Sajeev Menon MD ADRENAL INSUFFICIENCY? FATIGUE? OUTLINE OBJECTIVES PATIENT 1 PATIENT 1 : CLINICAL COURSE
|
|
|
- Cecily Freeman
- 5 years ago
- Views:
Transcription

1 ADRENAL INSUFFICIENCY? FATIGUE? Sajeev Menon MD Endocrinologist KCIM OBJECTIVES OUTLINE Review primary and adrenal insufficiency including clinical and laboratory findings To appropriately interpret the results of basal and dynamic tests of adrenal function. Discuss the treatment of adrenal insufficiency including new options List the drugs that interfere with the HPA axis and cortisol metabolism Discuss Relative Adrenal Insufficiency and dispel the myth of Adrenal Fatigue Four case studies in the inpatient and outpatient settings - which address the learning objectives. PATIENT 1 PATIENT 1 : CLINICAL COURSE 17 yr old Caucasian male Collapses in London in 1947 Hypotension, Na 129 meq/l, K 4.9 meq/l Hx of diarrhea and weight loss Evaluated at Mayo clinic, diagnosed to have Addison s disease He has one year to live Deoxycorticosterone acetate (DOCA) pellets under his skin every 3 months : introduction of cortisone (Kendall/Hench at Mayo Clinic) 1954: Archives of Surgery report after back surgery 1955: BMR -15, compatible with hypothyroidism. Younger sister develops Addison s disease 1963: Dies of GSW. Post mortem: no adrenal tissue 1





2 SYMPTOMS OF ADRENAL INSUFFICIENCY HYPERPIGMENTATION Weakness, fatigue 100% Anorexia 100% Nausea 86% Vomiting 75% Abdominal Pain 31% Salt Craving 16% Postural dizziness 12% Muscle or joint pain 6-12 % 2
 Hyperkalemia 64% (low aldosterone) Hypercalcemia 6% Azotemia 55% Mild anemia 40% Eosinophilia 17% Lymphocytosis Varies Cosyntropin")
 30 mg/kg p.o at 2300. Labs 0800.")
3 HYPERPIGMENTATION BIOCHEMICAL DIAGNOSIS OF PAI Paired cortisol and ACTH Serum cortisol < 5 mcg/dl Plasma ACTH >2 x upper normal Elevated renin/pra Low DHEA / DHEAS PAI: OTHER TYPICAL FINDINGS ADDITIONAL DIAGNOSTIC TESTS Hyponatremia 88% (low cortisol) Hyperkalemia 64% (low aldosterone) Hypercalcemia 6% Azotemia 55% Mild anemia 40% Eosinophilia 17% Lymphocytosis Varies Cosyntropin Stimulation Test mcg ACTH IM or IV min: >18-20 mcg/dl Normal Low dose Cosyntropin Test (1 mcg) - Not recommended ADDITIONAL DIAGNOSTIC TESTS ANTIBODIES Insulin Tolerance Test mcg/kg Regular insulin IV bolus Glucose < 40 mg/dl and Cortisol > 18 mcg/dl Metyrapone test (11 beta hydroxylase inhibitor) 30 mg/kg p.o at Labs Deoxycortisol > 7 mcg/dl - Normal - Cortisol < 5 mcg / dl - Required to fail 3


4 DIAGNOSTIC ALGORITHM TREATMENT OF ADRENAL INSUFFICIENCY Adrenal crisis is a life threatening emergency and requires immediate treatment. The goal of treatment is correction of hypotension and reversal of electrolyte abnormalities and cortisol deficiency. IVF (NS), IV HCN Mineralocorticoid administration is not necessary in the acute setting. HCN in 2-3 divided doses is the drug of choice for management of chronic primary adrenal insufficiency. TREATMENT OF ADRENAL INSUFFICIENCY TREATMENT OF ADRENAL INSUFFICIENCY Chronic management invariably requires Fludrocortisone. Adjust the dose to lower PRA to the upper normal range. ACTH measurement is usually not helpful or necessary. UFC is not completely reliable to assist in HCN dose titration. DHEA maybe helpful is some women. The adrenal glands only produce 8-12 mg (6-7 mg/sq m/day) of cortisol daily. Doses of HCN mg daily in divided doses is adequate in most patients. There is no physiologic prednisone dose. SERUM CORTISOL PROFILE : PLENADREN VS HC SUBCUTANEOUS PUMP THERAPY 4

 PATIENT 2 PATIENT 2 : NEXT BEST TEST? Labs : Normal CBC and CMP.")

5 PATIENT 2 SALIVARY CORTISOL GRAPH 20 yr old Caucasian male Seems quite nervous Has palpitations, anxiety with panic attacks, fatigue Normal exam and BP. Weight has been stable. BMI 22. Integrative Family Wellness Center : Salivary cortisol profile showed adrenal fatigue. Treated with adrenal support (no active steroids listed) PATIENT 2 PATIENT 2 : NEXT BEST TEST? Labs : Normal CBC and CMP. Morning serum cortisol : 1.4 mcg/dl CST (250 mcg IV) Cortisol increased from 1.8 to 11.6 ACTH at baseline was < 5 pg/ml FT4, IGF-1, TSH, PL and total testosterone - WNL Pituitary MRI was done and found to be normal. Subsequently other tests were considered: -Long chain fatty acid profile -21 hydroxylase antibodies -Synthetic glucocorticoid screen -17 hydroxyprogesterone 5
6 PATIENT 2 : CLINICAL COURSE A few days later, his father calls to inform that patient was found to be abusing Buprenorphine. OPIOID INDUCED ADRENAL INSUFFICIENCY Heroin addicts (60-70%) have impaired cortisol response to stimulation. Methadone attenuates ACTH / Cortisol response to Naloxone. Clinically significant adrenal insufficiency / crisis seems rare. OR is it? There are 17,000 deaths annually from narcotic overdose. DRUG INDUCED ADRENAL INSUFFICIENCY Corticosteroids and progesterone (medroxy progesterone) Opioids Adrenostatic/lytic and GR antagonist Ipilimumab (CTLA-4 Mab, can cause hypophysitis) Psychotropic drugs: benzodiazepine, atypical antipsychotics etc PATIENT 3 PATIENT 3 : LAB TESTS 75 yr old, diabetic gentleman Admitted with lobar pneumonia a week ago Developed hypotension and oliguria 36 hours ago Transferred to ICU Intubated, broad spectrum ABX, IVF, Insulin gtt Glucose 128 mg/dl Na 133 meq/l K 3.7 meq/l Cl 94 meq/l HCO3 28 meq/l Ca 7.9 mg/dl Albumin 1.9 mg/dl 6

7 PATIENT 3 : LAB TESTS RELATIVE ADRENAL INSUFFICIENCY Serum cortisol 11 mcg/dl at baseline and 17.5 mcg/dl after stimulation. Aldosterone 3.5 ng/dl PRA 12 ng/ml/h ACTH 17 pg/ml This concept was based on an initial report by Rothwell in 1991 Definition: Incremental cortisol response to Cosyntropin < 9 mcg/dl Important prognostic feature in septic shock Subsequent reports used the same definition Used to define need for HC therapy (Annane et al; JAMA 288:862;2002) (Serious limitation most patients responding to HCN had received Etomidate) Rapid increase in similar publications *Arafah B; JCEM : 91: 3725 PATIENT 3 : WHAT IS THE BEST NEXT STEP? 1. Administer hydrocortisone and fludrocortisone 2. Initiate high dose dexamethasone MEASURE FREE CORTISOL Measuring free cortisol in critical illness may identify patients with true adrenal insufficiency and distinguish them from patients with low cortisol related to decreased binding proteins. 3. Measure free cortisol 4. Obtain pituitary MRI However this test is not available in most labs and even if available might not be reported back for a few days. Raff H, et al. Endocrine 34: 68-74, 2008 SM1 FREE CORTISOL FREE CORTISOL LEVELS DURING CRITICAL ILLNESS PREDICT MORTALITY Free cortisol levels during critical illness predict mortality 7
8 Slide 42 SM1 Sajeev, 10/15/2016
