MANAGEMENT OF LIVER CIRRHOSIS: PRACTICE ESSENTIALS AND PATIENT SELF-MANAGEMENT
|
|
|
- Shannon Owen
- 5 years ago
- Views:
Transcription
1 MANAGEMENT OF LIVER CIRRHOSIS: PRACTICE ESSENTIALS AND PATIENT SELF-MANAGEMENT Sherona Bau, ACNP The Pfleger Liver Institute 200 UCLA Medical Plaza, Suite 214 Los Angeles, CA September 30, 2017
2 I have no disclosure. DISCLOSURE
3 OBJECTIVES What is liver cirrhosis Causes of liver cirrhosis Management of liver cirrhosis Patient Self-Management of liver cirrhosis
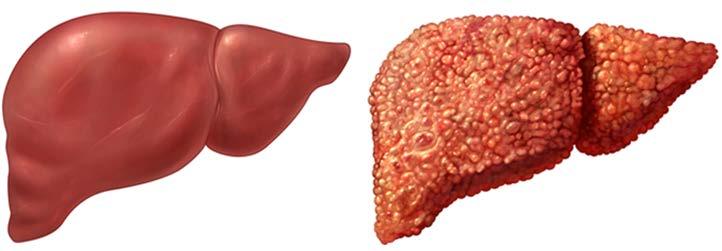
4 LIVER CIRRHOSIS A late stage of progressive hepatic fibrosis characterized by distortion of the hepatic architecture and the formation of regenerative nodules. It is generally considered to be irreversible in its advanced stages The ideal treatment for decompensated liver cirrhosis may be liver transplantation. 4
5 LIVER DISEASES THAT LEAD TO LIVER CIRRHOSIS Hepatitis B Hepatitis C Autoimmune hepatitis Primary biliary cholangitis Primary sclerosing cholangitis Alcoholic liver disease Nonalcoholic steatohepatitis Hemochromatosis 5
6 PHYSICAL EXAMINATION Spider angiomata Palmar erythema Scleral icterus or jaundice BLE edema Ascites Anorexia 6

7 SPIDER ANGIOMATA 7

8 PALMAR ERYTHEMA 8

9 SCLERAL ICTERUS 9

10 EDEMA 10

11 ASCITES 11





12 TESTS FOR LIVER CIRRHOSIS ASSESSMENT Liver Biopsy Serum Biomarkers Elastography Routine Imaging Physical Examination
13 Histologic Staging Hepatitis C Normal Stage 1 2 Cirrhotic 3 4
14 LAB FINDINGS Aspartate aminotransferase (AST) and alanine aminotransferase (ALT) are usually moderately elevated. Normal AST and ALT do not preclude cirrhosis Low platelet counts < 150,000 Low albumin < 3.5 Bilirubin may be normal or elevated in cirrhosis progresses

15 SEROLOGIC TESTS 15
16 IMAGING OR EGD FINDINGS Ultrasound of abdomen can show Nodular liver Portal hypertension Splenomegaly Ascites Upper endoscopy may show esophageal varices MRElastography

17 PREDICTION OF PROGNOSIS Child-Pugh Classification MELD score (Model for end-stage liver disease)
18 CHILD-PUGH CLASSIFICATION OF CIRRHOSIS Parameter Point 1 point 2 points 3 points Prothrombin >6 Albumin > <2.8 Ascites none mild Moderatesevere Encephalopathy none Grade 1-2 Grade 3 or 4 Grade A: 5-6 points Grade B: 7-9 points Grade C: points 18

19 MELD-NA SCORE
20 MANAGEMENT OF CIRRHOSIS Treatment goals for patients with cirrhosis: Slow the progression of liver damage Manage symptoms and reduce the risk for complications Treatment by a multi-disciplinary team is the ideal approach. 20
21 MANAGEMENT OF LIVER CIRRHOSIS Hepatocellular Carcinoma screening (US of abdomen + AFP) every 6 months EGD to screen esophageal varices Low sodium diet No raw fish or raw shellfish to prevent Vibrio vulnificus infection Avoid constipation Alcohol abstinence Small snacks between meals to maintain nutrient
22 DECOMPENSATED LIVER CIRRHOSIS Ascites Portal Hypertension Esophageal varices bleeding Encephalopathy Jaundice Muscle wasting Thrombocytopenia 22
23 ASCITES Diuretics Sodium monitoring Low sodium diet, < 2 gram per day Paracentesis as needed 23
24 ASCITES Diuretics If kidney function and electrolytes allow, single morning doses of oral spironolactone 100mg and furosemide 40mg. Spironolactone can increase potassium versus furosemide can lower potassium. The doses of both drugs an increased at the same time every 5-7 days. 24
25 ASCITES Amiloride 10-40mg per day can be substituted for spironolactone in patients with tender gynecomastia. Hydrochlorothiazide can cause rapidly development of hyponatremia when using with spironolactone and furosemide, it should be used extreme caution. 25
26 ASCITES Paracentesis Paracentesis can be performed as needed if a patient developed refractory ascites (diuretics-resistant tense ascites). Transjugular intrahepatic portosystemic shunt (TIPS) for refractory ascites 26
27 PORTAL HYPERTENSION Portal hypertension is resistance to portal blood flow and is aggravated by increased portal collateral blood flow. The resistance most often occurs within the liver (as is the case in cirrhosis), but it can also be prehepatic (eg, portal vein thrombosis) or posthepatic (eg, Budd-Chiari syndrome). 27
28 MANIFESTATIONS OF PORTAL HYPERTENSION Variceal hemorrhage Portal hypertensive gastropathy Ascites Hepatorenal syndrome Hepatic hydrothorax Hepatopulmonary syndrome Pulmonary hypertension 28
29 MANAGEMENT OF PORTAL HYPERTENSION Transjugular intrahepatic portosystemic shunt (TIPS) Purpose of a TIPS is to Decompress the portal venous system Prevent rebleeding from varices Stop or reduce the formation of ascites 29

30 TRANSJUGULAR INTRAHEPATIC PORTOSYSTEMIC SHUNT
31 COMPLICATIONS OF TIPS 31
32 ESOPHAGEAL VARICES As a result of portal hypertension Screening for esophageal varices through upper endoscopy 32
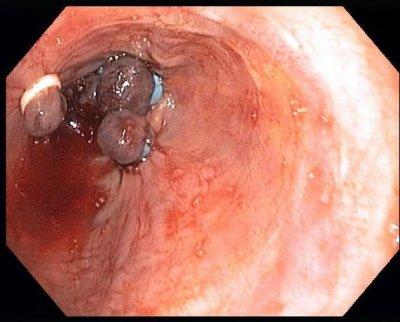
33 ESOPHAGEAL VARICES
34 MANAGEMENT OF ESOPHAGEAL VARICES Esophageal varices non-bleeding Primary prophylaxis beta blockers Esophageal varices bleeding Esophagogastroduodenoscopy (EGD) with banding TIPs with rebleeding 34
35 ENCEPHALOPATHY Hepatic Encephalopathy (HE) HE is a brain dysfunction caused by liver insufficiency and/or Portal Systemic Shunting Wide spectrum of neurological or psychiatric abnormalities ranging from subclinical alterations to coma Clinically overt HE will occur in 30%-40% of those with cirrhosis and in most patients repeatedly Subjects with recurrent overt HE have a 40% cumulative risk of another recurrence within 6 months, despite standard treatment 35
36 GRADE OF ENCEPHALOPATHY Grade Definition I Changes in behavior with minimal change in level of consciousness II Gross disorientation, drowsiness, possibly asterixis, inappropriate behavior III Marked confusion, incoherent speech, sleeping most of the time but arousable to vocal stimuli IV Comatose, unresponsive to pain, decorticate or decerebrate posturing


