Heart Failure Symposium: Case Presentation (The crash and burn and the smoldering patient)
|
|
|
- Abraham Smith
- 5 years ago
- Views:
Transcription
1 Heart Failure Symposium: (The crash and burn and the smoldering patient) Patrick C. Magnus, MBBS, MPH Clinical Fellow Section of Cardiology Dartmouth Hitchcock Medical Center (Case 1) 66 year old man, transferred from an OSH, for further management of an NSTEMI 6 days prior to presentation he describes episodes of feeling just not myself associated with episodes of dizziness, blurred vision, diaphoresis and pain between his shoulder blades lasting 10 minutes He had multiples similar episodes in the ensuing days On the morning of presentation he was awoken with similar symptoms but more severe, additionally he felt confused and developed anterior chest tightness 2 Past Medical/Surgical History Allergies Anxiety disorder Asthma Oral cancer (Base of tongue) s/p resection and radiation therapy complicated by radiation induced osteonecrosis of the jaw requiring long term Abx therapy (Doxycycline) Medications: ASA 81 mg Saw Palmetto Glucosamine/Chondroitin B complex Vitamin D Lorazepam Cetirizine Doxycycline Allergies: Wood dust 3 1
2 Family History: Heart disease (Mother) Cancer (Father) Social History: Divorced Retired carpenter Active, primarily hunting Former smoker, 25 pack year 4 Findings at OSH: Vitals: BP 103/64 P 93 R 16 O2 96% Continues to have on going chest pain Physical examination unrevealing except for low O2 sats Na 140 K 3.8 Cl 103 CO2 27 BUN 21 Cr 1.6 Glu 220 Mg 1.7 Ca 9.1 WBC 16.1 H/H 14.8/45.2 Plt 216 Trop 2.56 D Dimer 582 CXR: Increased pulmonary vascular congestion; Pulmonary edema ECG 5 6 2
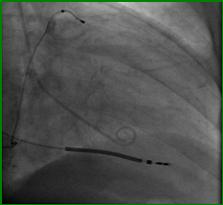
3 Initial Management: Oxygen (4 liters to maintain O2 sats) ASA 324 mg Clopidogrel 300 mg Heparin Nitroglycerin gtt Morphine sulphate Transferred to DHMC 7 On arrival to DHMC ICCU, he continues to have low level chest discomfort Physical examination: BP 118/72, P 87 (regular), R 16, O2 100% (4L O2) Ht 6 1, Wt 200lbs (BMI 26.4) General: Oriented, pleasant, mildly dyspneic but in no overt distress Resp: Bibasilar crackles, no wheeze Cards: S1, S2, +S3. JVP not elevated, No rubs or murmurs. Good pulses bilaterally Abd: Soft and NT. No organomegaly. Normal bowel sounds. No bruits Ext: No peripheral edema noted. Extremities are warm and appear well perfused 8 Cath lab course: Ao 93/61 (73), LVEDP 40 Developed worsening hypoxemia and increasing upper airway secretions and hypotension (MAP~50 mmhg) Intubated in the lab Limited echo in cath lab showed severely hypokinetic lateral and inferolateral walls, no significant MR 9 3




4 10 Diagnosis: Posterior STEMI complicated by cardiogenic shock 11 CVCC Course: Dopamine continued at 10 mcg/kg/min Up titrated Lasix drip started Spikes a temp and is pan cultured Worsening pulmonary edema Peak Trop/CK: 41.7/


5 CVCC Course: Afib with RVR with rates in the 120s DCCV fails to restore sinus rhythm Propofol added for additional sedation Amiodarone started Norepinephrine added for worsening hypotension Echo shows: EF 35 40% Anterolateral, inferolateral and inferior WMAs. PASP~38mmHg, Moderate to severe MR Right heart cath HD#3: LVEDP 18 mmhg PA PCWP CO CI SVR PVR PA Sat 46/ / / % Milrinone started: SVR ~ , CI Urine output improves Spikes temps, cultures and started on broad spectrum antibiotics 15 5
6 HD #4 5: Pressors and inotropic support weaned MAPs in the 60s IABP weaned and subsequently pulled Cultures negative x 48 hrs and Abx stopped Continues to spike temps (102) Extubated 16 Over the next few days: Diuresis is continued BUN/Cr continue to rise (91/2.1) Worsening O2 sats requiring re intubation CXR now showing bilateral moderate pleural effusions and left lower lobe infiltrate Broad spectrum antibiotics restarted for HAP Decreased urine output and MAP~50 mmhg Right heart cath: PA PCWP CO CI SVR 48/ Supported with Norepinephrine, Milrinone and Saline infusions Hemodynamics stabilize and renal function improve and he is extubated on HD#14 Eventually transferred from the CVCC to the ICCU and his HAP is treated Discharged to rehab after ~40 days 18 6
7 Summary: 66 y.o with posterior STEMI complicated by cardiogenic shock requiring IABP support, prolonged inotropic support and pressor support 19 (Case 2) 71 year old man with a h/o Chronic lymphocytic leukemia, Hypertension, Hyperlipidemia, Diabetes mellitus, and Bladder Ca Presents to DHMC with worsening SOB and weight gain Seen by the cardiology consult service for acute decompensated systolic heart failure refractory to standard diuretic therapy: 4 months earlier in Florida diagnosed with dilated ischemic cardiomyopathy EF~20% Underwent PCI to LAD and OM CRT D 2 admissions for ADSHF 20 Medical regimen: ASA Spironolactone Furosemide Carvedilol Atorvastatin Clopidogrel Allopurinol Meclizine Paroxitine KCl Metformin Albuterol Physical Examination: Overweight man, mild resp distress BP 87/70P 91 T 36.6 O2 96% Wt 224lbs Ht 5 11 (BMI 31.5 kg/m2) JVP 10 cm Bilateral crackles Distant heart sounds, no murmurs Bilateral leg edema 21 7






8 Data: Pro BNP 5,705 pg/ml WBC 16 20,000 Hb/Hct 9.7/27 Plt 201 BUN/Cr 16/0.77 Cardiac biomarkers negative ECG Paced rhythm
9 Right Heart Cath: RA RV PA PCWP CO CI PA Sat PVR TPR SVR TSR 14 42/17 47/ / /1.3 43% (33) Dobutamine 2.5 mcg/kg/min RA PA PCWP CI 23 58/ Dobutamine 5 mcg/kg/min RA PA PCWP CI 6 47/ Clinical status improves with Dobutamine Unable to wean inotropic support Arrangements made for out patient continuous infusion Develops more frequent ventricular arrhythmias Runs of NSVT ~20 beats 26 Transferred to Tufts Medical Center Undergoes implantation of HeartMate II Post op course complicated by: Need for re exploration for pericardial effusion and thrombus Atrial tachycardia requiring DCCV 27 9
10 Eventually discharged and is being followed as an out patient by the heart failure service Functionally NYHA class III Able to do ADLs No serious issues with VAD to date 28 Summary: 71 y.o with multiple medical comorbidities who presents with decompensated systolic heart failure (Ischemic CMP) Failed outpatient diuretic therapy Inotrope dependent Increased arrhythmia burden Undergoes LVAD implantation as destination therapy 29 Thank you Questions/Comments 10
Ventricular Assist Device: Are Early Interventions Superior? Hamang Patel, MD Section of Cardiomyopathy & Heart Transplantation
 Ventricular Assist Device: Are Early Interventions Superior? Hamang Patel, MD Section of Cardiomyopathy & Heart Transplantation Objectives Current rationale behind use of MCS Patient Selection Earlier?
