National Program for Nodular Goiter (PRONBONO). Multicenter study of single palpable thyroid nodules
|
|
|
- Shana Tucker
- 5 years ago
- Views:
Transcription
1 National Program for Nodular Goiter (PRONBONO). Multicenter study of single palpable thyroid nodules Corino M., Faure E., Deutsch S. and other members of the Thyroid Department of SAEM: Abalovich M., Alcaraz G., Balzaretti M., Becerra H., Brenta G.,Cabezón C. Ferreiro, L., Frascaroli G., Gauna A., Gutiérrez S., Iorcansky S., Lowenstein A., Maza Puig C., Melado G., Niepomniszcze H., Orlandi A., Puscar A., Reyes A., Rezzónico J., Ridruejo C., Roccatagliata G., Sartorio G., Schnitman M., Silva Croome M. del C., Storani M.E., Vázquez G. FASEN (Argentine Federation of Endocrinology Societies) Thyroid Department of SAEM. (Argentine Society of Endocrinology and Metabolism) ABSTRACT Introduction: the presence of palpable thyroid nodules in the general population is one of the most common clinical signs of thyroid disease in daily practice. Objectives: 1) To assess the prevalence of pathologies, clinical and cytological findings of single palpable thyroid nodules (SPTN) in Argentina. 2) To analyze regional differences in Argentina. Methods: Prospective study of 739 patients with STPN who were evaluated at centres in Buenos Aires, Bahía Blanca, Mendoza, and La Pampa between 1/1/00 and 12/31/01. Clinical examination, thyroid ultrasound scan (US), TSH, TPOAb and fine needle aspirations (FNA) were performed. Statistics: Pearson Correlation, X2 & Fisher Tests. Results: Age (X ± SD) 46 ± 14ys: 93.1 % were women. Previous history of neck radiation & familial thyroid disease were found in 1.6 and 29.9 %, respectively. Clinical findings: dysphagia: 7.9 %; dysphonia: 3.5%; nodule growth: 19.2 %; hard consistence: 24.7 %; fixation to adjacent structure: 1.5 % and lymphadenopathies (ADP): 3 %. Biochemical findings: TSH was normal in 81.2 % & TPOAb+ in 30.3 %. US features: solid: 53.1 %; hypoechoic: 63.8 %; microcalcifications: 10.3 %; incomplete halo: 15 %; more than 1 nodule: 30.5 %; thyroid heterogeneity: 60.2 % and ADP: 3.8 %. Cytology: Only 1 FNA was needed in 86.8%. Unsatisfactory (excluding cysts): 3.2 %; benign: 77.2%; suspicious: 12.6 % and cancer: 7 % (42 papillary, 2 medullary and 3 non-specified). A significant correlation (p<0.02) was established between malignant nodules and rapid growth, hard, fixed, solid nodule, incomplete halo and ADP, though these parameters were more frequent (in absolute number) in benign nodules. Surgery was mainly indicated based on FNA results. Histological diagnosis of 96 patients who underwent surgery showed 51 carcinomas, of which only 2 were cytologically benign, and 31 adenomas. Conclusion: Palpable single nodules were more frequent in middle aged euthyroid women. One third had familial thyroid pathology, similar to the presence of TPOAb. On US, nodules were predominantly solid, hypoechoic, single with heterogeneous thyroid gland. FNA was predominantly benign. Rapid growth, hard, fixed, solid nodule, incomplete halo and ADP were associated with malignancy, but benignity was more common. In most patients, surgery was recommended based on cytological findings. Our results are similar to those reported in other geographic areasno financial conflicts of interest exist. Key words: single palpable thyroid nodules; thyroid cytology and ultrasound INTRODUCTION The presence of palpable thyroid nodules in the general population is commonly found in daily practice. Fine needle aspiration has been accepted as the diagnostic method of choice in the initial evaluation of thyroid nodules. The clinical and ultrasound features of nodules are a supplementary factor to make a proper diagnosis. Nodular thyroid disease has a prevalence ranging between 2.5% and 7 % (1-3), predominantly in women in iodine-sufficient areas. Thus, nodular thyroid disease involves a diagnosis dilemma for specialists to differentiate malignant nodules. Post-surgical findings have shown that between 5 and
2 15% of all nodules which underwent surgery are malignant (4-5). Factors such as age, gender, radiation exposure and family history lead to suspect malignancy when a thyroid nodule is found. However, it is not clear if there are other parameters to predict malignancy. As a consequence of that, members of the FASEN decided to study the predictive malignancy value of the clinical and ultrasound features of single palpable nodular goiter. The Thyroid Department of SAEM prepared a study protocol known as National Program of Nodular Goiter (PRONBONO) whose objectives were: 1) to establish the prevalence of different pathologies through fine needle aspiration in single palpable nodular goiter and analyze its features and correlation with cytological findings and histology in patients who underwent surgery; 2) to analyze the existence of regional differences. Study Author Year n Prevalence Age Women Men Framingham (US) Whickham (UK) Vander % % 1.5% Tunbridge % % 0.8% MATERIAL AND METHODS Study design: prospective, cross-sectional and multicenter. We prospectively studied patients with single palpable nodular goiter who presented between 1/JAN/2000 and 31/DEC/2001 at 19 sites: 16 in the city of Buenos Aires and Greater Buenos Aires, 1 in the city of Bahía Blanca, 1 in Mendoza and 1 in Santa Rosa, La Pampa. The inclusion criteria for this study were: patients presenting for the first time with a single palpable nodule, who underwent fine needle aspiration, with or without prior treatment for thyroid disease. The exclusion criteria were multi-nodular goiter or diffuse goiter found by palpation. Medical records of all patients were prepared including history of neck radiation, prior thyroid treatment as well as surgeries; non-thyroid autoimmune disease and family history of thyroid disease and Multiple Endocrine Neoplasia. Patients were questioned about nodule evolution, growth in the last 6 months and presence of local symptoms such as pain, dysphagia and dysphonia. Neck examination included nodule palpatory findings: longitudinal and transverse diameters, consistency (hard, soft, firm and/or elastic), adherence to deep planes, pain on palpation and features of the rest of the gland. In patients with enlarged lymph nodes, their number, location and size were reported. Laboratory parameters included TSH levels (with ultrasensitive methodology depending on each site) and the presence of antithyroid antibodies (ultrasensitive TPOAb or anti-m by hemagglutination test) considering them either positive or negative depending on the reference range of each method. The US scan had to be performed by a thyroid-experienced operator using a mhz transducer. The operator had to fill in a form with information about nodule size (specifying three diameters: AP-T-L); characteristics: solid, cystic or mixed; echogenicity, presence or absence of posterior enhancement or acoustic shadow, calcifications (micro, macro or egg shell); presence of nodular halo; number of nodules;
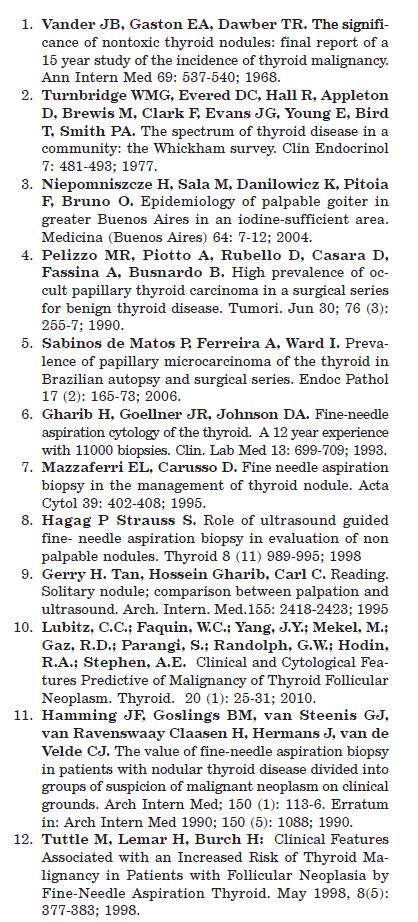
