Mikhail Alper, PA-C California Gastroenterology Associates Fresno/Madera, CA. Dr. Robert Gish Dr. Sammy Saab Dr. Naeem Akhtar
|
|
|
- Elizabeth Hill
- 5 years ago
- Views:
Transcription



1 Mikhail Alper, PA-C California Gastroenterology Associates Fresno/Madera, CA Dr. Robert Gish Dr. Sammy Saab Dr. Naeem Akhtar 1
2 AST, ALT Alkaline Phosphatase GGT Bilirubin Albumin Protime/INR True liver function tests Also: Lactate, glucose, cholesterol, clotting factors Ammonia very poor liver function test, poor correlation with HE status Aspartate aminotransferase, alanine aminotransferase Enzymes that are in the hepatocyte and function during gluconeogenesis Leak out of the hepatocytes in times of injury and can be measured in the serum Normally present in serum at levels ~20-30 U/L <30 for men <20 for women 2
3 AST: liver > cardiac muscle > skeletal muscle > kidney > brain > pancreas > lung > leukocytes > erythrocytes Less specific for liver damage Can increase with strenuous exercise, MI Located in cytosol and mitochondria of hepatocytes Cleared more rapidly than ALT ALT Mainly from cytosol of hepatocytes more specific for liver damage Exists in liver in membrane of hepatocyte where it lines the canaliculus Liver > bone > intestine Placenta Normally changes with age
4 GGT: gamma-glutamyltransferase Found in hepatocytes and biliary epithelial cells 5 nucleotidase Both these enzymes can be used to confirm alk phos elevation is coming from liver GGT is also sensitive to alcohol ingestion Breakdown product of heme 70-80% of normal production is from breakdown of hemoglobin in senescent RBC Conjugation of bilirubin occurs in ER of hepatocyte, and conjugated bilirubin is then transported into bile (rate limiting step) Almost 100% of bilirubin in healthy people is indirect 4
5 Increased bilirubin can occur from: Overproduction of bilirubin Uncomplicated hemolysis (rarely levels >5 mg/dl) Impaired uptake, conjugation, or excretion Gilbert Syndrome, others Blockage of bile duct Regurgitation from damaged hepatocytes of bile ducts Hepatocellular damage Urinary bilirubin is only conjugated Important plasma protein synthesized by the liver Half-life 20 days Levels <3.5 mg/dl should raise the suspicion of chronic liver disease or inflammatory disease ***not specific for liver disease Also reduced in heavy alcohol consumption, chronic inflammation, protein malnutrition 5
6 Liver synthesizes all major coagulation proteins: I, II, V, VII, IX, X, XII, XII Protime measured II, VII, IX, X: vitamin K dependent factors Can be elevated in liver disease or Vitamin K deficiency *** one of the most important abnormalities to signify development of fulminant hepatic failure in course of acute liver disease, with bilirubin and encephalopathy Degree of elevation is a prognostic factor in many liver diseases Men>30 Women >20 6
7 Population based survey in US estimated abnormal ALT in 8.9% of population Symptomatic vs Asymptomatic? Acute vs Chronic? Hepatitic vs Cholestatic? Hepatitic: Viral Hepatitis: A, B, C, D, E Alcoholic and Nonalcoholic Steatohepatitis Autoimmune Hemochromatosis Wilson s disease Alpha-1 antitrypsin defficiency Cholestatic: Obstruction Gallstones, malignancy, parasites Primary Biliary Cirrhosis Primary Sclerosing Cholangitis Infiltrative diseases: metastatic cancer, sarcoidosis, amyloidosis Either: Drugs Thyroid disorders Celiac disease Vascular disease: CHF, Budd Chiari syndrome, Sinusoidal obstructive syndrome 7
8 First step is to repeat the test!! Many things can cause a one-time elevation of liver tests Mild elevations should be monitored for at least 6 months before a full serologic work-up is done Exception is viral hepatitis serologies in high risk people Think of situations where a high test is normal Alkaline phosphatase in pregnancy AST in marathon runners History How long has elevation been present? Any symptoms: pruritus, fatigue, RUQ pain, arthralgias, myalgias, rash, anorexia, fever, weight loss, changes in urine/stool Symptoms of more severe liver disease: jaundice, ascites, LE edema, GI bleeding, confusion or slowed thinking Other Medical Problems? Family history of liver disease? Personal or family history of autoimmune disease or thyroid disease? 8
9 What medications do you take? When did you start them? Any change in doses? Over the counter medications? Herbals? ask specifically!! How much do you drink? be specific!!! Any recent travel? Born abroad? Have you had any blood transfusions? Have you ever had hemodialysis? Do you work in healthcare? Any needlesticks? Any tattoos? Have you ever injected drugs, even once? Have you ever snorted drugs, even once? Any recent mushroom ingestion? Any unprotected sex? Multiple sex partners? Are you a Vietnam veteran? 9
10 Look for signs of chronic liver disease Spider angiomata Firm liver edge Splenomegaly Leukonychia Ascites LE edema Abdominal wall collateral vessels Proximal and temporal muscle wasting Look for signs of other diseases: acanthosis nigricans, signs of thyroid disease, xanthomas, etc Check cardiac exam for JVD, hepatojugular reflex Most of the time, with the history and physical you should have a good idea what s the likely culprit of the elevated liver tests! 10
11 54 year old woman came for routine screening colonoscopy No significant PMH On no medications Tattoo on the left hand ( I have it since age 16 ) PE normal I told her that tattoo is the risk factor for HCV Hepatitis C: Antibody positive What now? Check HCV RNA, genotype HCV GT 1A, Viral load is >1mln IU/ML Liver Bx stage 3 fibrosis ALT 47, AST 27, CBC, INR, Albumin, Bili normal other viral serologies are negative HAV Ab total+, HBVsAb+ 11
12 HCV Ab (hepatitis C antibody) (+) in chronic or previous infection Sensitive screening test with elevated ALT or age or history of blood exposure Detectable 8-16 weeks after exposure to virus False positives in autoimmune diseases or hypergammaglobulinemia False negatives in immunosuppressed CDC guidelines to screen baby boomers born One time HCV Ab test Code V
13 Presents for routine screening colonoscopy PMH: unremarkable Social: no Hx of drug use Born in China, math professor at local college Family history: unremarkable PE: normal Have you ever been screened for HBV? His answer is no Hepatitis B s Ag: positive HBsAb: negative HBcAb: positive HBVcAb IgM negative What now? HBV DNA 1.5 billion IU/mL, HBeAg pos, anti- HBe neg, Genotype C, HDV Ab- Diagnosis? Chronic Hepatitis B 13
14 Labs: CBC normal except low platelets 45 Pt has cirrhosis BMP normal AST 36, ALT 33, Alk. phos 70, T.bili 0.5 INR, Albumin normal US and AFP normal What now? EGD grade 3 esophageal varices Next step EGD with banding Start patient on antiviral Tx indefinitely Refer to liver transplant center for evaluation 14
15 HBsAg Prevalence (%) 350 million chronic carriers worldwide Ninth leading cause of death Nearly 75% of HBV chronic carriers are Asian 8: High 2-7: Intermediate <2: Low HBsAg HBsAb HBcAb HBV DNA IgM IgG Interpretation Acute infection Chronic infection Immunized Past Exposure False pos or Past Exp 15
16 HBe Ag: only applicable in patients who are chronically infected or carriers Positive: increased infectivity Negative: precore mutant of virus if DNA positive, still can be infective, still has advancing disease Levels of HBV DNA are important to decide if patient needs Tx (with elevated ALT level) Who should be treated? Active Inactive Immunetolerant Viral Load High Low High ALT Elevated Normal Normal Action Treat Observe Observe Periodic Screening for Hepatocellular Carcinoma NEVER D/C HBV Tx of a Cirrhotic patient 16