Ventricular Assist Device: Are Early Interventions Superior? Hamang Patel, MD Section of Cardiomyopathy & Heart Transplantation Objectives Current rationale behind use of MCS Patient Selection Earlier?
Medical Treatment for acute Decompensated Heart Failure. Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011
 Medical Treatment for acute Decompensated Heart Failure Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011 2010 HFSA guidelines for ADHF 2009 focused update of the 2005 American College
Medical Treatment for acute Decompensated Heart Failure Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011 2010 HFSA guidelines for ADHF 2009 focused update of the 2005 American College
A walk through a STEMI
 A walk through a STEMI M.M. s Story Kim Robison Ashley Corcoran Situation M.M. is an 82 year old male brought in by private vehicle on 10/22/17 to the Emergency Department Pt. c/o left arm numbness, pain
A walk through a STEMI M.M. s Story Kim Robison Ashley Corcoran Situation M.M. is an 82 year old male brought in by private vehicle on 10/22/17 to the Emergency Department Pt. c/o left arm numbness, pain
Management of Heart Failure in the Hospitalized Patient. Ronald Witteles, M.D. Stanford University School of Medicine October 27, 2012
 Management of Heart Failure in the Hospitalized Patient Ronald Witteles, M.D. Stanford University School of Medicine October 27, 2012 I have nothing to disclose Disclosures What is Heart Failure? Not as
Management of Heart Failure in the Hospitalized Patient Ronald Witteles, M.D. Stanford University School of Medicine October 27, 2012 I have nothing to disclose Disclosures What is Heart Failure? Not as
New Concepts in Acute Coronary Syndromes Beyond 2000 (XX) Interactive Case Presentations
 Interactive Case Presentations") New Concepts in Acute Coronary Syndromes Beyond 2000 (XX) Interactive Case Presentations Dr. Richard Bon Surrey Memorial Hospital, Surrey, BC Canadian Cardiovascular Congress 2014 October 26, 2014 Conflicts
New Concepts in Acute Coronary Syndromes Beyond 2000 (XX) Interactive Case Presentations Dr. Richard Bon Surrey Memorial Hospital, Surrey, BC Canadian Cardiovascular Congress 2014 October 26, 2014 Conflicts
5AB Dysrhythmia Interpretation and Management 2016
 5AB Dysrhythmia Interpretation and Management 2016 How to complete your biennial ECG review: A website has been created that contains the basic review information. Use this as a reference during your review.
5AB Dysrhythmia Interpretation and Management 2016 How to complete your biennial ECG review: A website has been created that contains the basic review information. Use this as a reference during your review.
Clinical Case. Female, 62 years January 2016
 Clinical Case Female, 62 years January 2016 Dr. Ramón Corbalán H. Facultad de Medicina División de Enfermedades Cardiovasculares Pontificia Universidad Católica de Chile Clinical Hx Background: Ostheoartritis
Clinical Case Female, 62 years January 2016 Dr. Ramón Corbalán H. Facultad de Medicina División de Enfermedades Cardiovasculares Pontificia Universidad Católica de Chile Clinical Hx Background: Ostheoartritis
March yr. old male, newspaper writer, with worsening dyspnea /orthopnea past few months
 Case 1 March 2016 59 yr. old male, newspaper writer, with worsening dyspnea /orthopnea past few months PMH diabetes, celiac disease Reports chest discomfort, positional coughing and pedal edema last 10
Case 1 March 2016 59 yr. old male, newspaper writer, with worsening dyspnea /orthopnea past few months PMH diabetes, celiac disease Reports chest discomfort, positional coughing and pedal edema last 10
Difficult Data Definitions and Scenario s
 Difficult Data Definitions and Scenario s Presenter Disclosure Information Cornelia Anderson BSN, RN To following relationships exist related to this presentation: No Disclosures Objectives Discuss key
Difficult Data Definitions and Scenario s Presenter Disclosure Information Cornelia Anderson BSN, RN To following relationships exist related to this presentation: No Disclosures Objectives Discuss key
State-of-the-Art Management of Chronic Systolic Heart Failure
 State-of-the-Art Management of Chronic Systolic Heart Failure Michael McCulloch, MD 17 th Annual Cardiovascular Update Intermountain Medical Center December 16, 2017 Disclosures: I have no financial disclosures
State-of-the-Art Management of Chronic Systolic Heart Failure Michael McCulloch, MD 17 th Annual Cardiovascular Update Intermountain Medical Center December 16, 2017 Disclosures: I have no financial disclosures
 100 100 100 100 100 200 200 200 200 200 300 300 300 300 300 400 400 400 400 400 500 500 500 500 500 Interpret this ECG Include rhythm, STEMI-location, Axis deviation, BBB, hypertrophy. What interventions
100 100 100 100 100 200 200 200 200 200 300 300 300 300 300 400 400 400 400 400 500 500 500 500 500 Interpret this ECG Include rhythm, STEMI-location, Axis deviation, BBB, hypertrophy. What interventions
Management of acute decompensated heart failure and cardiogenic shock. Arintaya Phrommintikul Department of Medicine CMU
 Management of acute decompensated heart failure and cardiogenic shock Arintaya Phrommintikul Department of Medicine CMU Acute heart failure: spectrum Case 64 y/o M with Hx of non-ischemic DCM (LVEF=25-30%)
Management of acute decompensated heart failure and cardiogenic shock Arintaya Phrommintikul Department of Medicine CMU Acute heart failure: spectrum Case 64 y/o M with Hx of non-ischemic DCM (LVEF=25-30%)
DAY1_CARDIOVASCULAR PRACTICE QUESTIONS
 DAY1_CARDIOVASCULAR PRACTICE QUESTIONS 1 P age 1. A 59-year-old male is admitted complaining of chest pain and dyspnea. ST elevation and T-wave inversion were seen on the ECG in V2, V3, and V4. IV thrombolytic
DAY1_CARDIOVASCULAR PRACTICE QUESTIONS 1 P age 1. A 59-year-old male is admitted complaining of chest pain and dyspnea. ST elevation and T-wave inversion were seen on the ECG in V2, V3, and V4. IV thrombolytic
Rounds in the ICU. Eran Segal, MD Director General ICU Sheba Medical Center
 Rounds in the ICU Eran Segal, MD Director General ICU Sheba Medical Center Real Clinical cases (including our mistakes) Emphasis on hemodynamic monitoring Usually no single correct answer We will conduct
Rounds in the ICU Eran Segal, MD Director General ICU Sheba Medical Center Real Clinical cases (including our mistakes) Emphasis on hemodynamic monitoring Usually no single correct answer We will conduct