3 type of nodular and glandular contour; features of the rest of the thyroid parenchyma, as well as the presence of lymph nodes. For the cytological study, a group of recognized cytologists specialized in thyroid pathology previously determined the protocol methodology and established consistent criteria. The number of FNA repetitions necessary to reach a diagnosis, gross (liquiddrops or volume, solid) and microscopic description were recorded. The material was classified as unsatisfactory, benign, unspecified cyst, follicular proliferation, Hürthle Cell Tumor, malignant and tumor not originated in thyroid epithelium. The histological report of patients who had to undergo surgery was the statistical analysis of data, we used: The statistical analysis was performed using Pearson correlation, Chi Square Test and Fisher s Exact Test. RESULTS The data obtained from 739 patients with single palpable nodular goiter were analyzed. The proportion of patients evaluated at the above-mentioned sites is detailed in Table I. The group studied included 688 women (93%) and 51 men (7%), woman to man ratio: 13/1, age ( ± SD): 46.3 ± 14 years old (range: 16 to 81 years old). Twenty-nine point nine per cent (n=219) of patients had a family history of thyroid disease and one patient, of multiple endocrine neoplasia (MEN). Eighteen per cent (n=121) had received prior treatment with thyroid hormones, while 4.3% (n=31) had undergone thyroid surgery. 12 (1.6%) patients had been exposed to neck radiation. The patient-reported duration of goiters (expressed in months) ranged from 0.1 to 480 (40 years), with a mean of 25.8 months. As regards symptoms, 19.2% of patients reported nodule growth in the last six months; 7.9%, dysphagia; 6.4%, pain and 3.5% dysphonia. On thyroid palpation, nodules had a longitudinal diameter of 23.7 mm (± 12.5) (5-80 range) and mm (± 11) (4-60 range) in transverse diameter. In terms of consistence, 43.1% of nodules were firm, 24.7% were hard, 20.8% were elastic and 11.4% were soft. The rest of the gland was normal in 67.5% of patients. On neck palpation, we found tender nodules in 6.5% of patients, fixed nodules in 1.5% and lymph node enlargement in 3%. TSH levels were measured in 675 patients. The mean was 2.9 miu/l with a SD of ± 8.7 ( ). In 81.9% of patients (553/675), TSH levels were within the normal range. In 10.1% (68/675), above the highest limit and in 8% (54/675), below the lowest limit, based upon the methodology used and the range applied. The presence of anti-thyroid antibodies was evaluated in 638 patients, 30.3% of which were positive (n=193). In the ultrasound scan, nodule diameters expressed in mm ± SD were: anteroposterior: 18.3 ± 10.3; transverse 17.2 ± 10.4; longitudinal 21.6 ± 12.5; there being a highly significant linear correlation between palpation and ultrasound both in transverse (r 0.620) and longitudinal measurements (r 0.703) (p<0.0001). Pearson correlation coefficients were calculated and a highly significant linear correlation was found between Palpation and Ultrasound both in transverse and longitudinal measurements. (P<0.0001). Figure 1. When analyzing the ultrasound scan variables studied, we found that 53.1% of nodules were solid, 33.3% were mixed and 13.6% were cysts. Regarding echogenicity, 63.8% of nodules were hypoechoic, 17.9% were hyperechoic and 18.4% were isoechoic
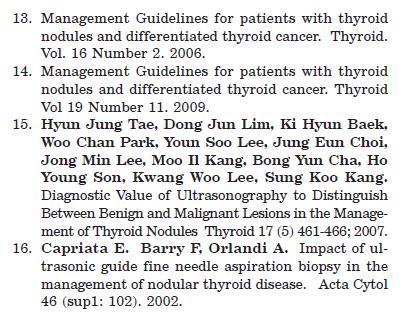
4 compared to the remaining parenchyma. Calcifications were found in 27.3% of nodules (microcalcifications in 10.3% and macrocalcifications in 7%), complete halo (CH) in 17.1% and incomplete halo (IH) in 15% of cases. Single nodules were found on ultrasound in 69.5% of patients and multiple nodules, in 30.5%. The remaining thyroid parenchyma was heterogeneous in 60.2% of patients and nodular contour was regular in 77.7% of patients. Enlarged lymph nodes were reported in 3.8% of patients and muscular planes were free in 100% of patients. As regards fine needle aspiration, cytological diagnosis was made in 86.8% of nodules through a single procedure, and in 13.2% of cases, repeat aspiration was necessary to reach a diagnosis. The cytological material was macroscopically solid in 59.6% of patients and liquid material was obtained in 40.4% of cases. Cytological reports showed that 77.2% of samples were benign, 7% were malignant, 12.6% were doubtful and 3.2% were unsatisfactory. Table II shows the different cytological diagnoses found and their rates. In our population, benign cytology was more common between 40 and 60 years of age (68.64%). By contrast, malignancy was more common between 30 and 50 years of age (72.2%), in younger patients. Figure 2. Table I. Proportion of patients from the different participating sites Site Rate Percentage Alvarez Bazterrica Británico Churruca Clínicas Cpe Durand Fernandez Frances Inst megan Italiano Militar Penna Perinat Posadas Ramos Rivadavia San Isidro Total Sites of the city of Buenos Aires; 2 Sites of Greater Buenos Aires. CPE of Mendoza, Instituto MEGAN of La Pampa, Hospital PENNA of Bahía Blanca.
5 Transverse ultrasound (mm) Longitudinal ultrasound (mm) Transverse palpation (mm) Longitudinal palpation (mm) Figure 1. Correlation between palpation and ultrasound diameters. Pearson correlation coefficients were calculated and there was a highly significant linear correlation between Palpation and Ultrasound both in transverse and longitudinal measurement. (P<0.0001). TABLE II. Cytological findings and rates Cytological report N % Colloid goiter Thyroiditis Epithelial hyperplasia Colloid cyst Benign 77.2% benign Unspecified Colloid cyst Benign Unspecified Epithelial hyperplasia and hyperfunction Follicular proliferation doubtful Hürthle cell tumor Papillary carcinoma Medullary carcinoma % malignant Malignant unspecified Unsatisfactory % unsatisfactory
 Solid (p<0.01) Solid macroscopy (p<0.001) Hard consistency (p<0.001) Fixed nodule (p<0.")
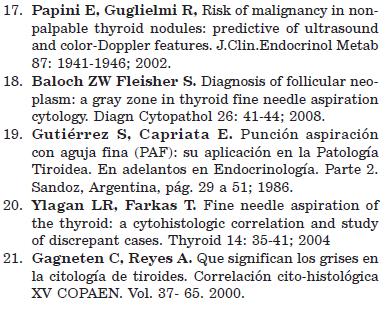
6 Age Age Age distribution of patients with benign cytology Age distribution of patients with malignant cytology Figure 2. Age distribution in benign and malignant cytology. TABLE III. Nodule features associated with malignant cytology Clinical US Fine Needle Aspiration Recent growth (p<0.02) Solid (p<0.01) Solid macroscopy (p<0.001) Hard consistency (p<0.001) Fixed nodule (p<0.01) Incomplete halo (p<0.01) Single nodule (p<0.01) Enlarged lymph nodes (p<0.04) Statistical Results In the population studied, we did not find a statistically significant correlation between malignancy and gender. (p = NS). Nodular growth in the last 6 months (p<0.02); hard consistency (p<0.001) and adherence to surrounding structures (p<0.01) were the clinical features associated with malignancy. (Table III). In 83.3% of smears with malignant cytology, the material obtained was solid, in correlation with malignancy. (p<0.001) (Table III). The presence of a single solid nodule with incomplete halo on US correlated with malignancy (p<0.01), as well as the presence of enlarged lymph nodes. (p<0.04) (Figure 3). According to the medical and/or cytological criterion, 96 patients underwent surgery. Histological findings were as follows (Figure 4): - 25 follicular adenomas - 6 Hürthle cell adenomas - 6 colloid goiters - 4 follicular cell hyperplasia - 2 thyroiditis - 1 colloid cyst - 40 papillary carcinomas - 6 follicular carcinomas - 2 medullary carcinomas - 3 without histological report
.")
7 Of the 48 carcinomas that underwent surgery, cytology was negative in 4 cases (8.3% FALSE NEGATIVE). In 47 malignant cytological findings that underwent surgery, 2 had benign histology (4.2% FALSE POSITIVE). As regards the 41 patients with cytology consistent with follicular proliferation and/or Hürthle cell tumor with indication for surgery, histological findings were as follows: - 24 follicular adenomas - 6 Hürthle cell adenomas - 2 hyperplasias of follicular cells - 2 colloid goiters - 4 papillary carcinomas - 3 follicular carcinomas That is, 17.07% of follicular proliferation and/or Hürthle cell tumor were carcinomas according to their histological findings. Yes Yes Yes Yes Solid IH SN Lymph node enlargement Benign Malignant Figure 3. US features associated with malignancy. There is a significant correlation between malignant cytology and solid nodules on US: P<0.01; incomplete nodular halo (HI); P<0.06; single nodule on US; p <0.06 and the presence of neck lymph nodes; P<0.08. (References: Quiste coloide = Colloid cyst; Tiroiditis = Thyroiditis; Adenomas foliculares = follicular adenomas; Bocio hiperplasia = hyperplasia goiter; Sin datos = No data; Maligno = malignant) Figure 4: Percentage of histological findings in 96 cases where surgery was recommended.
