12 July Barbara Wismer, MD, MPH Tom Waddell Health Center San Francisco Department of Public Health
|
|
|
- Alfred Shelton
- 5 years ago
- Views:
Transcription


1 12 July 2012 Barbara Wismer, MD, MPH Tom Waddell Health Center San Francisco Department of Public Health


2 It s in the literature It s in the news It s on our minds

3 } HCH Clinicians Network priority } National survey of HCH clinicians in 2010 (n=101) } Results showed clinicians: Lacked resources for optimal pain management Lacked access to non-pharmacologic pain interventions Were uncomfortable prescribing opioids, especially if substance use disorders Found successful pain management gratifying


4 What are your thoughts + feelings about working with patients who have chronic pain?

5 Provide framework + tools for evaluation + management of chronic pain Functional goals Multimodal treatment Universal precautions Provide recommendations for practice adaptations for patients experiencing homelessness
![} [T]he magnitude of the pain suffered by individuals and the associated costs constitute a crisis for America, both human and economic.](/docs-images/89/98362092/images/6-2.jpg "[A]pproaching pain at both the individual and the broader population levels will require a transformation in how Americans think and act individually and collectively regarding pain and suffering.")
6 } [T]he magnitude of the pain suffered by individuals and the associated costs constitute a crisis for America, both human and economic. [A]pproaching pain at both the individual and the broader population levels will require a transformation in how Americans think and act individually and collectively regarding pain and suffering. [T]his transformation represents a moral and national imperative.
7 } Why do we need a cultural transformation? Mismatch between knowledge + application Focus is on diagnostic tests + medical treatment rather than interdisciplinary, biopsychosocial approaches to address psychological (emotional + cognitive) effects Patients have important role to play (self management) Pain not recognized as a serious disease in itself to be treated directly + worthy or research
8 } Pain is a public health issue Affects ~100 million adults Reduces quality of life Affects different groups disparately Costs $ billion annually Can be addressed by public health interventions More consistent data collection Public education
9 Rates* of opioid pain reliever (OPR) overdose death, OPR treatment admissions, and kilograms of OPR sold --- United States, *Age-adjusted rates per 100,000 population for OPR deaths, crude rates per 10,000 population for OPR abuse treatment admissions, and crude rates per 10,000 population for kilograms of OPR sold. Paulozzi LJ, et al. Overdoses of Prescription Opioid Pain Relievers United States, MMWR (2010):87-92.
10 Definitions/Model Diagnosis/Evaluation Plan/Management Service Delivery Design

11 } An unpleasant sensory + emotional experience associated with actual or potential tissue damage, or described in terms of such damage } International Association for the Study of Pain

12 } Pain that persists beyond normal tissue healing time, which is assumed to be 3 months } For this talk, chronic pain = chronic noncancer pain } International Association for the Study of Pain

13 All impact function in the context of pain/suffering. Biopsychosocial%20Model%20of%20Pain.htm
14 } Pain involves 2-way communication between peripheral + central nervous systems, + involves areas of the brain involved with emotions + thoughts } This impacts functions + behaviors } Pain/suffering exacerbated by impact of pain on function/behaviors, which worsens negative mood, physical inactivity, social isolation Negatively reinforcing } Suggests a variety of treatment modalities may be needed; most successful combination may take time to determine; may require team

15 } Homelessness increases risk of chronic pain, exacerbates suffering, + makes pain management more challenging More frequent injuries + assaults Less optimal + timely treatment Exposure to the elements More frequent behavioral health problems Higher risk of misuse/abuse of opioids Less treatment options
16 Definitions/Model Diagnosis/Evaluation Plan/Management Service Delivery Design
17 } History Ask + listen Pain, function, quality of life Behavioral health Living situation } Physical exam Trauma informed care } Further testing/referral if indicated
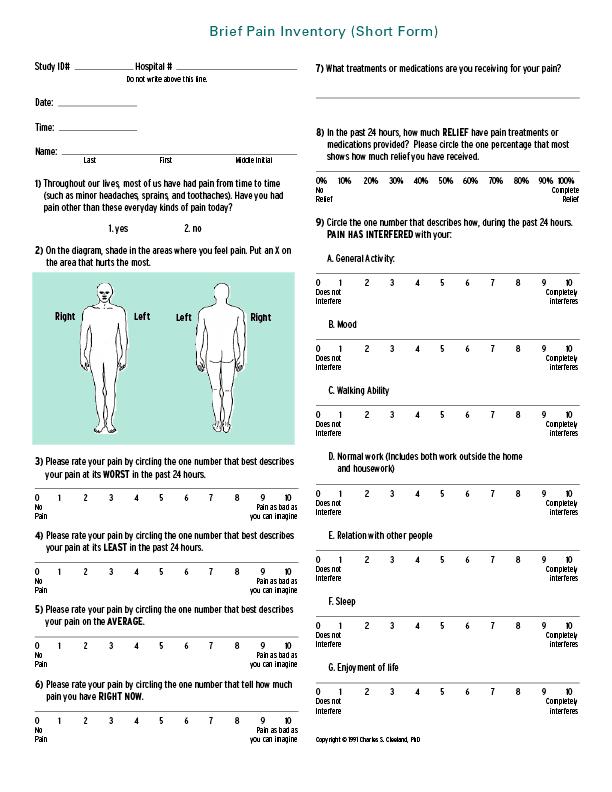
18 } Use of standard measures can help track progress, as well as effectiveness of treatment } Examples: numeric/faces pain scales, Brief Pain Inventory (Short Form), PEG (3-item scale)
19
20
21 What number best describes your pain on average in the past week? No pain Pain as bad as you can imagine What number best describes how, during the past week, pain has interfered with your enjoyment of life? Does not interfere Completely interferes What number best describes how, during the past week, pain has interfered with your general activity? Does not Completely interfere interferes Krebs EE, et al. Development and Initial Validation of the PEG, a Three-Item Scale Assessing Pain Intensity and Interference. JGIM 24.6 (2009):733-8.
22 } Important but challenging Pain + addiction frequently co-occur, have overlap in neurophysiology, can have similar effects on all aspects of health, cause/impact each other Both conditions must be managed simultaneously for best chance of success Patients may not be (initially) forthcoming about use or history, for many reasons Reassess frequently, using non-judgmental approach Consider assessment tools, urine drug testing
23 } Pain + mental health disorders frequently cooccur, symptoms can overlap, + outcomes for one can affect the other Anxiety Depression Post-Traumatic Stress Disorder } Psychological factors can influence pain Coping, acceptance, self-efficacy } Pain associated with suicide not related to mental illness
24 } Approach to engaging with people who have history of trauma that recognizes the presence of trauma symptoms + acknowledges role that trauma has played in their lives provides a framework for safety } Examples for physical exam: Explain what comprehensive exam will entail Ask permission to perform exam; explain what you will do before touching patient } National Center for Trauma Informed Care (
25 Definitions/Model Diagnosis/Evaluation Plan/Management Service Delivery Design
26 Focus on function Multimodal approach Opioids Universal precautions Follow up/ Aberrant drug related behaviors
27 } Rationale Generally cannot eliminate pain - at most, 2-3 point decrease on pain scale possible but small decreases in pain can lead to significant improvements in function More (objectively) measurable Respects individual differences More likely to increase quality of life + reduce burden of pain Particularly valuable when using opioids can help determine if addiction present
28 } What do you plan to do with this treatment that you can t do now? } What does pain keep you from doing? } If the answer is Feel better, or Everything consider: Asking about ADLs, sleep, walking/other physical activity, care of family/pets, hobbies, social activities with family/friends } Must be realistic, achievable, meaningful, measurable } Remain flexible



29 You see a 45 year old homeless man in primary care who has low back pain after failed disk surgery complicated by infection. He can t do anything because of the pain. He s couch surfing + spends most of the day inside drinking to ease the pain. His relationships are strained because he s irritable from the pain + from lack of sleep. He s ashamed to visit his family. He can t seem to get out to apply for benefits. He wants something from you to help with his pain. What functional goals might make sense?
30 Improved sleep Getting outside daily Applying for general assistance Reuniting with family


31 Psychological Self care, pacing, relaxation, coping, sleep hygiene Cognitive behavioral therapy Physical Multiple causes/impacts of pain suggest a multimodal approach Physical activity Physical therapy/physiatry, injections, surgery Pharmacological Non-opioids, opioids Complementary/alternative medicine Acupuncture, meditation, yoga, massage Other conditions Mental health Substance use Education, promote self management Self esteem, self efficacy Psychosocial needs Finances, housing, relationships, stress
32 Other conditions Psychological Psychosocial Physical Education Pharmacolog ical
33 } Based on concept that pain influenced not only by underlying pathophysiology but also thoughts, feelings, + behaviors } Can decrease pain, improve function, reduce disability, improve mood, reduce anxiety related to activity, improve relationships } Evidence-based } } Keefe FJ. (1996). Cognitive behavioral therapy for managing pain. The Clinical Psychologist, 49.3 (1996):4-5. Otis JD. Managing Chronic Pain: A Cognitive-Behavioral Therapy Approach. New York: Oxford University Press, 2007.