17 c/o severe fatigue of new onset, jaundice, mild pruritus of few days duration PMHx DM1 Dx at age 9, Acne No ETOH Meds: minocycline started 4 weeks ago, Insulin No Hx of contacts with viral hepatitis, travel PE: heent: mild scleral icterus abd: nl bs, no organomegaly, no tenderness or palpable mass I got a call from her DM1 M.D. to see her today for very high LFT Labs: alb 4.2, t. bili 10.2, alk phos 246, INR 0.9, PT normal AST 1180, ALT 1252; CBC normal, BMP normal Acute viral hepatitis serologies neg. AIH/PBH negative as well as the rest of liver w/up What is the most likely diagnosis? 17
18 Drug induced cholestasis secondary to minocycline. Symptoms resolved within 2 weeks of drug d/c, liver profile normalized in 10 weeks. 18
19 A note: acetaminophen is the most common cause of DILI, and also the most common cause of acute liver failure in US Normal dose for acetaminophen toxicity is 6 to12 grams/d, but toxicity can occur in much lower doses in certain circumstances, 2 gm/d Alcohol use Fasting state Presents with fatigue, myalgias PMH: hypothyroidism, HTN Meds: Synthroid, Atenolol, MVI, Ca Soc: married, no ETOH FHx: father with vitiligo PE: appears fatigued, Abd with mild RUQ tenderness to deep palpation 19
20 CBC, BMP normal AST 345, ALT 480, TBili 2.0, Alk phos 207 Alb 3.8, INR 1.0 US: mild hepatomegaly, otherwise normal Differential diagnosis? What further labs? ANA >1:1280 F-actin >1:320 Quantitative Ig: Elevated IgG Viral Markers, AMA negative, IgM normal Diagnosis: Bx confirmed (plasma cells) Autoimmune Hepatitis 20
21 Middle-aged (or teenage) woman, nondrinker without viral hepatitis Fatigue, arthralgias/myalgias, oligomenorrhea, jaundice Increased AST/ALT, gamma globulins Positive ANA and SMA Interface hepatitis with lymphoplasmacytic infiltrate Responds to corticosteroids Tx immunosuppressive meds Presents with new onset diabetes, found to have elevated LTs PMH: DM II newly diagnosed, OA in hips FH: liver disease? Soc: drinks 3 beers/day, no drug use PE: normal 21
22 CBC, BMP normal AST 65, ALT 80, Alk phos 125, TBili 0.6 Alb 3.6, INR 1.0 US: increased echogenicity of the liver Differential? Tests? Fe % sat 75%, Ferritin 1200 Viral studies negative Differential: ETOH (ASH) vs NAH vs Hemochromatosis or all three? HFE gene test: C282Y homozygote 22
23 Inherited abnormality of iron absorption Affects 0.5% of Caucasian people Rare in other races C282Y/H63D gene abnormalities Iron overload seen in C282Y homozygotes and sometimes compound heterozygotes (C282Y/H63D) No role for gene testing without elevated iron tests? Use for family members Iron tests esp ferritin can be falsely elevated in alcohol, acute inflammation, non fasting state Seen in 25% of heavy drinkers >5 drinks/day in men, much lower in women AST>ALT AST in mitochondria, and alcohol is a mitochondrial toxin Also seen when cirrhosis develops in other diseases Cirrhosis can develop without LT abnormalities! Alcohol hepatitis rarely has AST>300s 23
24 A 59 year old female presents with complaints of itching, dry mouth, and RUQ abdominal pain. She also notices some pigmentation changes on her eyelids. Her medical history includes frequent UTI s and osteopenia. What labs are you most interested in seeing for this patient? You obtain the following labs: AST=56, ALT=73, Alk. Phos=367, GGT=110, Platelets 98, Albumin 3.2, INR 1.2, creatinine 1.3, T.Bili 1.4 ANA/ASMA is negative Anti-Mitochondrial Ab (AMA) is positive IgM elevated What is the diagnosis? 24

25 Destruction of bile ducts Predominantly women Ages AMA positive in 95% of cases ANA positive in 60% of cases Commonly present with fatigue, pruritus Treatment with Ursodiol can improve the course of disease Fat Soluble Vitamin Deficiency Hyperlipidemia Gallstones Renal Tubular Acidosis Xanthomata Osteopenia Urinary Tract Infections Steatorrhea Malignancy Heathcote EJ. Hepatology 2000;31: Kaplan MM. N Engl J Med 1996;335:
26 3 months later she decompensated with severe ascites and hepatic encephalopathy Pt was transferred to liver transplant center where she got a liver transplant A 36 y.o. female with a history of Ulcerative Colitis presents with recurrent low-grade fevers, RUQ abdominal pain, pruritus and jaundice. Alk Phos is high at 394 T.Bili high at 4.6 AST 87, ALT 84. What test would confirm the diagnosis? What cancer is this patient at risk for? 26
27 ERCP is most commonly used Percutaneous cholangiography is rarely used now because it is invasive MRCP is gaining popularity because it is noninvasive, and cost-effective Increased risk for cholangiocarcinoma No role of screening currently 90+% associated with inflammatory bowel disease More commonly UC than Crohn s p-anca positive in 80% 27
28 37 year old Hispanic woman Elevated liver tests on routine labs C/o RUQ abdominal pain with radiation to the back PMH: DM, HTN, Hyperlipidemia, obesity Meds: metformin, lisinopril, ASA, pravastatin FHx: both parents died of CAD, brother with DM PE: acanthosis nigricans on neck, BMI 66.4 Abdominal US Dx cholelithiasis On lap choly surgeon see macroscopically nodular liver, he takes a Bx Confirmed liver cirrhosis with NASH EGD Dx Grade 3 esophageal varices Banding done Pt had bariatric surgery 3m later decompensated, but was saved with successful liver transplant 28
29 Serologically, a diagnosis of exclusion Abnormal buildup of fat in hepatocytes, sometimes causing inflammation Increasing incidence due to increase in obesity Risk factors: obesity, hypertriglyceridemia, HTN, insulin resistance, family history Treatment: weight loss, treat risk factors Statins are ok to use!!! In US 30 mln have NAFLD and 10 mln have NASH NASH can lead to liver cirrhosis and liver CA Alpha-1-antitrypsin Abnormal excretion of alpha-1-antitrypsin protein out of hepatocytes: increased buildup in liver, low levels in lung causing emphysema Check Phenotype: ZZ is abnormal Results of a-1-antitrypsin level can change with various disease states, so less specific Wilson s disease Abnormal copper excretion Low ceruloplasmin (copper binding protein) High 24 hour urine copper Generally young people Kayser-Fleisher rings on the edge of the iris Neurological and psychiatric symptoms 29
30 Full H&P Have patient completely quit ETOH Stop ALL unnecessary medications Emphasize to patient to avoid herbal supplements/teas 30
31 If LT abnormalities are 3x ULN Check acute viral serologies: HAV IgM, HBsAg, HBsAb, HBcAb (IgM), HCV Ab ANA, ASMA, panca AMA if cholestatic Fe studies Alpha-1-antitrypsin phenotype Ceruloplasmin if age <45 Quant Ig TSH Celiac Panel Compensated Decompensated 31
32 Portal Hypertension -Ascites - Two year mortality rate estimated at 50% 1 Spontaneous Bacterial Peritonitis (SBP) patients w/ ascites have a 10-25% chance of developing SBP within 1 year 2 -Varices Estimated mortality from first episode of variceal hemorrhage is 30-50% 3 Hepatic Encephalopathy (HE) <50% survival at 1 year after diagnosis; <25% survival at 3 years 4 Hepatorenal syndrome Hepatocellular Carcinoma (HCC) 3 in 10,000 may die from complications of the liver Bx Do not do it unless it is necessary Tissue is an issue With new expensive HCV Tx we will be forced to Bx every HCV pt, to establish stage of fibrosis 32





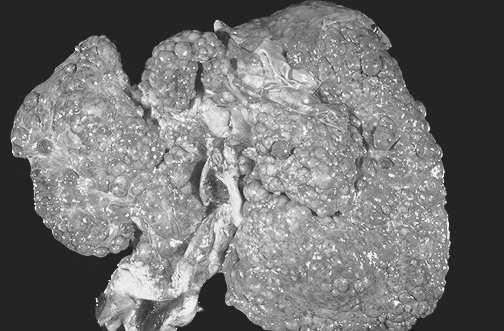
33 Normal Liver Edward Klatt, MD, Department of Pathology, University of Utah: Stage 1 Stage 2 Stage 3 Stage 4 Slide courtesy of Sammy Saab, MD, MPH, AGAF 33

34 34


35 35



36 PE: Fluid Wave Shifting dullness Puddle sign Causes: cirrhosis 75% malignancy 10% cardiac 3% TB 2% Pancreatitis 1% 36
, impairment of")