9 PATIENT 3 : CORTICUS TRIAL Although ACTH levels actually decline, decreased cortisol clearance and slightly increased production rates sustain cortisol levels during critical illness and may require a dose adaptation when HCN treatment is considered. Despite elevated PRA, low aldosterone is seen in 20% of critically ill patients. DHEA levels may also be subnormal. 499 ICU patients with septic shock were randomized. 233 (47%) had abnormal CST, defined as <9 mcg/dl increase in total cortisol. (30 increasing to 32 was considered abnormal and 28 increasing to 46 was considered normal) 125 received HCN for 11 days. 108 received placebo. There was no decrease in mortality with HCN. *Sprung CL et al NEJM 2008: 358: CORTICUS TRIAL Hydrocortisone reversed shock more quickly BUT caused more superinfection and new sepsis / shock. It had no impact on mortality or length of stay Cosyntropin testing did not predict responsiveness to HC Despite that study, some intensivists continue to use the term : relative adrenal insufficiency. RELATIVE ADRENAL INSUFFICIENCY IN CRITICAL ILLNESS Weak scientific evidence Iatrogenic steroids, propofol, opioids, psychotropic meds Total cortisol is misleading due to low CBG Steroid therapy is unhelpful High steroid levels = worse prognosis The adrenal glands never fatigue! RELATIVE ADRENAL INSUFFICIENCY IN CRITICAL ILLNESS HPA axis is generally highly activated; not as well apparent from measurements of serum total cortisol levels. Secretion of other ACTH dependent steroids (DHEA) is also increased. When HCN is used, the therapeutic response is not typical of that in adrenal insufficiency. NEW ONSET ADRENAL INSUFFICIENCY IN THE ICU It does exist BUT.. NOT AS CURRENTLY DEFINED It is a rare event Can be iatrogenic (e.g. etomidate) Should be considered for patients at risk. 8
10 DIAGNOSIS OF ADRENAL INSUFFICIENCY DURING CRITICAL ILLNESS DIAGNOSIS OF ADRENAL INSUFFICIENCY DURING CRITICAL ILLNESS Diagnosis is difficult Always suspect it in patients at risk Always look for a cause Consider limitations of tests (serum cortisol) Can rely on random serum cortisol as long as binding protein abnormalities are taken into account Take advantage of ACTH dependent steroids (DHEAS). Cosyntropin test is NOT necessary Serum free cortisol is desirable but not readily available Can rely on random serum total cortisol Recommendations are based on data in nearly 300 patients DIAGNOSIS OF ADRENAL INSUFFICIENCY DURING CRITICAL ILLNESS DIAGNOSIS OF ADRENAL INSUFFICIENCY DURING CRITICAL ILLNESS In the absence of binding protein abnormalities: Expected total cortisol is often >15 mcg/dl If cortisol is 10-15, consider the diagnosis If cortisol is < 10, diagnosis is likely. If unclear, can treat and diagnose later When binding proteins are low: Cortisol should be at least > 11 If cortisol is 8-11, consider the diagnosis If level is <8, diagnosis is likely. TREATMENT OF ADRENAL INSUFFICIENCY IN CRITICAL ILLNESS Principles of therapy Provide appropriate doses of glucocorticoids for the critical illness. No definitive studies regarding dosage Lower doses maybe effective based on data in critically ill patients with AI Recent data do show decreased cortisol clearance during critical illness. At times high doses may be needed to treat associated inflammatory processes. TREATMENT OF ADRENAL INSUFFICIENCY IN CRITICALLY ILL PATIENTS WITH KNOWN OR NEWLY DIAGNOSED ADRENAL INSUFFICIENCY CRITICAL ILLNESS WITHOUT SHOCK: Use HCN 25 mg Q 6 Hrs Taper as clinically indicated In patients with primary disease, add Fludrocortisone when total daily dose of HCN is < 50 mg/day CRITICAL ILLNESS WITH SHOCK: Use HCN 50 mg Q 6 Hrs Taper as clinically indicated No need for Fludrocortisone 9



11 HCN 25 mg IV every 6 hrs USE OF GLUCOCORTICOIDS IN PATIENTS WITH SEPTIC SHOCK BUT WITHOUT ADRENAL INSUFFICIENCY Data is limited. It is possible that HCN might benefit a small number of patients with septic shock and severe inflammatory response. GC therapy in this setting may represent pharmacologic therapy of an inflammatory disease. There are no available tests that can identify patients who might benefit from this therapy. Patients who received Etomidate should be treated with HCN for at least 24 hours. ADRENAL FUNCTION DURING CHRONIC STRESS AIDS patients PTSD Chronic Fatigue Syndrome PATIENT 4 Patient is a 46 year old Caucasian male He has a high stress job. Travels a lot. Doesn t sleep well. Reports anxiety, palpitations, near syncope and dizziness. Medical history is negative for any significant illness. Does not take any meds. Vitals: P 80 BP 130/74 BMI 29.6 Normal physical exam. Referred to Integrative Family Wellness Center 10

12 11

13 I HAVE ADRENAL INSUFFICIENCY SUMMARY: LIST OF DO S When someone tells you that. he or she probably does not! 99.9% is iatrogenic 100% should have weight loss Should have a Lazarean response to treatment. There is no such thing as Adrenal Fatigue. Corticosteroids dull pain. Do suspect exogenous GC Do suspect Narcotics Do determine etiology of primary adrenal insufficiency Do check Albumin in the ICU setting Do measure DHEAS for confirmation Do consider adrenal insufficiency for unexplained hyponatremia SUMMARY: LIST OF DON TS Don t accept adrenal fatigue as a diagnosis Don t diagnose Relative Adrenal Insufficiency Don t recommend CST in ICU Don t forget narcotics and GC Don t overtreat chronically Don t forget Fludrocortisone Don t follow ACTH in primary adrenal insufficiency Thank you! 12
Lawrence S. Kirschner, MD, PhD Professor of Medicine
 Adrenal Insufficiency: Current Practice 2012 Lawrence S. Kirschner, MD, PhD Professor of Medicine Division of Endocrinology, Diabetes, and Metabolism The Ohio State University s Wexner Medical Center Overview
Adrenal Insufficiency: Current Practice 2012 Lawrence S. Kirschner, MD, PhD Professor of Medicine Division of Endocrinology, Diabetes, and Metabolism The Ohio State University s Wexner Medical Center Overview
Assessing Adrenal Function in Ill, Hospitalized Patients. Bruce Redmon, MD Division of Endocrinology, Diabetes and Metabolism
 Assessing Adrenal Function in Ill, Hospitalized Patients Bruce Redmon, MD Division of Endocrinology, Diabetes and Metabolism Disclosures Very surprised when I received an email two weeks ago disclosing
Assessing Adrenal Function in Ill, Hospitalized Patients Bruce Redmon, MD Division of Endocrinology, Diabetes and Metabolism Disclosures Very surprised when I received an email two weeks ago disclosing
Subclinical Problems in the ICU:
 Subclinical Problems in the ICU: Corticosteroid Insufficiency C. S. Cutillar, M.D., FPCP, FPSEM Associate Professor Cebu Institute of Medicine H-P-A Axis during Critical Illness CRH ACTH H-P-A Axis during
Subclinical Problems in the ICU: Corticosteroid Insufficiency C. S. Cutillar, M.D., FPCP, FPSEM Associate Professor Cebu Institute of Medicine H-P-A Axis during Critical Illness CRH ACTH H-P-A Axis during
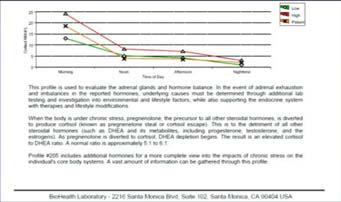
The endocrine system is made up of a complex group of glands that secrete hormones.
