CV outcomes Studies and Implications for diabetes management. Seraj Abualnaja, MD, FRCPC Consultant Interventional cardiologist DSFH
|
|
|
- Ezra Miller
- 5 years ago
- Views:
Transcription


1 CV outcomes Studies and Implications for diabetes management Seraj Abualnaja, MD, FRCPC Consultant Interventional cardiologist DSFH
2 Case 49 y female with the following medical problems DM typ2 Hypertension Dyslipidemia CKD, GFR 40 CAD s/p PCI 2 times, all related to angina Preserved LVEF 50%
3 Her diabetic complications includes the following: 1- Diabetic retinopathy 2- CKD with FGR of Vascuolpaty : 4- CAD s/p PCI times 5- PVD, with moderate atherosclerosis in lower limb arterial system 6- Recurrent admission to the hospital for CHF
4 Her labs are as follow : HBA1C is almost always above 10 LDL is always controlled below 70 mg/dl, last one was 60 She has normocytic anemia, Hg is always above 10 ECG : normal Echo : LVEF 52 %, no significant valve pathology
5 She presented with atypical and +ve MPI in inferior wall She has PCI to LAD and RCA before ( twice in RCA) and once in LAD All are DES She is on the following meds : ASA and plavix for the last 3 years Metformin, Sitagliptin and Insulin Lipitor of 40 mg daily Concor 10 mg daily Amlodipine 10 mg daily
6
7
8 So this time she was booked for CABG which was done for her LAD, OM and PDA She has prolonged ICU staying She was discharged after 3 weeks She was readmitted with sternal wound infection, debridement was done Another prolonged admission in the hospital but eventually she was discharged Another readmission for CHF symptoms and worsening creatinine She had aggressive diuresis and improved Still preserved LV function Creatinine is back to the base line (1.5)
9 Endocrine consultation was done for her blood sugar control Sitagliptin was stopped Empagliflozin was started as well as Insulin In follow up last week : She is euvolemic. She is NYHA class I-II. CCS class I BP is 130/60. HBA1C is 8.1

10 Life expectancy is reduced by 12 years in diabetes patients with previous CVD* 60 yrs End of life No diabetes Diabetes 6 yrs Diabetes + MI 12 yrs In this case, CVD is represented by MI or stroke *Male, 60 years of age with history of MI or stroke CVD, cardiovascular disease; MI, myocardial infarction 10
 3 3 2 This will rise to 642 million by 2040 1 1 0 CV death All-cause mortality 11 CI, confidence interval; CV,")
11 Type 2 diabetes is increasingly prevalent Hazard ratio (95% CI) (diabetes vs no diabetes) At least 68% of people >65 years with diabetes Globally, 415 million people are living with die of heart disease diabetes 1 2 Mortality risk associated with diabetes (n=820,900) This will rise to 642 million by CV death All-cause mortality 11 CI, confidence interval; CV, cardiovascular
12 Age-adjusted CVD death risk/10,000 person-years CV death is increased in patients with diabetes and multiple risk factors Number of risk factors Diabetes No diabetes Risk factors were serum cholesterol 200 mg/dl, current smoker, SBP 120 mmhg CV, cardiovascular; 12
13 Despite advances in therapies, life expectancy is reduced by multiple morbidities of T2D, stroke and MI All-cause mortality by disease status of participants at baseline Disease status at baseline HR (95% Cl) Diabetes, stroke and MI 6.9 (5.7, 8.3) Stroke and MI 3.5 (3.1, 4.0) Diabetes and stroke 3.8 (3.5, 4.2) Diabetes and MI 3.7 (3.3, 4.1) MI 2.0 (1.9, 2.2) Stroke 2.1 (2.0, 2.2) Diabetes 1.9 (1.8, 2.0) None 1.0 (ref) HR (95% CI) CI, confidence interval; HR, hazard ratio; MI, myocardial infarction; T2D, type 2 diabetes The Emerging Risk Factors Collaboration. JAMA 2015;314:52
14 Hlatky et al, lancet, 2009,373;

15 People with diabetes are at increased risk of heart failure 2 5 People with diabetes have a 2- to 5-fold higher risk of developing HF 1 Diabetes confers a 60 80% greater probability of CV death and all-cause mortality in those with established HF 2,3 * * 15
 0.6 0.4 RR=1.73 0.2 p<0.0001 0.")
16 Survival proportion Diabetes worsens heart failure prognosis Poorer HF survival with diabetes than without diabetes 1.0 LVEF 50% Diabetes No diabetes 0.8 LVEF <50% Diabetes No diabetes p= RR= Time (years) RR= p< Time (years) Kaplan Meier survival curves of HF patients hospitalised with LVEF 50% (n=498) and <50% (n=754) HF, heart failure; LVEF, left ventricular ejection fraction Varela-Roman A et al. Eur J Heart Failure 2005;7:859 16

17 Evolution of T2D agents DPP-4 inhibitors SGLT2 inhibitors Older T2D agents Newer T2D agents Lente class of insulins produced Recombinant human insulin produced GLP-1 receptor agonists Glimepiride: 3rd generation SU Insulin degludec SUs first used Metformin introduced in the UK 2nd generation SUs available Insulin glargine available 2 Three new classes introduced: -glucosidase inhibitors, meglitinides and TZDs DPP-4, dipeptidyl peptidase-4; GLP-1, glucagon-like peptide-1; SGLT2, sodium-
18 Antidiabetic treatments & cardiovascular disease: the evolution Antidiabetic treatments & relation to cardiovascular disease 18 (tolbutamide, rosiglitazone) Antidiabetic treatments that does not increase cardiovascular disease (DPP-4 I, saxagliptin)????can antidiabetic treatments reduce cardiovascular disease (SGLT2 inhibitors, GLP-1RA)
19 Overview of CVOTs of glucose-lowering drugs SAVOR-TIMI 53 1 (n=16,492) 1,222 3P-MACE EXAMINE 2 (n=5380) 621 3P-MACE TECOS 4 (n=14,724) P-MACE OMNEON 13 (n=4000) 4P-MACE CARMELINA 12 (n=8300) 4P-MACE + renal CAROLINA 11 (n=6000) 631 4P-MACE DPP-4 inhibitor CVOTs SGLT2 inhibitor CVOTs GLP1 CVOTs ELIXA 3 (n=6068) 844 4P-MACE EMPA-REG OUTCOME 5 (n=7028) 691 3P-MACE LEADER 6 (n=9340) 611 3P-MACE SUSTAIN-6 7 (n=3297) 3P-MACE CANVAS-R 8 (n=5700) Albuminuria CANVAS 10 (n=4365) 420 3P-MACE EXSCEL 14 (n=14,000) P-MACE ITCA CVOT 9 (n=4000) 4P-MACE CREDENCE 17 (n=3700) Renal + 5P-MACE HARMONY Outcomes 19 (n=9400) 3P-MACE REWIND 16 (n=9622) P-MACE DECLARE-TIMI (n=17,150) P-MACE Ertugliflozin CVOT 18 (n=3900) 3P-MACE
20
21 DPP4 inhibitor s SGLT2 inhibitor s Complet ed and ongoing CVOTs GLP1 receptor agonists
 amide DPP4 inhibitors Adapted from Drucker.")
