Breast Cancer: Current Approaches to Diagnosis and Treatment
|
|
|
- Norma Marion Hopkins
- 5 years ago
- Views:
Transcription
1 Breast Cancer: Current Approaches to Diagnosis and Treatment Barbara L. Smith, MD, Ph.D. Massachusetts General Hospital Division of Surgical Oncology No Disclosures
2 Incidence of Breast Cancer USA in 8 American women affected 1 in 1000 American men 266,120 new invasive breast cancers 63,960 new carcinoma in situ cases 40,920 breast cancer deaths USA: >3.1 million breast cancer survivors
3 Identifying high risk patients By risk profile At the time of cancer diagnosis
4 Risk Factors for Breast Cancer positive family history / risk gene mutations Increasing age prior breast cancer LCIS, atypical hyperplasia, radial scar hormonal factors lifestyle - diet, weight gain, alcohol radiation exposure
5 Goals for High Risk Patients Accurate assessment of degree of risk Communication of risk to patient Discussion of options for managing risk Early detection More frequent screening Additional screening modalities Prevention Chemoprevention Prophylactic mastectomy, oophorectomy
6 BRCA1/2 Mutations and Risk BRCA gene mutations account for 5-10% of breast cancer cases in the U.S. BRCA mutation carriers 60-80% develop breast cancer by age % develop ovarian cancer by age 70 Increased male breast cancer, pancreatic cancer
7 Beyond BRCA testing: New multi gene panels Tests for multiple genes available more rapidly and at reduced cost 9-gene panel now standard for breast cancer BRCA1, BRCA2, P53, PTEN, PALB2, CDH1, ATM, CHEK2, STK11 - results <2 weeks Larger panels available for families with other cancers Caveat: Interpreting impact of mutations in less familiar genes remains difficult
8 Criteria for Risk Gene Testing Breast cancer at age 45 or younger Triple negative breast cancer age 59 or younger 3 or more relatives with breast cancer Families with both breast and ovarian cancer or male breast cancer Ashkenazi Jewish women Lower threshold for testing founder mutation panel
9 Screening Mammography: Timing and frequency still controversial U.S. Preventive Services Task Force 2009: No routine mammograms for women 40-49; woman to discuss with MD For women ages 50 to 74, mammography screening every two years American Cancer Society 2015: Ages 40-44: annual mammogram optional Annual mammogram ages >55: mammogram every 2 years or annual
10 American Cancer Society breast exam guidelines Clinical breast exam every 3 years ages 20-40, annually after 40 Women should report breast changes promptly to their health care provider Breast self exam optional
11 Improved imaging options for early detection of breast cancer Improvements in mammography Tomosynthesis Whole breast ultrasound Breast MRI Identification of high risk patients More intensive screening Prevention interventions
12 Breast tomosynthesis Looks at breast tissue as individual slices instead of all at once Can see lesions missed by conventional mammography fewer callbacks 3D imaging that is cheaper than MRI Becoming standard of care imaging
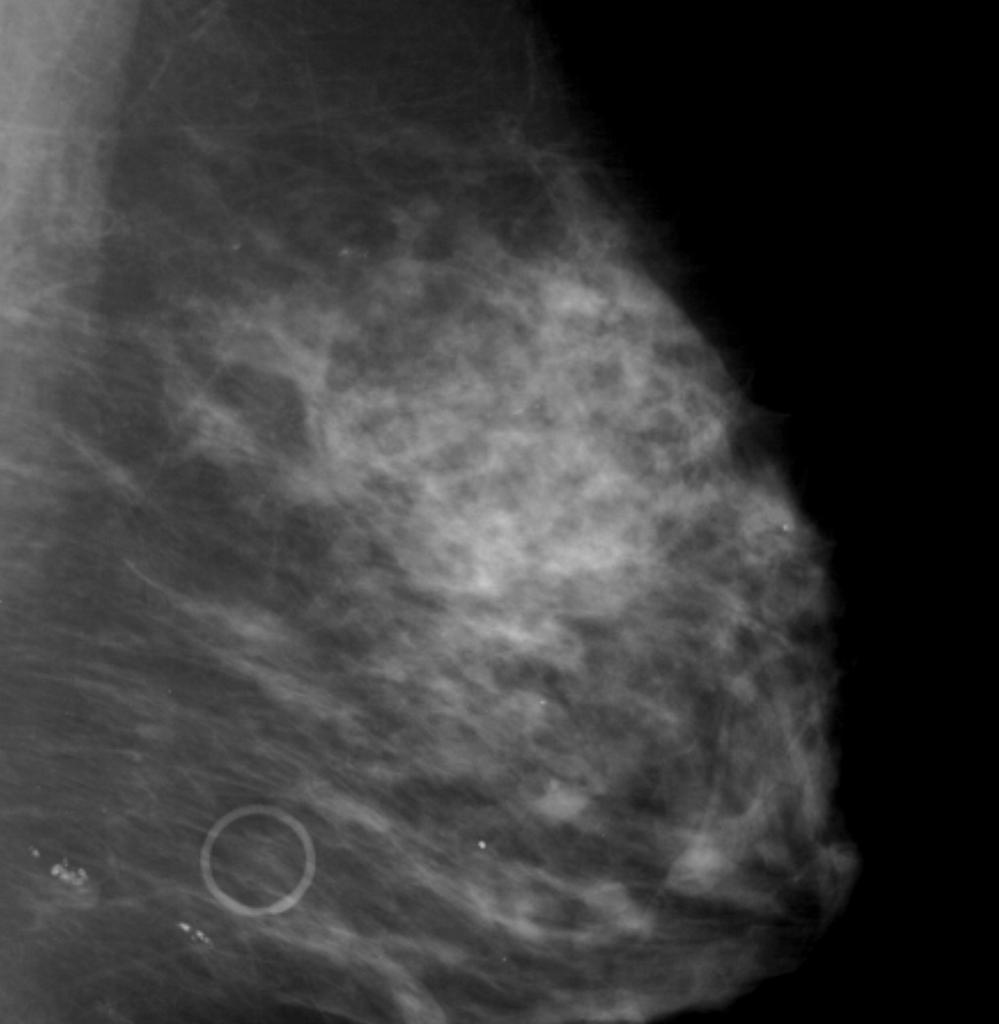
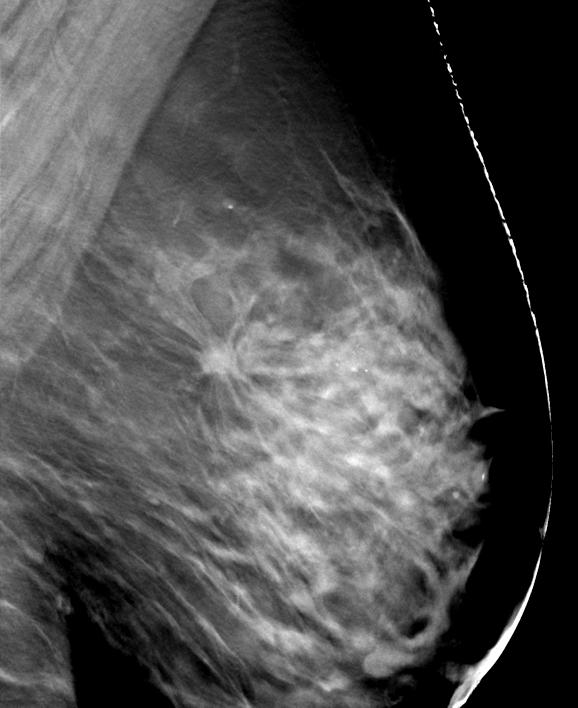
13 CONVENTIONAL MAMMOGRAM TOMOSYNTHESIS SLICE


14 MRI detects some tumors missed by mammography Mammogram MRI
15 Current Indications for Breast MRI To distinguish recurrent tumor from scar tissue following lumpectomy and radiation Additional evaluation of mammogram or ultrasound abnormalities Extent of tumor after diagnosis Assessment of silicone implant rupture Screening high risk women: >20-25% lifetime risk
16 ACS MRI Screening Guidelines Saslow CA: Cancer J Clin 2007;57:75-89 Recommended (based on evidence) BRCA gene mutation untested 1 st degree relatives >20-25% lifetime risk by risk models Recommended (based on expert consensus) chest irradiation ages Li-Fraumeni Syndrome and 1 st degree relatives Cowden, Bannayan-Riley-Ruvalcaba syndromes Insufficient evidence for or against Lifetime risk 15-20%, LCIS, ALH, ADH, prior breast cancer, dense breasts
17 Current issues in breast cancer management Early detection and improved treatment has resulted in many healthy, long term survivors Sequellae of cancer treatment, QOL issues, cost, more important than in past Local and distant recurrence risk continues 10+ years Ongoing risk of new primary cancers
18 Breast Cancer Treatment 2019 Surgery remove bulk of tumor, define stage Mastectomy or lumpectomy Axillary staging Reconstruction, oncoplastic surgery Radiation Treat microscopic residual disease Reduce the extent of surgery Systemic therapy treat metastatic deposits Chemotherapy, endocrine therapy, targeted agents
19 Local Therapies: Surgery and Radiation
20 Mastectomy vs. Lumpectomy: 20-year Data No Difference in Survival NSABP B-06 Milan I Trial


21 Lumpectomy vs. Mastectomy 20 year follow-up: lumpectomy and mastectomy provide equivalent survival Technical improvements in lumpectomy and radiation 10-year local recurrence rates now 2-5% further reduces relative benefit of mastectomy
22 Local recurrence reduces survival Oxford Overview Lancet 2005;366: ,000 patients in 78 trials 75% of local recurrences within 1 st 5 years Increased local recurrence at 5 years = decreased survival at 15 years 4:1 ratio - 1 excess death for each 4 local failures
23 Lumpectomy: Prevent recurrence Oxford Overview: 1 excess death per 4 local recurrences Margins: Negative for invasive, > 2mm for DCIS Radiation with boost Systemic therapy decreases local recurrence Many series <5% local failure at 10 years (40% local failure without radiation) Current results approaching risk of chest wall recurrence after mastectomy



24 Ductal carcinoma in situ DCIS 20-25% of all breast cancer diagnoses 98-99% survival if treated Without treatment, some but not all, progress to invasive breast cancer Time to progression may be long Low grade Intermediate grade High grade
25 DCIS: Local recurrence and survival Mastectomy vs. Lumpectomy Mastectomy: Fowble 1989 Oncology 3:51 Local recurrence <1% Breast cancer mortality 1.7% at 15 years Lumpectomy: NSABP B-17 8-year data Lumpectomy: 26.8% ipsilateral recurrence Lumpectomy + RT: 12.1% ipsilateral recurrence Equivalent survival, 1-2% breast cancer mortality 50% of recurrences after lumpectomy are invasive Use of radiation is debated
26 Surgical options for high risk patients No increase in local failure in BRCA1/2 mutation carriers with breast conservation Higher rate of contralateral new primaries Bilateral mastectomy is an option for treatment and risk reduction in mutation carriers and other high risk patients Prophylactic salpingo-oophorectomy reduces both breast and ovarian cancer risk in BRCA mutation carriers
27 Indications for mastectomy 2017 Tumor large relative to breast size Consider pre-op systemic therapy to shrink tumor Contraindications to radiation New cancer in previously irradiated breast Breast cancer in high risk patient Patient preference