8 DISCUSSION This cross-sectional, prospective and multicenter study conducted in the Argentine Republic enabled us to establish the features of the population with single palpable thyroid nodule, and their correlation with the clinical parameters evaluated, US findings, cytology and histology of patients who were operated on. In clinical practice, risk assessment for malignancy of a thyroid nodule is based upon a set of multiple features: gender, age, personal history, family history, growth, gland features, enlarged lymph nodes, nodule size, laboratory test such as TSH level, determination of antibodies and fine needle aspiration considered the most reliable parameter to rule out malignancy in thyroid nodule. The contribution made by Gharib- Goelner (6) in 1993, (18163 patients) and Mazzaferri-Caruso (7) in 1995 (9119 patients) reaffirm the importance of the cytological findings in nodular pathology. In the epidemiological data of our study, most nodules occurred in women, with a female/male ratio of 13:1 and an age range corresponding to middle age. In consistency with these findings, Hagag et al (8) reported in 254 patients a mean age of 44±9.5 years and the same ratio for gender (13:1). In 542 patients participating in a study at Hospital de Clinicas, Niepomniszcze et al (3) reported a female/male ratio of 4:1 with a wide age range (2-85 years). These data show a high prevalence of nodular pathology in women. Thirty percent of our patients had a family history of thyroid disease or positive antibodies. In consistency with these data, Hagag et al (8) reported 29.7% of positive thyroid autoimmunity in their population. Eighty-nine percent of the 151 patients studied by Gerry et al (9) were euthyroid. We found that TSH levels were within normal ranges in 82% of the population. As regards nodule size, in recent studies, Lubitz et al (10) analyzed cytological and clinical findings in 144 patients with nodules suspicious for malignancy. Women accounted for 75% of the population with nodule; the mean age was 55 years; nodules > 4 cm were significantly associated with malignancy. In our study, nodular size had no statistical correlation with malignancy. As regards symptoms associated with malignancy, we found that nodular growth in the last 6 months was one of the most representative signs. However, neither spontaneous pain nor tenderness to palpation, or dysphagia or dysphonia was indicative of nodules with malignant cytology. Our findings are consistent with the classification made by Hamming in 1990 (11), and which is currently in effect. This classification establishes risk groups defined by clinical findings, where rapid growth and nodule hardness are included as highly suspicious for malignancy. According to his data, such features are associated with 71% of histological prevalence of carcinoma. In this study, clinical signs associated with cytological malignancy were rapid growth, fixation and hardness, in agreement with other authors such as Tuttle et al (12). It should be noted that the American Thyroid Association takes into account these data to prepare the recommendations for the management of patients with nodules and differentiated thyroid carcinoma. ATA 2006 (13) and 2009 (14). Ultrasound is a diagnostic method commonly used to evaluate thyroid nodules. It should be noted that the combination of different US features have a strong predictive value for malignancy as shown by Hyun Jung et al (15). Such authors describe several US properties associated with suspicion for malignancy, such as single, solid, hypoechoic nodule, calcifications and enlarged lymph node. In a group of cases in Argentina, in ultrasound-guided FNA, Capriata, Orlandi et al (16) found that 51% of solid and hypoechoic nodules were associated with malignancy. In 2002, in the study of non palpable nodules, Papini et al (17) assessed the value of US and color Doppler in thyroid nodules and agreed that microcalcifications,
9 hypoechogenicity and irregular nodular margins were predictors of malignancy, as well as the presence of multiple intranodular newly-formed vessels on Doppler ultrasound. In our study, the presence of a single, solid nodule with incomplete halo on US correlated with malignant cytology in 93.2% of patients. In malignant pathology, enlarged lymph nodes occurred in 25% of cases. As regards cytological findings, in patients, Gharib et al (6) found benignity in 69%, follicular proliferation in 10%, malignancy in 3.5% and inadequate specimen in 17%, with this being one of the first published studies with a large sample size. Lubitz et al (10) reported in 144 patients malignancy in 11% and benignity in 88.9%. In 2008, Baloch et al (18) reported in aspirated nodules, 5 to 10% risk of malignancy and 15 to 30% risk of follicular neoplasm. In PRONBONO, diagnosis was made with a single procedure in 87% of patients. Benign pathology was the most frequent result; the percentage of unsatisfactory material was low (3%) and malignancy accounted for 7%. According to age, carcinoma occurred at 30 to 50 years of age and there was no statistical correlation between gender and malignancy. In a national study performed by Gutiérrez, Capriata et al (19), 352 patients who underwent fine needle aspiration were evaluated; the percentage of cancer in patients who underwent surgery was 7.6%, similar to our findings. In 2004, Ylagan et al (20) established a cyto-histological correlation in nodules > 4 cm and found 5% of false negatives. Our pathology results determined that 4.2% were false positives and 8.3% were false negatives. Gagneten et al (21) reported cyto-histological correlation in 107 patients and found the following histology in 21 follicular proliferations: 33% adenoma, 28.6% carcinoma, 33.3% hyperplasia and 4.8% chronic thyroiditis. In PRONBONO, in the 41 patients operated on with cytology of follicular proliferation, benign pathology (adenoma) was the most common, and 17% carcinomas were diagnosed: 4 papillary and 3 follicular. CONCLUSIONS Most nodules occurred in middle-aged, asymptomatic, euthyroid female patients. The presence of 30% of family thyroid pathology was similar to the presence of positive antibodies. On US, most single, solid and incomplete halo nodules were associated with malignancy. Even if the percentage of false positives and negatives is consistent with the literature, the number of false negatives should tend to decrease. The low percentage of unsatisfactory material and the good correlation between palpation and ultrasound measurement should be highlighted. These results at population level do not imply diagnostic accuracy at individual patient level. In this multicenter study, we could not achieve the objective of establishing regional differences in nodular pathology, probably due to the low number or absence of data from all geographic areas in the country. REFERENCES
10
11
Sonographic Features of Thyroid Nodules & Guidelines for Management
 Sonographic Features of Thyroid Nodules & Guidelines for Management Mark A. Lupo, MD, FACE, ECNU Thyroid & Endocrine Center of Florida Assistant Clinical Professor of Medicine Florida State University,
Sonographic Features of Thyroid Nodules & Guidelines for Management Mark A. Lupo, MD, FACE, ECNU Thyroid & Endocrine Center of Florida Assistant Clinical Professor of Medicine Florida State University,
Approach to Thyroid Nodules
 Approach to Thyroid Nodules Alice Y.Y. Cheng, MD, FRCPC Twitter: @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Approach to Thyroid Nodules Alice Y.Y. Cheng, MD, FRCPC Twitter: @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Oh, I get it, the TSH goes up and down
 Evaluation and Management of the Thyroid Nodule Oh, I get it, the TSH goes up and down UCSF Head and Neck Conference October 24, 2008 Peter A. Singer, M.D. Professor and Chief Clinical Endocrinology University
Evaluation and Management of the Thyroid Nodule Oh, I get it, the TSH goes up and down UCSF Head and Neck Conference October 24, 2008 Peter A. Singer, M.D. Professor and Chief Clinical Endocrinology University
Thyroid Nodules: What to do next?
 Thyroid Nodules: What to do next? Ally P. H. Prebtani Professor of Medicine Internal Medicine, Endocrinology & Metabolism McMaster University Canada Copyright 2017 by Sea Courses Inc. All rights reserved.
Thyroid Nodules: What to do next? Ally P. H. Prebtani Professor of Medicine Internal Medicine, Endocrinology & Metabolism McMaster University Canada Copyright 2017 by Sea Courses Inc. All rights reserved.
Contents. Basic Ultrasound Principles and Terminology. Ultrasound Nodule Characteristics
 Contents Basic Ultrasound Principles and Terminology Basic Ultrasound Principles... 1 Ultrasound System... 2 Linear Transducer for Superficial Images and Ultrasound-Guided FNA... 3 Scanning Planes... 4
Contents Basic Ultrasound Principles and Terminology Basic Ultrasound Principles... 1 Ultrasound System... 2 Linear Transducer for Superficial Images and Ultrasound-Guided FNA... 3 Scanning Planes... 4
of Thyroid Lesions Comet Tail Crystals
 2 Ultrasound Features of Thyroid Lesions There are many different features indicating a certain benign or malignant tumor type, but many of these are overlapping signs. Combining several features is considered
2 Ultrasound Features of Thyroid Lesions There are many different features indicating a certain benign or malignant tumor type, but many of these are overlapping signs. Combining several features is considered
Thyroid in a Nutshell Dublin Catherine Kirkpatrick Consultant Sonographer ULHT
