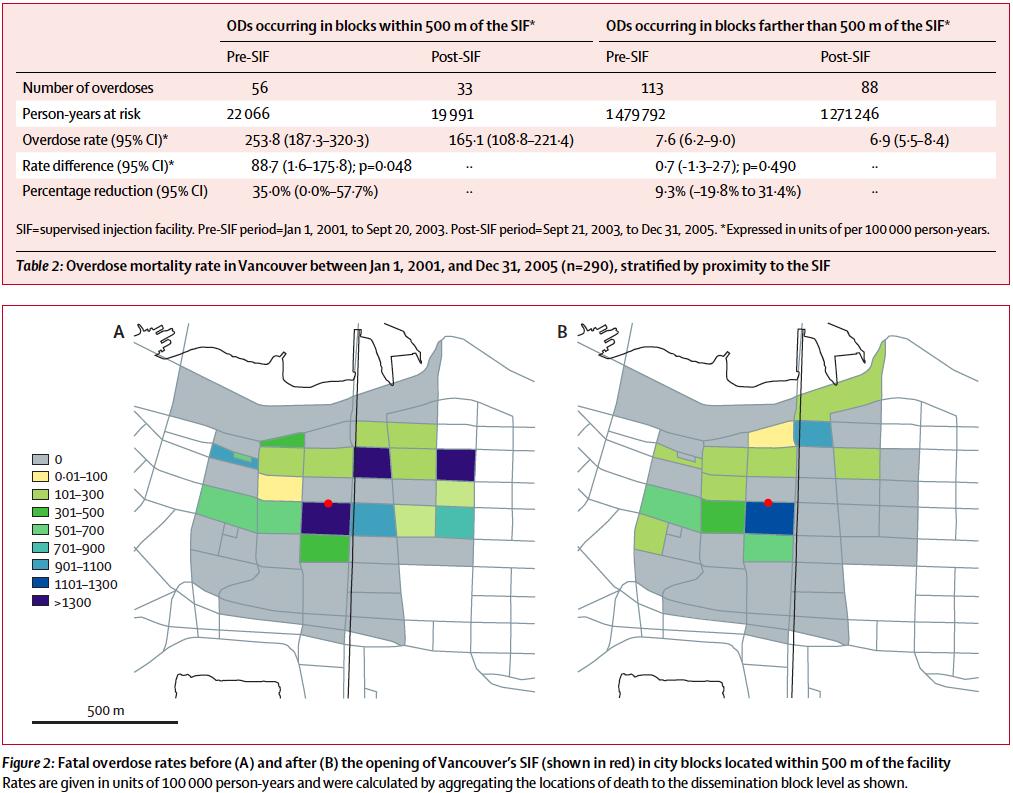
22 Supervised injection facilities Marshall et al. Lancet 2011:377;



23

 and > 4000 overdose rescues documented (4")
24 Enrollment locations: Program data from people with location reported: Users: 19,694 Non-Users: 10,250 Currently > 31,000 enrollees (16 per day) and > 4000 overdose rescues documented (4 per day)

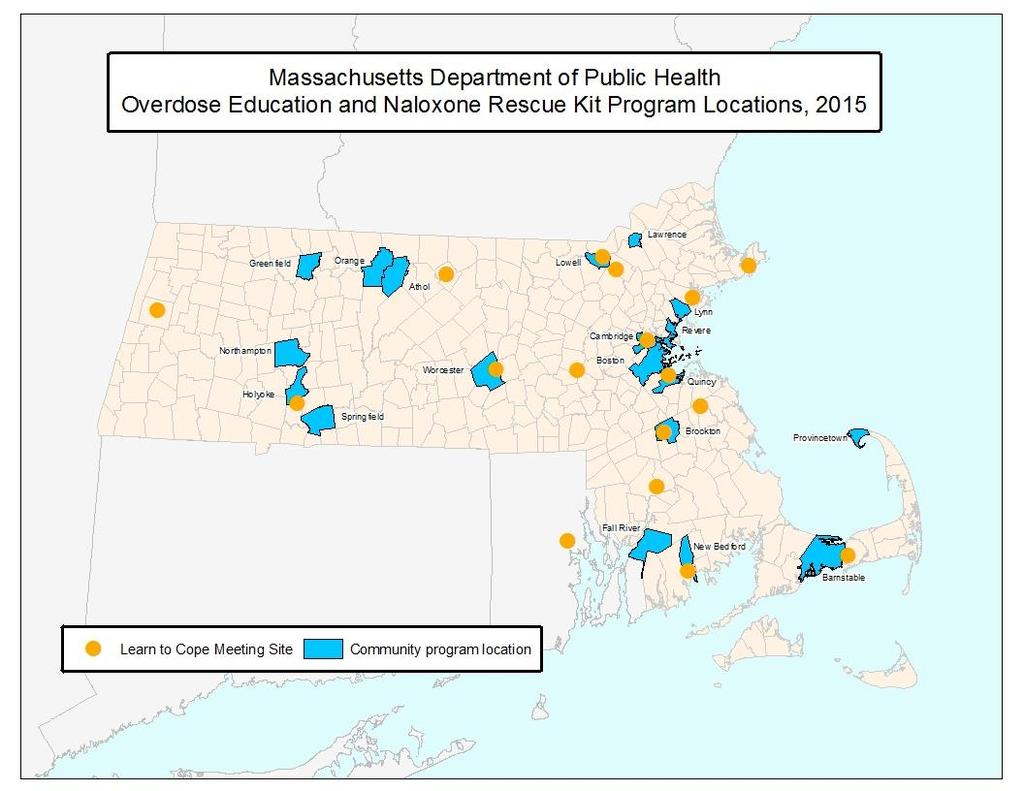
25 Opioid Overdose Related Deaths: Massachusetts OEND programs Towns without Number of Deaths No Deaths


26 Fatal opioid OD rates by OEND implementation Naloxone coverage per 100K Opioid overdose death rate 27% reduction 46% reduction Walley et al. BMJ 2013; 346: f174.





27 The AMA has been a longtime supporter of increasing the availability of Naloxone for patients, first responders and bystanders who can help save lives and has provided resources to bolster legislative efforts to increase access to this medication in several states. assn.org/ama/pub/news/news/2014/ naxolene-product-approval.page APhA supports the pharmacist s role in selecting appropriate therapy and dosing and initiating and providing education about the proper use of opioid reversal agents to prevent opioid-related deaths due to overdose ASAM Board of Directors April 2010 Naloxone has been proven to be an effective, fast-acting, inexpensive and non-addictive opioid antagonist with minimal side effects... Naloxone can be administered quickly and effectively by trained professional and lay individuals who observe the initial signs of an opioid overdose reaction



28 How to prescribe naloxone Three formulations 1. Injectable Dispense: 2x Naloxone 0.4mg/ml single dose vial or 1x 0.4mg/ml 10ml vial 2x IM syringe (3ml 25g 1 syringes recommended) Directions: For opioid overdose, inject 1ml IM in shoulder or thigh. Repeat after 3 minutes, if no or minimal response 2. Nasal (off-label) Dispense: 2x Naloxone 2mg/2ml prefilled luer-lock syringe 2x Mucosal Atomizer Device nasal adapter Directions: For opioid overdose, spray 1ml in each nostril. Repeat after 3 minutes, if no or minimal response 3. Ezvio Auto-injector -



29 Overdose Education and Naloxone Rescue What people need to know: 1.Prevention - the risks: Mixing substances Abstinence- low tolerance Using alone Unknown source Chronic medical disease Long acting opioids last longer 2.Recognition Unresponsive to sternal rub with slowed breathing Blue lips, pinpoint pupils 3.Response - What to do Call for help Rescue breathe Administer naloxone, continue breathing Recovery position Stay until help arrives Patient education videos and materials at prescribetoprevent.org
30 Polypharmacy
31 Overdose deaths in NYC Unintentional overdose deaths in NYC 100% 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% >1 substance Opioids Cocaine Alcohol BZD NYC Vital Signs. NYC DPMH. 2010

32 Rates of ED visits involving misuse or abuse of select pharmaceuticals per 100k, by age and drug:
33 Street pills Benzodiazepines Clonazepam (Klonopin) pins Alprazolam (Xanax) bars Diazepam (Valium) Also Z drugs ambien and lunesta Clonidine (Catapress) deans Promethazine (Phenergan) finnegans Queitiapine (Seroquel) Gabapentin (Neurontin) johnnies Pregabalin (Lyrica) super johnnies Buproprion (Wellbutrin)


