OBESITY MANAGEMENT: DIET/EXERCISE, NEW DRUGS AND/OR SURGERY?
|
|
|
- Richard May
- 6 years ago
- Views:
Transcription
1 OBESITY MANAGEMENT: DIET/EXERCISE, NEW DRUGS AND/OR SURGERY? ERIC VOLCKMANN, MD DIRECTOR OF BARIATRIC SURGERY OCTOBER 20, 2017
2 OBJECTIVES Define prevalence and health effects of obesity Discuss different therapies for weight loss including diet & lifestyle modification, physical activity, medications, and surgery Compare and contrast commonly performed bariatric surgical procedures Review non-surgical procedures for weight loss
 Based on a ratio of")

3 WHAT IS OBESITY BMI Calculator BMI (body mass index) Based on a ratio of height and weight Body composition not accounted for Defined as BMI 30 kg/m 2

![Obesity [body mass index (BMI) 30] is an epidemic in the United](/docs-images/77/76167661/images/4-2.jpg "States Obesity rate in Utah in 2015 was 25.")
4 PREVALENCE OF OBESITY IN THE U.S. Obesity [body mass index (BMI) 30] is an epidemic in the United States Obesity rate in Utah in 2015 was 25.4% 2016 Centers for Disease Control and Protection Data and Statistics:
5 EFFECTS OF OBESITY: HEALTH RISKS Increased morbidity Type II diabetes High blood pressure/dyslipidemia Cardiovascular disease and stroke Osteoarthritis Obstructive sleep apnea and respiratory problems Gallbladder disease Endometrial, breast, prostate, and colon cancer Increased complications of pregnancy, menstrual irregularity & PCOS, stress incontinence & depression Increased mortality Obese individuals (BMI 30 kg/m 2 ) have % all cause increase in mortality vs. normal weight individuals (BMI kg/m 2 ) 1998 NIH Clinical Guidelines on the Identification, evaluation, and treatment of Overweight, and Obesity in Adults
6 EFFECTS OF OBESITY: QUALITY OF LIFE Common Patient Complaints Chronic fatigue and joint pain Unable to participate in activities that they enjoy Difficulty with activities of daily living and hygiene Can t fit into seats on airplanes, in movie theaters, and on amusement park rides Social stigma and discrimination Multiple medications for weight-related medical problems
7 EFFECTS OF OBESITY: FINANCIAL COST Obesity is expensive: High lifetime direct medical costs Medical costs rise with increasing BMI Obesity related costs are expected to continue to rise in the next 15 years High cost to employers: lost productivity absenteeism (second only to depression) Bray GA, et al. Lancet. 2016
8 MODERN APPROACH TO OBESITY: Acknowledges multifactorial nature of obesity : Genetic, epigenetic, physiological, behavioral, sociocultural, and environmental factors Factors lead to energy imbalance: Foundation of any weight effort loss includes: Lifestyle change Diet Physical activity Bray GA, et al. Lancet. 2016
9 MODERN APPROACH TO OBESITY For Individuals who struggle with weight loss but would benefit from it: Pharmacologic therapy Approved medications for chronic weight management Medications contributing to weight gain Surgical therapy New non-surgical procedures

10 AACE/ACE OBESITY GUIDELINES- PREVENTION Garvey WT, et al. Endocr Pract. 2016

11 AACE/ACE OBESITY GUIDELINES- LIFESTYLE Important Points: Diet macronutrient composition generally affects weight loss less than adherence rates. Best to provide low energy diets that are likely to be adhered to and provide health benefits. Type of physical activity (e.g. aerobic vs. resistance and intensity level) doesn t appear to affect overall weight loss. Garvey WT, et al. Endocr Pract. 2016
 and BMI 27 kg/m 2 with comorbidities or 30 kg/m 2 and higher. Consider surgery at BMI 35 kg/m 2 with comorbidity. Garvey WT, et al. Endocr Pract.")
12 AACE/ACE OBESITY GUIDELINES- MANAGEMENT Important Points: AACE/ACE staging emphasizes complications > BMI Pharmacotherapy added with failure of meaningful weight loss (> 5% total body weight) and BMI 27 kg/m 2 with comorbidities or 30 kg/m 2 and higher. Consider surgery at BMI 35 kg/m 2 with comorbidity. Garvey WT, et al. Endocr Pract. 2016
13 AHA/ACC/TOS OBESITY GUIDELINES- MANAGEMENT Recommendation 1 grade A (strong) Use BMI as a screening test for patients who might be at risk for CVD, type 2 DM, and all-cause mortality Use waist circumference as an indicator of risk for CVD, type 2 DM, and all-cause mortality. Recommendation 2 grade A Counsel patients that weight loss (3% 5%) results in improvements in triglycerides, diabetes measures, and prediabetes. Greater amounts will improve blood pressure & cholesterol levels. Recommendation 3 grade A Prescribe a reduced caloric diet as part of a comprehensive lifestyle intervention regardless of macronutrient content of the diet. Recommendation 4 grade A Patients needing weight loss should receive a comprehensive program that is at least 6 months or longer in length including diet, physical activity, and behavior modification. Medications are considered appropriate for those with BMI >30 or >27 with a comorbidity (expert opinion). Recommendation 5 grade A Consider bariatric surgery for patients with BMI >35 plus a comorbidity or >40 Apovian CM, et al. Circulation 2015
14 PHARMACOTHERAPY-GENERAL PRINICIPLES Many medications are associated with weight gain or loss Obese patients should avoid medications that produce weight gain (when possible) and use weight neutral medications or those associated with weight loss 5 medications approved for long-term weight loss in U.S. Orlistat, Lorcaserin, Phentermine/topiramate ER, Naltrexone SR/ bupropion SR, and Liraglutide [Phentermine FDA-approved for short term use only (12 weeks)] Medications should be used in conjunction with lifestyle modification Prescriber and patient should be familiar with complications No medication is effective in every patient (3-4 months for meaningful weight loss) Bray GA, et al. Lancet. 2016

15 PHARMACOTHERAPY-MEDICATIONS THAT AFFECT WEIGHT Bray GA, et al. Lancet. 2016
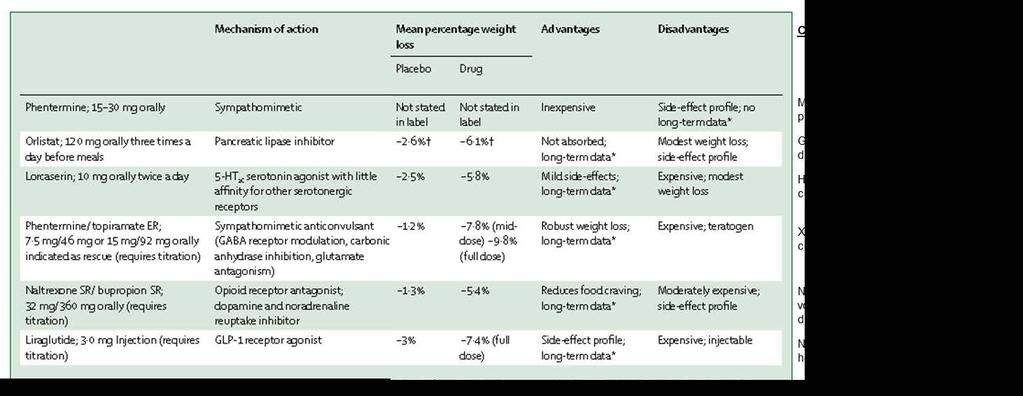
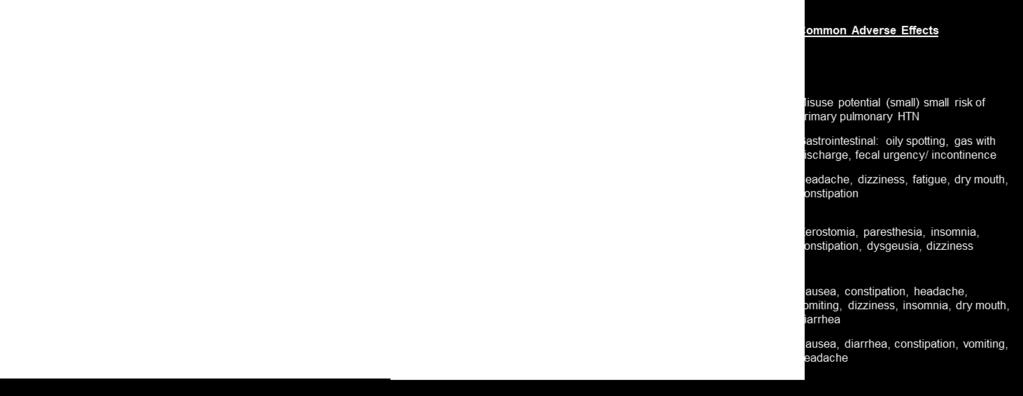
16 PHARMACOTHERAPY-AVAILABLE MEDICATIONS Bray GA, et al. Lancet Wharton, S, Can J. Diabetes 2016
17 PHARMACOTHERAPY-EFFECTIVENESS 2016 Systematic Review and Meta-analysis of 28 RCTs of FDAapproved medications for long-term obesity treatment Among overweight or obese adults, all approved medications were associated with achieving at least 5% weight loss at 52 weeks Phentermine-topiramate and liraglutide were associated with the highest odds of achieving at least 5% weight loss Khera R, et al. JAMA. 2016
18 SURGICAL TREATMENT OPTIONS Malabsorptive & Restrictive Roux-en-Y Gastric Bypass Biliopancreatic Diversion with Duodenal Switch Purely Restrictive Sleeve Gastrectomy Laparoscopic Adjustable Gastric Banding (e.g. Lap-Band )
19 QUALIFICATION FOR BARIATRIC SURGERY Patients with clinically severe obesity Based on 1991 NIH Consensus Conference Statement on Gastrointestinal Surgery for Obesity BMI 40 (equivalent to being about 100 lbs. overweight) BMI 35 with weight related medical problem Type II Diabetes Hypertension, hyperlipidemia, coronary artery disease Obstructive sleep apnea Osteoarthritis 1998 NIH Clinical Guidelines on the Identification, evaluation, and treatment of Overweight, and Obesity in Adults
20 CANDIDATES FOR BARIATRIC SURGERY Well-informed, well-motivated individuals who: Meet weight and health criteria for surgery Understand and accept operative risks Modify dietary habits and lifestyle Tool for weight loss Commit to long-term follow-up care Lifelong commitment and not a short term fix"
21 PATHWAY TO SURGERY Information session Insurance verification- Covered benefit? Complete intake form, smoking policy, sleep apnea screening form, and 2-day food record Initial appointment with surgeon Evaluations: dietician (evaluation & 3-6 mos. education/medically supervised weight loss), psychologist (psychological testing), medical, endoscopy and/or upper GI series Preoperative visit with surgeon +/- anesthesiologist Scheduled bariatric surgery procedure Insurance pre-authorization VLCD 4 weeks before surgery

22 BENEFITS OF SURGERY: WEIGHT-RELATED MEDICAL PROBLEMS Buchwald H, et al. JAMA 2004
23 BENEFITS OF SURGERY: MORTALITY Diabetic-related causes decreased by 92% Cancer deaths decreased by 60% Coronary causes decreased by 56% All cause mortality decreased by 40% Adams TD, et al. NEJM 2007