 1 10. Endocrinology I MEDCHEM 535 Diagnostic Medicinal Chemistry Endocrinology The endocrine system is made up of a complex group of glands that secrete hormones. These hormones control reproduction, metabolism,
1 10. Endocrinology I MEDCHEM 535 Diagnostic Medicinal Chemistry Endocrinology The endocrine system is made up of a complex group of glands that secrete hormones. These hormones control reproduction, metabolism,
Adrenal Insufficiency
 Adrenal Insufficiency Normal adrenal physiology Clinical features, Laboratory findings Common causes of primary adrenal insufficiency Evaluation of suspected adrenal insufficiency Acute and chronic management
Adrenal Insufficiency Normal adrenal physiology Clinical features, Laboratory findings Common causes of primary adrenal insufficiency Evaluation of suspected adrenal insufficiency Acute and chronic management
Endocrine and Metabolic Complications in the ICU
 Endocrine and Metabolic Complications in the ICU Linda Liu, M.D. Associate Professor UCSF Department of Anesthesia UC SF 1 New Progress Discovery of complex neuro-endocrine adaptation to critical illness
Endocrine and Metabolic Complications in the ICU Linda Liu, M.D. Associate Professor UCSF Department of Anesthesia UC SF 1 New Progress Discovery of complex neuro-endocrine adaptation to critical illness
Adrenal Insufficiency During Pregnancy
 Disclosures Adrenal Insufficiency During Pregnancy Research funding from Diurnal Limited via NIH CRADA mechanism Deborah P. Merke, M.D., M.S. Bethesda, MD Outline Primary Adrenal Insufficiency Physiological
Disclosures Adrenal Insufficiency During Pregnancy Research funding from Diurnal Limited via NIH CRADA mechanism Deborah P. Merke, M.D., M.S. Bethesda, MD Outline Primary Adrenal Insufficiency Physiological
Clinical Guideline. SPEG MCN Protocols Sub Group SPEG Steering Group
 Clinical Guideline SECONDARY CARE MANAGEMENT OF SUSPECTED ADRENAL CRISIS IN CHILDREN AND YOUNG PEOPLE Date of First Issue 24/01/2015 Approved 28/09/2017 Current Issue Date 16/06/2017 Review Date 01/09/2019
Clinical Guideline SECONDARY CARE MANAGEMENT OF SUSPECTED ADRENAL CRISIS IN CHILDREN AND YOUNG PEOPLE Date of First Issue 24/01/2015 Approved 28/09/2017 Current Issue Date 16/06/2017 Review Date 01/09/2019
58 Year-old Male with Alcoholic Cirrhosis Presents with Hyponatremia. Jess Hwang 11/8/12
 58 Year-old Male with Alcoholic Cirrhosis Presents with Hyponatremia Jess Hwang 11/8/12 HPI Fluid leaking from umbilical hernia secondary to his ascites Went to OR for drain placement which was complicated
58 Year-old Male with Alcoholic Cirrhosis Presents with Hyponatremia Jess Hwang 11/8/12 HPI Fluid leaking from umbilical hernia secondary to his ascites Went to OR for drain placement which was complicated
Objectives. Pathophysiology of Steroids. Question 1. Pathophysiology 3/1/2010. Steroids in Septic Shock: An Update
 Objectives : An Update Michael W. Perry PharmD, BCPS PGY2 Critical Care Resident Palmetto Health Richland Hospital Review the history of steroids in sepsis Summarize the current guidelines for steroids
Objectives : An Update Michael W. Perry PharmD, BCPS PGY2 Critical Care Resident Palmetto Health Richland Hospital Review the history of steroids in sepsis Summarize the current guidelines for steroids
How to Recognize Adrenal Disease
 How to Recognize Adrenal Disease CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi
How to Recognize Adrenal Disease CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi
Outline. Adrenal Insufficiency The Real & The Mythical. Primary vs Secondary
 Outline Adrenal Insufficiency The Real & The Mythical Leslie Eiland, MD Assistant Professor of Medicine Medical Director, Endocrine Telehealth Program Division of Diabetes, Endocrinology & Metabolism Adrenal
Outline Adrenal Insufficiency The Real & The Mythical Leslie Eiland, MD Assistant Professor of Medicine Medical Director, Endocrine Telehealth Program Division of Diabetes, Endocrinology & Metabolism Adrenal
Adrenal insufficiency 25/09/57
 Adrenal insufficiency นายแพทย อ ดมศ กด เล ศส ทธ พร โรงพยาบาลมหาราชนครราชส มา 25/09/57 Adrenal insufficiency Cause Primary VS secondary Acute VS Chronic Diagnosis Critically ill VS non-critically ill Treatment
Adrenal insufficiency นายแพทย อ ดมศ กด เล ศส ทธ พร โรงพยาบาลมหาราชนครราชส มา 25/09/57 Adrenal insufficiency Cause Primary VS secondary Acute VS Chronic Diagnosis Critically ill VS non-critically ill Treatment
Pituitary Gland Disorders
 Pituitary Gland Disorders 1 2 (GH-RH) (CRH) (TRH) (TRH) (GTRH) (GTRH) 3 Classification of pituitary disorders: 1. Hypersecretory diseases: a. Acromegaly and gigantism: Usually caused by (GH)-secreting
Pituitary Gland Disorders 1 2 (GH-RH) (CRH) (TRH) (TRH) (GTRH) (GTRH) 3 Classification of pituitary disorders: 1. Hypersecretory diseases: a. Acromegaly and gigantism: Usually caused by (GH)-secreting
Endocrine Crises. Fred Pieracci, MD, MPH TACS Fellow
 Endocrine Crises Fred Pieracci, MD, MPH TACS Fellow 4.14.14 Endocrine Crises Rare Highly lethal Elusive Easily treatable 1. Thyroid 1. Thyroid storm 2. Myxedema coma Outline 2. Parathyroid: 1. Severe hypercalcemia
Endocrine Crises Fred Pieracci, MD, MPH TACS Fellow 4.14.14 Endocrine Crises Rare Highly lethal Elusive Easily treatable 1. Thyroid 1. Thyroid storm 2. Myxedema coma Outline 2. Parathyroid: 1. Severe hypercalcemia
Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill
 Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill Joe Palumbo PGY-2 Critical Care Pharmacy Resident Buffalo General Medical Center Disclosures
Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill Joe Palumbo PGY-2 Critical Care Pharmacy Resident Buffalo General Medical Center Disclosures
Diseases of the Adrenal gland
 Diseases of the Adrenal gland Adrenal insufficiency Cushing disease vs syndrome Pheochromocytoma Hyperaldostronism What are the layers of the adrenal gland?? And what does each layer produce?? What are
Diseases of the Adrenal gland Adrenal insufficiency Cushing disease vs syndrome Pheochromocytoma Hyperaldostronism What are the layers of the adrenal gland?? And what does each layer produce?? What are
Adrenal Disorders for the USMLE, Step One: Abnormalities of the Fasciculata: Hypocortisolism
 Adrenal Disorders for the USMLE, Step One: Abnormalities of the Fasciculata: Hypocortisolism Howard Sachs, MD Patients Course, 2017 Associate Professor of Clinical Medicine UMass Medical School Manifestations
Adrenal Disorders for the USMLE, Step One: Abnormalities of the Fasciculata: Hypocortisolism Howard Sachs, MD Patients Course, 2017 Associate Professor of Clinical Medicine UMass Medical School Manifestations
Adrenal Gland Disorders
 1 Adrenal Gland Disorders Adrenal cortex steroid hormones (corticosteroids) 1. Glucocorticoids Regulate metabolism and blood glucose Critical to physiologic stress response 2. Mineralocorticoids Regulate
1 Adrenal Gland Disorders Adrenal cortex steroid hormones (corticosteroids) 1. Glucocorticoids Regulate metabolism and blood glucose Critical to physiologic stress response 2. Mineralocorticoids Regulate
Recommendations differ slightly in defining a suppressed patient, but general guidelines are below (Table 1):
:") PJ Nicholoff Steroid Protocol Background/Assessment Normal basal secretion of cortisol from the adrenal gland is approximately 5-7 mg/m2/day or 8-10 mg/day for adults. This amount increases during minor
PJ Nicholoff Steroid Protocol Background/Assessment Normal basal secretion of cortisol from the adrenal gland is approximately 5-7 mg/m2/day or 8-10 mg/day for adults. This amount increases during minor
ADDISON S DISEASE THE FACTS YOU NEED TO KNOW
 ADDISON S DISEASE THE FACTS YOU NEED TO KNOW WHAT IS Addison's disease is a severe or total deficiency of the hormones made in the adrenal cortex, caused by its destruction. There are normally two adrenal
ADDISON S DISEASE THE FACTS YOU NEED TO KNOW WHAT IS Addison's disease is a severe or total deficiency of the hormones made in the adrenal cortex, caused by its destruction. There are normally two adrenal
Running head: THE OPTIMAL TREATMENT FOR ADDISON S DISEASE
 Running head: THE OPTIMAL TREATMENT FOR ADDISON S DISEASE 1 Kelly Wetmore Merrimack College 2 Introduction Addison s disease is a rare autoimmune disorder caused by the body s destruction of its own adrenal
Running head: THE OPTIMAL TREATMENT FOR ADDISON S DISEASE 1 Kelly Wetmore Merrimack College 2 Introduction Addison s disease is a rare autoimmune disorder caused by the body s destruction of its own adrenal
Critical illness and endocrinology. ICU Fellowship Training Radboudumc
 Critical illness and endocrinology ICU Fellowship Training Radboudumc Critical illness Ultimate form of severe physical stress Generates an orchestrated endocrine response to provide the energy for fight
Critical illness and endocrinology ICU Fellowship Training Radboudumc Critical illness Ultimate form of severe physical stress Generates an orchestrated endocrine response to provide the energy for fight
Evaluation and Management of Pituitary Failure. Dr S. Ali Imran MBBS, FRCP (Edin), FRCPC Professor of Medicine Dalhousie University, Halifax, NS
, FRCPC Professor of Medicine Dalhousie University, Halifax, NS") Evaluation and Management of Pituitary Failure Dr S. Ali Imran MBBS, FRCP (Edin), FRCPC Professor of Medicine Dalhousie University, Halifax, NS Conflict of Interest None Objectives Diagnostic approach
Evaluation and Management of Pituitary Failure Dr S. Ali Imran MBBS, FRCP (Edin), FRCPC Professor of Medicine Dalhousie University, Halifax, NS Conflict of Interest None Objectives Diagnostic approach
Managing Addison s Disease
 Managing Addison s Disease Dr Charles R Buchanan Consultant Paediatric Endocrinologist Kings College Hospital, London Thomas Addison 1793-1860 Guy s Hospial Described Symptoms 1855 My experience 25 years
Managing Addison s Disease Dr Charles R Buchanan Consultant Paediatric Endocrinologist Kings College Hospital, London Thomas Addison 1793-1860 Guy s Hospial Described Symptoms 1855 My experience 25 years
DIAGNOSING AND TREATING CORTISOL INSUFFICIENCY IN ICU MOHD BASRI MAT NOR, IIUM, KUANTAN, MALAYSIA
 DIAGNOSING AND TREATING CORTISOL INSUFFICIENCY IN ICU MOHD BASRI MAT NOR, IIUM, KUANTAN, MALAYSIA Content Glucocorticoid physiology and effects of critical illness on HPA axis Assessment of tissue cortisol
DIAGNOSING AND TREATING CORTISOL INSUFFICIENCY IN ICU MOHD BASRI MAT NOR, IIUM, KUANTAN, MALAYSIA Content Glucocorticoid physiology and effects of critical illness on HPA axis Assessment of tissue cortisol
Ahmed Al Nahari Pediatric Endocrinology Fellow March 11,2016
 Ahmed Al Nahari Pediatric Endocrinology Fellow March 11,2016 Scholar: Review the literature in an evidenced based manner to determine the difference in our clinical setting. Advocate: Develop a better
Ahmed Al Nahari Pediatric Endocrinology Fellow March 11,2016 Scholar: Review the literature in an evidenced based manner to determine the difference in our clinical setting. Advocate: Develop a better
Should Roids Be the Rage in Septic Shock? Lauren Powell, MSN, RN, CCRN, AGACNP-BC CHI Baylor St. Luke s Medical Center, Houston, TX
 Should Roids Be the Rage in Septic Shock? Lauren Powell, MSN, RN, CCRN, AGACNP-BC CHI Baylor St. Luke s Medical Center, Houston, TX Learning Objectives 1. Review the mechanism of action for the use of
Should Roids Be the Rage in Septic Shock? Lauren Powell, MSN, RN, CCRN, AGACNP-BC CHI Baylor St. Luke s Medical Center, Houston, TX Learning Objectives 1. Review the mechanism of action for the use of
ASTHMA TREATMENT AND THE HPA AXIS
 ASTHMA TREATMENT AND THE HPA AXIS Paul A. Greenberger, M.D. 7/12/2010 10:30-10:50 10:50 Objectives To review HPA axis suppression and its clinical significance in adults and children To describe methods
ASTHMA TREATMENT AND THE HPA AXIS Paul A. Greenberger, M.D. 7/12/2010 10:30-10:50 10:50 Objectives To review HPA axis suppression and its clinical significance in adults and children To describe methods
Adrenal Insufficiency in Children
 Adrenal Insufficiency in Children Stephanie Hsu, MD, PhD Assistant Professor Director of Quality Improvement and Patient Safety Pediatric Endocrinology Children s Hospital Colorado and the Barbara Davis
Adrenal Insufficiency in Children Stephanie Hsu, MD, PhD Assistant Professor Director of Quality Improvement and Patient Safety Pediatric Endocrinology Children s Hospital Colorado and the Barbara Davis
Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone
 Disease of the Adrenals 1 Zona Glomerulosa Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone leads to salt
Disease of the Adrenals 1 Zona Glomerulosa Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone leads to salt
Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences. Endocrinology. (Review) Year 5 Internal Medicine
 Year 5 Internal Medicine") Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences Endocrinology (Review) Year 5 Internal Medicine Presented by: Dr. Mona Arekat Prepared by: Ali Jassim Alhashli Case (1):
Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences Endocrinology (Review) Year 5 Internal Medicine Presented by: Dr. Mona Arekat Prepared by: Ali Jassim Alhashli Case (1):
Management of Primary Adrenal Insufficiency: An Endocrine Society Clinical Practice Guideline
 Management of Primary Adrenal Insufficiency: An Endocrine Society Clinical Practice Guideline Task Force Members Stefan R. Bornstein, MD, PhD Bruno Allolio, MD Wiebke Arlt, MD, DSc, FRCP, FMedSci Andreas
Management of Primary Adrenal Insufficiency: An Endocrine Society Clinical Practice Guideline Task Force Members Stefan R. Bornstein, MD, PhD Bruno Allolio, MD Wiebke Arlt, MD, DSc, FRCP, FMedSci Andreas
4/23/2015. Objectives DISCLOSURES
 2015 PENS Conference Savannah, GA Novel Cases of Congenital Hyperreninemic Hypaldosteronism Jan M. Foote DISCLOSURES I have no actual or potential conflicts of interest in relation to this presentation.
2015 PENS Conference Savannah, GA Novel Cases of Congenital Hyperreninemic Hypaldosteronism Jan M. Foote DISCLOSURES I have no actual or potential conflicts of interest in relation to this presentation.
