MSCC CARE PATHWAYS & CASE STUDIES. By Michael Balloch Spine CNS
|
|
|
- Sandra Weaver
- 5 years ago
- Views:
Transcription
1 MSCC CARE PATHWAYS & CASE STUDIES By Michael Balloch Spine CNS
2 Aims To be familiar with the routes of MSCC prentaion
3 How the guidelines work in practice Routes of presentation Generic intervention Managing patients not known to have cancer Factors influencing the decision for surgical intervention or oncology management Case studies
4 Routes of Presentation GP Self referral CNS Community or Hospital Palliative Care Teams Transfer from DGH A&E NGH WPH Direct NGH
5 Generic Interventions Patient history: Symptoms Duration, intensity, progression PMH Co-morbidities, Performance status Neurological assessment Baseline & daily re-assessments MRI whole spine
6 Flat bed rest until spinal stability has been assessed Pain control High dose Dexamethasone (PPI cover) VTE prophylaxis General Nursing care and psychological support
7 Known Cancer Diagnosis Liaison with Oncology team regarding prognosis and PS prior to this episode Surgical intervention If not a surgical candidate for Radiothapy
8 Not a known cancer Eliminate cancers where surgery is not necessarily the primary treatment: Prostate PSA and DRI (Degaralix) Myeloma myeloma screen + Benz jones Lymphoma examination / history, Lymphoma kit (Chemotherapy is optimal treatment for Haematological malignancies)
9 Consider germ cell tumours (particularly in younger men) Total HCG, AFP and Plap CT Chest, Abdomen & Pelvis If likely Renal Cell patient will need embolisation prior to surgery.
10 Factors influencing the choice of primary treatment Is this a cancer which is better treated by chemotherapy / hormone blockade? Is this technically possible? Is the patient able to tolerate the procedure and the recovery period? (prognosis / PS)
11 Patient symptoms suggestive of MSCC High suspicion MSCC / History of cancer with: NEW onset of pain Back pain band-like Radicular pain Neurological changes Weakness to limbs Altered sensation Urinary / faecal incontinence
12 Role of Radiotherapy Given if surgery not technically possible or due to patient limiting factors Post surgery usually 6 weeks post-op (rehab and wound healing)
13 CASE STUDY 1
14 Case one DT 49 year old Male Presenting to Rotherham hospital worsening back pain Left sided hip and leg pain Clinically well obs stable PMH Squamous Cell carcinoma right side of his neck Gout HTN Never smoked Doesn t drink Social Lives with wife & four children
15 Examination NGH 2/12/15 Neurological exam Digital Rectal Examination (DRE) Normal tone / sensation Rectum empty Lower limb Exam Tone: R normal, L slightly flaccid Power: R 5/5, L 4/5 Reflex: R Present, L Absent Sensation: R Peripheral neuropathy, L reduced L4 No bladder / bowel dysfunction
16 High or low suggestion of MSCC?
17 Patient symptoms suggestive of MSCC High suspicion of MSCC History of cancer with: NEW onset of pain Back pain band-like Radicular pain Neurological changes Weakness to limbs Altered sensation Urinary / faecal incontinence

18
19 X-ray Implies fracture at L4 No history of trauma? Pathological

20

21
22
23
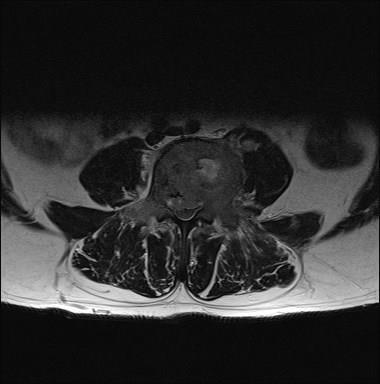
24 MRI Confirming Metastatic lesion L4, causing compression? From pre Ca? Unknown Already done Myeloma screen, PSA 2.3
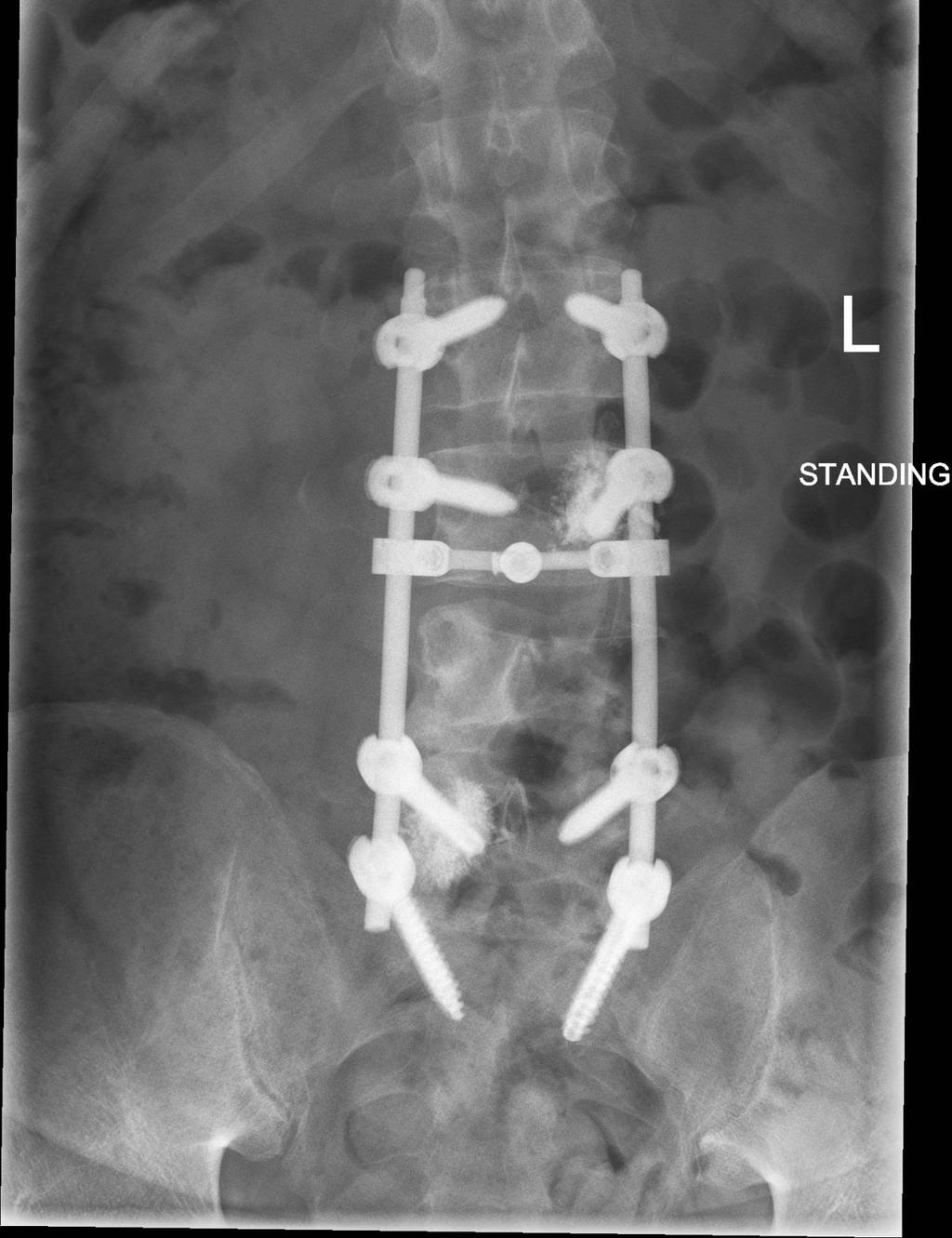
25 Decompression at L4 & stabilisation from L2-S1 3/12/15 Bone biopsy Head & Neck MDT +/- oncology F/U Chase Biopsy Palliative Care involvement Discharged 9/12/15
26

27
28 20/12/16 Re- admitted 2 weeks post discharge at 22:00 Increased Back pain Reduced mobility Normal tone Reduced neurology from L2/3 Reduced reflexes Worse on mobilisation