37 Can lead to a variety of disturbances, including impairment of quality of life (QOL), impairment of social and work function, and coma or death 1 Patient may present with Reports of mental or personality changes from family or friends 2 Asterixis 2 Decreased energy level Impaired sleep-wake cycle Impaired cognition, consciousness, or motor function Poor concentration, memory problem HE = hepatic encephalopathy. 1. M 37
38 46% of patient with liver cirrhosis may develop overt HE The goal of the treatment should be focused on the prevention of the future episodes because of the possible irreversibility of the psychomotor changes Dr. Robert Gish Tx protocol: Lactulose to titrate to 2BM/d and Rifaximin 550mg BID If 2BM/d pre-lactulose, then monotherapy with Rifaximin. Abdominal US every 6 months Ultrasound with doppler flow of portal vein, hepatic veins, hepatic artery I do check AFP as well every 6 months. 38
39 Download app GI calc Creatinine, Total Bilirubin and INR Consider referral to Liver transplant center for evaluation if MELD >15 and/or HCC 39
40 40
A Review of Liver Function Tests. James Gray Gastroenterology Vancouver
 A Review of Liver Function Tests James Gray Gastroenterology Vancouver Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
A Review of Liver Function Tests James Gray Gastroenterology Vancouver Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
EVALUATION OF ABNORMAL LIVER TESTS
 EVALUATION OF ABNORMAL LIVER TESTS MIA MANABAT DO PGY6 MOA 119 TH ANNUAL SPRING SCIENTIFIC CONVENTION MAY 19, 2018 EVALUATION OF ABNORMAL LIVER TESTS Review of liver enzymes vs liver function tests Clinical
EVALUATION OF ABNORMAL LIVER TESTS MIA MANABAT DO PGY6 MOA 119 TH ANNUAL SPRING SCIENTIFIC CONVENTION MAY 19, 2018 EVALUATION OF ABNORMAL LIVER TESTS Review of liver enzymes vs liver function tests Clinical
Approach to the Patient with Liver Disease
 Approach to the Patient with Liver Disease Diagnosis of liver disease Careful history taking Physical examination Laboratory tests Radiologic examination and imaging studies Liver biopsy Liver diseases
Approach to the Patient with Liver Disease Diagnosis of liver disease Careful history taking Physical examination Laboratory tests Radiologic examination and imaging studies Liver biopsy Liver diseases
Patterns of abnormal LFTs and their differential diagnosis
 Patterns of abnormal LFTs and their differential diagnosis Professor Matthew Cramp South West Liver Unit and Peninsula Schools of Medicine and Dentistry, Plymouth Outline liver function tests / tests of
Patterns of abnormal LFTs and their differential diagnosis Professor Matthew Cramp South West Liver Unit and Peninsula Schools of Medicine and Dentistry, Plymouth Outline liver function tests / tests of
Patterns of abnormal LFTs and their differential diagnosis
 Patterns of abnormal LFTs and their differential diagnosis Professor Matthew Cramp South West Liver Unit and Peninsula Schools of Medicine and Dentistry, Plymouth Outline liver function / liver function
Patterns of abnormal LFTs and their differential diagnosis Professor Matthew Cramp South West Liver Unit and Peninsula Schools of Medicine and Dentistry, Plymouth Outline liver function / liver function
Hepatocytes produce. Proteins Clotting factors Hormones. Bile Flow
 R.J.Bailey MD Hepatocytes produce Proteins Clotting factors Hormones Bile Flow Trouble.. for the liver! Trouble for the Liver Liver Gall Bladder Common Alcohol Hep C Fatty Liver Cancer Drugs Viruses Uncommon
R.J.Bailey MD Hepatocytes produce Proteins Clotting factors Hormones Bile Flow Trouble.. for the liver! Trouble for the Liver Liver Gall Bladder Common Alcohol Hep C Fatty Liver Cancer Drugs Viruses Uncommon
I have no disclosures relevant to this presentation LIVER TESTS: WHAT IS INCLUDED? LIVER TESTS: HOW TO UTILIZE THEM OBJECTIVES
 LIVER TESTS: HOW TO UTILIZE THEM I have no disclosures relevant to this presentation José Franco, MD Professor of Medicine, Surgery and Pediatrics Medical College of Wisconsin OBJECTIVES Differentiate
LIVER TESTS: HOW TO UTILIZE THEM I have no disclosures relevant to this presentation José Franco, MD Professor of Medicine, Surgery and Pediatrics Medical College of Wisconsin OBJECTIVES Differentiate
ABNORMAL LIVER FUNCTION TESTS. Dr Uthayanan Chelvaratnam Hepatology Consultant North Bristol NHS Trust
 ABNORMAL LIVER FUNCTION TESTS Dr Uthayanan Chelvaratnam Hepatology Consultant North Bristol NHS Trust INTRODUCTION Liver function tests Cases Non invasive fibrosis measurement Questions UK MORTALITY RATE
ABNORMAL LIVER FUNCTION TESTS Dr Uthayanan Chelvaratnam Hepatology Consultant North Bristol NHS Trust INTRODUCTION Liver function tests Cases Non invasive fibrosis measurement Questions UK MORTALITY RATE
Abnormal Liver Chemistries. Lauren Myers, MMsc. PA-C Oregon Health and Science University
 Abnormal Liver Chemistries Lauren Myers, MMsc. PA-C Oregon Health and Science University Disclosure 1. The speaker/planner Lauren Myers, MMSc, PA-C have no relevant financial relationships to disclose
Abnormal Liver Chemistries Lauren Myers, MMsc. PA-C Oregon Health and Science University Disclosure 1. The speaker/planner Lauren Myers, MMSc, PA-C have no relevant financial relationships to disclose
Approach to Abnormal Liver Tests
 Approach to Abnormal Liver Tests Scott W. Biggins, MD, MAS Assistant Professor Division of Gastroenterology UCSF Scott.Biggins@ucsf.edu (Thanks to Hal Yee, MD) This Morning s Presentation Clinical vignettes
Approach to Abnormal Liver Tests Scott W. Biggins, MD, MAS Assistant Professor Division of Gastroenterology UCSF Scott.Biggins@ucsf.edu (Thanks to Hal Yee, MD) This Morning s Presentation Clinical vignettes
WEEK. MPharm Programme. Liver Biochemistry. Slide 1 of 49 MPHM14 Liver Biochemistry
 MPharm Programme Liver Biochemistry Slide 1 of 49 MPHM Liver Biochemistry Learning Outcomes Assess and evaluate the signs and symptoms of illness Assess and critically appraise a patients medication regimen,
MPharm Programme Liver Biochemistry Slide 1 of 49 MPHM Liver Biochemistry Learning Outcomes Assess and evaluate the signs and symptoms of illness Assess and critically appraise a patients medication regimen,
Diseases of liver. Dr. Mohamed. A. Mahdi 4/2/2019. Mob:
 Diseases of liver Dr. Mohamed. A. Mahdi Mob: 0123002800 4/2/2019 Cirrhosis Cirrhosis is a complication of many liver disease. Permanent scarring of the liver. A late-stage liver disease. The inflammation
Diseases of liver Dr. Mohamed. A. Mahdi Mob: 0123002800 4/2/2019 Cirrhosis Cirrhosis is a complication of many liver disease. Permanent scarring of the liver. A late-stage liver disease. The inflammation
Autoimmune Hepatobiliary Diseases PROF. DR. SABEHA ALBAYATI CABM,FRCP
 Autoimmune Hepatobiliary Diseases PROF. DR. SABEHA ALBAYATI CABM,FRCP Autoimmune hepatobiliary diseases The liver is an important target for immunemediated injury. Three disease phenotypes are recognized:
Autoimmune Hepatobiliary Diseases PROF. DR. SABEHA ALBAYATI CABM,FRCP Autoimmune hepatobiliary diseases The liver is an important target for immunemediated injury. Three disease phenotypes are recognized:
Jaundice. Agnieszka Dobrowolska- Zachwieja, MD, PhD
 Jaundice Agnieszka Dobrowolska- Zachwieja, MD, PhD Jaundice definition Jaundice, as in the French jaune, refers to the yellow discoloration of the skin. It arises from the abnormal accumulation of bilirubin
Jaundice Agnieszka Dobrowolska- Zachwieja, MD, PhD Jaundice definition Jaundice, as in the French jaune, refers to the yellow discoloration of the skin. It arises from the abnormal accumulation of bilirubin