22 DPP4 inhibitors: Mechanism of action Food intake Pancreas Glucose-dependent insulin secretion β-cells Increases glucose utilisation by muscle and adipose tissue α-cells Intestine Active GLP1 (7-36) Glucose-dependent glucagon suppression DPP4 Decreases hepatic glucose release improving overall glucose control Inactive GLP1 (9-36) amide DPP4 inhibitors Adapted from Drucker. Expert Opin Invest Drugs 2003;12: and Ahrén Curr Diab Rep. 2003;3: amino acids cleaved from amino terminus




23 Selected mechanistic trials indicate potential CV effects of the DPP4 inhibitor class Myocardial infarct size 1,2 Endothelial function 3 Triglycerides 8 Inflammation and oxidative stress 4 Left ventricular function 6,7 Atherosclerotic plaque volume 5 1. Ye et al. Am J Physiol Heart Circ Physiol 2010;298:H Hocher et al. Int J Cardiol 2013;167: van Poppel et al. Diabetes Care 2011;34: Kröller-Schön et al. Cardiovasc Res 2012;96: Ta et al. J Cardiovasc Pharmacol 2011;58: Sauvé et al. Diabetes 2010;59: Read et al. Circ Cardiovasc Imaging 2010;3: Matikainen et al. Diabetologia 2006;49:
24 Patients with primary endpoint (%) SAVOR-TIMI 53: Saxagliptin was non-inferior to placebo on primary 3P-MACE endpoint HR 1.00 (95% CI ) p < for non-inferiority p = 0.99 for superiority Saxagliptin Placebo Days No. at risk Placebo Saxagliptin Scirica et al. N Engl J Med 2013;369:
25 Hospitalisation for heart failure (%) SAVOR-TIMI 53: Increased risk of hospitalisation for heart failure in saxagliptin arm HR 1.27 (05% CI ); p = % 2.8% Saxagliptin Placebo Days Placebo Saxagliptin Scirica et al. Circulation 2014;130:
26 Patients with an event (%) TECOS: Sitagliptin was non-inferior to placebo on primary 4P-MACE endpoint Sitagliptin Placebo HR (95% CI): 0.98 ( ) p < Months in the trial Patients at risk: Sitagliptin Placebo *CV death, non-fatal MI, non-fatal stroke, hospitalisation for unstable angina. Green et al. N Engl J Med 2015; DOI: /NEJMoa
27 TECOS: No significant difference in rate of hospitalisation for heart failure (ITT analysis) Outcome Placebo Sitagliptin HR (95% CI) HHF * 228 (3.1%) 1.07/100 pt-y 228 (3.1%) 1.09/100 pt-y 1.00 ( ) p = 0.98 CV Death + HHF * 525 (7.2%) 2.50/100 pt-y 538 (7.3%) 2.54/100 pt-y 1.02 ( ) p = 0.74 ITT population. Adjusted for history of heart failure at baseline * Pre-specified analyses Green et al. N Engl J Med 2015; DOI: /NEJMoa Back 27
28
29 Summary of CV outcomes trials with DPP4 inhibitors Intervention Main inclusion criteria SAVOR-TIMI 53 1 EXAMINE 2 TECOS 3 CAROLINA 4 CARMELINA 5 Saxagliptin/ placebo History of or multiple risk factors for CVD Alogliptin/ placebo ACS within days before randomisation Sitagliptin/ placebo CVD Linagliptin/ glimepiride 2 specified traditional CV risk factors or manifest CVD Linagliptin/ placebo High risk of CV events (e.g. albuminuria, prior CVD) No. of patients 16, , Primary outcome 3P-MACE 3P-MACE 4P-MACE 4P-MACE 4P-MACE Key secondary outcome Target no. of events Median follow-up (y) Estimated completion Expanded MACE 4P-MACE 3P-MACE 3P-MACE 3P-MACE; renal composite * 4* 7 Completed Completed Completed *Ongoing. 1. Scirica et al. N Engl J Med 2013;369: White et al. N Engl J Med 2013;369: Green et al. N Engl J Med 2015; DOI: /NEJMoa Marx et al. Diabetes Vasc Dis Res 2015;12: NCT Scirica et al. Am Heart J 2011;162: e6. 7. Data on file (BI trial no trial protocol). 8. NCT
30 For the primary outcome, all completed CVOTs fall within the FDA mandated upper 95% CI limit of 1.3 Number of events (event rate, % per 100 person-years) Placebo + usual care Comparator + usual care DPP4 inhibitor trials SAVOR-TIMI (3.7%) 613 (3.7%) HR (95% CI) FDA mandated upper 95% CI for CV safety EXAMINE (11.8% ) 305 (11.3% ) * TECOS (4.17%) 839 (4.06%) GLP1 agonist trials ELIXA (13.4 %) 399 (13.2 %) *Upper boundary of 1-sided repeated CI. Total event rate, %. 1. Scirica et al. N Engl J Med 2013;369: White et al. N Engl J Med 2013;369: Green et al. N Engl J Med 2015; DOI: /NEJMoa Pfeffer et al. ADA, 8 Jun 2015, Boston, USA (oral presentation) Favours comparator Favours placebo 30
31 Hospitalisation for heart failure (HHF) data for all completed CVOTs Number of events (%) Placebo + usual care Comparator + usual care HR (95% CI) SAVOR-TIMI 53 (HHF) (2.8) 289 (3.5) EXAMINE (HHF analysis 1) 2 79 (2.9) 85 (3.1) EXAMINE (HHF analysis 2) 2 89 (3.3) 106 (3.9) TECOS (HHF) (3.1) 228 (3.1) TECOS (HHF + CV death) (7.2) 538 (7.3) ELIXA (HHF) 4 ELIXA (HHF + CV death) 4 Analysis 1 = as component of expanded MACE. Analysis 2 = as component of post-hoc composite of CV death and HHF. 1. Scirica et al. N Engl J Med 2013;369: White et al. N Engl J Med 2013;369: Green et al. N Engl J Med 2015; DOI: /NEJMoa Pfeffer et al. ADA, 8 Jun 2015, Boston, USA (oral presentation). 127 (4.2) 253 (8.3) 122 (4.0) 248 (8.2) Favours comparator Favours placebo
32 DPP4 inhibitor SGLT2 inhibitor s Complet ed and ongoing CVOTs GLP1 receptor agonists




33 Pancreas Insulin secretion Glucagon secretion Insulin biosynthesis β-cell proliferation β -cell apoptosis Liver Glucose output GLP1 has various potential effects on the CV system: Data derived from non-clinical and mechanistic proof-of-concept studies Incretin hormone 1,2 Brain Appetite Neuroprotection Muscle and adipose tissue Insulin sensitivity (direct or indirect?) Endothelial function Nitric oxide production Myocardial contractility (data conflict) Systolic function in myocardial infarction Systolic function in cardiomyopathy Infarct size Heart Ischaemic pre-conditioning Post-ischaemic recovery Myocardial glucose uptake Clinical trial data show that GLP1 receptor agonists are associated with small increases in heart rate and modest reductions in body weight and blood pressure 3 1. Jax. Clin Res Cardiol 2009;98: Grieve. Br J Pharmacol 2009;157: (modified). 3. Robinson et al. BMJ Open 2013;3:pii e
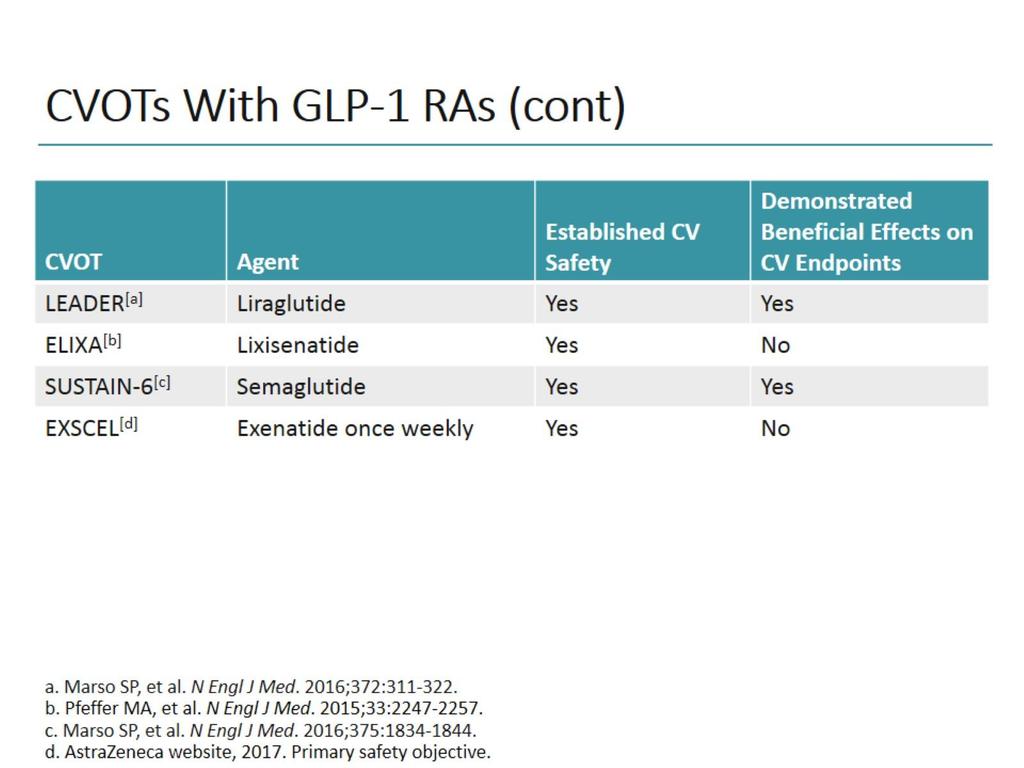
34 Summary of CV outcomes trials with GLP1 receptor agonists Intervention Main inclusion criteria No. of patients Primary outcome Key 2 outcome Target no. of events Estimated followup Estimated completion ELIXA 1,2 Lixisenatide/ placebo History of ACS P-MACE Expanded MACE years median Completed LEADER 3 Liraglutide/ placebo Vascular disease, or risk factors, or CRF, or CHF P-MACE Expanded MACE > 611 Up to ~5 years Nov-15 SUSTAIN-6 4 Semaglutide/ placebo Evidence of CV disease P-MACE Expanded MACE Not specified Up to ~3 years Jan-16 EXSCEL 5 Exenatide ER*/ placebo No CV criteria specified 14,000 3P-MACE All-cause mortality; HHF Not specified Up to ~7.5 years Apr-18 REWIND 6 Dulaglutide/ placebo Pre-existing vascular disease or 2 CV risk factors P-MACE Microvascular composite Not specified Up to ~6.5 years Apr-19 HARMONY OUTCOMES 7 Albiglutide/ placebo Established CVD P-MACE Expanded MACE Not specified 3 5 years May-19 *Once weekly. 1. NCT Bentley-Lewis et al. Am Heart J 2015;0:1-8.e7. 3. Marso et al. Am Heart J 2013;166: e5. 4. NCT NCT NCT NCT
35 Summary of ELIXA findings ELIXA 1 ACS HbA 1c % n = 6068 Lixisenatide Placebo 2.1 year median follow-up 4P-MACE 1.02 (95% CI ) Randomisation years of median follow-up No difference in 4P-MACE with lixisenatide vs placebo HR 1.02 (95% CI ) No difference in HHF with lixisenatide vs placebo HR 0.96 (95% CI ) No difference in CV death + HHF with lixisenatide vs placebo HR 0.97 (95% CI ) 1. Pfeffer et al. ADA, 8 Jun 2015, Boston, USA (oral presentation).