34 Benzos Widespread Use Uncommon drug of choice Due to their significant margin of safety and effectiveness BZDs among the most prescribed psychotropic medications worldwide Prescribed to women more than men Lagnaoui Eur J Clin Pharmacol 2004; 60: On WHO essential drug list that should be available in all countries In the lab, people self-administer benzos but weak re-inforcers vs. alcohol, opioid, cocaine, and amphetamine Jones et al. DAD 2012; 125: Few drug treatment patients cite benzos as their drug of choice Cole and Chiarello. J Psychiatr Res. 1990; 24 Suppl 2:
35 Self-medication One physician survey reported that: 26% of psychiatrists 11% of other physcians Used unsupervised benzodiazepines in the past year Principles of Addiction Medicine, 4 th edition p.535.
36 Prescribers are ambivalent On the one hand Rarely drug of choice Given the amounts prescribed, benzo abuse is remarkably low Work fast: few side effects Benefit maintained over time On the other hand Non-medical use very common Concerning subgroups Other sedating meds Elderly Other addictions Hard to discontinue Does not improve long-term course of PTSD Co-morbid depression may worsen Schenck CH; Mahowald MW Am J Med 1996 Mar;100(3): Stevens, Pollack. J Clin Psychiatry 2005; 66s2: 21-27
37 What should be done about pills with a street value? Prescribe with caution Educate patients Safety first Teens, mixing meds, safe storage Function over feelings Risk of tolerance to benefits and withdrawal Communicate between prescribers Discontinue if risks outweigh the benefits
38 Case You are called to admit a 29 yo woman with polydrug overdose, complicated by aspiration, and a left arm cellulitis. She was found unresponsive in the bathroom of a restaurant with a syringe, cooker and filters. She works as a waitress and has been injecting heroin daily since age 23. She also uses cocaine on the weekends and drinks alcohol after work. She sometimes does sex work, when she does not have enough money. She is prescribed clonazepam, clonidine and gabapentin for panic disorder and mood stabilization. She tried methadone and buprenorphine in the past when she was pregnant. She intends to continue using again when she leaves the hospital. Despite your best brief intervention and motivational interviewing She is not interested in treatment at this time.
39 Case You are called to admit a 29 yo woman with polydrug overdose, complicated by aspiration, and a left arm cellulitis. She was found unresponsive in the bathroom of a restaurant with a syringe, cooker and filters. Works as a waiter Injecting heroin daily since age 23. Uses cocaine on the weekends and drinks alcohol after work Trades sex for drugs, when money is short Prescribed clonazepam, clonidine and gabapentin for panic disorder and mood stabilization Treated with methadone and buprenorphine in the past when pregnant Intends to use again on discharge Despite your best brief intervention and motivational interviewing She is not interested in treatment at this time.
40 Case 1. Discuss her addiction treatment options conduct a brief intervention Residential treatment, intensive outpatient, pharmacotherapy, 12-step groups 2. Review her injection and other drug use routine for knowledge and readiness Educate/ re-enforce safer use strategies NSP, keeping substances safe from others, not using alone, tester shots, PrEP 3. Ask her about her overdose experience Make a plan with her to reduce her own overdose risk and how to respond to others Prescribe naloxone rescue kit if available 4. Work to reduce sexual risk Condoms PEP and PrEP 5. Screen her for interpersonal violence. Offer IPV and sex worker services info 5. Express concern about her polypharmacy and polysubstance use and discuss strategies to reduce Speak to the prescriber of her clonazepam, clonidine, and gabapentin so the prescriber is aware of the overdose Encourage closer monitoring and a risk-benefit analysis for safety
41 Learning objectives At the end of this session, you should be able to: 1. Define harm reduction and apply it to patient care 2. Teach overdose prevention strategies 3. Minimize the risk of polypharmacy among patients
42 Go to prescribetoprevent.org Prescribe to Prevent: Overdose Prevention and Naloxone Rescue Kits for Prescribers and Pharmacists Alexander Y. Walley, MD, MSc Boston University School of Medicine Jeffrey Bratberg, PharmD, BCPS University of Rhode Island College of Pharmacy Corey Davis, JD, MSPH The Network for Public Health Law
43 Thanks! Alex Walley, MD, MSc Acknowledgments: Sarah Wakeman for several harm reduction slides


44 Bathrooms are injection facilities How to make them safer? Make your bathrooms safer - outfit bathrooms with: Secure biohazard boxes Good lighting Mirrors Doors that open out Call button Intercomm system Safer injection equipment Naloxone rescue kit

45 Prevalence of HIV infection among people who inject drugs Mather et al. Lancet 2008:372
46 Number of needle-syringes distributed per PWID per year Mather et al. Lancet 2010:375
47 Availability of methadone and buprenorphine maintenance Mather et al. Lancet 2010:375
48 Summary Injection drug use involves several steps, each with risks of infection Engaging with patients can help prevent harm Encourage users to: Find a clean setting Use sterile water Cook Dental pellets for filter if possible Clean, fresh syringe One-Wipe alcohol swipe Needleless syringes for sharing Vitamin C for solids


49 How do you incorporate overdose education and naloxone rescue kits into medical practice? 1. Prescribe naloxone rescue kits PrescribeToPrevent.org 2. Work with your overdose education and naloxone distribution program


50 Overdose Prevention in Medical Settings Review medications Communicate with other prescribers Take a substance use history Check the prescription monitoring program Overdose history: Where is the patient at as far as overdose? Ask your patients whether they have overdosed, witnessed an overdose or received training to prevent, recognize, or respond to an overdose Have you ever overdosed? What were you taking? How did you survive? What is your plan to protect yourself from overdose? How do you keep your medications safe? Are they locked up?

51 Overdose Prevention in Medical Settings Overdose witness history: How many overdoses have you witnessed? Were any fatal? What did you do? What is your plan if you witness an overdose in the future? How do you: recognize an overdose? call for help? rescue breathe? give naloxone? Do you have a naloxone rescue kit? Do you feel comfortable using it? 51
52 DEA NFLIS 2006 Report Prescription drugs seized by law enforcement and analyzed forensics labs: Drug Rx Dispensed Items seized per 10k Rx Dispensed Diazepam 65M 6.06 Alprazolam 169M 5.96 Morphine 23M 5.80 Oxycodone 161M 5.29 Clonazepam 82M 3.55 Hydrocodone 550M 1.63 Codeine 165M 1.06
53 If prescribing Consider when prescribing pills with a street value Intent Are you treating a diagnosed medical problem? Effect Does the medication improve the patient s functional status or worsen it? Monitoring Are you assessing the patient at the peak or trough effect of the medication?