9/28/2016. Elevated Liver Function Tests: A Case Based Approach. Objectives. Identify patterns of abnormal liver function tests
 Elevated Liver Function Tests: A Case Based Approach Terrance M. James, NP C The Oregon Clinic Hepatology 503 963 2707 tejames@orclinic.com Objectives Identify patterns of abnormal liver function tests
Elevated Liver Function Tests: A Case Based Approach Terrance M. James, NP C The Oregon Clinic Hepatology 503 963 2707 tejames@orclinic.com Objectives Identify patterns of abnormal liver function tests
4/27/2018. Disclosures LIVER FUNCTION TESTS LIVER FUNCTION TESTS LIVER FUNCTION TESTS APPROACH TO THE PATIENT WITH ABNORMAL LIVER TESTS
 APPROACH TO THE PATIENT WITH ABNORMAL TESTS Kimberly A. Brown, M.D, FAST, FAASLD, AGAF Chief, Division of Gastroenterology and Hepatology Henry Ford Hospital Henry Ford Health System Detroit, Michigan
APPROACH TO THE PATIENT WITH ABNORMAL TESTS Kimberly A. Brown, M.D, FAST, FAASLD, AGAF Chief, Division of Gastroenterology and Hepatology Henry Ford Hospital Henry Ford Health System Detroit, Michigan
Initial Evaluation for HCV Therapy. Hope McGratty PA-C, MPH
 Initial Evaluation for HCV Therapy Hope McGratty PA-C, MPH Conflict of Interest Disclosure Statement None Who are we talking about today? Treatment naïve Chronic infection This patient seems complicated
Initial Evaluation for HCV Therapy Hope McGratty PA-C, MPH Conflict of Interest Disclosure Statement None Who are we talking about today? Treatment naïve Chronic infection This patient seems complicated
Disclosure. Evaluation of Abnormal Hepatic Enzymes
 Evaluation of Abnormal Hepatic Enzymes Bruce D. Askey, MS, ANP-BC Associate Lecturer North Andover, MA Adult Nurse Practitioner Dept. of Hepatology/Gastroenterology Guthrie Clinic Sayre, Pa Disclosure
Evaluation of Abnormal Hepatic Enzymes Bruce D. Askey, MS, ANP-BC Associate Lecturer North Andover, MA Adult Nurse Practitioner Dept. of Hepatology/Gastroenterology Guthrie Clinic Sayre, Pa Disclosure
IN THE NAME OF GOD. D r. MANIJE DEZFULI AZAD UNIVERCITY OF TEHRAN BOOALI HOSPITAL INFECTIOUS DISEASES SPECIALIST
 IN THE NAME OF GOD AZAD UNIVERCITY OF TEHRAN BOOALI HOSPITAL D r. MANIJE DEZFULI INFECTIOUS DISEASES SPECIALIST Acute Viral Hepatitis The Anatomy of the Liver Hepatic Physiology Liver: Largest solid organ
IN THE NAME OF GOD AZAD UNIVERCITY OF TEHRAN BOOALI HOSPITAL D r. MANIJE DEZFULI INFECTIOUS DISEASES SPECIALIST Acute Viral Hepatitis The Anatomy of the Liver Hepatic Physiology Liver: Largest solid organ
End Stage Liver Disease & Disease Specific Indications for Liver Transplant. Susan Kang, RN, MSN, ANP-BC
 End Stage Liver Disease & Disease Specific Indications for Liver Transplant Susan Kang, RN, MSN, ANP-BC Introduction (https://www.srtr.org) What does the liver do? STORAGE METABOLIC DETOXIFICATION SYNTHETIC
End Stage Liver Disease & Disease Specific Indications for Liver Transplant Susan Kang, RN, MSN, ANP-BC Introduction (https://www.srtr.org) What does the liver do? STORAGE METABOLIC DETOXIFICATION SYNTHETIC
End Stage Liver Disease & Disease Specific Indications for Liver Transplant Susan Kang, RN, MSN, ANP BC
 End Stage Liver Disease & Disease Specific Indications for Liver Transplant Susan Kang, RN, MSN, ANP BC Introduction (https://www.srtr.org) 1 What does the liver do? STORAGE METABOLIC DETOXIFICATION SYNTHETIC
End Stage Liver Disease & Disease Specific Indications for Liver Transplant Susan Kang, RN, MSN, ANP BC Introduction (https://www.srtr.org) 1 What does the liver do? STORAGE METABOLIC DETOXIFICATION SYNTHETIC
HEPETIC SYSTEMS BIOCHEMICAL HEPATOCYTIC SYSTEM HEPATOBILIARY SYSTEM RETICULOENDOTHELIAL SYSTEM
 EVALUATION OF LIVER FUNCTION R. Mohammadi Biochemist (Ph.D.) Faculty member of Medical Faculty HEPETIC SYSTEMS BIOCHEMICAL HEPATOCYTIC SYSTEM HEPATOBILIARY SYSTEM RETICULOENDOTHELIAL SYSTEM METABOLIC FUNCTION
EVALUATION OF LIVER FUNCTION R. Mohammadi Biochemist (Ph.D.) Faculty member of Medical Faculty HEPETIC SYSTEMS BIOCHEMICAL HEPATOCYTIC SYSTEM HEPATOBILIARY SYSTEM RETICULOENDOTHELIAL SYSTEM METABOLIC FUNCTION
Interpreting Liver Function Tests
 PSH Clinical Guidelines Statement 2017 Interpreting Liver Function Tests Dr. Asad A Chaudhry Consultant Hepatologist, Chaudhry Hospital, Gujranwala, Pakistan. Liver function tests (LFTs) generally refer
PSH Clinical Guidelines Statement 2017 Interpreting Liver Function Tests Dr. Asad A Chaudhry Consultant Hepatologist, Chaudhry Hospital, Gujranwala, Pakistan. Liver function tests (LFTs) generally refer
Management of Hepatitis C in Primary Care BABAFEMI ONABANJO, MD & BEN ALFRED, FNP UMASS FAMILY HEALTH CENTER WORCESTER
 Management of Hepatitis C in Primary Care BABAFEMI ONABANJO, MD & BEN ALFRED, FNP UMASS FAMILY HEALTH CENTER WORCESTER Objective Epidemiology Screening criteria Appropriate work up Treatment Guidelines
Management of Hepatitis C in Primary Care BABAFEMI ONABANJO, MD & BEN ALFRED, FNP UMASS FAMILY HEALTH CENTER WORCESTER Objective Epidemiology Screening criteria Appropriate work up Treatment Guidelines
Noncalculous Biliary Disease Dean Abramson, M.D. Gastroenterologists, P.C. Cedar Rapids. Cholestasis
 Noncalculous Biliary Disease Dean Abramson, M.D. Gastroenterologists, P.C. Cedar Rapids Cholestasis Biochemical hallmark Impaired bile flow from liver to small intestine Alkaline phosphatase is primary
Noncalculous Biliary Disease Dean Abramson, M.D. Gastroenterologists, P.C. Cedar Rapids Cholestasis Biochemical hallmark Impaired bile flow from liver to small intestine Alkaline phosphatase is primary
MANAGEMENT OF LIVER CIRRHOSIS: PRACTICE ESSENTIALS AND PATIENT SELF-MANAGEMENT
 MANAGEMENT OF LIVER CIRRHOSIS: PRACTICE ESSENTIALS AND PATIENT SELF-MANAGEMENT Sherona Bau, ACNP The Pfleger Liver Institute 200 UCLA Medical Plaza, Suite 214 Los Angeles, CA 90095 September 30, 2017 I
MANAGEMENT OF LIVER CIRRHOSIS: PRACTICE ESSENTIALS AND PATIENT SELF-MANAGEMENT Sherona Bau, ACNP The Pfleger Liver Institute 200 UCLA Medical Plaza, Suite 214 Los Angeles, CA 90095 September 30, 2017 I
Hepatitis. Dr. Mohamed. A. Mahdi 5/2/2019. Mob:
 Hepatitis Dr. Mohamed. A. Mahdi Mob: 0123002800 5/2/2019 Hepatitis Hepatitis means the inflammation of the liver. May cause by viruses or bacteria, parasites, radiation, drugs, chemical and toxins (alcohol).
Hepatitis Dr. Mohamed. A. Mahdi Mob: 0123002800 5/2/2019 Hepatitis Hepatitis means the inflammation of the liver. May cause by viruses or bacteria, parasites, radiation, drugs, chemical and toxins (alcohol).
Catherine Kerschen DO, FACOI Michigan State University College of Osteopathic Medicine
 Catherine Kerschen DO, FACOI Michigan State University College of Osteopathic Medicine none none Risk Factors for Alcoholic Liver Disease Amount of alcohol consumed Duration of alcohol consumption Gender
Catherine Kerschen DO, FACOI Michigan State University College of Osteopathic Medicine none none Risk Factors for Alcoholic Liver Disease Amount of alcohol consumed Duration of alcohol consumption Gender
Acute Hepatitis: An Approach to Infectious and Other Causes. Mary Anne Cooper MSc, MD, MEd, FRCPC
 : An Approach to Infectious and Other Causes Mary Anne Cooper MSc, MD, MEd, FRCPC Faculty: Dr. Mary Anne Cooper Relationships with commercial interests: Consulting Fees: Lupin Pharmaceuticals, Canada Objectives
: An Approach to Infectious and Other Causes Mary Anne Cooper MSc, MD, MEd, FRCPC Faculty: Dr. Mary Anne Cooper Relationships with commercial interests: Consulting Fees: Lupin Pharmaceuticals, Canada Objectives
What are LFTs? What are LFTs? 3/20/2017. Evaluation of Abnormal Liver Chemistry Tests. Transaminases. Alkaline phosphatase.
