Research Article Imaging-Cytology Correlation of Thyroid Nodules with Initially Benign Cytology
|
|
|
- Millicent Fleming
- 5 years ago
- Views:
Transcription
1 International Endocrinology, Article ID , 8 pages Research Article Imaging-Cytology Correlation of Thyroid Nodules with Initially Benign Cytology Shin Hye Hwang, 1 Ji Min Sung, 2 Eun-Kyung Kim, 1 Hee Jung Moon, 1 and Jin Young Kwak 1 1 Department of Radiology, Research Institute of Radiological Science, Yonsei University College of Medicine, 50 Yonsei-ro, Seodaemun-gu, Seoul , Republic of Korea 2 Department of Biostatistics, Bundang CHA Medical Center, Graduate School of Health and Welfare, CHA University, Seongnam , Republic of Korea Correspondence should be addressed to Jin Young Kwak; docjin@yuhs.ac Received 8 June 2014; Revised 17 August 2014; Accepted 15 September 2014; Published 13 October 2014 Academic Editor: Emanuel Christ Copyright 2014 Shin Hye Hwang et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Objective. To determine the role of imaging-cytology correlation in reducing false negative results of fine-needle aspiration (FNA) at thyroid nodules. Methods. This retrospective study included 667 nodules 1 cm or larger in 649 patients diagnosed as benign at initial cytologic evaluation and that underwent follow-up ultrasound (US) or FNA following a radiologist s opinion on concordance between imaging and cytologic results. We compared the risk of malignancy of nodules classified into subgroups according to the initial US features and imaging-cytology correlation. Results. Among included nodules, 11 nodules were proven to be malignant (1.6%) in follow-up FNA or surgery. The malignancy rate was higher in nodules with suspicious US features (11.4%) than in nodules without suspicious US features (0.5%, P < 0.001). When a thyroid nodule had discordant US findings on image review after having benign FNA results, malignancy rate increased to 23.3%, significantly higher than that of nodules with suspicious US features (P < 0.001). However, no significant difference was found in the risk of malignancy between the nodules without suspicious US features (0.5%) and imaging-cytology concordant nodules (0.6%, P = 0.438). Conclusions. Repeat FNA can be effectively limited to patients with cytologically benign thyroid nodules showing discordance in imaging-cytology correlation after initial biopsy, which reduces unnecessary repeat aspirations. 1. Introduction Fine-needle aspiration (FNA) is the standard method used to determine treatment plans for thyroid nodules. Based on the Bethesda system, the most generally accepted system for reporting thyroid cytology, the benign category implies a less than 3% risk of malignancy [1]. Follow-up ultrasound (US) is recommended when the nodule has benign cytologic result [2]. Repeat FNA is recommended when a nodule shows significant growth or morphologic transformation with suspicious US features on follow-up [3, 4]. However, the practical risk of malignancy in nodules with benign cytology varies in each institute, ranging from 2% to 18% [5], and it has even been reported to have gone up to 62% [6]. Therefore, some investigators recommend routine repeat FNA for thyroid nodules with benign cytology [7, 8]. Considering cost-effectiveness and diagnostic value, repeat FNA has been considered when the nodule shows any suspicious feature on the initial US [9, 10]. However, known US features associated with malignancy show an extremely variable probability of malignancy [11]. Microcalcifications, marked hypoechogenicity, and irregular or spiculated margin show a high risk of malignancy, while solid composition and hypoechogenicity show a relatively low positive predictive value (PPV) [11 13]. Based on these results, each suspicious US feature may not be considered as an equal risk factor for malignancy. Radiologists specialized in breast imaging have been confronted with the same problem in the core needle biopsy of a breast lesion. Correlation of pathologic results with sonographic findings has been used in some institutions to
2 2 International Endocrinology 3119 thyroid nodules in 2866 patients undergoing FNA 43 thyroid nodules in 42 patients with history of prior FNA on the same nodule 3076 thyroid nodules in 2829 patients with benign cytologic results 1162 thyroid nodules in 1087 patients whose FNA results were not benign 1914 thyroid nodules in 1819 patients 713 thyroid nodules in 694 patients smaller than 1 cm 1201 thyroid nodules in 1169 patients 420 thyroid nodules in 413 patients whose surgical pathology, follow-up FNA, or follow-up US findings were not available 781 thyroid nodules in 761 patients 114 thyroid nodules in 112 patients without additional radiologist s report regarding imaging-cytologic correlation 667 thyroid nodules in 649 patients Figure 1: Flow chart of case enrollment. verify that the lesion was adequately sampled. Discordant benign breast nodules are recommended for rebiopsy to confirm the diagnosis. This approach was suggested owing to the wide range of false negative rates of this category [14]. Based on different malignancy rates of suspicious US features in thyroid nodules and considering approaching steps in management of breast lesions, we conjecture that an imagingcytology correlation can be a better diagnostic approach for patient management than initial US features in a thyroid nodule with benign cytology. Therefore, we investigated theroleofimaging-cytologycorrelationtoreducethefalse negative rates of cytology at thyroid nodules as compared with the use of initial US features. 2. Materials and Methods 2.1. Patients. The Institutional Review Board of the Severance Hospital approved of this retrospective study and required neither patient approval nor informed consent for our review of patients images and records. However, written informed consents were obtained from all patients for USguided FNAs (US-FNAs) prior to each procedure as a daily practice. Our institutional registry for the thyroid nodule was settled since 2006 including all patients with thyroid nodules who underwent US examinations and US-FNAs at our institution. From March 2006 to December 2006, 3119 consecutive thyroid nodules in 2866 patients underwent US- FNAs. Among them, we included 667 nodules in 649 patients (men, 83; women, 566), which fulfilled the following criteria: (a)theyhadnohistoryofpriorfnaonthesamenodule;(b) they were reported as benign (category II) in the initial FNA. Nodules reported as nondiagnostic, atypia or follicular lesions of undetermined significance, follicular neoplasm or suspicious for a follicular neoplasm, suspicious for malignancy, and malignant were excluded; (c) they were equal to or larger than 1 cm; (d) they underwent further evaluation such as follow-up US, follow-up FNA, or thyroid surgery. In nodules which had not underwent operation, determinative cytologic reports (category II or category VI) on follow-up US were used as standard reference. If a nodule decreased in size on follow-up US, the nodule was also included as a benign nodule; (e) there were available radiologic reports that included an additional radiologist s opinion about the concordance or discordance between imaging and cytologic results in postbiopsy correlation (Figure 1). Mean age of the patients was 49.1 years (range, years). Mean lesion size of the thyroid nodules was 20.7 mm (range, mm). Median follow-up of 601 nodules in 584 patients which were included based on followup FNA or US without surgical pathology was 1509 days from the date of initial FNA to the last followup (IQR, 1522 days; range, days). The other nodules were included based on their surgical pathology as a standard reference Imaging Methods and Analysis. All US examinations were performed using a 7 to 15 MHz linear array transducer (HDI 5000; Philips Medical Systems, Bothell, Wash) or a 5 to 12 MHz linear probe (iu22, Philips Medical Systems) by 1 of 5 board-certified radiologists with 1 to 12 years of experience in thyroid imaging. All US-FNAs were performed by the same radiologist who performed the US examinations. The nodule size was defined as the largest diameter on US. US features of all thyroid nodules that underwent US-FNAs were prospectively recorded by the previously described methods [19]. US features suspicious for malignancy were determined using previously published criteria from our institution: marked hypoechogenicity, microlobulated or irregular margin, microcalcifications, and taller than wider shape. When overall echogenicity of a nodule was darker than that of the surrounding strap muscle, it was defined as marked hypoechogenicity to differentiate it from hypoechogenicity based on the parenchymal echogenicity of the thyroid gland. Microlobulated margin meant that a nodule had many small lobular contours on the surface. Microcalcifications were defined as tiny hyperechoic foci either with or without acoustic shadowing. Only calcifications equal to or less than 1 mm in diameter were indicated. If microcalcifications were detected with macrocalcifications, the lesion was considered to have microcalcifications as a worrisome finding. If hyperechoic foci accompanied comet-tail artifacts on conventional US, they were considered as colloids [20]. An anteroposterior to transverse dimension ratio greater than 1 was defined as taller than wider shape US-Guided Fine-Needle Aspiration. US-FNAs were performed on either thyroid nodules with suspicious assessment or the largest nodule among nodules with probably benign
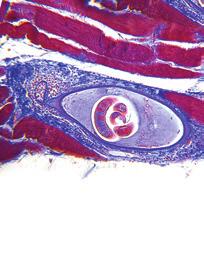
3 International Endocrinology 3 assessment on US. If there were multiple nodules with suspicious US findings in one patient or if the patient or physician requested a biopsy of a benign-looking nodule coexisting with a nodule showing suspicious US features, FNAswereperformedonmultiplenodulesinonepatient. A free-hand biopsy technique was used with either a 23- gauge needle attached to a 20 ml disposable plastic syringe and an aspirator or a 23-gauge needle attached to a 2 ml disposable plastic syringe, depending on the performing radiologist s preference. Each lesion was aspirated at least twice, and the aspirated materials were expelled onto a slide and immediately placed in 95% alcohol for Papanicolaou staining. The remaining materials were rinsed with saline and processed for cell blocking. The cytopathologist was not on site during the biopsy. Five cytopathologists interpreted the slides. Additional special staining was performed according totherequirementofthecytopathologist.aninadequate specimen was defined as less than 6 groups of cells containing more than 10 cells [3]. Adequate specimens were categorized as benign, indeterminate, suspicious for malignancy, or malignant samples Imaging-Cytology Correlation and Postaspiration Management. The radiologist who performed FNA routinely reviewed the initial US images within a week of the FNA after the cytologic results were reported. For benign cytologic results, radiologists who performed the US-FNAs decided and reported whether the cytology was concordant or discordant with the imaging findings. As researchers at our institution always try to assess lesions based on their most worrisome finding, the saved images should represent these worrisome US features. Image-cytology correlation was done based on these images. The final conclusion was not derived from the number of suspicious US features but from the subjective decision made by the radiologist who performed the US-FNA. In our institution, concordant lesions included some nodules which had suspicious US features on the initial US but were acceptable for the benign cytology in postbiopsy image review as well as the nodules without features suspicious for malignancy on the initial US. Concordant benign thyroid nodules were recommended for follow-up by US after one year. In contrast, discordant lesions included nodules which were initially suspected for malignancy on US and were still thought to be suspicious for cancer even after obtaining benign cytology. Repeat FNAs were usually recommended for discordant benign thyroid nodules after 6 12 months [21]. Among the 667 nodules that met all the inclusion criteria, 586 nodules (87.9%, 586 of 667) were reviewed by radiologists who had more than three years of experience in thyroid imaging and FNA whereas the remaining nodules were managed by less experienced radiologist Statistical Analysis. We compared the clinical characteristics of patients between benign and malignant nodules by using the χ 2 test for categorical variables and independent t-test for continuous variables. We also compared the risk of malignancy as well as the clinical characteristics between concordant and discordant nodules by using χ 2 or Fisher s exact test for categorical variables and independent t-test for continuous variables. The baseline characteristics were also compared between patients with included and excluded nodules among thyroid nodules equal to or larger than 1 cm with the same methods. The risk of malignancy was calculated for several subgroups classified according to initial US features and imagingcytology concordance. Using the generalized estimating equation, we compared the risk of malignancy in thyroid nodules with initially benign cytologic results with those of the remaining subgroups and also compared the risk of malignancy of thyroid nodules among subgroups. Significance was assumed when the two-sided P value was less than.05. Logistic regression analysis was performed to assess the odds ratio for the risk of malignancy. Odds ratios with relative 95% confidence intervals (CIs) were also calculated. Statistical analysis was performed using commercial statistical software (SAS version 9.1, SAS Inc., Cary, NC, USA). 3. Results Among 667 nodules with initially benign cytologic results, 656 nodules were benign (98.4%) and 11 nodules were malignant (1.6%) based on cytopathology (Table 1). The mean age of patients with malignant nodules was not significantly different from that of patients with benign nodules (P = 0.277). Gender of patients was not associated with malignancy (P = 0.734). The mean size of malignant nodules (17.6 ± 12.5 mm) was not significantly different from that of benign nodules (20.7 ± 10.1 mm, P = 0.315). There were 70 nodules with initial suspicious US features and 597 nodules without initial suspicious US features. The risk of malignancy was higher in nodules with initial suspicious US features (11.4%, 8 of 70) than in nodules without initial suspicious US features (0.5%, 3 of 597; P < 0.001, Table 1). When reviewing US images after initial FNA results were reported, 40 out of 70 nodules which had suspicious features on initial US evaluation were finally concluded as concordant with benign cytology (Figures 2 and 3). Therefore, in 667 nodules with benign cytology, 637 nodules were concordant with cytology, whereas 30 nodules were discordant with benign cytology.thereasonsthat40noduleswithrevisedradiologic diagnosis after imaging-cytologic correlation were initially classified as suspicious nodules were microcalcifications (n = 16), microlobulated or irregular margin (n = 9), tallerthan wider shape (n = 3), or marked hypoechogenicity(n = 1) in order of frequency, respectively, and more than one characteristic of the above features in 11 nodules. Between the concordant and discordant group, gender of the patients was not significantly different (P = 0.159). Thepatients with discordant nodules were significantly older than other patients with concordant nodules (53.5 ± 10.5 years versus 48.9 ± 12.0 years; P = 0.038). The mean size of discordant nodules was significantly smaller than that of concordant nodules (16.0±6.6 mm versus 20.9±10.2 mm;p < 0.001). The rate of malignancy was significantly higher in the discordant group (23. 3%; 7 of 30) than in the concordant group (0.6%, 4of637;P < 0.001).
