7.3 Suggested Evaluation and Treatment for Immunerelated Adverse Events Gastrointestinal Tract
|
|
|
- Lucas Day
- 6 years ago
- Views:
Transcription
1 7.3 Suggested Evaluation and Treatment for Immunerelated Adverse Events Early diagnosis and treatment intervention for high-grade iraes can help prevent the occurrence of complications, such as GI perforation. Gastrointestinal (diarrhea) and skin (rash)-related toxicities are the most common iraes reported in studies with ipilimumab. Suggested evaluation procedures for suspected iraes of the GI tract, liver, skin, eye, pituitary, and adrenal gland are described below. When symptomatic therapy is inadequate or inappropriate, an irae should be treated with systemic corticosteroids followed by a gradual taper. Infrequently, subjects with iraes may require courses of corticosteroid or other immunosuppressive agents that exceed 4 weeks in duration. It is recommended that subjects receiving immunosuppressive agents beyond 4 to 6 weeks should also receive antimicrobial prophylaxis to protect against the emergence of opportunistic infections. Such prophylaxis should include protection against Pneumocystis jiroveci (formerly P carinii) and prevalent fungal strains, as well as considerations for any additional pathogens that may be indicated by the medical history (e.g., herpes simplex virus, cytomegalovirus) or the environment (e.g., occupation, recent travel) of the subject. Consultation with infectious disease specialists may be considered. Immune-related (ir)ae management algorithms for general iraes, and ipilimumabrelated diarrhea, hepatotoxicity, endocrinopathy, and neuropathy have been developed and are attached in Appendices 6, 7, 8, 9, and 10 respectively Gastrointestinal Tract The differential diagnosis for subjects presenting with abdominal pain should include colitis, perforation, or pancreatitis. Additionally, a few subjects with abdominal pain also had acute swelling of the cecal wall on CT scan that may have represented localized inflammation. Diarrhea (defined as either first watery stool, or increase in frequency 50% above baseline with urgency or nocturnal bowel movement, or bloody stool) should be further evaluated and infectious or alternate etiologies ruled out. Subjects should be advised to inform the investigator if any diarrhea occurs, even if it is mild. An algorithm for managing subjects with diarrhea or suspected colitis is provided in Appendix 7. The majority of subjects with ipilimumab-induced diarrhea or colitis responded to symptomatic therapy or corticosteroids. Permanent discontinuation of ipilimumab and starting high dose corticosteroid therapy (e.g., methylprednisolone 2 mg/kg once or twice per day or equivalent) is strongly recommended for ipilimumab related Grade 3 diarrhea/colitis and steroids should be slowly tapered according to symptomatic response over at least 1 month. Subjects with ipilimumab-related Grade 2 diarrhea/colitis have to skip ipilimumab dosing and may be initially treated conservatively with loperamide, fluid replacement or budesonide, but should be immediately switched to corticosteroids (prednisone 1 mg/kg or equivalent) if symptoms persist for 3-5 days or worsen. Most subjects with diarrhea/colitis will rapidly respond to initiation of corticosteroids. The dose should be Approved v6.0
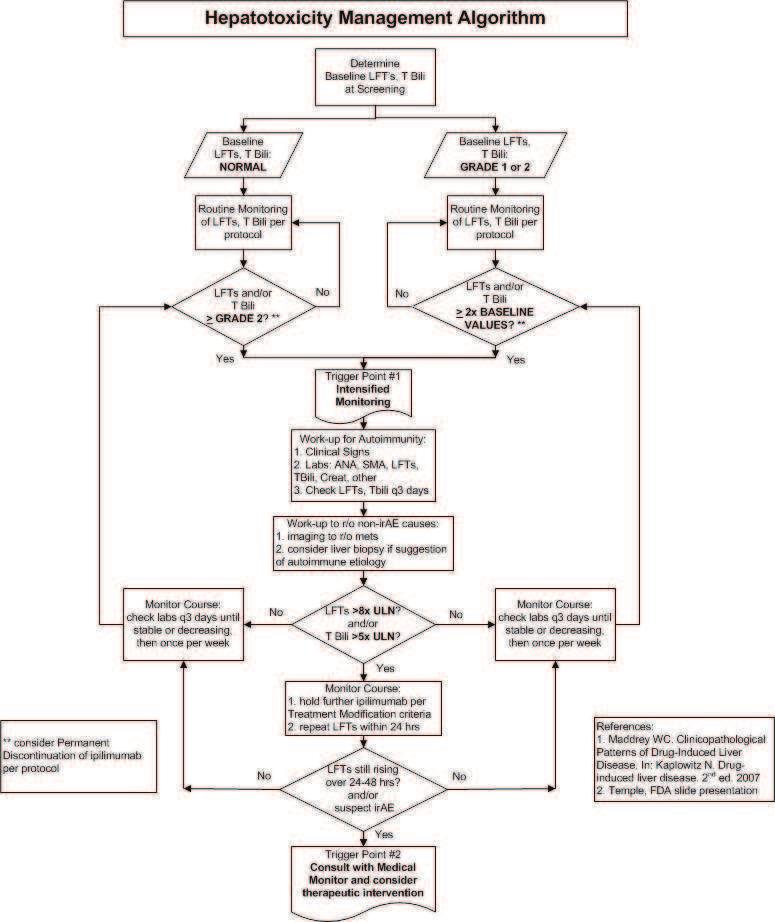
2 gradually tapered over at least a 1-month duration. Lower doses of prednisone may be considered for less severe cases of colitis. It is suggested that prednisone (for oral administration) or methylprednisolone (for IV administration) be the corticosteroids of choice in the treatment of colitis. Caution should be taken in the use of narcotics in patients with abdominal pain or colitis/diarrhea as narcotic use may mask the signs of colonic perforation. Infrequently, subjects will appear refractory to corticosteroids or will flare following taper of corticosteroids. In these subjects, unless contraindicated (i.e., sepsis, perforation and other serious infections), a single dose of infliximab at 5 mg/kg may provide benefit. For patients with concomitant hepatitis, use of mycophenolate mofetil is recommended in place of infliximab. For patients with long term immunosuppressive therapy, administer antimicrobial prophylactics as appropriate per institutional guidelines. Such cases should be discussed with the sponsor study medical monitor. If the event is prolonged or severe or is associated with signs of systemic inflammation oracute phase reactants (e.g., increased CRP or platelet count; or bandemia), it is recommended that sigmoidoscopy (or colonoscopy, if appropriate) with colonic biopsy of 3 to 5 specimens for standard paraffin block be performed. If possible, 1 to 2 biopsy specimens should be snap-frozen and stored. All subjects with confirmed colitis should also have an ophthalmologic examination, including a slitlamp exam, to rule out uveitis. Tests should also be performed for stool calprotectin and WBCs as outlined in Appendix Liver Liver function tests should always be performed and reviewed prior to administration of all ipilimumab doses. Patients treated with ipilimumab may develop elevation in LFT in the absence of clinical symptoms. In addition, subjects presenting with right upper quadrant abdominal pain, unexplained nausea, or vomiting should have LFTs performed immediately and reviewed before administering the next dose of study drug. Any increase in LFT should be evaluated to rule out non-inflammatory causes of hepatotoxicity including infections, disease progression or medications and followed with frequent LFT monitoring at 3-day intervals until resolution. Any LFTs Grade 2 (for subjects with normal baseline LFT) or LFT 2 times baseline values (for subjects with baseline LFT of Grade 1 or 2) should prompt treating physicians to: (1) contact the medical monitor; (2) increase frequency of monitoring LFTs to at least every 3 days until LFT have stabilized or improved; (3) investigate to rule out non-irae etiologies; and (4) initiate an autoimmunity evaluation. Disease progression, other malignancies, concurrent medications, viral hepatitis, and toxic etiologies should be considered and addressed, as appropriate. Imaging of the liver, gall bladder, and bile ducts should be considered to rule out neoplastic or other non-irae-related causes for the increased LFTs. An ANA, perinuclear anti-neutrophil cytoplasmic antibody (panca), and anti-smooth muscle antibody test should be performed if an autoimmune etiology is considered. If the LFTs are > 5 times the upper limit of normal (ULN) or total bilirubin is > 3 times the ULN, then ipilimumab dosing should be held according to the dose modification guidelines. Subjects with LFT elevations > 8x the ULN that are judged to be due to ipilimumab should initiate high-dose corticosteroid therapy (e.g., methylprednisolone 2 mg/kg once or twice daily or equivalent) and permanently stop administration of ipilimumab. In subjects with > 8x ULN, LFT should be performed daily until stable or declining for Approved v6.0
3 5 consecutive days. LFT should be monitored for at least 2 consecutive weeks to ensure sustained treatment response. If symptoms or LFT elevations are controlled, the corticosteroid dose should be gradually tapered over a period of at least 1 month. Flare in LFTs during this taper may be treated with an increase in the dose of steroid and a slower taper. In subjects without response to corticosteroid therapy within 3 to 5 days or who have an LFT flare during steroid tapering that is not responsive to an increase in steroids, addition of immunosuppression with mycophenolate mofetil should be considered after a gastroenterology/hepatology consult. Patients receiving immunosuppression for more than 4 weeks should be evaluated for prophylaxis of opportunistic infections per institutional guidelines. An algorithm for evaluating subjects with elevated LFT is provided in Appendix Skin A dermatologist should evaluate persistent or severe rash or pruritus. A biopsy should be performed if appropriate and if possible, photos of the rash should also be obtained. Patients with low-grade ipilimumab-mediated skin toxicity (Grade 1 or 2) may remain on therapy and could be treated with symptomatic therapy (e.g., antihistamines). Low-grade symptoms persisting for 1 to 2 weeks and relapsing should be treated with topical or oral corticosteroid therapy (e.g., prednisone 1 mg/kg once daily or equivalent). High-grade (Grade 3 or 4) symptoms require high-dose IV corticosteroid therapy (e.g., methylprednisolone 2 mg/kg once or twice per day or equivalent) to control initial symptoms. A skin biopsy should be performed if appropriate. Once rash or pruritis is controlled, the initiation of corticosteroid taper should be based on clinical judgment; however, the corticosteroid dose should be gradually tapered over a period of at least 1 month. Patients with any high-grade skin related toxicity (Grade 3 regardless of causality) have to skip ipilimumab and may only continue treatment with