37 FAMILY/PATIENT EDUCATION FOR ENCEPHALOPATHY Being confused Memory problems Mood changes Trouble speaking, drawing, and writing clearly Problems with sleep Some people have trouble falling asleep. Others sleep too much. Moving more slowly than normal Flapping hands

38 ASTERIXIS
39 PRECIPITATING CAUSES Dehydration Urinary tract infection Large volume paracentesis Constipation Large amount of red meat consumption Sleeping medication

40 MANAGEMENT OF ENCEPHALOPATHY Lactulose 30cc bid Goal 2 to 3 bowel movements per day Rifaximin 550mg po bid Avoid benzodiazepines Avoid pain medication 40
41 PATIENT SELF-MANAGEMENT FOR LIVER CIRRHOSIS Avoid NSAIDs Ok to take Tylenol no more than 2g/day Alcohol Constipation Raw shellfish Herbal supplement
42 PATIENT SELF-MANAGEMENT FOR LIVER CIRRHOSIS Daily weight Strict low sodium diet less than 1500mg per day. Low sodium should be < 140mg / serving Small snack between meals

43 FOOD HIGH IN SODIUM


44 FOOD HIGH IN SODIUM

45 FOOD HIGH IN SODIUM


46 FOOD HIGH IN SODIUM

47 FOOD HIGH IN SODIUM
48 FOOD HIGH IN SODIUM Deli meats hot dog - 700mg/serving Vegetable juices tomato juice - 700mg/serving Canned vegetable 1300mg/can Frozen meals 1800mg/serving Ketchup - 150mg/tablespoon, Soy sauce 1000mg/tablespoon Bread or tortillas 250 mg per serving Daily products cottage cheese, buttermilk or American cheese up to 400mg/ounce
49 CONCLUSION Liver cirrhosis is late stage of hepatic fibrosis potentially irreversible Manage symptoms and prevent decompensations Screening for hepatocellular carcinoma every 6 months Patient and family members play an important roles for prognosis of liver cirrhosis