 1 (9.1) Female 574 (87.5) 10 (90.9) Mean nodule size (mm) 20.7 ± 10.1 17.6 ± 12.5 0.315 US final assessment before FNA <0.")
 (b) Figure 2: Initially suspicious but concordant nodule after imaging-cytology correlation.")


4 4 International Endocrinology Table 1: Baseline characteristics of 667 thyroid nodules with benign cytology. Reference standard Benign Malignant P value Number of nodules Mean age (years) 49.1 ± ± Gender Male 82 (12.5) 1 (9.1) Female 574 (87.5) 10 (90.9) Mean nodule size (mm) 20.7 ± ± US final assessment before FNA <0.001 Probably benign 594 (90.5) 3 (27.3) Suspicious malignant 62 (9.5) 8 (72.7) FNA: fine-needle aspiration. Data in parentheses are percentages. Data are the means ± standard deviations. (a) (b) Figure 2: Initially suspicious but concordant nodule after imaging-cytology correlation. US scans ((a) transverse; (b) longitudinal) in a 41- year-old female without remarkable medical history show a 16 mm sized predominantly solid mass (arrows) with microlobulated margin in the lower pole of the right lobe of the thyroid gland. The nodule was taller than wider on transverse scan. The initial cytologic result was adenomatous hyperplasia which was concordant with US findings considering relatively low PPV of these US finding in imaging-cytology correlation after biopsy. A follow-up US was recommended and nodule size gradually decreased from 16 mm to 13 mm with decrease of the cystic portion in follow-up US evaluations until July 2013 without any other significant changes in US features. (a) (b) Figure 3: Initially suspicious but concordant nodule after imaging-cytology correlation. US scans ((a) transverse; (b) longitudinal) in a 54- year-old female without remarkable medical history show a 12 mm sized solid mass (arrows) with internal echogenic foci in the lower pole of the right lobe of the thyroid gland. The initial cytologic result was adenomatous hyperplasia which was concordant with US findings in imaging-cytology correlation after biopsy. At the time of imaging-cytology correlation, the echogenic foci (arrowheads) were thought to be related to colloids instead of microcalcifications from psammoma bodies. She underwent surgery (left total and right subtotal thyroidectomy) due to papillary carcinoma in the contralateral lobe of the thyroid gland. The mass in the right lobe was finally confirmed as adenomatous hyperplasia on pathology. About 44.5% (534 of 1201) of 1 cm or larger nodules with benign cytology in initial FNA were excluded because they had neither standard reference, such as follow-up US, followup FNA, or thyroid surgery, nor available radiologist s additional reports regarding imaging-cytologic correlation. The mean age of patients with included nodules was statistically different from the other patients (49.1±12.0 versus 50.7±13.1 years; P = 0.033). Patient gender (P = 0.392) and mean nodule size (P = 0.601) were not significantly different between included and excluded nodules. There were 60
5 International Endocrinology 5 Table 2: Comparison of baseline characteristics of nodules according to inclusion criteria among 1 cm or larger 1201 thyroid nodules with benign cytology. Included nodules Excluded nodules P value Number of nodules Mean age (years) 49.1 ± ± Gender Male 83 (12.4) 76 (14.2) Female 584 (87.6) 458 (85.8) Mean nodule size (mm) 20.7 ± ± US final assessment Probably benign 597 (89.5) 474 (88.8) Suspicious malignant 70 (10.5) 60 (11.2) Data in parentheses are percentages. Data are the means ± standard deviations. Table 3: Risk of malignancy according to initial US features and imaging-cytologic correlation in thyroid nodules with benign cytologic results. Number of nodules Number of malignant nodules Risk of malignancy (%) Benign cytology alone (0.8, 2.9) Initial no suspicious US (0.1, 1.5) Initial suspicious US (5.1, 21.3) Concordant lesiontobenign cytologyinpostbiopsycorrelation (0.2, 1.6) Discordant lesiontobenign cytology inpostbiopsycorrelation (9.9, 42.3) Data in parentheses are 95% confidence intervals. nodules with suspicious findings in the initial US evaluation of excluded nodules (11.2%, 60 of 534), and the proportion was not significantly different from that of included nodules (10.5%, 70 of 667; Table 2). When comparing the risk of malignancy between benign cytology alone and each subgroup by a combination of benign cytology with initial US findings or postbiopsy concordance, all combinations had significantly different risk values from cytology alone (Table 3, Figure 4). Also, when comparing the risk of malignancy between discordant lesions and lesions with suspicious features on initial US, the former (23.3%, 7 of 30) was significantly higher than the latter (11.4%, 8 of 70). However, there was no significant difference in the risk of malignancy between concordant lesions (0.6%, 4 of 637) and lesions without suspicious features on initial US (0.5%, 3 of 597; P = 0.438)(Figure 4). 4. Discussion Although FNA is a widely used tool for the diagnosis of thyroid nodules, the most significant problem it has is false negative results which bring out misses and delays in treatmentof the cancer [22]. Errors in cytologic reports have arisen from the overinterpretation of nondiagnostic specimens as diagnostic ones [23, 24]. Therefore, many reports discussed the differentiation of a nondiagnostic specimen from a diagnostic one in the cytologic interpretation of thyroid FNA [1, 3]. Diagnostic errors of thyroid FNA can Rate of malignancy (%) % Benign cytology alone (11 of 667) P = P = Initial no suspicious US (3 of 597) P = % 0.6% Concordant lesion to benign cytology in postbiopsy correlation (4 of 637) Initial suspicious US (8 of 70) 11.4% 23.3% Discordant lesion to benign cytology in postbiopsy correlation (7 of 30) Figure 4: Comparison of malignancy rates in thyroid nodules with benign cytology according to initial US features or imagingcytology concordance. Error bars for 95% confidence intervals. P value < Concordant lesions include some nodules which had suspicious US features on initial US but were acceptable for benign cytology in postbiopsy image review as well as nodules without suspicious US features on initial US. Discordant lesions include nodules which were initially suspected for malignancy on US and were still regarded as suspicious even after obtaining benign cytology.