ipilimumab if the initial symptoms have improved to Grade 1, while patients with grade 4 skin toxicities have to permanently discontinue ipilimumab Endocrine Most subjects with hypopituitarism presented with nonspecific complaints such as fatigue, visual field defects, confusion, or impotence. Some have had headache as the predominant presentation. The majority of subjects with hypopituitarism demonstrated enlarged pituitary glands based on brain MRI. Low adrenocorticotropic hormone (ACTH) and cortisol were the most common biochemical abnormality; low TSH, free T4, T3, testosterone or prolactin have also been reported in some subjects. Subjects with unexplained symptoms such as fatigue, myalgias, impotence, mental status changes, or constipation should be investigated for the presence of thyroid, pituitary or adrenal endocrinopathies. An endocrinologist should be consulted if an endocrinopathy is suspected. If there are any signs of adrenal crisis such as severe dehydration, hypotension, or shock, IV corticosteroids with mineralocorticoid activity (e.g., methylprednisolone) should be initiated immediately. If the patient s symptoms are suggestive of an endocrinopathy but the patient is not in adrenal crisis, an endocrine laboratory results should be evaluated before corticosteroid therapy is initiated. Endocrine work up should include at least thyroid stimulating hormone (TSH) and free T4 levels should be obtained to determine if thyroid abnormalities are present. TSH, prolactin and a morning cortisol level will help to differentiate primary adrenal insufficiency from primary pituitary insufficiency. Radiographic imaging (e.g., Approved v6.0
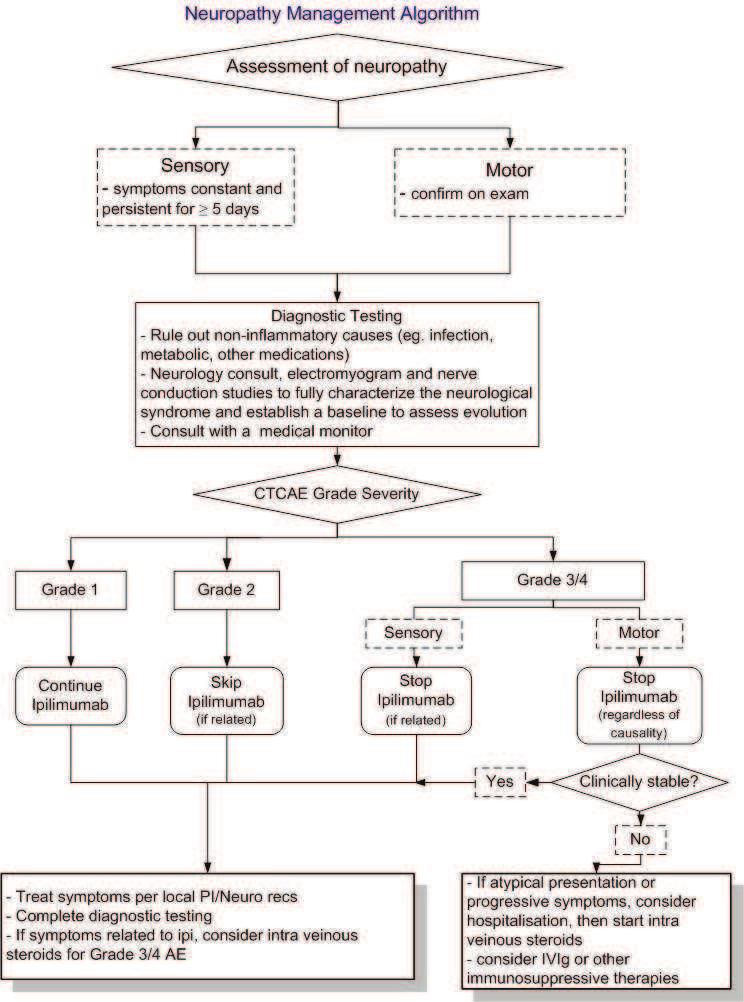
4 MRI) with pituitary cuts should be performed. If the pituitary scan and/or endocrine laboratorytests are abnormal, a short course of high dose corticosteroids (e.g., dexamethasone 4 mg every 6 hours or equivalent) should be considered in an attempt to treat the presumed pituitary inflammation, but it is currently unknown if this will reverse the pituitary dysfunction. Abrupt discontinuation of corticosteroids should be avoided due to possible prolonged adrenal suppression. Once symptoms or laboratory abnormalities are controlled, and overall patient improvement is evident, the initiation of steroid taper should be based on clinical judgment; however the corticosteroid dose should be gradually tapered over a period of at least 1 month. Appropriate hormone replacement therapy should be instituted if an endocrinopathy isdocumented, and it is possible that subjects may require life-long hormone replacement. An endocrinopathy management algorithm is presented in Appendix Neuropathy Subjects presenting with sensory symptoms lasting more than 5 days or motor symptoms confirmed by physical examinations should be evaluated and noninflammatory causes such as disease progression, infections (including Lyme disease), metabolic syndromes and medications (such as taxanes and/or platinum salts) should be ruled out. A neurology consult should be obtained and diagnostic characterization of the neurological syndrome (electromyogram, nerve conduction studies) should be started. The next dose of ipilimumab should be skipped if the event of a Grade 2 neuropathy (sensitive or motor) is related to study drug. The administration of ipilimumab should be permanently discontinued in patients with Grade 3 or 4 sensory neuropathy suspected to be related to study drug. Patients should be treated according to institutional guidelines and the administration of IV steroids (e.g., methylprednisolone 2 mg/kg once or twice per day or equivalent) should be considered. The administration of ipilimumab should be permanently discontinued in patients with Grade 3 or 4 motor neuropathy regardless of the causality to study drug. Patients with Grade 3 or 4 motor neuropathy who are clinically stable should be treated according to institution guidelines and the administration of IV steroids therapy (e.g., methylprednisolone 2 mg/kg once or twice per day or equivalent) should be considered. Patients with Grade 3 or 4 motor neuropathy who are not clinically stable or who have atypical symptoms should be hospitalized and the IV administration of steroids should be initiated and IV immunoglobulin (IVIg) or other immunosuppressive therapies (as appropriate) should be considered. A neuropathy management algorithm is presented in Appendix Other Ocular inflammation (episcleritis or uveitis) was reported in a few subjects. These conditions responded to topical corticosteroid therapy. An ophthalmologist should evaluate visual complaints with examination of the conjunctiva, anterior and posterior chambers, and retina. Visual field testing and an electroretinogram should also be performed. Examination and testing should be documented on the appropriate case report form (CRF). Ipilimumab-related uveitis or episcleritis may be treated with topical corticosteroid eye drops. Symptoms of abdominal pain associated with elevations of amylase and lipase suggestive of pancreatitis may be associated with anti-ctla-4 monoclonal antibody administration. The differential diagnosis of acute abdominal pain should include pancreatitis. Appropriate evaluation should include serum amylase and lipase tests. Approved v6.0

5 Diarrhea Management Algorithm Diarrhea GRADE 1 Increase of < 4 stools per day over baseline; mild increase in ostomy output compared with baseline GRADE 2 Increase of 4-6 stools per day over baseline; IV fluids indicated < 24 hrs; moderate increase in ostomy output compared to baseline; not interfering with ADL GRADE 3 Increase of 7 stools per day over baseline; incontinence; IV fluids 24 hrs; hospitalization; severe increase in ostomy output compared to baseline; interfering with ADL GRADE 4 Lifethreatening consequences (eg, hemodynamic collapse) GRADE 5 Death 187
6 Endocrinopathy management algorithm Suspect endocrinopathy (based on clinical signs and symptoms) 1 Suspect adrenal crisis No 1. Check endocrine labs 2 (draw before giving steroids) 2. MRI head with pituitary cuts, Visual field testing if appropriate 3. Consult medical monitor 4. Consider endocrinologist consult Endocrine labs abnormal OR Head MRI abnormal Yes Condition stablized 1 Clinical signs and symptoms that may be indicative of underlying endocrinopathy headache, visual field defects, fatigue, weakness, asthenia, failure to thrive, anorexia, nausea and vomiting, lethargy, impotence, amenorrhea, fever, coma, new onset atrial fibrillation, hypotension, hypoglycemia, hyponatremia, eosinophilia Suspect adrenal crisis 1. Rule out sepsis 2. If strong suspicion of adrenal crisis (eg. exhibits signs of severe dehydration, hypotension, or shock out of proportion to severity of current illness) then start stress dose IV steroids (with mineralocorticoid activity), fluids, consult endocrinologist 3. If symptoms suggestive of endocrinopathy but patient is not in crisis then it may be appropriate to wait for lab results before starting steroid therapy 2 Suggested endocrine labwork: 1. TSH, free T4, T3 2. ACTH, AM serum cortisol => if abnormal, co-syntropin stimulation test 3. LH, FSH, testosterone, prolactin No Yes 3 Ipilimumab dosing: 1. Rule-out other etiologies for patient symptoms 2. Initiate more frequent patient follow-up 3. Repeat endocrine labs in 1-3 wks If lab and radiologic results are negative but symptoms persist: 1. consult Endocrinologist 2. consider repeating head MRI in 1 month 1. Initiate short course of high dose steroid treatment to reverse inflammation 2. Initiate appropriate hormone replacement to reverse endocrinopathy 3. Consult endocrinologist as needed 4. Review ipilimumab dose modification criteria per protocol 3 Long term follow-up 1. Taper high dose steroids 4 2. Continue hormone replacement as needed 3. Monitor endocrine labs as appropriate 4. Repeat MRI as clinically indicated a) Upon resolution or adequate treatment of endocrinopathy, patients may continue ipilimumab dosing with appropriate hormone replacement unless limited by protocol. b) The risk of having a recurrence of endocrinopathy with subsequent ipilimumab dosing after experiencing initial IRAE is currently unknown 4 Prolonged replacement steroid therapy: a) Patients may require chronic hydrocortisone replacement to maintain homeostatic levels b) Beware of complete discontinuation of steroids due to prolonged adrenal suppression Footnote For numbered footnotes ( 1,2,3,4 ), please refer to further explanation and text found in the corresponding dotted line boxes to the right side of the algorithm 192