34 Treatment rationale Thoughts + behaviors affect pain experience Patients play role in controlling pain Coping skills training Relaxation Activity pacing/pleasant activity scheduling Distraction Cognitive restructuring Also includes stress + anger management, sleep hygiene, relapse prevention Application of coping skills
35 } Individual or group } Benefit of groups: More time efficient Allows learning coping skills from one another Illustrates not alone Provides social support


36 } Non-opioids Analgesics Muscle relaxants Anticonvulsants Antidepressants Topicals } Use type of pain (nocioceptive, neuropathic)/ condition as guides } Consider other symptoms/conditions

37 } Make plan for safe storage of medications Locked box Arrangement for storage at clinic or shelter } Adapt prescribing/dispensing as indicated

38 Indications Universal precautions approach Considerations in patients with substance use disorders Follow-up
39 } More severe pain/impaired function/quality of life } Insufficient improvement with other treatments or other treatments contraindicated } Benefits outweigh risks/harms } Opioids are part of good medical care, but must have appropriate structures/processes in place to prescribe them if not, develop contacts to refer elsewhere
40 } Approach Additional structure Ongoing assessment For all patients } Rationale High rates of substance abuse/dependence Increased risk of opioid misuse, abuse, diversion Difficulty predicting/detecting misuse, abuse, diversion } Gourlay et al. Universal Precautions in Pain Medicine: A Rational Approach to the Treatment of Chronic Pain Pain Medicine 6(2):
41 Diagnosis with appropriate differential Psychological assessment including risk of addictive disorders Informed consent Treatment agreement Pre/post intervention assessment of pain level/ function
42 Appropriate trial of opioid therapy +/- adjunctive medication Reassessment of pain score/ level of function Regularly assess Four A s Periodically review pain diagnosis/ comorbid conditions, including addictive disorders Document- ation 4A s=analgesia, activity, adverse effects, aberrant behavior (ADBR)

43 } Study of a subset of indigent patients with HIV } Patients who were on chronic opioids + their PC providers (PCPs) surveyed } Purpose: accuracy of PCP estimation of opioid misuse + illicit substance use } Vijayaraghavan M, et al. Primary Care Providers Judgments of Opioid Analgesic Misuse in a Community-Based Cohort of HIV-Infected Indigent Adults. JGIM 26.4 (2010):412-8.
44 } Results: Misuse 20% patients reported misuse PCPs estimated 50% of patients misused No concordance (kappa score 0.09, p=0.10) Illicit substance use 43% of patients reports illicit substance use PCPs estimated 50% of patients used illicit substances Concordance (kappa score 0.37, p<0.001)
45 } Results: PCPs more like to think younger patients (AOR 0.89 (95%CI )), African American patients (AOR 2.53 (95%CI )), + patients who used illicit substances (AOR 3.33 (95%CI ) had misused opioids Per patients, younger + African American patients not more likely to report misuse of opioids; those who used illicit substances were (AOR 3.01 (95%CI ))
46 } Conclusions: No concordance between patient report of opioid misuse + PCP estimate of patient misuse PCPs more likely to overestimate misuse in younger + African American patients } Use Universal Precautions!
47 } Managing addiction risk in patients with substance use disorders on opioids Risk of relapse increased, especially if past opioid addiction Universal precautions approach Consider urine drug testing More frequent visits Smaller supply of medication Inclusion of family/friends/others Increased support/adherence Collateral information
48 } When starting opioids: Minimize euphoric effects of opioids Avoid prescribing supratherapeutic doses Use slow-onset opioids Use forms less easily convertible to be injected, smoked, snorted Titrate rapidly to avoid prolonged dose finding } While on opioids: For minor relapse: increase support (SA counseling, short dispensing intervals, frequent urine drug testing treatment programs) For active addiction: discontinue/taper opioids For opioid addiction: refer to methadone maintenance therapy Consider buprenorphine off label, but legal for chronic pain + opioid addiction
49 4A s Analgesia (pain control) Activities of daily living (function) Adverse events (side effects) Aberrant drug related behavior
50 } Aberrant drug-related behavior Behavior outside the treatment agreement Examples: Request for early refill Missed appointment Report of lost/stolen medications Disruptive/violent behavior Appearing intoxicated or high, or with withdrawal symptoms Stealing/forging prescriptions Selling medications
51 } Aberrant drug-related behavior Take a uniform approach Use a non-judgmental harm reduction (motivational interviewing) approach Assess functional status
52 Determine a differential diagnosis Worsening of physical condition Additional acute pain syndrome Worsening of mental illness or substance abuse Misuse of opioids Pseudo-addiction Diversion Conditions of homelessness Not clear Address based on etiology/ severity of issue Increase in opioid dose Increase in structure (more frequent prescribing/dispensing, safe storage space) Intensification of mental health/ substance use treatment (including residential treatment) Additional information: urine drug testing, pill counts, Prescription Monitoring Program Discontinuation of opioids Further consultation (e.g., peer, team, or specialist review)
53 } Urine drug testing Can be an additional tool during initial + ongoing assessment for substance use disorders Can be used to monitor treatment adherence, as well as non-prescribed opioid use, to help reduce diversion/misuse/abuse by patients on opioids Pills counts + Prescription Monitoring Program data additional options
54 } Urine drug testing Be clear about rationale for use + what response to results will be Explain to patient Expectation of regulatory agencies of monitoring of adherence + substance use Focus on risks/benefits of opioids, patient safety Understand patients may have negative associations Know characteristics of test + how to interpret Do not forego monitoring of function
55 } Randomized trial of patients with chronic back/neck pain on opioids who had increased risk for or actual prescription opioid misuse } Question: Does an intervention of individual + group substance misuse counseling, selfreport compliance checklists, + regular urine drug testing improve compliance? } Jamison RN. Substance misuse treatment for high-risk chronic pain patients on opioid therapy: A randomized trial. Pain (2010):
56 } Intervention: cognitive behavioral training program for prevention of substance misuse Knowledge + training for substance misuse awareness + recovery Enhancing + maintaining motivation to abstain from illicit substance use Coping with urges to misuse medication Problem solving related to substance misuse Lifestyle balance 1 or more group sessions Monthly individual motivational counseling sessions Substance misuse education worksheets Monthly opioid compliance checklist Monthly urine drug tests
57 } Results: After 6 months, 26% of intervention patients (vs 74% of control patients) had positive scores on DMI DMI (drug misuse index) based on patient self report (prescription drug use questionnaire), physician report (addiction behaviors checklist), + urine drug test
58 } Conclusion: A brief cognitive behavioral/ motivational intervention can decrease misuse among high risk patients on opioids for chronic back/neck pain
59 Definitions/Model Diagnosis/Evaluation Plan/Management Service Delivery Design
60 Teams Groups Policies/Procedures Other

61 } Multiple causes/impacts of pain suggest a multimodal approach Teams provide the scope of perspectives + skills needed } Chronic pain management is time-consuming + stressful Teams also increase resources + support } Team members: Primary care provider, nurse, social worker, case manager, addiction specialist, psychiatrist/psychologist Pharmacist, physical therapist, pain specialist Providers from other agencies (mental health clinics, methadone treatment programs, residential/day treatment programs)
 } May improve ability to address needs of challenging patients } Can couple with individual encounter with medical provider } Can allow more patients to benefit from services")
62 } Interactive education } Self management goal setting } Medication refills/form completion } Other treatments (CBT, physical therapy) } Other benefits (decreased isolation, peer support, empowerment decreased staff burnout) } May improve ability to address needs of challenging patients } Can couple with individual encounter with medical provider } Can allow more patients to benefit from services
63 } Can systematize practice, provide support, protect therapeutic relationship, improve management of challenging patients, establish monitoring/tracking/review mechanisms } Based on practice guidelines, universal precautions
64 } Self care } Clinic safety safety plan/training } Opportunities for discussion Peer to peer / Multidisciplinary / Case conferencing Differences in practice styles / Difficult cases } Opportunities for ongoing education + skill building Functional goals, multimodal treatment Difficult conversations (substance use, addressing aberrant behavior, discontinuing opioids)
65 Provide framework + tools for evaluation + management of chronic pain Functional goals Multimodal treatment Universal precautions Provide recommendations for practice adaptations for patients experiencing homelessness
66 } Wismer B, et al. Adapting Your Practice: Recommendations for the Care of Homeless Adults with Chronic Non-Malignant Pain. Nashville: HCH Clinicians Network, National HCH Council, Inc, } Chou R, et al. Clinical Guidelines for the Use of Chronic Opioid Therapy in Chronic Noncancer Pain. Journal of Pain 10.2 (2009):
67 } SAMHSA. Managing Chronic Pain in Adults With or in Recovery from Substance Use Disorders. TIP Series 54. HHS Publication No. (SMA) Rockville, MD: SAMHSA, } Fishman SM. Responsible Opioid Prescribing: A Physician s Guide. Washington, DC: Waterford Life Sciences, 2007.