28 Improving cosmetic outcomes after lumpectomy and mastectomy
29 Oncoplastic surgery: Lumpectomies Better Cosmesis for Large lesions Extensive tissue mobilization after lumpectomy to recreate breast contour Addition of mastopexy or reduction mammoplasty to lumpectomy single or 2-stage procedure Cosmetic skin closure
30 Improvements in mastectomy and reconstruction surgery Skin-sparing mastectomy Nipple sparing mastectomy Immediate reconstruction more options Single stage implant reconstructions Muscle sparing autologous tissue flaps

31 Nipple sparing mastectomy: Advantages Superior cosmetic outcome Increases chance of single stage implant reconstruction 6 wks post-op, bilateral mastectomies, single stage implant reconstructions 0-1% nipple/areola recurrence in therapeutic NSM series
32 The anatomy of a safe nipple sparing mastectomy

33 Location of blood vessels relative to nipple ducts: Factor VIII staining Only 1/3 of vessels travel with ducts 2/3 of vessels are in nipple skin Rusby, Brachtel, Taghian, Michaelson, Koerner, Smith. Am J Surg 194:

34 Nipple margin anatomy Subareolar/ nipple duct margin Ductal tissue within nipple Superficial retroareolar tissue Tumor in subareolar/ nipple duct margin requires nipple excision
35 Nipple recurrence rates are low after nipple sparing mastectomy for breast cancer Year N % Local rec # NAC rec Petit Smith F/U mo Benediktsson Vaughan Kim Paepke Jensen Gerber
36 The nipple is just another margin Increasing evidence for oncologic safety of nipple sparing with clear margins Patient selection No direct nipple involvement on exam or imaging Awareness of RT, smoking, age >55, breast >800cc and incision impact on complication rate Careful nipple margin assessment Excision of nipples with positive margins
37 Managing the axilla Treat axillary disease Define stage to guide radiation and medical therapy
38 Staging the axilla: Sentinel Node Biopsy Node status remains a strong prognostic factor Lymphatic drainage is to a specific sentinel node A negative sentinel node predicts with high accuracy that remaining nodes are negative Less morbidity than axillary dissection Lymphedema 1-2% Only rare chronic pain or reduced mobility Axillary dissection: 25% edema/chronic pain Now standard of care for clinically node negative

39 Sentinel node mapping Radioactive and/or blue particles injected near tumor or areola Particles accumulate in 1 st node encountered Sentinel node excised and examined for metastasis
40 Is axillary dissection necessary for a positive sentinel node? ACOS-OG Z eligible patients Lumpectomy and positive sentinel node Whole breast radiation Randomized to axillary dissection or no further axillary surgery Other eligibility criteria: Only 1 or 2 positive nodes No extracapsular extension Systemic therapy
41 Recurrence Z0011 Local-regional Recurrence Giuliano et al Ann Surg 252: ALND (420 pts) SLND (436 pts) Local (Breast) Regional (Axilla, Supraclavicular) Total Locoregional 15 (3.6%) 8 (1.8%) 2 (0.5%) 4 (0.9%) 17 (4.1%) 12 (2.8%) P = 0.11 Median follow-up = 6.3 years

42 Z yr outcomes: axillary dissection vs. SNB+RT in sentinel node+ breast cancer No survival difference with axillary dissection No difference in disease free survival Giuliano JAMA 2017;318:918
43 AMAROS Trial: Radiation vs. dissection 1425 sentinel node (+) patients 10-year follow-up Radiation Dissection p-value Local recurrence 1.82% 0.93% NS Distant disease free survival 78.2% 81.7% NS Overall survival 81.4% 84.6% NS - Included lumpectomies and mastectomies - 3 rd radiation field to axilla SABCS 2018
44 Z0011 and AMAROS Conclusions For clinically node negative patients, 3 or fewer positive sentinel nodes: Routine use of axillary node dissection in this patient population is not justified
45 Post Z0011: Which patients still need axillary dissection? Clinically node positive >3 positive sentinel nodes Gross extranodal tumor extension Residual palpable nodes after SLNB Patients who will not receive radiation and systemic therapy Patients for whom dissection data will change other therapy
46 Why add radiation after lumpectomy? NSABP-B06 trial Lumpectomy alone vs. lumpectomy + radiation In-breast recurrence rates 40% without radiation 3-5% with current radiation
47 Radiation after lumpectomy: More options and lower costs Whole breast irradiation Standard: 25 fractions plus 8 fraction boost Canadian 16 fractions Partial breast irradiation equivalent control External beam twice daily for 5 days External beam once daily for 10 days Brachytherapy catheters 5 days Elderly, ER+ may safely omit radiation
48 Do Women Over 70 Need Radiation? CALGB 9343: 636 women >70 Tumor < 2cm, ER+, clinical N0 All had lumpectomy and tamoxifen Randomized to radiation or no radiation Hughes ASCO 2010
49 Do women over 70 need radiation? CALGB 9343: 12 yr follow-up Hughes ASCO 2010 Tam-RT Tam P-value # patients ns Any local recurrence 2% 9% < Breast recurrence 2% 8% ns Axillary recurrence 0% 1% ns Mastectomy rate 2% 4% ns Distant metastases 7% 5% ns All-cause mortality 39% 37% ns Breast-ca specific death 4% 2% ns
50 Do women over 70 need radiation? CALGB 9343: 12 yr follow-up Hughes ASCO 2010 Tam-RT Tam P-value # patients ns Any local recurrence 2% 9% < Breast recurrence 2% 8% ns Axillary recurrence 0% 1% ns Mastectomy rate 2% 4% ns Distant metastases 7% 5% ns All-cause mortality 39% 37% ns Breast-ca specific death 4% 2% ns
51 Conclusions: For favorable ER+ tumors in women age >70 Radiation decreases locoregional recurrence 2% vs. 9% at 12 years median f/u However, radiation Has no impact on overall, distant disease-free or breast cancer specific survival Has no significant impact on mastectomy rate Does add to morbidity Axillary surgery had no impact on local recurrence or survival
52 Role of radiation after mastectomy Reduces risk of local recurrence by 50-75% Good local control improves survival Benefits patients at high risk for local failure Node positive T3 tumors LVI, young age, close margins
53 Post mastectomy radiation benefit Oxford Overview Lancet 2014;383; women in 22 randomized trials, 10 yr f/u: MRM +/- RT to chest wall and regional nodes Number +nodes N RR overall recurrence ( ) ( ) > ( ) Radiation vs. No Radiation p-value RR breast ca mortality > ( ) ( ) ( ) p-value >
54 Medical Therapies for Breast Cancer
55 Adjuvant Systemic Therapy IV and oral medications given to clinically disease-free patients based on predicted risk of metastatic disease Cytotoxic chemotherapy Endocrine therapy anti-estrogen Targeted therapy drugs and antibodies
56 Who should receive systemic therapy? What is this patient s risk of fatal metastasis? What treatments are available to reduce the risk of metastasis? How much do these treatments reduce risk of relapse? What are the side effects of applicable treatments for this patient?
57 Systemic Therapy: Impact vs. Toxicity Cytotoxic chemotherapy 20-30% reduction in recurrence Greater benefits in selected tumors and patients? Endocrine anti-estrogen therapy 50% reduction in recurrence in hormone receptor positive tumors Anti-HER2 monoclonal antibody therapy 50% reduction in recurrence for sensitive tumors ** All systemic therapies decrease local recurrence



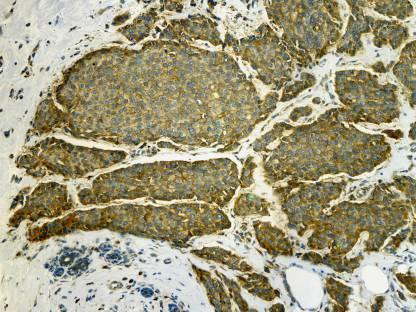
58 Tumor factors guide treatment H&E ER PR Her-2
59 Patient 1 Patient cm node (-) 1.2 cm node (-) ER+ PR+ ER+ PR+ Adjuvant tamoxifen Metastatic disease 3yrs after initiation of tamoxifen Adjuvant tamoxifen Disease free at 12 yrs
60 Prognostic Factors Guide Treatment Classic and standard prognostic factors Tumor size, histologic features, nodal status Estrogen and progesterone receptor HER2 overexpression Newer factors Gene expression profiling of individual tumors For prognosis For response to specific treatments Targeted therapy

61 Gene Expression Subtypes and Clinical Outcome Sorlie et al. PNAS 2003,100:
62 Re-classification of breast cancers: Gene expression profiling 70%: Luminal A, ER+, PR+, HER2-, favorable less aggressive treatment possible 15%: HER2+ - ER+: Luminal B - ER-: HER2+ benefit from anti-her2 therapy - trastuzumab 15%: Basal-like, triple negative : ER-, PR-, HER2- poor prognosis, poor response to current chemotherapy
63 Local and Distant Recurrence Rates by Subtype 799 Breast Conservation Cases Nguyen JCO 26: 2373, 2008 Group Receptors LumA n=599 LumB n=78 HER2+ n=33 Basal n=89 ER/PR+, HER2- ER/PR+, HER2+ ER/PR- /HER2+ ER/PR-, HER2-5-year local failure Adjusted HR (95%CI) p-value 5-yr distant failure Adjusted HR (95%CI) p-value 0.7% Baseline 3.0% Baseline 1.3% NS 11.5% 12.4% 6.8% 6.7 ( ) p= ( ) p= ( ), p= % NS 14.8% 2.1 ( ), p=0.07
64 Which ER+ patients will do well with tamoxifen alone? 30-40% of ER+ cases fail to respond or develop resistance to tamoxifen Patient 1 Patient cm LN- 1.2 cm LN- ER+ PR+ ER+ PR+ Adjuvant tamoxifen Metastatic disease 3yrs after initiation of tamoxifen Adjuvant tamoxifen Disease free at 12 yrs
 derived from weighted sum of expression")
65 OncotypeDx: 21 Gene Assay Recurrence Score (RS) Algorithm Measure expression of genes related to HER2, ER, proliferation, invasion and genes CD68, GSTM1, BAG1 Score (0-100) derived from weighted sum of expression levels
66 Oncotype DX Recurrence Score 21 Gene Assay Measure expression of genes related to HER2, ER, proliferation, invasion and genes CD68, GSTM1, BAG1 Score (0-100) derived from weighted sum of expression levels
67 Who needs chemotherapy? Tailor Rx Trial Rx by Oncotype result 10,253 ER+, HER2- breast cancers Oncotype performed Low risk (0-10) patients (16%) 99% DFS at 5 years without chemo Intermediate risk (11-25) 6907 patients (67%) Randomized: chemo + endocrine vs. endocrine alone No difference in overall or disease free survival at 9yrs Sparano NEJM 2015;373: Sparano NEJM 2018; 379:111-21
68 Who needs chemotherapy? Clinical vs. genomic risk assessment 70-gene assay MINDACT trial Clinical risk and Mammaprint genomic risk assessed Discordant randomized to chemo or no chemo High clinical low genomic Low clinical high genomic Chemo based on clinical risk 95% 5-yr DDFS Chemo based on genomic risk 94.5% 5-yr DDFS with much lower use of chemotherapy Cardosa NEJM :717
69 Improving response to endocrine therapy with CDK inhibition: Palbociclib ER+ breast cancer growth depends on cyclin-dependent kinases (CDK4, CDK6), for G1 to S phase cell cycle progression. Palbociclib - CDK4 and CDK6 inhibitor + endocrine therapy - Improves progression free survival in advanced disease - Some neutropenia, anemia, hair loss Being explored in earlier stage disease Turner N Engl J Med 2015;373:
70 Targeted anti-her2 antibody therapy improves outcomes in HER2+ cancers 15% of breast cancers NSABP B-31 AC-T chemo +/- trastuzumab Dual antibody blockade with trastuzumab + pertuzumab Incremental improvement in outcomes with dual blockade Benefit in metastatic and early stage disease % Free of distant recurrence
71 Triple negative breast cancer (TNBC) Absence of targets for existing medical therapies Estrogen and progesterone receptor negative HER2 negative Poor prognosis Rapid growth High rates of local and systemic recurrence New options? Platinum based chemo, PARP inhibitors, androgen receptor agents
72 Metastatic breast cancer
73 Stage IV breast cancer Stage IV breast cancer survival linked to Pattern and extent of initial metastases Estrogen receptor status Tumor grade Gene expression profile Median survival range months Local disease may progress and become symptomatic while distant disease remains controlled
74 Stage IV breast cancer: Goals of therapy Symptom control with minimal morbidity Slow progression of disease Endocrine Rx rather than chemotherapy for ER+ Targeted therapies anti HER2 antibodies Radiation for symptomatic bone lesions, CNS Surgery reserved for local symptoms
75 Preventing Breast Cancer
76 Prevention: Tamoxifen - 50% Reduction in Breast Cancers - NSABP P-1 Trial Equal risk reduction in: all age groups +/- LCIS all ranges of predicted risk # relatives with breast cancer?greater risk reduction in those with ADH Less efficacy in BRCA1 than BRCA2 carriers
77 NSABP P-1 Trial: Adverse Effects by Age Tamoxifen risks mainly in women over 50 Age < 50 Relative risk Age > 50 Relative risk Endometrial cancer CVA DVT
78 Other endocrine therapy prevention agents Raloxifene extrogen agonist-antagonist 50% reduction in invasive, less reduction in situ Thromboembolic risk, menopausal symptoms No increase endometrial cancer Exemestane aromatase inhibitor 65% risk reduction Menopausal and joint symptoms JAMA :2727 NEJM 364:
79 Limits of Current Prevention Strategies All current prevention agents reduce a fraction of estrogen receptor positive tumors None of the currently available agents reduce the risk of estrogen receptor negative tumors
80 Prophylactic Mastectomy Effective prevention approach 90% reduction in risk Prophylactic BSO reduces risk in premenopausal BRCA Significant psychological and physical impact Increasing use of nipple-sparing mastectomy Careful assessment of magnitude of risk Increasing role for genetic testing prior to prophylactic mastectomy Thorough review of limitations and benefits with patient
81 NSM is safe in BRCA mutation carriers Endorsed by current NCCN guidelines # NSM # pts # pts cancer months f/u # NAC recurrence Jakub 2016 Yao 2015 Manning 2014 Peled 2014 Hartmann

82 Bilateral prophylactic nipple sparing mastectomies BRCA mutation carrier - Pre-op Single stage implant reconstruction 6 weeks post op
83 Breast Cancer 2019 Equivalent outcomes with smaller surgery Lumpectomy, sentinel node biopsy Nipple sparing mastectomy Radiation after lumpectomy, after mastectomy if advanced disease Shorter more focused options for some Medical therapies targeted to tumor subtypes and genomic profile More endocrine therapy, less chemotherapy Anti-HER2 antibody therapy
Breast Cancer. Dr. Andres Wiernik 2017
 Breast Cancer Dr. Andres Wiernik 2017 Agenda: The Facts! (Epidemiology/Risk Factors) Biological Classification/Phenotypes of Breast Cancer Treatment approach Local Systemic Agenda: The Facts! (Epidemiology/Risk
Breast Cancer Dr. Andres Wiernik 2017 Agenda: The Facts! (Epidemiology/Risk Factors) Biological Classification/Phenotypes of Breast Cancer Treatment approach Local Systemic Agenda: The Facts! (Epidemiology/Risk
Breast Cancer. Most common cancer among women in the US. 2nd leading cause of death in women. Mortality rates though have declined
 Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women Mortality rates though have declined 1 in 8 women will develop breast cancer Breast Cancer Breast cancer increases
Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women Mortality rates though have declined 1 in 8 women will develop breast cancer Breast Cancer Breast cancer increases
Breast Cancer. Saima Saeed MD
 Breast Cancer Saima Saeed MD Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women 1 in 8 women will develop breast cancer Incidence/mortality rates have declined Breast
Breast Cancer Saima Saeed MD Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women 1 in 8 women will develop breast cancer Incidence/mortality rates have declined Breast
Breast Cancer Basics. Clinical Oncology for Public Health Professionals. Ben Ho Park, MD, PhD
 This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this
Evolving Practices in Breast Cancer Management
 Evolving Practices in Breast Cancer Management The Georgia Tumor Registrars Association 2016 Priscilla R. Strom, MD, FACS Objectives 1. understand newer indications for neoadjuvant treatment 2. understand
Evolving Practices in Breast Cancer Management The Georgia Tumor Registrars Association 2016 Priscilla R. Strom, MD, FACS Objectives 1. understand newer indications for neoadjuvant treatment 2. understand
Debate Axillary dissection - con. Prof. Dr. Rodica Anghel Institute of Oncology Bucharest
 Debate Axillary dissection - con Prof. Dr. Rodica Anghel Institute of Oncology Bucharest Summer School of Oncology, third edition Updated Oncology 2015: State of the Art News & Challenging Topics Bucharest,
Debate Axillary dissection - con Prof. Dr. Rodica Anghel Institute of Oncology Bucharest Summer School of Oncology, third edition Updated Oncology 2015: State of the Art News & Challenging Topics Bucharest,
Results of the ACOSOG Z0011 Trial
 DCIS and Early Breast Cancer Symposium JUNE 15-17 2012 CAPPADOCIA Results of the ACOSOG Z0011 Trial Kelly K. Hunt, M.D. Professor of Surgery Axillary Node Dissection Staging, Regional control, Survival
DCIS and Early Breast Cancer Symposium JUNE 15-17 2012 CAPPADOCIA Results of the ACOSOG Z0011 Trial Kelly K. Hunt, M.D. Professor of Surgery Axillary Node Dissection Staging, Regional control, Survival
It is a malignancy originating from breast tissue
 59 Breast cancer 1 It is a malignancy originating from breast tissue including both early stages which are potentially curable, and metastatic breast cancer (MBC) which is usually incurable. Most breast
59 Breast cancer 1 It is a malignancy originating from breast tissue including both early stages which are potentially curable, and metastatic breast cancer (MBC) which is usually incurable. Most breast
BREAST CANCER. Dawn Hershman, MD MS. Medicine and Epidemiology Co-Director, Breast Program HICCC Columbia University Medical Center.
 BREAST CANCER Dawn Hershman, MD MS Florence Irving Assistant Professor of Medicine and Epidemiology Co-Director, Breast Program HICCC Columbia University Medical Center Background Breast cancer is the
BREAST CANCER Dawn Hershman, MD MS Florence Irving Assistant Professor of Medicine and Epidemiology Co-Director, Breast Program HICCC Columbia University Medical Center Background Breast cancer is the
4/13/2010. Silverman, Buchanan Breast, 2003
 Tailoring Breast Cancer Treatment: Has Personalized Medicine Arrived? Judith Luce, M.D. San Francisco General Hospital Avon Comprehensive Breast Care Center Outline First, treatment of DCIS Sorting risk
Tailoring Breast Cancer Treatment: Has Personalized Medicine Arrived? Judith Luce, M.D. San Francisco General Hospital Avon Comprehensive Breast Care Center Outline First, treatment of DCIS Sorting risk
8/8/2011. PONDERing the Need to TAILOR Adjuvant Chemotherapy in ER+ Node Positive Breast Cancer. Overview
 Overview PONDERing the Need to TAILOR Adjuvant in ER+ Node Positive Breast Cancer Jennifer K. Litton, M.D. Assistant Professor The University of Texas M. D. Anderson Cancer Center Using multigene assay
Overview PONDERing the Need to TAILOR Adjuvant in ER+ Node Positive Breast Cancer Jennifer K. Litton, M.D. Assistant Professor The University of Texas M. D. Anderson Cancer Center Using multigene assay
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Adjuvant therapy, for early-stage triple-negative breast cancer, 740 742 in older early-stage breast cancer patients, 790 795 anti-her2-directed
Note: Page numbers of article titles are in boldface type. A Adjuvant therapy, for early-stage triple-negative breast cancer, 740 742 in older early-stage breast cancer patients, 790 795 anti-her2-directed
Advances in Breast Surgery. Catherine Campo, D.O. Breast Surgeon Meridian Health System April 17, 2015
 Advances in Breast Surgery Catherine Campo, D.O. Breast Surgeon Meridian Health System April 17, 2015 Objectives Understand the surgical treatment of breast cancer Be able to determine when a lumpectomy
Advances in Breast Surgery Catherine Campo, D.O. Breast Surgeon Meridian Health System April 17, 2015 Objectives Understand the surgical treatment of breast cancer Be able to determine when a lumpectomy
Implications of ACOSOG Z11 for Clinical Practice: Surgical Perspective
 :$;7)#*8'-87*4BCD'E7)F'31$4.$&'G$H'E7)F&'GE'>??ID >?,"'@4,$)4*,#74*8'!74/)$++'74',"$'A.,.)$'7%'()$*+,'!*42$)!7)74*67&'!3 6 August 2011 Implications of ACOSOG Z11 for Clinical
:$;7)#*8'-87*4BCD'E7)F'31$4.$&'G$H'E7)F&'GE'>??ID >?,"'@4,$)4*,#74*8'!74/)$++'74',"$'A.,.)$'7%'()$*+,'!*42$)!7)74*67&'!3 6 August 2011 Implications of ACOSOG Z11 for Clinical
2017 Breast Cancer Update
 2017 Breast Cancer Update Alberto J Montero, M.D., MBA Quality Improvement Officer, Taussig Cancer Institute, Lerner College of Medicine Cleveland Clinic N/A Disclosure Overview Epidemiology (US/Global)
2017 Breast Cancer Update Alberto J Montero, M.D., MBA Quality Improvement Officer, Taussig Cancer Institute, Lerner College of Medicine Cleveland Clinic N/A Disclosure Overview Epidemiology (US/Global)
Assessment of Risk Recurrence: Adjuvant Online, OncotypeDx & Mammaprint
 Assessment of Risk Recurrence: Adjuvant Online, OncotypeDx & Mammaprint William J. Gradishar, MD Professor of Medicine Robert H. Lurie Comprehensive Cancer Center of Northwestern University Classical
Assessment of Risk Recurrence: Adjuvant Online, OncotypeDx & Mammaprint William J. Gradishar, MD Professor of Medicine Robert H. Lurie Comprehensive Cancer Center of Northwestern University Classical
Increased Risk of Breast Cancer: Screening and Prevention. Elizabeth Pritchard, MD 4/5/2017
 Increased Risk of Breast Cancer: Screening and Prevention Elizabeth Pritchard, MD 4/5/2017 No disclosures Defining Risk Risk Factors Modifiable Lifestyle obesity physical activity alcohol consumption breast
Increased Risk of Breast Cancer: Screening and Prevention Elizabeth Pritchard, MD 4/5/2017 No disclosures Defining Risk Risk Factors Modifiable Lifestyle obesity physical activity alcohol consumption breast
Advances in Localized Breast Cancer
 Advances in Localized Breast Cancer Melissa Camp, MD, MPH and Fariba Asrari, MD June 18, 2018 Moderated by Elissa Bantug 1 Advances in Surgery for Breast Cancer Melissa Camp, MD June 18, 2018 2 Historical
Advances in Localized Breast Cancer Melissa Camp, MD, MPH and Fariba Asrari, MD June 18, 2018 Moderated by Elissa Bantug 1 Advances in Surgery for Breast Cancer Melissa Camp, MD June 18, 2018 2 Historical
Prophylactic Mastectomy State of the Art
 Memorial Sloan-Kettering Cancer Center 1275 York Avenue, New York, NY 10065 6 th Brazilian Breast Cancer Conference Sao Paulo, Brazil 9 March 2012 Prophylactic Mastectomy State of the Art Monica Morrow
Memorial Sloan-Kettering Cancer Center 1275 York Avenue, New York, NY 10065 6 th Brazilian Breast Cancer Conference Sao Paulo, Brazil 9 March 2012 Prophylactic Mastectomy State of the Art Monica Morrow
ANNEX 1 OBJECTIVES. At the completion of the training period, the fellow should be able to:
 1 ANNEX 1 OBJECTIVES At the completion of the training period, the fellow should be able to: 1. Breast Surgery Evaluate and manage common benign and malignant breast conditions. Assess the indications
1 ANNEX 1 OBJECTIVES At the completion of the training period, the fellow should be able to: 1. Breast Surgery Evaluate and manage common benign and malignant breast conditions. Assess the indications
Surgery for Breast Cancer
 Surgery for Breast Cancer 1750 Mastectomy - Petit 1894 Radical mastectomy Halsted Extended, Super radical mastectomy 1948 Modified radical mastectomy Patey 1950-60 WLE & RT Baclesse, Mustakallio 1981-85
Surgery for Breast Cancer 1750 Mastectomy - Petit 1894 Radical mastectomy Halsted Extended, Super radical mastectomy 1948 Modified radical mastectomy Patey 1950-60 WLE & RT Baclesse, Mustakallio 1981-85
Classification System
 Classification System A graduate of the Breast Oncology training program should be able to care for all aspects of disease and/or provide comprehensive management. When referring to a discipline of training
Classification System A graduate of the Breast Oncology training program should be able to care for all aspects of disease and/or provide comprehensive management. When referring to a discipline of training
Sentinel Lymph Node Biopsy for Breast Cancer
 Sentinel Lymph Node Biopsy for Breast Cancer Registrar Tutorial Adam Cichowitz Surgical Registrar The Royal Melbourne Hospital Sentinel Lymph Node Biopsy Axillary LN status important prognostic factor
Sentinel Lymph Node Biopsy for Breast Cancer Registrar Tutorial Adam Cichowitz Surgical Registrar The Royal Melbourne Hospital Sentinel Lymph Node Biopsy Axillary LN status important prognostic factor
Breast Cancer. Excess Estrogen Exposure. Alcohol use + Pytoestrogens? Abortion. Infertility treatment?
 Breast Cancer Breast Cancer Excess Estrogen Exposure Nulliparity or late pregnancy + Early menarche + Late menopause + Cystic ovarian disease + External estrogens exposure + Breast Cancer Excess Estrogen
Breast Cancer Breast Cancer Excess Estrogen Exposure Nulliparity or late pregnancy + Early menarche + Late menopause + Cystic ovarian disease + External estrogens exposure + Breast Cancer Excess Estrogen
Principles of breast radiation therapy
 ANZ 1601/BIG 16-02 EXPERT ESMO Preceptorship Program 2017 Principles of breast radiation therapy Boon H Chua Professor Director of Cancer and Haematology Services UNSW Sydney and Prince of Wales Hospital
ANZ 1601/BIG 16-02 EXPERT ESMO Preceptorship Program 2017 Principles of breast radiation therapy Boon H Chua Professor Director of Cancer and Haematology Services UNSW Sydney and Prince of Wales Hospital
The Role of Sentinel Lymph Node Biopsy and Axillary Dissection
 The Role of Sentinel Lymph Node Biopsy and Axillary Dissection Henry Mark Kuerer, MD, PhD, FACS Department of Surgical Oncology University of Texas MD Anderson Cancer Center SLN Biopsy Revolutionized surgical
The Role of Sentinel Lymph Node Biopsy and Axillary Dissection Henry Mark Kuerer, MD, PhD, FACS Department of Surgical Oncology University of Texas MD Anderson Cancer Center SLN Biopsy Revolutionized surgical
Implications of ACOSOG Z11 for Clinical Practice: Surgical Perspective
 Memorial Sloan-Kettering Cancer Center 1275 York Avenue, New York, NY 10065 10th International Congress on the Future of Breast Cancer Coronado, CA 6 August 2011 Implications of ACOSOG Z11 for Clinical
Memorial Sloan-Kettering Cancer Center 1275 York Avenue, New York, NY 10065 10th International Congress on the Future of Breast Cancer Coronado, CA 6 August 2011 Implications of ACOSOG Z11 for Clinical
The Case FOR Oncoplastic Surgery in Small Breasts. Barbara L. Smith, MD, PhD Massachusetts General Hospital Harvard Medical School Boston, MA USA
 The Case FOR Oncoplastic Surgery in Small Breasts Barbara L. Smith, MD, PhD Massachusetts General Hospital Harvard Medical School Boston, MA USA Changing issues in breast cancer management Early detection
The Case FOR Oncoplastic Surgery in Small Breasts Barbara L. Smith, MD, PhD Massachusetts General Hospital Harvard Medical School Boston, MA USA Changing issues in breast cancer management Early detection
So, Who are the appropriate individuals that should consider genetic counseling and genetic testing?
 Hello, I m Banu Arun, Professor of Breast Medical Oncology and Co-Director of Clinical Cancer Genetics at the University of Texas MD Anderson Cancer Center. Today I will be discussing with you Hereditary
Hello, I m Banu Arun, Professor of Breast Medical Oncology and Co-Director of Clinical Cancer Genetics at the University of Texas MD Anderson Cancer Center. Today I will be discussing with you Hereditary
Breast Cancer FAQ. How does Breast Cancer spread? Breast cancer spreads by invading into
 FAQ Breast Cancer What is Breast Cancer? Breast Cancer is the second leading cause of cancer deaths in women today (second to lung cancer) and is the most common cancer among women excluding non-melanoma
FAQ Breast Cancer What is Breast Cancer? Breast Cancer is the second leading cause of cancer deaths in women today (second to lung cancer) and is the most common cancer among women excluding non-melanoma
Breast Cancer Update 2018 The Latest in Diagnosis and Treatment SARATH K, PALAKODETI, DO, FAACS GENERAL, BREAST, AND COSMETIC SURGEON TOLEDO CLINIC
 Breast Cancer Update 2018 The Latest in Diagnosis and Treatment SARATH K, PALAKODETI, DO, FAACS GENERAL, BREAST, AND COSMETIC SURGEON TOLEDO CLINIC Objectives Identify breast lesions and masses, and know
Breast Cancer Update 2018 The Latest in Diagnosis and Treatment SARATH K, PALAKODETI, DO, FAACS GENERAL, BREAST, AND COSMETIC SURGEON TOLEDO CLINIC Objectives Identify breast lesions and masses, and know
OBJECTIVES 8/25/2017. An attempt to organize the chaos
 High Risk for Breast Cancer and Genetics: Who? What? Where? When? An attempt to organize the chaos Presented at Winds of Change Conference November 3, 2017 by Carol Hager, MSN, CRNP and Allison Haener,
High Risk for Breast Cancer and Genetics: Who? What? Where? When? An attempt to organize the chaos Presented at Winds of Change Conference November 3, 2017 by Carol Hager, MSN, CRNP and Allison Haener,
Why Do Axillary Dissection? Nodal Treatment and Survival NSABP B04. Revisiting Axillary Dissection for SN Positive Patients
 Memorial Sloan-Kettering Cancer Center 1275 York Avenue, New York, NY 10065 10th International Congress on the Future of Breast Cancer Coronado, CA Why Do Axillary Dissection? 6 August 2011 Implications
Memorial Sloan-Kettering Cancer Center 1275 York Avenue, New York, NY 10065 10th International Congress on the Future of Breast Cancer Coronado, CA Why Do Axillary Dissection? 6 August 2011 Implications
Management of BRCA Positive Breast Cancer. Archana Ganaraj, MD February 17, 2018 UPDATE ON WOMEN S HEALTH
 Management of BRCA Positive Breast Cancer Archana Ganaraj, MD February 17, 2018 UPDATE ON WOMEN S HEALTH The number of American women who have lost their lives to breast cancer outstrips the total number
Management of BRCA Positive Breast Cancer Archana Ganaraj, MD February 17, 2018 UPDATE ON WOMEN S HEALTH The number of American women who have lost their lives to breast cancer outstrips the total number
BREAST CONSERVATION TREATMENT IN EARLY STAGE DISEASE AND DCIS LAWRENCE J. SOLIN, MD, FACR, FASTRO
 BREAST CONSERVATION TREATMENT IN EARLY STAGE DISEASE AND DCIS LAWRENCE J. SOLIN, MD, FACR, FASTRO Chairman Department of Radiation Oncology Albert Einstein Medical Center Philadelphia, PA Professor (Adjunct)
BREAST CONSERVATION TREATMENT IN EARLY STAGE DISEASE AND DCIS LAWRENCE J. SOLIN, MD, FACR, FASTRO Chairman Department of Radiation Oncology Albert Einstein Medical Center Philadelphia, PA Professor (Adjunct)
PMRT for N1 breast cancer :CONS. Won Park, M.D., Ph.D Department of Radiation Oncology Samsung Medical Center
 PMRT for N1 breast cancer :CONS Won Park, M.D., Ph.D Department of Radiation Oncology Samsung Medical Center DBCG 82 b & c Overgaard et al Radiot Oncol 2007 1152 pln(+), 8 or more nodes removed Systemic
PMRT for N1 breast cancer :CONS Won Park, M.D., Ph.D Department of Radiation Oncology Samsung Medical Center DBCG 82 b & c Overgaard et al Radiot Oncol 2007 1152 pln(+), 8 or more nodes removed Systemic
Rationale For & Design of TAILORx. Joseph A. Sparano, MD Albert Einstein College of Medicine Montefiore-Einstein Cancer Center Bronx, New York
 Rationale For & Design of TAILORx Joseph A. Sparano, MD Albert Einstein College of Medicine Montefiore-Einstein Cancer Center Bronx, New York Declining Breast Cancer Mortality & Event Rates in Adjuvant
Rationale For & Design of TAILORx Joseph A. Sparano, MD Albert Einstein College of Medicine Montefiore-Einstein Cancer Center Bronx, New York Declining Breast Cancer Mortality & Event Rates in Adjuvant
BREAST SURGERY PROGRESS TEST Name:
 General Surgery Residency Program Excellent surgeons BREAST SURGERY PROGRESS TEST Name: Choose the BEST answer for the following questions. 1. All of the following factors are associated with an increased
General Surgery Residency Program Excellent surgeons BREAST SURGERY PROGRESS TEST Name: Choose the BEST answer for the following questions. 1. All of the following factors are associated with an increased
State of the Art in 2000 State of the Art today Gazing forward
 2010 Buschke Lecture: The Relationship between Local Recurrence and Survival in Breast Cancer Jay R. Harris Dana-Farber Cancer Institute (DFCI) Brigham and Women s Hospital (BWH) Harvard Medical School
2010 Buschke Lecture: The Relationship between Local Recurrence and Survival in Breast Cancer Jay R. Harris Dana-Farber Cancer Institute (DFCI) Brigham and Women s Hospital (BWH) Harvard Medical School
Extended Hormonal Therapy
 Extended Hormonal Therapy Dr. Caroline Lohrisch, Medical Oncologist, BC Cancer Agency Vancouver Centre November 1, 2014 www.fpon.ca Optimal Endocrine Therapy for Women with Hormone Receptor Positive Early
Extended Hormonal Therapy Dr. Caroline Lohrisch, Medical Oncologist, BC Cancer Agency Vancouver Centre November 1, 2014 www.fpon.ca Optimal Endocrine Therapy for Women with Hormone Receptor Positive Early
Certified Breast Care Nurse (CBCN ) Test Content Outline (Effective 2018)
 Test Content Outline (Effective 2018)") Certified Breast Care Nurse (CBCN ) Test Content Outline (Effective 2018) I. Coordination of Care - 26% A. Breast health, screening, early detection, risk assessment and reduction 1. Issues related to
Certified Breast Care Nurse (CBCN ) Test Content Outline (Effective 2018) I. Coordination of Care - 26% A. Breast health, screening, early detection, risk assessment and reduction 1. Issues related to
Breast Cancer Imaging
 Breast Cancer Imaging I. Policy University Health Alliance (UHA) will cover breast imaging when such services meet the medical criteria guidelines (subject to limitations and exclusions) indicated below.
Breast Cancer Imaging I. Policy University Health Alliance (UHA) will cover breast imaging when such services meet the medical criteria guidelines (subject to limitations and exclusions) indicated below.
Breast Cancer Pathway Map
 Care Ontario Pathway Map 03.18 Printer Friendly Version Note: print 11x17 landscape for best results, some features and content are only available on web version of pathway map Prevention Screening Diagnosis
Care Ontario Pathway Map 03.18 Printer Friendly Version Note: print 11x17 landscape for best results, some features and content are only available on web version of pathway map Prevention Screening Diagnosis
BREAST CANCER BREAST CANCER
 BREAST CANCER George Raptis, M.D., M.B.A Division of Medical Oncology & Hematology College of Physicians & Surgeons Columbia University BREAST CANCER Epidemiology - Commonest cancer in women - About 235,000
BREAST CANCER George Raptis, M.D., M.B.A Division of Medical Oncology & Hematology College of Physicians & Surgeons Columbia University BREAST CANCER Epidemiology - Commonest cancer in women - About 235,000
38 years old, premenopausal, had L+snbx. Pathology: IDC Gr.II T-1.9cm N+2/4sn ER+100%st, PR+60%st, Her2-neg, KI %
 38 years old, premenopausal, had L+snbx Pathology: IDC Gr.II T-1.9cm N+2/4sn ER+100%st, PR+60%st, Her2-neg, KI67 5-10% Question: What will you do now? 1. Give adjuvant chemotherapy 2. Send for Oncotype
38 years old, premenopausal, had L+snbx Pathology: IDC Gr.II T-1.9cm N+2/4sn ER+100%st, PR+60%st, Her2-neg, KI67 5-10% Question: What will you do now? 1. Give adjuvant chemotherapy 2. Send for Oncotype
Breast Cancer. Breast Cancer. Established breast cancer risk factors. Established breast cancer risk factors. Cancer incidence.
 Breast Cancer A buffet of breast cancer topics Wendy Y. Chen, MD MPH Dana-Farber Cancer Institute Brigham and Women s Hospital Disclosures: none Not related to anything presented in this lecture Wendy
Breast Cancer A buffet of breast cancer topics Wendy Y. Chen, MD MPH Dana-Farber Cancer Institute Brigham and Women s Hospital Disclosures: none Not related to anything presented in this lecture Wendy
Case Scenario 1 History and Physical 3/15/13 Imaging Pathology
 Case Scenario 1 History and Physical 3/15/13 The patient is an 84 year old white female who presented with an abnormal mammogram. The patient has a five year history of refractory anemia with ringed sideroblasts
Case Scenario 1 History and Physical 3/15/13 The patient is an 84 year old white female who presented with an abnormal mammogram. The patient has a five year history of refractory anemia with ringed sideroblasts
Jose A Torres, MD 1/12/2017
 Jose A Torres, MD 1/12/2017 Background Globally leading cause of cancer related death in women ~249,000 Americans diagnosed with invasive breast cancer ~40,890 will die of their disease Breast cancer risk
Jose A Torres, MD 1/12/2017 Background Globally leading cause of cancer related death in women ~249,000 Americans diagnosed with invasive breast cancer ~40,890 will die of their disease Breast cancer risk
When do you need PET/CT or MRI in early breast cancer?
 When do you need PET/CT or MRI in early breast cancer? Elizabeth A. Morris MD FACR Chief, Breast Imaging Service Memorial Sloan-Kettering Cancer Center NY, NY Objectives What is the role of MRI in initial
When do you need PET/CT or MRI in early breast cancer? Elizabeth A. Morris MD FACR Chief, Breast Imaging Service Memorial Sloan-Kettering Cancer Center NY, NY Objectives What is the role of MRI in initial
Invasive Breast Cancer
 Invasive Breast Cancer Eileen Rakovitch MD MSc FRCPC Sunnybrook Health Sciences Centre Medical Director, Louise Temerty Breast Cancer Centre LC Campbell Chair in Breast Cancer Research Associate Professor,
Invasive Breast Cancer Eileen Rakovitch MD MSc FRCPC Sunnybrook Health Sciences Centre Medical Director, Louise Temerty Breast Cancer Centre LC Campbell Chair in Breast Cancer Research Associate Professor,
Evolution of Breast Surgery
 Evolution of Breast Surgery Natasha Rueth MD Surgical Oncologist Piper Breast Center and Alina Health Surgical Specialists Minneapolis, MN Definitions Radical Mastectomy: Removal of breast, chest muscles,
Evolution of Breast Surgery Natasha Rueth MD Surgical Oncologist Piper Breast Center and Alina Health Surgical Specialists Minneapolis, MN Definitions Radical Mastectomy: Removal of breast, chest muscles,
BREAST CONSERVATION TREATMENT IN EARLY STAGE DISEASE AND DCIS LAWRENCE J. SOLIN, MD, FACR, FASTRO
 BREAST CONSERVATION TREATMENT IN EARLY STAGE DISEASE AND DCIS LAWRENCE J. SOLIN, MD, FACR, FASTRO Chairman Department of Radiation Oncology Albert Einstein Healthcare Network Philadelphia, PA Professor
BREAST CONSERVATION TREATMENT IN EARLY STAGE DISEASE AND DCIS LAWRENCE J. SOLIN, MD, FACR, FASTRO Chairman Department of Radiation Oncology Albert Einstein Healthcare Network Philadelphia, PA Professor
Breast Cancer Earlier Disease. Stefan Aebi Luzerner Kantonsspital
 Breast Cancer Earlier Disease Stefan Aebi Luzerner Kantonsspital stefan.aebi@onkologie.ch Switzerland Breast Cancer Earlier Disease Diagnosis and Prognosis Local Therapy Surgery Radiation therapy Adjuvant
Breast Cancer Earlier Disease Stefan Aebi Luzerner Kantonsspital stefan.aebi@onkologie.ch Switzerland Breast Cancer Earlier Disease Diagnosis and Prognosis Local Therapy Surgery Radiation therapy Adjuvant
Breast Cancer? Breast cancer is the most common. What s New in. Janet s Case
 Focus on CME at The University of Calgary What s New in Breast Cancer? Theresa Trotter, MD, FRCPC Breast cancer is the most common malignancy affecting women in Canada, accounting for almost a third of
Focus on CME at The University of Calgary What s New in Breast Cancer? Theresa Trotter, MD, FRCPC Breast cancer is the most common malignancy affecting women in Canada, accounting for almost a third of
Page 1. AHN-JHU Breast Cancer Symposium. Novel Local Regional Clinical Trials. Background. Neoadjuvant Chemotherapy Benefit.
 AHN-JHU Breast Cancer Symposium Novel Local Regional Clinical Trials March 22, 2019 Thomas B. Julian, MD, FACS Associate Medical Director, Cancer Program Development, ANH Cancer Institute Background In
AHN-JHU Breast Cancer Symposium Novel Local Regional Clinical Trials March 22, 2019 Thomas B. Julian, MD, FACS Associate Medical Director, Cancer Program Development, ANH Cancer Institute Background In
Case Scenario 1: This case has been slightly modified from the case presented during the live session to add clarity.
 Case Scenario 1: This case has been slightly modified from the case presented during the live session to add clarity. Background: 46 year old married premenopausal female with dense breasts has noticed
Case Scenario 1: This case has been slightly modified from the case presented during the live session to add clarity. Background: 46 year old married premenopausal female with dense breasts has noticed
16/09/2015. ACOSOG Z011 changing practice. Presentation outline. Nodal mets #1 prognostic tool. Less surgery no change in oncologic outcomes
 ACOSOG Z011 changing practice The end of axillary US/FNA? Preoperative staging of the axilla in the era of Z011 Adena S Scheer MD MSc FRCSC Surgical Oncologist, St. Michael s Hospital Assistant Professor,
ACOSOG Z011 changing practice The end of axillary US/FNA? Preoperative staging of the axilla in the era of Z011 Adena S Scheer MD MSc FRCSC Surgical Oncologist, St. Michael s Hospital Assistant Professor,
Breast cancer staging update. Ekaterini Tsiapali, MD, FACS MedStar Regional Breast Program Site Director
 Breast cancer staging update Ekaterini Tsiapali, MD, FACS MedStar Regional Breast Program Site Director 1 1 Review of the AJCC 8 th edition breast cancer staging Review of genomic assays as stage modifiers
Breast cancer staging update Ekaterini Tsiapali, MD, FACS MedStar Regional Breast Program Site Director 1 1 Review of the AJCC 8 th edition breast cancer staging Review of genomic assays as stage modifiers
Advances in Breast Cancer
 Advances in Breast Cancer Developed in collaboration Learning Objectives Upon completion, participants should be able to: Apply genomic medicine to treatment decisions for patients with HR+/HER2- early
Advances in Breast Cancer Developed in collaboration Learning Objectives Upon completion, participants should be able to: Apply genomic medicine to treatment decisions for patients with HR+/HER2- early
Surgical treatment of BRCA mutated patients. Viviana Galimberti MD European Institute of Oncology Milan, Italy
 Surgical treatment of BRCA mutated patients Viviana Galimberti MD European Institute of Oncology Milan, Italy No pharmaceutical company funding was used I declare I have no conflicts of interest as regards
Surgical treatment of BRCA mutated patients Viviana Galimberti MD European Institute of Oncology Milan, Italy No pharmaceutical company funding was used I declare I have no conflicts of interest as regards
OBJECTIVES CASE 1. Breast Cancer Risk Factors, Genetics, Screening, Diagnosis AGE. Risks of developing breast cancer
 Breast Cancer Risk Factors, Genetics, Screening, Diagnosis Bhuvaneswari Ramaswamy, MD, MRCP Assistant Professor of Internal Medicine Breast Cancer Fellowship Program Director Medical Director of Clinical
Breast Cancer Risk Factors, Genetics, Screening, Diagnosis Bhuvaneswari Ramaswamy, MD, MRCP Assistant Professor of Internal Medicine Breast Cancer Fellowship Program Director Medical Director of Clinical
Excerpts from the American College of Surgeons Educational Courses about Breast Disease:
 1 Excerpts from the American College of Surgeons Educational Courses about Breast Disease: Gynecomastia Gynecomastia is a benign enlargement of the male breast that can be unilateral or bilateral. It typically
1 Excerpts from the American College of Surgeons Educational Courses about Breast Disease: Gynecomastia Gynecomastia is a benign enlargement of the male breast that can be unilateral or bilateral. It typically
Contemporary Classification of Breast Cancer
 Contemporary Classification of Breast Cancer Laura C. Collins, M.D. Vice Chair of Anatomic Pathology Professor of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA Outline
Contemporary Classification of Breast Cancer Laura C. Collins, M.D. Vice Chair of Anatomic Pathology Professor of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA Outline
Conservative Surgery and Radiation Stage I and II Breast Cancer
 Conservative Surgery and Radiation Stage I and II Breast Cancer Variant 1: Premenopausal 41-year-old woman, 1.1-cm GII IDC, upper outer quadrant (UOQ), ER/PR ( ), HER2 ( ), primary excised with lumpectomy,
Conservative Surgery and Radiation Stage I and II Breast Cancer Variant 1: Premenopausal 41-year-old woman, 1.1-cm GII IDC, upper outer quadrant (UOQ), ER/PR ( ), HER2 ( ), primary excised with lumpectomy,
A Slow Starvation: Adjuvant Endocrine Therapy of Breast Cancer
 A Slow Starvation: Adjuvant Endocrine Therapy of Breast Cancer Dr. Susan Ellard Surgical Oncology Update October 24, 2009 Disclosure slide Participant in various meetings or advisory boards sponsored by
A Slow Starvation: Adjuvant Endocrine Therapy of Breast Cancer Dr. Susan Ellard Surgical Oncology Update October 24, 2009 Disclosure slide Participant in various meetings or advisory boards sponsored by
Balancing Evidence and Clinical Practice in the Treatment of Localized Breast Cancer May 5, 2006
 Balancing Evidence and Clinical Practice in the Treatment of Localized Breast Cancer May 5, 2006 Deborah Hamolsky MS, RN : DCIS Carol Franc Buck Breast Care Center UCSF Comprehensive Cancer Center Jane
Balancing Evidence and Clinical Practice in the Treatment of Localized Breast Cancer May 5, 2006 Deborah Hamolsky MS, RN : DCIS Carol Franc Buck Breast Care Center UCSF Comprehensive Cancer Center Jane
Case 1. BREAST CANCER From Diagnosis to Treatment: The Role of Primary Care
 BREAST CANCER From Diagnosis to Treatment: The Role of Primary Care Leah Karliner, MD MAS University of California San Francisco Primary Care Medicine Update 2009 April 2009 Case 1 AR, a 60 year old African
BREAST CANCER From Diagnosis to Treatment: The Role of Primary Care Leah Karliner, MD MAS University of California San Francisco Primary Care Medicine Update 2009 April 2009 Case 1 AR, a 60 year old African
Breast Cancer: Selected Topics for the Primary Care Clinician
 Breast Cancer: Selected Topics for the Primary Care Clinician Leah Karliner, MD MAS October 2009 Primary Care Medicine: Principles and Practice OUTLINE Incidence and Mortality Risk Factors and Risk Reduction/Prevention
Breast Cancer: Selected Topics for the Primary Care Clinician Leah Karliner, MD MAS October 2009 Primary Care Medicine: Principles and Practice OUTLINE Incidence and Mortality Risk Factors and Risk Reduction/Prevention
Radiation and DCIS. The 16 th Annual Conference on A Multidisciplinary Approach to Comprehensive Breast Care and Imaging
 Radiation and DCIS The 16 th Annual Conference on A Multidisciplinary Approach to Comprehensive Breast Care and Imaging Einsley-Marie Janowski, MD, PhD Assistant Professor Department of Radiation Oncology
Radiation and DCIS The 16 th Annual Conference on A Multidisciplinary Approach to Comprehensive Breast Care and Imaging Einsley-Marie Janowski, MD, PhD Assistant Professor Department of Radiation Oncology
Surgical Advances in the Treatment of Breast Cancer. Laura Kruper, MD, MSCE Chief, Breast Surgery
 Surgical Advances in the Treatment of Breast Cancer Laura Kruper, MD, MSCE Chief, Breast Surgery Nothing to disclose DISCLOSURE LESS IS MORE Radiation Lymph nodes Reconstruction Less is More! Radiation
Surgical Advances in the Treatment of Breast Cancer Laura Kruper, MD, MSCE Chief, Breast Surgery Nothing to disclose DISCLOSURE LESS IS MORE Radiation Lymph nodes Reconstruction Less is More! Radiation
Update on New Perspectives in Endocrine-Sensitive Breast Cancer. James R. Waisman, MD
 Update on New Perspectives in Endocrine-Sensitive Breast Cancer James R. Waisman, MD Nothing to disclose DISCLOSURE TAILORx Oncotype Recurrence Score TAILORx Study Design Sparano, J Clin Oncol 2008;26:721-728
Update on New Perspectives in Endocrine-Sensitive Breast Cancer James R. Waisman, MD Nothing to disclose DISCLOSURE TAILORx Oncotype Recurrence Score TAILORx Study Design Sparano, J Clin Oncol 2008;26:721-728
1. Screening, Diagnosis and Surgical Management of Breast Cancer
 1. Screening, Diagnosis and Surgical Management of Breast Cancer Dr Melanie Walker, MBBS, FRACS (Breast Surgeon) Oncoplastic Breast Surgery Combination of optimal cancer surgery with plastic surgical techniques
1. Screening, Diagnosis and Surgical Management of Breast Cancer Dr Melanie Walker, MBBS, FRACS (Breast Surgeon) Oncoplastic Breast Surgery Combination of optimal cancer surgery with plastic surgical techniques
How can we Personalize RT as part of Breast-Conserving Therapy?
 How can we Personalize RT as part of Breast-Conserving Therapy? Jay R. Harris Dana-Farber Cancer Institute (DFCI) Brigham and Women s Hospital (BWH) Harvard Medical School Disclosures I have no COI disclosures
How can we Personalize RT as part of Breast-Conserving Therapy? Jay R. Harris Dana-Farber Cancer Institute (DFCI) Brigham and Women s Hospital (BWH) Harvard Medical School Disclosures I have no COI disclosures
Angela Gilliam, MD University of Colorado Surgical Grand Rounds November 3, 2008
 Angela Gilliam, MD University of Colorado Surgical Grand Rounds November 3, 2008 Breast Cancer Most common cancer in American women 180,000 new cases per year Second most common cause of cancer death 44,000
Angela Gilliam, MD University of Colorado Surgical Grand Rounds November 3, 2008 Breast Cancer Most common cancer in American women 180,000 new cases per year Second most common cause of cancer death 44,000
Educational Goals and Objectives for Rotations on: Breast, Wound and Plastic Surgery
 Educational Goals and Objectives for Rotations on: Breast, Wound and Plastic Surgery Goal The goal of the Breast Surgery rotation is to develop the knowledge, skills and attitudes necessary to evaluate,
Educational Goals and Objectives for Rotations on: Breast, Wound and Plastic Surgery Goal The goal of the Breast Surgery rotation is to develop the knowledge, skills and attitudes necessary to evaluate,
What is Cancer? Petra Ketterl, MD Medical Oncology and Functional Medicine
 What is Cancer? Petra Ketterl, MD Medical Oncology and Functional Medicine What is Cancer? Layman s terms: cancer starts when cells grow out of control (in any place in the body) and crowd out normal cells
What is Cancer? Petra Ketterl, MD Medical Oncology and Functional Medicine What is Cancer? Layman s terms: cancer starts when cells grow out of control (in any place in the body) and crowd out normal cells
Breast Cancer Diagnosis, Treatment and Follow-up
 Breast Cancer Diagnosis, Treatment and Follow-up What is breast cancer? Each of the body s organs, including the breast, is made up of many types of cells. Normally, healthy cells grow and divide to produce
Breast Cancer Diagnosis, Treatment and Follow-up What is breast cancer? Each of the body s organs, including the breast, is made up of many types of cells. Normally, healthy cells grow and divide to produce
ESMO Breast Cancer Preceptorship Singapore November Special Issues in Treatment of Young Women with Breast Cancer
 ESMO Breast Cancer Preceptorship Singapore November 2017 Special Issues in Treatment of Young Women with Breast Cancer Prudence Francis MD Peter MacCallum Cancer Centre Melbourne, Australia Conflict of
ESMO Breast Cancer Preceptorship Singapore November 2017 Special Issues in Treatment of Young Women with Breast Cancer Prudence Francis MD Peter MacCallum Cancer Centre Melbourne, Australia Conflict of
Sesiones interhospitalarias de cáncer de mama. Revisión bibliográfica 4º trimestre 2015
 Sesiones interhospitalarias de cáncer de mama Revisión bibliográfica 4º trimestre 2015 Selected papers Prospective Validation of a 21-Gene Expression Assay in Breast Cancer TAILORx. NEJM 2015 OS for fulvestrant
Sesiones interhospitalarias de cáncer de mama Revisión bibliográfica 4º trimestre 2015 Selected papers Prospective Validation of a 21-Gene Expression Assay in Breast Cancer TAILORx. NEJM 2015 OS for fulvestrant
So much has changed. Breast Cancer Update. Terri Cusick MD FACS
 So much has changed. Breast Cancer Update Terri Cusick MD FACS Disclosure: Myriad Genetics Speakers Beaureau Biggest Changes Nipple sparing mastectomies Chemotherapy decisions based on tumor biology
So much has changed. Breast Cancer Update Terri Cusick MD FACS Disclosure: Myriad Genetics Speakers Beaureau Biggest Changes Nipple sparing mastectomies Chemotherapy decisions based on tumor biology
Ines Buccimazza 16 TH UP CONTROVERSIES AND PROBLEMS IN SURGERY SYMPOSIUM
 BILATERAL MASTECTOMY IS NOT ROUTINELY JUSTIFIED IN PATIENTS WITH BILATERAL AXILLARY LYMPHADENOPATHY AND ONLY ONE DETECTABLE PRIMARY BREAST CANCER LESION SURGERY SYMPOSIUM Ines Buccimazza Breast Unit Department
BILATERAL MASTECTOMY IS NOT ROUTINELY JUSTIFIED IN PATIENTS WITH BILATERAL AXILLARY LYMPHADENOPATHY AND ONLY ONE DETECTABLE PRIMARY BREAST CANCER LESION SURGERY SYMPOSIUM Ines Buccimazza Breast Unit Department
Diseases of the breast (2 of 2) Breast cancer
 Breast cancer") Diseases of the breast (2 of 2) Breast cancer Epidemiology & etiology The most common type of cancer & the 2 nd most common cause of cancer death in women 1 of 8 women in USA Affects 7% of women Peak at
Diseases of the breast (2 of 2) Breast cancer Epidemiology & etiology The most common type of cancer & the 2 nd most common cause of cancer death in women 1 of 8 women in USA Affects 7% of women Peak at
Clinical Trials of Proton Therapy for Breast Cancer. Andrew L. Chang, MD 張維安 Study Chair
 Clinical Trials of Proton Therapy for Breast Cancer Andrew L. Chang, MD 張維安 Study Chair AndrewLChangMD@gmail.com Disclosure Proton Center Development Corporation Scripps San Diego Proton Therapy Center
Clinical Trials of Proton Therapy for Breast Cancer Andrew L. Chang, MD 張維安 Study Chair AndrewLChangMD@gmail.com Disclosure Proton Center Development Corporation Scripps San Diego Proton Therapy Center
BREAST MRI. Elizabeth A. Rafferty, M.D. Avon Comprehensive Breast Center Massachusetts General Hospital Harvard Medical School
 BREAST MRI Elizabeth A. Rafferty, M.D. Avon Comprehensive Breast Center Massachusetts General Hospital Harvard Medical School BREAST MRI Any assessment of the breast parenchyma requires the administration
BREAST MRI Elizabeth A. Rafferty, M.D. Avon Comprehensive Breast Center Massachusetts General Hospital Harvard Medical School BREAST MRI Any assessment of the breast parenchyma requires the administration
Multigene Testing in NCCN Breast Cancer Treatment Guidelines, v1.2011
 Multigene Testing in NCCN Breast Cancer Treatment Guidelines, v1.2011 Robert W. Carlson, M.D. Professor of Medicine Stanford University Chair, NCCN Breast Cancer Treatment Guidelines Panel Selection of
Multigene Testing in NCCN Breast Cancer Treatment Guidelines, v1.2011 Robert W. Carlson, M.D. Professor of Medicine Stanford University Chair, NCCN Breast Cancer Treatment Guidelines Panel Selection of
Hereditary Breast and Ovarian Cancer Rebecca Sutphen, MD, FACMG
 Hereditary Breast and Ovarian Cancer 2015 Rebecca Sutphen, MD, FACMG Among a consecutive series of 11,159 women requesting BRCA testing over one year, 3874 responded to a mailed survey. Most respondents
Hereditary Breast and Ovarian Cancer 2015 Rebecca Sutphen, MD, FACMG Among a consecutive series of 11,159 women requesting BRCA testing over one year, 3874 responded to a mailed survey. Most respondents
The Changing Landscape of Breast Cancer Management and Treatment
 The Changing Landscape of Breast Cancer Management and Treatment Nathalie Johnson, MD, FACS Medical Director of the Legacy Cancer Institute and Breast Health Centers Objectives Review current screening
The Changing Landscape of Breast Cancer Management and Treatment Nathalie Johnson, MD, FACS Medical Director of the Legacy Cancer Institute and Breast Health Centers Objectives Review current screening
Breast Surgery When Less is More and More is Less. E MacIntosh, MD June 6, 2015
 Breast Surgery When Less is More and More is Less E MacIntosh, MD June 6, 2015 Presenter Disclosure Faculty: E. MacIntosh Relationships with commercial interests: None Mitigating Potential Bias Not applicable
Breast Surgery When Less is More and More is Less E MacIntosh, MD June 6, 2015 Presenter Disclosure Faculty: E. MacIntosh Relationships with commercial interests: None Mitigating Potential Bias Not applicable
Genomic Profiling of Tumors and Loco-Regional Recurrence
 1 Genomic Profiling of Tumors and Loco-Regional Recurrence Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program UF Health Cancer Center at Orlando Health Professor of Surgery,
1 Genomic Profiling of Tumors and Loco-Regional Recurrence Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program UF Health Cancer Center at Orlando Health Professor of Surgery,
Follow-up Care of Breast Cancer Patients
 Follow-up Care of Breast Cancer Patients Dr. Simon D. Baxter, MD, FRCPC Medical Oncologist BC Cancer Kelowna Clinical Instructor, Dept of Medicine University of British Columbia 24 November 2018 Disclosures
Follow-up Care of Breast Cancer Patients Dr. Simon D. Baxter, MD, FRCPC Medical Oncologist BC Cancer Kelowna Clinical Instructor, Dept of Medicine University of British Columbia 24 November 2018 Disclosures
Recent Update in Surgery for the Management of Breast Cancer
 Recent Update in Surgery for the Management of Breast Cancer Wonshik Han, MD, PhD Professor, Department of Surgery, Seoul National University College of Medicine Chief of Breast Care Center, Seoul National
Recent Update in Surgery for the Management of Breast Cancer Wonshik Han, MD, PhD Professor, Department of Surgery, Seoul National University College of Medicine Chief of Breast Care Center, Seoul National
Breast Imaging: Multidisciplinary Approach. Madelene Lewis, MD Assistant Professor Associate Program Director Medical University of South Carolina
 Breast Imaging: Multidisciplinary Approach Madelene Lewis, MD Assistant Professor Associate Program Director Medical University of South Carolina No Disclosures Objectives Discuss a multidisciplinary breast
Breast Imaging: Multidisciplinary Approach Madelene Lewis, MD Assistant Professor Associate Program Director Medical University of South Carolina No Disclosures Objectives Discuss a multidisciplinary breast
Molecular Characterization of Breast Cancer: The Clinical Significance
 Molecular Characterization of : The Clinical Significance Shahla Masood, M.D. Professor and Chair Department of Pathology and Laboratory Medicine University of Florida College of Medicine-Jacksonville
Molecular Characterization of : The Clinical Significance Shahla Masood, M.D. Professor and Chair Department of Pathology and Laboratory Medicine University of Florida College of Medicine-Jacksonville
NHOLUA. September 20, 2016 Lincoln, NE
 NHOLUA September 20, 2016 Lincoln, NE UNDERWRITING BREAST CANCER, A NEW APPROACH Dr Robert Lund Basics in Determination of Breast Cancer Prognosis Age at Diagnosis Tumor Size Lymph Node Status Title of
NHOLUA September 20, 2016 Lincoln, NE UNDERWRITING BREAST CANCER, A NEW APPROACH Dr Robert Lund Basics in Determination of Breast Cancer Prognosis Age at Diagnosis Tumor Size Lymph Node Status Title of
Surgical Considerations in Breast Cancer treated with Neoadjuvant Therapy
 Surgical Considerations in Breast Cancer treated with Neoadjuvant Therapy Rebecca Warburton MD Department of Surgery, University of British Columbia Mount Saint Joseph Hospital, Providence Health Care
Surgical Considerations in Breast Cancer treated with Neoadjuvant Therapy Rebecca Warburton MD Department of Surgery, University of British Columbia Mount Saint Joseph Hospital, Providence Health Care
NIPPLE SPARING MASTECTOMY
 NIPPLE SPARING MASTECTOMY 29th Annual Montefiore-Einstein Controversies in Surgery Symposium Virgilio Sacchini, MD Memorial Sloan-Kettering Cancer Center Professor of Clinical Surgery Weill Cornell Medical
NIPPLE SPARING MASTECTOMY 29th Annual Montefiore-Einstein Controversies in Surgery Symposium Virgilio Sacchini, MD Memorial Sloan-Kettering Cancer Center Professor of Clinical Surgery Weill Cornell Medical
Radiotherapy Implications of ACOSOG Z-11 for Clinical Practice. Julia White, MD Professor of Radiation Oncology Medical College of Wisconsin
 1 Radiotherapy Implications of ACOSOG Z-11 for Clinical Practice Julia White, MD Professor of Radiation Oncology Medical College of Wisconsin Disclosures: none Agenda 1. ACOSOG Z-11: Another perspective
1 Radiotherapy Implications of ACOSOG Z-11 for Clinical Practice Julia White, MD Professor of Radiation Oncology Medical College of Wisconsin Disclosures: none Agenda 1. ACOSOG Z-11: Another perspective
HBOC Syndrome A review of BRCA 1/2 testing, Cancer Risk Assessment, Counseling and Beyond.
 HBOC Syndrome A review of BRCA 1/2 testing, Cancer Risk Assessment, Counseling and Beyond. Conni Murphy, ARNP Cancer Risk Assessment and Genetics Program Jupiter Medical Center Learning Objectives Identify
HBOC Syndrome A review of BRCA 1/2 testing, Cancer Risk Assessment, Counseling and Beyond. Conni Murphy, ARNP Cancer Risk Assessment and Genetics Program Jupiter Medical Center Learning Objectives Identify
BREAST MRI. Elizabeth A. Rafferty, M.D. Avon Comprehensive Breast Center Massachusetts General Hospital Harvard Medical School
 BREAST MRI Elizabeth A. Rafferty, M.D. Avon Comprehensive Breast Center Massachusetts General Hospital Harvard Medical School BREAST MRI Any assessment of the breast parenchyma requires the administration
BREAST MRI Elizabeth A. Rafferty, M.D. Avon Comprehensive Breast Center Massachusetts General Hospital Harvard Medical School BREAST MRI Any assessment of the breast parenchyma requires the administration
SYSTEMIC THERAPY OPTIONS FOR BREAST CANCER IN 2014
 SYSTEMIC THERAPY OPTIONS FOR BREAST Oncology Day 2014 CANCER IN 2014 Dr. Katherine Enright, M.D., M.P.H., F.R.C.P.(C) Katherine.enright@Trilliumhealthpartners.ca OBJECTIVES 1. Outline an approach to the
SYSTEMIC THERAPY OPTIONS FOR BREAST Oncology Day 2014 CANCER IN 2014 Dr. Katherine Enright, M.D., M.P.H., F.R.C.P.(C) Katherine.enright@Trilliumhealthpartners.ca OBJECTIVES 1. Outline an approach to the