 Thyroid in a Nutshell Dublin 2017 Catherine Kirkpatrick Consultant Sonographer ULHT Acknowledgements Dr. Steve Colley Dr. Rhodri Evans Dr. Rhian Rhys Dr. Andrew McQueen Aims Anatomy & Physiology Incidence
Thyroid in a Nutshell Dublin 2017 Catherine Kirkpatrick Consultant Sonographer ULHT Acknowledgements Dr. Steve Colley Dr. Rhodri Evans Dr. Rhian Rhys Dr. Andrew McQueen Aims Anatomy & Physiology Incidence
AACE/ACE Advanced Endocrine Neck Ultrasound Training Course 2016
 AACE/ACE Advanced Endocrine Neck Ultrasound Training Course 2016 This 9mm left inferior nodule should remind us all why we re here! There is no absolute number of images required for documentation
AACE/ACE Advanced Endocrine Neck Ultrasound Training Course 2016 This 9mm left inferior nodule should remind us all why we re here! There is no absolute number of images required for documentation
COMPARISON OF ULTRASOUND FINDINGS WITH CYTOLOGIC RESULTS IN THYROID NODULES
 COMPARISON OF ULTRASOUND FINDINGS WITH CYTOLOGIC RESULTS IN THYROID NODULES E. Razmpa 1, H. Ghanaati 2, B. Naghibzadeh 3, P. Mazloom 1 and A. Kashfi 1 1) Department of Otolaryngology, School of Medicine,
COMPARISON OF ULTRASOUND FINDINGS WITH CYTOLOGIC RESULTS IN THYROID NODULES E. Razmpa 1, H. Ghanaati 2, B. Naghibzadeh 3, P. Mazloom 1 and A. Kashfi 1 1) Department of Otolaryngology, School of Medicine,
Endocrinology and Metabolic Disorder Unit Regina Apostolorum Hospital
 Enrico Papini Endocrinology and Metabolic Disorder Unit Regina Apostolorum Hospital Albano Laziale, Italy The Following Faculty have provide no information regarding significant relationship with commercial
Enrico Papini Endocrinology and Metabolic Disorder Unit Regina Apostolorum Hospital Albano Laziale, Italy The Following Faculty have provide no information regarding significant relationship with commercial
Warinthorn Phuttharak*, Charoonsak Somboonporn, Gatenapa Hongdomnern
 Colour Doppler Ultrasonography in the Diagnosis of Malignancy in Thyroid Nodules RESEARCH COMMUNICATION Diagnostic Performance of Gray-scale versus Combined Grayscale with Colour Doppler Ultrasonography
Colour Doppler Ultrasonography in the Diagnosis of Malignancy in Thyroid Nodules RESEARCH COMMUNICATION Diagnostic Performance of Gray-scale versus Combined Grayscale with Colour Doppler Ultrasonography
5/3/2017. Ahn et al N Engl J Med 2014; 371
 Alan Failor, M.D. Clinical Professor of Medicine Division of Metabolism, Endocrinology and Nutrition University of Washington April 20, 2017 No disclosures to report 1. Appropriately evaluate s in adult
Alan Failor, M.D. Clinical Professor of Medicine Division of Metabolism, Endocrinology and Nutrition University of Washington April 20, 2017 No disclosures to report 1. Appropriately evaluate s in adult
Objectives. How to Investigate Thyroid Nodules like A Pro
 How to Investigate Thyroid Nodules like A Pro Chris Sadler, MA, PA C, CDE, DFAAPA Medical Science Outcomes Liaison Intarcia Diabetes and Endocrine Associates La Jolla, CA Past President ASEPA Disclosures
How to Investigate Thyroid Nodules like A Pro Chris Sadler, MA, PA C, CDE, DFAAPA Medical Science Outcomes Liaison Intarcia Diabetes and Endocrine Associates La Jolla, CA Past President ASEPA Disclosures
Objectives. 1)To recall thyroid nodule ultrasound characteristics that increase the risk of malignancy
To recall thyroid nodule ultrasound characteristics that increase the risk of malignancy") Evaluation and Management of Thyroid Nodules in Primary Care Chris Sadler, MA, PA C, CDE, DFAAPA Medical Science Outcomes Liaison Intarcia Diabetes and Endocrine Associates La Jolla, CA Past President
Evaluation and Management of Thyroid Nodules in Primary Care Chris Sadler, MA, PA C, CDE, DFAAPA Medical Science Outcomes Liaison Intarcia Diabetes and Endocrine Associates La Jolla, CA Past President
Thyroid Nodules: US Risk Stratification. Alex Tessnow, MD, FACE, ECNU University of Texas Southwestern Associate Professor of Medicine Dallas, Texas
 Thyroid Nodules: US Risk Stratification Alex Tessnow, MD, FACE, ECNU University of Texas Southwestern Associate Professor of Medicine Dallas, Texas Which of the following is true? A. All echogenic foci
Thyroid Nodules: US Risk Stratification Alex Tessnow, MD, FACE, ECNU University of Texas Southwestern Associate Professor of Medicine Dallas, Texas Which of the following is true? A. All echogenic foci
Study of validity of ultrasonographic diagnosis in relation to Fine Needle Aspiration Cytology (FNAC) diagnosis
 diagnosis") Original article: Study of validity of ultrasonographic diagnosis in relation to Fine Needle Aspiration Cytology (FNAC) diagnosis *Dr Rajvi Matalia, ** Dr Y.P.Sachdev, ***Dr D.S.Kulkarni *Junior Resident,
Original article: Study of validity of ultrasonographic diagnosis in relation to Fine Needle Aspiration Cytology (FNAC) diagnosis *Dr Rajvi Matalia, ** Dr Y.P.Sachdev, ***Dr D.S.Kulkarni *Junior Resident,
Thyroid Nodules. Dr. HAKIMI, SpAK Dr. MELDA DELIANA, SpAK Dr. SISKA MAYASARI LUBIS, SpA
 Thyroid Nodules ENDOCRINOLOGY DIVISION ENDOCRINOLOGY DIVISION Dr. HAKIMI, SpAK Dr. MELDA DELIANA, SpAK Dr. SISKA MAYASARI LUBIS, SpA Anatomical Considerations The Thyroid Nodule Congenital anomalies Thyroglossal
Thyroid Nodules ENDOCRINOLOGY DIVISION ENDOCRINOLOGY DIVISION Dr. HAKIMI, SpAK Dr. MELDA DELIANA, SpAK Dr. SISKA MAYASARI LUBIS, SpA Anatomical Considerations The Thyroid Nodule Congenital anomalies Thyroglossal
Differentiated Thyroid Carcinoma
 Differentiated Thyroid Carcinoma The GOOD cancer? Jennifer Sipos, MD Associate Professor of Medicine Director, Benign Thyroid Program Division of Endocrinology, Diabetes and Metabolism The Ohio State University
Differentiated Thyroid Carcinoma The GOOD cancer? Jennifer Sipos, MD Associate Professor of Medicine Director, Benign Thyroid Program Division of Endocrinology, Diabetes and Metabolism The Ohio State University
Imaging in Pediatric Thyroid disorders: US and Radionuclide imaging. Deepa R Biyyam, MD Attending Pediatric Radiologist
 Imaging in Pediatric Thyroid disorders: US and Radionuclide imaging Deepa R Biyyam, MD Attending Pediatric Radiologist Imaging in Pediatric Thyroid disorders: Imaging modalities Outline ACR-SNM-SPR guidelines
Imaging in Pediatric Thyroid disorders: US and Radionuclide imaging Deepa R Biyyam, MD Attending Pediatric Radiologist Imaging in Pediatric Thyroid disorders: Imaging modalities Outline ACR-SNM-SPR guidelines
Evaluation of thyroid nodules: prediction and selection of malignant nodules for FNA (cytology)
") Evaluation of thyroid nodules: prediction and selection of malignant nodules for FNA (cytology) Poster No.: C-0221 Congress: ECR 2014 Type: Authors: Keywords: DOI: Scientific Exhibit E. Papadaki, I. Tritou,
Evaluation of thyroid nodules: prediction and selection of malignant nodules for FNA (cytology) Poster No.: C-0221 Congress: ECR 2014 Type: Authors: Keywords: DOI: Scientific Exhibit E. Papadaki, I. Tritou,
Thyroid Nodule Management
 Thyroid Nodule Management Shane O. LeBeau, MD Clinical Associate Professor of Medicine Clinical Lead, Endocrine Thyroid Unit Division of Endocrinology, Diabetes and Metabolism University of Pittsburgh
Thyroid Nodule Management Shane O. LeBeau, MD Clinical Associate Professor of Medicine Clinical Lead, Endocrine Thyroid Unit Division of Endocrinology, Diabetes and Metabolism University of Pittsburgh
Sonographic Features of Benign Thyroid Nodules
 Article Sonographic Features of Benign Thyroid Nodules Interobserver Reliability and Overlap With Malignancy Jeffrey R. Wienke, MD, Wui K. Chong, MD, Julia R. Fielding, MD, Kelly H. Zou, PhD, Carol A.
Article Sonographic Features of Benign Thyroid Nodules Interobserver Reliability and Overlap With Malignancy Jeffrey R. Wienke, MD, Wui K. Chong, MD, Julia R. Fielding, MD, Kelly H. Zou, PhD, Carol A.
Introduction: Ultrasound guided Fine Needle Aspiration: When and how
 International Course of Thyroid Ultrasonography and minimally invasive procedure 7-8 October 2016 University of Pisa, Italy Introduction: Ultrasound guided Fine Needle Aspiration: When and how Teresa Rago
International Course of Thyroid Ultrasonography and minimally invasive procedure 7-8 October 2016 University of Pisa, Italy Introduction: Ultrasound guided Fine Needle Aspiration: When and how Teresa Rago
Thyroid Nodules: US Risk Stratification and FNA Guidelines
 Thyroid Nodules: US Risk Stratification and FNA Guidelines Mark A. Lupo, MD, FACE, ECNU Thyroid & Endocrine Center of Florida Assistant Clinical Professor of Medicine Florida State University, College
Thyroid Nodules: US Risk Stratification and FNA Guidelines Mark A. Lupo, MD, FACE, ECNU Thyroid & Endocrine Center of Florida Assistant Clinical Professor of Medicine Florida State University, College
Case-based discussion:
 Case-based discussion: Pailin Kongmebhol, M.D. Department of Radiology Faculty of Medicine Chiang Mai University There are many guidelines for managing thyroid nodules Two important guidelines: 2015 American
Case-based discussion: Pailin Kongmebhol, M.D. Department of Radiology Faculty of Medicine Chiang Mai University There are many guidelines for managing thyroid nodules Two important guidelines: 2015 American
In adults, clinically palpable thyroid nodules are
 ORIGINAL ARTICLE ASSOCIATION OF SONOGRAPHICALLY DETECTED CALCIFICATION WITH THYROID CARCINOMA Ning Wang, PhD, Yuanhong Xu, PhD, Chunlin Ge, PhD, Renxuan Guo, PhD, Kejian Guo, MD, PhD General Surgery Department
ORIGINAL ARTICLE ASSOCIATION OF SONOGRAPHICALLY DETECTED CALCIFICATION WITH THYROID CARCINOMA Ning Wang, PhD, Yuanhong Xu, PhD, Chunlin Ge, PhD, Renxuan Guo, PhD, Kejian Guo, MD, PhD General Surgery Department