50 50
Cirrhosis and Portal Hypertension Gastroenterology Teaching Project American Gastroenterological Association
 CIRRHOSIS AND PORTAL HYPERTENSION Cirrhosis and Portal Hypertension Gastroenterology Teaching Project American Gastroenterological Association WHAT IS CIRRHOSIS? What is Cirrhosis? DEFINITION OF CIRRHOSIS
CIRRHOSIS AND PORTAL HYPERTENSION Cirrhosis and Portal Hypertension Gastroenterology Teaching Project American Gastroenterological Association WHAT IS CIRRHOSIS? What is Cirrhosis? DEFINITION OF CIRRHOSIS
Liver failure &portal hypertension
 Liver failure &portal hypertension Objectives: by the end of this lecture each student should be able to : Diagnose liver failure (acute or chronic) List the causes of acute liver failure Diagnose and
Liver failure &portal hypertension Objectives: by the end of this lecture each student should be able to : Diagnose liver failure (acute or chronic) List the causes of acute liver failure Diagnose and
Management of Chronic Liver Failure/Cirrhosis Complications in Hospitals. By: Dr. Kevin Dolehide
 Management of Chronic Liver Failure/Cirrhosis Complications in Hospitals By: Dr. Kevin Dolehide Overview DX Cirrhosis and Prognosis Compensated Decompensated Complications Of Cirrhosis Management Of Complications
Management of Chronic Liver Failure/Cirrhosis Complications in Hospitals By: Dr. Kevin Dolehide Overview DX Cirrhosis and Prognosis Compensated Decompensated Complications Of Cirrhosis Management Of Complications
CHAPTER 1. Alcoholic Liver Disease
 CHAPTER 1 Alcoholic Liver Disease Major Lesions of Alcoholic Liver Disease Alcoholic fatty liver - >90% of binge and chronic drinkers Alcoholic hepatitis precursor of cirrhosis Alcoholic cirrhosis end
CHAPTER 1 Alcoholic Liver Disease Major Lesions of Alcoholic Liver Disease Alcoholic fatty liver - >90% of binge and chronic drinkers Alcoholic hepatitis precursor of cirrhosis Alcoholic cirrhosis end
Steps in Assessing Fibrosis 4/30/2015. Overview of Liver Disease Associated With HCV
 Overview of Liver Disease Associated With HCV Marion G. Peters, MD John V. Carbone, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California San Francisco San Francisco,
Overview of Liver Disease Associated With HCV Marion G. Peters, MD John V. Carbone, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California San Francisco San Francisco,
Treating patients with end-stage liver disease: Are we ready? Dr. Mino R. Mitri, M.D., C.M., M.Ed., FRCPC
 Treating patients with end-stage liver disease: Are we ready? Dr. Mino R. Mitri, M.D., C.M., M.Ed., FRCPC mino.mitri@ubc.ca No Conflict of Interest 157 patients 157 patients 6 transplanted Criteria Liver
Treating patients with end-stage liver disease: Are we ready? Dr. Mino R. Mitri, M.D., C.M., M.Ed., FRCPC mino.mitri@ubc.ca No Conflict of Interest 157 patients 157 patients 6 transplanted Criteria Liver
Definition: fibrosis and nodular regeneration resulting from hepatocellular injury
 Cirrhosis Understanding the liver: Patterns of LFT Abnormalities - Hepatocellular/Transaminitis: o Ratio of AST: ALT >2:1 ETOH (keep in mind AST is also produced by red cells, heart muscle) o If Aminotransferases
Cirrhosis Understanding the liver: Patterns of LFT Abnormalities - Hepatocellular/Transaminitis: o Ratio of AST: ALT >2:1 ETOH (keep in mind AST is also produced by red cells, heart muscle) o If Aminotransferases
Chronic Hepatic Disease
 Chronic Hepatic Disease 10 th Leading Cause of Death Liver Functions Energy Metabolism Protein Synthesis Solubilization, Transport, and Storage Protects and Clears drugs, damaged cells Causes of Liver
Chronic Hepatic Disease 10 th Leading Cause of Death Liver Functions Energy Metabolism Protein Synthesis Solubilization, Transport, and Storage Protects and Clears drugs, damaged cells Causes of Liver
EDUCATION PRACTICE. Management of Refractory Ascites. Clinical Scenario. The Problem
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2005;3:1187 1191 EDUCATION PRACTICE Management of Refractory Ascites ANDRÉS CÁRDENAS and PERE GINÈS Liver Unit, Institute of Digestive Diseases, Hospital Clínic,
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2005;3:1187 1191 EDUCATION PRACTICE Management of Refractory Ascites ANDRÉS CÁRDENAS and PERE GINÈS Liver Unit, Institute of Digestive Diseases, Hospital Clínic,
Etiology of liver cirrhosis
 Liver cirrhosis 1 Liver cirrhosis Liver cirrhosis is the progressive replacement of normal hepatic cells by fibrous scar tissue, This scarring is accompanied by the loss of viable hepatocytes, which are
Liver cirrhosis 1 Liver cirrhosis Liver cirrhosis is the progressive replacement of normal hepatic cells by fibrous scar tissue, This scarring is accompanied by the loss of viable hepatocytes, which are
End-Stage Liver Disease (ESLD): A Guide for HIV Physicians
: A Guide for HIV Physicians") Slide 1 of 32 End-Stage Liver Disease (ESLD): A Guide for HIV Physicians Marion G. Peters, MD John V. Carbone, MD, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California
Slide 1 of 32 End-Stage Liver Disease (ESLD): A Guide for HIV Physicians Marion G. Peters, MD John V. Carbone, MD, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California
The Continuum of Care for Advanced Liver Disease: Partnering with the Liver Specialist. K V Speeg, MD, PhD UT Health San Antonio
 The Continuum of Care for Advanced Liver Disease: Partnering with the Liver Specialist K V Speeg, MD, PhD UT Health San Antonio Objectives Review staging of liver disease Review consequences of end-stage
The Continuum of Care for Advanced Liver Disease: Partnering with the Liver Specialist K V Speeg, MD, PhD UT Health San Antonio Objectives Review staging of liver disease Review consequences of end-stage
ESLD a Guide for HIV Physicians. Marion Peters University of California San Francisco June 2015
 ESLD a Guide for HIV Physicians Marion Peters University of California San Francisco June 2015 Disclosures Honararia from Johnson and Johnson Roche Merck Gilead Spouse employee of Hoffman La Roche Natural
ESLD a Guide for HIV Physicians Marion Peters University of California San Francisco June 2015 Disclosures Honararia from Johnson and Johnson Roche Merck Gilead Spouse employee of Hoffman La Roche Natural
Approach to the Patient with Liver Disease
 Approach to the Patient with Liver Disease Diagnosis of liver disease Careful history taking Physical examination Laboratory tests Radiologic examination and imaging studies Liver biopsy Liver diseases
Approach to the Patient with Liver Disease Diagnosis of liver disease Careful history taking Physical examination Laboratory tests Radiologic examination and imaging studies Liver biopsy Liver diseases
PORTAL HYPERTENSION An Introduction to the Culprit of Many Liver Failure Complications
 PORTAL HYPERTENSION An Introduction to the Culprit of Many Liver Failure Complications Edy G. Trujillo, RN, MSN, ACNP-BC Liver Transplant RRUCLA Medical Center July 31, 2018 What Do We All Look Forward
PORTAL HYPERTENSION An Introduction to the Culprit of Many Liver Failure Complications Edy G. Trujillo, RN, MSN, ACNP-BC Liver Transplant RRUCLA Medical Center July 31, 2018 What Do We All Look Forward
Causes of Liver Disease in US
 Learning Objectives Updates in Outpatient Cirrhosis Management Jennifer Guy, MD MAS Director, Liver Cancer Program California Pacific Medical Center guyj@sutterhealth.org Review cirrhosis epidemiology,
Learning Objectives Updates in Outpatient Cirrhosis Management Jennifer Guy, MD MAS Director, Liver Cancer Program California Pacific Medical Center guyj@sutterhealth.org Review cirrhosis epidemiology,
Management of Cirrhosis Related Complications