Acute Myocardial Infarction Complicated by Cardiogenic Shock
 Acute Myocardial Infarction Complicated by Cardiogenic Shock Navin K. Kapur, MD, FACC, FSCAI Assistant Professor, Division of Cardiology Director, Acute Circulatory Support Program Director, Interventional
Acute Myocardial Infarction Complicated by Cardiogenic Shock Navin K. Kapur, MD, FACC, FSCAI Assistant Professor, Division of Cardiology Director, Acute Circulatory Support Program Director, Interventional
CASE STUDIES IN ADVANCED HEART FAILURE
 CASE STUDIES IN ADVANCED HEART FAILURE Navin Rajagopalan, MD Director, Congestive Heart Failure Medical Director, Cardiac Transplantation Gill Heart Institute, Cardiovascular Medicine DISCLOSURES NOTHING
CASE STUDIES IN ADVANCED HEART FAILURE Navin Rajagopalan, MD Director, Congestive Heart Failure Medical Director, Cardiac Transplantation Gill Heart Institute, Cardiovascular Medicine DISCLOSURES NOTHING
8:30-10:30 WS #4: Cardiology :00-13:00 WS #11: Cardiology 101 (Repeated)
") Professor Ralph Stewart Cardiologist Auckland City Hospital Green Lane Cardiovascular Research Unit Auckland Heart Group Fiona Stewart Cardiologist Green Lane Hospital National Women's Hospital Professor
Professor Ralph Stewart Cardiologist Auckland City Hospital Green Lane Cardiovascular Research Unit Auckland Heart Group Fiona Stewart Cardiologist Green Lane Hospital National Women's Hospital Professor
Echocardiographic Structural Assessment Pre- LVAD
 None Disclosures Echocardiographic Structural Assessment Pre- LVAD LVEF ( 25% for DT LVAD) Right ventricle Valvular disease Intra- cardiac shunts Intra- cardiac thrombi Ascending aorta Case 1 50 yo M
None Disclosures Echocardiographic Structural Assessment Pre- LVAD LVEF ( 25% for DT LVAD) Right ventricle Valvular disease Intra- cardiac shunts Intra- cardiac thrombi Ascending aorta Case 1 50 yo M
Protocol Identifier Subject Identifier Visit Description. [Y] Yes [N] No. [Y] Yes [N] N. If Yes, admission date and time: Day Month Year
![Protocol Identifier Subject Identifier Visit Description. [Y] Yes [N] No. [Y] Yes [N] N. If Yes, admission date and time: Day Month Year](/thumbs/76/74263761.jpg "Protocol Identifier Subject Identifier Visit Description. [Y] Yes [N] No. [Y] Yes [N] N. If Yes, admission date and time: Day Month Year") PAST MEDICAL HISTORY Has the subject had a prior episode of heart failure? o Does the subject have a prior history of exposure to cardiotoxins, such as anthracyclines? URGENT HEART FAILURE VISIT Did heart
PAST MEDICAL HISTORY Has the subject had a prior episode of heart failure? o Does the subject have a prior history of exposure to cardiotoxins, such as anthracyclines? URGENT HEART FAILURE VISIT Did heart
3 European Journal of Heart Failure 2016; 18,
 Impella Assisted Cesarean Delivery in a 27 6/7 Weeks Gestation 30 Year Old Female with Newly Diagnosed Cardiomyopathy & Multifocal Incessant Ventricular Tachycardia Brendan J Carry, MD, Jason Costa, MD,
Impella Assisted Cesarean Delivery in a 27 6/7 Weeks Gestation 30 Year Old Female with Newly Diagnosed Cardiomyopathy & Multifocal Incessant Ventricular Tachycardia Brendan J Carry, MD, Jason Costa, MD,
Acute Circulatory Support Should We or Shouldn t We?
 Acute Circulatory Support Should We or Shouldn t We? Navin K. Kapur, MD, FACC, FSCAI Assistant Professor, Division of Cardiology Director, Acute Circulatory Support Program Director, Interventional Research
Acute Circulatory Support Should We or Shouldn t We? Navin K. Kapur, MD, FACC, FSCAI Assistant Professor, Division of Cardiology Director, Acute Circulatory Support Program Director, Interventional Research
Tips & tricks on how to treat an acute heart failure patient with low cardiac output and diuretic resistance
 Tips & tricks on how to treat an acute heart failure patient with low cardiac output and diuretic resistance J. Parissis Attikon University Hospital, Athens, Greece Disclosures ALARM investigator received
Tips & tricks on how to treat an acute heart failure patient with low cardiac output and diuretic resistance J. Parissis Attikon University Hospital, Athens, Greece Disclosures ALARM investigator received
Case Summary. Workshop Overview. Mr. M
 9:00 10:30 Workshop Overview Mr. M Who is this document primarily intended to reach? What is the format? How soon should I see a newly referred heart failure patient? How often should my heart failure
9:00 10:30 Workshop Overview Mr. M Who is this document primarily intended to reach? What is the format? How soon should I see a newly referred heart failure patient? How often should my heart failure
Nora Goldschlager, M.D. SFGH Division of Cardiology UCSF
 CLASSIFICATION OF HEART FAILURE Nora Goldschlager, M.D. SFGH Division of Cardiology UCSF DISCLOSURES: NONE CLASSIFICATION C OF HEART FAILURE NYHA I IV New paradigm Stage A: Pts at high risk of developing
CLASSIFICATION OF HEART FAILURE Nora Goldschlager, M.D. SFGH Division of Cardiology UCSF DISCLOSURES: NONE CLASSIFICATION C OF HEART FAILURE NYHA I IV New paradigm Stage A: Pts at high risk of developing
ACUTE HEART FAILURE. Julie Gorchynski MD, MSc, FACEP, FAAEM. Department of Emergency Medicine Emergency Residency Program UTHSC, San Antonio TCEP 2014
 ACUTE HEART FAILURE Julie Gorchynski MD, MSc, FACEP, FAAEM Department of Emergency Medicine Emergency Residency Program UTHSC, San Antonio TCEP 2014 No disclosures Objectives Overview Cases Current Therapy
ACUTE HEART FAILURE Julie Gorchynski MD, MSc, FACEP, FAAEM Department of Emergency Medicine Emergency Residency Program UTHSC, San Antonio TCEP 2014 No disclosures Objectives Overview Cases Current Therapy
Ventricular Assist Devices and Emergency Services
 Ventricular Assist Devices and Emergency Services Margaret Murray, DNP, FAHA Clinical Nurse Specialist- Cardiac Surgery, Cardiac Transplant and Ventricular Assist Devices ma.murray@hosp.wisc.edu Janean
Ventricular Assist Devices and Emergency Services Margaret Murray, DNP, FAHA Clinical Nurse Specialist- Cardiac Surgery, Cardiac Transplant and Ventricular Assist Devices ma.murray@hosp.wisc.edu Janean
Acute heart failure, beyond conventional treatment: persisting low output
 Acute heart failure, beyond conventional treatment: persisting low output Alexandre Mebazaa, FESC Hôpital Lariboisière, Université Paris 7 U942 Inserm Conflict of Interest Lecture fee: Orion No other conflicts