36
37
38
39 For the primary outcome, all completed CVOTs fall within the FDA mandated upper 95% CI limit of 1.3 Number of events (event rate, % per 100 person-years) Placebo + usual care Comparator + usual care DPP4 inhibitor trials SAVOR-TIMI (3.7%) 613 (3.7%) HR (95% CI) FDA mandated upper 95% CI for CV safety EXAMINE (11.8% ) 305 (11.3% ) * TECOS (4.17%) 839 (4.06%) GLP1 agonist trials ELIXA (13.4 %) 399 (13.2 %) *Upper boundary of 1-sided repeated CI. Total event rate, %. 1. Scirica et al. N Engl J Med 2013;369: White et al. N Engl J Med 2013;369: Green et al. N Engl J Med 2015; DOI: /NEJMoa Pfeffer et al. ADA, 8 Jun 2015, Boston, USA (oral presentation) Favours comparator Favours placebo
40 Hospitalisation for heart failure (HHF) data for all completed CVOTs Number of events (%) Placebo + usual care Comparator + usual care HR (95% CI) SAVOR-TIMI 53 (HHF) (2.8) 289 (3.5) EXAMINE (HHF analysis 1) 2 79 (2.9) 85 (3.1) EXAMINE (HHF analysis 2) 2 89 (3.3) 106 (3.9) TECOS (HHF) (3.1) 228 (3.1) TECOS (HHF + CV death) (7.2) 538 (7.3) ELIXA (HHF) 4 ELIXA (HHF + CV death) 4 Analysis 1 = as component of expanded MACE. Analysis 2 = as component of post-hoc composite of CV death and HHF. 1. Scirica et al. N Engl J Med 2013;369: White et al. N Engl J Med 2013;369: Green et al. N Engl J Med 2015; DOI: /NEJMoa Pfeffer et al. ADA, 8 Jun 2015, Boston, USA (oral presentation). 127 (4.2) 253 (8.3) 122 (4.0) 248 (8.2) Favours comparator Favours placebo 40
41


42 DPP4 inhibitor s SGLT2 inhibitor s Complet ed and ongoing CVOTs GLP1 receptor agonists







43 Filtered glucose load > 180 g/day Urinary glucose excretion via SGLT2 inhibition 1 SGLT2 inhibitor SGLT2 SGLT1 SGLT2 inhibitors reduce glucose reabsorption in the proximal tubule, leading to urinary glucose excretion * and osmotic diuresis 1. Bakris et al. Kidney Int 2009;75;
 Albuminuria SNS SNS activity activity (?) (?) Weight Visceral adiposity Glucose Insulin Oxidative stress Uric Acid LDL-C HDL-C Triglycerides Inzucchi et al.")
44 SGLT2 inhibitors modulate a range of factors related to CV risk Based on clinical and mechanistic studies Blood pressure Arterial stiffness Novel Pathways (?) Albuminuria SNS SNS activity activity (?) (?) Weight Visceral adiposity Glucose Insulin Oxidative stress Uric Acid LDL-C HDL-C Triglycerides Inzucchi et al. Diab Vasc Dis Res 2015;12:
45 Follow-up EMPA-REG OUTCOME : Study design Aim Compound-specific To determine CV safety of empagliflozin vs placebo + usual care for glycaemic control and CV risk in patients with T2D and high CV risk Screening (n = 11,507) 2 weeks Placebo run-in 12 weeks of stable background glucose-lowering therapy R Background therapy adjustment allowed after Week 12 Placebo + usual care Empagliflozin 10 mg QD + usual care Empagliflozin 25 mg QD + usual care Visit 1 Visit 2 Visit 3 Visits 4 7 every 4 weeks Visits 8 10 every 12 weeks Visits every 14 weeks End of study visit -3-2 Zinman et al. Cardiovasc Diabetol 2014;13: Week days
46
47





48 EMPA-REG OUTCOME summary Empagliflozin in addition to standard of care reduced CV risk and improved overall survival in adults with T2D and established CV disease Relative risk reduction: 3P-MACE CV death All-cause mortality HHF 14% 38% 32% 35% The overall safety profile of empagliflozin was consistent with previous clinical trials and current label information 3P-MACE, 3-point major adverse cardiovascular 48
49

50
Can We Reduce Heart Failure by Treating Diabetes? CVOT Data on SGLT2 Inhibitors and GLP-1Receptor Agonists
 Can We Reduce Heart Failure by Treating Diabetes? CVOT Data on SGLT2 Inhibitors and GLP-1Receptor Agonists Robert R. Henry, MD Professor of Medicine University of California, San Diego Relevant Conflict
Can We Reduce Heart Failure by Treating Diabetes? CVOT Data on SGLT2 Inhibitors and GLP-1Receptor Agonists Robert R. Henry, MD Professor of Medicine University of California, San Diego Relevant Conflict
Update on Diabetes Cardiovascular Outcome Trials
 Update on Diabetes Cardiovascular Outcome Trials Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of Miami Miller School of Medicine
Update on Diabetes Cardiovascular Outcome Trials Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of Miami Miller School of Medicine
Management of Type 2 Diabetes Cardiovascular Outcomes Trials Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas
 Management of Type 2 Diabetes Cardiovascular Outcomes Trials 2018 Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas Speaker Disclosure Dr. Blevins has disclosed that he has received grant support
Management of Type 2 Diabetes Cardiovascular Outcomes Trials 2018 Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas Speaker Disclosure Dr. Blevins has disclosed that he has received grant support
Update on Cardiovascular Outcome Trials in Diabetes Jay S. Skyler, MD, MACP
 Update on Cardiovascular Outcome Trials in Diabetes Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research InsAtute University of Miami Miller School of Medicine
Update on Cardiovascular Outcome Trials in Diabetes Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research InsAtute University of Miami Miller School of Medicine
Cardiovascular Outcomes With Newer Diabetes Drugs: Results From The EMPA-REG and LEADER Trials
 Cardiovascular Outcomes With Newer Diabetes Drugs: Results From The EMPA-REG and LEADER Trials Rajiv Roy, MD Endocrinology Sharp Rees-Stealy Medical Group Background Between 1990 and 2010: Incidence of
Cardiovascular Outcomes With Newer Diabetes Drugs: Results From The EMPA-REG and LEADER Trials Rajiv Roy, MD Endocrinology Sharp Rees-Stealy Medical Group Background Between 1990 and 2010: Incidence of
Current principles of diabetes management
 Current principles of diabetes management Prof. Martin Haluzík, MD, DSc. 3 Department of Medicine, General University Hospital and 1st Faculty of Medicine, Charles University in Prague, Czech Republic
Current principles of diabetes management Prof. Martin Haluzík, MD, DSc. 3 Department of Medicine, General University Hospital and 1st Faculty of Medicine, Charles University in Prague, Czech Republic
CANVAS Program Independent commentary
 CANVAS Program Independent commentary Cliff Bailey Aston University, Birmingham, UK 2017 Disclosures and disclaimers Clifford J Bailey CJB has attended advisory boards, undertaken ad hoc consultancy, received
CANVAS Program Independent commentary Cliff Bailey Aston University, Birmingham, UK 2017 Disclosures and disclaimers Clifford J Bailey CJB has attended advisory boards, undertaken ad hoc consultancy, received
01/09/2017. Outline. SGLT 2 inhibitor? Diabetes Patients: Complex and Heterogeneous. Association between diabetes and cardiovascular events
 MICROVASCULAR COMPLICATIONS Incidence of outcome g 1 Cardioprotective Effects of SGLT2s Relevant for Which T2 Diabetes Patient? SGLT 2 inhibitor? 58 year old, waist circumference 5 cm, PMH: IHD On statin,
MICROVASCULAR COMPLICATIONS Incidence of outcome g 1 Cardioprotective Effects of SGLT2s Relevant for Which T2 Diabetes Patient? SGLT 2 inhibitor? 58 year old, waist circumference 5 cm, PMH: IHD On statin,
Diabete: terapia nei pazienti a rischio cardiovascolare
 Diabete: terapia nei pazienti a rischio cardiovascolare Giorgio Sesti Università Magna Graecia di Catanzaro Cardiovascular mortality in relation to diabetes mellitus and a prior MI: A Danish Population
Diabete: terapia nei pazienti a rischio cardiovascolare Giorgio Sesti Università Magna Graecia di Catanzaro Cardiovascular mortality in relation to diabetes mellitus and a prior MI: A Danish Population
Diabetes and Heart Failure: The Role of SGLT2 Inhibitors
 22 nd Annual Heart Failure 2018 Symposium Diabetes and Heart Failure: The Role of SGLT2 Inhibitors Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Elliot Corday Professor of Cardiovascular Medicine UCLA Division
22 nd Annual Heart Failure 2018 Symposium Diabetes and Heart Failure: The Role of SGLT2 Inhibitors Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Elliot Corday Professor of Cardiovascular Medicine UCLA Division
Clinical Relevance of Blood Pressure Lowering Effect of Modern Antidiabetic Drugs
 Clinical Relevance of Blood Pressure Lowering Effect of Modern Antidiabetic Drugs Professor Guntram Schernthaner Medical University of Vienna, Austria guntram.schernthaner@meduniwien.ac.at Agenda Glucose
Clinical Relevance of Blood Pressure Lowering Effect of Modern Antidiabetic Drugs Professor Guntram Schernthaner Medical University of Vienna, Austria guntram.schernthaner@meduniwien.ac.at Agenda Glucose
Cardiologists and HbA1c: Novel Diabetes Drugs and Cardiovascular Disease Outcomes
 Biomarkers 2018 Cardiologists and HbA1c: Novel Diabetes Drugs and Cardiovascular Disease Outcomes Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Elliot Corday Professor of Cardiovascular Medicine UCLA Division
Biomarkers 2018 Cardiologists and HbA1c: Novel Diabetes Drugs and Cardiovascular Disease Outcomes Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Elliot Corday Professor of Cardiovascular Medicine UCLA Division
Updates in Diabetes and Cardiovascular Disease Management: Are You Making the Link?