6 6 International Endocrinology Table 4: Reported rate of malignancy in nodules with benign cytology according to US finding. Total number of nodules Rate of malignancy (%) Overall Suspicious US No suspicious US Kwak et al. [9] (26/1343) 20.4 (19/93) 0.6 (7/1250) Koike et al. [15] (20/168) 47.1 (8/17) 7.9 (12/151) Lee et al. [16] (6/560) 3.7 (4/108) 0.4 (2/452) Maia et al. [17] (10/35) 38.5 (5/13) 22.7 (5/22) Choi et al. [18] (12/700) 4.7 (8/169) 0.8 (4/531) Data in parentheses are numbers used to calculate percentages. Multicenter study from 7 university-affiliated hospitals. Suspicious US features Marked hypoechogenicity, microlobulated or irregular margin, microcalcification, and taller than wider shape Ill-defined margin, irregular shape, solid echo structure, heterogeneous internal echogenicity, hypoechogenicity, presence of calcification, absence of halo, and invasion of adjacent organs Marked hypoechogenicity, microlobulated or irregular margin, microcalcification, and taller than wider shape Hypoechogenicity, microcalcification, border irregularity, and central flow by Doppler study Marked hypoechogenicity, not well-defined margin, microcalcifications, and taller than wide shape also be caused by the mistakes of cytopathologists and the inherent nature of thyroid nodules due to overlapping cytologic criteria among hyperplastic adenomatoid nodule in goiter, follicular adenoma, well-differentiated follicular carcinoma, and follicular variant of papillary carcinoma [25]. Moreover, reported false negative rates are variable among institutions and operators due to variable sampling skills [5, 6]. Several guidelines recommend follow-up US in thyroid nodules with benign cytology unless the nodule shows significant growth or morphologic change in follow-up US [1, 3, 4]. However, it has been argued that follow-up might be not enough in some nodules because of the inevitable falsenegativediagnosisandthepossibleriskofdelayed treatment [6, 22].Toreducefalsenegativeresultsofthyroid FNAs, there have been two suggested approaches; first, routine repeat FNA in thyroid nodules with benign cytology [26, 27] and,second,selectiverepeatfna[8, 10, 28, 29]. Intheaspectofcost-effectiveness,itismorerationalto consider performing follow-up FNA selectively for nodules with a high-risk of malignancy rather than performing a total inspection of cytologically benign nodules in initial FNA. Basedonseveralreports,therateofmalignancyinbenign thyroid nodules with suspicious US features was % which was significantly higher than that of benign thyroid nodules without suspicious US features (Table 4)[9, 15 18]. Although the US criteria applied to each study had subtle differences, initial US features may be reliable factors in determining whether to repeat FNA or not [17]. Going one step further from simply matching cytologic results against imaging findings evaluated before biopsy, the postbiopsy correlation of US features with cytologic results could be an alternative in determining whether the nodule should be reaspirated to confirm its cytology or not. Imaging-pathologic correlation after biopsy has been found to be useful in validating biopsy results of breast lesions, and discordance has been suggested as an indication for excision because of its higher upgrade rate than that of concordant lesions [30 32]. However, there has been no organized study that applies imaging-cytology correlation to patient management and considers how to accept results of postbiopsy correlation in regard to reducing false negative diagnosis in thyroid nodules. In this study, 1.6% of nodules with benign cytology in initial FNA were finally proven to be malignant. As expected, the malignancy rate of thyroid nodules (11.4%) with suspicious features on initial US was significantly higher than that of nodules (0.5%) without suspicious features on initial US, and the malignancy rate of nodules (23.3%) with discordant imaging findings was also significantly higher compared to concordant nodules (0.6%) in postbiopsy imaging-cytologic correlations. Furthermore, the rate of malignancy was higher in the nodules showing imaging-cytology discordance compared to nodules showing suspicious feature on the initial US. However, there was no significant difference in the risk of malignancy between concordant nodules in postbiopsy correlation and nodules without suspicious features on initial US. This result lets us conclude that imaging-cytology
7 International Endocrinology 7 correlation is a more effective approach than using initial US features alone when deciding follow-up management in patients with cytologically benign thyroid nodules without a statistical increase in missing malignancy. In this study, 40 of 70 nodules with suspicious features on initial US were determined as concordant with benign cytology after postbiopsy imaging-cytology correlation. This change can be explained by the subjective nature of US evaluation. Although many descriptions of each suspicious US feature are present, interobserver and intraobserver variability still exist for the US assessment of thyroid nodules. Among US characteristics, margin and calcification showed relatively less consistency between observers [33] and nodules in most patients whose radiologic assessments were changed after obtaining benign cytology were initially assumed as suspicious nodule due to calcification (16 of 40), margin (9 of 40), or multiple features (11 of 40) including them in our study. Also, there have been difficulties in deciding whether a thyroid nodule shows echogenic spots on US. Echogenic spots can be due to microcalcifications related to cancer or crystals related to colloids [34]. Therefore, postbiopsy imaging-cytology correlation can be a good diagnostic approach in deciding whether to repeat FNA or not at a thyroid nodule with benign cytology. There were several limitations to this study. First, some nodules were excluded in analysis despite having benign cytologic results due to loss of follow-up and absence of additional reports. Selection bias may be unavoidable. However, the initial US assessment was not significantly different between included nodules and excluded nodules which were 1 cm or larger with benign cytology in the initial FNA. Second, interobserver and intraobserver variability among radiologists are possible in the interpretation of US images and among cytologists, especially when reviewing follicular lesions. Third, there might be a bias arising from the postbiopsy review process itself which was based on saved images instead of on a review in real-time US. Although we always tried to save any images showing worrisome US findings and the postbiopsy review was preferably done within a week of biopsy by the performer, an observer bias might not have been completely removed from the final results. Fourth, suspicious US features such as calcification, margin, vascularity, and echogenicity have been differently applied to thyroid nodules by various guidelines and different institutions. Therefore, the result of this study needs to be validated in other institutions. Fifth, most (87.9%) of the nodules in this study were reviewed by highly experienced radiologists in thyroid imaging. Therefore, the results may not be reproducible in other institutions. 5. Conclusions Repeat FNA can be effectively limited to patients with cytologically benign thyroid nodules showing discordance in imaging-cytology correlation, which reduces unnecessary repeat aspirations as well as decreasing false negative results. Conflict of Interests The authors have no conflict of interests. References [1] E. S. Cibas and S. Z. Ali, The bethesda system for reporting thyroid cytopathology, Thyroid, vol. 19, no. 11, pp , [2] L. J. Layfield, J. Abrams, B. Cochand-Priollet et al., Postthyroid FNA testing and treatment options: a synopsis of the national cancer institute thyroid fine needle aspiration state of the science conference, Diagnostic Cytopathology, vol. 36, no. 6, pp ,2008. [3] D. S. Cooper, G. M. Doherty, B. R. Haugen et al., Revised American thyroid association management guidelines for patients with thyroid nodules and differentiated thyroid cancer, Thyroid,vol.19,no.11,pp ,2009. [4] H. Gharib, E. Papini, R. Paschke et al., American Association of Clinical Endocrinologists, Associazione Medici Endocrinologi, and European Thyroid Association medical guidelines for clinical practice for the diagnosis and management of thyroid nodules: executive summary of recommendations, Endocrinological Investigation, vol. 33, supplement 5, pp , [5] C.-C. C. Wang, L. Friedman, G. C. Kennedy et al., A large multicenter correlation study of thyroid nodule cytopathology and histopathology, Thyroid, vol. 21, no. 3, pp , [6] K.A.Al-Hureibi,A.A.Al-Hureibi,Y.A.Abdulmughni,S.M. Aulaqi,M.S.Salman,andE.M.Al-Zooba, Thediagnostic value of fine needle aspiration cytology in thyroid swellings in a University Hospital, Yemen, Saudi Medical Journal, vol. 24, no. 5,pp ,2003. [7] F. Gabalec, J. Čáp,A.Ryška, T. Vašátko, and V. Ceeová, Benign fine-needle aspiration cytology of thyroid nodule: to repeat or not to repeat? European Endocrinology, vol.161,no. 6, pp , [8]J.M.Chehade,A.B.Silverberg,J.Kim,C.Case,andA.D. Mooradian, Role of repeated fine-needle aspiration of thyroid nodules with benign cytologic features, Endocrine Practice,vol. 7, no. 4, pp , [9] J. Y. Kwak, H. Koo, J. H. Youk et al., Value of US correlation of a thyroid nodule with initially benign cytologic results, Radiology,vol.254,no.1,pp ,2010. [10] J. van Roosmalen, B. van Hemel, A. Suurmeijer et al., Diagnostic value and cost considerations of routine fine-needle aspirations in the follow-up of thyroid nodules with benign readings, Thyroid, vol. 20,no. 12,pp , [11] M. C. Frates, C. B. Benson, J. W. Charboneau et al., Management of thyroid nodules detected at US: society of radiologists in ultrasound consensus conference statement, Radiology,vol. 237, no. 3, pp , [12] J. Y. Kwak, K. H. Han, J. H. Yoon et al., Thyroid imaging reporting and data system for us features of nodules: a step in establishing better stratification of cancer risk, Radiology, vol. 260, no. 3, pp , [13] J.Y.Kwak,I.Jung,J.H.Baeketal., Thyroidimagingreporting and data system for ultrasound features of thyroid nodules: multicentric korean retrospective study, Korean Radiology, vol. 14, no. 1, pp , [14] L. W. Bassett, M. C. Mahoney, and S. K. Apple, Interventional breast imaging: current procedures and assessing for concordance with pathology, Radiologic Clinics of North America,vol. 45,no.5,pp ,2007. [15] E. Koike, H. Yamashita, S. Noguchi et al., Effect of combining ultrasonography and ultrasound-guided fine-needle aspiration
8 8 International Endocrinology biopsy findings for the diagnosis of thyroid nodules, European Surgery,vol.167,no.9,pp ,2001. [16]M.-J.Lee,S.W.Hong,W.Y.Chung,J.Y.Kwak,M.J.Kim, and E.-K. Kim, Cytological results of ultrasound-guided fineneedle aspiration cytology for thyroid nodules: emphasis on correlation with sonographic findings, Yonsei Medical Journal, vol. 52, no. 5, pp , [17]F.F.R.Maia,P.S.Matos,E.J.Pavin,J.Vassallo,andD.E. Zantut-Wittmann, Value of repeat ultrasound-guided fineneedle aspiration in thyroid nodule with a first benign cytologic result: impact of ultrasound to predict malignancy, Endocrine, vol. 40, no. 2, pp , [18] Y. J. Choi, I. Jung, S. J. Min et al., Thyroid nodule with benign cytology: is clinical follow-up enough? PLoS ONE, vol.8,no. 5, Article ID e63834, [19] E.-K. Kim, S. P. Cheong, Y. C. Woung et al., New sonographic criteria for recommending fine-needle aspiration biopsy of nonpalpable solid nodules of the thyroid, The American Journal of Roentgenology,vol.178,no.3,pp ,2002. [20] L. Anderson, W. D. Middleton, S. A. Teefey et al., Hashimoto thyroiditis: part 1, sonographic analysis of the nodular form of Hashimoto thyroiditis, The American Roentgenology, vol.195,no.1,pp ,2010. [21] W.-J. Moon, J. H. Baek, S. L. Jung et al., Ultrasonography and the ultrasound-based management of thyroid nodules: consensus statement and recommendations, Korean Radiology,vol.12,no.1,pp.1 14,2011. [22] M. W. Yeh, O. Demircan, P. Ituarte, and O. H. Clark, Falsenegative fine-needle aspiration cytology results delay treatment and adversely affect outcome in patients with thyroid carcinoma, Thyroid,vol.14,no.3,pp , [23] R. Bakhos, S. M. Selvaggi, S. DeJong et al., Fine-needle aspiration of the thyroid: rate and causes of cytohistopathologic discordance, Diagnostic Cytopathology, vol.23,no.4,pp , [24] S. S. Raab, C. M. Vrbin, D. M. Grzybicki et al., Errors in thyroid gland fine-needle aspiration, The American Clinical Pathology,vol.125,no.6,pp ,2006. [25] M. K. Sidawy, D. M. del Vecchio, and S. M. Knoll, Fine-needle aspiration of thyroid nodules: correlation between cytology and histology and evaluation of discrepant cases, Cancer,vol.81,no. 4, pp , [26]M.B.Flanagan,N.P.Ohori,S.E.Carty,andJ.L.Hunt, Repeat thyroid nodule fine-needle aspiration in patients with initial benign cytologic results, The American Clinical Pathology,vol.125,no.5,pp ,2006. [27] Y. C. Oertel, L. Miyahara-Felipe, M. G. Mendoza, and K. Yu, Value of repeated fine needle aspirations of the thyroid: an analysis of over ten thousand FNAs, Thyroid, vol. 17,no. 11,pp , [28] A. Lucas, M. Llatjos, I. Salinas, J. Reverter, E. Pizarro, and A. Sanmarti, Fine-needle aspiration cytology of benign nodular thyroid disease. Value of re-aspiration, European Endocrinology,vol.132,no.6,pp ,1995. [29] S. H. Merchant, R. Izquierdo, and K. K. Khurana, Is repeated fine-needle aspiration cytology useful in the management of patients with benign nodular thyroid disease? Thyroid,vol.10, no. 6, pp , [30] V. I. Shah, U. Raju, D. Chitale, V. Deshpande, N. Gregory, and V. Strand, False-negative core needle biopsies of the breast: an analysis of clinical, radiologic, and pathologic findings in 27 consecutive cases of missed breast cancer, Cancer, vol. 97, no. 8, pp , [31] J. H. Youk, E. K. Kim, M. J. Kim et al., Concordant or discordant? Imaging-pathology correlation in a sonographyguided core needle biopsy of a breast lesion, Korean Radiology,vol.12,no.2,pp ,2011. [32] E. J. Son, E.-K. Kim, J. H. Youk, M. J. Kim, J. Y. Kwak, and S. H. Choi, Imaging-histologic discordance after sonographically guided percutaneous breast biopsy: a prospective observational study, Ultrasound in Medicine and Biology, vol. 37, no. 11, pp , [33] S. J. Park, S. H. Park, Y. J. Choi et al., Interobserver variability and diagnostic performance in US assessment of thyroid nodule according to size, Ultraschall in der Medizin, vol. 33, no. 7, pp. E186 E190, [34] P. Jun, L. C. Chow, and R. B. Jeffrey, The sonographic features of papillary thyroid carcinomas: pictorial essay, Ultrasound Quarterly,vol.21,no.1,pp.39 45,2005.