Acute heart failure, beyond conventional treatment: persisting low output Alexandre Mebazaa, FESC Hôpital Lariboisière, Université Paris 7 U942 Inserm Conflict of Interest Lecture fee: Orion No other conflicts
A case of post myocardial infarction ventricular septal rupture CHRISTOFOROS KOBOROZOS, MD
 A case of post myocardial infarction ventricular septal rupture CHRISTOFOROS KOBOROZOS, MD NAVAL HOSPITAL OF ATHENS case presentation Female, 81yo Hx: diabetes mellitus, hypertension, chronic anaemia presented
A case of post myocardial infarction ventricular septal rupture CHRISTOFOROS KOBOROZOS, MD NAVAL HOSPITAL OF ATHENS case presentation Female, 81yo Hx: diabetes mellitus, hypertension, chronic anaemia presented
Post-Cardiac Surgery Evaluation
 Post-Cardiac Surgery Evaluation 20th Annual Heart Conference October 15, 2016 Gary A Mayman PROFESSOR PEDIATRICS UNIVERSITY OF NEVADA Look Touch Listen Temperature, pulse, respiratory rate, & blood pressure
Post-Cardiac Surgery Evaluation 20th Annual Heart Conference October 15, 2016 Gary A Mayman PROFESSOR PEDIATRICS UNIVERSITY OF NEVADA Look Touch Listen Temperature, pulse, respiratory rate, & blood pressure
Cardiogenic Shock. Carlos Cafri,, MD
 Cardiogenic Shock Carlos Cafri,, MD SHOCK= Inadequate Tissue Mechanisms: Perfusion Inadequate oxygen delivery Release of inflammatory mediators Further microvascular changes, compromised blood flow and
Cardiogenic Shock Carlos Cafri,, MD SHOCK= Inadequate Tissue Mechanisms: Perfusion Inadequate oxygen delivery Release of inflammatory mediators Further microvascular changes, compromised blood flow and
Medical Management of Acute Heart Failure
 Critical Care Medicine and Trauma Medical Management of Acute Heart Failure Mary O. Gray, MD, FAHA Associate Professor of Medicine University of California, San Francisco Staff Cardiologist and Training
Critical Care Medicine and Trauma Medical Management of Acute Heart Failure Mary O. Gray, MD, FAHA Associate Professor of Medicine University of California, San Francisco Staff Cardiologist and Training
Acute heart failure in a patient with lower urinary tract infection Case report of an infection-induced Reverse Takotsubo syndrome
 Acute heart failure in a patient with lower urinary tract infection Case report of an infection-induced Reverse Takotsubo syndrome N.Μoschos, A.Dimitra, E.Tsakiri, D.Stavrianakis, A.Nouli CARDIOLOGY DEPARTMENT
Acute heart failure in a patient with lower urinary tract infection Case report of an infection-induced Reverse Takotsubo syndrome N.Μoschos, A.Dimitra, E.Tsakiri, D.Stavrianakis, A.Nouli CARDIOLOGY DEPARTMENT
Intravenous Infusions
 Intravenous Infusions 1) An IV insulin infusion can be used for patients: a) with out of control diabetes b) with DKA (Diabetic Ketoacidosis) c) after a heart attack 2) Hyperglycemia is an adaptive response
Intravenous Infusions 1) An IV insulin infusion can be used for patients: a) with out of control diabetes b) with DKA (Diabetic Ketoacidosis) c) after a heart attack 2) Hyperglycemia is an adaptive response
NOT ANOTHER TALK ABOUT A - FIB
 NOT ANOTHER TALK ABOUT A - FIB CASES KUDOS AND A CHALLENGE Case 1 67 y/o female s/p R mastectomy 3 months earlier Second course of adjuvant chemotherapy Muga scan E.F. 35% What do we do next? Case 1 Cardiology
NOT ANOTHER TALK ABOUT A - FIB CASES KUDOS AND A CHALLENGE Case 1 67 y/o female s/p R mastectomy 3 months earlier Second course of adjuvant chemotherapy Muga scan E.F. 35% What do we do next? Case 1 Cardiology
A LONG WAY TO HEART FAILURE T H I E R R Y C. G I L L E B E R T, G H E N T U N I V E R S I T Y, B E L G I U M
 A LONG WAY TO HEART FAILURE T H I E R R Y C. G I L L E B E R T, G H E N T U N I V E R S I T Y, B E L G I U M 1 M.A.M, 1943 Chronic low back pain Arterial hypertension and hyperlipidaemia Intolerance for
A LONG WAY TO HEART FAILURE T H I E R R Y C. G I L L E B E R T, G H E N T U N I V E R S I T Y, B E L G I U M 1 M.A.M, 1943 Chronic low back pain Arterial hypertension and hyperlipidaemia Intolerance for
Management of the Patient with Acute Decompensated Heart Failure. Disclosures. I have received funding from:
 Management of the Patient with Acute Decompensated Heart Failure William K. Cornwell III, MD Advanced Heart Failure, LVAD and Cardiac Transplant University of Colorado Anschutz Medical Campus Disclosures
Management of the Patient with Acute Decompensated Heart Failure William K. Cornwell III, MD Advanced Heart Failure, LVAD and Cardiac Transplant University of Colorado Anschutz Medical Campus Disclosures
Intravenous Inotropic Support an Overview
 Intravenous Inotropic Support an Overview Shaul Atar, MD Western Galilee Medical Center, Nahariya Affiliated with the Faculty of Medicine of the Galilee, Safed, Israel INOTROPES in Acute HF (not vasopressors)
Intravenous Inotropic Support an Overview Shaul Atar, MD Western Galilee Medical Center, Nahariya Affiliated with the Faculty of Medicine of the Galilee, Safed, Israel INOTROPES in Acute HF (not vasopressors)
Heart Failure Dr ahmed almutairi Assistant professor internal medicin dept
 Heart Failure Dr ahmed almutairi Assistant professor internal medicin dept (MBBS)(SBMD) Introduction Epidemiology Pathophysiology diastolic/systolic Risk factors Signs and symptoms Classification of HF
Heart Failure Dr ahmed almutairi Assistant professor internal medicin dept (MBBS)(SBMD) Introduction Epidemiology Pathophysiology diastolic/systolic Risk factors Signs and symptoms Classification of HF
The NEW Heart Failure Guidelines
 The NEW Heart Failure Guidelines Daily Practice HF scenario of the Case Presentations HF as a complex and heterogeneous syndrome Several proposed pathophysiological mechanisms involving the heart and the
The NEW Heart Failure Guidelines Daily Practice HF scenario of the Case Presentations HF as a complex and heterogeneous syndrome Several proposed pathophysiological mechanisms involving the heart and the
Chris Fox, MD Professor and Interim Chair Department of Emergency
 Close Calls with the Executioner: Where POCUS Avoided Misdiagnosis Chris Fox, MD Professor and Interim Chair Department of Emergency Medicine En route with 22 year old female Asthma attack witnessed by
Close Calls with the Executioner: Where POCUS Avoided Misdiagnosis Chris Fox, MD Professor and Interim Chair Department of Emergency Medicine En route with 22 year old female Asthma attack witnessed by
The Case of Lucia Nazzareno Galiè, M.D.
