How a fully integrated Acute Oncology Service can benefit the busy medical unit
|
|
|
- Allen Crawford
- 6 years ago
- Views:
Transcription
1 How a fully integrated Acute Oncology Service can benefit the busy medical unit Dr. Pauline Leonard MD FRCP Consultant Medical Oncologist Whittington Health
2 Over the next 35 mins Briefly remind you of the evidence that led to the development of Acute Oncology services Describe the three types of Cancer emergencies To help define the importance of collaborative working Focus on one area that is under recognised Illustrate challenges with case presentations Interactive questions
 inappropriately")
3 NCEPOD % admitted during last 30 days 52% after #1 43% admitted with G3/4 toxicity 34% admitted General Medicine 21% treated were PS 3 or 4 15% admitted to another Trust 19% assessors felt Systemic Anti Cancer Therapy (SACT) inappropriately given
4 A key recommendation from National Chemotherapy Advisory Group (NCAG) report 2009 Development of an Acute Oncology Service in all Trusts which have an Emergency department for Management of patients who develop severe complications following chemo or as a consequence of their cancer Management of patients who present as emergencies with previously undiagnosed cancer AOS brings together expertise from oncology disciplines, emergency medicine, and general medicine and general surgery
5 Three types of Cancer emergencies Type 1 Patients who present who a new diagnosis of cancer Type 2 Patients who present with toxicities of treatment - Chemotherapy - Radiotherapy Type 3 Patients who present with symptoms from disease
6 What is the most common type of Cancer presentation? Type 1 ( new cancer diagnosis) Type 2 (treatment toxicity) For e.g. febrile neutropenia Type 3 ( disease related symptom) Pain, breathlessness
7 Our experience at WH Four not three types of patient presentations 53% of all patients who present to ED with a diagnosis of cancer have an unrelated problem Survivors of disease Living with disease but present Accident Exacerbation of co-morbidity New pathology Type 1 28% Type 2 22% Type 3a 50% 20% EOLC
8 Managing emergency presentations of Cancer on the Acute take
9 Routes to Diagnosis GP/OP referral Two Week Wait Emergency presentation Acute leukaemia 17% 3% 61% 12% 0% 4% 0% 4% 100% 380 Bladder 22% 36% 18% 13% 0% 6% 1% 5% 100% 1,167 Brain & CNS 18% 2% 49% 20% 0% 5% 0% 5% 100% 740 Breast 8% 40% 5% 5% 28% 2% 0% 13% 100% 5,646 Cervix 21% 17% 12% 8% 23% 3% 1% 15% 100% 308 Chronic leukaemia 26% 6% 45% 13% 0% 4% 1% 4% 100% 629 Colorectal 19% 29% 24% 12% 0% 8% 0% 7% 100% 4,515 Kidney 22% 26% 23% 16% 0% 5% 0% 8% 100% 928 Larynx 35% 34% 8% 14% 0% 5% 0% 3% 100% 216 Lung 15% 26% 38% 10% 0% 4% 1% 7% 100% 3,893 Melanoma 23% 39% 4% 8% 0% 5% 0% 22% 100% 1,686 Multiple myeloma 20% 14% 44% 13% 0% 4% 1% 5% 100% 606 Non-Hodgkin's lymphoma 25% 22% 25% 13% 0% 6% 1% 9% 100% 1,349 Oesophagus 15% 32% 21% 14% 0% 13% 0% 4% 100% 912 Oral 32% 27% 5% 14% 0% 4% 1% 17% 100% 458 Ovary 20% 29% 28% 11% 0% 3% 1% 8% 100% 853 Pancreas 13% 20% 45% 10% 0% 5% 1% 7% 100% 917 Prostate 26% 28% 11% 11% 0% 7% 0% 16% 100% 4,865 Stomach 14% 24% 31% 13% 0% 11% 1% 6% 100% 801 tbc (other) 21% 18% 34% 12% 0% 4% 1% 9% 100% 4,323 Testis 14% 47% 9% 15% 0% 4% 0% 11% 100% 259 Uterus 28% 36% 8% 12% 0% 5% 0% 12% 100% 918 Total 19% 28% 22% 11% 5% 5% 1% 10% 100% 36,369 Other outpatient Screen detected Inpatient elective DCO Unknown Total Number of patients All cancer Routes to Diagnosis: by cancer type All malignant registrations South West 2007 excluding C44 and multiples
 39.4 (32.9-45.8) 40.4 (29-51.5) EUROCARE Relative Survival Bladder 78.3 (74.6-81.5) 34.0 (27.3-40.8) 79.2 (73.")
10 Relative one year survival: by cancer type Malignant registrations, South West 2007, excluding multiples and DCOs Cancer type GP/OP referral (+TWW) Relative 95% CIs Survival Emergency Relative 95% CIs Survival Other route Relative 95% CIs Survival Acute leukaemia 39.7 ( ) 39.4 ( ) 40.4 ( ) EUROCARE Relative Survival Bladder 78.3 ( ) 34.0 ( ) 79.2 ( ) 85.3 Brain & CNS 68.4 ( ) 34.0 ( ) 60.6 ( ) 39.1 Breast 97.7 ( ) 50.8 ( ) 98.2 ( ) 95 Colorectal 84.5 ( ) 48.4 ( ) 79.5 ( ) 74.7 Kidney 81.1 ( ) 24.0 ( ) 72.4 ( ) 74.7 Lung 39.8 ( ) ) 32.4 ( ) 36.1 Multiple myeloma 83.6 ( ) 53.1 ( ) 73.0 ( ) 70.5 Non-Hodgkin's lymphoma 86.6 ( ) 43.7 ( ) 80.9 ( ) 73.1 Oesophagus 43.8 ( ) 22.4 ( ) 45.5 ( ) 36.3 Other 81.1 ( ) 27.2 ( ) 77.8 ( ) Ovary 83.4 ( ) 38.8 ( ) 72.1 ( ) 70.7 Pancreas 21.0 ( ) 6.0 ( ) 22.3 ( ) 19.2 Prostate 98.0 ( ) 48.2 ( ) 98.3 ( ) 92.2 Stomach 49.1 ( ) 17.7 ( ) 47.6 (41-54) 44.1


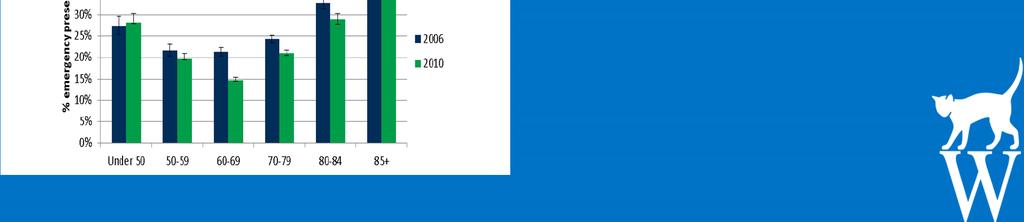
11 The older person is over represented in Emergency presentations of cancer

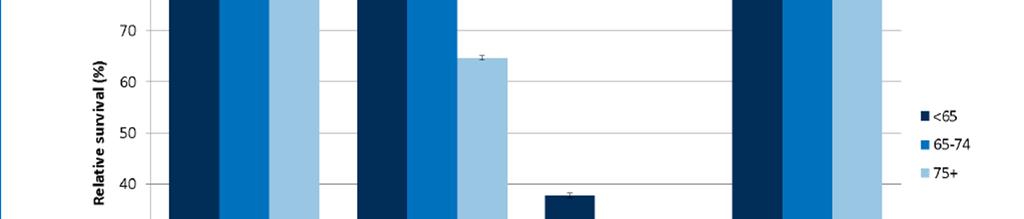
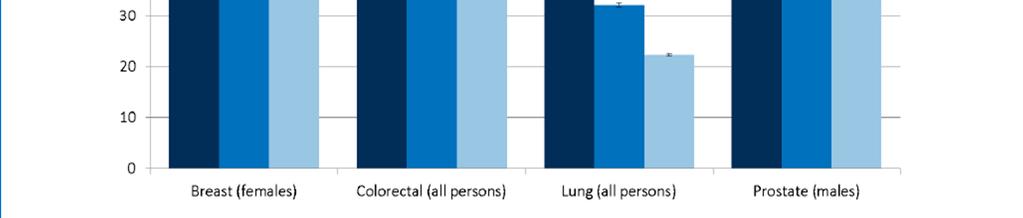
12 Survival decreases with age


13 Time to appreciate each others perspective by understanding the interpretation of specific assessment tools
14 Survival by Charslon Index at Diagnosis: All cases Kaplan-Meier; Charlson Index at diagnosis 1 y r analysis time CI=0 CI=2-3 CI=1 CI=4+ N=34,513 Courtesy: Anna Rich et al, Nottingham University
15 Prospective audit of emergency admissions of cancer Dec 2012 March 2013 Cancer New ED diagnoses Total Dec Feb Percentage of diagnoses by ED (Dec Feb) National figure for percentage of diagnoses by ED (06-08) Examples of CUP pathways which ensure early triage to specific tumour MDT Lung % 39% Pancreas % 50% Hepatobiliary + GB % 48% NHL % 27% Myeloma % 37% MUO % 37% Gynae % 15% Colorectal % 26% CNS % 62% AML % 54% Bone sarcoma % 25% H&N- Oropharynx % 9% Mesothelioma % 36% Oesophagus % 22% Stomach % 33% Prostate % 10%
16 Prospective audit of emergency admissions of cancer Dec 2012 March 2013 Cancer New ED diagnoses (RIP) Total Dec Feb Percentage of diagnoses by ED (Dec Feb) National figure for percentage of diagnoses by ED (06-08) Examples of CUP pathways which ensure early triage to specific tumour MDT Lung % 39% Pancreas % 50% Hepatobiliary + GB 3 (2) 5 60% 48% NHL % 27% Myeloma % 37% MUO % 37% Gynae % 15% Colorectal 2 (1) 14 14% 26% CNS % 62% AML 2 (1) 2 100% 54% Bone sarcoma % 25% H&N- Oropharynx % 9% Mesothelioma % 36% Oesophagus % 22% Stomach % 33% Prostate % 10%
17 Histological confirmation Treatment Frequency How many had histology? Radical chemo/radiotherapy 6 6 Potentially curative surgery 6 6 Palliative chemo/radiotherapy 10 9 Palliative surgery/ therapeutic intervention 2 1 Symptom control (75%) 33/44 patients had histological confirmation

18 MUO NICE guidance 2010
19 Why are clinicians reluctant to tailor investigations to the individual patient? Fear of missing the treatable? may not be cancer may have a better prognosis mutation positive cancer Belief that histological diagnosis a stronger determinant than prognosis determined by PS/comorbidities? Clinician discomfort with a clinical diagnosis Do something is easier than having an honest discussion about poor prognosis?