54 Injecting Solids Oxycontin, Percocet, Crack All bases, need acid to dissolve Vinegar is caustic Lemon juice as solvent linked to disseminated candida Buchanan et al. DAD 2006:81: Ideal is Vitamin C powder
Optimizing Safety in Patients with Addictions
 Optimizing Safety in Patients with Addictions CRIT program April 2014 Alex Walley, MD, MSc Assistant Professor of Medicine Learning objectives At the end of this session, you should be able to: 1. Define
Optimizing Safety in Patients with Addictions CRIT program April 2014 Alex Walley, MD, MSc Assistant Professor of Medicine Learning objectives At the end of this session, you should be able to: 1. Define
Mainstreaming naloxone rescue kits from harm reduction programs to pharmacies, police and fire responders
 Mainstreaming naloxone rescue kits from harm reduction programs to pharmacies, police and fire responders Alexander Y. Walley, MD, MSc Boston University School of Medicine ThINC Bergen 2015 Conference
Mainstreaming naloxone rescue kits from harm reduction programs to pharmacies, police and fire responders Alexander Y. Walley, MD, MSc Boston University School of Medicine ThINC Bergen 2015 Conference
Optimizing Safety in People with Addictions
 We encourage you to use these slides when teaching. If you do, please cite this source and note any changes made. - The Immersion Training in Addiction Medicine Program Optimizing Safety in People with
We encourage you to use these slides when teaching. If you do, please cite this source and note any changes made. - The Immersion Training in Addiction Medicine Program Optimizing Safety in People with
Responding to the Opioid Epidemic
 Responding to the Opioid Epidemic Jessica Gray, MD Addiction Medicine Fellow Boston Medical Center ROME New England August 17, 2017 Disclosures for Jessica Gray, MD No conflicts Learning Objectives Describe
Responding to the Opioid Epidemic Jessica Gray, MD Addiction Medicine Fellow Boston Medical Center ROME New England August 17, 2017 Disclosures for Jessica Gray, MD No conflicts Learning Objectives Describe
Opioid Harm Reduction
 Opioid Harm Reduction Lucas G. Hill, PharmD Clinical Assistant Professor, The University of Texas at Austin College of Pharmacy Clinical Pharmacist, CommUnityCare FQHCs Director, Operation Naloxone Mark
Opioid Harm Reduction Lucas G. Hill, PharmD Clinical Assistant Professor, The University of Texas at Austin College of Pharmacy Clinical Pharmacist, CommUnityCare FQHCs Director, Operation Naloxone Mark
Take Home Naloxone: Law Update and Considerations for Pharmacy Professionals
 Take Home Naloxone: Law Update and Considerations for Pharmacy Professionals Clint Ross, PharmD, BCPP Clinical Pharmacy Specialist Psychiatry Residency Program Director Psychiatric Pharmacy Medical University
Take Home Naloxone: Law Update and Considerations for Pharmacy Professionals Clint Ross, PharmD, BCPP Clinical Pharmacy Specialist Psychiatry Residency Program Director Psychiatric Pharmacy Medical University
Naloxone: Preventing Opioid Overdose in the Community. Sharon Stancliff, MD Medical Director Harm Reduction Coalition
 Naloxone: Preventing Opioid Overdose in the Community Sharon Stancliff, MD Medical Director Harm Reduction Coalition DISCLOSURES Sharon Stancliff MD has nothing to disclose LEARNING OBJECTIVES 1. Discuss
Naloxone: Preventing Opioid Overdose in the Community Sharon Stancliff, MD Medical Director Harm Reduction Coalition DISCLOSURES Sharon Stancliff MD has nothing to disclose LEARNING OBJECTIVES 1. Discuss
Naloxone Non-Patient Specific Prescription and Pharmacist Dispensing Protocol, New York City
 Section 1: Purpose Naloxone Non-Patient Specific Prescription and Pharmacist Dispensing Protocol, New York City As some of health care s most accessible practitioners, pharmacists are uniquely positioned
Section 1: Purpose Naloxone Non-Patient Specific Prescription and Pharmacist Dispensing Protocol, New York City As some of health care s most accessible practitioners, pharmacists are uniquely positioned
Reducing opioid overdose mortality: role of communityadministered
 Reducing opioid overdose mortality: role of communityadministered naloxone Vennus Ballen, MD, MPH; Lara Maldjian, MPH New York City Department of Health and Mental Hygiene Clinical Director s Network (CDN)
Reducing opioid overdose mortality: role of communityadministered naloxone Vennus Ballen, MD, MPH; Lara Maldjian, MPH New York City Department of Health and Mental Hygiene Clinical Director s Network (CDN)
Anyone Can Become Addicted. Anyone.
 Anyone Can Become Addicted. Anyone. PAStop.org Family Toolkit Seeking Drug Abuse Treatment: Know What to Ask Trying to identify the right treatment programs for a loved one can be a difficult process.
Anyone Can Become Addicted. Anyone. PAStop.org Family Toolkit Seeking Drug Abuse Treatment: Know What to Ask Trying to identify the right treatment programs for a loved one can be a difficult process.
Opioid Overdose: Risks, Clinical Features, Treatment, and Reduction of Negative Consequences
 Opioid Overdose: Risks, Clinical Features, Treatment, and Reduction of Negative Consequences Joji Suzuki, MD Assistant Professor of Psychiatry Harvard Medical School Director, Division of Addiction Psychiatry
Opioid Overdose: Risks, Clinical Features, Treatment, and Reduction of Negative Consequences Joji Suzuki, MD Assistant Professor of Psychiatry Harvard Medical School Director, Division of Addiction Psychiatry
Revised 16 February, of 7
 341 State Street Suite G Madison, WI 53703 ph: (608) 251 4454 f: (608) 251 3853 6333 University Avenue, Middleton WI 53562 ph: (608) 310 5389 f: (608) 285 9603 INTRANASAL OR INTRAMUSCULAR NALOXONE PROTOCOL:
341 State Street Suite G Madison, WI 53703 ph: (608) 251 4454 f: (608) 251 3853 6333 University Avenue, Middleton WI 53562 ph: (608) 310 5389 f: (608) 285 9603 INTRANASAL OR INTRAMUSCULAR NALOXONE PROTOCOL:
Understanding and Combating the Heroin Epidemic
 Understanding and Combating the Heroin Epidemic Kelly Dunn, Ph.D. Assistant Professor; Johns Hopkins School of Medicine Department of Psychiatry and Behavioral Sciences 1 Talk Outline What is causing the
Understanding and Combating the Heroin Epidemic Kelly Dunn, Ph.D. Assistant Professor; Johns Hopkins School of Medicine Department of Psychiatry and Behavioral Sciences 1 Talk Outline What is causing the
Naloxone Standardized Procedures Illinois Departments of DFPR, DPH & DHS Opioid Antagonist Initiative
 Naloxone Standardized Procedures Illinois Departments of DFPR, DPH & DHS Opioid Antagonist Initiative Background: In September 2015, Illinois passed a new law, PA99-0480, expanding access to the opioid
Naloxone Standardized Procedures Illinois Departments of DFPR, DPH & DHS Opioid Antagonist Initiative Background: In September 2015, Illinois passed a new law, PA99-0480, expanding access to the opioid
Benzodiazepines. CRIT program May Alex Walley, MD, MSc Assistant Professor of Medicine Boston University School of Medicine
 Benzodiazepines CRIT program May 2010 Alex Walley, MD, MSc Assistant Professor of Medicine Boston University School of Medicine Medical Director, Opioid Treatment Program Boston Public Health Commission
Benzodiazepines CRIT program May 2010 Alex Walley, MD, MSc Assistant Professor of Medicine Boston University School of Medicine Medical Director, Opioid Treatment Program Boston Public Health Commission
Naloxone HCI 4 mg/0.1. nostril. Repeat after 3 minutes if minimal or no
 THE SOUTH CAROLINA BOARD OF MEDICAL EXAMINERS AND THE SOUTH CAROLINA BOARD OF PHARMACY S JOINT PROTOCOL TO INITIATE DISPENSING OF NALOXONE HCI WITHOUT A PRESCRIPTION This joint protocol authorizes any
THE SOUTH CAROLINA BOARD OF MEDICAL EXAMINERS AND THE SOUTH CAROLINA BOARD OF PHARMACY S JOINT PROTOCOL TO INITIATE DISPENSING OF NALOXONE HCI WITHOUT A PRESCRIPTION This joint protocol authorizes any
Take Home Naloxone: What Pharmacists Need to Know
 Take Home Naloxone: What Pharmacists Need to Know Sheri L. Fandrey, BSP, PhD Knowledge Exchange Lead Manitoba Addictions Knowledge Exchange Conflict of Interest/Disclosure Dr. Sheri Fandrey Has no conflicts