 The Case of Lucia Nazzareno Galiè, M.D. DIMES Disclosures Consulting fees and research support from Actelion Pharmaceuticals Ltd, Bayer HealthCare, Eli Lilly and Co, GlaxoSmithKline and Pfizer Ltd Clinical
The Case of Lucia Nazzareno Galiè, M.D. DIMES Disclosures Consulting fees and research support from Actelion Pharmaceuticals Ltd, Bayer HealthCare, Eli Lilly and Co, GlaxoSmithKline and Pfizer Ltd Clinical
A Diagnostic Dilemma saved by sound
 A Diagnostic Dilemma saved by sound Dr Syam Ravindranath MBBS DNB, Dr Ash Mukherjee FCEM FACEM We p r e s e n t a d i a g n o s t i c a l l y c h a l l e n g i n g s c e n a r i o in a 59 y e a r old f
A Diagnostic Dilemma saved by sound Dr Syam Ravindranath MBBS DNB, Dr Ash Mukherjee FCEM FACEM We p r e s e n t a d i a g n o s t i c a l l y c h a l l e n g i n g s c e n a r i o in a 59 y e a r old f
Sepsis Combine experience and Evidence. Eran Segal, MD Director General ICU, Sheba Medical Center, Israel
 Sepsis Combine experience and Evidence Eran Segal, MD Director General ICU, Sheba Medical Center, Israel The Science of Sepsis A complex and diverse clinical entity Outcome is affected by: Infecting organism
Sepsis Combine experience and Evidence Eran Segal, MD Director General ICU, Sheba Medical Center, Israel The Science of Sepsis A complex and diverse clinical entity Outcome is affected by: Infecting organism
Images have been removed from the PowerPoint slides in this handout due to copyright restrictions.
 Heart Failure Heart Failure Introduction and History AHA 2015 Statistics About 6 million Americans 870,000 new cases each year 1 in 9 deaths related to HF Almost 1 million hospitalizations each year (cost
Heart Failure Heart Failure Introduction and History AHA 2015 Statistics About 6 million Americans 870,000 new cases each year 1 in 9 deaths related to HF Almost 1 million hospitalizations each year (cost
Severe Hypertension. Pre-referral considerations: 1. BP of arm and Leg 2. Ambulatory BP 3. Renal causes
 Severe Hypertension *Prior to making a referral, call office or Doc Halo, to speak with a Cardiologist or APP to discuss patient and possible treatment options. Please only contact the patient's cardiologist.
Severe Hypertension *Prior to making a referral, call office or Doc Halo, to speak with a Cardiologist or APP to discuss patient and possible treatment options. Please only contact the patient's cardiologist.
Acute Coronary Syndromes
 Overview Acute Coronary Syndromes Rabeea Aboufakher, MD, FACC, FSCAI Section Chief of Cardiology Altru Health System Grand Forks, ND Epidemiology Pathophysiology Clinical features and diagnosis STEMI management
Overview Acute Coronary Syndromes Rabeea Aboufakher, MD, FACC, FSCAI Section Chief of Cardiology Altru Health System Grand Forks, ND Epidemiology Pathophysiology Clinical features and diagnosis STEMI management
Relax and Learn At the Farm 2012
 Relax and Learn At the Farm Session 9: Invasive Hemodynamic Assessment and What to Do with the Data Carol Jacobson RN, MN Cardiovascular Nursing Education Associates Function of CV system is to deliver
Relax and Learn At the Farm Session 9: Invasive Hemodynamic Assessment and What to Do with the Data Carol Jacobson RN, MN Cardiovascular Nursing Education Associates Function of CV system is to deliver
Device Therapy for Heart Failure
 Device Therapy for Heart Failure Dr. Shelley Zieroth FRCPC Assistant Professor, Cardiology, University of Manitoba Director of Cardiac Transplant and Heart Failure Clinics St Boniface General Hospital,
Device Therapy for Heart Failure Dr. Shelley Zieroth FRCPC Assistant Professor, Cardiology, University of Manitoba Director of Cardiac Transplant and Heart Failure Clinics St Boniface General Hospital,
Cardiogenic Shock in Acute MI
 Cardiogenic Shock in Acute MI Mark Sheldon, MD UNMH Interventional Cardiology Objectives Overview Treatment Definition Shock profiles Causes Medical Mechanical Illustrative case Questions? Revascularization
Cardiogenic Shock in Acute MI Mark Sheldon, MD UNMH Interventional Cardiology Objectives Overview Treatment Definition Shock profiles Causes Medical Mechanical Illustrative case Questions? Revascularization
Staging Sepsis for the Emergency Department: Physician
 Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Controversies in Cardiogenic Shock. Timothy D. Henry, MD Cedars-Sinai Heart Institute
 Controversies in Cardiogenic Shock Timothy D. Henry, MD Cedars-Sinai Heart Institute Key Issues Cardiac Arrest-Cardiogenic shock interaction New SCAI Classification Refractory Shock Shock with Multivessel
Controversies in Cardiogenic Shock Timothy D. Henry, MD Cedars-Sinai Heart Institute Key Issues Cardiac Arrest-Cardiogenic shock interaction New SCAI Classification Refractory Shock Shock with Multivessel
Level 1: Acute CHF with Hypotension (SBP < 90 torr)
") PENNSYLVANIA HOSPITAL ED ACUTE CONGESTIVE HEART FAILURE STANDING DERS Level 1: Acute CHF with Hypotension (SBP < 90 torr) Intake: Vital signs Pulse oximetry Weight Allergies: Obtain old chart Obtain old
PENNSYLVANIA HOSPITAL ED ACUTE CONGESTIVE HEART FAILURE STANDING DERS Level 1: Acute CHF with Hypotension (SBP < 90 torr) Intake: Vital signs Pulse oximetry Weight Allergies: Obtain old chart Obtain old
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
Heart Failure from a GP perspective
 Heart Failure from a GP perspective Jane Gilmour, Alison Wright Clinical Nurse Specialists for Heart Failure The Heart failure Team Dr Ganesan Kumar- Consultant Cardiologist Dr D Maras- Staff Grade Cardiology
Heart Failure from a GP perspective Jane Gilmour, Alison Wright Clinical Nurse Specialists for Heart Failure The Heart failure Team Dr Ganesan Kumar- Consultant Cardiologist Dr D Maras- Staff Grade Cardiology
Medical Management of Acutely Decompensated Heart Failure. William T. Abraham, MD Director, Division of Cardiovascular Medicine
 Medical Management of Acutely Decompensated Heart Failure William T. Abraham, MD Director, Division of Cardiovascular Medicine Orlando, Florida October 7-9, 2011 Goals of Acute Heart Failure Therapy Alleviate
Medical Management of Acutely Decompensated Heart Failure William T. Abraham, MD Director, Division of Cardiovascular Medicine Orlando, Florida October 7-9, 2011 Goals of Acute Heart Failure Therapy Alleviate
Keynote Address II Managing Acute Heart Failure: What Can We Do to Improve Outcomes?
 Keynote Address II Managing Acute Heart Failure: What Can We Do to Improve Outcomes? 24 th Annual San Diego Heart Failure Symposium June 1-2, 2018 La Jolla, CA Barry Greenberg, MD Distinguished Professor
Keynote Address II Managing Acute Heart Failure: What Can We Do to Improve Outcomes? 24 th Annual San Diego Heart Failure Symposium June 1-2, 2018 La Jolla, CA Barry Greenberg, MD Distinguished Professor
CHF ICU to community. Disclosure slide CHF. Diagnosis. Diagnosis. Diagnostic modalties Therapeutic modalities. Talks. Advisory boards.