 Evaluation of Abnormal Liver Chemistry Tests James Panetta, DO What are LFTs? Transaminases Alkaline phosphatase Bilirubin Gamma-glutamyl transpeptidase What are LFTs? 5 nucleosidase Lactate Dehydrogenase
Evaluation of Abnormal Liver Chemistry Tests James Panetta, DO What are LFTs? Transaminases Alkaline phosphatase Bilirubin Gamma-glutamyl transpeptidase What are LFTs? 5 nucleosidase Lactate Dehydrogenase
Primary Sclerosing Cholangitis and Cholestatic liver diseases. Ahsan M Bhatti MD, FACP Bhatti Gastroenterology Consultants
 Primary Sclerosing Cholangitis and Cholestatic liver diseases Ahsan M Bhatti MD, FACP Bhatti Gastroenterology Consultants I have nothing to disclose Educational Objectives What is PSC? Understand the cholestatic
Primary Sclerosing Cholangitis and Cholestatic liver diseases Ahsan M Bhatti MD, FACP Bhatti Gastroenterology Consultants I have nothing to disclose Educational Objectives What is PSC? Understand the cholestatic
What to do with abnormal LFTs? Andrew M Smith Hepatobiliary Surgeon
 What to do with abnormal LFTs? Andrew M Smith Hepatobiliary Surgeon "it looks like there's something wrong.with your television set. Matt Groenig, creator of The Simpsons Probability of an abnormal screening
What to do with abnormal LFTs? Andrew M Smith Hepatobiliary Surgeon "it looks like there's something wrong.with your television set. Matt Groenig, creator of The Simpsons Probability of an abnormal screening
ACG Clinical Guideline: Evaluation of Abnormal Liver Chemistries
 ACG Clinical Guideline: Evaluation of Abnormal Liver Chemistries Paul Y. Kwo, MD, FACG, FAASLD 1, Stanley M. Cohen, MD, FACG, FAASLD 2, and Joseph K. Lim, MD, FACG, FAASLD 3 1 Division of Gastroenterology/Hepatology,
ACG Clinical Guideline: Evaluation of Abnormal Liver Chemistries Paul Y. Kwo, MD, FACG, FAASLD 1, Stanley M. Cohen, MD, FACG, FAASLD 2, and Joseph K. Lim, MD, FACG, FAASLD 3 1 Division of Gastroenterology/Hepatology,
2. Liver blood tests and what they mean p2 Acute and chronic liver screen
 Hepatology referral pathways for GP 1 Scope For use within hepatology Contents 2. Liver blood tests and what they mean p2 Acute and chronic liver screen p2 Common reasons for hepatology referral 3. Raised
Hepatology referral pathways for GP 1 Scope For use within hepatology Contents 2. Liver blood tests and what they mean p2 Acute and chronic liver screen p2 Common reasons for hepatology referral 3. Raised
Cirrhosis and Portal Hypertension Gastroenterology Teaching Project American Gastroenterological Association
 CIRRHOSIS AND PORTAL HYPERTENSION Cirrhosis and Portal Hypertension Gastroenterology Teaching Project American Gastroenterological Association WHAT IS CIRRHOSIS? What is Cirrhosis? DEFINITION OF CIRRHOSIS
CIRRHOSIS AND PORTAL HYPERTENSION Cirrhosis and Portal Hypertension Gastroenterology Teaching Project American Gastroenterological Association WHAT IS CIRRHOSIS? What is Cirrhosis? DEFINITION OF CIRRHOSIS
CHAPTER 1. Alcoholic Liver Disease
 CHAPTER 1 Alcoholic Liver Disease Major Lesions of Alcoholic Liver Disease Alcoholic fatty liver - >90% of binge and chronic drinkers Alcoholic hepatitis precursor of cirrhosis Alcoholic cirrhosis end
CHAPTER 1 Alcoholic Liver Disease Major Lesions of Alcoholic Liver Disease Alcoholic fatty liver - >90% of binge and chronic drinkers Alcoholic hepatitis precursor of cirrhosis Alcoholic cirrhosis end
Laboratory Tests and Diagnostic Procedures in Liver Disease: Adventures in Liverland
 Laboratory Tests and Diagnostic Procedures in Liver Disease: Adventures in Liverland Sanjiv Chopra, MD, MACP Professor of Medicine Harvard Medical School Editor In Chief Hepatology Section Up To Date Serum
Laboratory Tests and Diagnostic Procedures in Liver Disease: Adventures in Liverland Sanjiv Chopra, MD, MACP Professor of Medicine Harvard Medical School Editor In Chief Hepatology Section Up To Date Serum
Outline. Updates in the Clinical Management of Hepatitis B and C. Who should be screened for HBV? Chronic Hepatitis B 10/7/2018
 Outline Updates in the Clinical Management of Hepatitis B and C Jennifer C. Lai, MD, MBA Transplant Hepatologist Associate Professor of Medicine In Residence University of California, San Francisco Initial
Outline Updates in the Clinical Management of Hepatitis B and C Jennifer C. Lai, MD, MBA Transplant Hepatologist Associate Professor of Medicine In Residence University of California, San Francisco Initial
Transmission of HCV in the United States (CDC estimate)
") Transmission of HCV in the United States (CDC estimate) Past and Future US Incidence and Prevalence of HCV Infection Decline among IDUs Overall incidence Overall prevalence Infected 20+ years Armstrong
Transmission of HCV in the United States (CDC estimate) Past and Future US Incidence and Prevalence of HCV Infection Decline among IDUs Overall incidence Overall prevalence Infected 20+ years Armstrong
2. Liver blood tests and what they mean p2 Acute and chronic liver screen
 1 Scope For use within hepatology Contents 2. Liver blood tests and what they mean p2 Acute and chronic liver screen p2 Common reasons for referral 3. Raised ALT +/- GGT p3 4. Non alcoholic fatty liver
1 Scope For use within hepatology Contents 2. Liver blood tests and what they mean p2 Acute and chronic liver screen p2 Common reasons for referral 3. Raised ALT +/- GGT p3 4. Non alcoholic fatty liver
Fat, ballooning, plasma cells and a +ANA. Yikes! USCAP 2016 Evening Specialty Conference Cynthia Guy
 Fat, ballooning, plasma cells and a +ANA. Yikes! USCAP 2016 Evening Specialty Conference Cynthia Guy Goals Share an interesting case Important because it highlights a common problem that we re likely to
Fat, ballooning, plasma cells and a +ANA. Yikes! USCAP 2016 Evening Specialty Conference Cynthia Guy Goals Share an interesting case Important because it highlights a common problem that we re likely to
Morning Report Presentation. Sarah Hughes, MD January 11, 2005
 Morning Report Presentation Sarah Hughes, MD January 11, 2005 Primary Biliary Cirrhosis! PBC is a chronic, progressive, cholestatic liver disease of unknown cause that usually affects middle-aged women
Morning Report Presentation Sarah Hughes, MD January 11, 2005 Primary Biliary Cirrhosis! PBC is a chronic, progressive, cholestatic liver disease of unknown cause that usually affects middle-aged women
Interpreting Your Tests
 Interpreting Your Tests Lisa M. Forman, MD, MSCE Associate Professor of Medicine Section Hepatology and Liver Transplantation University of Colorado Denver Outline Bile Duct Anatomy Lab Tests LFTs Tumor
Interpreting Your Tests Lisa M. Forman, MD, MSCE Associate Professor of Medicine Section Hepatology and Liver Transplantation University of Colorado Denver Outline Bile Duct Anatomy Lab Tests LFTs Tumor
Overview. The Liver and Biliary System 10 cases to guide you. Liver Function. Background/Patterns. Case #1
 Overview The Liver and Biliary System 10 cases to guide you Chapy Venkatesan, MD Department of Medicine VCU School of Medicine Inova Campus 1 To be familiar with the approach to differential diagnosis
Overview The Liver and Biliary System 10 cases to guide you Chapy Venkatesan, MD Department of Medicine VCU School of Medicine Inova Campus 1 To be familiar with the approach to differential diagnosis
ABIM Review Hepatobiliary
 ABIM Review Hepatobiliary Danielle Brandman, MD, MAS Assistant Professor of Medicine University of California San Francisco ABIM Certification Exam ABIM Certification Exam Hepatobiliary Review Diagnostic
ABIM Review Hepatobiliary Danielle Brandman, MD, MAS Assistant Professor of Medicine University of California San Francisco ABIM Certification Exam ABIM Certification Exam Hepatobiliary Review Diagnostic
Management of Chronic Liver Failure/Cirrhosis Complications in Hospitals. By: Dr. Kevin Dolehide
 Management of Chronic Liver Failure/Cirrhosis Complications in Hospitals By: Dr. Kevin Dolehide Overview DX Cirrhosis and Prognosis Compensated Decompensated Complications Of Cirrhosis Management Of Complications
Management of Chronic Liver Failure/Cirrhosis Complications in Hospitals By: Dr. Kevin Dolehide Overview DX Cirrhosis and Prognosis Compensated Decompensated Complications Of Cirrhosis Management Of Complications
World Health Organization. Western Pacific Region
 Basic modules for hepatitis 1 Basic Module 1 Liver anatomy and physiology 2 Position of liver Midline Located in right upper abdomen Protected by the right rib cage Right upper Measures: 12 15 cm in vertical
Basic modules for hepatitis 1 Basic Module 1 Liver anatomy and physiology 2 Position of liver Midline Located in right upper abdomen Protected by the right rib cage Right upper Measures: 12 15 cm in vertical
Chronic Hepatic Disease
