A patient with acute heart failure and renal impairment ACCA Masterclass 2017
|
|
|
- Mervyn Rogers
- 5 years ago
- Views:
Transcription
1 A patient with acute heart failure and renal impairment Dr Sofie Gevaert
2 Mister P. J.M., 67-years-old Cardiac risk factors: Ex-smoker, AHT, Type 2 diabetes, BMI 43, Hyperlipidaemia Medical history: 2009: Hospitalisation for heart failure: HFpEF 2009: Sick sinus syndrome: DDD pacemaker 1/2016 NSTEMI: PCI D1 2014: Paroxismal atrial fibrillation COPD GOLD II 11/2011 NSTEMI, PCI LAD: 1 month triple R/: VKA-ASA-Clopidogrel Gastro-intestinal bleed with need for transfusion: stop aspirin CKD stage 3B: Serum creatinin 2.09mg/dl, egfr 30.3mL/min/1.73m 2 Echocardiography 11/2016: Concentric LVH, EDD 52mm, nl systolic LVF Pseudonormal relaxation pattern, E/E 16 Mild TR: 41mmHg, VCI>17mm, resp variation TAPSE 11mm
3 12/2016: hospitalization for AHF Complaints: Dyspnoea NYHA III, progressive over 6 days after resp infection treated with AB Peripheral edema Weight + 5kg Medication: Allopurinol 100mg OD Atorvastatin 80mg, OD Bisoprolol 2.5 mg daily Bumetanide 1mg OD Clopidogrel 75mg Pantoprazole 40mg Ramipril 5mg OD Warfarine INR Salmeterol/fluticason inhaler
4 12/2016: hospitalization for AHF Clinical exam BP 116/60 mmhg, HR 63 BPM, SaO 2 92%, RR 18 Jugular distension ++ Normal heart sounds Decreased breathing, rales Peripheral edema ++



5 Clinical Profile? H Y P O _ P E R F U S + I O n CONGESTION - + ESC guidelines AHF 2015


6 ACCA toolkit 2015


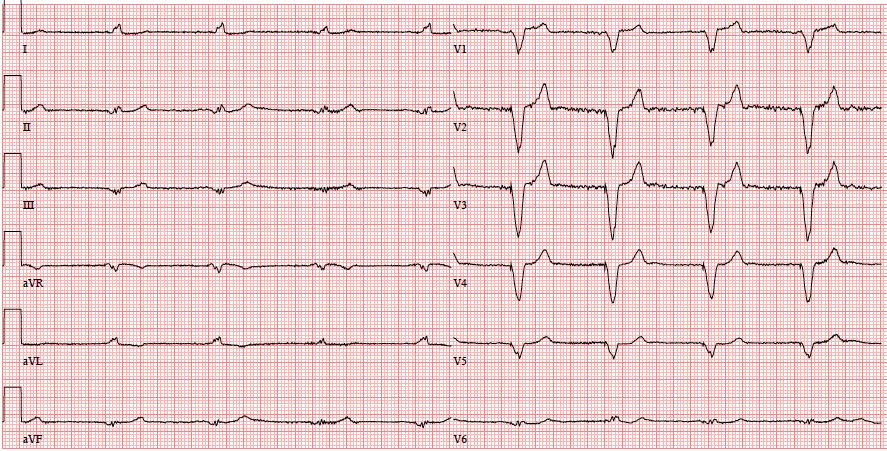
7 Chest X-ray-ECG
8 Lab results Hct 36.3% (39-49) K mmol/l Serum Creatinin 2.85 mg/dl ( ), egfr: 22 ml/min/1.73 m 2 probnp: 2,400 pg/ml ( 125) PH 7.37, po 2 55, pco

9 Timing echocardiography? Immediately <48 hours of admission Before discharge Not necessary, recent echo ESC guidelines AHF 2015
10 Echocardiogaphy Moderate views Restrictive relaxation pattern, E/E med 26 TR grade 2+: 54mmHg, VCI>17mm no resp. variation TAPSE 11mm ADHF triggered by respiratory infection


11 Initial treatment? IV diuretics IV diuretics and vasodilators Ultrafiltration ESC guidelines AHF 2015


12 Diuretics-Ultrafiltration ESC guidelines AHF 2015
13 Referral CCU: IV diuretics and vasodilators Continuous infusion bumetanide 0.5mg/h for 24h Continuous infusion isosorbide dinitrate 2mg/h Negative fluid balance -3L 1st 24h oral diuretics at increased dose Improvement kidney function: 2.0 mg/dl (egfr 34mL/min) at discharge Discharge after 72h: Weight -5 kg Oral dose Bumetanide increased to 2mg Daily weight, salt restriction Follow-up 4 weeks
14 Readmission 1 week later Complaints: Dyspnoea NYHA III, progressive 3 days, peripheral edema, weight +4 kilo Medication: Allopurinol 100mg OD Atorvastatine 80mg, OD Bisoprolol 2.5 mg daily Bumetanide 2mg OD Clopidogrel 75mg Pantoprazole 40mg Ramipril 5mg OD Warfarine INR
15 Clinical exam BP 128/55 mmhg, HR 56 BPM, SaO 2 94% Jugular distension Normal heart sounds Rales basal Moderate peripheral edema Lab results Serum creatinin:2.3 mg/dl (+0.3mg/dL, GFR 28mL/min)


16 Could UF have prevented rehospitalization? ADHF Adjustable UF (up to 500mL/h) vs. diuretic R/ at discretion physician UNLOAD trial, Costanzo et al, JACC 2007
17 Compliance problem? Diuretic resistance? Decongestion treatment? IV diuretics Increase oral dose Add thiazide or other Ultrafiltration
18 Referral to ward for IV diuretics day Bumetanide Diuresis (ml) Serum creatinine h: 0.48mg/h mg/h IV SAT Stop IV 23.00h 260 (complete?) 2.51
19 Referral to ward for IV diuretics day Bumetanide Diuresis (ml) Serum creatinine h:0.48mg/h mg/h IV SAT Stop IV 23.00h 260 (complete?) SUN 1 mg PO mg PO
20 Referral to ward for IV diuretics day Bumetanide Diuresis (ml) Serum creatinine h:0.48mg/h mg/h IV SAT Stop IV 23.00h 260 (complete?) SUN 1 mg PO mg PO
21 Too rapid decongestion AKI KDIGO definition of AKI Increase in Scr level of 0.3 mg/dl (26.5 μmol/l) <48h Increase in Scr level of 1.5 times baseline <7 d Urine output <0.5mL/Kg/h >6h

22 KDIGO staging of AKI Stage Scr increase Urine output times baseline or 0.3mg/dL <0.5mL/kg/h for 6-12h times baseline <0.5mL/kg/h for 12h 3 3times baseline or 4mg/dL or RRT <0.3mL/kg/h for 24h or Anuria for 12h
")

23 Could UF have prevented AKI? ADHF+WRF: Fixed UF rate (200mL/h) vs. defined stepped pharmacological R/ CARESS trial, Bart et al, NEJM 2012



24 No difference in changes kidney function AVOID trial, Costanzo, Bart et al, JACC HF 2016
25 3 weeks later, third admission Complaints: Dyspnoea NYHA IV, progressive since discharge, peripheral edema, weight +4 kg Medication: Allopurinol 100mg OD Amlodipine 5 mg OD Atorvastatine 80mg, OD Bisoprolol 2.5 mg daily Bumetanide 2-3mg OD, depending on weight Clopidogrel 75mg Pantoprazole 40mg Ramipril 5mg OD Warfarine INR
26 Clinical exam BP 116/60 mmhg, HR 63 BPM, SaO 2 88% Jugular distension New systolic murmur? Decreased breathing, rales Peripheral edema Lab results Serum creatinin 2.2mg/dL

27 ESC guidelines AHF 2015


28
29 RUPTURED CHORDA of ant. LEAFLET MV Cardiac surgery Repair not succesful bioprosthesis CE Magna Ease Postoperative: AKI, anuria Dialysis
30 Thank you
31 How to avoid too rapid/much decongestion? Decongestion goal CLOSE monitoring of? BP weight Δ renal function/urine output Monitoring of intravascular volume Hct as surrogate marker? Monitoring of CO? CVO 2 as surrogate marker of CO?? Vazir et al, Int J card 2016
Cardiorenal syndrome. Sofie Gevaert. Ghent University Hospital, Belgium
 Cardiorenal syndrome Sofie Gevaert Ghent University Hospital, Belgium Disclosures Consultancy Astra Zeneca Boegringer MSD Novartis 68 y old man, ADHF ICMP, ejection fraction 35 %: progressive dyspnea,
Cardiorenal syndrome Sofie Gevaert Ghent University Hospital, Belgium Disclosures Consultancy Astra Zeneca Boegringer MSD Novartis 68 y old man, ADHF ICMP, ejection fraction 35 %: progressive dyspnea,
Recognizing and Treating Patients with the Cardio-Renal Syndrome
 Recognizing and Treating Patients with the Cardio-Renal Syndrome Joachim H. Ix, MD, MAS, FASN Professor of Medicine Chief; Division of Nephrology-Hypertension University of California San Diego 1 Conflicts
Recognizing and Treating Patients with the Cardio-Renal Syndrome Joachim H. Ix, MD, MAS, FASN Professor of Medicine Chief; Division of Nephrology-Hypertension University of California San Diego 1 Conflicts
Tips & tricks on how to treat an acute heart failure patient with low cardiac output and diuretic resistance
 Tips & tricks on how to treat an acute heart failure patient with low cardiac output and diuretic resistance J. Parissis Attikon University Hospital, Athens, Greece Disclosures ALARM investigator received
Tips & tricks on how to treat an acute heart failure patient with low cardiac output and diuretic resistance J. Parissis Attikon University Hospital, Athens, Greece Disclosures ALARM investigator received
Heart Failure Clinician Guide JANUARY 2016
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Heart Failure Clinician Guide JANUARY 2018
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
NT-proBNP: Evidence-based application in primary care
 NT-proBNP: Evidence-based application in primary care Associate Professor Rob Doughty The University of Auckland, Auckland City Hospital, Auckland Heart Group NT-proBNP: Evidence in Primary Care The problem
NT-proBNP: Evidence-based application in primary care Associate Professor Rob Doughty The University of Auckland, Auckland City Hospital, Auckland Heart Group NT-proBNP: Evidence in Primary Care The problem
Heart Failure A Disease for the Internist?
 Heart Failure A Disease for the Internist? Dr Chris Davidson Sussex Cardiac Centre BRIGHTON UK Hot Topics in Heart Failure Drug treatments Valsartan / neprilysin inhib Investigations BNP and others Devices
Heart Failure A Disease for the Internist? Dr Chris Davidson Sussex Cardiac Centre BRIGHTON UK Hot Topics in Heart Failure Drug treatments Valsartan / neprilysin inhib Investigations BNP and others Devices
Pivotal Role of Renal Function in Acute Heart failure
 Pivotal Role of Renal Function in Acute Heart failure Doron Aronson MD, FESC Department of Cardiology RAMBAM Health Care Campus Haifa, Israel Classification and definitions of cardiorenal syndromes CRS
Pivotal Role of Renal Function in Acute Heart failure Doron Aronson MD, FESC Department of Cardiology RAMBAM Health Care Campus Haifa, Israel Classification and definitions of cardiorenal syndromes CRS
The Art and Science of Diuretic therapy
 The Art and Science of Diuretic therapy Dr. Fayez EL Shaer Associate Professour of cardiology Consultant cardiologist MD, MSc, PhD, CBNC, NBE FESC, ACCP, FASNC,HFA KKUH, KFCC Heart failure: fluid overload
The Art and Science of Diuretic therapy Dr. Fayez EL Shaer Associate Professour of cardiology Consultant cardiologist MD, MSc, PhD, CBNC, NBE FESC, ACCP, FASNC,HFA KKUH, KFCC Heart failure: fluid overload
The Cardiorenal Syndrome in Heart Failure
 The Cardiorenal Syndrome in Heart Failure Van N Selby, MD Assistant Professor of Medicine Advanced Heart Failure Program, UCSF October 9, 2015 Disclosures None 1 Cardiorenal Syndrome (CRS) A pathophysiologic
The Cardiorenal Syndrome in Heart Failure Van N Selby, MD Assistant Professor of Medicine Advanced Heart Failure Program, UCSF October 9, 2015 Disclosures None 1 Cardiorenal Syndrome (CRS) A pathophysiologic
8:30-10:30 WS #4: Cardiology :00-13:00 WS #11: Cardiology 101 (Repeated)
") Professor Ralph Stewart Cardiologist Auckland City Hospital Green Lane Cardiovascular Research Unit Auckland Heart Group Fiona Stewart Cardiologist Green Lane Hospital National Women's Hospital Professor
Professor Ralph Stewart Cardiologist Auckland City Hospital Green Lane Cardiovascular Research Unit Auckland Heart Group Fiona Stewart Cardiologist Green Lane Hospital National Women's Hospital Professor
Acute heart failure, beyond conventional treatment: persisting low output
 Acute heart failure, beyond conventional treatment: persisting low output Alexandre Mebazaa, FESC Hôpital Lariboisière, Université Paris 7 U942 Inserm Conflict of Interest Lecture fee: Orion No other conflicts
Acute heart failure, beyond conventional treatment: persisting low output Alexandre Mebazaa, FESC Hôpital Lariboisière, Université Paris 7 U942 Inserm Conflict of Interest Lecture fee: Orion No other conflicts
Using Lung Ultrasound to Diagnose and Manage Acute Heart Failure
 Using Lung Ultrasound to Diagnose and Manage Acute Heart Failure Jennifer Martindale, MD Assistant Professor Department of Emergency Medicine SUNY Downstate/Kings County Hospital Brooklyn, NY What is acute
Using Lung Ultrasound to Diagnose and Manage Acute Heart Failure Jennifer Martindale, MD Assistant Professor Department of Emergency Medicine SUNY Downstate/Kings County Hospital Brooklyn, NY What is acute
Case 1. Case 2. What do you think about reducing or discontinuing some of the above now that his LVEF has normalized?
 Case 1 A primary care colleague inquires what to do with a patient (HFrEF in NSR) who has a digoxin level of 2.8ng/ml. Level was obtained at 10am, patient takes all medications at one time upon arising
Case 1 A primary care colleague inquires what to do with a patient (HFrEF in NSR) who has a digoxin level of 2.8ng/ml. Level was obtained at 10am, patient takes all medications at one time upon arising
Heart-failure or Kidney Failure?
 Heart-failure or Kidney Failure? Dr Ajith James Consultant Nephrologist Barts Health and BHRUT Mr AR 65 yrs Case Type 2 DM, IHD-MI 1998, 2003. PCI x 3. CABG 2008, HT CCF with LVEF 30% 2014. NYHA Class
Heart-failure or Kidney Failure? Dr Ajith James Consultant Nephrologist Barts Health and BHRUT Mr AR 65 yrs Case Type 2 DM, IHD-MI 1998, 2003. PCI x 3. CABG 2008, HT CCF with LVEF 30% 2014. NYHA Class
Management of Acute Heart Failure
 Management of Acute Heart Failure Uri Elkayam, MD Professor of Medicine University of Southern California School of Medicine Los Angeles, California elkayam@usc.edu ADHF Treatments Goals.2 Improve symptoms.
Management of Acute Heart Failure Uri Elkayam, MD Professor of Medicine University of Southern California School of Medicine Los Angeles, California elkayam@usc.edu ADHF Treatments Goals.2 Improve symptoms.
HeFSSA Practitioners Program 2017 Theme The Patient Journey: Feel Good and Live Long. Case Study 2
 HeFSSA Practitioners Program 2017 Theme The Patient Journey: Feel Good and Live Long Case Study 2 HEART FAILURE WITH MID-RANGE EJECTION FRACTION TREATMENT OPTIONS CLINICAL CASE MEDICAL HISTORY 59-year-old
HeFSSA Practitioners Program 2017 Theme The Patient Journey: Feel Good and Live Long Case Study 2 HEART FAILURE WITH MID-RANGE EJECTION FRACTION TREATMENT OPTIONS CLINICAL CASE MEDICAL HISTORY 59-year-old
Cardio-Renal Syndrome in Acute Heart Failure:
 Cardio-Renal Syndrome in Acute Heart Failure: Target for Therapy Marvin A. Konstam, M.D. Research support and/or consulting relevant to this lecture: Merck, Otsuka, Johnson & Johnson; Amgen; Cardiokine
Cardio-Renal Syndrome in Acute Heart Failure: Target for Therapy Marvin A. Konstam, M.D. Research support and/or consulting relevant to this lecture: Merck, Otsuka, Johnson & Johnson; Amgen; Cardiokine
Overcoming the Cardiorenal Syndrome
 Overcoming the Cardiorenal Syndrome October 29, 2016 Randall C Starling MD MPH FACC FESC FHFSA FHFA Professor of Medicine Heart & Vascular Institute Cleveland Clinic Lerner College of Medicine Cleveland
Overcoming the Cardiorenal Syndrome October 29, 2016 Randall C Starling MD MPH FACC FESC FHFSA FHFA Professor of Medicine Heart & Vascular Institute Cleveland Clinic Lerner College of Medicine Cleveland
Heart Failure and Renal Disease Cardiorenal Syndrome
 Advanced Heart Failure: Clinical Challenges Heart Failure and Renal Disease Cardiorenal Syndrome 17 th Apr 2015 Ju-Hee Lee, M.D Cardiovascular Center, Chungbuk National University Hospital Chungbuk National
Advanced Heart Failure: Clinical Challenges Heart Failure and Renal Disease Cardiorenal Syndrome 17 th Apr 2015 Ju-Hee Lee, M.D Cardiovascular Center, Chungbuk National University Hospital Chungbuk National
Mechanical versus bioprosthetic valve. Intern: Supervisor: VS
 Mechanical versus bioprosthetic valve Intern: Supervisor: VS Patient basic data ID: N102110716 Name: Age: 64 years old Sex: male Occupation: Admission date: 0960528 Chief complaint Exertional dyspnea for
Mechanical versus bioprosthetic valve Intern: Supervisor: VS Patient basic data ID: N102110716 Name: Age: 64 years old Sex: male Occupation: Admission date: 0960528 Chief complaint Exertional dyspnea for
IN-HF on line: patient settings (Enrollement period= )
") IN-HF on line: atient settings (Enrollement eriod= 1995-2018) N of centers (total) 187 N of centers (ts. AHF only) 13 N of centers (ts. CHF only) 71 N of centers (both ts. AHF and CHF) 103 N of atients
IN-HF on line: atient settings (Enrollement eriod= 1995-2018) N of centers (total) 187 N of centers (ts. AHF only) 13 N of centers (ts. CHF only) 71 N of centers (both ts. AHF and CHF) 103 N of atients
Acute Kidney Injury in the Hospitalized Patient
 Acute Kidney Injury in the Hospitalized Patient Biff F. Palmer, M.D. Professor of Internal Medicine University of Texas Southwestern Medical Center, Dallas Texas Classification of Acute Kidney Injury 1
Acute Kidney Injury in the Hospitalized Patient Biff F. Palmer, M.D. Professor of Internal Medicine University of Texas Southwestern Medical Center, Dallas Texas Classification of Acute Kidney Injury 1
Medical Management of Acute Heart Failure
 Critical Care Medicine and Trauma Medical Management of Acute Heart Failure Mary O. Gray, MD, FAHA Associate Professor of Medicine University of California, San Francisco Staff Cardiologist and Training
Critical Care Medicine and Trauma Medical Management of Acute Heart Failure Mary O. Gray, MD, FAHA Associate Professor of Medicine University of California, San Francisco Staff Cardiologist and Training
Clinical Case. Female, 62 years January 2016
 Clinical Case Female, 62 years January 2016 Dr. Ramón Corbalán H. Facultad de Medicina División de Enfermedades Cardiovasculares Pontificia Universidad Católica de Chile Clinical Hx Background: Ostheoartritis
Clinical Case Female, 62 years January 2016 Dr. Ramón Corbalán H. Facultad de Medicina División de Enfermedades Cardiovasculares Pontificia Universidad Católica de Chile Clinical Hx Background: Ostheoartritis
Case Presentation. This presentation is the intellectual property of the author. Contact them for permission to reprint and/or distribute.
 Worsening Renal Function in Heart Failure Patients Mark Drazner, MD, MSc Clinical Chief of Cardiology Medical Director, CHF/VAD/Transplant James M. Wooten Chair in Cardiology UT Southwestern Medical Center
Worsening Renal Function in Heart Failure Patients Mark Drazner, MD, MSc Clinical Chief of Cardiology Medical Director, CHF/VAD/Transplant James M. Wooten Chair in Cardiology UT Southwestern Medical Center
Treating the patient with acute heart failure. What do we really know? Principles of acute heart failure treatment
 ESC 2012 27Aug - 3Sep, 2012, Munich, Germany Treating the patient with acute heart failure. What do we really know? Principles of acute heart failure treatment Marco Metra, MD, FESC Cardiology University
ESC 2012 27Aug - 3Sep, 2012, Munich, Germany Treating the patient with acute heart failure. What do we really know? Principles of acute heart failure treatment Marco Metra, MD, FESC Cardiology University
Ruolo dei Marcatori Bioumorali nello scompenso cardiaco
 Ruolo dei Marcatori Bioumorali nello scompenso cardiaco Head Emergency Medicine Sant Andrea Hospital Director Postgraduate School of Emergency Medicine Faculty od Medicine and Psycology Sapienza University
Ruolo dei Marcatori Bioumorali nello scompenso cardiaco Head Emergency Medicine Sant Andrea Hospital Director Postgraduate School of Emergency Medicine Faculty od Medicine and Psycology Sapienza University
Heart Failure. Dr. William Vosik. January, 2012
 Heart Failure Dr. William Vosik January, 2012 Questions for clinicians to ask Is this heart failure? What is the underlying cause? What are the associated disease processes? Which evidence-based treatment
Heart Failure Dr. William Vosik January, 2012 Questions for clinicians to ask Is this heart failure? What is the underlying cause? What are the associated disease processes? Which evidence-based treatment
Renal Optimization Strategies Evaluation in Acute Heart Failure (ROSE AHF): A Randomized Clinical Trial
: A Randomized Clinical Trial") Renal Optimization Strategies Evaluation in Acute Heart Failure (ROSE AHF): A Randomized Clinical Trial Horng H Chen MD on behalf of the NHLBI Heart Failure Clinical Research Network Background AHF + Renal
Renal Optimization Strategies Evaluation in Acute Heart Failure (ROSE AHF): A Randomized Clinical Trial Horng H Chen MD on behalf of the NHLBI Heart Failure Clinical Research Network Background AHF + Renal
Impact of Nicorandil on Renal Function in Patients With Acute Heart Failure and Pre-Existing Renal Dysfunction
 Impact of Nicorandil on Renal Function in Patients With Acute Heart Failure and Pre-Existing Renal Dysfunction Masahito Shigekiyo, Kenji Harada, Ayumi Okada, Naho Terada, Hiroyoshi Yoshikawa, Akira Hirono,
Impact of Nicorandil on Renal Function in Patients With Acute Heart Failure and Pre-Existing Renal Dysfunction Masahito Shigekiyo, Kenji Harada, Ayumi Okada, Naho Terada, Hiroyoshi Yoshikawa, Akira Hirono,
Management of acute decompensated heart failure and cardiogenic shock. Arintaya Phrommintikul Department of Medicine CMU
 Management of acute decompensated heart failure and cardiogenic shock Arintaya Phrommintikul Department of Medicine CMU Acute heart failure: spectrum Case 64 y/o M with Hx of non-ischemic DCM (LVEF=25-30%)
Management of acute decompensated heart failure and cardiogenic shock Arintaya Phrommintikul Department of Medicine CMU Acute heart failure: spectrum Case 64 y/o M with Hx of non-ischemic DCM (LVEF=25-30%)
LITERATURE REVIEW: HEART FAILURE. Chief Residents
 LITERATURE REVIEW: HEART FAILURE Chief Residents Heart Failure EF 40% HFrEF Problem with contractility EF 40-50% HFmrEF EF > 50% HFpEF Problem with filling/relaxation RISK FACTORS Post MI HTN DM Obesity
LITERATURE REVIEW: HEART FAILURE Chief Residents Heart Failure EF 40% HFrEF Problem with contractility EF 40-50% HFmrEF EF > 50% HFpEF Problem with filling/relaxation RISK FACTORS Post MI HTN DM Obesity
ACUTE HEART FAILURE in the ED. Pr. Samir Nouira Emergency Department Fattouma Bourguiba University Hospital Monastir Tunisia
 ACUTE HEART FAILURE in the ED Pr. Samir Nouira Emergency Department Fattouma Bourguiba University Hospital Monastir Tunisia ACUTE HEART FAILURE 80% Acute Heart Failure Syndrome Sensitivity Specificity
ACUTE HEART FAILURE in the ED Pr. Samir Nouira Emergency Department Fattouma Bourguiba University Hospital Monastir Tunisia ACUTE HEART FAILURE 80% Acute Heart Failure Syndrome Sensitivity Specificity
Advanced Heart Failure Management. Dr Andrew Hannah Consultant Cardiologist Aberdeen Royal Infirmary
 Advanced Heart Failure Management Dr Andrew Hannah Consultant Cardiologist Aberdeen Royal Infirmary Grading of heart failure Mr WY age 73 3/12 dyspnoea, fatigue and some ankle oedema PMH: hypertension
Advanced Heart Failure Management Dr Andrew Hannah Consultant Cardiologist Aberdeen Royal Infirmary Grading of heart failure Mr WY age 73 3/12 dyspnoea, fatigue and some ankle oedema PMH: hypertension
Case Summary. Workshop Overview. Mr. M
 9:00 10:30 Workshop Overview Mr. M Who is this document primarily intended to reach? What is the format? How soon should I see a newly referred heart failure patient? How often should my heart failure
9:00 10:30 Workshop Overview Mr. M Who is this document primarily intended to reach? What is the format? How soon should I see a newly referred heart failure patient? How often should my heart failure
Cardiology. Presented by: Dr Paul Bethell GP Lead for Planned Care
 Cardiology Presented by: Dr Paul Bethell GP Lead for Planned Care 16 th April 2015 Integrated Cardiology Service for Ipswich and East Suffolk CCG IHT 6 consultants - all with specialist areas PCI CoW rapid
Cardiology Presented by: Dr Paul Bethell GP Lead for Planned Care 16 th April 2015 Integrated Cardiology Service for Ipswich and East Suffolk CCG IHT 6 consultants - all with specialist areas PCI CoW rapid
Acute kidney injury and outcomes in acute decompensated heart failure in Korea
 Acute kidney injury and outcomes in acute decompensated heart failure in Korea Mi-Seung Shin 1, Seong Woo Han 2, Dong-Ju Choi 3, Eun Seok Jeon 4, Jae-Joong Kim 5, Myeong-Chan Cho 6, Shung Chull Chae 7,
Acute kidney injury and outcomes in acute decompensated heart failure in Korea Mi-Seung Shin 1, Seong Woo Han 2, Dong-Ju Choi 3, Eun Seok Jeon 4, Jae-Joong Kim 5, Myeong-Chan Cho 6, Shung Chull Chae 7,
WORSENING OF RENAL FUNCTION AFTER RAS INHIBITION IN DECOMPENSATED HEART FAILURE: CLINICAL IMPLICATIONS
 WORSENING OF RENAL FUNCTION AFTER RAS INHIBITION IN DECOMPENSATED HEART FAILURE: CLINICAL IMPLICATIONS George Bakris, MD, FASH, FAHA, FASN Professor of Medicine Director, Comprehensive Hypertension Center
WORSENING OF RENAL FUNCTION AFTER RAS INHIBITION IN DECOMPENSATED HEART FAILURE: CLINICAL IMPLICATIONS George Bakris, MD, FASH, FAHA, FASN Professor of Medicine Director, Comprehensive Hypertension Center
Medical Treatment for acute Decompensated Heart Failure. Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011
 Medical Treatment for acute Decompensated Heart Failure Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011 2010 HFSA guidelines for ADHF 2009 focused update of the 2005 American College
Medical Treatment for acute Decompensated Heart Failure Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011 2010 HFSA guidelines for ADHF 2009 focused update of the 2005 American College
SUPPLEMENTAL MATERIAL
 SUPPLEMENTAL MATERIAL Table S1: Number and percentage of patients by age category Distribution of age Age
SUPPLEMENTAL MATERIAL Table S1: Number and percentage of patients by age category Distribution of age Age
TRIPLE THERAPY, NOACs with concurrent indication for DAPT. Paul Wright Lead Cardiac Pharmacist The Heart, UCLH NHS Foundation Trust
 TRIPLE THERAPY, NOACs with concurrent indication for DAPT Paul Wright Lead Cardiac Pharmacist The Heart, UCLH NHS Foundation Trust Content Why consider triple therapy What we know of triple therapy Current
TRIPLE THERAPY, NOACs with concurrent indication for DAPT Paul Wright Lead Cardiac Pharmacist The Heart, UCLH NHS Foundation Trust Content Why consider triple therapy What we know of triple therapy Current
SGK 2016 Session: Postgraduate Course in Heart Failure Lausanne, 15. June 2016 Heart Failure Guidelines 2016
 SGK 2016 Session: Postgraduate Course in Heart Failure Lausanne, 15. June 2016 Heart Failure Guidelines 2016 Matthias Nägele, MD University Hospital Zurich Disclosures I have nothing to disclose. The new
SGK 2016 Session: Postgraduate Course in Heart Failure Lausanne, 15. June 2016 Heart Failure Guidelines 2016 Matthias Nägele, MD University Hospital Zurich Disclosures I have nothing to disclose. The new
Slide 1. Slide 2. Slide 3. Managing Acute Heart Failure Trials and Tribulations. Declaration of
 Slide 1 Managing Acute Heart Failure Trials and Tribulations Martin R Cowie MD MSc FRCP FRCP (Ed) FESC Professor of Cardiology, Imperial College London m.cowie@imperial.ac.uk @ProfMartinCowie Slide 2 Declaration
Slide 1 Managing Acute Heart Failure Trials and Tribulations Martin R Cowie MD MSc FRCP FRCP (Ed) FESC Professor of Cardiology, Imperial College London m.cowie@imperial.ac.uk @ProfMartinCowie Slide 2 Declaration
Practical Points in Cardiorenal Syndrome
 Practical Points in Cardiorenal Syndrome Vichai Senthong, MD. Cardiovascular Unit, Faculty of Medicine Khon Kaen university HFCT Annual Scientific Meeting June 16, 2017, Eastin Grand Sathorn Hotel, Bangkok
Practical Points in Cardiorenal Syndrome Vichai Senthong, MD. Cardiovascular Unit, Faculty of Medicine Khon Kaen university HFCT Annual Scientific Meeting June 16, 2017, Eastin Grand Sathorn Hotel, Bangkok
The Role of Oral Anticoagulants in Atrial Fibrillation: What You Need to Know Now. Bradley A. Hardin, MD Richard F.
 The Role of Oral Anticoagulants in Atrial Fibrillation: What You Need to Know Now Bradley A. Hardin, MD Richard F. Otten, MD, FACC Outline Atrial Fibrillation Overview Overview of New Oral Anticoagulants
The Role of Oral Anticoagulants in Atrial Fibrillation: What You Need to Know Now Bradley A. Hardin, MD Richard F. Otten, MD, FACC Outline Atrial Fibrillation Overview Overview of New Oral Anticoagulants
Copeptin in heart failure: Associations with clinical characteristics and prognosis
 Copeptin in heart failure: Associations with clinical characteristics and prognosis D. Berliner, N. Deubner, W. Fenske, S. Brenner, G. Güder, B. Allolio, R. Jahns, G. Ertl, CE. Angermann, S. Störk for
Copeptin in heart failure: Associations with clinical characteristics and prognosis D. Berliner, N. Deubner, W. Fenske, S. Brenner, G. Güder, B. Allolio, R. Jahns, G. Ertl, CE. Angermann, S. Störk for
ACUTE KIDNEY INJURY. Stuart Linas U. Colorado SOM
 ACUTE KIDNEY INJURY Stuart Linas U. Colorado SOM Marked increases in incidence of dialysis-requiring AKI in last decade JASN 24 37 2013 Question 1 Of patients who recover from an episode of AKI, what percentage
ACUTE KIDNEY INJURY Stuart Linas U. Colorado SOM Marked increases in incidence of dialysis-requiring AKI in last decade JASN 24 37 2013 Question 1 Of patients who recover from an episode of AKI, what percentage
Topic: Chronic Heart Failure Cases for Monday s March 21th lecture.
 1 Phar6122: CV section Date: 3/10/05 Topic: Chronic Heart Failure Cases for Monday s March 21th lecture. Directions: This handout includes three chronic heart failure cases of increasing difficulty. In
1 Phar6122: CV section Date: 3/10/05 Topic: Chronic Heart Failure Cases for Monday s March 21th lecture. Directions: This handout includes three chronic heart failure cases of increasing difficulty. In
A LONG WAY TO HEART FAILURE T H I E R R Y C. G I L L E B E R T, G H E N T U N I V E R S I T Y, B E L G I U M
 A LONG WAY TO HEART FAILURE T H I E R R Y C. G I L L E B E R T, G H E N T U N I V E R S I T Y, B E L G I U M 1 M.A.M, 1943 Chronic low back pain Arterial hypertension and hyperlipidaemia Intolerance for
A LONG WAY TO HEART FAILURE T H I E R R Y C. G I L L E B E R T, G H E N T U N I V E R S I T Y, B E L G I U M 1 M.A.M, 1943 Chronic low back pain Arterial hypertension and hyperlipidaemia Intolerance for
Solving the Revolving Door
 Solving the Revolving Door Managing Heart Failure at Transitions of Care and Beyond Brent N. Reed, PharmD, BCCP Associate Professor University of Maryland School of Pharmacy ATRIUM Cardiology Collaborative
Solving the Revolving Door Managing Heart Failure at Transitions of Care and Beyond Brent N. Reed, PharmD, BCCP Associate Professor University of Maryland School of Pharmacy ATRIUM Cardiology Collaborative
E/Ea is NOT an essential estimator of LV filling pressures
 Euroecho Kopenhagen Echo in Resynchronization in 2010 E/Ea is NOT an essential estimator of LV filling pressures Wilfried Mullens, MD, PhD December 10, 2010 Ziekenhuis Oost Limburg Genk University Hasselt
Euroecho Kopenhagen Echo in Resynchronization in 2010 E/Ea is NOT an essential estimator of LV filling pressures Wilfried Mullens, MD, PhD December 10, 2010 Ziekenhuis Oost Limburg Genk University Hasselt
Rationale for renal replacement therapy in ICU: indications, approaches and outcomes. Richard Beale
 Rationale for renal replacement therapy in ICU: indications, approaches and outcomes Richard Beale RIFLE classification (ADQI group) 2004 Outcome AKIN classification Definition: Abrupt (within 48 hrs)
Rationale for renal replacement therapy in ICU: indications, approaches and outcomes Richard Beale RIFLE classification (ADQI group) 2004 Outcome AKIN classification Definition: Abrupt (within 48 hrs)
Identification of patients with heart failure and PREserved systolic Function : an Epidemiologic Regional study
 Identification of patients with heart failure and PREserved systolic Function : an Epidemiologic Regional study Dr. Antonio Magaña M.D. (on behalf I-PREFER investigators group) Stockholm, Sweden, August
Identification of patients with heart failure and PREserved systolic Function : an Epidemiologic Regional study Dr. Antonio Magaña M.D. (on behalf I-PREFER investigators group) Stockholm, Sweden, August
ARIC HEART FAILURE HOSPITAL RECORD ABSTRACTION FORM. General Instructions: ID NUMBER: FORM NAME: H F A DATE: 10/13/2017 VERSION: CONTACT YEAR NUMBER:
 ARIC HEART FAILURE HOSPITAL RECORD ABSTRACTION FORM General Instructions: The Heart Failure Hospital Record Abstraction Form is completed for all heart failure-eligible cohort hospitalizations. Refer to
ARIC HEART FAILURE HOSPITAL RECORD ABSTRACTION FORM General Instructions: The Heart Failure Hospital Record Abstraction Form is completed for all heart failure-eligible cohort hospitalizations. Refer to
DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE
 DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE Mefri Yanni, MD Bagian Kardiologi dan Kedokteran Vaskular RS.DR.M.Djamil Padang The 3rd Symcard Padang, Mei 2013 Outline Diagnosis Diagnosis Treatment options
DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE Mefri Yanni, MD Bagian Kardiologi dan Kedokteran Vaskular RS.DR.M.Djamil Padang The 3rd Symcard Padang, Mei 2013 Outline Diagnosis Diagnosis Treatment options
How to define the target population?
 Heart Failure 2011 22-24 May. Gothenburg, Sweden Mortality or morbidity as target in acute heart failure trials How to define the target population? Marco Metra, Brescia The Burden of Acute HF Acute HF
Heart Failure 2011 22-24 May. Gothenburg, Sweden Mortality or morbidity as target in acute heart failure trials How to define the target population? Marco Metra, Brescia The Burden of Acute HF Acute HF
A patient with decompensated HF
 A patient with decompensated HF Professor Michel KOMAJDA University Pierre & Marie Curie Pitie Salpetriere Hospital Department of Cardiology Paris (France) Declaration Of Interest 2010 Speaker : Servier,
A patient with decompensated HF Professor Michel KOMAJDA University Pierre & Marie Curie Pitie Salpetriere Hospital Department of Cardiology Paris (France) Declaration Of Interest 2010 Speaker : Servier,
HEART FAILURE. Ali Mehr, MD, FACC
 HEART FAILURE Ali Mehr, MD, FACC Advanced Heart Failure and Transplant Cardiologist Director, Echocardiography Lab Phoenix VA Health Care System Associate Professor of Medicine University of Arizona, COM,
HEART FAILURE Ali Mehr, MD, FACC Advanced Heart Failure and Transplant Cardiologist Director, Echocardiography Lab Phoenix VA Health Care System Associate Professor of Medicine University of Arizona, COM,
2016 Update to Heart Failure Clinical Practice Guidelines
 2016 Update to Heart Failure Clinical Practice Guidelines Mitchell T. Saltzberg, MD, FACC, FAHA, FHFSA Medical Director of Advanced Heart Failure Froedtert & Medical College of Wisconsin Stages, Phenotypes
2016 Update to Heart Failure Clinical Practice Guidelines Mitchell T. Saltzberg, MD, FACC, FAHA, FHFSA Medical Director of Advanced Heart Failure Froedtert & Medical College of Wisconsin Stages, Phenotypes
Protocol Identifier Subject Identifier Visit Description. [Y] Yes [N] No. [Y] Yes [N] N. If Yes, admission date and time: Day Month Year
![Protocol Identifier Subject Identifier Visit Description. [Y] Yes [N] No. [Y] Yes [N] N. If Yes, admission date and time: Day Month Year](/thumbs/76/74263761.jpg "Protocol Identifier Subject Identifier Visit Description. [Y] Yes [N] No. [Y] Yes [N] N. If Yes, admission date and time: Day Month Year") PAST MEDICAL HISTORY Has the subject had a prior episode of heart failure? o Does the subject have a prior history of exposure to cardiotoxins, such as anthracyclines? URGENT HEART FAILURE VISIT Did heart
PAST MEDICAL HISTORY Has the subject had a prior episode of heart failure? o Does the subject have a prior history of exposure to cardiotoxins, such as anthracyclines? URGENT HEART FAILURE VISIT Did heart
Sandwell Community Heart Failure Team. Community Heart failure Specialist Nurses: Hilda O Keeffe- Henry and Jacqui Elson-Whittaker
 Sandwell Community Heart Failure Team Community Heart failure Specialist Nurses: Hilda O Keeffe- Henry and Jacqui Elson-Whittaker NICE 2010 Incidence and Prevalence 900,000 people in the UK with HF Same
Sandwell Community Heart Failure Team Community Heart failure Specialist Nurses: Hilda O Keeffe- Henry and Jacqui Elson-Whittaker NICE 2010 Incidence and Prevalence 900,000 people in the UK with HF Same
Chronic. Outline. Congestive^ Heart Failure: Update on Effective Monitoring and Treatment. Heart Failure Epidemiology
 Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
Management of Advanced Systolic Heart Failure. Robert W. Hull MD FACC Associate Professor of Medicine West Virginia University
 Management of Advanced Systolic Heart Failure Robert W. Hull MD FACC Associate Professor of Medicine West Virginia University American College of Cardiology Foundation (ACCF) American Heart Association
Management of Advanced Systolic Heart Failure Robert W. Hull MD FACC Associate Professor of Medicine West Virginia University American College of Cardiology Foundation (ACCF) American Heart Association
Section 3: Prevention and Treatment of AKI
 http://www.kidney-international.org & 2012 KDIGO Summary of ommendation Statements Kidney International Supplements (2012) 2, 8 12; doi:10.1038/kisup.2012.7 Section 2: AKI Definition 2.1.1: AKI is defined
http://www.kidney-international.org & 2012 KDIGO Summary of ommendation Statements Kidney International Supplements (2012) 2, 8 12; doi:10.1038/kisup.2012.7 Section 2: AKI Definition 2.1.1: AKI is defined
AF in the ER: Common Scenarios CASE 1. Fast facts. Diagnosis. Management
 AF in the ER: Common Scenarios Atrial fibrillation is a common problem with a wide spectrum of presentations. Below are five common emergency room scenarios and the management strategies for each. Evan
AF in the ER: Common Scenarios Atrial fibrillation is a common problem with a wide spectrum of presentations. Below are five common emergency room scenarios and the management strategies for each. Evan
Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes
 Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes Seung-Jae Joo and other KAMIR-NIH investigators Department of Cardiology, Jeju National
Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes Seung-Jae Joo and other KAMIR-NIH investigators Department of Cardiology, Jeju National
What is Your Diagnosis?
 What is Your Diagnosis? A STORM R Dulgheru, Liege, Belgium Faculty disclosure Raluca Dulgheru I have no financial relationships to disclose. Case presentation 52 years old male Ongoing oppressive chest
What is Your Diagnosis? A STORM R Dulgheru, Liege, Belgium Faculty disclosure Raluca Dulgheru I have no financial relationships to disclose. Case presentation 52 years old male Ongoing oppressive chest
CKD & HT. Anne-Marie Angus
 CKD & HT Anne-Marie Angus Hypertension definitions Persisting BP >140/90 and HBPM >135/85 Stage 1 >140/90 (HBPM >135/85) Stage 2 >160/100 (HBPM >150/90) Severe >180/100 White coat HT Why treat? A major
CKD & HT Anne-Marie Angus Hypertension definitions Persisting BP >140/90 and HBPM >135/85 Stage 1 >140/90 (HBPM >135/85) Stage 2 >160/100 (HBPM >150/90) Severe >180/100 White coat HT Why treat? A major
Aldosterone Antagonism in Heart Failure: Now for all Patients?
 Aldosterone Antagonism in Heart Failure: Now for all Patients? Inder Anand, MD, FRCP, D Phil (Oxon.) Professor of Medicine, University of Minnesota, Director Heart Failure Program, VA Medical Center 111C
Aldosterone Antagonism in Heart Failure: Now for all Patients? Inder Anand, MD, FRCP, D Phil (Oxon.) Professor of Medicine, University of Minnesota, Director Heart Failure Program, VA Medical Center 111C
HFpEF, Mito or Realidad?
 HFpEF, Mito or Realidad? Ileana L. Piña, MD, MPH Professor of Medicine and Epidemiology/Population Health Associate Chief for Academic Affairs -- Cardiology Montefiore-Einstein Medical Center Bronx, NY
HFpEF, Mito or Realidad? Ileana L. Piña, MD, MPH Professor of Medicine and Epidemiology/Population Health Associate Chief for Academic Affairs -- Cardiology Montefiore-Einstein Medical Center Bronx, NY
The right heart: the Cinderella of heart failure
 The right heart: the Cinderella of heart failure Piotr Ponikowski, MD, PhD, FESC Medical University, Centre for Heart Disease Clinical Military Hospital Wroclaw, Poland none Disclosure Look into the Heart
The right heart: the Cinderella of heart failure Piotr Ponikowski, MD, PhD, FESC Medical University, Centre for Heart Disease Clinical Military Hospital Wroclaw, Poland none Disclosure Look into the Heart
Summary/Key Points Introduction
 Summary/Key Points Introduction Scope of Heart Failure (HF) o 6.5 million Americans 20 years of age have HF o 960,000 new cases of HF diagnosed annually o 5-year survival rate for HF is ~50% Classification
Summary/Key Points Introduction Scope of Heart Failure (HF) o 6.5 million Americans 20 years of age have HF o 960,000 new cases of HF diagnosed annually o 5-year survival rate for HF is ~50% Classification
ENDPOINTS FOR AKI STUDIES
 ENDPOINTS FOR AKI STUDIES Raymond Vanholder, University Hospital, Ghent, Belgium SUMMARY! AKI as an endpoint! Endpoints for studies in AKI 2 AKI AS AN ENDPOINT BEFORE RIFLE THE LIST OF DEFINITIONS WAS
ENDPOINTS FOR AKI STUDIES Raymond Vanholder, University Hospital, Ghent, Belgium SUMMARY! AKI as an endpoint! Endpoints for studies in AKI 2 AKI AS AN ENDPOINT BEFORE RIFLE THE LIST OF DEFINITIONS WAS
Evaluation and Management of Acute Decompensated Heart Failure (HF) with Reduced Ejection Fraction Systolic Heart Failure (HFrEF)(EF<40%
 with Reduced Ejection Fraction Systolic Heart Failure (HFrEF)(EF<40%") Evaluation and Management of Acute Decompensated Heart Failure (HF) with Reduced Ejection Fraction Systolic Heart Failure (HFrEF)(EF
Evaluation and Management of Acute Decompensated Heart Failure (HF) with Reduced Ejection Fraction Systolic Heart Failure (HFrEF)(EF
HEART FAILURE: PHARMACOTHERAPY UPDATE
 HEART FAILURE: PHARMACOTHERAPY UPDATE 3 HEART FAILURE REVIEW 1 5.1 million x1.25 = 6.375 million 40 years old = MICHAEL F. AKERS, PHARM.D. CLINICAL PHARMACIST CENTRACARE HEALTH, ST. CLOUD HOSPITAL HF Diagnosis
HEART FAILURE: PHARMACOTHERAPY UPDATE 3 HEART FAILURE REVIEW 1 5.1 million x1.25 = 6.375 million 40 years old = MICHAEL F. AKERS, PHARM.D. CLINICAL PHARMACIST CENTRACARE HEALTH, ST. CLOUD HOSPITAL HF Diagnosis
Dr Micheal Looney Consultant Anaesthetist Connolly Hospital Blanchardstown. To Delay or Not to Delay Hip Fracture Surgery
 Dr Micheal Looney Consultant Anaesthetist Connolly Hospital Blanchardstown To Delay or Not to Delay Hip Fracture Surgery "You may delay, but time will not, and lost time is never found again." Benjamin
Dr Micheal Looney Consultant Anaesthetist Connolly Hospital Blanchardstown To Delay or Not to Delay Hip Fracture Surgery "You may delay, but time will not, and lost time is never found again." Benjamin
ARNI (Angiotensin Receptor blocker / Neprilysin Inhibitors [Sacubutril/Valsartan]) Heart Failure Medication Initiation and Titration
![ARNI (Angiotensin Receptor blocker / Neprilysin Inhibitors [Sacubutril/Valsartan]) Heart Failure Medication Initiation and Titration](/thumbs/77/76069192.jpg "ARNI (Angiotensin Receptor blocker / Neprilysin Inhibitors [Sacubutril/Valsartan]) Heart Failure Medication Initiation and Titration") ARNI (Angiotensin Receptor blocker / Neprilysin Inhibitors [Sacubutril/Valsartan]) Heart Failure Medication and Symptomatic HF despite ACEI/ARB and B-blocker therapy Bilateral renal artery stenosis Moderate/Severe
ARNI (Angiotensin Receptor blocker / Neprilysin Inhibitors [Sacubutril/Valsartan]) Heart Failure Medication and Symptomatic HF despite ACEI/ARB and B-blocker therapy Bilateral renal artery stenosis Moderate/Severe
Can We Achieve Precision Solute Control with CRRT?
 Can We Achieve Precision Solute Control with CRRT? Claudio Ronco, M.D. David Selewski, M.D. Rolando Claure-Del Granado, M.D. AKI & CRRT Conference February, 2019 Disclosures I have no actual or potential
Can We Achieve Precision Solute Control with CRRT? Claudio Ronco, M.D. David Selewski, M.D. Rolando Claure-Del Granado, M.D. AKI & CRRT Conference February, 2019 Disclosures I have no actual or potential
Dr A Pokrajac MD MSc MRCP Consultant
 Dr A Pokrajac MD MSc MRCP Consultant Onset at 5-15 years of T1DM Can be present at diagnosis of T2DM Detect in regular MA/Cr screening (2X first urine sample, no UTI, no other causes) Contributing Factors
Dr A Pokrajac MD MSc MRCP Consultant Onset at 5-15 years of T1DM Can be present at diagnosis of T2DM Detect in regular MA/Cr screening (2X first urine sample, no UTI, no other causes) Contributing Factors
Navigating the identification, diagnosis and management of pulmonary hypertension using the updated ESC/ERS guidelines
 Navigating the identification, diagnosis and management of pulmonary hypertension using the updated ESC/ERS guidelines Host: Marc Humbert Speaker: Simon Gibbs Marc HUMBERT, MD, PhD Professor of Respiratory
Navigating the identification, diagnosis and management of pulmonary hypertension using the updated ESC/ERS guidelines Host: Marc Humbert Speaker: Simon Gibbs Marc HUMBERT, MD, PhD Professor of Respiratory
Atrial Fibrillation Version 2 11/4/15 This order set must be used with an admission order set if patient not already admitted.
 Patient Name: Diagnosis: Allergies with reaction type: Atrial Fibrillation Version 2 11/4/15 This order set must be used with an admission order set if patient not already admitted. Telemetry Medical Telemetry:
Patient Name: Diagnosis: Allergies with reaction type: Atrial Fibrillation Version 2 11/4/15 This order set must be used with an admission order set if patient not already admitted. Telemetry Medical Telemetry:
State of the Art: acute heart failure Is it just congestion?
 ESC CONGRESS 2017 Barcelona, 26. 30. August 2017 State of the Art: acute heart failure Is it just congestion? S.B. Felix, FESC Klinik für Innere Medizin B Ernst-Moritz-Arndt-Universität Greifswald 1456
ESC CONGRESS 2017 Barcelona, 26. 30. August 2017 State of the Art: acute heart failure Is it just congestion? S.B. Felix, FESC Klinik für Innere Medizin B Ernst-Moritz-Arndt-Universität Greifswald 1456
Patient Case Mrs X Provided compliments of Mary Gunther, BScPharm, ACPR
 Patient Case Mrs X Provided compliments of Mary Gunther, BScPharm, ACPR ID: Mrs X is a female in her mid sixties admitted for a CHF exacerbation CC: 1. 2 week history of increasing weakness, weight gain,
Patient Case Mrs X Provided compliments of Mary Gunther, BScPharm, ACPR ID: Mrs X is a female in her mid sixties admitted for a CHF exacerbation CC: 1. 2 week history of increasing weakness, weight gain,
Patient Encounters in the Primary Care Setting
 Patient Encounters in the Primary Care Setting Carmine D Amico, D.O. Clinical Cases Overview Learning objectives Clinical case presentations Questions for audience participation 1 Clinical Cases Learning
Patient Encounters in the Primary Care Setting Carmine D Amico, D.O. Clinical Cases Overview Learning objectives Clinical case presentations Questions for audience participation 1 Clinical Cases Learning
Biomarkers for optimal management of heart failure. Cardiorenal syndrome. Veli-Pekka Harjola Helsinki University Central Hospital Helsinki, Finland
 Biomarkers for optimal management of heart failure Cardiorenal syndrome Veli-Pekka Harjola Helsinki University Central Hospital Helsinki, Finland Presenter Disclosure Information V-P Harjola The following
Biomarkers for optimal management of heart failure Cardiorenal syndrome Veli-Pekka Harjola Helsinki University Central Hospital Helsinki, Finland Presenter Disclosure Information V-P Harjola The following
Can We Achieve Precision Solute Control with CRRT?
 Can We Achieve Precision Solute Control with CRRT? Claudio Ronco, M.D. David Selewski, M.D. Rolando Claure-Del Granado, M.D. AKI & CRRT Conference February, 2019 Disclosures I have no actual or potential
Can We Achieve Precision Solute Control with CRRT? Claudio Ronco, M.D. David Selewski, M.D. Rolando Claure-Del Granado, M.D. AKI & CRRT Conference February, 2019 Disclosures I have no actual or potential
WEEK. MPharm Programme. Acute Kidney Injury. Alan M. Green MPHM13: Acute Kidney Injury. Slide 1 of 47
 MPharm Programme Acute Kidney Injury Alan M. Green 2017 Slide 1 of 47 Overview Renal Function What is it? Why does it matter? What causes it? Who is at risk? What can we (Pharmacists) do? How do you recognise
MPharm Programme Acute Kidney Injury Alan M. Green 2017 Slide 1 of 47 Overview Renal Function What is it? Why does it matter? What causes it? Who is at risk? What can we (Pharmacists) do? How do you recognise
Real World Experience with Renal Denervation Therapy
 JCR 2013 Real World Experience with Renal Denervation Therapy Seung-Hyuk Choi Division of Cardiology Samsung Medical Center Seoul, Korea Hypertension A Major Public Health Burden Astonishing prevalence
JCR 2013 Real World Experience with Renal Denervation Therapy Seung-Hyuk Choi Division of Cardiology Samsung Medical Center Seoul, Korea Hypertension A Major Public Health Burden Astonishing prevalence
Cardiology. Self Learning Package. Module 5: Pharmacology: Treatment of Acute Coronary. Prevention
 Cardiology Self Learning Package Module 5: Pharmacology: Treatment of Acute Coronary Syndromes, Module 5: Pharmacology: Hyperlipidaemia, Treatment of Acute Coronary Hypertension, Symdrome, Hyperlipidaemia,
Cardiology Self Learning Package Module 5: Pharmacology: Treatment of Acute Coronary Syndromes, Module 5: Pharmacology: Hyperlipidaemia, Treatment of Acute Coronary Hypertension, Symdrome, Hyperlipidaemia,
The FORMA Early Feasibility Study: 30-Day Outcomes of Transcatheter Tricuspid Valve Therapy in Patients with Severe Secondary Tricuspid Regurgitation
 The FORMA Early Feasibility Study: 30-Day Outcomes of Transcatheter Tricuspid Valve Therapy in Patients with Severe Secondary Tricuspid Regurgitation Susheel Kodali, MD Director, Structural Heart & Valve
The FORMA Early Feasibility Study: 30-Day Outcomes of Transcatheter Tricuspid Valve Therapy in Patients with Severe Secondary Tricuspid Regurgitation Susheel Kodali, MD Director, Structural Heart & Valve
Chronic. Outline. Congestive^ Heart Failure: Update on Effective Monitoring and Treatment. Heart Failure Epidemiology. Michael G.
 Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
CKD and risk management : NICE guideline
 CKD and risk management : NICE guideline 2008-2014 Shahed Ahmed Consultant Nephrologist shahed.ahmed@rlbuht.nhs.uk Key points : Changing parameters of CKD and NICE guidance CKD and age related change of
CKD and risk management : NICE guideline 2008-2014 Shahed Ahmed Consultant Nephrologist shahed.ahmed@rlbuht.nhs.uk Key points : Changing parameters of CKD and NICE guidance CKD and age related change of
IS IT. The Canadian Cardiovascular Society AND WHATSHOULD I DO?
 IS IT The Canadian Cardiovascular Society AND WHATSHOULD I DO? Pocket Guide Version: January 2015 About this Pocket Guide ii This pocket guide is a quick-reference tool that features diagnostic and treatment
IS IT The Canadian Cardiovascular Society AND WHATSHOULD I DO? Pocket Guide Version: January 2015 About this Pocket Guide ii This pocket guide is a quick-reference tool that features diagnostic and treatment
Contemporary Management of Heart Failure. Keerthy K Narisetty, MD Comprehensive Heart Failure Management Program BHHI Primary Care Symposium
 Contemporary Management of Heart Failure Keerthy K Narisetty, MD Comprehensive Heart Failure Management Program BHHI Primary Care Symposium Disclosures I have no relevant relationships with commercial
Contemporary Management of Heart Failure Keerthy K Narisetty, MD Comprehensive Heart Failure Management Program BHHI Primary Care Symposium Disclosures I have no relevant relationships with commercial
Hyponatremia as a Cardiovascular Biomarker
 Hyponatremia as a Cardiovascular Biomarker Uri Elkayam, MD Professor of Medicine University of Southern California Keck School of Medicine elkayam@usc.edu Disclosure Research grant from Otsuka for the
Hyponatremia as a Cardiovascular Biomarker Uri Elkayam, MD Professor of Medicine University of Southern California Keck School of Medicine elkayam@usc.edu Disclosure Research grant from Otsuka for the
I know the trials in heart failure but how do I manage my patient? Dosing of neurohormones antagonists
 I know the trials in heart failure but how do I manage my patient? Dosing of neurohormones antagonists Alessandro Fucili (Ferrara, IT) Massimo F Piepoli (Piacenza, IT) Clinical Case: 82 year old woman
I know the trials in heart failure but how do I manage my patient? Dosing of neurohormones antagonists Alessandro Fucili (Ferrara, IT) Massimo F Piepoli (Piacenza, IT) Clinical Case: 82 year old woman
Nephrology. 3 rd Year Revision Session 06/05/17 Cathal Hannan
 Nephrology 3 rd Year Revision Session 06/05/17 Cathal Hannan Aims Acute Kidney Injury-recognition and management Sample OSCE Station Clinically relevant renal physiology Aetiology of Chronic Kidney Disease
Nephrology 3 rd Year Revision Session 06/05/17 Cathal Hannan Aims Acute Kidney Injury-recognition and management Sample OSCE Station Clinically relevant renal physiology Aetiology of Chronic Kidney Disease
Chronic. Congestive^ Heart Failure: Update on Effective Monitoring and Treatment. Michael G. Shlipak, MD, MPH
 Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
Heart Failure and Renal Failure. Gerasimos Filippatos, MD, FESC, FHFA President HFA
 Heart Failure and Renal Failure Gerasimos Filippatos, MD, FESC, FHFA President HFA Definition Epidemiology Pathophysiology Management (?) Recommendations for NHLBI in cardiorenal interactions related to
Heart Failure and Renal Failure Gerasimos Filippatos, MD, FESC, FHFA President HFA Definition Epidemiology Pathophysiology Management (?) Recommendations for NHLBI in cardiorenal interactions related to