24 BENEFITS OF SURGERY: DURABLE WEIGHT LOSS Systematic review of literature and meta-analysis of 22,094 bariatric patients Low failure rate with mean excess body weight loss (EBWL) of 61.2% Retrospective review of 272 gastric bypass patients 67.6% EBWL at mean of 11.4 years 71.9% (morbid obesity) 59.7% (super obesity) Buchwald H, et al. JAMA 2004 Christou, Ann Surg 2006
25 CONTRAINDICATIONS TO SURGERY Age over 70* / adolescents* Smoking, smokeless tobacco, electronic cigarette, Alcohol or drug abuse Non-ambulatory patients* Severe cardiac or pulmonary comorbities* Organ failure or Impending failure* Inability to comply with nutritional requirements Mental illness (untreated) Women should avoid pregnancy for 1-2 years after surgery (2 years preferred) *Relative Contraindications
26 ROUX-EN-Y GASTRIC BYPASS

27 ROUX-EN-Y GASTRIC BYPASS 30 ml pouch ~15-16 mm stoma 150 cm Roux limb Biliopancreatic limb Common channel
28 ROUX-EN-Y GASTRIC BYPASS Gold standard bariatric surgical procedure About 60-80% excess body weight (EBW) loss in months with >75% control of comorbidities Cures GERD Effects on type II diabetes independent of wt. loss Patients typically regain less than 15 percent of their weight after 5-10 years Difficult to reverse 300% increase of alcohol potency Risk of ulcers (NO NSAIDs, steroids, tobacco) Higher risk of vitamin and mineral deficiencies? Dumping Syndrome (+/-?)

29 VERTICAL SLEEVE GASTRECTOMY

30 VERTICAL SLEEVE GASTRECTOMY 2006, Ethicon Endo-Surgery. Inc.
31 SLEEVE GASTRECTOMY No malabsorption with similar follow-up to gastric bypass Excess body weight loss between gastric banding and gastric bypass (50-70% EBWL) Lower risk of ulcers compared to gastric bypass Few long term studies > 5 years May worsen/cause GERD (Barrett s esophagus) Gastric stenosis Not reversible Staple line leaks difficult to manage
32 LAPAROSCOPIC ADJUSTABLE GASTRIC BANDING (LAGB)

 Small")

33 LAPAROSCOPIC ADJUSTABLE GASTRIC BANDING (LAGB) Small gastric pouch Adjustable band Port for adjustments
34 ADJUSTABLE GASTRIC BANDING (LAGB) Creates small gastric pouch limiting food consumption Causes feeling of fullness with small amounts of food Patients lose up to 50% of their EBW by 1 ½ -5 years Goal weight loss: 1-2 lbs/week or 4-8 lbs/month Monthly evaluations during 1 st 12 months Resolution of type II diabetes mirrors weight loss Adjustable and reversible May worsen/cause GERD Up to 25% fail to lose 30% of EBW by 5 years


35 OTHER BARIATRIC PROCEDURES Biliopancreatic Diversion with Duodenal Switch Vertical Banded Gastroplasty 150 cm 100 cm
36 PERIOPERATIVE COMPLICATIONS May include: Anesthetic related risks (cardiac, pulmonary) Bleeding Infection (wound infection) Incisional pain: larger laparoscopic incisions Anastomotic/Staple line leaks <<1% - 4% depending on procedure DVT, pulmonary embolism: < 0.5% Mortality: less than 0.2%
 Summary of Key Statistics")
37 BARIATRIC SURGERY SAFETY Bariatric Outcomes Longitudinal Database (BOLD) Summary of Key Statistics (Oct 2010)
38 LONG-TERM SURGICAL RISKS Long-term risks may include: Gallstones (when present) Prevent with Actigall (ursodiol) while rapid weight loss (6 mos.) Difficulty adjusting to body image Ulcers/strictures May need endoscopy to dilate No NSAIDS, steroids, or smoking (lifelong) Hernias (including internal) Gastric band slippage, erosion, infection, malfunction Esophageal dilation Vitamin deficiency (B12, iron, calcium, vitamin D, others)
39 ADJUSTABLE GASTRIC BANDING (LAGB) Long-Term Studies High rates of reoperation (40-60%) Band slippage - GERD, dysphagia, band intolerance Band erosion - Failure of/insufficient weight loss Esophageal dilation - Port/tubing malfunction Frequent follow-up (monthly in 1 st yr. best outcomes) Labor intensive for patients and providers
40 MEDICAL VS. SURGICAL THERAPY FOR TYPE II DM STAMPEDE (Surgical Treatment and Medications Potentially Eradicate Diabetes Efficiently) trial 3 year outcomes of bariatric surgery vs. intensive medical therapy Intensive medical therapy vs. medical therapy plus Roux-en-Y gastric bypass or sleeve gastrectomy 150 patients with uncontrolled type II DM (Hgb A1c > 7.0%) and BMI kg/m 2 Primary outcome measure: Hgb A1c 6.0%. Met by 38% of RYGBP patients, 24% sleeve patients, 5% medical group (91% follow-up at 3 yrs) Mean % weight loss from baseline: RYGBP: 24.5% ± 9.1%; sleeve 21.1% ± 8.9%; medical 4.2% ± 8.3% Bariatric surgery results in glycemic control in significantly more patients than did medical therapy alone Schauer PR, et al. NEJM 2014


41 ESTIMATE OF BARIATRIC SURGERY NUMBERS, Procedure numbers from 2011, 2012, 2013, 2014 and 2015 based on the best estimates from BOLD, ASC/MBSAQIP, and National Inpatient Sample data and outpatient estimations
42 RYGBP VS. SLEEVE GASTRECTOMY IN SUPER OBESITY Retrospective review of the Bariatric Outcomes Longitudinal Database from 2007 to 2012 in super obese (BMI 50 kg/m 2 ) patients 50,987 patients underwent RYGBP (N = 42,119) vs. SG (N = 8868) Similar adjusted overall 30-day complication rate for RYGBP vs. SG (11.5 vs 11.1%) RYGBP had higher adjusted rates of 30-day mortality (0.3 vs. 0.2%, p = 0.042), reoperation (4.0 vs. 2.4%, p <0.001), and readmission (6.9 vs. 5.5%, p < 0.001) vs. SG RYGBP had significantly greater %TWL than SG at 12 months (34.5 vs %, p 0.001) and at 3 and 6 months postoperatively RYGBP also had increased resolution of all measured comorbidities: DM (61.6 vs. 50.8%, p < 0.001), HTN (53.9 vs. 32.5%, p < 0.001), GERD (53.9 vs. 32.5%, p < 0.001), hyperlipidemia (39.7 vs 32.5%, p < 0.001), and obstructive sleep apnea (42.8 vs. 40.6%, p = 0.058) at 12 months compare to SG In the superobese, there was no difference in 30 day complications between RYGBP and SG, but readmissions and reoperations were higher for RYGBP; however, RYGBP was considerably more effective in controlling comorbid conditions. Celio AC, et al. Surg Endosc. 2016
43 RYGBP VS. SLEEVE GASTRECTOMY EUROPEAN DATA Retrospective review of patients from the International Federation for the Surgery of Obesity and Metabolic Disorders (IFSO) European Chapter Center of Excellence program from 2010 to ,025 patients underwent RYGBP (N = 10,622) vs. SG (N = 6413) Steadily increasing numbers of SG performed from 2010 to 2015 Higher early (<30 day) complication rate for RYGBP vs. SG (3.02 vs. 2.12%, p = ), with the majority related to marginal ulcers, obstruction, and other complications Equivalent 30-day mortality and readmission rates for RYGBP vs. SG (0.009% vs %, NS; 1.94 vs. 1.61%, NS) Reoperation (75.2 vs. 50.5%, p <0.0001) was higher for SG vs. RYGBP, with a significant difference in intraabdominal abscess rate (0.30 vs. 0.09%, p = 0.004) Significantly better % excess weight loss were seen following RYGBP in all postoperative years (60.36 vs %, p = at year 5), and better remission rates were seen for diabetes, hypertension, dyslipidemia, and sleep apnea in the first year (only). OA treatment results better for SG in all years (p < ) Melissas J, et al. Obes Surg. 2016

44 GASTRIC INTERVENTIONS: NEW DEVICES FOR WEIGHT LOSS ASGE Bariatric Endoscopy Task Force and ASGE Technology Committee, Gastrointest Endosc. 2015
45 GASTRIC INTERVENTIONS: IMPORTANT CONSIDERATIONS All interventions are intended to be used in conjunction with lifestyle modification All interventions are currently not covered by insurers and are performed on a self-pay basis Produce less weight loss than surgery and more than lifestyle invention [%EBWL ~ 25-30%/ TBWL 6.81% ± 5.1% (Obalon)] Balloons FDA approved for BMI low as 30 for 6 months of consecutive use. Procedures are less invasive than surgery but still have potential complications and side-effects
46 CONCLUSIONS Obesity is an epidemic with significant adverse effects on health and quality of life Multiple factors contribute to obesity resulting in energy imbalance that causes weight gain Diet and lifestyle modification along with physical activity form the basis of any weight loss effort and remain important when pharmacotherapy or surgery is implemented Bariatric surgery should be considered for patients with a BMI 40 or 35 with a comorbid condition and is safe and effective The cost, efficacy, and side-effect/complication profile of new therapies and procedures help to determine their role in the management of obesity
47 QUESTION: Which of the following is a true statement regarding gastric bypass?: a) Gastric bypass has a lower rate of complications than sleeve gastrectomy b) Excess body weight loss and comorbidity resolution rates for gastric bypass and sleeve gastrectomy are equivalent c) Gastric bypass effectively treats gastroesophageal reflux disease (GERD) d) Gastric bypass is increasing as a percentage of weight loss operations performed annually in the United States
48 QUESTION: Which of the following is a true statement regarding gastric bypass?: Correct Answer: c) Gastric bypass effectively treats gastroesophageal reflux disease (GERD) Rationale: Although the risk of early complications after gastric bypass is very low, it is higher than what is seen for sleeve gastrectomy; however, gastric bypass results in greater weight loss and comorbidity improvement. Gastric bypass effectively treats gastroesophageal reflux symptoms and is the preferred antireflux operation in individuals with clinically severe obesity. Sleeve Gastrectomy vs Roux-en-Y Gastric Bypass. Data from IFSO-European Chapter Center of Excellence Program. Melissas J, et al. Obes Surg Oct 20. Surgery for Gastroesophageal Reflux Disease in the Morbidly Obese Patient. Duke MC, Farrell TM. J Laparoendosc Adv Surg Tech A Nov 18
49 DISCUSSION Additional information: The Obesity Society Resources: American Society of Metabolic and Bariatric Surgery: NHLBI, Obesity Guidelines:
Viriato Fiallo, MD Ursula McMillian, MD
 Viriato Fiallo, MD Ursula McMillian, MD Objectives Define obesity and effects on society and healthcare Define bariatric surgery Discuss recent medical management versus surgery research Evaluate different
Viriato Fiallo, MD Ursula McMillian, MD Objectives Define obesity and effects on society and healthcare Define bariatric surgery Discuss recent medical management versus surgery research Evaluate different
Surgical Therapy for Morbid Obesity. Janeen Jordan, PGY 5 Surgical Grand Rounds April 7, 2008
 Surgical Therapy for Morbid Obesity Janeen Jordan, PGY 5 Surgical Grand Rounds April 7, 28 Obesity BMI > 3 kg/m 2 Moderate 35-4 kg/m 2 Morbid >4 kg/m 2 1.7 BILLION Overweight Adults in the world 63 MILLION
Surgical Therapy for Morbid Obesity Janeen Jordan, PGY 5 Surgical Grand Rounds April 7, 28 Obesity BMI > 3 kg/m 2 Moderate 35-4 kg/m 2 Morbid >4 kg/m 2 1.7 BILLION Overweight Adults in the world 63 MILLION
Weight Loss Surgery. Outline 3/30/12. What Every GI Nurse Needs to Know. Define Morbid Obesity & its Medical Consequences. Treatments for Obesity
 3/30/12 Weight Loss Surgery What Every GI Nurse Needs to Know Kenneth A Cooper, D.O. March 31, 2012 Outline Define Morbid Obesity & its Medical Consequences Treatments for Obesity Bariatric (Weight-loss)
3/30/12 Weight Loss Surgery What Every GI Nurse Needs to Know Kenneth A Cooper, D.O. March 31, 2012 Outline Define Morbid Obesity & its Medical Consequences Treatments for Obesity Bariatric (Weight-loss)
ADVANCE AT YOUR OWN PACE
 ADVANCE AT YOUR OWN PACE Welcome and Introductions Obesity and Its Impact on Health Surgeon Introduction Surgical Weight Loss Options AGENDA OSVALDO ANEZ, MD 28 years of experience Performed approximately
ADVANCE AT YOUR OWN PACE Welcome and Introductions Obesity and Its Impact on Health Surgeon Introduction Surgical Weight Loss Options AGENDA OSVALDO ANEZ, MD 28 years of experience Performed approximately
Bariatric Surgery: Indications and Ethical Concerns
 Bariatric Surgery: Indications and Ethical Concerns Ramzi Alami, M.D. F.A.C.S Assistant Professor of Surgery American University of Beirut Medical Center Beirut, Lebanon Nothing to Disclose Determined
Bariatric Surgery: Indications and Ethical Concerns Ramzi Alami, M.D. F.A.C.S Assistant Professor of Surgery American University of Beirut Medical Center Beirut, Lebanon Nothing to Disclose Determined
SURGICAL MANAGEMENT OF OBESITY. Anne Lidor, MD, MPH Professor of Surgery Chief, Division of Minimally Invasive and Bariatric Surgery
 SURGICAL MANAGEMENT OF OBESITY Anne Lidor, MD, MPH Professor of Surgery Chief, Division of Minimally Invasive and Bariatric Surgery Multi-Factorial Causes of Morbid Obesity include: Genetic Environmental
SURGICAL MANAGEMENT OF OBESITY Anne Lidor, MD, MPH Professor of Surgery Chief, Division of Minimally Invasive and Bariatric Surgery Multi-Factorial Causes of Morbid Obesity include: Genetic Environmental
Lecture Goals. Body Mass Index. Obesity Definitions. Bariatric Surgery What the PCP Needs to Know 11/17/2009. Indications for bariatric Surgeries
 Bariatric Surgery What the PCP Needs to Know Mouna Abouamara Assistant Professor Internal Medicine James H Quillen College Of Medicine Lecture Goals Indications for bariatric Surgeries Different types
Bariatric Surgery What the PCP Needs to Know Mouna Abouamara Assistant Professor Internal Medicine James H Quillen College Of Medicine Lecture Goals Indications for bariatric Surgeries Different types
A Bariatric Patient in my Waiting Room: Choosing the Right Patient for the Right Operation: Bariatric Surgery Indications
 A Bariatric Patient in my Waiting Room: Choosing the Right Patient for the Right Operation: Bariatric Surgery Indications Shahzeer Karmali MD FRCSC FACS Associate Professor Surgery University of Alberta
A Bariatric Patient in my Waiting Room: Choosing the Right Patient for the Right Operation: Bariatric Surgery Indications Shahzeer Karmali MD FRCSC FACS Associate Professor Surgery University of Alberta
Bariatric surgery: Impact on Co-morbidities and Weight Loss Expectations ALIYAH KANJI, MD FRCSC MIS AND BARIATRIC SURGERY SEPTEMBER 22, 2018
 Bariatric surgery: Impact on Co-morbidities and Weight Loss Expectations ALIYAH KANJI, MD FRCSC MIS AND BARIATRIC SURGERY SEPTEMBER 22, 2018 Disclosures None Objectives Review expected weight loss from
Bariatric surgery: Impact on Co-morbidities and Weight Loss Expectations ALIYAH KANJI, MD FRCSC MIS AND BARIATRIC SURGERY SEPTEMBER 22, 2018 Disclosures None Objectives Review expected weight loss from
Disclosures. Obesity and Its Challenges: Outline. Outline 5/2/2013. Lan Vu, MD Division of Pediatric Surgery Department of Surgery
 Obesity and Its Challenges: Bariatric Surgery: Why or Why Not I have nothing to disclose Disclosures Lan Vu, MD Division of Pediatric Surgery Department of Surgery Outline Growing obesity epidemic Not
Obesity and Its Challenges: Bariatric Surgery: Why or Why Not I have nothing to disclose Disclosures Lan Vu, MD Division of Pediatric Surgery Department of Surgery Outline Growing obesity epidemic Not
Policy Specific Section: April 14, 1970 June 28, 2013
 Medical Policy Bariatric Surgery Type: Medical Necessity and Investigational / Experimental Policy Specific Section: Surgery Original Policy Date: Effective Date: April 14, 1970 June 28, 2013 Definitions
Medical Policy Bariatric Surgery Type: Medical Necessity and Investigational / Experimental Policy Specific Section: Surgery Original Policy Date: Effective Date: April 14, 1970 June 28, 2013 Definitions
10/16/2014. Normal Weight: BMI Overweight: BMI >25 Obese: BMI >30 Morbidly Obese: BMI >40 or >35 with 2 comorbidities
 Brinton Clark, MD, MPH Department of Medical Education Providence Portland Medical Center October 25 th, 2014 Oregon Society of Physician Assistants Fall Conference 45 yo woman with BMI=40kg/m2 (weight
Brinton Clark, MD, MPH Department of Medical Education Providence Portland Medical Center October 25 th, 2014 Oregon Society of Physician Assistants Fall Conference 45 yo woman with BMI=40kg/m2 (weight
Not over when the surgery is done: surgical complications of obesity
 Not over when the surgery is done: surgical complications of obesity Gianluca Bonanomi, MD, FRCS Consultant Surgeon and Honorary Senior Lecturer Chelsea and Westminster Hospital London The Society for
Not over when the surgery is done: surgical complications of obesity Gianluca Bonanomi, MD, FRCS Consultant Surgeon and Honorary Senior Lecturer Chelsea and Westminster Hospital London The Society for
Bariatric Surgery: A Cost-effective Treatment of Obesity?
 Bariatric Surgery: A Cost-effective Treatment of Obesity? Shaneeta M. Johnson MD FACS FASMBS 2018 NMA Professional Development Seminar Congressional Black Caucus Foundation Annual Legislative Conference
Bariatric Surgery: A Cost-effective Treatment of Obesity? Shaneeta M. Johnson MD FACS FASMBS 2018 NMA Professional Development Seminar Congressional Black Caucus Foundation Annual Legislative Conference
6/23/2011. Bariatric Surgery: What the Primary Care Provider Should Know. Case Presentation: Rachelle
 Bariatric Surgery: What the Primary Care Provider Should Know 2,000 B.C. 2,000 A.D. Case Presentation: Rachelle 35 year-old woman with morbid obesity. 5 1 236 lbs BMI 44.5 PMHx: mild depression obstructive
Bariatric Surgery: What the Primary Care Provider Should Know 2,000 B.C. 2,000 A.D. Case Presentation: Rachelle 35 year-old woman with morbid obesity. 5 1 236 lbs BMI 44.5 PMHx: mild depression obstructive
Morbid Obesity A Curable Disease?
 Morbid Obesity A Curable Disease? Piotr Gorecki, M.D. F.A.C.S. Associate Professor of Clinical Surgery Weill Medical College of Cornell University Chief of Laparoscopic Surgery New York Methodist Hospital
Morbid Obesity A Curable Disease? Piotr Gorecki, M.D. F.A.C.S. Associate Professor of Clinical Surgery Weill Medical College of Cornell University Chief of Laparoscopic Surgery New York Methodist Hospital
ENTRY CRITERIA: C. Approved Comorbidities: Diabetes
 KAISER PERMANENTE OHIO BARIATRIC SURGERY (GASTROPLASTY) Methodology: Expert Opinion Issue Date: 12-05 Champion: Surgery Review Date: 4-10, 4-12 Key Stakeholders: Surgery, IM Depts. Next Update: 4-14 RELEVANCE:
KAISER PERMANENTE OHIO BARIATRIC SURGERY (GASTROPLASTY) Methodology: Expert Opinion Issue Date: 12-05 Champion: Surgery Review Date: 4-10, 4-12 Key Stakeholders: Surgery, IM Depts. Next Update: 4-14 RELEVANCE:
Goals 1/9/2018. Obesity over the last decade Surgery has become a safer management strategy Surgical options for management
 The Current State of Surgical Intervention in Management of Morbid Obesity Goals Obesity over the last decade Surgery has become a safer management strategy Surgical options for management 1 Goals Obesity
The Current State of Surgical Intervention in Management of Morbid Obesity Goals Obesity over the last decade Surgery has become a safer management strategy Surgical options for management 1 Goals Obesity
Laparoscopic Adjustable Gastric Band The Safest, Effective Procedure for Treating Obesity and Obesity Related Disease
 Laparoscopic Adjustable Gastric Band The Safest, Effective Procedure for Treating Obesity and Obesity Related Disease Erik Peltz, D.O. April 7 th, 2008 University of Colorado Health Science Center Department
Laparoscopic Adjustable Gastric Band The Safest, Effective Procedure for Treating Obesity and Obesity Related Disease Erik Peltz, D.O. April 7 th, 2008 University of Colorado Health Science Center Department
Bariatric surgery. KHALAJ A.R. M.D Obesity Clinic Mostafa Khomini Hospital Shahed University Tehran
 Bariatric surgery KHALAJ A.R. M.D Obesity Clinic Mostafa Khomini Hospital Shahed University Tehran WWW.IRANOBESITY.COM Why Surgery? What is Indication of Surgery? What is ContraIndication of surgery? What
Bariatric surgery KHALAJ A.R. M.D Obesity Clinic Mostafa Khomini Hospital Shahed University Tehran WWW.IRANOBESITY.COM Why Surgery? What is Indication of Surgery? What is ContraIndication of surgery? What
Weight Loss Surgery Program
 Weight Loss Surgery Program More than 500,000 Americans die prematurely each year from obesity-related complications, and it is one of the leading causes of preventable death. If you want to do something
Weight Loss Surgery Program More than 500,000 Americans die prematurely each year from obesity-related complications, and it is one of the leading causes of preventable death. If you want to do something
Chapter 4 Section 13.2
 TRICARE Policy Manual 6010.60-M, April 1, 2015 Surgery Chapter 4 Section 13.2 Issue Date: November 9, 1982 Authority: 32 CFR 199.2(b) and 32 CFR 199.4(e)(15) Copyright: CPT only 2006 American Medical Association
TRICARE Policy Manual 6010.60-M, April 1, 2015 Surgery Chapter 4 Section 13.2 Issue Date: November 9, 1982 Authority: 32 CFR 199.2(b) and 32 CFR 199.4(e)(15) Copyright: CPT only 2006 American Medical Association
Bariatric Surgery Update
 Bariatric Surgery Update Alexander Perez, MD, FACS Professor of Surgery Chief, Division Minimally Invasive and Foregut Surgery Speaker Disclosure Dr. Perez has disclosed that the has no actual or potential
Bariatric Surgery Update Alexander Perez, MD, FACS Professor of Surgery Chief, Division Minimally Invasive and Foregut Surgery Speaker Disclosure Dr. Perez has disclosed that the has no actual or potential
Bariatric Surgery: The Primary Care Approach
 The 8 th Annual Conference of the Lebanese Society of Family Medicine October 25 th 2009 Bariatric Surgery: The Primary Care Approach Bassem Y. Safadi, MD, FACS Associate Professor of Clinical Surgery
The 8 th Annual Conference of the Lebanese Society of Family Medicine October 25 th 2009 Bariatric Surgery: The Primary Care Approach Bassem Y. Safadi, MD, FACS Associate Professor of Clinical Surgery
Here are some types of gastric bypass surgery:
 Gastric Bypass- Definition By Mayo Clinic staff Weight-loss (bariatric) surgeries change your digestive system, often limiting the amount of food you can eat. These surgeries help you lose weight and can
Gastric Bypass- Definition By Mayo Clinic staff Weight-loss (bariatric) surgeries change your digestive system, often limiting the amount of food you can eat. These surgeries help you lose weight and can
Bariatric Surgery MM /11/2001. HMO; PPO; QUEST 05/01/2012 Section: Surgery Place(s) of Service: Outpatient; Inpatient
 of Service: Outpatient; Inpatient") Bariatric Surgery Policy Number: Original Effective Date: MM.06.003 09/11/2001 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST 05/01/2012 Section: Surgery Place(s) of Service: Outpatient;
Bariatric Surgery Policy Number: Original Effective Date: MM.06.003 09/11/2001 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST 05/01/2012 Section: Surgery Place(s) of Service: Outpatient;
Benefits of Bariatric Surgery
 Benefits of Bariatric Surgery Dr Tan Bo Chuan Registrar, Department of Surgery GP Forum 27 May 2017 Improvements of Co-morbidities Type 2 diabetes mellitus Hypertension Hyperlipidemia Degenerative joint
Benefits of Bariatric Surgery Dr Tan Bo Chuan Registrar, Department of Surgery GP Forum 27 May 2017 Improvements of Co-morbidities Type 2 diabetes mellitus Hypertension Hyperlipidemia Degenerative joint
WEIGHT LOSS SURGERY A Primer on Current Options and Outcomes. Caitlin A. Halbert DO, MS, FACS, FASMBS April 5, 2018
 WEIGHT LOSS SURGERY A Primer on Current Options and Outcomes Caitlin A. Halbert DO, MS, FACS, FASMBS April 5, 2018 A Little Bit About Me Bariatric Surgical Services Reflux Surgery General Surgery Overview
WEIGHT LOSS SURGERY A Primer on Current Options and Outcomes Caitlin A. Halbert DO, MS, FACS, FASMBS April 5, 2018 A Little Bit About Me Bariatric Surgical Services Reflux Surgery General Surgery Overview
Commonly Performed Bariatric Procedures in Singapore. Lin Jinlin Associate Consultant General, Upper GI and Bariatric Surgery Changi General Hospital
 Commonly Performed Bariatric Procedures in Singapore Lin Jinlin Associate Consultant General, Upper GI and Bariatric Surgery Changi General Hospital Scope 1. Introduction 2. Principles of bariatric surgery
Commonly Performed Bariatric Procedures in Singapore Lin Jinlin Associate Consultant General, Upper GI and Bariatric Surgery Changi General Hospital Scope 1. Introduction 2. Principles of bariatric surgery
Removal of a lap band and revision to an alternative bariatric procedure in one procedure.
 How to Discuss the Case with Insurance Plan Medical Director, Letter of Medical Necessity, and Increasing the Chance of Letters of Medical Necessity are a well-known requirement when requesting authorization
How to Discuss the Case with Insurance Plan Medical Director, Letter of Medical Necessity, and Increasing the Chance of Letters of Medical Necessity are a well-known requirement when requesting authorization
Chapter 4 Section 13.2
 Surgery Chapter 4 Section 13.2 Issue Date: November 9, 1982 Authority: 32 CFR 199.2(b) and 32 CFR 199.4(e)(15) 1.0 CPT 1 PROCEDURE CODES 43644, 43770-43774, 43842, 43846, 43848 2.0 HCPCS PROCEDURE CODES
Surgery Chapter 4 Section 13.2 Issue Date: November 9, 1982 Authority: 32 CFR 199.2(b) and 32 CFR 199.4(e)(15) 1.0 CPT 1 PROCEDURE CODES 43644, 43770-43774, 43842, 43846, 43848 2.0 HCPCS PROCEDURE CODES
Disclosures OBESITY. Overview. Obesity: Definition. Prevalence of Obesity is Rising. Obesity as a Risk Factor. None
 Disclosures None OBESITY Florencia Halperin, M.D. Medical Director, Program for Management Brigham and Women s Hospital Instructor in Medicine, Harvard Medical School Overview Obesity: Definition Definition
Disclosures None OBESITY Florencia Halperin, M.D. Medical Director, Program for Management Brigham and Women s Hospital Instructor in Medicine, Harvard Medical School Overview Obesity: Definition Definition
Overview. Stanley J. Rogers, MD, FACS Associate Clinical Professor of Surgery University of California San Francisco
 GASTROINTESTINAL COMPLICATIONS AFTER BARIATRIC SURGERY Stanley J. Rogers, MD, FACS Associate Clinical Professor of Surgery University of California San Francisco UCSF DEPARTMENT OF SURGERY Original Article
GASTROINTESTINAL COMPLICATIONS AFTER BARIATRIC SURGERY Stanley J. Rogers, MD, FACS Associate Clinical Professor of Surgery University of California San Francisco UCSF DEPARTMENT OF SURGERY Original Article
SOUND HEALTH & WELLNESS TRUST
 WEIGHT LOSS SURGERY POLICY SOUNDPLUS PPO AND SOUND PPO PLANS All procedures approved by the Plan must be pre-authorized by Aetna (the Trust s Utilization Management Vendor) and care must be provided by
WEIGHT LOSS SURGERY POLICY SOUNDPLUS PPO AND SOUND PPO PLANS All procedures approved by the Plan must be pre-authorized by Aetna (the Trust s Utilization Management Vendor) and care must be provided by
Bariatric Surgery Update
 Friday General Session Bariatric Surgery Update Alex Perez, MD Chief, Division of Minimally Invasive and Foregut Surgery James E. Thompson, MD Family Distinguished Professor in Surgical Simulation Co Director,
Friday General Session Bariatric Surgery Update Alex Perez, MD Chief, Division of Minimally Invasive and Foregut Surgery James E. Thompson, MD Family Distinguished Professor in Surgical Simulation Co Director,
Effect of Bariatric Surgery on Cardio-Metabolic Outcomes
 Effect of Bariatric Surgery on Cardio-Metabolic Outcomes Disclosure Research support from Bariatric Advantage (supplements donated for research study) Anne Schafer, MD Associate Professor of Medicine and
Effect of Bariatric Surgery on Cardio-Metabolic Outcomes Disclosure Research support from Bariatric Advantage (supplements donated for research study) Anne Schafer, MD Associate Professor of Medicine and
JAMA February 10, 2010 Laparoscopic Adjustable Banding in Severely Obese Adolescents: A Randomized Trial
 JAMA February 10, 2010 Laparoscopic Adjustable Banding in Severely Obese Adolescents: A Randomized Trial Daniel DeUgarte, MD Division of Pediatric Surgery Surgical Director, UCLA FIT Program Bariatric
JAMA February 10, 2010 Laparoscopic Adjustable Banding in Severely Obese Adolescents: A Randomized Trial Daniel DeUgarte, MD Division of Pediatric Surgery Surgical Director, UCLA FIT Program Bariatric
Reoperation Bariatric Surgery:
 Reoperative Bariatric Surgery, Achieving Insurance Authorization Achieving insurance authorization for reoperative bariatric procedures is not difficult provided that prior insurance company authorization
Reoperative Bariatric Surgery, Achieving Insurance Authorization Achieving insurance authorization for reoperative bariatric procedures is not difficult provided that prior insurance company authorization
Bariatric Surgery. The Oregon Bariatric Center Surgical Team
 Bariatric Surgery The Oregon Bariatric Center Surgical Team Colin MacColl, MD, Medical Director, Bariatric Surgeon Jessica Folek, MD, Bariatric Surgeon I have no disclosures Disclosures Objectives What
Bariatric Surgery The Oregon Bariatric Center Surgical Team Colin MacColl, MD, Medical Director, Bariatric Surgeon Jessica Folek, MD, Bariatric Surgeon I have no disclosures Disclosures Objectives What
The Surgical Management of Obesity
 The Surgical Management of Obesity Omar al noubani MD,MRCS وك ل وا و اش ز ب وا و ال ت س رف وا األعراف ما مأل ابن آدم وعاء شر ا من بطنه Persons who are naturally fat are apt to die earlier than those who
The Surgical Management of Obesity Omar al noubani MD,MRCS وك ل وا و اش ز ب وا و ال ت س رف وا األعراف ما مأل ابن آدم وعاء شر ا من بطنه Persons who are naturally fat are apt to die earlier than those who
Bariatric Surgery. Options & Outcomes
 Bariatric Surgery Options & Outcomes Obesity Obesity now leading cause of premature death & illness in Australia 67% of Australians are overweight or obese Australia 4 th fattest nation in OECD Obesity
Bariatric Surgery Options & Outcomes Obesity Obesity now leading cause of premature death & illness in Australia 67% of Australians are overweight or obese Australia 4 th fattest nation in OECD Obesity
MEDICAL COVERAGE POLICY. SERVICE: Bariatric (Weight Loss) Surgery Policy Number: 053 Effective Date: 08/01/2017 Last Review: 05/16/2017
 Surgery Policy Number: 053 Effective Date: 08/01/2017 Last Review: 05/16/2017") Important note Even though this policy may indicate that a particular service or supply is considered covered, this conclusion is not necessarily based upon the terms of your particular benefit plan. Each
Important note Even though this policy may indicate that a particular service or supply is considered covered, this conclusion is not necessarily based upon the terms of your particular benefit plan. Each
Endorsed by Executive Council June 17, American Society for Metabolic and Bariatric Surgery
 Endorsed by Executive Council June 17, 2007 American Society for Metabolic and Bariatric Surgery POSITION STATEMENT ON SLEEVE GASTRECTOMY AS A BARIATRIC PROCEDURE Clinical Issues Committee Preamble. The
Endorsed by Executive Council June 17, 2007 American Society for Metabolic and Bariatric Surgery POSITION STATEMENT ON SLEEVE GASTRECTOMY AS A BARIATRIC PROCEDURE Clinical Issues Committee Preamble. The
10/28/11. Bariatric Surgery: What the Primary Care Provider Should Know. Case Presentation: Rachelle
 Bariatric Surgery: What the Primary Care Provider Should Know 2,000 B.C. 2,000 A.D. Case Presentation: Rachelle 35 year-old woman with morbid obesity. 5 1 236 lbs BMI 44.5 PMHx: mild depression obstructive
Bariatric Surgery: What the Primary Care Provider Should Know 2,000 B.C. 2,000 A.D. Case Presentation: Rachelle 35 year-old woman with morbid obesity. 5 1 236 lbs BMI 44.5 PMHx: mild depression obstructive
Choice Critria in Bariatric Surgery. Giovanni Camerini
 Choice Critria in Bariatric Surgery Giovanni Camerini Surgical vs Medical treatment Indications for Bariatric Surgery (WHO 1992) BMI of at least 40; BMI of 35 in case of serious diseases related to obesity;
Choice Critria in Bariatric Surgery Giovanni Camerini Surgical vs Medical treatment Indications for Bariatric Surgery (WHO 1992) BMI of at least 40; BMI of 35 in case of serious diseases related to obesity;
Surgical Treatment of Obesity. 1. Understand who is an appropriate candidate for referral for surgical weight loss.
 Surgical Treatment of Obesity Learning Objectives: 1. Understand who is an appropriate candidate for referral for surgical weight loss. 2. Appreciate impact of operative weight reduction to improve co-morbid
Surgical Treatment of Obesity Learning Objectives: 1. Understand who is an appropriate candidate for referral for surgical weight loss. 2. Appreciate impact of operative weight reduction to improve co-morbid
11/11/2011. Bariatric Surgery for Sleep Apnea. Case Presentation: Rachelle. Case Presentation: Rachelle. Case Presentation: Rachelle
 Bariatric Surgery for Sleep Apnea 2,000 B.C. 2,000 A.D. 35 year-old woman with morbid obesity. 5 1 236 lbs BMI 44.5 PMHx: mild depression obstructive sleep apnea (AHI 42, on CPAP) asthma polycystic ovarian
Bariatric Surgery for Sleep Apnea 2,000 B.C. 2,000 A.D. 35 year-old woman with morbid obesity. 5 1 236 lbs BMI 44.5 PMHx: mild depression obstructive sleep apnea (AHI 42, on CPAP) asthma polycystic ovarian
Bariatric Surgery. Overview of Procedural Options
 Bariatric Surgery Overview of Procedural Options The Obesity Epidemic In 1991, NO state had an obesity rate above 20% 1 As of 2010, more than two-thirds of states (38) now have adult obesity rates above
Bariatric Surgery Overview of Procedural Options The Obesity Epidemic In 1991, NO state had an obesity rate above 20% 1 As of 2010, more than two-thirds of states (38) now have adult obesity rates above
Gastrointestinal Surgery for Severe Obesity 2.0 Contact Hours Presented by: CEU Professor
 Gastrointestinal Surgery for Severe Obesity 2.0 Contact Hours Presented by: CEU Professor 7 www.ceuprofessoronline.com Copyright 8 2007 The Magellan Group, LLC All Rights Reserved. Reproduction and distribution
Gastrointestinal Surgery for Severe Obesity 2.0 Contact Hours Presented by: CEU Professor 7 www.ceuprofessoronline.com Copyright 8 2007 The Magellan Group, LLC All Rights Reserved. Reproduction and distribution
Bariatric Surgery Corporate Medical Policy
 Bariatric Surgery Corporate Medical Policy File name: Bariatric Surgery File code: UM.SURG.01 Origination: 07/2008 Last Review: 06/2018 Next Review: 06/2019 Effective Date: 10/01/2018 Description/Summary
Bariatric Surgery Corporate Medical Policy File name: Bariatric Surgery File code: UM.SURG.01 Origination: 07/2008 Last Review: 06/2018 Next Review: 06/2019 Effective Date: 10/01/2018 Description/Summary
Requirements & Checklist
 Group Health Benefits Program for Bariatric Surgery: Requirements & Checklist Adopted October, 2011 Effective January 1, 2012 (Updated 9/20/2012) 1 Bariatric Surgery: Benefit Rules IS BARIATRIC SURGERY
Group Health Benefits Program for Bariatric Surgery: Requirements & Checklist Adopted October, 2011 Effective January 1, 2012 (Updated 9/20/2012) 1 Bariatric Surgery: Benefit Rules IS BARIATRIC SURGERY
SURGICAL TREATMENT FOR OBESITY: WHATS THE BEST OPTION? Natan Zundel, MD, FACS
 SURGICAL TREATMENT FOR OBESITY: WHATS THE BEST OPTION? Natan Zundel, MD, FACS Professor of Surgery Vice-Chairman Department of Surgery Florida International University Herbert Wertheim College of Medicine
SURGICAL TREATMENT FOR OBESITY: WHATS THE BEST OPTION? Natan Zundel, MD, FACS Professor of Surgery Vice-Chairman Department of Surgery Florida International University Herbert Wertheim College of Medicine
Jordan Garrison Jr. MD, FACS, FASMBS
 Jordan Garrison Jr. MD, FACS, FASMBS A life-long progressive, lifethreatening, geneticallyrelated, costly, multifactorial disease of excess fat storage with multiple comorbidities ~ 25% industrialized
Jordan Garrison Jr. MD, FACS, FASMBS A life-long progressive, lifethreatening, geneticallyrelated, costly, multifactorial disease of excess fat storage with multiple comorbidities ~ 25% industrialized
10/29/2011. Metabolic, Obstetric, and Gynecological Consequences of Bariatric Surgery. Case Presentation: Rachelle. Jonathan Carter, MD
 Metabolic, Obstetric, and Gynecological Consequences of Bariatric Surgery 2,000 B.C. 2,000 A.D. Case Presentation: Rachelle 35 year-old woman with morbid obesity. 5 1 236 lbs BMI 44.5 PMHx: mild depression
Metabolic, Obstetric, and Gynecological Consequences of Bariatric Surgery 2,000 B.C. 2,000 A.D. Case Presentation: Rachelle 35 year-old woman with morbid obesity. 5 1 236 lbs BMI 44.5 PMHx: mild depression
OBESITY 2008: DIET, EXERCISE, DRUGS, AND SURGERY
 OBESITY 2008: DIET, EXERCISE, DRUGS, AND SURGERY Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest CLASSIFICATION OF OVERWEIGHT
OBESITY 2008: DIET, EXERCISE, DRUGS, AND SURGERY Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest CLASSIFICATION OF OVERWEIGHT
Medicare Part C Medical Coverage Policy
 Morbid Obesity Surgery Origination: June 30, 1988 Review Date: October 18, 2017 Next Review: October, 2019 Medicare Part C Medical Coverage Policy DESCRIPTION OF PROCEDURE OR SERVICE Bariatric surgery
Morbid Obesity Surgery Origination: June 30, 1988 Review Date: October 18, 2017 Next Review: October, 2019 Medicare Part C Medical Coverage Policy DESCRIPTION OF PROCEDURE OR SERVICE Bariatric surgery
Bariatric Surgery Work Up, Patient Selection and Follow Up
 Bariatric Surgery Work Up, Patient Selection and Follow Up A/Professor Tania Markovic Metabolism & Obesity Services, RPAH Boden Institute of Obesity, Nutrition, Exercise & Eating Disorders SLHD Bariatric
Bariatric Surgery Work Up, Patient Selection and Follow Up A/Professor Tania Markovic Metabolism & Obesity Services, RPAH Boden Institute of Obesity, Nutrition, Exercise & Eating Disorders SLHD Bariatric
Bariatric Surgery Center Centegra Health System Huntley IL
 Bariatric Surgery Center Centegra Health System Huntley IL We Honor and Value Your Individuality! Here for Different Reasons Tried Everything Better Health Reduce or Eliminate Medications Become More
Bariatric Surgery Center Centegra Health System Huntley IL We Honor and Value Your Individuality! Here for Different Reasons Tried Everything Better Health Reduce or Eliminate Medications Become More
International Health Brief
 International Health Brief Bariatric Surgery In this Health Brief, we look at the growing utilization of bariatric surgery as a means of achieving rapid weight loss, and consider if it should be covered
International Health Brief Bariatric Surgery In this Health Brief, we look at the growing utilization of bariatric surgery as a means of achieving rapid weight loss, and consider if it should be covered
Metabolic & Bariatric Surgery Program Information Session
 Metabolic & Bariatric Surgery Program Information Session Why have Bariatric Surgery at MUSC? The Expert Experience Most established program in the area Dedicated interdisciplinary team Recognized and
Metabolic & Bariatric Surgery Program Information Session Why have Bariatric Surgery at MUSC? The Expert Experience Most established program in the area Dedicated interdisciplinary team Recognized and
Obesity and Bariatric Surgery Michel M. Murr, MD, FACS
 Obesity and Bariatric Surgery Michel M. Murr, MD, FACS Director of Bariatric Center Chief of Surgery, TGH Professor of Surgery, USF Disclosure Covidien: educational grants Obesity and Bariatric Surgery
Obesity and Bariatric Surgery Michel M. Murr, MD, FACS Director of Bariatric Center Chief of Surgery, TGH Professor of Surgery, USF Disclosure Covidien: educational grants Obesity and Bariatric Surgery
Bariatric Surgery: How complex is this? Pradeep Pallati, MD, FACS, FASMBS
 Bariatric Surgery: How complex is this? Pradeep Pallati, MD, FACS, FASMBS Nothing to Disclose Types of Bariatric Surgery Restrictive Malabsorptive Combination Restrictive and Malabsorptive Newer Endoluminal
Bariatric Surgery: How complex is this? Pradeep Pallati, MD, FACS, FASMBS Nothing to Disclose Types of Bariatric Surgery Restrictive Malabsorptive Combination Restrictive and Malabsorptive Newer Endoluminal
Bariatric Surgery. Bariatric surgery could be your best option for living a healthy life. Let s find out together.
 Bariatric Surgery Bariatric surgery could be your best option for living a healthy life. Let s find out together. 1 What is obesity? Obesity is a complex health issue, characterized by an excessive amount
Bariatric Surgery Bariatric surgery could be your best option for living a healthy life. Let s find out together. 1 What is obesity? Obesity is a complex health issue, characterized by an excessive amount
(1) Upper Gastrointestinal Surgical Unit, The Alfred Hospital (2) Monash University Centre for Obesity Research and Education (CORE)
 Upper Gastrointestinal Surgical Unit, The Alfred Hospital (2) Monash University Centre for Obesity Research and Education (CORE)") Yazmin Johari (1,2), Geri Ooi (1,2), Paul Burton (1,2), Shourye Dwivedi (2), Cheryl Laurie (2), Kalai Shaw (1), Richard Chen (1,2), Wendy Brown (1,2), Peter Nottle (1) (1) Upper Gastrointestinal Surgical
Yazmin Johari (1,2), Geri Ooi (1,2), Paul Burton (1,2), Shourye Dwivedi (2), Cheryl Laurie (2), Kalai Shaw (1), Richard Chen (1,2), Wendy Brown (1,2), Peter Nottle (1) (1) Upper Gastrointestinal Surgical
Jacek Szopinski MD, PhD. This presentation contains pictures and schemes addopted from lecture by S.Dabrowiecki MD PhD with his kind permission
 Jacek Szopinski MD, PhD This presentation contains pictures and schemes addopted from lecture by S.Dabrowiecki MD PhD with his kind permission The definition of beauty evolves Problem we have to deal
Jacek Szopinski MD, PhD This presentation contains pictures and schemes addopted from lecture by S.Dabrowiecki MD PhD with his kind permission The definition of beauty evolves Problem we have to deal
Adipocytes, Obesity, Bariatric Surgery and its Complications
 Adipocytes, Obesity, Bariatric Surgery and its Complications Daniel C. Morris, MD, FACEP, FAHA Senior Staff Physician Department of Emergency Medicine Objectives Basic science of adipocyte Adipocyte tissue
Adipocytes, Obesity, Bariatric Surgery and its Complications Daniel C. Morris, MD, FACEP, FAHA Senior Staff Physician Department of Emergency Medicine Objectives Basic science of adipocyte Adipocyte tissue
Management of the Bariatric. Farah A. Husain MD, FACS, FASMBS Division Chief, Bariatric Services. Surgery Patient 2017
 Management of the Bariatric Farah A. Husain MD, FACS, FASMBS Division Chief, Bariatric Services Surgery Patient 2017 Financial Disclosures None Objectives Identify the most commonly performed bariatric
Management of the Bariatric Farah A. Husain MD, FACS, FASMBS Division Chief, Bariatric Services Surgery Patient 2017 Financial Disclosures None Objectives Identify the most commonly performed bariatric
U N D E R S T A N D I N G. Severe Obesity. An educational resource provided by the Obesity Action Coalition
 U N D E R S T A N D I N G Severe Obesity An educational resource provided by the Obesity Action Coalition Understanding Severe Obesity It is estimated that more than eight million Americans are affected
U N D E R S T A N D I N G Severe Obesity An educational resource provided by the Obesity Action Coalition Understanding Severe Obesity It is estimated that more than eight million Americans are affected
National Position Statement
 National Position Statement Weight Loss Surgery (Bariatric Surgery) and its Use in Treating Obesity or Treating and Preventing Diabetes Background Approximately twenty five per cent (25%) of Australian
National Position Statement Weight Loss Surgery (Bariatric Surgery) and its Use in Treating Obesity or Treating and Preventing Diabetes Background Approximately twenty five per cent (25%) of Australian
Obesity Management in Patients with Diabetes Jamy D. Ard, MD Sunday, February 11, :15 a.m. 11:00 a.m.
 Obesity Management in Patients with Diabetes Jamy D. Ard, MD Sunday, February 11, 2018 10:15 a.m. 11:00 a.m. Type 2 diabetes mellitus (T2DM) is closely associated with obesity, primarily through the link
Obesity Management in Patients with Diabetes Jamy D. Ard, MD Sunday, February 11, 2018 10:15 a.m. 11:00 a.m. Type 2 diabetes mellitus (T2DM) is closely associated with obesity, primarily through the link
OBESITY/OVERWEIGHT. Fastest spreading disaster of the century- Bariatric Surgical treatment. By Dr. Vladimir Shchukin Consultant General Surgeon
 OBESITY/OVERWEIGHT Fastest spreading disaster of the century- Bariatric Surgical treatment By Dr. Vladimir Shchukin Consultant General Surgeon Indications for surgical treatment Indication for Gastric
OBESITY/OVERWEIGHT Fastest spreading disaster of the century- Bariatric Surgical treatment By Dr. Vladimir Shchukin Consultant General Surgeon Indications for surgical treatment Indication for Gastric
Laparoscopic Weight Loss Surgery (Bariatric Surgery) A simple guide to help answer your questions
 A simple guide to help answer your questions") Laparoscopic Weight Loss Surgery (Bariatric Surgery) A simple guide to help answer your questions Weight problems are growing in the US More than 100 million Americans are overweight Half of these people
Laparoscopic Weight Loss Surgery (Bariatric Surgery) A simple guide to help answer your questions Weight problems are growing in the US More than 100 million Americans are overweight Half of these people
Technique. Matthew Bettendorf, MD Essentia Health Duluth Clinic. Laparoscopic approach One 12mm port, Four 5mm ports
 Matthew Bettendorf, MD Essentia Health Duluth Clinic Technique Laparoscopic approach One 12mm port, Four 5mm ports Single staple line with no anastamosis 85% gastrectomy Goal to remove
Matthew Bettendorf, MD Essentia Health Duluth Clinic Technique Laparoscopic approach One 12mm port, Four 5mm ports Single staple line with no anastamosis 85% gastrectomy Goal to remove
Baritec Inc. Baritec GaBP Ring Certification. Marcio Café, M.D. Mark J. Kannia, Sales / Marketing Director C.Bruce Fields, Project Engineer CSTO
 Baritec Inc Baritec GaBP Ring Certification Marcio Café, M.D. Mark J. Kannia, Sales / Marketing Director C.Bruce Fields, Project Engineer Presented to Minister of Heath. Brazil. December 2005 C.S.T.O.
Baritec Inc Baritec GaBP Ring Certification Marcio Café, M.D. Mark J. Kannia, Sales / Marketing Director C.Bruce Fields, Project Engineer Presented to Minister of Heath. Brazil. December 2005 C.S.T.O.
FRESH START. Time For A BARIATRIC SURGERY! WHAT IS BARIATRIC SURGERY? UHS Medical Times EVERYTHING YOU NEED TO KNOW ABOUT علاج ال دانة وجراحة السمنة
 UHS Medical Times 1 Newsletter September 2018 علاج ال دانة وجراحة السمنة MINIMALLY INVASIVE Time For A FRESH START EVERYTHING YOU NEED TO KNOW ABOUT BARIATRIC SURGERY! While any surgical procedure carries
UHS Medical Times 1 Newsletter September 2018 علاج ال دانة وجراحة السمنة MINIMALLY INVASIVE Time For A FRESH START EVERYTHING YOU NEED TO KNOW ABOUT BARIATRIC SURGERY! While any surgical procedure carries
What is obesity? OBESITY. Obesity is a health issue in which someone has so much extra fat that it negatively impacts their health.
 OBESITY What is obesity? Obesity is a health issue in which someone has so much extra fat that it negatively impacts their health. Obesity is most often measured by body mass index (BMI), which looks at
OBESITY What is obesity? Obesity is a health issue in which someone has so much extra fat that it negatively impacts their health. Obesity is most often measured by body mass index (BMI), which looks at
BARIATRIC SURGERY. Weight Loss Surgery. A variety of surgical procedures to reduce weight performed on people who have obesity. Therapy Male & Female
 BARIATRIC SURGERY Weight Loss Surgery A variety of surgical procedures to reduce weight performed on people who have obesity. Therapy Male & Female About Bariatric surgery Bariatric surgery offers a treatment
BARIATRIC SURGERY Weight Loss Surgery A variety of surgical procedures to reduce weight performed on people who have obesity. Therapy Male & Female About Bariatric surgery Bariatric surgery offers a treatment
A SYSTEMATIC APPROACH TO
 A SYSTEMATIC APPROACH TO OBESITY Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Prevalence of Obesity (Adults): 2008
A SYSTEMATIC APPROACH TO OBESITY Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Prevalence of Obesity (Adults): 2008
Access to Proven Therapies
 Access to Proven Therapies Obesity is a life-threatening disease affecting 34% of adults in the U.S. Between 2000 and 2005, obesity increased by 24%, morbid obesity by 50%, and super obesity by 75%. 18%
Access to Proven Therapies Obesity is a life-threatening disease affecting 34% of adults in the U.S. Between 2000 and 2005, obesity increased by 24%, morbid obesity by 50%, and super obesity by 75%. 18%
Subject: Weight Loss Surgery Effective Date: 1/1/2000 Review Date: 8/1/2017
 Subject: Weight Loss Surgery Effective Date: 1/1/2000 Review Date: 8/1/2017 DESCRIPTION OSU Health Plans supports covered members with a spectrum of service for obesity and weight loss attempts. The coverage
Subject: Weight Loss Surgery Effective Date: 1/1/2000 Review Date: 8/1/2017 DESCRIPTION OSU Health Plans supports covered members with a spectrum of service for obesity and weight loss attempts. The coverage
Bradley J. Needleman, MD, FACS Associate Professor of Clinical Surgery
 Bariatric Surgery: Current Status Bradley J. Needleman, MD, FACS Associate Professor of Clinical Surgery Director, Bariatric Surgery Program Center for Minimally Invasive Surgery The Ohio State University
Bariatric Surgery: Current Status Bradley J. Needleman, MD, FACS Associate Professor of Clinical Surgery Director, Bariatric Surgery Program Center for Minimally Invasive Surgery The Ohio State University
Bariatric Surgery Outcomes
 Bariatric Surgery Outcomes Kristoffel R. Dumon, MD a, Kenric M. Murayama, MD b, * KEYWORDS Bariatric surgery Outcomes Obesity Obesity is a global health problem and the exponential increase in obesity
Bariatric Surgery Outcomes Kristoffel R. Dumon, MD a, Kenric M. Murayama, MD b, * KEYWORDS Bariatric surgery Outcomes Obesity Obesity is a global health problem and the exponential increase in obesity
2/10/2014 CARDIOVASCULAR BENEFITS OF BARIATRIC SURGERY. Disclosures. My Background
 CARDIOVASCULAR BENEFITS OF BARIATRIC SURGERY Anthony M Gonzalez, MD, FACS, FASMBS Associate Professor of Surgery, FIU College of Medicine Chief of Surgery, Baptist Hospital of Miami Medical Director Bariatric
CARDIOVASCULAR BENEFITS OF BARIATRIC SURGERY Anthony M Gonzalez, MD, FACS, FASMBS Associate Professor of Surgery, FIU College of Medicine Chief of Surgery, Baptist Hospital of Miami Medical Director Bariatric
Obesity and Weight Loss Surgery for the Primary Care Physician
 Saturday General Session Obesity and Weight Loss Surgery for the Primary Care Physician Nicole Basa, MD Bariatric and General Surgeon Cedar Park Surgeons, PA Cedar Park, Texas Educational Objectives By
Saturday General Session Obesity and Weight Loss Surgery for the Primary Care Physician Nicole Basa, MD Bariatric and General Surgeon Cedar Park Surgeons, PA Cedar Park, Texas Educational Objectives By
The Bariatric and Heartburn Center of Northeast Ohio
 The Bariatric and Heartburn Center of Northeast Ohio A message from Dr. Chlysta: Walter J. Chlysta MD, FACS, FASMBS 1900 23 rd Street, Suite 403 Cuyahoga Falls, OH 44223 Phone 330-926-3443 Fax 330-255-5092
The Bariatric and Heartburn Center of Northeast Ohio A message from Dr. Chlysta: Walter J. Chlysta MD, FACS, FASMBS 1900 23 rd Street, Suite 403 Cuyahoga Falls, OH 44223 Phone 330-926-3443 Fax 330-255-5092
Current Trends in Bariatric Surgery
 Current Trends in Bariatric Surgery 9.28.2017 Abraham Krikhely, MD, FACS, FASMBS Assistant Professor of Surgery, CUMC Center of Minimal Access, Metabolic and Weight Loss Surgery Outline Why consider surgery
Current Trends in Bariatric Surgery 9.28.2017 Abraham Krikhely, MD, FACS, FASMBS Assistant Professor of Surgery, CUMC Center of Minimal Access, Metabolic and Weight Loss Surgery Outline Why consider surgery
6/10/2016. Bariatric Surgery: Impact on Diabetes and CVD Risk. Disclosures BARIATRIC PROCEDURES
 Bariatric Surgery: Impact on Diabetes and CVD Risk Anthony M Gonzalez, MD, FACS, FASMBS Medical Director Bariatric Surgery, South Miami Hospital Chief of Surgery, Baptist Hospital of Miami Associate Professor
Bariatric Surgery: Impact on Diabetes and CVD Risk Anthony M Gonzalez, MD, FACS, FASMBS Medical Director Bariatric Surgery, South Miami Hospital Chief of Surgery, Baptist Hospital of Miami Associate Professor
Surgical management of super super obese patients: Roux-en-Y gastric bypass versus sleeve gastrectomy
 Surg Endosc (2016) 30:2097 2102 DOI 10.1007/s00464-015-4465-6 and Other Interventional Techniques Surgical management of super super obese patients: Roux-en-Y gastric bypass versus sleeve gastrectomy Raquel
Surg Endosc (2016) 30:2097 2102 DOI 10.1007/s00464-015-4465-6 and Other Interventional Techniques Surgical management of super super obese patients: Roux-en-Y gastric bypass versus sleeve gastrectomy Raquel
Bariatric Surgery and Post Operative Patient Care Alisha M. Fuller DNP, CBN, FNP BC Tristate Bariatrics Clinical Director, NP Manager
 Bariatric Surgery and Post Operative Patient Care Alisha M. Fuller DNP, CBN, FNP BC Tristate Bariatrics Clinical Director, NP Manager Presentation Objectives Causes of Obesity Measuring Obesity Medical/Psychological/Social
Bariatric Surgery and Post Operative Patient Care Alisha M. Fuller DNP, CBN, FNP BC Tristate Bariatrics Clinical Director, NP Manager Presentation Objectives Causes of Obesity Measuring Obesity Medical/Psychological/Social
OBESITY AND WEIGHT LOSS SURGERY FOR THE PRIMARY CARE PHYSICIAN
 OBESITY AND WEIGHT LOSS SURGERY FOR THE PRIMARY CARE PHYSICIAN Nicole Basa, M.D., F.A.C.S., F.A.S.M.B.S Assistant Professor of Surgery Texas A&M Medical School Bariatric Medical Director- Cedar Park Regional
OBESITY AND WEIGHT LOSS SURGERY FOR THE PRIMARY CARE PHYSICIAN Nicole Basa, M.D., F.A.C.S., F.A.S.M.B.S Assistant Professor of Surgery Texas A&M Medical School Bariatric Medical Director- Cedar Park Regional
SURGICAL TREATMENT FOR OBESITY: WHAT S THE BEST OPTION? Natan Zundel, MD, FACS, FASMBS
 SURGICAL TREATMENT FOR OBESITY: WHAT S THE BEST OPTION? Natan Zundel, MD, FACS, FASMBS Professor of Surgery Vice-Chairman Department of Surgery Florida International University Herbert Wertheim College
SURGICAL TREATMENT FOR OBESITY: WHAT S THE BEST OPTION? Natan Zundel, MD, FACS, FASMBS Professor of Surgery Vice-Chairman Department of Surgery Florida International University Herbert Wertheim College
Update on Treating Obesity: A Multidisciplinary Approach. Marie Harkins, FNP BC, CDE Cayuga Center for Healthy Living
 Update on Treating Obesity: A Multidisciplinary Approach Marie Harkins, FNP BC, CDE Cayuga Center for Healthy Living Objectives 1. Define obesity as a disease 2. List the stepwise approach to obesity treatment
Update on Treating Obesity: A Multidisciplinary Approach Marie Harkins, FNP BC, CDE Cayuga Center for Healthy Living Objectives 1. Define obesity as a disease 2. List the stepwise approach to obesity treatment
Bariatric Care Center Outcomes Report
 Bariatric Care Center 215 Outcomes Report Since my surgery, my life is happier; I am happier with myself. Lisa Mark, Weight Loss Surgery Patient 2 Bariatric Care Center Contents Surgical Procedure Volume
Bariatric Care Center 215 Outcomes Report Since my surgery, my life is happier; I am happier with myself. Lisa Mark, Weight Loss Surgery Patient 2 Bariatric Care Center Contents Surgical Procedure Volume
Objectives. Size Does Matter. Definitions
 Size Does Matter Bariatric Surgery New Procedures. What are the results? What is the future? Ashley Vergis MMEd MD FRCSC FACS Clinical Lead WRHA Bariatric Surgery Initiative Assistant Professor, Department
Size Does Matter Bariatric Surgery New Procedures. What are the results? What is the future? Ashley Vergis MMEd MD FRCSC FACS Clinical Lead WRHA Bariatric Surgery Initiative Assistant Professor, Department
Marc Bessler, M.D.*, Amna Daud, M.D., M.P.H., Teresa Kim, M.D., Mary DiGiorgi, M.P.H.
 Surgery for Obesity and Related Diseases 3 (2007) 480 485 Original article Prospective randomized trial of banded versus nonbanded gastric bypass for the super obese: early results Marc Bessler, M.D.*,
Surgery for Obesity and Related Diseases 3 (2007) 480 485 Original article Prospective randomized trial of banded versus nonbanded gastric bypass for the super obese: early results Marc Bessler, M.D.*,
Prevalence of Obesity (Adults) Prevalence of Obesity (Children) CURRENT STRATEGIES IN. Obesity: 33.8% Men: 32.2% Women: 35.5%
 Prevalence of Obesity (Children) CURRENT STRATEGIES IN. Obesity: 33.8% Men: 32.2% Women: 35.5%") CURRENT STRATEGIES IN OBESITY Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Prevalence of Obesity (Adults) Obesity:
CURRENT STRATEGIES IN OBESITY Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Prevalence of Obesity (Adults) Obesity:
Medical Policy Bariatric Surgery. Document Number: 042 Commercial and Qualified Health Plans MassHealth Authorization required X X
 Medical Policy Bariatric Surgery Document Number: 042 Commercial and Qualified Health Plans MassHealth Authorization required X X No Prior Authorization Overview The purpose of this document is to describe
Medical Policy Bariatric Surgery Document Number: 042 Commercial and Qualified Health Plans MassHealth Authorization required X X No Prior Authorization Overview The purpose of this document is to describe
OBESITY:Pharmacotherapy Vs Surgery
 OBESITY:Pharmacotherapy Vs Surgery Dr. Ranajit Sen Chowdhury Associate Professor Department of Medicine Sir Salimullah Medical College & Mitford Hospital. 1 Historical Perspective Paleolithic Era > 25,000
OBESITY:Pharmacotherapy Vs Surgery Dr. Ranajit Sen Chowdhury Associate Professor Department of Medicine Sir Salimullah Medical College & Mitford Hospital. 1 Historical Perspective Paleolithic Era > 25,000
Bariatric Surgery vs. Intensive Medical Therapy in Obese Diabetic Patients: 3-Year Outcomes
 Bariatric Surgery vs. Intensive Medical Therapy in Obese Diabetic Patients: 3-Year Outcomes Results of the STAMPEDE Trial Philip R Schauer, Deepak L Bhatt, John P Kirwan, Kathy Wolski, Stacy A Brethauer,
Bariatric Surgery vs. Intensive Medical Therapy in Obese Diabetic Patients: 3-Year Outcomes Results of the STAMPEDE Trial Philip R Schauer, Deepak L Bhatt, John P Kirwan, Kathy Wolski, Stacy A Brethauer,
Long Term Follow-up. 6 Month 1 Year Annual enter year #: What is the assessment date: / / Unknown. Is the patient alive? Yes No
 Long Term Follow-up 6 Month 1 Year Annual enter year #: What is the assessment date: / / Unknown Is the patient alive? Yes No Was an exam performed by a bariatric physician or PA/NP? Yes No Was the patient
Long Term Follow-up 6 Month 1 Year Annual enter year #: What is the assessment date: / / Unknown Is the patient alive? Yes No Was an exam performed by a bariatric physician or PA/NP? Yes No Was the patient