20 Role of Oncologist in AOS Sharing expertise in managing Oncological emergencies irrespective of tumour type Sub-specialisation has eroded confidence in generic skills Advisory capacity in how best to proceed in patients who present with a new suspected cancer Where case does not fit into recognised established pathways Individualised treatment plans incorporating PS & comorbidities
21 Managing emergency presentations of MUO/CUP
22 Routes to Diagnosis: Cancer unknown Primary 57% of all CUP/MUO present via ED Compared with 23% all cancers 45% were older than 85 years 4% under 50 yrs CUP accounts for 9% of all ED presenting cancers Compared to 23% Lung 11% CRC 1 year survival is 16% Better survival via managed routes 24-37%

23 Cerebral metastasis or primary brain cancer? Patient JM Patient AA
24 Which patient has a Primary Cerebral Lymphoma? Patient JM Patient AA Can t tell
25 What would you do next? Urgent referral to Neurosurgical unit Start high dose dexamethasone & refer to Neurosurgical unit Start high dexamethasone and request full staging CT Thorax, abdomen & Pelvis Start high dose Dexamethasone and request MRI head
26 Suggested next steps Assess patients fitness and wishes Trial 16mg dexamethasone stat then 8mg BD If keen and fit for treatment Needs full Thorax, Abdo & pelvis staging CT If no disseminated disease refer to neurosurgical centre or brain mets MDT Biopsy of brain mass Optimal surgical debulking

27 Metastatic Spinal cord compression 59yrs female Short history of weakness & loss of sensation right hand with pain in neck Contacted directly by MRI Vertebral collapse C7, T1,T2 & T3 with impending cord compression Organised by phone urgent RT & team approach Patient transferred UCLH and treated Post RT biopsy Metastatic breast ca
28 Suggested approach Clinical suspicion Assess PS, overall fitness and patients wishes If poor PS, multiple co-morbidities surgery will not be offered Give stat dose of Dexamethasone 16mg po with PPI cover Request WHOLE SPINE MRI Reserved 8am slot in MRI If previously undiagnosed cancer Needs full staging with CT Thorax/Abdo & Pelvis Known cancer Need to liaise with pt oncologist re: appropriateness Consider updated staging
29 When to transfer? Once all info collated needs local discussion with AOS and admitting team Prognosis Patient wishes Referapatient Neurosurgery Surgeons do not operate on MSCC out of hours operating times Prefer a stabilised patient Radiotherapy 7 day service

30 Liver metastases only How do we manage this case? -determine fitness -PS -renal & liver function -assess symptoms -explore wishes -Biopsy if chemo appropriate Unless management can be enhanced by addressing symptoms - There is no routine role for top & tail
31 No role for routine use of screening tumour markers Unless Suspected germ cell tumour AFP, bhcg, LDH Hepatocellular carcinoma AFP Equivocal Pancreatic mass** Ca 19.9 MSCC PSA Medullary cell thyroid carcinoma Serum Calcitonin

32 Superior venal caval obstruction 80 yrs Increasing SOB CT shows SVCO What about a diagnosis? First priority is patient safety and comfort?svc stent Steroids RT Biopsy confirmed adeno Lung EGFR WT
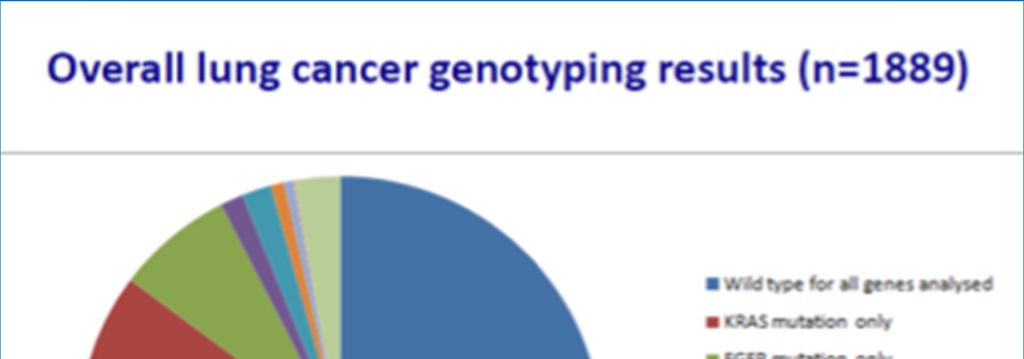

33 Stratified medicine project - CRUK 8.3%



34 Early AOS can improve experience of care yrs female 6m history back pain Abnormal x-ray reported & orthopaedic team alerted MRI pelvis & CT Thorax/Abdo done AOS involved Seen at RNOH Sarcoma MDT Prof no chemo RIP
35 Type 2 presentations
36 Toxicities of treatment Patient alerts Early recognition of emergency Specialist management Assess to agreed pathways of care Updated easy accessible protocols Sepsis 6 Regular education Shared knowledge Recognition of newer treatments
37 Type 3 presentations
38 Symptoms of disease Manage symptom Investigate appropriately Understand ceilings of care Early involvement of palliative care services


39 AOS meets Acute Medical take - celebrating our shared expertise
40 Take home messages AOS brings together expertise from oncology disciplines, emergency medicine, and general medicine, care of the elderly, palliative care and general surgery The way we have previously done things needs to be challenged Integrated working (when done well) can Provide a better experience of care Ensure patient centred pathways Improve outcomes and avoid potentially avoidable co-morbidity and death Provide educational opportunities Embed value based care


41 Whittington Health AOS? Adam Belton CNS Haem/AOS Dr Ali Rismani Haem /AOS Cons Dr Pauline Leonard AOS Lead Medical Oncologist Lung/GI/HPB & CUP Dr Emma Spurrell Consultant Medical Oncologist Breast/AOS Dr Mulyati Mohamed Speciality Dr Oncology
How an Acute Oncology service can help with managing Cancer of unknown primary
 How an Acute Oncology service can help with managing Cancer of unknown primary Dr Pauline Leonard MD FRCP Consultant Medical Oncologist Lead Cancer Clinician Whittington Health Definitions Patients who
How an Acute Oncology service can help with managing Cancer of unknown primary Dr Pauline Leonard MD FRCP Consultant Medical Oncologist Lead Cancer Clinician Whittington Health Definitions Patients who
Lessons learnt from establishing an Acute Oncology service. Dr. Pauline Leonard MD FRCP Consultant Medical Oncologist Whittington Health
 Lessons learnt from establishing an Acute Oncology service Dr. Pauline Leonard MD FRCP Consultant Medical Oncologist Whittington Health Over next 45 minutes.. Lessons learnt from: setting up a new service
Lessons learnt from establishing an Acute Oncology service Dr. Pauline Leonard MD FRCP Consultant Medical Oncologist Whittington Health Over next 45 minutes.. Lessons learnt from: setting up a new service
Cancer of Unknown Primary (CUP) Protocol
 Protocol") 1 Department of Oncology. Cancer of Unknown Primary (CUP) Protocol Version: Document type: Document sponsor Designation Document author [ s] Designation[s] Approving committee / Group Ratified by: Date
1 Department of Oncology. Cancer of Unknown Primary (CUP) Protocol Version: Document type: Document sponsor Designation Document author [ s] Designation[s] Approving committee / Group Ratified by: Date
Identifying and counting people living with treatable but not curable cancer
 Identifying and counting people living with treatable but not curable cancer Rachel White Joanna Pethick, Archie Macnair, Gregory Fallica, Jennifer Than and Jane Maher September 2018 Who are the people
Identifying and counting people living with treatable but not curable cancer Rachel White Joanna Pethick, Archie Macnair, Gregory Fallica, Jennifer Than and Jane Maher September 2018 Who are the people
North of Scotland Cancer Network Clinical Management Guideline for Metastatic Malignancy of Undefined Primary Origin (MUO)
") North of Scotland Cancer Network Clinical Management Guideline for Metastatic Malignancy of Undefined Primary Origin (MUO) UNCONTROLLED WHEN PRINTED DOCUMENT CONTROL Original Prepared by NMcL April 2016
North of Scotland Cancer Network Clinical Management Guideline for Metastatic Malignancy of Undefined Primary Origin (MUO) UNCONTROLLED WHEN PRINTED DOCUMENT CONTROL Original Prepared by NMcL April 2016
