HYPO- AND HYPERTHYROIDISM. Esztella Mikolás MD Semmelweis University 2nd Department of Medicine
|
|
|
- Bryce Oliver
- 5 years ago
- Views:
Transcription
1 HYPO- AND HYPERTHYROIDISM Esztella Mikolás MD Semmelweis University 2nd Department of Medicine
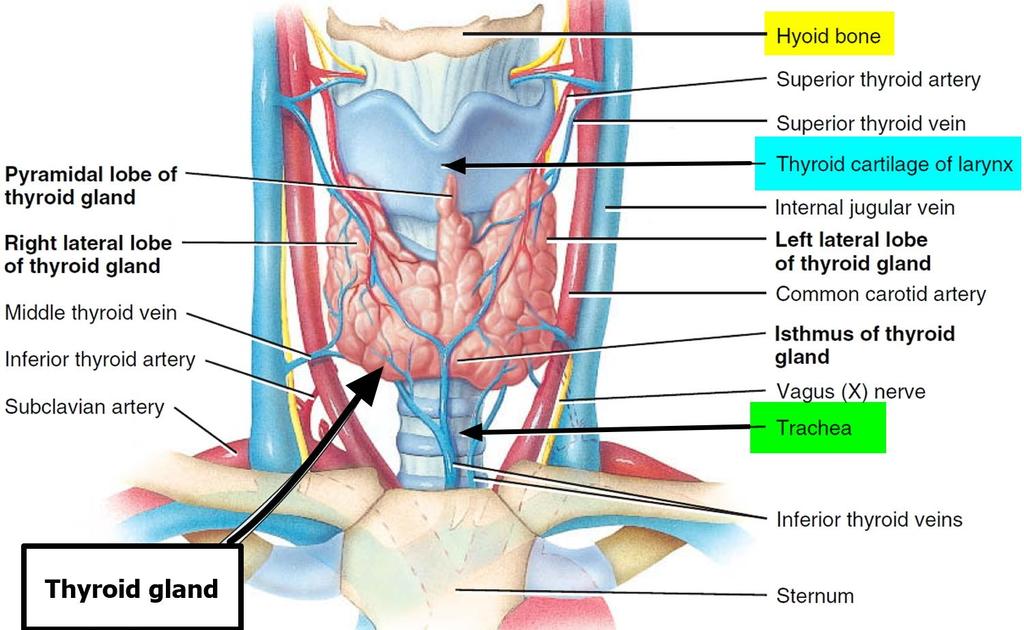
2 Anatomy

3 Histology
. DOI:10.15347/wj m/2014.008.")
4 Thyroxin synthesis and excretion Häggström, Mikael (2014). "Medical gallery of Mikael Häggström 2014". WikiJournal of Medicine 1 (2). DOI: /wj m/ ISSN Production is regulated by TSH (thyroid-stimulating hormone) level and iodine supply

5 Regulation of thyroid hormone secretion Hypothalamic-pituitary-thyroid axis From the collection of Dr Sheikh-Ali
6 Physiological effects thyroid hormone receptors (nuclear): TR-alpha 1: widely expressed (heart, skeletal muscles, bone) TR-alpha 2: antagonistic TR-beta 1: brain, liver, kidney TR-beta 2: pituitary gland, hypothalamus increase basal metabolic rate and thermogenesis stimulate water- and electrolyte transport accelerate the substrate-turnover, the amino acid and lipid metabolism potentiate the effect of catecholamine compounds regulate growth and neurological development
7 TSH - thyroid stimulating hormone normal range: mu/l depends on age, iodine supply, BMI, pregnancy, ethnicity, test method, etc.
8 T3 and T4 Biologically active portion: FT4 (free T4) ~0,015% FT3 (free T3)~0,33% normal range: FT4: pmol/l FT3: pmol/l T3 is 2-10-fold more potent Binding proteins: thyroxine binding protein, transthyretin, albumin
9 Conversion Deiodinase 1: expressed mainly in liver and kidney, with lesser expression in the thyroid Produces small amount of circulating T 3 (approx. 24%) Preserves iodide by removing iodine from inactive metabolites of T 3 and T 4 in the liver and kidney Deiodinase 2: central nervous system, pituitary gland, thyroid, heart, brown adipose tissue, and skeletal muscle T4=>T3 conversion (approx 60%) Deiodinase 3: brain and skin T4=>T2 T4=>rT3 Pol et al, DOI: /s
10 HYPOTHYROIDISM
11 Definition and frequency subclinical hypothyroidism: elevated TSH, normal FT4 prevalence: 4-10% manifest hypothyroidism: elevated TSH, low FT4 prevalence: 0,2-1% secondary hypothyroidism: elevated/normal/low TSH, low/normal FT4
12 Clinical symptoms general: fatigue, headache, cold intolerance, weight gain, anemia cardiac: pericardial fluid, heart contractility and pulse rate decrease, but hypertension (peripheral resistance increases) metabolic: dyslipidemia, hyponatremia GI tract: constipation, dysphagia skin: pale, cold, atrophic, myxedema, hair loss, weak, fragile nails neurological: ataxia, dementia, cognitive dysfunction, hypo-areflexia respiratory system: hypoventilation, sleep apnea reproductive system: amenorrhea, decrease of sex drive, infertility, hyperprolactinemia musculoskeletal: elevation of creatin-kinase, myopathy, myalgia, rhabdomyolysis
13 Etiology primary hypothyroidism (99%): autoimmune thyroiditis iatrogenic (radioiodine treatment, surgery, amiodarone) congenital iodine insufficiency malignancy transient (Wolff-Chaikoff effect, thyroiditis, thyreostatic treatment, Li-carbonate, IFalpha, IL-2) secondary hypothyroidism: pituitary tertiary hypothyroidism: hypothalamic origin thyroid hormone resistance

14 /d/df/hypothyroidism.jpg
15 Diagnostic protocol aspecific symptoms (elderly!) history: previous irradiation, thyreostatic treatment, amiodarone, surgery TSH, if out of normal range FT4 thyroid specific antibodies neck ultrasonography
16
17 Treatment I. Main goals (ATA 2014): to provide resolution of the patients' symptoms and hypothyroid signs, including biological and physiologic markers of hypothyroidism to achieve normalization of serum thyrotropin with improvement in thyroid hormone concentrations to avoid overtreatment (iatrogenic thyrotoxicosis), especially in the elderly.
18 When to treat: manifest hypothyroidism subclinical hypothyroidism: Treatment II. TSH>10 mu/l goiter ischemic heart disease pregnancy atpo positivity older than 70, TSH>8 mu/l + any of above symptomatic disease
19 Treatment III. levothyroxine (L-T4): µg/kg ( µg) T 1/2 : 7-8 days => orally once daily absorbed only at low ph value => 30 min before meal start with lower dose, especially in elderly and/or in case of cardiac disease (25-50 µg) first TSH control after 4 weeks TSH control 6 weeks after every dose adjustments if stable - yearly
20 Pregnancy placental deiodinase => ~45% higher L-T4 dose needed trimester specific target values: 1st: mu/l 2nd: mu/l 3rd: mu/l subclinical cases have to be treated closer TSH control screening in case of atpo or atg positivity, autoimmune history, goiter, any relevant symptoms present, positive family history, radioiodine therapy, surgery, miscarriage routine screening?
21 Elderly I. Age-Specific Distribution of Serum Thyrotropin and Antithyroid Antibodies in the U.S. Population: Implications for the Prevalence of Subclinical Hypothyroidism Martin I. Surks, and Joseph G. Hollowell J Clin Endocrinol Metab DOI:
22 Elderly II. sensitivity of feedback mechanism decrease with age alteration of biological activity of TSH decrease of thyroidal sensitivity to TSH apathetic hyperthyroidism
23 Thyroiditis acute infective thyroiditis radiation-induced thyroiditis palpation-induced thyroiditis subacute de Quervain thyroiditis painless thyroiditis drug induced (amiodarone, alpha-interferon, IL-2) chronic Hashimoto-thyroiditis infective thyroiditis (immunodeficiency)
24 De Quervain thyroiditis (subacute granulomatosis thyroiditis) etiology: viral infection (?) female:male=5:1 clinical signs: myalgia, fatigue, thyroid is painful, swollen laboratory markers: high sedimentation rate, elevated CRP, elevated TG level, moderate leucocytosis low 24 hour radioiodine uptake hyper-, eu-, hypothyroidism, euthyroidism therapy: NSAID, corticosteroids, propranolol recovery in 3-6 months short term relapse ~20%, long term relapse ~4%
25 Hashimoto thyroiditis organ-specific autoimmune disease => 90% follicular destruction => chronic hypothyroidism female: male=10:1 prevalence: 2-7% (female) histology: infiltration of lymphocytes, Hürtle-Askanazy cells, follicular destruction, fibrosis (FGF-23) atpo and atg positivity >95% laboratory markers: sedimentation, CRP mildly elevated radioiodine uptake: salt and pepper pattern clinical signs: mild thyroid enlargement, sensitivity, transitional hyperthyroidism, permanent hypothyroidism, rare endocrine orbitopathy therapy: levothyroxine substitution ( µg) TSH target: 2.5 mu/l prednisolon in acute phase if necessary

26 Normal Hashimoto-thyroiditis De-Quervain-thyroiditis
27 Congenital hypothyroidism hypothyroidism is present at birth incidence: primary form: 1: secondary form: 1: more frequent in girls and twins in Hungary screened since 1984 only 1/3 of the world is screened!

28 Orphanet Journal of Rare Diseases20105:17
29 HYPERTHYROIDISM
30 Definition subclinical hyperthyroidism: low TSH (0.1 mu/l>), normal FT4 manifest hyperthyroidism: low TSH (0.1 mu/l>), high FT4 prevalence: ~0.75% secondary hyperthyroidism: elevated/normal TSH, elevated FT4
31 Clinical symptoms general: weakness, fatigue, high body temperature, hot intolerance, weight loss with good appetite, resting tremor skin: warm, wet skin, intense sweating cardiac: tachycardia, systolic blood pressure elevation, lower diastolic pressure, positive inotropic effect metabolic: high metabolic rate GI tract: diarrhea neurological: tremor, hyperactivity respiratory system: hyperventilation reproductive system: irregular period, amenorrhea, sex hormone binding protein musculoskeletal: muscle weakness
32 Etiology Thyroid hormone overproduction TSH-receptor stimulation Graves-Basedow-disease mola hydatiosa choriocarcinoma TSH overproduction TSH-producing pituitary adenoma thyroid hormone resistance Thyroid autonomy toxic adenoma toxic multinodular struma Unregulated hormone excretion subacute Hashimoto silent (painless) thyroiditis postpartum iodine induced Extra thyroidal hormone production DTC struma ovarii Factitious hyperthyroidism
33 Diagnosis I. Anamnesis and physical examination Laboratory markers: low TSH, elevated FT4 and FT3 levels TSH can remain low for months after treatment FT4 and FT3 indicate severity better grey zone TSH µu/l => repeat test 1-3 months later
34 Diagnosis II. Radiology: ultrasonography (hypervascularisation, nodules) 99m Tc gamma scan low uptake => thyroiditis high uptake => Graves-Basedow disease focal high uptake => toxic adenoma
35 Graves-Basedow disease incidence: 5-10/ year-old female patients TSH-receptor stimulating IgG antibody (TSHR-Ab) in half of all cases genetic predisposition: HLA-A1, -B8, DR3 physical signs: thyroid can be enlarged, look for signs of EOP or pretibial myxedema
 www.")
36 Graves-Basedow disease -> Thyroid inferno pattern (increased vascularity and arteriovenous shunting)

37 Gamma scan
38 Treatment I. Thyreostatic treatment thionamides thiamazol (methimazol) mg/die => dose reduction continue for at least one year in euthyreotic state TSH in every 6-8 weeks propylthiouracil (PTU) mg/die => dose reduction carbimazol Side effects agranulocytosis 1:1000 => radioiodine or surgery ANCA positive vasculitis fulminant hepatitis (PTU)
39 Treatment II. Radioiodine (RI) treatment 131 I-isotope orally dose: 70 Gy expected to be effective in 2-6 months in case of severe, active EOP RI is contraindicated! preventive corticosteroid for 6-12 weeks in risk groups (smokers, EOP in history, year-old females) Subtotal thyroidectomy - indications Basedow-Graves disease + cold thyroid nodule RI not possible size reduction needed
40 Endocrine orbitopathy I. inflammation of the orbital tissue and ocular muscles 10-30% present in Basedow-Graves disease TSH-R is expressed on orbital fibroblasts => lymphocyte and macrophage activation => increase of glycosaminoglycan and sulphated mucopolysaccharide formation edema, thickening of orbital muscles, exophthalmos smoking increases risk by 70%! diagnosis: MRI T1 - muscle thickening ATA classification clinical activity score

41 Endocrine orbitopathy II. treatment indications: loss of sight, subluxation of eyeball, change in color sight, cornea blurriness, progressive exophthalmos, papillary edema, permanently visible cornea treatment: euthyreosis avoidance of smoking immunosuppression corticosteroid (per os or iv) pentoxyphyllin selenium retrobulbar irradiation (contraindicated in diabetes mellitus) surgical decompression antalgic treatment

42

43 Toxic adenoma (TA) hot nodules on gamma camera malignancy is extremely rare compensated TA: normal thyroid tissue function decreases decompensated TA: normal thyroid tissue is completely suppressed subclinical cases have to be treated therapy: RI 300 Gy radio ablation laser ablation surgery
 surgery Kamal A.S. Al-Shoumer, Hossein Gharib entokey.")
44 Toxic multinodular goiter mainly in older age can be contrast- or drug induced therapy: RI 150 Gy (contraindication: significant trachea compr.) surgery Kamal A.S. Al-Shoumer, Hossein Gharib entokey.com
45 THYROID EMERGENCIES
46 Thyreotoxicosis (thyroid storm) potentially life threatening condition provoking factors: RI treatment, surgery, trauma, myocardial infarction, iodine exposition symptoms: fever, sweat, flush, tachycardy, cardiac failure, vomiting, diarrhea, loss of conciousness, coma FT3 and FT4 is increased but not extreme Treatment thyreostatic treatment (thiamazole 80 mg per day/ PTU 250 mg/6 hours) iodine compounds (Lugol iodine or potassium iodine) glucocorticoids beta-blockers sedatives
47 Myxedema coma multi organ failure more common in elderly symptoms: severe myxedema, hypotension, bradycardia, low body temperature, hypoventillation (CO2-retention), SIADH, convulsion, coma treatment: iv 500 µg levothyroxine (or µg T3 every 12 hours) 100 µg levothyroxine per day 5-10 mg/hour hydrocortisone hyperosmolar fluids only

48 THANK YOU FOR YOUR ATTENTION!
Diseases of thyroid & parathyroid glands (1 of 2)
") Diseases of thyroid & parathyroid glands (1 of 2) Thyroid diseases Thyrotoxicosis Hypothyroidism Thyroiditis Graves disease Goiters Neoplasms Chronic Lymphocytic (Hashimoto) Thyroiditis Subacute Granulomatous
Diseases of thyroid & parathyroid glands (1 of 2) Thyroid diseases Thyrotoxicosis Hypothyroidism Thyroiditis Graves disease Goiters Neoplasms Chronic Lymphocytic (Hashimoto) Thyroiditis Subacute Granulomatous
Disorders of the Thyroid Gland
 Disorders of the Thyroid Gland István Takács MD., PhD, 1st Department of Medicine, Semmelweis University Connection to the dentistry: close to each other higher operation risk radiating pain macroglossia
Disorders of the Thyroid Gland István Takács MD., PhD, 1st Department of Medicine, Semmelweis University Connection to the dentistry: close to each other higher operation risk radiating pain macroglossia
Effect of thyroid hormones of metabolism Thyroid Diseases
 Effect of thyroid hormones of metabolism Thyroid Diseases Medical Perspective Aspects That Will Be Addressed Regulation of thyroid hormone secretion Basic physiology Hyperthyroidism Hypothyroidism Thyroiditis
Effect of thyroid hormones of metabolism Thyroid Diseases Medical Perspective Aspects That Will Be Addressed Regulation of thyroid hormone secretion Basic physiology Hyperthyroidism Hypothyroidism Thyroiditis
Thyroid disorders. Dr Enas Abusalim
 Thyroid disorders Dr Enas Abusalim Thyroid physiology The hypothalamic pituitary thyroid axis And peripheral conversion of T4 to T3, WHERE, AND BY WHAT ENZYME?? Only relatively small concentrations of
Thyroid disorders Dr Enas Abusalim Thyroid physiology The hypothalamic pituitary thyroid axis And peripheral conversion of T4 to T3, WHERE, AND BY WHAT ENZYME?? Only relatively small concentrations of
CHAPTER-II Thyroid Diseases. by: j. jayasutha lecturer department of Pharmacy practice Srm college of pharmacy srm university
 CHAPTER-II Thyroid Diseases by: j. jayasutha lecturer department of Pharmacy practice Srm college of pharmacy srm university Aspects That Will Be Addressed Hyperthyroidism Hypothyroidism Thyroiditis Hyperthyroidism
CHAPTER-II Thyroid Diseases by: j. jayasutha lecturer department of Pharmacy practice Srm college of pharmacy srm university Aspects That Will Be Addressed Hyperthyroidism Hypothyroidism Thyroiditis Hyperthyroidism
Hyperthyroidism Diagnosis and Treatment. April Janet A. Schlechte, M.D.