The Thyroid Nodule: From the Ultrasound Image to the Anatomopathological Diagnosis
 The Thyroid Nodule: From the Ultrasound Image to the Anatomopathological Diagnosis Poster No.: C-2229 Congress: ECR 2014 Type: Educational Exhibit Authors: T. González de la Huebra Labrador, A. Herrero
The Thyroid Nodule: From the Ultrasound Image to the Anatomopathological Diagnosis Poster No.: C-2229 Congress: ECR 2014 Type: Educational Exhibit Authors: T. González de la Huebra Labrador, A. Herrero
Evaluation and Management of Thyroid Nodules. Nick Vernetti, MD, FACE Palm Medical Group Las Vegas, Nevada
 Evaluation and Management of Thyroid Nodules Nick Vernetti, MD, FACE Palm Medical Group Las Vegas, Nevada Disclosure Consulting Amgen Speaking Amgen Objectives Understand the significance of incidental
Evaluation and Management of Thyroid Nodules Nick Vernetti, MD, FACE Palm Medical Group Las Vegas, Nevada Disclosure Consulting Amgen Speaking Amgen Objectives Understand the significance of incidental
Tania Gallant MD, FRCPC Internal Medicine Update April
 Tania Gallant MD, FRCPC Internal Medicine Update April 28 2017 Disclosures Honoraria/Ad board: Sanofi-Aventis, Janssen, Merck Frosst, Eli-Lilly, Astra Zeneca, Boehringer-Ingelheim Objectives By the end
Tania Gallant MD, FRCPC Internal Medicine Update April 28 2017 Disclosures Honoraria/Ad board: Sanofi-Aventis, Janssen, Merck Frosst, Eli-Lilly, Astra Zeneca, Boehringer-Ingelheim Objectives By the end
Role of ultrasonography in recognition of malignant potential of thyroid nodules on the basis of their internal composition
 Role of ultrasonography in recognition of malignant potential of thyroid nodules on the basis of their internal composition Nodular thyroid is a common clinical entity. All patients were evaluated by grey
Role of ultrasonography in recognition of malignant potential of thyroid nodules on the basis of their internal composition Nodular thyroid is a common clinical entity. All patients were evaluated by grey
Repeat Thyroid Nodule Fine-Needle Aspiration in Patients With Initial Benign Cytologic Results
 Anatomic Pathology / REPEAT THYROID FINE-NEEDLE ASPIRATION Repeat Thyroid Nodule Fine-Needle Aspiration in Patients With Initial Benign Cytologic Results Melina B. Flanagan, MD, MSPH, 1 N. Paul Ohori,
Anatomic Pathology / REPEAT THYROID FINE-NEEDLE ASPIRATION Repeat Thyroid Nodule Fine-Needle Aspiration in Patients With Initial Benign Cytologic Results Melina B. Flanagan, MD, MSPH, 1 N. Paul Ohori,
Principal Site Investigator ENHANCE (Evaluation of Thyroid FNA Genomic Signature) study: An IRB approved study with funding to Rochester Regional
 study: An IRB approved study with funding to Rochester Regional") October 20 th 2018 Principal Site Investigator ENHANCE (Evaluation of Thyroid FNA Genomic Signature) study: An IRB approved study with funding to Rochester Regional Health from Veracyte Review ultrasound
October 20 th 2018 Principal Site Investigator ENHANCE (Evaluation of Thyroid FNA Genomic Signature) study: An IRB approved study with funding to Rochester Regional Health from Veracyte Review ultrasound
THYROID NODULES: THE ROLE OF ULTRASOUND
 THYROID NODULES: THE ROLE OF ULTRASOUND NOVEMBER 2017 DR. DEAN DURANT DEFINITION Thyroid nodule: Focal area within the thyroid gland with echogenicity different from surrounding parenchyma. THYROID NODULES
THYROID NODULES: THE ROLE OF ULTRASOUND NOVEMBER 2017 DR. DEAN DURANT DEFINITION Thyroid nodule: Focal area within the thyroid gland with echogenicity different from surrounding parenchyma. THYROID NODULES
AACE-AME 2016 Thyroid Nodule Update
 AACE-AME 2016 Thyroid Nodule Update 26 th Annual AACE Meeting & Clinical Congress Austin May 1-5, 2017 Hossein Gharib, MD, MACP, MACE Professor, Mayo Clinic College of Medicine Past President, American
AACE-AME 2016 Thyroid Nodule Update 26 th Annual AACE Meeting & Clinical Congress Austin May 1-5, 2017 Hossein Gharib, MD, MACP, MACE Professor, Mayo Clinic College of Medicine Past President, American
A rare case of solitary toxic nodule in a 3yr old female child a case report
 Volume 3 Issue 1 2013 ISSN: 2250-0359 A rare case of solitary toxic nodule in a 3yr old female child a case report *Chandrasekaran Maharajan * Poongkodi Karunakaran *Madras Medical College ABSTRACT A three
Volume 3 Issue 1 2013 ISSN: 2250-0359 A rare case of solitary toxic nodule in a 3yr old female child a case report *Chandrasekaran Maharajan * Poongkodi Karunakaran *Madras Medical College ABSTRACT A three
Thyroid Nodules. Hossein Gharib, MD, MACP, MACE
 Thyroid Nodules Hossein Gharib, MD, MACP, MACE Professor of Medicine Mayo Clinic College of Medicine President Elect, American College of Endocrinology University Course January 2008 CP1294362-1 Thyroid
Thyroid Nodules Hossein Gharib, MD, MACP, MACE Professor of Medicine Mayo Clinic College of Medicine President Elect, American College of Endocrinology University Course January 2008 CP1294362-1 Thyroid
Thyroid pathology: What radiologists need to know.
 Thyroid pathology: What radiologists need to know. Poster No.: C-1310 Congress: ECR 2014 Type: Educational Exhibit Authors: C. de la Torre, A. Sánchez Tovar, M. Molinero Pérez, R. Rodriguez Ortega, M.
Thyroid pathology: What radiologists need to know. Poster No.: C-1310 Congress: ECR 2014 Type: Educational Exhibit Authors: C. de la Torre, A. Sánchez Tovar, M. Molinero Pérez, R. Rodriguez Ortega, M.
Thyroid Nodule Risk Stratification and FNA Guidelines
 Thyroid Nodule Risk Stratification and FNA Guidelines Mark A. Lupo, MD, FACE, ECNU Thyroid & Endocrine Center of Florida Assistant Clinical Professor of Medicine Florida State University, College of Medicine
Thyroid Nodule Risk Stratification and FNA Guidelines Mark A. Lupo, MD, FACE, ECNU Thyroid & Endocrine Center of Florida Assistant Clinical Professor of Medicine Florida State University, College of Medicine
The radiological spectrum of thyroid malignancy
 The radiological spectrum of thyroid malignancy Poster No.: C-2575 Congress: ECR 2012 Type: Educational Exhibit Authors: K. Cortis, W. Scicluna, A. Mizzi ; Rabat/MT, Birkirkara/MT Keywords: Ultrasound-Colour
The radiological spectrum of thyroid malignancy Poster No.: C-2575 Congress: ECR 2012 Type: Educational Exhibit Authors: K. Cortis, W. Scicluna, A. Mizzi ; Rabat/MT, Birkirkara/MT Keywords: Ultrasound-Colour
Thyroid Nodules. Family Medicine Refresher Course Geeta Lal MD, FACS April 2, No financial disclosures
 Thyroid Nodules Family Medicine Refresher Course Geeta Lal MD, FACS April 2, 2014 No financial disclosures Objectives Review epidemiology Work up of Thyroid nodules Indications for FNAB Evolving role of
Thyroid Nodules Family Medicine Refresher Course Geeta Lal MD, FACS April 2, 2014 No financial disclosures Objectives Review epidemiology Work up of Thyroid nodules Indications for FNAB Evolving role of
Ultrasonography of the Neck as an Adjunct to FNA. Nicole Massoll M.D.
 Ultrasonography of the Neck as an Adjunct to FNA Nicole Massoll M.D. Basic Features of Head and Neck Ultrasound and Anatomy Nicole Massoll M.D. University of Arkansas for Medical Sciences, Little Rock
Ultrasonography of the Neck as an Adjunct to FNA Nicole Massoll M.D. Basic Features of Head and Neck Ultrasound and Anatomy Nicole Massoll M.D. University of Arkansas for Medical Sciences, Little Rock
Korean Thyroid Imaging Reporting and Data System features of follicular thyroid adenoma and carcinoma: a single-center study
 Korean Thyroid Imaging Reporting and Data System features of follicular thyroid adenoma and carcinoma: a single-center study Jung Won Park 1, Dong Wook Kim 1, Donghyun Kim 1, Jin Wook Baek 1, Yoo Jin Lee
Korean Thyroid Imaging Reporting and Data System features of follicular thyroid adenoma and carcinoma: a single-center study Jung Won Park 1, Dong Wook Kim 1, Donghyun Kim 1, Jin Wook Baek 1, Yoo Jin Lee
Adina Alazraki, MD, FAAP Assistant Professor Radiology and Pediatrics Emory University and Children s Healthcare of Atlanta
 Adina Alazraki, MD, FAAP Assistant Professor Radiology and Pediatrics Emory University and Children s Healthcare of Atlanta Review recently published pediatric guidelines for management of thyroid nodules
Adina Alazraki, MD, FAAP Assistant Professor Radiology and Pediatrics Emory University and Children s Healthcare of Atlanta Review recently published pediatric guidelines for management of thyroid nodules
Sonographic imaging of pediatric thyroid disorders in childhood. Experiences and report in 150 cases
 Sonographic imaging of pediatric thyroid disorders in childhood. Experiences and report in 150 cases M. Mearadji International Foundation for Pediatric Imaging Aid Sonographic technique. Use of high frequency
Sonographic imaging of pediatric thyroid disorders in childhood. Experiences and report in 150 cases M. Mearadji International Foundation for Pediatric Imaging Aid Sonographic technique. Use of high frequency
Evaluation and Management of Thyroid Nodules. Overview of Thyroid Nodules and Their Management. Thyroid Nodule detection: U/S versus Exam
 Overview of Thyroid Nodules and Their Management Matthew D. Ringel, M.D. Professor of Medicine Divisions of Endocrinology and Oncology, The Ohio State University Co-Director, Thyroid Cancer Unit Arthur
Overview of Thyroid Nodules and Their Management Matthew D. Ringel, M.D. Professor of Medicine Divisions of Endocrinology and Oncology, The Ohio State University Co-Director, Thyroid Cancer Unit Arthur
Laly Jose, Sara Ammu Chacko, Simi.
