First Percutaneous Laser Ablation Network (PLAN) educational initiative on laser ablation for liver tumors
|
|
|
- Piers Lawson
- 5 years ago
- Views:
Transcription

 educational")


1 7-8 July, Naples, Italy First Percutaneous Laser Ablation Network (PLAN) educational initiative on laser ablation for liver tumors IMPROVING THE PATIENT S LIFE THROUGH MEDICAL EDUCATION
2 Disclosure Giovan Giuseppe Di Costanzo Department of Transplantation Liver Unit Cardarelli Hospital Naples, Italy Advisory board Bayer, Abbvie.
3 Objectives Acquire knowledge of the laser physics and interaction laser-tissue Learning the basic concepts of the laser ablation with multifiber technique Laser ablation in literature Complications post-laser ablation Ablation of hard-to-treat hepatic nodules Translating all the aforementioned into clinical practice: towards a tailored approach Clinical cases
4 INTRODUCTION HYPERTERMIC ABLATION
 b) thermal")
 c) non")
5 Percutaneous ablation a) chemical (PEI, PAI) b) thermal - hyperthermic (RFA, MW, LA) - hypothermic (CRYO) c) non thermal (IRE)
6 Image-guided Tumor Ablation: Standardization of Terminology and Reporting Criteria The term Laser Ablation (LA) should replace terminology such as laser interstitial tumor therapy (or LITT), laser coagulation therapy, and laser interstitial photocoagulation. This term should be used for all types of ablation using light energy. Radiology 2014
7 Hyperthermic injury Mechanisms - Direct - Indirect or delayed Chu et al, Nature Reviews 2014
8 Chu et al, Nature Reviews 2014 Hyperthermic injury Direct effects - Changes to cell membrane integrity - Mitochondrial disfunction - Inhibition of DNA replication *- tumor tissue is more thermosensitive than normal tissue
9 Laser Ablation of Biological Tissue Biological effect of heat on tissue Thermoablation: induced necrosis of tissue due to local temperature increasing Temperature effects on tissue >300 C >100 C Fusion, sublimation Charring, carbonizzation 100 C Vapour bubble creation, mechanical rupture 60 C >50 C 42 C - 50 C Denaturation of protein and collagene, coagulation Decreased enzymatic activity, lost of cellular recovery mechanism Hyperthermia, bond destruction, modification of cell membrane Cancer cells have a heath resistance threshold lower than non cancer cells
10 Brace et al.radiology 2007
11 Temperatue [ C] Laser Ablation of Biological Tissue Biological effect of heat on tissue Irreversible necrosis of cells occurs for a joint action of local temperature and exposure time Cellular death occurs within few seconds for a temperature > 60 C irreversible cellular damage At 50 C irreversible damage occurs for an exposure time of few minutes reversible cellular damage Exposure time [s] For temperatures lower than 50 C necrosis occurs for exposure time in the order of decades of minutes Critical temperature for cellular death. Henriques (1947), Eichler, Seiler (1991)
12 Chu et al, Nature Reviews 2014 Hyperthermic injury Indirect or delayed effects - Induction of apoptosis - Vascular damage > ischemia - Release of lysosomal contents - Granulocytes chemotaxis - Cytokine release - Stimulation of immune response

13 Chu et al, Nature Reviews 2014

14 Microscopic changes after laser ablation At 6 At 12 h At 24 h At 48 h At 7 days Fujitomi, Lasers Surg & Med, 1999

15 Nikfarjam, Laser Surg Med 2005
16 Progressive Microvascular Injury in Liver and Colorectal Liver Metastases Following Laser Ablation Nikfarjam, Laser Surg Med 2005

17 Induction of Th1 immune responses following laser ablation in a murine model of colorectal liver metastases Lin et al. J Transl Med 2011
18 Lin et al. J Transl Med 2011
19 LASER PHYSICS INTERACTION LASER-TISSUE

20 Laser Ablation of Biological Tissue L.A.S.E.R. Light Amplification by Stimulated Emission of Radiation In laser ablation tissue heating occurs by means of Laser radiation which is absorbed by tissue increasing the local temperature
21 Laser working principles Monochromatic: single wavelenght Collimation: low divergence, concentrating high energies in limited areas Coherence: temporal and spatial, all the photons are in phase

22 Aesthet Surg J. 2013: doi: / x Date of download: 2/9/ The American Society for Aesthetic Plastic Surgery, Inc.
23 Absorption coefficient [cm-1] Laser Ablation of Biological Tissue Laser to tissue interaction A wavelength range (λ) exists, where light has good penetration into tissues: all thermal ablation applications are applied in this wavelength range known as therapeutic window Therapeutic window Nd:YAG Water H2O In therapeutic window, tissues show a low radiation absorption and consequently excellent light penetration Therapeutic window is limited at lower wavelength due to hemoglobin absorption (oxygenated HbO2 and not oxygenated Hb ) and at upper wavelength due to water absorption 10-1 Hemoglobin Hb Wavelenght [nm]
.")

24 Laser Ablation of Biological Tissue Why it s better to talk about energy (instead of time) If a man digs a hole in the ground, his body will consume a quantity of energy (that it previously takes by food). Energy is the work we must do to achieve a particular result If the man takes one day or 1 hour to terminate the work depends on the power he s able to put on Power is the ratio between Work and Time If we want to ablate a nodule of a specified volume we have a specific work to do and hence we have to spend a fixed energy i.e the energy dose. The Power we use for accomplished this duty define the time duration of treatment. The higher the power we use, the less is the treatment time



25 Laser Ablation of Biological Tissue Laser Ablation of tissue is a threshold phenomenon Ablation threshold 1,4-1,5W Over ablation threshold Under ablation threshold


26 Laser Ablation of Biological Tissue Ex-vixo bovine experimentation 3 Volume vs Power (Fixed dose 1200J) Power [W] Minor axis [cm] Mayor axis [cm] Volume [cm^3]
![Volume [ml] Laser Ablation of Biological](/docs-images/93/113057152/images/27-0.jpg "Tissue Coagulation Volume vs Energy Dose")



27 Volume [ml] Laser Ablation of Biological Tissue Coagulation Volume vs Energy Dose with a single fiber Energy 600J Energy 1200J Energy 1800J Energy 2400J Coagulation Volume Calculation evaluation of the ellipsoidal area over the treated zone computation of the volume by rotation of the ellipse 3,0 2,5 2,0 1,5 1,0 0,5 0, Energy [J]
 If threshold for ablation is achieved a cavity starts to grow with vapor formation Ablation front is moving forward.")
28 Laser Ablation of Biological Tissue Thermal damage dynamics during Laser irradiation* Start lasing Initial spherical coagulation occurs around the fiber tip (changing in optical properties from native to coagulated tissue) If threshold for ablation is achieved a cavity starts to grow with vapor formation Ablation front is moving forward. Tissue is coagulated, dehydrated and vaporized in a cyclic leading to a well defined cavity in the center Moving front velocity decreases with cavity enlargement leading to an asymptotic limit of treated volume *R M Verdaasdonk, Explosive onset of continuous wave laser tissue ablation Physics in Medicine & Biology, Volume 35, Number 8
29 Laser Ablation of Biological Tissue Thermal damage dimension produced by a single source Laser ablation produces a volume of necrosis of mm x 8-10 mm for standard parameters (5W and 1800J, fiber flat tip) in the liver tissue Longitudinal section Cross section thickness 8-10 mm Lenght mm

")


30 Laser Ablation of Biological Tissue In-Vivo Laser Ablation: biological effects at histology Porcine hepatic tissue in vivo (1h after treatment) Hyperaemic margin 4x Fiber position Necrosis margin 10x 4x <Dehydrated Tissue <Coagulated Tissue with vacuoles < Carbonized Tissue Not treated healthy tissue 4x

")
31 Laser Ablation of Biological Tissue Flat-tip ablation: tissue charring Charring occurs due to high temperature achieve during LA even if carbon layer is very thin (range micron) 10x

32 From: Elesta brochure

33

34

35

36

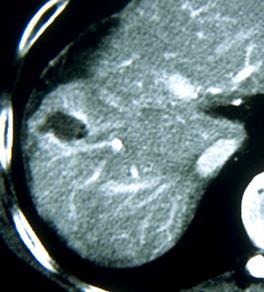
37 CT at 24 hours


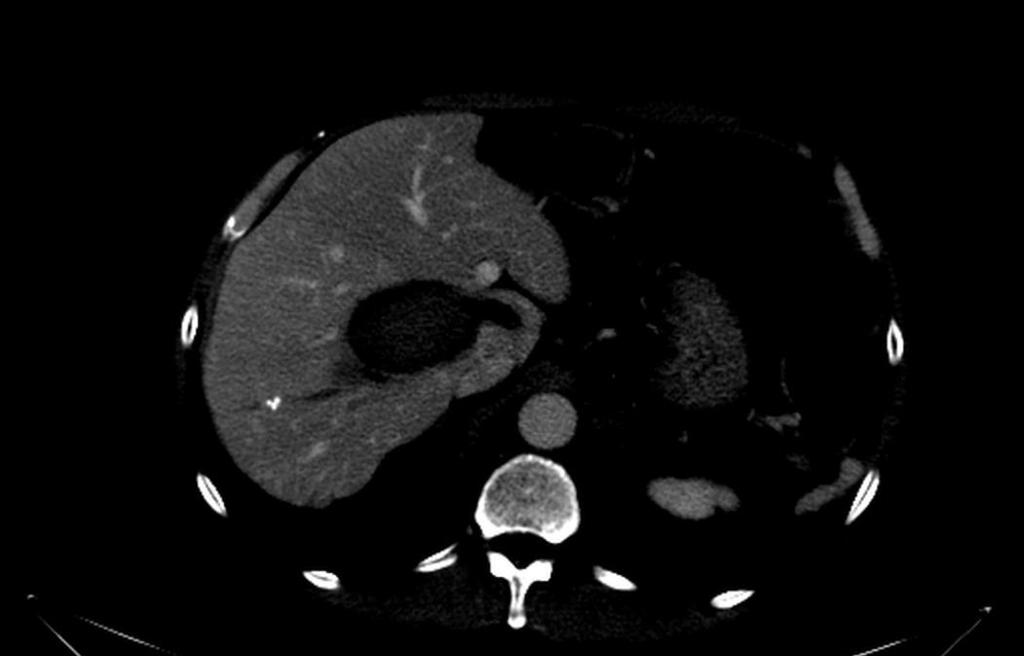
38 CT at 4 weeks

39 Hot cylindrical tip and flat tip


40 Precision: sharp transition zone between dead and viable tissue Transition zone in RF and Cryo can be 5-10 mm Visualase transition zone is less than 1 mm
41 Laser technology Diffuser tips are used to improve applicator heating profiles, and higher powers can offset the reduced penetration depth by increasing local temperatures, but when higher powers are used, fibers must been cooled to avoid skin burns or probe failure. hot cylindrical tip Cooling increases the diameter of each applicator. Larger ablation volumes are typically realized by using multiple applicators, which can be operated independently and simultaneously.

42 Laser technology the main disavantages is a caliber of 9 F (3mm); it is really hard to place without risks this type of device in cirrhotic patients!!!