Steroid in Paediatric Sepsis. Dr Pon Kah Min Hospital Pulau Pinang
 Steroid in Paediatric Sepsis Dr Pon Kah Min Hospital Pulau Pinang Contents Importance of steroid in sepsis Literature Review for adult studies Literature Review for paediatric studies Conclusions. Rationale
Steroid in Paediatric Sepsis Dr Pon Kah Min Hospital Pulau Pinang Contents Importance of steroid in sepsis Literature Review for adult studies Literature Review for paediatric studies Conclusions. Rationale
The analysis of Glucocorticoid Steroids in Plasma, Urine and Saliva by UPLC/MS/MS
 The analysis of Glucocorticoid Steroids in Plasma, Urine and Saliva by UPLC/MS/MS Brett McWhinney, Supervising Scientist, HPLC Section, Pathology Central, Pathology Queensland Overview 1. Overview of Pathology
The analysis of Glucocorticoid Steroids in Plasma, Urine and Saliva by UPLC/MS/MS Brett McWhinney, Supervising Scientist, HPLC Section, Pathology Central, Pathology Queensland Overview 1. Overview of Pathology
Inflammation. Sepsis Ladder
 Maureen Maloney-Poldek MSN, RN Chamberlain College of Nursing Pathophysiology of sepsis and septic shock How sepsis affects the endocrine system Pathophysiology of adrenal insufficiency Clinical manifestations
Maureen Maloney-Poldek MSN, RN Chamberlain College of Nursing Pathophysiology of sepsis and septic shock How sepsis affects the endocrine system Pathophysiology of adrenal insufficiency Clinical manifestations
Endocrine Emergencies: Recognition and Management
 Endocrine Emergencies: Recognition and Management John Wass Department of Endocrinology, Oxford University, UK An Update on Acute Medical Emergencies for Psychiatrists Royal College of Psychiatrists' address
Endocrine Emergencies: Recognition and Management John Wass Department of Endocrinology, Oxford University, UK An Update on Acute Medical Emergencies for Psychiatrists Royal College of Psychiatrists' address
Adrenal Insufficiency in Critical Illness
 Adrenal Insufficiency in Critical Illness Mark Stuart Cooper, BM BCh, MRCP, PhD Paul Michael Stewart, MD, FRCP, FmedSci One of the more controversial areas in critical care in recent decades relates to
Adrenal Insufficiency in Critical Illness Mark Stuart Cooper, BM BCh, MRCP, PhD Paul Michael Stewart, MD, FRCP, FmedSci One of the more controversial areas in critical care in recent decades relates to
Hypoadrenocorticism. Marc Bercovitch DVM, Dip. ACVIM. Adrenal anatomy and hormone actions/regulation
 Hypoadrenocorticism Marc Bercovitch DVM, Dip. ACVIM Adrenal anatomy and hormone actions/regulation The adrenal gland is composed of an outer cortex and an inner medulla. Catecholamines are secreted by
Hypoadrenocorticism Marc Bercovitch DVM, Dip. ACVIM Adrenal anatomy and hormone actions/regulation The adrenal gland is composed of an outer cortex and an inner medulla. Catecholamines are secreted by
Audit of Adrenal Function Tests. Kate Davies Senior Lecturer in Children s Nursing London South Bank University London, UK
 Audit of Adrenal Function Tests Kate Davies Senior Lecturer in Children s Nursing London South Bank University London, UK Introduction Audit Overview of adrenal function tests Education Audit why? Explore
Audit of Adrenal Function Tests Kate Davies Senior Lecturer in Children s Nursing London South Bank University London, UK Introduction Audit Overview of adrenal function tests Education Audit why? Explore
Assistant Professor of Endocrinology
 Pathophysiology Of Adrenal Disorder Dr.Rezvan Salehidoost Assistant Professor of Endocrinology Pathophysiology Of Adrenal Disorder The adrenal glands lie at the superior pole of each kidney and are composed
Pathophysiology Of Adrenal Disorder Dr.Rezvan Salehidoost Assistant Professor of Endocrinology Pathophysiology Of Adrenal Disorder The adrenal glands lie at the superior pole of each kidney and are composed
In memory of Thomas Addison M.D. Son of Joseph and Sarah Addison. Died June 29th 1860 aged 66 years. For 36 years physician to Guy s Hospital London.
 In memory of Thomas Addison M.D. Son of Joseph and Sarah Addison. Died June 29th 1860 aged 66 years. For 36 years physician to Guy s Hospital London. Adrenal insufficiency & Sick Day Rules Case history
In memory of Thomas Addison M.D. Son of Joseph and Sarah Addison. Died June 29th 1860 aged 66 years. For 36 years physician to Guy s Hospital London. Adrenal insufficiency & Sick Day Rules Case history
Adrenal Glands: the source of the stress system Ricardo Correa, M.D., Es.D., F.A.C.P., F.A.C.R., C.M.Q.
 Adrenal Glands: the source of the stress system Ricardo Correa, M.D., Es.D., F.A.C.P., F.A.C.R., C.M.Q. Assistant Professor of Medicine University of Arizona College of Medicine-Phoenix and The Warren
Adrenal Glands: the source of the stress system Ricardo Correa, M.D., Es.D., F.A.C.P., F.A.C.R., C.M.Q. Assistant Professor of Medicine University of Arizona College of Medicine-Phoenix and The Warren
More than meets the eye
 More than meets the eye Ana Paula Abreu, MD, PhD American Association of Clinical Endocrinologists New England Chapter Annual Meeting September 8, 2018 Disclosures No conflict of interest or significant
More than meets the eye Ana Paula Abreu, MD, PhD American Association of Clinical Endocrinologists New England Chapter Annual Meeting September 8, 2018 Disclosures No conflict of interest or significant
CPY 605 ADVANCED ENDOCRINOLOGY
 CPY 605 ADVANCED ENDOCRINOLOGY THE ADRENAL CORTEX PRESENTED BY WAINDIM NYIAMBAM YVONNE HS09A187 INTRODUCTION Two adrenal glands lie on top of each kidney. Each gland between 6 and 8g in weight is composed
CPY 605 ADVANCED ENDOCRINOLOGY THE ADRENAL CORTEX PRESENTED BY WAINDIM NYIAMBAM YVONNE HS09A187 INTRODUCTION Two adrenal glands lie on top of each kidney. Each gland between 6 and 8g in weight is composed
Proceedings of the Southern European Veterinary Conference - SEVC -
 Close this window to return to IVIS www.ivis.org Proceedings of the Southern European Veterinary Conference - SEVC - Sep. 30-Oct. 3, 2010, Barcelona, Spain Next SEVC Conference: Sep. 30-Oct. 2, 2011 -
Close this window to return to IVIS www.ivis.org Proceedings of the Southern European Veterinary Conference - SEVC - Sep. 30-Oct. 3, 2010, Barcelona, Spain Next SEVC Conference: Sep. 30-Oct. 2, 2011 -
ULTIMATE BEAUTY OF BIOCHEMISTRY. Dr. Veena Bhaskar S Gowda Dept of Biochemistry 30 th Nov 2017
 ULTIMATE BEAUTY OF BIOCHEMISTRY Dr. Veena Bhaskar S Gowda Dept of Biochemistry 30 th Nov 2017 SUSPECTED CASE OF CUSHING S SYNDROME Clinical features Moon face Obesity Hypertension Hunch back Abdominal
ULTIMATE BEAUTY OF BIOCHEMISTRY Dr. Veena Bhaskar S Gowda Dept of Biochemistry 30 th Nov 2017 SUSPECTED CASE OF CUSHING S SYNDROME Clinical features Moon face Obesity Hypertension Hunch back Abdominal
THE VALUE OF 24 HOUR PROFILES IN ASSESSING CORTISOL REPLACEMENT IN HYPOPITUITARISM
 THE VALUE OF 24 HOUR PROFILES IN ASSESSING CORTISOL REPLACEMENT IN HYPOPITUITARISM Professor Peter Hindmarsh and Kathy Geertsma Cortisol is produced in the body by the adrenal glands and the levels in
THE VALUE OF 24 HOUR PROFILES IN ASSESSING CORTISOL REPLACEMENT IN HYPOPITUITARISM Professor Peter Hindmarsh and Kathy Geertsma Cortisol is produced in the body by the adrenal glands and the levels in
Cushing s syndrome and adrenal insufficiency
 Cushing s syndrome and adrenal insufficiency Clinician expectations 1 ALIREZA ESTEGHAMATI,MD PROFESSOR OF ENDOCRINOLOGY TUMS APRIL 2016 Main Challenges Rare but important Mild forms (unrecognized) Cyclic
Cushing s syndrome and adrenal insufficiency Clinician expectations 1 ALIREZA ESTEGHAMATI,MD PROFESSOR OF ENDOCRINOLOGY TUMS APRIL 2016 Main Challenges Rare but important Mild forms (unrecognized) Cyclic
Practical Management of Steroids in Non-Endocrine Practice
 Practical Management of Steroids in Non-Endocrine Practice Dr Miguel Debono MD MRCP PhD Consultant Physician in Endocrinology and Honorary Senior Lecturer February 2016 Outline Epidemiology of steroids
Practical Management of Steroids in Non-Endocrine Practice Dr Miguel Debono MD MRCP PhD Consultant Physician in Endocrinology and Honorary Senior Lecturer February 2016 Outline Epidemiology of steroids
7.3 Suggested Evaluation and Treatment for Immunerelated Adverse Events Gastrointestinal Tract
 7.3 Suggested Evaluation and Treatment for Immunerelated Adverse Events Early diagnosis and treatment intervention for high-grade iraes can help prevent the occurrence of complications, such as GI perforation.