 Management of Cirrhosis Related Complications Ke-Qin Hu, MD, FAASLD Professor of Clinical Medicine Director of Hepatology University of California, Irvine Disclosure I have no disclosure related to this
Management of Cirrhosis Related Complications Ke-Qin Hu, MD, FAASLD Professor of Clinical Medicine Director of Hepatology University of California, Irvine Disclosure I have no disclosure related to this
Liver Failure. The most severe clinical consequence of liver disease is liver failure:
 Liver diseases I The major primary diseases of the liver are: - Viral hepatitis, - Nonalcoholic fatty liver disease (NAFLD), - Alcoholic liver disease, - Hepatocellular carcinoma (HCC) Hepatic damage also
Liver diseases I The major primary diseases of the liver are: - Viral hepatitis, - Nonalcoholic fatty liver disease (NAFLD), - Alcoholic liver disease, - Hepatocellular carcinoma (HCC) Hepatic damage also
Complications of Cirrhosis
 Complications of Cirrhosis Causes of Cirrhosis Alcohol Chronic Viral Hepatitis (B/C) Haemochromatosis Autoimmune Hepatitis NAFLD/NASH Primary Biliary Cirrhosis Primary Sclerosing Cholangitis 1-AT deficiency
Complications of Cirrhosis Causes of Cirrhosis Alcohol Chronic Viral Hepatitis (B/C) Haemochromatosis Autoimmune Hepatitis NAFLD/NASH Primary Biliary Cirrhosis Primary Sclerosing Cholangitis 1-AT deficiency
Conflict of interest disclosures. Complications of end stage liver disease. None. The many complications of Cirrhosis. Portal Hypertension.
 Complications of end stage liver disease Conflict of interest disclosures None Amir Qamar, MD Instructor of Medicine Brigham and Women s s Hospital Harvard Medical School Boston, MA 02115 The many complications
Complications of end stage liver disease Conflict of interest disclosures None Amir Qamar, MD Instructor of Medicine Brigham and Women s s Hospital Harvard Medical School Boston, MA 02115 The many complications
following the last documented transfusion; thereafter, evaluate the residual impairment(s).
.") Adult Listings 5.01 Category of Impairments, Digestive System 5.02 Gastrointestinal hemorrhaging from any cause, requiring blood transfusion (with or without hospitalization) of at least 2 units of blood
Adult Listings 5.01 Category of Impairments, Digestive System 5.02 Gastrointestinal hemorrhaging from any cause, requiring blood transfusion (with or without hospitalization) of at least 2 units of blood
COMPLICATIONS OF CIRRHOSIS: ASCITES & HEPATIC ENCEPHALOPATHY
 COMPLICATIONS OF CIRRHOSIS: ASCITES & HEPATIC ENCEPHALOPATHY DR. ESTER YAGUDAYEVA CLINICAL PHARMACIST HOSPICE PHARMACY SOLUTIONS OBJECTIVES Understand the prognosis of End Stage Liver Disease (ESLD) Identify
COMPLICATIONS OF CIRRHOSIS: ASCITES & HEPATIC ENCEPHALOPATHY DR. ESTER YAGUDAYEVA CLINICAL PHARMACIST HOSPICE PHARMACY SOLUTIONS OBJECTIVES Understand the prognosis of End Stage Liver Disease (ESLD) Identify
Faculty Disclosure. Objectives. Cirrhosis Management for the Family Physician 18/11/2014
 Cirrhosis Management for the Family Physician Mang Ma, MD, FRCP Professor University of Alberta Faculty: Mang Ma Faculty Disclosure Relationships with commercial interests: Advisory Board: Merck, Gilead
Cirrhosis Management for the Family Physician Mang Ma, MD, FRCP Professor University of Alberta Faculty: Mang Ma Faculty Disclosure Relationships with commercial interests: Advisory Board: Merck, Gilead
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A ACLF. See Acute-on-chronic liver failure (ACLF) Acute kidney injury (AKI) in ACLF patients, 967 Acute liver failure (ALF), 957 964 causes
Index Note: Page numbers of article titles are in boldface type. A ACLF. See Acute-on-chronic liver failure (ACLF) Acute kidney injury (AKI) in ACLF patients, 967 Acute liver failure (ALF), 957 964 causes
DISEASE LEVEL MEDICAL EVIDENCE PROTOCOL
 DISEASE LEVEL MEDICAL EVIDENCE PROTOCOL 1. This Protocol sets out the medical evidence that must be delivered to the Administrator for proof of Disease Level. It is subject to such further and other Protocols
DISEASE LEVEL MEDICAL EVIDENCE PROTOCOL 1. This Protocol sets out the medical evidence that must be delivered to the Administrator for proof of Disease Level. It is subject to such further and other Protocols
WEEK. MPharm Programme. Liver Biochemistry. Slide 1 of 49 MPHM14 Liver Biochemistry
 MPharm Programme Liver Biochemistry Slide 1 of 49 MPHM Liver Biochemistry Learning Outcomes Assess and evaluate the signs and symptoms of illness Assess and critically appraise a patients medication regimen,
MPharm Programme Liver Biochemistry Slide 1 of 49 MPHM Liver Biochemistry Learning Outcomes Assess and evaluate the signs and symptoms of illness Assess and critically appraise a patients medication regimen,
Ascites Management. Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology
 Ascites Management Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Disclosure 1. The speaker Atif Zaman, MD MPH have no relevant
Ascites Management Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Disclosure 1. The speaker Atif Zaman, MD MPH have no relevant
Decompensated chronic liver disease
 Decompensated chronic liver disease Definition of decompensated chronic liver disease Patients with chronic liver disease can present with acute decompensation due to various causes. The decompensation
Decompensated chronic liver disease Definition of decompensated chronic liver disease Patients with chronic liver disease can present with acute decompensation due to various causes. The decompensation
PORTAL HYPERTENSION. Tianjin Medical University LIU JIAN
 PORTAL HYPERTENSION Tianjin Medical University LIU JIAN DEFINITION Portal hypertension is present if portal venous pressure exceeds 10mmHg (1.3kPa). Normal portal venous pressure is 5 10mmHg (0.7 1.3kPa),
PORTAL HYPERTENSION Tianjin Medical University LIU JIAN DEFINITION Portal hypertension is present if portal venous pressure exceeds 10mmHg (1.3kPa). Normal portal venous pressure is 5 10mmHg (0.7 1.3kPa),
LIVER CIRRHOSIS. The liver extracts nutrients from the blood and processes them for later use.
 LIVER CIRRHOSIS William Sanchez, M.D. & Jayant A. Talwalkar, M.D., M.P.H. Advanced Liver Disease Study Group Miles and Shirley Fiterman Center for Digestive Diseases Mayo College of Medicine Rochester,
LIVER CIRRHOSIS William Sanchez, M.D. & Jayant A. Talwalkar, M.D., M.P.H. Advanced Liver Disease Study Group Miles and Shirley Fiterman Center for Digestive Diseases Mayo College of Medicine Rochester,
Tranjugular Intrahepatic Portosystemic Shunt
 Tranjugular Intrahepatic Portosystemic Shunt Christopher Selhorst July 25, 2005 BIDMC Radiology Overview Portal Hypertension Indications, Contraindications The Procedure Case Review Complications Outcomes
Tranjugular Intrahepatic Portosystemic Shunt Christopher Selhorst July 25, 2005 BIDMC Radiology Overview Portal Hypertension Indications, Contraindications The Procedure Case Review Complications Outcomes
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acute variceal bleeding management of, 251 262 balloon tamponade of esophagus in, 257 258 endoscopic therapies in, 255 257. See also Endoscopy,
Index Note: Page numbers of article titles are in boldface type. A Acute variceal bleeding management of, 251 262 balloon tamponade of esophagus in, 257 258 endoscopic therapies in, 255 257. See also Endoscopy,
Management of Ascites and Hepatorenal Syndrome. Florence Wong University of Toronto. June 4, /16/ Gore & Associates: Consultancy
 Management of Ascites and Hepatorenal Syndrome Florence Wong University of Toronto June 4, 2016 6/16/2016 1 Disclosures Gore & Associates: Consultancy Sequana Medical: Research Funding Mallinckrodt Pharmaceutical:
Management of Ascites and Hepatorenal Syndrome Florence Wong University of Toronto June 4, 2016 6/16/2016 1 Disclosures Gore & Associates: Consultancy Sequana Medical: Research Funding Mallinckrodt Pharmaceutical:
DISCLOSURES. This activity is jointly provided by Northwest Portland Area Indian Health Board and Cardea
 DISCLOSURES This activity is jointly provided by Northwest Portland Area Indian Health Board and Cardea Cardea Services is approved as a provider of continuing nursing education by Montana Nurses Association,
DISCLOSURES This activity is jointly provided by Northwest Portland Area Indian Health Board and Cardea Cardea Services is approved as a provider of continuing nursing education by Montana Nurses Association,
Contraindications. Indications. Complications. Currently TIPS is considered second or third line therapy for:
 Contraindications Absolute Relative Primary prevention variceal bleeding HCC if centrally located Active congestive heart failure Obstruction all hepatic veins Thomas D. Boyer, M.D. University of Arizona
Contraindications Absolute Relative Primary prevention variceal bleeding HCC if centrally located Active congestive heart failure Obstruction all hepatic veins Thomas D. Boyer, M.D. University of Arizona
CIRRHOSIS Definition
 Cirrhosis Update Robert S. Brown, Jr., MD, MPH Vice Chair, Transitions of Care Interim Chief, Division of Gastroenterology & Hepatology Weill Cornell Medical College CIRRHOSIS Definition Irreversible fibrous
Cirrhosis Update Robert S. Brown, Jr., MD, MPH Vice Chair, Transitions of Care Interim Chief, Division of Gastroenterology & Hepatology Weill Cornell Medical College CIRRHOSIS Definition Irreversible fibrous
Virtual Mentor American Medical Association Journal of Ethics December 2008, Volume 10, Number 12:
 Virtual Mentor American Medical Association Journal of Ethics December 2008, Volume 10, Number 12: 805-809. CLINICAL PEARL Indications for Use of TIPS in Treating Portal Hypertension Elizabeth C. Verna,
Virtual Mentor American Medical Association Journal of Ethics December 2008, Volume 10, Number 12: 805-809. CLINICAL PEARL Indications for Use of TIPS in Treating Portal Hypertension Elizabeth C. Verna,
Cirrhosis Patient Teaching Information
 Cirrhosis Patient Teaching Information CIRRHOSIS What is Cirrhosis: Cirrhosis is the end stages of a liver disease. Over time, from years to decades, fibrosis (or scar tissue) progresses through stages
Cirrhosis Patient Teaching Information CIRRHOSIS What is Cirrhosis: Cirrhosis is the end stages of a liver disease. Over time, from years to decades, fibrosis (or scar tissue) progresses through stages
What Is Cirrhosis? CIRRHOSIS. Cirrhosis occurs when the liver is. by chronic conditions and diseases. permanently scarred or injured
 What Is Cirrhosis? Cirrhosis occurs when the liver is permanently scarred or injured by chronic conditions and diseases. Common causes of cirrhosis include: Long-term alcohol abuse. Chronic viral hepatitis
What Is Cirrhosis? Cirrhosis occurs when the liver is permanently scarred or injured by chronic conditions and diseases. Common causes of cirrhosis include: Long-term alcohol abuse. Chronic viral hepatitis
Module 1 Introduction of hepatitis
 Module 1 Introduction of hepatitis 1 Training Objectives At the end of the module, trainees will be able to ; Demonstrate improved knowledge of the global epidemiology of the viral hepatitis Understand
Module 1 Introduction of hepatitis 1 Training Objectives At the end of the module, trainees will be able to ; Demonstrate improved knowledge of the global epidemiology of the viral hepatitis Understand
Management of Cirrhotic Complications Uncontrolled Ascites. Siwaporn Chainuvati, MD Siriraj Hospital Mahidol University
 Management of Cirrhotic Complications Uncontrolled Ascites Siwaporn Chainuvati, MD Siriraj Hospital Mahidol University Topic Definition, pathogenesis Current therapeutic options Experimental treatments
Management of Cirrhotic Complications Uncontrolled Ascites Siwaporn Chainuvati, MD Siriraj Hospital Mahidol University Topic Definition, pathogenesis Current therapeutic options Experimental treatments
Nursing Care & Management of the Pre-Liver Transplant Population. Christine Kiamzon, RN, MSN, PCCN 8 North Educator
 Nursing Care & Management of the Pre-Liver Transplant Population Christine Kiamzon, RN, MSN, PCCN 8 North Educator Objectives 1. Identify key nursing interventions in caring for pre-transplant ESLD patients.
Nursing Care & Management of the Pre-Liver Transplant Population Christine Kiamzon, RN, MSN, PCCN 8 North Educator Objectives 1. Identify key nursing interventions in caring for pre-transplant ESLD patients.
Nursing Care & Management of the Pre-Liver Transplant Population
 Nursing Care & Management of the Pre-Liver Transplant Population Christine Kiamzon, RN, MSN, PCCN 8 North Educator Objectives 1. Identify key nursing interventions in caring for pre-transplant ESLD patients.
Nursing Care & Management of the Pre-Liver Transplant Population Christine Kiamzon, RN, MSN, PCCN 8 North Educator Objectives 1. Identify key nursing interventions in caring for pre-transplant ESLD patients.
The Yellow Patient. Dr Chiradeep Raychaudhuri, Consultant Hepatologist, Hull University Teaching Hospitals NHS Trust
 The Yellow Patient Dr Chiradeep Raychaudhuri, Consultant Hepatologist, Hull University Teaching Hospitals NHS Trust there s a yellow patient in bed 40. It s one of yours. Liver Cirrhosis Why.When.What.etc.
The Yellow Patient Dr Chiradeep Raychaudhuri, Consultant Hepatologist, Hull University Teaching Hospitals NHS Trust there s a yellow patient in bed 40. It s one of yours. Liver Cirrhosis Why.When.What.etc.
Renal Care and Liver Disease: Disease Trajectory and Hospice Eligibility
 Renal Care and Liver Disease: Disease Trajectory and Hospice Eligibility Terri L. Maxwell PhD, APRN VP, Strategic Initiatives Weatherbee Resources/HEN Course Materials & Disclosure Course materials including
Renal Care and Liver Disease: Disease Trajectory and Hospice Eligibility Terri L. Maxwell PhD, APRN VP, Strategic Initiatives Weatherbee Resources/HEN Course Materials & Disclosure Course materials including
Diagnostic Procedures. Measurement of Hepatic venous pressure in management of cirrhosis. Clinician s opinion
 5 th AISF Post-Meeting Course Diagnostic and Therapeutic Invasive Procedures in Hepatology Rome, February 25 th Diagnostic Procedures Measurement of Hepatic venous pressure in management of cirrhosis Clinician
5 th AISF Post-Meeting Course Diagnostic and Therapeutic Invasive Procedures in Hepatology Rome, February 25 th Diagnostic Procedures Measurement of Hepatic venous pressure in management of cirrhosis Clinician
Liver Diseases. Yasmine Lashine MD, PhD
 Liver Diseases Yasmine Lashine MD, PhD ILOs Recognize different causes of Live failure Recall and understand clinical picture and complication of Liver failure Discuss causes and clinical picture of hepatic
Liver Diseases Yasmine Lashine MD, PhD ILOs Recognize different causes of Live failure Recall and understand clinical picture and complication of Liver failure Discuss causes and clinical picture of hepatic
Hepatocytes produce. Proteins Clotting factors Hormones. Bile Flow
 R.J.Bailey MD Hepatocytes produce Proteins Clotting factors Hormones Bile Flow Trouble.. for the liver! Trouble for the Liver Liver Gall Bladder Common Alcohol Hep C Fatty Liver Cancer Drugs Viruses Uncommon
R.J.Bailey MD Hepatocytes produce Proteins Clotting factors Hormones Bile Flow Trouble.. for the liver! Trouble for the Liver Liver Gall Bladder Common Alcohol Hep C Fatty Liver Cancer Drugs Viruses Uncommon
Learning Objectives. After attending this presentation, participants will be able to:
 Learning Objectives After attending this presentation, participants will be able to: Describe HCV in 2015 Describe how to diagnose advanced liver disease and cirrhosis Identify the clinical presentation