 Chronic Hepatic Disease 10 th Leading Cause of Death Liver Functions Energy Metabolism Protein Synthesis Solubilization, Transport, and Storage Protects and Clears drugs, damaged cells Causes of Liver
Chronic Hepatic Disease 10 th Leading Cause of Death Liver Functions Energy Metabolism Protein Synthesis Solubilization, Transport, and Storage Protects and Clears drugs, damaged cells Causes of Liver
What Is Cirrhosis? CIRRHOSIS. Cirrhosis occurs when the liver is. by chronic conditions and diseases. permanently scarred or injured
 What Is Cirrhosis? Cirrhosis occurs when the liver is permanently scarred or injured by chronic conditions and diseases. Common causes of cirrhosis include: Long-term alcohol abuse. Chronic viral hepatitis
What Is Cirrhosis? Cirrhosis occurs when the liver is permanently scarred or injured by chronic conditions and diseases. Common causes of cirrhosis include: Long-term alcohol abuse. Chronic viral hepatitis
Approach to the Patient with Abnormal Liver Enzymes
 Approach to the Patient with Abnormal Liver Enzymes Donald Gardenier, DNP, FNP-BC Assistant Professor and Clinical Program Director Icahn School of Medicine at Mount Sinai New York, NY Conflict of Interest
Approach to the Patient with Abnormal Liver Enzymes Donald Gardenier, DNP, FNP-BC Assistant Professor and Clinical Program Director Icahn School of Medicine at Mount Sinai New York, NY Conflict of Interest
Steps in Assessing Fibrosis 4/30/2015. Overview of Liver Disease Associated With HCV
 Overview of Liver Disease Associated With HCV Marion G. Peters, MD John V. Carbone, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California San Francisco San Francisco,
Overview of Liver Disease Associated With HCV Marion G. Peters, MD John V. Carbone, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California San Francisco San Francisco,
CITY AND HACKNEY CCG ABNORMAL LIVER FUNCTION TESTS (LFTs) in ADULTS
 in ADULTS") CITY AND HACKNEY CCG ABNORMAL LIVER FUNCTION TESTS (LFTs) in ADULTS Interpreting abnormal liver function tests (LFTs) and trying to diagnose any underlying liver disease is a common scenario in Primary
CITY AND HACKNEY CCG ABNORMAL LIVER FUNCTION TESTS (LFTs) in ADULTS Interpreting abnormal liver function tests (LFTs) and trying to diagnose any underlying liver disease is a common scenario in Primary
CrackCast Episode 28 Jaundice
 CrackCast Episode 28 Jaundice Episode overview: 1) Describe heme metabolism 2) List common pre-hepatic/hepatic/post-hepatic causes of jaundice Wisecracks: 1) What are clinical signs of liver disease? 2)
CrackCast Episode 28 Jaundice Episode overview: 1) Describe heme metabolism 2) List common pre-hepatic/hepatic/post-hepatic causes of jaundice Wisecracks: 1) What are clinical signs of liver disease? 2)
NAFLD, NASH, and alcoholic liver disease
 NAFLD, NASH, and alcoholic liver disease Jonathan Congeni MD NAFLD, NASH, and alcoholic liver disease Disease overview Epidemiology Pathogenesis Clinical features Labs and imaging Evaluation options Focus
NAFLD, NASH, and alcoholic liver disease Jonathan Congeni MD NAFLD, NASH, and alcoholic liver disease Disease overview Epidemiology Pathogenesis Clinical features Labs and imaging Evaluation options Focus
Learning Objectives. Case 1. Case Presentations. Interpretation of Liver Tests. Interpretation of Liver Tests. Presenter Disclosure Information
 Presenter Disclosure Information 11:05 11:45am Interpretation of Liver Tests SPEAKER Steven-Huy Han, MD, AGAF, FAASLD The following relationships exist related to this presentation: Steven-Huy Han, MD,
Presenter Disclosure Information 11:05 11:45am Interpretation of Liver Tests SPEAKER Steven-Huy Han, MD, AGAF, FAASLD The following relationships exist related to this presentation: Steven-Huy Han, MD,
Alpha-1 Antitrypsin Deficiency: Liver Disease
 Alpha-1 Antitrypsin Deficiency: Liver Disease Who is at risk to develop Alpha-1 liver disease? Alpha-1 liver disease may affect children and adults who have abnormal Alpha-1 antitrypsin genes. Keys to
Alpha-1 Antitrypsin Deficiency: Liver Disease Who is at risk to develop Alpha-1 liver disease? Alpha-1 liver disease may affect children and adults who have abnormal Alpha-1 antitrypsin genes. Keys to
LIVER DISEASES. Anatomy
 LIVER DISEASES Anatomy PHYSIOLOGY Bilirubin metabolism: 250-300 mg/d SER Bile UDPG-A B. diglucuronide Unc. B B. monoglucuronide Albumin Glucuronyltransferase 100-200 mg/d Bacteria 4mg In urine urobilinogen
LIVER DISEASES Anatomy PHYSIOLOGY Bilirubin metabolism: 250-300 mg/d SER Bile UDPG-A B. diglucuronide Unc. B B. monoglucuronide Albumin Glucuronyltransferase 100-200 mg/d Bacteria 4mg In urine urobilinogen
Liver failure &portal hypertension
 Liver failure &portal hypertension Objectives: by the end of this lecture each student should be able to : Diagnose liver failure (acute or chronic) List the causes of acute liver failure Diagnose and
Liver failure &portal hypertension Objectives: by the end of this lecture each student should be able to : Diagnose liver failure (acute or chronic) List the causes of acute liver failure Diagnose and
Disclosure. Objectives. Smash the Nash: A practical approach to fatty liver disease
 Smash the Nash: A practical approach to fatty liver disease Bruce D. Askey, MS, ANP-BC Associate Lecturer North Andover, MA Adult Nurse Practitioner Dept. of Hepatology/Gastroenterology Guthrie Clinic
Smash the Nash: A practical approach to fatty liver disease Bruce D. Askey, MS, ANP-BC Associate Lecturer North Andover, MA Adult Nurse Practitioner Dept. of Hepatology/Gastroenterology Guthrie Clinic
Biochemical Investigations in Liver Disease. Dr Roshitha de Silva Department of Pathology Faculty of Medicine University of Kelaniya
 Biochemical Investigations in Liver Disease Dr Roshitha de Silva Department of Pathology Faculty of Medicine University of Kelaniya Biochemical markers Albumin ALP ALT, AST Gamma-glutamyl transpeptidase
Biochemical Investigations in Liver Disease Dr Roshitha de Silva Department of Pathology Faculty of Medicine University of Kelaniya Biochemical markers Albumin ALP ALT, AST Gamma-glutamyl transpeptidase
PITFALLS IN THE DIAGNOSIS OF MEDICAL LIVER DISEASE WITH TWO CONCURRENT ETIOLOGIES I HAVE NOTHING TO DISCLOSE CURRENT ISSUES IN ANATOMIC PATHOLOGY 2017
 CURRENT ISSUES IN ANATOMIC PATHOLOGY 2017 I HAVE NOTHING TO DISCLOSE Linda Ferrell PITFALLS IN THE DIAGNOSIS OF MEDICAL LIVER DISEASE WITH TWO CONCURRENT ETIOLOGIES Linda Ferrell, MD, UCSF THE PROBLEM
CURRENT ISSUES IN ANATOMIC PATHOLOGY 2017 I HAVE NOTHING TO DISCLOSE Linda Ferrell PITFALLS IN THE DIAGNOSIS OF MEDICAL LIVER DISEASE WITH TWO CONCURRENT ETIOLOGIES Linda Ferrell, MD, UCSF THE PROBLEM
Biochemistry Liver Function Tests (LFTs)
") HbA NH 2 H 2 O 2 KClO3 Cl 2 O 7 PO 4 CH2O NAOH KMnO 4 M E D I C I N E KING SAUD UNIVERSITY Co 2 COOH MgCl 2 H 2 O Important Extra Information Doctors slides Doctors notes SO 2 HCN CCl 4 CuCl 2 SiCl 4 Biochemistry
HbA NH 2 H 2 O 2 KClO3 Cl 2 O 7 PO 4 CH2O NAOH KMnO 4 M E D I C I N E KING SAUD UNIVERSITY Co 2 COOH MgCl 2 H 2 O Important Extra Information Doctors slides Doctors notes SO 2 HCN CCl 4 CuCl 2 SiCl 4 Biochemistry
ABIM Review Hepatobiliary
 Hepatobiliary Review ABIM Review Hepatobiliary Oren Fix, MD, MSc Assistant Professor of Medicine University of California San Francisco Diagnostic algorithms for cholestatic versus hepatitic pattern of
Hepatobiliary Review ABIM Review Hepatobiliary Oren Fix, MD, MSc Assistant Professor of Medicine University of California San Francisco Diagnostic algorithms for cholestatic versus hepatitic pattern of
Session 11: The ABCs of LFTs Learning Objectives
 Session 11: The ABCs of LFTs Learning Objectives 1. Define 3 key components of the patient history that should be further evaluated when liver function testing reveals elevated aminotransferases. 2. Identify
Session 11: The ABCs of LFTs Learning Objectives 1. Define 3 key components of the patient history that should be further evaluated when liver function testing reveals elevated aminotransferases. 2. Identify
Drug therapy in patient with hepatic impairment
 Drug therapy in patient with hepatic impairment Arzneimitteltherapie bei Leberinsuffizienz Dominik Wilke 03/04 Mai 2018 43. ADKA-Kongress, Stuttgart Functions of the Liver I Metabolism (Carbohydrates,
Drug therapy in patient with hepatic impairment Arzneimitteltherapie bei Leberinsuffizienz Dominik Wilke 03/04 Mai 2018 43. ADKA-Kongress, Stuttgart Functions of the Liver I Metabolism (Carbohydrates,
Pediatric PSC A children s tale
 Pediatric PSC A children s tale September 8 th PSC Partners seeking a cure Tamir Miloh Assistant Professor Pediatric Hepatology Mount Sinai Hospital, NY Incidence Primary Sclerosing Cholangitis (PSC) ;