43 2 fiber approach Laser Ablation of Biological Tissue Multi-fiber approach: Volume Amplification If required by the size or shape of the lesion to be treated, it is possible to use a multi-fiber approach. 3 cm Simultaneous delivery Ex vivo pig liver treated by 2 fibers spaced at 15mm Power 5W, Energy delivered 3600J, Time duration 6 minutes
44 Micro-invasiveness : Strong points of Laser Ablation Very thin needles and fiber optic (300 microns) are totally atraumatic for the patient: fewer complications and side effects, less risk of infection and bleeding, no general anaesthesia, short recovery times. These needles do not cause scarring and ensure excellent aesthetic results Control of the shape of coagulative necrosis : laser ablation produces highly repeatable thermal lesions with clearly defined edges; the multifiber approach in a geometrically known area gives rise to lesions with a predictable and controllable shape confinement in respect of the viable parts and critical areas of the organs; Safety: the quartz optic fibers (dielectric material) do not interact with external electromagnetic field, are biocompatible and ensure electric isolation between instrumentation and patient. Can also be used in magnetic resonance. Speed: Laser Ablation of Biological Tissue A single illumination lasts 4-6 minutes
45 Laser Ablation of Biological Tissue Energy dose per treatment: Laser Ablation vs MWA vs RFA Laser Ablation exploits a very effective mechanism of conversion from EM field to heat Laser MW RF Is like cooking an egg at fixed time Key point Fast treatment time Laser Ablation employ lowest energy dose to achieve tumor ablation as compared to MW and RF
46 BASIC CONCEPTS OF THE LASER ABLATION WITH MULTIFIBER TECHNIQUE

47 Laser ablation <15mm 15 mm 15 mm >25mm <25mm
48 Laser Ablation of Biological Tissue Multi-fiber approach In Multi-fiber approach laser energy is delivered simultaneously. The result is a synergic coalescence action allows for obtaining large volumes of ablation with perfect control of the edges even with large-sized lesions. possibility of treating extensive lesions; possibility of adapting the treatment to the shape and position of the lesion; possibility of treating critical lesions (high risk due to being close to vital structures); positioning of the fine needles with minimum trauma for the organ with the possibility of multiple re-positioning; the multi-fiber technique with fine needles is extremely well tolerated by the patient (reduced risk of side effects)
49 J. Heisterkamp, Lasers Med Sci 1999 Laser Ablation of Biological Tissue Multi-fiber approach: ablation volume vs mutual fiber distance

50 1 cm 2 cm 4 cm J. Heisterkamp, Lasers Med Sci 1999

51 Laser Ablation of Biological Tissue Multi-fiber approach: importance of fiber mutual distance Anatomic slices 4mm-spaced in ex-vivo ablation of porcine liver Power = 5W Energy = 1800J MD= 3.2cm; md = 2.3 cm; Depth = 3.2 cm; Volume = 12.3cm^3 Fiber distance of 1.5cm assures single fiber volume coalescence maximum volume of coagulation
52 Laser system based on EchoLaser device Laser Type: Solid state (diode) Number of Sources: 4 independent in activation and emission Wavelength: 1064nm Emission Mode: CW Maximum Power (CW): 7 W per fibre Output Mode: Multimode Aiming Beam: Diode laser nm Nominal Ocular Hazard Distance (NOHD): 4 m Control Panel: LCD Colour Touch Screen SMA 905 optical connector 1.5m length 300 μm core diameter
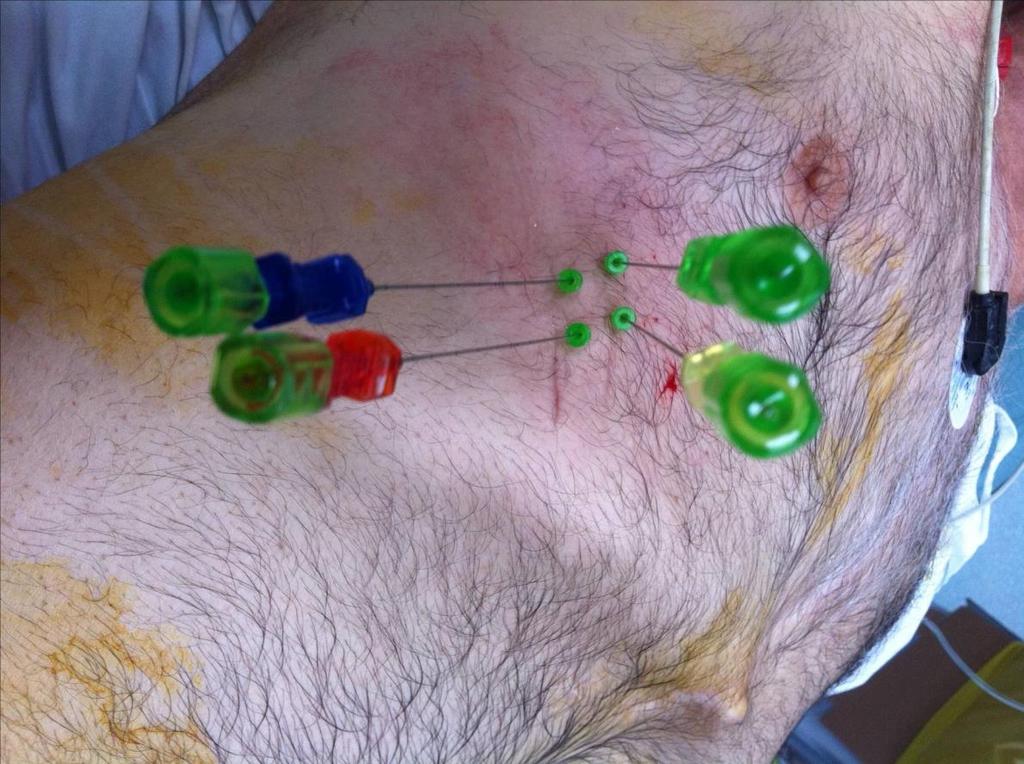
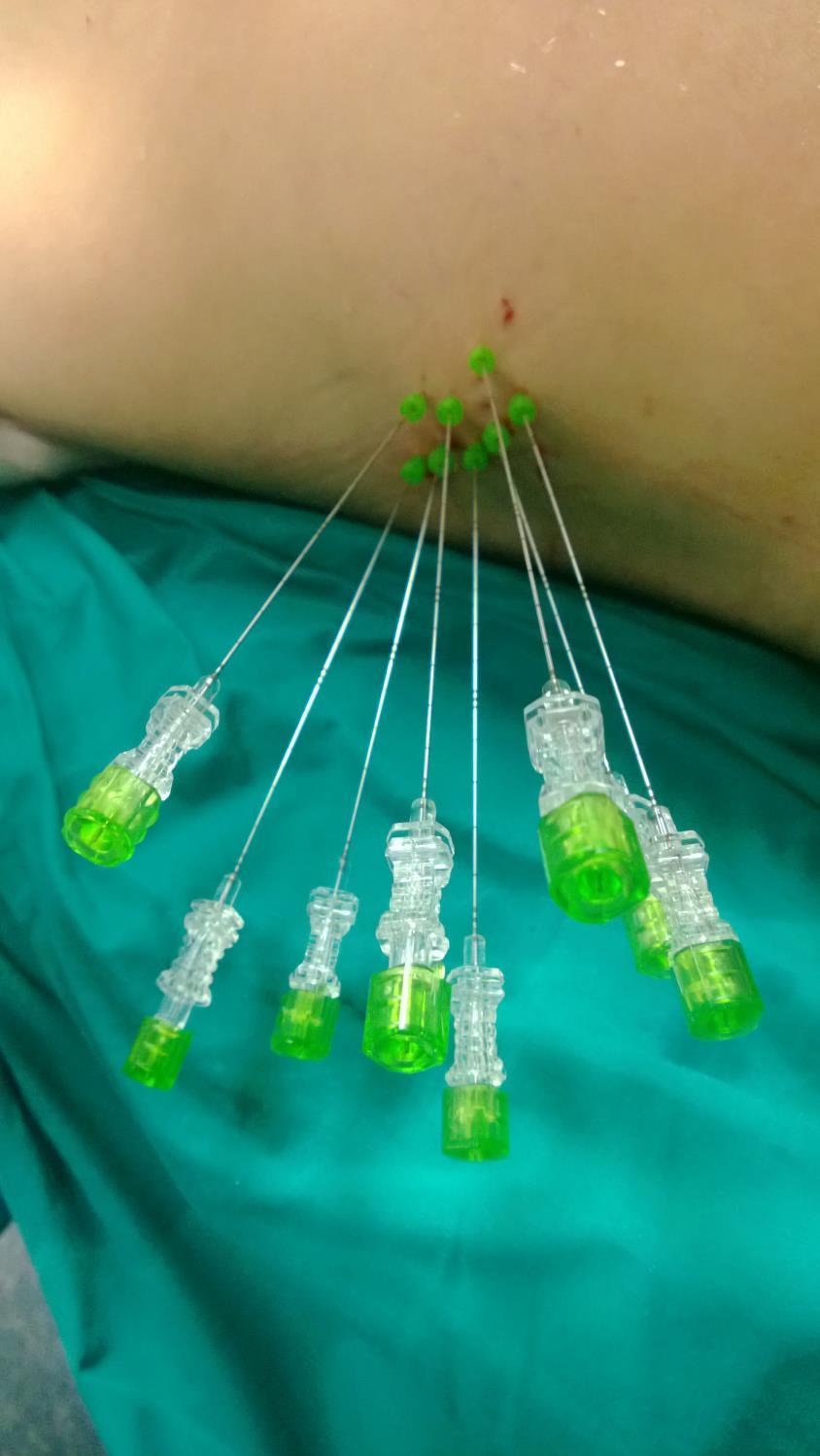
53 Laser kit According to nodule volume, one to eight 300 µm optic fibers advanced in 21-G (0.7mm) needle are positioned into the target lesion under US guide. A single optimal illumination is considered when Joules/fiber are delivered in 4-6 min at 5 W.
54 Laser technology CM Pacella, G.Bizzarri, Z. Rossi La fotocoagulazione interstiziale laser nel trattamento del piccolo epatocarcinoma. Esperienza preliminare in dieci casi. IX Corso Nazionale di Aggiornamento in Ecografia Operativa. Salsomaggiore Terme, Marzo 1991.
 laser source : flat-tip fiber (0.33mm) needle 21 G = 0.8mm optical fiber = 0.")
55 Pacella s technique: flat tip technique introducer sheath : needle 21G (0.8mm) laser source : flat-tip fiber (0.33mm) needle 21 G = 0.8mm optical fiber = 0.33mm laser beam =18mm needle 21G=0.8mm optical fiber=0.3mm 10mm
56 Laser Ablation (LA) liver ablation technique: different US guidance systems Claudio Maurizio Pacella, Regina Apostolorum Hospital, Rome, Italy Giovan Giuseppe Di Costanzo, Cardarelli Hospital, Naples, Italy





57 Laser Ablation (LA) liver ablation technique: different US guidance systems Claudio Maurizio Pacella, Regina Apostolorum Hospital, Rome, Italy Giovan Giuseppe Di Costanzo, Cardarelli Hospital, Naples, Italy



58





59 Laser Ablation of Biological Tissue Multi-fiber approach 4 fiber approach Porcine liver ex vivo 4 fibers at 1.5cm, 5W, 7200J, 6 minutes 3cm HCC treated with multi-fiber technique with 5W, 7200J, 6 minutes

60

61

62

63

64

65

66

67

68

69

70

71

72

73

74

75

76

77

78
79


80
81 LASER ABLATION IS A VERY FLEXIBLE TECHNIQUE: IT MAY ADAPT TO DIFFERENT SHAPE OF CANCER NODULES

82

83

84

85
86 LASER ABLATION IN LITERATURE
87 Author Yr Pts/Ts Ts size CA (%) LR (%) OS/ 3yr (%) OS/5yr (%) Major Compl (%) Mortality (%) Giorgio 2000 Pacella / Child C 30/30 30/15 > TACE Child C Pacella 2001 Eichler 2001 Pacella 2005 Pacella 2006 Pacella 2009 Francica 2012 Francica 2012 Eichler 2012 Di Costanzo 2013 Di Costanzo 2013 (RCT) 74/92 Child A / ys (m) 82/ /169 Child A 432/548* Child A 106/116 58/66 116/132 a.m. 7.5mm w.d local & distant (m) 53 (m) 65 (m) w.d. 68 (m) w.d / / /80 (LA) 70/77 (RF)
88 Effectiveness and outcome data tumor size, tumor location, and complete ablation were the main factors affecting the outcomes. using multiple bare fibres introduced through 21-gauge needles positioned under US-guidance, the reported complete response rate ranges from 82% to 97%. in lesions in high-risk sites, complete response is 95.5%. in patients with monofocal HCC 4 cm or three nodules 3 cm each, reported cumulative survival rates at 3 and at 5 years range from 52% to 68% and from 15% to 34%, respectively.
89 Effectiveness and outcome data in a multicenter study, Child s class A patients had a 5-year cumulative survival of 41%; the median survival time was 65 mo with tumor size 3 cm and 68 mo in patients with well-differentiated tumor size 2 cm. the ideal candidates for LA are younger patients with serum albumin within the normal range and a tumor size 2 cm in whom it is very likely that complete ablation will be achieved. the median time to recurrence was 24 mo and the median disease-free survival time was 26 mo. like RFA and microwaves ablation (MWA), LA resulted safe and effective also in the treatment of cirrhotic patients awaiting liver transplantation

90
91 Size Complete ablation 2 cm (n=215) 85.1% 2-3 cm (n=242) 81.8% 3-4 cm (n=91) 60.4% Overall (n= 548) 79.6% Pacella, et al JCO 2009
92 Pacella, et al JCO 2009

93 Pacella, et al JCO 2009

94
95

96
97 Radiofrequency ablation versus laser ablation for the treatment of small hepatocellular carcinoma in cirrhosis: a randomized controlled trial GG Di Costanzo, R Tortora, G D'Adamo, A Galeota Lanza, F Lampasi, L Addario, M De Luca, F Zanfardino, MT Tartaglione, S Mattera, CM Pacella Liver Unit, Cardarelli Hospital, Napoli, Italy ClinicalTrials.gov identifier: NCT J Gastroenterol Hepatol, 2015
98 LA pros LA vs RFA - Thin needles (21 vs 17G) - Less time for ablation of the tissue (for a nodule of 3cm: 4-6 vs 12 min) - More precise - Less expensive (cost of the devices: RFA 1,600 - LA 300 per fiber) LA cons - Multiple needle insertion
99 Primary Outcome Measure Complete tumor ablation (CTA) Absence of any intratumoral contrast enhancement on CT or MRI imaging four weeks after treatment Secondary Outcome Measures Time to local recurrence (TTLR) Time from complete tumor ablation to reappearance of arterial enhancement on CT or MRI in a treated tumor Overall survival (OS) Time from randomization to death J Gastroenterol Hepatol, 2015