Learning Objectives After attending this presentation, participants will be able to: Describe HCV in 2015 Describe how to diagnose advanced liver disease and cirrhosis Identify the clinical presentation
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Accelerated intravascular coagulation and fibrinolysis (AICF) in liver disease, 390 391 Acid suppression in liver disease, 403 404 ACLF.
Index Note: Page numbers of article titles are in boldface type. A Accelerated intravascular coagulation and fibrinolysis (AICF) in liver disease, 390 391 Acid suppression in liver disease, 403 404 ACLF.
CLINICAL How Should a Hospitalized Patient with Newly Diagnosed Cirrhosis Be Evaluated and Managed?
 CLINICAL How Should a Hospitalized Patient with Newly Diagnosed Cirrhosis Be Evaluated and Managed? The Hospitalist. 2016 August;2016(8) Author(s): Raj Sehgal, MD; Joshua Hanson, MD, MPH; Division OF The
CLINICAL How Should a Hospitalized Patient with Newly Diagnosed Cirrhosis Be Evaluated and Managed? The Hospitalist. 2016 August;2016(8) Author(s): Raj Sehgal, MD; Joshua Hanson, MD, MPH; Division OF The
A Review of Liver Function Tests. James Gray Gastroenterology Vancouver
 A Review of Liver Function Tests James Gray Gastroenterology Vancouver Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
A Review of Liver Function Tests James Gray Gastroenterology Vancouver Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Denver Shunts vs TIPS for Ascites
 Denver Shunts vs TIPS for Ascites Hooman Yarmohammadi MD Assistant Professor of Radiology Interventional Radiology & Image Guided Therapies Memorial Sloan-Kettering Cancer Center, New York, USA Hooman
Denver Shunts vs TIPS for Ascites Hooman Yarmohammadi MD Assistant Professor of Radiology Interventional Radiology & Image Guided Therapies Memorial Sloan-Kettering Cancer Center, New York, USA Hooman
Podcast (Video Recorded Lecture Series): Portal HTN and Derivatives for the USMLE Step One Exam. Ultrasound (w/ doppler) Reversal of flow Portal Vein
: Portal HTN and Derivatives for the USMLE Step One Exam. Ultrasound (w/ doppler) Reversal of flow Portal Vein") Podcast (Video Recorded Lecture Series): Portal HTN and Derivatives for the USMLE Step One Exam Hepatic Vein (Budd Chiari) Ultrasound (w/ doppler) Reversal of flow Portal Vein Howard J. Sachs, MD www.12daysinmarch.com
Podcast (Video Recorded Lecture Series): Portal HTN and Derivatives for the USMLE Step One Exam Hepatic Vein (Budd Chiari) Ultrasound (w/ doppler) Reversal of flow Portal Vein Howard J. Sachs, MD www.12daysinmarch.com
Esophageal Varices Beta-Blockers or Band Ligation. Cesar Yaghi MD Hotel-Dieu de France University Hospital Universite Saint Joseph
 Esophageal Varices Beta-Blockers or Band Ligation Cesar Yaghi MD Hotel-Dieu de France University Hospital Universite Saint Joseph Esophageal Varices Beta-Blockers or Band Ligation? Risk of esophageal variceal
Esophageal Varices Beta-Blockers or Band Ligation Cesar Yaghi MD Hotel-Dieu de France University Hospital Universite Saint Joseph Esophageal Varices Beta-Blockers or Band Ligation? Risk of esophageal variceal
The Liver for the Nonhepatologist
 The Liver for the Nonhepatologist Michael R. Charlton, MBBS, FRCP Professor of Medicine University of Chicago Chicago, Illinois Overview Initial assessment of liver disease How do you diagnose cirrhosis?
The Liver for the Nonhepatologist Michael R. Charlton, MBBS, FRCP Professor of Medicine University of Chicago Chicago, Illinois Overview Initial assessment of liver disease How do you diagnose cirrhosis?
Alpha-1 Antitrypsin Deficiency: Liver Disease
 Alpha-1 Antitrypsin Deficiency: Liver Disease Who is at risk to develop Alpha-1 liver disease? Alpha-1 liver disease may affect children and adults who have abnormal Alpha-1 antitrypsin genes. Keys to
Alpha-1 Antitrypsin Deficiency: Liver Disease Who is at risk to develop Alpha-1 liver disease? Alpha-1 liver disease may affect children and adults who have abnormal Alpha-1 antitrypsin genes. Keys to
Ask the Experts Patient Education Program. Understanding the Progression of Liver Disease: Fibrosis
 J. Clint Stanfill, MD April 24, 2018 Ask the Experts Patient Education Program Understanding the Progression of Liver Disease: Fibrosis Fibrosis -replacement of normal liver -reactive phenomenon - stronger
J. Clint Stanfill, MD April 24, 2018 Ask the Experts Patient Education Program Understanding the Progression of Liver Disease: Fibrosis Fibrosis -replacement of normal liver -reactive phenomenon - stronger
The Management of Ascites & Hepatorenal Syndrome. Florence Wong University of Toronto. Falk Symposium March 14, 2008
 The Management of Ascites & Hepatorenal Syndrome Florence Wong University of Toronto Falk Symposium March 14, 2008 Management of Ascites Sodium Restriction Mandatory at all stages of ascites in order to
The Management of Ascites & Hepatorenal Syndrome Florence Wong University of Toronto Falk Symposium March 14, 2008 Management of Ascites Sodium Restriction Mandatory at all stages of ascites in order to
PALLIATIVE CARE IN END-STAGE LIVER DISEASE
 PALLIATIVE CARE IN END-STAGE LIVER DISEASE Ken S. Ota, DO Family Medicine Banner Good Samaritan Medical Center Learning Objectives: Describe the common bio-psycho-social issues in end-stage liver disease
PALLIATIVE CARE IN END-STAGE LIVER DISEASE Ken S. Ota, DO Family Medicine Banner Good Samaritan Medical Center Learning Objectives: Describe the common bio-psycho-social issues in end-stage liver disease
Ontario s Adult Referral and Listing Criteria for Liver Transplantation
 Ontario s Adult Referral and Listing Criteria for Liver Transplantation Version 3.0 Trillium Gift of Life Network Ontario s Adult Referral & Listing Criteria for Liver Transplantation PATIENT REFERRAL
Ontario s Adult Referral and Listing Criteria for Liver Transplantation Version 3.0 Trillium Gift of Life Network Ontario s Adult Referral & Listing Criteria for Liver Transplantation PATIENT REFERRAL
Jaundice. Agnieszka Dobrowolska- Zachwieja, MD, PhD
 Jaundice Agnieszka Dobrowolska- Zachwieja, MD, PhD Jaundice definition Jaundice, as in the French jaune, refers to the yellow discoloration of the skin. It arises from the abnormal accumulation of bilirubin
Jaundice Agnieszka Dobrowolska- Zachwieja, MD, PhD Jaundice definition Jaundice, as in the French jaune, refers to the yellow discoloration of the skin. It arises from the abnormal accumulation of bilirubin
CHAPTER 7. End Stage Liver Disease in the ICU: Walking a Tightrope. Lynn A. Kelso, MSN, APRN, FCCM, FAANP University of Kentucky College of Nursing
 CHAPTER 7 End Stage Liver Disease in the ICU: Walking a Tightrope Lynn A. Kelso, MSN, APRN, FCCM, FAANP University of Kentucky College of Nursing Besey Oren, Assistant Professor Istanbul University Health
CHAPTER 7 End Stage Liver Disease in the ICU: Walking a Tightrope Lynn A. Kelso, MSN, APRN, FCCM, FAANP University of Kentucky College of Nursing Besey Oren, Assistant Professor Istanbul University Health
Cirrhosis of the Liver
 235 60th Street, West New York, NJ 07093 T: (201) 854-4646 F: (201) 854-4647 810 Main Street, Hackensack, NJ 07601 T: (201) 488-0095 Cirrhosis of the Liver The liver, the largest organ in the body, is
235 60th Street, West New York, NJ 07093 T: (201) 854-4646 F: (201) 854-4647 810 Main Street, Hackensack, NJ 07601 T: (201) 488-0095 Cirrhosis of the Liver The liver, the largest organ in the body, is
Management of the Cirrhotic Patient in the ICU
 Management of the Cirrhotic Patient in the ICU Peter E. Morris, MD Professor & Chief, Pulmonary, Critical Care and Sleep Medicine University of Kentucky Conflict of Interest Funding US National Institutes