Cancer of Unknown Primary (CUP)
") Cancer of Unknown Primary (CUP) Pathways and Guidelines V1.0 London Cancer September 2013 The following pathways and guidelines document has been compiled by the London Cancer CUP technical subgroup and
Cancer of Unknown Primary (CUP) Pathways and Guidelines V1.0 London Cancer September 2013 The following pathways and guidelines document has been compiled by the London Cancer CUP technical subgroup and
MSCC CARE PATHWAYS & CASE STUDIES. By Michael Balloch Spine CNS
 MSCC CARE PATHWAYS & CASE STUDIES By Michael Balloch Spine CNS Aims To be familiar with the routes of MSCC prentaion How the guidelines work in practice Routes of presentation Generic intervention Managing
MSCC CARE PATHWAYS & CASE STUDIES By Michael Balloch Spine CNS Aims To be familiar with the routes of MSCC prentaion How the guidelines work in practice Routes of presentation Generic intervention Managing
Cancer of Unknown Primary Service
 Cancer of Unknown Primary Service Dr Maurice Fernando Consultant In Specialist Palliative Care and CUP lead Doncaster and Bassetlaw Hospitals NHS FT Wakefield meeting -14-07-2016 CUP service CUP MDT
Cancer of Unknown Primary Service Dr Maurice Fernando Consultant In Specialist Palliative Care and CUP lead Doncaster and Bassetlaw Hospitals NHS FT Wakefield meeting -14-07-2016 CUP service CUP MDT
Unknown Primary Service for patients at Chesterfield Royal Hospital
 Unknown Primary Service for patients at Chesterfield Royal Hospital David Brooks Macmillan Consultant in Palliative Medicine Louise Merriman GP Cancer Lead With thanks to Macmillan Cancer Support, who
Unknown Primary Service for patients at Chesterfield Royal Hospital David Brooks Macmillan Consultant in Palliative Medicine Louise Merriman GP Cancer Lead With thanks to Macmillan Cancer Support, who
Update on Management of Malignant Spinal Cord Compression. Heino Hugel Consultant in Palliative Medicine University Hospital Aintree
 Update on Management of Malignant Spinal Cord Compression Heino Hugel Consultant in Palliative Medicine University Hospital Aintree Current Guidelines The symptoms of MSCC may be subtle and therefore careful
Update on Management of Malignant Spinal Cord Compression Heino Hugel Consultant in Palliative Medicine University Hospital Aintree Current Guidelines The symptoms of MSCC may be subtle and therefore careful
PATHWAY MANAGEMENT OF METASTATIC SPINAL CORD COMPRESSION (MSCC) THE CHRISTIE, GREATER MANCHESTER & CHESHIRE
 THE CHRISTIE, GREATER MANCHESTER & CHESHIRE") PATHWAY MANAGEMENT OF METASTATIC SPINAL CORD COMPRESSION (MSCC) THE CHRISTIE, GREATER MANCHESTER & CHESHIRE Procedure Reference: Document Owner: Dr V. Misra Version: Accountable Committee: V3 MSCC Network
PATHWAY MANAGEMENT OF METASTATIC SPINAL CORD COMPRESSION (MSCC) THE CHRISTIE, GREATER MANCHESTER & CHESHIRE Procedure Reference: Document Owner: Dr V. Misra Version: Accountable Committee: V3 MSCC Network
Acute Oncology: Service Provision in Smaller Cancer Centres Ernie Marshall Clatterbridge Centre for Oncology
 Acute Oncology: Service Provision in Smaller Cancer Centres Ernie Marshall Clatterbridge Centre for Oncology Whiston Hospital St Helen s Hospital 350,000 population ~1000 beds Regional Plastics Unit DGH
Acute Oncology: Service Provision in Smaller Cancer Centres Ernie Marshall Clatterbridge Centre for Oncology Whiston Hospital St Helen s Hospital 350,000 population ~1000 beds Regional Plastics Unit DGH
Acute Oncology Martin Eatock Consultant Medical Oncologist NICaN Medical Director
 Acute Oncology 2014 Martin Eatock Consultant Medical Oncologist NICaN Medical Director Patients admitted with cancer have a longer than average stay Berger et al. Clin Medicine (2013) Questions If your
Acute Oncology 2014 Martin Eatock Consultant Medical Oncologist NICaN Medical Director Patients admitted with cancer have a longer than average stay Berger et al. Clin Medicine (2013) Questions If your
Recognition & Treatment of Malignant Spinal Cord Compression Study Day
 Recognition & Treatment of Malignant Spinal Cord Compression Study Day 11 th May 2017 Dr Bernie Foran Consultant Clinical Oncologist & Honorary Senior Lecturer Weston Park Hospital Outline of Talk Clinical
Recognition & Treatment of Malignant Spinal Cord Compression Study Day 11 th May 2017 Dr Bernie Foran Consultant Clinical Oncologist & Honorary Senior Lecturer Weston Park Hospital Outline of Talk Clinical
What is Acute Oncology? Kay McCallum Acute Oncology Advanced Nurse Practitioner John Radcliffe Hospital Oxford September 2015
 What is Acute Oncology? Kay McCallum Acute Oncology Advanced Nurse Practitioner John Radcliffe Hospital Oxford September 2015 What is Acute Oncology? Outline of Talk Concept of Acute Oncology Service (AOS)
What is Acute Oncology? Kay McCallum Acute Oncology Advanced Nurse Practitioner John Radcliffe Hospital Oxford September 2015 What is Acute Oncology? Outline of Talk Concept of Acute Oncology Service (AOS)
Metastatic Spinal Disease
 Metastatic Spinal Disease Mr Neil Chiverton Consultant Spinal Surgeon, Sheffield Objectives The scale and nature of the problem NICE recommendations Surgical decision making Case illustrations Incidence
Metastatic Spinal Disease Mr Neil Chiverton Consultant Spinal Surgeon, Sheffield Objectives The scale and nature of the problem NICE recommendations Surgical decision making Case illustrations Incidence
Clinical indications for positron emission tomography
 Clinical indications for positron emission tomography Oncology applications Brain and spinal cord Parotid Suspected tumour recurrence when anatomical imaging is difficult or equivocal and management will
Clinical indications for positron emission tomography Oncology applications Brain and spinal cord Parotid Suspected tumour recurrence when anatomical imaging is difficult or equivocal and management will
COSD & Source of Referral
 COSD & Source of Referral A Brief guide October 2014 Michael Sharpe Data Improvement Manager National Cancer Registration Service What is COSD? Cancer and Outcomes Services Dataset Clinical dataset for
COSD & Source of Referral A Brief guide October 2014 Michael Sharpe Data Improvement Manager National Cancer Registration Service What is COSD? Cancer and Outcomes Services Dataset Clinical dataset for
PATHWAY FOR INVESTIGATION OF ADULTS PRESENTING WITH ASCITES. U/S Abdo/pelvis shows ascites without obvious evidence of 1 liver disease
 PATHWAY FOR INVESTIGATION OF ADULTS PRESENTING WITH ASCITES U/S Abdo/pelvis shows ascites without obvious evidence of 1 liver disease Refer back to original requester with this paperwork and review previous
PATHWAY FOR INVESTIGATION OF ADULTS PRESENTING WITH ASCITES U/S Abdo/pelvis shows ascites without obvious evidence of 1 liver disease Refer back to original requester with this paperwork and review previous
Acute Oncology Services Clinical Forum: Metastatic Spinal Cord Compression. Tuesday 17 th September 2013
 Acute Oncology Services Clinical Forum: Metastatic Spinal Cord Compression Tuesday 17 th September 2013 Welcome, Introduction and Aims of the Event Dr Tom Newsom-Davis, LCA AOS Pathway Chair Why MSCC?