100 Sample size calculation Noninferiority RCT: complete necrosis of HCC nodules: (LA 86% 1-2 RFA 96% 3-5 ) noninferiority margin = 10% power of 80% for a 1-sided test significant level patients would be required in each group 1. Pacella, 2006; 2. Pacella, 2009; 3.Lencioni, 2003; 4.Lin, 2004; 5. Shiina, 2005.
101 Inclusion Criteria Patients (18-85ys) with unresectable HCC or who refused surgery A solitary HCC 5.0cm in diameter, or multiple HCC 3 lesions, each 3.0cm in diameter Child-Pugh class A or B Platelet count of > 40,000/mm 3, INR < 2.0 No previous treatment of HCC
102 Exclusion Criteria History of encephalopathy or refractory ascites Vascular invasion or extrahepatic metastasis Nodules unsuitable for RFA/LA: a. tumors located within 5 mm of liver hilum or the main bile duct branches ; b. not visible on US; Other severe concomitant diseases that may reduce life expectancy
103 432 naive patients (1/09-09/12) n % Resection n % BCLC 0-A BCLC B BCLC C OLT RFA/LA unfeasible Decompensated Comorbidity/ref usal Enrolled J Gastroenterol Hepatol, 2015
104 Patients and methods 140 patients with 157 HCC nodules randomly received either RFA (n=70) or LA (n=70) treatment. If indicated, over a period of 6 months, treatment was repeated up to three times. 4 weeks after ablation, CT or MRI imaging was used to evaluate the necrosis of the HCC nodules according to mrecist.
105 Treatment failure: if, after 3 ablations, CT or MRI showed a residual nodule activity In case of treatment failure, transarterial chemoembolization was used To evaluate TTLR and OS in the two treatment groups, Kaplan-Meier figures and log-rank test were used
106 Results RFA n=70 LA n=70 Males, n (%) 53 (75.7) 47 (67.1) Median age (range) 70 (50-83) 70 (36-84) HCV, n (%) 53 (75.7) 60 (85.7) Child A, n (%) 63 (90.0) 67 (95.7) Median MELD score (range) 9.0 (6-17) 8.5 (6-21) F1 varices, n (%) 16/64 (25.0) 16/62 (25.8) F2-F3 varices, n (%) 20/64 (31.3) 15/62 (24.2) Platelet count <100, (58.6) 37 (52.9) J Gastroenterol Hepatol, 2015
107 RFA n=70 LA n=70 Single nodule, n (%) 63 (90.0) 61 (87.1) Number of nodules Diameter mm, median (range) 25 (14-44) 25 (7-50) Diameter 30mm, n (%) 20 (26.0) 30 (37.5) Subcapsular/exophytic 9 13 Adjacent large vessels 2 8 Edmondson grade I-II, n (%) 27/48 (56.3) 36/54 (66.7) AFP ng/ml,median (range) 9 (1-1025) 20.5 (1-1526) AFP >200ng/mL, n (%) 4 (5) 9 (13) Median follow-up, months (range) 23 (6-52) 24 (5-55) J Gastroenterol Hepatol, 2015
108 Complete tumor ablation RFA LA Δ (95% CI) per patient, n (%; 95%CI) 68/70 (97.1; ) 67/70 (95.7; ) +1.4%* (-6.0% +9%) per nodule, n (%; 95%CI) 75/77 (97.4; ) 77/80 (96.3; ) +1.1%* (-5.7% +8.1%) J Gastroenterol Hepatol, 2015
109 Mean survival: - RFA = 71.2 months (95%CI, ) - LA = 74.0 months (95%CI, ) P = 0.579
110
111 Conclusions This is the first study that validates the use of LA for the treatment of HCC. LA resulted not inferior to RFA in achieving the CTA and therefore it should be considered as an evaluable alternative for thermal ablation of small HCC in cirrhotic patients. J Gastroenterol Hepatol, 2015
112 COMPLICATIONS POST-LASER ABLATION

 = 0.")
= 1.")
113 Complications Radiology 2008 In a multicenter study involving nine centers in Italy with 520 patients who underwent 1064 laser sessions for 647 HCCs. Milano Udine Bologna Deaths (4/520) = 0.76% Albano Laziale Pozzuoli Ancona Benevento Major complications (15/1004 )= 1.5% Casoria Minor complications (62/1004) = 7.2% Side effects 416/1011 = 41.1%
114 Complications Deaths (4/520) = 0.76%* Major complications (15/1004 )= 1.5%** Minor complications (62/1004) = 7.2%*** Side effects 416/1011 = 41.1% * all with HCCs > 3 cm, two Child-Pugh C **associated with excess of energy and high risk location ** *associated with excess of energy, high bilirubin level and low protrombin time low rate of intrahepatic and peritoneal bleeding (1.1%) and hepatic abscess 0.4%. No seeding

115

116

117

118
119 ABLATION OF HARD-TO- TREAT HEPATIC NODULES
120 Hard-to-treat nodules 1. Position a) high-risk location Adjacent large vessels: vena cava, first or second branch of the portal vein, the base of hepatic vein Adjacent to extrahepatic organs: gallbladder, gastrointestinal tract b) difficult-to-reach location I segment or liver dome Behind large vessels Behind TIPS 2. Size (> 3cm) 3. Multifocality
121 1. Thin needles LA pros 1. Very precise deliver of energy 1. Greatest flexibility 1. No heat sink effect
122

123






124 Lesions close to gallbladder ronconi0003.jpg






125 Exophitic lesion close to gallbladder and g.i. bowel




126 Exophitic lesion close to the stomach


127 Extrahepatic growth




128 Extrahepatic growth Before LA After LA
129
130

131

132

133

134
135
136

137
138
139
140

141

142

143

144
145 Heat-sink effect The term heat-sink effect refers to the buffering effect of patent blood vessels or ventilated bronchi adjacent to the ablation zone. The shape of the thermal zone of ablation is altered away from the vessel, and the overall ablation size is diminished. Although this phenomenon serves to protect blood vessels and prevent bleeding from large vessels, it is also a major source of incomplete tumor ablation in many studies involving thermal ablation. Image-guided Tumor Ablation: Standardization of Terminology and Reporting Criteria Radiology 2014

146 Heat sink effect Statli, et al; Diagn Interv Radiol 2012


147

148

149
150 LARGE HCC

151

152 Two-square configuration of the laser sources into large lesion of 6-cm-diameter mass


153
154 Total amount of energy that can be used : up to 50,000 joules Duration of treatment: up to 42 minutes

155

156
157

158

159

160

161

162
163

164

165
166 MULTIFOCAL HCC
 1 HCC or 3 nodules < 3 cm, PS 0 Intermediate stage (B) Multinodular, PS 0 Advanced stage (C) Portal invasion, N1, M1, PS 1 2 End stage (D) 1 HCC Portal pressure/ bilirubin Increased 3 nodules 3")
167 Treatment algorithm EASL, EORTC guidelines HCC Stage 0 PS 0, Child Pugh A Stage A C PS 0 2, Child Pugh A B Stage D PS > 2, Child Pugh C Very early stage (0) 1 HCC < 2 cm Carcinoma in situ Early stage (A) 1 HCC or 3 nodules < 3 cm, PS 0 Intermediate stage (B) Multinodular, PS 0 Advanced stage (C) Portal invasion, N1, M1, PS 1 2 End stage (D) 1 HCC Portal pressure/ bilirubin Increased 3 nodules 3 cm Associated diseases Normal No Yes Resection Liver transplantation PEI/RFA TACE sorafenib BSC Curative treatments (30%) Target: 20% Target: 40% Target: 10% 5-year survival (40 70%) OS: 20 mo (45-14) OS: 11 mo (6-14) OS: <3 mo PS, performance status; TACE, transarterial chemoembolization; BSC, Best Supportive Care EASL EORTC Clinical Practice Guidelines: Management of hepatocellular carcinoma Journal of Hepatology 2012 vol. 56 j Available on:

168 Laser ablation is superior to TACE in large sized hepatocellular carcinoma: a case control study LA TACE mm 51-60mm >61mm overall

169

170

171
172

173
174

175

176

177

178

179

180

181

182
183 TRANSLATING ALL THE AFOREMENTIONED INTO CLINICAL PRACTICE: TOWARDS A TAILORED APPROACH
184 TRANSLATING ALL THE AFOREMENTIONED INTO CLINICAL PRACTICE: TOWARDS A PATIENT-TAILORED APPROACH The reported local effectiveness and long-term outcomes obtained with LA are comparable with those of RFA. Specifically, in the subgroup of Child s class A cirrhotic patients with lesions 2 cm (BCLC 0-A) treated by LA, 5-year survival was equivalent to that of RFA. Thanks to thin needles and to the more effective tumoricidal action of heat compared to ethanol, we believe that LA could replace PEI in the treatment both of residual minimal viable tissue and of nodules at high-risk sites when RFA is not technically feasible.
185 TRANSLATING ALL THE AFOREMENTIONED INTO CLINICAL PRACTICE: TOWARDS A PATIENT-TAILORED APPROACH To completely ablate larger tumors (usually defined greater than 3 cm), a single ablation with RFA may be not be sufficient to entirely encompass the target volume. In these cases, multiple ovelapping ablations or simultaneous use of multiple applicators may be required to successfully treat the entire tumor and ablative margin, though accurate targeting and applicator placement can often be tecnically challenging.
186 TRANSLATING ALL THE AFOREMENTIONED INTO CLINICAL PRACTICE: TOWARDS A PATIENT-TAILORED APPROACH To obtain larger volumes of necrosis, a variety of devices of different shapes and designs used either with different algorithms or activated in different modes (consecutive, simultaneous, or switching) has been developed. In the treatment of large HCC ( 5 cm), conventional RFA is limited mainly by incomplete ablation, with reported complete ablation rate of 74% after single session in lesions between 3 and 5 cm and of 62% in tumours > 5 cm after multiple sessions. Using three internally cooled bipolar electrodes complete, ablation rates of 81% has been reported. Guglielmi A et al. Hepatogastroenterology ; 50: [PMID: ] Seror O et al, Radiology 2008; 248: [PMID: DOI: /radiol ]
187 TRANSLATING ALL THE AFOREMENTIONED INTO CLINICAL PRACTICE: TOWARDS A PATIENT-TAILORED APPROACH Therefore, multiple heat sources are needed to obtain large volumes of necrosis; the laser technique with multiple thin needle fibres and simultaneous approach satisfies this need. Indeed, LA obtains interesting results with thin, very simple devices that are much less sophisticated and less expensive than those used by RFA. According to the size and shape of the lesions, one to eight fibers are used. For a single illumination, laser light is employed for 4-6 min. For nodules > 3.0 cm, multiple illuminations and the pullback technique are employed. The introduction of the novel needle guide has made it possible to obtain a complete ablation of lesions up to 5 cm.





188 With single source With four sources
189 TRANSLATING ALL THE AFOREMENTIONED INTO CLINICAL PRACTICE: TOWARDS A PATIENT-TAILORED APPROACH It is possible to customize the ablative treatment according to the size and location of the lesion to be treated. Laser techniques can be used effectively in patients with very early and early HCC (BCLC 0 and A) because of their high percentage of complete response. No specific methods are used for treating lesions in high-risk (i.e., near gallbladder, main biliary duct, hepatic hilum, adjacent hollow viscera, or exophytic location) and/or hard-toreach locations (e.g., in the dome of the liver, in the caudate lobe. Additionally, this technique makes it is relatively easy to obtain a safety margin 5 mm in a higher percentage of cases (62%) than that reported by other authors with RFA.