7.3 Suggested Evaluation and Treatment for Immunerelated Adverse Events Early diagnosis and treatment intervention for high-grade iraes can help prevent the occurrence of complications, such as GI perforation.
NOTTINGHAM UNIVERSITY HOSPITAL NHS TRUST: Clinical Chemistry Guidelines
 Adrenocortical Insufficiency Guideline Document Information Policy Reference: Adrenocortical Insufficiency Issue: 1: Version 3 Author Job Title: Peter Prinsloo Consultant in Chemical Pathology STATUS:
Adrenocortical Insufficiency Guideline Document Information Policy Reference: Adrenocortical Insufficiency Issue: 1: Version 3 Author Job Title: Peter Prinsloo Consultant in Chemical Pathology STATUS:
University of Texas Southwestern Medical Center Department of Internal Medicine Grand Rounds October 26, 2018
 University of Texas Southwestern Medical Center Department of Internal Medicine Grand Rounds October 26, 2018 Title: Immune Checkpoint Inhibitor related Endocrinopathies Speaker: Sadia Ali, M.D. This is
University of Texas Southwestern Medical Center Department of Internal Medicine Grand Rounds October 26, 2018 Title: Immune Checkpoint Inhibitor related Endocrinopathies Speaker: Sadia Ali, M.D. This is
TEST REPORT # SB. Patient Name: Comprehensive Male Profile I Patient Phone Number: TEST NAME RESULTS 08/12/18 RANGE
 TEST REPORT Ordering Provider: David Getuwell, MD 8605 SW Creekside Place Beaverton, OR 97008 Phone: 503-466-2445 Fax: 503-466-1636 Samples Received 08/15/2018 Report Date 08/20/2018 Samples Collected
TEST REPORT Ordering Provider: David Getuwell, MD 8605 SW Creekside Place Beaverton, OR 97008 Phone: 503-466-2445 Fax: 503-466-1636 Samples Received 08/15/2018 Report Date 08/20/2018 Samples Collected
John Sutton, DO, FACOI, FACE, CCD. Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989
 John Sutton, DO, FACOI, FACE, CCD Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989 Gonadal Physiology and Disease 3 No Disclosures Gonadal Axis Hypothalamic-pituitary-gonadal Feedback mechanisms
John Sutton, DO, FACOI, FACE, CCD Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989 Gonadal Physiology and Disease 3 No Disclosures Gonadal Axis Hypothalamic-pituitary-gonadal Feedback mechanisms
DIAGNOSIS OF CANINE HYPERADRENOCORTICISM: A CASE-BASED APPROACH Ellen N. Behrend, VMD, PhD, DACVIM
 DIAGNOSIS OF CANINE HYPERADRENOCORTICISM: A CASE-BASED APPROACH Ellen N. Behrend, VMD, PhD, DACVIM Case 1: Signalment: 10 yr old, CM, Miniature poodle; History: Presented for teeth cleaning; PE: Severe
DIAGNOSIS OF CANINE HYPERADRENOCORTICISM: A CASE-BASED APPROACH Ellen N. Behrend, VMD, PhD, DACVIM Case 1: Signalment: 10 yr old, CM, Miniature poodle; History: Presented for teeth cleaning; PE: Severe
Controversies in Hospital Medicine: Critical Care. Vasopressors, Steroids, and Insulin Therapy
 Controversies in Hospital Medicine: Critical Care Vasopressors, Steroids, and Insulin Therapy Douglas Fish, Pharm.D. Professor of Pharmacy, University of Colorado Denver Clinical Specialist in Critical
Controversies in Hospital Medicine: Critical Care Vasopressors, Steroids, and Insulin Therapy Douglas Fish, Pharm.D. Professor of Pharmacy, University of Colorado Denver Clinical Specialist in Critical
Addison s Disease. Disclosures. Ringo 9/8/2016. Consulting, AVL Laboratories, St. Louis, MO. Signalment: 2 ½ year old, MC, Gt Dane History:
 Addison s Disease Stanley I. Rubin, DVM, MS Diplomate ACVIM Clinical Professor Department of Veterinary Clinical Medicine Disclosures Consulting, AVL Laboratories, St. Louis, MO Ringo Signalment: 2 ½ year
Addison s Disease Stanley I. Rubin, DVM, MS Diplomate ACVIM Clinical Professor Department of Veterinary Clinical Medicine Disclosures Consulting, AVL Laboratories, St. Louis, MO Ringo Signalment: 2 ½ year
Adrenal disease Real and Unreal. Objectives. Real
 Adrenal disease Real and Unreal J R Minkoff MD, FACP Endocrinology Clinical Professor of Family and Community Medicine UCSF Objectives Participants will: 1) understand the signs, symptoms, diagnosis and
Adrenal disease Real and Unreal J R Minkoff MD, FACP Endocrinology Clinical Professor of Family and Community Medicine UCSF Objectives Participants will: 1) understand the signs, symptoms, diagnosis and
Melanoma Immunotherapy. Nursing Perspective on Immune-Related Adverse Events: Patient education, Monitoring & Management
 Melanoma Immunotherapy Nursing Perspective on Immune-Related Adverse Events: Patient education, Monitoring & Management Mike Buljan, NP UCSF Medical Center Melanoma Oncology Disclosures None Only FDA-approved
Melanoma Immunotherapy Nursing Perspective on Immune-Related Adverse Events: Patient education, Monitoring & Management Mike Buljan, NP UCSF Medical Center Melanoma Oncology Disclosures None Only FDA-approved
Protocol for Hypoadrenalism / Addison s Disease
 Protocol for Hypoadrenalism / Addison s Disease Relevance This protocol is relevant to all diagnosing clinicians, ie GPs and Nurses. HCAs and other staff should be aware of the possible presenting symptoms
Protocol for Hypoadrenalism / Addison s Disease Relevance This protocol is relevant to all diagnosing clinicians, ie GPs and Nurses. HCAs and other staff should be aware of the possible presenting symptoms
BVIG SBMI Brigitte Velkeniers Karel Fostier
 BVIG SBMI 2010 Brigitte Velkeniers Karel Fostier Case index patient 1 Patient 75 years old treated for arteritis temporalis during 2 years Initial high dose medrol during two months, with tapering and
BVIG SBMI 2010 Brigitte Velkeniers Karel Fostier Case index patient 1 Patient 75 years old treated for arteritis temporalis during 2 years Initial high dose medrol during two months, with tapering and
Differential Diagnosis of Cushing s Syndrome
 Differential Diagnosis of Cushing s Syndrome Cushing s the Diagnostic Challenge Julia Kharlip, MD and Caitlin White, MD Endocrinology, Diabetes and Metabolism Perelman School of Medicine at the University
Differential Diagnosis of Cushing s Syndrome Cushing s the Diagnostic Challenge Julia Kharlip, MD and Caitlin White, MD Endocrinology, Diabetes and Metabolism Perelman School of Medicine at the University
Adrenocortical Insufficiency: Addison's Disease
 280 PHYSIOLOGY CASES AND PROBLEMS Case 49 Adrenocortical Insufficiency: Addison's Disease Susan Oglesby is a 41-year-old divorced mother of two teenagers. She has always been in excellent health. She recently
280 PHYSIOLOGY CASES AND PROBLEMS Case 49 Adrenocortical Insufficiency: Addison's Disease Susan Oglesby is a 41-year-old divorced mother of two teenagers. She has always been in excellent health. She recently
62-year-old woman with severe headache. Celeste Thomas November 1, 2012
 62-year-old woman with severe headache Celeste Thomas November 1, 2012 History of Present Illness History of hypertension and hyperlipidemia Presented to outside hospital after awakening from sleep with
62-year-old woman with severe headache Celeste Thomas November 1, 2012 History of Present Illness History of hypertension and hyperlipidemia Presented to outside hospital after awakening from sleep with
THE VALUE OF 24 HOUR PROFILES IN CONGENITAL ADRENAL HYPERPLASIA
 THE VALUE OF 24 HOUR PROFILES IN CONGENITAL ADRENAL HYPERPLASIA This leaflet is a joint production between Professor Peter Hindmarsh and Kathy Geertsma The series editor is Professor Peter Hindmarsh Professor
THE VALUE OF 24 HOUR PROFILES IN CONGENITAL ADRENAL HYPERPLASIA This leaflet is a joint production between Professor Peter Hindmarsh and Kathy Geertsma The series editor is Professor Peter Hindmarsh Professor
Kristen Dillard, M.D. Endorama December 6, 2012
 Kristen Dillard, M.D. Endorama December 6, 2012 12 7/12 yo girl with h/o Cushing s disease presented to OSH with concern for CVA Consumed ½plate of food the night before, had raisins and diet soda on the
Kristen Dillard, M.D. Endorama December 6, 2012 12 7/12 yo girl with h/o Cushing s disease presented to OSH with concern for CVA Consumed ½plate of food the night before, had raisins and diet soda on the
Endocrinology Emergencies & Glycemic Control in the ICU
 Endocrinology Emergencies & Glycemic Control in the ICU Mark Franklin, MD Dartmouth-Hitchcock Medical Center - Lebanon, NH Avera Health eicu - Sioux Falls, SD Objectives Recognize and understand the treatment
Endocrinology Emergencies & Glycemic Control in the ICU Mark Franklin, MD Dartmouth-Hitchcock Medical Center - Lebanon, NH Avera Health eicu - Sioux Falls, SD Objectives Recognize and understand the treatment
W. Heath Giles, M.D. University of Tennessee College of Medicine Chattanooga Assistant Professor of Surgery Associate Residency Program Director
 W. Heath Giles, M.D. University of Tennessee College of Medicine Chattanooga Assistant Professor of Surgery Associate Residency Program Director It is our duty to each learner to honor your right to expect
W. Heath Giles, M.D. University of Tennessee College of Medicine Chattanooga Assistant Professor of Surgery Associate Residency Program Director It is our duty to each learner to honor your right to expect
CORTICOSTEROID USE IN SEPTIC SHOCK THE ONGOING DEBATE DIEM HO, PHARMD PGY1 PHARMACY RESIDENT VALLEY BAPTIST MEDICAL CENTER BROWNSVILLE
 CORTICOSTEROID USE IN SEPTIC SHOCK THE ONGOING DEBATE DIEM HO, PHARMD PGY1 PHARMACY RESIDENT VALLEY BAPTIST MEDICAL CENTER BROWNSVILLE 1 ABBREVIATIONS ACCP = American College of Chest Physicians ARF =
CORTICOSTEROID USE IN SEPTIC SHOCK THE ONGOING DEBATE DIEM HO, PHARMD PGY1 PHARMACY RESIDENT VALLEY BAPTIST MEDICAL CENTER BROWNSVILLE 1 ABBREVIATIONS ACCP = American College of Chest Physicians ARF =
Hypoadrenocorticism or Addison's Disease (Inadequate Production of Hormones by the Adrenal Glands) Basics
 Basics") Hypoadrenocorticism or Addison's Disease (Inadequate Production of Hormones by the Adrenal Glands) Basics OVERVIEW A hormonal disorder resulting from decreased production of hormones (glucocorticoids and/or
Hypoadrenocorticism or Addison's Disease (Inadequate Production of Hormones by the Adrenal Glands) Basics OVERVIEW A hormonal disorder resulting from decreased production of hormones (glucocorticoids and/or
ASY-857.1: Synacthen Stimulated 17OH-progesterone Test
 ASY-857.1: Synacthen Stimulated 17OH-progesterone ASY-857.2: Associated Documents a Synacthen Standing Order form (ref 0827/2) G:\Division\NDO\common\ETCProtocols\0827 Standing Order Synacthen 2016.pdf
ASY-857.1: Synacthen Stimulated 17OH-progesterone ASY-857.2: Associated Documents a Synacthen Standing Order form (ref 0827/2) G:\Division\NDO\common\ETCProtocols\0827 Standing Order Synacthen 2016.pdf
Cortisol (serum, plasma)
") Cortisol (serum, plasma) 1 Name and description of analyte 1.1 Name of analyte Cortisol 1.2 Alternative names Hydrocortisone, 11β; 17, 21 trihydroxypregn 4 ene 3,20 dione 1.3 NMLC code 1.4 Description
Cortisol (serum, plasma) 1 Name and description of analyte 1.1 Name of analyte Cortisol 1.2 Alternative names Hydrocortisone, 11β; 17, 21 trihydroxypregn 4 ene 3,20 dione 1.3 NMLC code 1.4 Description
Take Home Messages in Endocrinology
 Conflict of Interest/Disclosures Take Home Messages in Endocrinology None Carolyn Becker, MD 2 Diabetes Thyroid Pituitary Adrenal Hypoglycemia Overview Diagnostic Criteria for T2DM Diabetes should be diagnosed
Conflict of Interest/Disclosures Take Home Messages in Endocrinology None Carolyn Becker, MD 2 Diabetes Thyroid Pituitary Adrenal Hypoglycemia Overview Diagnostic Criteria for T2DM Diabetes should be diagnosed
CHOLESTEROL IS THE PRECURSOR OF STERIOD HORMONES
 HORMONES OF ADRENAL CORTEX R. Mohammadi Biochemist (Ph.D.) Faculty member of Medical Faculty CHOLESTEROL IS THE PRECURSOR OF STERIOD HORMONES CONVERSION OF CHOLESTROL TO PREGNENOLONE MINERALOCORTICOCOIDES
HORMONES OF ADRENAL CORTEX R. Mohammadi Biochemist (Ph.D.) Faculty member of Medical Faculty CHOLESTEROL IS THE PRECURSOR OF STERIOD HORMONES CONVERSION OF CHOLESTROL TO PREGNENOLONE MINERALOCORTICOCOIDES
The adrenal gland consists of the cortex & the medulla. Medulla secretes epinephrine, whereas cortex synthesizes & secretes two major classes of
 Adrenocorticosteroids Dr. Entisar Al-Mukhtar The adrenal gland consists of the cortex & the medulla. Medulla secretes epinephrine, whereas cortex synthesizes & secretes two major classes of steroid hormones:
Adrenocorticosteroids Dr. Entisar Al-Mukhtar The adrenal gland consists of the cortex & the medulla. Medulla secretes epinephrine, whereas cortex synthesizes & secretes two major classes of steroid hormones:
PROBLEMS WITH REGULATION AND METABOLISM. Objectives A & P 8/11/2011
 PROBLEMS WITH REGULATION AND METABOLISM Lemone and Burke Chapters 18-20 Objectives Review A & P Recall age related changes Identify diagnostic tests Describe etiology, pathophysiology, clinical manifestation,
PROBLEMS WITH REGULATION AND METABOLISM Lemone and Burke Chapters 18-20 Objectives Review A & P Recall age related changes Identify diagnostic tests Describe etiology, pathophysiology, clinical manifestation,
The Adrenals Are a key factor in all hormonal issues Because the adrenals can convert one hormone to another they play a role like no other in the bod
 The Players Part II The Adrenals Are a key factor in all hormonal issues Because the adrenals can convert one hormone to another they play a role like no other in the body Can affect all hormone systems
The Players Part II The Adrenals Are a key factor in all hormonal issues Because the adrenals can convert one hormone to another they play a role like no other in the body Can affect all hormone systems
Urgent and Emergent Pituitary Conditions
 Urgent and Emergent Pituitary Conditions PANKAJ A. GORE, MD DIRECTOR, BRAIN AND SKULL BASE T UMOR SURGERY PROVIDENCE B R AIN AND S PINE I NSTITUTE Urgent and Emergent Pituitary Conditions Neurosurgical
Urgent and Emergent Pituitary Conditions PANKAJ A. GORE, MD DIRECTOR, BRAIN AND SKULL BASE T UMOR SURGERY PROVIDENCE B R AIN AND S PINE I NSTITUTE Urgent and Emergent Pituitary Conditions Neurosurgical
Pseudo-Endocrine Disorders Practical Management Strategies
 Pseudo-Endocrine Disorders Practical Management Strategies 2018 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Pseudo-Endocrine
Pseudo-Endocrine Disorders Practical Management Strategies 2018 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Pseudo-Endocrine
Pseudo-Endocrine Disorders Practical Management Strategies
 Pseudo-Endocrine Disorders Practical Management Strategies 2018 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Internet
Pseudo-Endocrine Disorders Practical Management Strategies 2018 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Internet
Adrenal gland consist of: Outer Cortex and Inner Medulla Hormones secreted by Adrenal Cortex are: Glucocorticoid, Mineralocorticoid and Sex Steroids