9 MEDIATORS of INFLAMMATION The Scientific World Journal Gastroenterology Research and Practice Diabetes Research International Endocrinology Immunology Research Disease Markers Submit your manuscripts at BioMed Research International PPAR Research Obesity Ophthalmology Evidence-Based Complementary and Alternative Medicine Stem Cells International Oncology Parkinson s Disease Computational and Mathematical Methods in Medicine AIDS Behavioural Neurology Research and Treatment Oxidative Medicine and Cellular Longevity
Imaging-cytology correlation of thyroid nodules with initially benign cytology
 Imaging-cytology correlation of thyroid nodules with initially benign cytology Poster No.: C-1815 Congress: ECR 2013 Type: Scientific Exhibit Authors: S. H. Hwang, E.-K. Kim, J. Y. Kwak; Seoul/KR Keywords:
Imaging-cytology correlation of thyroid nodules with initially benign cytology Poster No.: C-1815 Congress: ECR 2013 Type: Scientific Exhibit Authors: S. H. Hwang, E.-K. Kim, J. Y. Kwak; Seoul/KR Keywords:
Repeat Ultrasound-Guided Fine-Needle Aspiration for Thyroid Nodules 10 mm or Larger Can Be Performed 10.7 Months After Initial Nondiagnostic Results
 Neuroradiology/Head and Neck Imaging Original Research Moon et al. Repeat US-Guided FNA of Thyroid Nodules After Nondiagnostic Results Neuroradiology/Head and Neck Imaging Original Research Hee Jung Moon
Neuroradiology/Head and Neck Imaging Original Research Moon et al. Repeat US-Guided FNA of Thyroid Nodules After Nondiagnostic Results Neuroradiology/Head and Neck Imaging Original Research Hee Jung Moon
Sonographic Differentiation of Thyroid Nodules With Eggshell Calcifications
 Article Sonographic Differentiation of Thyroid Nodules With Eggshell Calcifications Byung Moon Kim, MD, Min Jung Kim, MD, Eun-Kyung Kim, MD, Jin Young Kwak, MD, Soon Won Hong, MD, Eun Ju Son, MD, Ki Hwang
Article Sonographic Differentiation of Thyroid Nodules With Eggshell Calcifications Byung Moon Kim, MD, Min Jung Kim, MD, Eun-Kyung Kim, MD, Jin Young Kwak, MD, Soon Won Hong, MD, Eun Ju Son, MD, Ki Hwang
Papillary Thyroid Carcinoma Manifested Solely as Microcalcifications on Sonography
 Sonography of Papillary Thyroid Carcinoma Head and Neck Imaging Clinical Observations Jin Young Kwak 1 Eun-Kyung Kim 1 Eun Ju Son 1 Min Jung Kim 1 Ki Keun Oh 1 Ji Young Kim 2 Kwang Il Kim 2 Kwak JY, Kim
Sonography of Papillary Thyroid Carcinoma Head and Neck Imaging Clinical Observations Jin Young Kwak 1 Eun-Kyung Kim 1 Eun Ju Son 1 Min Jung Kim 1 Ki Keun Oh 1 Ji Young Kim 2 Kwang Il Kim 2 Kwak JY, Kim
Research Article Does Tumor Size Influence the Diagnostic Accuracy of Ultrasound-Guided Fine-Needle Aspiration Cytology for Thyroid Nodules?
 International Endocrinology Volume 2016, Article ID 3803647, 6 pages http://dx.doi.org/10.1155/2016/3803647 Research Article Does Tumor Size Influence the Diagnostic Accuracy of Ultrasound-Guided Fine-Needle
International Endocrinology Volume 2016, Article ID 3803647, 6 pages http://dx.doi.org/10.1155/2016/3803647 Research Article Does Tumor Size Influence the Diagnostic Accuracy of Ultrasound-Guided Fine-Needle
Korean Thyroid Imaging Reporting and Data System features of follicular thyroid adenoma and carcinoma: a single-center study
 Korean Thyroid Imaging Reporting and Data System features of follicular thyroid adenoma and carcinoma: a single-center study Jung Won Park 1, Dong Wook Kim 1, Donghyun Kim 1, Jin Wook Baek 1, Yoo Jin Lee
Korean Thyroid Imaging Reporting and Data System features of follicular thyroid adenoma and carcinoma: a single-center study Jung Won Park 1, Dong Wook Kim 1, Donghyun Kim 1, Jin Wook Baek 1, Yoo Jin Lee
Differentiation of Thyroid Nodules With Macrocalcifications
 CME Article Differentiation of Thyroid Nodules With Macrocalcifications Role of Suspicious Sonographic Findings Min Jung Kim, MD, Eun-Kyung Kim, MD, Jin Young Kwak, MD, Cheong Soo Park, MD, Woong Youn
CME Article Differentiation of Thyroid Nodules With Macrocalcifications Role of Suspicious Sonographic Findings Min Jung Kim, MD, Eun-Kyung Kim, MD, Jin Young Kwak, MD, Cheong Soo Park, MD, Woong Youn
Warinthorn Phuttharak*, Charoonsak Somboonporn, Gatenapa Hongdomnern
 Colour Doppler Ultrasonography in the Diagnosis of Malignancy in Thyroid Nodules RESEARCH COMMUNICATION Diagnostic Performance of Gray-scale versus Combined Grayscale with Colour Doppler Ultrasonography
Colour Doppler Ultrasonography in the Diagnosis of Malignancy in Thyroid Nodules RESEARCH COMMUNICATION Diagnostic Performance of Gray-scale versus Combined Grayscale with Colour Doppler Ultrasonography
Repeat Thyroid Nodule Fine-Needle Aspiration in Patients With Initial Benign Cytologic Results
 Anatomic Pathology / REPEAT THYROID FINE-NEEDLE ASPIRATION Repeat Thyroid Nodule Fine-Needle Aspiration in Patients With Initial Benign Cytologic Results Melina B. Flanagan, MD, MSPH, 1 N. Paul Ohori,
Anatomic Pathology / REPEAT THYROID FINE-NEEDLE ASPIRATION Repeat Thyroid Nodule Fine-Needle Aspiration in Patients With Initial Benign Cytologic Results Melina B. Flanagan, MD, MSPH, 1 N. Paul Ohori,
European Journal of Radiology
 European Journal of Radiology 82 (2013) 321 326 Contents lists available at SciVerse ScienceDirect European Journal of Radiology jo ur n al hom epage: www.elsevier.com/locate/ejrad Ultrasonographic criteria
European Journal of Radiology 82 (2013) 321 326 Contents lists available at SciVerse ScienceDirect European Journal of Radiology jo ur n al hom epage: www.elsevier.com/locate/ejrad Ultrasonographic criteria
Thyroid Nodules: US Risk Stratification and FNA Guidelines
 Thyroid Nodules: US Risk Stratification and FNA Guidelines Mark A. Lupo, MD, FACE, ECNU Thyroid & Endocrine Center of Florida Assistant Clinical Professor of Medicine Florida State University, College
Thyroid Nodules: US Risk Stratification and FNA Guidelines Mark A. Lupo, MD, FACE, ECNU Thyroid & Endocrine Center of Florida Assistant Clinical Professor of Medicine Florida State University, College
Downloaded from by John Hanna on 11/09/15 from IP address Copyright ARRS. For personal use only; all rights reserved
 Neuroradiology/Head and Neck Imaging Original Research Zhu et al. Ultrasound Versus Afirma Testing of FNA-Indeterminate Thyroid Nodules Neuroradiology/Head and Neck Imaging Original Research Qing-Li Zhu
Neuroradiology/Head and Neck Imaging Original Research Zhu et al. Ultrasound Versus Afirma Testing of FNA-Indeterminate Thyroid Nodules Neuroradiology/Head and Neck Imaging Original Research Qing-Li Zhu
Sonographic differentiation of benign and malignant thyroid nodules: Prospective study
 Sonographic differentiation of benign and malignant thyroid nodules: Prospective study Poster No.: C-1720 Congress: ECR 2010 Type: Scientific Exhibit Topic: Head and Neck Authors: D. W. Kim, Y. H. Lee;
Sonographic differentiation of benign and malignant thyroid nodules: Prospective study Poster No.: C-1720 Congress: ECR 2010 Type: Scientific Exhibit Topic: Head and Neck Authors: D. W. Kim, Y. H. Lee;
US-FNA is an easy-to-use and accurate tool for evaluating
 Published September 15, 2011 as 10.3174/ajnr.A2686 ORIGINAL RESEARCH D.W. Kim E.J. Lee S.J. Jung J.H. Ryu Y.M. Kim Role of Sonographic Diagnosis in Managing Bethesda Class III Nodules BACKGROUND AND PURPOSE:
Published September 15, 2011 as 10.3174/ajnr.A2686 ORIGINAL RESEARCH D.W. Kim E.J. Lee S.J. Jung J.H. Ryu Y.M. Kim Role of Sonographic Diagnosis in Managing Bethesda Class III Nodules BACKGROUND AND PURPOSE:
Thyroid Nodules with Macrocalcification: Sonographic Findings Predictive of Malignancy
 Original Article http://dx.doi.org/10.3349/ymj.2014.55.2.339 pissn: 0513-5796, eissn: 1976-2437 Yonsei Med J 55(2):339-344, 2014 Thyroid Nodules with Macrocalcification: Sonographic Findings Predictive
Original Article http://dx.doi.org/10.3349/ymj.2014.55.2.339 pissn: 0513-5796, eissn: 1976-2437 Yonsei Med J 55(2):339-344, 2014 Thyroid Nodules with Macrocalcification: Sonographic Findings Predictive
of Thyroid Lesions Comet Tail Crystals
 2 Ultrasound Features of Thyroid Lesions There are many different features indicating a certain benign or malignant tumor type, but many of these are overlapping signs. Combining several features is considered
2 Ultrasound Features of Thyroid Lesions There are many different features indicating a certain benign or malignant tumor type, but many of these are overlapping signs. Combining several features is considered
Neuroradiology/Head and Neck Imaging Original Research
 Neuroradiology/Head and Neck Imaging Original Research Hobbs et al. FNA of Thyroid Nodules Neuroradiology/Head and Neck Imaging Original Research Hasan A. Hobbs 1 Manisha Bahl 1 Rendon C. Nelson 1,2 James
Neuroradiology/Head and Neck Imaging Original Research Hobbs et al. FNA of Thyroid Nodules Neuroradiology/Head and Neck Imaging Original Research Hasan A. Hobbs 1 Manisha Bahl 1 Rendon C. Nelson 1,2 James
Evaluation of thyroid nodules: prediction and selection of malignant nodules for FNA (cytology)
") Evaluation of thyroid nodules: prediction and selection of malignant nodules for FNA (cytology) Poster No.: C-0221 Congress: ECR 2014 Type: Authors: Keywords: DOI: Scientific Exhibit E. Papadaki, I. Tritou,
Evaluation of thyroid nodules: prediction and selection of malignant nodules for FNA (cytology) Poster No.: C-0221 Congress: ECR 2014 Type: Authors: Keywords: DOI: Scientific Exhibit E. Papadaki, I. Tritou,
Thyroid Nodules: US Risk Stratification. Alex Tessnow, MD, FACE, ECNU University of Texas Southwestern Associate Professor of Medicine Dallas, Texas
 Thyroid Nodules: US Risk Stratification Alex Tessnow, MD, FACE, ECNU University of Texas Southwestern Associate Professor of Medicine Dallas, Texas Which of the following is true? A. All echogenic foci
Thyroid Nodules: US Risk Stratification Alex Tessnow, MD, FACE, ECNU University of Texas Southwestern Associate Professor of Medicine Dallas, Texas Which of the following is true? A. All echogenic foci
High thyroglobulin (Tg) in a lymph node indicates metastatic
 in a lymph node indicates metastatic") ORIGINAL RESEARCH HEAD & NECK Optimized Cutoff Value and Indication for Washout Thyroglobulin Level According to Ultrasound Findings in Patients with Well-Differentiated Thyroid Cancer J.Y. Jung, J.H.