 International Journal of Scientific & Engineering Research, Volume 5, Issue 9, September-2014 512 Ultrasound Guided Fine Needle Aspiration Cytology with Evaluation of Pathological Distribution of Thyroid
International Journal of Scientific & Engineering Research, Volume 5, Issue 9, September-2014 512 Ultrasound Guided Fine Needle Aspiration Cytology with Evaluation of Pathological Distribution of Thyroid
Sonographic differentiation of benign and malignant thyroid nodules: Prospective study
 Sonographic differentiation of benign and malignant thyroid nodules: Prospective study Poster No.: C-1720 Congress: ECR 2010 Type: Scientific Exhibit Topic: Head and Neck Authors: D. W. Kim, Y. H. Lee;
Sonographic differentiation of benign and malignant thyroid nodules: Prospective study Poster No.: C-1720 Congress: ECR 2010 Type: Scientific Exhibit Topic: Head and Neck Authors: D. W. Kim, Y. H. Lee;
Thyroid nodules - medical and surgical management. Endocrinology and Endocrine Surgery Manchester Royal Infirmary
 Thyroid nodules - medical and surgical management JRE Davis NR Parrott Endocrinology and Endocrine Surgery Manchester Royal Infirmary Thyroid nodules - prevalence Thyroid nodules common, increase with
Thyroid nodules - medical and surgical management JRE Davis NR Parrott Endocrinology and Endocrine Surgery Manchester Royal Infirmary Thyroid nodules - prevalence Thyroid nodules common, increase with
Review of Literatures
 Review of Literatures Fine needle biopsy was popular in the Scandinavian countries some four decades ago. Though FNAC for any palpable tumor was first introduced in America in the 1920s by Martin, Ellis
Review of Literatures Fine needle biopsy was popular in the Scandinavian countries some four decades ago. Though FNAC for any palpable tumor was first introduced in America in the 1920s by Martin, Ellis
AACE/ACE Principles of Endocrine Neck Sonography Course
 AACE/ACE Principles of Endocrine Neck Sonography Course Primary objective of thyroid ultrasound: assess for malignant disease Nodular Disease Benign Malignant Goiter Iodine deficient Thyroiditis Organification
AACE/ACE Principles of Endocrine Neck Sonography Course Primary objective of thyroid ultrasound: assess for malignant disease Nodular Disease Benign Malignant Goiter Iodine deficient Thyroiditis Organification
European Journal of Radiology
 European Journal of Radiology 82 (2013) 321 326 Contents lists available at SciVerse ScienceDirect European Journal of Radiology jo ur n al hom epage: www.elsevier.com/locate/ejrad Ultrasonographic criteria
European Journal of Radiology 82 (2013) 321 326 Contents lists available at SciVerse ScienceDirect European Journal of Radiology jo ur n al hom epage: www.elsevier.com/locate/ejrad Ultrasonographic criteria
Sonographic Differentiation of Thyroid Nodules With Eggshell Calcifications
 Article Sonographic Differentiation of Thyroid Nodules With Eggshell Calcifications Byung Moon Kim, MD, Min Jung Kim, MD, Eun-Kyung Kim, MD, Jin Young Kwak, MD, Soon Won Hong, MD, Eun Ju Son, MD, Ki Hwang
Article Sonographic Differentiation of Thyroid Nodules With Eggshell Calcifications Byung Moon Kim, MD, Min Jung Kim, MD, Eun-Kyung Kim, MD, Jin Young Kwak, MD, Soon Won Hong, MD, Eun Ju Son, MD, Ki Hwang
The Frozen Section: Diagnostic Challenges and Pitfalls
 The Frozen Section: Diagnostic Challenges and Pitfalls William C. Faquin, M.D., Ph.D. Director, Head and Neck Pathology Massachusetts General Hospital & Massachusetts Eye and Ear Infirmary Harvard Medical
The Frozen Section: Diagnostic Challenges and Pitfalls William C. Faquin, M.D., Ph.D. Director, Head and Neck Pathology Massachusetts General Hospital & Massachusetts Eye and Ear Infirmary Harvard Medical
Ultrasound-Guided Fine-Needle Aspiration of Thyroid Nodules: New events
 Ultrasound-Guided Fine-Needle Aspiration of Thyroid Nodules: New events Sandrine Rorive, M.D., PhD. Erasme Hospital - Université Libre de Bruxelles (ULB) INTRODUCTION The assessment of thyroid nodules
Ultrasound-Guided Fine-Needle Aspiration of Thyroid Nodules: New events Sandrine Rorive, M.D., PhD. Erasme Hospital - Université Libre de Bruxelles (ULB) INTRODUCTION The assessment of thyroid nodules
Can Color Doppler Sonography Aid in the Prediction of Malignancy of Thyroid Nodules?
 Article Can Color Doppler Sonography Aid in the Prediction of Malignancy of Thyroid Nodules? Mary C. Frates, MD, Carol B. Benson, MD, Peter M. Doubilet, MD, PhD, Edmund S. Cibas, MD, Ellen Marqusee, MD
Article Can Color Doppler Sonography Aid in the Prediction of Malignancy of Thyroid Nodules? Mary C. Frates, MD, Carol B. Benson, MD, Peter M. Doubilet, MD, PhD, Edmund S. Cibas, MD, Ellen Marqusee, MD
Repeat Ultrasound-Guided Fine-Needle Aspiration for Thyroid Nodules 10 mm or Larger Can Be Performed 10.7 Months After Initial Nondiagnostic Results
 Neuroradiology/Head and Neck Imaging Original Research Moon et al. Repeat US-Guided FNA of Thyroid Nodules After Nondiagnostic Results Neuroradiology/Head and Neck Imaging Original Research Hee Jung Moon
Neuroradiology/Head and Neck Imaging Original Research Moon et al. Repeat US-Guided FNA of Thyroid Nodules After Nondiagnostic Results Neuroradiology/Head and Neck Imaging Original Research Hee Jung Moon
Practical Approach to Thyroid Nodules:Ultrasound Criteria for Performing FNA Revisited
 Practical Approach to Thyroid Nodules:Ultrasound Criteria for Performing FNA Revisited Poster No.: C-0100 Congress: ECR 2013 Type: Educational Exhibit Authors: S. Kuzmich, S. Sritharan, S. MUKUNDHAN, M.
Practical Approach to Thyroid Nodules:Ultrasound Criteria for Performing FNA Revisited Poster No.: C-0100 Congress: ECR 2013 Type: Educational Exhibit Authors: S. Kuzmich, S. Sritharan, S. MUKUNDHAN, M.
A Study of Thyroid Swellings and Correlation between FNAC and Histopathology Results
 International Journal of Current Microbiology and Applied Sciences ISSN: 2319-7706 Volume 6 Number 4 (2017) pp. 265-269 Journal homepage: http://www.ijcmas.com Original Research Article https://doi.org/10.20546/ijcmas.2017.604.030
International Journal of Current Microbiology and Applied Sciences ISSN: 2319-7706 Volume 6 Number 4 (2017) pp. 265-269 Journal homepage: http://www.ijcmas.com Original Research Article https://doi.org/10.20546/ijcmas.2017.604.030
Update on Thyroid FNA The Bethesda System. Shikha Bose M.D. Associate Professor Cedars Sinai Medical Center
 Update on Thyroid FNA The Bethesda System Shikha Bose M.D. Associate Professor Cedars Sinai Medical Center Thyroid Nodules Frequent occurrence Palpable: 4-7% of adults Ultrasound: 10-31% Majority benign
Update on Thyroid FNA The Bethesda System Shikha Bose M.D. Associate Professor Cedars Sinai Medical Center Thyroid Nodules Frequent occurrence Palpable: 4-7% of adults Ultrasound: 10-31% Majority benign
Background to the Thyroid Nodule
 William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital THYROID FNA: PART I Background to the
William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital THYROID FNA: PART I Background to the
Gray Scale and Colour Doppler Sonography in the Evaluation of Follicular Neoplasms of Thyroid
 DOI: 10.7860/IJARS/2018/24979:2393 Radiology Section Original Article Gray Scale and Colour Doppler Sonography in the Evaluation of Follicular Neoplasms of Thyroid Pradeep Hagalahalli Nagarajegowda, VISHWANATH
DOI: 10.7860/IJARS/2018/24979:2393 Radiology Section Original Article Gray Scale and Colour Doppler Sonography in the Evaluation of Follicular Neoplasms of Thyroid Pradeep Hagalahalli Nagarajegowda, VISHWANATH
5/18/2013. Most thyroid nodules are benign. Thyroid nodules: new techniques in evaluation
 Most thyroid nodules are benign Thyroid nodules: new techniques in evaluation Incidence Etiology Risk factors Diagnosis Gene classification system Treatment Postgraduate Course in General Surgery Jessica
Most thyroid nodules are benign Thyroid nodules: new techniques in evaluation Incidence Etiology Risk factors Diagnosis Gene classification system Treatment Postgraduate Course in General Surgery Jessica
Ultrasound Evaluation of Thyroid Nodules. October 2016
 Ultrasound Evaluation of Thyroid Nodules October 2016 Thyroid Nodules Primary goal is to determine if a nodule is malignant and needs surgery, or is benign and does not need surgery. Concerning Clinical
Ultrasound Evaluation of Thyroid Nodules October 2016 Thyroid Nodules Primary goal is to determine if a nodule is malignant and needs surgery, or is benign and does not need surgery. Concerning Clinical
Thyroid Nodule. Disclosure. Learning Objectives P A P A P A 3/18/2014. Nothing to disclose.
 Thyroid Nodule Evaluating the patient with a thyroid nodule and some management options. Miguel V. Valdez PA C Disclosure Nothing to disclose. Learning Objectives Examination of thyroid gland Options for
Thyroid Nodule Evaluating the patient with a thyroid nodule and some management options. Miguel V. Valdez PA C Disclosure Nothing to disclose. Learning Objectives Examination of thyroid gland Options for
Thyroid nodules. Most thyroid nodules are benign
 Thyroid nodules Postgraduate Course in General Surgery Jessica E. Gosnell MD Assistant Professor March 22, 2011 Most thyroid nodules are benign thyroid nodules occur in 77% of the world s population palpable
Thyroid nodules Postgraduate Course in General Surgery Jessica E. Gosnell MD Assistant Professor March 22, 2011 Most thyroid nodules are benign thyroid nodules occur in 77% of the world s population palpable
NODULAR GOITRE EVALUATIONIN THE REGION OF THE HEALTHCARE CENTER OF NOVI PAZAR
 48 MEDICINSKI GLASNIK / str. 48-57 Mersudin Mulić *, Bilsana Mulić NODULAR GOITRE EVALUATIONIN THE REGION OF THE HEALTHCARE CENTER OF NOVI PAZAR Summary: The term thyroid nodus refers to any irregular
48 MEDICINSKI GLASNIK / str. 48-57 Mersudin Mulić *, Bilsana Mulić NODULAR GOITRE EVALUATIONIN THE REGION OF THE HEALTHCARE CENTER OF NOVI PAZAR Summary: The term thyroid nodus refers to any irregular
Women s Health in General Practice Symposium 2015 Thyroid & Parathyroid Cases
 Women s Health in General Practice Symposium 2015 Thyroid & Parathyroid Cases Bill Fleming Epworth Freemasons Hospital 1 Common Endocrine Presentations anatomical problems thyroid nodule / goitre embryological
Women s Health in General Practice Symposium 2015 Thyroid & Parathyroid Cases Bill Fleming Epworth Freemasons Hospital 1 Common Endocrine Presentations anatomical problems thyroid nodule / goitre embryological
Thyroid Ultrasonography: clinical and radiological correlations
 Thyroid Ultrasonography: clinical and radiological correlations Dr.M.Thijs Radiology Anatomy Inflammatory Thyroid Disease Benign lesions Thyroid tumors Thyroglossal duct cyst Anatomy Transverse Longitudinal
Thyroid Ultrasonography: clinical and radiological correlations Dr.M.Thijs Radiology Anatomy Inflammatory Thyroid Disease Benign lesions Thyroid tumors Thyroglossal duct cyst Anatomy Transverse Longitudinal
Work Up & Evaluation of Thyroid Nodules In 2013: State of The Art
 Work Up & Evaluation of Thyroid Nodules In 2013: State of The Art BC Surgical Oncology Network, Fall Update Todd McMullen MD PhD FRCSC FACS Endocrine Surgeon Divisions of General Surgery and Oncology Director,
Work Up & Evaluation of Thyroid Nodules In 2013: State of The Art BC Surgical Oncology Network, Fall Update Todd McMullen MD PhD FRCSC FACS Endocrine Surgeon Divisions of General Surgery and Oncology Director,
USGFNA of thyroid nodules
 US Guided FNA (USGFNA) of neck masses INTERVENTIONAL HEAD & NECK ULTRASOUND Brendan C. Stack, Jr., MD., FACS, FACE Professor Otolaryngology-Head and Neck Surgery Indications Technique Interpretation Results
US Guided FNA (USGFNA) of neck masses INTERVENTIONAL HEAD & NECK ULTRASOUND Brendan C. Stack, Jr., MD., FACS, FACE Professor Otolaryngology-Head and Neck Surgery Indications Technique Interpretation Results
challenge is to distinguish the few clinically significant malignant nodules from many benign ones (Table 1).
.") Indian Journal of Mednodent and Allied Sciences Vol. 3, No. 2, June 2015, pp- 71-76 IndianJournals.com A product of Diva Enterprises Pvt. Ltd. DOI : 10.5958/2347-6206.2015.00018.7 Original Research Ultrasound
Indian Journal of Mednodent and Allied Sciences Vol. 3, No. 2, June 2015, pp- 71-76 IndianJournals.com A product of Diva Enterprises Pvt. Ltd. DOI : 10.5958/2347-6206.2015.00018.7 Original Research Ultrasound
Original Research Article
 ROLE OF ULTRASONOGRAPHY IN THE EVALUATION OF THYROID NODULES WITH FNAC CORRELATION Surabhi Chakraborty 1, Prashantha Ishwar 2 1Junior Resident, Department of Radiodiagnosis, Adichunchanagiri Institute
ROLE OF ULTRASONOGRAPHY IN THE EVALUATION OF THYROID NODULES WITH FNAC CORRELATION Surabhi Chakraborty 1, Prashantha Ishwar 2 1Junior Resident, Department of Radiodiagnosis, Adichunchanagiri Institute
HEAD AND NECK ENDOCRINE SURGERY
 HEAD AND NECK ENDOCRINE SURGERY OCTOBER 22-23, 2010 THE MARK HOPKINS SAN FRANCISCO, CA THYROID FNA AND CYTOPATHOLOGY THEODORE R. MILLER, MD THE THYROID NODULE Prevalence of palpable nodule: Female ~ 6%
HEAD AND NECK ENDOCRINE SURGERY OCTOBER 22-23, 2010 THE MARK HOPKINS SAN FRANCISCO, CA THYROID FNA AND CYTOPATHOLOGY THEODORE R. MILLER, MD THE THYROID NODULE Prevalence of palpable nodule: Female ~ 6%
Thyroid nodules 3/22/2011. Most thyroid nodules are benign. Thyroid nodules: differential diagnosis
 Most thyroid nodules are benign Thyroid nodules Postgraduate Course in General Surgery thyroid nodules occur in 77% of the world s population palpable thyroid nodules occur in about 5% of women and 1%
Most thyroid nodules are benign Thyroid nodules Postgraduate Course in General Surgery thyroid nodules occur in 77% of the world s population palpable thyroid nodules occur in about 5% of women and 1%
ArticleInfo. Spring School of Thyroidology organized by the Polish Thyroid Association 2014: abstracts of invited lectures
 Ultrasound and cytological diagnostics of thyroid - its proper application in case of coexisting disturbing clinical signs and symptoms, suggestive of active proliferative lesion Andrzej Lewiński, Aff1
Ultrasound and cytological diagnostics of thyroid - its proper application in case of coexisting disturbing clinical signs and symptoms, suggestive of active proliferative lesion Andrzej Lewiński, Aff1
Evaluation of Neck Mass. Disclosure. Learning Objectives 3/24/2014. Karen T. Pitman MD, FACS Banner MDACC, Gilbert AZ. Nothing to disclose
 Evaluation of Neck Mass Karen T. Pitman MD, FACS Banner MDACC, Gilbert AZ Nothing to disclose Disclosure Learning Objectives 1. Describe a systematic method to evaluate a patient with a neck mass 2. Select
Evaluation of Neck Mass Karen T. Pitman MD, FACS Banner MDACC, Gilbert AZ Nothing to disclose Disclosure Learning Objectives 1. Describe a systematic method to evaluate a patient with a neck mass 2. Select
Index terms: Thyroid Ultrasonography Pathology Cancer. DOI: /kjr
 Histopathologic Findings Related to the Indeterminate or Inadequate Results of Fine-Needle Aspiration Biopsy and Correlation with Ultrasonographic Findings in Papillary Thyroid Carcinomas So Lyung Jung,
Histopathologic Findings Related to the Indeterminate or Inadequate Results of Fine-Needle Aspiration Biopsy and Correlation with Ultrasonographic Findings in Papillary Thyroid Carcinomas So Lyung Jung,
Thyroid & Salivary glands.