 1 UNIVERSITY OF PAPUA NEW GUINEA SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY AND MOLECULAR BIOLOGY PBL MBBS Year III; BMLS & BDS Year 3 ADRENAL
1 UNIVERSITY OF PAPUA NEW GUINEA SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY AND MOLECULAR BIOLOGY PBL MBBS Year III; BMLS & BDS Year 3 ADRENAL
Endocrine System Physiology
 M53_MARI0000_00_SE_EX04.qxd 7/15/11 4:32 PM Page 369 4 E X E R C I S E Endocrine System Physiology Advance Preparation/Comments Consider covering the following topics to prepare students for the simulation:
M53_MARI0000_00_SE_EX04.qxd 7/15/11 4:32 PM Page 369 4 E X E R C I S E Endocrine System Physiology Advance Preparation/Comments Consider covering the following topics to prepare students for the simulation:
SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY & MOLECULAR BIOLOGY
 1 SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY & MOLECULAR BIOLOGY PBL SEMINAR: SEX HORMONES PART 1 An Overview What are steroid hormones? Steroid
1 SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY & MOLECULAR BIOLOGY PBL SEMINAR: SEX HORMONES PART 1 An Overview What are steroid hormones? Steroid
27 F with new onset hypertension and weight gain. Rajesh Jain Endorama 10/01/2015
 27 F with new onset hypertension and weight gain Rajesh Jain Endorama 10/01/2015 HPI 27 F with hypertension x 1 year BP 130-140/90 while on amlodipine 5 mg daily She also reports weight gain, 7 LB, mainly
27 F with new onset hypertension and weight gain Rajesh Jain Endorama 10/01/2015 HPI 27 F with hypertension x 1 year BP 130-140/90 while on amlodipine 5 mg daily She also reports weight gain, 7 LB, mainly
Subclinical Cushing s Syndrome
 Subclinical Cushing s Syndrome AACE 26th Annual Scientific & Clinical Congress Associate Clinical Professor of Medicine and Clinical Chief University of Miami Miller Scholl of Medicine Miami, Florida aayala2@miami.edu
Subclinical Cushing s Syndrome AACE 26th Annual Scientific & Clinical Congress Associate Clinical Professor of Medicine and Clinical Chief University of Miami Miller Scholl of Medicine Miami, Florida aayala2@miami.edu
Take-Home Messages and Clinical Pearls
 Take-Home Messages and Clinical Pearls Carolyn Becker MD Master Clinician Educator Division of Endocrinology, Diabetes and Hypertension Brigham and Women s Hospital Associate Professor of Medicine Harvard
Take-Home Messages and Clinical Pearls Carolyn Becker MD Master Clinician Educator Division of Endocrinology, Diabetes and Hypertension Brigham and Women s Hospital Associate Professor of Medicine Harvard
John Park, MD Assistant Professor of Medicine
 John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
PITUITARY: JUST THE BASICS PART 2 THE PATIENT
 PITUITARY: JUST THE BASICS PART 2 THE PATIENT DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and
PITUITARY: JUST THE BASICS PART 2 THE PATIENT DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and
74. Hormone synthesis in the adrenal cortex. The glucocorticoids: biosynthesis, regulation, effects. Adrenal cortex is vital for life!
 74. Hormone synthesis in the adrenal cortex. The glucocorticoids: biosynthesis, regulation, effects. Adrenal cortex is vital for life! 5 g each Zona glomerulosa : Mineralocorticoids ALDOSTERON Zona fasciculata:
74. Hormone synthesis in the adrenal cortex. The glucocorticoids: biosynthesis, regulation, effects. Adrenal cortex is vital for life! 5 g each Zona glomerulosa : Mineralocorticoids ALDOSTERON Zona fasciculata:
Objectives. Outline. Brief overview of the autoimmune disorders Overview of autoimmune endocrine diseases in: Case discussion Summary
 Autoimmune Endocrine Disorders: Who and How to Evaluate A Case Based Discussion Jennifer M. Barker MD Pediatric Endocrinology Children s Hospital Colorado University of Colorado Anschutz Medical Campus
Autoimmune Endocrine Disorders: Who and How to Evaluate A Case Based Discussion Jennifer M. Barker MD Pediatric Endocrinology Children s Hospital Colorado University of Colorado Anschutz Medical Campus
Lou Haenel, IV,D.O., FACOI, FACE Roper Endocrinology Charleston, SC
 Lou Haenel, IV,D.O., FACOI, FACE Roper Endocrinology Charleston, SC Myxedema Coma Life-threatening hypothyroidism resulting from untreated or inadequately treated hypothyroidism Precipitated by severe
Lou Haenel, IV,D.O., FACOI, FACE Roper Endocrinology Charleston, SC Myxedema Coma Life-threatening hypothyroidism resulting from untreated or inadequately treated hypothyroidism Precipitated by severe
The Case of the Complicated Yorkie. Case Summary. Case Summary. February 27, Solve It! Series Web Conference: The Case of the Complicated Yorkie
 The Case of the Complicated Yorkie Anthony P. Carr, Dr. med. vet. Diplomate ACVIM Gidget is just one of those dogs, currently on the second medical records folder First seen when 8 months old, up to date
The Case of the Complicated Yorkie Anthony P. Carr, Dr. med. vet. Diplomate ACVIM Gidget is just one of those dogs, currently on the second medical records folder First seen when 8 months old, up to date
Conflict of Interest Disclosure
 Incidence and Preventative Strategies of Adrenal Crisis in Congenital Adrenal Hyperplasia PadmasreeVeeraraghavan 1, Diala El-Maouche 1, Deborah P. Merke 1,2 1 National Institutes of Health Clinical Center,
Incidence and Preventative Strategies of Adrenal Crisis in Congenital Adrenal Hyperplasia PadmasreeVeeraraghavan 1, Diala El-Maouche 1, Deborah P. Merke 1,2 1 National Institutes of Health Clinical Center,
Pharmacology of Corticosteroids
 Pharmacology of Corticosteroids Dr. Aliah Alshanwani Dept. of Pharmacology College of Medicine, KSU Feb 2018 1 The Corticosteroids are steroid hormones produced by the adrenal cortex. They consist of two
Pharmacology of Corticosteroids Dr. Aliah Alshanwani Dept. of Pharmacology College of Medicine, KSU Feb 2018 1 The Corticosteroids are steroid hormones produced by the adrenal cortex. They consist of two
Should we use steroids in sepsis? J.G. van der Hoeven
 Should we use steroids in sepsis? J.G. van der Hoeven Why I don t like it It is boring.. It usually results in emotional outcries in the audience If any, the effects on outcome are very small You are not
Should we use steroids in sepsis? J.G. van der Hoeven Why I don t like it It is boring.. It usually results in emotional outcries in the audience If any, the effects on outcome are very small You are not
The Journal of Bioscience and Medicine 3, 1 (2013) Article
 Article") The Journal of Bioscience and Medicine 3, 1 (2013) Article Early postoperative serum cortisol measurements guide management in a steroid-sparing protocol and predict need for long-term steroid replacement
The Journal of Bioscience and Medicine 3, 1 (2013) Article Early postoperative serum cortisol measurements guide management in a steroid-sparing protocol and predict need for long-term steroid replacement
Evidence-Based. Management of Severe Sepsis. What is the BP Target?
 Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Endocrinological Outcome Among Treated Craniopharyngioma Patients
 Endocrinological Outcome Among Treated Craniopharyngioma Patients Afaf Al Sagheir, MD Head & Consultant, Section of Endocrinology/Diabetes Department of Pediatrics KFSH&RC Introduction Craniopharyngiomas
Endocrinological Outcome Among Treated Craniopharyngioma Patients Afaf Al Sagheir, MD Head & Consultant, Section of Endocrinology/Diabetes Department of Pediatrics KFSH&RC Introduction Craniopharyngiomas