Acute Oncology Services Clinical Forum: Metastatic Spinal Cord Compression Tuesday 17 th September 2013 Welcome, Introduction and Aims of the Event Dr Tom Newsom-Davis, LCA AOS Pathway Chair Why MSCC?
National Standards for Acute Oncology Services
 Cancer National Specialist Advisory Group National Standards for Acute Oncology Services June 2016 TABLE OF CONTENTS 1. PURPOSE... 2 2. INTRODUCTION... 2 3. STRATEGIC CONTEXT... 4 4. SCOPE OF ACUTE ONCOLOGY
Cancer National Specialist Advisory Group National Standards for Acute Oncology Services June 2016 TABLE OF CONTENTS 1. PURPOSE... 2 2. INTRODUCTION... 2 3. STRATEGIC CONTEXT... 4 4. SCOPE OF ACUTE ONCOLOGY
Palliative care - the opportunities. Dr David Brooks Macmillan Consultant in Palliative Medicine Chesterfield Royal Hospital
 Palliative care - the opportunities Dr David Brooks Macmillan Consultant in Palliative Medicine Chesterfield Royal Hospital Our Commitment to you for end of life care The Government Response to the
Palliative care - the opportunities Dr David Brooks Macmillan Consultant in Palliative Medicine Chesterfield Royal Hospital Our Commitment to you for end of life care The Government Response to the
Oncologic Emergencies: When to call the Radiation Oncologist
 Oncologic Emergencies: When to call the Radiation Oncologist Dr. Shrinivas Rathod Radiation Oncologist Radiation Oncology Program CancerCare Manitoba and University of Manitoba Disclosures Speaker s name:
Oncologic Emergencies: When to call the Radiation Oncologist Dr. Shrinivas Rathod Radiation Oncologist Radiation Oncology Program CancerCare Manitoba and University of Manitoba Disclosures Speaker s name:
CUP Investigation and Management Guidelines V1 West Midlands SCN Acute Oncology, MSCC and CUP ERG /PJJ/
 Policy and Guidelines for the Investigation, Diagnosis and management of Patients with malignancy of an Unknown Origin (MUO) and Cancer of an Unknown Primary (CUP) 1 West Midlands Clinical Networks and
Policy and Guidelines for the Investigation, Diagnosis and management of Patients with malignancy of an Unknown Origin (MUO) and Cancer of an Unknown Primary (CUP) 1 West Midlands Clinical Networks and
SOUTH THAMES CHILDREN S CANCER NETWORK GROUP. REFERRAL PROTOCOLS AND DIAGNOSIS AND STAGING PROTOCOLS October 2014
 SOUTH THAMES CHILDREN S CANCER NETWORK GROUP REFERRAL PROTOCOLS AND DIAGNOSIS AND STAGING PROTOCOLS October 2014 Contents 1. Leukaemia Referral, Diagnostic and Staging Guidelines 2. Lymphoma Referral,
SOUTH THAMES CHILDREN S CANCER NETWORK GROUP REFERRAL PROTOCOLS AND DIAGNOSIS AND STAGING PROTOCOLS October 2014 Contents 1. Leukaemia Referral, Diagnostic and Staging Guidelines 2. Lymphoma Referral,
Referral guide for acute oncology emergencies
 Referral guide for acute oncology emergencies 1 st Edition v 1.0 London Cancer March 2013 To be used in conjunction with London Cancer clinical guidelines for acute oncology emergencies; A Guide to Acute
Referral guide for acute oncology emergencies 1 st Edition v 1.0 London Cancer March 2013 To be used in conjunction with London Cancer clinical guidelines for acute oncology emergencies; A Guide to Acute
Palliative Care Emergencies
 Palliative Care Emergencies LAURA BARNFIELD What might constitute an emergency in Palliative Care? 1 Palliative Care Emergencies Major haemorrhage Metastatic Spinal Cord Compression (MSCC) Superior Vena
Palliative Care Emergencies LAURA BARNFIELD What might constitute an emergency in Palliative Care? 1 Palliative Care Emergencies Major haemorrhage Metastatic Spinal Cord Compression (MSCC) Superior Vena
Cancer and Data in the New NHS May Di Riley, Director Clinical Outcomes
 Cancer and Data in the New NHS May 2011 Di Riley, Director Clinical Outcomes Overarching NHS context Financial constraints White Paper GP Commissioning/Commissioning Board Public Health England National
Cancer and Data in the New NHS May 2011 Di Riley, Director Clinical Outcomes Overarching NHS context Financial constraints White Paper GP Commissioning/Commissioning Board Public Health England National
Somerset, Wiltshire, Avon and Gloucestershire (SWAG) Cancer Services. Cancer of Unknown Primary Network Site Specific Group. Clinical Guidelines
 Cancer Services. Cancer of Unknown Primary Network Site Specific Group. Clinical Guidelines") Somerset, Wiltshire, Avon and Gloucestershire (SWAG) Cancer Services Cancer of Unknown Primary Network Site Specific Group Revision due: April 2019 Page 1 of 11 VERSION CONTROL THIS IS A CONTROLLED DOCUMENT.
Somerset, Wiltshire, Avon and Gloucestershire (SWAG) Cancer Services Cancer of Unknown Primary Network Site Specific Group Revision due: April 2019 Page 1 of 11 VERSION CONTROL THIS IS A CONTROLLED DOCUMENT.
Metastatic Spinal Cord Compression (MSCC) Clinical guidelines and pathway
 Clinical guidelines and pathway") Metastatic Spinal Cord Compression (MSCC) Clinical guidelines and pathway Version 2: May 2012 To be read in conjunction with NICE CG75 Developed by consensus by: Dr Peter Robson, Consultant Oncologist,
Metastatic Spinal Cord Compression (MSCC) Clinical guidelines and pathway Version 2: May 2012 To be read in conjunction with NICE CG75 Developed by consensus by: Dr Peter Robson, Consultant Oncologist,
MANAGEMENT OF PATIENTS WITH METASTATIC SPINAL CORD COMPRESSION
 CLINICAL POLICY MANAGEMENT OF PATIENTS WITH METASTATIC SPINAL CORD COMPRESSION DOCUMENT REF: PCLASCORD (Version No. 1.4) Name and designation of policy author(s) Approved by (committee, group, manager)
CLINICAL POLICY MANAGEMENT OF PATIENTS WITH METASTATIC SPINAL CORD COMPRESSION DOCUMENT REF: PCLASCORD (Version No. 1.4) Name and designation of policy author(s) Approved by (committee, group, manager)
DEPARTMENT OF ONCOLOGY ELECTIVE
 DEPARTMENT OF ONCOLOGY ELECTIVE 2015-2016 www.uwo.ca/oncology Oncology Elective Program Administrator: Ms. Kimberly Trudgeon Room A4-901C (Admin) LHSC London Regional Cancer Centre (Victoria Campus) Phone:
DEPARTMENT OF ONCOLOGY ELECTIVE 2015-2016 www.uwo.ca/oncology Oncology Elective Program Administrator: Ms. Kimberly Trudgeon Room A4-901C (Admin) LHSC London Regional Cancer Centre (Victoria Campus) Phone:
How can we facilitate cross-boundary working in Greater Manchester?