Pediatric PSC A children s tale September 8 th PSC Partners seeking a cure Tamir Miloh Assistant Professor Pediatric Hepatology Mount Sinai Hospital, NY Incidence Primary Sclerosing Cholangitis (PSC) ;
Hepatitis A Virus: Old Things Made New
 Hepatitis A Virus: Old Things Made New Cody A. Chastain, MD Assistant Professor of Medicine Viral Hepatitis Program Division of Infectious Diseases Vanderbilt University Medical Center Cody.A.Chastain@VUMC.org
Hepatitis A Virus: Old Things Made New Cody A. Chastain, MD Assistant Professor of Medicine Viral Hepatitis Program Division of Infectious Diseases Vanderbilt University Medical Center Cody.A.Chastain@VUMC.org
Metabolic Liver Disease
 Metabolic Liver Disease Peter Eichenseer, MD No relationships to disclose. Outline Overview Alpha-1 antitrypsin deficiency Wilson s disease Hereditary hemochromatosis Pathophysiology Clinical features
Metabolic Liver Disease Peter Eichenseer, MD No relationships to disclose. Outline Overview Alpha-1 antitrypsin deficiency Wilson s disease Hereditary hemochromatosis Pathophysiology Clinical features
Pathophysiology I Liver and Biliary Disease
 Pathophysiology I Liver and Biliary Disease The Liver The liver is located in the right upper portion of the abdominal cavity just beneath the right side of the rib cage. The liver has many functions that
Pathophysiology I Liver and Biliary Disease The Liver The liver is located in the right upper portion of the abdominal cavity just beneath the right side of the rib cage. The liver has many functions that
Podcast (Video Recorded Lecture Series): Portal HTN and Derivatives for the USMLE Step One Exam. Ultrasound (w/ doppler) Reversal of flow Portal Vein
: Portal HTN and Derivatives for the USMLE Step One Exam. Ultrasound (w/ doppler) Reversal of flow Portal Vein") Podcast (Video Recorded Lecture Series): Portal HTN and Derivatives for the USMLE Step One Exam Hepatic Vein (Budd Chiari) Ultrasound (w/ doppler) Reversal of flow Portal Vein Howard J. Sachs, MD www.12daysinmarch.com
Podcast (Video Recorded Lecture Series): Portal HTN and Derivatives for the USMLE Step One Exam Hepatic Vein (Budd Chiari) Ultrasound (w/ doppler) Reversal of flow Portal Vein Howard J. Sachs, MD www.12daysinmarch.com
Hepatitis B screening and surveillance in primary care
 Hepatitis B screening and surveillance in primary care Catherine Stedman Associate Professor of Medicine, University of Otago, Christchurch Gastroenterology Department, Christchurch Hospital Disclosures
Hepatitis B screening and surveillance in primary care Catherine Stedman Associate Professor of Medicine, University of Otago, Christchurch Gastroenterology Department, Christchurch Hospital Disclosures
LIVER CIRRHOSIS. The liver extracts nutrients from the blood and processes them for later use.
 LIVER CIRRHOSIS William Sanchez, M.D. & Jayant A. Talwalkar, M.D., M.P.H. Advanced Liver Disease Study Group Miles and Shirley Fiterman Center for Digestive Diseases Mayo College of Medicine Rochester,
LIVER CIRRHOSIS William Sanchez, M.D. & Jayant A. Talwalkar, M.D., M.P.H. Advanced Liver Disease Study Group Miles and Shirley Fiterman Center for Digestive Diseases Mayo College of Medicine Rochester,
Hepatology for the Nonhepatologist
 Hepatology for the Nonhepatologist Kenneth E. Sherman, MD, PhD Gould Professor of Medicine Director, Division of Digestive Diseases University of Cincinnati College of Medicine Cincinnati, Ohio Learning
Hepatology for the Nonhepatologist Kenneth E. Sherman, MD, PhD Gould Professor of Medicine Director, Division of Digestive Diseases University of Cincinnati College of Medicine Cincinnati, Ohio Learning
2013 UPDATES IN HEPATITIS B & C
 2013 UPDATES IN HEPATITIS B & C Jennifer C. Lai, MD, MBA Division of Gastroenterology/Hepatology University of California, San Francisco Financial disclosures: none Outline: HBV & HCV Case-based presentations
2013 UPDATES IN HEPATITIS B & C Jennifer C. Lai, MD, MBA Division of Gastroenterology/Hepatology University of California, San Francisco Financial disclosures: none Outline: HBV & HCV Case-based presentations
Adams Memorial Hospital Decatur, Indiana EXPLANATION OF LABORATORY TESTS
 Adams Memorial Hospital Decatur, Indiana EXPLANATION OF LABORATORY TESTS Your health is important to us! The test descriptions listed below are for educational purposes only. Laboratory test interpretation
Adams Memorial Hospital Decatur, Indiana EXPLANATION OF LABORATORY TESTS Your health is important to us! The test descriptions listed below are for educational purposes only. Laboratory test interpretation
Mr Ricky Gellissen Imperial College Healthcare NHS Trust, London, UK
 Mr Ricky Gellissen Imperial College Healthcare NHS Trust, London, UK Ms Sally Bufton University Hospital Birmingham NHS Foundation Trust, Queen Elizabeth Hospital, Birmingham Mrs Janet Catt Royal Free
Mr Ricky Gellissen Imperial College Healthcare NHS Trust, London, UK Ms Sally Bufton University Hospital Birmingham NHS Foundation Trust, Queen Elizabeth Hospital, Birmingham Mrs Janet Catt Royal Free
Interpreting Liver Tests What Do They Mean? Roman E. Perri, MD
 Interpreting Liver Tests What Do They Mean? Roman E. Perri, MD The assessment of patients with abnormal liver tests is common in both primary care and gastroenterology clinics. However, among patients
Interpreting Liver Tests What Do They Mean? Roman E. Perri, MD The assessment of patients with abnormal liver tests is common in both primary care and gastroenterology clinics. However, among patients
Disorders of the Liver, Gallbladder and Pancreas
 Disorders of the Liver, Gallbladder and Pancreas Objectives: Disorders of the liver Disorders of the gall bladder Disorders of the pancreas Part 1: Disorders of the Liver 1 Jaundice: is a manifestation
Disorders of the Liver, Gallbladder and Pancreas Objectives: Disorders of the liver Disorders of the gall bladder Disorders of the pancreas Part 1: Disorders of the Liver 1 Jaundice: is a manifestation
Viral Hepatitis. Dr Melissa Haines Gastroenterologist Waikato Hospital
 Viral Hepatitis Dr Melissa Haines Gastroenterologist Waikato Hospital Viral Hepatitis HAV HBV HCV HDV HEV Other viral: CMV, EBV, HSV Unknown Hepatitis A Hepatitis A Transmitted via the faecal-oral route
Viral Hepatitis Dr Melissa Haines Gastroenterologist Waikato Hospital Viral Hepatitis HAV HBV HCV HDV HEV Other viral: CMV, EBV, HSV Unknown Hepatitis A Hepatitis A Transmitted via the faecal-oral route
Mrs Janet Catt. Pre-Conference Nurse s Course. Royal Free London NHS Foundation Trust. Janet Catt MSc RN Lead Nurse Specialist Practic 12/12/2014
 Pre-Conference Nurse s Course in partnership with Mrs Janet Catt Royal Free London NHS Foundation Trust Janet Catt MSc RN Lead Nurse Specialist Practic 1 Liver blood tests monitoring cirrhosis HIV/HCV
Pre-Conference Nurse s Course in partnership with Mrs Janet Catt Royal Free London NHS Foundation Trust Janet Catt MSc RN Lead Nurse Specialist Practic 1 Liver blood tests monitoring cirrhosis HIV/HCV
Dr Mere Kende. MBBS,Mmed(Path), MAACB, MACTM, MACRRM Lecturer -SMHS
, MAACB, MACTM, MACRRM Lecturer -SMHS") Dr Mere Kende MBBS,Mmed(Path), MAACB, MACTM, MACRRM Lecturer -SMHS Reasons for LFT Classification of Liver Diseases Signs and Symptoms of Liver Disease Routine Liver Tests Jaundice Examples of Liver Diseases
Dr Mere Kende MBBS,Mmed(Path), MAACB, MACTM, MACRRM Lecturer -SMHS Reasons for LFT Classification of Liver Diseases Signs and Symptoms of Liver Disease Routine Liver Tests Jaundice Examples of Liver Diseases
Cirrhosis of the Liver
 235 60th Street, West New York, NJ 07093 T: (201) 854-4646 F: (201) 854-4647 810 Main Street, Hackensack, NJ 07601 T: (201) 488-0095 Cirrhosis of the Liver The liver, the largest organ in the body, is
235 60th Street, West New York, NJ 07093 T: (201) 854-4646 F: (201) 854-4647 810 Main Street, Hackensack, NJ 07601 T: (201) 488-0095 Cirrhosis of the Liver The liver, the largest organ in the body, is
-Liver function tests -
 -Liver function tests - Biochimestry teamwork Osamah Al-Jarallah Abdulaziz Al-Shamlan Abdullah Al-Mazyad Turki Al-Otaibi Khalid Al-Khamis Saud Al-awad KhaledAlmohaimede Meshal Al-Otaibi Al-Anood Asiri
-Liver function tests - Biochimestry teamwork Osamah Al-Jarallah Abdulaziz Al-Shamlan Abdullah Al-Mazyad Turki Al-Otaibi Khalid Al-Khamis Saud Al-awad KhaledAlmohaimede Meshal Al-Otaibi Al-Anood Asiri
Module 1 Introduction of hepatitis
 Module 1 Introduction of hepatitis 1 Training Objectives At the end of the module, trainees will be able to ; Demonstrate improved knowledge of the global epidemiology of the viral hepatitis Understand
Module 1 Introduction of hepatitis 1 Training Objectives At the end of the module, trainees will be able to ; Demonstrate improved knowledge of the global epidemiology of the viral hepatitis Understand
Gastrointes*nal and Liver Pathology. Kris*ne Kra5s, M.D.