190 Laser ablation curative ablation
191 Clinical effectiveness Influence of necrosis excess (>5 mm)* 1,0 0,9 0,8 Cumulative Proportion Surviving (Kaplan-Meier) Complete Censored Cox s test p=.035 Group 1 necrosis excess>5 mm. Group 0 necrosis excess<5 mm. Cumulative Proportion Surviving 0,7 0,6 0,5 0,4 0,3 0,2 0,1 0,0-0, Time Group 1, Group 0, An ablation zone with an ablative margin of 5 mm or greater was the most important factor for local control of hepatocellular carcinoma T Nakazawa AJR 2007
192 TRANSLATING ALL THE AFOREMENTIONED INTO CLINICAL PRACTICE: TOWARDS A PATIENT-TAILORED APPROACH As for the water-cooled laser applicators, it must be emphasized that their main advantage is their MRI compatibility, which allows pre-procedure planning and intraprocedure treatment monitoring using a variety of temperature-sensitive techniques. The Frankfurt group has provided compelling long-term survival data in patients treated with this method for the ablation of hepatic metastases and has recently published two papers on primary liver lesions in cirrhotic patients with a high percentage of complete response and low local recurrence. However, to achieve these excellent results, the authors used a large cross-sectional probe diameter (3 mm) that requires large bore cannula (9 gauge) for percutaneous treatment.
193 TRANSLATING ALL THE AFOREMENTIONED INTO CLINICAL PRACTICE: TOWARDS A PATIENT-TAILORED APPROACH In addition, the diffusion of MRI-guided LA is restricted by machine availability and by complexity of the procedure, requiring between 60 and 120 min to be completed. However, we think that although interventional MRI guidance is undoubtedly more accurate than US for monitoring ablation, its use would greatly limit the number of centers capable of performing tumor ablation, with ablation procedures being relegated to only those facilities with such specialized equipment.





194 Hot cylindrical tip



195
196 TRANSLATING ALL THE AFOREMENTIONED INTO CLINICAL PRACTICE: TOWARDS A PATIENT-TAILORED APPROACH Thus, given that US is readily available, its use has proven to be successful on a practical level in these last 20 years, compared to the potential benefits of less available technologies. These data show that touted advantages of a particular system do not have equal weight in the clinical scenario. Last but not least, we must add the costs of this option to its overall complexity.
197 TRANSLATING ALL THE AFOREMENTIONED INTO CLINICAL PRACTICE: TOWARDS A PATIENT-TAILORED APPROACH A new ablation laser system consisting of 980-nm diode laser with a power of 15-W and diffuser-tipped optical fiber inserted through a 17-gauge internally cooled catheter was recently introduced in field practice. This system achieves a large, well-circumscribed ellipsoid ablation zone up to 2.0 x 2.3 cm in a single application lasting about three minutes, and up to 3.7 x 3.2 cm with two parallel applicators placed 1.5 cm apart.
 at 15ml/min 15W 120 seconds Time Compressed 2 min = 20 sec")
198 Ex vivo ablation demo Bovine Liver Tissue Temperate: 37 C 17 Ga Cooling Catheter 400mm Diffusing Tip Fiber Cooling (room temp. saline) at 15ml/min 15W 120 seconds Time Compressed 2 min = 20 sec

199 Results Ultrasound Visualization during LITT Ablation In Vivo Time Compressed 2 min = 10 sec
200 TRANSLATING ALL THE AFOREMENTIONED INTO CLINICAL PRACTICE: TOWARDS A PATIENT-TAILORED APPROACH Due to its characteristics, this system has been applied thus far to focal malignant lesions of the prostate and the brain; research and clinical applications on hepatic focal lesions are underway (oral communication). Therefore, the limitations of the previous system, which used high-calibre devices, can be overcome by this technical solution. Further, the execution time of the entire manoeuvre can be shortened significantly by using real-time RM guidance.
201 TRANSLATING ALL THE AFOREMENTIONED INTO CLINICAL PRACTICE: TOWARDS A PATIENT-TAILORED APPROACH Therefore, with laser technical improvements such as the new small cylindrical diffuser or the novel needle guide system, it possible to employ an array of applicators to increase the ablation zone without increasing invasiveness, procedural complexity, times of ablation, or costs. In clinical practice, a trade-off must be made between these multiple factors and the operator s skill, the available technology, and the biology of the tumor.
202 Costs Using multiple small-bore needles, the price of each laser disposable kit including a needle and a fiber is about 300 (US$ 400). Therefore, the cost of a single LA session varies in relation to the number of devices used: one kit is required for nodules 1.0 cm; 2 kits for nodules ranging from 1.0 to 2.0 cm, and 4 kits for larger nodules. Treatment can be performed in outpatient surgery by an operator, a nurse, and an anaesthesiologist and requires about minutes (from targeting to final US assessment).
203 TRANSLATING ALL THE AFOREMENTIONED INTO CLINICAL PRACTICE: TOWARDS A PATIENT-TAILORED APPROACH Survival outcomes of patients with HCC <3 cm treated by percutaneous approach are competitive with those of surgery. However, a careful multidisciplinary evaluation of the age and comorbidities of the patients and of the location of these tumours is needed. In HCC >3 cm resection or combined treatment (TACE + RFA or PEI) has been suggested to improve survival, but available studies do not yet provide useful conclusions as the enrollment criteria of patients was too stringent. Studies are needed to define which population can benefit from the combined treatments.
204 TRANSLATING ALL THE AFOREMENTIONED INTO CLINICAL PRACTICE: TOWARDS A PATIENT-TAILORED APPROACH While outcomes after combined treatment (LA plus TACE) are interesting, they were obtained with a technique that is the opposite of what is commonly used in referral centers. When surgery is unfeasible, a combined/sequential approach (PEI plus RFA, TACE plus PEI, RFA, or MW) should be considered on an individual basis for multinodular nodules and for nodules > 3 cm, after multidisciplinary evaluation. A meta-analysis of RFA following TACE reported no significant difference in survival rates between RFA plus TACE and RFA for small HCC. On the contrary, this sequential treatment improved overall survival rate in patients with intermediate and large HCC. Therefore, the main indication of combined therapies is for lesions >3 cm and <8 cm.
205 TRANSLATING ALL THE AFOREMENTIONED INTO CLINICAL PRACTICE: TOWARDS A PATIENT-TAILORED APPROACH LA before TACE, instead, reduces the tumor burden and brings the lesion back within the range of TACE effectiveness. In other words, LA results in a minimal amount of tumor tissue, which can be destroyed with selective TACE using a lesser amount of embolizing material. Because it is possible to destroy lesions up to 5-6 cm with laser technique we think that this combined method might be effective in treating lesions larger than 6 cm both in cirrhotic patients and in non-cirrhotic patients, thereby avoiding surgery, as currently suggested by some authors.




206 Combined treatment: LA followed by TACE
207 TRANSLATING ALL THE AFOREMENTIONED INTO CLINICAL PRACTICE: TOWARDS A PATIENT-TAILORED APPROACH The safety of the procedure was investigated in a multicenter study sufficiently representative both of the type and of the number of possible complications when using either multiple thin needles or large water-cooled devices. The data reported above compare favourably with the more widely used RFA and MWA technique. The mortality rates of RFA range from 0 to 1.5% of cases and major complications from 1.5% to 5.8% of cases. The mortality and major complications rates of MWA have been reported as 0% to 5.1% and 2.6% to 5.1%, respectively.
208 CLINICAL CASES
209 Nodule adjacent to gallbladder
210 1

211

212

213
214 2
215
216
217

218
219 3
220

221
222
223
224 Nodule near heart
225 1

226
227
228
229 2
230
231
232
233
234 Nodule I segment

235
236

237
238 Nodule between porta and cava vein
239
240
241
242
243 Nodule near diaphragm
244
245
246
247 Nodule 5 cm
248

249
250
251 Nodule 7.5 cm
252
253
254
255
256
257
258
259 Nodule behind TIPS
260

261 tips Cava vein
262
263
264

265
266
267 Nodule adjacent cava vein

268

269
270
271
272
273 Portal thrombosis
274 1
275
276
277
278
279 2
280
281
282 Retreatment of a large HCC
283 file:///.file/id=
284
285
286
287
288 Conclusions (1) - LA is not inferior to RFA in the treatment of small HCC. - LA is safe and cheaper than RFA/MWA. - The use of thin needles allows the treatment of HCC in high-risk sites and in hard-to-reach locations.
289 Conclusions (2) - Thanks to the novel guide system which facilitates the parallel insertion of multiple needles, LA is more effective in achieving with safety large volumes of necrosis. - Using LA, it is possible to treat effectively and safely multiple lesions of different sizes in different sites in the same session.
290 Conclusions (3) - More in general, we think that the reference centres that treat more than 50 patients/year should be equipped with all the available techniques so as to be able to use the best and the most suitable for each type of lesion in each patient.
291 Optimizing tumor ablation OPTIMAL ABLATION BIOLOGY
292 Take-home message - Laser is an ideal energy source to perform ablation of liver tumors: very precise, highly efficient at low powers, minimally invasive - Laser ablation is not inferior to the most widely used radiofrequency ablation - It is a very flexible techniques that can be used for the treatment of nodules with different shape - Laser ablation has the advantage of being less traumatic than other techniques - Complication rate is not higher of that observed after other ablation technique - It can be used to treat cancers in every location, in particular hard-to-treat tumors - It is cheaper and more simple than other ablative methods