Take Home Naloxone: What Pharmacists Need to Know Sheri L. Fandrey, BSP, PhD Knowledge Exchange Lead Manitoba Addictions Knowledge Exchange Conflict of Interest/Disclosure Dr. Sheri Fandrey Has no conflicts
Prescription Opioids
 What are prescription opioids? Prescription Opioids Opioids are a class of drugs naturally found in the opium poppy plant. Some prescription opioids are made from the plant directly, and others are made
What are prescription opioids? Prescription Opioids Opioids are a class of drugs naturally found in the opium poppy plant. Some prescription opioids are made from the plant directly, and others are made
Overdose Prevention and Response and Relay, a post-overdose initiative
 Overdose Prevention and Response and Relay, a post-overdose initiative Emily Winkelstein, Community Engagement Manager Bureau of Alcohol and Drug Use Prevention, Care and Treatment Agenda How overdose
Overdose Prevention and Response and Relay, a post-overdose initiative Emily Winkelstein, Community Engagement Manager Bureau of Alcohol and Drug Use Prevention, Care and Treatment Agenda How overdose
OPIOID OVERDOSE EPIDEMIC: What Healthcare Providers Need to Know
 OPIOID OVERDOSE EPIDEMIC: What Healthcare Providers Need to Know WHAT S NEW UPDATE CUMBERLAND, MD Renata J. Henry, M.Ed. Director, Central East ATTC March 16, 2016 Behavioral Health is Essential to Health
OPIOID OVERDOSE EPIDEMIC: What Healthcare Providers Need to Know WHAT S NEW UPDATE CUMBERLAND, MD Renata J. Henry, M.Ed. Director, Central East ATTC March 16, 2016 Behavioral Health is Essential to Health
2018 APM Winter Meeting San Antonio, TX
 Moving target: The opioid crisis in the era of illicit fentanyl Alexander Y. Walley, MD, MSc Associate Professor of Medicine, BUSM Director, Addiction Medicine Fellowship, BMC Medical Director, Opioid
Moving target: The opioid crisis in the era of illicit fentanyl Alexander Y. Walley, MD, MSc Associate Professor of Medicine, BUSM Director, Addiction Medicine Fellowship, BMC Medical Director, Opioid
Overdose Prevention: Empowering School Personnel & Families
 Overdose Prevention: Empowering School Personnel & Families Christopher Welsh M.D. University of Maryland School of Medicine NCADD-Maryland Scientific Advisory Committee INITIATION OF DRUG USE >12 Y.O.(2013;
Overdose Prevention: Empowering School Personnel & Families Christopher Welsh M.D. University of Maryland School of Medicine NCADD-Maryland Scientific Advisory Committee INITIATION OF DRUG USE >12 Y.O.(2013;
Overdose Prevention, Recognition & Response Education Train-the-Trainer
 Overdose Prevention, Recognition & Response Education Train-the-Trainer Bernie Lieving, MSW Overdose Prevention Education Coordinator Santa Fe Prevention Alliance & Office of Substance Abuse Prevention
Overdose Prevention, Recognition & Response Education Train-the-Trainer Bernie Lieving, MSW Overdose Prevention Education Coordinator Santa Fe Prevention Alliance & Office of Substance Abuse Prevention
Washington State s Overdose Epidemic
 Caleb Banta-Green PhD MPH MSW Senior Research Scientist- Alcohol and Drug Abuse Institute Affiliate Associate Professor- School of Public Health Affiliate Faculty- Harborview Injury Prevention & Research
Caleb Banta-Green PhD MPH MSW Senior Research Scientist- Alcohol and Drug Abuse Institute Affiliate Associate Professor- School of Public Health Affiliate Faculty- Harborview Injury Prevention & Research
Naloxone Information for Community Pharmacies in Georgia: What You Need to Know
 Naloxone Information for Community Pharmacies in Georgia: What You Need to Know Your pharmacy may start receiving an increased volume of prescriptions for naloxone (Narcan ) due to legal changes in 2014.
Naloxone Information for Community Pharmacies in Georgia: What You Need to Know Your pharmacy may start receiving an increased volume of prescriptions for naloxone (Narcan ) due to legal changes in 2014.
Naloxone for Opioid Safety
 Naloxone for Opioid Safety Phillip O. Coffin, MD MIA San Francisco Department of Public Health University of California San Francisco Disclosure Information Gilead, Donated ledipasvir-sofosbuvir, Study,
Naloxone for Opioid Safety Phillip O. Coffin, MD MIA San Francisco Department of Public Health University of California San Francisco Disclosure Information Gilead, Donated ledipasvir-sofosbuvir, Study,
Opportunities for Opioid Safety and Community-Based Overdose Management
 Opportunities for Opioid Safety and Community-Based Overdose Management DANTE COLLINS ERICA C. ERNST MAYA DOE-SIMKINS SEPTEMBER 13, 2013 Overview Prevalence & data Overdose prevention Making an overdose
Opportunities for Opioid Safety and Community-Based Overdose Management DANTE COLLINS ERICA C. ERNST MAYA DOE-SIMKINS SEPTEMBER 13, 2013 Overview Prevalence & data Overdose prevention Making an overdose
Naloxone and Combating the Opioid Epidemic
 Objectives Naloxone and Combating the Opioid Epidemic Jeff Jacobson PharmD Southpointe Pharmacy Discuss the current opioid crisis Define the role of Naloxone in opioid overdose Analyze the barriers to
Objectives Naloxone and Combating the Opioid Epidemic Jeff Jacobson PharmD Southpointe Pharmacy Discuss the current opioid crisis Define the role of Naloxone in opioid overdose Analyze the barriers to
Medication-Assisted Treatment. What Is It and Why Do We Use It?
 Medication-Assisted Treatment What Is It and Why Do We Use It? What is addiction, really? o The four C s of addiction: Craving. Loss of Control of amount or frequency of use. Compulsion to use. Use despite
Medication-Assisted Treatment What Is It and Why Do We Use It? What is addiction, really? o The four C s of addiction: Craving. Loss of Control of amount or frequency of use. Compulsion to use. Use despite
NARCAN: THE HISTORY, APPLICATIONS AND FUTURE
 NARCAN: THE HISTORY, APPLICATIONS AND FUTURE TABLE OF CONTENTS 3 Intro 4 What is Naloxone? 8 How Naloxone is Administered 12 Where to Find Narcan in California The United States accounts for about five
NARCAN: THE HISTORY, APPLICATIONS AND FUTURE TABLE OF CONTENTS 3 Intro 4 What is Naloxone? 8 How Naloxone is Administered 12 Where to Find Narcan in California The United States accounts for about five
COMBATING THE OPIATE CRISIS IN OHIO THROUGH COMPREHENSIVE RESPONSE 2018 HOUSING OHIO CONFERENCE APRIL 9 TH, Objectives: Key Terms
 COMBATING THE OPIATE CRISIS IN OHIO THROUGH COMPREHENSIVE RESPONSE 2018 HOUSING OHIO CONFERENCE APRIL 9 TH, 2018 2 Objectives: qreview names of different types of opioids qidentify the signs and symptoms
COMBATING THE OPIATE CRISIS IN OHIO THROUGH COMPREHENSIVE RESPONSE 2018 HOUSING OHIO CONFERENCE APRIL 9 TH, 2018 2 Objectives: qreview names of different types of opioids qidentify the signs and symptoms
NALOXONE LEARNING ABOUT NALOXONE COULD SAVE A LIFE
 NALOXONE LEARNING ABOUT NALOXONE COULD SAVE A LIFE WHAT IT IS WHAT IT IS NARCAN (naloxone HCl) Nasal Spray is the first and only FDA-approved nasal form of naloxone for the emergency treatment of a known
NALOXONE LEARNING ABOUT NALOXONE COULD SAVE A LIFE WHAT IT IS WHAT IT IS NARCAN (naloxone HCl) Nasal Spray is the first and only FDA-approved nasal form of naloxone for the emergency treatment of a known
Preventing overdose fatalities: The role of naloxone and of supervised injection facilities Sharon Stancliff, MD Medical Director Harm Reduction
 Preventing overdose fatalities: The role of naloxone and of supervised injection facilities Sharon Stancliff, MD Medical Director Harm Reduction Coalition New York, NY Sleestan@gmail.com Strategies to
Preventing overdose fatalities: The role of naloxone and of supervised injection facilities Sharon Stancliff, MD Medical Director Harm Reduction Coalition New York, NY Sleestan@gmail.com Strategies to
Substance use and misuse
 An open learning programme for pharmacists and pharmacy technicians Substance use and misuse Educational solutions for the NHS pharmacy workforce DLP 160 Contents iii About CPPE open learning programmes