7 The most current experience with immune-related hepatitis has allowed further development of this management algorithm to include recommendations for treatment. HEPATOTOXICITY THERAPEUTIC INTERVENTION ALGORITHM Situation: rising liver function tests (LFTs) > 8X ULN or suspected immune-mediated hepatitis 1) Admit subject to hospital for evaluation and close monitoring 2) Stop further ipilimumab dosing until hepatotoxicity is resolved. Consider permanent discontinuation of ipilimumab per protocol (Section of protocol) 3) Start at least 120 mg methylprednisolone sodium succinate per day, given IV as a single or divided dose 4) Check liver laboratory test values (LFTs, T-bilirubin) daily until stable or showing signs of improvement for at least 3 consecutive days 5) If no decrease in LFTs after 3 days or rebound hepatitis occurs despite treatment with corticosteroids, then add mycophenolate mofetil 1g BID per institutional guidelines for immunosuppression of liver transplants (supportive treatment as required, including prophylaxis for opportunistic infections per institutional guidelines) 6) If no improvement after 5 to 7 days, consider adding 0.10 to 0.15 mg/kg/day of tacrolimus (trough level 5-20 ng/ml) 7) If target trough level is achieved with tacrolimus but no improvement is observed after 5 to 7 days, consider infliximab, 5 mg/kg, once 8) Continue to check LFTs daily for at least 2 weeks to monitor sustained response to treatment A flow chart of the algorithm is depicted in the following page. 189
8 190
9 194
Ipilimumab in Melanoma
 Ipilimumab in Melanoma Indication: Advanced (unresectable or metastatic) melanoma in adults who have received prior therapy LCNDG criteria to be met: Histologically confirmed unresectable stage III or
Ipilimumab in Melanoma Indication: Advanced (unresectable or metastatic) melanoma in adults who have received prior therapy LCNDG criteria to be met: Histologically confirmed unresectable stage III or
BC Cancer Protocol Summary for Treatment of Advanced Non- Small Cell Lung Cancer Using Pembrolizumab
 BC Cancer Protocol Summary for Treatment of Advanced Non- Small Cell Lung Cancer Using Pembrolizumab Protocol Code Tumour Group Contact Physician ULUAVPMB Lung Dr. Christopher Lee ELIGIBILITY: Advanced
BC Cancer Protocol Summary for Treatment of Advanced Non- Small Cell Lung Cancer Using Pembrolizumab Protocol Code Tumour Group Contact Physician ULUAVPMB Lung Dr. Christopher Lee ELIGIBILITY: Advanced
BCCA Protocol Summary for the Treatment of Unresectable or Metastatic Melanoma Using Nivolumab
 BCCA Protocol Summary for the Treatment of Unresectable or Metastatic Melanoma Using Nivolumab Protocol Code Tumour Group Contact Physician USMAVNIV Skin and Melanoma Dr. Kerry Savage ELIGIBILITY: Unresectable
BCCA Protocol Summary for the Treatment of Unresectable or Metastatic Melanoma Using Nivolumab Protocol Code Tumour Group Contact Physician USMAVNIV Skin and Melanoma Dr. Kerry Savage ELIGIBILITY: Unresectable
Nivolumab and Ipilimumab
 Nivolumab and Ipilimumab Indication Advanced (unresectable or metastatic) melanoma. (NICE TA400) ICD-10 codes Codes prefixed with C43 Regimen details Cycles 1-4 Nivolumab and Ipilimumab every 3 weeks Day
Nivolumab and Ipilimumab Indication Advanced (unresectable or metastatic) melanoma. (NICE TA400) ICD-10 codes Codes prefixed with C43 Regimen details Cycles 1-4 Nivolumab and Ipilimumab every 3 weeks Day
Immune checkpoint inhibitors in clinical practice: update on management of immune-related toxicities
 Review Article on Lung Cancer Diagnostics and Treatments 2015: A Renaissance of Patient Care Immune checkpoint inhibitors in clinical practice: update on management of immune-related toxicities Jeryl Villadolid
Review Article on Lung Cancer Diagnostics and Treatments 2015: A Renaissance of Patient Care Immune checkpoint inhibitors in clinical practice: update on management of immune-related toxicities Jeryl Villadolid
OPTIMAL MANAGEMENT OF IMMUNE- RELATED ADVERSE EVENTS ASSOCIATED WITH CHECKPOINT INHIBITORS
 OPTIMAL MANAGEMENT OF IMMUNE- RELATED ADVERSE EVENTS ASSOCIATED WITH CHECKPOINT INHIBITORS Alberto Fusi Charité Comprehensive Cancer Centre Berlin, Germany 1 Immune check point blockade with CTLA-4, anti-pd-1
OPTIMAL MANAGEMENT OF IMMUNE- RELATED ADVERSE EVENTS ASSOCIATED WITH CHECKPOINT INHIBITORS Alberto Fusi Charité Comprehensive Cancer Centre Berlin, Germany 1 Immune check point blockade with CTLA-4, anti-pd-1
Adverse effects of Immunotherapy. Asha Nayak M.D
 Adverse effects of Immunotherapy Asha Nayak M.D None Financial Disclosures Objectives Understand intensity of the AEs. Understanding unique side-effects. Develop effective monitoring and management guidelines.
Adverse effects of Immunotherapy Asha Nayak M.D None Financial Disclosures Objectives Understand intensity of the AEs. Understanding unique side-effects. Develop effective monitoring and management guidelines.
ANNEX I SUMMARY OF PRODUCT CHARACTERISTICS
 ANNEX I SUMMARY OF PRODUCT CHARACTERISTICS 1 1. NAME OF THE MEDICINAL PRODUCT YERVOY 5 mg/ml concentrate for solution for infusion 2. QUALITATIVE AND QUANTITATIVE COMPOSITION Each ml of concentrate contains
ANNEX I SUMMARY OF PRODUCT CHARACTERISTICS 1 1. NAME OF THE MEDICINAL PRODUCT YERVOY 5 mg/ml concentrate for solution for infusion 2. QUALITATIVE AND QUANTITATIVE COMPOSITION Each ml of concentrate contains
Immunotherapy: Toxicity Management. Dr. Megan Lyle Medical Oncologist Liz Plummer Cancer Care Centre Cairns Hospital
 Immunotherapy: Toxicity Management Dr. Megan Lyle Medical Oncologist Liz Plummer Cancer Care Centre Cairns Hospital Disclosures Honoraria and travel support from BMS, MSD, Novartis Advisory board for MSD
Immunotherapy: Toxicity Management Dr. Megan Lyle Medical Oncologist Liz Plummer Cancer Care Centre Cairns Hospital Disclosures Honoraria and travel support from BMS, MSD, Novartis Advisory board for MSD
BCCA Protocol Summary for Treatment of Advanced Non-Small Cell Lung Cancer Using Nivolumab
 BCCA Protocol Summary for Treatment of Advanced Non-Small Cell Lung Cancer Using Nivolumab Protocol Code Tumour Group Contact Physician ULUAVNIV Lung Dr. Christopher Lee ELIGIBILITY: Advanced non-small
BCCA Protocol Summary for Treatment of Advanced Non-Small Cell Lung Cancer Using Nivolumab Protocol Code Tumour Group Contact Physician ULUAVNIV Lung Dr. Christopher Lee ELIGIBILITY: Advanced non-small
PEMBROLIZUMAB (KEYTRUDA ) for the treatment of advanced melanoma or previously treated NSCLC
 for the treatment of advanced melanoma or previously treated NSCLC") DRUG ADMINISTRATION SCHEDULE Day Drug Dose Route Diluent Rate Day 1 Pembrolizumab 2mg/kg IV Infusion 100mL 0.9% Sodium Chloride* Or 100mL 5% Glucose* *Final concentration must be between 1 to 10mg/mL Over
DRUG ADMINISTRATION SCHEDULE Day Drug Dose Route Diluent Rate Day 1 Pembrolizumab 2mg/kg IV Infusion 100mL 0.9% Sodium Chloride* Or 100mL 5% Glucose* *Final concentration must be between 1 to 10mg/mL Over
CANCER IMMUNOTHERAPY. Pocket Guide
 CANCER IMMUNOTHERAPY Pocket Guide Unique Clinical Features Tumor Response Kinetics Response patterns associated with immune checkpoint blockade may differ from those associated with conventional therapies,
CANCER IMMUNOTHERAPY Pocket Guide Unique Clinical Features Tumor Response Kinetics Response patterns associated with immune checkpoint blockade may differ from those associated with conventional therapies,
Melanoma Immunotherapy. Nursing Perspective on Immune-Related Adverse Events: Patient education, Monitoring & Management
 Melanoma Immunotherapy Nursing Perspective on Immune-Related Adverse Events: Patient education, Monitoring & Management Mike Buljan, NP UCSF Medical Center Melanoma Oncology Disclosures None Only FDA-approved
Melanoma Immunotherapy Nursing Perspective on Immune-Related Adverse Events: Patient education, Monitoring & Management Mike Buljan, NP UCSF Medical Center Melanoma Oncology Disclosures None Only FDA-approved
BCCA Protocol Summary for Treatment of Metastatic or Advanced Renal Cell Carcinoma Using Nivolumab
 BCCA Protocol Summary for Treatment of Metastatic or Advanced Renal Cell Carcinoma Using Nivolumab Protocol Code Tumour Group Contact Physician UGUAVNIV Genitourinary Dr. C. Kollmannsberger ELIGIBILITY:
BCCA Protocol Summary for Treatment of Metastatic or Advanced Renal Cell Carcinoma Using Nivolumab Protocol Code Tumour Group Contact Physician UGUAVNIV Genitourinary Dr. C. Kollmannsberger ELIGIBILITY:
Managing Checkpoint Inhibitor Toxicities. Megan L. Menon, Pharm.D., BCOP Roswell Park Cancer Institute
 Managing Checkpoint Inhibitor Toxicities Megan L. Menon, Pharm.D., BCOP Roswell Park Cancer Institute Approved Indications Ipilimumab Nivolumab Pembrolizumab* Atezolizumab Avelumab Durvalumab Ipi + Nivol
Managing Checkpoint Inhibitor Toxicities Megan L. Menon, Pharm.D., BCOP Roswell Park Cancer Institute Approved Indications Ipilimumab Nivolumab Pembrolizumab* Atezolizumab Avelumab Durvalumab Ipi + Nivol
Healthcare Professional. Frequently Asked. Questions. Brochure
 YERVOY (ipilimumab) Healthcare Professional Frequently Asked Questions Brochure YERVOY is indicated for the treatment of advanced (unresectable or metastatic) melanoma in adults. 1 This medicinal product
YERVOY (ipilimumab) Healthcare Professional Frequently Asked Questions Brochure YERVOY is indicated for the treatment of advanced (unresectable or metastatic) melanoma in adults. 1 This medicinal product
Ipilimumab (skin) Indication Advanced (unresectable or metastatic) melanoma in patients who have received prior therapy.