 Gastrointes*nal and Liver Pathology Kris*ne Kra5s, M.D. GI Pathology Outline Esophagus Stomach Intes*ne Liver Gallbladder Pancreas GI Pathology Outline Esophagus Stomach Intes*ne Liver Hepa**s Alcoholic
Gastrointes*nal and Liver Pathology Kris*ne Kra5s, M.D. GI Pathology Outline Esophagus Stomach Intes*ne Liver Gallbladder Pancreas GI Pathology Outline Esophagus Stomach Intes*ne Liver Hepa**s Alcoholic
GI DISEASE WORKSHOP CASE STUDIES
 GI DISEASE WORKSHOP CASE STUDIES American Academy of Insurance Medicine Triennial Course in Insurance Medicine 2012 Clifton Titcomb Jr., MD (Hannover Re) James Topic, MD (Protective Life) 1 CASE #1 Application
GI DISEASE WORKSHOP CASE STUDIES American Academy of Insurance Medicine Triennial Course in Insurance Medicine 2012 Clifton Titcomb Jr., MD (Hannover Re) James Topic, MD (Protective Life) 1 CASE #1 Application
Gastrointestinal System: Accessory Organ Disorders
 Gastrointestinal System: Accessory Organ Disorders Mary DeLetter, PhD, RN Associate Professor Dept. of Baccalaureate and Graduate Nursing Eastern Kentucky University Disorders of Accessory Organs Portal
Gastrointestinal System: Accessory Organ Disorders Mary DeLetter, PhD, RN Associate Professor Dept. of Baccalaureate and Graduate Nursing Eastern Kentucky University Disorders of Accessory Organs Portal
Pittsburgh CME Conference November 7-9, 2014
 Disclosures: Pennsylvania Academy of Family Physicians Foundation Pittsburgh CME Conference November 7-9, 2014 Abnormal LFT s Now What? (Patient Safety) Bruce Gebhardt, MD St. Vincent Health System, Erie,
Disclosures: Pennsylvania Academy of Family Physicians Foundation Pittsburgh CME Conference November 7-9, 2014 Abnormal LFT s Now What? (Patient Safety) Bruce Gebhardt, MD St. Vincent Health System, Erie,
Review: How to work up your patient with Hepatitis C
 Review: How to work up your patient with Hepatitis C You screened your patient, and now the HCV antibody test is positive. What do you do next? The antibody test only means they have been exposed to HCV.
Review: How to work up your patient with Hepatitis C You screened your patient, and now the HCV antibody test is positive. What do you do next? The antibody test only means they have been exposed to HCV.
The Continuum of Care for Advanced Liver Disease: Partnering with the Liver Specialist. K V Speeg, MD, PhD UT Health San Antonio
 The Continuum of Care for Advanced Liver Disease: Partnering with the Liver Specialist K V Speeg, MD, PhD UT Health San Antonio Objectives Review staging of liver disease Review consequences of end-stage
The Continuum of Care for Advanced Liver Disease: Partnering with the Liver Specialist K V Speeg, MD, PhD UT Health San Antonio Objectives Review staging of liver disease Review consequences of end-stage
Overview of PSC Jayant A. Talwalkar, MD, MPH Associate Professor of Medicine Mayo Clinic Rochester, MN
 Overview of PSC Jayant A. Talwalkar, MD, MPH Associate Professor of Medicine Mayo Clinic Rochester, MN 2012 Annual Conference PSC Partners Seeking a Cure May 5, 2012 Primary Sclerosing Cholangitis Multifocal
Overview of PSC Jayant A. Talwalkar, MD, MPH Associate Professor of Medicine Mayo Clinic Rochester, MN 2012 Annual Conference PSC Partners Seeking a Cure May 5, 2012 Primary Sclerosing Cholangitis Multifocal
Transplant Hepatology
 Transplant Hepatology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified
Transplant Hepatology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified
A Rational Evidence-based Approach to Abnormal Liver Tests
 A Rational Evidence-based Approach to Abnormal Liver Tests Jane D. Ricaforte-Campos, MD FPCP, FPSG, FPSDE 2013 HSP Post-graduate Course Radisson Blu Hotel, Cebu City misnomer Liver Function Tests Does
A Rational Evidence-based Approach to Abnormal Liver Tests Jane D. Ricaforte-Campos, MD FPCP, FPSG, FPSDE 2013 HSP Post-graduate Course Radisson Blu Hotel, Cebu City misnomer Liver Function Tests Does
Not All Patients With Liver Disease Have HCV Diagnosis and Management of Some Common Non HCV Liver Diseases
 Not All Patients With Liver Disease Have HCV Diagnosis and Management of Some Common Non HCV Liver Diseases Prevalence of Chronic Liver Disorders in the United States Nonalcoholic Fatty Liver Disorder
Not All Patients With Liver Disease Have HCV Diagnosis and Management of Some Common Non HCV Liver Diseases Prevalence of Chronic Liver Disorders in the United States Nonalcoholic Fatty Liver Disorder
HEPATOLOGY COPYRIGHTED MATERIAL
 PART 1 HEPATOLOGY COPYRIGHTED MATERIAL CHAPTER 1 Approach to the Patient with Abnormal Liver Tests Charissa Y. Chang Division of Liver Diseases, Icahn School of Medicine at Mount Sinai, New York, NY,
PART 1 HEPATOLOGY COPYRIGHTED MATERIAL CHAPTER 1 Approach to the Patient with Abnormal Liver Tests Charissa Y. Chang Division of Liver Diseases, Icahn School of Medicine at Mount Sinai, New York, NY,
Liver Disease. By: Michael Martins
 Liver Disease By: Michael Martins Recently I have been getting a flurry of patients that have some serious liver complications. This week s literature review will be the dental management of the patients
Liver Disease By: Michael Martins Recently I have been getting a flurry of patients that have some serious liver complications. This week s literature review will be the dental management of the patients
Definition: fibrosis and nodular regeneration resulting from hepatocellular injury
 Cirrhosis Understanding the liver: Patterns of LFT Abnormalities - Hepatocellular/Transaminitis: o Ratio of AST: ALT >2:1 ETOH (keep in mind AST is also produced by red cells, heart muscle) o If Aminotransferases
Cirrhosis Understanding the liver: Patterns of LFT Abnormalities - Hepatocellular/Transaminitis: o Ratio of AST: ALT >2:1 ETOH (keep in mind AST is also produced by red cells, heart muscle) o If Aminotransferases
Primary Care Approach to Diagnosis and Management of Chronic Hepatitis C Brian Viviano, D.O.
 Primary Care Approach to Diagnosis and Management of Chronic Hepatitis C Brian Viviano, D.O. Objectives Epidemiology of chronic hepatitis C CDC guidelines on screening or hepatitis C Diagnosing hepatitis
Primary Care Approach to Diagnosis and Management of Chronic Hepatitis C Brian Viviano, D.O. Objectives Epidemiology of chronic hepatitis C CDC guidelines on screening or hepatitis C Diagnosing hepatitis
ABIM Review Hepatology
 ABIM Review Hepatology Norah Terrault, MD, MPH Associate Professor University of California San Francisco July 15, 2009 Liver Review Diagnostic algorithms for cholestatic versus hepatitic pattern of liver
ABIM Review Hepatology Norah Terrault, MD, MPH Associate Professor University of California San Francisco July 15, 2009 Liver Review Diagnostic algorithms for cholestatic versus hepatitic pattern of liver