68
69 } SOAPP-R (Screener + Opioid Assessment for Patients with Pain Revised) } ORT (Opioid Risk Tool) } Somewhat effective in identifying those at higher risk for aberrant behaviors (behaviors outside the treatment plan)
70 } ORT (Opioid Risk Tool) } Different scores (0-5) for different items, female/male respondents Family history substance abuse Personal history substance abuse Age History preadolescent sexual abuse Psychological disease } Low risk (0-3 total); moderate (4-7); high (>=8) (predicts future ADRB)
71 } COMM (Current Opioid Misuse Measure) } Predicts current ADRB } 18 questions about past 30 days Thinking, function Treatment elsewhere Suicidality, anger Misuse (taking others meds, med use)
72 } Yellow Flag Committee Multidisciplinary group that meets monthly to review hard cases of patients on opioids, or patients on high dose opioids Any staff can suggest patient for review Any staff member can attend Provider + team present patient Provider, team, + committee generate recommendations for care Recommendations placed in patient record
73 } Yellow Flag Committee results so far Provides opportunity for provider review Provider/promotes team dialogue around hard cases Provides support for provider + team Recommendations often followed Hopefully will promote more consistency in care
Addressing the Opioid Epidemic: Prescribing Opioids for Non-Cancer Pain
 Addressing the Opioid Epidemic: Prescribing Opioids for Non-Cancer Pain Ajay D. Wasan, MD, MSc Professor of Anesthesiology and Psychiatry Vice Chair for Pain Medicine, Department of Anesthesiology University
Addressing the Opioid Epidemic: Prescribing Opioids for Non-Cancer Pain Ajay D. Wasan, MD, MSc Professor of Anesthesiology and Psychiatry Vice Chair for Pain Medicine, Department of Anesthesiology University
Opioids in the Management of Chronic Pain: An Overview
 Opioids in the Management of Chronic Pain: An Overview Appropriate treatment of chronic pain may include both pharmacologic and non-pharmacologic modalities. The Board realizes that controlled substances,
Opioids in the Management of Chronic Pain: An Overview Appropriate treatment of chronic pain may include both pharmacologic and non-pharmacologic modalities. The Board realizes that controlled substances,
Universal Precautions and Opioid Risk. Assessment. Questions: How often do you screen your patients for risk of misuse when prescribing opioids?
 Learning objectives 1. Identify the contribution of psychosocial and spiritual factors to pain 2. Incorporate strategies for identifying and mitigating opioid misuse 3. Incorporate non-pharmaceutical modalities
Learning objectives 1. Identify the contribution of psychosocial and spiritual factors to pain 2. Incorporate strategies for identifying and mitigating opioid misuse 3. Incorporate non-pharmaceutical modalities
MAT for Opioid Dependence. MAT and Pain Management. Epidemiology. Epidemiology. Factors Impacting Pain Perception 9/23/2014
 MAT for Opioid Dependence Methadone maintenance treatment (MMT) Buprenorphine/naloxone (suboxone) Buprenorhine/naloxone (BupNX) Buprenorphine SL Parenteral naltrexone (P-ntx) Oral naltrexone (ntx) MAT
MAT for Opioid Dependence Methadone maintenance treatment (MMT) Buprenorphine/naloxone (suboxone) Buprenorhine/naloxone (BupNX) Buprenorphine SL Parenteral naltrexone (P-ntx) Oral naltrexone (ntx) MAT
Opioids: Use and Misuse/Steven Feinberg, MD; Scott Levy, MD, MPH, FACOEM
 Western Occupational Health Conference September 14, 2012 Opioid - Use & Misuse Scott Levy, MD MPH FACOEM Steven Feinberg, MD, MPH Disclosure Information Western Occupational Health Conference 2012 Steven
Western Occupational Health Conference September 14, 2012 Opioid - Use & Misuse Scott Levy, MD MPH FACOEM Steven Feinberg, MD, MPH Disclosure Information Western Occupational Health Conference 2012 Steven
Responding to the Opioid Epidemic: Behavioral Health Specialists Role on the Interprofessional Team
 Responding to the Opioid Epidemic: Behavioral Health Specialists Role on the Interprofessional Team Cheryl L Mejta, Ph.D. Nancy H Burley, Ed.D. Serena Wadhwa, Psy. D., LCPC, RYT, CADC Objectives Identify
Responding to the Opioid Epidemic: Behavioral Health Specialists Role on the Interprofessional Team Cheryl L Mejta, Ph.D. Nancy H Burley, Ed.D. Serena Wadhwa, Psy. D., LCPC, RYT, CADC Objectives Identify
Use of Opioids for Chronic Non Malignant Pain (CNMP)
") I. PURPOSE Use of Opioids for Chronic Non Malignant Pain (CNMP) We the Safe Opioid Prescribing and Review Committee (SOPARC) are inspired to support a shift in opioid prescribing that improves clinical
I. PURPOSE Use of Opioids for Chronic Non Malignant Pain (CNMP) We the Safe Opioid Prescribing and Review Committee (SOPARC) are inspired to support a shift in opioid prescribing that improves clinical
Chronic Pain & Depression: A Roller Coaster Ride. Lori Higa, BSN, RN-BC
 Chronic Pain & Depression: A Roller Coaster Ride Lori Higa, BSN, RN-BC Objectives By the end of this Webinar you will be able to: Help patient to be a good self-advocate Discuss treatment options with
Chronic Pain & Depression: A Roller Coaster Ride Lori Higa, BSN, RN-BC Objectives By the end of this Webinar you will be able to: Help patient to be a good self-advocate Discuss treatment options with
Approaches to Responsible Opioid Prescribing. The Opioid Naïve Patient
 Approaches to Responsible Opioid Prescribing The Opioid Naïve Patient Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Approaches to Responsible Opioid Prescribing The Opioid Naïve Patient Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
CDC Guideline for Prescribing Opioids for Chronic Pain. Centers for Disease Control and Prevention National Center for Injury Prevention and Control
 CDC Guideline for Prescribing Opioids for Chronic Pain Centers for Disease Control and Prevention National Center for Injury Prevention and Control THE EPIDEMIC Chronic Pain and Prescription Opioids 11%
CDC Guideline for Prescribing Opioids for Chronic Pain Centers for Disease Control and Prevention National Center for Injury Prevention and Control THE EPIDEMIC Chronic Pain and Prescription Opioids 11%
Recommendations in Opioid Prescribing Guidelines for Chronic Pain
 Recommendations in Opioid Prescribing Guidelines for Chronic Pain The use of opioids for treating chronic pain has been increasing. 1 In 2010, an estimated 20% of patients presenting to physician offices
Recommendations in Opioid Prescribing Guidelines for Chronic Pain The use of opioids for treating chronic pain has been increasing. 1 In 2010, an estimated 20% of patients presenting to physician offices
Utah. Prescribing and Dispensing Profile. Research current through November 2015.
 Prescribing and Dispensing Profile Utah Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points of view
Prescribing and Dispensing Profile Utah Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points of view
Nancy Elder, MD, MSPH Cincinnati, Ohio
 Nancy Elder, MD, MSPH Cincinnati, Ohio My neck has hurt ever since my motorcycle crash in 2001. You got to help me, Doc! Great. Another drug seeking patient wanting narcotics. When I was working and had
Nancy Elder, MD, MSPH Cincinnati, Ohio My neck has hurt ever since my motorcycle crash in 2001. You got to help me, Doc! Great. Another drug seeking patient wanting narcotics. When I was working and had
Rule Governing the Prescribing of Opioids for Pain
 Rule Governing the Prescribing of Opioids for Pain 1.0 Authority This rule is adopted pursuant to Sections 14(e) and 11(e) of Act 75 (2013) and Sections 2(e) and 2a of Act 173 (2016). 2.0 Purpose This
Rule Governing the Prescribing of Opioids for Pain 1.0 Authority This rule is adopted pursuant to Sections 14(e) and 11(e) of Act 75 (2013) and Sections 2(e) and 2a of Act 173 (2016). 2.0 Purpose This
Chronic Pain Management in the Primary Care Setting
 Chronic Pain Management in the Primary Care Setting Keeping you and your patients safe. Joel Porter, MD October 1, 2015 Chronic Pain Management Chronic pain is a major public health problem Existing chronic