An open learning programme for pharmacists and pharmacy technicians Substance use and misuse Educational solutions for the NHS pharmacy workforce DLP 160 Contents iii About CPPE open learning programmes
Five Things the Family Physician Needs to Know about Addiction and Harm Reduction
 Five Things the Family Physician Needs to Know about Addiction and Harm Reduction Dr. Sharon Koivu Palliative Care Physician Consultant, London Health Sciences Centre, Department of Family Medicine, Western
Five Things the Family Physician Needs to Know about Addiction and Harm Reduction Dr. Sharon Koivu Palliative Care Physician Consultant, London Health Sciences Centre, Department of Family Medicine, Western
OVERDOSE IN UTAH PREVENTION AND RESPONSE. Meghan Balough, MPH Heather Bush, B.S. Suicide Conference October 6, 2017
 OVERDOSE IN UTAH PREVENTION AND RESPONSE Meghan Balough, MPH Heather Bush, B.S. Suicide Conference October 6, 2017 Questions How many people have known someone who has experienced an overdose? How many
OVERDOSE IN UTAH PREVENTION AND RESPONSE Meghan Balough, MPH Heather Bush, B.S. Suicide Conference October 6, 2017 Questions How many people have known someone who has experienced an overdose? How many
NALOXONE: HEALTHCARE PROFESSIONALS TRAINING GUIDE FOR ADMINISTRATION AND DISPENSING
 NALOXONE: HEALTHCARE PROFESSIONALS TRAINING GUIDE FOR ADMINISTRATION AND DISPENSING Kaitlyn Bernard, PharmD PGY-1 Pharmacy Practice Resident November 18, 2017 Objectives Explain the impact of the opioid
NALOXONE: HEALTHCARE PROFESSIONALS TRAINING GUIDE FOR ADMINISTRATION AND DISPENSING Kaitlyn Bernard, PharmD PGY-1 Pharmacy Practice Resident November 18, 2017 Objectives Explain the impact of the opioid
Prescription Drug Misuse/Abuse in Seniors. April Rovero Founder/Executive Director
 Prescription Drug Misuse/Abuse in Seniors April Rovero Founder/Executive Director Deaths per 100,000 Population 30 25 Overdose Demographics Drug Poisoning Death Rates by Age: United States (2010) 20 15
Prescription Drug Misuse/Abuse in Seniors April Rovero Founder/Executive Director Deaths per 100,000 Population 30 25 Overdose Demographics Drug Poisoning Death Rates by Age: United States (2010) 20 15
Working with People Who Use Drugs in HIV Care Settings. August 29, 2017 Workshop C 2:00 3:30 p.m.
 Working with People Who Use Drugs in HIV Care Settings August 29, 2017 Workshop C 2:00 3:30 p.m. Working with People Who Use Drugs in HIV Care Settings Facilitator: Liz Hall, CDPH Office of AIDS Matt Curtis,
Working with People Who Use Drugs in HIV Care Settings August 29, 2017 Workshop C 2:00 3:30 p.m. Working with People Who Use Drugs in HIV Care Settings Facilitator: Liz Hall, CDPH Office of AIDS Matt Curtis,
some things you should know about opioids before starting a prescription an informational booklet for opioid pain treatment
 some things you should know about opioids before starting a prescription an informational booklet for opioid pain treatment This booklet was created to help you learn about opioids. You probably have lots
some things you should know about opioids before starting a prescription an informational booklet for opioid pain treatment This booklet was created to help you learn about opioids. You probably have lots
Opioid Use Disorder Treatment Initiation in Diverse Settings
 Opioid Use Disorder Treatment Initiation in Diverse Settings Sarah Wakeman, MD, FASAM Medical Director, Mass General Substance Use Disorder Initiative Assistant Professor, Harvard Medical School Disclosures
Opioid Use Disorder Treatment Initiation in Diverse Settings Sarah Wakeman, MD, FASAM Medical Director, Mass General Substance Use Disorder Initiative Assistant Professor, Harvard Medical School Disclosures
Potential Solutions to Epidemic Substance Abuse in US and Europe
 Potential Solutions to Epidemic Substance Abuse in US and Europe Richard C. Dart, MD, PhD Director, Rocky Mountain Poison and Drug Center, Denver Health 1 Professor, University of Colorado School of Medicine
Potential Solutions to Epidemic Substance Abuse in US and Europe Richard C. Dart, MD, PhD Director, Rocky Mountain Poison and Drug Center, Denver Health 1 Professor, University of Colorado School of Medicine
Naloxone Opioid Rescue Kits. Aaron Kochar, JD
 Naloxone Opioid Rescue Kits Aaron Kochar, JD Common Opioids Codeine Lorcet Demerol Vicodin Oxycontin Hydrocodone Methadone Used as a Medication- Assisted Treatment Liquid methadone (difficult to divert/abuse)
Naloxone Opioid Rescue Kits Aaron Kochar, JD Common Opioids Codeine Lorcet Demerol Vicodin Oxycontin Hydrocodone Methadone Used as a Medication- Assisted Treatment Liquid methadone (difficult to divert/abuse)
PREVENTING OPIATE OVERDOSES IN SCHOOLS. Head 2 Toe 2017 April 20, 2017 Winona Stoltzfus BSN, MD, School Health Officer and Acting RHO SE Region
 PREVENTING OPIATE OVERDOSES IN SCHOOLS Head 2 Toe 2017 April 20, 2017 Winona Stoltzfus BSN, MD, School Health Officer and Acting RHO SE Region WHY IS THIS EVEN A QUESTION FOR SCHOOLS? In 2014, 467,000
PREVENTING OPIATE OVERDOSES IN SCHOOLS Head 2 Toe 2017 April 20, 2017 Winona Stoltzfus BSN, MD, School Health Officer and Acting RHO SE Region WHY IS THIS EVEN A QUESTION FOR SCHOOLS? In 2014, 467,000
Prescribe to Prevent: Overdose Prevention and Naloxone Rescue Kits for Prescribers and Pharmacists. September 2016 TRANSCRIPT
 Prescribe to Prevent: Overdose Prevention and Naloxone Rescue Kits for Prescribers and Pharmacists September 2016 TRANSCRIPT Prescribe to Prevent Title Slide Welcome to Prescribe to Prevent: Overdose Prevention
Prescribe to Prevent: Overdose Prevention and Naloxone Rescue Kits for Prescribers and Pharmacists September 2016 TRANSCRIPT Prescribe to Prevent Title Slide Welcome to Prescribe to Prevent: Overdose Prevention
Carol Strike, PhD & Tara Marie Watson, PhD and the Working Group on Best Practice for Harm Reduction Programs in Canada
 Carol Strike, PhD & Tara Marie Watson, PhD and the Working Group on Best Practice for Harm Reduction Programs in Canada Project goals and methods Reduce transmission of HIV and STBBI Improve the quality,
Carol Strike, PhD & Tara Marie Watson, PhD and the Working Group on Best Practice for Harm Reduction Programs in Canada Project goals and methods Reduce transmission of HIV and STBBI Improve the quality,
Massachusetts Department of Public Health Opioid Overdose Education and Naloxone Distribution. MDPH Naloxone pilot project Core Competencies
 Massachusetts Department of Public Health Opioid Overdose Education and Naloxone Distribution MDPH Naloxone pilot project Core Competencies Acknowledgements: Thank you to the Boston Public Health Commission
Massachusetts Department of Public Health Opioid Overdose Education and Naloxone Distribution MDPH Naloxone pilot project Core Competencies Acknowledgements: Thank you to the Boston Public Health Commission
Opioid Overdose Education and Naloxone Distribution
 Opioid Overdose Education and Naloxone Distribution Emily Stoukides, PharmD PGY-2 Ambulatory Care Pharmacy Resident Nicole Brunet, PharmD, BCPP Clinical Pharmacy Specialist, Mental Health Disclosures Emily
Opioid Overdose Education and Naloxone Distribution Emily Stoukides, PharmD PGY-2 Ambulatory Care Pharmacy Resident Nicole Brunet, PharmD, BCPP Clinical Pharmacy Specialist, Mental Health Disclosures Emily
Trends and Challenges: The Kentucky Opioid Crisis. Jason Smith, MD PhD University of Louisville
 Trends and Challenges: The Kentucky Opioid Crisis Jason Smith, MD PhD University of Louisville Brief Introduction I am by no means an expert I have no financial disclosures Jokes are meant to be lighthearted
Trends and Challenges: The Kentucky Opioid Crisis Jason Smith, MD PhD University of Louisville Brief Introduction I am by no means an expert I have no financial disclosures Jokes are meant to be lighthearted
Naloxone Statewide Standing Order. Cheryl A. Viracola, PharmD Pharmacy Programs Manager, Community Care of Wake and Johnston Counties
 Naloxone Statewide Standing Order Cheryl A. Viracola, PharmD Pharmacy Programs Manager, Community Care of Wake and Johnston Counties Objectives Review the US & NC trends on opioid overdose Understand key