 Thyroid & Salivary glands. www.headandneckultrasound.co.uk Rhodri M Evans Incidence of nodules. 3 7% have palpable nodule 30 70% have nodules detected on Ultrasound x 10 Increase in incidence of nodules
Thyroid & Salivary glands. www.headandneckultrasound.co.uk Rhodri M Evans Incidence of nodules. 3 7% have palpable nodule 30 70% have nodules detected on Ultrasound x 10 Increase in incidence of nodules
Cytology for the Endocrinologist. Nicole Massoll M.D
 Cytology for the Endocrinologist Nicole Massoll M.D Objectives Discuss slide preperation Definitions of adequacy ROSE (Rapid On-Site Evaluation) Thyroid Cytology Adequacy Nicole Massoll M.D. University
Cytology for the Endocrinologist Nicole Massoll M.D Objectives Discuss slide preperation Definitions of adequacy ROSE (Rapid On-Site Evaluation) Thyroid Cytology Adequacy Nicole Massoll M.D. University
Su-kyoung Jeh, MD 1 So Lyung Jung, MD 2 Bum Soo Kim, MD 2 Yoen Soo Lee, MD 3
 Evaluating the Degree of Conformity of Papillary Carcinoma and Follicular Carcinoma to the Reported Ultrasonographic Findings of Malignant Thyroid Tumor Su-kyoung Jeh, MD 1 So Lyung Jung, MD 2 Bum Soo
Evaluating the Degree of Conformity of Papillary Carcinoma and Follicular Carcinoma to the Reported Ultrasonographic Findings of Malignant Thyroid Tumor Su-kyoung Jeh, MD 1 So Lyung Jung, MD 2 Bum Soo
Role of Ultrasound in Thyroid Pathologies
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861. Volume 9, Issue 4 (Sep.- Oct. 2013), PP 70-98 Role of Ultrasound in Thyroid Pathologies Dr. Awad Mohamed Elkhadir
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861. Volume 9, Issue 4 (Sep.- Oct. 2013), PP 70-98 Role of Ultrasound in Thyroid Pathologies Dr. Awad Mohamed Elkhadir
Shadow because the air
 Thyroid Ultrasound Thyroid US examination needs: 1. high frequency transducer 2. extended patient's neck 3. check all the neck area because the swelling could be in areas other than the thyroid such as
Thyroid Ultrasound Thyroid US examination needs: 1. high frequency transducer 2. extended patient's neck 3. check all the neck area because the swelling could be in areas other than the thyroid such as
The Comparison of Scintigraphic and Ultrasonographic Evaluation Criteria of Thyroid Nodules with Histopathologic Findings
 Research Article The Comparison of Scintigraphic and Ultrasonographic Evaluation Criteria of Thyroid Nodules with Histopathologic Findings Seracettin Eğin * Department of General Surgery, University of
Research Article The Comparison of Scintigraphic and Ultrasonographic Evaluation Criteria of Thyroid Nodules with Histopathologic Findings Seracettin Eğin * Department of General Surgery, University of
MTP: Thyroid Nodules
 Canadian Endocrine Update MTP: Thyroid Nodules Deric Morrison MD, FRCP, ECNU Assistant Professor, Division of Endocrinology and Metabolism, Western University April 2014 Faculty/Presenter Disclosure Faculty:
Canadian Endocrine Update MTP: Thyroid Nodules Deric Morrison MD, FRCP, ECNU Assistant Professor, Division of Endocrinology and Metabolism, Western University April 2014 Faculty/Presenter Disclosure Faculty:
Thyroid nodules, when to perform a fine needle aspiration
 Thyroid nodules, when to perform a fine needle aspiration Poster No.: C-1828 Congress: ECR 2015 Type: Educational Exhibit Authors: A. I. Fernández Martín, E. Pertusa Santos, E. Dominguez 1 1 1 2 1 Franjo,
Thyroid nodules, when to perform a fine needle aspiration Poster No.: C-1828 Congress: ECR 2015 Type: Educational Exhibit Authors: A. I. Fernández Martín, E. Pertusa Santos, E. Dominguez 1 1 1 2 1 Franjo,
Interpreting the Thyroid Ultrasound Report
 Interpreting the Thyroid Ultrasound Report Michael Neuman, MD Radiology Specialists of the Northwest February 2, 2018 Goals Review indications for thyroid ultrasound Review the role of ultrasound in evaluation
Interpreting the Thyroid Ultrasound Report Michael Neuman, MD Radiology Specialists of the Northwest February 2, 2018 Goals Review indications for thyroid ultrasound Review the role of ultrasound in evaluation
AACE 2018 Advanced Endocrine Neck Ultrasound and UGFNA Course
 AACE 2018 Advanced Endocrine Neck Ultrasound and UGFNA Course Describe the sonographic appearance of diffuse thyroid diseases: autoimmune thyroid disease Review non thyroidal findings that can be encountered
AACE 2018 Advanced Endocrine Neck Ultrasound and UGFNA Course Describe the sonographic appearance of diffuse thyroid diseases: autoimmune thyroid disease Review non thyroidal findings that can be encountered
Risk of Thyroid Cancer Based on Thyroid Ultrasound Imaging Characteristics
 Risk of Thyroid Cancer Based on Thyroid Ultrasound Imaging Characteristics Diabetes Update and Advances in Endocrinology & Metabolism Vickie A Feldstein MD Rebecca Smith- Bindman MD Department of Radiology
Risk of Thyroid Cancer Based on Thyroid Ultrasound Imaging Characteristics Diabetes Update and Advances in Endocrinology & Metabolism Vickie A Feldstein MD Rebecca Smith- Bindman MD Department of Radiology
Evaluation of Thyroid Nodules
 Evaluation of Thyroid Nodules Stephan Kowalyk, MD January 25 28, 2018 1 Primary goal Exclude malignancy Incidental thyroid nodules If found on CT, MRI, PET scan, carotid Doppler ULTRASOUND!! January 25
Evaluation of Thyroid Nodules Stephan Kowalyk, MD January 25 28, 2018 1 Primary goal Exclude malignancy Incidental thyroid nodules If found on CT, MRI, PET scan, carotid Doppler ULTRASOUND!! January 25
4/22/2010. Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey.
 Management of Differentiated Thyroid Cancer: Head Neck Surgeon Perspective Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey Thyroid gland Small endocrine gland:
Management of Differentiated Thyroid Cancer: Head Neck Surgeon Perspective Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey Thyroid gland Small endocrine gland:
Volume 2 Issue ISSN
 Volume 2 Issue 3 2012 ISSN 2250-0359 Correlation of fine needle aspiration and final histopathology in thyroid disease: a series of 702 patients managed in an endocrine surgical unit *Chandrasekaran Maharajan
Volume 2 Issue 3 2012 ISSN 2250-0359 Correlation of fine needle aspiration and final histopathology in thyroid disease: a series of 702 patients managed in an endocrine surgical unit *Chandrasekaran Maharajan
Endocrine University, 2016 AACE-ACE-MAYO CLINIC
 Endocrine University, 2016 AACE-ACE-MAYO CLINIC Dev Abraham MD, MRCP (UK), ECNU Professor of Medicine (clinical), Division of Endocrinology Adjunct Professor of Surgery and Pathology Medical Director,
Endocrine University, 2016 AACE-ACE-MAYO CLINIC Dev Abraham MD, MRCP (UK), ECNU Professor of Medicine (clinical), Division of Endocrinology Adjunct Professor of Surgery and Pathology Medical Director,
Compliance of British Thyroid Ultrasound "U" Guidelines Are we all speaking the "Unified" Thyroid language?
 Compliance of British Thyroid Ultrasound "U" Guidelines Are we all speaking the "Unified" Thyroid language? Poster No.: C-1158 Congress: ECR 2016 Type: Scientific Exhibit Authors: P. Gopalan, S. Singh,
Compliance of British Thyroid Ultrasound "U" Guidelines Are we all speaking the "Unified" Thyroid language? Poster No.: C-1158 Congress: ECR 2016 Type: Scientific Exhibit Authors: P. Gopalan, S. Singh,
Thyroid & Parathyroid glands Ultrasound evaluation.
 Thyroid & Parathyroid glands Ultrasound evaluation. www.headandneckultrasound.co.uk Rhodri M Evans Incidence 70 Thyroid Nodules 30 Palpation 50 Age 100 Incidence 70 Thyroid Nodules US/Autopsy 30 Palpation
Thyroid & Parathyroid glands Ultrasound evaluation. www.headandneckultrasound.co.uk Rhodri M Evans Incidence 70 Thyroid Nodules 30 Palpation 50 Age 100 Incidence 70 Thyroid Nodules US/Autopsy 30 Palpation
Management of Thyroid Nodules. February 2 nd, 2018 Sarah Hopkins
 Management of Thyroid Nodules February 2 nd, 2018 Sarah Hopkins No disclosures Goals: Review Initial Evaluation of Thyroid Nodules Review Indications for Biopsy Approach to Multinodular Goiter Review Management
Management of Thyroid Nodules February 2 nd, 2018 Sarah Hopkins No disclosures Goals: Review Initial Evaluation of Thyroid Nodules Review Indications for Biopsy Approach to Multinodular Goiter Review Management
Normal thyroid tissue
 Thyroid Pathology Overview Normal thyroid tissue Normal thyroid tissue with follicles filled with colloid. Thyroid cells form follicles, spheres of epithelial cells (always single layered in health, usually
Thyroid Pathology Overview Normal thyroid tissue Normal thyroid tissue with follicles filled with colloid. Thyroid cells form follicles, spheres of epithelial cells (always single layered in health, usually
Ultrasound 5/1/2017. Ultrasound in the FNA Clinic. Uses of Ultrasound Outside of. Cardiology
 Ultrasound in the FNA Clinic Martha Bishop Pitman, M.D. Director, Cytopathology Massachusetts General Hospital Professor of Pathology Harvard Medical School Boston, MA Uses of Ultrasound Outside of Radiology
Ultrasound in the FNA Clinic Martha Bishop Pitman, M.D. Director, Cytopathology Massachusetts General Hospital Professor of Pathology Harvard Medical School Boston, MA Uses of Ultrasound Outside of Radiology
2017 ATA Victoria Advanced Thyroid US
 2017 ATA Victoria Advanced Thyroid US DIFFUSE THYROID CONDITIONS Stephanie L. Lee, M.D., Ph.D. Director of the BMC Thyroid Nodule and Cancer Center Section of Endocrinology, Diabetes and Nutrition Boston
2017 ATA Victoria Advanced Thyroid US DIFFUSE THYROID CONDITIONS Stephanie L. Lee, M.D., Ph.D. Director of the BMC Thyroid Nodule and Cancer Center Section of Endocrinology, Diabetes and Nutrition Boston
AACE/AME/ETA Guidelines
 AACE/AME/ETA Guidelines American Association of Clinical Endocrinologists, Associazione Medici Endocrinologi, and European Thyroid Association Medical Guidelines for Clinical Practice for the Diagnosis
AACE/AME/ETA Guidelines American Association of Clinical Endocrinologists, Associazione Medici Endocrinologi, and European Thyroid Association Medical Guidelines for Clinical Practice for the Diagnosis
Index. radiologic.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A ACC. See Adrenal cortical carcinoma. Acromegaly and the pituitary gland, 551 Acute suppurative thyroiditis, 405, 406 Addison, Thomas and
Index Note: Page numbers of article titles are in boldface type. A ACC. See Adrenal cortical carcinoma. Acromegaly and the pituitary gland, 551 Acute suppurative thyroiditis, 405, 406 Addison, Thomas and