Chronic Pain Management in the Primary Care Setting Keeping you and your patients safe. Joel Porter, MD October 1, 2015 Chronic Pain Management Chronic pain is a major public health problem Existing chronic
The Biopsychosocial Model of Treating Chronic Pain Opioids Seldom Work. Program Learning Objectives. Key Points
 The Biopsychosocial Model of Treating Chronic Pain Opioids Seldom Work American Board of Vocational Experts April 2016 Dr. Jasen Michael Walker CEC Associates, Incorporated Program Learning Objectives
The Biopsychosocial Model of Treating Chronic Pain Opioids Seldom Work American Board of Vocational Experts April 2016 Dr. Jasen Michael Walker CEC Associates, Incorporated Program Learning Objectives
Cognitive Behavioral and Motivational Approaches to Chronic Pain. Joseph Merrill MD, MPH University of Washington October 14, 2017
 Cognitive Behavioral and Motivational Approaches to Chronic Pain Joseph Merrill MD, MPH University of Washington October 14, 2017 Motivational and Cognitive Behavioral Approaches Assessment basics Components
Cognitive Behavioral and Motivational Approaches to Chronic Pain Joseph Merrill MD, MPH University of Washington October 14, 2017 Motivational and Cognitive Behavioral Approaches Assessment basics Components
New Guidelines for Opioid Prescribing
 New Guidelines for Opioid Prescribing What They Mean for Elders with Chronic Pain Manu Thakral, PhD, ARNP Kaiser Permanente Washington Health Research Institute Kaiser Permanente Washington Health Research
New Guidelines for Opioid Prescribing What They Mean for Elders with Chronic Pain Manu Thakral, PhD, ARNP Kaiser Permanente Washington Health Research Institute Kaiser Permanente Washington Health Research
New Guidelines for Prescribing Opioids for Chronic Pain
 New Guidelines for Prescribing Opioids for Chronic Pain Andrew Lowe, Pharm.D. CAPA Meeting October 6, 2016 THE EPIDEMIC Chronic Pain and Prescription Opioids 11% of Americans experience daily (chronic)
New Guidelines for Prescribing Opioids for Chronic Pain Andrew Lowe, Pharm.D. CAPA Meeting October 6, 2016 THE EPIDEMIC Chronic Pain and Prescription Opioids 11% of Americans experience daily (chronic)
Based on Tip 54. Managing Chronic Pain in Adults With or in Recovery From Substance Use Disorders KAP KEYS FOR CLINICIANS
 Based on Tip 54 Managing Chronic Pain in Adults With or in Recovery From Substance Use Disorders KAP KEYS FOR CLINICIANS KAP Keys Based on TIP 54 Introduction KAP Keys were developed to accompany the Treatment
Based on Tip 54 Managing Chronic Pain in Adults With or in Recovery From Substance Use Disorders KAP KEYS FOR CLINICIANS KAP Keys Based on TIP 54 Introduction KAP Keys were developed to accompany the Treatment
Chronic Pain Pharmacist role in the clinic
 Chronic Pain Pharmacist role in the clinic WSPA Annual Meeting 2015 Alvin Goo, PharmD Clinical Associate Professor University of Washington Schools of Pharmacy and Family Medicine Speakers Declaration
Chronic Pain Pharmacist role in the clinic WSPA Annual Meeting 2015 Alvin Goo, PharmD Clinical Associate Professor University of Washington Schools of Pharmacy and Family Medicine Speakers Declaration
Knock Out Opioid Abuse in New Jersey:
 Knock Out Opioid Abuse in New Jersey: A Resource for Safer Prescribing GUIDELINE FOR PRESCRIBING OPIOIDS FOR CHRONIC PAIN IMPROVING PRACTICE THROUGH RECOMMENDATIONS CDC s Guideline for Prescribing Opioids
Knock Out Opioid Abuse in New Jersey: A Resource for Safer Prescribing GUIDELINE FOR PRESCRIBING OPIOIDS FOR CHRONIC PAIN IMPROVING PRACTICE THROUGH RECOMMENDATIONS CDC s Guideline for Prescribing Opioids
Opioid Prescribing for Acute Pain. Care for People 15 Years of Age and Older
 Opioid Prescribing for Acute Pain Care for People 15 Years of Age and Older Summary This quality standard provides guidance on the appropriate prescribing, monitoring, and tapering of opioids to treat
Opioid Prescribing for Acute Pain Care for People 15 Years of Age and Older Summary This quality standard provides guidance on the appropriate prescribing, monitoring, and tapering of opioids to treat
ADVANCED BEHAVIORAL HEALTH, INC. Clinical Level of Care Guidelines
 The Clinical Level of Care Guidelines contained on the following pages have been developed as a guide to assist care managers, physicians and providers in making medical necessity decisions about the least
The Clinical Level of Care Guidelines contained on the following pages have been developed as a guide to assist care managers, physicians and providers in making medical necessity decisions about the least
IDDT Fidelity Action Planning Guidelines
 1a. Multidisciplinary Team IDDT Fidelity Action Planning Guidelines Definition: All clients targeted for IDDT receive care from a multidisciplinary team. A multi-disciplinary team consists of, in addition
1a. Multidisciplinary Team IDDT Fidelity Action Planning Guidelines Definition: All clients targeted for IDDT receive care from a multidisciplinary team. A multi-disciplinary team consists of, in addition
Pain Management and Addiction: Clinical Challenges
 Pain Management and Addiction: Clinical Challenges MMS Pain Management Forum March 12, 2010 Associate Professor of Medicine Boston University School of Medicine Boston Medical Center Conflicts of Interest
Pain Management and Addiction: Clinical Challenges MMS Pain Management Forum March 12, 2010 Associate Professor of Medicine Boston University School of Medicine Boston Medical Center Conflicts of Interest
Opioid Review and MAT Clinic CDC Guidelines
 1 Opioid Review and MAT Clinic CDC Guidelines January 10, 2018 Housekeeping Use chat feature to inform everyone who s at your clinic Click chat on Zoom option bar Chat Everyone the names of those who are
1 Opioid Review and MAT Clinic CDC Guidelines January 10, 2018 Housekeeping Use chat feature to inform everyone who s at your clinic Click chat on Zoom option bar Chat Everyone the names of those who are
Opiate Use Disorder and Opiate Overdose
 Opiate Use Disorder and Opiate Overdose Irene Ortiz, MD Medical Director Molina Healthcare of New Mexico and South Carolina Clinical Professor University of New Mexico School of Medicine Objectives DSM-5
Opiate Use Disorder and Opiate Overdose Irene Ortiz, MD Medical Director Molina Healthcare of New Mexico and South Carolina Clinical Professor University of New Mexico School of Medicine Objectives DSM-5
ECHO: Healthy Alternatives for Pain Management. and AB 474 Compliance Check lists
 ECHO: Healthy Alternatives for Pain Management and AB 474 Compliance Check lists BEFORE I CAN WRITE AN INITIAL PRESCRIPTION Have I established a bona fide relationship with the patient? Have I established
ECHO: Healthy Alternatives for Pain Management and AB 474 Compliance Check lists BEFORE I CAN WRITE AN INITIAL PRESCRIPTION Have I established a bona fide relationship with the patient? Have I established
Post-Traumatic Stress Disorder
 Post-Traumatic Stress Disorder Teena Jain 2017 Post-Traumatic Stress Disorder What is post-traumatic stress disorder, or PTSD? PTSD is a disorder that some people develop after experiencing a shocking,
Post-Traumatic Stress Disorder Teena Jain 2017 Post-Traumatic Stress Disorder What is post-traumatic stress disorder, or PTSD? PTSD is a disorder that some people develop after experiencing a shocking,
I. Chronic Pain Information Page 2-3. II. The Role of the Primary Care Physician in Chronic Pain Management Page 3-4
 SUTTER MEDICAL FOUNDATION (SMF) 2750 GATEWAY OAKS DRIVE, #150 SACRAMENTO, CA 95833 SPA PCP Treatment & Referral Guidelines PAIN MANAGEMENT Developed June 1, 2003 Revised (Format Revisions) November 13,
SUTTER MEDICAL FOUNDATION (SMF) 2750 GATEWAY OAKS DRIVE, #150 SACRAMENTO, CA 95833 SPA PCP Treatment & Referral Guidelines PAIN MANAGEMENT Developed June 1, 2003 Revised (Format Revisions) November 13,
Canadian Guideline for Opioids for Chronic Non-Cancer Pain. Speaker Disclosure. Objectives. Canadian Guideline for Opioids for Chronic Non-Cancer Pain
 Canadian Guideline for Opioids for Chronic Non-Cancer Pain John Fraser Community Hospital Program New Glasgow November 1, 2017 This speaker has been asked to disclose to the audience any involvement with