 How can we facilitate cross-boundary working in Greater Manchester? Emma Halkyard Nurse Clinician Cross boundary working: where are we now? Our patients are complex Our pathways are complex Our treatments
How can we facilitate cross-boundary working in Greater Manchester? Emma Halkyard Nurse Clinician Cross boundary working: where are we now? Our patients are complex Our pathways are complex Our treatments
Disclosures. Disclosures 27/01/2019. Modern approach and pitfalls in metastatic spine surgery. None.. Jeremy Reynolds
 Modern approach and pitfalls in metastatic spine surgery Jeremy Reynolds Spine Lead Oxford Bone and Soft Tissue Sarcoma Service MSCC Lead Thames Valley Cancer Network Clinical Lead Oxford Spine 1 Disclosures
Modern approach and pitfalls in metastatic spine surgery Jeremy Reynolds Spine Lead Oxford Bone and Soft Tissue Sarcoma Service MSCC Lead Thames Valley Cancer Network Clinical Lead Oxford Spine 1 Disclosures
Guidelines for the Management of Prostate Cancer West Midlands Expert Advisory Group for Urological Cancer
 Guidelines for the Management of Prostate Cancer West Midlands Expert Advisory Group for Urological Cancer West Midlands Clinical Networks and Clinical Senate Coversheet for Network Expert Advisory Group
Guidelines for the Management of Prostate Cancer West Midlands Expert Advisory Group for Urological Cancer West Midlands Clinical Networks and Clinical Senate Coversheet for Network Expert Advisory Group
Supplementary Online Content
 Supplementary Online Content Henson KE, Brock R, Charnock J, Wickramasinghe B, Will O, Pitman A. Risk of suicide after cancer diagnosis in England. JAMA Psychiatry. Published online November 21, 2018.
Supplementary Online Content Henson KE, Brock R, Charnock J, Wickramasinghe B, Will O, Pitman A. Risk of suicide after cancer diagnosis in England. JAMA Psychiatry. Published online November 21, 2018.
GUIDELINES FOR RADIOTHERAPY IN SPINAL CORD COMPRESSION THE CHRISTIE, GREATER MANCHESTER & CHESHIRE. Version:
 GUIDELINES FOR RADIOTHERAPY IN SPINAL CORD COMPRESSION THE CHRISTIE, GREATER MANCHESTER & CHESHIRE Procedure Reference: Document Owner: Dr V. Misra Version: Accountable Committee: V4 Acute Oncology Group
GUIDELINES FOR RADIOTHERAPY IN SPINAL CORD COMPRESSION THE CHRISTIE, GREATER MANCHESTER & CHESHIRE Procedure Reference: Document Owner: Dr V. Misra Version: Accountable Committee: V4 Acute Oncology Group
National Optimal Lung Cancer Pathways. Dr Sadia Anwar Nottingham University Hospitals NHS Trust Clinical Lead for Lung Cancer
 National Optimal Lung Cancer Pathways Dr Sadia Anwar ttingham University Hospitals NHS Trust Clinical Lead for Lung Cancer Overview How NOLCP evolved How it relates to national guidance Pathways Implementation
National Optimal Lung Cancer Pathways Dr Sadia Anwar ttingham University Hospitals NHS Trust Clinical Lead for Lung Cancer Overview How NOLCP evolved How it relates to national guidance Pathways Implementation
Faster Cancer Treatment Indicators: Use cases
 Faster Cancer Treatment Indicators: Use cases 2014 Date: October 2014 Version: Owner: Status: v01 Ministry of Health Cancer Services Final Citation: Ministry of Health. 2014. Faster Cancer Treatment Indicators:
Faster Cancer Treatment Indicators: Use cases 2014 Date: October 2014 Version: Owner: Status: v01 Ministry of Health Cancer Services Final Citation: Ministry of Health. 2014. Faster Cancer Treatment Indicators:
MDT IMPROVEMENT PROJECT. Professor Muntzer Mughal, UCLH
 MDT IMPROVEMENT PROJECT Professor Muntzer Mughal, UCLH 1995..assessment and management of rare cancers in multidisciplinary teams.. 2000 the care of all patients with cancer should be formally reviewed
MDT IMPROVEMENT PROJECT Professor Muntzer Mughal, UCLH 1995..assessment and management of rare cancers in multidisciplinary teams.. 2000 the care of all patients with cancer should be formally reviewed
National Cancer Registration and Analysis Service Short Report: Chemotherapy, Radiotherapy and Surgical Tumour Resections in England: (V2)
") National Cancer Registration and Analysis Service Short Report: Chemotherapy, Radiotherapy and Surgical Tumour Resections in England: 13-14 (V2) Produced as part of the Cancer Research UK - Public Health
National Cancer Registration and Analysis Service Short Report: Chemotherapy, Radiotherapy and Surgical Tumour Resections in England: 13-14 (V2) Produced as part of the Cancer Research UK - Public Health
Information Services Division NHS National Services Scotland
 Cancer in Scotland October 2012 First published in June 2004, revised with each National Statistics publication Next due for revision April 2013 Information Services Division NHS National Services Scotland
Cancer in Scotland October 2012 First published in June 2004, revised with each National Statistics publication Next due for revision April 2013 Information Services Division NHS National Services Scotland
Bladder Cancer Guidelines
 Bladder Cancer Guidelines Agreed by Urology CSG: October 2011 Review Date: September 2013 Bladder Cancer 1. Referral Guidelines The following patients should be considered as potentially having bladder
Bladder Cancer Guidelines Agreed by Urology CSG: October 2011 Review Date: September 2013 Bladder Cancer 1. Referral Guidelines The following patients should be considered as potentially having bladder
Aviva Group Protection Our guide to cancer
 ww For employers use only. Aviva Group Protection Our guide to cancer 1 2 In 2013, 131 million working days were lost due to sickness absence in the UK, at an average of 4.4 working days per employee 1.
ww For employers use only. Aviva Group Protection Our guide to cancer 1 2 In 2013, 131 million working days were lost due to sickness absence in the UK, at an average of 4.4 working days per employee 1.
Dr Hilary Williams. Consultant in Medical Oncology at Velindre Cancer Centre
 Dr Hilary Williams. Consultant in Medical Oncology at Velindre Cancer Centre Hilary.williams4@wales.nhs.uk Thinking about Acute Oncology. Why do we need acute oncology locally? What the Hub VCC provides
Dr Hilary Williams. Consultant in Medical Oncology at Velindre Cancer Centre Hilary.williams4@wales.nhs.uk Thinking about Acute Oncology. Why do we need acute oncology locally? What the Hub VCC provides
Macmillan Publications
 S1 S2 S3 S3 S3 S4 S5 S6 S7 S8 S8 S9 S10 S11 S11 S12 S13 S14 S15 S17 S18 S19 Bladder Cancer: Non-Invasive, Invasive and Advanced Bone Cancer: Primary, Secondary Colon Cancer, Anal Cancer, Rectal Cancer
S1 S2 S3 S3 S3 S4 S5 S6 S7 S8 S8 S9 S10 S11 S11 S12 S13 S14 S15 S17 S18 S19 Bladder Cancer: Non-Invasive, Invasive and Advanced Bone Cancer: Primary, Secondary Colon Cancer, Anal Cancer, Rectal Cancer
National Cancer Intelligence Network short report
 National Cancer Intelligence Network short report Produced in partnership with Cancer Research UK Version 2.0 - reissued June 2015 Cancer survival in the UK is lower than in many comparable countries.
National Cancer Intelligence Network short report Produced in partnership with Cancer Research UK Version 2.0 - reissued June 2015 Cancer survival in the UK is lower than in many comparable countries.