ORIGINAL RESEARCH HEAD & NECK Optimized Cutoff Value and Indication for Washout Thyroglobulin Level According to Ultrasound Findings in Patients with Well-Differentiated Thyroid Cancer J.Y. Jung, J.H.
Thyroid Nodule Risk Stratification and FNA Guidelines
 Thyroid Nodule Risk Stratification and FNA Guidelines Mark A. Lupo, MD, FACE, ECNU Thyroid & Endocrine Center of Florida Assistant Clinical Professor of Medicine Florida State University, College of Medicine
Thyroid Nodule Risk Stratification and FNA Guidelines Mark A. Lupo, MD, FACE, ECNU Thyroid & Endocrine Center of Florida Assistant Clinical Professor of Medicine Florida State University, College of Medicine
Practical Approach to Thyroid Nodules:Ultrasound Criteria for Performing FNA Revisited
 Practical Approach to Thyroid Nodules:Ultrasound Criteria for Performing FNA Revisited Poster No.: C-0100 Congress: ECR 2013 Type: Educational Exhibit Authors: S. Kuzmich, S. Sritharan, S. MUKUNDHAN, M.
Practical Approach to Thyroid Nodules:Ultrasound Criteria for Performing FNA Revisited Poster No.: C-0100 Congress: ECR 2013 Type: Educational Exhibit Authors: S. Kuzmich, S. Sritharan, S. MUKUNDHAN, M.
Sonographic Features of Thyroid Nodules & Guidelines for Management
 Sonographic Features of Thyroid Nodules & Guidelines for Management Mark A. Lupo, MD, FACE, ECNU Thyroid & Endocrine Center of Florida Assistant Clinical Professor of Medicine Florida State University,
Sonographic Features of Thyroid Nodules & Guidelines for Management Mark A. Lupo, MD, FACE, ECNU Thyroid & Endocrine Center of Florida Assistant Clinical Professor of Medicine Florida State University,
ORIGINAL ARTICLE. 304 Ultrasonography 34(4), October 2015 e-ultrasonography.org
, October 2015 e-ultrasonography.org") Differentiation of benign and malignant thyroid nodules based on the proportion of sponge-like areas on ultrasonography: imaging-pathologic correlation Jee Young Kim 1, So Lyung Jung 2, Mee Kyung Kim 3,
Differentiation of benign and malignant thyroid nodules based on the proportion of sponge-like areas on ultrasonography: imaging-pathologic correlation Jee Young Kim 1, So Lyung Jung 2, Mee Kyung Kim 3,
The Thyroid Nodule: From the Ultrasound Image to the Anatomopathological Diagnosis
 The Thyroid Nodule: From the Ultrasound Image to the Anatomopathological Diagnosis Poster No.: C-2229 Congress: ECR 2014 Type: Educational Exhibit Authors: T. González de la Huebra Labrador, A. Herrero
The Thyroid Nodule: From the Ultrasound Image to the Anatomopathological Diagnosis Poster No.: C-2229 Congress: ECR 2014 Type: Educational Exhibit Authors: T. González de la Huebra Labrador, A. Herrero
Mandana Moosavi 1 and Stuart Kreisman Background
 Case Reports in Endocrinology Volume 2016, Article ID 6471081, 4 pages http://dx.doi.org/10.1155/2016/6471081 Case Report A Case Report of Dramatically Increased Thyroglobulin after Lymph Node Biopsy in
Case Reports in Endocrinology Volume 2016, Article ID 6471081, 4 pages http://dx.doi.org/10.1155/2016/6471081 Case Report A Case Report of Dramatically Increased Thyroglobulin after Lymph Node Biopsy in
THYROID NODULES: THE ROLE OF ULTRASOUND
 THYROID NODULES: THE ROLE OF ULTRASOUND NOVEMBER 2017 DR. DEAN DURANT DEFINITION Thyroid nodule: Focal area within the thyroid gland with echogenicity different from surrounding parenchyma. THYROID NODULES
THYROID NODULES: THE ROLE OF ULTRASOUND NOVEMBER 2017 DR. DEAN DURANT DEFINITION Thyroid nodule: Focal area within the thyroid gland with echogenicity different from surrounding parenchyma. THYROID NODULES
Su-kyoung Jeh, MD 1 So Lyung Jung, MD 2 Bum Soo Kim, MD 2 Yoen Soo Lee, MD 3
 Evaluating the Degree of Conformity of Papillary Carcinoma and Follicular Carcinoma to the Reported Ultrasonographic Findings of Malignant Thyroid Tumor Su-kyoung Jeh, MD 1 So Lyung Jung, MD 2 Bum Soo
Evaluating the Degree of Conformity of Papillary Carcinoma and Follicular Carcinoma to the Reported Ultrasonographic Findings of Malignant Thyroid Tumor Su-kyoung Jeh, MD 1 So Lyung Jung, MD 2 Bum Soo
Can Color Doppler Sonography Aid in the Prediction of Malignancy of Thyroid Nodules?
 Article Can Color Doppler Sonography Aid in the Prediction of Malignancy of Thyroid Nodules? Mary C. Frates, MD, Carol B. Benson, MD, Peter M. Doubilet, MD, PhD, Edmund S. Cibas, MD, Ellen Marqusee, MD
Article Can Color Doppler Sonography Aid in the Prediction of Malignancy of Thyroid Nodules? Mary C. Frates, MD, Carol B. Benson, MD, Peter M. Doubilet, MD, PhD, Edmund S. Cibas, MD, Ellen Marqusee, MD
Diagnostic benefits of ultrasound-guided. CNB) versus mammograph-guided biopsy for suspicious microcalcifications. without definite breast mass
 versus mammograph-guided biopsy for suspicious microcalcifications. without definite breast mass") Volume 118 No. 19 2018, 531-543 ISSN: 1311-8080 (printed version); ISSN: 1314-3395 (on-line version) url: http://www.ijpam.eu ijpam.eu Diagnostic benefits of ultrasound-guided biopsy versus mammography-guided
Volume 118 No. 19 2018, 531-543 ISSN: 1311-8080 (printed version); ISSN: 1314-3395 (on-line version) url: http://www.ijpam.eu ijpam.eu Diagnostic benefits of ultrasound-guided biopsy versus mammography-guided
Taller-Than-Wide Sign of Thyroid Malignancy: Comparison Between Ultrasound and CT
 Neuroradiology/Head and Neck Imaging Original Research Yoon et al. Taller-Than-Wide Sign of Thyroid Malignancy Neuroradiology/Head and Neck Imaging Original Research Soo Jeong Yoon 1 Dae Young Yoon 1,2
Neuroradiology/Head and Neck Imaging Original Research Yoon et al. Taller-Than-Wide Sign of Thyroid Malignancy Neuroradiology/Head and Neck Imaging Original Research Soo Jeong Yoon 1 Dae Young Yoon 1,2
Thyroid Cytopathology: Weighing In The Bethesda System
 Thyroid Cytopathology: Weighing In The Bethesda System V8 Conflicts No financial consideration Bias Work in the Canadian environment where litigation is less Thyroid cytology is often referred in by small
Thyroid Cytopathology: Weighing In The Bethesda System V8 Conflicts No financial consideration Bias Work in the Canadian environment where litigation is less Thyroid cytology is often referred in by small
Sonographic Features of Benign Thyroid Nodules
 Article Sonographic Features of Benign Thyroid Nodules Interobserver Reliability and Overlap With Malignancy Jeffrey R. Wienke, MD, Wui K. Chong, MD, Julia R. Fielding, MD, Kelly H. Zou, PhD, Carol A.
Article Sonographic Features of Benign Thyroid Nodules Interobserver Reliability and Overlap With Malignancy Jeffrey R. Wienke, MD, Wui K. Chong, MD, Julia R. Fielding, MD, Kelly H. Zou, PhD, Carol A.