Canadian Guideline for Opioids for Chronic Non-Cancer Pain John Fraser Community Hospital Program New Glasgow November 1, 2017 This speaker has been asked to disclose to the audience any involvement with
What recovery means: Independent living. Control of symptoms. Active remission of substance use. Competitive employment
 What recovery means: Independent living Control of symptoms Active remission of substance use Competitive employment Socialization with peers who do not use Satisfaction with life Getting finances in order
What recovery means: Independent living Control of symptoms Active remission of substance use Competitive employment Socialization with peers who do not use Satisfaction with life Getting finances in order
The Opioid Misuse Crisis and Non- Pharmacological Pain Management. Collaboration with SPTAs, Divisions and Schools
 The Opioid Misuse Crisis and Non- Pharmacological Pain Management Collaboration with SPTAs, Divisions and Schools Learning Objectives Participants will be able to describe the role of non-pharmacological
The Opioid Misuse Crisis and Non- Pharmacological Pain Management Collaboration with SPTAs, Divisions and Schools Learning Objectives Participants will be able to describe the role of non-pharmacological
Subject: Pain Management (Page 1 of 7)
") Subject: Pain Management (Page 1 of 7) Objectives: Managing pain and restoring function are basic goals in helping a patient with chronic non-cancer pain. Federal and state guidelines require that all
Subject: Pain Management (Page 1 of 7) Objectives: Managing pain and restoring function are basic goals in helping a patient with chronic non-cancer pain. Federal and state guidelines require that all
KANSAS Kansas State Board of Healing Arts. Source: Kansas State Board of Healing Arts. Approved: October 17, 1998
 KANSAS Kansas State Board of Healing Arts Source: Kansas State Board of Healing Arts Approved: October 17, 1998 GUIDELINES FOR THE USE OF CONTROLLED SUBSTANCES FOR THE TREATMENT OF PAIN Section 1: Preamble
KANSAS Kansas State Board of Healing Arts Source: Kansas State Board of Healing Arts Approved: October 17, 1998 GUIDELINES FOR THE USE OF CONTROLLED SUBSTANCES FOR THE TREATMENT OF PAIN Section 1: Preamble
RECOMMENDATIONS FOR HEALTH CARE PROVIDERS
 Ending Addiction Changes Everything RECOMMENDATIONS FOR HEALTH CARE PROVIDERS CRITICAL ADDICTION PREVENTION, TREATMENT AND MANAGEMENT SERVICES TO INCLUDE IN ROUTINE HEALTH CARE PRACTICE JULY 2013 In the
Ending Addiction Changes Everything RECOMMENDATIONS FOR HEALTH CARE PROVIDERS CRITICAL ADDICTION PREVENTION, TREATMENT AND MANAGEMENT SERVICES TO INCLUDE IN ROUTINE HEALTH CARE PRACTICE JULY 2013 In the
Integrated Care for Depression, Anxiety and PTSD. Introduction: Overview of Clinical Roles and Ideas
 Integrated Care for Depression, Anxiety and PTSD University of Washington An Evidence-based d Approach for Behavioral Health Professionals (LCSWs, MFTs, and RNs) Alameda Health Consortium November 15-16,
Integrated Care for Depression, Anxiety and PTSD University of Washington An Evidence-based d Approach for Behavioral Health Professionals (LCSWs, MFTs, and RNs) Alameda Health Consortium November 15-16,
TREATING OPIOID ADDICTION IN HOMELESS POPULATIONS
 TREATING OPIOID ADDICTION IN HOMELESS POPULATIONS Challenges and Opportunities Providing Medication Assisted Treatment (Buprenorphine) August 18, 2016 SPEAKERS TODAY Nilesh Kalyanaraman, MD, Chief Health
TREATING OPIOID ADDICTION IN HOMELESS POPULATIONS Challenges and Opportunities Providing Medication Assisted Treatment (Buprenorphine) August 18, 2016 SPEAKERS TODAY Nilesh Kalyanaraman, MD, Chief Health
Pain, prescription opioid use and misuse among homeless populations: What do we know? Margot Kushel MD HCH Pre-conference on Pain May 15, 2012
 Pain, prescription opioid use and misuse among homeless populations: What do we know? Margot Kushel MD HCH Pre-conference on Pain May 15, 2012 What are we talking about when we talk about pain? What s
Pain, prescription opioid use and misuse among homeless populations: What do we know? Margot Kushel MD HCH Pre-conference on Pain May 15, 2012 What are we talking about when we talk about pain? What s
Foundations of Safe and Effective Pain Management
 Foundations of Safe and Effective Pain Management Evidence-based Education for Nurses, 2018 Module 1: The Multi-dimensional Nature of Pain Module 2: Pain Assessment and Documentation Module 3: Management
Foundations of Safe and Effective Pain Management Evidence-based Education for Nurses, 2018 Module 1: The Multi-dimensional Nature of Pain Module 2: Pain Assessment and Documentation Module 3: Management
Prescribing drugs of dependence in general practice, Part C
 HO O Prescribing drugs of dependence in general practice, Part C Key recommendations and practice points for management of pain with opioid therapy H H HO N CH3 Acute pain Acute pain is an unpleasant sensory
HO O Prescribing drugs of dependence in general practice, Part C Key recommendations and practice points for management of pain with opioid therapy H H HO N CH3 Acute pain Acute pain is an unpleasant sensory
Wisconsin Opioid Prescribing Guideline Draft Scope and purpose of the guideline
 Wisconsin Opioid Prescribing Guideline Draft Scope and purpose of the guideline: To help providers make informed decisions about acute and chronic pain treatment -pain lasting longer than three months
Wisconsin Opioid Prescribing Guideline Draft Scope and purpose of the guideline: To help providers make informed decisions about acute and chronic pain treatment -pain lasting longer than three months
Proposed Revision to Med (i)
") Proposed Revision to Med 501.02 (i) I. Purpose This rule has been adopted to enable the Board to best protect public health and safety while providing a framework for licensees to effectively treat and
Proposed Revision to Med 501.02 (i) I. Purpose This rule has been adopted to enable the Board to best protect public health and safety while providing a framework for licensees to effectively treat and
Condensed Clinical Practice Guideline Treatment Of Patients With Schizophrenia
 Condensed Clinical Practice Guideline Treatment Of Patients With Schizophrenia I. Key Points a. Schizophrenia is a chronic illness affecting all aspects of person s life i. Treatment Planning Goals 1.
Condensed Clinical Practice Guideline Treatment Of Patients With Schizophrenia I. Key Points a. Schizophrenia is a chronic illness affecting all aspects of person s life i. Treatment Planning Goals 1.
ASPMN Conference Baltimore, Maryland
 ASPMN Conference Baltimore, Maryland Prescribing Controlled Substances Managing Risk and Optimizing Outcomes September 13, 2012 Tracey Fremd, NP Tracey Fremd Consulting, Inc. Most Common Uses for Controlled
ASPMN Conference Baltimore, Maryland Prescribing Controlled Substances Managing Risk and Optimizing Outcomes September 13, 2012 Tracey Fremd, NP Tracey Fremd Consulting, Inc. Most Common Uses for Controlled
Standard of Practice for Prescribing Opioids (Excluding Cancer, Palliative, and End-of-Life Care)
") Standard of Practice for Prescribing Opioids (Excluding Cancer, Palliative, and End-of-Life Care) Preamble This Standard establishes the standards of practice and ethical requirements of all physicians
Standard of Practice for Prescribing Opioids (Excluding Cancer, Palliative, and End-of-Life Care) Preamble This Standard establishes the standards of practice and ethical requirements of all physicians
Opioid Analgesics: Responsible Prescribing in the Midst of an Epidemic
 Opioid Analgesics: Responsible Prescribing in the Midst of an Epidemic Lucas Buffaloe, MD Associate Professor of Clinical Family and Community Medicine University of Missouri Health Care Goals for today
Opioid Analgesics: Responsible Prescribing in the Midst of an Epidemic Lucas Buffaloe, MD Associate Professor of Clinical Family and Community Medicine University of Missouri Health Care Goals for today
Management of Pain - A Comparison of Current Guidelines
 Management of Pain - A Comparison of Current Guidelines The Centers for Disease Control and Prevention (CDC) released a guideline in 2016 regarding the prescribing of opioids for chronic non-cancer pain