29 High or low suggestions for MSCC?
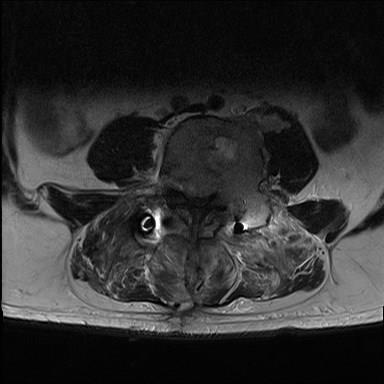
30 MRI Reports wide spread spinal Mets Deterioration at L4 since previous scan Worsening of the central canal stenosis

31
32
33 Plan 22/12/15 Dexamethasone & PPI CT Chest Abdo Pelvis D/W oncology Will see as OPA in 2days 2 nd Biopsy Problem No one able to do CT biopsy
34 Plan Further Decompression of L4 & open biopsy. Home for Xmas Back Boxing day for theatre
35 Able to mobilise better/ pain a lot better. Discharged home 29/12/16 Follow up with Oncology CUP Community Palliative Care DN wound check Follow up Spinal team 8 weeks
36
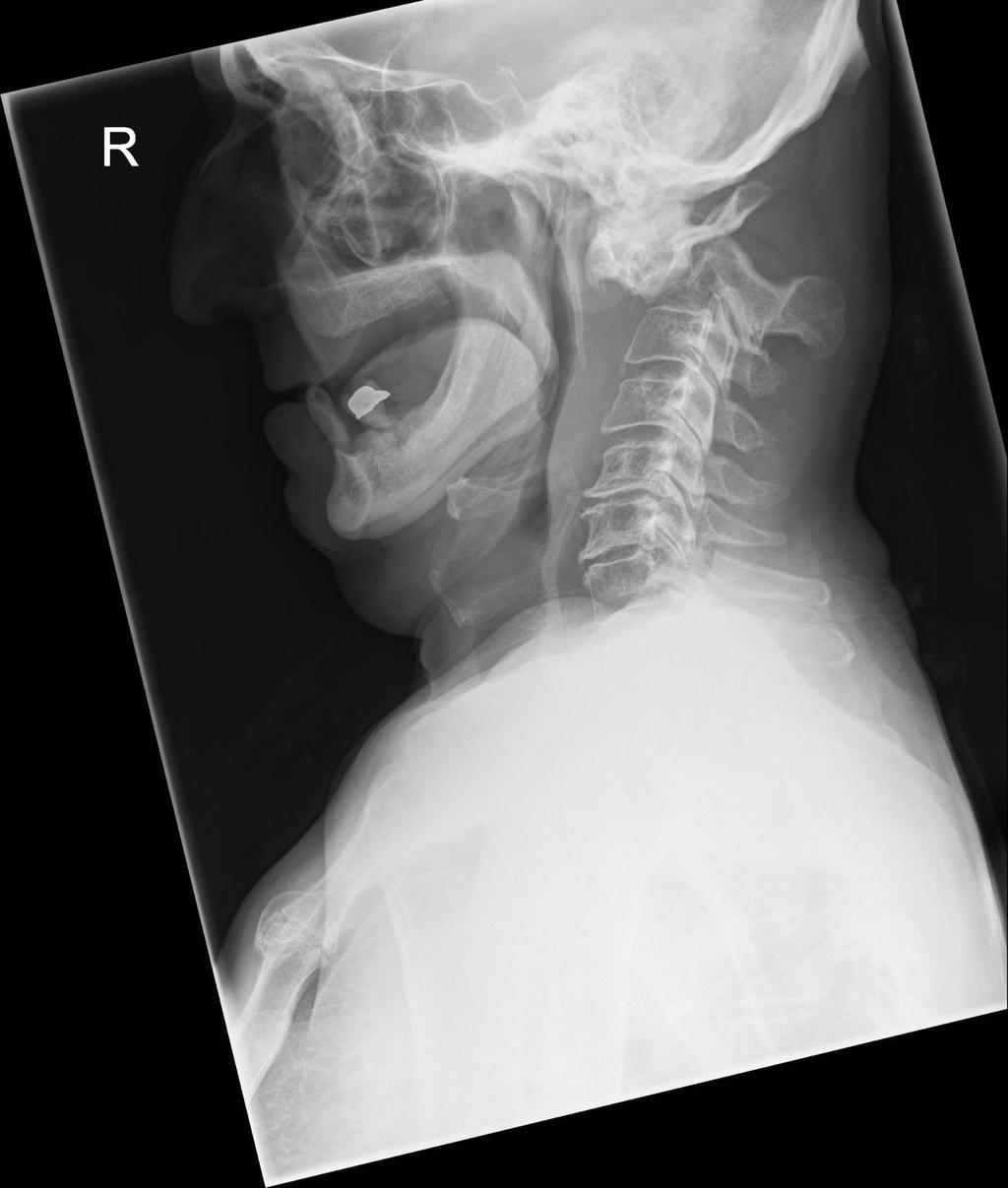
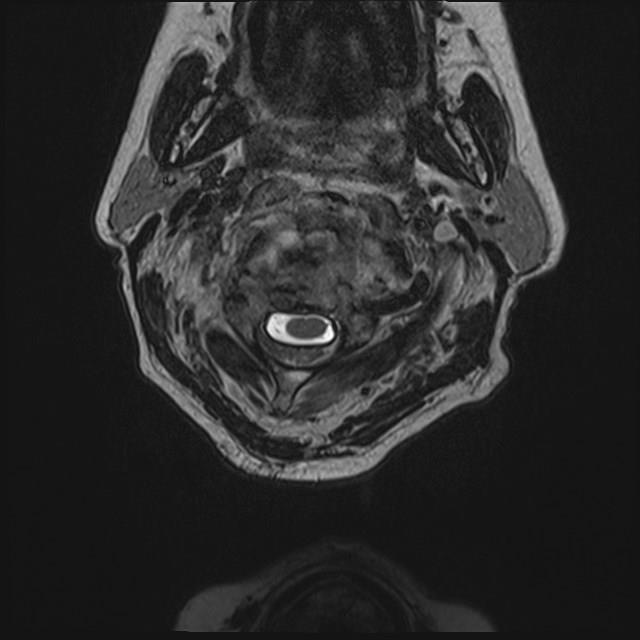
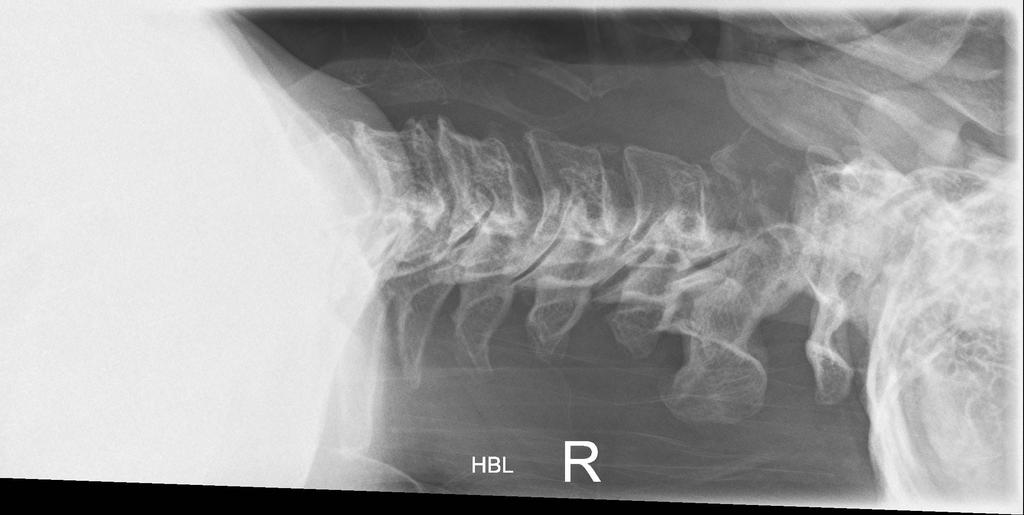
37 Case TW 68 year old male Neck/ Right arm pain PMH Recent DVT Deranged clotting Prostate Ca (under WPH) PS-0
38 Presenting DRI neck pain normal neurology Had X-ray Any suggestions of MSCC? High or low?
39
40 Plan at DRI MRI cervical CT neck with contrast Referred / transfer to NGH

41
42
43
44 NGH On examination appears to have normal upper and lower limb neurology Aspen Collar Lay flat for pain What do we do?
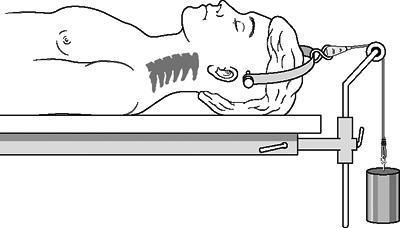
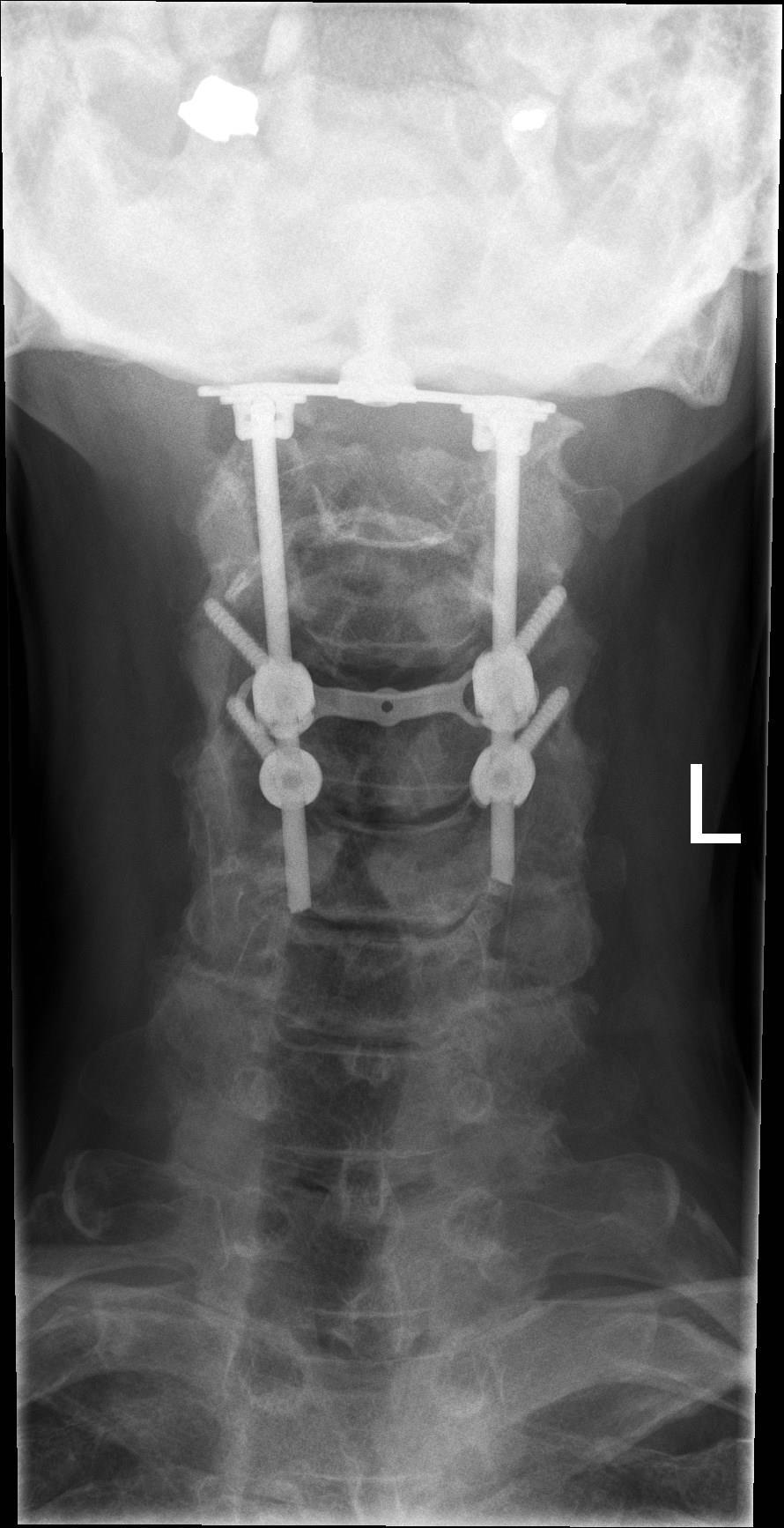
45 Plan Immobilise (Keep Flat) Discuss options with patient For Gardner-Wells traction Reduce the dislocation & realign the spine Theatre at some point Posterior stabilisation of C0-C4 Other considerations Deranged clotting pre DVT Haematologists involvement
46

47
48
49 Posterior C0-C4 stabilisation & decompression 16/03/16

50
51
52 22/03/16 Doing well post operatively Progressing with mobilising Pain controlled Sitting out No neurological deterioration Complication Chest infection Difficulty swallowing SALT Review Soft diet Planning for biopsy on metastatic deposit on his hip As not safe to obtain one from c spine He has done as an inpatient
53
Recognition & Treatment of Malignant Spinal Cord Compression Study Day
 Recognition & Treatment of Malignant Spinal Cord Compression Study Day 11 th May 2017 Dr Bernie Foran Consultant Clinical Oncologist & Honorary Senior Lecturer Weston Park Hospital Outline of Talk Clinical
Recognition & Treatment of Malignant Spinal Cord Compression Study Day 11 th May 2017 Dr Bernie Foran Consultant Clinical Oncologist & Honorary Senior Lecturer Weston Park Hospital Outline of Talk Clinical
Metastatic Spinal Disease
 Metastatic Spinal Disease Mr Neil Chiverton Consultant Spinal Surgeon, Sheffield Objectives The scale and nature of the problem NICE recommendations Surgical decision making Case illustrations Incidence
Metastatic Spinal Disease Mr Neil Chiverton Consultant Spinal Surgeon, Sheffield Objectives The scale and nature of the problem NICE recommendations Surgical decision making Case illustrations Incidence
PATHWAY MANAGEMENT OF METASTATIC SPINAL CORD COMPRESSION (MSCC) THE CHRISTIE, GREATER MANCHESTER & CHESHIRE
 THE CHRISTIE, GREATER MANCHESTER & CHESHIRE") PATHWAY MANAGEMENT OF METASTATIC SPINAL CORD COMPRESSION (MSCC) THE CHRISTIE, GREATER MANCHESTER & CHESHIRE Procedure Reference: Document Owner: Dr V. Misra Version: Accountable Committee: V3 MSCC Network
PATHWAY MANAGEMENT OF METASTATIC SPINAL CORD COMPRESSION (MSCC) THE CHRISTIE, GREATER MANCHESTER & CHESHIRE Procedure Reference: Document Owner: Dr V. Misra Version: Accountable Committee: V3 MSCC Network
Recognition & Treatment of Malignant Spinal Cord Compression
 Recognition & Treatment of Malignant Spinal Cord Compression Acute Oncology Study Day 15 th March 2018 Dr Bernie Foran Consultant Clinical Oncologist & Honorary Senior Lecturer Yorkshire & the Humber Weston
Recognition & Treatment of Malignant Spinal Cord Compression Acute Oncology Study Day 15 th March 2018 Dr Bernie Foran Consultant Clinical Oncologist & Honorary Senior Lecturer Yorkshire & the Humber Weston
Palliative Care Emergencies
 Palliative Care Emergencies LAURA BARNFIELD What might constitute an emergency in Palliative Care? 1 Palliative Care Emergencies Major haemorrhage Metastatic Spinal Cord Compression (MSCC) Superior Vena
Palliative Care Emergencies LAURA BARNFIELD What might constitute an emergency in Palliative Care? 1 Palliative Care Emergencies Major haemorrhage Metastatic Spinal Cord Compression (MSCC) Superior Vena
Recognition & Treatment of Malignant Spinal Cord Compression Study Day
 Recognition & Treatment of Malignant Spinal Cord Compression Study Day 16 th October 2014 Dr Bernie Foran Consultant Clinical Oncologist & Honorary Senior Lecturer Weston Park Hospital Outline of Talk
Recognition & Treatment of Malignant Spinal Cord Compression Study Day 16 th October 2014 Dr Bernie Foran Consultant Clinical Oncologist & Honorary Senior Lecturer Weston Park Hospital Outline of Talk
Cancer of Unknown Primary (CUP) Protocol
 Protocol") 1 Department of Oncology. Cancer of Unknown Primary (CUP) Protocol Version: Document type: Document sponsor Designation Document author [ s] Designation[s] Approving committee / Group Ratified by: Date
1 Department of Oncology. Cancer of Unknown Primary (CUP) Protocol Version: Document type: Document sponsor Designation Document author [ s] Designation[s] Approving committee / Group Ratified by: Date
Spinal cord compression: what it means and how it can be treated
 Spinal cord compression: what it means and how it can be treated Patient Information Oncology Department Author ID: Acute Oncology Nurse Specialist Leaflet Number: CC 036 Version: 2.1 Name of Leaflet:
Spinal cord compression: what it means and how it can be treated Patient Information Oncology Department Author ID: Acute Oncology Nurse Specialist Leaflet Number: CC 036 Version: 2.1 Name of Leaflet:
Developing spinal cord compression care guidelines at WPH
 Developing spinal cord compression care guidelines at WPH Spinal cord compression team: Sue Banks, Jean Buchanan, Dr Bernie Foran, Suzanne Hodson, Liz Kirkham, Rebecca Mills, Jan Siddall, Rebecca Walsh,
Developing spinal cord compression care guidelines at WPH Spinal cord compression team: Sue Banks, Jean Buchanan, Dr Bernie Foran, Suzanne Hodson, Liz Kirkham, Rebecca Mills, Jan Siddall, Rebecca Walsh,
Developing spinal cord compression care guidelines at WPH
 Developing spinal cord compression care guidelines at WPH Spinal cord compression team: Sue Banks, Jean Buchanan, Bernie Foran, Suzanne Hodson, Jane Mason, Rebecca Mills, Jan Siddall, Rebecca Walsh, Clare
Developing spinal cord compression care guidelines at WPH Spinal cord compression team: Sue Banks, Jean Buchanan, Bernie Foran, Suzanne Hodson, Jane Mason, Rebecca Mills, Jan Siddall, Rebecca Walsh, Clare
Louisa Fleure. Advanced Prostate Cancer Clinical Nurse Specialist. Guys and St Thomas NHS Trust
 Louisa Fleure Advanced Prostate Cancer Clinical Nurse Specialist Guys and St Thomas NHS Trust The classification of advanced prostate cancer The incidence of patients presenting with, or developing advanced
Louisa Fleure Advanced Prostate Cancer Clinical Nurse Specialist Guys and St Thomas NHS Trust The classification of advanced prostate cancer The incidence of patients presenting with, or developing advanced
MANAGEMENT OF PATIENTS WITH METASTATIC SPINAL CORD COMPRESSION
 CLINICAL POLICY MANAGEMENT OF PATIENTS WITH METASTATIC SPINAL CORD COMPRESSION DOCUMENT REF: PCLASCORD (Version No. 1.4) Name and designation of policy author(s) Approved by (committee, group, manager)
CLINICAL POLICY MANAGEMENT OF PATIENTS WITH METASTATIC SPINAL CORD COMPRESSION DOCUMENT REF: PCLASCORD (Version No. 1.4) Name and designation of policy author(s) Approved by (committee, group, manager)
Update on Management of Malignant Spinal Cord Compression. Heino Hugel Consultant in Palliative Medicine University Hospital Aintree
 Update on Management of Malignant Spinal Cord Compression Heino Hugel Consultant in Palliative Medicine University Hospital Aintree Current Guidelines The symptoms of MSCC may be subtle and therefore careful
Update on Management of Malignant Spinal Cord Compression Heino Hugel Consultant in Palliative Medicine University Hospital Aintree Current Guidelines The symptoms of MSCC may be subtle and therefore careful
How a fully integrated Acute Oncology Service can benefit the busy medical unit
 How a fully integrated Acute Oncology Service can benefit the busy medical unit Dr. Pauline Leonard MD FRCP Consultant Medical Oncologist Whittington Health Over the next 35 mins Briefly remind you of
How a fully integrated Acute Oncology Service can benefit the busy medical unit Dr. Pauline Leonard MD FRCP Consultant Medical Oncologist Whittington Health Over the next 35 mins Briefly remind you of
Malignant Spinal cord Compression. Dr. Thiru Thirukkumaran Palliative Care Services - Northwest Tasmania
 Malignant Spinal cord Compression Dr. Thiru Thirukkumaran Palliative Care Services - Northwest Tasmania Background Statistics of SCC -1 Incidence of SCC Vertebral body metastases 85 % Para-vertebral (Lymphoma)
Malignant Spinal cord Compression Dr. Thiru Thirukkumaran Palliative Care Services - Northwest Tasmania Background Statistics of SCC -1 Incidence of SCC Vertebral body metastases 85 % Para-vertebral (Lymphoma)
Metastatic Spinal Cord Compression
 Metastatic Spinal Cord Compression Dr Zacharias Tasigiannopoulos Clinical Oncologist Colney centre Department of Oncology Norwich, UK Introduction 2-5% of cancer patients have an episode of MSCC Initial
Metastatic Spinal Cord Compression Dr Zacharias Tasigiannopoulos Clinical Oncologist Colney centre Department of Oncology Norwich, UK Introduction 2-5% of cancer patients have an episode of MSCC Initial
North of Scotland Cancer Network Clinical Management Guideline for Metastatic Malignancy of Undefined Primary Origin (MUO)
") North of Scotland Cancer Network Clinical Management Guideline for Metastatic Malignancy of Undefined Primary Origin (MUO) UNCONTROLLED WHEN PRINTED DOCUMENT CONTROL Original Prepared by NMcL April 2016
North of Scotland Cancer Network Clinical Management Guideline for Metastatic Malignancy of Undefined Primary Origin (MUO) UNCONTROLLED WHEN PRINTED DOCUMENT CONTROL Original Prepared by NMcL April 2016
Cancer of Unknown Primary (CUP)
") Cancer of Unknown Primary (CUP) Pathways and Guidelines V1.0 London Cancer September 2013 The following pathways and guidelines document has been compiled by the London Cancer CUP technical subgroup and
Cancer of Unknown Primary (CUP) Pathways and Guidelines V1.0 London Cancer September 2013 The following pathways and guidelines document has been compiled by the London Cancer CUP technical subgroup and
Spinal cord compression
 Spinal cord compression Urology Department Patient Information Leaflet Introduction If you have been diagnosed with cancer, you need to know about spinal cord compression and the warning signs. This leaflet
Spinal cord compression Urology Department Patient Information Leaflet Introduction If you have been diagnosed with cancer, you need to know about spinal cord compression and the warning signs. This leaflet
Oncologic Emergencies: When to call the Radiation Oncologist
 Oncologic Emergencies: When to call the Radiation Oncologist Dr. Shrinivas Rathod Radiation Oncologist Radiation Oncology Program CancerCare Manitoba and University of Manitoba Disclosures Speaker s name:
Oncologic Emergencies: When to call the Radiation Oncologist Dr. Shrinivas Rathod Radiation Oncologist Radiation Oncology Program CancerCare Manitoba and University of Manitoba Disclosures Speaker s name:
CP80 Version: V01. Acute Oncology Management Service Date approved: 8 th May 2015 Date ratified: 1 st June 2015 Review date: 1 st June 2017
 STANDARD OPERATING PROCEDURE (SOP) AND PATHWAY FOR THE MANAGEMENT OF PATIENTS WITH METASTATIC SPINAL CORD COMPRESSION (MSCC) WITHIN THE CHRISTIE (Refer to the Manchester Cancer Network MSCC Pathway flowchart)
STANDARD OPERATING PROCEDURE (SOP) AND PATHWAY FOR THE MANAGEMENT OF PATIENTS WITH METASTATIC SPINAL CORD COMPRESSION (MSCC) WITHIN THE CHRISTIE (Refer to the Manchester Cancer Network MSCC Pathway flowchart)
Cancer of Unknown Primary Service
 Cancer of Unknown Primary Service Dr Maurice Fernando Consultant In Specialist Palliative Care and CUP lead Doncaster and Bassetlaw Hospitals NHS FT Wakefield meeting -14-07-2016 CUP service CUP MDT
Cancer of Unknown Primary Service Dr Maurice Fernando Consultant In Specialist Palliative Care and CUP lead Doncaster and Bassetlaw Hospitals NHS FT Wakefield meeting -14-07-2016 CUP service CUP MDT
Radiotherapy for lymphoma
 Radiotherapy for lymphoma The name of your consultant is: The radiographer who explained the treatment to you is: You can contact us on: What is radiotherapy? Radiotherapy treats cancer by using high energy
Radiotherapy for lymphoma The name of your consultant is: The radiographer who explained the treatment to you is: You can contact us on: What is radiotherapy? Radiotherapy treats cancer by using high energy
Acute Oncology Services Clinical Forum: Metastatic Spinal Cord Compression. Tuesday 17 th September 2013
 Acute Oncology Services Clinical Forum: Metastatic Spinal Cord Compression Tuesday 17 th September 2013 Welcome, Introduction and Aims of the Event Dr Tom Newsom-Davis, LCA AOS Pathway Chair Why MSCC?
Acute Oncology Services Clinical Forum: Metastatic Spinal Cord Compression Tuesday 17 th September 2013 Welcome, Introduction and Aims of the Event Dr Tom Newsom-Davis, LCA AOS Pathway Chair Why MSCC?
Suspected spinal cord compression form
 Suspected spinal cord compression form Enter this form into the notes at the appropriate date in the Progress / Evaluation sheets. Please copy this form to Lisa Lewis, Medical PA (ext 4551), for audit
Suspected spinal cord compression form Enter this form into the notes at the appropriate date in the Progress / Evaluation sheets. Please copy this form to Lisa Lewis, Medical PA (ext 4551), for audit
Spinal Cord Compression Diagnosis and Management. Information for Shared Care Centres and Community Staff
 Reference: CG1412 Written by: Dr Daniel Yeomanson Peer reviewer Dr Jeanette Payne Approved: August 2016 Approved by D&TC: 10 th June 2016 Review Due: August 2019 Intended Audience This document contains
Reference: CG1412 Written by: Dr Daniel Yeomanson Peer reviewer Dr Jeanette Payne Approved: August 2016 Approved by D&TC: 10 th June 2016 Review Due: August 2019 Intended Audience This document contains
Management of Acute Oncological emergencies
 Management of Acute Oncological emergencies Malignant Spinal cord compression (MSCC) Neutropenic sepsis Superior vena caval obstruction Hypercalcemia Hyponatremia Bowel obstruction Brain Metastasis with
Management of Acute Oncological emergencies Malignant Spinal cord compression (MSCC) Neutropenic sepsis Superior vena caval obstruction Hypercalcemia Hyponatremia Bowel obstruction Brain Metastasis with
Louisa Fleure. Advanced Prostate Cancer Clinical Nurse Specialist. Guys and St Thomas NHS Trust
 Louisa Fleure Advanced Prostate Cancer Clinical Nurse Specialist Guys and St Thomas NHS Trust The classification of advanced prostate cancer The incidence of patients presenting with, or developing advanced
Louisa Fleure Advanced Prostate Cancer Clinical Nurse Specialist Guys and St Thomas NHS Trust The classification of advanced prostate cancer The incidence of patients presenting with, or developing advanced
GUIDELINES FOR RADIOTHERAPY IN SPINAL CORD COMPRESSION THE CHRISTIE, GREATER MANCHESTER & CHESHIRE. Version:
 GUIDELINES FOR RADIOTHERAPY IN SPINAL CORD COMPRESSION THE CHRISTIE, GREATER MANCHESTER & CHESHIRE Procedure Reference: Document Owner: Dr V. Misra Version: Accountable Committee: V4 Acute Oncology Group
GUIDELINES FOR RADIOTHERAPY IN SPINAL CORD COMPRESSION THE CHRISTIE, GREATER MANCHESTER & CHESHIRE Procedure Reference: Document Owner: Dr V. Misra Version: Accountable Committee: V4 Acute Oncology Group
Metastatic Spinal Cord Compression (MSCC) Clinical guidelines and pathway
 Clinical guidelines and pathway") Metastatic Spinal Cord Compression (MSCC) Clinical guidelines and pathway Version 2: May 2012 To be read in conjunction with NICE CG75 Developed by consensus by: Dr Peter Robson, Consultant Oncologist,
Metastatic Spinal Cord Compression (MSCC) Clinical guidelines and pathway Version 2: May 2012 To be read in conjunction with NICE CG75 Developed by consensus by: Dr Peter Robson, Consultant Oncologist,
Prostate Cancer THE BIG 5 CANCERS AFFECTING MEN IN SA IT IS ESTIMATED THAT 1 IN 19 SOUTH AFRICAN MEN WILL DEVELOP PROSTATE CANCER SYMPTOMS SCREENING
 #1 Prostate Cancer IT IS ESTIMATED THAT 1 IN 19 SOUTH AFRICAN MEN WILL DEVELOP PROSTATE CANCER Prostate cancer often occurs without any symptoms Symptoms more likely if advanced: Frequent urination, esp
#1 Prostate Cancer IT IS ESTIMATED THAT 1 IN 19 SOUTH AFRICAN MEN WILL DEVELOP PROSTATE CANCER Prostate cancer often occurs without any symptoms Symptoms more likely if advanced: Frequent urination, esp
PATHWAY FOR INVESTIGATION OF ADULTS PRESENTING WITH ASCITES. U/S Abdo/pelvis shows ascites without obvious evidence of 1 liver disease
 PATHWAY FOR INVESTIGATION OF ADULTS PRESENTING WITH ASCITES U/S Abdo/pelvis shows ascites without obvious evidence of 1 liver disease Refer back to original requester with this paperwork and review previous
PATHWAY FOR INVESTIGATION OF ADULTS PRESENTING WITH ASCITES U/S Abdo/pelvis shows ascites without obvious evidence of 1 liver disease Refer back to original requester with this paperwork and review previous
Faster Cancer Treatment Indicators: Use cases
 Faster Cancer Treatment Indicators: Use cases 2014 Date: October 2014 Version: Owner: Status: v01 Ministry of Health Cancer Services Final Citation: Ministry of Health. 2014. Faster Cancer Treatment Indicators:
Faster Cancer Treatment Indicators: Use cases 2014 Date: October 2014 Version: Owner: Status: v01 Ministry of Health Cancer Services Final Citation: Ministry of Health. 2014. Faster Cancer Treatment Indicators:
Malignant Spinal Cord Compression (MSCC) Clinical Advisor Coordinator
 Clinical Advisor Coordinator") Malignant Spinal Cord Compression (MSCC) Clinical Advisor Coordinator Induction Training 2016 Version Control This is a controlled document please destroy all previous versions on receipt of a new version.
Malignant Spinal Cord Compression (MSCC) Clinical Advisor Coordinator Induction Training 2016 Version Control This is a controlled document please destroy all previous versions on receipt of a new version.
Spinal injury. Structure of the spine
 Spinal injury Structure of the spine Some understanding of the structure of the spine (spinal column) and the spinal cord is important as it helps your Neurosurgeon explain about the part of the spine
Spinal injury Structure of the spine Some understanding of the structure of the spine (spinal column) and the spinal cord is important as it helps your Neurosurgeon explain about the part of the spine
Liver and Pancreatic Case discussion
 The Royal Marsden Liver and Pancreatic Case discussion Dr Ian Chau Consultant Medical Oncologist The Royal Marsden 77 year old gentleman with 2 months history of vague abdominal ache and clinically finding
The Royal Marsden Liver and Pancreatic Case discussion Dr Ian Chau Consultant Medical Oncologist The Royal Marsden 77 year old gentleman with 2 months history of vague abdominal ache and clinically finding
Somerset, Wiltshire, Avon and Gloucestershire (SWAG) Cancer Services. Cancer of Unknown Primary Network Site Specific Group. Clinical Guidelines
 Cancer Services. Cancer of Unknown Primary Network Site Specific Group. Clinical Guidelines") Somerset, Wiltshire, Avon and Gloucestershire (SWAG) Cancer Services Cancer of Unknown Primary Network Site Specific Group Revision due: April 2019 Page 1 of 11 VERSION CONTROL THIS IS A CONTROLLED DOCUMENT.
Somerset, Wiltshire, Avon and Gloucestershire (SWAG) Cancer Services Cancer of Unknown Primary Network Site Specific Group Revision due: April 2019 Page 1 of 11 VERSION CONTROL THIS IS A CONTROLLED DOCUMENT.
Guidelines for the Management of Prostate Cancer West Midlands Expert Advisory Group for Urological Cancer
 Guidelines for the Management of Prostate Cancer West Midlands Expert Advisory Group for Urological Cancer West Midlands Clinical Networks and Clinical Senate Coversheet for Network Expert Advisory Group
Guidelines for the Management of Prostate Cancer West Midlands Expert Advisory Group for Urological Cancer West Midlands Clinical Networks and Clinical Senate Coversheet for Network Expert Advisory Group
PROSTATE CANCER STRATIFIED FOLLOW UP. Hilary Baker Lead CNS for Uro-oncology MSc, BSc, RGN.
 PROSTATE CANCER STRATIFIED FOLLOW UP Hilary Baker Lead CNS for Uro-oncology MSc, BSc, RGN. LEARNING OBJECTIVES To refresh your knowledge about prostate cancer. To discuss the purpose and patient benefits
PROSTATE CANCER STRATIFIED FOLLOW UP Hilary Baker Lead CNS for Uro-oncology MSc, BSc, RGN. LEARNING OBJECTIVES To refresh your knowledge about prostate cancer. To discuss the purpose and patient benefits
Management of Cancer Associated Thrombosis (CAT) where data is lacking. Tim Nokes Haematologist, Derriford Hospital, Plymouth
 where data is lacking. Tim Nokes Haematologist, Derriford Hospital, Plymouth") Management of Cancer Associated Thrombosis (CAT) where data is lacking Tim Nokes Haematologist, Derriford Hospital, Plymouth Contents Overview of the statistics and aetiology for Cancer Associated Thrombosis
Management of Cancer Associated Thrombosis (CAT) where data is lacking Tim Nokes Haematologist, Derriford Hospital, Plymouth Contents Overview of the statistics and aetiology for Cancer Associated Thrombosis
The use of surgery in the elderly. for management of metastatic epidural spinal cord compression
 The use of surgery in the elderly Bone Tumor Simulators for management of metastatic epidural spinal cord compression Justin E. Bird, M.D. Assistant Professor Orthopaedic Oncology and Spine Surgery Epidemiology
The use of surgery in the elderly Bone Tumor Simulators for management of metastatic epidural spinal cord compression Justin E. Bird, M.D. Assistant Professor Orthopaedic Oncology and Spine Surgery Epidemiology
Fractures of the Thoracic and Lumbar Spine
 A spinal fracture is a serious injury. Nader M. Hebela, MD Fellow of the American Academy of Orthopaedic Surgeons http://orthodoc.aaos.org/hebela Cleveland Clinic Abu Dhabi Cleveland Clinic Abu Dhabi Neurological
A spinal fracture is a serious injury. Nader M. Hebela, MD Fellow of the American Academy of Orthopaedic Surgeons http://orthodoc.aaos.org/hebela Cleveland Clinic Abu Dhabi Cleveland Clinic Abu Dhabi Neurological
Attachment #2 Overview of Follow-up
 Attachment #2 Overview of Follow-up Provided below is a general overview of follow-up and this may vary based on specific patient or cancer characteristics. Of note, Labs and imaging can be performed closer
Attachment #2 Overview of Follow-up Provided below is a general overview of follow-up and this may vary based on specific patient or cancer characteristics. Of note, Labs and imaging can be performed closer
Bone Metastases. Sukanda Denjanta, M.Sc., BCOP Pharmacy Department, Chiangrai Prachanukroh Hospital
 Bone Metastases Sukanda Denjanta, M.Sc., BCOP Pharmacy Department, Chiangrai Prachanukroh Hospital 1 Outline Pathophysiology Signs & Symptoms Diagnosis Treatment Spinal Cord Compression 2 General Information
Bone Metastases Sukanda Denjanta, M.Sc., BCOP Pharmacy Department, Chiangrai Prachanukroh Hospital 1 Outline Pathophysiology Signs & Symptoms Diagnosis Treatment Spinal Cord Compression 2 General Information
The management and treatment options for secondary bone disease. Dr Jason Lester Clinical Oncologist Velindre Cancer Centre
 The management and treatment options for secondary bone disease Dr Jason Lester Clinical Oncologist Velindre Cancer Centre Aims Overview of bone metastases management in castrate-refractory prostate cancer
The management and treatment options for secondary bone disease Dr Jason Lester Clinical Oncologist Velindre Cancer Centre Aims Overview of bone metastases management in castrate-refractory prostate cancer
Brain and Central Nervous System Cancers
 Brain and Central Nervous System Cancers NICE guidance link: https://www.nice.org.uk/guidance/ta121 Clinical presentation of brain tumours History and Examination Consider immediate referral Management
Brain and Central Nervous System Cancers NICE guidance link: https://www.nice.org.uk/guidance/ta121 Clinical presentation of brain tumours History and Examination Consider immediate referral Management
Case Scenario 1. 4/19/13 Bone Scan: No scintigraphic findings to suggest skeletal metastases.
 Case Scenario 1 3/8/13 H&P 68 YR W/M presents w/elevated PSA. Patient is a non-smoker, current alcohol use. Physical Exam: On digital rectal exam the sphincter tone is normal and there is a 1 cm nodule
Case Scenario 1 3/8/13 H&P 68 YR W/M presents w/elevated PSA. Patient is a non-smoker, current alcohol use. Physical Exam: On digital rectal exam the sphincter tone is normal and there is a 1 cm nodule
Appendix 4 Urology Care Pathways
 Appendix 4 Urology Care Pathways Cancer Care Pathways outline the steps and stages in the patient journey from referral through to diagnostics, staging, treatment, follow up, rehabilitation and if applicable
Appendix 4 Urology Care Pathways Cancer Care Pathways outline the steps and stages in the patient journey from referral through to diagnostics, staging, treatment, follow up, rehabilitation and if applicable
North West London Trauma Network Spinal Pathway and Protocols
 North West London Trauma Network Spinal Pathway and Protocols 1. Spinal Clearance in the Trauma Patient Inclusions: All trauma patients who are not alert and orientated, unable to cooperate (including
North West London Trauma Network Spinal Pathway and Protocols 1. Spinal Clearance in the Trauma Patient Inclusions: All trauma patients who are not alert and orientated, unable to cooperate (including
Navigators Lead the Way
 RN Navigators Their Role in patients with Cancers of the GI tract Navigators Lead the Way Nurse Navigator Defined Nurse Navigator A clinically trained individual responsible for the identification and
RN Navigators Their Role in patients with Cancers of the GI tract Navigators Lead the Way Nurse Navigator Defined Nurse Navigator A clinically trained individual responsible for the identification and
3.1 Investigations for Patients Presenting with Haematuria Table 1
 3.1 Investigations for Patients Presenting with Haematuria Table 1 Patients at risk of bacterial endocarditis should be given antibiotic prophylaxis as per local guidelines. Patients with heart valve replacements
3.1 Investigations for Patients Presenting with Haematuria Table 1 Patients at risk of bacterial endocarditis should be given antibiotic prophylaxis as per local guidelines. Patients with heart valve replacements
Femoral Neck (Hip) Fracture
 Fracture") Patient Information Leaflet Femoral Neck (Hip) Fracture Produced By: Orthopaedic Department September 2013 Review due September 2016 1 If you require this leaflet in another language, large print or another
Patient Information Leaflet Femoral Neck (Hip) Fracture Produced By: Orthopaedic Department September 2013 Review due September 2016 1 If you require this leaflet in another language, large print or another
Diagnosis and Classification of Prostate Cancer
 Patient Information English 32 Diagnosis and Classification of Prostate Cancer The underlined terms are listed in the glossary. prostate biopsy is the only test that can confirm a prostate cancer diagnosis.
Patient Information English 32 Diagnosis and Classification of Prostate Cancer The underlined terms are listed in the glossary. prostate biopsy is the only test that can confirm a prostate cancer diagnosis.
Attachment #2 Overview of Follow-up
 Attachment #2 Overview of Follow-up Provided below is a general overview of follow-up and this may vary based on specific patient or cancer characteristics. Of note, Labs and imaging can be performed closer
Attachment #2 Overview of Follow-up Provided below is a general overview of follow-up and this may vary based on specific patient or cancer characteristics. Of note, Labs and imaging can be performed closer
Decision Making Flowchart for Metastatic Spinal Cord Compression and Pathological Spinal Fractures
 Decision Making Flowchart for Metastatic Spinal Cord Compression and Pathological Spinal Fractures All Referrals (see notes): Spinal Surgeons Locally or Trauma SpR at UHW Oncology SpR at Velindre / Singleton
Decision Making Flowchart for Metastatic Spinal Cord Compression and Pathological Spinal Fractures All Referrals (see notes): Spinal Surgeons Locally or Trauma SpR at UHW Oncology SpR at Velindre / Singleton
A schematic of the rectal probe in contact with the prostate is show in this diagram.
 Hello. My name is William Osai. I am a nurse practitioner in the GU Medical Oncology Department at The University of Texas MD Anderson Cancer Center in Houston. Today s presentation is Part 2 of the Overview
Hello. My name is William Osai. I am a nurse practitioner in the GU Medical Oncology Department at The University of Texas MD Anderson Cancer Center in Houston. Today s presentation is Part 2 of the Overview
Cancer of Unknown Primary
 Cancer of Unknown Primary Helen Rickards Acute Oncology and Cancer of Unknown Primary CNS 18 th May 2017 Defining CUP Incidence Patient Pathways getting a diagnosis Patient assessment The patient s perspective
Cancer of Unknown Primary Helen Rickards Acute Oncology and Cancer of Unknown Primary CNS 18 th May 2017 Defining CUP Incidence Patient Pathways getting a diagnosis Patient assessment The patient s perspective
Posterior Cervical Decompression
 Posterior Cervical Decompression Issue 5: March 2016 Review date: February 2019 Following your recent MRI scan and consultation with your spinal surgeon, you have been diagnosed with a narrowing of your
Posterior Cervical Decompression Issue 5: March 2016 Review date: February 2019 Following your recent MRI scan and consultation with your spinal surgeon, you have been diagnosed with a narrowing of your
Cervical cancer presentation
 Carcinoma of the cervix: Carcinoma of the cervix is the second commonest cancer among women worldwide, with only breast cancer occurring more commonly. Worldwide, cervical cancer accounts for about 500,000
Carcinoma of the cervix: Carcinoma of the cervix is the second commonest cancer among women worldwide, with only breast cancer occurring more commonly. Worldwide, cervical cancer accounts for about 500,000
Guidelines for the Management of Bladder Cancer West Midlands Expert Advisory Group for Urological Cancer
 Guidelines for the Management of Bladder Cancer West Midlands Expert Advisory Group for Urological Cancer West Midlands Clinical Networks and Clinical Senate Coversheet for Network Expert Advisory Group
Guidelines for the Management of Bladder Cancer West Midlands Expert Advisory Group for Urological Cancer West Midlands Clinical Networks and Clinical Senate Coversheet for Network Expert Advisory Group
Screening tests. When you need them and when you don t
 Screening tests When you need them and when you don t S creening tests help doctors look for diseases when you don t have symptoms. The tests can Screenings find problems early, when they are easier to
Screening tests When you need them and when you don t S creening tests help doctors look for diseases when you don t have symptoms. The tests can Screenings find problems early, when they are easier to
CLINICAL GUIDELINES. Primary Care Guideline Summary Lumbar Spine Thomas J. Gilbert M.D., M.P.P. 3/17/15 revision
 CLINICAL GUIDELINES Primary Care Guideline Summary Lumbar Spine Thomas J. Gilbert M.D., M.P.P. 3/17/15 revision TRIAGE At the initial visit, a focused history and physical examination is performed to assign
CLINICAL GUIDELINES Primary Care Guideline Summary Lumbar Spine Thomas J. Gilbert M.D., M.P.P. 3/17/15 revision TRIAGE At the initial visit, a focused history and physical examination is performed to assign
Radiotherapy for Rectal Cancer. Kevin Palumbo Adelaide Radiotherapy Centre
 Radiotherapy for Rectal Cancer Kevin Palumbo Adelaide Radiotherapy Centre Overview CRC are common (3 rd commonest cancer) rectal Ca approx 25-30% of all CRC. Presentation PR bleeding: beware attributing
Radiotherapy for Rectal Cancer Kevin Palumbo Adelaide Radiotherapy Centre Overview CRC are common (3 rd commonest cancer) rectal Ca approx 25-30% of all CRC. Presentation PR bleeding: beware attributing
SOUTH THAMES CHILDREN S CANCER NETWORK GROUP. REFERRAL PROTOCOLS AND DIAGNOSIS AND STAGING PROTOCOLS October 2014
 SOUTH THAMES CHILDREN S CANCER NETWORK GROUP REFERRAL PROTOCOLS AND DIAGNOSIS AND STAGING PROTOCOLS October 2014 Contents 1. Leukaemia Referral, Diagnostic and Staging Guidelines 2. Lymphoma Referral,
SOUTH THAMES CHILDREN S CANCER NETWORK GROUP REFERRAL PROTOCOLS AND DIAGNOSIS AND STAGING PROTOCOLS October 2014 Contents 1. Leukaemia Referral, Diagnostic and Staging Guidelines 2. Lymphoma Referral,
Testicular Cancer. Regional Follow-up Guidelines
 Urological Cancers Managed Clinical Network Testicular Cancer Regional Follow-up Guidelines Prepared by Drs J White/ A Waterston, J Salmond, J Wallace, Mr D Hendry, Approved by Urological Cancers MCN and
Urological Cancers Managed Clinical Network Testicular Cancer Regional Follow-up Guidelines Prepared by Drs J White/ A Waterston, J Salmond, J Wallace, Mr D Hendry, Approved by Urological Cancers MCN and
LOTHIAN LUMBAR SPINE PATHWAYS
 LOTHIAN LUMBAR SPINE PATHWAYS Patient Completes STarT Back form Assess patient and screen for Red Flags. If present refer to Appendix 1 Establish if Neurogenic. If so refer to Appendix 2 Children under
LOTHIAN LUMBAR SPINE PATHWAYS Patient Completes STarT Back form Assess patient and screen for Red Flags. If present refer to Appendix 1 Establish if Neurogenic. If so refer to Appendix 2 Children under
performed to help sway the clinician in what the appropriate diagnosis is, which can substantially alter the treatment of management.
 Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Common Treatment Related Sideeffects. Radical Prostatectomy Urinary Effects. Survivorship what is the unmet need?
 Side Effects of Prostate Cancer Treatment Christian Smith Clinician Nurse, Velindre Cancer Centre Common Treatment Related Sideeffects Urinary RP, EBRT, Brachy Bowel EBRT & Brachy Sexual All treatment
Side Effects of Prostate Cancer Treatment Christian Smith Clinician Nurse, Velindre Cancer Centre Common Treatment Related Sideeffects Urinary RP, EBRT, Brachy Bowel EBRT & Brachy Sexual All treatment
Rehabilitation and Metastatic Spinal Cord Compression
 Rehabilitation and Metastatic Spinal Cord Compression Pradeep Thumbikat MS, MSc, FRCS Consultant in Spinal Cord Injuries Sheffield Teaching Hospitals 1 Evidence for Rehabilitation Differences and similarities
Rehabilitation and Metastatic Spinal Cord Compression Pradeep Thumbikat MS, MSc, FRCS Consultant in Spinal Cord Injuries Sheffield Teaching Hospitals 1 Evidence for Rehabilitation Differences and similarities
Dr Hilary Williams. Consultant in Medical Oncology at Velindre Cancer Centre
 Dr Hilary Williams. Consultant in Medical Oncology at Velindre Cancer Centre Hilary.williams4@wales.nhs.uk Thinking about Acute Oncology. Why do we need acute oncology locally? What the Hub VCC provides
Dr Hilary Williams. Consultant in Medical Oncology at Velindre Cancer Centre Hilary.williams4@wales.nhs.uk Thinking about Acute Oncology. Why do we need acute oncology locally? What the Hub VCC provides
Scoliosis. This leaflet gives you information on scoliosis and what you can do to help manage the symptoms you are experiencing.
 Scoliosis This leaflet gives you information on scoliosis and what you can do to help manage the symptoms you are experiencing. What is Scoliosis? The term scoliosis refers to the abnormal twisting and
Scoliosis This leaflet gives you information on scoliosis and what you can do to help manage the symptoms you are experiencing. What is Scoliosis? The term scoliosis refers to the abnormal twisting and
AllinaHealthSystems 1
 2018 Dimensions in Oncology Genitourinary Cancer Disclosures I have no financial or commercial relationships relevant to this presentation. Matthew O Shaughnessy, MD, PhD Director of Urologic Oncology
2018 Dimensions in Oncology Genitourinary Cancer Disclosures I have no financial or commercial relationships relevant to this presentation. Matthew O Shaughnessy, MD, PhD Director of Urologic Oncology
Guidelines for the Management. Malignant Spinal Cord Compression. Final Guideline
 Guidelines for the Management Of Malignant Spinal Cord Compression Final Guideline 1. Introduction 1.1 Aetiology of MSCC 1.2 Use of the guidelines 2. Summary of Pathway 2.1 Algorithms 2.2 Role of the MSCC
Guidelines for the Management Of Malignant Spinal Cord Compression Final Guideline 1. Introduction 1.1 Aetiology of MSCC 1.2 Use of the guidelines 2. Summary of Pathway 2.1 Algorithms 2.2 Role of the MSCC
NICE BULLETIN Diagnosis & treatment of prostate cancer
 Diagnosis & treatment of prostate cancer NICE provided the content for this booklet which is independent of any company or product advertised Diagnosis and treatment of prostate cancer Introduction In
Diagnosis & treatment of prostate cancer NICE provided the content for this booklet which is independent of any company or product advertised Diagnosis and treatment of prostate cancer Introduction In
Laparotomy for large retroperitoneal mass:
 Laparotomy for large retroperitoneal mass: procedure-specific information UHB is a no smoking Trust To see all of our current patient information leaflets please visit www.uhb.nhs.uk/patient-information-leaflets.htm
Laparotomy for large retroperitoneal mass: procedure-specific information UHB is a no smoking Trust To see all of our current patient information leaflets please visit www.uhb.nhs.uk/patient-information-leaflets.htm
The Complex/Challenging Spine Patient Steve Wisniewski, M.D. Department of PM&R
 The Complex/Challenging Spine Patient Steve Wisniewski, M.D. Department of PM&R 2011 MFMER slide-1 Disclosures None 2011 MFMER slide-2 Learning Objectives Review indications for obtaining imaging studies
The Complex/Challenging Spine Patient Steve Wisniewski, M.D. Department of PM&R 2011 MFMER slide-1 Disclosures None 2011 MFMER slide-2 Learning Objectives Review indications for obtaining imaging studies
Ambulatory lung biopsy: a new model for the NHS. Dr Sam Hare Barnet Hospital Royal Free London NHS Trust
 Ambulatory lung biopsy: a new model for the NHS Dr Sam Hare Barnet Hospital Royal Free London NHS Trust Lung cancer Leading cause of UK cancer mortality UK: 2 nd lowest European survival rate 62-day RTT
Ambulatory lung biopsy: a new model for the NHS Dr Sam Hare Barnet Hospital Royal Free London NHS Trust Lung cancer Leading cause of UK cancer mortality UK: 2 nd lowest European survival rate 62-day RTT
Spinal cord compression as a first presentation of cancer: A case report
 J Pain Manage 2013;6(4):319-322 ISSN: 1939-5914 Nova Science Publishers, Inc. Spinal cord compression as a first presentation of cancer: A case report Nicholas Lao, BMSc(C), Michael Poon, MD(C), Marko
J Pain Manage 2013;6(4):319-322 ISSN: 1939-5914 Nova Science Publishers, Inc. Spinal cord compression as a first presentation of cancer: A case report Nicholas Lao, BMSc(C), Michael Poon, MD(C), Marko
JUSTIFICATION PROTOCOLS FOR CT SCANNING ALBURY WODONGA HEALTH WODONGA CAMPUS
 JUSTIFICATION PROTOCOLS FOR CT SCANNING ALBURY WODONGA HEALTH WODONGA CAMPUS JUSTIFICATION PROTOCOLS FOR CT SCANNING INTRODUCTION: In accordance with the Victorian Radiation Act 2005 Wodonga Medical Imaging,
JUSTIFICATION PROTOCOLS FOR CT SCANNING ALBURY WODONGA HEALTH WODONGA CAMPUS JUSTIFICATION PROTOCOLS FOR CT SCANNING INTRODUCTION: In accordance with the Victorian Radiation Act 2005 Wodonga Medical Imaging,
MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER
 10 MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER Recommendations from the EAU Working Party on Muscle Invasive and Metastatic Bladder Cancer G. Jakse (chairman), F. Algaba, S. Fossa, A. Stenzl, C. Sternberg
10 MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER Recommendations from the EAU Working Party on Muscle Invasive and Metastatic Bladder Cancer G. Jakse (chairman), F. Algaba, S. Fossa, A. Stenzl, C. Sternberg
Cancers of unknown primary : Knowing the unknown. Prof. Ahmed Hossain Professor of Medicine SSMC
 Cancers of unknown primary : Knowing the unknown Prof. Ahmed Hossain Professor of Medicine SSMC Definition Cancers of unknown primary site (CUPs) Represent a heterogeneous group of metastatic tumours,
Cancers of unknown primary : Knowing the unknown Prof. Ahmed Hossain Professor of Medicine SSMC Definition Cancers of unknown primary site (CUPs) Represent a heterogeneous group of metastatic tumours,
HIGH LEVEL - Science
 Learning Outcomes HIGH LEVEL - Science Describe the structure and function of the back and spine (8a) Outline the functional anatomy and physiology of the spinal cord and peripheral nerves (8a) Describe
Learning Outcomes HIGH LEVEL - Science Describe the structure and function of the back and spine (8a) Outline the functional anatomy and physiology of the spinal cord and peripheral nerves (8a) Describe
Coversheet for Network Site Specific Group Agreed Documentation. Diagnosis and Staging Protocol
 Coversheet for Network Site Specific Group Agreed Documentation Document Title Diagnosis and Staging Protocol Document Date July 2010 Consultation Process Consultation was by the West Midlands Children
Coversheet for Network Site Specific Group Agreed Documentation Document Title Diagnosis and Staging Protocol Document Date July 2010 Consultation Process Consultation was by the West Midlands Children
CANCER. Mrs. Davis Health Education
 CANCER Mrs. Davis Health Education Cancer Terms: Tumors: Masses of useless tissue Benign: Non-cancerous Malignant: Cancerous Metastasis: Spread of cancer from the point where it originated to other parts
CANCER Mrs. Davis Health Education Cancer Terms: Tumors: Masses of useless tissue Benign: Non-cancerous Malignant: Cancerous Metastasis: Spread of cancer from the point where it originated to other parts
Disclosures. Disclosures 27/01/2019. Modern approach and pitfalls in metastatic spine surgery. None.. Jeremy Reynolds
 Modern approach and pitfalls in metastatic spine surgery Jeremy Reynolds Spine Lead Oxford Bone and Soft Tissue Sarcoma Service MSCC Lead Thames Valley Cancer Network Clinical Lead Oxford Spine 1 Disclosures
Modern approach and pitfalls in metastatic spine surgery Jeremy Reynolds Spine Lead Oxford Bone and Soft Tissue Sarcoma Service MSCC Lead Thames Valley Cancer Network Clinical Lead Oxford Spine 1 Disclosures
COSD & Source of Referral
 COSD & Source of Referral A Brief guide October 2014 Michael Sharpe Data Improvement Manager National Cancer Registration Service What is COSD? Cancer and Outcomes Services Dataset Clinical dataset for
COSD & Source of Referral A Brief guide October 2014 Michael Sharpe Data Improvement Manager National Cancer Registration Service What is COSD? Cancer and Outcomes Services Dataset Clinical dataset for
Guidelines for the Shared Care of Patients on hormonal therapy for Prostate Cancer
 Peterborough City Hospital Department of Urology Guidelines for the Shared Care of Patients on hormonal therapy for Prostate Cancer Hormonal Therapy - How does it work? Prostate Cancer relies on the presence
Peterborough City Hospital Department of Urology Guidelines for the Shared Care of Patients on hormonal therapy for Prostate Cancer Hormonal Therapy - How does it work? Prostate Cancer relies on the presence
Surveillance after Treatment of Malignancies. John M. Burke, M.D. March 2013
 Surveillance after Treatment of Malignancies John M. Burke, M.D. March 2013 Disclosures Advisory Boards Spectrum Alexion Genomic Health Dendreon Seattle Genetics Learning Objectives Improve ability to
Surveillance after Treatment of Malignancies John M. Burke, M.D. March 2013 Disclosures Advisory Boards Spectrum Alexion Genomic Health Dendreon Seattle Genetics Learning Objectives Improve ability to
Clinical Biochemistry Department City Hospital
 Cancer Biochemistry and Tumour Markers Clinical Biochemistry Department City Hospital In this lecture Cancer basics Definition of Tumour Marker (TM) What is the perfect TM? History of TMs Examples of TMs
Cancer Biochemistry and Tumour Markers Clinical Biochemistry Department City Hospital In this lecture Cancer basics Definition of Tumour Marker (TM) What is the perfect TM? History of TMs Examples of TMs
Your Orthotics service is changing
 Your Orthotics service is changing Important for referrers on changes effective from January 2015 Why is the service changing? As demand for the orthotics service increases and budgets remain relatively
Your Orthotics service is changing Important for referrers on changes effective from January 2015 Why is the service changing? As demand for the orthotics service increases and budgets remain relatively
Suspecting Tumors, or Could it be cancer?
 Suspecting Tumors, or Could it be cancer? Donna E. Reece, M.D. Princess Margaret Cancer Centre University Health Network Toronto, ON CANADA 07 February 2018 Background Low back pain is common However,
Suspecting Tumors, or Could it be cancer? Donna E. Reece, M.D. Princess Margaret Cancer Centre University Health Network Toronto, ON CANADA 07 February 2018 Background Low back pain is common However,
Greater Manchester Commissioning Hub: Cancer Programme. The ACE Programme. Wave 2 Multidisciplinary Diagnostic Centres
 Greater Manchester Commissioning Hub: Cancer Programme The ACE Programme Wave 2 Multidisciplinary Diagnostic Centres Background / Context GM Pilot focuses on 2 areas of Greater Manchester: Oldham South
Greater Manchester Commissioning Hub: Cancer Programme The ACE Programme Wave 2 Multidisciplinary Diagnostic Centres Background / Context GM Pilot focuses on 2 areas of Greater Manchester: Oldham South
What to expect following spinal cord injury. Information for patients Therapy Services
 What to expect following spinal cord injury Information for patients Therapy Services Introduction This leaflet aims to explain what spinal cord injury is and what to expect over the next few months. What
What to expect following spinal cord injury Information for patients Therapy Services Introduction This leaflet aims to explain what spinal cord injury is and what to expect over the next few months. What
Chapter 3. Neoplasms. Copyright 2015 Cengage Learning.
 Chapter 3 Neoplasms Terminology Related to Neoplasms and Tumors Neoplasm New growth Tumor Swelling or neoplasm Leukemia Malignant disease of bone marrow Hematoma Bruise or contusion Classification of Neoplasms
Chapter 3 Neoplasms Terminology Related to Neoplasms and Tumors Neoplasm New growth Tumor Swelling or neoplasm Leukemia Malignant disease of bone marrow Hematoma Bruise or contusion Classification of Neoplasms
TRAJECTORY OF ILLNESS IN END OF LIFE CARE
 TRAJECTORY OF ILLNESS IN END OF LIFE CARE By Dr Helen Fryer OBJECTIVES To be aware of the three commonest trajectories of decline in the UK To understand the challenges faced in delivering effective Palliative
TRAJECTORY OF ILLNESS IN END OF LIFE CARE By Dr Helen Fryer OBJECTIVES To be aware of the three commonest trajectories of decline in the UK To understand the challenges faced in delivering effective Palliative
Glossary of Terms Primary Urethral Cancer
 Patient Information English Glossary of Terms Primary Urethral Cancer Advanced cancer A tumour that grows into deeper layers of tissue, adjacent organs, or surrounding muscles. Anaesthesia (general, spinal,
Patient Information English Glossary of Terms Primary Urethral Cancer Advanced cancer A tumour that grows into deeper layers of tissue, adjacent organs, or surrounding muscles. Anaesthesia (general, spinal,
One Stop Prostate Biopsy Protocol Author Consultation Date Approved
 One Stop Prostate Biopsy Protocol Author Consultation Date Approved Urology Nurse Practioner PROTOCOL FOR MEN ATTENDING A ONE STOP PROSTATE BIOPSY CLINIC RATIONALE Prostate cancer is the most common cancer
One Stop Prostate Biopsy Protocol Author Consultation Date Approved Urology Nurse Practioner PROTOCOL FOR MEN ATTENDING A ONE STOP PROSTATE BIOPSY CLINIC RATIONALE Prostate cancer is the most common cancer
Radiotherapy symptoms control in bone mets. Francesco Cellini GemelliART. Ernesto Maranzano,MD. Session 5: Symptoms management
 Session 5: Symptoms management Radiotherapy symptoms control in bone mets Francesco Cellini GemelliART Ernesto Maranzano,MD Director of Oncology Department Chief of Radiation Oncology Centre S. Maria Hospital
Session 5: Symptoms management Radiotherapy symptoms control in bone mets Francesco Cellini GemelliART Ernesto Maranzano,MD Director of Oncology Department Chief of Radiation Oncology Centre S. Maria Hospital