Index terms: Thyroid Ultrasonography Pathology Cancer. DOI: /kjr
 Histopathologic Findings Related to the Indeterminate or Inadequate Results of Fine-Needle Aspiration Biopsy and Correlation with Ultrasonographic Findings in Papillary Thyroid Carcinomas So Lyung Jung,
Histopathologic Findings Related to the Indeterminate or Inadequate Results of Fine-Needle Aspiration Biopsy and Correlation with Ultrasonographic Findings in Papillary Thyroid Carcinomas So Lyung Jung,
Malignant-looking thyroid nodules with size reduction: core needle biopsy results
 Malignant-looking thyroid nodules with size reduction: core needle biopsy results Ha Young Lee 1,2, Jung Hwan Baek 1, Eun Ju Ha 1,3, Jee Won Park 1,4, Jeong Hyun Lee 1, Dong Eun Song 5, Young Kee Shong
Malignant-looking thyroid nodules with size reduction: core needle biopsy results Ha Young Lee 1,2, Jung Hwan Baek 1, Eun Ju Ha 1,3, Jee Won Park 1,4, Jeong Hyun Lee 1, Dong Eun Song 5, Young Kee Shong
Dong Wook Kim, MD 1 Auh Whan Park, MD 1 Eun Joo Lee, MD 1 Hye Jung Choo, MD 1 Sang Hyo Kim, MD 2 Sang Hyub Lee, MD 2 Jae Wook Eom, MD 3
 Ultrasound-Guided Fine-Needle Aspiration Biopsy of Thyroid Nodules Smaller Than 5 mm in the Maximum Diameter: Assessment of Efficacy and Pathological Findings Dong Wook Kim, MD 1 Auh Whan Park, MD 1 Eun
Ultrasound-Guided Fine-Needle Aspiration Biopsy of Thyroid Nodules Smaller Than 5 mm in the Maximum Diameter: Assessment of Efficacy and Pathological Findings Dong Wook Kim, MD 1 Auh Whan Park, MD 1 Eun
The prevalence of thyroid nodules in the general
 Sonographically Guided Fine Needle Aspiration of Thyroid Nodule: Discrepancies between Cytologic and Histopathologic Findings Young Hen Lee, MD, 1 Nam Joon Lee, MD, 1 Jung Hyuk Kim, MD, 1 Sang-il Suh,
Sonographically Guided Fine Needle Aspiration of Thyroid Nodule: Discrepancies between Cytologic and Histopathologic Findings Young Hen Lee, MD, 1 Nam Joon Lee, MD, 1 Jung Hyuk Kim, MD, 1 Sang-il Suh,
Research Article Correlation of Fine Needle Aspiration Cytology with Histopathology in the Diagnosis of Solitary Thyroid Nodule
 SAGE-Hindawi Access to Research Thyroid Research Volume 2010, Article ID 379051, 5 pages doi:10.4061/2010/379051 Research Article Correlation of Fine Needle Aspiration Cytology with Histopathology in the
SAGE-Hindawi Access to Research Thyroid Research Volume 2010, Article ID 379051, 5 pages doi:10.4061/2010/379051 Research Article Correlation of Fine Needle Aspiration Cytology with Histopathology in the
Indications for Fine Needle Aspiration in Thyroid Nodules
 Review Article Endocrinol Metab 2013;28:81-85 http://dx.doi.org/10.3803/enm.2013.28.2.81 pissn 2093-596X eissn 2093-5978 Indications for Fine Needle Aspiration in Thyroid Nodules Jin Young Kwak Department
Review Article Endocrinol Metab 2013;28:81-85 http://dx.doi.org/10.3803/enm.2013.28.2.81 pissn 2093-596X eissn 2093-5978 Indications for Fine Needle Aspiration in Thyroid Nodules Jin Young Kwak Department
Jung Hyun Yoon, Eun-Kyung Kim, Ji Hyun Youk, Hee Jung Moon, and Jin Young Kwak
 International Journal of Endocrinology, Article ID 321595, 9 pages http://dx.doi.org/10.1155/2014/321595 Clinical Study Better Understanding in the Differentiation of Thyroid Follicular Adenoma, Follicular
International Journal of Endocrinology, Article ID 321595, 9 pages http://dx.doi.org/10.1155/2014/321595 Clinical Study Better Understanding in the Differentiation of Thyroid Follicular Adenoma, Follicular
Endocrinology and Metabolic Disorder Unit Regina Apostolorum Hospital
 Enrico Papini Endocrinology and Metabolic Disorder Unit Regina Apostolorum Hospital Albano Laziale, Italy The Following Faculty have provide no information regarding significant relationship with commercial
Enrico Papini Endocrinology and Metabolic Disorder Unit Regina Apostolorum Hospital Albano Laziale, Italy The Following Faculty have provide no information regarding significant relationship with commercial
Risk of Thyroid Cancer Based on Thyroid Ultrasound Imaging Characteristics
 Risk of Thyroid Cancer Based on Thyroid Ultrasound Imaging Characteristics Diabetes Update and Advances in Endocrinology & Metabolism Vickie A Feldstein MD Rebecca Smith- Bindman MD Department of Radiology
Risk of Thyroid Cancer Based on Thyroid Ultrasound Imaging Characteristics Diabetes Update and Advances in Endocrinology & Metabolism Vickie A Feldstein MD Rebecca Smith- Bindman MD Department of Radiology
Abstract. a a a a a
 RESEARCH ARTICLE Utility of including BRAF mutation analysis with ultrasonographic and cytological diagnoses in ultrasonography-guided fineneedle aspiration of thyroid nodules Da Som Kim 1, Dong Wook Kim
RESEARCH ARTICLE Utility of including BRAF mutation analysis with ultrasonographic and cytological diagnoses in ultrasonography-guided fineneedle aspiration of thyroid nodules Da Som Kim 1, Dong Wook Kim
Ultrasonographic Findings of Medullary Thyroid Carcinoma: a Comparison with Papillary Thyroid Carcinoma
 Ultrasonographic Findings of Medullary Thyroid Carcinoma: a Comparison with Papillary Thyroid Carcinoma Sung-Hun Kim, MD 1 Bum-Soo Kim, MD 1 So-Lyung Jung, MD 1 Jung-Whee Lee, MD 1 Po-Sung Yang, MD 1 Bong-Joo
Ultrasonographic Findings of Medullary Thyroid Carcinoma: a Comparison with Papillary Thyroid Carcinoma Sung-Hun Kim, MD 1 Bum-Soo Kim, MD 1 So-Lyung Jung, MD 1 Jung-Whee Lee, MD 1 Po-Sung Yang, MD 1 Bong-Joo
Roberto Negro, 1 Ermenegildo Colosimo, 2 and Gabriele Greco Methods. 1. Introduction
 Hindawi yroid Research Volume 2017, Article ID 9536479, 4 pages https://doi.org/10.1155/2017/9536479 Research Article Outcome, Pain Perception, and Health-Related Quality of Life in Patients Submitted
Hindawi yroid Research Volume 2017, Article ID 9536479, 4 pages https://doi.org/10.1155/2017/9536479 Research Article Outcome, Pain Perception, and Health-Related Quality of Life in Patients Submitted
Principal Site Investigator ENHANCE (Evaluation of Thyroid FNA Genomic Signature) study: An IRB approved study with funding to Rochester Regional
 study: An IRB approved study with funding to Rochester Regional") October 20 th 2018 Principal Site Investigator ENHANCE (Evaluation of Thyroid FNA Genomic Signature) study: An IRB approved study with funding to Rochester Regional Health from Veracyte Review ultrasound
October 20 th 2018 Principal Site Investigator ENHANCE (Evaluation of Thyroid FNA Genomic Signature) study: An IRB approved study with funding to Rochester Regional Health from Veracyte Review ultrasound
Evaluation of diagnostic efficacy of ultrasound scoring system to select thyroid nodules requiring fine needle aspiration biopsy
 Int J Clin Exp Med 2013;6(8):641-648 www.ijcem.com /ISSN:1940-5901/IJCEM1304014 Original Article Evaluation of diagnostic efficacy of ultrasound scoring system to select thyroid nodules requiring fine
Int J Clin Exp Med 2013;6(8):641-648 www.ijcem.com /ISSN:1940-5901/IJCEM1304014 Original Article Evaluation of diagnostic efficacy of ultrasound scoring system to select thyroid nodules requiring fine
Positive predictive value and inter-observer agreement of TIRADS for ultrasound features of thyroid nodules
 Positive predictive value and inter-observer agreement of TIRADS for ultrasound features of thyroid nodules Poster No.: C-0594 Congress: ECR 2014 Type: Scientific Exhibit Authors: C. Anuradha, K. Abhishek,
Positive predictive value and inter-observer agreement of TIRADS for ultrasound features of thyroid nodules Poster No.: C-0594 Congress: ECR 2014 Type: Scientific Exhibit Authors: C. Anuradha, K. Abhishek,
Contrast-enhanced ultrasound of solitary thyroid nodules - qualitative and quantitative evaluation: initial results
 Contrast-enhanced ultrasound of solitary thyroid nodules - qualitative and quantitative evaluation: initial results Poster No.: C-2436 Congress: ECR 2015 Type: Authors: Keywords: DOI: Scientific Exhibit
Contrast-enhanced ultrasound of solitary thyroid nodules - qualitative and quantitative evaluation: initial results Poster No.: C-2436 Congress: ECR 2015 Type: Authors: Keywords: DOI: Scientific Exhibit
Biopsy of Thyroid Nodules: Comparison of Three Sets of Guidelines
 Neuroradiology/Head and Neck Imaging Original Research Ahn et al. Biopsy of Thyroid Nodules Neuroradiology/Head and Neck Imaging Original Research FOCUS ON: Sung Soo Ahn 1 Eun-Kyung Kim 1 Dae Ryong Kang
Neuroradiology/Head and Neck Imaging Original Research Ahn et al. Biopsy of Thyroid Nodules Neuroradiology/Head and Neck Imaging Original Research FOCUS ON: Sung Soo Ahn 1 Eun-Kyung Kim 1 Dae Ryong Kang
Gray Scale and Colour Doppler Sonography in the Evaluation of Follicular Neoplasms of Thyroid
 DOI: 10.7860/IJARS/2018/24979:2393 Radiology Section Original Article Gray Scale and Colour Doppler Sonography in the Evaluation of Follicular Neoplasms of Thyroid Pradeep Hagalahalli Nagarajegowda, VISHWANATH
DOI: 10.7860/IJARS/2018/24979:2393 Radiology Section Original Article Gray Scale and Colour Doppler Sonography in the Evaluation of Follicular Neoplasms of Thyroid Pradeep Hagalahalli Nagarajegowda, VISHWANATH
Relationship between patterns of calcification in thyroid nodules and histopathologic findings
 Endocrine Journal 2013, 60 (2), 155-160 Or i g i n a l Relationship between patterns of calcification in thyroid nodules and histopathologic findings Bu Kyung Kim 1), Young Sik Choi 1), Hye Jung Kwon 1),
Endocrine Journal 2013, 60 (2), 155-160 Or i g i n a l Relationship between patterns of calcification in thyroid nodules and histopathologic findings Bu Kyung Kim 1), Young Sik Choi 1), Hye Jung Kwon 1),
The Thyroid Imaging Reporting and Data System (TIRADS) for ultrasound of the thyroid : a pratical approach
 for ultrasound of the thyroid : a pratical approach") The Thyroid Imaging Reporting and Data System (TIRADS) for ultrasound of the thyroid : a pratical approach Poster No.: C-2425 Congress: ECR 2015 Type: Educational Exhibit Authors: M. Ben Lassoued, B. Souissi,
The Thyroid Imaging Reporting and Data System (TIRADS) for ultrasound of the thyroid : a pratical approach Poster No.: C-2425 Congress: ECR 2015 Type: Educational Exhibit Authors: M. Ben Lassoued, B. Souissi,
Improving the Long Term Management of Benign Thyroid Nodules
 25 th Annual Scientific AACE Clinical Congress Improving the Long Term Management of Benign Thyroid Nodules Stephanie L. Lee, MD, PhD Director, Thyroid Health Center Section of Endocrinology, Diabetes
25 th Annual Scientific AACE Clinical Congress Improving the Long Term Management of Benign Thyroid Nodules Stephanie L. Lee, MD, PhD Director, Thyroid Health Center Section of Endocrinology, Diabetes
Mixed Echoic Thyroid Nodules on Ultrasound: Approach to Management
 Original Article http://dx.doi.org/10.3349/ymj.2012.53.4.812 pissn: 0513-5796, eissn: 1976-2437 Yonsei Med J 53(4):812-819, 2012 Mixed Echoic Thyroid Nodules on Ultrasound: Approach to Management Yu-Mee
Original Article http://dx.doi.org/10.3349/ymj.2012.53.4.812 pissn: 0513-5796, eissn: 1976-2437 Yonsei Med J 53(4):812-819, 2012 Mixed Echoic Thyroid Nodules on Ultrasound: Approach to Management Yu-Mee
Thyroid Nodule Management
 Thyroid Nodule Management Shane O. LeBeau, MD Clinical Associate Professor of Medicine Clinical Lead, Endocrine Thyroid Unit Division of Endocrinology, Diabetes and Metabolism University of Pittsburgh
Thyroid Nodule Management Shane O. LeBeau, MD Clinical Associate Professor of Medicine Clinical Lead, Endocrine Thyroid Unit Division of Endocrinology, Diabetes and Metabolism University of Pittsburgh
Thyroid Nodules. No conflicts. Overview 5/16/2017. UCSF Internal Medicine Updates May 22, 2017 Elizabeth Murphy, MD, DPhil
 Thyroid Nodules UCSF Internal Medicine Updates May 22, 2017 Elizabeth Murphy, MD, DPhil No conflicts Overview Thyroid nodule and cancer review Ultrasound FNA cytology Nodule follow up Putting it all together
Thyroid Nodules UCSF Internal Medicine Updates May 22, 2017 Elizabeth Murphy, MD, DPhil No conflicts Overview Thyroid nodule and cancer review Ultrasound FNA cytology Nodule follow up Putting it all together
Ultrasonography of the Neck as an Adjunct to FNA. Nicole Massoll M.D.