Management of Pain - A Comparison of Current Guidelines The Centers for Disease Control and Prevention (CDC) released a guideline in 2016 regarding the prescribing of opioids for chronic non-cancer pain
POLYSUBSTANCE USE IN THE TREATMENT OF OPIOID USE DISORDER WITH BUPRENORPHINE
 Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences POLYSUBSTANCE USE IN THE TREATMENT OF OPIOID USE DISORDER WITH BUPRENORPHINE MARK DUNCAN, MD November 8, 2018 SPEAKER
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences POLYSUBSTANCE USE IN THE TREATMENT OF OPIOID USE DISORDER WITH BUPRENORPHINE MARK DUNCAN, MD November 8, 2018 SPEAKER
Substance Use Disorders in Primary Care
 Substance Use Disorders in Primary Care Jin Hee Yoon-Hudman, MD Assistant Vice President, Medical Director, Behavioral Health Healthfirst Fall Symposium Prevention as a Priority in Value-Based Healthcare,
Substance Use Disorders in Primary Care Jin Hee Yoon-Hudman, MD Assistant Vice President, Medical Director, Behavioral Health Healthfirst Fall Symposium Prevention as a Priority in Value-Based Healthcare,
Medication-Assisted Treatment. What Is It and Why Do We Use It?
 Medication-Assisted Treatment What Is It and Why Do We Use It? What is addiction, really? o The four C s of addiction: Craving. Loss of Control of amount or frequency of use. Compulsion to use. Use despite
Medication-Assisted Treatment What Is It and Why Do We Use It? What is addiction, really? o The four C s of addiction: Craving. Loss of Control of amount or frequency of use. Compulsion to use. Use despite
Pain Management at Stony Brook Medicine
 Pain Management at Stony Brook Medicine Pain Management Policy All patients must have effective pain management Appropriate screening and pain assessment Documentation Care and treatment Pain education
Pain Management at Stony Brook Medicine Pain Management Policy All patients must have effective pain management Appropriate screening and pain assessment Documentation Care and treatment Pain education
Pharmacist s Role In Pain Management. Katrina Lynn, Pharm D PSHP Annual Assembly: October 12, 2017
 Pharmacist s Role In Pain Management Katrina Lynn, Pharm D PSHP Annual Assembly: October 12, 2017 1 Presentation Objectives Briefly discuss Geisinger Health System and the use of Pain Management Pharmacists
Pharmacist s Role In Pain Management Katrina Lynn, Pharm D PSHP Annual Assembly: October 12, 2017 1 Presentation Objectives Briefly discuss Geisinger Health System and the use of Pain Management Pharmacists
Revised 9/30/2016. Primary Care Provider Pain Management Toolkit
 Revised 9/30/2016 Primary Care Provider Pain Management Toolkit TABLE OF CONTENTS 1. INTRODUCTION Page 1 2. NON-OPIOID SERVICES &TREATMENTS FOR CHRONIC PAIN Page 2 2.1 Medical Services Page 2 2.2 Behavioral
Revised 9/30/2016 Primary Care Provider Pain Management Toolkit TABLE OF CONTENTS 1. INTRODUCTION Page 1 2. NON-OPIOID SERVICES &TREATMENTS FOR CHRONIC PAIN Page 2 2.1 Medical Services Page 2 2.2 Behavioral
SUBSTANCE ABUSE IN THE ELDERLY. The Invisible Epidemic
 SUBSTANCE ABUSE IN THE ELDERLY The Invisible Epidemic IS IT POSSIBLE TO TEACH AN OLD DOG NEW TRICKS? GUIDELINES All forms of addiction know no age limit. Don t blame all problems on aging. Few realize
SUBSTANCE ABUSE IN THE ELDERLY The Invisible Epidemic IS IT POSSIBLE TO TEACH AN OLD DOG NEW TRICKS? GUIDELINES All forms of addiction know no age limit. Don t blame all problems on aging. Few realize
Approved Procedures for Prescribing and Monitoring Controlled Substances in South Carolina
 Approved Procedures for Prescribing and Monitoring Controlled Substances in South Carolina Robert B. Hanlin, M.D., FAAFP Vice Chair, Medical Staff Affairs Greenville Health System Greenville, SC Disclosures
Approved Procedures for Prescribing and Monitoring Controlled Substances in South Carolina Robert B. Hanlin, M.D., FAAFP Vice Chair, Medical Staff Affairs Greenville Health System Greenville, SC Disclosures
SUMMARY OF ARIZONA OPIOID PRESCRIBING GUIDELINES FOR THE TREATMENT OF CHRONIC NON-TERMINAL PAIN (CNTP)
") 9 SUMMARY OF ARIZONA OPIOID PRESCRIBING GUIDELINES FOR THE TREATMENT OF CHRONIC NON-TERMINAL PAIN (CNTP) SUMMARY OF ARIZONA OPIOID PRESCRIBING GUIDELINES FOR THE TREATMENT OF ACUTE PAIN NONOPIOID TREATMENTS
9 SUMMARY OF ARIZONA OPIOID PRESCRIBING GUIDELINES FOR THE TREATMENT OF CHRONIC NON-TERMINAL PAIN (CNTP) SUMMARY OF ARIZONA OPIOID PRESCRIBING GUIDELINES FOR THE TREATMENT OF ACUTE PAIN NONOPIOID TREATMENTS
Alberta Alcohol and Drug Abuse Commission. POSITION ON ADDICTION AND MENTAL HEALTH February 2007
 Alberta Alcohol and Drug Abuse Commission POSITION ON ADDICTION AND MENTAL HEALTH POSITION The Alberta Alcohol and Drug Abuse Commission (AADAC) recognizes that among clients with addiction problems, there
Alberta Alcohol and Drug Abuse Commission POSITION ON ADDICTION AND MENTAL HEALTH POSITION The Alberta Alcohol and Drug Abuse Commission (AADAC) recognizes that among clients with addiction problems, there
Summary of Recommendations...3. PEG: A Three-Item Scale Assessing Pain (Appendix A) Chronic Pain Flow Sheet Acute Pain Flow Sheet...
 Chronic Pain Flow Sheet Acute Pain Flow Sheet...") Table of Contents Summary of Recommendations....3 PEG: A Three-Item Scale Assessing Pain (Appendix A)...12 Chronic Pain Flow Sheet...13 Acute Pain Flow Sheet...14 Pocket Guide: Tapering Opioids for Chronic
Table of Contents Summary of Recommendations....3 PEG: A Three-Item Scale Assessing Pain (Appendix A)...12 Chronic Pain Flow Sheet...13 Acute Pain Flow Sheet...14 Pocket Guide: Tapering Opioids for Chronic
Interdisciplinary Management of Opioid Use Disorder in Rural Primary Care Settings
 Interdisciplinary Management of Opioid Use Disorder in Rural Primary Care Settings BRIAN GARVEY, MD, MPH REBECCA CANTONE, MD OREGON HEALTH & SCIENCE UNIVERSITY SCAPPOOSE RURAL HEALTH CENTER Disclosures
Interdisciplinary Management of Opioid Use Disorder in Rural Primary Care Settings BRIAN GARVEY, MD, MPH REBECCA CANTONE, MD OREGON HEALTH & SCIENCE UNIVERSITY SCAPPOOSE RURAL HEALTH CENTER Disclosures
Best Practices in Prescribing Opioids for Chronic Non-cancer Pain
 Best Practices in Prescribing Opioids for Chronic Non-cancer Pain Disclosures S C O T T S T E I G E R, M D, F A C P, D A B A M A S S I S T A N T C L I N I C A L P R O F E S S O R D I V I S I O N O F G
Best Practices in Prescribing Opioids for Chronic Non-cancer Pain Disclosures S C O T T S T E I G E R, M D, F A C P, D A B A M A S S I S T A N T C L I N I C A L P R O F E S S O R D I V I S I O N O F G
Promoting Healthy Coping & Addressing Negative Emotion in Diabetes Management. Capstone Meeting Tucson, Arizona October 18 20, 2006
 Promoting Healthy Coping & Addressing Negative Emotion in Diabetes Management Capstone Meeting Tucson, Arizona October 18 20, 2006 Anonymous, Northwest PCP: You know, when I have a patient who has been
Promoting Healthy Coping & Addressing Negative Emotion in Diabetes Management Capstone Meeting Tucson, Arizona October 18 20, 2006 Anonymous, Northwest PCP: You know, when I have a patient who has been
Scope of the Opiate Problem 6/5/18. Chronic Pain Management and the Use of Opioid Medications: The CDC Guideline and Beyond. Overview.
 Chronic Pain Management and the Use of Opioid Medications: The CDC Guideline and Beyond David Anisman, MD Medical Director, Farmington Health Center (Primary Care) Associate Medical Director, Community
Chronic Pain Management and the Use of Opioid Medications: The CDC Guideline and Beyond David Anisman, MD Medical Director, Farmington Health Center (Primary Care) Associate Medical Director, Community
Chronic Disease Management for Pain: It CAN be done in primary care!
 Chronic Disease Management for Pain: It CAN be done in primary care! Sondra Adkinson, PharmD, DAAPM, CPE Thomas B. Gregory, Pharm.D., BCPS, DASPE, CPE Chris Herndon, PharmD, BCPS, CPE Disclosures Adkinson:
Chronic Disease Management for Pain: It CAN be done in primary care! Sondra Adkinson, PharmD, DAAPM, CPE Thomas B. Gregory, Pharm.D., BCPS, DASPE, CPE Chris Herndon, PharmD, BCPS, CPE Disclosures Adkinson:
Safe and Competent Opioid Prescribing