 CHF ICU to community CHF Diagnostic modalties Therapeutic modalities ICU Pacer/ ICD Medication CHF clinic ASV - Nejm. Sept. 17,2015. Advanced care directives Disclosure slide Talks most companies Advisory
CHF ICU to community CHF Diagnostic modalties Therapeutic modalities ICU Pacer/ ICD Medication CHF clinic ASV - Nejm. Sept. 17,2015. Advanced care directives Disclosure slide Talks most companies Advisory
Unstable: Hypotension/Shock, Fever, Altered Mental Status, Chest discomfort, Acute Heart Failure Saturation <94%, Systolic BP < 90mmHg
 Bradycardia Heart Rate less than 50/min Stable: Monitor Seek expert help Treat Reversible Causes Unstable Signs and Symptoms: chest pain, shortness of breath, altered mental status, weak, Hypotension,
Bradycardia Heart Rate less than 50/min Stable: Monitor Seek expert help Treat Reversible Causes Unstable Signs and Symptoms: chest pain, shortness of breath, altered mental status, weak, Hypotension,
Referral for Heart Transplantation - who and when?
 Transplant Referral for heart transplantation - who and when Sarah Fitzsimons Chairs: Kathy Ferrier & Richard Troughton Referral for Heart Transplantation - who and when? CSANZ June 2018 1 Introduction
Transplant Referral for heart transplantation - who and when Sarah Fitzsimons Chairs: Kathy Ferrier & Richard Troughton Referral for Heart Transplantation - who and when? CSANZ June 2018 1 Introduction
Evaluation and Management of Acute Decompensated Heart Failure (HF) with Reduced Ejection Fraction Systolic Heart Failure (HFrEF)(EF<40%
 with Reduced Ejection Fraction Systolic Heart Failure (HFrEF)(EF<40%") Evaluation and Management of Acute Decompensated Heart Failure (HF) with Reduced Ejection Fraction Systolic Heart Failure (HFrEF)(EF
Evaluation and Management of Acute Decompensated Heart Failure (HF) with Reduced Ejection Fraction Systolic Heart Failure (HFrEF)(EF
AllinaHealthSystem 1
 : Definition End-organ hypoperfusion secondary to cardiac failure Venoarterial ECMO: Patient Selection Michael A. Samara, MD FACC Advanced Heart Failure, Cardiac Transplant & Mechanical Circulatory Support
: Definition End-organ hypoperfusion secondary to cardiac failure Venoarterial ECMO: Patient Selection Michael A. Samara, MD FACC Advanced Heart Failure, Cardiac Transplant & Mechanical Circulatory Support
Sepsis and Hemodynamic Support in September 15, 2017 Carleen Risaliti
 Sepsis and Hemodynamic Support in 2017 September 15, 2017 Carleen Risaliti Objectives Review fluid resuscitation guidelines in septic shock Discuss volume assessment v. fluid responsiveness Evaluate pros
Sepsis and Hemodynamic Support in 2017 September 15, 2017 Carleen Risaliti Objectives Review fluid resuscitation guidelines in septic shock Discuss volume assessment v. fluid responsiveness Evaluate pros
Critical Care Treatment Guidelines
 Critical Care Treatment Guidelines West Virginia Office of Emergency Medical Services CCT Guidelines CCT Guidelines TABLE OF CONTENTS Preface Acknowledgments Using the Guidelines INITIAL TREATMENT / UNIVERSAL
Critical Care Treatment Guidelines West Virginia Office of Emergency Medical Services CCT Guidelines CCT Guidelines TABLE OF CONTENTS Preface Acknowledgments Using the Guidelines INITIAL TREATMENT / UNIVERSAL
Diagnosis & Management of Heart Failure. Abena A. Osei-Wusu, M.D. Medical Fiesta
 Diagnosis & Management of Heart Failure Abena A. Osei-Wusu, M.D. Medical Fiesta Learning Objectives: 1) Become familiar with pathogenesis of congestive heart failure. 2) Discuss clinical manifestations
Diagnosis & Management of Heart Failure Abena A. Osei-Wusu, M.D. Medical Fiesta Learning Objectives: 1) Become familiar with pathogenesis of congestive heart failure. 2) Discuss clinical manifestations
DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE
 DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE Mefri Yanni, MD Bagian Kardiologi dan Kedokteran Vaskular RS.DR.M.Djamil Padang The 3rd Symcard Padang, Mei 2013 Outline Diagnosis Diagnosis Treatment options
DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE Mefri Yanni, MD Bagian Kardiologi dan Kedokteran Vaskular RS.DR.M.Djamil Padang The 3rd Symcard Padang, Mei 2013 Outline Diagnosis Diagnosis Treatment options
Heart Failure. Jay Shavadia
 Heart Failure Jay Shavadia Definition Clinical syndrome characterized by: Symptoms: breathlessness at rest or on exercise, fatigue, tiredness or ankle swelling AND Signs: tachycardia, tachypnea, pulmonary
Heart Failure Jay Shavadia Definition Clinical syndrome characterized by: Symptoms: breathlessness at rest or on exercise, fatigue, tiredness or ankle swelling AND Signs: tachycardia, tachypnea, pulmonary
Hemodynamic improvement upon levosimendan treatment in low cardiac output patients following coronary artery bypass graft
 Hemodynamic improvement upon levosimendan treatment in low cardiac output patients following coronary artery bypass graft M. Buerke, K. Krohe, M. Russ, C. Schneider, H. Lemm, R. Prondzinsky, I. Friedrich,
Hemodynamic improvement upon levosimendan treatment in low cardiac output patients following coronary artery bypass graft M. Buerke, K. Krohe, M. Russ, C. Schneider, H. Lemm, R. Prondzinsky, I. Friedrich,
เอกราช อร ยะช ยพาณ ชย
 25 September 2017 เอกราช อร ยะช ยพาณ ชย Heart Failure and Transplant Cardiology aekarach.a@chula.ac.th Presentation at 1 Agenda Physiology of the heart Pathophysiology of shock Pathophysiology of heart
25 September 2017 เอกราช อร ยะช ยพาณ ชย Heart Failure and Transplant Cardiology aekarach.a@chula.ac.th Presentation at 1 Agenda Physiology of the heart Pathophysiology of shock Pathophysiology of heart
Acute Liver Failure: Supporting Other Organs
 Acute Liver Failure: Supporting Other Organs Michael A. Gropper, MD, PhD Professor of Anesthesia and Physiology Director, Critical Care Medicine University of California San Francisco Acute Liver Failure
Acute Liver Failure: Supporting Other Organs Michael A. Gropper, MD, PhD Professor of Anesthesia and Physiology Director, Critical Care Medicine University of California San Francisco Acute Liver Failure
5 Important Things to Know About Heart Failure. Kia Afshar, MD
 5 Important Things to Know About Heart Failure Kia Afshar, MD Disclosures I have no conflicts of interest to disclose I will not be discussing any off label medications and/or devices Objectives 1) Understand
5 Important Things to Know About Heart Failure Kia Afshar, MD Disclosures I have no conflicts of interest to disclose I will not be discussing any off label medications and/or devices Objectives 1) Understand
2/14/2018 CASE STUDIES: COMPLICATIONS OF MYOCARDIAL INFARCTION. Judy Hung, MD Cardiology Division Massachusetts General Hospital Boston, MA CASE 1
 CASE STUDIES: COMPLICATIONS OF MYOCARDIAL INFARCTION Judy Hung, MD Cardiology Division Massachusetts General Hospital Boston, MA CASE 1 1 PRESENTATION 57 yo male with a past medical history of hypertension
CASE STUDIES: COMPLICATIONS OF MYOCARDIAL INFARCTION Judy Hung, MD Cardiology Division Massachusetts General Hospital Boston, MA CASE 1 1 PRESENTATION 57 yo male with a past medical history of hypertension
Case Presentation. This presentation is the intellectual property of the author. Contact them for permission to reprint and/or distribute.