293 Thank you
294 7-8 July, Naples, Italy First Percutaneous Laser Ablation Network (PLAN) educational initiative on laser ablation for liver tumors IMPROVING THE PATIENT S LIFE THROUGH MEDICAL EDUCATION
Percutaneous ablation: indications, techniques and results
 Percutaneous ablation: indications, techniques and results Giovan Giuseppe Di Costanzo Dipartimento dei Trapianti UOSC Epatologia AORN A Cardarelli - Napoli Treatment algorithm EASL, EORTC guidelines HCC
Percutaneous ablation: indications, techniques and results Giovan Giuseppe Di Costanzo Dipartimento dei Trapianti UOSC Epatologia AORN A Cardarelli - Napoli Treatment algorithm EASL, EORTC guidelines HCC
Case Studies of Laser Ablation for Liver Tumors
 Case Studies of Laser Ablation for Liver Tumors Dr Giovan Giuseppe Di Costanzo, Head Physician, Department of Liver Pathophysiology - Cardarelli Hospital, Naples Case 1: HCC near vascular structures A
Case Studies of Laser Ablation for Liver Tumors Dr Giovan Giuseppe Di Costanzo, Head Physician, Department of Liver Pathophysiology - Cardarelli Hospital, Naples Case 1: HCC near vascular structures A
Hepatocellular Carcinoma: Diagnosis and Management
 Hepatocellular Carcinoma: Diagnosis and Management Nizar A. Mukhtar, MD Co-director, SMC Liver Tumor Board April 30, 2016 1 Objectives Review screening/surveillance guidelines Discuss diagnostic algorithm
Hepatocellular Carcinoma: Diagnosis and Management Nizar A. Mukhtar, MD Co-director, SMC Liver Tumor Board April 30, 2016 1 Objectives Review screening/surveillance guidelines Discuss diagnostic algorithm
Celsion Symposium New Paradigms in HCC Staging: HKLC vs. BCLC Staging
 Celsion Symposium New Paradigms in HCC Staging: HKLC vs. BCLC Staging Ronnie T.P. Poon, MBBS, MS, PhD Chair Professor of Hepatobiliary and Pancreatic Surgery Chief of Hepatobiliary and Pancreatic Surgery
Celsion Symposium New Paradigms in HCC Staging: HKLC vs. BCLC Staging Ronnie T.P. Poon, MBBS, MS, PhD Chair Professor of Hepatobiliary and Pancreatic Surgery Chief of Hepatobiliary and Pancreatic Surgery
Advances in percutaneous ablation for hepatocellular carcinoma
 Advances in percutaneous ablation for hepatocellular carcinoma P. Nahon1,2,3 1 Hepatology, Jean Verdier Hospital, APHP, Bondy, France 2 Paris 13 university, Sorbonne Paris Cité, UFRSMBH, Bobigny, France
Advances in percutaneous ablation for hepatocellular carcinoma P. Nahon1,2,3 1 Hepatology, Jean Verdier Hospital, APHP, Bondy, France 2 Paris 13 university, Sorbonne Paris Cité, UFRSMBH, Bobigny, France
Hepatocellular Carcinoma: A major global health problem. David L. Wood, MD Interventional Radiology Banner Good Samaritan Medical Center
 Hepatocellular Carcinoma: A major global health problem David L. Wood, MD Interventional Radiology Banner Good Samaritan Medical Center Hepatocellular Carcinoma WORLDWIDE The #2 Cancer Killer Overall cancer
Hepatocellular Carcinoma: A major global health problem David L. Wood, MD Interventional Radiology Banner Good Samaritan Medical Center Hepatocellular Carcinoma WORLDWIDE The #2 Cancer Killer Overall cancer
Interventional Radiology in Liver Cancer. Nakarin Inmutto MD
 Interventional Radiology in Liver Cancer Nakarin Inmutto MD Liver cancer Primary liver cancer Hepatocellular carcinoma Cholangiocarcinoma Metastasis Interventional Radiologist Diagnosis Imaging US / CT
Interventional Radiology in Liver Cancer Nakarin Inmutto MD Liver cancer Primary liver cancer Hepatocellular carcinoma Cholangiocarcinoma Metastasis Interventional Radiologist Diagnosis Imaging US / CT
Liver Directed Therapy for Hepatocellular Carcinoma
 Liver Directed Therapy for Hepatocellular Carcinoma Anil K Pillai MD, FRCR, Associate Professor, Department of Radiology UT Houston Health Science Center, Houston, TX, United States. Hepatocellular cancer
Liver Directed Therapy for Hepatocellular Carcinoma Anil K Pillai MD, FRCR, Associate Professor, Department of Radiology UT Houston Health Science Center, Houston, TX, United States. Hepatocellular cancer
TREATMENT FOR HCC AND CHOLANGIOCARCINOMA. Shawn Pelletier, MD
 TREATMENT FOR HCC AND CHOLANGIOCARCINOMA Shawn Pelletier, MD Treatment for HCC Treatment strategies Curative first line therapy Thermal ablation vs Resection vs Transplant Other first line therapies TACE
TREATMENT FOR HCC AND CHOLANGIOCARCINOMA Shawn Pelletier, MD Treatment for HCC Treatment strategies Curative first line therapy Thermal ablation vs Resection vs Transplant Other first line therapies TACE
Liver resection for HCC
 8 th LIVER INTEREST GROUP Annual Meeting Cape Town 2017 Liver resection for HCC Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre The liver is almost unique in that treatment of the
8 th LIVER INTEREST GROUP Annual Meeting Cape Town 2017 Liver resection for HCC Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre The liver is almost unique in that treatment of the
Disclosure. Speaker name: Prof. Maciej Pech I have the following potential conflicts of interest to report:
 Disclosure Speaker name: Prof. Maciej Pech I have the following potential conflicts of interest to report: Consulting Employment in industry Stockholder of a healthcare company Owner of a healthcare company
Disclosure Speaker name: Prof. Maciej Pech I have the following potential conflicts of interest to report: Consulting Employment in industry Stockholder of a healthcare company Owner of a healthcare company
Hepatocellular Carcinoma. Markus Heim Basel
 Hepatocellular Carcinoma Markus Heim Basel Outline 1. Epidemiology 2. Surveillance 3. (Diagnosis) 4. Staging 5. Treatment Epidemiology of HCC Worldwide, liver cancer is the sixth most common cancer (749
Hepatocellular Carcinoma Markus Heim Basel Outline 1. Epidemiology 2. Surveillance 3. (Diagnosis) 4. Staging 5. Treatment Epidemiology of HCC Worldwide, liver cancer is the sixth most common cancer (749
Locoregional Therapy for Hepatoma
 Locoregional Therapy for Hepatoma Robert D. Crane, MD Interventional Radiology Virginia Mason How do we know a liver mass is HCC? HCC : Bx Of pts getting liver transplant only ~ 5% had Bx to establish
Locoregional Therapy for Hepatoma Robert D. Crane, MD Interventional Radiology Virginia Mason How do we know a liver mass is HCC? HCC : Bx Of pts getting liver transplant only ~ 5% had Bx to establish
Surveillance for Hepatocellular Carcinoma
 Surveillance for Hepatocellular Carcinoma Marion G. Peters, MD John V. Carbone, MD, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California San Francisco Recorded on April
Surveillance for Hepatocellular Carcinoma Marion G. Peters, MD John V. Carbone, MD, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California San Francisco Recorded on April
9th Paris Hepatitis Conference
 9th Paris Hepatitis Conference Paris, 12 January 2016 Treatment of hepatocellular carcinoma: beyond international guidelines Massimo Colombo Chairman Department of Liver, Kidney, Lung and Bone Marrow Units
9th Paris Hepatitis Conference Paris, 12 January 2016 Treatment of hepatocellular carcinoma: beyond international guidelines Massimo Colombo Chairman Department of Liver, Kidney, Lung and Bone Marrow Units
Staging & Current treatment of HCC
 Staging & Current treatment of HCC Dr.: Adel El Badrawy Badrawy; ; M.D. Staging & Current ttt of HCC Early stage HCC is typically silent. HCC is often advanced at first manifestation. The selective ttt
Staging & Current treatment of HCC Dr.: Adel El Badrawy Badrawy; ; M.D. Staging & Current ttt of HCC Early stage HCC is typically silent. HCC is often advanced at first manifestation. The selective ttt
General summary GENERAL SUMMARY
 General summary GENERAL SUMMARY In Chapter 2.1 the long-term results and prognostic factors of radiofrequency ablation (RFA) for unresectable colorectal liver metastases (CRLM) in a single center with
General summary GENERAL SUMMARY In Chapter 2.1 the long-term results and prognostic factors of radiofrequency ablation (RFA) for unresectable colorectal liver metastases (CRLM) in a single center with
Paul Martin MD FACG. University of Miami
 Paul Martin MD FACG University of Miami 1 Liver cirrhosis of any cause Chronic C o c hepatitis epat t s B Risk increases with Male gender Age Diabetes Smoking ~5% increase in HCV-related HCC between 1991-28
Paul Martin MD FACG University of Miami 1 Liver cirrhosis of any cause Chronic C o c hepatitis epat t s B Risk increases with Male gender Age Diabetes Smoking ~5% increase in HCV-related HCC between 1991-28
Advances in percutaneous ablation and systemic therapies for hepatocellular carcinoma
 Advances in percutaneous ablation and systemic therapies for hepatocellular carcinoma Paris Hepatology Congress 2019 Pierre Nahon Service d Hépatologie Hôpital Jean Verdier Bondy Université Paris 13 INSERM
Advances in percutaneous ablation and systemic therapies for hepatocellular carcinoma Paris Hepatology Congress 2019 Pierre Nahon Service d Hépatologie Hôpital Jean Verdier Bondy Université Paris 13 INSERM
Locoregional Treatments for HCC Applications in Transplant Candidates. Locoregional Treatments for HCC Applications in Transplant Candidates
 Locoregional Treatments for HCC Applications in Transplant Candidates Matthew Casey, MD March 31, 2016 Locoregional Treatments for HCC Applications in Transplant Candidates *No disclosures *Off-label uses
Locoregional Treatments for HCC Applications in Transplant Candidates Matthew Casey, MD March 31, 2016 Locoregional Treatments for HCC Applications in Transplant Candidates *No disclosures *Off-label uses
EASL-EORTC Guidelines
 Pamplona, junio de 2008 CLINICAL PRACTICE GUIDELINES: PARADIGMS IN MANAGEMENT OF HCC EASL-EORTC Guidelines Bruno Sangro Clínica Universidad de Navarra. CIBERehd. Pamplona, Spain Levels of Evidence according
Pamplona, junio de 2008 CLINICAL PRACTICE GUIDELINES: PARADIGMS IN MANAGEMENT OF HCC EASL-EORTC Guidelines Bruno Sangro Clínica Universidad de Navarra. CIBERehd. Pamplona, Spain Levels of Evidence according
Liver transplantation: Hepatocellular carcinoma
 Liver transplantation: Hepatocellular carcinoma Alejandro Forner BCLC Group. Liver Unit. Hospital Clínic. University of Barcelona 18 de marzo 2015 3r Curso Práctico de Transplante de Órganos Sólidos Barcelona
Liver transplantation: Hepatocellular carcinoma Alejandro Forner BCLC Group. Liver Unit. Hospital Clínic. University of Barcelona 18 de marzo 2015 3r Curso Práctico de Transplante de Órganos Sólidos Barcelona
Hepatocellular Carcinoma (HCC): Who Should be Screened and How Do We Treat? Tom Vorpahl MSN, RN, ACNP-BC
: Who Should be Screened and How Do We Treat? Tom Vorpahl MSN, RN, ACNP-BC") Hepatocellular Carcinoma (HCC): Who Should be Screened and How Do We Treat? Tom Vorpahl MSN, RN, ACNP-BC Objectives Identify patient risk factors for hepatocellular carcinoma (HCC) Describe strategies
Hepatocellular Carcinoma (HCC): Who Should be Screened and How Do We Treat? Tom Vorpahl MSN, RN, ACNP-BC Objectives Identify patient risk factors for hepatocellular carcinoma (HCC) Describe strategies
Management of HepatoCellular Carcinoma
 9th Symposium GIC St Louis - 2010 Management of HepatoCellular Carcinoma Overview Pierre A. Clavien, MD, PhD Department of Surgery University Hospital Zurich Zurich, Switzerland Hepatocellular carcinoma
9th Symposium GIC St Louis - 2010 Management of HepatoCellular Carcinoma Overview Pierre A. Clavien, MD, PhD Department of Surgery University Hospital Zurich Zurich, Switzerland Hepatocellular carcinoma
ONCOLOGIC PERCUTANEOUS INTERVENTION: 2015 UPDATE HANH VU NGHIEM, MD OAKLAND UNIVERSITY WILLIAM BEAUMONT SCHOOL OF MEDICINE
 ONCOLOGIC PERCUTANEOUS INTERVENTION: 2015 UPDATE HANH VU NGHIEM, MD OAKLAND UNIVERSITY WILLIAM BEAUMONT SCHOOL OF MEDICINE ONCOLOGIC PERCUTANEOUS IMAGE GUIDED TUMOR ABLATION Evolving, growing and increasingly
ONCOLOGIC PERCUTANEOUS INTERVENTION: 2015 UPDATE HANH VU NGHIEM, MD OAKLAND UNIVERSITY WILLIAM BEAUMONT SCHOOL OF MEDICINE ONCOLOGIC PERCUTANEOUS IMAGE GUIDED TUMOR ABLATION Evolving, growing and increasingly
Radiofrequency Ablation of Liver Tumors