 Indication Advanced (unresectable or metastatic) melanoma in patients who have received prior therapy.") Ipilimumab (skin) Indication Advanced (unresectable or metastatic) melanoma in patients who have received prior therapy. (NICE TA268) ICD-10 codes Codes prefixed with C43 Regimen details Day Drug Dose
Ipilimumab (skin) Indication Advanced (unresectable or metastatic) melanoma in patients who have received prior therapy. (NICE TA268) ICD-10 codes Codes prefixed with C43 Regimen details Day Drug Dose
Nursing Perspective on iraes: Patient Education, Monitoring and Management
 Nursing Perspective on iraes: Patient Education, Monitoring and Management Rebecca Lewis, CRNP Nurse Practitioner University of Pittsburgh-HCC Shadyside Disclosures No relevant financial relationships
Nursing Perspective on iraes: Patient Education, Monitoring and Management Rebecca Lewis, CRNP Nurse Practitioner University of Pittsburgh-HCC Shadyside Disclosures No relevant financial relationships
Risk Minimisation Information for Healthcare Professionals. Guide for Prescribing
 Risk Minimisation Information for Healthcare Professionals Guide for Prescribing YERVOY (ipilimumab), as monotherapy, is indicated for the treatment of patients with unresectable or metastatic melanoma
Risk Minimisation Information for Healthcare Professionals Guide for Prescribing YERVOY (ipilimumab), as monotherapy, is indicated for the treatment of patients with unresectable or metastatic melanoma
ATEZOLIZUMAB (TECENTRIQ )
") DRUG ADMINISTRATION SCHEDULE Day Drug Daily Dose Route Diluent Rate Day 1 Atezolizumab 1200 mg IV Infusion 250mL 0.9% Sodium Chloride Over 60 minutes* *The initial dose of atezolizumab must be administered
DRUG ADMINISTRATION SCHEDULE Day Drug Daily Dose Route Diluent Rate Day 1 Atezolizumab 1200 mg IV Infusion 250mL 0.9% Sodium Chloride Over 60 minutes* *The initial dose of atezolizumab must be administered
ATEZOLIZUMAB (TECENTRIQ ) in urothelial carcinoma
 in urothelial carcinoma") DRUG ADMINISTRATION SCHEDULE Day Drug Daily Dose Route Diluent Rate Day 1 Atezolizumab 1200 mg IV Infusion 250mL 0.9% Sodium Chloride Over 60 minutes* *The initial dose of atezolizumab must be administered
DRUG ADMINISTRATION SCHEDULE Day Drug Daily Dose Route Diluent Rate Day 1 Atezolizumab 1200 mg IV Infusion 250mL 0.9% Sodium Chloride Over 60 minutes* *The initial dose of atezolizumab must be administered
Overcoming Toxicities Associated with Novel Checkpoint Inhibitor Immunotherapy. Tara C. Gangadhar, MD Assistant Professor of Medicine ICI Boston 2016
 Overcoming Toxicities Associated with Novel Checkpoint Inhibitor Immunotherapy Tara C. Gangadhar, MD Assistant Professor of Medicine ICI Boston 2016 Overcoming toxicity A new context for evaluating toxicity
Overcoming Toxicities Associated with Novel Checkpoint Inhibitor Immunotherapy Tara C. Gangadhar, MD Assistant Professor of Medicine ICI Boston 2016 Overcoming toxicity A new context for evaluating toxicity
Checkpoint inhibitors: Strategies to checkmate T-cell mediated toxicity. Disclosure Statement. Learning Objectives
 Checkpoint inhibitors: Strategies to checkmate T-cell mediated toxicity Adam J. DiPippo, PharmD Clinical Pharmacy Specialist Leukemia Texas Society of Health-System Pharmacists 2017 Annual Seminar April
Checkpoint inhibitors: Strategies to checkmate T-cell mediated toxicity Adam J. DiPippo, PharmD Clinical Pharmacy Specialist Leukemia Texas Society of Health-System Pharmacists 2017 Annual Seminar April
BCCA Protocol Summary for the Treatment of Unresectable or Metastatic Melanoma Using Ipilimumab
 BCCA Protocol Summary for the Treatment of Unresectable or Metastatic Melanoma Using Ipilimumab Protocol Code Tumour Group Contact Physician USMAVIPI Skin and Melanoma Dr. Kerry Savage ELIGIBILITY: Unresectable
BCCA Protocol Summary for the Treatment of Unresectable or Metastatic Melanoma Using Ipilimumab Protocol Code Tumour Group Contact Physician USMAVIPI Skin and Melanoma Dr. Kerry Savage ELIGIBILITY: Unresectable
Immunotherapy Treatment Developments in Medical Oncology
 Immunotherapy Treatment Developments in Medical Oncology A/Prof Phillip Parente Director Cancer Services Eastern Health Executive MOGA ATC Medical Oncology RACP www.racpcongress.com.au Summary of The Desired
Immunotherapy Treatment Developments in Medical Oncology A/Prof Phillip Parente Director Cancer Services Eastern Health Executive MOGA ATC Medical Oncology RACP www.racpcongress.com.au Summary of The Desired
HEY Guidelines for the management of Toxicities associated with immune checkpoint inhibitors.
 Hull and East Yorkshire Hospital NHS Trust Queen s centre for Oncology and Haematology Castle Hill Hospital HEY Guidelines for the management of Toxicities associated with immune checkpoint inhibitors.
Hull and East Yorkshire Hospital NHS Trust Queen s centre for Oncology and Haematology Castle Hill Hospital HEY Guidelines for the management of Toxicities associated with immune checkpoint inhibitors.
Immune-Related Adverse Reaction (irar) Management Guide
 Management Guide") REGIMEN Immune-Related Adverse Reaction (irar) Management Guide OPDIVO as monotherapy is indicated for the treatment of locally advanced or metastatic squamous non-small cell lung cancer (NSCLC) with progression
REGIMEN Immune-Related Adverse Reaction (irar) Management Guide OPDIVO as monotherapy is indicated for the treatment of locally advanced or metastatic squamous non-small cell lung cancer (NSCLC) with progression
NECN CHEMOTHERAPY HANDBOOK PROTOCOL
 Nivolumab (Opdivo ) for treatment of advanced melanoma and Renal Cell Cancer (Also advanced/ metastatic NSCLC EMAS patients only -Nov 2016) DRUG ADMINISTRATION SCHEDULE (SINGLE AGENT Day Drug Daily dose
Nivolumab (Opdivo ) for treatment of advanced melanoma and Renal Cell Cancer (Also advanced/ metastatic NSCLC EMAS patients only -Nov 2016) DRUG ADMINISTRATION SCHEDULE (SINGLE AGENT Day Drug Daily dose
Nivolumab Ipilimumab Combination Therapy
 INDICATIONS FOR USE: Nivolumab Ipilimumab Combination INDICATION ICD10 Regimen Code *Reimbursement Status Nivolumab in combination with ipilimumab is indicated for the treatment of advanced (unresectable
INDICATIONS FOR USE: Nivolumab Ipilimumab Combination INDICATION ICD10 Regimen Code *Reimbursement Status Nivolumab in combination with ipilimumab is indicated for the treatment of advanced (unresectable
Immune-Mediated Adverse Events Management Handbook
 Immune-Mediated Adverse Events Management Handbook Your guide to addressing the immune-mediated adverse events (imaes) associated with patients taking PD-L1 inhibition therapy Indications and Usage IMFINZI
Immune-Mediated Adverse Events Management Handbook Your guide to addressing the immune-mediated adverse events (imaes) associated with patients taking PD-L1 inhibition therapy Indications and Usage IMFINZI
Atezolizumab Non-small cell lung cancer
 Systemic Anti Cancer Treatment Protocol Atezolizumab Non-small cell lung cancer PROTOCOL REF: MPHAATNSCLC (Version No: 1.0) Approved for use in: Locally advanced/metastatic non squamous or squamous non-small
Systemic Anti Cancer Treatment Protocol Atezolizumab Non-small cell lung cancer PROTOCOL REF: MPHAATNSCLC (Version No: 1.0) Approved for use in: Locally advanced/metastatic non squamous or squamous non-small
Ipilimumab Monotherapy
 INDICATIONS FOR USE: Ipilimumab INDICATION ICD10 Regimen Code *Reimbursement Indicator Treatment of advanced (unresectable or metastatic) melanoma in adults C43 00105a ODMS *If a reimbursement indicator
INDICATIONS FOR USE: Ipilimumab INDICATION ICD10 Regimen Code *Reimbursement Indicator Treatment of advanced (unresectable or metastatic) melanoma in adults C43 00105a ODMS *If a reimbursement indicator
Management of Immune Checkpoint Inhibitor Related Toxicities
 Management of Immune Checkpoint Inhibitor Related Toxicities Katie Wolfram, PharmD Clinical Pharmacist, Oncology Memorial Hospital of South Bend A Webinar for HealthTrust Members November 12, 2018 Disclosures
Management of Immune Checkpoint Inhibitor Related Toxicities Katie Wolfram, PharmD Clinical Pharmacist, Oncology Memorial Hospital of South Bend A Webinar for HealthTrust Members November 12, 2018 Disclosures
Immunotherapy in Lung Cancer
 Immunotherapy in Lung Cancer Jamie Poust Pharm. D., BCOP Oncology Pharmacist University of Colorado Hospital Objectives Describe the recent advances in immunotherapy for patients with lung cancer Outline
Immunotherapy in Lung Cancer Jamie Poust Pharm. D., BCOP Oncology Pharmacist University of Colorado Hospital Objectives Describe the recent advances in immunotherapy for patients with lung cancer Outline
Immunotherapy. Immunotherapy Triage
 Immunotherapy Immunotherapy Triage The most commonly used drug is Ipilimumab for Metastatic Melanoma, but use of immunotherapy is developing in lung cancer and in clinical trials. Drugs include Nivolumab
Immunotherapy Immunotherapy Triage The most commonly used drug is Ipilimumab for Metastatic Melanoma, but use of immunotherapy is developing in lung cancer and in clinical trials. Drugs include Nivolumab
DOSING GUIDE. Indications. Important Safety Information. Enable the immune system. RECOGNIZE. RESPOND.
 DOSING GUIDE For patients with unresectable Stage III NSCLC following concurrent CRT For patients with locally advanced or metastatic UC previously treated with platinum-based therapy Enable the immune
DOSING GUIDE For patients with unresectable Stage III NSCLC following concurrent CRT For patients with locally advanced or metastatic UC previously treated with platinum-based therapy Enable the immune
Managing Adverse Events Associated with Immuno-oncologic Agents
 Managing Adverse Events Associated with Immuno-oncologic Agents Jennifer Diehl RN, BSN, OCN Cutaneous Oncology Program Moffitt Cancer Center Tampa, FL September 10, 2015 12-1 p.m. EST ICLIO ecourse 05
Managing Adverse Events Associated with Immuno-oncologic Agents Jennifer Diehl RN, BSN, OCN Cutaneous Oncology Program Moffitt Cancer Center Tampa, FL September 10, 2015 12-1 p.m. EST ICLIO ecourse 05
Immunotherapy toxicities. Dr Fiona Taylor
 Immunotherapy toxicities Dr Fiona Taylor Outline Understand toxicities Anticipate toxicities Key steps to safely using and achieving the most benefits from immunotherapies for patients Manage toxicities
Immunotherapy toxicities Dr Fiona Taylor Outline Understand toxicities Anticipate toxicities Key steps to safely using and achieving the most benefits from immunotherapies for patients Manage toxicities
Serologic Markers CONVENTIONAL ANTIBODIES ANTIBODIES UNCONVENTIONAL. AIH Type I
 Autoimmune Hepatitis By Thomas Frazier Objective What we need to know about AIH Diagnosis Treatment Difficulties in both Liver transplantation concerns AASLD Guidelines: Hepatology. 2010 Jun;51(6):2193-213.
Autoimmune Hepatitis By Thomas Frazier Objective What we need to know about AIH Diagnosis Treatment Difficulties in both Liver transplantation concerns AASLD Guidelines: Hepatology. 2010 Jun;51(6):2193-213.
15/05/2015. No conflict of interest for this presentation. The first in-class phosphotidlyinositol3-kinase delta (PI3K delta) inhibitor
 inhibitor") Disclosure Idelalisib - A Review No conflict of interest for this presentation Pamela Rudkin PhC Hematology Oncology Pharmacist General Hospital Site Eastern Health Care Corporation Objectives At the completion
Disclosure Idelalisib - A Review No conflict of interest for this presentation Pamela Rudkin PhC Hematology Oncology Pharmacist General Hospital Site Eastern Health Care Corporation Objectives At the completion
PITUITARY: JUST THE BASICS PART 2 THE PATIENT
 PITUITARY: JUST THE BASICS PART 2 THE PATIENT DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and
PITUITARY: JUST THE BASICS PART 2 THE PATIENT DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and
Toxicity of Systemic Melanoma Therapies. Alex Guminski Melanoma Institute Australia Royal North Shore Hospital University of Sydney
 Toxicity of Systemic Melanoma Therapies Alex Guminski Melanoma Institute Australia Royal North Shore Hospital University of Sydney Disclosures Advisory Board Novartis, BMS, Sanofi, Pfizer Travel support
Toxicity of Systemic Melanoma Therapies Alex Guminski Melanoma Institute Australia Royal North Shore Hospital University of Sydney Disclosures Advisory Board Novartis, BMS, Sanofi, Pfizer Travel support
Immune-Mediated Adverse Reactions Management Guide
 Immune-Mediated Adverse Reactions Management Guide Please see Important Safety Information for OPDIVO on pages 35 39 and US Full Prescribing Information for OPDIVO. Please refer to the end of the Important
Immune-Mediated Adverse Reactions Management Guide Please see Important Safety Information for OPDIVO on pages 35 39 and US Full Prescribing Information for OPDIVO. Please refer to the end of the Important
Treatment of Inflammatory Bowel Disease. Michael Weiss MD, FACG
 Treatment of Inflammatory Bowel Disease Michael Weiss MD, FACG What is IBD? IBD is an immune-mediated chronic intestinal disorder, characterized by chronic or relapsing inflammation within the GI tract.
Treatment of Inflammatory Bowel Disease Michael Weiss MD, FACG What is IBD? IBD is an immune-mediated chronic intestinal disorder, characterized by chronic or relapsing inflammation within the GI tract.
Summary of the risk management plan (RMP) for Opdivo (nivolumab)
 for Opdivo (nivolumab)") EMA/285771/2015 Summary of the risk management plan (RMP) for Opdivo (nivolumab) This is a summary of the risk management plan (RMP) for Opdivo, which details the measures to be taken in order to ensure
EMA/285771/2015 Summary of the risk management plan (RMP) for Opdivo (nivolumab) This is a summary of the risk management plan (RMP) for Opdivo, which details the measures to be taken in order to ensure
MANAGEMENT OF IMMUNOTHERAPY RELATED GI AND HEPATIC ADVERSE EVENTS
 MANAGEMENT OF IMMUNOTHERAPY RELATED GI AND HEPATIC ADVERSE EVENTS Wai K. Leung Li Shu Fan Medical Foundation Professor in Gastroenterology Associate Dean (Human Capital), LKS Faculty of Medicine, University
MANAGEMENT OF IMMUNOTHERAPY RELATED GI AND HEPATIC ADVERSE EVENTS Wai K. Leung Li Shu Fan Medical Foundation Professor in Gastroenterology Associate Dean (Human Capital), LKS Faculty of Medicine, University
MANAGEMENT OF IMMUNE-RELATED SIDE EFFECTS OF IMMUNE CHECKPOINT INHIBITORS
 MANAGEMENT OF IMMUNE-RELATED SIDE EFFECTS OF IMMUNE CHECKPOINT INHIBITORS John B.A.G. Haanen MD PhD CONTENT OF THIS PRESENTATION General aspects of immune related adverse events related to immune checkpoint
MANAGEMENT OF IMMUNE-RELATED SIDE EFFECTS OF IMMUNE CHECKPOINT INHIBITORS John B.A.G. Haanen MD PhD CONTENT OF THIS PRESENTATION General aspects of immune related adverse events related to immune checkpoint
University of Texas Southwestern Medical Center Department of Internal Medicine Grand Rounds October 26, 2018
 University of Texas Southwestern Medical Center Department of Internal Medicine Grand Rounds October 26, 2018 Title: Immune Checkpoint Inhibitor related Endocrinopathies Speaker: Sadia Ali, M.D. This is
University of Texas Southwestern Medical Center Department of Internal Medicine Grand Rounds October 26, 2018 Title: Immune Checkpoint Inhibitor related Endocrinopathies Speaker: Sadia Ali, M.D. This is
Corticosteroids. Abdulmoein Al-Agha, FRCPCH Professor of Pediatric Endocrinology, King Abdulaziz University Hospital,
 Corticosteroids Abdulmoein Al-Agha, FRCPCH Professor of Pediatric Endocrinology, King Abdulaziz University Hospital, http://aagha.kau.edu.sa History 1855 Addison's disease 1856 Adrenal glands essential
Corticosteroids Abdulmoein Al-Agha, FRCPCH Professor of Pediatric Endocrinology, King Abdulaziz University Hospital, http://aagha.kau.edu.sa History 1855 Addison's disease 1856 Adrenal glands essential
PRODUCT MONOGRAPH YERVOY. ipilimumab. Intravenous Infusion, 5 mg ipilimumab / ml. 10 ml and 40 ml vials. Antineoplastic
 PRODUCT MONOGRAPH Pr YERVOY ipilimumab Intravenous Infusion, 5 mg ipilimumab / ml 10 ml and 40 ml vials Antineoplastic Bristol-Myers Squibb Canada Montreal Canada Date of Authorization: 01 August 2017
PRODUCT MONOGRAPH Pr YERVOY ipilimumab Intravenous Infusion, 5 mg ipilimumab / ml 10 ml and 40 ml vials Antineoplastic Bristol-Myers Squibb Canada Montreal Canada Date of Authorization: 01 August 2017
ADDISON S DISEASE THE FACTS YOU NEED TO KNOW
 ADDISON S DISEASE THE FACTS YOU NEED TO KNOW WHAT IS Addison's disease is a severe or total deficiency of the hormones made in the adrenal cortex, caused by its destruction. There are normally two adrenal
ADDISON S DISEASE THE FACTS YOU NEED TO KNOW WHAT IS Addison's disease is a severe or total deficiency of the hormones made in the adrenal cortex, caused by its destruction. There are normally two adrenal
Clinical Guideline. SPEG MCN Protocols Sub Group SPEG Steering Group
 Clinical Guideline SECONDARY CARE MANAGEMENT OF SUSPECTED ADRENAL CRISIS IN CHILDREN AND YOUNG PEOPLE Date of First Issue 24/01/2015 Approved 28/09/2017 Current Issue Date 16/06/2017 Review Date 01/09/2019
Clinical Guideline SECONDARY CARE MANAGEMENT OF SUSPECTED ADRENAL CRISIS IN CHILDREN AND YOUNG PEOPLE Date of First Issue 24/01/2015 Approved 28/09/2017 Current Issue Date 16/06/2017 Review Date 01/09/2019
Gemcitabine + Capecitabine (ESPAC-4 Trial)
") Gemcitabine + Capecitabine (ESPAC-4 Trial) European Study Group For Pancreatic Cancer - Trial 4. Combination versus single agent chemotherapy in resectable pancreatic ductal and ampullary cancers. ***
Gemcitabine + Capecitabine (ESPAC-4 Trial) European Study Group For Pancreatic Cancer - Trial 4. Combination versus single agent chemotherapy in resectable pancreatic ductal and ampullary cancers. ***
Sajeev Menon MD ADRENAL INSUFFICIENCY? FATIGUE? OUTLINE OBJECTIVES PATIENT 1 PATIENT 1 : CLINICAL COURSE
 ADRENAL INSUFFICIENCY? FATIGUE? Sajeev Menon MD Endocrinologist KCIM OBJECTIVES OUTLINE Review primary and adrenal insufficiency including clinical and laboratory findings To appropriately interpret the
ADRENAL INSUFFICIENCY? FATIGUE? Sajeev Menon MD Endocrinologist KCIM OBJECTIVES OUTLINE Review primary and adrenal insufficiency including clinical and laboratory findings To appropriately interpret the
Special pediatric considerations are noted when applicable, otherwise adult provisions apply.
 DRUG NAME: Avelumab SYNONYM(S): MSB0010718C 1 COMMON TRADE NAME(S): BAVENCIO CLASSIFICATION: monoclonal antibody Special pediatric considerations are noted when applicable, otherwise adult provisions apply.
DRUG NAME: Avelumab SYNONYM(S): MSB0010718C 1 COMMON TRADE NAME(S): BAVENCIO CLASSIFICATION: monoclonal antibody Special pediatric considerations are noted when applicable, otherwise adult provisions apply.
Immune-related Adverse Events (IrAEs)
") West of Scotland Cancer Network Guideline for Management of Immune-related Adverse Events Scope This guidance refers to management of immune-related adverse events caused directly by immunotherapy. Immune-related
West of Scotland Cancer Network Guideline for Management of Immune-related Adverse Events Scope This guidance refers to management of immune-related adverse events caused directly by immunotherapy. Immune-related
MANAGEMENT OF IMMUNE-RELATED GI AND LIVER TOXICITY
 MANAGEMENT OF IMMUNE-RELATED GI AND LIVER TOXICITY Alberto Fusi Charité Comprehensive Cancer Centre - Berlin St. George s University - London TAO Meeting - Cancer Toxicity Management Paris - 8th-9th December
MANAGEMENT OF IMMUNE-RELATED GI AND LIVER TOXICITY Alberto Fusi Charité Comprehensive Cancer Centre - Berlin St. George s University - London TAO Meeting - Cancer Toxicity Management Paris - 8th-9th December
CHRONIC DIARRHEA DR. PHILIP K. BLUSTEIN M.D. F.R.C.P.(C) DEFINITION: *LOOSE, WATERY STOOLS *MORE THAN 3 TIMES A DAY *FOR MORE THAN 4 WEEKS
 DEFINITION: *LOOSE, WATERY STOOLS *MORE THAN 3 TIMES A DAY *FOR MORE THAN 4 WEEKS") DR. PHILIP K. BLUSTEIN M.D. F.R.C.P.(C) 415 14 TH ST. NW. CALGARY AB T2N2A1 PHONE (403) 270-9555 FAX (403) 270-7479 CHRONIC DIARRHEA DEFINITION: *LOOSE, WATERY STOOLS *MORE THAN 3 TIMES A DAY *FOR MORE
DR. PHILIP K. BLUSTEIN M.D. F.R.C.P.(C) 415 14 TH ST. NW. CALGARY AB T2N2A1 PHONE (403) 270-9555 FAX (403) 270-7479 CHRONIC DIARRHEA DEFINITION: *LOOSE, WATERY STOOLS *MORE THAN 3 TIMES A DAY *FOR MORE
Summary of the Risk Management Plan (RMP) V. 1.6, July 2017 for BAVENCIO. Avelumab 200 mg/10 ml. Concentrate for Solution for Infusion
 V. 1.6, July 2017 for BAVENCIO. Avelumab 200 mg/10 ml. Concentrate for Solution for Infusion") Summary of the Risk Management Plan (RMP) V. 1.6, July 2017 for BAVENCIO Avelumab 200 mg/10 ml Concentrate for Solution for Infusion Marketing Authorisation Number 66380 Marketing Authorisation Holder:
Summary of the Risk Management Plan (RMP) V. 1.6, July 2017 for BAVENCIO Avelumab 200 mg/10 ml Concentrate for Solution for Infusion Marketing Authorisation Number 66380 Marketing Authorisation Holder:
PRODUCT MONOGRAPH. Pr YERVOY. Ipilimumab for injection. Intravenous Infusion, 5 mg ipilimumab / ml. 10 ml and 40 ml vials.
 PRODUCT MONOGRAPH Pr YERVOY Ipilimumab for injection Intravenous Infusion, 5 mg ipilimumab / ml 10 ml and 40 ml vials Antineoplastic Bristol-Myers Squibb Canada Montreal Canada Date of Authorization: December
PRODUCT MONOGRAPH Pr YERVOY Ipilimumab for injection Intravenous Infusion, 5 mg ipilimumab / ml 10 ml and 40 ml vials Antineoplastic Bristol-Myers Squibb Canada Montreal Canada Date of Authorization: December
NOTTINGHAM UNIVERSITY HOSPITAL NHS TRUST: Clinical Chemistry Guidelines
 Adrenocortical Insufficiency Guideline Document Information Policy Reference: Adrenocortical Insufficiency Issue: 1: Version 3 Author Job Title: Peter Prinsloo Consultant in Chemical Pathology STATUS:
Adrenocortical Insufficiency Guideline Document Information Policy Reference: Adrenocortical Insufficiency Issue: 1: Version 3 Author Job Title: Peter Prinsloo Consultant in Chemical Pathology STATUS:
Nivolumab Monotherapy 240mg -14 days
 Nivolumab Monotherapy 240mg -14 days This regimen supercedes NCCP Regimen 00349 Nivolumab Monotherapy as of May 2018 due to a change in the licensed dosing posology. INDICATIONS FOR USE: INDICATION ICD10
Nivolumab Monotherapy 240mg -14 days This regimen supercedes NCCP Regimen 00349 Nivolumab Monotherapy as of May 2018 due to a change in the licensed dosing posology. INDICATIONS FOR USE: INDICATION ICD10
Cardiff & Vale (C&V) UHB Corporate Medicines Management Group (c MMG) SHARED CARE. Drug: AZATHIOPRINE Protocol number: CV 04
 UHB Corporate Medicines Management Group (c MMG) SHARED CARE. Drug: AZATHIOPRINE Protocol number: CV 04") Cardiff & Vale (C&V) UHB Corporate Medicines Management Group (c MMG) SHARED CARE Drug: AZATHIOPRINE Protocol number: CV 04 Indication: RENAL, PANCREAS OR COMBINED RENAL PANCREAS TRANSPLANTATION LIVER
Cardiff & Vale (C&V) UHB Corporate Medicines Management Group (c MMG) SHARED CARE Drug: AZATHIOPRINE Protocol number: CV 04 Indication: RENAL, PANCREAS OR COMBINED RENAL PANCREAS TRANSPLANTATION LIVER
Cardiff & Vale (C&V) UHB Corporate Medicines Management Group (c MMG) SHARED CARE. Drug: MYCOPHENOLATE MOFETIL/SODIUM Protocol number: CV 15
 UHB Corporate Medicines Management Group (c MMG) SHARED CARE. Drug: MYCOPHENOLATE MOFETIL/SODIUM Protocol number: CV 15") Cardiff & Vale (C&V) UHB Corporate Medicines Management Group (c MMG) SHARED CARE Drug: MYCOPHENOLATE MOFETIL/SODIUM Protocol number: CV 15 Indication: RENAL, PANCREAS OR COMBINED RENAL PANCREAS TRANSPLANTATION
Cardiff & Vale (C&V) UHB Corporate Medicines Management Group (c MMG) SHARED CARE Drug: MYCOPHENOLATE MOFETIL/SODIUM Protocol number: CV 15 Indication: RENAL, PANCREAS OR COMBINED RENAL PANCREAS TRANSPLANTATION
Adverse events in immunotherapy. Ramy Ibrahim, MD Clinical VP Immuno-Oncology Global Medicine Development AstraZeneca
 Adverse events in immunotherapy Ramy Ibrahim, MD Clinical VP Immuno-Oncology Global Medicine Development AstraZeneca Unique features of immune-related Adverse Events iraes Non-specific Inflammation of
Adverse events in immunotherapy Ramy Ibrahim, MD Clinical VP Immuno-Oncology Global Medicine Development AstraZeneca Unique features of immune-related Adverse Events iraes Non-specific Inflammation of
Complications of Immunotherapy
 Complications of Immunotherapy Sarah Norskog, PharmD, BCOP Oncology Pharmacy Specialist University of Colorado Hospital Disclosures I have no relevant financial relationships with commercial interests
Complications of Immunotherapy Sarah Norskog, PharmD, BCOP Oncology Pharmacy Specialist University of Colorado Hospital Disclosures I have no relevant financial relationships with commercial interests
Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone
 Disease of the Adrenals 1 Zona Glomerulosa Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone leads to salt
Disease of the Adrenals 1 Zona Glomerulosa Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone leads to salt
Immunotherapy toxicity guidelines
 Immunotherapy toxicity guidelines These guidelines cover the management of patients who are treated with: CDLA-4 monoclonal antibody - Ipilimumab PD-1 monoclonal antibodies: Pembrolizumab & Nivolumab This
Immunotherapy toxicity guidelines These guidelines cover the management of patients who are treated with: CDLA-4 monoclonal antibody - Ipilimumab PD-1 monoclonal antibodies: Pembrolizumab & Nivolumab This
BC Cancer Protocol for Treatment of Platinum Resistant Epithelial Ovarian Cancer with Bevacizumab and PACLitaxel
 BC Cancer Protocol for Treatment of Platinum Resistant Epithelial Ovarian Cancer with Bevacizumab and PACLitaxel Protocol Code Tumour Group Contact Physician UGOOVBEVP Gynecologic Oncology Dr. Anna Tinker
BC Cancer Protocol for Treatment of Platinum Resistant Epithelial Ovarian Cancer with Bevacizumab and PACLitaxel Protocol Code Tumour Group Contact Physician UGOOVBEVP Gynecologic Oncology Dr. Anna Tinker
M0BCore Safety Profile
 M0BCore Safety Profile Active substance: Aciclovir Pharmaceutical form(s)/strength: Tablets 200, 400 or 800 mg Dispersible tablets 200, 400 or 800 mg Oral suspensions 200 mg or 400 mg per 5 ml. Freeze
M0BCore Safety Profile Active substance: Aciclovir Pharmaceutical form(s)/strength: Tablets 200, 400 or 800 mg Dispersible tablets 200, 400 or 800 mg Oral suspensions 200 mg or 400 mg per 5 ml. Freeze
Adrenal Insufficiency in Children
 Adrenal Insufficiency in Children Stephanie Hsu, MD, PhD Assistant Professor Director of Quality Improvement and Patient Safety Pediatric Endocrinology Children s Hospital Colorado and the Barbara Davis
Adrenal Insufficiency in Children Stephanie Hsu, MD, PhD Assistant Professor Director of Quality Improvement and Patient Safety Pediatric Endocrinology Children s Hospital Colorado and the Barbara Davis
COPYRIGHT 2012 THE TRANSVERSE MYELITIS ASSOCIATION. ALL RIGHTS RESERVED
 The Transverse Myelitis Association...advocating for those with acute disseminated encephalomyelitis, neuromyelitis optica, optic neuritis and transverse myelitis ACUTE DISSEMINATED ENCEPHALOMYELITIS (ADEM)
The Transverse Myelitis Association...advocating for those with acute disseminated encephalomyelitis, neuromyelitis optica, optic neuritis and transverse myelitis ACUTE DISSEMINATED ENCEPHALOMYELITIS (ADEM)
TOXICITY RELATED TO IO IN LUNG CANCER
 TOXICITY RELATED TO IO IN LUNG CANCER Dr. Jorge A. Alatorre Alexander Head of the Thoracic Oncology Clinic at Instituto Nacional de Enfermedades Respiratorias American British Cowdray Medical Center Mexico
TOXICITY RELATED TO IO IN LUNG CANCER Dr. Jorge A. Alatorre Alexander Head of the Thoracic Oncology Clinic at Instituto Nacional de Enfermedades Respiratorias American British Cowdray Medical Center Mexico
Managing immune related toxicity. Karijn Suijkerbuijk May 27 th 2017
 Managing immune related toxicity Karijn Suijkerbuijk May 27 th 2017 Disclosures Advisory role: BMS, Merck Travel support: Amgen, Novartis, Roche Whybother? Patients are dying from toxicity Eggermont ipilimumab
Managing immune related toxicity Karijn Suijkerbuijk May 27 th 2017 Disclosures Advisory role: BMS, Merck Travel support: Amgen, Novartis, Roche Whybother? Patients are dying from toxicity Eggermont ipilimumab
Urgent and Emergent Pituitary Conditions
 Urgent and Emergent Pituitary Conditions PANKAJ A. GORE, MD DIRECTOR, BRAIN AND SKULL BASE T UMOR SURGERY PROVIDENCE B R AIN AND S PINE I NSTITUTE Urgent and Emergent Pituitary Conditions Neurosurgical
Urgent and Emergent Pituitary Conditions PANKAJ A. GORE, MD DIRECTOR, BRAIN AND SKULL BASE T UMOR SURGERY PROVIDENCE B R AIN AND S PINE I NSTITUTE Urgent and Emergent Pituitary Conditions Neurosurgical
ANNEX I SUMMARY OF PRODUCT CHARACTERISTICS
 ANNEX I SUMMARY OF PRODUCT CHARACTERISTICS 1 1. NAME OF THE MEDICINAL PRODUCT YERVOY 5 mg/ml concentrate for solution for infusion 2. QUALITATIVE AND QUANTITATIVE COMPOSITION Each ml of concentrate contains
ANNEX I SUMMARY OF PRODUCT CHARACTERISTICS 1 1. NAME OF THE MEDICINAL PRODUCT YERVOY 5 mg/ml concentrate for solution for infusion 2. QUALITATIVE AND QUANTITATIVE COMPOSITION Each ml of concentrate contains
Cancer Immunotherapy: Promises and Challenges. Disclosures
 Cancer Immunotherapy: Promises and Challenges David B. Page, MD Medical Oncology PMG East Hematology & Oncology Earle A. Chiles Research Institute Portland, Oregon Disclosures Consulting: Celldex, Nektar,
Cancer Immunotherapy: Promises and Challenges David B. Page, MD Medical Oncology PMG East Hematology & Oncology Earle A. Chiles Research Institute Portland, Oregon Disclosures Consulting: Celldex, Nektar,
BC Cancer Protocol Summary for Adjuvant Therapy for Breast Cancer Using Weekly PACLitaxel and Trastuzumab (HERCEPTIN)
") BC Cancer Protocol Summary for Adjuvant Therapy for Breast Cancer Using Weekly PACLitaxel and Trastuzumab (HERCEPTIN) Protocol Code: Tumour Group: Contact Physician: UBRAJTTW Breast Dr. Angela Chan ELIGIBILITY:
BC Cancer Protocol Summary for Adjuvant Therapy for Breast Cancer Using Weekly PACLitaxel and Trastuzumab (HERCEPTIN) Protocol Code: Tumour Group: Contact Physician: UBRAJTTW Breast Dr. Angela Chan ELIGIBILITY:
DERBY-BURTON LOCAL CANCER NETWORK FILENAME Peruse.DOC CONTROLLED DOC NO: CCPG R29
 Pertuzumab + Trastuzumab + Docetaxel (Peruse study) A Multicenter, open-label, single arm study of Pertuzumab in combination with Trastuzumab and a Taxane in first-line treatment of patients with HER2-positive