 Worsening Renal Function in Heart Failure Patients Mark Drazner, MD, MSc Clinical Chief of Cardiology Medical Director, CHF/VAD/Transplant James M. Wooten Chair in Cardiology UT Southwestern Medical Center
Worsening Renal Function in Heart Failure Patients Mark Drazner, MD, MSc Clinical Chief of Cardiology Medical Director, CHF/VAD/Transplant James M. Wooten Chair in Cardiology UT Southwestern Medical Center
ECG Workshop. Nezar Amir
 ECG Workshop Nezar Amir Myocardial Ischemia ECG Infarct ECG in STEMI is dynamic & evolving Common causes of ST shift Infarct Localisation Left main artery occlusion: o diffuse ST-depression with ST elevation
ECG Workshop Nezar Amir Myocardial Ischemia ECG Infarct ECG in STEMI is dynamic & evolving Common causes of ST shift Infarct Localisation Left main artery occlusion: o diffuse ST-depression with ST elevation
A patient with acute heart failure and renal impairment ACCA Masterclass 2017
 A patient with acute heart failure and renal impairment Dr Sofie Gevaert Mister P. J.M., 67-years-old Cardiac risk factors: Ex-smoker, AHT, Type 2 diabetes, BMI 43, Hyperlipidaemia Medical history: 2009:
A patient with acute heart failure and renal impairment Dr Sofie Gevaert Mister P. J.M., 67-years-old Cardiac risk factors: Ex-smoker, AHT, Type 2 diabetes, BMI 43, Hyperlipidaemia Medical history: 2009:
Congestive Heart Failure or Heart Failure
 Congestive Heart Failure or Heart Failure Dr Hitesh Patel Ascot Cardiology Group Heart Failure Workshop April, 2014 Question One What is the difference between congestive heart failure and heart failure?
Congestive Heart Failure or Heart Failure Dr Hitesh Patel Ascot Cardiology Group Heart Failure Workshop April, 2014 Question One What is the difference between congestive heart failure and heart failure?
IN-HF on line: patient settings (Enrollement period= )
") IN-HF on line: atient settings (Enrollement eriod= 1995-2018) N of centers (total) 187 N of centers (ts. AHF only) 13 N of centers (ts. CHF only) 71 N of centers (both ts. AHF and CHF) 103 N of atients
IN-HF on line: atient settings (Enrollement eriod= 1995-2018) N of centers (total) 187 N of centers (ts. AHF only) 13 N of centers (ts. CHF only) 71 N of centers (both ts. AHF and CHF) 103 N of atients
Acute heart failure & all it's friends - managing the complicated CHF patient in the ED
 27th Annual Update in Emergency Medicine Acute heart failure & all it's friends - managing the complicated CHF patient in the ED February 24, 2014 Clare Atzema, MD MSc FRCPC Staff Physician, Sunnybrook
27th Annual Update in Emergency Medicine Acute heart failure & all it's friends - managing the complicated CHF patient in the ED February 24, 2014 Clare Atzema, MD MSc FRCPC Staff Physician, Sunnybrook
NITROGLYCERIN A NEW LOOK FOR AN OLD FRIEND. Casey Patrick MD Jordan Anderson LP, CCP-C Texas EMS November 19, 2018
 NITROGLYCERIN A NEW LOOK FOR AN OLD FRIEND Casey Patrick MD Jordan Anderson LP, CCP-C Texas EMS November 19, 2018 OBJECTIVES Review pathophysiology of CHF Differentiate between acute pulmonary edema (APE),
NITROGLYCERIN A NEW LOOK FOR AN OLD FRIEND Casey Patrick MD Jordan Anderson LP, CCP-C Texas EMS November 19, 2018 OBJECTIVES Review pathophysiology of CHF Differentiate between acute pulmonary edema (APE),
Case year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50
 Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
Heart Failure: Guideline-Directed Management and Therapy
 Heart Failure: Guideline-Directed Management and Therapy Guideline-Directed Management and Therapy (GDMT) was developed by the American College of Cardiology and American Heart Association to define the
Heart Failure: Guideline-Directed Management and Therapy Guideline-Directed Management and Therapy (GDMT) was developed by the American College of Cardiology and American Heart Association to define the
CABG Surgery following STEMI
 CABG Surgery following STEMI Susana Harrington, MS,APRN-NP Cardio-Thoracic Surgery Nebraska Methodist Hospital February 15, 2018 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction:
CABG Surgery following STEMI Susana Harrington, MS,APRN-NP Cardio-Thoracic Surgery Nebraska Methodist Hospital February 15, 2018 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction:
Professional Development Presents. May 2016 Medication of the Month. Milrinone Drip IN2731
 Med of the Month For any question regarding May 2016 Med of the Month: Milrinone Drip You may contact: Sherr Ann Arabit MSN, RN-BC, CCRN/Professional Development Department Ext 4196 Professional Development
Med of the Month For any question regarding May 2016 Med of the Month: Milrinone Drip You may contact: Sherr Ann Arabit MSN, RN-BC, CCRN/Professional Development Department Ext 4196 Professional Development
HYPOTENSION IS DANGEROUS C. R Y A N K E A Y, M D, F A C E P 1 6 M A R C H
 HYPOTENSION IS DANGEROUS C. R Y A N K E A Y, M D, F A C E P 1 6 M A R C H 2 0 1 8 OBJECTIVES Case-based overview of pressors Debunking pressor myths Utilizing push-dose pressors CASE 1 82-year old male,
HYPOTENSION IS DANGEROUS C. R Y A N K E A Y, M D, F A C E P 1 6 M A R C H 2 0 1 8 OBJECTIVES Case-based overview of pressors Debunking pressor myths Utilizing push-dose pressors CASE 1 82-year old male,
Acute heart failure: ECMO Cardiology & Vascular Medicine 2012
 Acute heart failure: ECMO Cardiology & Vascular Medicine 2012 Lucia Jewbali cardiologist-intensivist 14 beds/8 ICU beds Acute coronary syndromes Heart failure/ Cardiogenic shock Post cardiotomy Heart
Acute heart failure: ECMO Cardiology & Vascular Medicine 2012 Lucia Jewbali cardiologist-intensivist 14 beds/8 ICU beds Acute coronary syndromes Heart failure/ Cardiogenic shock Post cardiotomy Heart
Complicated PTCA of Left Main Total Occlusion in NSTEMI
 Complicated PTCA of Left Main Total Occlusion in NSTEMI Dr AM Thirugnanam MD, FSCAI, PhD Sr. Interventional Cardiologist Ipcard Cardiac Care Center, Hyderabad, India Disclosure Statement of Financial Interest
Complicated PTCA of Left Main Total Occlusion in NSTEMI Dr AM Thirugnanam MD, FSCAI, PhD Sr. Interventional Cardiologist Ipcard Cardiac Care Center, Hyderabad, India Disclosure Statement of Financial Interest
How to do Primary Angioplasty. - Patients with Cardiogenic Shock
 How to do Primary Angioplasty - Patients with Cardiogenic Shock Advanced Cardiovascular Intervention 2011 Dan Blackman Leeds General Infirmary MY CONFLICTS OF INTEREST ARE: Research Grants Medicines Company
How to do Primary Angioplasty - Patients with Cardiogenic Shock Advanced Cardiovascular Intervention 2011 Dan Blackman Leeds General Infirmary MY CONFLICTS OF INTEREST ARE: Research Grants Medicines Company
Case I: Shock. A) What additional history would you like from the nursing home staff, patient s chart, and ambulance team?