 Hyperthyroidism Diagnosis and Treatment Family Practice Refresher Course April 2015 Janet A. Schlechte, M.D. Disclosure of Financial Relationships Janet A. Schlechte, M.D. has no relationships with any
Hyperthyroidism Diagnosis and Treatment Family Practice Refresher Course April 2015 Janet A. Schlechte, M.D. Disclosure of Financial Relationships Janet A. Schlechte, M.D. has no relationships with any
DISORDERS OF THE THYROID GLAND SIGNS, SYMPTOMS, & TREATMENT ENDOCRINE SYSTEM AT A GLANCE OBJECTIVES ANATOMY OF THE THYROID
 OBJECTIVES DISORDERS OF THE THYROID GLAND SIGNS, SYMPTOMS, & TREATMENT Stephanie Blackburn, MHS, MLS(ASCP) CM LSU Health Shreveport Clinical Laboratory Science Program Discuss the synthesis and action
OBJECTIVES DISORDERS OF THE THYROID GLAND SIGNS, SYMPTOMS, & TREATMENT Stephanie Blackburn, MHS, MLS(ASCP) CM LSU Health Shreveport Clinical Laboratory Science Program Discuss the synthesis and action
Approach to thyroid dysfunction
 Approach to thyroid dysfunction Alice Y.Y. Cheng, MD, FRCPC Twitter: @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or
Approach to thyroid dysfunction Alice Y.Y. Cheng, MD, FRCPC Twitter: @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or
HYPERTHYROIDISM. Hypothalamus. Thyrotropin-releasing hormone (TRH) Anterior pituitary gland. Thyroid-stimulating hormone (TSH) Thyroid gland T4, T3
 Anterior pituitary gland. Thyroid-stimulating hormone (TSH) Thyroid gland T4, T3") HYPERTHYROIDISM Hypothalamus Thyrotropin-releasing hormone (TRH) Anterior pituitary gland Thyroid-stimulating hormone (TSH) Thyroid gland T4, T3 In hyperthyroidism, there is an increased production of
HYPERTHYROIDISM Hypothalamus Thyrotropin-releasing hormone (TRH) Anterior pituitary gland Thyroid-stimulating hormone (TSH) Thyroid gland T4, T3 In hyperthyroidism, there is an increased production of
Lecture title. Name Family name Country
 Lecture title Name Family name Country Nguyen Thy Khue, MD, PhD Department of Endocrinology HCMC University of Medicine and Pharmacy, MEDIC Clinic Hochiminh City, Viet Nam Provided no information regarding
Lecture title Name Family name Country Nguyen Thy Khue, MD, PhD Department of Endocrinology HCMC University of Medicine and Pharmacy, MEDIC Clinic Hochiminh City, Viet Nam Provided no information regarding
OUTLINE. Regulation of Thyroid Hormone Production Common Tests to Evaluate the Thyroid Hyperthyroidism - Graves disease, toxic nodules, thyroiditis
 THYROID DISEASE OUTLINE Regulation of Thyroid Hormone Production Common Tests to Evaluate the Thyroid Hyperthyroidism - Graves disease, toxic nodules, thyroiditis OUTLINE Hypothyroidism - Hashimoto s thyroiditis,
THYROID DISEASE OUTLINE Regulation of Thyroid Hormone Production Common Tests to Evaluate the Thyroid Hyperthyroidism - Graves disease, toxic nodules, thyroiditis OUTLINE Hypothyroidism - Hashimoto s thyroiditis,
Sample Type - Serum Result Reference Range Units. Central Thyroid Regulation Surrey & Activity KT3 4Q. Peripheral Thyroid D Function mark
 Thyroid Plus Sample Type - Serum Result Reference Range Units Central Thyroid Regulation Surrey & Activity KT3 4Q Total Thyroxine (T4)
Thyroid Plus Sample Type - Serum Result Reference Range Units Central Thyroid Regulation Surrey & Activity KT3 4Q Total Thyroxine (T4)
BELIEVE MIDWIFERY SERVICES
 TITLE: THYROID DISEASE IN PREGNANCY EFFECTIVE DATE: July, 2013 POLICY STATEMENT: Pregnancy changes significantly the values influenced by the serum thyroid binding hormone level (i.e., total thyroxine,
TITLE: THYROID DISEASE IN PREGNANCY EFFECTIVE DATE: July, 2013 POLICY STATEMENT: Pregnancy changes significantly the values influenced by the serum thyroid binding hormone level (i.e., total thyroxine,
The Number Games and Thyroid Function Arshia Panahloo Consultant Endocrinologist St George s Hospital
 The Number Games and Thyroid Function Arshia Panahloo Consultant Endocrinologist St George s Hospital Presentation Today: Common thyroid problems and treatments Pregnancy related thyroid problems The suppressed
The Number Games and Thyroid Function Arshia Panahloo Consultant Endocrinologist St George s Hospital Presentation Today: Common thyroid problems and treatments Pregnancy related thyroid problems The suppressed
Thyroid Plus. Central Thyroid Regulation & Activity. Peripheral Thyroid Function. Thyroid Auto Immunity. Key Guide. Patient: DOB: Sex: F MRN:
 Thyroid Plus Patient: DOB: Sex: F MRN: Order Number: Completed: Received: Collected: Sample Type - Serum Result Reference Range Units Central Thyroid Regulation & Activity Total Thyroxine (T4) 127 127
Thyroid Plus Patient: DOB: Sex: F MRN: Order Number: Completed: Received: Collected: Sample Type - Serum Result Reference Range Units Central Thyroid Regulation & Activity Total Thyroxine (T4) 127 127
4) Thyroid Gland Defects - Dr. Tara
 Thyroid Gland Defects - Dr. Tara") 4) Thyroid Gland Defects - Dr. Tara Thyroid Pituitary Axis TRH secreted in the hypothalamus stimulates production and Secretion of TSH TSH stimulates secretion of T3, T4 T4 has negative feedback on secretion
4) Thyroid Gland Defects - Dr. Tara Thyroid Pituitary Axis TRH secreted in the hypothalamus stimulates production and Secretion of TSH TSH stimulates secretion of T3, T4 T4 has negative feedback on secretion
Hyperthyroidism. Objectives. Clinical Manifestations. Slide 1. Slide 2. Slide 3. Implications for Primary Care. hyperthyroidism
 1 Hyperthyroidism Implications for Primary Care Laura A. Ruby, DNP, CRNP Wellspan Endocrinology 2 Objectives! Discuss the clinical manifestations of hyperthyroidism! Review the use of the diagnostic studies!
1 Hyperthyroidism Implications for Primary Care Laura A. Ruby, DNP, CRNP Wellspan Endocrinology 2 Objectives! Discuss the clinical manifestations of hyperthyroidism! Review the use of the diagnostic studies!
Thyroid and Antithyroid Drugs. Munir Gharaibeh, MD, PhD, MHPE Faculty of Medicine April 2014
 Thyroid and Antithyroid Drugs Munir Gharaibeh, MD, PhD, MHPE Faculty of Medicine April 2014 Anatomy and histology of the thyroid gland Located in neck adjacent to the 5 th cervical vertebra (C5). Composed
Thyroid and Antithyroid Drugs Munir Gharaibeh, MD, PhD, MHPE Faculty of Medicine April 2014 Anatomy and histology of the thyroid gland Located in neck adjacent to the 5 th cervical vertebra (C5). Composed
Grave s disease (1 0 )
") THYROID DYSFUNCTION Grave s disease (1 0 ) Autoimmune - activating AB s to TSH receptor High concentrations of circulating thyroid hormones Weight loss, tachycardia, tiredness Diffuse goitre - TSH stimulating
THYROID DYSFUNCTION Grave s disease (1 0 ) Autoimmune - activating AB s to TSH receptor High concentrations of circulating thyroid hormones Weight loss, tachycardia, tiredness Diffuse goitre - TSH stimulating
Thyroid gland defects. Dr. Tara Husain
 Thyroid gland defects Dr. Tara Husain Thyroid Pituitary Axis TRH secreted in the hypothalamus stimulates production and Secretion of TSH TSH stimulates secretion of T3,T4 T4 has negative feed back on secretion
Thyroid gland defects Dr. Tara Husain Thyroid Pituitary Axis TRH secreted in the hypothalamus stimulates production and Secretion of TSH TSH stimulates secretion of T3,T4 T4 has negative feed back on secretion
03-Dec-17. Thyroid Disorders GOITRE. Grossly enlarged thyroid - in hypothyroidism in hyperthyroidism - production of anatomical symptoms
 Thyroid Disorders GOITRE Grossly enlarged thyroid - in hypothyroidism in hyperthyroidism - production of anatomical symptoms 1 Physiological Goiter load on thyroid supply of I - limited stress due to:
Thyroid Disorders GOITRE Grossly enlarged thyroid - in hypothyroidism in hyperthyroidism - production of anatomical symptoms 1 Physiological Goiter load on thyroid supply of I - limited stress due to:
The Thyroid: No mystery. Just need all the pieces to the puzzle.
 The Thyroid: No mystery. Just need all the pieces to the puzzle. Todd Chennell, MS, RN ANP-C Endocrine surgery University of Rochester 2018 1 According to the American Thyroid Association, 12 percent of
The Thyroid: No mystery. Just need all the pieces to the puzzle. Todd Chennell, MS, RN ANP-C Endocrine surgery University of Rochester 2018 1 According to the American Thyroid Association, 12 percent of
19th Century Thyroidology
 1 19th Century Thyroidology Dr. Kinnicutt s patient (1893) A cold, tired, constipated middle aged woman Slow pulse rate Low body temperature From physiology it was likely patient needed thyroid replacement
1 19th Century Thyroidology Dr. Kinnicutt s patient (1893) A cold, tired, constipated middle aged woman Slow pulse rate Low body temperature From physiology it was likely patient needed thyroid replacement
Non Thyroid Surgery. In patients with Thyroid disorders
 Non Thyroid Surgery In patients with Thyroid disorders The Thyroid disease problem. Is Thyroid disease a problem with anaesthetic? Why worry? The Physiology The evidence. A pragmatic approach From: The
Non Thyroid Surgery In patients with Thyroid disorders The Thyroid disease problem. Is Thyroid disease a problem with anaesthetic? Why worry? The Physiology The evidence. A pragmatic approach From: The
Thyroid Disorders. January 2019
 Thyroid Disorders January 2019 What is the Thyroid? The thyroid is a small butterfly-shaped gland inside the neck, located in front of the trachea (windpipe) and below the larynx (voicebox). It produces
Thyroid Disorders January 2019 What is the Thyroid? The thyroid is a small butterfly-shaped gland inside the neck, located in front of the trachea (windpipe) and below the larynx (voicebox). It produces
Quality Control and Interpretation of Laboratory. Nursing and Midwifery. Dr. M. Navidhamidi
 Quality Control and Interpretation of Laboratory Tests of Thyroid Hormones for Nursing and Midwifery Dr. M. Navidhamidi Tehran University of Medical Sciences ١ Physiopathology of Thyroid Gland ٢ Thyroid
Quality Control and Interpretation of Laboratory Tests of Thyroid Hormones for Nursing and Midwifery Dr. M. Navidhamidi Tehran University of Medical Sciences ١ Physiopathology of Thyroid Gland ٢ Thyroid
Update In Hyperthyroidism
 Update In Hyperthyroidism CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi Copyright
Update In Hyperthyroidism CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi Copyright
Alvin C. Powers, M.D. 1/27/06
 Thyroid Histology Follicular Cells ECF side Apical lumen Thyroid Follicles -200-400 um Parafollicular or C-cells Colloid Photos from University of Manchester and tutorial created by Dr. James Crimando,
Thyroid Histology Follicular Cells ECF side Apical lumen Thyroid Follicles -200-400 um Parafollicular or C-cells Colloid Photos from University of Manchester and tutorial created by Dr. James Crimando,
Pathophysiology of Thyroid Disorders. PHCL 415 Hadeel Alkofide April 2010
 Pathophysiology of Thyroid Disorders PHCL 415 Hadeel Alkofide April 2010 1 Learning Objectives Understand the pathophysiology of hyperthyroidism & hypothyroidism Describe the signs & symptoms of hyperthyroidism
Pathophysiology of Thyroid Disorders PHCL 415 Hadeel Alkofide April 2010 1 Learning Objectives Understand the pathophysiology of hyperthyroidism & hypothyroidism Describe the signs & symptoms of hyperthyroidism
Laura Trask, MD FACP Central Maine Endocrinology Lewiston, ME
 Laura Trask, MD FACP Central Maine Endocrinology Lewiston, ME 795-7520 traskla@cmhc.org No disclosures Objectives To have an understanding of hyperthyroidism To have an understanding of the management
Laura Trask, MD FACP Central Maine Endocrinology Lewiston, ME 795-7520 traskla@cmhc.org No disclosures Objectives To have an understanding of hyperthyroidism To have an understanding of the management
DRUGS. 4- Two molecules of DIT combine within the thyroglobulinto form L-thyroxine (T4)' One molecule of MIT & one molecule of DIT combine to form T3
' One molecule of MIT & one molecule of DIT combine to form T3") THYROID HORMONEs & ANTITHYROID The thyroid secretes 2 types of hormones: DRUGS 1- Iodine containing amino acids (are important for growth, development and metabolism) and these are: triodothyronine, tetraiodothyronine,(
THYROID HORMONEs & ANTITHYROID The thyroid secretes 2 types of hormones: DRUGS 1- Iodine containing amino acids (are important for growth, development and metabolism) and these are: triodothyronine, tetraiodothyronine,(
B-Resistance to the action of hormones, Hormone resistance characterized by receptor mediated, postreceptor.
 Disorders of the endocrine system 38 Disorders of endocrine system mainly are caused by: A-Deficiency or an excess of a single hormone or several hormones: - deficiency :can be congenital or acquired.
Disorders of the endocrine system 38 Disorders of endocrine system mainly are caused by: A-Deficiency or an excess of a single hormone or several hormones: - deficiency :can be congenital or acquired.
Slide notes: This presentation provides information on Graves disease, a systemic autoimmune disease. Epidemiology, pathology, complications,
 1 This presentation provides information on Graves disease, a systemic autoimmune disease. Epidemiology, pathology, complications, including ophthalmic complications, treatments (both permanent solutions
1 This presentation provides information on Graves disease, a systemic autoimmune disease. Epidemiology, pathology, complications, including ophthalmic complications, treatments (both permanent solutions
Thyroid Hormones (T 4 & T 3 )
") 1 Thyroid Hormones (T 4 & T 3 ) Normalize growth and development, body temperature, and energy levels. Used as thyroid replacement therapy in hypothyroidism. Thyroxine (T 4 ) is peripherally metabolized
1 Thyroid Hormones (T 4 & T 3 ) Normalize growth and development, body temperature, and energy levels. Used as thyroid replacement therapy in hypothyroidism. Thyroxine (T 4 ) is peripherally metabolized
Imaging in Pediatric Thyroid disorders: US and Radionuclide imaging. Deepa R Biyyam, MD Attending Pediatric Radiologist
 Imaging in Pediatric Thyroid disorders: US and Radionuclide imaging Deepa R Biyyam, MD Attending Pediatric Radiologist Imaging in Pediatric Thyroid disorders: Imaging modalities Outline ACR-SNM-SPR guidelines
Imaging in Pediatric Thyroid disorders: US and Radionuclide imaging Deepa R Biyyam, MD Attending Pediatric Radiologist Imaging in Pediatric Thyroid disorders: Imaging modalities Outline ACR-SNM-SPR guidelines
HYPOTHYROIDISM AND HYPERTHYROIDISM
 HYPOTHYROIDISM AND HYPERTHYROIDISM SHAHIDA PERVEEN, AMBREEN Post RN BSCN Semester II FACULTY SIR RAJA April 13, 016 Objectives: State the functions of thyroid hormone. Understand the pathologic mechanism
HYPOTHYROIDISM AND HYPERTHYROIDISM SHAHIDA PERVEEN, AMBREEN Post RN BSCN Semester II FACULTY SIR RAJA April 13, 016 Objectives: State the functions of thyroid hormone. Understand the pathologic mechanism
Toxic MNG Thyroiditis 5-15
 Hyperthyroidism Facts Prevalence 0.5-1.0%, more common in women Thyrotoxicosis is excess thyroid hormones from endogenous or exogenous sources Hyperthyroidism is excess thyroid hormones from thyroid gland
Hyperthyroidism Facts Prevalence 0.5-1.0%, more common in women Thyrotoxicosis is excess thyroid hormones from endogenous or exogenous sources Hyperthyroidism is excess thyroid hormones from thyroid gland
Disorders of Thyroid Function
 Disorders of Thyroid Function Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Thyroid Hormone Axis Hypothalamus TRH
Disorders of Thyroid Function Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Thyroid Hormone Axis Hypothalamus TRH
Dharma Lindarto Div. Endokrin-Metabolisme dan Diabetes. Dep Ilmu Penyakit Dalam FK USU / RSUP HAM Medan
 HYPERTHYROIDISM Dharma Lindarto Div. Endokrin-Metabolisme dan Diabetes. Dep Ilmu Penyakit Dalam FK USU / RSUP HAM Medan Anatomy of the Thyroid Gland Tiroid Disease Multi N Aspect fungtion morphology eutiroid,
HYPERTHYROIDISM Dharma Lindarto Div. Endokrin-Metabolisme dan Diabetes. Dep Ilmu Penyakit Dalam FK USU / RSUP HAM Medan Anatomy of the Thyroid Gland Tiroid Disease Multi N Aspect fungtion morphology eutiroid,
John Sutton, DO, FACOI, FACE, CCD. Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989
 John Sutton, DO, FACOI, FACE, CCD Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989 No Disclosures Disease Of the Thyroid Iodide Metabolism/Synthesis of Thyroid Hormone Trap Oxidation Organification(catalyzed
John Sutton, DO, FACOI, FACE, CCD Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989 No Disclosures Disease Of the Thyroid Iodide Metabolism/Synthesis of Thyroid Hormone Trap Oxidation Organification(catalyzed
Thyroid Disease. I have no disclosures. Overview TSH. Matthew Kim, M.D. July, 2012
 Thyroid Disease I have no disclosures Matthew Kim, M.D. July, 2012 Overview Thyroid Function Tests Hyperthyroidism Hypothyroidism Subclinical Thyroid Disease Thyroid Nodules Questions TSH Best single screening
Thyroid Disease I have no disclosures Matthew Kim, M.D. July, 2012 Overview Thyroid Function Tests Hyperthyroidism Hypothyroidism Subclinical Thyroid Disease Thyroid Nodules Questions TSH Best single screening
university sciences of Isfahan university Com
 Introduce R. Gholamnezhad Lecturer of school of nursing & midwifery of Iran university Ph.D student tof Immunology, Sh School of medical sciences of Isfahan university E-Mail: Gholami278@gmail. Com Interpreting
Introduce R. Gholamnezhad Lecturer of school of nursing & midwifery of Iran university Ph.D student tof Immunology, Sh School of medical sciences of Isfahan university E-Mail: Gholami278@gmail. Com Interpreting
Thyrotoxicosis in Pregnancy: Diagnose and Management
 Thyrotoxicosis in Pregnancy: Diagnose and Management Yuanita Asri Langi email: meralday@yahoo.co.id Endocrinology & Metabolic Division, Internal Medicine Department, Prof.dr.R.D. Kandou Hospital/ Sam Ratulangi
Thyrotoxicosis in Pregnancy: Diagnose and Management Yuanita Asri Langi email: meralday@yahoo.co.id Endocrinology & Metabolic Division, Internal Medicine Department, Prof.dr.R.D. Kandou Hospital/ Sam Ratulangi
Thyroid hormone. Functional anatomy of thyroid gland
 Thyroid hormone ส ว ฒณ ค ปต ว ฒ ต กจ ฑาธ ช ห อง 101 Aims Functional anatomy of thyroid gland Synthesis, secretion and metabolism of the thyroid hormones The mechanism of thyroid hormone action Role of
Thyroid hormone ส ว ฒณ ค ปต ว ฒ ต กจ ฑาธ ช ห อง 101 Aims Functional anatomy of thyroid gland Synthesis, secretion and metabolism of the thyroid hormones The mechanism of thyroid hormone action Role of
Hyperthyroidism, Inflammatory Disorders
 Hyperthyroidism, Inflammatory Disorders free T4 Howard J. Sachs, MD www.12daysinmarch.com Hyperthyroidism, Inflammatory Disorders The total T4 may be elevated in pregnancy and with OCP use Graves I 123
Hyperthyroidism, Inflammatory Disorders free T4 Howard J. Sachs, MD www.12daysinmarch.com Hyperthyroidism, Inflammatory Disorders The total T4 may be elevated in pregnancy and with OCP use Graves I 123
Thyroid and Antithyroid Drugs. Dr. Alia Shatanawi Feb,
 Thyroid and Antithyroid Drugs Dr. Alia Shatanawi Feb, 24 2014 Anatomy and histology of the thyroid gland Located in neck adjacent to the 5 th cervical vertebra (C5). Composed of epithelial cells which
Thyroid and Antithyroid Drugs Dr. Alia Shatanawi Feb, 24 2014 Anatomy and histology of the thyroid gland Located in neck adjacent to the 5 th cervical vertebra (C5). Composed of epithelial cells which
Understanding Thyroid Labs
 Understanding Thyroid Labs Chris Sadler, MA, PA-C, CDE, DFAAPA Senior Medical Science Liaison CVM Janssen Scientific Affairs Diabetes and Endocrine Associates La Jolla, CA Disclosures Employee of Janssen
Understanding Thyroid Labs Chris Sadler, MA, PA-C, CDE, DFAAPA Senior Medical Science Liaison CVM Janssen Scientific Affairs Diabetes and Endocrine Associates La Jolla, CA Disclosures Employee of Janssen
Pathophysiology of the th E d n ocr i ne S S t ys em B. Marinov, MD, PhD Endocrine system Central: Hypothalamus
 Pathophysiology of the Endocrine System B. Marinov, MD, PhD Pathophysiology Department Medical University of Plovdiv Endocrine system Central: Hypothalamus Pituitary Pineal Peripheral Thymus Thyroid Parathyroid
Pathophysiology of the Endocrine System B. Marinov, MD, PhD Pathophysiology Department Medical University of Plovdiv Endocrine system Central: Hypothalamus Pituitary Pineal Peripheral Thymus Thyroid Parathyroid
TANJA KEMP INTERNAL MEDICINE: ENDOCRINOLOGY
 ENDOCRINE DISORDERS IN THE ELDERLY (part 2) TANJA KEMP INTERNAL MEDICINE: ENDOCRINOLOGY Pituitary axis Target organs of the pituitary gland Negative feedback Hypothalamus-Pituitary-Thyroid axis Thyroid
ENDOCRINE DISORDERS IN THE ELDERLY (part 2) TANJA KEMP INTERNAL MEDICINE: ENDOCRINOLOGY Pituitary axis Target organs of the pituitary gland Negative feedback Hypothalamus-Pituitary-Thyroid axis Thyroid
Common Issues in Management of Hypothyroidism
 Common Issues in Management of Hypothyroidism Family Medicine Refresher Course April 5, 2018 Janet A. Schlechte, M.D. Disclosure of Financial Relationships Janet A. Schlechte, M.D. has no relationships
Common Issues in Management of Hypothyroidism Family Medicine Refresher Course April 5, 2018 Janet A. Schlechte, M.D. Disclosure of Financial Relationships Janet A. Schlechte, M.D. has no relationships
Hypothalamo-Pituitary-Thyroid Axis
 SMGr up Hypothalamo-Pituitary-Thyroid Axis Orluwene Chituru Godwill 1 * and Ohiri John U 1 1 Chemical Pathology Department, University of Port Harcourt Teaching Hospital, Nigeria *Corresponding author:
SMGr up Hypothalamo-Pituitary-Thyroid Axis Orluwene Chituru Godwill 1 * and Ohiri John U 1 1 Chemical Pathology Department, University of Port Harcourt Teaching Hospital, Nigeria *Corresponding author:
Sanjay B. Dixit, M.D. BHS Endocrinology Associates November 11, 2017
 Sanjay B. Dixit, M.D. BHS Endocrinology Associates November 11, 2017 I will not be discussing this Outline of discussion Laboratory tests for thyroid function Diagnosis of hypothyroidism Treatment of
Sanjay B. Dixit, M.D. BHS Endocrinology Associates November 11, 2017 I will not be discussing this Outline of discussion Laboratory tests for thyroid function Diagnosis of hypothyroidism Treatment of
None. Thyroid Potpourri for the Primary Care Physician. Evaluating Thyroid Function. Disclosures. Learning Objectives
 Thyroid Potpourri for the Primary Care Physician Ramya Vedula DO, MPH, ECNU Endocrinology, Diabetes and Metabolism Princeton Medical Group Assistant Professor of Clinical Medicine Rutgers Robert Wood Johnson
Thyroid Potpourri for the Primary Care Physician Ramya Vedula DO, MPH, ECNU Endocrinology, Diabetes and Metabolism Princeton Medical Group Assistant Professor of Clinical Medicine Rutgers Robert Wood Johnson
THYROID DISEASE IN CHILDREN
 THYROID DISEASE IN CHILDREN Michelle Schweiger, D.O. Center for Pediatric and Adolescent Endocrinology Cleveland Clinic Foundation Neither I nor any immediate family members have any financial interests
THYROID DISEASE IN CHILDREN Michelle Schweiger, D.O. Center for Pediatric and Adolescent Endocrinology Cleveland Clinic Foundation Neither I nor any immediate family members have any financial interests
THYROTOXICOSIS DR.J.BALA KUMAR 2 ND YR SURGERY PG
 THYROTOXICOSIS DR.J.BALA KUMAR 2 ND YR SURGERY PG What is the difference between thyrotoxicosis and hyperthyroidism Thyrotoxicosis Thyrotoxicosis is defined as the state of thyroid hormone excess and is
THYROTOXICOSIS DR.J.BALA KUMAR 2 ND YR SURGERY PG What is the difference between thyrotoxicosis and hyperthyroidism Thyrotoxicosis Thyrotoxicosis is defined as the state of thyroid hormone excess and is
Mastering Thyroid Disorders. Douglas C. Bauer, MD UCSF Division of General Internal Medicine
 Mastering Thyroid Disorders Douglas C. Bauer, MD UCSF Division of General Internal Medicine Cases 68 yr old female with new atrial fibrillation and no other findings except TSH=0.04, normal free T4 79
Mastering Thyroid Disorders Douglas C. Bauer, MD UCSF Division of General Internal Medicine Cases 68 yr old female with new atrial fibrillation and no other findings except TSH=0.04, normal free T4 79
25/10/56. Hypothyroidism Myxedema in adults Cretinism congenital deficiency of thyroid hormone Hashimoto thyroiditis. Simple goiter (nontoxic goiter)
") THERAPEUTIC USES OF THYROID HORMONE Supeecha Wittayalertpunya Wannarasmi Ketchart Nov 2013 Hyperthyroidism (Thyrotoxicosis) Grave s disease (diffuse toxic goiter) Toxic uninodular & Toxic multinodular
THERAPEUTIC USES OF THYROID HORMONE Supeecha Wittayalertpunya Wannarasmi Ketchart Nov 2013 Hyperthyroidism (Thyrotoxicosis) Grave s disease (diffuse toxic goiter) Toxic uninodular & Toxic multinodular
Thyroid Gland. Patient Information
 Thyroid Gland Patient Information Contact details for Endocrine and Thyroid Clinics Hawke s Bay Fallen Soldiers Memorial Hospital Villa 16 Phone: 06 8788109 ext 5891 Text: 0274 102 559 Email: endoclinic@hbdhb.govt.nz
Thyroid Gland Patient Information Contact details for Endocrine and Thyroid Clinics Hawke s Bay Fallen Soldiers Memorial Hospital Villa 16 Phone: 06 8788109 ext 5891 Text: 0274 102 559 Email: endoclinic@hbdhb.govt.nz
Some Issues in the Management of Hypothyroidism
 Some Issues in the Management of Hypothyroidism Family Medicine Refresher Course April 6, 2016 Janet A. Schlechte, M.D. Disclosure of Financial Relationships Janet A. Schlechte, M.D. has no relationships
Some Issues in the Management of Hypothyroidism Family Medicine Refresher Course April 6, 2016 Janet A. Schlechte, M.D. Disclosure of Financial Relationships Janet A. Schlechte, M.D. has no relationships
Thyroid Function TSH Analyte Information
 Thyroid Function TSH Analyte Information 1 2013-05-01 Thyroid-stimulating hormone (TSH) Introduction Thyroid-stimulating hormone (thyrotropin, TSH) is a glycoprotein with molecular weight of approximately
Thyroid Function TSH Analyte Information 1 2013-05-01 Thyroid-stimulating hormone (TSH) Introduction Thyroid-stimulating hormone (thyrotropin, TSH) is a glycoprotein with molecular weight of approximately
An Approach to: Thyroid Function Tests. Rinkoo Dalan Consultant Department of Endocrinology Tan Tock Seng Hospital
 An Approach to: Thyroid Function Tests Rinkoo Dalan Consultant Department of Endocrinology Tan Tock Seng Hospital Regulation of Thyroid axis Hypothalamus TRH T3,T4 ---- TRH Median Eminence (base of brain)
An Approach to: Thyroid Function Tests Rinkoo Dalan Consultant Department of Endocrinology Tan Tock Seng Hospital Regulation of Thyroid axis Hypothalamus TRH T3,T4 ---- TRH Median Eminence (base of brain)
Anaesthesia In Thyroid Disorder. Dr. Umme Salma Ayesha Hoque MBBS, DA Medical Officer Department of Anaesthesiology and SICU BIRDEM General Hospital
 Anaesthesia In Thyroid Disorder Dr. Umme Salma Ayesha Hoque MBBS, DA Medical Officer Department of Anaesthesiology and SICU BIRDEM General Hospital Anatomy Endocrine gland : Consist of two lobe Located
Anaesthesia In Thyroid Disorder Dr. Umme Salma Ayesha Hoque MBBS, DA Medical Officer Department of Anaesthesiology and SICU BIRDEM General Hospital Anatomy Endocrine gland : Consist of two lobe Located
Endocrine system pathology
 Endocrine system pathology Central endocrine system peripheral endocrine system: thyroid gland parathyroid gland pancreas adrenal glands Thyroid gland. the weight of normal thyroid gland is about 15 grams.
Endocrine system pathology Central endocrine system peripheral endocrine system: thyroid gland parathyroid gland pancreas adrenal glands Thyroid gland. the weight of normal thyroid gland is about 15 grams.
Decoding Your Thyroid Tests and Results
 Decoding Your Thyroid Tests and Results Wondering about your thyroid test results? Learn about each test and what low, optimal, and high results may mean so you can work with your doctor to choose appropriate
Decoding Your Thyroid Tests and Results Wondering about your thyroid test results? Learn about each test and what low, optimal, and high results may mean so you can work with your doctor to choose appropriate
Pathology. Hyperthyroidism (Overactive Thyroid), Graves Disease (Basedow Disease) and more. Definitions. See online here
, Graves Disease (Basedow Disease) and more. Definitions. See online here") Pathology Hyperthyroidism (Overactive Thyroid), Graves Disease (Basedow Disease) and more See online here Hyperthyroidism is caused by the excess of thyroid hormones T3 and T4. Graves disease is the most
Pathology Hyperthyroidism (Overactive Thyroid), Graves Disease (Basedow Disease) and more See online here Hyperthyroidism is caused by the excess of thyroid hormones T3 and T4. Graves disease is the most
THYROID DISEASE IN PREGNANCY
 THYROID DISEASE IN PREGNANCY https://www.wddty.com/magazine/2016/june/depression-its-not-your-brain-its-your-thyroid.html Grand Rounds December 5, 2018 Maria Kolojeski, DO (PGY3) REVIEW OF THYROID HORMONES
THYROID DISEASE IN PREGNANCY https://www.wddty.com/magazine/2016/june/depression-its-not-your-brain-its-your-thyroid.html Grand Rounds December 5, 2018 Maria Kolojeski, DO (PGY3) REVIEW OF THYROID HORMONES
Disclosures. Learning objectives. Case 1A. Autoimmune Thyroid Disease: Medical and Surgical Issues. I have nothing to disclose.
 Disclosures Autoimmune Thyroid Disease: Medical and Surgical Issues I have nothing to disclose. Chrysoula Dosiou, MD, MS Clinical Assistant Professor Division of Endocrinology Stanford University School
Disclosures Autoimmune Thyroid Disease: Medical and Surgical Issues I have nothing to disclose. Chrysoula Dosiou, MD, MS Clinical Assistant Professor Division of Endocrinology Stanford University School
Thyroid Screen (Serum)
") Thyroid Screen (Serum) Patient: DOB: Sex: F MRN: Order Number: Completed: Received: Collected: Sample Type - Serum Result Reference Range Units Central Thyroid Regulation & Activity Total Thyroxine (T4)
Thyroid Screen (Serum) Patient: DOB: Sex: F MRN: Order Number: Completed: Received: Collected: Sample Type - Serum Result Reference Range Units Central Thyroid Regulation & Activity Total Thyroxine (T4)
HORMONES OF THE POSTERIOR PITUITARY
 HORMONES OF THE POSTERIOR PITUITARY HORMONES OF THE POSTERIOR PITUITARY In contrast to the hormones of the anterior lobe of the pituitary, those of the posterior lobe, vasopressin and oxytocin, are not
HORMONES OF THE POSTERIOR PITUITARY HORMONES OF THE POSTERIOR PITUITARY In contrast to the hormones of the anterior lobe of the pituitary, those of the posterior lobe, vasopressin and oxytocin, are not
GOITER and Shortness of Breath. Case A: GOITER. Learning Objectives. Common Thyroid Disorders for
 2:25 3:05pm Diagnosing and Treating Thyroid Disorders SPEAKER John Tayek, MD Presenter Disclosure Information The following relationships exist related to this presentation: John Tayek, MD, serves on the
2:25 3:05pm Diagnosing and Treating Thyroid Disorders SPEAKER John Tayek, MD Presenter Disclosure Information The following relationships exist related to this presentation: John Tayek, MD, serves on the
Hypothyroidism in Women
 Illustration istock Collection / thinkstockphotos.com T Hypothyroidism in Women Donna Dunn Thyroid disease is a major health issue in the United States. Approximately 20 million Americans have been diagnosed
Illustration istock Collection / thinkstockphotos.com T Hypothyroidism in Women Donna Dunn Thyroid disease is a major health issue in the United States. Approximately 20 million Americans have been diagnosed
THYROID FUNCTION TEST and RADIONUCLIDE THERAPY
 THYROID FUNCTION TEST and RADIONUCLIDE THERAPY Ajalaya Teyateeti, M.D. Division of Nuclear Medicine Department of Radiology I. Thyroid function test OUTLINE Application and interpretation of in vitro TFT
THYROID FUNCTION TEST and RADIONUCLIDE THERAPY Ajalaya Teyateeti, M.D. Division of Nuclear Medicine Department of Radiology I. Thyroid function test OUTLINE Application and interpretation of in vitro TFT
Hyperthyroidism. Causes. Diagnosis. Christopher Theberge
 Hyperthyroidism Pronunciations: (Hyperthyroidism) Hyperthyroidism (overactive thyroid) is a condition where the thyroid gland synthesizes and secretes the thyroid hormones thyroxine (T4) and triiodothyronine
Hyperthyroidism Pronunciations: (Hyperthyroidism) Hyperthyroidism (overactive thyroid) is a condition where the thyroid gland synthesizes and secretes the thyroid hormones thyroxine (T4) and triiodothyronine
Thyroid in the elderly. Akbar Soltani M.D. Endocrinology and Metabolism Research Center (EMRC) Shariati Hospital
 Shariati Hospital") Thyroid in the elderly Akbar Soltani M.D. Endocrinology and Metabolism Research Center (EMRC) Shariati Hospital soltania@tuma.ac.ir Case 1 A 79 year old female is seen because of a 6 month history of fatigue,
Thyroid in the elderly Akbar Soltani M.D. Endocrinology and Metabolism Research Center (EMRC) Shariati Hospital soltania@tuma.ac.ir Case 1 A 79 year old female is seen because of a 6 month history of fatigue,
Management of Common Thyroid Disorders
 Cases Management of Common Thyroid Disorders Douglas C. Bauer, MD UCSF Division of General Internal Medicine No Disclosures 68 yr old female with new atrial fibrillation and no other findings except TSH=0.04,
Cases Management of Common Thyroid Disorders Douglas C. Bauer, MD UCSF Division of General Internal Medicine No Disclosures 68 yr old female with new atrial fibrillation and no other findings except TSH=0.04,
Endocrine part two. Presented by Dr. Mohammad Saadeh The requirements for the Clinical Chemistry Philadelphia University Faculty of pharmacy
 Endocrine part two Presented by Dr. Mohammad Saadeh The requirements for the Clinical Chemistry Philadelphia University Faculty of pharmacy Cushing's disease: increased secretion of adrenocorticotropic
Endocrine part two Presented by Dr. Mohammad Saadeh The requirements for the Clinical Chemistry Philadelphia University Faculty of pharmacy Cushing's disease: increased secretion of adrenocorticotropic
Thyroiditis Diagnosis and Management issues. Prof. Md. Enamul Karim Professor of Medicine Dhaka Medical College
 Thyroiditis Diagnosis and Management issues Prof. Md. Enamul Karim Professor of Medicine Dhaka Medical College Definition Thyroiditis is a general term that refers to inflammation of the thyroid gland.
Thyroiditis Diagnosis and Management issues Prof. Md. Enamul Karim Professor of Medicine Dhaka Medical College Definition Thyroiditis is a general term that refers to inflammation of the thyroid gland.
Update on Gestational Thyroid Disease. Aidan McElduff The Discipline of Medicine, The University of Sydney
 IADPSG 2016 Update on Gestational Thyroid Disease Aidan McElduff The Discipline of Medicine, The University of Sydney IADPSG 2016 DISCLOSURES and AIM Nil to disclose Aim: to provide an overview 2017 Guidelines
IADPSG 2016 Update on Gestational Thyroid Disease Aidan McElduff The Discipline of Medicine, The University of Sydney IADPSG 2016 DISCLOSURES and AIM Nil to disclose Aim: to provide an overview 2017 Guidelines
Thyroid Disorders. Hypothyroidism. Low Total T4 Antiseizure meds Glucocorticoids. Free T4. Howard J. Sachs, MD.
 Thyroid Disorders Free T4 Low Total T4 Antiseizure meds Glucocorticoids Hypothyroidism Howard J. Sachs, MD www.12daysinmarch.com Primary Hypothyroidism High TSH Low free T4 Primary = End organ failure
Thyroid Disorders Free T4 Low Total T4 Antiseizure meds Glucocorticoids Hypothyroidism Howard J. Sachs, MD www.12daysinmarch.com Primary Hypothyroidism High TSH Low free T4 Primary = End organ failure
The Thyroid and Pregnancy OUTLINE OF DISCUSSION 3/19/10. Francis S. Greenspan March 19, Normal Physiology. 2.
 The Thyroid and Pregnancy Francis S. Greenspan March 19, 2010 OUTLINE OF DISCUSSION 1. Normal Physiology 2. Hypothyroidism 3. Hyperthyroidism 4. Thyroid Nodules and Cancer NORMAL PHYSIOLOGY Iodine Requirements:
The Thyroid and Pregnancy Francis S. Greenspan March 19, 2010 OUTLINE OF DISCUSSION 1. Normal Physiology 2. Hypothyroidism 3. Hyperthyroidism 4. Thyroid Nodules and Cancer NORMAL PHYSIOLOGY Iodine Requirements:
Hypothyroidism. Definition:
 Definition: Hypothyroidism Primary hypothyroidism is characterized biochemically by a high serum thyroidstimulating hormone (TSH) concentration and a low serum free thyroxine (T4) concentration. Subclinical
Definition: Hypothyroidism Primary hypothyroidism is characterized biochemically by a high serum thyroidstimulating hormone (TSH) concentration and a low serum free thyroxine (T4) concentration. Subclinical
Iodine 131 thyroid Therapy. Sara G. Johnson, MBA, CNMT, NCT President SNMMI-TS VA Healthcare System San Diego
 Iodine 131 thyroid Therapy Sara G. Johnson, MBA, CNMT, NCT President SNMMI-TS VA Healthcare System San Diego OBJECTIVES Describe the basics of thyroid gland anatomy and physiology Outline the disease process
Iodine 131 thyroid Therapy Sara G. Johnson, MBA, CNMT, NCT President SNMMI-TS VA Healthcare System San Diego OBJECTIVES Describe the basics of thyroid gland anatomy and physiology Outline the disease process
Amiodarone Toxicities
 Amiodarone Toxicities Student Rounds Review Ashlie McGuire - Aug. 4, 2016 Amiodarone Use: Antiarrhythmic agent Supraventricular and ventricular tachycardia Favourable for HF patients due to minimal inotropic
Amiodarone Toxicities Student Rounds Review Ashlie McGuire - Aug. 4, 2016 Amiodarone Use: Antiarrhythmic agent Supraventricular and ventricular tachycardia Favourable for HF patients due to minimal inotropic
Approach to Thyroid Dysfunction in the Elderly
 Approach to Thyroid Dysfunction in the Elderly Fernando Melaragno Endocrinology Objective The objective of this lecture is to review the epidemiology, clinical presentation, risks and complications, and
Approach to Thyroid Dysfunction in the Elderly Fernando Melaragno Endocrinology Objective The objective of this lecture is to review the epidemiology, clinical presentation, risks and complications, and
THYROID DISEASE AND TESTING. Jack L. Snitzer, D.O., FACOI, FACE, CCD
 THYROID DISEASE AND TESTING Jack L. Snitzer, D.O., FACOI, FACE, CCD MAPA MEETING 2018 JACK L. SNITZER, D.O. 410-572-8848 JACK.SNITZER@PENINSULA.ORG NO CONFLICTS OF INTEREST THYROID THYROID Goiter Hyperthyroidism
THYROID DISEASE AND TESTING Jack L. Snitzer, D.O., FACOI, FACE, CCD MAPA MEETING 2018 JACK L. SNITZER, D.O. 410-572-8848 JACK.SNITZER@PENINSULA.ORG NO CONFLICTS OF INTEREST THYROID THYROID Goiter Hyperthyroidism
Management of Common Thyroid Disorders
 Management of Common Thyroid Disorders Douglas C. Bauer, MD UCSF Division of General Internal Medicine No Disclosures Cases 68 yr old woman with new atrial fibrillation and no other findings except TSH=0.04,
Management of Common Thyroid Disorders Douglas C. Bauer, MD UCSF Division of General Internal Medicine No Disclosures Cases 68 yr old woman with new atrial fibrillation and no other findings except TSH=0.04,
Thyroid nodules. Most thyroid nodules are benign
 Thyroid nodules Postgraduate Course in General Surgery Jessica E. Gosnell MD Assistant Professor March 22, 2011 Most thyroid nodules are benign thyroid nodules occur in 77% of the world s population palpable
Thyroid nodules Postgraduate Course in General Surgery Jessica E. Gosnell MD Assistant Professor March 22, 2011 Most thyroid nodules are benign thyroid nodules occur in 77% of the world s population palpable
HYPOTHYROIDISM IN CHILDREN. IAP UG Teaching slides
 HYPOTHYROIDISM IN CHILDREN 1 OBJECTIVES Introduction Congenital hypothyroidism Etiology, clinical features, diagnosis, approach, treatment and prognosis Acquired hypothyroidism Etiology, clinical features,
HYPOTHYROIDISM IN CHILDREN 1 OBJECTIVES Introduction Congenital hypothyroidism Etiology, clinical features, diagnosis, approach, treatment and prognosis Acquired hypothyroidism Etiology, clinical features,
Graves Disease in Pediatrics
 Graves Disease in Pediatrics Graves disease is a common cause of an overactive thyroid. It occurs in about 1 in 5000 children and teens. It occurs more often in females than males. This booklet is designed
Graves Disease in Pediatrics Graves disease is a common cause of an overactive thyroid. It occurs in about 1 in 5000 children and teens. It occurs more often in females than males. This booklet is designed
Southern Derbyshire Shared Care Pathology Guidelines. Hyperthyroidism
 Southern Derbyshire Shared Care Pathology Guidelines Hyperthyroidism Purpose of Guideline The management and referral criteria of patients with newly diagnosed hyperthyroidism. Background Hyperthyroidism
Southern Derbyshire Shared Care Pathology Guidelines Hyperthyroidism Purpose of Guideline The management and referral criteria of patients with newly diagnosed hyperthyroidism. Background Hyperthyroidism
Amiodarone Induced Thyrotoxicosis Treatment? (AIT)
") Amiodarone Induced Thyrotoxicosis Treatment? (AIT) Presentation of a Case Report Annelies Tonnelier Brigitte Velkeniers 14-12-2013 1 1. Background 1. Case report 2. Investigations 3. Diagnosis 4. Treatment
Amiodarone Induced Thyrotoxicosis Treatment? (AIT) Presentation of a Case Report Annelies Tonnelier Brigitte Velkeniers 14-12-2013 1 1. Background 1. Case report 2. Investigations 3. Diagnosis 4. Treatment
Six Things That Changed How I Manage Graves Disease
 Six Things That Changed How I Manage Graves Disease Anthony DeWilde, OD FAAO Kansas City VAMC 6 Things 1. Thyroid status 2. Pathogenesis 3. Ocular signs/symptoms 4. Labs 5. Smoking 6. Mental Health Graves
Six Things That Changed How I Manage Graves Disease Anthony DeWilde, OD FAAO Kansas City VAMC 6 Things 1. Thyroid status 2. Pathogenesis 3. Ocular signs/symptoms 4. Labs 5. Smoking 6. Mental Health Graves
Thyroid Disorders Towards a Healthy Endocrine System
 Thyroid Disorders Towards a Healthy Endocrine System What are Thyroid Disorders? The thyroid is a butterfly-shaped gland in the middle of the lower neck. Through the release of hormones, the thyroid regulates
Thyroid Disorders Towards a Healthy Endocrine System What are Thyroid Disorders? The thyroid is a butterfly-shaped gland in the middle of the lower neck. Through the release of hormones, the thyroid regulates
LESSON ASSIGNMENT. Thyroid, Antithyroid, and Parathyroid Preparations. After completing this lesson, you should be able to:
 LESSON ASSIGNMENT LESSON 7 Thyroid, Antithyroid, and Parathyroid Preparations. LESSON ASSIGNMENT Paragraphs 7-1 through 7-12. LESSON OBJECTIVES After completing this lesson, you should be able to: 7-1.
LESSON ASSIGNMENT LESSON 7 Thyroid, Antithyroid, and Parathyroid Preparations. LESSON ASSIGNMENT Paragraphs 7-1 through 7-12. LESSON OBJECTIVES After completing this lesson, you should be able to: 7-1.
Page 1. Understanding Common Thyroid Disorders. Cases. Topics Covered
 Cases Understanding Common Thyroid Disorders Douglas C. Bauer, MD UCSF Division of General Internal Medicine No Disclosures 66 yr old female with 1 yr of fatigue and lassitude and no findings except TSH=8.2,
Cases Understanding Common Thyroid Disorders Douglas C. Bauer, MD UCSF Division of General Internal Medicine No Disclosures 66 yr old female with 1 yr of fatigue and lassitude and no findings except TSH=8.2,
Hypothyroidism in pregnancy. Nor Shaffinaz Yusoff Azmi Jabatan Perubatan Hospital Sultanah Bahiyah Kedah
 Hypothyroidism in pregnancy Nor Shaffinaz Yusoff Azmi Jabatan Perubatan Hospital Sultanah Bahiyah Kedah Agenda 1. Epidemiology and clinical characteristics of maternal hypothyroidism 2. Prevention and
Hypothyroidism in pregnancy Nor Shaffinaz Yusoff Azmi Jabatan Perubatan Hospital Sultanah Bahiyah Kedah Agenda 1. Epidemiology and clinical characteristics of maternal hypothyroidism 2. Prevention and
Women s Health in General Practice Symposium 2015 Thyroid & Parathyroid Cases
 Women s Health in General Practice Symposium 2015 Thyroid & Parathyroid Cases Bill Fleming Epworth Freemasons Hospital 1 Common Endocrine Presentations anatomical problems thyroid nodule / goitre embryological
Women s Health in General Practice Symposium 2015 Thyroid & Parathyroid Cases Bill Fleming Epworth Freemasons Hospital 1 Common Endocrine Presentations anatomical problems thyroid nodule / goitre embryological
 Thyroid Hormones Exophthalmos GOITRE / GOITER Hyperthyroidism GOITRE / GOITER Endemic Goiter, a Hypertrophy of the Thyroid Gland Resulting from Iodine Deficiency ENDEMIC GOITRES: were common in Central
Thyroid Hormones Exophthalmos GOITRE / GOITER Hyperthyroidism GOITRE / GOITER Endemic Goiter, a Hypertrophy of the Thyroid Gland Resulting from Iodine Deficiency ENDEMIC GOITRES: were common in Central
Thyroid. Dr Jessica Triay November 2018
 Thyroid Dr Jessica Triay November 2018 Hypothyroidism in Pregnancy Clinical update: Hypothyroidism in Pregnancy Take home messages Additional evidence supportive for more relaxed TSH targets for those
Thyroid Dr Jessica Triay November 2018 Hypothyroidism in Pregnancy Clinical update: Hypothyroidism in Pregnancy Take home messages Additional evidence supportive for more relaxed TSH targets for those
NSC 830: Drugs Affecting the Thyroid BROOKE BENTLEY, PHD, APRN
 NSC 830: Drugs Affecting the Thyroid BROOKE BENTLEY, PHD, APRN Hypothalamus-Pituitary-Thyroid Hormone Axis TSH: Normal = 0.5-5 mu/l Free T4: 1.3-3.8 ng/dl 1 Hypothyroidism: Thyroid Agents Natural Health
NSC 830: Drugs Affecting the Thyroid BROOKE BENTLEY, PHD, APRN Hypothalamus-Pituitary-Thyroid Hormone Axis TSH: Normal = 0.5-5 mu/l Free T4: 1.3-3.8 ng/dl 1 Hypothyroidism: Thyroid Agents Natural Health