 Updates in Diabetes and Cardiovascular Disease Management: Are You Making the Link? Denise Kolanczyk, PharmD, BCPS AQ Cardiology 1 Erika Hellenbart, PharmD, BCPS 2 Jennifer D Souza, PharmD, CDE, BC ADM
Updates in Diabetes and Cardiovascular Disease Management: Are You Making the Link? Denise Kolanczyk, PharmD, BCPS AQ Cardiology 1 Erika Hellenbart, PharmD, BCPS 2 Jennifer D Souza, PharmD, CDE, BC ADM
Preventing Serious Health Consequences of Type 2 Diabetes
 Preventing Serious Health Consequences of Type 2 Diabetes The Evidence Hertzel C. Gerstein MD MSc FRCPC Professor and Population Health Institute Chair in Diabetes Research McMaster University and Hamilton
Preventing Serious Health Consequences of Type 2 Diabetes The Evidence Hertzel C. Gerstein MD MSc FRCPC Professor and Population Health Institute Chair in Diabetes Research McMaster University and Hamilton
Multi-factor approach to reduce cardiovascular risk in diabetes
 Multi-factor approach to reduce cardiovascular risk in diabetes Prof. Nicola Napoli, MD PhD Division of Endocrinology and Diabetes Università Campus Bio-Medico di Roma Washington University in St Louis
Multi-factor approach to reduce cardiovascular risk in diabetes Prof. Nicola Napoli, MD PhD Division of Endocrinology and Diabetes Università Campus Bio-Medico di Roma Washington University in St Louis
Medical therapy advances London/Manchester RCP February/June 2016
 Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
Case Studies in Type 2 Diabetes Mellitus: Focus on Cardiovascular Outcomes Trials
 Case Studies in Type 2 Diabetes Mellitus: Focus on Cardiovascular Outcomes Trials Louis Kuritzky MD Clinical Assistant Professor Emeritus Department of Community Health and Family Medicine College of Medicine
Case Studies in Type 2 Diabetes Mellitus: Focus on Cardiovascular Outcomes Trials Louis Kuritzky MD Clinical Assistant Professor Emeritus Department of Community Health and Family Medicine College of Medicine
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications
 Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
The EMPA-REG OUTCOME trial: Design and results. David Fitchett, MD University of Toronto, Canada
 The EMPA-REG OUTCOME trial: Design and results David Fitchett, MD University of Toronto, Canada Asian Cardio Diabetes Forum April 23 24, 2016 Kuala Lumpur, Malaysia Life Expectancy Is Reduced by ~12 Years
The EMPA-REG OUTCOME trial: Design and results David Fitchett, MD University of Toronto, Canada Asian Cardio Diabetes Forum April 23 24, 2016 Kuala Lumpur, Malaysia Life Expectancy Is Reduced by ~12 Years
Newer Therapies for Type 2 Diabetes
 Newer Therapies for Type 2 Diabetes Sandra Indacochea Sobel, MD Clinical Assistant Professor of Medicine Clinical Chief of Endocrinology, UPMC Mercy Division of Endocrinology, Diabetes, and Metabolism
Newer Therapies for Type 2 Diabetes Sandra Indacochea Sobel, MD Clinical Assistant Professor of Medicine Clinical Chief of Endocrinology, UPMC Mercy Division of Endocrinology, Diabetes, and Metabolism
In compliance with the accrediting board policies, the American Diabetes Association requires the following disclosure to the participants:
 In compliance with the accrediting board policies, the American Diabetes Association requires the following disclosure to the participants: Entity Activity Financial Consideration Comments Novo Nordisk
In compliance with the accrediting board policies, the American Diabetes Association requires the following disclosure to the participants: Entity Activity Financial Consideration Comments Novo Nordisk
GLP 1 agonists Winning the Losing Battle. Dr Bernard SAMIA. KCS Congress: Impact through collaboration
 GLP 1 agonists Winning the Losing Battle Dr Bernard SAMIA KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures I have
GLP 1 agonists Winning the Losing Battle Dr Bernard SAMIA KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures I have
Cardiologists and HbA1c: Novel Diabetes Drugs and the Cardiologist as Diabetician
 Biomarkers 2019 Cardiologists and HbA1c: Novel Diabetes Drugs and the Cardiologist as Diabetician Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Elliot Corday Professor of Cardiovascular Medicine UCLA Division
Biomarkers 2019 Cardiologists and HbA1c: Novel Diabetes Drugs and the Cardiologist as Diabetician Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Elliot Corday Professor of Cardiovascular Medicine UCLA Division
LEADER Liraglutide and cardiovascular outcomes in type 2 diabetes
 LEADER Liraglutide and cardiovascular outcomes in type 2 diabetes Presented at DSBS seminar on mediation analysis August 18 th Søren Rasmussen, Novo Nordisk. LEADER CV outcome study To determine the effect
LEADER Liraglutide and cardiovascular outcomes in type 2 diabetes Presented at DSBS seminar on mediation analysis August 18 th Søren Rasmussen, Novo Nordisk. LEADER CV outcome study To determine the effect
New Strategies for Cardiovascular Risk reduction in Diabetes
 New Strategies for Cardiovascular Risk reduction in Diabetes Dr. Godwin LEUNG Tat Chi MB ChB(HK), MRCP (UK), FHKCP, FHKAM (Medicine) FRCP (Glasg), FACC Specialist in Cardiology % event as first CV event
New Strategies for Cardiovascular Risk reduction in Diabetes Dr. Godwin LEUNG Tat Chi MB ChB(HK), MRCP (UK), FHKCP, FHKAM (Medicine) FRCP (Glasg), FACC Specialist in Cardiology % event as first CV event
Can Treating Diabetes with SGLT2 inhibitors Prevent Heart Failure?
 UCSD Hawaii 2017 Symposium Can Treating Diabetes with SGLT2 inhibitors Prevent Heart Failure? Gregg C. Fonarow, MD, FACC, FAHA Elliot Corday Professor of Cardiovascular Medicine UCLA Division of Cardiology
UCSD Hawaii 2017 Symposium Can Treating Diabetes with SGLT2 inhibitors Prevent Heart Failure? Gregg C. Fonarow, MD, FACC, FAHA Elliot Corday Professor of Cardiovascular Medicine UCLA Division of Cardiology
GLP-1 RECEPTOR AGONIST SHOULD I TRY IT? VERONICA BRADY, PHD, BC-ADM, CDE PROJECT ECHO JUNE 21, 2018
 GLP-1 RECEPTOR AGONIST SHOULD I TRY IT? VERONICA BRADY, PHD, BC-ADM, CDE PROJECT ECHO JUNE 21, 2018 SOMETHING TO CONSIDER IF YOU COULD PRESCRIBE A MEDICATION FOR YOUR PATIENT WITH DIABETES THAT: DECREASED
GLP-1 RECEPTOR AGONIST SHOULD I TRY IT? VERONICA BRADY, PHD, BC-ADM, CDE PROJECT ECHO JUNE 21, 2018 SOMETHING TO CONSIDER IF YOU COULD PRESCRIBE A MEDICATION FOR YOUR PATIENT WITH DIABETES THAT: DECREASED
The Death of Sulfonylureas? A Review of New Diabetes Medications
 The Death of Sulfonylureas? A Review of New Diabetes Medications Kelly Hoenig, Pharm.D., BCPS Cedar Rapids Family Medicine Residency 2/4/17 Objectives Review GLP-1 Agonists, DPP-IV Inhibitors and SGLT-2
The Death of Sulfonylureas? A Review of New Diabetes Medications Kelly Hoenig, Pharm.D., BCPS Cedar Rapids Family Medicine Residency 2/4/17 Objectives Review GLP-1 Agonists, DPP-IV Inhibitors and SGLT-2
Update on Cardiovascular Outcome Trials in Diabetes. Rury R. Holman, FMedSci NIHR Senior Investigator 11 th February 2013
 Update on Cardiovascular Outcome Trials in Diabetes Rury R. Holman, FMedSci NIHR Senior Investigator 11 th February 2013 Residual Vascular Risk in People with Diabetes 2 Analyses based on 530,083 participants
Update on Cardiovascular Outcome Trials in Diabetes Rury R. Holman, FMedSci NIHR Senior Investigator 11 th February 2013 Residual Vascular Risk in People with Diabetes 2 Analyses based on 530,083 participants
Cardiovascular Impact of Medications for Treating Type 2 Diabetes
 Friday CME Breakfast Lecture Cardiovascular Impact of Medications for Treating Type 2 Diabetes Thomas Blevins, MD Endocrinologist, Private Practice Texas Diabetes and Endocrinology Austin, Texas Educational
Friday CME Breakfast Lecture Cardiovascular Impact of Medications for Treating Type 2 Diabetes Thomas Blevins, MD Endocrinologist, Private Practice Texas Diabetes and Endocrinology Austin, Texas Educational
Diabetes Management in CAD Patients. Stuart R. Chipkin, MD Research Professor School of Public Health and Health Sciences University of Massachusetts
 Diabetes Management in CAD Patients Stuart R. Chipkin, MD Research Professor School of Public Health and Health Sciences University of Massachusetts Disclosure Stuart R. Chipkin, MD, FACE Nothing to disclose
Diabetes Management in CAD Patients Stuart R. Chipkin, MD Research Professor School of Public Health and Health Sciences University of Massachusetts Disclosure Stuart R. Chipkin, MD, FACE Nothing to disclose
Help the Heart. An Update on GLP-1 Agonists and SGLT2 Inhibitors. Tara Hawley, PharmD PGY1 Pharmacy Resident Mayo Clinic Health System Eau Claire
 Help the Heart An Update on GLP-1 Agonists and SGLT2 Inhibitors Tara Hawley, PharmD PGY1 Pharmacy Resident Mayo Clinic Health System Eau Claire Mayo Clinic Grand Rounds May 16, 2017 2017 MFMER slide-1
Help the Heart An Update on GLP-1 Agonists and SGLT2 Inhibitors Tara Hawley, PharmD PGY1 Pharmacy Resident Mayo Clinic Health System Eau Claire Mayo Clinic Grand Rounds May 16, 2017 2017 MFMER slide-1
Top HF Trials to Impact Your Practice
 Top HF Trials to Impact Your Practice Biykem Bozkurt, MD, FACC The Mary and Gordon Cain Chair & Professor of Medicine Medical Care Line Executive, DeBakey VA Medical Center, Director, Winters Center for
Top HF Trials to Impact Your Practice Biykem Bozkurt, MD, FACC The Mary and Gordon Cain Chair & Professor of Medicine Medical Care Line Executive, DeBakey VA Medical Center, Director, Winters Center for
Diabetes new challenges, new agents, new order
 Diabetes new challenges, new agents, new order Ken Earle St Georges University Hospitals NHS Foundation Trust Overview Cardiovascular disease unmet needs Treating evident and residual risk Integrating
Diabetes new challenges, new agents, new order Ken Earle St Georges University Hospitals NHS Foundation Trust Overview Cardiovascular disease unmet needs Treating evident and residual risk Integrating
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES
 ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
Halting the Rise, Newest Non- Insulin Options for Lowering A1c
 Halting the Rise, Newest Non- Insulin Options for Lowering A1c Alecia Rottinghaus, PharmD PGY-1 Pharmacy Resident Iowa City Veterans Affairs Health Care System January 29 th, 2019 Disclosures Alecia Rottinghaus
Halting the Rise, Newest Non- Insulin Options for Lowering A1c Alecia Rottinghaus, PharmD PGY-1 Pharmacy Resident Iowa City Veterans Affairs Health Care System January 29 th, 2019 Disclosures Alecia Rottinghaus
Halting the Rise, Newest Non- Insulin Options for Lowering A1c
 Halting the Rise, Newest Non- Insulin Options for Lowering A1c Alecia Rottinghaus, PharmD PGY-1 Pharmacy Resident Iowa City Veterans Affairs Health Care System January 29 th, 2019 Disclosures Alecia Rottinghaus
Halting the Rise, Newest Non- Insulin Options for Lowering A1c Alecia Rottinghaus, PharmD PGY-1 Pharmacy Resident Iowa City Veterans Affairs Health Care System January 29 th, 2019 Disclosures Alecia Rottinghaus
2019 Update on Recent Guideline Releases for Diabetes, Hypertension, and Dyslipidemia: Can We, Please, All Just Get on the Same Page?!
 2019 Update on Recent Guideline Releases for Diabetes, Hypertension, and Dyslipidemia: Can We, Please, All Just Get on the Same Page?! Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM Assistant Professor,
2019 Update on Recent Guideline Releases for Diabetes, Hypertension, and Dyslipidemia: Can We, Please, All Just Get on the Same Page?! Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM Assistant Professor,
Review of FDA Guidance on Cardiovascular Outcomes for Diabetes Medication Trials and Application to Clinical Management
 Katherine S. O Neal Pharm.D., MBA, BCACP, CDE, BC-ADM, AE-C Associate Professor The University of Oklahoma Health Sciences Center College of Pharmacy Department of Internal Medicine Oklahoma City, OK Member,
Katherine S. O Neal Pharm.D., MBA, BCACP, CDE, BC-ADM, AE-C Associate Professor The University of Oklahoma Health Sciences Center College of Pharmacy Department of Internal Medicine Oklahoma City, OK Member,
Actualités en diabétologie Quoi de neuf en 2016? S. Aouiche Service de diabétologie CHU Mustapha Alger.Pr BOUDIBA
 Actualités en diabétologie Quoi de neuf en 2016? S. Aouiche Service de diabétologie CHU Mustapha Alger.Pr BOUDIBA Deux médicaments valent mieux qu un dans le traitement du patient diabétique Jochen.SEUFERT
Actualités en diabétologie Quoi de neuf en 2016? S. Aouiche Service de diabétologie CHU Mustapha Alger.Pr BOUDIBA Deux médicaments valent mieux qu un dans le traitement du patient diabétique Jochen.SEUFERT
No Increased Cardiovascular Risk for Lixisenatide in ELIXA
 ON ISSUES IN THE MANAGEMENT OF TYPE 2 DIABETES JUNE 2015 Coverage of data from ADA 2015, June 5 9 in Boston, Massachusetts No Increased Cardiovascular Risk for Lixisenatide in ELIXA First Cardiovascular
ON ISSUES IN THE MANAGEMENT OF TYPE 2 DIABETES JUNE 2015 Coverage of data from ADA 2015, June 5 9 in Boston, Massachusetts No Increased Cardiovascular Risk for Lixisenatide in ELIXA First Cardiovascular
LATE BREAKING STUDIES IN DM AND CAD. Will this change the guidelines?
 LATE BREAKING STUDIES IN DM AND CAD Will this change the guidelines? Objectives 1. Discuss current guidelines for prevention of CHD in diabetes. 2. Discuss the FDA Guidance for Industry regarding evaluating
LATE BREAKING STUDIES IN DM AND CAD Will this change the guidelines? Objectives 1. Discuss current guidelines for prevention of CHD in diabetes. 2. Discuss the FDA Guidance for Industry regarding evaluating
Terapia con agonisti GLP1 e outcome cardiovascolare. Edoardo Mannucci
 Terapia con agonisti GLP e outcome cardiovascolare Edoardo Mannucci Conflitti di interessi Negli ultimi due anni, E. Mannucci ha ricevuto compensi per relazioni e/o consulenze da: Abbott, AstraZeneca,
Terapia con agonisti GLP e outcome cardiovascolare Edoardo Mannucci Conflitti di interessi Negli ultimi due anni, E. Mannucci ha ricevuto compensi per relazioni e/o consulenze da: Abbott, AstraZeneca,
Newer Diabetes Treatments Drug Class Update with New Drug Evaluation: Semaglutide and Ertugliflozin
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
The Clinical Unmet need in the patient with Diabetes and ACS
 The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
La lezione dei trials di safety cardiovascolare. Edoardo Mannucci
 La lezione dei trials di safety cardiovascolare Edoardo Mannucci Conflitti di interessi Negli ultimi due anni, E. Mannucci ha ricevuto compensi per relazioni e/o consulenze da: Abbott, AstraZeneca, Boehringer
La lezione dei trials di safety cardiovascolare Edoardo Mannucci Conflitti di interessi Negli ultimi due anni, E. Mannucci ha ricevuto compensi per relazioni e/o consulenze da: Abbott, AstraZeneca, Boehringer
Cardiovascular risk in diabetes: What the Cardiologist Needs to Know. Hani Sabbour MD FACC FHRS
 Cardiovascular risk in diabetes: What the Cardiologist Needs to Know Hani Sabbour MD FACC FHRS Years of life lost Hazard ratio (95% CI) (diabetes vs. no diabetes) CVD is the leading cause of death among
Cardiovascular risk in diabetes: What the Cardiologist Needs to Know Hani Sabbour MD FACC FHRS Years of life lost Hazard ratio (95% CI) (diabetes vs. no diabetes) CVD is the leading cause of death among
Diabetes and Cardiovascular Risk Management Denise M. Kolanczyk, PharmD, BCPS-AQ Cardiology
 Diabetes and Cardiovascular Risk Management Denise M. Kolanczyk, PharmD, BCPS-AQ Cardiology Disclosures In compliance with the accrediting board policies, the American Diabetes Association requires the
Diabetes and Cardiovascular Risk Management Denise M. Kolanczyk, PharmD, BCPS-AQ Cardiology Disclosures In compliance with the accrediting board policies, the American Diabetes Association requires the
Type 2 diabetes and cardiovascular risk: the role of GLP-1
 Type 2 diabetes and cardiovascular risk: the role of GLP-1 Dr Isidora Kitsou-Mylona, PhD Novo Nordisk Regional Medical Advisor Business Area Africa, Gulf & India Disclaimer I am an employee of Novo Nordisk
Type 2 diabetes and cardiovascular risk: the role of GLP-1 Dr Isidora Kitsou-Mylona, PhD Novo Nordisk Regional Medical Advisor Business Area Africa, Gulf & India Disclaimer I am an employee of Novo Nordisk
The Role Of SGLT-2 Inhibitors In Clinical Practice. Anne Peters, MD Professor, USC Keck School of Medicine Director, USC Clinical Diabetes Programs
 The Role Of SGLT-2 Inhibitors In Clinical Practice Anne Peters, MD Professor, USC Keck School of Medicine Director, USC Clinical Diabetes Programs Disclosure of Potential Conflicts of Interest Consultantship
The Role Of SGLT-2 Inhibitors In Clinical Practice Anne Peters, MD Professor, USC Keck School of Medicine Director, USC Clinical Diabetes Programs Disclosure of Potential Conflicts of Interest Consultantship
Novel anti-diabetic therapies
 Prof. Manfredi Rizzo, MD, PhD ASSOCIATE PROFESSOR OF INTERNAL MEDICINE School of Medicine University of Palermo, Italy & ASSOCIATE PROFESSOR OF INTERNAL MEDICINE School of Medicine University of South
Prof. Manfredi Rizzo, MD, PhD ASSOCIATE PROFESSOR OF INTERNAL MEDICINE School of Medicine University of Palermo, Italy & ASSOCIATE PROFESSOR OF INTERNAL MEDICINE School of Medicine University of South
What s New in Type 2 Diabetes? 2018 Diabetes Updates
 What s New in Type 2 Diabetes? 2018 Diabetes Updates Gretchen Ray, PharmD, PhC, BCACP, CDE Associate Professor, UNM College of Pharmacy January 28, 2018 gray@salud.unm.edu OBJECTIVES Describe the most
What s New in Type 2 Diabetes? 2018 Diabetes Updates Gretchen Ray, PharmD, PhC, BCACP, CDE Associate Professor, UNM College of Pharmacy January 28, 2018 gray@salud.unm.edu OBJECTIVES Describe the most
Educational Objectives
 Educational Objectives Recognize the rationale for cardiovascular outcome trials (CVOTs) in T2DM and review data from recent CVOTs of anti hyperglycemic agents Examine alignment of managed care T2DM treatment
Educational Objectives Recognize the rationale for cardiovascular outcome trials (CVOTs) in T2DM and review data from recent CVOTs of anti hyperglycemic agents Examine alignment of managed care T2DM treatment
NEW DIABETES CARE MEDICATIONS
 NEW DIABETES CARE MEDICATIONS James Bonucchi DO, ECNU, FACE Adult Medicine and Endocrinology Specialists Disclosures Speakers bureau Sanofi AZ BI Diabetes Diabetes cost ADA 2017 data Ever increasing disorder.
NEW DIABETES CARE MEDICATIONS James Bonucchi DO, ECNU, FACE Adult Medicine and Endocrinology Specialists Disclosures Speakers bureau Sanofi AZ BI Diabetes Diabetes cost ADA 2017 data Ever increasing disorder.
Drug Class Update with New Drug Evaluation: Non-insulin Diabetes Treatments (SGLT-2 Inhibitors and GLP-1 Receptor Agonists)
") Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Cardiovascular Outcome Trials of Diabetes Medications: Translating Results into Practice
 Presenter Disclosure Information Cardiovascular Outcome Trials of Diabetes Medications: Translating Results into Practice Carol Hatch Wysham, MD Clinical Professor of Medicine University of Washington
Presenter Disclosure Information Cardiovascular Outcome Trials of Diabetes Medications: Translating Results into Practice Carol Hatch Wysham, MD Clinical Professor of Medicine University of Washington
Causes of death in Diabetes
 Rates of CV events in Diabetes patients Respiratory4.2 Cancer 7.6 Diabetes 1.3 CV disease 17.3 Causes of death in Diabetes 250 200 150 100 50 0 per 10,000 person-years 97 151 243 Framingham 5 X increase
Rates of CV events in Diabetes patients Respiratory4.2 Cancer 7.6 Diabetes 1.3 CV disease 17.3 Causes of death in Diabetes 250 200 150 100 50 0 per 10,000 person-years 97 151 243 Framingham 5 X increase
Dapagliflozin and cardiovascular outcomes in type 2
 EARN 3 FREE CPD POINTS diabetes Leader in digital CPD for Southern African healthcare professionals Dapagliflozin and cardiovascular outcomes in type 2 diabetes Introduction People with type 2 diabetes
EARN 3 FREE CPD POINTS diabetes Leader in digital CPD for Southern African healthcare professionals Dapagliflozin and cardiovascular outcomes in type 2 diabetes Introduction People with type 2 diabetes
Soo LIM, MD, PHD Internal Medicine Seoul National University Bundang Hospital
 Soo LIM, MD, PHD Internal Medicine Seoul National University Bundang Hospital Agenda Association between Cardiovascular Disease and Type 2 Diabetes Importance of HbA1c Management esp. High risk patients
Soo LIM, MD, PHD Internal Medicine Seoul National University Bundang Hospital Agenda Association between Cardiovascular Disease and Type 2 Diabetes Importance of HbA1c Management esp. High risk patients
CARDIOVASCULAR RISK FACTOR CONTROL IN TYPE 2 DIABETES MELLITUS AND NEW TRIAL EVIDENCE
 CARDIOVASCULAR RISK FACTOR CONTROL IN TYPE 2 DIABETES MELLITUS AND NEW TRIAL EVIDENCE *Peter M. Nilsson Department of Clinical Sciences, Lund University, Skåne University Hospital, Malmö, Sweden *Correspondence
CARDIOVASCULAR RISK FACTOR CONTROL IN TYPE 2 DIABETES MELLITUS AND NEW TRIAL EVIDENCE *Peter M. Nilsson Department of Clinical Sciences, Lund University, Skåne University Hospital, Malmö, Sweden *Correspondence
Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol
 Inhibitors Drug Class Prior Authorization Protocol") Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has
Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has
Overview T2DM medications. Winnie Ho
 Overview T2DM medications Winnie Ho Diabetes in Australia 1.7 million Australians with diabetes, of these 85% have T2DM 2-fold excess risk CV death in patients with diabetes Risk factor for progression
Overview T2DM medications Winnie Ho Diabetes in Australia 1.7 million Australians with diabetes, of these 85% have T2DM 2-fold excess risk CV death in patients with diabetes Risk factor for progression
Cardiovascular Consequences of Diabetes Mellitus
 Cardiovascular Consequences of Diabetes Mellitus William J. Elliott, M.D., Ph.D. 05 MAY 18 Disclosure Statement The speaker s research and educational activities have been supported in the past (but NOT
Cardiovascular Consequences of Diabetes Mellitus William J. Elliott, M.D., Ph.D. 05 MAY 18 Disclosure Statement The speaker s research and educational activities have been supported in the past (but NOT
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy
 Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Evaluating the Cardiovascular Benefits of Antidiabetic Medications
 Evaluating the Cardiovascular Benefits of Antidiabetic Medications Target Audience: Pharmacists ACPE#: 0202-0000-18-054-L01-P Activity Type: Application-based Disclosures Stuart T. Haines has no relevant
Evaluating the Cardiovascular Benefits of Antidiabetic Medications Target Audience: Pharmacists ACPE#: 0202-0000-18-054-L01-P Activity Type: Application-based Disclosures Stuart T. Haines has no relevant
Heart Failure Management in T2 DM A Practical Approach. David Fitchett MD St Michael s Hospital Toronto
 Heart Failure Management in T2 DM A Practical Approach David Fitchett MD St Michael s Hospital Toronto Faculty: Faculty Disclosure David Fitchett MD,, FRCP(C) Associate Professor of Medicine, University
Heart Failure Management in T2 DM A Practical Approach David Fitchett MD St Michael s Hospital Toronto Faculty: Faculty Disclosure David Fitchett MD,, FRCP(C) Associate Professor of Medicine, University
Disclosures. Objectives. Bryan Cardiology Conference DM2 & Cardiovascular Outcome Trials 8/28/2017
 Bryan Cardiology Conference DM2 & Cardiovascular Outcome Trials Shannon Wakeley MD Complete Endocrinology 9/2/2017 Disclosures Speakers Bureau: Astra Zeneca, Sanofi, Abbvie, Boehringer-Ingelheim, Medtronic,
Bryan Cardiology Conference DM2 & Cardiovascular Outcome Trials Shannon Wakeley MD Complete Endocrinology 9/2/2017 Disclosures Speakers Bureau: Astra Zeneca, Sanofi, Abbvie, Boehringer-Ingelheim, Medtronic,
Keep Calm and Focus on the Evidence for the Management of Diabetes. Diabetes Update 2018
 Keep Calm and Focus on the Evidence for the Management of Diabetes Diabetes Update 2018 Nicole C.Pezzino, PharmD, BCACP, CDE Assistant Professor, Wilkes University Pharmacist, Weis Markets Nicole.pezzino@wilkes.edu
Keep Calm and Focus on the Evidence for the Management of Diabetes Diabetes Update 2018 Nicole C.Pezzino, PharmD, BCACP, CDE Assistant Professor, Wilkes University Pharmacist, Weis Markets Nicole.pezzino@wilkes.edu
DISCLOSURES. Learning objectives NAVIGATING THE TREATMENT OF TYPE 2 DIABETES: WHAT S NEW? Investigator Initiated Trial Support:
 NAVIGATING THE TREATMENT OF TYPE 2 DIABETES: WHAT S NEW? Jane E-B Reusch MD Professor of Medicine, Biochemistry and Bioengineering Associate Director Center for Women s Health Research University of Colorado
NAVIGATING THE TREATMENT OF TYPE 2 DIABETES: WHAT S NEW? Jane E-B Reusch MD Professor of Medicine, Biochemistry and Bioengineering Associate Director Center for Women s Health Research University of Colorado
Type 2 Diabetes Management: Case 1: Reducing Hypoglycemic Risk Case 2: Reducing Cardiovascular Risk
 Type 2 Diabetes Management M. Susan Burke, MD, FACP Clinical Associate Professor of Medicine Sidney Kimmel Medical College at Thomas Jefferson University Senior Advisor, Lankenau Medical Associates Lankenau
Type 2 Diabetes Management M. Susan Burke, MD, FACP Clinical Associate Professor of Medicine Sidney Kimmel Medical College at Thomas Jefferson University Senior Advisor, Lankenau Medical Associates Lankenau
What s New in Type 2 Diabetes? 2018 Diabetes Updates
 What s New in Type 2 Diabetes? 2018 Diabetes Updates Jessica Conklin, PharmD, PhC, BCACP, CDE, AAHIP Associate Professor, UNM College of Phar macy jeconklin@salud.unm.edu Luis Gonzales, PharmD, PhC UNM
What s New in Type 2 Diabetes? 2018 Diabetes Updates Jessica Conklin, PharmD, PhC, BCACP, CDE, AAHIP Associate Professor, UNM College of Phar macy jeconklin@salud.unm.edu Luis Gonzales, PharmD, PhC UNM
Incretin-based Therapies for Type 2 Diabetes Comparisons Between Glucagon-like Peptide-1 Receptor Agonists and Dipeptidyl Peptidase-4 Inhibitors
 Incretin-based Therapies for Type 2 Diabetes Comparisons Between Glucagon-like Peptide-1 Receptor Agonists and Dipeptidyl Peptidase-4 Inhibitors Timothy Bailey, MD, FACE, CPI Director, AMCR Institute,
Incretin-based Therapies for Type 2 Diabetes Comparisons Between Glucagon-like Peptide-1 Receptor Agonists and Dipeptidyl Peptidase-4 Inhibitors Timothy Bailey, MD, FACE, CPI Director, AMCR Institute,
6/1/2018. Lou Haenel, IV, DO, FACE, FACOI Endocrinology Roper St Francis Charleston, SC THE OMINOUS OCTET: HOW PATHOPHYSIOLOGY AND THERAPY MERGE
 Lou Haenel, IV, DO, FACE, FACOI Endocrinology Roper St Francis Charleston, SC THE OMINOUS OCTET: HOW PATHOPHYSIOLOGY AND THERAPY MERGE 1 2 3 Sulfonylureas Glipizide Glyburide Glimeperide 4 Metformin Gold
Lou Haenel, IV, DO, FACE, FACOI Endocrinology Roper St Francis Charleston, SC THE OMINOUS OCTET: HOW PATHOPHYSIOLOGY AND THERAPY MERGE 1 2 3 Sulfonylureas Glipizide Glyburide Glimeperide 4 Metformin Gold
Individualizing Management of T2DM in the Hospital Setting to Reduce Macro and Microvascular Complications
 Individualizing Management of T2DM in the Hospital Setting to Reduce Macro and Microvascular Complications This CME activity is provided by Integrity Continuing Education. This CEU/CNE activity is co-provided
Individualizing Management of T2DM in the Hospital Setting to Reduce Macro and Microvascular Complications This CME activity is provided by Integrity Continuing Education. This CEU/CNE activity is co-provided
The Flozins Quest for Clarity?
 The Flozins Quest for Clarity? Choosing Wisely with Academic Detailing 2018 ARE THEY THE REAL DEAL Disclosure statements The Academic Detailing Service is operated by Dalhousie Continuing Professional
The Flozins Quest for Clarity? Choosing Wisely with Academic Detailing 2018 ARE THEY THE REAL DEAL Disclosure statements The Academic Detailing Service is operated by Dalhousie Continuing Professional
The Diabetes Link to Heart Disease
 The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
Update Diabetes Therapie. Marc Y Donath
 Update Diabetes Therapie Marc Y Donath Recent CV outcome studies in Diabetes N Engl J Med. 2015 373:2117-28 (Empa-Reg outcome study) N Engl J Med. 2016 June 13 (LEADER trial) N Engl J Med. 2017 June 12
Update Diabetes Therapie Marc Y Donath Recent CV outcome studies in Diabetes N Engl J Med. 2015 373:2117-28 (Empa-Reg outcome study) N Engl J Med. 2016 June 13 (LEADER trial) N Engl J Med. 2017 June 12
Gli endpoint micro-vascolari nei trial di outcome cardiovascolare
 Gli endpoint micro-vascolari nei trial di outcome cardiovascolare Giorgio Sesti University Magna Graecia of Catanzaro ITALY Potenziali conflitti di interesse Il Prof Giorgio Sesti dichiara di aver ricevuto
Gli endpoint micro-vascolari nei trial di outcome cardiovascolare Giorgio Sesti University Magna Graecia of Catanzaro ITALY Potenziali conflitti di interesse Il Prof Giorgio Sesti dichiara di aver ricevuto
Peter Stein, MD Janssen Research and Development
 New Agents and Technologies in the Pipeline for the Treatment of Patients with Diabetes Peter Stein, MD Janssen Research and Development Agents in Phase 3 Development for T2DM Long-acting GLP-1 analogues
New Agents and Technologies in the Pipeline for the Treatment of Patients with Diabetes Peter Stein, MD Janssen Research and Development Agents in Phase 3 Development for T2DM Long-acting GLP-1 analogues
The Burden of the Diabetic Heart
 The Burden of the Diabetic Heart Dr. Ghaida Kaddaha (MBBS, MRCP-UK, FRCP-london) Diabetes Unit Rashid Hospital Dubai U.A.E Risk of CVD in Diabetes Morbidity and mortality from CVD is 2-4 fold higher than
The Burden of the Diabetic Heart Dr. Ghaida Kaddaha (MBBS, MRCP-UK, FRCP-london) Diabetes Unit Rashid Hospital Dubai U.A.E Risk of CVD in Diabetes Morbidity and mortality from CVD is 2-4 fold higher than
Type 2 Diabetes: Where Do We Start with Treatment? DIABETES EDUCATION. Diabetes Mellitus: Complications and Co-Morbid Conditions
 Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
THE EVOLUTION OF CLINICAL TRIALS IN T2DM: FROM TARGETING A1C TO TARGETING CARDIOVASCULAR OUTCOMES
 Learning Objectives 1) Evaluate the interrelationship between diabetes, glycemic control, and cardiovascular disease. 2) Examine the evolution of type 2 diabetes (T2DM) drug development and factors leading
Learning Objectives 1) Evaluate the interrelationship between diabetes, glycemic control, and cardiovascular disease. 2) Examine the evolution of type 2 diabetes (T2DM) drug development and factors leading
2016 Georgia Society of Health-System Pharmacists Summer Meeting CV Risk Factors: Emerging Data on Management of Type 2 Diabetes and Hypertension
 2016 Georgia Society of Health-System Pharmacists Summer Meeting CV Risk Factors: Emerging Data on Management of Type 2 Diabetes and Hypertension Jeff Langford, PharmD BCPS Clinical Pharmacy Specialist,
2016 Georgia Society of Health-System Pharmacists Summer Meeting CV Risk Factors: Emerging Data on Management of Type 2 Diabetes and Hypertension Jeff Langford, PharmD BCPS Clinical Pharmacy Specialist,
Empagliflozin: Role in Treatment Options for Patients with Type 2 Diabetes Mellitus
 Diabetes Ther (2017) 8:33 53 DOI 10.1007/s13300-016-0211-x REVIEW Empagliflozin: Role in Treatment Options for Patients with Type 2 Diabetes Mellitus John E. Anderson. Eugene E. Wright Jr.. Charles F.
Diabetes Ther (2017) 8:33 53 DOI 10.1007/s13300-016-0211-x REVIEW Empagliflozin: Role in Treatment Options for Patients with Type 2 Diabetes Mellitus John E. Anderson. Eugene E. Wright Jr.. Charles F.
Cardiovascular Management of a Patient with Diabetes
 Cardiovascular Management of a Patient with Diabetes Dr Jeremy Krebs Clinical Leader Endocrinology and Diabetes Wellington Hospital Summary People with diabetes take a lot of medication Compliance and
Cardiovascular Management of a Patient with Diabetes Dr Jeremy Krebs Clinical Leader Endocrinology and Diabetes Wellington Hospital Summary People with diabetes take a lot of medication Compliance and
Diabetes and New Meds for Cardiovascular Risk Reduction. F. Dwight Chrisman, MD, FACC. Disclosures: BI Boehringer Ingelheim speaker
 Diabetes and New Meds for Cardiovascular Risk Reduction F. Dwight Chrisman, MD, FACC Disclosures: BI Boehringer Ingelheim speaker 1 Prevalence of DM DM state specific prevalence 2006 4%-6% 6-8% 8-10% 10-12%
Diabetes and New Meds for Cardiovascular Risk Reduction F. Dwight Chrisman, MD, FACC Disclosures: BI Boehringer Ingelheim speaker 1 Prevalence of DM DM state specific prevalence 2006 4%-6% 6-8% 8-10% 10-12%
Making Sense of New DM Therapies and Technologies
 Making Sense of New DM Therapies and Technologies Sandra Indacochea Sobel, MD Clinical Assistant Professor of Medicine Clinical Chief of Endocrinology, UPMC Mercy Division of Endocrinology, Diabetes, and
Making Sense of New DM Therapies and Technologies Sandra Indacochea Sobel, MD Clinical Assistant Professor of Medicine Clinical Chief of Endocrinology, UPMC Mercy Division of Endocrinology, Diabetes, and
IDF Regions and global projections of the number of people with diabetes (20-79 years), 2013 and Diabetes Atlas -sixth Edition: IDF 2013
, 2013 and Diabetes Atlas -sixth Edition: IDF 2013") IDF Regions and global projections of the number of people with diabetes (20-79 years), 2013 and 2035 Diabetes Atlas -sixth Edition: IDF 2013 Diabetes Atlas -sixth Edition: IDF 2013 Chronic complications
IDF Regions and global projections of the number of people with diabetes (20-79 years), 2013 and 2035 Diabetes Atlas -sixth Edition: IDF 2013 Diabetes Atlas -sixth Edition: IDF 2013 Chronic complications
Disclosures. Diabetes and Cardiovascular Risk Management. Learning Objectives. Atherosclerotic Cardiovascular Disease
 Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Management of Type 2 Diabetes Mellitus. Heather Corn, MD, MS Endocrinology, Diabetes, and Metabolism
 Management of Type 2 Diabetes Mellitus Heather Corn, MD, MS Endocrinology, Diabetes, and Metabolism Disclosures Working for Intermountain Healthcare Some of the views represented are the opinion of ABIM-certified
Management of Type 2 Diabetes Mellitus Heather Corn, MD, MS Endocrinology, Diabetes, and Metabolism Disclosures Working for Intermountain Healthcare Some of the views represented are the opinion of ABIM-certified
Diabetic Management of the Cardiac Patient
 Diabetic Management of the Cardiac Patient Dr Peter A Senior BMedSci MBBS PhD FRCP(E) Associate Professor, Director Division of Endocrinology, University of Alberta Disclosures Grants/Research Support:
Diabetic Management of the Cardiac Patient Dr Peter A Senior BMedSci MBBS PhD FRCP(E) Associate Professor, Director Division of Endocrinology, University of Alberta Disclosures Grants/Research Support:
Disclaimers 22/03/2018. Role of DPP-4 Inhibitors, GLP-1 Agonists, and SGLT-2 Inhibitors in the treatment of Diabetes Mellitus Type 2
 Disclaimers Role of DPP-4 Inhibitors, GLP-1 Agonists, and SGLT-2 Inhibitors in the treatment of Diabetes Mellitus Type 2 I have not received money or gifts from medical device companies or from the pharmaceutical
Disclaimers Role of DPP-4 Inhibitors, GLP-1 Agonists, and SGLT-2 Inhibitors in the treatment of Diabetes Mellitus Type 2 I have not received money or gifts from medical device companies or from the pharmaceutical
New Therapies for Type 2 Diabetes
 New for Type 2 Diabetes Joshua J. Joseph, MD Assistant Professor of Medicine Division of Endocrinology, Diabetes and Metabolism The Ohio State University Wexner Medical Center Financial Disclosures: None
New for Type 2 Diabetes Joshua J. Joseph, MD Assistant Professor of Medicine Division of Endocrinology, Diabetes and Metabolism The Ohio State University Wexner Medical Center Financial Disclosures: None
New Therapies for Type 2 Diabetes
 New for Type 2 Diabetes Joshua J. Joseph, MD Assistant Professor of Medicine Division of Endocrinology, Diabetes and Metabolism The Ohio State University Wexner Medical Center Financial Disclosures: None
New for Type 2 Diabetes Joshua J. Joseph, MD Assistant Professor of Medicine Division of Endocrinology, Diabetes and Metabolism The Ohio State University Wexner Medical Center Financial Disclosures: None
Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes
 Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes Genetics, environment, and lifestyle (obesity, inactivity, poor diet) Impaired fasting glucose Decreased β-cell
Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes Genetics, environment, and lifestyle (obesity, inactivity, poor diet) Impaired fasting glucose Decreased β-cell
GLP-1 agonists. Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK
 GLP-1 agonists Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What do GLP-1 agonists do? Physiology of postprandial glucose regulation Meal ❶ ❷ Insulin Rising plasma
GLP-1 agonists Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What do GLP-1 agonists do? Physiology of postprandial glucose regulation Meal ❶ ❷ Insulin Rising plasma
SGLT2 Inhibitors Improve CardioRenal Outcomes in DM2-Get Rid of the Sugar
 SGLT2 Inhibitors Improve CardioRenal Outcomes in DM2-Get Rid of the Sugar David Balis, MD University of Texas Southwestern Medical Center Internal Medicine Grand Rounds 10/6/17 This is to acknowledge that
SGLT2 Inhibitors Improve CardioRenal Outcomes in DM2-Get Rid of the Sugar David Balis, MD University of Texas Southwestern Medical Center Internal Medicine Grand Rounds 10/6/17 This is to acknowledge that
Emergence of the New Classes of Compounds for Managing Heart Disease in Diabetes Mellitus
 Emergence of the New Classes of Compounds for Managing Heart Disease in Diabetes Mellitus Mikhail Kosiborod, MD Professor of Medicine (Cardiology) Saint Luke s Mid America Heart Institute University of
Emergence of the New Classes of Compounds for Managing Heart Disease in Diabetes Mellitus Mikhail Kosiborod, MD Professor of Medicine (Cardiology) Saint Luke s Mid America Heart Institute University of
Therapeutic strategy to reduce Glucagon secretion
 Clinical focus on glucagon: α-cell as a companion of β-cell Therapeutic strategy to reduce Glucagon secretion Sunghwan Suh Dong-A University Conflict of interest disclosure None Committee of Scientific
Clinical focus on glucagon: α-cell as a companion of β-cell Therapeutic strategy to reduce Glucagon secretion Sunghwan Suh Dong-A University Conflict of interest disclosure None Committee of Scientific