Naloxone Statewide Standing Order Cheryl A. Viracola, PharmD Pharmacy Programs Manager, Community Care of Wake and Johnston Counties Objectives Review the US & NC trends on opioid overdose Understand key
The Unseen Consequences of Prescription Drug Abuse. Stephen Loyd, M.D.
 The Unseen Consequences of Prescription Drug Abuse Stephen Loyd, M.D. Stephen Loyd, M.D. Receives no commercial support, in any form, from pharmaceutical companies or anyone else Medical Director for Substance
The Unseen Consequences of Prescription Drug Abuse Stephen Loyd, M.D. Stephen Loyd, M.D. Receives no commercial support, in any form, from pharmaceutical companies or anyone else Medical Director for Substance
Opioid Safety: Prescribing Guidelines, Quality Measures and Care Coordination Best-Practices
 Opioid Safety: Prescribing Guidelines, Quality Measures and Care Coordination Best-Practices August 25, 2017 Presented by Michael Crooks, PharmD. Medication Safety and Care Coordination Task Lead 8/28/2017
Opioid Safety: Prescribing Guidelines, Quality Measures and Care Coordination Best-Practices August 25, 2017 Presented by Michael Crooks, PharmD. Medication Safety and Care Coordination Task Lead 8/28/2017
October 20, 2016 Scott K. Proescholdbell, MPH. Opioid Overdose and North Carolina s Public Health and Prevention Strategies
 October 20, 2016 Scott K. Proescholdbell, MPH Opioid Overdose and North Carolina s Public Health and Prevention Strategies Deaths per 100,000 population Death Rates* for Three Selected Causes of Injury,
October 20, 2016 Scott K. Proescholdbell, MPH Opioid Overdose and North Carolina s Public Health and Prevention Strategies Deaths per 100,000 population Death Rates* for Three Selected Causes of Injury,
Community Pharmacy Distribution of Naloxone
 Community Pharmacy Distribution of Naloxone College of Pharmacists of BC BC Centre for Disease Control Harm Reduction Program Sponsored in part by the BC Ministry of Health What is Naloxone? Naloxone is
Community Pharmacy Distribution of Naloxone College of Pharmacists of BC BC Centre for Disease Control Harm Reduction Program Sponsored in part by the BC Ministry of Health What is Naloxone? Naloxone is
RESIDENTIAL SUBSTANCE ABUSE TREATMENT (RSAT)
") RESIDENTIAL SUBSTANCE ABUSE TREATMENT (RSAT) Overdose Risk Reduction and Relapse Prevention This project was supported by grant No. 2016-MU-BX-K021 awarded by the Bureau of Justice Assistance. The Bureau
RESIDENTIAL SUBSTANCE ABUSE TREATMENT (RSAT) Overdose Risk Reduction and Relapse Prevention This project was supported by grant No. 2016-MU-BX-K021 awarded by the Bureau of Justice Assistance. The Bureau
Naloxone for Emergency Administration: A 2017 Update On FDA Guidance
 Naloxone for Emergency Administration: A 2017 Update On FDA Guidance Nathan A. Painter, PharmD, CDE Associate Clinical Professor University of California San Diego Skaggs School of Pharmacy and Pharmaceutical
Naloxone for Emergency Administration: A 2017 Update On FDA Guidance Nathan A. Painter, PharmD, CDE Associate Clinical Professor University of California San Diego Skaggs School of Pharmacy and Pharmaceutical
High-Decile Prescribers: All Gain, No Pain?
 High-Decile Prescribers: All Gain, No Pain? Len Paulozzi, MD, MPH National Center for Injury Prevention and Control Centers for Disease Control and Prevention National Center for Injury Prevention and
High-Decile Prescribers: All Gain, No Pain? Len Paulozzi, MD, MPH National Center for Injury Prevention and Control Centers for Disease Control and Prevention National Center for Injury Prevention and
Opiate Use Disorder and Opiate Overdose
 Opiate Use Disorder and Opiate Overdose Irene Ortiz, MD Medical Director Molina Healthcare of New Mexico and South Carolina Clinical Professor University of New Mexico School of Medicine Objectives DSM-5
Opiate Use Disorder and Opiate Overdose Irene Ortiz, MD Medical Director Molina Healthcare of New Mexico and South Carolina Clinical Professor University of New Mexico School of Medicine Objectives DSM-5
HARM REDUCTION & TREATMENT. Devin Reaves MSW
 HARM REDUCTION & TREATMENT Devin Reaves MSW The mission of PAHRC is to promote the health, dignity, and human rights of individuals who use drugs and communities impacted by drug use. Recognizing that
HARM REDUCTION & TREATMENT Devin Reaves MSW The mission of PAHRC is to promote the health, dignity, and human rights of individuals who use drugs and communities impacted by drug use. Recognizing that
Welcome to the Opioid Overdose Prevention Project
 Welcome to the Opioid Overdose Prevention Project Narcan Training TODAY S OBJECTIVES Define drug addiction Identify symptoms of addiction Treatment options including support for family members How to recognize
Welcome to the Opioid Overdose Prevention Project Narcan Training TODAY S OBJECTIVES Define drug addiction Identify symptoms of addiction Treatment options including support for family members How to recognize
The Missouri Opioid-Heroin Overdose Prevention and Education (MO-HOPE) Project Mission: to reduce opioid overdose deaths in Missouri through expanded
 Project Mission: to reduce opioid overdose deaths in Missouri through expanded") The Missouri Opioid-Heroin Overdose Prevention and Education (MO-HOPE) Project Mission: to reduce opioid overdose deaths in Missouri through expanded access to naloxone, overdose education, prevention,
The Missouri Opioid-Heroin Overdose Prevention and Education (MO-HOPE) Project Mission: to reduce opioid overdose deaths in Missouri through expanded access to naloxone, overdose education, prevention,
Braintree Public Schools
 Braintree Public Schools Policy and Procedures for School Nurse, Athletic Director and Athletic Trainer Management of Potential Life Threatening Opioid Overdose Program Policy In order to recognize and
Braintree Public Schools Policy and Procedures for School Nurse, Athletic Director and Athletic Trainer Management of Potential Life Threatening Opioid Overdose Program Policy In order to recognize and
GOALS AND OBJECTIVES
 SUBOXONE AND VIVITROL: ARE THERE DISPARITIES SURFACING IN MEDICATION ASSISTED TREATMENTS? P R E S E N T E D B Y D R. K I AM E M AH A N I A H & D R. M Y E C H I A M I N T E R - J O R D AN GOALS AND OBJECTIVES
SUBOXONE AND VIVITROL: ARE THERE DISPARITIES SURFACING IN MEDICATION ASSISTED TREATMENTS? P R E S E N T E D B Y D R. K I AM E M AH A N I A H & D R. M Y E C H I A M I N T E R - J O R D AN GOALS AND OBJECTIVES
Chad Sabora, BS, MS, JD Missouri Network for Opiate Reform and Recovery. Drug Policy, Harm Reduction, and What s Next
 Chad Sabora, BS, MS, JD Missouri Network for Opiate Reform and Recovery Drug Policy, Harm Reduction, and What s Next The start or lack thereof of Drug Policy in the United States The Harrison Narcotics
Chad Sabora, BS, MS, JD Missouri Network for Opiate Reform and Recovery Drug Policy, Harm Reduction, and What s Next The start or lack thereof of Drug Policy in the United States The Harrison Narcotics
Opioid Overdose Prevention for Law Enforcement and First Responders. Sponsored by the NC Office of EMS
 Opioid Overdose Prevention for Law Enforcement and First Responders Sponsored by the NC Office of EMS Overview The goal of this presentation is to help inform the public safety community of North Carolina
Opioid Overdose Prevention for Law Enforcement and First Responders Sponsored by the NC Office of EMS Overview The goal of this presentation is to help inform the public safety community of North Carolina
Oregon s PDMP: An epidemiological assist tool
 Oregon s PDMP: An epidemiological assist tool Todd Beran Center for Prevention and Health Promotion Oregon Health Authority PDMP TTAC Webinar February 13, 2013 1 Acknowledgements Lisa Millet, MSH, Section
Oregon s PDMP: An epidemiological assist tool Todd Beran Center for Prevention and Health Promotion Oregon Health Authority PDMP TTAC Webinar February 13, 2013 1 Acknowledgements Lisa Millet, MSH, Section
Opioids Research to Practice