 Radiofrequency Ablation of Liver Tumors Michael M. Awad, Michael A. Choti Indications and Contraindications Indications Unresectable malignant tumors of the liver (e.g., hepatocellular carcinoma, colorectal
Radiofrequency Ablation of Liver Tumors Michael M. Awad, Michael A. Choti Indications and Contraindications Indications Unresectable malignant tumors of the liver (e.g., hepatocellular carcinoma, colorectal
WHAT IS THE BEST APPROACH FOR TRANS-ARTERIAL THERAPY IN HCC?
 WHAT IS THE BEST APPROACH FOR TRANS-ARTERIAL THERAPY IN HCC? Dr. Alexander Kim Chief, Vascular and Interventional Radiology, Medstar Georgetown University Hospital, USA DISCLAIMER Please note: The views
WHAT IS THE BEST APPROACH FOR TRANS-ARTERIAL THERAPY IN HCC? Dr. Alexander Kim Chief, Vascular and Interventional Radiology, Medstar Georgetown University Hospital, USA DISCLAIMER Please note: The views
RFA-based Combination Therapy 肝病研究中心, 肝臟科 林口長庚醫院, 長庚醫學大學 (CHANG GUNG MEMORIAL HOSPITAL, LINKUO) 林成俊 (CHEN-CHUN LIN)
 林成俊 (CHEN-CHUN LIN)") RFA-based Combination Therapy 肝病研究中心, 肝臟科 林口長庚醫院, 長庚醫學大學 (CHANG GUNG MEMORIAL HOSPITAL, LINKUO) 林成俊 (CHEN-CHUN LIN) CONTENTS Introduction RFA-based Combination Therapy Ethanol injection (PEI) Saline perfusion
RFA-based Combination Therapy 肝病研究中心, 肝臟科 林口長庚醫院, 長庚醫學大學 (CHANG GUNG MEMORIAL HOSPITAL, LINKUO) 林成俊 (CHEN-CHUN LIN) CONTENTS Introduction RFA-based Combination Therapy Ethanol injection (PEI) Saline perfusion
Thermal Ablation of Liver Tumours: How the Scenario Has Changed in the Last Decade
 Thermal Ablation of Liver Tumours: How the Scenario Has Changed in the Last Decade Authors: Paola Tombesi, Francesca Di Vece, Lara Bianchi, *Sergio Sartori Section of Interventional Ultrasound, St. Anna
Thermal Ablation of Liver Tumours: How the Scenario Has Changed in the Last Decade Authors: Paola Tombesi, Francesca Di Vece, Lara Bianchi, *Sergio Sartori Section of Interventional Ultrasound, St. Anna
Hepatocellular carcinoma: from guidelines to individualized treatment
 AISF 2012 Rome, 22-24 February 2012 Hepatocellular carcinoma: from guidelines to individualized treatment A.D. 1088 Luigi Bolondi Professor of Medicine, Chairman Department of Digestive Diseases and Internal
AISF 2012 Rome, 22-24 February 2012 Hepatocellular carcinoma: from guidelines to individualized treatment A.D. 1088 Luigi Bolondi Professor of Medicine, Chairman Department of Digestive Diseases and Internal
New Energy Sources for Local Ablation Therapy. Jeong Kyong Lee, MD Ewha Womans University
 New Energy Sources for Local Ablation Therapy Jeong Kyong Lee, MD Ewha Womans University New Energy Sources for Local Ablation Therapy Microwave Ablation Irreversible Electroporation Cryoablation Microwave
New Energy Sources for Local Ablation Therapy Jeong Kyong Lee, MD Ewha Womans University New Energy Sources for Local Ablation Therapy Microwave Ablation Irreversible Electroporation Cryoablation Microwave
Unmet needs in intermediate HCC. Korea University Guro Hospital Ji Hoon Kim
 Unmet needs in intermediate HCC Korea University Guro Hospital Ji Hoon Kim BCLC HCC Stage 0 PST 0, Child Pugh A Stage A C PST 0 2, Child Pugh A B Stage D PST > 2, Child Pugh C Very early stage (0) 1 HCC
Unmet needs in intermediate HCC Korea University Guro Hospital Ji Hoon Kim BCLC HCC Stage 0 PST 0, Child Pugh A Stage A C PST 0 2, Child Pugh A B Stage D PST > 2, Child Pugh C Very early stage (0) 1 HCC
Liver Tumors. Patient Education. Treatment options 8 4A. About the Liver. Surgical Specialties
 Patient Education Treatment options This handout describes different kinds of tumors that form in the liver and how they are treated. About the Liver Your liver is the largest organ in your abdomen. It
Patient Education Treatment options This handout describes different kinds of tumors that form in the liver and how they are treated. About the Liver Your liver is the largest organ in your abdomen. It
Percutaneous Ultrasound-guided Radiofrequency Ablation of Colorectal Liver Metastases
 Chin J Radiol 2005; 30: 153-158 153 Percutaneous Ultrasound-guided Radiofrequency Ablation of Colorectal Liver Metastases YI-YOU CHIOU YI-HONG CHOU JEN-HUEY CHIANG HSIN-KAI WANG CHENG-YEN CHANG Department
Chin J Radiol 2005; 30: 153-158 153 Percutaneous Ultrasound-guided Radiofrequency Ablation of Colorectal Liver Metastases YI-YOU CHIOU YI-HONG CHOU JEN-HUEY CHIANG HSIN-KAI WANG CHENG-YEN CHANG Department
Surveillance for HCC Who, how Diagnosis of HCC Surveillance for HCC in Practice
 Surveillance for Hepatocellular Carcinoma Hashem B. El-Serag, MD, MPH Dan L. Duncan Professor of Medicine Chief, Gastroenterology and Hepatology Houston VA & Baylor College of Medicine Houston, TX Outline
Surveillance for Hepatocellular Carcinoma Hashem B. El-Serag, MD, MPH Dan L. Duncan Professor of Medicine Chief, Gastroenterology and Hepatology Houston VA & Baylor College of Medicine Houston, TX Outline
Ruolo della interventistica per le secondarietà epatiche e di altre sedi
 Ruolo della interventistica per le secondarietà epatiche e di altre sedi Giancarlo Bizzarri Dipartimento di Diagnostica per Immagini e Radiologia Interventistica Ospedale Regina Apostolorum, Albano Laziale
Ruolo della interventistica per le secondarietà epatiche e di altre sedi Giancarlo Bizzarri Dipartimento di Diagnostica per Immagini e Radiologia Interventistica Ospedale Regina Apostolorum, Albano Laziale
Transarterial Chemoembolisation (TACE) with Drug-Eluting Beads
 with Drug-Eluting Beads") Transarterial Chemoembolisation (TACE) with Drug-Eluting Beads A minimally invasive treatment for liver cancer Provided as an educational service by Biocompatibles UK Ltd, a BTG International group company
Transarterial Chemoembolisation (TACE) with Drug-Eluting Beads A minimally invasive treatment for liver cancer Provided as an educational service by Biocompatibles UK Ltd, a BTG International group company
Radiofrequency Ablation versus Microwave Ablation in HCC and Liver Metastases
 Radiofrequency Ablation versus Microwave Ablation in HCC and Liver Metastases Thomas J. Vogl, B. Panahi, N. Nour-Eldin I D I R: Institute of Diagnostic and Interventional Radiology Goethe University Frankfurt,
Radiofrequency Ablation versus Microwave Ablation in HCC and Liver Metastases Thomas J. Vogl, B. Panahi, N. Nour-Eldin I D I R: Institute of Diagnostic and Interventional Radiology Goethe University Frankfurt,
Advances of Thermal Ablation. Dr Chandan J Das. MD,DNB, MNAMS Associate Professor of Radiology, All India Institute of Medical Sciences, New-Delhi.
 Advances of Thermal Ablation Dr Chandan J Das. MD,DNB, MNAMS Associate Professor of Radiology, All India Institute of Medical Sciences, New-Delhi. Nothing to disclose Disclaimer Goals of Minimally Invasive
Advances of Thermal Ablation Dr Chandan J Das. MD,DNB, MNAMS Associate Professor of Radiology, All India Institute of Medical Sciences, New-Delhi. Nothing to disclose Disclaimer Goals of Minimally Invasive
Tumor incidence varies significantly, depending on geographical location.
 Hepatocellular carcinoma is the 5 th most common malignancy worldwide with male-to-female ratio 5:1 in Asia 2:1 in the United States Tumor incidence varies significantly, depending on geographical location.
Hepatocellular carcinoma is the 5 th most common malignancy worldwide with male-to-female ratio 5:1 in Asia 2:1 in the United States Tumor incidence varies significantly, depending on geographical location.
The Egyptian Journal of Hospital Medicine (October 2017) Vol.69(1), Page
 Vol.69(1), Page") The Egyptian Journal of Hospital Medicine (October 2017) Vol.69(1), Page 1674-1679 Radioembolization in Treatment of Hepatocellular Carcinoma with Portal Vein Invasion Elsahhar Ahmed Hetta, Osama Mohamed
The Egyptian Journal of Hospital Medicine (October 2017) Vol.69(1), Page 1674-1679 Radioembolization in Treatment of Hepatocellular Carcinoma with Portal Vein Invasion Elsahhar Ahmed Hetta, Osama Mohamed
Hepatobiliary Malignancies Retrospective Study at Truman Medical Center
 Hepatobiliary Malignancies 206-207 Retrospective Study at Truman Medical Center Brandon Weckbaugh MD, Prarthana Patel & Sheshadri Madhusudhana MD Introduction: Hepatobiliary malignancies are cancers which
Hepatobiliary Malignancies 206-207 Retrospective Study at Truman Medical Center Brandon Weckbaugh MD, Prarthana Patel & Sheshadri Madhusudhana MD Introduction: Hepatobiliary malignancies are cancers which
UPDATE TO THE MANAGEMENT OF PATIENTS WITH HCC HCA
 UPDATE TO THE MANAGEMENT OF PATIENTS WITH HCC HUSSEIN K. MOHAMED MD, FACS. Transplant and Hepato-biliary Surgery Largo Medical Center HCA DISCLOSURE I have no financial relationship(s) relevant to the
UPDATE TO THE MANAGEMENT OF PATIENTS WITH HCC HUSSEIN K. MOHAMED MD, FACS. Transplant and Hepato-biliary Surgery Largo Medical Center HCA DISCLOSURE I have no financial relationship(s) relevant to the
In- and exclusion criteria
 In- and exclusion criteria Kerstin Schütte Department of Gastroenterology, Hepatology and Infectious Diseases University of Magdeburg Overview: Study population Inclusion criteria I - General criteria
In- and exclusion criteria Kerstin Schütte Department of Gastroenterology, Hepatology and Infectious Diseases University of Magdeburg Overview: Study population Inclusion criteria I - General criteria
Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary)
") Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary) Staff Reviewers: Dr. Yoo Joung Ko (Medical Oncologist, Sunnybrook Odette Cancer
Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary) Staff Reviewers: Dr. Yoo Joung Ko (Medical Oncologist, Sunnybrook Odette Cancer
HEPATIC METASTASES. We can state 3 types of metastases depending on their treatment options:
 HEPATIC METASTASES 1. Definition Metastasis means the spread of cancer. Cancerous cells can separate from the primary tumor and enter the bloodstream or the lymphatic system (the one that produces, stores,
HEPATIC METASTASES 1. Definition Metastasis means the spread of cancer. Cancerous cells can separate from the primary tumor and enter the bloodstream or the lymphatic system (the one that produces, stores,
IS THERE A DIFFERENCE IN LIVER CANCER RATES IN PATIENTS WHO RECEIVE TREATMENT FOR HEPATITIS?
 IS THERE A DIFFERENCE IN LIVER CANCER RATES IN PATIENTS WHO RECEIVE TREATMENT FOR HEPATITIS? Dr. Sammy Saab David Geffen School of Medicine, Los Angeles, USA April 2018 DISCLAIMER Please note: The views
IS THERE A DIFFERENCE IN LIVER CANCER RATES IN PATIENTS WHO RECEIVE TREATMENT FOR HEPATITIS? Dr. Sammy Saab David Geffen School of Medicine, Los Angeles, USA April 2018 DISCLAIMER Please note: The views
PEER-REVIEW REPORT CLASSIFICATION LANGUAGE EVALUATION SCIENTIFIC MISCONDUCT CONCLUSION. [ Y] Accept [ ] Grade B: Very good
![PEER-REVIEW REPORT CLASSIFICATION LANGUAGE EVALUATION SCIENTIFIC MISCONDUCT CONCLUSION. [ Y] Accept [ ] Grade B: Very good](/thumbs/96/127805416.jpg "PEER-REVIEW REPORT CLASSIFICATION LANGUAGE EVALUATION SCIENTIFIC MISCONDUCT CONCLUSION. [ Y] Accept [ ] Grade B: Very good") Reviewer s code: 03656588 Reviewer s country: China Date reviewed: 2017-06-08 [ ] Grade A: Excellent [ Y] Accept [ ] Grade B: Very good [ ] High priority for [ Y] Grade C: Good language [ ] Major revision
Reviewer s code: 03656588 Reviewer s country: China Date reviewed: 2017-06-08 [ ] Grade A: Excellent [ Y] Accept [ ] Grade B: Very good [ ] High priority for [ Y] Grade C: Good language [ ] Major revision
HCC RADIOLOGIC DIAGNOSIS
 UCSF Transplant 2010 THE BEFORE AND AFTER HEPATOCELLULAR CARCINOMA MANAGEMENT Francis Yao, M.D. Professor of Clinical Medicine and Surgery Medical Director, Liver Transplantation University of California,
UCSF Transplant 2010 THE BEFORE AND AFTER HEPATOCELLULAR CARCINOMA MANAGEMENT Francis Yao, M.D. Professor of Clinical Medicine and Surgery Medical Director, Liver Transplantation University of California,
MULTI-DISCIPLINARY MANAGEMENT OF INTERMEDIATE STAGE HCC
 Dr Apoorva Gogna MBBS FRCR FAMS Consultant Interventional Radiology Center Department of Diagnostic Radiology SingaporeGeneral Hospital MULTI-DISCIPLINARY MANAGEMENT OF INTERMEDIATE STAGE HCC CASE HISTORY