National Update: Living With and Beyond Cancer Implementing Strategic Priority 4 of the National Cancer Taskforce
 National Update: Living With and Beyond Cancer Implementing Strategic Priority 4 of the National Cancer Taskforce Duleep Allirajah Head of Policy, Macmillan Cancer Support Total Prevalence - now Total
National Update: Living With and Beyond Cancer Implementing Strategic Priority 4 of the National Cancer Taskforce Duleep Allirajah Head of Policy, Macmillan Cancer Support Total Prevalence - now Total
CP80 Version: V01. Acute Oncology Management Service Date approved: 8 th May 2015 Date ratified: 1 st June 2015 Review date: 1 st June 2017
 STANDARD OPERATING PROCEDURE (SOP) AND PATHWAY FOR THE MANAGEMENT OF PATIENTS WITH METASTATIC SPINAL CORD COMPRESSION (MSCC) WITHIN THE CHRISTIE (Refer to the Manchester Cancer Network MSCC Pathway flowchart)
STANDARD OPERATING PROCEDURE (SOP) AND PATHWAY FOR THE MANAGEMENT OF PATIENTS WITH METASTATIC SPINAL CORD COMPRESSION (MSCC) WITHIN THE CHRISTIE (Refer to the Manchester Cancer Network MSCC Pathway flowchart)
A research briefing paper by Macmillan Cancer Support
 A research briefing paper by Macmillan Cancer Support Introduction Key findings 3 People with cancer are surviving longer 4 Median survival time has seen dramatic improvement for some cancers 5 Median
A research briefing paper by Macmillan Cancer Support Introduction Key findings 3 People with cancer are surviving longer 4 Median survival time has seen dramatic improvement for some cancers 5 Median
Clinical Biochemistry Department City Hospital
 Cancer Biochemistry and Tumour Markers Clinical Biochemistry Department City Hospital In this lecture Cancer basics Definition of Tumour Marker (TM) What is the perfect TM? History of TMs Examples of TMs
Cancer Biochemistry and Tumour Markers Clinical Biochemistry Department City Hospital In this lecture Cancer basics Definition of Tumour Marker (TM) What is the perfect TM? History of TMs Examples of TMs
Information Services Division NHS National Services Scotland
 Cancer in Scotland April 2013 First published in June 2004, revised with each National Statistics publication Next due for revision October 2013 Information Services Division NHS National Services Scotland
Cancer in Scotland April 2013 First published in June 2004, revised with each National Statistics publication Next due for revision October 2013 Information Services Division NHS National Services Scotland
Cancer Association of South Africa (CANSA) Fact Sheet on the Top Ten Cancers per Population Group
 Fact Sheet on the Top Ten Cancers per Population Group") Cancer Association of South Africa (CANSA) Fact Sheet on the Top Ten Cancers per Population Group Introduction There are more than 200 different types of cancer. It is also referred to as malignancies,
Cancer Association of South Africa (CANSA) Fact Sheet on the Top Ten Cancers per Population Group Introduction There are more than 200 different types of cancer. It is also referred to as malignancies,
Epidemiology, aetiology and the patient pathway in oesophageal and pancreatic cancers
 Epidemiology, aetiology and the patient pathway in oesophageal and pancreatic cancers Dr Ian Chau Consultant Medical Oncologist Women's cancers Breast cancer introduction 3 What profession are you in?
Epidemiology, aetiology and the patient pathway in oesophageal and pancreatic cancers Dr Ian Chau Consultant Medical Oncologist Women's cancers Breast cancer introduction 3 What profession are you in?
PROSTATE CANCER STRATIFIED FOLLOW UP. Hilary Baker Lead CNS for Uro-oncology MSc, BSc, RGN.
 PROSTATE CANCER STRATIFIED FOLLOW UP Hilary Baker Lead CNS for Uro-oncology MSc, BSc, RGN. LEARNING OBJECTIVES To refresh your knowledge about prostate cancer. To discuss the purpose and patient benefits
PROSTATE CANCER STRATIFIED FOLLOW UP Hilary Baker Lead CNS for Uro-oncology MSc, BSc, RGN. LEARNING OBJECTIVES To refresh your knowledge about prostate cancer. To discuss the purpose and patient benefits
Outcomes Report: Accountability Measures and Quality Improvements
 Outcomes Report: Accountability Measures and Quality Improvements The FH Memorial Medical Center s Cancer Committee ensures that patients with cancer are treated according to the nationally accepted measures.
Outcomes Report: Accountability Measures and Quality Improvements The FH Memorial Medical Center s Cancer Committee ensures that patients with cancer are treated according to the nationally accepted measures.
LCA Lung Clinical Forum. 21 st October 2014
 LCA Lung Clinical Forum 21 st October 2014 Welcome Dr Liz Sawicka Chair - LCA Lung Pathway Group Succession planning Dr Kate Haire Consultant in Public Health Medicine, LCA Commissioning Intentions for
LCA Lung Clinical Forum 21 st October 2014 Welcome Dr Liz Sawicka Chair - LCA Lung Pathway Group Succession planning Dr Kate Haire Consultant in Public Health Medicine, LCA Commissioning Intentions for
North of Scotland Cancer Network: Horizon Scanning Report for NoSPG Peter Gent & Mr Peter King North of Scotland Cancer Network
 North of Scotland Cancer Network: Horizon Scanning Report for NoSPG Peter Gent & Mr Peter King North of Scotland Cancer Network Introduction Cancer Incidence & Projected Trends National ISD reported that
North of Scotland Cancer Network: Horizon Scanning Report for NoSPG Peter Gent & Mr Peter King North of Scotland Cancer Network Introduction Cancer Incidence & Projected Trends National ISD reported that
NCIN Conference Feedback 2015
 NCIN Conference Feedback 2015 Parallel Sessions Treatments (Black type is the topic; blue type are comments) The use of population and research data in the development of guidelines for cancer treatment
NCIN Conference Feedback 2015 Parallel Sessions Treatments (Black type is the topic; blue type are comments) The use of population and research data in the development of guidelines for cancer treatment
Cancer of Unknown Primary
 Cancer of Unknown Primary Helen Rickards Acute Oncology and Cancer of Unknown Primary CNS 18 th May 2017 Defining CUP Incidence Patient Pathways getting a diagnosis Patient assessment The patient s perspective
Cancer of Unknown Primary Helen Rickards Acute Oncology and Cancer of Unknown Primary CNS 18 th May 2017 Defining CUP Incidence Patient Pathways getting a diagnosis Patient assessment The patient s perspective
Decision Making Flowchart for Metastatic Spinal Cord Compression and Pathological Spinal Fractures
 Decision Making Flowchart for Metastatic Spinal Cord Compression and Pathological Spinal Fractures All Referrals (see notes): Spinal Surgeons Locally or Trauma SpR at UHW Oncology SpR at Velindre / Singleton
Decision Making Flowchart for Metastatic Spinal Cord Compression and Pathological Spinal Fractures All Referrals (see notes): Spinal Surgeons Locally or Trauma SpR at UHW Oncology SpR at Velindre / Singleton
Guidelines for the Management. Malignant Spinal Cord Compression. Final Guideline
 Guidelines for the Management Of Malignant Spinal Cord Compression Final Guideline 1. Introduction 1.1 Aetiology of MSCC 1.2 Use of the guidelines 2. Summary of Pathway 2.1 Algorithms 2.2 Role of the MSCC
Guidelines for the Management Of Malignant Spinal Cord Compression Final Guideline 1. Introduction 1.1 Aetiology of MSCC 1.2 Use of the guidelines 2. Summary of Pathway 2.1 Algorithms 2.2 Role of the MSCC
Upper GI Malignancies Imaging Guidelines for the Management of Gastric, Oesophageal & Pancreatic Cancers 2012
 Upper GI Malignancies Imaging Guidelines for the Management of Gastric, Oesophageal & Pancreatic Cancers 2012 Version Control This is a controlled document please destroy all previous versions on receipt
Upper GI Malignancies Imaging Guidelines for the Management of Gastric, Oesophageal & Pancreatic Cancers 2012 Version Control This is a controlled document please destroy all previous versions on receipt
Manchester Cancer Colorectal Pathway Board: Guidelines for management of colorectal hepatic metastases
 Manchester Cancer Colorectal Pathway Board: Guidelines for management of colorectal hepatic metastases Date: April 2015 Date for review: April 2018 1. Principles The recognised specialist HPB MDT for Greater
Manchester Cancer Colorectal Pathway Board: Guidelines for management of colorectal hepatic metastases Date: April 2015 Date for review: April 2018 1. Principles The recognised specialist HPB MDT for Greater
Work Programme/Service Delivery Plan 2010/2013
 Essex and East Suffolk Gynaecological Cancer Network Site Specific Group Work Programme/Service Delivery Plan 2010/2013 Version Number 1.2 Author Members of the NSSG Date Written June 2010 Reviewed May
Essex and East Suffolk Gynaecological Cancer Network Site Specific Group Work Programme/Service Delivery Plan 2010/2013 Version Number 1.2 Author Members of the NSSG Date Written June 2010 Reviewed May
Cancer Association of South Africa (CANSA) Fact Sheet on the Top Ten Cancers per Population Group
 Fact Sheet on the Top Ten Cancers per Population Group") Cancer Association of South Africa (CANSA) Fact Sheet on the Top Ten Cancers per Population Group Introduction There are more than 200 different types of cancer. It is also referred to as malignancies,
Cancer Association of South Africa (CANSA) Fact Sheet on the Top Ten Cancers per Population Group Introduction There are more than 200 different types of cancer. It is also referred to as malignancies,
Tumour Markers. For these reasons, only a handful of tumour markers are commonly used by most doctors.
 Tumour Markers What are Tumour Markers? Tumour markers are substances that can be found in the body when cancer is present. They are usually found in the blood or urine. They can be products of cancer
Tumour Markers What are Tumour Markers? Tumour markers are substances that can be found in the body when cancer is present. They are usually found in the blood or urine. They can be products of cancer
Cancer in the South West Peninsula - a baseline assessment
 Cancer in the South West Peninsula - a baseline assessment 1 The Cancer Reform Strategy 1.1 The Cancer Reform Strategy, published in December 2007 1, built on the progress already achieved since the publication
Cancer in the South West Peninsula - a baseline assessment 1 The Cancer Reform Strategy 1.1 The Cancer Reform Strategy, published in December 2007 1, built on the progress already achieved since the publication
Annual Report. Cape Cod Hospital and Falmouth Hospital Regional Cancer Network Expert physicians. Quality hospitals. Superior care.
