Heart Failure: Current Management Strategies
|
|
|
- Sheryl Booker
- 5 years ago
- Views:
Transcription

1 Heart Failure: Current Management Strategies CSHP Fall Education Session- September 30th, 2017 Carolyn MacKinnon & Tamara Matchett BscPharm, ACPR Candidates

2 Objectives 1. Describe the pathophysiology & presentation of heart failure 2. Identify current management strategies for heart failure 3. Discuss heart failure treatment updates and how they may apply to practice
3 Patient Case ID - 68 year old male CC - Increasing SOBOE PMHx - HF-rEF x 5 years, NYHA II - COPD Physical Exam - BP 110/60 mmhg - HR 72 bpm - Minimal pedal edema Labs -Na 138, K 4.2, SCr 86mmol/l (CrCl 61ml/min), NT-proBNP 2480 pg/ml Diagnostic tests -LVEF: 35% Medications: - Bisoprolol 10 mg daily - Telmisartan 40 mg daily - Spironolactone 25 mg daily - Furosemide 40mg daily
4 What is your next step? A. B. C. D. Start sacubitril/valsartan 24mg/26mg Start ivabradine 7.5mg BID Change spironolactone to eplerenone Start hydralazine/nitrates
5 Congestive Heart Failure = Heart Failure


6 Epidemiology About 600,000 Canadians living with heart failure 50,000 Canadians diagnosed/year Risk of CV death is INCREASED after HF hospitalization Costs to the health care system is over $2.8 million/year More common in men than women before age 65
 and/or contractility (systolic) Leading causes: heart damage from previous myocardial infarction and")
7 Pathophysiology Inability for heart to pump sufficient blood for body s metabolic needs ventricular filling (diastolic) and/or contractility (systolic) Leading causes: heart damage from previous myocardial infarction and hypertension
8 Reduced Ejection Fraction Preserved Ejection Fraction 2017 Comprehensive Update of the CCS Guidelines for the Management of Heart Failure
9 Out with the Old... Terminology Terminology LVEF LVEF Preserved EF (HF-pEF) >40% Preserved EF (HF-pEF) 50% 41-49% Reduced EF (HF-rEF) <40% Mid-range EF (HF-mEF) Reduced EF (HF-rEF) 40%
10 Symptoms Primary manifestations: dyspnea & fatigue Edema Orthopnea Exercise intolerance Cough Mental status changes (confusion)
11 New York Heart Association (NYHA) Classification Class Patient Symptoms I No limitation of physical activity. Ordinary physical activity does not cause undue fatigue, palpitation, dyspnea II Slight limitation of physical activity. Comfortable at rest. Ordinary physical activity results in fatigue, palpitation, dyspnea III Marked limitation of physical activity. Comfortable at rest. Less than ordinary activity causes fatigue, palpitation, or dyspnea IV Unable to carry on any physical activity without discomfort. Symptoms of HF at rest. Discomfort increases with physical activity.
12 Diagnosis Clinical history and physical exam Symptoms, functional limitation, risk factors, comorbidities, vital signs, volume status Initial investigations CXR, ECG, CBC, electrolytes, renal function Natriuretic peptides NT-proBNP or BNP Ventricular function Echo, LVEF
13 HF Management Strategies to Date
 40% Survival benefit shown with : Beta blockers, ACE inhibitors/ angiotensin receptor blockers, aldosterone antagonists, F channel inhibitors, angiotensin receptor neprilysin")
14 Therapies improving survival HF with preserved EF (HF-pef) 50% No therapies improving survival HF with mid range EF (HF-mef) 41-49% No therapies improving survival HF with reduced EF (HF-ref) 40% Survival benefit shown with : Beta blockers, ACE inhibitors/ angiotensin receptor blockers, aldosterone antagonists, F channel inhibitors, angiotensin receptor neprilysin inhibitor
15 Canadian Cardiovascular Society (CCS) Guidelines

16 Guideline Timeline 2006: Heart Failure Diagnosis and Management Guidelines : Annual Updates 2015: Heart Failure Companion: Bridging Guidelines to Your Practice 2017: Comprehensive Update of the Canadian Cardiovascular Society Guidelines for the Management of Heart Failure
17
18 Angiotensin Receptor Neprilysin Inhibitor (ARNI)
19 Angiotensin receptor neprilysin inhibitor (ARNI) Sacubitril (neprilysin inhibitor) + = Valsartan (Ang II receptor blocker) LCZ696
20 Sacubitril/Valsartan (Entresto) Natriuretic Peptide System Renin Angiotensin System Angiotensin I Natriuretic peptides Neprilysin X Sacubitril Angiotensin II Inactive fragments Angiotensin II Receptor Valsartan Vasodilation Blood pressure Sympathetic tone Aldosterone Hypertrophy X Vasoconstriction Blood pressure Sympathetic tone Aldosterone Hypertrophy
21
22 PARADIGM-HF P Patients with HF NYHA class II-IV with EF 40% I LCZ mg twice daily (Sacubitril 97mg/ Valsartan 103 mg twice daily) C Enalapril 10 mg twice daily O Composite of death from cardiovascular causes or hospitalization for heart failure
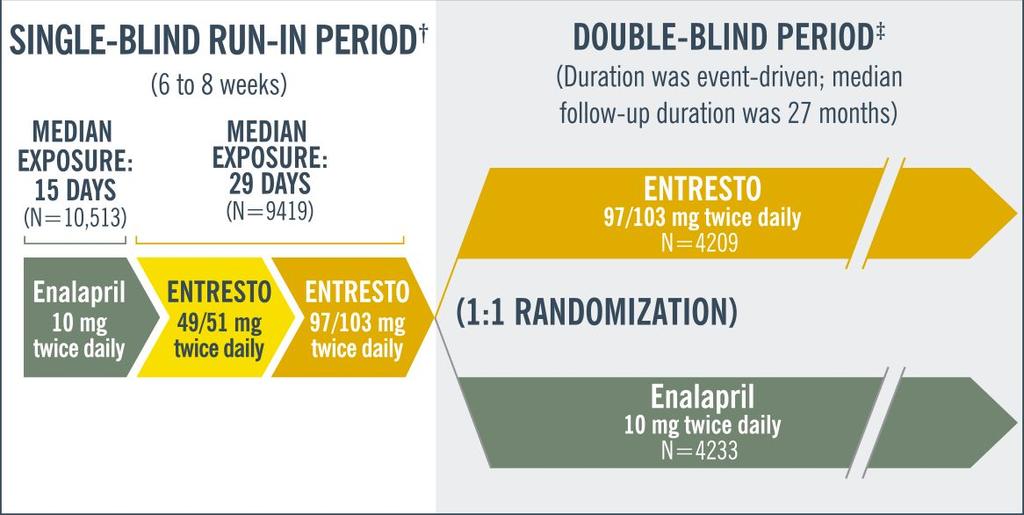
23 PARADIGM-HF
24 Primary outcome: CV mortality or first hospitalization for HF RRR 20% Entresto vs enalapril: 21.8% vs 26.5%, p<0.001 ARR: 4.7% NNT: 21
25 PARADIGM-HF: Outcomes Efficacy 3.2% ARR in CV death : NNT 31 3% ARR in first hospitalization : NNT % ARR in death from any cause: NNT 44 All statistically significant
, hyperkalemia or renal impairment (3.3% vs 4.5%, all p<0.05) More likely to cause symptomatic hypotension (4.3% vs 5.6%) Mean SBP at 8 months 3.")
26 PARADIGM-HF: Outcomes Safety Less likely to be discontinued due to adverse event (10.7% vs 12.3%, p=0.03) Less likely to cause cough (11.3% vs 14.3%), hyperkalemia or renal impairment (3.3% vs 4.5%, all p<0.05) More likely to cause symptomatic hypotension (4.3% vs 5.6%) Mean SBP at 8 months 3.2 mmhg lower in Entresto group
27 When do we use it?
28 When do we use it? CCS Guidelines: an ARNI should be used in place of an ACEi or ARB, in patients with HFrEF NYHA Class II to IV, who remain symptomatic despite treatment with maximum tolerated doses of ACEI/ARB + BB + MRA
29 Checklist Ejection fraction <40% NYHA Class II or III BP 100 mm Hg egfr 30 ml/min Potassium < 5.2 mmol/l ACEi/ARB, BB, MRA at max tolerated dose
30 Entresto (LCZ696)- Supplied Low dose Moderate dose High (target) dose 24mg/26mg Sacubitril/Valsartan 49mg/51mg Sacubitril/Valsartan 97mg/103mg Sacubitril/Valsartan aka 50mg aka 100mg aka 200mg 103mg of valsartan in Entresto = 160mg of valsartan in Diovan
31 Entresto (LCZ696)- Dosing Baseline Initial Dose Titration 49/51mg BID Increase to target 97/103mg BID over 2-4 weeks Lower dose of RAAS inhibitor, higher 24/26mg BID risk of hypotension (low BP, > 75yrs poor renal function), or moderate hepatic impairment Increase to target 97/103mg over 6 weeks Higher dose of RAAS inhibitor ACEI Enalapril 10mg/d lisinopril 10mg/d perindopril 4mg/d ramipril 5 mg/d ARB candesartan 16mg/d irbesartan 150 mg/d losartan 50 mg/d olmesartan 10 mg/d telmisartan 40 mg/d valsartan 160 mg/d

32 Entresto (LCZ696) Switching: From ACEI From ARB Risk of angioedema Stop ACEI 36 hours prior to first dose of Entresto Initiate Entresto at the time the next dose is due
33 Safety & Precautions Contraindications: hx of angioedema Adverse effects: hypotension, hyperkalemia, dizziness, renal impairment, angioedema, may increase statin levels, alzheimers? Monitor: K+, SCr, BP 1 week after initiation, after each dose increase and with each practitioner visit
34 Safety & Precautions Drug interactions: ACE/ARB, aliskiren (RAAS), potassium sparing diuretics, trimethoprim, K supplements ( K), NSAIDs ( SCr), lithium (lithium toxicity), statins? (statin toxicity)
35 Safety & Precautions Elevates BNP levels- use NT pro BNP Should not be initiated in patients with acutely decompensated heart failure, or clinically-relevant ischemic events, such as acute myocardial or cerebral infarction


36 Coverage Entresto cards Covers cost of prescription
37 Coverage Recently added to NB formulary : Special Authorization NYHA class II or III HF who meet the following criteria: LVEF < 40%. NYHA class II to III symptoms despite at least four weeks of treatment with a stable dose of ACEI or ARB and BB and AA BNP 150 pg/ml or NT-proBNP 600 pg/ml.
38 F-Channel Inhibitors
39 Ivabradine (LancoraTM)
40
41 SHIFT 2010 P Adults in sinus rhythm, with resting HR 70 bpm, LVEF 35%, stable symptomatic chronic HF (NYHA II-IV) for 4 wk, HF hospitalization within 12 mo, and on guideline-directed therapy (ACE/ARB, BB, +/- aldosterone antagonist) I Ivabradine 5 mg BID/ 7.5 mg BID/ 2.5 mg BID C Placebo O CV death or HF hospitalization

42 SHIFT Study Design * o Placeb Blinding & random allocation Median follow up 22.9 mo Assessed resting heart rate at 2 weeks, then every 4 months, which guided dose adjustments. *HR in bpm
43 Primary Outcome: CV mortality or HF hospitalization RRR: 18% Ivabradine vs placebo: 24.5% vs 28.7%, p< ARR: 5% NNT: 20
44 Results 2o endpoints (ivabradine vs placebo) 1 % ARR in CV mortality: NNT 100 5% ARR in Hospital Admission for HF: NNT 20 2 % ARR in Death from HF: NNT 50 4% ARR in All-cause hospital admissions: NNT 25 *HR was 8 bpm lower in ivabradine group at end of study Statistically significant
45 Subgroup Analysis Patients receiving 50% target beta blocker dose (56% in each group) Primary endpoint and secondary mortality endpoints: not significantly reduced HF hospital admissions: significantly reduced by 19%
* Visual changes (3%) Fewer all serious adverse events found in study group *not statistically")
46 SHIFT Adverse Events Symptomatic bradycardia (5%) Asymptomatic bradycardia (6%) Atrial Fibrillation (9%)* Visual changes (3%) Fewer all serious adverse events found in study group *not statistically significant


47 Ivabradine(Lancora) Safety & Precautions Contraindications: acute HF, BP <90/50, resting HR <60 bpm, hepatic impairment, pacemaker, prolonged QT Adverse effects: bradycardia, AFib, visual changes, vertigo, heart block, ventricular tachycardia*, hypotension*, venticular fibrillation*, torsades de pointes* Drug interactions: strong and moderate CYP3A4 inhibitors, CYP3A4 inducers, QTc prolonging agents, K+ depleting diuretics, amiodarone, simvastatin *Post-Market/Case Reports (<1%)

.")
48 Safety & Precautions, cont d No safety data for CrCl <15mL/min Pregnancy and breastfeedings risks cannot be ruled out Limited data in patients with cardiac devices (ICD or CRT). Caution and close cardiac monitoring is recommended.
49 When do we use it? CCS Guidelines: Ivabradine should be considered in patients with HFrEF who: Are symptomatic despite treatment with appropriate doses of ACEi + BB + MRA Have a resting HR > 70 bpm, Are in sinus rhythm Had a prior HF hospitalization within 12 months
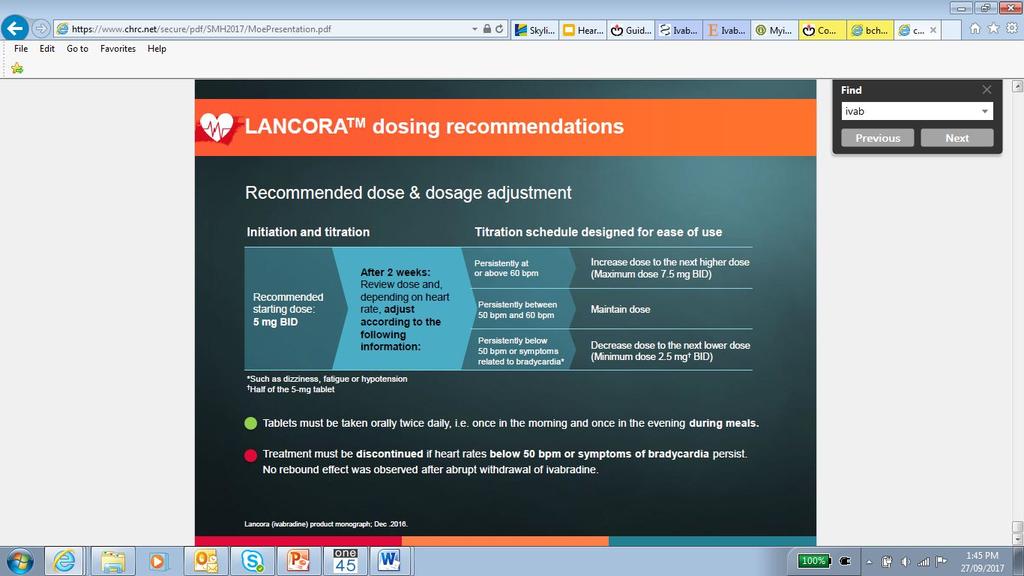
 as long as tolerated, and not to a specific HR Start ivabradine at the lowest dose in patients > 75years of age (e.g. 2.5mg po BID).")
50 Administration & Dosing BID with meals Initiate at 5 mg BID. Titrate to target dose of 7.5 mg BID (max dose) as long as tolerated, and not to a specific HR Start ivabradine at the lowest dose in patients > 75years of age (e.g. 2.5mg po BID). Discontinuation of treatment should be considered if despite use of the highest dose (7.5 mg BID) for several months, there has been no clear decrease in the patient s resting heart rate.

51 Ivabradine(Lancora) Coverage Currently not covered by NBPDP Cost per day is approximately $2.50
52 Patient Case ID - 68 year old male CC - Increasing SOBOE PMHx - HF-rEF x 5 years, NYHA II - COPD Physical Exam - BP 110/60 mmhg - HR 72 bpm - Minimal pedal edema Labs -Na 138, K 4.2, SCr 86mmol/l (CrCl 61ml/min), NT-proBNP 2480 pg/ml Diagnostic tests -LVEF: 35% Medications: - Bisoprolol 10 mg daily - Telmisartan 80 mg daily - Spironolactone 25 mg daily - Furosemide 40mg daily

53 What is your next step? A. B. C. D. Start sacubitril/valsartan 24mg/26mg Start ivabradine 7.5mg BID Change spironolactone to eplerenone Start hydralazine/nitrates Option A. Start low dose Entresto BP >100 K < 5.2 egfr > 30ml/min on stable doses on ARB, BB and MRA
54 Summary : Entresto and Ivabradine Both medications should only be considered after standard triple therapy has been completed with ACEi + BB + MRB Entresto Limited by BP and hyperkalemia BP 100 mmhg K+ < 5.2 Reduced CV death, hospitalization for HF and all cause mortality Ivabradine Limited by HR CCS: > 70 bpm Reduced death from HF, hospitalization for HF, and all cause-hospitalization
55 Thank You
56 References BC s Heart Failure Network. Bcheartfailure.ca [Accessed September 2017] Canadian Cardiovascular Society Guidelines Library. ccs.ca [Accessed September 2017] 2015 Heart Failure Bridging Guidelines, 2017 Guidelines CADTH Common Drug Review: Ivabradine. Cadth.ca [Accessed September 2017] Chen-Huan, C. Critical questions about PARADIGM-HF and the future. Acta Cadiol Sin 2016;32: Entresto Product Monograph. Novartis [Accessed September 2017] Heart and Stroke Foundation. Heartandstroke.ca [Accessed: September 2017] Lancora Product Monograph. Servier. RxTx. [Accessed September 2017] McMurray, J. J. V. et al. Angiotensin Neprilysin Inhibition versus Enalapril in Heart Failure. N Engl J Med 2014 Sept ; 371: (PARADIGM-HF) Pharmacotherapy: A Pathophysiologic Approach. 7th edition. Dipiro Swedberg K., et al.ivabradine and outcomes in chronic heart failure (SHIFT): a randomised placebo-controlled study.lancet Sep 11;376(9744): Swedberg K., et al. Rationale and design of a randomized, double-blind, placebo-controlled outcome trial of ivabradine in chronic heart failure: the Systolic Heart Failure Treatment with the If Inhibitor Ivabradine Trial (SHIFT).Eur J Heart Fail Jan;12(1):75-81 Truven Health 2017: Micromedex.[Accessed September 2017]
57
58
59
60
What s New in Heart Failure? Marie-France Gauthier, BSc, PharmD, ACPR Clinical Pharmacist at Montfort Hospital
 What s New in Heart Failure? Marie-France Gauthier, BSc, PharmD, ACPR Clinical Pharmacist at Montfort Hospital Disclosures I have no current or past relationships with commercial entities Learning objectives
What s New in Heart Failure? Marie-France Gauthier, BSc, PharmD, ACPR Clinical Pharmacist at Montfort Hospital Disclosures I have no current or past relationships with commercial entities Learning objectives
Beyond ACE-inhibitors for Heart Failure. Jacob Townsend, MD NCVH Birmingham 2015
 Beyond ACE-inhibitors for Heart Failure Jacob Townsend, MD NCVH Birmingham 2015 % Decrease in Mortality Current Therapy HFrEF 0% Angiotensin receptor blocker ACE inhibitor Beta blocker Mineralocorticoid
Beyond ACE-inhibitors for Heart Failure Jacob Townsend, MD NCVH Birmingham 2015 % Decrease in Mortality Current Therapy HFrEF 0% Angiotensin receptor blocker ACE inhibitor Beta blocker Mineralocorticoid
Disclosures. This speaker has indicated there are no relevant financial relationships to be disclosed.
 Disclosures This speaker has indicated there are no relevant financial relationships to be disclosed. And the Beat Goes On: New Medications for Heart Failure Alison M. Walton, PharmD, BCPS The Case of
Disclosures This speaker has indicated there are no relevant financial relationships to be disclosed. And the Beat Goes On: New Medications for Heart Failure Alison M. Walton, PharmD, BCPS The Case of
2017 CCS HF Guidelines Medical Therapy for HFrEF When What Order and How Much?
 2017 CCS HF Guidelines Medical Therapy for HFrEF When What Order and How Much? Dr. Shelley Zieroth University of Manitoba @ShelleyZieroth @CanHFSociety Disclosures Consulting/Advisory Board: Amgen, Astra
2017 CCS HF Guidelines Medical Therapy for HFrEF When What Order and How Much? Dr. Shelley Zieroth University of Manitoba @ShelleyZieroth @CanHFSociety Disclosures Consulting/Advisory Board: Amgen, Astra
HEART FAILURE: PHARMACOTHERAPY UPDATE
 HEART FAILURE: PHARMACOTHERAPY UPDATE 3 HEART FAILURE REVIEW 1 5.1 million x1.25 = 6.375 million 40 years old = MICHAEL F. AKERS, PHARM.D. CLINICAL PHARMACIST CENTRACARE HEALTH, ST. CLOUD HOSPITAL HF Diagnosis
HEART FAILURE: PHARMACOTHERAPY UPDATE 3 HEART FAILURE REVIEW 1 5.1 million x1.25 = 6.375 million 40 years old = MICHAEL F. AKERS, PHARM.D. CLINICAL PHARMACIST CENTRACARE HEALTH, ST. CLOUD HOSPITAL HF Diagnosis
Treating HF Patients with ARNI s Why, When and How?
 Treating HF Patients with ARNI s Why, When and How? 19 th Annual San Diego Heart Failure Symposium for Primary Care Physicians January 11-12, 2019 La Jolla, CA Barry Greenberg M.D. Distinguished Professor
Treating HF Patients with ARNI s Why, When and How? 19 th Annual San Diego Heart Failure Symposium for Primary Care Physicians January 11-12, 2019 La Jolla, CA Barry Greenberg M.D. Distinguished Professor
LCZ696 A First-in-Class Angiotensin Receptor Neprilysin Inhibitor
 The Angiotensin Receptor Neprilysin Inhibitor LCZ696 in Heart Failure with Preserved Ejection Fraction The Prospective comparison of ARNI with ARB on Management Of heart failure with preserved ejection
The Angiotensin Receptor Neprilysin Inhibitor LCZ696 in Heart Failure with Preserved Ejection Fraction The Prospective comparison of ARNI with ARB on Management Of heart failure with preserved ejection
New Winners in the World of Heart Failure. Laura Steffens PharmD Candidate 2016 CICU Presentation August 12, 2015
 New Winners in the World of Heart Failure Laura Steffens PharmD Candidate 2016 CICU Presentation August 12, 2015 Jessup 2014 Shaking Things Up 2003: FDA approved eplerenone for the treatment of heart failure
New Winners in the World of Heart Failure Laura Steffens PharmD Candidate 2016 CICU Presentation August 12, 2015 Jessup 2014 Shaking Things Up 2003: FDA approved eplerenone for the treatment of heart failure
1/4/18. Heart Failure Guideline Review and Update. Disclosure. Pharmacist Objectives. Pharmacy Technician Objectives. What is Heart Failure?
 Disclosure Heart Failure Guideline Review and Update I have had no financial relationship over the past 12 months with any commercial sponsor with a vested interest in this presentation. Natalie Beiter,
Disclosure Heart Failure Guideline Review and Update I have had no financial relationship over the past 12 months with any commercial sponsor with a vested interest in this presentation. Natalie Beiter,
Heart Failure New Drugs- Updated Guidelines
 Heart Failure New Drugs- Updated Guidelines Eileen Handberg, PhD, ANP-BC, FAHA, FACC Professor of Medicine Division of Cardiovascular Medicine University of Florida Disclosures 1. 3 2. 6 3. 8 4. 11 Dunlay
Heart Failure New Drugs- Updated Guidelines Eileen Handberg, PhD, ANP-BC, FAHA, FACC Professor of Medicine Division of Cardiovascular Medicine University of Florida Disclosures 1. 3 2. 6 3. 8 4. 11 Dunlay
Sacubitril/valsartan: A New Management Strategy for the Treatment of Heart Failure. Elizabeth Pogge, PharmD, MPH, BCPS, FASCP
 Sacubitril/valsartan: A New Management Strategy for the Treatment of Heart Failure Elizabeth Pogge, PharmD, MPH, BCPS, FASCP Disclosure Elizabeth Pogge reports no actual or potential conflicts of interest
Sacubitril/valsartan: A New Management Strategy for the Treatment of Heart Failure Elizabeth Pogge, PharmD, MPH, BCPS, FASCP Disclosure Elizabeth Pogge reports no actual or potential conflicts of interest
Congestive Heart Failure: Outpatient Management
 The Chattanooga Heart Institute Cardiovascular Symposium Congestive Heart Failure: Outpatient Management E. Philip Lehman MD, MPP Disclosure No financial disclosures. Objectives Evidence-based therapy
The Chattanooga Heart Institute Cardiovascular Symposium Congestive Heart Failure: Outpatient Management E. Philip Lehman MD, MPP Disclosure No financial disclosures. Objectives Evidence-based therapy
Neprilysin Inhibitor (Entresto ) Prior Authorization and Quantity Limit Program Summary
 Prior Authorization and Quantity Limit Program Summary") Neprilysin Inhibitor (Entresto ) Prior Authorization and Quantity Limit Program Summary FDA APPROVED INDICATIONS DOSAGE 1 Indication Entresto Reduce the risk of cardiovascular (sacubitril/valsartan) death
Neprilysin Inhibitor (Entresto ) Prior Authorization and Quantity Limit Program Summary FDA APPROVED INDICATIONS DOSAGE 1 Indication Entresto Reduce the risk of cardiovascular (sacubitril/valsartan) death
From PARADIGM-HF to Clinical Practice. Waleed AlHabeeb, MD, MHA Associate Professor of Medicine President of the Saudi Heart Failure Group
 From PARADIGM-HF to Clinical Practice Waleed AlHabeeb, MD, MHA Associate Professor of Medicine President of the Saudi Heart Failure Group PARADIGM-HF: Inclusion Criteria Chronic HF NYHA FC II IV with LVEF
From PARADIGM-HF to Clinical Practice Waleed AlHabeeb, MD, MHA Associate Professor of Medicine President of the Saudi Heart Failure Group PARADIGM-HF: Inclusion Criteria Chronic HF NYHA FC II IV with LVEF
2017 Summer MAOFP Update
 2017 Summer MAOFP Update. Cardiology Update 2017 Landmark Trials Change Practice Guidelines David J. Strobl, DO, FNLA Heart Failure: Epidemiology More than 4 million patients affected 400,000 new cases
2017 Summer MAOFP Update. Cardiology Update 2017 Landmark Trials Change Practice Guidelines David J. Strobl, DO, FNLA Heart Failure: Epidemiology More than 4 million patients affected 400,000 new cases
Heart Failure Clinician Guide JANUARY 2016
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Heart Failure Clinician Guide JANUARY 2018
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Disclosures. Advances in Chronic Heart Failure Management 6/12/2017. Van N Selby, MD UCSF Advanced Heart Failure Program June 19, 2017
 Advances in Chronic Heart Failure Management Van N Selby, MD UCSF Advanced Heart Failure Program June 19, 2017 I have nothing to disclose Disclosures 1 Goal statement To review recently-approved therapies
Advances in Chronic Heart Failure Management Van N Selby, MD UCSF Advanced Heart Failure Program June 19, 2017 I have nothing to disclose Disclosures 1 Goal statement To review recently-approved therapies
Use of Sacubitril/Valsartan in Heart Failure
 Use of Sacubitril/Valsartan in Heart Failure & the PARADIGM-HF trial Sarah Mackenzie, PharmD student, University of Toronto Presentation Outline Overview of: Entresto PARADIGM-HF trial Critical Appraisal
Use of Sacubitril/Valsartan in Heart Failure & the PARADIGM-HF trial Sarah Mackenzie, PharmD student, University of Toronto Presentation Outline Overview of: Entresto PARADIGM-HF trial Critical Appraisal
Rationale and Practical Aspects of Sacubitril- Valsartan and Ivabradine Use in Heart Failure Patients
 Rationale and Practical Aspects of Sacubitril- Valsartan and Ivabradine Use in Heart Failure Patients Javed Butler, MD, MPH, MBA Patrick H. Lehan Professor of Medicine Professor of Physiology Chairman,
Rationale and Practical Aspects of Sacubitril- Valsartan and Ivabradine Use in Heart Failure Patients Javed Butler, MD, MPH, MBA Patrick H. Lehan Professor of Medicine Professor of Physiology Chairman,
Disclosure Statement. Heart Failure: Refreshers and Updates. Objectives. CHF: Chronic Heart Failure. Definitions. Definitions 2/19/2018
 Disclosure Statement Heart Failure: Refreshers and Updates Tracy K. Pettinger, PharmD Clinical Associate Professor College of Pharmacy The planners and presenter of this presentation have disclosed no
Disclosure Statement Heart Failure: Refreshers and Updates Tracy K. Pettinger, PharmD Clinical Associate Professor College of Pharmacy The planners and presenter of this presentation have disclosed no
Sacubitril/Valsartan in HFrEF for All Protagonist View George Honos MD FRCPC FCCS FACC
 Sacubitril/Valsartan in HFrEF for All Protagonist View George Honos MD FRCPC FCCS FACC Head of Cardiology Medical Manager / CV Program CHUM Disclosure Statement Within the past two years: I have had an
Sacubitril/Valsartan in HFrEF for All Protagonist View George Honos MD FRCPC FCCS FACC Head of Cardiology Medical Manager / CV Program CHUM Disclosure Statement Within the past two years: I have had an
Updates in Heart Failure (HF) 2016: ACC / AHA and ESC
 2016: ACC / AHA and ESC") Updates in Heart Failure (HF) 2016: ACC / AHA and ESC Patrick McBride, MD, MPH Professor of Medicine & Family Medicine, UW School of Medicine and Public Health Special thanks to: Clyde W. Yancy, MD, MSc
Updates in Heart Failure (HF) 2016: ACC / AHA and ESC Patrick McBride, MD, MPH Professor of Medicine & Family Medicine, UW School of Medicine and Public Health Special thanks to: Clyde W. Yancy, MD, MSc
Systolic Dysfunction Clinical /Hemodynamic Guide for Management From Neprilysin Inhibitors to Ivabradine
 Systolic Dysfunction Clinical /Hemodynamic Guide for Management From Neprilysin Inhibitors to Ivabradine Donna Mancini MD Choudhrie Professor of Cardiology Columbia University Speaker Disclosure Amgen
Systolic Dysfunction Clinical /Hemodynamic Guide for Management From Neprilysin Inhibitors to Ivabradine Donna Mancini MD Choudhrie Professor of Cardiology Columbia University Speaker Disclosure Amgen
Entresto Development of sacubitril/valsartan (LCZ696) for the treatment of heart failure with reduced ejection fraction
 for the treatment of heart failure with reduced ejection fraction") Cardio-Metabolic Franchise Entresto Development of sacubitril/valsartan (LCZ696) for the treatment of heart failure with reduced ejection fraction Randy L Webb, PhD Rutgers Workshop October 21, 2016 Heart
Cardio-Metabolic Franchise Entresto Development of sacubitril/valsartan (LCZ696) for the treatment of heart failure with reduced ejection fraction Randy L Webb, PhD Rutgers Workshop October 21, 2016 Heart
Disclosures. Overview. Goal statement. Advances in Chronic Heart Failure Management 5/22/17
 Disclosures Advances in Chronic Heart Failure Management I have nothing to disclose Van N Selby, MD UCSF Advanced Heart Failure Program May 22, 2017 Goal statement To review recently-approved therapies
Disclosures Advances in Chronic Heart Failure Management I have nothing to disclose Van N Selby, MD UCSF Advanced Heart Failure Program May 22, 2017 Goal statement To review recently-approved therapies
Initiating New Medications in the Management of Heart Failure
 Initiating New Medications in the Management of Heart Failure Sandra Oliver-McNeil DNP, MSN, ACNP-BC, CHFN Associate Professor (Clinical) Wayne State University College of Nursing Objectives The participant
Initiating New Medications in the Management of Heart Failure Sandra Oliver-McNeil DNP, MSN, ACNP-BC, CHFN Associate Professor (Clinical) Wayne State University College of Nursing Objectives The participant
DISCLOSURES ACHIEVING SUCCESS THROUGH FAILURE: UPDATE ON HEART FAILURE WITH PRESERVED EJECTION FRACTION NONE
 ACHIEVING SUCCESS THROUGH FAILURE: UPDATE ON HEART FAILURE WITH PRESERVED EJECTION FRACTION Lori M. Tam, MD Providence Heart Institute DISCLOSURES NONE 1 OUTLINE Systolic vs. Diastolic Heart Failure New
ACHIEVING SUCCESS THROUGH FAILURE: UPDATE ON HEART FAILURE WITH PRESERVED EJECTION FRACTION Lori M. Tam, MD Providence Heart Institute DISCLOSURES NONE 1 OUTLINE Systolic vs. Diastolic Heart Failure New
Satish K Surabhi, MD.FACC,FSCAI,RPVI Medical Director, Cardiac Cath Labs AnMed Health Heart & Vascular Care
 Satish K Surabhi, MD.FACC,FSCAI,RPVI Medical Director, Cardiac Cath Labs AnMed Health Heart & Vascular Care None Fig. 1. Progression of Heart Failure.With each hospitalization for acute heart failure,
Satish K Surabhi, MD.FACC,FSCAI,RPVI Medical Director, Cardiac Cath Labs AnMed Health Heart & Vascular Care None Fig. 1. Progression of Heart Failure.With each hospitalization for acute heart failure,
Contemporary Management of Heart Failure. Keerthy K Narisetty, MD Comprehensive Heart Failure Management Program BHHI Primary Care Symposium
 Contemporary Management of Heart Failure Keerthy K Narisetty, MD Comprehensive Heart Failure Management Program BHHI Primary Care Symposium Disclosures I have no relevant relationships with commercial
Contemporary Management of Heart Failure Keerthy K Narisetty, MD Comprehensive Heart Failure Management Program BHHI Primary Care Symposium Disclosures I have no relevant relationships with commercial
RAAS blocker + B Blocker Troubleshooting
 RAAS blocker + B Blocker Troubleshooting Heart Failure ECHO Clinic Virtual Heart Failure Consultation and Education Prof Ken McDonald & Dr. Patricia Campbell 13 th March 2017 HF activates 3 neurohormonal
RAAS blocker + B Blocker Troubleshooting Heart Failure ECHO Clinic Virtual Heart Failure Consultation and Education Prof Ken McDonald & Dr. Patricia Campbell 13 th March 2017 HF activates 3 neurohormonal
UPDATES IN MANAGEMENT OF HF
 UPDATES IN MANAGEMENT OF HF Jennifer R Brown MD, MS Heart Failure Specialist Medstar Cardiology Associates DC ACP Meeting Fall 2017 Disclosures: speaker bureau for novartis speaker bureau for actelion
UPDATES IN MANAGEMENT OF HF Jennifer R Brown MD, MS Heart Failure Specialist Medstar Cardiology Associates DC ACP Meeting Fall 2017 Disclosures: speaker bureau for novartis speaker bureau for actelion
Outline. Classification by LVEF Conventional Therapy New Therapies. Ivabradine Sacubitril/valsartan
 New Pharmacological Therapies for Heart Failure Mark Drazner, MD, MSc Clinical Chief of Cardiology Medical Director, CHF/VAD/Transplant James M. Wooten Chair in Cardiology UT Southwestern Medical Center
New Pharmacological Therapies for Heart Failure Mark Drazner, MD, MSc Clinical Chief of Cardiology Medical Director, CHF/VAD/Transplant James M. Wooten Chair in Cardiology UT Southwestern Medical Center
Drugs acting on the reninangiotensin-aldosterone
 Drugs acting on the reninangiotensin-aldosterone system John McMurray Eugene Braunwald Scholar in Cardiovascular Diseases, Brigham and Women s Hospital, Boston & Visiting Professor, Harvard Medical School
Drugs acting on the reninangiotensin-aldosterone system John McMurray Eugene Braunwald Scholar in Cardiovascular Diseases, Brigham and Women s Hospital, Boston & Visiting Professor, Harvard Medical School
Long-Term Care Updates
 Long-Term Care Updates July 2015 By Amy Friedman Wilson, PharmD Heart failure (HF) is a clinical condition in which ventricular filling or ejection of blood is structurally or functionally impaired. 1
Long-Term Care Updates July 2015 By Amy Friedman Wilson, PharmD Heart failure (HF) is a clinical condition in which ventricular filling or ejection of blood is structurally or functionally impaired. 1
Updates in Congestive Heart Failure
 Updates in Congestive Heart Failure GREGORY YOST, DO JOHNSTOWN CARDIOVASCULAR ASSOCIATES 1/28/2018 Disclosures Edwards speaker on Sapien3 valves (TAVR) Stages A-D and NYHA Classes I-IV Stage A: High risk
Updates in Congestive Heart Failure GREGORY YOST, DO JOHNSTOWN CARDIOVASCULAR ASSOCIATES 1/28/2018 Disclosures Edwards speaker on Sapien3 valves (TAVR) Stages A-D and NYHA Classes I-IV Stage A: High risk
Heart Failure with Reduced EF. Dino Recchia, MD, FACC, FHFSA
 Heart Failure with Reduced EF Dino Recchia, MD, FACC, FHFSA Heart Failure HF is the end phenotype of almost all CV disorders Complex clinical syndrome resulting from any structural or functional impairment
Heart Failure with Reduced EF Dino Recchia, MD, FACC, FHFSA Heart Failure HF is the end phenotype of almost all CV disorders Complex clinical syndrome resulting from any structural or functional impairment
The CCS Heart Failure Companion: Bridging Guidelines to your Practice
 The CCS Heart Failure Companion: Bridging Guidelines to your Practice Looking for practical answers concerning optimal heart failure care? The CCS Heart Failure Guidelines Companion can help. The Canadian
The CCS Heart Failure Companion: Bridging Guidelines to your Practice Looking for practical answers concerning optimal heart failure care? The CCS Heart Failure Guidelines Companion can help. The Canadian
Target dose achievement of evidencebased medications in patients with heart failure with reduced ejection fraction attending a heart failure clinic
 Target dose achievement of evidencebased medications in patients with heart failure with reduced ejection fraction attending a heart failure clinic June Chen 1, Charlotte Galenza 1, Justin Ezekowitz 2,3,
Target dose achievement of evidencebased medications in patients with heart failure with reduced ejection fraction attending a heart failure clinic June Chen 1, Charlotte Galenza 1, Justin Ezekowitz 2,3,
SGK 2016 Session: Postgraduate Course in Heart Failure Lausanne, 15. June 2016 Heart Failure Guidelines 2016
 SGK 2016 Session: Postgraduate Course in Heart Failure Lausanne, 15. June 2016 Heart Failure Guidelines 2016 Matthias Nägele, MD University Hospital Zurich Disclosures I have nothing to disclose. The new
SGK 2016 Session: Postgraduate Course in Heart Failure Lausanne, 15. June 2016 Heart Failure Guidelines 2016 Matthias Nägele, MD University Hospital Zurich Disclosures I have nothing to disclose. The new
ARNI (Angiotensin Receptor blocker / Neprilysin Inhibitors [Sacubutril/Valsartan]) Heart Failure Medication Initiation and Titration
![ARNI (Angiotensin Receptor blocker / Neprilysin Inhibitors [Sacubutril/Valsartan]) Heart Failure Medication Initiation and Titration](/thumbs/77/76069192.jpg "ARNI (Angiotensin Receptor blocker / Neprilysin Inhibitors [Sacubutril/Valsartan]) Heart Failure Medication Initiation and Titration") ARNI (Angiotensin Receptor blocker / Neprilysin Inhibitors [Sacubutril/Valsartan]) Heart Failure Medication and Symptomatic HF despite ACEI/ARB and B-blocker therapy Bilateral renal artery stenosis Moderate/Severe
ARNI (Angiotensin Receptor blocker / Neprilysin Inhibitors [Sacubutril/Valsartan]) Heart Failure Medication and Symptomatic HF despite ACEI/ARB and B-blocker therapy Bilateral renal artery stenosis Moderate/Severe
Akash Ghai MD, FACC February 27, No Disclosures
 Akash Ghai MD, FACC February 27, 2015 No Disclosures Epidemiology Lifetime risk is > 20% for American s older than 40 years old. > 650,000 new cases diagnosed each year. Incidence increases with age: 2%
Akash Ghai MD, FACC February 27, 2015 No Disclosures Epidemiology Lifetime risk is > 20% for American s older than 40 years old. > 650,000 new cases diagnosed each year. Incidence increases with age: 2%
Disclosure of Relationships
 Disclosure of Relationships Over the past 12 months Dr Ruilope has served as Consultant and Speakers Bureau member of Astra-Zeneca, Bayer, Daiichi-Sankyo, Menarini, Novartis, Otsuka, Pfizer, Relypsa, Servier
Disclosure of Relationships Over the past 12 months Dr Ruilope has served as Consultant and Speakers Bureau member of Astra-Zeneca, Bayer, Daiichi-Sankyo, Menarini, Novartis, Otsuka, Pfizer, Relypsa, Servier
New Medications In the Field of Cardiology
 New Medications In the Field of Cardiology Hazal Babadagli, BScPharm, PharmD April 7, 2017 Outline Mechanism of action Evidence behind the medication Implications to disease management Contraindications
New Medications In the Field of Cardiology Hazal Babadagli, BScPharm, PharmD April 7, 2017 Outline Mechanism of action Evidence behind the medication Implications to disease management Contraindications
Disclosures for Presenter
 A Comparison of Angiotensin Receptor- Neprilysin Inhibition (ARNI) With ACE Inhibition in the Long-Term Treatment of Chronic Heart Failure With a Reduced Ejection Fraction Milton Packer, John J.V. McMurray,
A Comparison of Angiotensin Receptor- Neprilysin Inhibition (ARNI) With ACE Inhibition in the Long-Term Treatment of Chronic Heart Failure With a Reduced Ejection Fraction Milton Packer, John J.V. McMurray,
ARxCH. Annual Review of Changes in Healthcare. Entresto: An Overview for Pharmacists
 Entresto: An Overview for Pharmacists David Comshaw, PharmD Candidate 2019 1 Gyen Musgrave, PharmD Candidate 2019 1 Suzanne Surowiec, PharmD, BCACP 1 Jason Guy, PharmD 1 1 University of Findlay College
Entresto: An Overview for Pharmacists David Comshaw, PharmD Candidate 2019 1 Gyen Musgrave, PharmD Candidate 2019 1 Suzanne Surowiec, PharmD, BCACP 1 Jason Guy, PharmD 1 1 University of Findlay College
Management of chronic heart failure: pharmacology. Giuseppe M.C. Rosano, MD, PhD, FHFA
 Management of chronic heart failure: pharmacology. Giuseppe M.C. Rosano, MD, PhD, FHFA Declaration of potential conflict of interests Type of job or financial support Salary Ordinary funds Position in
Management of chronic heart failure: pharmacology. Giuseppe M.C. Rosano, MD, PhD, FHFA Declaration of potential conflict of interests Type of job or financial support Salary Ordinary funds Position in
Practical considerations for the use of ARNI in CHF: clinical cases. J. Parissis, Heart Failure Clinic, University of Athens, Athens, Greece
 Practical considerations for the use of ARNI in CHF: clinical cases J. Parissis, Heart Failure Clinic, University of Athens, Athens, Greece Disclosures: Research grants and honoraria for lectures from
Practical considerations for the use of ARNI in CHF: clinical cases J. Parissis, Heart Failure Clinic, University of Athens, Athens, Greece Disclosures: Research grants and honoraria for lectures from
How Do You Mend a Broken Heart: The New Agents to Treat HF Paradigm Shift or Just the Same Old Drugs?
 How Do You Mend a Broken Heart: The New Agents to Treat HF Paradigm Shift or Just the Same Old Drugs? Gregg C. Fonarow, MD FACC, FAHA, FHFSA Co-Chief UCLA Division of Cardiology Director, Ahmanson-UCLA
How Do You Mend a Broken Heart: The New Agents to Treat HF Paradigm Shift or Just the Same Old Drugs? Gregg C. Fonarow, MD FACC, FAHA, FHFSA Co-Chief UCLA Division of Cardiology Director, Ahmanson-UCLA
Introduction to Heart Failure. Mauricio Velez, M.D. Transplant Cardiologist APACVS 2018 April 5-7 Miami, FL
 Introduction to Heart Failure Mauricio Velez, M.D. Transplant Cardiologist APACVS 2018 April 5-7 Miami, FL Disclosures No relevant financial relationships to disclose Objectives and Outline Define heart
Introduction to Heart Failure Mauricio Velez, M.D. Transplant Cardiologist APACVS 2018 April 5-7 Miami, FL Disclosures No relevant financial relationships to disclose Objectives and Outline Define heart
2/15/2017. Disclosures. Heart Failure = Big Problem. Heart Failure Update Reducing Hospitalizations and Improving Patient Outcomes 02/18/2017
 Heart Failure Update Reducing Hospitalizations and Improving Patient Outcomes 02/18/2017 Julio A. Barcena, M.D. South Miami Heart Specialists Disclosures I have no relevant commercial relationships to
Heart Failure Update Reducing Hospitalizations and Improving Patient Outcomes 02/18/2017 Julio A. Barcena, M.D. South Miami Heart Specialists Disclosures I have no relevant commercial relationships to
Combination of renin-angiotensinaldosterone. how to choose?
 Combination of renin-angiotensinaldosterone system inhibitors how to choose? Karl Swedberg Professor of Medicine Sahlgrenska Academy University of Gothenburg karl.swedberg@gu.se Disclosures Research grants
Combination of renin-angiotensinaldosterone system inhibitors how to choose? Karl Swedberg Professor of Medicine Sahlgrenska Academy University of Gothenburg karl.swedberg@gu.se Disclosures Research grants
Outline. Chronic Heart Failure: Update on Effective Monitoring and Treatment. Heart Failure Epidemiology. Michael G.
 Chronic Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center Scientific
Chronic Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center Scientific
ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure
 Patients t with acute heart failure frequently develop chronic heart failure Patients with chronic heart failure frequently decompensate acutely ESC Guidelines for the Diagnosis and A clinical response
Patients t with acute heart failure frequently develop chronic heart failure Patients with chronic heart failure frequently decompensate acutely ESC Guidelines for the Diagnosis and A clinical response
Heart Failure 101 The Basic Principles of Diagnosis & Management
 Heart Failure 101 The Basic Principles of Diagnosis & Management Bill Tran, MD Non Invasive Cardiologist February 24, 2018 What the eye does not see and the mind does not know, does not exist. DH Lawrence
Heart Failure 101 The Basic Principles of Diagnosis & Management Bill Tran, MD Non Invasive Cardiologist February 24, 2018 What the eye does not see and the mind does not know, does not exist. DH Lawrence
Guidelines for the Prescribing of Sacubitril / Valsartan
 Hull & East Riding Prescribing Committee Guidelines for the Prescribing of Sacubitril / Valsartan 1. BACKGROUND Sacubitril valsartan is an angiotensin receptor neprilysin inhibitor, including both a neprilysin
Hull & East Riding Prescribing Committee Guidelines for the Prescribing of Sacubitril / Valsartan 1. BACKGROUND Sacubitril valsartan is an angiotensin receptor neprilysin inhibitor, including both a neprilysin
A patient with decompensated HF
 A patient with decompensated HF Professor Michel KOMAJDA University Pierre & Marie Curie Pitie Salpetriere Hospital Department of Cardiology Paris (France) Declaration Of Interest 2010 Speaker : Servier,
A patient with decompensated HF Professor Michel KOMAJDA University Pierre & Marie Curie Pitie Salpetriere Hospital Department of Cardiology Paris (France) Declaration Of Interest 2010 Speaker : Servier,
ACE inhibitors: still the gold standard?
 ACE inhibitors: still the gold standard? Session: Twenty-five years after CONSENSUS What have we learnt about the RAAS in heart failure? Lars Køber, MD, D.Sci Department of Cardiology Rigshospitalet University
ACE inhibitors: still the gold standard? Session: Twenty-five years after CONSENSUS What have we learnt about the RAAS in heart failure? Lars Køber, MD, D.Sci Department of Cardiology Rigshospitalet University
State-of-the-Art Management of Chronic Systolic Heart Failure
 State-of-the-Art Management of Chronic Systolic Heart Failure Michael McCulloch, MD 17 th Annual Cardiovascular Update Intermountain Medical Center December 16, 2017 Disclosures: I have no financial disclosures
State-of-the-Art Management of Chronic Systolic Heart Failure Michael McCulloch, MD 17 th Annual Cardiovascular Update Intermountain Medical Center December 16, 2017 Disclosures: I have no financial disclosures
Heart Failure Update. Bibiana Cujec MD May 2015
 Heart Failure Update Bibiana Cujec MD May 2015 Disclosures Participation in clinical trial GUIDE IT (BNP in management of HF) Plan Review of new trials/ccs guidelines Management of heart failure: cases
Heart Failure Update Bibiana Cujec MD May 2015 Disclosures Participation in clinical trial GUIDE IT (BNP in management of HF) Plan Review of new trials/ccs guidelines Management of heart failure: cases
Known Actions of Digoxin
 Known Actions of Digoxin Hemodynamic effects in heart failure Increases cardiac output, no effect on blood pressure Decreases PCWP Increases LVEF (
Known Actions of Digoxin Hemodynamic effects in heart failure Increases cardiac output, no effect on blood pressure Decreases PCWP Increases LVEF (
Cardiovascular Pharmacotherapy
 Cardiovascular Pharmacotherapy Overview Mechanism of cardiovascular drugs Indications and clinical use in cardiology Renin-Angiotensin Inhibitors: Angiotensin-Converting Enzyme Inhibitors, Angiotensin
Cardiovascular Pharmacotherapy Overview Mechanism of cardiovascular drugs Indications and clinical use in cardiology Renin-Angiotensin Inhibitors: Angiotensin-Converting Enzyme Inhibitors, Angiotensin
Heart Failure. Subjective SOB (shortness of breath) Peripheral edema. Orthopnea (2-3 pillows) PND (paroxysmal nocturnal dyspnea)
 Peripheral edema. Orthopnea (2-3 pillows) PND (paroxysmal nocturnal dyspnea)") Pharmacology I. Definitions A. Heart Failure (HF) Heart Failure Ezra Levy, Pharm.D. HF Results when one or both ventricles are unable to pump sufficient blood to meet the body s needs There are 2 types
Pharmacology I. Definitions A. Heart Failure (HF) Heart Failure Ezra Levy, Pharm.D. HF Results when one or both ventricles are unable to pump sufficient blood to meet the body s needs There are 2 types
Estimated 5.7 million Americans with HF. 915, 000 new HF cases annually, HF incidence approaches
 Heart Failure: Management of a Chronic Disease Jenny Bauerly RN, CHFN, APRN-BC Heart Failure (HF) Definition A complex clinical syndrome that can result from any structural or functional cardiac disorder
Heart Failure: Management of a Chronic Disease Jenny Bauerly RN, CHFN, APRN-BC Heart Failure (HF) Definition A complex clinical syndrome that can result from any structural or functional cardiac disorder
ANGIOTENSIN RECEPTOR-NEPRILYSIN INHIBITORS IN HEART FAILURE FROM CHD
 ANGIOTENSIN RECEPTOR-NEPRILYSIN INHIBITORS IN HEART FAILURE FROM CHD Karen Stout, MD FACC Professor, Medicine/Pediatrics University of Washington Seattle, WA USA No disclosures Case 35 year old man with
ANGIOTENSIN RECEPTOR-NEPRILYSIN INHIBITORS IN HEART FAILURE FROM CHD Karen Stout, MD FACC Professor, Medicine/Pediatrics University of Washington Seattle, WA USA No disclosures Case 35 year old man with
Congestive Heart Failure 2015
 Definition Congestive Heart Failure 215 JP Mehegan/ Mercy Cardiology n Cardiac failure; Congestive heart failure; Chronic heart failure (synonyms) n When the heart is unable to pump sufficiently and at
Definition Congestive Heart Failure 215 JP Mehegan/ Mercy Cardiology n Cardiac failure; Congestive heart failure; Chronic heart failure (synonyms) n When the heart is unable to pump sufficiently and at
Update in Congestive Hear Failure DRAGOS VESBIANU MD
 Update in Congestive Hear Failure DRAGOS VESBIANU MD Case 58 yo AAM c/o shortness of breath for 3 weeks. Used to walk one mile per day and now he has noticed that he gets short of breath after 2 blocks.
Update in Congestive Hear Failure DRAGOS VESBIANU MD Case 58 yo AAM c/o shortness of breath for 3 weeks. Used to walk one mile per day and now he has noticed that he gets short of breath after 2 blocks.
New Paradigms in Rx of Symptomati Heart Failure:Role of Ivabradine & Angiotensin Neprilysin Inhibition
 New Paradigms in Rx of Symptomati Heart Failure:Role of Ivabradine & Angiotensin Neprilysin Inhibition Prakash Deedwania, MD, FACC, FACP, FCCP, FAHA Professor of Medicine, UCSF School of Medicine, Director,
New Paradigms in Rx of Symptomati Heart Failure:Role of Ivabradine & Angiotensin Neprilysin Inhibition Prakash Deedwania, MD, FACC, FACP, FCCP, FAHA Professor of Medicine, UCSF School of Medicine, Director,
CADTH CANADIAN DRUG EXPERT COMMITTEE FINAL RECOMMENDATION
 CADTH CANADIAN DRUG EXPERT COMMITTEE FINAL RECOMMENDATION SACUBITRIL/VALSARTAN (Entresto Novartis Pharmaceuticals) Indication: Heart Failure With Reduced Ejection Fraction Recommendation: The Canadian
CADTH CANADIAN DRUG EXPERT COMMITTEE FINAL RECOMMENDATION SACUBITRIL/VALSARTAN (Entresto Novartis Pharmaceuticals) Indication: Heart Failure With Reduced Ejection Fraction Recommendation: The Canadian
Checklist for Treating Heart Failure. Alan M. Kaneshige MD, FACC, FASE Oklahoma Heart Institute
 Checklist for Treating Heart Failure Alan M. Kaneshige MD, FACC, FASE Oklahoma Heart Institute Novartis Disclosure Heart Failure (HF) a complex clinical syndrome that arises secondary to abnormalities
Checklist for Treating Heart Failure Alan M. Kaneshige MD, FACC, FASE Oklahoma Heart Institute Novartis Disclosure Heart Failure (HF) a complex clinical syndrome that arises secondary to abnormalities
Overview & Update on the Utilization of the Natriuretic Peptides in Heart Failure
 June 28, 2016 Overview & Update on the Utilization of the Natriuretic Peptides in Heart Failure Linda C. Rogers, PhD, DABCC, FACB. Agenda Overview of the Natriuretic Peptides and Efficacy studies Similarities
June 28, 2016 Overview & Update on the Utilization of the Natriuretic Peptides in Heart Failure Linda C. Rogers, PhD, DABCC, FACB. Agenda Overview of the Natriuretic Peptides and Efficacy studies Similarities
Heart Failure: Combination Treatment Strategies
 Heart Failure: Combination Treatment Strategies M. McDonald MD, FRCP State of the Heart Symposium May 28, 2011 None Disclosures Case 69 F, prior MIs (LV ejection fraction 25%), HTN No demonstrable ischemia
Heart Failure: Combination Treatment Strategies M. McDonald MD, FRCP State of the Heart Symposium May 28, 2011 None Disclosures Case 69 F, prior MIs (LV ejection fraction 25%), HTN No demonstrable ischemia
Highlight Session Heart failure and cardiomyopathies Michel KOMAJDA Paris France
 Highlight Session 2014 Heart failure and cardiomyopathies Michel KOMAJDA Paris France # esccongress www.escardio.org/esc2014 HEART FAILURE AND CARDIOMYOPATHIES TOPIC 1 Drug Therapy TOPIC 2 Device Therapy
Highlight Session 2014 Heart failure and cardiomyopathies Michel KOMAJDA Paris France # esccongress www.escardio.org/esc2014 HEART FAILURE AND CARDIOMYOPATHIES TOPIC 1 Drug Therapy TOPIC 2 Device Therapy
Management of chronic heart failure: update J. Parissis Attikon University Hospital
 Management of chronic heart failure: update 2015 J. Parissis Attikon University Hospital Disclosures: received honoraria for lectures from Servier, Pfizer, Novartis Discharges in Thousands Heart Failure
Management of chronic heart failure: update 2015 J. Parissis Attikon University Hospital Disclosures: received honoraria for lectures from Servier, Pfizer, Novartis Discharges in Thousands Heart Failure
Chronic Heart Failure Therapies: Transforming the Landscape
 Chronic Heart Failure Therapies: Transforming the Landscape Dr. Nadia Giannetti Chief of Cardiology Medical Director, Heart Failure and Heart Transplant Program McGill University Health Center Conflict
Chronic Heart Failure Therapies: Transforming the Landscape Dr. Nadia Giannetti Chief of Cardiology Medical Director, Heart Failure and Heart Transplant Program McGill University Health Center Conflict
The ACC Heart Failure Guidelines
 The ACC Heart Failure Guidelines Fakhr Alayoubi, Msc,R Ph President of SCCP Cardiology Clinical Pharmacist Assistant Professor At King Saud University King Khalid University Hospital Riyadh-KSA 2017 ACC/AHA/HFSA
The ACC Heart Failure Guidelines Fakhr Alayoubi, Msc,R Ph President of SCCP Cardiology Clinical Pharmacist Assistant Professor At King Saud University King Khalid University Hospital Riyadh-KSA 2017 ACC/AHA/HFSA
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Neprilysin Inhibitor (Entresto ) Page 1 of 6 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Neprilysin Inhibitor (Entresto ) Prime Therapeutics will review Prior
Neprilysin Inhibitor (Entresto ) Page 1 of 6 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Neprilysin Inhibitor (Entresto ) Prime Therapeutics will review Prior
PROGRESS AT LAST?: REVIEWING RECENTLY UPDATED ACCF/AHA HEART FAILURE GUIDELINES
 PROGRESS AT LAST?: REVIEWING RECENTLY UPDATED ACCF/AHA HEART FAILURE GUIDELINES Jon Linder, Pharm.D. PGY1 Pharmacy Resident Iowa City VA Health Care System Objectives for Pharmacists Summarize the burden
PROGRESS AT LAST?: REVIEWING RECENTLY UPDATED ACCF/AHA HEART FAILURE GUIDELINES Jon Linder, Pharm.D. PGY1 Pharmacy Resident Iowa City VA Health Care System Objectives for Pharmacists Summarize the burden
Guideline-Directed Medical Therapy
 Guideline-Directed Medical Therapy Cardiovascular Outcomes Assessment of the MitraClip Percutaneous Therapy for Heart Failure Patients with Functional Mitral Regurgitation OPTIMAL THERAPY (As defined in
Guideline-Directed Medical Therapy Cardiovascular Outcomes Assessment of the MitraClip Percutaneous Therapy for Heart Failure Patients with Functional Mitral Regurgitation OPTIMAL THERAPY (As defined in
Patient details GP details Specialist details Name GP Name Dr Specialist Name Dr R. Horton
 Rationale for Initiation, Continuation and Discontinuation (RICaD) Sacubitril/Valsartan (Entresto) For the treatment of symptomatic heart failure with reduced ejection fraction (NICE TA388) This document
Rationale for Initiation, Continuation and Discontinuation (RICaD) Sacubitril/Valsartan (Entresto) For the treatment of symptomatic heart failure with reduced ejection fraction (NICE TA388) This document
2017 Canadian Cardiovascular Society Heart Failure Guideline
 2017 Canadian Cardiovascular Society Heart Failure Guideline A Preview Gordon Moe, MSC, MD, FRCP(C), FACC, FAHA Presenter Disclosure Dr. Gordon Moe Presenter Topic: CCS 2017 HF guidelines update Relationships
2017 Canadian Cardiovascular Society Heart Failure Guideline A Preview Gordon Moe, MSC, MD, FRCP(C), FACC, FAHA Presenter Disclosure Dr. Gordon Moe Presenter Topic: CCS 2017 HF guidelines update Relationships
Therapeutic Targets and Interventions
 Therapeutic Targets and Interventions Ali Valika, MD, FACC Advanced Heart Failure and Pulmonary Hypertension Advocate Medical Group Midwest Heart Foundation Disclosures: 1. Novartis: Speaker Honorarium
Therapeutic Targets and Interventions Ali Valika, MD, FACC Advanced Heart Failure and Pulmonary Hypertension Advocate Medical Group Midwest Heart Foundation Disclosures: 1. Novartis: Speaker Honorarium
Pravin Manga Division of Cardiology Department of Medicine University of Witwatersrand
 Pravin Manga Division of Cardiology Department of Medicine University of Witwatersrand Overview Definition Epidemiology Biomarkers Treatment Clinical Heart Failure: Syndrome in which patients have typical
Pravin Manga Division of Cardiology Department of Medicine University of Witwatersrand Overview Definition Epidemiology Biomarkers Treatment Clinical Heart Failure: Syndrome in which patients have typical
Heart Failure (HF): Scope of the Problem. Temporal Trends in Age-Adjusted Survival After HF Diagnosis. More malignant than most cancers
: Scope of the Problem. Temporal Trends in Age-Adjusted Survival After HF Diagnosis. More malignant than most cancers") Patients in US (millions) Heart Failure (HF): Scope of the Problem 1 4 2 3.5 4. 1. 1991 21 237 US prevalence*: 5. million US annual incidence: 7, Annual mortality: 22,754 5-1% depending on severity Cost:
Patients in US (millions) Heart Failure (HF): Scope of the Problem 1 4 2 3.5 4. 1. 1991 21 237 US prevalence*: 5. million US annual incidence: 7, Annual mortality: 22,754 5-1% depending on severity Cost:
Aldosterone Antagonism in Heart Failure: Now for all Patients?
 Aldosterone Antagonism in Heart Failure: Now for all Patients? Inder Anand, MD, FRCP, D Phil (Oxon.) Professor of Medicine, University of Minnesota, Director Heart Failure Program, VA Medical Center 111C
Aldosterone Antagonism in Heart Failure: Now for all Patients? Inder Anand, MD, FRCP, D Phil (Oxon.) Professor of Medicine, University of Minnesota, Director Heart Failure Program, VA Medical Center 111C
Contemporary Advanced Heart Failure Therapy
 Contemporary Advanced Heart Failure Therapy Andrew Boyle, MD Professor of Medicine Medical Director of Advanced Heart Failure Thomas Jefferson University Philadelphia, PA Audience Response Question 40
Contemporary Advanced Heart Failure Therapy Andrew Boyle, MD Professor of Medicine Medical Director of Advanced Heart Failure Thomas Jefferson University Philadelphia, PA Audience Response Question 40
Heart Failure Medical and Surgical Treatment
 Heart Failure Medical and Surgical Treatment Daniel S. Yip, M.D. Medical Director, Heart Failure and Transplantation Mayo Clinic Second Annual Lakeland Regional Health Cardiovascular Symposium February
Heart Failure Medical and Surgical Treatment Daniel S. Yip, M.D. Medical Director, Heart Failure and Transplantation Mayo Clinic Second Annual Lakeland Regional Health Cardiovascular Symposium February
A New Future In Heart Failure (Should we reshuffle the deck?)
") A New Future In Heart Failure (Should we reshuffle the deck?) DR. HEMANT SAHA, MD, MRCP(UK) AGA KHAN UNIVERSITY HOSPITAL, NAIROBI Disclosures Nothing to disclose. Objectives 1. Historical Perspectives
A New Future In Heart Failure (Should we reshuffle the deck?) DR. HEMANT SAHA, MD, MRCP(UK) AGA KHAN UNIVERSITY HOSPITAL, NAIROBI Disclosures Nothing to disclose. Objectives 1. Historical Perspectives
HeFSSA Practitioners Program 2017 Theme The Patient Journey: Feel Good and Live Long. Case Study 2
 HeFSSA Practitioners Program 2017 Theme The Patient Journey: Feel Good and Live Long Case Study 2 HEART FAILURE WITH MID-RANGE EJECTION FRACTION TREATMENT OPTIONS CLINICAL CASE MEDICAL HISTORY 59-year-old
HeFSSA Practitioners Program 2017 Theme The Patient Journey: Feel Good and Live Long Case Study 2 HEART FAILURE WITH MID-RANGE EJECTION FRACTION TREATMENT OPTIONS CLINICAL CASE MEDICAL HISTORY 59-year-old
ENTRESTO (sacubitril and valsartan) oral tablet
 oral tablet") ENTRESTO (sacubitril and valsartan) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This
ENTRESTO (sacubitril and valsartan) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This
Heart Failure Medications: Who Needs What Drug Now? Disclosures
 Heart Failure Medications: Who Needs What Drug Now? Simon Jackson MD FRCPC MMedEd Professor of Medicine (Cardiology) Dalhousie 1 Disclosures Honoraria and educational grants from: Actelion (medications
Heart Failure Medications: Who Needs What Drug Now? Simon Jackson MD FRCPC MMedEd Professor of Medicine (Cardiology) Dalhousie 1 Disclosures Honoraria and educational grants from: Actelion (medications
Balanced information for better care. Heart failure: Managing risk and improving patient outcomes
 Balanced information for better care Heart failure: Managing risk and improving patient outcomes Heart failure increases hospitalization Heart failure is the most common medical reason for hospitalization
Balanced information for better care Heart failure: Managing risk and improving patient outcomes Heart failure increases hospitalization Heart failure is the most common medical reason for hospitalization
LITERATURE REVIEW: HEART FAILURE. Chief Residents
 LITERATURE REVIEW: HEART FAILURE Chief Residents Heart Failure EF 40% HFrEF Problem with contractility EF 40-50% HFmrEF EF > 50% HFpEF Problem with filling/relaxation RISK FACTORS Post MI HTN DM Obesity
LITERATURE REVIEW: HEART FAILURE Chief Residents Heart Failure EF 40% HFrEF Problem with contractility EF 40-50% HFmrEF EF > 50% HFpEF Problem with filling/relaxation RISK FACTORS Post MI HTN DM Obesity
HEART FAILURE. Heart Failure in the US. Heart Failure (HF) 3/2/2014
 3/2/2014") HEART FAILURE Martina Frost, PA-C Desert Cardiology of Tucson Northwest Medical Center March 2014 Heart Failure in the US Prevalence - ~5 million 650,000 new cases annually 300,000 deaths annually Leading
HEART FAILURE Martina Frost, PA-C Desert Cardiology of Tucson Northwest Medical Center March 2014 Heart Failure in the US Prevalence - ~5 million 650,000 new cases annually 300,000 deaths annually Leading
Heart Failure. Dr. William Vosik. January, 2012
 Heart Failure Dr. William Vosik January, 2012 Questions for clinicians to ask Is this heart failure? What is the underlying cause? What are the associated disease processes? Which evidence-based treatment
Heart Failure Dr. William Vosik January, 2012 Questions for clinicians to ask Is this heart failure? What is the underlying cause? What are the associated disease processes? Which evidence-based treatment
heart failure John McMurray University of Glasgow.
 A to Z of RAAS blockade in heart failure John McMurray BHF Cardiovascular Research Centre University of Glasgow. RAAS inhibition in CHF ACE inhibition in patients with low LVEF CHF CONSENSUS Enalapril
A to Z of RAAS blockade in heart failure John McMurray BHF Cardiovascular Research Centre University of Glasgow. RAAS inhibition in CHF ACE inhibition in patients with low LVEF CHF CONSENSUS Enalapril
DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
Hypertension (JNC-8)
") Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Heart Failure Pharmacotherapy An Update
 Heart Failure Pharmacotherapy An Update Kenneth Mishler, PharmD, MBA Objectives Review the epidemiology of heart failure (HF) Review evidence based guidelines for the use of mediations used to treat HF
Heart Failure Pharmacotherapy An Update Kenneth Mishler, PharmD, MBA Objectives Review the epidemiology of heart failure (HF) Review evidence based guidelines for the use of mediations used to treat HF