Dr Apoorva Gogna MBBS FRCR FAMS Consultant Interventional Radiology Center Department of Diagnostic Radiology SingaporeGeneral Hospital MULTI-DISCIPLINARY MANAGEMENT OF INTERMEDIATE STAGE HCC CASE HISTORY
RADIATION SEGMENTECTOMY. Robert J Lewandowski, MD
 RADIATION SEGMENTECTOMY Robert J Lewandowski, MD Robert Lewandowski, M.D. Consultant/Advisory Board: Cook Medical, LLC, Arsenal, BTG International, Boston Scientific Corp., ABK Reference Unlabeled/Unapproved
RADIATION SEGMENTECTOMY Robert J Lewandowski, MD Robert Lewandowski, M.D. Consultant/Advisory Board: Cook Medical, LLC, Arsenal, BTG International, Boston Scientific Corp., ABK Reference Unlabeled/Unapproved
Surgical management of HCC. Evangelos Prassas Hepatobiliary and Pancreatic Surgery / Liver Transplantation Kings College Hospital / London
 Surgical management of HCC Evangelos Prassas Hepatobiliary and Pancreatic Surgery / Liver Transplantation Kings College Hospital / London Global distribution of HCC and staging systems WEST 1. Italy (Milan,
Surgical management of HCC Evangelos Prassas Hepatobiliary and Pancreatic Surgery / Liver Transplantation Kings College Hospital / London Global distribution of HCC and staging systems WEST 1. Italy (Milan,
RFA of Tumors of the Lung: How and Why. Radiofrequency Ablation. Radiofrequency Ablation. RFA of pulmonary metastases. Radiofrequency Ablation of Lung
 RFA of Tumors of the Lung: How and Why Radiofrequency Ablation of Lung Ernest Scalzetti MD SUNY Upstate Medical University Syracuse NY FDA WARNING: Off-label use of a medical device Radiofrequency Ablation
RFA of Tumors of the Lung: How and Why Radiofrequency Ablation of Lung Ernest Scalzetti MD SUNY Upstate Medical University Syracuse NY FDA WARNING: Off-label use of a medical device Radiofrequency Ablation
Paolo Giorgio Arcidiacono MD FASGE
 LOCAL ABLATIVE TREATMENT OF PANCREATIC SOLID LESIONS. WHERE ARE WE NOW? Paolo Giorgio Arcidiacono MD FASGE Pancreato-Biliary Endoscopy & Endosonography Division Pancreas Translational & Clinical Research
LOCAL ABLATIVE TREATMENT OF PANCREATIC SOLID LESIONS. WHERE ARE WE NOW? Paolo Giorgio Arcidiacono MD FASGE Pancreato-Biliary Endoscopy & Endosonography Division Pancreas Translational & Clinical Research
CHIRURGIA EPATOBILIARE IN WEEK SURGERY?
 U.O.C. di Chirurgia Epatobiliare e dei Trapianti Epatici Università degli Studi di Padova CHIRURGIA EPATOBILIARE IN WEEK SURGERY? Umberto Cillo, MD, PhD, FEBS cillo@unipd.it Quali sono gli ingredienti
U.O.C. di Chirurgia Epatobiliare e dei Trapianti Epatici Università degli Studi di Padova CHIRURGIA EPATOBILIARE IN WEEK SURGERY? Umberto Cillo, MD, PhD, FEBS cillo@unipd.it Quali sono gli ingredienti
Selection Criteria and Insertion of SIRT into HCC Treatment Guidelines
 Selection Criteria and Insertion of SIRT into HCC Treatment Guidelines 2 nd Asia Pacific Symposium on Liver- Directed Y-90 Microspheres Therapy 1st November 2014, Singapore Pierce Chow FRCSE PhD SIRT in
Selection Criteria and Insertion of SIRT into HCC Treatment Guidelines 2 nd Asia Pacific Symposium on Liver- Directed Y-90 Microspheres Therapy 1st November 2014, Singapore Pierce Chow FRCSE PhD SIRT in
RF Ablation: indication, technique and imaging follow-up
 RF Ablation: indication, technique and imaging follow-up Trongtum Tongdee, M.D. Radiology Department, Faculty of Medicine, Siriraj Hospital, Mahidol University, Bangkok, Thailand Objective Basic knowledge
RF Ablation: indication, technique and imaging follow-up Trongtum Tongdee, M.D. Radiology Department, Faculty of Medicine, Siriraj Hospital, Mahidol University, Bangkok, Thailand Objective Basic knowledge
Corporate Medical Policy
 Corporate Medical Policy Cryosurgical Ablation of Primary or Metastatic Liver Tumors File Name: Origination: Last CAP Review: Next CAP Review: Last Review: cryosurgical_ablation_of_primary_or_metastatic_liver_tumors
Corporate Medical Policy Cryosurgical Ablation of Primary or Metastatic Liver Tumors File Name: Origination: Last CAP Review: Next CAP Review: Last Review: cryosurgical_ablation_of_primary_or_metastatic_liver_tumors
Study Objective and Design
 Randomized, Open Label, Multicenter, Phase II Trial of Transcatheter Arterial Chemoembolization (TACE) Therapy in Combination with Sorafenib as Compared With TACE Alone in Patients with Hepatocellular
Randomized, Open Label, Multicenter, Phase II Trial of Transcatheter Arterial Chemoembolization (TACE) Therapy in Combination with Sorafenib as Compared With TACE Alone in Patients with Hepatocellular
Damian Dupuy, MD. Image Guided Intervention (IGI) Studies 10:25 11:05 AM
 Studies 10:25 11:05 AM") Damian Dupuy, MD Image Guided Intervention (IGI) Studies 10:25 11:05 AM Image Guided Intervention (IGI) Studies Damian E. Dupuy, M.D., FACR Professor of Diagnostic Imaging The Warren Alpert Medical School
Damian Dupuy, MD Image Guided Intervention (IGI) Studies 10:25 11:05 AM Image Guided Intervention (IGI) Studies Damian E. Dupuy, M.D., FACR Professor of Diagnostic Imaging The Warren Alpert Medical School
6/16/2016. Treating Hepatocellular Carcinoma: Deciphering the Clinical Data. Liver Regeneration. Liver Regeneration
 Treating : Deciphering the Clinical Data Derek DuBay, MD Associate Professor of Surgery Director of Liver Transplant Liver Transplant and Hepatobiliary Surgery UAB Department of Surgery Liver Regeneration
Treating : Deciphering the Clinical Data Derek DuBay, MD Associate Professor of Surgery Director of Liver Transplant Liver Transplant and Hepatobiliary Surgery UAB Department of Surgery Liver Regeneration
100% pure beta emitter Decays to zirconium-90 Physical half-life of 64.1 hours (2.67 days) 94% of radiation delivered within 11 days
 94% of radiation delivered within 11 days") 100% pure beta emitter Decays to zirconium-90 Physical half-life of 64.1 hours (2.67 days) 94% of radiation delivered within 11 days TheraSphere [US package insert]. Surrey, UK: Biocompatibles UK Ltd,
100% pure beta emitter Decays to zirconium-90 Physical half-life of 64.1 hours (2.67 days) 94% of radiation delivered within 11 days TheraSphere [US package insert]. Surrey, UK: Biocompatibles UK Ltd,
Proton Beam Therapy for Hepatocellular Carcinoma. Li Jiamin, MD Wanjie Proton Therapy Center
 Proton Beam Therapy for Hepatocellular Carcinoma Li Jiamin, MD Wanjie Proton Therapy Center 1 1 Hepatocelluar carcinoma (HCC) is one of the most common cancers worldwide It is the eighth most common neoplasm
Proton Beam Therapy for Hepatocellular Carcinoma Li Jiamin, MD Wanjie Proton Therapy Center 1 1 Hepatocelluar carcinoma (HCC) is one of the most common cancers worldwide It is the eighth most common neoplasm
AMSER Case of the Month: June 2018
 AMSER Case of the Month: June 2018 64 year old male undergoing evaluation for liver transplant By Timothy Morgan, MS IV Lake Erie College of Osteopathic Medicine Jonathan Potts, MD Interventional Radiology,
AMSER Case of the Month: June 2018 64 year old male undergoing evaluation for liver transplant By Timothy Morgan, MS IV Lake Erie College of Osteopathic Medicine Jonathan Potts, MD Interventional Radiology,
Liver Perfusion Analysis New Frontiers in Dynamic Volume Imaging. Case Study Brochure Chang Gung Memorial Hospital.
 New Frontiers in Dynamic Volume Imaging dynamic volume CT Case Study Brochure Chang Gung Memorial Hospital http://www.toshibamedicalsystems.com Toshiba Medical Systems Corporation 2010-2011. All rights
New Frontiers in Dynamic Volume Imaging dynamic volume CT Case Study Brochure Chang Gung Memorial Hospital http://www.toshibamedicalsystems.com Toshiba Medical Systems Corporation 2010-2011. All rights
Treatment of Hepatocellular Carcinoma. Andrew J. Muir, MD MHS Division of Gastroenterology Duke University Medical Center
 Treatment of Hepatocellular Carcinoma Andrew J. Muir, MD MHS Division of Gastroenterology Duke University Medical Center Epidemiology of HCC: world The 5 th most common cancer worldwide > 500, 000 new
Treatment of Hepatocellular Carcinoma Andrew J. Muir, MD MHS Division of Gastroenterology Duke University Medical Center Epidemiology of HCC: world The 5 th most common cancer worldwide > 500, 000 new
Liver Cancer: Diagnosis and Treatment Options
 Liver Cancer: Diagnosis and Treatment Options Fred Poordad, MD Chief, Hepatology University Transplant Center Professor of Medicine UT Health, San Antonio VP, Academic and Clinical Affairs, Texas Liver
Liver Cancer: Diagnosis and Treatment Options Fred Poordad, MD Chief, Hepatology University Transplant Center Professor of Medicine UT Health, San Antonio VP, Academic and Clinical Affairs, Texas Liver
Laser Interstitial Thermal Therapy (LITT) in Neuro-Oncology. Tim Lucas, MD, PhD Neurosurgery
 in Neuro-Oncology. Tim Lucas, MD, PhD Neurosurgery") Laser Interstitial Thermal Therapy (LITT) in Neuro-Oncology Tim Lucas, MD, PhD Neurosurgery Timothy.Lucas@uphs.upenn.edu 2016 Laser Interstitial Thermal Therapy (LITT) in Neuro-Oncology Tim Lucas, MD,
Laser Interstitial Thermal Therapy (LITT) in Neuro-Oncology Tim Lucas, MD, PhD Neurosurgery Timothy.Lucas@uphs.upenn.edu 2016 Laser Interstitial Thermal Therapy (LITT) in Neuro-Oncology Tim Lucas, MD,
RADIOFREQUENCY ABLATION
 RADIOFREQUENCY ABLATION ELIZABETH DAVID M D FRCPC VASCULAR A ND INTERVENTIONAL RADIOLOGIST SUNNYBROOK HEALTH SCIENCES CENTRE GIST GASTROINTESTINAL STROMAL TUMORS Stromal or mesenchymal neoplasms affecting
RADIOFREQUENCY ABLATION ELIZABETH DAVID M D FRCPC VASCULAR A ND INTERVENTIONAL RADIOLOGIST SUNNYBROOK HEALTH SCIENCES CENTRE GIST GASTROINTESTINAL STROMAL TUMORS Stromal or mesenchymal neoplasms affecting
HCC Imaging and Advances in Locoregional Therapy. David S. Kirsch MD Ochsner Clinic Foundation
 HCC Imaging and Advances in Locoregional Therapy David S. Kirsch MD Ochsner Clinic Foundation -Nothing to disclose Hepatic Imaging Primary imaging modalities include: US CT MR Angiography Nuclear medicine
HCC Imaging and Advances in Locoregional Therapy David S. Kirsch MD Ochsner Clinic Foundation -Nothing to disclose Hepatic Imaging Primary imaging modalities include: US CT MR Angiography Nuclear medicine
State-of-the-art minimally invasive interventions for liver tumors
 William Lo, HMS MD/PhD candidate, MS III Gillian Lieberman, MD State-of-the-art minimally invasive interventions for liver tumors William Lo, HMS MD/PhD candidate, MS III Gillian Lieberman, MD
William Lo, HMS MD/PhD candidate, MS III Gillian Lieberman, MD State-of-the-art minimally invasive interventions for liver tumors William Lo, HMS MD/PhD candidate, MS III Gillian Lieberman, MD
9/10/2018. Liver Transplant for Hepatocellular Carcinoma (HCC): What is New? DISCLOSURES
: What is New? DISCLOSURES") UCSF Transplant 2018: Pioneering Advances in Transplantation DISCLOSURES Liver Transplant for Hepatocellular Carcinoma (HCC): What is New? I have no relevant commercial interests or relationships to report
UCSF Transplant 2018: Pioneering Advances in Transplantation DISCLOSURES Liver Transplant for Hepatocellular Carcinoma (HCC): What is New? I have no relevant commercial interests or relationships to report
Appendix 5. EFSUMB Newsletter. Gastroenterological Ultrasound
 EFSUMB Newsletter 87 Examinations should encompass the full range of pathological conditions listed below A log book listing the types of examinations undertaken should be kept Training should usually
EFSUMB Newsletter 87 Examinations should encompass the full range of pathological conditions listed below A log book listing the types of examinations undertaken should be kept Training should usually
TACE: coming of age?
 Invasive procedures in the diagnosis and treatment of liver diseases: focal lesions F.Farinati Gastroenterologia, Padova TACE: coming of age? AISF 2005 TACE: LEVELS OF EVIDENCE Degree of certainty Methodology
Invasive procedures in the diagnosis and treatment of liver diseases: focal lesions F.Farinati Gastroenterologia, Padova TACE: coming of age? AISF 2005 TACE: LEVELS OF EVIDENCE Degree of certainty Methodology
Hepatocellular carcinoma: Intra-arterial treatments
 Hepatocellular carcinoma: Intra-arterial treatments Irene Bargellini U.O. Radiologia Interventistica Azienda Ospedaliero Universitaria Pisana IRENE BARGELLINI,MD UO RADIOLOGIA INTERVENTISTICA, AZIENDA
Hepatocellular carcinoma: Intra-arterial treatments Irene Bargellini U.O. Radiologia Interventistica Azienda Ospedaliero Universitaria Pisana IRENE BARGELLINI,MD UO RADIOLOGIA INTERVENTISTICA, AZIENDA
Learning Objectives. After attending this presentation, participants will be able to:
 Learning Objectives After attending this presentation, participants will be able to: Describe HCV in 2015 Describe how to diagnose advanced liver disease and cirrhosis Identify the clinical presentation
Learning Objectives After attending this presentation, participants will be able to: Describe HCV in 2015 Describe how to diagnose advanced liver disease and cirrhosis Identify the clinical presentation
Il treatment plan nella terapia sistemica dell epatocarcinoma
 Il treatment plan nella terapia sistemica dell epatocarcinoma M. Iavarone, MD PhD CRC A.M. e A. Migliavacca Center for the Study of Liver Disease Division of Gastroenterology and Hepatology Fondazione
Il treatment plan nella terapia sistemica dell epatocarcinoma M. Iavarone, MD PhD CRC A.M. e A. Migliavacca Center for the Study of Liver Disease Division of Gastroenterology and Hepatology Fondazione
Liver Cancer And Tumours
 Liver Cancer And Tumours What causes liver cancer? Many factors may play a role in the development of cancer. Because the liver filters blood from all parts of the body, cancer cells from elsewhere can
Liver Cancer And Tumours What causes liver cancer? Many factors may play a role in the development of cancer. Because the liver filters blood from all parts of the body, cancer cells from elsewhere can
TRANSEARTERIAL CHEMO- EMBOLIZATION FOR HEPATIC METASTASES FROM NEURO-ENDOCINE NEOPLASIA AND HEPATOMA DR SAMIA AHMAD
 UNIVERSITY OF PRETORIA STEVE BIKO ACADEMIC HOSPITAL SOUTH AFRICA TRANSEARTERIAL CHEMO- EMBOLIZATION FOR HEPATIC METASTASES FROM NEURO-ENDOCINE NEOPLASIA AND HEPATOMA DR SAMIA AHMAD 1 INTRODUCTION Hepatic
UNIVERSITY OF PRETORIA STEVE BIKO ACADEMIC HOSPITAL SOUTH AFRICA TRANSEARTERIAL CHEMO- EMBOLIZATION FOR HEPATIC METASTASES FROM NEURO-ENDOCINE NEOPLASIA AND HEPATOMA DR SAMIA AHMAD 1 INTRODUCTION Hepatic
Radiofrequency Ablation (RFA) / Microwave Ablation (MWA) of Lung Tumors
 / Microwave Ablation (MWA) of Lung Tumors") Scan for mobile link. Radiofrequency Ablation (RFA) / Microwave Ablation (MWA) of Lung Tumors Radiofrequency ablation (RFA) and microwave ablation (MWA) are treatments that use image guidance to place
Scan for mobile link. Radiofrequency Ablation (RFA) / Microwave Ablation (MWA) of Lung Tumors Radiofrequency ablation (RFA) and microwave ablation (MWA) are treatments that use image guidance to place
RETHINKING OUR APPROACH TO INTERMEDIATE-SIZE HCC
 SATELLITE SYMPOSIUM Emerging Horizons in HCC: From Palliation to Cure RETHINKING OUR APPROACH TO INTERMEDIATE-SIZE HCC Professor Riccardo Lencioni, MD, FSIR, EBIR University of Pisa School of Medicine,
SATELLITE SYMPOSIUM Emerging Horizons in HCC: From Palliation to Cure RETHINKING OUR APPROACH TO INTERMEDIATE-SIZE HCC Professor Riccardo Lencioni, MD, FSIR, EBIR University of Pisa School of Medicine,
BSD-2000 Hyperthermia System
 BSD-2000 Hyperthermia System Hyperthermia: another weapon in the fight against cancer What is Hyperthermia The BSD-2000 Hyperthermia System (BSD- 2000) is used to deliver therapeutic heating (hyperthermia)
BSD-2000 Hyperthermia System Hyperthermia: another weapon in the fight against cancer What is Hyperthermia The BSD-2000 Hyperthermia System (BSD- 2000) is used to deliver therapeutic heating (hyperthermia)
Radioembolization with Lipiodol for the Treatment of Hepatocellular Carcinoma and Liver Metastases
 Radioembolization with Lipiodol for the Treatment of Hepatocellular Carcinoma and Liver Metastases Pr Francesco Giammarile CHLS Lyon Faculté de Lyon Sud «Aut tace aut loquere meliora silentio» Malignant
Radioembolization with Lipiodol for the Treatment of Hepatocellular Carcinoma and Liver Metastases Pr Francesco Giammarile CHLS Lyon Faculté de Lyon Sud «Aut tace aut loquere meliora silentio» Malignant
Liver imaging takes a step forward with Ingenia
 Publication for the Philips MRI Community ISSUE 49 2013 / 2 Liver imaging takes a step forward with Ingenia Lyon South Hospital strives to move from several studies first CT, then MR or PET to using just
Publication for the Philips MRI Community ISSUE 49 2013 / 2 Liver imaging takes a step forward with Ingenia Lyon South Hospital strives to move from several studies first CT, then MR or PET to using just
SIRT for Intermediate and Advanced HCC
 Pamplona, junio de 2008 SIRT for Intermediate and Advanced HCC Bruno Sangro Clínica Universidad de Navarra. CIBERehd. Pamplona, Spain 90 Y-RE MRI SPECT FUSION 90 Y-RE = Yttrium-90 radioembolization Sangro
Pamplona, junio de 2008 SIRT for Intermediate and Advanced HCC Bruno Sangro Clínica Universidad de Navarra. CIBERehd. Pamplona, Spain 90 Y-RE MRI SPECT FUSION 90 Y-RE = Yttrium-90 radioembolization Sangro
Percutaneous Radiofrequency Ablation of Lung Malignant Tumours: Survival, disease progression and complication rates
 Percutaneous Radiofrequency Ablation of Lung Malignant Tumours: Survival, disease progression and complication rates Poster No.: C-2576 Congress: ECR 2012 Type: Authors: Keywords: DOI: Scientific Exhibit
Percutaneous Radiofrequency Ablation of Lung Malignant Tumours: Survival, disease progression and complication rates Poster No.: C-2576 Congress: ECR 2012 Type: Authors: Keywords: DOI: Scientific Exhibit
UPDATE OF EASL CLINICAL PRACTICE GUIDELINES: MANAGEMENT OF HEPATOCELLULAR CARCINOMA*
 UPDATE OF EASL CLINICAL PRACTICE GUIDELINES: MANAGEMENT OF HEPATOCELLULAR CARCINOMA* Dr. Catherine Frenette Medical Director of Liver Transplantation, Scripps Green Hospital, La Jolla, CA, USA May 2018
UPDATE OF EASL CLINICAL PRACTICE GUIDELINES: MANAGEMENT OF HEPATOCELLULAR CARCINOMA* Dr. Catherine Frenette Medical Director of Liver Transplantation, Scripps Green Hospital, La Jolla, CA, USA May 2018
HCC: Is it an oncological disease? - No
 June 13-15, 2013 Berlin, Germany Prof. Oren Shibolet Head of the Liver Unit, Department of Gastroenterology Tel-Aviv Sourasky Medical Center and Tel-Aviv University HCC: Is it an oncological disease? -
June 13-15, 2013 Berlin, Germany Prof. Oren Shibolet Head of the Liver Unit, Department of Gastroenterology Tel-Aviv Sourasky Medical Center and Tel-Aviv University HCC: Is it an oncological disease? -
Liver 6/5/14. Collecting Cancer Data: Liver NAACCR Webinar Series. June 5, 2014
 Collecting Cancer Data: Liver 2013 2014 NAACCR Webinar Series June 5, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Collecting Cancer Data: Liver 2013 2014 NAACCR Webinar Series June 5, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
SEQUENCING OF HCC TREATMENT. Dr. Amit G. Singal Medical Director, UT Southwestern Medical Center, USA
 SEQUENCING OF HCC TREATMENT Dr. Amit G. Singal Medical Director, UT Southwestern Medical Center, USA February 2018 DISCLAIMER Please note: The views expressed within this presentation are the personal
SEQUENCING OF HCC TREATMENT Dr. Amit G. Singal Medical Director, UT Southwestern Medical Center, USA February 2018 DISCLAIMER Please note: The views expressed within this presentation are the personal
NAACCR Webinar Series 1
 Collecting Cancer Data: Liver 2013 2014 NAACCR Webinar Series June 5, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Collecting Cancer Data: Liver 2013 2014 NAACCR Webinar Series June 5, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Jose Ramos. Role of Surgery in isolated hepatic metastasis from breast carcinoma, melanoma or sarcoma
 Role of Surgery in isolated hepatic metastasis from breast carcinoma, melanoma or sarcoma Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Evolution of liver resection Better understanding
Role of Surgery in isolated hepatic metastasis from breast carcinoma, melanoma or sarcoma Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Evolution of liver resection Better understanding
The Egyptian Journal of Hospital Medicine (July 2014) Vol. 56, Page
 Vol. 56, Page") The Egyptian Journal of Hospital Medicine (July 2014) Vol. 56, Page 289-299 Role of Percutaneous Microwave Ablation in Treatment of Hepatocellular Carcinoma Ahmed Tharwat Sayed, MSc *, Sahar M El Fiky,
The Egyptian Journal of Hospital Medicine (July 2014) Vol. 56, Page 289-299 Role of Percutaneous Microwave Ablation in Treatment of Hepatocellular Carcinoma Ahmed Tharwat Sayed, MSc *, Sahar M El Fiky,
HCC su cirrosi: terapia delle forme avanzate con farmaci bersaglio. C è ancora spazio per l ablazione percutanea?
 HCC su cirrosi: terapia delle forme avanzate con farmaci bersaglio. C è ancora spazio per l ablazione percutanea? Paestum 15 Maggio 2014 Prof A. Giorgio Director Interventional Ultrasound Units Athena
HCC su cirrosi: terapia delle forme avanzate con farmaci bersaglio. C è ancora spazio per l ablazione percutanea? Paestum 15 Maggio 2014 Prof A. Giorgio Director Interventional Ultrasound Units Athena
CELON POWER SYSTEM FOR TUMOR ABLATION Bipolar and Multipolar RFA
 1 CELON POWER SYSTEM FOR TUMOR ABLATION Bipolar and Multipolar RFA SAFE, EFFECTIVE AND UNIQUE Bipolar and multipolar radiofrequency ablation (RFA) with the CELON Power System allows an effective treatment
1 CELON POWER SYSTEM FOR TUMOR ABLATION Bipolar and Multipolar RFA SAFE, EFFECTIVE AND UNIQUE Bipolar and multipolar radiofrequency ablation (RFA) with the CELON Power System allows an effective treatment
Radiofrequency Ablation of Primary or Metastatic Liver Tumors
 Radiofrequency Ablation of Primary or Metastatic Liver Tumors Policy Number: 7.01.91 Last Review: 9/2018 Origination: 2/1996 Next Review: 9/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC)
Radiofrequency Ablation of Primary or Metastatic Liver Tumors Policy Number: 7.01.91 Last Review: 9/2018 Origination: 2/1996 Next Review: 9/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC)
Lasers in Gastroenterology, Otorhinolaryngology & Pulmonology
 Lasers in Gastroenterology, Otorhinolaryngology & Pulmonology Eloise Anguluan Laser-Tissue Interactions Fall Semester 2016 Gastroenterology the branch of medicine which deals with disorders of the stomach
Lasers in Gastroenterology, Otorhinolaryngology & Pulmonology Eloise Anguluan Laser-Tissue Interactions Fall Semester 2016 Gastroenterology the branch of medicine which deals with disorders of the stomach
How to evaluate tumor response? Yonsei University College of Medicine Kim, Beom Kyung
 How to evaluate tumor response? Yonsei University College of Medicine Kim, Beom Kyung End points in research for solid cancers Overall survival (OS) The most ideal one, but requires long follow-up duration
How to evaluate tumor response? Yonsei University College of Medicine Kim, Beom Kyung End points in research for solid cancers Overall survival (OS) The most ideal one, but requires long follow-up duration
Radiation Therapy for Liver Malignancies
 Outline Radiation Therapy for Liver Malignancies Albert J. Chang, M.D., Ph.D. Department of Radiation Oncology, UCSF March 23, 2014 Rationale for developing liver directed therapies Liver directed therapies
Outline Radiation Therapy for Liver Malignancies Albert J. Chang, M.D., Ph.D. Department of Radiation Oncology, UCSF March 23, 2014 Rationale for developing liver directed therapies Liver directed therapies
Analysis of efficacy and safety of TACE in combination with RFA and MWA in the treatment of middle and large primary hepatic carcinoma
 JBUON 2019; 24(1): 163-170 ISSN: 1107-0625, online ISSN: 2241-6293 www.jbuon.com E-mail: editorial_office@jbuon.com ORIGINAL ARTICLE Analysis of efficacy and safety of TACE in combination with RFA and
JBUON 2019; 24(1): 163-170 ISSN: 1107-0625, online ISSN: 2241-6293 www.jbuon.com E-mail: editorial_office@jbuon.com ORIGINAL ARTICLE Analysis of efficacy and safety of TACE in combination with RFA and