 Ultrasonography of the Neck as an Adjunct to FNA Nicole Massoll M.D. Basic Features of Head and Neck Ultrasound and Anatomy Nicole Massoll M.D. University of Arkansas for Medical Sciences, Little Rock
Ultrasonography of the Neck as an Adjunct to FNA Nicole Massoll M.D. Basic Features of Head and Neck Ultrasound and Anatomy Nicole Massoll M.D. University of Arkansas for Medical Sciences, Little Rock
ArticleInfo. Spring School of Thyroidology organized by the Polish Thyroid Association 2014: abstracts of invited lectures
 Ultrasound and cytological diagnostics of thyroid - its proper application in case of coexisting disturbing clinical signs and symptoms, suggestive of active proliferative lesion Andrzej Lewiński, Aff1
Ultrasound and cytological diagnostics of thyroid - its proper application in case of coexisting disturbing clinical signs and symptoms, suggestive of active proliferative lesion Andrzej Lewiński, Aff1
Primary Thyroid Lymphoma
 Article Primary Thyroid Lymphoma Role of Ultrasound-Guided Needle Biopsy Jin Young Kwak, MD, Eun-Kyung Kim, MD, Kyung Hee Ko, MD, Woo Ik Yang, MD, Min Jung Kim, MD, Eun Ju Son, MD, Ki Keun Oh, MD, Ki Whang
Article Primary Thyroid Lymphoma Role of Ultrasound-Guided Needle Biopsy Jin Young Kwak, MD, Eun-Kyung Kim, MD, Kyung Hee Ko, MD, Woo Ik Yang, MD, Min Jung Kim, MD, Eun Ju Son, MD, Ki Keun Oh, MD, Ki Whang
Thyroid Nodules: What to do next?
 Thyroid Nodules: What to do next? Ally P. H. Prebtani Professor of Medicine Internal Medicine, Endocrinology & Metabolism McMaster University Canada Copyright 2017 by Sea Courses Inc. All rights reserved.
Thyroid Nodules: What to do next? Ally P. H. Prebtani Professor of Medicine Internal Medicine, Endocrinology & Metabolism McMaster University Canada Copyright 2017 by Sea Courses Inc. All rights reserved.
Research Article Papillary Thyroid Cancer, Macrofollicular Variant: The Follow-Up and Analysis of Prognosis of 5 Patients
 yroid Research, Article ID 818134, 4 pages http://dx.doi.org/10.1155/2014/818134 Research Article Papillary Thyroid Cancer, Macrofollicular Variant: The Follow-Up and Analysis of Prognosis of 5 Patients
yroid Research, Article ID 818134, 4 pages http://dx.doi.org/10.1155/2014/818134 Research Article Papillary Thyroid Cancer, Macrofollicular Variant: The Follow-Up and Analysis of Prognosis of 5 Patients
Thyroid nodules, when to perform a fine needle aspiration
 Thyroid nodules, when to perform a fine needle aspiration Poster No.: C-1828 Congress: ECR 2015 Type: Educational Exhibit Authors: A. I. Fernández Martín, E. Pertusa Santos, E. Dominguez 1 1 1 2 1 Franjo,
Thyroid nodules, when to perform a fine needle aspiration Poster No.: C-1828 Congress: ECR 2015 Type: Educational Exhibit Authors: A. I. Fernández Martín, E. Pertusa Santos, E. Dominguez 1 1 1 2 1 Franjo,
CMEArticle A method in the madness in ultrasound evaluation of thyroid nodules
 Singapore Med J 2012; 53(11) : 766 CMEArticle A method in the madness in ultrasound evaluation of thyroid nodules Amogh Hegde 1, MD, FRCR, Anil Gopinathan 1, MD, FRCR, Rafidah Abu Bakar 2, MMedUS, BSc,
Singapore Med J 2012; 53(11) : 766 CMEArticle A method in the madness in ultrasound evaluation of thyroid nodules Amogh Hegde 1, MD, FRCR, Anil Gopinathan 1, MD, FRCR, Rafidah Abu Bakar 2, MMedUS, BSc,
Oh, I get it, the TSH goes up and down
 Evaluation and Management of the Thyroid Nodule Oh, I get it, the TSH goes up and down UCSF Head and Neck Conference October 24, 2008 Peter A. Singer, M.D. Professor and Chief Clinical Endocrinology University
Evaluation and Management of the Thyroid Nodule Oh, I get it, the TSH goes up and down UCSF Head and Neck Conference October 24, 2008 Peter A. Singer, M.D. Professor and Chief Clinical Endocrinology University
Update on Thyroid FNA The Bethesda System. Shikha Bose M.D. Associate Professor Cedars Sinai Medical Center
 Update on Thyroid FNA The Bethesda System Shikha Bose M.D. Associate Professor Cedars Sinai Medical Center Thyroid Nodules Frequent occurrence Palpable: 4-7% of adults Ultrasound: 10-31% Majority benign
Update on Thyroid FNA The Bethesda System Shikha Bose M.D. Associate Professor Cedars Sinai Medical Center Thyroid Nodules Frequent occurrence Palpable: 4-7% of adults Ultrasound: 10-31% Majority benign
Case Report Tubular Carcinoma of the Breast: Advantages and Limitations of Breast Tomosynthesis
 Case Reports in Radiology Volume 2016, Article ID 3906195, 4 pages http://dx.doi.org/10.1155/2016/3906195 Case Report Tubular Carcinoma of the Breast: Advantages and Limitations of Breast Tomosynthesis
Case Reports in Radiology Volume 2016, Article ID 3906195, 4 pages http://dx.doi.org/10.1155/2016/3906195 Case Report Tubular Carcinoma of the Breast: Advantages and Limitations of Breast Tomosynthesis
Case-based discussion:
 Case-based discussion: Pailin Kongmebhol, M.D. Department of Radiology Faculty of Medicine Chiang Mai University There are many guidelines for managing thyroid nodules Two important guidelines: 2015 American
Case-based discussion: Pailin Kongmebhol, M.D. Department of Radiology Faculty of Medicine Chiang Mai University There are many guidelines for managing thyroid nodules Two important guidelines: 2015 American
Columnar Cell Variant of Papillary Thyroid Carcinoma: Ultrasonographic and Clinical Differentiation between the Indolent and Aggressive Types
 Brief Communication Thyroid https://doi.org/10.3348/kjr.2018.19.5.1000 pissn 1229-6929 eissn 2005-8330 Korean J Radiol 2018;19(5):1000-1005 Columnar Cell Variant of Papillary Thyroid Carcinoma: Ultrasonographic
Brief Communication Thyroid https://doi.org/10.3348/kjr.2018.19.5.1000 pissn 1229-6929 eissn 2005-8330 Korean J Radiol 2018;19(5):1000-1005 Columnar Cell Variant of Papillary Thyroid Carcinoma: Ultrasonographic
Medicine. Observational Study. 1. Introduction. 2. Materials and methods. 3. Results OPEN
 Observational Study Medicine Ultrasonographic features and clinicopathologic characteristics of macrofollicular variant papillary thyroid carcinoma Yong Sang Lee, MD a,c, Soo Young Kim, MD a,c, Soon Won
Observational Study Medicine Ultrasonographic features and clinicopathologic characteristics of macrofollicular variant papillary thyroid carcinoma Yong Sang Lee, MD a,c, Soo Young Kim, MD a,c, Soon Won
Volume 2 Issue ISSN
 Volume 2 Issue 3 2012 ISSN 2250-0359 Correlation of fine needle aspiration and final histopathology in thyroid disease: a series of 702 patients managed in an endocrine surgical unit *Chandrasekaran Maharajan
Volume 2 Issue 3 2012 ISSN 2250-0359 Correlation of fine needle aspiration and final histopathology in thyroid disease: a series of 702 patients managed in an endocrine surgical unit *Chandrasekaran Maharajan
Cytology for the Endocrinologist. Nicole Massoll M.D
 Cytology for the Endocrinologist Nicole Massoll M.D Objectives Discuss slide preperation Definitions of adequacy ROSE (Rapid On-Site Evaluation) Thyroid Cytology Adequacy Nicole Massoll M.D. University
Cytology for the Endocrinologist Nicole Massoll M.D Objectives Discuss slide preperation Definitions of adequacy ROSE (Rapid On-Site Evaluation) Thyroid Cytology Adequacy Nicole Massoll M.D. University
Thyroid nodules with minimal cystic changes have a low risk of malignancy
 Thyroid nodules with minimal cystic changes have a low risk of malignancy Dong Gyu Na 1, Ji-hoon Kim 2, Dae Sik Kim 1,3, Soo Jin Kim 1,4 1 Department of Radiology, Human Medical Imaging and Intervention
Thyroid nodules with minimal cystic changes have a low risk of malignancy Dong Gyu Na 1, Ji-hoon Kim 2, Dae Sik Kim 1,3, Soo Jin Kim 1,4 1 Department of Radiology, Human Medical Imaging and Intervention
The Comparison of Scintigraphic and Ultrasonographic Evaluation Criteria of Thyroid Nodules with Histopathologic Findings
 Research Article The Comparison of Scintigraphic and Ultrasonographic Evaluation Criteria of Thyroid Nodules with Histopathologic Findings Seracettin Eğin * Department of General Surgery, University of
Research Article The Comparison of Scintigraphic and Ultrasonographic Evaluation Criteria of Thyroid Nodules with Histopathologic Findings Seracettin Eğin * Department of General Surgery, University of
A Study of Thyroid Swellings and Correlation between FNAC and Histopathology Results
 International Journal of Current Microbiology and Applied Sciences ISSN: 2319-7706 Volume 6 Number 4 (2017) pp. 265-269 Journal homepage: http://www.ijcmas.com Original Research Article https://doi.org/10.20546/ijcmas.2017.604.030
International Journal of Current Microbiology and Applied Sciences ISSN: 2319-7706 Volume 6 Number 4 (2017) pp. 265-269 Journal homepage: http://www.ijcmas.com Original Research Article https://doi.org/10.20546/ijcmas.2017.604.030
Diffuse Sclerosing Variant of Papillary Thyroid Carcinoma
 PITORL ESSY iffuse Sclerosing Variant of Papillary Thyroid arcinoma Sonography and Specimen Radiography Hyun Kyung Jung, M, Soon Won Hong, M, Eun-Kyung Kim, M, Jung Hyun Yoon, M, Jin Young Kwak, M The
PITORL ESSY iffuse Sclerosing Variant of Papillary Thyroid arcinoma Sonography and Specimen Radiography Hyun Kyung Jung, M, Soon Won Hong, M, Eun-Kyung Kim, M, Jung Hyun Yoon, M, Jin Young Kwak, M The
Study of validity of ultrasonographic diagnosis in relation to Fine Needle Aspiration Cytology (FNAC) diagnosis
 diagnosis") Original article: Study of validity of ultrasonographic diagnosis in relation to Fine Needle Aspiration Cytology (FNAC) diagnosis *Dr Rajvi Matalia, ** Dr Y.P.Sachdev, ***Dr D.S.Kulkarni *Junior Resident,
Original article: Study of validity of ultrasonographic diagnosis in relation to Fine Needle Aspiration Cytology (FNAC) diagnosis *Dr Rajvi Matalia, ** Dr Y.P.Sachdev, ***Dr D.S.Kulkarni *Junior Resident,
original article INTRODUCTION Thyroid nodules are a common finding within ABSTRACT
 original article Reliability of Thyroid Imaging Reporting and Data System (TI-RADS), and ultrasonographic classification of the American Thyroid Association (ATA) in differentiating benign from malignant
original article Reliability of Thyroid Imaging Reporting and Data System (TI-RADS), and ultrasonographic classification of the American Thyroid Association (ATA) in differentiating benign from malignant
Clinical Outcome for Atypia of Undetermined Significance in Thyroid Fine-Needle Aspirations Should Repeated FNA Be the Preferred Initial Approach?