Management of the Cirrhotic Patient in the ICU Peter E. Morris, MD Professor & Chief, Pulmonary, Critical Care and Sleep Medicine University of Kentucky Conflict of Interest Funding US National Institutes
Michele Bettinelli RN CCRN Lahey Health and Medical Center
 Michele Bettinelli RN CCRN Lahey Health and Medical Center Differentiate the types of varices Identify glue preparations utilized when treating gastric varices Review the process of glue administration
Michele Bettinelli RN CCRN Lahey Health and Medical Center Differentiate the types of varices Identify glue preparations utilized when treating gastric varices Review the process of glue administration
Life After SVR for Cirrhotic HCV
 Life After SVR for Cirrhotic HCV KIM NEWNHAM MN, NP CIRRHOSIS CARE CLINIC UNIVERSITY OF ALBERTA Objectives To review the benefits of HCV clearance in cirrhotic patients To review some of the emerging data
Life After SVR for Cirrhotic HCV KIM NEWNHAM MN, NP CIRRHOSIS CARE CLINIC UNIVERSITY OF ALBERTA Objectives To review the benefits of HCV clearance in cirrhotic patients To review some of the emerging data
The Liver for the Nonhepatologist
 The Liver for the Nonhepatologist Michael R. Charlton, MBBS, FRCP Hepatology Director and Medical Director of Liver Transplantation Intermountain Medical Center Salt Lake City, Utah FORMATTED: 05-14-15
The Liver for the Nonhepatologist Michael R. Charlton, MBBS, FRCP Hepatology Director and Medical Director of Liver Transplantation Intermountain Medical Center Salt Lake City, Utah FORMATTED: 05-14-15
VARICEAL BLEEDING. Ram Subramanian MD Hepatology & Critical Care Medical Director of Liver Transplant Emory University, Atlanta.
 VARICEAL BLEEDING Ram Subramanian MD Hepatology & Critical Care Medical Director of Liver Transplant Emory University, Atlanta Disclosures: None OUTLINE Pathophysiology of portal hypertension Splanchnic
VARICEAL BLEEDING Ram Subramanian MD Hepatology & Critical Care Medical Director of Liver Transplant Emory University, Atlanta Disclosures: None OUTLINE Pathophysiology of portal hypertension Splanchnic
Management of Hepatic Encephalopathy
 Management of Hepatic Encephalopathy Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Disclosure 1. The speaker Atif Zaman, MD MPH
Management of Hepatic Encephalopathy Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Disclosure 1. The speaker Atif Zaman, MD MPH
Current Liver Allocation Policies
 C Current Liver Allocation Policies Policy 3.6 Organ Distribution 3.6 Allocation of Livers. Unless otherwise approved according to Policies 3.1.7 (Local and Alternative Local Unit), 3.1.8 (Sharing Arrangement
C Current Liver Allocation Policies Policy 3.6 Organ Distribution 3.6 Allocation of Livers. Unless otherwise approved according to Policies 3.1.7 (Local and Alternative Local Unit), 3.1.8 (Sharing Arrangement
Ascites. Matthew Johnson M.D.
 Ascites Matthew Johnson M.D. The most common complication of portal hypertension 50% of patients who have compensated cirrhosis develop ascites by 10 years Survival after ascites develops: 1-year: 85%
Ascites Matthew Johnson M.D. The most common complication of portal hypertension 50% of patients who have compensated cirrhosis develop ascites by 10 years Survival after ascites develops: 1-year: 85%
Course Handouts & Post Test
 End Stage Liver Disease (ESLD) End Stage Renal Disease (ESRD) Disease Trajectory and Hospice Eligibility Terri Maxwell PhD, APRN VP, Strategic Initiatives Weatherbee Resources Inc. & Hospice Education
End Stage Liver Disease (ESLD) End Stage Renal Disease (ESRD) Disease Trajectory and Hospice Eligibility Terri Maxwell PhD, APRN VP, Strategic Initiatives Weatherbee Resources Inc. & Hospice Education
Use of transjugular intrahepatic portosystemic shunt in liver disease
 Vol. XVIII No. 3 JOURNAL OF VASCULAR NURSING PAGE 83 Use of transjugular intrahepatic portosystemic shunt in liver disease Patricia Ann Radovich, RN, MSN, CCRN, FCCM Persons with cirrhosis have many complications.
Vol. XVIII No. 3 JOURNAL OF VASCULAR NURSING PAGE 83 Use of transjugular intrahepatic portosystemic shunt in liver disease Patricia Ann Radovich, RN, MSN, CCRN, FCCM Persons with cirrhosis have many complications.
Hepatic Encephalopathy
 Hepatic Encephalopathy John Barber UMassMedical Student, Class of 2019 www.12daysinmarch.com Outline Overview Normal Physiology Pathology Symptoms Diagnosis Treatment Overview Ammonia (NH 3 ) is a byproduct
Hepatic Encephalopathy John Barber UMassMedical Student, Class of 2019 www.12daysinmarch.com Outline Overview Normal Physiology Pathology Symptoms Diagnosis Treatment Overview Ammonia (NH 3 ) is a byproduct
Portal hypertension and ascites
 Portal hypertension and ascites Muhammad S Mirza Guruprasad P Aithal Abstract Portal pressure is the product of portal blood flow and resistance; an increase in either leads to increased portal pressure.
Portal hypertension and ascites Muhammad S Mirza Guruprasad P Aithal Abstract Portal pressure is the product of portal blood flow and resistance; an increase in either leads to increased portal pressure.
Management in Cirrhosis
 Management in Cirrhosis Outline Introduction Cause of cirrhosis and management General management in cirrhosis Management complication and surveillance Clue of Chronic Liver Disease and Cirrhosis Risk
Management in Cirrhosis Outline Introduction Cause of cirrhosis and management General management in cirrhosis Management complication and surveillance Clue of Chronic Liver Disease and Cirrhosis Risk
The Importance of Diagnosing Covert Hepatic Encephalopathy
 The Importance of Diagnosing Covert Hepatic Encephalopathy Program Disclosure This activity has been planned and implemented in accordance with the Essential Areas and Policies of the Accreditation Council
The Importance of Diagnosing Covert Hepatic Encephalopathy Program Disclosure This activity has been planned and implemented in accordance with the Essential Areas and Policies of the Accreditation Council
ABNORMAL LIVER FUNCTION TESTS. Dr Uthayanan Chelvaratnam Hepatology Consultant North Bristol NHS Trust
 ABNORMAL LIVER FUNCTION TESTS Dr Uthayanan Chelvaratnam Hepatology Consultant North Bristol NHS Trust INTRODUCTION Liver function tests Cases Non invasive fibrosis measurement Questions UK MORTALITY RATE
ABNORMAL LIVER FUNCTION TESTS Dr Uthayanan Chelvaratnam Hepatology Consultant North Bristol NHS Trust INTRODUCTION Liver function tests Cases Non invasive fibrosis measurement Questions UK MORTALITY RATE
Evaluation Process for Liver Transplant Candidates
 Evaluation Process for Liver Transplant Candidates 2 Objectives Identify components of the liver transplant referral to evaluation Describe the role of the liver transplant coordinator Describe selection
Evaluation Process for Liver Transplant Candidates 2 Objectives Identify components of the liver transplant referral to evaluation Describe the role of the liver transplant coordinator Describe selection
Management of Hepatitis C in Primary Care BABAFEMI ONABANJO, MD & BEN ALFRED, FNP UMASS FAMILY HEALTH CENTER WORCESTER
 Management of Hepatitis C in Primary Care BABAFEMI ONABANJO, MD & BEN ALFRED, FNP UMASS FAMILY HEALTH CENTER WORCESTER Objective Epidemiology Screening criteria Appropriate work up Treatment Guidelines
Management of Hepatitis C in Primary Care BABAFEMI ONABANJO, MD & BEN ALFRED, FNP UMASS FAMILY HEALTH CENTER WORCESTER Objective Epidemiology Screening criteria Appropriate work up Treatment Guidelines
CIRROSI E IPERTENSIONE PORTALE NELLA DONNA
 Cagliari, 16 settembre 2017 CIRROSI E IPERTENSIONE PORTALE NELLA DONNA Vincenza Calvaruso, MD, PhD Ricercatore di Gastroenterologia Gastroenterologia & Epatologia, Di.Bi.M.I.S. Università degli Studi di
Cagliari, 16 settembre 2017 CIRROSI E IPERTENSIONE PORTALE NELLA DONNA Vincenza Calvaruso, MD, PhD Ricercatore di Gastroenterologia Gastroenterologia & Epatologia, Di.Bi.M.I.S. Università degli Studi di
Managing Cirrhosis. Cirrhosis of the liver is a progressive, fibrosing. Ascites. By Cameron Ghent, MD, FRCPC. Complications of Cirrhosis
 Focus on CME at the University of Western Ontario Managing Cirrhosis By Cameron Ghent, MD, FRCPC Cirrhosis of the liver is a progressive, fibrosing process resulting in nodule formation and microvascular
Focus on CME at the University of Western Ontario Managing Cirrhosis By Cameron Ghent, MD, FRCPC Cirrhosis of the liver is a progressive, fibrosing process resulting in nodule formation and microvascular
MANAGEMENT OF ACUTE HEPATIC FAILURE
 MANAGEMENT OF ACUTE HEPATIC FAILURE -NEW CONCEPT PROF. DR.MD ZAKIR HOSSAIN PROFESSOR & HEAD DEPARTMENT OF MEDICINE RANGPUR MEDICAL COLLEGE & HOSPITAL Rangpur Medical College & Hospital Begum Rokeya Shakhawat
MANAGEMENT OF ACUTE HEPATIC FAILURE -NEW CONCEPT PROF. DR.MD ZAKIR HOSSAIN PROFESSOR & HEAD DEPARTMENT OF MEDICINE RANGPUR MEDICAL COLLEGE & HOSPITAL Rangpur Medical College & Hospital Begum Rokeya Shakhawat
Gastrointestinal System: Accessory Organ Disorders
 Gastrointestinal System: Accessory Organ Disorders Mary DeLetter, PhD, RN Associate Professor Dept. of Baccalaureate and Graduate Nursing Eastern Kentucky University Disorders of Accessory Organs Portal
Gastrointestinal System: Accessory Organ Disorders Mary DeLetter, PhD, RN Associate Professor Dept. of Baccalaureate and Graduate Nursing Eastern Kentucky University Disorders of Accessory Organs Portal
Assessment of Liver Function: Implications for HCC Treatment
 Assessment of Liver Function: Implications for HCC Treatment A/P Dan Yock Young MBBS, PhD, MRCP, MMed. FAMS Chair, University Medicine Cluster. NUHS Head, Department of Medicine, National University of
Assessment of Liver Function: Implications for HCC Treatment A/P Dan Yock Young MBBS, PhD, MRCP, MMed. FAMS Chair, University Medicine Cluster. NUHS Head, Department of Medicine, National University of
Interpreting Your Tests
 Interpreting Your Tests Lisa M. Forman, MD, MSCE Associate Professor of Medicine Section Hepatology and Liver Transplantation University of Colorado Denver Outline Bile Duct Anatomy Lab Tests LFTs Tumor
Interpreting Your Tests Lisa M. Forman, MD, MSCE Associate Professor of Medicine Section Hepatology and Liver Transplantation University of Colorado Denver Outline Bile Duct Anatomy Lab Tests LFTs Tumor
Hepatic dysfunction: Can we recognize it sooner? And intervene earlier
 Hepatic dysfunction: Can we recognize it sooner? And intervene earlier Juliet M.Lopez, M.D. Chief, General Surgery Division Raymond G Murphy Veterans Administration Medical Center, ABQ, NM Prometheus Hepatic
Hepatic dysfunction: Can we recognize it sooner? And intervene earlier Juliet M.Lopez, M.D. Chief, General Surgery Division Raymond G Murphy Veterans Administration Medical Center, ABQ, NM Prometheus Hepatic
King Abdul-Aziz University Hospital (KAUH) is a tertiary
 is a tertiary") Modelling Factors Causing Mortality in Oesophageal Varices Patients in King Abdul Aziz University Hospital Sami Bahlas Abstract Objectives: The objective of this study is to reach a model defining factors
Modelling Factors Causing Mortality in Oesophageal Varices Patients in King Abdul Aziz University Hospital Sami Bahlas Abstract Objectives: The objective of this study is to reach a model defining factors
Pretreatment Evaluation
 Pretreatment Evaluation Disclosures Research supported by Gilead Sciences Inc.: Site investigator for HIV/HCV SWITCH Registry Study Key personnel for FOCUS HCV Screening Program through Vanderbilt University
Pretreatment Evaluation Disclosures Research supported by Gilead Sciences Inc.: Site investigator for HIV/HCV SWITCH Registry Study Key personnel for FOCUS HCV Screening Program through Vanderbilt University
Hepatology for the Nonhepatologist
 Hepatology for the Nonhepatologist Kenneth E. Sherman, MD, PhD Gould Professor of Medicine Director, Division of Digestive Diseases University of Cincinnati College of Medicine Cincinnati, Ohio Learning
Hepatology for the Nonhepatologist Kenneth E. Sherman, MD, PhD Gould Professor of Medicine Director, Division of Digestive Diseases University of Cincinnati College of Medicine Cincinnati, Ohio Learning
4/3/2014. Elizabeth Thompson, PharmD April Understand the importance of the liver and basic physiology.
 Liver Disease Elizabeth Thompson, PharmD thompse@sarmc.org April 2014 Objectives Understand the importance of the liver and basic physiology. Review hepatic disorders Recognize liver function scoring systems
Liver Disease Elizabeth Thompson, PharmD thompse@sarmc.org April 2014 Objectives Understand the importance of the liver and basic physiology. Review hepatic disorders Recognize liver function scoring systems
Complications of Cirrhosis
 What is Cirrhosis? Complications of Cirrhosis Paul J. Gaglio, MD Center for Liver Disease and Transplantation Columbia University College of Physicians and Surgeons NAFLD 1 PHYSICAL EXAM FINDINGS Decreased
What is Cirrhosis? Complications of Cirrhosis Paul J. Gaglio, MD Center for Liver Disease and Transplantation Columbia University College of Physicians and Surgeons NAFLD 1 PHYSICAL EXAM FINDINGS Decreased
Drug therapy in patient with hepatic impairment
 Drug therapy in patient with hepatic impairment Arzneimitteltherapie bei Leberinsuffizienz Dominik Wilke 03/04 Mai 2018 43. ADKA-Kongress, Stuttgart Functions of the Liver I Metabolism (Carbohydrates,
Drug therapy in patient with hepatic impairment Arzneimitteltherapie bei Leberinsuffizienz Dominik Wilke 03/04 Mai 2018 43. ADKA-Kongress, Stuttgart Functions of the Liver I Metabolism (Carbohydrates,
RISK STRATIFICATION IN CIRRHOSIS: FOCUS ON UMBILICAL HERNIA Sam Hawkins MD PGY5
 RISK STRATIFICATION IN CIRRHOSIS: FOCUS ON UMBILICAL HERNIA Sam Hawkins MD PGY5 PATIENT PRESENTATION 73M w/ Hep B Cirrhosis, HTN, DM II Liver disease followed at OSH x2 years (when moved from China), on
RISK STRATIFICATION IN CIRRHOSIS: FOCUS ON UMBILICAL HERNIA Sam Hawkins MD PGY5 PATIENT PRESENTATION 73M w/ Hep B Cirrhosis, HTN, DM II Liver disease followed at OSH x2 years (when moved from China), on
ACG & AASLD Joint Clinical Guideline: Prevention and Management of Gastroesophageal Varices and Variceal Hemorrhage in Cirrhosis
 ACG & AASLD Joint Clinical Guideline: Prevention and Management of Gastroesophageal Varices and Variceal Hemorrhage in Cirrhosis Guadalupe Garcia-Tsao, M.D., 1 Arun J. Sanyal, M.D., 2 Norman D. Grace,
ACG & AASLD Joint Clinical Guideline: Prevention and Management of Gastroesophageal Varices and Variceal Hemorrhage in Cirrhosis Guadalupe Garcia-Tsao, M.D., 1 Arun J. Sanyal, M.D., 2 Norman D. Grace,
GI bleeding in chronic liver disease
 GI bleeding in chronic liver disease Stuart McPherson Consultant Hepatologist Liver Unit, Freeman Hospital, Newcastle upon Tyne and Institute of Cellular Medicine, Newcastle University. Case 54 year old
GI bleeding in chronic liver disease Stuart McPherson Consultant Hepatologist Liver Unit, Freeman Hospital, Newcastle upon Tyne and Institute of Cellular Medicine, Newcastle University. Case 54 year old
Controversies in Management of Portal Hypertension and Cirrhosis Complications in the Transplant Candidate
 Controversies in Management of Portal Hypertension and Cirrhosis Complications in the Transplant Candidate Patrick Northup, MD, FAASLD, FACG Medical Director, Liver Transplantation University of Virginia
Controversies in Management of Portal Hypertension and Cirrhosis Complications in the Transplant Candidate Patrick Northup, MD, FAASLD, FACG Medical Director, Liver Transplantation University of Virginia