Pertuzumab + Trastuzumab + Docetaxel (Peruse study) A Multicenter, open-label, single arm study of Pertuzumab in combination with Trastuzumab and a Taxane in first-line treatment of patients with HER2-positive
Immunotherapy for Melanoma. Michael Postow, MD Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center
 Immunotherapy for Melanoma Michael Postow, MD Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center Conflicts of Interest Bristol-Myers Squibb: -Research support -Participated
Immunotherapy for Melanoma Michael Postow, MD Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center Conflicts of Interest Bristol-Myers Squibb: -Research support -Participated
ICLIO Webinar: Immuno-Oncology: From a Community Radiologist Perspective Michael J. DeLeo III, MD
 ICLIO Webinar: Immuno-Oncology: From a Community Radiologist Perspective Michael J. DeLeo III, MD Foundation Medical Partners Southern New Hampshire Health System December 1, 2016 accc-iclio.org Overview
ICLIO Webinar: Immuno-Oncology: From a Community Radiologist Perspective Michael J. DeLeo III, MD Foundation Medical Partners Southern New Hampshire Health System December 1, 2016 accc-iclio.org Overview
NCCP Chemotherapy Regimen. Brentuximab vedotin Monotherapy
 Brentuximab INDICATIONS FOR USE: INDICATION ICD10 Regimen Code *Reimbursement Status Treatment of adult patients with relapsed or refractory CD30+ Hodgkin lymphoma (HL): Following autologous stem cell
Brentuximab INDICATIONS FOR USE: INDICATION ICD10 Regimen Code *Reimbursement Status Treatment of adult patients with relapsed or refractory CD30+ Hodgkin lymphoma (HL): Following autologous stem cell
Corticosteroids. Veterinary Pharmacology Endocrine System. University of Tehran Faculty of Veterinary Medicine Academic Year
 Veterinary Pharmacology Endocrine System Corticosteroids University of Tehran Faculty of Veterinary Medicine Academic Year 2008-9 Goudarz Sadeghi, DVM, PhD, DSc Associate Professor of Pharmacology Introduction
Veterinary Pharmacology Endocrine System Corticosteroids University of Tehran Faculty of Veterinary Medicine Academic Year 2008-9 Goudarz Sadeghi, DVM, PhD, DSc Associate Professor of Pharmacology Introduction
Safety Immune Related Adverse Events (irae) Focus on NSCLC Aaron Hansen, BSc, MBBS, FRACP
 Focus on NSCLC Aaron Hansen, BSc, MBBS, FRACP") Safety Immune Related Adverse Events (irae) Focus on NSCLC Aaron Hansen, BSc, MBBS, FRACP Division of Medical Oncology and Hematology Bras Drug Development Program Princess Margaret Cancer Centre, Toronto,
Safety Immune Related Adverse Events (irae) Focus on NSCLC Aaron Hansen, BSc, MBBS, FRACP Division of Medical Oncology and Hematology Bras Drug Development Program Princess Margaret Cancer Centre, Toronto,
Pituitary Apoplexy. Updated: April 22, 2018 CLINICAL RECOGNITION
 Pituitary Apoplexy Zeina C Hannoush, MD. Assistant Professor of Clinical Medicine. Division of Endocrinology, Diabetes and Metabolism. University of Miami, Miller School of Medicine. Roy E Weiss, MD, PhD,
Pituitary Apoplexy Zeina C Hannoush, MD. Assistant Professor of Clinical Medicine. Division of Endocrinology, Diabetes and Metabolism. University of Miami, Miller School of Medicine. Roy E Weiss, MD, PhD,
Cycle 1 PERTuzumab (day 1) and trastuzumab (day 2) loading doses: Drug Dose BC Cancer Administration Guideline
 and trastuzumab (day 2) loading doses: Drug Dose BC Cancer Administration Guideline") BC Cancer Protocol Summary for Palliative Therapy for Metastatic Breast Cancer Using PERTuzumab, Trastuzumab (HERCEPTIN), and PACLItaxel as First-Line Treatment for Advanced Breast Cancer Protocol Code:
BC Cancer Protocol Summary for Palliative Therapy for Metastatic Breast Cancer Using PERTuzumab, Trastuzumab (HERCEPTIN), and PACLItaxel as First-Line Treatment for Advanced Breast Cancer Protocol Code:
Azathioprine toxicity criteria and severity descriptors for the listing of biological agents for rheumatoid arthritis on the PBS
 Azathioprine toxicity criteria and severity descriptors for the listing of biological agents for rheumatoid arthritis on the PBS Only valid for adult patients Azathioprine must be at a dose of at least
Azathioprine toxicity criteria and severity descriptors for the listing of biological agents for rheumatoid arthritis on the PBS Only valid for adult patients Azathioprine must be at a dose of at least
Critical illness and endocrinology. ICU Fellowship Training Radboudumc
 Critical illness and endocrinology ICU Fellowship Training Radboudumc Critical illness Ultimate form of severe physical stress Generates an orchestrated endocrine response to provide the energy for fight
Critical illness and endocrinology ICU Fellowship Training Radboudumc Critical illness Ultimate form of severe physical stress Generates an orchestrated endocrine response to provide the energy for fight
Adrenal Gland Disorders
 1 Adrenal Gland Disorders Adrenal cortex steroid hormones (corticosteroids) 1. Glucocorticoids Regulate metabolism and blood glucose Critical to physiologic stress response 2. Mineralocorticoids Regulate
1 Adrenal Gland Disorders Adrenal cortex steroid hormones (corticosteroids) 1. Glucocorticoids Regulate metabolism and blood glucose Critical to physiologic stress response 2. Mineralocorticoids Regulate
ABACAVIR HYPERSENSITIVITY REACTION
 ABACAVIR HYPERSENSITIVITY REACTION Key Risk Minimisation Points: Abacavir Hypersensitivity Reaction (HSR) Abacavir is associated with a risk for hypersensitivity reactions (HSR) characterised by fever
ABACAVIR HYPERSENSITIVITY REACTION Key Risk Minimisation Points: Abacavir Hypersensitivity Reaction (HSR) Abacavir is associated with a risk for hypersensitivity reactions (HSR) characterised by fever
RAVE DATA ENTRY GUIDELINES S1400 & SUB-STUDIES. Protocol Ver. 1/8/18
 RAVE DATA ENTRY GUIDELINES S1400 & SUB-STUDIES Protocol Ver. 1/8/18 S1400 Forms Case Report Forms Onstudy: Patient & Disease Description Form 3 Onstudy: Prior Treatment Form 4 Source Documentation: Baseline
RAVE DATA ENTRY GUIDELINES S1400 & SUB-STUDIES Protocol Ver. 1/8/18 S1400 Forms Case Report Forms Onstudy: Patient & Disease Description Form 3 Onstudy: Prior Treatment Form 4 Source Documentation: Baseline
NEW CONCEPTS IN CROHN S DISEASE GLENDON BURRESS, MD PEDIATRIC GASTROENTEROLOGY ROCKFORD, IL
 NEW CONCEPTS IN CROHN S DISEASE GLENDON BURRESS, MD PEDIATRIC GASTROENTEROLOGY ROCKFORD, IL CROHN S DISEASE Chronic disease of uncertain etiology Etiology- genetic, environmental, and infectious Transmural
NEW CONCEPTS IN CROHN S DISEASE GLENDON BURRESS, MD PEDIATRIC GASTROENTEROLOGY ROCKFORD, IL CROHN S DISEASE Chronic disease of uncertain etiology Etiology- genetic, environmental, and infectious Transmural
Clostridium difficile Infection (CDI) Management Guideline
 Management Guideline") Clostridium difficile Infection (CDI) Management Guideline Do not test all patients with loose or watery stools for CDI o CDI is responsible for
Clostridium difficile Infection (CDI) Management Guideline Do not test all patients with loose or watery stools for CDI o CDI is responsible for
Evolving Treatment Strategies in the Management of Metastatic Melanoma: Novel Therapies for Improved Patient Outcomes. Disclosures
 Evolving Treatment Strategies in the Management of Metastatic Melanoma: Novel Therapies for Improved Patient Outcomes Fall Managed Care Forum November 11, 2016 Matthew Taylor, M.D. Disclosures Consulting/Advisory
Evolving Treatment Strategies in the Management of Metastatic Melanoma: Novel Therapies for Improved Patient Outcomes Fall Managed Care Forum November 11, 2016 Matthew Taylor, M.D. Disclosures Consulting/Advisory
Durvalumab (previously known as MEDI 4736) Maintenance (Arm A3) PLATFORM study
 Maintenance (Arm A3) PLATFORM study") Durvalumab (previously known as MEDI 4736) Maintenance (Arm A3) PLATFORM study PLAnning Treatment For Oesophago-gastric cancer: a Randomised Maintenance therapy trial. ***See Protocol for further details***
Durvalumab (previously known as MEDI 4736) Maintenance (Arm A3) PLATFORM study PLAnning Treatment For Oesophago-gastric cancer: a Randomised Maintenance therapy trial. ***See Protocol for further details***
DERBY-BURTON CANCER NETWORK CONTROLLED DOC NO:
 OBINUTUZUMAB+CHLORAMBUCIL Regimen RDH; Day 1 and 2 Dose to be given on Ward Available for Routine Use in Burton in-patient Derby in-patient Burton day-case Derby day-case Burton community Derby community
OBINUTUZUMAB+CHLORAMBUCIL Regimen RDH; Day 1 and 2 Dose to be given on Ward Available for Routine Use in Burton in-patient Derby in-patient Burton day-case Derby day-case Burton community Derby community
Pearls in Child Neurology. Edgard Andrade, MD, FAAP Assistant Professor University of Florida
 Pearls in Child Neurology Edgard Andrade, MD, FAAP Assistant Professor University of Florida Outline 1. Autism 2. Bell s Palsy 3. First unprovoked seizure in children 4. Migraine headache Objectives 1.
Pearls in Child Neurology Edgard Andrade, MD, FAAP Assistant Professor University of Florida Outline 1. Autism 2. Bell s Palsy 3. First unprovoked seizure in children 4. Migraine headache Objectives 1.
INFLAMMATORY BOWEL DISEASE
 1. Medical Condition INFLAMMATORY BOWEL DISEASE (IBD) specifically includes Crohn s disease (CD) and ulcerative colitis (UC) but also includes IBD unclassified (IBDu), seen in about 10% of cases. These
1. Medical Condition INFLAMMATORY BOWEL DISEASE (IBD) specifically includes Crohn s disease (CD) and ulcerative colitis (UC) but also includes IBD unclassified (IBDu), seen in about 10% of cases. These