 Anatomic Pathology / Clinical Outcome for AUS Thyroid FNA Clinical Outcome for Atypia of Undetermined Significance in Thyroid Fine-Needle Aspirations Should Repeated FNA Be the Preferred Initial Approach?
Anatomic Pathology / Clinical Outcome for AUS Thyroid FNA Clinical Outcome for Atypia of Undetermined Significance in Thyroid Fine-Needle Aspirations Should Repeated FNA Be the Preferred Initial Approach?
Original Article Breast Imaging
 Original Article Breast Imaging http://dx.doi.org/10.3348/kjr.2014.15.6.697 pissn 1229-6929 eissn 2005-8330 Korean J Radiol 2014;15(6):697-703 Percutaneous Ultrasound-Guided Vacuum-Assisted Removal versus
Original Article Breast Imaging http://dx.doi.org/10.3348/kjr.2014.15.6.697 pissn 1229-6929 eissn 2005-8330 Korean J Radiol 2014;15(6):697-703 Percutaneous Ultrasound-Guided Vacuum-Assisted Removal versus
Ultrasound Evaluation of Thyroid Nodules. October 2016
 Ultrasound Evaluation of Thyroid Nodules October 2016 Thyroid Nodules Primary goal is to determine if a nodule is malignant and needs surgery, or is benign and does not need surgery. Concerning Clinical
Ultrasound Evaluation of Thyroid Nodules October 2016 Thyroid Nodules Primary goal is to determine if a nodule is malignant and needs surgery, or is benign and does not need surgery. Concerning Clinical
Introduction: Ultrasound guided Fine Needle Aspiration: When and how
 International Course of Thyroid Ultrasonography and minimally invasive procedure 7-8 October 2016 University of Pisa, Italy Introduction: Ultrasound guided Fine Needle Aspiration: When and how Teresa Rago
International Course of Thyroid Ultrasonography and minimally invasive procedure 7-8 October 2016 University of Pisa, Italy Introduction: Ultrasound guided Fine Needle Aspiration: When and how Teresa Rago
Introduction ORIGINAL ARTICLE. Sang Yu Nam 1,2, Jung Hee Shin 1, Eun Young Ko 1, Soo Yeon Hahn 1
 A comparison of lymphocytic thyroiditis with papillary thyroid carcinoma showing suspicious ultrasonographic findings in a background of heterogeneous parenchyma Sang Yu Nam 1,2, Jung Hee Shin 1, Eun Young
A comparison of lymphocytic thyroiditis with papillary thyroid carcinoma showing suspicious ultrasonographic findings in a background of heterogeneous parenchyma Sang Yu Nam 1,2, Jung Hee Shin 1, Eun Young
Case Report A Rare Cutaneous Adnexal Tumor: Malignant Proliferating Trichilemmal Tumor
 Case Reports in Medicine Volume 2015, Article ID 742920, 4 pages http://dx.doi.org/10.1155/2015/742920 Case Report A Rare Cutaneous Adnexal Tumor: Malignant Proliferating Trichilemmal Tumor Omer Alici,
Case Reports in Medicine Volume 2015, Article ID 742920, 4 pages http://dx.doi.org/10.1155/2015/742920 Case Report A Rare Cutaneous Adnexal Tumor: Malignant Proliferating Trichilemmal Tumor Omer Alici,
Dilemma in diagnosing thyroid adenoma A case report
 BRIEF REPORT Dilemma in diagnosing thyroid adenoma A case report Faria Nasreen, Shamsun Nahar Bailey National Institute of Nuclear Medicine & Allied Sciences, BAEC, Dhaka, Bangladesh Correspondence: Faria
BRIEF REPORT Dilemma in diagnosing thyroid adenoma A case report Faria Nasreen, Shamsun Nahar Bailey National Institute of Nuclear Medicine & Allied Sciences, BAEC, Dhaka, Bangladesh Correspondence: Faria
Echogenic Foci in Thyroid Nodules: Significance of Posterior Acoustic Artifacts
 Neuroradiology/Head and Neck Imaging Original Research Malhi et al. Echogenic Foci in Thyroid Nodules Neuroradiology/Head and Neck Imaging Original Research Harshawn Malhi 1 Michael D. Beland 2 Steven
Neuroradiology/Head and Neck Imaging Original Research Malhi et al. Echogenic Foci in Thyroid Nodules Neuroradiology/Head and Neck Imaging Original Research Harshawn Malhi 1 Michael D. Beland 2 Steven
Cystic Hypersecretory Carcinoma of the Breast:
 J Korean Soc Radiol 2010;62:287-294 Cystic Hypersecretory Carcinoma of the Breast: Sonographic Features with a Histological Correlation 1 Sang Yu Nam, M.D., Boo-Kyung Han, M.D., Jung Hee Shin, M.D., Eun
J Korean Soc Radiol 2010;62:287-294 Cystic Hypersecretory Carcinoma of the Breast: Sonographic Features with a Histological Correlation 1 Sang Yu Nam, M.D., Boo-Kyung Han, M.D., Jung Hee Shin, M.D., Eun
Clinical Significance of Distinguishing Between Follicular Lesion and Follicular Neoplasm in Thyroid Fine-Needle Aspiration Biopsy
 Ann Surg Oncol (2009) 16:3146 3153 DOI 10.1245/s10434-009-0666-3 ORIGINAL ARTICLE ENDOCRINE TUMORS Clinical Significance of Distinguishing Between Follicular Lesion and Follicular Neoplasm in Thyroid Fine-Needle
Ann Surg Oncol (2009) 16:3146 3153 DOI 10.1245/s10434-009-0666-3 ORIGINAL ARTICLE ENDOCRINE TUMORS Clinical Significance of Distinguishing Between Follicular Lesion and Follicular Neoplasm in Thyroid Fine-Needle
Relationship of Cytological with Histopathological Examination of Palpable Thyroid Nodule
 Relationship of Cytological with Histopathological Examination of Palpable Thyroid Nodule NAUSHEEN HENNA 1, SHAHZAD AHMED FAKHAR 2, NAVEED AKHTER 3, MUHAMMAD MASOOD AFZAL 4, KHIZER AFTAB AHMAD KHAN 5,
Relationship of Cytological with Histopathological Examination of Palpable Thyroid Nodule NAUSHEEN HENNA 1, SHAHZAD AHMED FAKHAR 2, NAVEED AKHTER 3, MUHAMMAD MASOOD AFZAL 4, KHIZER AFTAB AHMAD KHAN 5,
The Indeterminate Thyroid Fine-Needle Aspiration
 The Indeterminate Thyroid Fine-Needle Aspiration Experience From an Academic Center Using Terminology Similar to That Proposed in the 2007 National Cancer Institute Thyroid Fine Needle Aspiration State
The Indeterminate Thyroid Fine-Needle Aspiration Experience From an Academic Center Using Terminology Similar to That Proposed in the 2007 National Cancer Institute Thyroid Fine Needle Aspiration State
Approach to Thyroid Nodules
 Approach to Thyroid Nodules Alice Y.Y. Cheng, MD, FRCPC Twitter: @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Approach to Thyroid Nodules Alice Y.Y. Cheng, MD, FRCPC Twitter: @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
AACE/ACE Advanced Endocrine Neck Ultrasound Training Course 2016
 AACE/ACE Advanced Endocrine Neck Ultrasound Training Course 2016 This 9mm left inferior nodule should remind us all why we re here! There is no absolute number of images required for documentation
AACE/ACE Advanced Endocrine Neck Ultrasound Training Course 2016 This 9mm left inferior nodule should remind us all why we re here! There is no absolute number of images required for documentation
Role of ultrasonography in recognition of malignant potential of thyroid nodules on the basis of their internal composition
 Role of ultrasonography in recognition of malignant potential of thyroid nodules on the basis of their internal composition Nodular thyroid is a common clinical entity. All patients were evaluated by grey
Role of ultrasonography in recognition of malignant potential of thyroid nodules on the basis of their internal composition Nodular thyroid is a common clinical entity. All patients were evaluated by grey
Reliability of the ultrasound classification system of thyroid nodules in predicting malignancy
 ORIGINAL ARTICLE Reliability of the ultrasound classification system of thyroid nodules in predicting malignancy Farihah Abd Ghani, MB BCh BAO (NUI) 1, Nurismah Md Isa, MPath 2, Husyairi Harunarashid,
ORIGINAL ARTICLE Reliability of the ultrasound classification system of thyroid nodules in predicting malignancy Farihah Abd Ghani, MB BCh BAO (NUI) 1, Nurismah Md Isa, MPath 2, Husyairi Harunarashid,
Role of Ultrasonography to Differentiate Benign and Malignant Thyroid Nodules in Correlation with Fine-needle Aspiration Cytology
 Original Article Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2016/434 Role of Ultrasonography to Differentiate Benign and Malignant Thyroid Nodules in Correlation with Fine-needle Aspiration
Original Article Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2016/434 Role of Ultrasonography to Differentiate Benign and Malignant Thyroid Nodules in Correlation with Fine-needle Aspiration
Pathology Reporting of Thyroid Core Needle Biopsy: A Proposal of the Korean. Endocrine Pathology Thyroid Core Needle Biopsy Study Group
 Pathology Reporting of Thyroid Core Needle Biopsy: A Proposal of the Korean Endocrine Pathology Thyroid Core Needle Biopsy Study Group Chan Kwon Jung 1 Hye Sook Min 2,3 Hyo Jin Park 2 Dong Eun Song 4 Jang
Pathology Reporting of Thyroid Core Needle Biopsy: A Proposal of the Korean Endocrine Pathology Thyroid Core Needle Biopsy Study Group Chan Kwon Jung 1 Hye Sook Min 2,3 Hyo Jin Park 2 Dong Eun Song 4 Jang
Atypical Ductal Hyperplasia and Papillomas: A Comparison of Ultrasound Guided Breast Biopsy and Stereotactic Guided Breast Biopsy
 Atypical Ductal Hyperplasia and Papillomas: A Comparison of Ultrasound Guided Breast Biopsy and Stereotactic Guided Breast Biopsy Breast Cancer is the most common cancer diagnosed in women in the United
Atypical Ductal Hyperplasia and Papillomas: A Comparison of Ultrasound Guided Breast Biopsy and Stereotactic Guided Breast Biopsy Breast Cancer is the most common cancer diagnosed in women in the United
ISSN X (Print) Research Article. *Corresponding author Dr Kumud Julka
 Research Article. *Corresponding author Dr Kumud Julka") Scholars Journal of Applied Medical Sciences (SJAMS) Sch. J. App. Med. Sci., 2015; 3(2A):568-573 Scholars Academic and Scientific Publisher (An International Publisher for Academic and Scientific Resources)
Scholars Journal of Applied Medical Sciences (SJAMS) Sch. J. App. Med. Sci., 2015; 3(2A):568-573 Scholars Academic and Scientific Publisher (An International Publisher for Academic and Scientific Resources)
USGFNA of thyroid nodules
 US Guided FNA (USGFNA) of neck masses INTERVENTIONAL HEAD & NECK ULTRASOUND Brendan C. Stack, Jr., MD., FACS, FACE Professor Otolaryngology-Head and Neck Surgery Indications Technique Interpretation Results
US Guided FNA (USGFNA) of neck masses INTERVENTIONAL HEAD & NECK ULTRASOUND Brendan C. Stack, Jr., MD., FACS, FACE Professor Otolaryngology-Head and Neck Surgery Indications Technique Interpretation Results