 What additional history would you like from the nursing home staff, patient s chart, and ambulance team?") Case I: Shock It is your first night of call during your subinternship month, and you are asked by your resident to evaluate a patient in the emergency room. The patient is a 85yo female with a history
Case I: Shock It is your first night of call during your subinternship month, and you are asked by your resident to evaluate a patient in the emergency room. The patient is a 85yo female with a history
Introduction. Invasive Hemodynamic Monitoring. Determinants of Cardiovascular Function. Cardiovascular System. Hemodynamic Monitoring
 Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
POST-OP CARDIAC SURGERY PHYSICIAN S ORDER SHEET USE BALLPOINT PEN ONLY. CARDIAC INTENSIVE CARE UNIT
 PHYSICIAN S SHEET Automatically Activate, if not in agreement, cross out and initial Activated by Checking Box ALLERGIES: None known YES Patient s Height: Patient s Weight: ALL MEDICATION and INTRAVENOUS
PHYSICIAN S SHEET Automatically Activate, if not in agreement, cross out and initial Activated by Checking Box ALLERGIES: None known YES Patient s Height: Patient s Weight: ALL MEDICATION and INTRAVENOUS
Approach to the patient with Shortness of Breath
 Approach to the patient with Shortness of Breath Colin Edwards AUG 2015 Dyspnoea Basic concepts Definition: Dyspnoea is defined as abnormal or uncomfortable breathing in the context of what is normal for
Approach to the patient with Shortness of Breath Colin Edwards AUG 2015 Dyspnoea Basic concepts Definition: Dyspnoea is defined as abnormal or uncomfortable breathing in the context of what is normal for
A Great Clinical Paradox. Narendranath Epperla MD Sowjanya Bapani MD Steven Yale MD, FACP
 A Great Clinical Paradox Narendranath Epperla MD Sowjanya Bapani MD Steven Yale MD, FACP Initial Presentation 61 y/o Vietnam veteran with a past H/O hypertension, back pain and depression on Lisinopril,
A Great Clinical Paradox Narendranath Epperla MD Sowjanya Bapani MD Steven Yale MD, FACP Initial Presentation 61 y/o Vietnam veteran with a past H/O hypertension, back pain and depression on Lisinopril,
Central Sleep Apnea Problem Based Learning Module
 Central Sleep Apnea Problem Based Learning Module Vidya Krishnan, and Sutapa Mukherjee for the Sleep Education for Pulmonary Fellows and Practitioners, SRN ATS Committee 2015 Case Section I A 75 year old
Central Sleep Apnea Problem Based Learning Module Vidya Krishnan, and Sutapa Mukherjee for the Sleep Education for Pulmonary Fellows and Practitioners, SRN ATS Committee 2015 Case Section I A 75 year old
Management of Acute Shock and Right Ventricular Failure
 Management of Acute Shock and Right Ventricular Failure Nader Moazami, MD Department of Thoracic and Cardiovascular Surgery and Biomedical Engineering, Cleveland Clinic NONE Disclosures CARDIOGENIC SHOCK
Management of Acute Shock and Right Ventricular Failure Nader Moazami, MD Department of Thoracic and Cardiovascular Surgery and Biomedical Engineering, Cleveland Clinic NONE Disclosures CARDIOGENIC SHOCK
Perioperative Management of the Mechanical Circulatory Support Patient. American Association of Thoracic Surgeons Allied Health Symposium May 4, 2013
 Perioperative Management of the Mechanical Circulatory Support Patient American Association of Thoracic Surgeons Allied Health Symposium May 4, 2013 Disclosures None 2012 MFMER slide-2 Objectives Review
Perioperative Management of the Mechanical Circulatory Support Patient American Association of Thoracic Surgeons Allied Health Symposium May 4, 2013 Disclosures None 2012 MFMER slide-2 Objectives Review
Disclosures. Objectives 10/11/17. Short Term Mechanical Circulatory Support for Advanced Cardiogenic Shock. I have no disclosures to report
 Short Term Mechanical Circulatory Support for Advanced Cardiogenic Shock Christopher K. Gordon MSN, ACNP-BC Disclosures I have no disclosures to report 1. Pathophysiology 2. Epidemiology 3. Assessment
Short Term Mechanical Circulatory Support for Advanced Cardiogenic Shock Christopher K. Gordon MSN, ACNP-BC Disclosures I have no disclosures to report 1. Pathophysiology 2. Epidemiology 3. Assessment
Patient Encounters in the Primary Care Setting
 Patient Encounters in the Primary Care Setting Carmine D Amico, D.O. Clinical Cases Overview Learning objectives Clinical case presentations Questions for audience participation 1 Clinical Cases Learning
Patient Encounters in the Primary Care Setting Carmine D Amico, D.O. Clinical Cases Overview Learning objectives Clinical case presentations Questions for audience participation 1 Clinical Cases Learning
ARIC HEART FAILURE HOSPITAL RECORD ABSTRACTION FORM. General Instructions: ID NUMBER: FORM NAME: H F A DATE: 10/13/2017 VERSION: CONTACT YEAR NUMBER:
 ARIC HEART FAILURE HOSPITAL RECORD ABSTRACTION FORM General Instructions: The Heart Failure Hospital Record Abstraction Form is completed for all heart failure-eligible cohort hospitalizations. Refer to
ARIC HEART FAILURE HOSPITAL RECORD ABSTRACTION FORM General Instructions: The Heart Failure Hospital Record Abstraction Form is completed for all heart failure-eligible cohort hospitalizations. Refer to
Heart Failure. Cardiac Anatomy. Functions of the Heart. Cardiac Cycle/Hemodynamics. Determinants of Cardiac Output. Cardiac Output
 Cardiac Anatomy Heart Failure Professor Qing ZHANG Department of Cardiology, West China Hospital www.blaufuss.org Cardiac Cycle/Hemodynamics Functions of the Heart Essential functions of the heart to cover
Cardiac Anatomy Heart Failure Professor Qing ZHANG Department of Cardiology, West China Hospital www.blaufuss.org Cardiac Cycle/Hemodynamics Functions of the Heart Essential functions of the heart to cover
Case 1. Case 2. What do you think about reducing or discontinuing some of the above now that his LVEF has normalized?
 Case 1 A primary care colleague inquires what to do with a patient (HFrEF in NSR) who has a digoxin level of 2.8ng/ml. Level was obtained at 10am, patient takes all medications at one time upon arising
Case 1 A primary care colleague inquires what to do with a patient (HFrEF in NSR) who has a digoxin level of 2.8ng/ml. Level was obtained at 10am, patient takes all medications at one time upon arising
SHOCK. Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital
 SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction