Cardiovascular Management of a Patient with Diabetes
|
|
|
- Hubert Johns
- 6 years ago
- Views:
Transcription
1 Cardiovascular Management of a Patient with Diabetes Dr Jeremy Krebs Clinical Leader Endocrinology and Diabetes Wellington Hospital
2 Summary People with diabetes take a lot of medication Compliance and Side Effects Most die from CVD Everyone is not created equal Calculate individual CVD risk Primary vs Secondary Prevention If you decide to treat GO HARD!
3 Summary Weight and Exercise Stop Smoking Glucose control Legacy effect Treat early Avoid hypoglycaemia Blood Pressure Aim 130/80mmHg But not too low Lipids Statin first line Primary vs Secondary consider your target Maybe Fibrate if TG v high Maybe Ezetimibe or Nicotinic acid Aspirin Yes for secondary prevention Probably not for primary unless high risk
4 Events per 100 Patient Yrs No Diabetes No Prior Event No Diabetes Prior Event Diabetes No Prior Event Diabetes Prior Event Haffner S. NEJM 1998:339;229-34

5 Bulugahapitiya U. Diabetic Med 2009:26;

6 All Things Are Not Created Equal





7
8 All Things Are Not Created Equal Mrs T 39yr Type 2 diabetes 11 years BMI 36 kg/m 2 Smoker BP 148/84 mmhg TC 4.9 mmol/l TG 2.3 mmol/l HDL 0.8 mmol/l LDL 2.8 mmol/l UACR 4.5 Mr T 63yr Type 2 diabetes 4 years BMI 29 kg/m 2 BP 132/76 mmhg TC 4.8 mmol/l TG 0.9 mmol/l HDL 1.4 mmol/l LDL 2.8 mmol/l UACR 1.8


9

10 Targets for CVD Risk Factors for Patients with Diabetes NZ Primary Care Guidelines 2012

11 NZ Primary Care Guidelines 2012
12 Smoking Baseline BMI vs Mortality 57 Prospective studies individuals Mean age 46 yrs Prospective Studies Collaboration. Lancet ;1083
13 Glucose Control
14 NZ Cohort Study (Get Checked) adjusted hazard ratio for CV events by HbA1c. n= n= 5667 first events Median follow up 2.4yrs HR 1.08 ( ) per 1% HbA1c Elley CR. Diabetic Med 2008.
15 HbA 1c (%) 9 8 UKPDS HbA 1c cross-sectional, median values Conventional 7 Intensive % upper limit of normal range Years from randomisation
 25% for microvascular endpoints (p=0.0099) 24% for cataract extraction (p=0.046) 21% for retinopathy at twelve years (p=0.")
16 UKPDS Glucose Control Study Summary 12% for any diabetes related endpoint (p=0.029) 16% for myocardial infarction (p=0.052) 25% for microvascular endpoints (p=0.0099) 24% for cataract extraction (p=0.046) 21% for retinopathy at twelve years (p=0.015) 33% for albuminuria at twelve years (p= )
17 Legacy Effect of Earlier Glucose Control After median 8.5 years post-trial follow-up Aggregate Endpoint Any diabetes related endpoint RRR: 12% 9% P: Microvascular disease RRR: 25% 24% P: Myocardial infarction RRR: 16% 15% P: All-cause mortality RRR: 6% 13% P: RRR = Relative Risk Reduction, P = Log Rank
18 Recent Trials of Glycaemic Control Advance, Accord 10 year post diagnosis, middle age Despite intensive HBA1c management have failed to show CVD benefit
19 ACCORD Study The Action to Control Cardiovascular Risk in Diabetes Study Group N=10,000 1/3 already on insulin 1/3 prevalent CVD events Mean Age 62 Diabetes for 10 years HbA1c 8.3 Strategy of (ultra) intensive glycaemic control aiming for HbA1c 6 (achieved 6.3)
20 ACCORD Study The mean difference during the trial was 1.1%
21 Accord June 2008 Primary Outcome: First occurrence of nonfatal MI, stroke or death from Cardiovascular cause 352 vs 371 events HR 0.9 ( , p=0.16)
22 Accord Study Primary and Secondary Outcomes Intensive N (%) Standard N (%) HR (95% CI) P Primary 352 (6.86) 371 (7.23) 0.90 ( ) 0.16 Secondary Mortality 257 (5.01) 203 (3.96) 1.22 ( ) 0.04 Nonfatal MI 186 (3.63) 235 (4.59) 0.76 ( ) Nonfatal Stroke 67 (1.31) 61 (1.19) 1.06 ( ) 0.74 CVD Death 135 (2.63) 94 (1.83) 1.35 ( ) 0.02 CHF 152 (2.96) 124 (2.42) 1.18 ( ) 0.17
23 % of Participants Incidence of Hypoglycaemia (first event) per Year st 2nd 3rd 4th 5th 6th Year Postrandomization Intensive Standard






24 Major Targeted Sites of Oral Drug Classes Liver Pancreas Impaired insulin secretion Sulfonylureas GLP-1 mimetics DPP-4 inhibitors Muscle and fat Hepatic glucose overproduction Biguanides TZDs GLP-1 mimetics DPP-4 inhibitors Glucose level Gut Glucose absorption α-glucosidase inhibitors Biguanides Insulin resistance TZDs Biguanides DPP-4=dipeptidyl peptidase 4; TZDs=thiazolidinediones. Buse JB et al. In: Williams Textbook of Endocrinology. 10th ed. Philadelphia: WB Saunders; 2003: ; DeFronzo RA. Ann Intern Med. 1999;131: ; Inzucchi SE. JAMA 2002;287: ; Porte D et al. Clin Invest Med. 1995;18:
25 Type 2 Diabetes Algorithm Diet and Lifestyle No hypos Oral agent But weight gain, heart Good evidence failure, fractures. But weight gain,?ihd risk hypos Oral agent No hypos But GI side effects Metformin Weight neutral Oral agent No hypos Weight loss No hypos But Injectable SU Glitazone Acarbose Sitagliptin Exenetide Insulin
26 Blood Pressure

27 UKPDS

28 ACCORD BP trial

29
30 Lipids
31 Dyslipidaemia in Diabetes Typical dyslipidaemia in type 2 diabetes Elevated Triglycerides Suppressed HDL cholesterol Total and LDL cholesterol more variable So TREAT THE TG AND HDL
32 FIELD Study Fenofibrate vs Placebo N=9795 age 50-75yrs 2131 pre CVD 7664 no CVD Not on a statin (17% placebo and 8% fibrate group started) Primary Outcome Death or nonfatal MI RR 0.89 ( ) Total CV events. Death, MI, Stroke, Revascularisation Lancet 2005: 366;
33 FIELD Study
34 Statins in Diabetes Secondary Prevention Yes Go for it! Let the cardiologist zealots drive your LDL down! Primary Prevention Yes Maybe Listen to your heart (and your Endocrinologist)
35 CARDS Study Primary prevention study But! Retinopathy, albuminuria, smoking or hypertension 2838 patients 40-75yrs with diabetes Atorvastatin vs Placebo LDL<4.14 TG<6.78 Colhoun H. Lancet 2004: 364;685
36 CARDS study Colhoun H. Lancet 2004: 364;685
37 Statins in Diabetes Primary prevention studies Large Subgroups with Diabetes ALLHAT Pravastatin NS reduction in death or MI HPS Simvastatin Sig reduction both 1 and 2 ASCOT Atorvastatin NS
38 LDL How Low Do You Go? Primary Prevention Trials Secondary Prevention Trials
39 Add on to Statins Fibrates Maybe if TG high Ezetimibe Maybe if LDL still high Lowers LDL well in combination No outcome data Nicotinic Acid Maybe if LDL high and HDL low No outcome data

40 IMPROVE-IT Study

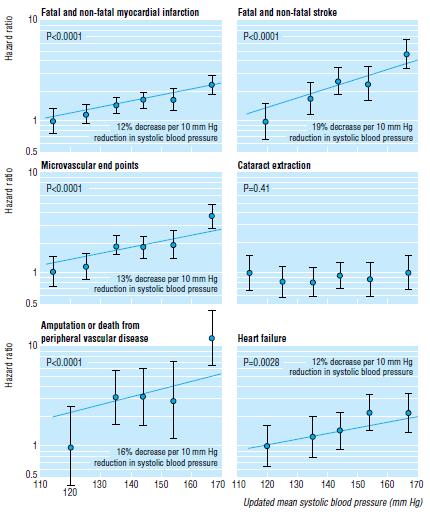
41 The Whole Package
42 Cumulative incidence of death (%) Steno-2 Post Trial: Mortality of any cause 70 Log-rank P= Years of follow-up Numbers at risk Conventional Intensive Gaede et al. NEJM 2008
43 Cumulative incidence of CVD events (%) Steno-2 Post Trial: Any CVD events Cumulative incidence of patients with a major CVD event during follow-up Log-rank P= Years of follow-up Numbers at risk Conventional Intensive Gaede et al. NEJM 2008
44 Steno 2 Number of microalbuminuric patients with type 2 diabetes needed to treat for 13 years to prevent one... Death Cardiovascular death Major cardiovascular event Progression to nephropathy Dialysis Laser treatment 5 patients 8 patients 3 patients 5 patients 16 patients 7 patients (from Gaede et al 2008 Steno 2, 13 year study)


45 Spot the Difference
46 Summary People with diabetes take a lot of medication Compliance and Side Effects Most die from CVD Everyone is not created equal Calculate individual CVD risk Primary vs Secondary Prevention If you decide to treat GO HARD!
47 Summary Weight and Exercise Stop Smoking Glucose control Legacy effect Treat early Avoid hypoglycaemia Blood Pressure Aim 130/80mmHg But not too low Lipids Statin first line Primary vs Secondary consider your target Maybe Fibrate if TG v high Maybe Ezetimibe or Nicotinic acid Aspirin Yes for secondary prevention Probably not for primary unless high risk
48
49 UKPDS: Improving HbA 1c Control Reduced Diabetes-Related Complications EVERY 1% reduction in HbA 1c Relative Risk N=3642 Diabetesrelated deaths REDUCED RISK (P<0.0001) 1% Myocardial infarctions Microvascular complications Amputations or deaths from peripheral vascular disorders UKPDF=United Kingdom Prospective Diabetes Study. Data adjusted for age, sex, and ethnic group, expressed for white men aged years at diagnosis and with mean duration of diabetes of 10 years. Stratton IM et al. UKPDS 35. BMJ 2000;321:
50 Management Goals for Diabetes Glycaemic control HbA1c % Blood Pressure Lipids NZ Guidelines Group: Dec 2002 <130/80 (125/75) TC<4.0mmol/L (LDL<2.0, HDL>1.0) TG<1.7mmol/L
51
52 Adults, % Less than 50% of Adults With Type 2 Diabetes Have Achieved HbA 1c Goals 60 US Population NHANES III ( ) (n=1204) NHANES (n=370) HbA 1c level <7% Blood pressure <130/80 mmhg Total cholesterol <200 mg/dl Achieved all 3 treatment goals CV Risk Factors NHANES=National Health and Nutrition Examination Survey of a US population. Adapted from Saydah SH et al. JAMA. 2004;291:
53 Antihyperglycemic Agents in Type 2 Diabetes Class A1C Reductio n Severe Hypoglycemia Weight Chang e CVD Risk Factor Improvement Dosing (times/day) Diabetes Comorbidity Contraindication s Metformin 1.5 No Neutral Minimal 1-2 Kidney, liver NPH, Glargine, Detemir Yes Gain TG R, Lispro, Aspart, Glulisine Yes Gain TG 1-2, Injected 1-4, Injected None None Glipizide ER, Glimepiride 1.5 Yes Gain None 1 None Pioglitazone No Gain Lipids, BP 1 CHF, liver Repaglinide Yes Gain None 3 None Nateglinide Rare Gain None 3 None Acarbose, Miglitol No Neutral Minimal 3 None Pramlintide No Loss Exenatide No Loss w/ weight loss w/ weight loss 3, Injected None 2, Injected Kidney Sitagliptin, saxagliptin No Neutral Minimal 1 None Adapted from: Nathan DM, et al. Diabetes Care. 2009; 32: ADA. Diabetes Care. 2010;33:S11-S61. WelChol PI. 1/2008. Cycloset PI. 10/2010. Victoza PI. 1/2010. Colesevelam ~0.5 No Neutral LDL 1-2 Severe TG s
54 Risks vs Benefits of Glucose Lowering therapy Bergenstal R et al. Am J Med 2010;123:374

55 From: Effect of Lower Targets for Blood Pressure and LDL Cholesterol on Atherosclerosis in Diabetes: Title and subtitle BreakThe SANDS Randomized Trial JAMA. 2008;299(14): doi: /jama Figure Legend: For intimal medial thickness, n = 454; P value <.001. For left ventricular mass index, n = 402; P value =.17. The no change category was defined as ± 0.01 mm for intimal medial thickness or ± 0.05 gm/m 2.7 for left ventricular mass index. P is for trend by each treatment group for intimal medial thickness and left ventricular mass index. Date of download: 6/7/2012 Copyright 2012 American Medical Association. All rights reserved.
56
57 Hazard ratios for the primary end point by subgroup of achieved LDL cholesterol (adjusted for age, sex, baseline calculated LDL cholesterol, diabetes, and prior MI) in the Pravastatin or Atorvastatin Evaluation and Infection Therapy-Thrombolysis in Myocardial Infarction 22 trial. Nesto R W Clin Diabetes 2008;26:8-13 Copyright 2011 American Diabetes Association, Inc.
58
59 Incidence per 1,000 patient-years Incidence rates of MI and microvascular endpoints by mean HbA 1c : UKPDS Microvascular disease 40 Myocardial infarction Updated mean HbA 1c (%) Study population: white, Asian Indian, and Afro-Caribbean UKPDS patients (n = 4,585) Adjusted for age, sex, and ethnic group Error bars = 95% CI Adapted from Stratton IM, et al. Br Med J 2000; 321:

60 Bulugahapitiya U. Diabetic Med 2009:26;

61 Success Comes From Using the Most Appropriate Tools
Diabetes Mellitus: Implications of New Clinical Trials and New Medications
 Diabetes Mellitus: Implications of New Clinical Trials and New Medications Estimates of Diagnosed Diabetes in Adults, 2005 Alka M. Kanaya, MD Asst. Professor of Medicine UCSF, Primary Care CME October
Diabetes Mellitus: Implications of New Clinical Trials and New Medications Estimates of Diagnosed Diabetes in Adults, 2005 Alka M. Kanaya, MD Asst. Professor of Medicine UCSF, Primary Care CME October
Diabete: terapia nei pazienti a rischio cardiovascolare
 Diabete: terapia nei pazienti a rischio cardiovascolare Giorgio Sesti Università Magna Graecia di Catanzaro Cardiovascular mortality in relation to diabetes mellitus and a prior MI: A Danish Population
Diabete: terapia nei pazienti a rischio cardiovascolare Giorgio Sesti Università Magna Graecia di Catanzaro Cardiovascular mortality in relation to diabetes mellitus and a prior MI: A Danish Population
Diabetes Treatment Update
 Diabetes Treatment Update Timothy C. Evans, MD PhD FACP University of Washington Department of Medicine Disclosure: Dr. Evans has no significant financial interest in any of the products or manufacturers
Diabetes Treatment Update Timothy C. Evans, MD PhD FACP University of Washington Department of Medicine Disclosure: Dr. Evans has no significant financial interest in any of the products or manufacturers
The Burden of the Diabetic Heart
 The Burden of the Diabetic Heart Dr. Ghaida Kaddaha (MBBS, MRCP-UK, FRCP-london) Diabetes Unit Rashid Hospital Dubai U.A.E Risk of CVD in Diabetes Morbidity and mortality from CVD is 2-4 fold higher than
The Burden of the Diabetic Heart Dr. Ghaida Kaddaha (MBBS, MRCP-UK, FRCP-london) Diabetes Unit Rashid Hospital Dubai U.A.E Risk of CVD in Diabetes Morbidity and mortality from CVD is 2-4 fold higher than
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy
 Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Comprehensive Diabetes Treatment
 Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
Diabetes Mellitus: A Cardiovascular Disease
 Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
Eugene Barrett M.D., Ph.D. University of Virginia 6/18/2007. Diagnosis and what is it Glucose Tolerance Categories FPG
 Diabetes Mellitus: Update 7 What is the unifying basis of this vascular disease? Eugene J. Barrett, MD, PhD Professor of Internal Medicine and Pediatrics Director, Diabetes Center and GCRC Health System
Diabetes Mellitus: Update 7 What is the unifying basis of this vascular disease? Eugene J. Barrett, MD, PhD Professor of Internal Medicine and Pediatrics Director, Diabetes Center and GCRC Health System
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES
 ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable?
 Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
The Diabetes Link to Heart Disease
 The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
Practical Diabetes. Nic Crook. (and don t use so many charts) Kuirau Specialists 1239 Ranolf Street Rotorua. Rotorua Hospital Private Bag 3023 Rotorua
 Kuirau Specialists 1239 Ranolf Street Rotorua. Rotorua Hospital Private Bag 3023 Rotorua") Practical Diabetes (and don t use so many charts) Nic Crook Rotorua Hospital Private Bag 3023 Rotorua Kuirau Specialists 1239 Ranolf Street Rotorua Worldwide rates of diabetes mellitus: predictions 80
Practical Diabetes (and don t use so many charts) Nic Crook Rotorua Hospital Private Bag 3023 Rotorua Kuirau Specialists 1239 Ranolf Street Rotorua Worldwide rates of diabetes mellitus: predictions 80
Why is Earlier and More Aggressive Treatment of T2 Diabetes Better?
 Blood glucose (mmol/l) Why is Earlier and More Aggressive Treatment of T2 Diabetes Better? Disclosures Dr Kennedy has provided CME, been on advisory boards or received travel or conference support from:
Blood glucose (mmol/l) Why is Earlier and More Aggressive Treatment of T2 Diabetes Better? Disclosures Dr Kennedy has provided CME, been on advisory boards or received travel or conference support from:
Initiating Insulin in Primary Care for Type 2 Diabetes Mellitus. Dr Manish Khanolkar, Diabetologist, Auckland Diabetes Centre
 Initiating Insulin in Primary Care for Type 2 Diabetes Mellitus Dr Manish Khanolkar, Diabetologist, Auckland Diabetes Centre Outline How big is the problem? Natural progression of type 2 diabetes What
Initiating Insulin in Primary Care for Type 2 Diabetes Mellitus Dr Manish Khanolkar, Diabetologist, Auckland Diabetes Centre Outline How big is the problem? Natural progression of type 2 diabetes What
Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes
 Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes Genetics, environment, and lifestyle (obesity, inactivity, poor diet) Impaired fasting glucose Decreased β-cell
Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes Genetics, environment, and lifestyle (obesity, inactivity, poor diet) Impaired fasting glucose Decreased β-cell
Diabetes Mellitus in Older Adults. Presenter Disclosure Information
 Diabetes Mellitus in Older Adults Medha Munshi, M.D. Joslin Diabetes Center Beth Israel Deaconess Medical Center Harvard Medical School Presenter Disclosure Information Medha Munshi Research grant from
Diabetes Mellitus in Older Adults Medha Munshi, M.D. Joslin Diabetes Center Beth Israel Deaconess Medical Center Harvard Medical School Presenter Disclosure Information Medha Munshi Research grant from
Ischemic Heart and Cerebrovascular Disease. Harold E. Lebovitz, MD, FACE Kathmandu November 2010
 Ischemic Heart and Cerebrovascular Disease Harold E. Lebovitz, MD, FACE Kathmandu November 2010 Relationships Between Diabetes and Ischemic Heart Disease Risk of Cardiovascular Disease in Different Categories
Ischemic Heart and Cerebrovascular Disease Harold E. Lebovitz, MD, FACE Kathmandu November 2010 Relationships Between Diabetes and Ischemic Heart Disease Risk of Cardiovascular Disease in Different Categories
The Clinical Unmet need in the patient with Diabetes and ACS
 The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
Clinical Overview of Combination Therapy with Sitagliptin and Metformin
 Clinical Overview of Combination Therapy with Sitagliptin and Metformin 1 Contents Pathophysiology of type 2 diabetes and mechanism of action of sitagliptin Clinical data overview of sitagliptin: Monotherapy
Clinical Overview of Combination Therapy with Sitagliptin and Metformin 1 Contents Pathophysiology of type 2 diabetes and mechanism of action of sitagliptin Clinical data overview of sitagliptin: Monotherapy
Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes
 Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes Obesity (BMI 30 kg/m 2 ) 1994 2000 2009 No Data 26.0% Diabetes 1994 2000 2009
Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes Obesity (BMI 30 kg/m 2 ) 1994 2000 2009 No Data 26.0% Diabetes 1994 2000 2009
How to Reduce CVD Complications in Diabetes?
 How to Reduce CVD Complications in Diabetes? Chaicharn Deerochanawong M.D. Diabetes and Endocrinology Unit Department of Medicine Rajavithi Hospital, Ministry of Public Health Framingham Heart Study 30-Year
How to Reduce CVD Complications in Diabetes? Chaicharn Deerochanawong M.D. Diabetes and Endocrinology Unit Department of Medicine Rajavithi Hospital, Ministry of Public Health Framingham Heart Study 30-Year
Abbreviations DPP-IV dipeptidyl peptidase IV DREAM Diabetes REduction Assessment with ramipril and rosiglitazone
 Index Abbreviations DPP-IV dipeptidyl peptidase IV DREAM Diabetes REduction Assessment with ramipril and rosiglitazone Medication GAD glutamic acid decarboxylase GLP-1 glucagon-like peptide 1 NPH neutral
Index Abbreviations DPP-IV dipeptidyl peptidase IV DREAM Diabetes REduction Assessment with ramipril and rosiglitazone Medication GAD glutamic acid decarboxylase GLP-1 glucagon-like peptide 1 NPH neutral
Joslin Diabetes Center Joslin Diabetes Forum 2013: The Impact of Comorbidities on Glucose Control Scenario 2: Reduced Renal Function
 Scenario 2: Reduced Renal Function 62 y.o. white man with type 2 diabetes for 18 years Hypertension and hypercholesterolemia Known proliferative retinopathy Current medications: Metformin 1000 mg bid Glyburide
Scenario 2: Reduced Renal Function 62 y.o. white man with type 2 diabetes for 18 years Hypertension and hypercholesterolemia Known proliferative retinopathy Current medications: Metformin 1000 mg bid Glyburide
CURRENT CONTROVERSIES IN DIABETES CARE
 CURRENT CONTROVERSIES IN DIABETES CARE Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Diabetes Mellitus: U.S. Impact
CURRENT CONTROVERSIES IN DIABETES CARE Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Diabetes Mellitus: U.S. Impact
Multiple Small Feedings of the Mind: Diabetes. Sonja K Fredrickson, MD, BC-ADM March 7, 2014
 Multiple Small Feedings of the Mind: Diabetes Sonja K Fredrickson, MD, BC-ADM March 7, 2014 Question 1: Setting A1c Goals Describe the evidence based approach to determining the target HgbA1c in different
Multiple Small Feedings of the Mind: Diabetes Sonja K Fredrickson, MD, BC-ADM March 7, 2014 Question 1: Setting A1c Goals Describe the evidence based approach to determining the target HgbA1c in different
Management of Type 2 Diabetes
 Management of Type 2 Diabetes Pathophysiology Insulin resistance and relative insulin deficiency/ defective secretion Not immune mediated No evidence of β cell destruction Increased risk with age, obesity
Management of Type 2 Diabetes Pathophysiology Insulin resistance and relative insulin deficiency/ defective secretion Not immune mediated No evidence of β cell destruction Increased risk with age, obesity
Diabetes new challenges, new agents, new order
 Diabetes new challenges, new agents, new order Ken Earle St Georges University Hospitals NHS Foundation Trust Overview Cardiovascular disease unmet needs Treating evident and residual risk Integrating
Diabetes new challenges, new agents, new order Ken Earle St Georges University Hospitals NHS Foundation Trust Overview Cardiovascular disease unmet needs Treating evident and residual risk Integrating
Mae Sheikh-Ali, M.D. Assistant Professor of Medicine Division of Endocrinology University of Florida College of Medicine- Jacksonville
 Mae Sheikh-Ali, M.D. Assistant Professor of Medicine Division of Endocrinology University of Florida College of Medicine- Jacksonville Pathogenesis of Diabetes Mellitus (DM) Criteria for the diagnosis
Mae Sheikh-Ali, M.D. Assistant Professor of Medicine Division of Endocrinology University of Florida College of Medicine- Jacksonville Pathogenesis of Diabetes Mellitus (DM) Criteria for the diagnosis
Dr Tahseen A. Chowdhury Royal London Hospital. New Guidelines in Diabetes: NICE or Nasty?
 Dr Tahseen A. Chowdhury Royal London Hospital New Guidelines in Diabetes: NICE or Nasty? I have no conflicts of interest I do not undertake talks / advisory bodies / research for any pharma company Consultant
Dr Tahseen A. Chowdhury Royal London Hospital New Guidelines in Diabetes: NICE or Nasty? I have no conflicts of interest I do not undertake talks / advisory bodies / research for any pharma company Consultant
Vipul Lakhani, MD Oregon Medical Group Endocrinology
 Vipul Lakhani, MD Oregon Medical Group Endocrinology Disclosures None Objectives Be able to diagnose diabetes and assess control Be able to identify appropriate classes of medications for diabetes treatment
Vipul Lakhani, MD Oregon Medical Group Endocrinology Disclosures None Objectives Be able to diagnose diabetes and assess control Be able to identify appropriate classes of medications for diabetes treatment
Type 2 Diabetes: Where Do We Start with Treatment? DIABETES EDUCATION. Diabetes Mellitus: Complications and Co-Morbid Conditions
 Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
ATP IV: Predicting Guideline Updates
 Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Joslin Diabetes Center Advances in Diabetes and Thyroid Disease 2013 Noninsulin Treatment of Diabetes: What the PCP Needs to Know
 Non Insulin Treatment of Type 2 Diabetes: What the PCP Needs to Know Martin J. Abrahamson, MD Senior Vice President for Medical Affairs Joslin Diabetes Center Associate Professor of Medicine Harvard Medical
Non Insulin Treatment of Type 2 Diabetes: What the PCP Needs to Know Martin J. Abrahamson, MD Senior Vice President for Medical Affairs Joslin Diabetes Center Associate Professor of Medicine Harvard Medical
Mr Rab Burtun. Dr David Kim. 8:30-10:30 WS #2: Diabetes Basic 11:00-13:00 WS #9: Diabetes Basic (Repeated)
") Dr David Kim Endocrinologist and General Physician Waitemata DHB and Apollo Specialist Clinic Albany Auckland Mr Rab Burtun Diabetes Nurse Specialist Waitemata DHB Waitakere Hospital Auckland 8:30-10:30
Dr David Kim Endocrinologist and General Physician Waitemata DHB and Apollo Specialist Clinic Albany Auckland Mr Rab Burtun Diabetes Nurse Specialist Waitemata DHB Waitakere Hospital Auckland 8:30-10:30
Volume 2; Number 14 September 2008 NICE CLINICAL GUIDELINE 66: TYPE 2 DIABETES THE MANAGEMENT OF TYPE 2 DIABETES (MAY 2008)
") Volume 2; Number 14 September 2008 NICE CLINICAL GUIDELINE 66: TYPE 2 DIABETES THE MANAGEMENT OF TYPE 2 DIABETES (MAY 2008) The purpose of this special edition of the PACE Bulletin is to summarize the
Volume 2; Number 14 September 2008 NICE CLINICAL GUIDELINE 66: TYPE 2 DIABETES THE MANAGEMENT OF TYPE 2 DIABETES (MAY 2008) The purpose of this special edition of the PACE Bulletin is to summarize the
Pharmacology Updates. Quang T Nguyen, FACP, FACE, FTOS 11/18/17
 Pharmacology Updates Quang T Nguyen, FACP, FACE, FTOS 11/18/17 14 Classes of Drugs Available for the Treatment of Type 2 DM in the USA ### Class A1c Reduction Hypoglycemia Weight Change Dosing (times/day)
Pharmacology Updates Quang T Nguyen, FACP, FACE, FTOS 11/18/17 14 Classes of Drugs Available for the Treatment of Type 2 DM in the USA ### Class A1c Reduction Hypoglycemia Weight Change Dosing (times/day)
Wayne Gravois, MD August 6, 2017
 Wayne Gravois, MD August 6, 2017 Americans with Diabetes (Millions) 40 30 Source: National Diabetes Statistics Report, 2011, 2017 Millions 20 10 0 1980 2009 2015 2007 - $174 Billion 2015 - $245 Billion
Wayne Gravois, MD August 6, 2017 Americans with Diabetes (Millions) 40 30 Source: National Diabetes Statistics Report, 2011, 2017 Millions 20 10 0 1980 2009 2015 2007 - $174 Billion 2015 - $245 Billion
01/09/2017. Outline. SGLT 2 inhibitor? Diabetes Patients: Complex and Heterogeneous. Association between diabetes and cardiovascular events
 MICROVASCULAR COMPLICATIONS Incidence of outcome g 1 Cardioprotective Effects of SGLT2s Relevant for Which T2 Diabetes Patient? SGLT 2 inhibitor? 58 year old, waist circumference 5 cm, PMH: IHD On statin,
MICROVASCULAR COMPLICATIONS Incidence of outcome g 1 Cardioprotective Effects of SGLT2s Relevant for Which T2 Diabetes Patient? SGLT 2 inhibitor? 58 year old, waist circumference 5 cm, PMH: IHD On statin,
Type 2 Diabetes Mellitus 2011
 2011 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Diabetes Mellitus Diagnosis 2011 Diabetes Mellitus Fasting Glucose
2011 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Diabetes Mellitus Diagnosis 2011 Diabetes Mellitus Fasting Glucose
NEW DIABETES CARE MEDICATIONS
 NEW DIABETES CARE MEDICATIONS James Bonucchi DO, ECNU, FACE Adult Medicine and Endocrinology Specialists Disclosures Speakers bureau Sanofi AZ BI Diabetes Diabetes cost ADA 2017 data Ever increasing disorder.
NEW DIABETES CARE MEDICATIONS James Bonucchi DO, ECNU, FACE Adult Medicine and Endocrinology Specialists Disclosures Speakers bureau Sanofi AZ BI Diabetes Diabetes cost ADA 2017 data Ever increasing disorder.
T2 Diabetes in Sep-16. Stephen Leow Disclosures. Why do we treat diabetes? Agenda. Targets
 Stephen Leow Disclosures I have received honoraria, sat on the advisory boards or received grants from Novo Nordisk, Sanofi Aventis, Eli Lilly, Boehringer Ingleheim, Jansenn Cilag, Mundipharma, BioCSL,
Stephen Leow Disclosures I have received honoraria, sat on the advisory boards or received grants from Novo Nordisk, Sanofi Aventis, Eli Lilly, Boehringer Ingleheim, Jansenn Cilag, Mundipharma, BioCSL,
American Diabetes Association 2018 Guidelines Important Notable Points
 American Diabetes Association 2018 Guidelines Important Notable Points The Standards of Medical Care in Diabetes-2018 by ADA include the most current evidencebased recommendations for diagnosing and treating
American Diabetes Association 2018 Guidelines Important Notable Points The Standards of Medical Care in Diabetes-2018 by ADA include the most current evidencebased recommendations for diagnosing and treating
Physiology of Normoglycemia
 Case 1 45 year-old male patient seen at the clinic (Medicine). Workplace stress (financial analyst); occasionally goes jogging. Two-year duration of T2DM. No previous cardiovascular events. Coexisting
Case 1 45 year-old male patient seen at the clinic (Medicine). Workplace stress (financial analyst); occasionally goes jogging. Two-year duration of T2DM. No previous cardiovascular events. Coexisting
The Metabolic Syndrome: Is It A Valid Concept? YES
 The Metabolic Syndrome: Is It A Valid Concept? YES Congress on Diabetes and Cardiometabolic Health Boston, MA April 23, 2013 Edward S Horton, MD Joslin Diabetes Center Harvard Medical School Boston, MA
The Metabolic Syndrome: Is It A Valid Concept? YES Congress on Diabetes and Cardiometabolic Health Boston, MA April 23, 2013 Edward S Horton, MD Joslin Diabetes Center Harvard Medical School Boston, MA
SIMPLICITY IN T2DM MANAGEMENT WITH DPP4 INHIBITORS: SPECIAL POPULATION
 SIMPLICITY IN T2DM MANAGEMENT WITH DPP4 INHIBITORS: SPECIAL POPULATION DR ROSE ZHAO-WEI TING ( 丁昭慧醫生 ) MBBS (HK), MRCP (UK), FHKCP, FHKAM (MEDICINE) Specialist in Endocrinology, Diabetes and Metabolism
SIMPLICITY IN T2DM MANAGEMENT WITH DPP4 INHIBITORS: SPECIAL POPULATION DR ROSE ZHAO-WEI TING ( 丁昭慧醫生 ) MBBS (HK), MRCP (UK), FHKCP, FHKAM (MEDICINE) Specialist in Endocrinology, Diabetes and Metabolism
Professor Rudy Bilous James Cook University Hospital
 Professor Rudy Bilous James Cook University Hospital Rate per 100 patient years Rate per 100 patient years 16 Risk of retinopathy progression 16 Risk of developing microalbuminuria 12 12 8 8 4 0 0 5 6
Professor Rudy Bilous James Cook University Hospital Rate per 100 patient years Rate per 100 patient years 16 Risk of retinopathy progression 16 Risk of developing microalbuminuria 12 12 8 8 4 0 0 5 6
Vascular complications
 Vascular complications December 8, 2018 Faculty Disclosure Faculty: Kim Connelly, MBBS, PhD, FRACP Associate Professor of Medicine, University of Toronto Cardiologist, St. Michael s Hospital Relationships
Vascular complications December 8, 2018 Faculty Disclosure Faculty: Kim Connelly, MBBS, PhD, FRACP Associate Professor of Medicine, University of Toronto Cardiologist, St. Michael s Hospital Relationships
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications
 Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009
 The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009 Learning Objectives 1. Understand the role of statin therapy in the primary and secondary prevention of stroke 2. Explain
The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009 Learning Objectives 1. Understand the role of statin therapy in the primary and secondary prevention of stroke 2. Explain
Review of guidelines for management of dyslipidemia in diabetic patients
 2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
A Fork in the Road: Navigating Through New Terrain
 A Fork in the Road: Navigating Through New Terrain Carol Hatch Wysham, MD Clinical Associate Professor of Medicine University of Washington School of Medicine Section Head, Rockwood Center for Diabetes
A Fork in the Road: Navigating Through New Terrain Carol Hatch Wysham, MD Clinical Associate Professor of Medicine University of Washington School of Medicine Section Head, Rockwood Center for Diabetes
Alia Gilani Health Inequalities Pharmacist
 Alia Gilani Health Inequalities Pharmacist THE SOUTH ASIAN HEALTH FOUNDATION (U.K.) (Registered Charity No. 1073178) 1. Case Study 2. Factors influencing prescribing 3. Special Considerations 4. Prescribing
Alia Gilani Health Inequalities Pharmacist THE SOUTH ASIAN HEALTH FOUNDATION (U.K.) (Registered Charity No. 1073178) 1. Case Study 2. Factors influencing prescribing 3. Special Considerations 4. Prescribing
Type 2 Diabetes. Treat to: limit complications maintain quality of life Improve survival
 Type 2 Diabetes Treat to: limit complications maintain quality of life Improve survival 1 Criteria for the diagnosis of diabetes 1. HbA1C 6.5% (rounded to 50mmol/mol). 2. FPG 7.0 mmol/l. 3. 2-h plasma
Type 2 Diabetes Treat to: limit complications maintain quality of life Improve survival 1 Criteria for the diagnosis of diabetes 1. HbA1C 6.5% (rounded to 50mmol/mol). 2. FPG 7.0 mmol/l. 3. 2-h plasma
CURRENT ISSUES IN DIABETES MANAGEMENT. Screening for Diabetes Advantages of HbA1c as a Diagnostic Test. Diagnosis of Diabetes 2013
 CURRENT ISSUES IN DIABETES MANAGEMENT Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening for Diabetes 2013 BMI
CURRENT ISSUES IN DIABETES MANAGEMENT Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening for Diabetes 2013 BMI
A Practical Approach to the Use of Diabetes Medications
 A Practical Approach to the Use of Diabetes Medications Juan Pablo Frias, M.D., FACE President, National Research Institute, Los Angles, CA Clinical Faculty, University of California, San Diego, CA OUTLINE
A Practical Approach to the Use of Diabetes Medications Juan Pablo Frias, M.D., FACE President, National Research Institute, Los Angles, CA Clinical Faculty, University of California, San Diego, CA OUTLINE
Disclosures. Diabetes and Cardiovascular Risk Management. Learning Objectives. Atherosclerotic Cardiovascular Disease
 Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
TREATMENT OF DIABETES AFTER METFORMIN GREGG GERETY, MD ALBANY MEDICAL COLLEGE, DIVISION OF COMMUNITY ENDOCRINOLOGY JULY 14, 2017
 TREATMENT OF DIABETES AFTER METFORMIN GREGG GERETY, MD ALBANY MEDICAL COLLEGE, DIVISION OF COMMUNITY ENDOCRINOLOGY JULY 14, 2017 Outline Review treatment algorithms from ADA/ EASD & ACE/AACE. Review positive
TREATMENT OF DIABETES AFTER METFORMIN GREGG GERETY, MD ALBANY MEDICAL COLLEGE, DIVISION OF COMMUNITY ENDOCRINOLOGY JULY 14, 2017 Outline Review treatment algorithms from ADA/ EASD & ACE/AACE. Review positive
Diabetes 2013: Achieving Goals Through Comprehensive Treatment. Session 2: Individualizing Therapy
 Diabetes 2013: Achieving Goals Through Comprehensive Treatment Session 2: Individualizing Therapy Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism
Diabetes 2013: Achieving Goals Through Comprehensive Treatment Session 2: Individualizing Therapy Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism
Cedars Sinai Diabetes. Michael A. Weber
 Cedars Sinai Diabetes Michael A. Weber Speaker Disclosures I disclose that I am a Consultant for: Ablative Solutions, Boston Scientific, Boehringer Ingelheim, Eli Lilly, Forest, Medtronics, Novartis, ReCor
Cedars Sinai Diabetes Michael A. Weber Speaker Disclosures I disclose that I am a Consultant for: Ablative Solutions, Boston Scientific, Boehringer Ingelheim, Eli Lilly, Forest, Medtronics, Novartis, ReCor
OBJECTIVES 4/7/2014. Diabetes Update Overview of the Diabetes Epidemic in the United States. ISHP Annual Spring Meeting
 Diabetes Update 2014 ISHP Annual Spring Meeting Hayley Miller MD April 13, 2014 OBJECTIVES Review diabetes guidelines. Understand diabetes management targets. Discuss current therapeutic strategies. Overview
Diabetes Update 2014 ISHP Annual Spring Meeting Hayley Miller MD April 13, 2014 OBJECTIVES Review diabetes guidelines. Understand diabetes management targets. Discuss current therapeutic strategies. Overview
CANA DAPA EMPA. Change in Baseline Body Weight (kg) *Doses evaluated in studies cited: CANA=100 or 300 mg, DAPA=5 or 10 mg, EMPA=10 or 25 mg.
 *Doses evaluated in studies cited: CANA=100 or 300 mg, DAPA=5 or 10 mg, EMPA=10 or 25 mg.") CANA DAPA EMPA Change in Baseline Body Weight (kg) 2 1 0-1 -2-3 -4-5 PBO SGLT2 inhibitor (low dose)* SGLT2 inhibitor (high dose)* *Doses evaluated in studies cited: CANA=100 or 300 mg, DAPA=5 or 10 mg,
CANA DAPA EMPA Change in Baseline Body Weight (kg) 2 1 0-1 -2-3 -4-5 PBO SGLT2 inhibitor (low dose)* SGLT2 inhibitor (high dose)* *Doses evaluated in studies cited: CANA=100 or 300 mg, DAPA=5 or 10 mg,
John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam
 Latest Insights from the JUPITER Study John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam Inflammation, hscrp, and Vascular Prevention
Latest Insights from the JUPITER Study John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam Inflammation, hscrp, and Vascular Prevention
Management of Diabetes Mellitus: A Primary Care Perspective. Screening for Diabetes Advantages of HbA1c as a Diagnostic Test
 Management of Diabetes Mellitus: A Primary Care Perspective Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening
Management of Diabetes Mellitus: A Primary Care Perspective Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening
Management of Diabetes Mellitus: A Primary Care Perspective
 Management of Diabetes Mellitus: A Primary Care Perspective Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening
Management of Diabetes Mellitus: A Primary Care Perspective Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening
CURRENT ISSUES IN DIABETES MANAGEMENT
 CURRENT ISSUES IN DIABETES MANAGEMENT Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening for Diabetes 2011 BMI
CURRENT ISSUES IN DIABETES MANAGEMENT Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening for Diabetes 2011 BMI
Preventive Cardiology Scientific evidence
 Preventive Cardiology Scientific evidence Professor David A Wood Garfield Weston Professor of Cardiovascular Medicine International Centre for Circulatory Health Imperial College London Primary prevention
Preventive Cardiology Scientific evidence Professor David A Wood Garfield Weston Professor of Cardiovascular Medicine International Centre for Circulatory Health Imperial College London Primary prevention
Placebo-Controlled Statin Trials Prevention Of CVD in Women"
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
7/8/2016. Sol Jacobs MD, FACE Division of Endocrinology Emory University School of Medicine
 Sol Jacobs MD, FACE Division of Endocrinology Emory University School of Medicine Participation in investigator initiated clinical research supported by: Merck Boehringer Ingelheim Novo Nordisk Astra Zeneca
Sol Jacobs MD, FACE Division of Endocrinology Emory University School of Medicine Participation in investigator initiated clinical research supported by: Merck Boehringer Ingelheim Novo Nordisk Astra Zeneca
IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS
 IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS Dr Bidhu Mohapatra, MBBS, MD, FRACP Consultant Physician Endocrinology and General Medicine Introduction 382 million people affected by diabetes
IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS Dr Bidhu Mohapatra, MBBS, MD, FRACP Consultant Physician Endocrinology and General Medicine Introduction 382 million people affected by diabetes
Current principles of diabetes management
 Current principles of diabetes management Prof. Martin Haluzík, MD, DSc. 3 Department of Medicine, General University Hospital and 1st Faculty of Medicine, Charles University in Prague, Czech Republic
Current principles of diabetes management Prof. Martin Haluzík, MD, DSc. 3 Department of Medicine, General University Hospital and 1st Faculty of Medicine, Charles University in Prague, Czech Republic
Placebo-Controlled Statin Trials EXPLAINING THE DECREASE IN DEATHS FROM CHD! PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN EXPLAINING THE DECREASE IN
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
Metformin should be considered in all patients with type 2 diabetes unless contra-indicated
 November 2001 N P S National Prescribing Service Limited PPR fifteen Prescribing Practice Review PPR Managing type 2 diabetes For General Practice Key messages Metformin should be considered in all patients
November 2001 N P S National Prescribing Service Limited PPR fifteen Prescribing Practice Review PPR Managing type 2 diabetes For General Practice Key messages Metformin should be considered in all patients
ACCORD, ADVANCE & VADT. Now what do I do in my practice?
 ACCORD, ADVANCE & VADT Now what do I do in my practice? Richard M. Bergenstal, MD International Diabetes Center Park Nicollet Health Services University of Minnesota Minneapolis, MN richard.bergenstal@parknicollet.com
ACCORD, ADVANCE & VADT Now what do I do in my practice? Richard M. Bergenstal, MD International Diabetes Center Park Nicollet Health Services University of Minnesota Minneapolis, MN richard.bergenstal@parknicollet.com
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
SCIENTIFIC STUDY REPORT
 PAGE 1 18-NOV-2016 SCIENTIFIC STUDY REPORT Study Title: Real-Life Effectiveness and Care Patterns of Diabetes Management The RECAP-DM Study 1 EXECUTIVE SUMMARY Introduction: Despite the well-established
PAGE 1 18-NOV-2016 SCIENTIFIC STUDY REPORT Study Title: Real-Life Effectiveness and Care Patterns of Diabetes Management The RECAP-DM Study 1 EXECUTIVE SUMMARY Introduction: Despite the well-established
Diabetes and Cardiovascular Risk Management Denise M. Kolanczyk, PharmD, BCPS-AQ Cardiology
 Diabetes and Cardiovascular Risk Management Denise M. Kolanczyk, PharmD, BCPS-AQ Cardiology Disclosures In compliance with the accrediting board policies, the American Diabetes Association requires the
Diabetes and Cardiovascular Risk Management Denise M. Kolanczyk, PharmD, BCPS-AQ Cardiology Disclosures In compliance with the accrediting board policies, the American Diabetes Association requires the
Cardiovascular Complications of Diabetes
 VBWG Cardiovascular Complications of Diabetes Nicola Abate, M.D., F.N.L.A. Professor and Chief Division of Endocrinology and Metabolism The University of Texas Medical Branch Galveston, Texas Coronary
VBWG Cardiovascular Complications of Diabetes Nicola Abate, M.D., F.N.L.A. Professor and Chief Division of Endocrinology and Metabolism The University of Texas Medical Branch Galveston, Texas Coronary
Pharmacology Update for the Adult Patient - Newer Oral Medications for Diabetes
 Pharmacology Update for the Adult Patient - Newer Oral Medications for Diabetes Brooke Hudspeth, PharmD, CDE, MLDE Director of Diabetes Prevention, Kroger Pharmacy Adjunct Assistant Professor, University
Pharmacology Update for the Adult Patient - Newer Oral Medications for Diabetes Brooke Hudspeth, PharmD, CDE, MLDE Director of Diabetes Prevention, Kroger Pharmacy Adjunct Assistant Professor, University
Diabetes Risk Assessment and Treatment
 Diabetes Risk Assessment and Treatment Todd T. Brown, MD, PhD Professor of Medicine and Epidemiology Division of Endocrinology, Diabetes, & Metabolism Johns Hopkins University Baltimore, Maryland, USA
Diabetes Risk Assessment and Treatment Todd T. Brown, MD, PhD Professor of Medicine and Epidemiology Division of Endocrinology, Diabetes, & Metabolism Johns Hopkins University Baltimore, Maryland, USA
Macrovascular Residual Risk. What risk remains after LDL-C management and intensive therapy?
 Macrovascular Residual Risk What risk remains after LDL-C management and intensive therapy? Defining Residual Vascular Risk The risk of macrovascular events and microvascular complications which persists
Macrovascular Residual Risk What risk remains after LDL-C management and intensive therapy? Defining Residual Vascular Risk The risk of macrovascular events and microvascular complications which persists
Update on CVD and Microvascular Complications in T2D
 Update on CVD and Microvascular Complications in T2D Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of Miami Miller School of Medicine
Update on CVD and Microvascular Complications in T2D Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of Miami Miller School of Medicine
Macrovascular Disease in Diabetes
 Macrovascular Disease in Diabetes William R. Hiatt, MD Professor of Medicine/Cardiology University of Colorado School of Medicine President, CPC Clinical Research Conflicts CPC Clinical Research (University-based
Macrovascular Disease in Diabetes William R. Hiatt, MD Professor of Medicine/Cardiology University of Colorado School of Medicine President, CPC Clinical Research Conflicts CPC Clinical Research (University-based
Glycemic control a matter of life and death
 Glycemic control a matter of life and death Linda Garcia Mellbin MD PhD Specialist in Cardiology & Internal medicine Dep of Cardiology Karolinska University Hospital /Karolinska Institutet Mortality (%)
Glycemic control a matter of life and death Linda Garcia Mellbin MD PhD Specialist in Cardiology & Internal medicine Dep of Cardiology Karolinska University Hospital /Karolinska Institutet Mortality (%)
Complications of Diabetes: Screening and Prevention. Dr Martin McIntyre Consultant Physician Royal Alexandra Hospital Paisley
 Complications of Diabetes: Screening and Prevention Dr Martin McIntyre Consultant Physician Royal Alexandra Hospital Paisley Diabetic Complications Microvascular: Retinopathy Nephropathy Neuropathy Macrovascular:
Complications of Diabetes: Screening and Prevention Dr Martin McIntyre Consultant Physician Royal Alexandra Hospital Paisley Diabetic Complications Microvascular: Retinopathy Nephropathy Neuropathy Macrovascular:
CONTROLLO GLICEMICO E RISCHIO CARDIOVASCOLARE. AGOSTINO CONSOLI DMSI - Università d Annunzio CHIETI ITALY. sul Paziente ad alto rischio CV*
 CONTROLLO GLICEMICO E RISCHIO CARDIOVASCOLARE AGOSTINO CONSOLI DMSI - Università d Annunzio CHIETI ITALY sul Paziente ad alto rischio CV* Does reducing hyperglycemia protect against cardiovascular risk?
CONTROLLO GLICEMICO E RISCHIO CARDIOVASCOLARE AGOSTINO CONSOLI DMSI - Università d Annunzio CHIETI ITALY sul Paziente ad alto rischio CV* Does reducing hyperglycemia protect against cardiovascular risk?
Multi-factor approach to reduce cardiovascular risk in diabetes
 Multi-factor approach to reduce cardiovascular risk in diabetes Prof. Nicola Napoli, MD PhD Division of Endocrinology and Diabetes Università Campus Bio-Medico di Roma Washington University in St Louis
Multi-factor approach to reduce cardiovascular risk in diabetes Prof. Nicola Napoli, MD PhD Division of Endocrinology and Diabetes Università Campus Bio-Medico di Roma Washington University in St Louis
Update on Diabetes. Ketan Dhatariya. Why it s Not Just About Glucose Lowering Any More. Consultant in Diabetes NNUH
 Update on Diabetes Why it s Not Just About Glucose Lowering Any More Ketan Dhatariya Consultant in Diabetes NNUH The Story So Far.. DCCT Retinopathy Neuropathy Nephropathy Intensive glucose control in
Update on Diabetes Why it s Not Just About Glucose Lowering Any More Ketan Dhatariya Consultant in Diabetes NNUH The Story So Far.. DCCT Retinopathy Neuropathy Nephropathy Intensive glucose control in
FUNDING: MICIS mandated by Maine Legislature, funded by fees collected from pharmaceutical companies as a cost of doing business in the state.
 GOAL: To improve clinical outcomes by delivering upto-date, evidence-based prescribing information, using data and guidelines developed by noncommercial sources FUNDING: MICIS mandated by Maine Legislature,
GOAL: To improve clinical outcomes by delivering upto-date, evidence-based prescribing information, using data and guidelines developed by noncommercial sources FUNDING: MICIS mandated by Maine Legislature,
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
Management of Type 2 Diabetes Mellitus. Heather Corn, MD, MS Endocrinology, Diabetes, and Metabolism
 Management of Type 2 Diabetes Mellitus Heather Corn, MD, MS Endocrinology, Diabetes, and Metabolism Disclosures Working for Intermountain Healthcare Some of the views represented are the opinion of ABIM-certified
Management of Type 2 Diabetes Mellitus Heather Corn, MD, MS Endocrinology, Diabetes, and Metabolism Disclosures Working for Intermountain Healthcare Some of the views represented are the opinion of ABIM-certified
Cardiovascular Risk Reduction and Other Co-morbidities in Type 2 Diabetes
 Cardiovascular Risk Reduction and Other Co-morbidities in Type 2 Diabetes Following this presentation, you will be able to: Describe the relationship between major CV risk factors and CVD outcomes Select
Cardiovascular Risk Reduction and Other Co-morbidities in Type 2 Diabetes Following this presentation, you will be able to: Describe the relationship between major CV risk factors and CVD outcomes Select
New Measure Recommended for Endorsement by PQA
 New Measure Recommended for Endorsement by PQA Measure: Statin Use in Persons with Diabetes Description: The percentage of patients ages 40 75 years who were dispensed a medication for diabetes that receive
New Measure Recommended for Endorsement by PQA Measure: Statin Use in Persons with Diabetes Description: The percentage of patients ages 40 75 years who were dispensed a medication for diabetes that receive
The target blood pressure in patients with diabetes is <130 mm Hg
 Controversies in hypertension, About Diabetes diabetes and and metabolic Cardiovascular syndrome Risk ESC annual congress August 29, 2011 The target blood pressure in patients with diabetes is
Controversies in hypertension, About Diabetes diabetes and and metabolic Cardiovascular syndrome Risk ESC annual congress August 29, 2011 The target blood pressure in patients with diabetes is
Preventing Serious Health Consequences of Type 2 Diabetes
 Preventing Serious Health Consequences of Type 2 Diabetes The Evidence Hertzel C. Gerstein MD MSc FRCPC Professor and Population Health Institute Chair in Diabetes Research McMaster University and Hamilton
Preventing Serious Health Consequences of Type 2 Diabetes The Evidence Hertzel C. Gerstein MD MSc FRCPC Professor and Population Health Institute Chair in Diabetes Research McMaster University and Hamilton
Diabetes in the UK: Update on Diabetes Treatment and Care. Why is diabetes increasing? Obesity Increased waist circumference.
 Update on Diabetes Treatment and Care Tahseen A Chowdhury Consultant Diabetologist Royal London and Mile End Hospitals Diabetes prevalence (thousands) Diabetes in the UK: 1995-21 3 25 2 15 1 5 Type 1 Type
Update on Diabetes Treatment and Care Tahseen A Chowdhury Consultant Diabetologist Royal London and Mile End Hospitals Diabetes prevalence (thousands) Diabetes in the UK: 1995-21 3 25 2 15 1 5 Type 1 Type
American Academy of Insurance Medicine
 American Academy of Insurance Medicine October 2012 Dr. Alison Moy Liberty Mutual Dr. John Kirkpatrick Thrivent Financial for Lutherans 1 59 year old male, diagnosed with T2DM six months ago Nonsmoker
American Academy of Insurance Medicine October 2012 Dr. Alison Moy Liberty Mutual Dr. John Kirkpatrick Thrivent Financial for Lutherans 1 59 year old male, diagnosed with T2DM six months ago Nonsmoker
Addressing Addressing Challenges in Type 2 Challenges in Type 2 Diabetes Diabetes Speaker:
 Addressing Challenges in Type 2 Diabetes Geneva Briggs, PharmD,, BCPS Addressing Challenges in Type 2 Diabetes Speaker: Dr. Geneva Clark Briggs, a board-certified Pharmacotherapy Specialist, received her
Addressing Challenges in Type 2 Diabetes Geneva Briggs, PharmD,, BCPS Addressing Challenges in Type 2 Diabetes Speaker: Dr. Geneva Clark Briggs, a board-certified Pharmacotherapy Specialist, received her
What s New in Type 2? Peter Hammond Consultant Physician Harrogate District Hospital
 What s New in Type 2? Peter Hammond Consultant Physician Harrogate District Hospital Therapy considerations in T2DM Thiazoledinediones DPP IV inhibitors GLP 1 agonists Insulin Type Delivery Horizon scanning
What s New in Type 2? Peter Hammond Consultant Physician Harrogate District Hospital Therapy considerations in T2DM Thiazoledinediones DPP IV inhibitors GLP 1 agonists Insulin Type Delivery Horizon scanning
Chief of Endocrinology East Orange General Hospital
 Targeting the Incretins System: Can it Improve Our Ability to Treat Type 2 Diabetes? Darshi Sunderam, MD Darshi Sunderam, MD Chief of Endocrinology East Orange General Hospital Age-adjusted Percentage
Targeting the Incretins System: Can it Improve Our Ability to Treat Type 2 Diabetes? Darshi Sunderam, MD Darshi Sunderam, MD Chief of Endocrinology East Orange General Hospital Age-adjusted Percentage
Changing Diabetes: The time is now!
 Midwest Cardiovascular Research Foundation Welcomes DANITA HARRISON, ARNP Ms. Harrison discloses speaking relationships with Lilly, Novo Nordisk and Pfizer. Changing Diabetes: The time is now! Danita Harrison
Midwest Cardiovascular Research Foundation Welcomes DANITA HARRISON, ARNP Ms. Harrison discloses speaking relationships with Lilly, Novo Nordisk and Pfizer. Changing Diabetes: The time is now! Danita Harrison