 Opioids Research to Practice CRIT Program May 2009 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Opioids Research to Practice CRIT Program May 2009 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
1/23/2015. Disclosure. Overview. A National Response to a Public Health Crisis Opioid Overdose and the Changing Spectrum of Care
 A National Response to a Public Health Crisis Opioid Overdose and the Changing Spectrum of Care Michael W. Dailey, MD FACEP Chief, Division of Prehospital and Operational Medicine Associate Professor of
A National Response to a Public Health Crisis Opioid Overdose and the Changing Spectrum of Care Michael W. Dailey, MD FACEP Chief, Division of Prehospital and Operational Medicine Associate Professor of
9/5/2011. Outline. 1. Past and Current Trends re: RX Abuse 2. Diversion Methods 3. Regulatory Reporting Requirements 4. Q/A
 Prescription Drug Abuse Crises Outline 1. Past and Current Trends re: RX Abuse 2. Diversion Methods 3. Regulatory Reporting Requirements 4. Q/A 1 1970s 1980s 2 The 1990s OXYCODONE Oxycodone/APAP OxyContin
Prescription Drug Abuse Crises Outline 1. Past and Current Trends re: RX Abuse 2. Diversion Methods 3. Regulatory Reporting Requirements 4. Q/A 1 1970s 1980s 2 The 1990s OXYCODONE Oxycodone/APAP OxyContin
Journal Club: Naloxone Programs in the Community and Their Success to Decrease Overdoses from Opioids
 Journal Club: Naloxone Programs in the Community and Their Success to Decrease Overdoses from Opioids Emily Junck, MD Hayes Wong, MD Paul Freeman, MD Special Guest: Caleb Banta-Green, PhD, MPH, MSW Special
Journal Club: Naloxone Programs in the Community and Their Success to Decrease Overdoses from Opioids Emily Junck, MD Hayes Wong, MD Paul Freeman, MD Special Guest: Caleb Banta-Green, PhD, MPH, MSW Special
Buprenorphine: An Introduction. Sharon Stancliff, MD Harm Reduction Coalition September 2008
 Buprenorphine: An Introduction Sharon Stancliff, MD Harm Reduction Coalition September 2008 Objective Participants will be able to: Discuss the role of opioid maintenance in reducing morbidity and mortality
Buprenorphine: An Introduction Sharon Stancliff, MD Harm Reduction Coalition September 2008 Objective Participants will be able to: Discuss the role of opioid maintenance in reducing morbidity and mortality
April 26, New Mexico Board of Pharmacy Prescription Monitoring Program (PMP) New Mexico Board of Pharmacy Prescription Monitoring Program (PMP)
 New Mexico Board of Pharmacy Prescription Monitoring Program (PMP)") New Mexico Board of Pharmacy Prescription Monitoring Program (PMP) New Mexico Nurse Practitioner Council New Mexico Board of Pharmacy Prescription Monitoring Program (PMP) Peter Ryba, PharmD PMP Director
New Mexico Board of Pharmacy Prescription Monitoring Program (PMP) New Mexico Nurse Practitioner Council New Mexico Board of Pharmacy Prescription Monitoring Program (PMP) Peter Ryba, PharmD PMP Director
Implementing the 2017 President s Challenge: Primary, Secondary & Tertiary Prevention of Addiction & Substance Misuse
 Implementing the 2017 President s Challenge: Primary, Secondary & Tertiary Prevention of Addiction & Substance Misuse Jay Butler, MD, President of ASTHO, Chief Medical Officer, Alaska Department of Health
Implementing the 2017 President s Challenge: Primary, Secondary & Tertiary Prevention of Addiction & Substance Misuse Jay Butler, MD, President of ASTHO, Chief Medical Officer, Alaska Department of Health
Patient Care Planning Group April 3, 2014
 Patient Care Planning Group April 3, 2014 Philip O. Toal, Ed.D,; LMHC, CET Administrator, Non-Residential Services The Center For Drug Free Living, a founding partner of Aspire Health Partners Participants
Patient Care Planning Group April 3, 2014 Philip O. Toal, Ed.D,; LMHC, CET Administrator, Non-Residential Services The Center For Drug Free Living, a founding partner of Aspire Health Partners Participants
Naloxone: What You Need to Know About Overdose Reversal In the Midst of an Opioid Epidemic
 Naloxone: What You Need to Know About Overdose Reversal In the Midst of an Opioid Epidemic Kyle Troksa, Pharm.D., AE-C PGY1 Resident Community Medical Center March 4th, 2018 Conflicts of Interest No conflicts
Naloxone: What You Need to Know About Overdose Reversal In the Midst of an Opioid Epidemic Kyle Troksa, Pharm.D., AE-C PGY1 Resident Community Medical Center March 4th, 2018 Conflicts of Interest No conflicts
Harm Reduction and Medical Respite (Dead People Don t Recover) Alice Moughamian, RN,CNS Dave Munson MD
 Alice Moughamian, RN,CNS Dave Munson MD") Harm Reduction and Medical Respite (Dead People Don t Recover) Alice Moughamian, RN,CNS Dave Munson MD Objectives Provide an overview of harm reduction by defining shared language and key terms. Collaboratively
Harm Reduction and Medical Respite (Dead People Don t Recover) Alice Moughamian, RN,CNS Dave Munson MD Objectives Provide an overview of harm reduction by defining shared language and key terms. Collaboratively
Take Home Naloxone elearning Module Script
 elearning Module Script Slide 1-3 Review the outline and the plan for the presentation. Slide 4 We do accept the cynicism of this poster. Slide 5 Read from the slide the definition of Harm Reduction Slide
elearning Module Script Slide 1-3 Review the outline and the plan for the presentation. Slide 4 We do accept the cynicism of this poster. Slide 5 Read from the slide the definition of Harm Reduction Slide
Drug Use and Young People. Long Island Council on Alcoholism and Drug Dependence, Inc. LICADD
 Drug Use and Young People Long Island Council on Alcoholism and Drug Dependence, Inc. LICADD 516-747-2606 631-979-1700 1-800-585-5422 www.licadd.org Not necessarily a new problem, nor unique to Long Island.
Drug Use and Young People Long Island Council on Alcoholism and Drug Dependence, Inc. LICADD 516-747-2606 631-979-1700 1-800-585-5422 www.licadd.org Not necessarily a new problem, nor unique to Long Island.
Calvert County Health Department Overdose Education and Naloxone Training
 Calvert County Health Department Overdose Education and Naloxone Training Maryland Overdose Response Program January 2015 Behavioral Health Administration Department of Health & Mental Hygiene dhmh.naloxone@maryland.gov
Calvert County Health Department Overdose Education and Naloxone Training Maryland Overdose Response Program January 2015 Behavioral Health Administration Department of Health & Mental Hygiene dhmh.naloxone@maryland.gov
Wasted AN INTRODUCTION TO SUBSTANCE ABUSE
 Wasted AN INTRODUCTION TO SUBSTANCE ABUSE Dr. Brian L. Bethel Child and Family Therapist Independent Trainer and Consultant LPCC-S, LCDC III, RPT-S www.brianlbethel.com INTERPLAY COUNSELING & CONSULTING
Wasted AN INTRODUCTION TO SUBSTANCE ABUSE Dr. Brian L. Bethel Child and Family Therapist Independent Trainer and Consultant LPCC-S, LCDC III, RPT-S www.brianlbethel.com INTERPLAY COUNSELING & CONSULTING
Presenters. Session Objectives. Session Overview. Cluster Investigations in Rural Wisconsin
 Public Health Nurses, Hepatitis C, Injection Drug Use and Heroin Sheila Guilfoyle Viral Hepatitis Prevention Coordinator Division of Public Health Wisconsin Department of Health Services Wisconsin Public
Public Health Nurses, Hepatitis C, Injection Drug Use and Heroin Sheila Guilfoyle Viral Hepatitis Prevention Coordinator Division of Public Health Wisconsin Department of Health Services Wisconsin Public
Opioids 101. Washington Prevention Summit. Alison Newman, MPH November 6, 2018
 Opioids 101 Washington Prevention Summit Alison Newman, MPH November 6, 2018 Opioids Class of drugs that work on the endorphin system. What are some examples? What are some of the risks? Opioid use disorder
Opioids 101 Washington Prevention Summit Alison Newman, MPH November 6, 2018 Opioids Class of drugs that work on the endorphin system. What are some examples? What are some of the risks? Opioid use disorder
Law Enforcement Naloxone Training Florida Department of Children and Families. Office of Substance Abuse and Mental Health
 Protecting, Leading, Uniting Since 1893 Law Enforcement Naloxone Training Florida Department of Children and Families Office of Substance Abuse and Mental Health 1. Learn how to recognize and respond to
Protecting, Leading, Uniting Since 1893 Law Enforcement Naloxone Training Florida Department of Children and Families Office of Substance Abuse and Mental Health 1. Learn how to recognize and respond to
People inject, sniff, snort, or smoke heroin. Some people mix heroin with crack cocaine, a practice called speedballing.
 What is heroin? Heroin is an opioid drug made from morphine, a natural substance taken from the seed pod of the various opium poppy plants grown in Southeast and Southwest Asia, Mexico, and Colombia. Heroin
What is heroin? Heroin is an opioid drug made from morphine, a natural substance taken from the seed pod of the various opium poppy plants grown in Southeast and Southwest Asia, Mexico, and Colombia. Heroin
Kentucky All Schedule Prescription Electronic Reporting (KASPER)
") Kentucky All Schedule Prescription Electronic Reporting (KASPER) Phyllis Millspaugh Manager, Behavioral Health Prevention and Promotion Kentucky Cabinet for Health and Family Services Using PDMP Data to
Kentucky All Schedule Prescription Electronic Reporting (KASPER) Phyllis Millspaugh Manager, Behavioral Health Prevention and Promotion Kentucky Cabinet for Health and Family Services Using PDMP Data to
Identification of Specific Drugs and Drug Diversion in Drug Overdose Fatalities
 Identification of Specific Drugs and Drug Diversion in Drug Overdose Fatalities Svetla Slavova, PhD Sara LaMantia, MS Terry Bunn, PhD Tracey Corey, MD 2016 Safe States Annual Meeting April 13, 2016, Albuquerque,
Identification of Specific Drugs and Drug Diversion in Drug Overdose Fatalities Svetla Slavova, PhD Sara LaMantia, MS Terry Bunn, PhD Tracey Corey, MD 2016 Safe States Annual Meeting April 13, 2016, Albuquerque,
OPIOID SAFE- PRESCRIBING TRAINING IMMERSION (OSTI)
") OPIOID SAFE- PRESCRIBING TRAINING IMMERSION (OSTI) Case 105- Prep Materials University of Massachusetts Medical School Opioid Conscious Curriculum Learner Prep Objectives The purpose of this prep material
OPIOID SAFE- PRESCRIBING TRAINING IMMERSION (OSTI) Case 105- Prep Materials University of Massachusetts Medical School Opioid Conscious Curriculum Learner Prep Objectives The purpose of this prep material
OHIO S PRESCRIPTION DRUG OVERDOSE EPIDEMIC:
 Cuyahoga County Board of Health OHIO S PRESCRIPTION DRUG OVERDOSE EPIDEMIC: NOVEMBER 5, 2014 CONTRIBUTING FACTORS AND ONGOING PREVENTION EFFORTS DEFINITIONS Opiate- originate from naturally-occurring elements
Cuyahoga County Board of Health OHIO S PRESCRIPTION DRUG OVERDOSE EPIDEMIC: NOVEMBER 5, 2014 CONTRIBUTING FACTORS AND ONGOING PREVENTION EFFORTS DEFINITIONS Opiate- originate from naturally-occurring elements
COUNTY OF SAN DIEGO. Opioid Update
 COUNTY OF SAN DIEGO Opioid Update Linda Bridgeman Smith, DUI & Prevention Services Manager Health & Human Services Agency, Behavioral Health Services Co-chair, Prescription Drug Abuse Task Force 1 HEADLINES
COUNTY OF SAN DIEGO Opioid Update Linda Bridgeman Smith, DUI & Prevention Services Manager Health & Human Services Agency, Behavioral Health Services Co-chair, Prescription Drug Abuse Task Force 1 HEADLINES
DISPENSING OR SELLING NALOXONE. Guidance for pharmacy professionals when dispensing or selling naloxone as a Schedule II drug.
 DISPENSING OR SELLING NALOXONE Guidance for pharmacy professionals when dispensing or selling naloxone as a Schedule II drug. UPDATED ON: April 21, 2017 Purpose The intent of this document is to provide
DISPENSING OR SELLING NALOXONE Guidance for pharmacy professionals when dispensing or selling naloxone as a Schedule II drug. UPDATED ON: April 21, 2017 Purpose The intent of this document is to provide
Harm Reduction Coalition DOPE Project Eliza Wheeler 1440 Broadway Suite 902 Oakland, CA
 Harm Reduction Coalition DOPE Project Eliza Wheeler 1440 Broadway Suite 902 Oakland, CA 94612 wheeler@harmreduction.org Drug Overdose Deaths in the US: In 2014, there were 47,055 drug overdose deaths in
Harm Reduction Coalition DOPE Project Eliza Wheeler 1440 Broadway Suite 902 Oakland, CA 94612 wheeler@harmreduction.org Drug Overdose Deaths in the US: In 2014, there were 47,055 drug overdose deaths in
Linking Opioid Treatment in Primary Care. Roxanne Lewin M.D.
 Roxanne Lewin M.D. The Facts Fewer than 10 percent of individuals with an alcohol use disorder and only about 20 percent of individuals with an opioid use disorder receive specialty treatment. Many individuals
Roxanne Lewin M.D. The Facts Fewer than 10 percent of individuals with an alcohol use disorder and only about 20 percent of individuals with an opioid use disorder receive specialty treatment. Many individuals
Opioids - Fentanyl - Naloxone. Public Health Nurse
 Opioids - Fentanyl - Naloxone Public Health Nurse What are Opioids? Opioids are a family of drugs that treat pain and can cause sleepiness. Prescription (legal) Opioids fall into 3 main categories: 1.
Opioids - Fentanyl - Naloxone Public Health Nurse What are Opioids? Opioids are a family of drugs that treat pain and can cause sleepiness. Prescription (legal) Opioids fall into 3 main categories: 1.
Pragmatic and Creative Responses to the Opioid Crisis in Connecticut
 Focusing on Highly Vulnerable Populations Track Pragmatic and Creative Responses to the Opioid Crisis in Connecticut A special thanks to our presenting sponsor: Presenters: Shawn Lang Deputy Director AIDS
Focusing on Highly Vulnerable Populations Track Pragmatic and Creative Responses to the Opioid Crisis in Connecticut A special thanks to our presenting sponsor: Presenters: Shawn Lang Deputy Director AIDS
Steve Alsum. The Grand Rapids Red Project (616)
") Steve Alsum The Grand Rapids Red Project steve@redprojectgr.org (616) 456-9063 Red Project: Mission/History/Programs Epidemiology of Overdose Overdose Prevention in Grand Rapids National Efforts Moving
Steve Alsum The Grand Rapids Red Project steve@redprojectgr.org (616) 456-9063 Red Project: Mission/History/Programs Epidemiology of Overdose Overdose Prevention in Grand Rapids National Efforts Moving
OPIOID USE DISORDER AND THE PSYCHIATRIC EMERGENCY ROOM THE VA CT MODEL
 OPIOID USE DISORDER AND THE PSYCHIATRIC EMERGENCY ROOM THE VA CT MODEL Brian Fuehrlein, MD PhD VA Connecticut Healthcare System and Yale University I have no conflicts of interest or relevant financial
OPIOID USE DISORDER AND THE PSYCHIATRIC EMERGENCY ROOM THE VA CT MODEL Brian Fuehrlein, MD PhD VA Connecticut Healthcare System and Yale University I have no conflicts of interest or relevant financial
Arwen Podesta, MD. ABIHM, ABAM, Forensic Psychiatry
 The State of Medicine in Addiction Recovery Arwen Podesta, MD ABIHM, ABAM, Forensic Psychiatry www.podestawellness.com 504-252-0026 http://www.addictionpolicy.org/ Overview Addiction is a serious, chronic
The State of Medicine in Addiction Recovery Arwen Podesta, MD ABIHM, ABAM, Forensic Psychiatry www.podestawellness.com 504-252-0026 http://www.addictionpolicy.org/ Overview Addiction is a serious, chronic
Needle and syringe distribution
 Needle and syringe distribution facilitate use of a sterile needle and syringe for each injection and reduce transmission of human immunodeficiency virus (HIV), hepatitis C (HCV), hepatitis B (HBV), and
Needle and syringe distribution facilitate use of a sterile needle and syringe for each injection and reduce transmission of human immunodeficiency virus (HIV), hepatitis C (HCV), hepatitis B (HBV), and
Annual Reports Questionnaire (ARQ) Part III: Extent, patterns and trends in drug use
 Part III: Extent, patterns and trends in drug use") Annual Reports Questionnaire (ARQ) Part III: Extent, patterns and trends in drug use Report of the Government of: Reporting Year: Completed on (date): Please return completed questionnaire to: arq@unodc.org
Annual Reports Questionnaire (ARQ) Part III: Extent, patterns and trends in drug use Report of the Government of: Reporting Year: Completed on (date): Please return completed questionnaire to: arq@unodc.org