 Annual Report Cape Cod Hospital and Falmouth Hospital Regional Cancer Network 2013 Expert physicians. Quality hospitals. Superior care. Cape Cod Hospital s Davenport- Mugar Hematology/Oncology Center and
Annual Report Cape Cod Hospital and Falmouth Hospital Regional Cancer Network 2013 Expert physicians. Quality hospitals. Superior care. Cape Cod Hospital s Davenport- Mugar Hematology/Oncology Center and
COPYRIGHTED MATERIAL. The modern management of cancer: an introductory note
 1 The modern management of cancer: an introductory note Cancer is a vast medical problem. It is now the major cause of mortality, both in the UK and elsewhere in the Western world [1] (Figure 1.1), diagnosed
1 The modern management of cancer: an introductory note Cancer is a vast medical problem. It is now the major cause of mortality, both in the UK and elsewhere in the Western world [1] (Figure 1.1), diagnosed
Acute Oncology. Protocols & Competencies Acute Oncology Introduction
 Acute Oncology Protocols & Competencies Acute Oncology Introduction Acute Oncology elearning Module Throughout the Acute Oncology FACTS elearning courses you will be able to access Network Protocols by
Acute Oncology Protocols & Competencies Acute Oncology Introduction Acute Oncology elearning Module Throughout the Acute Oncology FACTS elearning courses you will be able to access Network Protocols by
Appendix 4 Urology Care Pathways
 Appendix 4 Urology Care Pathways Cancer Care Pathways outline the steps and stages in the patient journey from referral through to diagnostics, staging, treatment, follow up, rehabilitation and if applicable
Appendix 4 Urology Care Pathways Cancer Care Pathways outline the steps and stages in the patient journey from referral through to diagnostics, staging, treatment, follow up, rehabilitation and if applicable
Macmillan-NICR Partnership: GP Federation Cancer Profiles (with Prevalence )
") Macmillan-NICR Partnership: GP Federation Cancer Profiles 2011-2015 (with Prevalence 1993-2015) 1 C a n c e r S t a t i s t i c s b y G P F e d e r a t i o n a r e a : 2 0 1 1-2015 Table of Contents Introduction...
Macmillan-NICR Partnership: GP Federation Cancer Profiles 2011-2015 (with Prevalence 1993-2015) 1 C a n c e r S t a t i s t i c s b y G P F e d e r a t i o n a r e a : 2 0 1 1-2015 Table of Contents Introduction...
Liver and Pancreatic Case discussion
 The Royal Marsden Liver and Pancreatic Case discussion Dr Ian Chau Consultant Medical Oncologist The Royal Marsden 77 year old gentleman with 2 months history of vague abdominal ache and clinically finding
The Royal Marsden Liver and Pancreatic Case discussion Dr Ian Chau Consultant Medical Oncologist The Royal Marsden 77 year old gentleman with 2 months history of vague abdominal ache and clinically finding
Guidelines for the Management of Renal Cancer West Midlands Expert Advisory Group for Urological Cancer
 Guidelines for the Management of Renal Cancer West Midlands Expert Advisory Group for Urological Cancer West Midlands Clinical Networks and Clinical Senate Coversheet for Network Expert Advisory Group
Guidelines for the Management of Renal Cancer West Midlands Expert Advisory Group for Urological Cancer West Midlands Clinical Networks and Clinical Senate Coversheet for Network Expert Advisory Group
The use of surgery in the elderly. for management of metastatic epidural spinal cord compression
 The use of surgery in the elderly Bone Tumor Simulators for management of metastatic epidural spinal cord compression Justin E. Bird, M.D. Assistant Professor Orthopaedic Oncology and Spine Surgery Epidemiology
The use of surgery in the elderly Bone Tumor Simulators for management of metastatic epidural spinal cord compression Justin E. Bird, M.D. Assistant Professor Orthopaedic Oncology and Spine Surgery Epidemiology
Greater Manchester Commissioning Hub: Cancer Programme. The ACE Programme. Wave 2 Multidisciplinary Diagnostic Centres
 Greater Manchester Commissioning Hub: Cancer Programme The ACE Programme Wave 2 Multidisciplinary Diagnostic Centres Background / Context GM Pilot focuses on 2 areas of Greater Manchester: Oldham South
Greater Manchester Commissioning Hub: Cancer Programme The ACE Programme Wave 2 Multidisciplinary Diagnostic Centres Background / Context GM Pilot focuses on 2 areas of Greater Manchester: Oldham South
Metastatic disease of the Spine
 Metastatic disease of the Spine Jwalant S. Mehta MS (Orth); MCh (Orth); D Orth; FRCS (Tr & Orth) Consultant Spine Surgeon The Royal Orthopaedic Hospital Birmingham Children s Hospital MSCC Metastatic Spinal
Metastatic disease of the Spine Jwalant S. Mehta MS (Orth); MCh (Orth); D Orth; FRCS (Tr & Orth) Consultant Spine Surgeon The Royal Orthopaedic Hospital Birmingham Children s Hospital MSCC Metastatic Spinal
Information Services Division NHS National Services Scotland
 Cancer in Scotland April 2017 First published in June 2004, revised with each National Statistics publication Next due for revision October 2017 Information Services Division NHS National Services Scotland
Cancer in Scotland April 2017 First published in June 2004, revised with each National Statistics publication Next due for revision October 2017 Information Services Division NHS National Services Scotland
Cancer Association of South Africa (CANSA) Fact Sheet on the Top Ten Cancers per Population Group
 Fact Sheet on the Top Ten Cancers per Population Group") Cancer Association of South Africa (CANSA) Fact Sheet on the Top Ten Cancers per Population Group Introduction There are more than 200 different types of cancer. It is also referred to as malignancies,
Cancer Association of South Africa (CANSA) Fact Sheet on the Top Ten Cancers per Population Group Introduction There are more than 200 different types of cancer. It is also referred to as malignancies,
Informatics in the new NHS : PHE and NCIN 9 months on. Nicky Coombes National Cancer Intelligence Network
 Informatics in the new NHS : PHE and NCIN 9 months on. Nicky Coombes National Cancer Intelligence Network What was then... Key Funding Accountability Regulation Advice Parliament NICE Department of Health
Informatics in the new NHS : PHE and NCIN 9 months on. Nicky Coombes National Cancer Intelligence Network What was then... Key Funding Accountability Regulation Advice Parliament NICE Department of Health
Trends and disparities in cancer in Aotearoa/ NZ
 Trends and disparities in cancer in Aotearoa/ NZ Professor Diana Sarfati #cancercrossroads @DiSarfati Why cancer? Estimated number of incident cases from 2018 to 2040 in New Zealand, all cancers, both
Trends and disparities in cancer in Aotearoa/ NZ Professor Diana Sarfati #cancercrossroads @DiSarfati Why cancer? Estimated number of incident cases from 2018 to 2040 in New Zealand, all cancers, both
APPENDIX ONE: ICD CODES
 APPENDIX ONE: ICD CODES ICD-10-AM ICD-9-CM Malignant neoplasms C00 C97 140 208, 238.6, 273.3 Lip, oral cavity and pharynx C00 C14 140 149 Digestive organs C15 C26 150 157, 159 Oesophagus 4 C15 150 excluding
APPENDIX ONE: ICD CODES ICD-10-AM ICD-9-CM Malignant neoplasms C00 C97 140 208, 238.6, 273.3 Lip, oral cavity and pharynx C00 C14 140 149 Digestive organs C15 C26 150 157, 159 Oesophagus 4 C15 150 excluding
came from a carcinoma and in 12 from a sarcoma. Ninety lesions were intrapulmonary and the as the chest wall and pleura. Details of the primary
 Thorax 1982;37:366-370 Thoracic metastases MARY P SHEPHERD From the Thoracic Surgical Unit, Harefield Hospital, Harefield ABSTRACI One hundred and four patients are reviewed who were found to have thoracic
Thorax 1982;37:366-370 Thoracic metastases MARY P SHEPHERD From the Thoracic Surgical Unit, Harefield Hospital, Harefield ABSTRACI One hundred and four patients are reviewed who were found to have thoracic
Malignant Spinal Cord Compression (MSCC) Clinical Advisor Coordinator
 Clinical Advisor Coordinator") Malignant Spinal Cord Compression (MSCC) Clinical Advisor Coordinator Induction Training 2016 Version Control This is a controlled document please destroy all previous versions on receipt of a new version.