 MILITARY Military Safe and Competent Opioid Prescribing Education (M-SCOPE) Program Safe and Competent Opioid Prescribing For Providers Working with Veterans and Military Service Personnel Daniel P. Alford,
MILITARY Military Safe and Competent Opioid Prescribing Education (M-SCOPE) Program Safe and Competent Opioid Prescribing For Providers Working with Veterans and Military Service Personnel Daniel P. Alford,
California. Prescribing and Dispensing Profile. Research current through November 2015.
 Prescribing and Dispensing Profile California Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
Prescribing and Dispensing Profile California Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
THE PROS & CONS OF THE CDC GUIDELINES FOR SAFE OPIOID PRESCRIBING
 THE PROS & CONS OF THE CDC GUIDELINES FOR SAFE OPIOID PRESCRIBING Ernest J Dole, PharmD, PhC, FASHP, BCPS Clinical Pharmacist University of New Mexico Hospitals And Clinical Associate Professor University
THE PROS & CONS OF THE CDC GUIDELINES FOR SAFE OPIOID PRESCRIBING Ernest J Dole, PharmD, PhC, FASHP, BCPS Clinical Pharmacist University of New Mexico Hospitals And Clinical Associate Professor University
The Psychology of Pain within the Biological Model. Michael Coupland, CPsych, CRC Integrated Medical Case Solutions (IMCS Group)
") The Psychology of Pain within the Biological Model Michael Coupland, CPsych, CRC Integrated Medical Case Solutions (IMCS Group) Integrated Medical Case Solutions National Panel of Psychologists Biopsychosocial
The Psychology of Pain within the Biological Model Michael Coupland, CPsych, CRC Integrated Medical Case Solutions (IMCS Group) Integrated Medical Case Solutions National Panel of Psychologists Biopsychosocial
OUTPATIENT TREATMENT WESTPORT, CONNECTICUT
 OUTPATIENT TREATMENT WESTPORT, CONNECTICUT ABOUT CLEARPOINT At Clearpoint, we focus on healing the whole person: mind, body, and spirit. Our comprehensive care methods set clients up for long-term success
OUTPATIENT TREATMENT WESTPORT, CONNECTICUT ABOUT CLEARPOINT At Clearpoint, we focus on healing the whole person: mind, body, and spirit. Our comprehensive care methods set clients up for long-term success
Opioid Prescribing Improvement Program
 Opioid Prescribing Improvement Program Jeff Schiff, MD, MBA, Medical Director of Minnesota Health Care Programs Sarah Rinn, MPH, Opioid Prescribing Improvement Program Coordinator Agenda Opioid Prescribing
Opioid Prescribing Improvement Program Jeff Schiff, MD, MBA, Medical Director of Minnesota Health Care Programs Sarah Rinn, MPH, Opioid Prescribing Improvement Program Coordinator Agenda Opioid Prescribing
Chronic Pain and Opioids
 S E S S I ON T H I RT Y- FIVE Chronic Pain and Opioids Introduction Welcome to the Chronic Pain and Opioids session of the Living in Balance program. This session focuses on issues related to managing
S E S S I ON T H I RT Y- FIVE Chronic Pain and Opioids Introduction Welcome to the Chronic Pain and Opioids session of the Living in Balance program. This session focuses on issues related to managing
The Integrative Pain Management Program: A Pilot Clinic Serving High-Risk Primary Care Patients with Chronic Pain
 The Integrative Pain Management Program: A Pilot Clinic Serving High-Risk Primary Care Patients with Chronic Pain IM4US CONFERENCE 25 AUGUST 2017 EMILY HURSTAK, MD, MPH, MAS SAN FRANCISCO DEPARTMENT OF
The Integrative Pain Management Program: A Pilot Clinic Serving High-Risk Primary Care Patients with Chronic Pain IM4US CONFERENCE 25 AUGUST 2017 EMILY HURSTAK, MD, MPH, MAS SAN FRANCISCO DEPARTMENT OF
Pain Management and PACT
 Pain Management and PACT Overview Chronic pain in primary care Integrating pain care management with PCMHI for PACT approach Research results: An intervention to help manage chronic pain in primary care
Pain Management and PACT Overview Chronic pain in primary care Integrating pain care management with PCMHI for PACT approach Research results: An intervention to help manage chronic pain in primary care
From Opioid Overdose Prevention to Community Resilience CAPT Jeffrey Coady, Psy.D., ABPP SAMHSA Regional Administrator (Region 5)
") From Opioid Overdose Prevention to Community Resilience CAPT Jeffrey Coady, Psy.D., ABPP SAMHSA Regional Administrator (Region 5) Region 5 Fatherhood Initiative October 24, 2017 Today s Presentation Public
From Opioid Overdose Prevention to Community Resilience CAPT Jeffrey Coady, Psy.D., ABPP SAMHSA Regional Administrator (Region 5) Region 5 Fatherhood Initiative October 24, 2017 Today s Presentation Public
Assessment and Management of Chronic Pain Guideline Summary
 I CSI I NSTITUTE FOR CLINICAL S YSTEMS IMPROVEMENT Implementation Tool: Assessment and Management of Chronic Pain Guideline Summary Assessment Algorithm A = Annotation 1 Patient has pain 2 Critical first
I CSI I NSTITUTE FOR CLINICAL S YSTEMS IMPROVEMENT Implementation Tool: Assessment and Management of Chronic Pain Guideline Summary Assessment Algorithm A = Annotation 1 Patient has pain 2 Critical first
Missouri Guidelines for the Use of Controlled Substances for the Treatment of Pain
 Substances for the Treatment of Pain Effective January 2007, the Board of Healing Arts appointed a Task Force to review the current statutes, rules and guidelines regarding the treatment of pain. This
Substances for the Treatment of Pain Effective January 2007, the Board of Healing Arts appointed a Task Force to review the current statutes, rules and guidelines regarding the treatment of pain. This
Medication Management
 Marina Treglia, AGPCNP BC April 4, 2019 Medication Management Identify patient criteria for risk mitigation in a medication management program at a multidisciplinary pain clinic Discuss opioid discontinuation
Marina Treglia, AGPCNP BC April 4, 2019 Medication Management Identify patient criteria for risk mitigation in a medication management program at a multidisciplinary pain clinic Discuss opioid discontinuation
NORTHWEST AIDS EDUCATION AND TRAINING CENTER. Opioid Use Disorders. Joseph Merrill M.D., M.P.H. University of Washington April 10, 2014
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER Opioid Use Disorders Joseph Merrill M.D., M.P.H. University of Washington April 10, 2014 Opioid Use Disorders Importance of opioid use disorders Screening and
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Opioid Use Disorders Joseph Merrill M.D., M.P.H. University of Washington April 10, 2014 Opioid Use Disorders Importance of opioid use disorders Screening and
No disclosures for any of the speakers!
 Opiate Use Disorders and Pain in the elderly: Integrating care with the pain specialist Gabriel Paulian M.D Christopher Ong, M.D Yuliet Sanchez, M.D Uma Suryadevara, M.D No disclosures for any of the speakers!
Opiate Use Disorders and Pain in the elderly: Integrating care with the pain specialist Gabriel Paulian M.D Christopher Ong, M.D Yuliet Sanchez, M.D Uma Suryadevara, M.D No disclosures for any of the speakers!
HOPE. Considerations. Considerations ISING. Safe Opioid Prescribing Guidelines for ACUTE Non-Malignant Pain
 Due to the high level of prescription drug use and abuse in Lake County, these guidelines have been developed to standardize prescribing habits and limit risk of unintended harm when prescribing opioid
Due to the high level of prescription drug use and abuse in Lake County, these guidelines have been developed to standardize prescribing habits and limit risk of unintended harm when prescribing opioid
Substance Abuse Level of Care Criteria
 Substance Abuse Level of Care Criteria Table of Contents SUBSTANCE ABUSE OUTPATIENT: Adolescent... 3 SUBSTANCE ABUSE PREVENTION: Adult... 7 OPIOID MAINTENANCE THERAPY: Adult... 8 SUBSTANCE ABUSE INTERVENTION:
Substance Abuse Level of Care Criteria Table of Contents SUBSTANCE ABUSE OUTPATIENT: Adolescent... 3 SUBSTANCE ABUSE PREVENTION: Adult... 7 OPIOID MAINTENANCE THERAPY: Adult... 8 SUBSTANCE ABUSE INTERVENTION:
Nociceptive Pain. Pathophysiologic Pain. Types of Pain. At Presentation. At Presentation. Nonpharmacologic Therapy. Modulation
 Learning Objectives Effective, Safe Analgesia An Approach to Appropriate Outpatient Chronic Pain Treatment By the end of this presentation, participants will be able to: Identify multiple factors that
Learning Objectives Effective, Safe Analgesia An Approach to Appropriate Outpatient Chronic Pain Treatment By the end of this presentation, participants will be able to: Identify multiple factors that
Effective Treatment: Doing the Right Thing, In the Right Way. Terrence D Walton, MSW, ICADC
 Effective Treatment: Doing the Right Thing, In the Right Way Terrence D Walton, MSW, ICADC Monitor Manage Impact 1. Understand the Treatment Field, including Evidenced Based Practices 2. Understand Your
Effective Treatment: Doing the Right Thing, In the Right Way Terrence D Walton, MSW, ICADC Monitor Manage Impact 1. Understand the Treatment Field, including Evidenced Based Practices 2. Understand Your
Pediatric Primary Care Mental Health Specialist Certification Exam. Detailed Content Outline
 Pediatric Primary Care Mental Health Specialist Certification Exam Detailed Content Outline Description of the Specialty The Pediatric Primary Care Mental Health Specialist (PMHS) builds upon the Advanced
Pediatric Primary Care Mental Health Specialist Certification Exam Detailed Content Outline Description of the Specialty The Pediatric Primary Care Mental Health Specialist (PMHS) builds upon the Advanced
Drug Overdoses A Public Health Problem. Marianne Cloeren, MD, MPH, FACOEM, FACP 10/2/2013. Objectives
 Drug Overdoses A Public Health Problem Marianne Cloeren, MD, MPH, FACOEM, FACP 10/2/2013 Objectives O Provide an overview of the trends in opioid prescriptions and impact O Consider implications for the
Drug Overdoses A Public Health Problem Marianne Cloeren, MD, MPH, FACOEM, FACP 10/2/2013 Objectives O Provide an overview of the trends in opioid prescriptions and impact O Consider implications for the
Vermont. Prescribing and Dispensing Profile. Research current through November 2015.
 Prescribing and Dispensing Profile Vermont Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points of
Prescribing and Dispensing Profile Vermont Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points of
Screener and Opioid Assessment for Patients with Pain- Revised (SOAPP -R)
") Screener and Opioid Assessment for Patients with Pain- Revised (SOAPP -R) The Screener and Opioid Assessment for Patients with Pain- Revised (SOAPP -R) is a tool for clinicians to help determine how much
Screener and Opioid Assessment for Patients with Pain- Revised (SOAPP -R) The Screener and Opioid Assessment for Patients with Pain- Revised (SOAPP -R) is a tool for clinicians to help determine how much
Readopt with amendment Med 502, effective (Document #11090), to read as follows:
, to read as follows:") Adopted Rules 11-2-16 1 Readopt with amendment Med 502, effective 5-3-16 (Document #11090), to read as follows: PART Med 502 OPIOID PRESCRIBING Med 502.01 Applicability. This part shall apply to the prescribing
Adopted Rules 11-2-16 1 Readopt with amendment Med 502, effective 5-3-16 (Document #11090), to read as follows: PART Med 502 OPIOID PRESCRIBING Med 502.01 Applicability. This part shall apply to the prescribing
ROLE PLAY #1: ASSESSMENT WITH THE 6 A s PATIENT ROLE
 ROLE PLAY #1: ASSESSMENT WITH THE 6 A s PATIENT ROLE You are a 58 year old man/woman and have a history of severe chronic low back pain for 20 years. You injured your back 20 years ago at work and have
ROLE PLAY #1: ASSESSMENT WITH THE 6 A s PATIENT ROLE You are a 58 year old man/woman and have a history of severe chronic low back pain for 20 years. You injured your back 20 years ago at work and have
Mood Disorders for Care Coordinators
 Mood Disorders for Care Coordinators David A Harrison, MD, PhD Assistant Professor, Dept of Psychiatry & Behavioral Sciences University of Washington School of Medicine Introduction 1 of 3 Mood disorders
Mood Disorders for Care Coordinators David A Harrison, MD, PhD Assistant Professor, Dept of Psychiatry & Behavioral Sciences University of Washington School of Medicine Introduction 1 of 3 Mood disorders
Applying Universal Precautions to Chronic Opioid Therapy 5P s Assessment
 Elements of Leverage Point #3: Applying Universal Precautions to Chronic Opioid Therapy 1. Diagnosis with reasonable differential 2. Psychological assessment including risk of addictive disorders Purpose
Elements of Leverage Point #3: Applying Universal Precautions to Chronic Opioid Therapy 1. Diagnosis with reasonable differential 2. Psychological assessment including risk of addictive disorders Purpose
Choosing Life: Empowerment, Action, Results! CLEAR Menu Sessions. Substance Use Risk 5: Drugs, Alcohol, and HIV
 Choosing Life: Empowerment, Action, Results! CLEAR Menu Sessions Substance Use Risk 5: This page intentionally left blank. Session Aims: (70 Minutes) To understand the health consequences of drugs and
Choosing Life: Empowerment, Action, Results! CLEAR Menu Sessions Substance Use Risk 5: This page intentionally left blank. Session Aims: (70 Minutes) To understand the health consequences of drugs and
Tennessee. Prescribing and Dispensing Profile. Research current through November 2015.
 Prescribing and Dispensing Profile Tennessee Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
Prescribing and Dispensing Profile Tennessee Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
Bipolar Disorder Clinical Practice Guideline Summary for Primary Care
 Bipolar Disorder Clinical Practice Guideline Summary for Primary Care DIAGNOSIS AND CLINICAL ASSESSMENT Bipolar Disorder is categorized by extreme mood cycling; manifested by periods of euphoria, grandiosity,
Bipolar Disorder Clinical Practice Guideline Summary for Primary Care DIAGNOSIS AND CLINICAL ASSESSMENT Bipolar Disorder is categorized by extreme mood cycling; manifested by periods of euphoria, grandiosity,
UNDERSTANDING DEPRESSION Young Adult: Get the Facts
 UNDERSTANDING DEPRESSION Young Adult: Get the Facts What does it mean when a heath care professional says depression? Hearing a health care professional say you have depression can be confusing. The good
UNDERSTANDING DEPRESSION Young Adult: Get the Facts What does it mean when a heath care professional says depression? Hearing a health care professional say you have depression can be confusing. The good
Learning Objectives. Serving Pregnant Women Affected by Substance Use Disorders in Healing to Wellness Court: Sharing Lessons
 Serving Pregnant Women Affected by Substance Use Disorders in Healing to Wellness Court: Sharing Lessons Marianna Corona Jennifer Foley September 12, 2017 Learning Objectives 2017 Improving Family Outcomes
Serving Pregnant Women Affected by Substance Use Disorders in Healing to Wellness Court: Sharing Lessons Marianna Corona Jennifer Foley September 12, 2017 Learning Objectives 2017 Improving Family Outcomes
Behavioral Comorbidities in Chronic Pain. Christopher Sletten, Ph.D. Mayo Clinic Florida MFMER slide-1
 Behavioral Comorbidities in Chronic Pain Christopher Sletten, Ph.D. Mayo Clinic Florida 2015 MFMER slide-1 Chronic Pain 2015 MFMER slide-2 Chronic Pain Characteristics Enduring symptoms Elusive causes
Behavioral Comorbidities in Chronic Pain Christopher Sletten, Ph.D. Mayo Clinic Florida 2015 MFMER slide-1 Chronic Pain 2015 MFMER slide-2 Chronic Pain Characteristics Enduring symptoms Elusive causes
Trigger. Myths About the Use of Medication in Recovery BUPRENORPHINE TREATMENT: A TRAINING FOR MULTIDISCIPLINARY ADDICTION PROFESSIONALS
 BUPRENORPHINE TREATMENT: A TRAINING FOR MULTIDISCIPLINARY ADDICTION PROFESSIONALS Module VI Counseling Buprenorphine Patients Myths About the Use of Medication in Recovery! Patients are still addicted!
BUPRENORPHINE TREATMENT: A TRAINING FOR MULTIDISCIPLINARY ADDICTION PROFESSIONALS Module VI Counseling Buprenorphine Patients Myths About the Use of Medication in Recovery! Patients are still addicted!
VOLUME B. Elements of Psychological Treatment
 VOLUME B Elements of Psychological Treatment VOLUME B MODULE 1 Drug dependence and basic counselling skills Biology of drug dependence Principles of drug dependence treatment Basic counselling skills for
VOLUME B Elements of Psychological Treatment VOLUME B MODULE 1 Drug dependence and basic counselling skills Biology of drug dependence Principles of drug dependence treatment Basic counselling skills for