Malignant Spinal Cord Compression (MSCC) Clinical Advisor Coordinator Induction Training 2016 Version Control This is a controlled document please destroy all previous versions on receipt of a new version.
Cancer in Ireland with estimates for
 Cancer in Ireland 1994-2015 with estimates for 2015-2017: Annual Report of the National Cancer Registry 2017 Page ABBREVIATIONS 95% CI 95% confidence interval APC Annual percentage change ASR Age-standardised
Cancer in Ireland 1994-2015 with estimates for 2015-2017: Annual Report of the National Cancer Registry 2017 Page ABBREVIATIONS 95% CI 95% confidence interval APC Annual percentage change ASR Age-standardised
NICE Quality Standards and COF
 NICE Quality Standards and COF David Baldwin Consultant Respiratory Physician NUH Hon Senior Lecturer Nottingham University Clinical lead NICE lung cancer GL Chair NICE QS Topic Expert Group Quality Standards
NICE Quality Standards and COF David Baldwin Consultant Respiratory Physician NUH Hon Senior Lecturer Nottingham University Clinical lead NICE lung cancer GL Chair NICE QS Topic Expert Group Quality Standards
BRIEFING PAPER THE USE OF RED FLAGS TO IDENTIFY SERIOUS SPINAL PATHOLOGY THE CHRISTIE, GREATER MANCHESTER & CHESHIRE. Version:
 BRIEFING PAPER THE USE OF RED FLAGS TO IDENTIFY SERIOUS SPINAL PATHOLOGY THE CHRISTIE, GREATER MANCHESTER & CHESHIRE Procedure Reference: Document Owner: Jackie Turnpenney Version: Accountable Committee:
BRIEFING PAPER THE USE OF RED FLAGS TO IDENTIFY SERIOUS SPINAL PATHOLOGY THE CHRISTIE, GREATER MANCHESTER & CHESHIRE Procedure Reference: Document Owner: Jackie Turnpenney Version: Accountable Committee:
Cancer of Unknown Primary (CUP)
") Cancer of Unknown Primary (CUP) Information for patients This information is for people with cancer of unknown primary (CUP) and covers symptoms, investigations/tests and treatment options. If there is
Cancer of Unknown Primary (CUP) Information for patients This information is for people with cancer of unknown primary (CUP) and covers symptoms, investigations/tests and treatment options. If there is
NOSCAN CLINICAL MANAGEMENT GUIDELINE (CMG) AND NOSCAN CHEMOTHERAPY REVIEW (NCR) STATUS DOCUMENT May Status (G / A / R) Status (G / A / R)
 AND NOSCAN CHEMOTHERAPY REVIEW (NCR) STATUS DOCUMENT May Status (G / A / R) Status (G / A / R)") Item 18-13c NOSCAN CLINICAL MANAGEMENT GUIDELINE (CMG) AND NOSCAN CHEMOTHERAPY REVIEW (NCR) STATUS DOCUMENT May 2013 BREAST CANCER MCN: Breast Disease: Breast Document ready to circulate lead to be discussed
Item 18-13c NOSCAN CLINICAL MANAGEMENT GUIDELINE (CMG) AND NOSCAN CHEMOTHERAPY REVIEW (NCR) STATUS DOCUMENT May 2013 BREAST CANCER MCN: Breast Disease: Breast Document ready to circulate lead to be discussed
SELF ASSESSMENT REPORT (MULTI-DISCIPLINARY TEAM)
") SELF ASSESSMENT REPORT (MULTI-DISCIPLINARY TEAM) Network Trust MDT MDT Lead Clinician ASWCN TAUNTON AND SOMERSET Taunton Lung MDT (11-2C-1) - 2011/12 Dr Sarah Foster Compliance Self Assessment LUNG MDT
SELF ASSESSMENT REPORT (MULTI-DISCIPLINARY TEAM) Network Trust MDT MDT Lead Clinician ASWCN TAUNTON AND SOMERSET Taunton Lung MDT (11-2C-1) - 2011/12 Dr Sarah Foster Compliance Self Assessment LUNG MDT
Manchester Cancer. Guidelines for Investigation and Management of Malignancy of Unknown Origin (MUO) / Cancer of Unknown Primary (CUP)
 / Cancer of Unknown Primary (CUP)") Manchester Cancer = Guidelines for Investigation and Management of Malignancy of Unknown Origin (MUO) / Cancer of Unknown Primary (CUP) 3 rd Edition December 2015 For Review February 2018 Contents Contents...
Manchester Cancer = Guidelines for Investigation and Management of Malignancy of Unknown Origin (MUO) / Cancer of Unknown Primary (CUP) 3 rd Edition December 2015 For Review February 2018 Contents Contents...
Palliative treatments for lung cancer: What can the oncologist do?
 Palliative treatments for lung cancer: What can the oncologist do? Neil Bayman Consultant Clinical Oncologist GM Cancer Palliative Care and Lung Cancer Education Event Manchester, 31 st January 2017 Most
Palliative treatments for lung cancer: What can the oncologist do? Neil Bayman Consultant Clinical Oncologist GM Cancer Palliative Care and Lung Cancer Education Event Manchester, 31 st January 2017 Most
Trends in Cancer Survival in NSW 1980 to 1996
 Trends in Cancer Survival in NSW 19 to 1996 Xue Q Yu Dianne O Connell Bruce Armstrong Robert Gibberd Cancer Epidemiology Research Unit Cancer Research and Registers Division The Cancer Council NSW August
Trends in Cancer Survival in NSW 19 to 1996 Xue Q Yu Dianne O Connell Bruce Armstrong Robert Gibberd Cancer Epidemiology Research Unit Cancer Research and Registers Division The Cancer Council NSW August
Cancer and Data in the New NHS May Di Riley, Director Clinical Outcomes
 Cancer and Data in the New NHS May 2011 Di Riley, Director Clinical Outcomes Alignment with NHS reforms Improving outcomes: A strategy for cancer sets out how the future direction for cancer will be aligned
Cancer and Data in the New NHS May 2011 Di Riley, Director Clinical Outcomes Alignment with NHS reforms Improving outcomes: A strategy for cancer sets out how the future direction for cancer will be aligned
Cancer Program Report 2014
 Cancer Program Report 2014 Queen of the Valley Hospital St Joseph Health Queen of the Valley Hospital - 2014 Site Table Site Total Class Sex Group Cases Analytic NonAn M F 0 I II ALL SITES 661 494 167
Cancer Program Report 2014 Queen of the Valley Hospital St Joseph Health Queen of the Valley Hospital - 2014 Site Table Site Total Class Sex Group Cases Analytic NonAn M F 0 I II ALL SITES 661 494 167
Cancer of Unknown Primary
 Cancer of Unknown Primary Helen Rickards Acute Oncology and Cancer of Unknown Primary CNS October 2014 Defining CUP Incidence Patient Pathways getting a diagnosis Patient assessment The patient s perspective
Cancer of Unknown Primary Helen Rickards Acute Oncology and Cancer of Unknown Primary CNS October 2014 Defining CUP Incidence Patient Pathways getting a diagnosis Patient assessment The patient s perspective
agreed MSCC pathways and guidelines).
.") Referral of Patients with Spinal Metastatic Disease and Suspected Metastatic Spinal Cord Compression (to be used in association with locally West Midlands Clinical Networks and Clinical Senate Coversheet
Referral of Patients with Spinal Metastatic Disease and Suspected Metastatic Spinal Cord Compression (to be used in association with locally West Midlands Clinical Networks and Clinical Senate Coversheet
Management of Acute Oncological emergencies
 Management of Acute Oncological emergencies Malignant Spinal cord compression (MSCC) Neutropenic sepsis Superior vena caval obstruction Hypercalcemia Hyponatremia Bowel obstruction Brain Metastasis with
Management of Acute Oncological emergencies Malignant Spinal cord compression (MSCC) Neutropenic sepsis Superior vena caval obstruction Hypercalcemia Hyponatremia Bowel obstruction Brain Metastasis with
Cancer Outcomes and Services Dataset: Implications for clinical teams
 Cancer Outcomes and Services Dataset: Implications for clinical teams Mick Peake Clinical Lead, NCIN National Clinical Lead, NHS Cancer Improvement Consultant & Senior Lecturer in Respiratory Medicine,
Cancer Outcomes and Services Dataset: Implications for clinical teams Mick Peake Clinical Lead, NCIN National Clinical Lead, NHS Cancer Improvement Consultant & Senior Lecturer in Respiratory Medicine,